Fixation of Multifragmentary Patella Fractures Using a ...€¦ · testing on transverse patella...
7
NOVEMBER 2013 | Volume 36 • Number 11 n Feature Article abstract Full article available online at Healio.com/Orthopedics. Search: 20131021-29 Fixation of Multifragmentary Patella Fractures Using a Bilateral Fixed-angle Plate SIMON THELEN, MD; MARCEL BETSCH, MD; JOHANNES SCHNEPPENDAHL, MD; JAN GRASSMANN, MD; MOHSSEN HAKIMI, PHD; CHRISTIAN EICHLER, MD; JOACHIM WINDOLF, PHD; MICHAEL WILD, PHD This biomechanical study is the first to compare 3 fixation methods—bilateral fixed- angle plate, modified anterior tension wiring, and cannulated lag screws with anterior tension wiring—in multifragmentary distal patella fractures. A T-shaped 3-part fracture simulating a multifragmentary articular distal patella fracture (AO/OTA 34-C2.2) was created in 18 human cadaver knee specimens. Three groups were created using homogenous ages and bone mineral densities based on the fixation method received. Repetitive testing over 100 cycles was performed by moving the knee against gravity from 90° flexion to full extension. Failure was defined as fracture displacement greater than 2 mm. In all patellae using fixed-angle plates, an anatomical fracture reduction could be maintained throughout cyclic testing, whereas anterior tension wiring and lag screws with tension wiring showed significant fracture displacement after 100 cycles, with mean fracture gaps of 2.061.3 and 1.961.6 mm, respectively. The differences in fracture gaps between the fixed-angle plate group and the other 2 groups were statistically significant. In both groups using tension wiring, half of the constructs (3 of 6 in each group) failed due to a fracture displacement greater than 2 mm. The bilateral fixed-angle plate was the only fixation method that sustainably stabilized a multifragmentary articular distal patella fracture during cyclic loading when compared with modified anterior tension wiring and cannulated lag screws with anterior tension wiring. The authors are from the Department of Trauma and Hand Surgery (ST, MB, JS, JG, MH, JW), Heinrich Heine University Hospital Düsseldorf, Düsseldorf; the Department of Anatomy II (CE), University of Cologne, Cologne; and the Department of Trauma and Orthopedic Surgery (MW), Klinikum Darmstadt, Darmstadt, Germany. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Marcel Betsch, MD, Department of Trauma and Hand Surgery, Heinrich Heine University Hospital Düsseldorf, Moorenstr 5, D-40225 Düsseldorf, Germany ([email protected]). doi: 10.3928/01477447-20131021-29 Figure: Biomechanical test setup showing a patella specimen fixed with a bilateral fixed-angle plate during tensile loading from 90° flexion to full ex- tension. e1437
-
Upload
nguyenkhanh -
Category
Documents
-
view
228 -
download
2
Transcript of Fixation of Multifragmentary Patella Fractures Using a ...€¦ · testing on transverse patella...

NOVEMBER 2013 | Volume 36 • Number 11
n Feature Article
abstractFull article available online at Healio.com/Orthopedics. Search: 20131021-29
Fixation of Multifragmentary Patella Fractures Using a Bilateral Fixed-angle PlateSimon Thelen, mD; marcel BeTSch, mD; JohanneS SchneppenDahl, mD; Jan GraSSmann, mD; mohSSen hakimi, phD; chriSTian eichler, mD; Joachim WinDolf, phD; michael WilD, phD
This biomechanical study is the first to compare 3 fixation methods—bilateral fixed-angle plate, modified anterior tension wiring, and cannulated lag screws with anterior tension wiring—in multifragmentary distal patella fractures.
A T-shaped 3-part fracture simulating a multifragmentary articular distal patella fracture (AO/OTA 34-C2.2) was created in 18 human cadaver knee specimens. Three groups were created using homogenous ages and bone mineral densities based on the fixation method received. Repetitive testing over 100 cycles was performed by moving the knee against gravity from 90° flexion to full extension. Failure was defined as fracture displacement greater than 2 mm. In all patellae using fixed-angle plates, an anatomical fracture reduction could be maintained throughout cyclic testing, whereas anterior tension wiring and lag screws with tension wiring showed significant fracture displacement after 100 cycles, with mean fracture gaps of 2.061.3 and 1.961.6 mm, respectively. The differences in fracture gaps between the fixed-angle plate group and the other 2 groups were statistically significant. In both groups using tension wiring, half of the constructs (3 of 6 in each group) failed due to a fracture displacement greater than 2 mm. The bilateral fixed-angle plate was the only fixation method that sustainably stabilized a multifragmentary articular distal patella fracture during cyclic loading when compared with modified anterior tension wiring and cannulated lag screws with anterior tension wiring.
