FINAL REPORT Demographic Profile of Mothers with Calgary ... calgary.pdf · Demographic Profile of...
133
FINAL REPORT Demographic Profile of Mothers with Postpartum Depression Attending the Calgary Regional Home Visitation Collaborative Healthy Families Program 2005-2007, their use of Community-based Postpartum Depression Support Programs/Resources and the Support and Interventions Provided by Home Visitors Patricia Hull, Research Coordinator Calgary Regional Home Visitation Collaborative July 30, 2007
Transcript of FINAL REPORT Demographic Profile of Mothers with Calgary ... calgary.pdf · Demographic Profile of...

FINAL REPORT
Demographic Profile of Mothers with Postpartum Depression Attending the
Calgary Regional Home Visitation Collaborative Healthy Families Program 2005-2007, their use of Community-based
Postpartum Depression Support Programs/Resources and the Support and Interventions Provided by Home Visitors
Patricia Hull, Research Coordinator Calgary Regional Home Visitation Collaborative July 30, 2007

Table of Contents
List of Figures……………………………………………………………………………i
List of Tables.....................................................................................................................iv
Appendices………………………………………………………………………………vi
Executive Summary…………………………………………………………………….vii
Acknowledgements…………………………………………………………………….viii
1. The Calgary Regional Home Visitation Collaborative (CRHVC) ........................... 1
1.1. History of the CRHVC ......................................................................................... 1
1.2. The Present Day CRHVC ..................................................................................... 1
1.2.1. The CRHVC Leadership Team ..................................................................... 3
1.2.2. The CRHVC Administration Team .............................................................. 3
1.2.3. The CRHVC Contracted Service Provider Agencies .................................. 3
1.2.4. The CRHVC Home Visitors........................................................................... 4
1.2.5. The CRHVC Supervisors Team .................................................................... 5
2. The 2004 CRHVC Evaluation Project - Link to the CRHVC 2005-2007
Postpartum Depression Research Project ................................................................ 5
3. The ALVA Foundation - Funding Support for the CRHVC 2005-2007
Postpartum Depression Research Project ................................................................ 6
4. Literature Review - Postpartum Depression.............................................................. 7
4. 1. Overview of Postpartum Depression.................................................................. 7
4. 2. The Edinburgh Postnatal Depression Scale (EPDS) ........................................ 7
4. 3. Prevalence of Postpartum Depression ............................................................... 8
4.4. Risk Factors for Postpartum Depression........................................................... 10
4.4.1. Risk Factors for Postpartum Depression that Relate to the Mother ....... 10
4.4.2. Risk Factors for Postpartum Depression that Relate to the Baby ........... 11
4. 5. The Impact of Postpartum Depression ............................................................ 11
4. 5. 1. The Impact of Postpartum Depression on the Mother............................... 11
4. 5. 2. The Impact of Postpartum Depression on the Infant/Child ...................... 12
4. 6. Onset and Duration of Postpartum Depression .............................................. 13
4. 7. Treatment of Postpartum Depression .............................................................. 13

4.8. The Role of Community Support/Home Visitation as an Intervention for
Postpartum Depression ...................................................................................... 14
5. Detection of Postpartum Depression in the CRHVC Healthy Families Program 15
5.1. Overview of the Support and Interventions Provided for Mothers with
Postpartum Depression Attending the CRHVC Healthy Families Program 16
6. The CRHVC 2005-2007 Postpartum Depression Research Project....................... 16
6.1. Goals of the CRHVC 2005-2007 Postpartum Depression Research Project.. 18
6.2. Schedule of Activities and Timeframes for the CRHVC 2005-2007
Postpartum Depression Research Project ........................................................ 18
6. 3. Guiding Principles for the CRHVC 2005-2007 Postpartum Depression
Research Project ................................................................................................. 18
6.4. Project Planning Activities - The CRHVC 2005-2007 Postpartum Depression
Research Project ................................................................................................. 19
6.4.1. Project Planning Phase - Design of the Pilot Phase, Implementation Phase
and Close-out Phase ...................................................................................... 19
6.4.2. Project Pilot Phase - Design and Testing of the Data Collection Forms.. 20
6.4.3. Project Implementation Phase - Data Collection and Interim Analysis .. 21
6.4.4. Project Close-out Phase - Data Analysis and Final Reporting ................. 22
7. Findings and Results of the CRHVC 2005-2007 Postpartum Depression Research
Project ........................................................................................................................ 22
7.1. Data Analysis and Overview of Findings........................................................... 22
7.1.1. Mothers with Postpartum Depression who Screened Positive on the First
Edinburgh Screen and Positive on the Second Edinburgh Screen .......... 23
7.1.2. Mothers with Postpartum Depression who Screened Positive on the First
Edinburgh Screen and Negative on the Second Edinburgh Screen ............... 30
7.1.3. Mothers with Postpartum Depression who Screened Negative on the First
EDPS and Positive on the Second Edinburgh Screen ............................... 38
7.1.4. Mothers with Postpartum Depression who Screened Positive on the First
Edinburgh Screen and Closed Early........................................................... 44
8. Consolidated Findings and Conclusions ................................................................... 52

8.1 Interventions for Postpartum Depression Prior to the Mothers’ Admission to
the CRHVC Healthy Families Program ........................................................... 54
8.2. First Language of Mothers with Postpartum Depression Attending the
CRHVC Healthy Families Program.................................................................. 55
8.3. Ages of Mothers with Postpartum Depression Attending the CRHVC Healthy
Families Program................................................................................................ 55
8.4. Educational Support and Information Provided by Home Visitors to Mothers
with Postpartum Depression Attending the CRHVC Healthy Families
Program ............................................................................................................... 55
8.5. Referrals Made by Home Visitors for Mothers with Postpartum Depression
Attending the CRHVC Healthy Families Program ......................................... 56
9.0 Benefits of Home Visitation as Perceived by Mothers with Postpartum
Depression Attending CRHVC Healthy Families Program 2005-2007 and
Reported to Home Visitors....................................................................................... 56
10. Risk Factors Identified by Home Visitors for Mothers with Postpartum
Depression Attending the CRHVC Healthy Families Program 2005-2007......... 59
11. Barriers to Attendance at Community-Based Based Support Programs for
Mothers with Postpartum Depression Attending the CRHVC Healthy Families
Program 2005-2007................................................................................................... 60
12. Postpartum Depression Goal Statements for Mothers with Postpartum
Depression Attending the CRHVC Healthy Families Program 2005-2007......... 67
13. Risk Factors Identified at the Time of Postpartum Screening for Mothers with
Postpartum Depression Attending CRHVC Healthy Families Program 2005-
2007............................................................................................................................. 71
14. Discussion and Conclusions of the CRHVC 2005-2007 Postpartum Depression
Research Project ....................................................................................................... 76
14.1. Comparison of the Results of the CRHVC 2005-2007 Postpartum Depression
Research Project with the Findings in the Literature ..................................... 76
14.1.1 Benefits of Participation in Home Visitation/CRHVC Healthy Families
Programs........................................................................................................ 76

14.1.2. Barriers to Attendance at Programs that Provide Support for
Postpartum Depression ................................................................................ 78
14.1.3. Risk Factors Related to Postpartum Depression for Mothers Attending
Home Visitation Programs........................................................................... 80
14.1.4. Demographic Profile of Mothers with Postpartum Depression Attending
Home Visitation/Healthy Families Programs............................................. 83
15. Conclusions and Recommendations of the CRHVC 2005-2007 Postpartum
Depression Research Project ................................................................................