The authors are from the Department of Trauma and Hand Surgery (ST, MB, JS, JG, MH, JW), Heinrich Heine University Hospital Düsseldorf, Düsseldorf; the Department of Anatomy II (CE), University of Cologne, Cologne; and the Department of Trauma and Orthopedic Surgery (MW), Klinikum Darmstadt, Darmstadt, Germany.
The authors have no relevant financial relationships to disclose.Correspondence should be addressed to: Marcel Betsch, MD, Department of Trauma and Hand
Surgery, Heinrich Heine University Hospital Düsseldorf, Moorenstr 5, D-40225 Düsseldorf, Germany ([email protected]).
doi: 10.3928/01477447-20131021-29
Figure: Biomechanical test setup showing a patella specimen fixed with a bilateral fixed-angle plate during tensile loading from 90° flexion to full ex-tension.
e1437

ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
With a reported prevalence of ap-proximately 1% of all human fractures,1-3 patella fractures
often present with a heterogeneous frac-ture pattern. The transverse 2-part frac-ture is the most common type, account-ing for 34% of all fractures, followed by multifragmentary distal patella fractures.2 Surgical treatment of patellar fractures is indicated in fractures with greater than 2 to 3 mm of displacement or articular in-congruity and if the extensor mechanism is disrupted.2,4 Despite partially unsatis-factory long-term study results,1,5-8 modi-fied anterior tension wiring with a vertical figure-of-eight pattern remains the most widely accepted procedure for the fixa-tion of patellar fractures,9-11 followed by the combination of cannulated lag screws with tension band wiring.3,4,12,13
Although recent biomechanical studies have investigated different osteosynthe-ses in simple transverse patella fractures, the current study is the first to biome-chanically evaluate different fixation tech-niques for a 3-part fracture involving the articular surface of the distal part of the patella, which is the second most frequent fracture site.2 A bilateral fixed-angle plate specifically designed and developed for the stabilization of patellar fractures was compared with modified anterior tension wiring with K-wires and cannulated lag screws with anterior tension wiring. It was hypothesized that a bilateral fixed-angle plate, which demonstrated superior strength and sustainability in preliminary testing on transverse patella fracture types,14-16 would also be able to retain the reduction of a more fragmentary fracture pattern superior to the current standard techniques.
Materials and MethodsEighteen knees were chosen from 76
human cadaveric specimens that were pre-served in formalin-based dilution for less than 6 months. Those with radiographic alterations, such as precedent fractures, orthopedic implants, or advanced retropa-
tellar arthritis, were excluded, and speci-mens of similar age and bone mineral density (BMD) were identified. Average cadaver age was 74.666.4 years (range, 61-87 years), and specimens included 6 women and 12 men. Bone mineral density was measured using a peripheral quantita-tive computed tomography (pqCT) scan-ner (XCT 3000; Stratec Medizintechnik, Pforzheim, Germany). Scans were per-formed at the previously marked trans-verse osteotomy line in the center of each patella. Mean BMD of the specimens, in-cluding cortical and cancellous bone sub-stance of the patellae, was 483.9623.2 mg/cm3. The selected specimens were di-vided into 3 groups of 6 specimens based on the type of internal fixation method each patella received. Age and BMD were distributed homogenously to minimize their influence on the results (Table 1).
The knees were dissected of soft tissue, leaving the knee joint capsule, ligaments, and extensor mechanism (including the medial and lateral retinaculum) intact. An articular T-shaped 3-part fracture (AO/OTA 34-C2.2) was created using an oscil-lating saw and osteotome by first horizon-tally osteotomizing the patellae in the pre-viously marked center and consecutively by dividing the inferior part vertically into 2 halves. Subsequently, all fractures were anatomically reduced and stabilized according to their predetermined type of osteosynthesis.
The modified anterior tension wire technique featured 2 parallel 2-mm stain-
less steel K-wires and a 1.25-mm stain-less steel wire loop forming a figure-of-eight on the anterior patella surface. The wire was twisted manually until it straightened, achieving a stable osteo-synthesis with anatomic reduction of the fracture gap. The cannulated lag screws with anterior tension wiring technique used 2 parallel cannulated lag screws (di-ameter, 4.0 mm; length, 36 mm; thread, 12 mm) (Synthes, Oberdorf, Switzer-land) that were inserted over previously placed parallel K-wires before passing a 1.25-mm stainless steel wire through them and forming a figure-of-eight on the anterior patella surface. This was fol-lowed by tightening the tension band by twisting the 1.25-mm wire ends until a stable, anatomically reduced osteosyn-thesis was obtained. The bilateral fixed-angle plate technique used a 2.7-mm titanium fixed-angle plate (Königsee Implantate, Allendorf, Germany), which features 5 holes on either side, with each allowing for polyaxial fixed-angle screw placement (Figure 1). Both branches of the plate were bent in a semicircular shape and placed on the medial and lat-eral edge of the patellae in an 80° angle to its anterior surface, sparing the inser-tion of the quadriceps and patella tendon. The reduced fracture was stabilized by attaching the plate to the patella with four 3.5-mm angle-stable locking screws on each side.
The testing protocol for all techniques was set up to simulate knee joint motion
Table 1
Specimen Age and Bone Mineral Density
Mean6SD
VariableModified Anterior
Tension WiringLag Screws1Tension
Wiring Fixed-angle Plate
Age, y 76.0611.1 77.065.2 73.062.4
BMD, mg/cm³ 473.8630.6 483.9625.6 484.3622.4
Abbreviation: BMD, bone mineral density.
e1438

NOVEMBER 2013 | Volume 36 • Number 11
Fixation oF MultiFragMentary Patella Fractures using a Bilateral Fixed-angle Plate | thelen et al
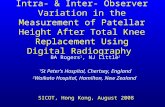
against gravity from 90° flexion to full ex-tension. The distal femur was fixed hori-zontally on the base of a load frame. Ten-sion was applied by seizing the proximal end of the quadriceps tendon into a metal clamp that was connected to the crossbar of a dynamic material testing machine (Model 5565; Instron Ltd, High Wy-combe, United Kingdom) with a braided steel cable that was vertically deflected by a pulley (Figure 1). According to similar reports, the weight of the lower leg was simulated by a 3.2-kg iron disk floating along the axis of the tibia 25 cm below the distal patellar pole.3,17
All patellae were cyclically tested by simulating knee joint motion from 90° flexion to full extension (0°) by pulling the quadriceps tendon (Figure 1). A pre-defined tensile load was not applied. In-stead, to ensure the desired range of mo-tion was achieved, an initial calibrating cycle from 90° flexion to full extension was performed to define the individually required travel distance of the load frame, which was then adopted as the main pa-rameter in each test cycle. In addition, the calibration cycle permitted measur-ing of the fracture gap after the first cycle. Each specimen underwent 100 cycles at a constant velocity of the load frame of 25 mm per minute until full extension was
reached. Failure was defined as widening of the fracture gap more than 2 mm. The fracture gap was measured at the medial and lateral border of the transverse osteot-omy line using a digital calliper. Measure-ments were conducted before and after the initial calibration cycle and after the last testing cycle. The original fracture gap be-fore testing was 0 mm for all specimens, indicating successful anatomic reduction.
For specimens that did not fail during cyclic testing (ie, those with a fracture gap of more than 2.0 mm), a destructive load-ing to failure followed. On the basis of the destructive test setup of a preceding study,16 load to failure was applied by increasing the tensile loads on the tendons of the dissected patellae. A 60° knee flexion angle was sim-ulated using an artificial femur condyle as a pivot point. Osteosynthesis failure in the destructive set-up was determined by a sud-den load decrease of more than 20% in the load-displacement diagram.
The statistical interpretation included an analysis of variance for independent variables, which was conducted for frac-ture gap widening of the 3 groups. A post-hoc t test followed subsequently if overall differences between the groups could be observed. Statistical boundaries were a confidence interval of 95% and a signifi-cance level of P value less than .05.
resultsTo achieve the required range of mo-
tion, each test cycle was controlled by the crossbar’s travel distance required to simulate knee joint range of motion from 90° flexion to full extension. The load measured to reach full extension during the calibration cycle was averaged over the 6 constructs of each group, resulting in a mean tensile load for each group. These mean tensile loads did not differ signifi-cantly between the groups during cyclic testing (P..3) (Table 2, Figure 2).
All 18 specimens withstood 100 cycles of tensile loading without implant cut-out or fracture. The fracture gaps after testing were compared with the values of the ana-tomically reduced fracture site before the first cycle.
Modified Anterior Tension WireA slightly widened fracture gap (mean,
0.960.6 mm) was found at a mean tensile load of 216.3636.9 N in 5 of 6 specimens after the first cycle. Mean fracture gap measurement after 100 cycles was 2.061.3 mm (Table 2). Three of 6 specimens failed due to fracture gap widening of more than 2 mm, whereas the other 3 specimens went on to destructive testing. Mean load at failure was 10916358 N (range, 744 to 1449 N).
Cannulated Lag Screws With Additional Anterior Tension Wiring
A mean tensile load of 256.7686.8 N was required to bring the 6 patellae from 90° flexion to full extension against gravity. Mean fracture gap measurement after the initial cycle was 0.760.8 mm. After 100 cycles, mean fracture gap measurements were 1.961.6 mm (Table 2; Figure 3). Three of 6 specimens in this group displayed a fracture gap ex-ceeding 2.0 mm after 100 cycles, which was regarded as fixation failure. The other 3 specimens were loaded until de-structive failure, reaching a mean load at failure of 768.36170.4 N (range, 584 to 920 N).
Figure 1: Biomechanical test-setup showing a patella specimen fixed with a bilateral fixed-angle plate during tensile loading from 90° flexion to full extension. The anatomically reduced T-shaped fracture (AO/OTA 34-C2.2) was stabilized by attaching the plate to the patella with four 3.5-mm angle-stable locking screws on each side. Each distal fragment is held by 2 screws. The hole overly-ing the vertical fracture gap of the inferior pole was spared. Note that the retinacula were left intact in all specimens.
1
e1439

ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
Fixed-angle PlateThe specimens in the fixed-angle plate
group showed distinguished characteris-tics compared with the above mentioned groups because all 6 maintained an ana-tomically reduced fracture gap of 0.0 mm throughout all 100 cycles of non-destructive testing (Table 2, Figure 3). The mean load required for the demanded range of motion was 242.0674.0 N and did not differ significantly from the other two groups (Table 2 and Figure 2). Since none of the patellae with fixed-angle plate osteosynthesis failed during 100 cycles, a destructive loading to failure followed for all 6 specimens. Here, a mean tensile load of 1214.76616.2 N (range, 623 N to 1909 N) was determined before it came to a sudden decrease in the load-displacement diagram indicating failure of the osteo-synthesis.
Direct comparison of the 3 fixation methods after 100 repetitive cycles of nondestructive loading revealed that the fixed-angle plate resulted in significantly less fracture gap widening than modi-fied anterior tension wiring (P,.01) and lag screws with tension wiring (P,.05) (Table 2, Figure 3). After the initial cali-bration cycle, no fracture displacement could be observed in the fixed-angle plate group compared with the 2 groups using the tension wire principle; however, these differences after the first load cycle were not significant (P..05) (Table 2). No sig-nificant difference in fracture dehiscence after 100 cycles could be found between the combination of lag screws plus tension wiring and anterior tension wiring alone (Table 2, Figure 3). Concerning the sub-sequent destructive loading, no statements about significances can be made because only 3 specimens in the modified tension wiring and 3 in the screw plus tension wir-ing group were tested to failure compared with all 6 specimens of the fixed-angle plate group. Still, fixed-angle plates failed at the highest mean loads (1214.76616.2 N) in comparison to the other techniques (Table 2).
discussionThe surgical goals in the treatment of
displaced patella fractures are analogous to other intra-articular fractures: accurate (step- and gapless) reduction with stable fixation of the articular surface, allowing for early postoperative motion.1,2,18 In the current study, the fixed-angle plate was the only device to completely and perma-nently retain an anatomic fracture reduc-tion throughout cyclic testing at nonde-structive loads, affirming the hypothesis stated at the outset. Fixation with the other compared techniques resulted in an aver-age fracture dehiscence of 2.061.3 mm for modified tension wiring or 1.961.6 mm for cannulated lag screws with ante-rior tension wiring. Such a displacement after 100 cycles of isometric motion of the flexed knee against gravity has to be regarded as unsatisfactory, given that a fracture gap of more than 2.0 mm is com-monly regarded as an indication for opera-tive treatment of the patella.4,6,18 However, these findings may explain the relatively high number of unsatisfactory clinical re-
sults, which may be representative of the common adverse effects of tension band wiring, such as failure of fixation, wire migration, and persisting postoperative pain resulting in revision surgery with hardware removal in up to 65% of pa-tients.2,5,7,8,19,20
Given the fairly poor outcome of ten-sion band wiring, other authors have in-vestigated methods to improve fixation of patella fractures.3,9-11,17,21-23 The combina-tion of cannulated lag screws with anterior tension wiring became an increasingly popular alternative12,13,24 after proving higher load-bearing capacity in biome-chanical studies.3,9 However, currently, all biomechanical studies were conducted using a relatively stable transverse 2-part fracture (AO/OTA 34-C1), which admit-tedly is the most common fracture type. On the other hand, it only contributes to one-third of all fractures of the patella.2 In transverse fractures, the most common fixation techniques—modified anterior tension wiring and cannulated lag screws with anterior tension wiring—provide
Table 2
Results
Mean6SD
VariableModified Anterior
Tension WiringLag Screws1
Tension WiringFixed-angle
Plate
Mean cyclic tensile load, N 216.3636.9a 256.7682.8a 242.0674.0a
Fracture gap before first cycle, mm
0.0 0.0 0.0
Fracture gap after first cycle, mm
0.960.6b 0.760.8b 0.0b
Fracture gap after 100 cycles, mm
2.061.3c,d 1.961.6c,e 0.0d,e
Mean destructive load at failure, N
10916358f 7686170f 12156616f
aNo significant difference in mean tensile loads in all groups (P>.3). bNo significant difference after first cycle between any groups (P>.05). cNo significant difference after 100 cycles between tension wiring vs screws1tension wiring (P>.9). dSignificant differences after 100 cycles between tension wiring vs fixed-angle plate (P<.01). eSignificant differences after 100 cycles between screws1tension wiring vs fixed-angle plate (P<.05). fNo testing for significant differences of failure loads possible due to uneven sample sizes.
e1440

NOVEMBER 2013 | Volume 36 • Number 11
Fixation oF MultiFragMentary Patella Fractures using a Bilateral Fixed-angle Plate | thelen et al
sufficient stability in different in vitro in-vestigations.3,9,11,21,22 The comparatively unsatisfying clinical results with failure of fixation of these osteosyntheses might be attributed to less stable multifragmen-tary fracture situations occurring in vivo. Therefore, a multifragmentary articu-lar fracture pattern (AO/OTA 34-C2.2) was created to evaluate the behavior of the current standard techniques in an in-creasingly unstable situation compared with the new bilateral fixed-angle plate
that already displayed superior mechani-cal characteristics in a simple transverse 2-part fracture (AO/OTA 34-C1.1).14-16
Although the insufficient fracture reten-tion of the tension wire group during cy-clic testing at subultimate loads might be explained by the initial tightening of the wire formation with consecutive fracture dehiscence, it might appear surprising that the combination of cannulated lag screws and tension wiring has likewise underper-formed. Conceivably, the cannulated lag
screws may have forfeited some of their compression force because, in the reduced bone quality of the aged cadaver specimens, the screw threads could not be anchored as firmly. Consequently, the lag screws may have acted more like a tension band con-struct. However, this problem is not owed solely to this in vitro test setup with aged and embalmed cadaver specimens. In a clinical setting (ie, when operating on live human specimens), it is arguable whether the initial compression of the lag screws can be maintained throughout the process of fracture consolidation. Micromotion at the screw-bone-interface during the post-operative rehabilitation phase might pro-mote loosening of the screw threads in the predominantly cancellous bone structure of the patella. Another possible explanation may be the relatively small size of the dis-tal fragments in this fracture model. This would confirm literature recommendations for the use of cannulated lag screws with tension wiring only in centered transverse patellar fractures.9,13 In contrast, the en-tirely undisplaced fracture gap of 0.0 mm throughout all test cycles displayed by the fixed-angle plate system underlines that the angle-stable interface of threaded screw heads and plate holes prevents loosening of the osteosynthesis with consecutive frac-ture displacement at nondestructive loads.
A limitation of the current study, as found in all biomechanical studies, is the restricted reproduction of the complex procedures occurring in vivo. The current study setup aimed to reproduce the com-plex loading pattern at the patella by sim-ulating quasi-active knee range of motion, allowing for not only mere tensile forces through the quadriceps and patellar ten-don, but also compressive forces along the posterior facet of the patella. Contrary to comparable biomechanical studies where a predefined load was applied to simulate knee motion from 90° flexion to full ex-tension,3,17,21,25 in the current study a test procedure was performed that assured full range of motion for each specimen to better reflect the individual anatomic con-
Figure 2: Mean ten-sile load (N) with standard deviation during cyclic non-destructive testing. No statistical differ-ence was found be-tween the 3 groups.
2
Figure 3: Mean frac-ture gap (mm) after 100 cycles. No sig-nificant difference between tension wire vs cannulated screws plus tension wire. *Significant difference (P,.01) between tension wire vs fixed-angle plate. **Significant difference (P,.05) between screw plus tension wire vs fixed-angle plate.
3
e1441

ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
ditions and physiologic circumstances. Mean loads applied for cyclic tensile test-ing in the current study all ranged around 250 N (Table 2), which is only slightly inferior to comparable experiments with predefined loads of mostly 300 N.17,25,26 The number of loading cycles in such a setup simulating repetitive motion of the knee joint against gravity may be a subject of discussion. Obviously, in the first 8 to 12 weeks of postoperative rehabilitation until fracture consolidation, an average patient would have to perform approxi-mately 100,000 cycles of flexion and ex-tension,2,27 which is impossible to repro-ducibly simulate in such a cadaver setup.
In the current study, 100 cycles from 90° flexion to full extension were executed, not in an attempt to simulate fatigue test-ing, but rather to register early fracture de-hiscence at loads below 300 N as a sign of failure of fixation. Loads of approximately 300 N can be considered physiological in the context of early postoperative rehabili-tation because forces acting on the patella during active extension of the knee against gravity match this value.28-30 The results of previous testing on synthetic patellae over 10,000 cycles depicted the most sig-nificant fracture dislocation to occur during the initial 100 cycles, after which a steady state was reached without further notable alterations.14 Working with human cadav-eric specimens naturally means working with aged specimens, such as those with a mean age of 74.666.4 years in the current study. It can be argued that patella fractures in vivo peak between 20 to 50 years.2,31 On the other hand, if a fixation device, such as a fixed-angle plate, is capable of securely stabilizing these unstable fractures, even in older specimens with reduced bone quality, it might add to its potential in younger and better bone stock.
To reduce potential bias of embalmed specimens of older donors, emphasis was placed on forming groups of specimens with homogeneous ages, sexes, and bone mineral densities by selecting from an exceptionally large pool of cadaver speci-
mens (76 in total) and by way of pqCT screening (Table 1). Thus, the adverse ef-fect of working with formalin-embalmed specimens32 might have been diminished or compensated. Furthermore, some data indicate that differences in the mechani-cal properties of frozen and embalmed bone are nonsignificant, suggesting either use in biomechanical studies.33 Concern-ing the simulated fracture pattern, the authors were aware of the fact that most multifragmentary fractures occurring in vivo involve extensive comminution of the patella. Creating a reproducible and comparable comminuted fracture pattern in vitro appeared to be hardly possible. Therefore, it was decided to create a trans-verse articular component together with a vertical split of the inferior pole resulting in a T-shaped fracture situation (AO/OTA 34-C2.2). Even if this exact fracture type is not the most common type, in the au-thors’ experience and according to litera-ture,2 the above mentioned fracture com-ponents (transverse and inferior pole) are those occurring most frequently in vivo. A completely extra-articular distal pole fracture was not simulated because small distal fragments cannot be addressed by modified tension wiring, cannulated lag screws, or fixed-angle plates.
In the current study, destructive ten-sile loading occurred for those speci-mens that did not fail during cyclic test-ing. All 6 specimens of the fixed-angle plate group went on to failure loading, where they exhibited the highest mean (1214.76616.2 N) and absolute (maxi-mum, 1909 N) load values, whereas half of the specimens in each of the other 2 groups had to be excluded before testing for failure loading. Therefore, evaluat-ing the results comparatively or using significance testing was inapplicable, particularly given the widespread load-to-failure values throughout the groups (Table 2). However, even supposing the minimum failure value of the fixed-angle plate (623 N) underlines its capacity to resist distinctively higher tensile loads
than the 300 N required for extension of the lower leg against gravity.28,34,35
Although not investigated in the cur-rent study, an important clinical aspect in the fixation of patellar fractures, apart from fixation stability, is its influence on patellar blood supply. Arterial blood sup-ply of the patella composes an extraosse-ous anastomotic ring running along the lateral margins of the patella, which might be jeopardized by circumferential ap-plication of fixation devices.36 Arguably, the fixed-angle plate might pose a risk to patellar perfusion due to its application at the medial and lateral margin of the pa-tella. Otherwise, due to its internal fixator principle, only punctual contact is made between the plate and bone, so the perios-teal blood supply might be mostly spared. In addition, the equally important intraos-seous arterial pattern, which enters the patella on its anterior surface and at the distal pole,36 is not affected by placement of the fixed-angle plate compared with anterior tension wiring, which requires di-rect and firm bony contact independent of the use of cannulated screws or K-wires. However, future clinical studies are neces-sary to investigate the outcome of fixed-angle plate osteosynthesis in patella frac-tures, including its potential influence on blood supply.
conclusionIn a bone density–matched human ca-
daveric model imitating a multifragmen-tary distal patella fracture (AO/OTA 34-C2.2), the fixed-angle plate was the only device to sustainably retain anatomic frac-ture reduction under cyclic loading at non-destructive loads. Both techniques of modified anterior tension wiring and can-nulated lag screws with anterior tension wiring displayed significantly more frac-ture dehiscence in this multifragmentary fracture pattern.
references 1. Bostman O, Kiviluoto O, Santavirta S, Nir-
hamo J, Wilppula E. Fractures of the patella
e1442

NOVEMBER 2013 | Volume 36 • Number 11
Fixation oF MultiFragMentary Patella Fractures using a Bilateral Fixed-angle Plate | thelen et al
treated by operation. Arch Orthop Trauma Surg. 1983; 102(2):78-81.
2. Bostrom A. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl. 1972; 143:1-80.
3. Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma. 1997; 11(5):351-356.
4. Melvin JS, Mehta S. Patellar fractures in adults. J Am Acad Orthop Surg. 2011; 19(4):198-207.
5. Gosal HS, Singh P, Field RE. Clinical experi-ence of patellar fracture fixation using metal wire or non-absorbable polyester—a study of 37 cases. Injury. 2001; 32(2):129-135.
6. Lebrun CT, Langford JR, Sagi HC. Functional outcomes after operatively treated patella frac-tures. J Orthop Trauma. 2012; 26(7):422-426.
7. Miller MA, Liu W, Zurakowski D, Smith RM, Harris MB, Vrahas MS. Factors predict-ing failure of patella fixation. J Trauma Acute Care Surg. 2012; 72(4):1051-1055.
8. Dy CJ, Little MT, Berkes MB, et al. Meta-analysis of re-operation, nonunion, and infec-tion after open reduction and internal fixation of patella fractures. J Trauma Acute Care Surg. 2012; 73(4):928-932.
9. Benjamin J, Bried J, Dohm M, McMurtry M. Biomechanical evaluation of various forms of fixation of transverse patellar fractures. J Orthop Trauma. 1987; 1(3):219-222.
10. Burvant JG, Thomas KA, Alexander R, Har-ris MB. Evaluation of methods of internal fixation of transverse patella fractures: a bio-mechanical study. J Orthop Trauma. 1994; 8(2):147-153.
11. Curtis MJ. Internal fixation for fractures of the patella. A comparison of two methods. J Bone Joint Surg Br. 1990; 72(2):280-282.
12. Qi L, Chang C, Xin T, et al. Double fixation of displaced patella fractures using bioab-sorbable cannulated lag screws and braided polyester suture tension bands. Injury. 2011; 42(10):1116-1120.
13. Berg EE. Open reduction internal fixation of displaced transverse patella fractures with figure-eight wiring through parallel cannu-lated compression screws. J Orthop Trauma. 1997; 11(8):573-576.
14. Thelen S, Schneppendahl J, Baumgartner R, et al. Cyclic long-term loading of a bilateral fixed-angle plate in comparison with ten-sion band wiring with K-wires or cannulated screws in transverse patella fractures. Knee Surg Sports Traumatol Arthrosc. 2012; 21(2): 311-317.
15. Thelen S, Schneppendahl J, Jopen E, et al. Biomechanical cadaver testing of a fixed-an-gle plate in comparison to tension wiring and screw fixation in transverse patella fractures. Injury. 2012; 43(8):1290-1295.
16. Wild M, Eichler C, Thelen S, Jungbluth P, Windolf J, Hakimi M. Fixed-angle plate osteosynthesis of the patella: an alterna-tive to tension wiring? Clin Biomech. 2010; 25(4):341-347.
17. Scilaris TA, Grantham JL, Prayson MJ, Mar-shall MP, Hamilton JJ, Williams JL. Biome-chanical comparison of fixation methods in transverse patella fractures. J Orthop Trau-ma. 1998; 12(5):356-359.
18. Müller ME, Allgöwer M, Schneider R, Wil-lenegger H. Manual of Internal Fixation: Techniques Recommended by the AO-ASIF. Heidelberg, Germany: Springer; 1990.
19. Kumar G, Mereddy PK, Hakkalamani S, Donnachie NJ. Implant removal fol-lowing surgical stabilization of patella fracture. Orthopedics. 2010; 33(5). doi: 10.3928/01477447-20100329-14
20. Catalano JB, Iannacone WM, Marczyk S, et al. Open fractures of the patella: long-term functional outcome. J Trauma. 1995; 39(3):439-444.
21. Weber MJ, Janecki CJ, McLeod P, Nelson CL, Thompson JA. Efficacy of various forms of fixation of transverse fractures of the pa-tella. J Bone Joint Surg Am. 1980; 62(2):215-220.
22. Baran O, Manisali M, Cecen B. Anatomical and biomechanical evaluation of the tension band technique in patellar fractures. Int Or-thop. 2009; 33(4):1113-1117.
23. Yang KH, Byun YS. Separate vertical wiring for the fixation of comminuted fractures of the inferior pole of the patella. J Bone Joint Surg Br. 2003; 85(8):1155-1160.
24. Tian Y, Zhou F, Ji H, Zhang Z, Guo Y. Can-nulated screw and cable are superior to modi-fied tension band in the treatment of trans-
verse patella fractures. Clin Orthop Relat Res. 2011; 469(12):3429-3435.
25. Schnabel B, Scharf M, Schwieger K, et al. Biomechanical comparison of a new staple technique with tension band wiring for trans-verse patella fractures. Clin Biomech. 2009; 24(10):855-859.
26. Patel VR, Parks BG, Wang Y, Ebert FR, Jin-nah RH. Fixation of patella fractures with braided polyester suture: a biomechanical study. Injury. 2000; 31(1):1-6.
27. Bostrom MP, Asnis SE, Ernberg JJ, et al. Fa-tigue testing of cerclage stainless steel wire fixation. J Orthop Trauma. 1994; 8(5):422-428.
28. Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res. 1979; (144):9-15.
29. Ritter G. Treatment of patella fractures. Bio-mechanics, surgery and after care. Hefte Un-fallheilkd. 1975; (120):61-67.
30. Ritter MA, Campbell ED. Postoperative pa-tellar complications with or without lateral release during total knee arthroplasty. Clin Orthop Relat Res. 1987; (219):163-168.
31. Lotke PA, Ecker ML. Transverse fractures of the patella. Clin Orthop Relat Res. 1981; (158):180-184.
32. Unger S, Blauth M, Schmoelz W. Effects of three different preservation methods on the mechanical properties of human and bovine cortical bone. Bone. 2011; 47(6):1048-1053.
33. van Haaren EH, van der Zwaard BC, van der Veen AJ, Heyligers IC, Wuisman PI, Smit TH. Effect of long-term preservation on the mechanical properties of cortical bone in goats. Acta Orthop. 2008; 79(5):708-716.
34. Kaufer H. Mechanical function of the patella. J Bone Joint Surg Am. 1971; 53(8):1551-1560.
35. Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathol-ogy. 1. Functional anatomy of the patello-femoral joint. J Bone Joint Surg Br. 1976; 58(3):287-290.
36. Scapinelli R. Blood supply of the human patella. Its relation to ischaemic necrosis after fracture. J Bone Joint Surg Br. 1967; 49(3):563-570.
e1443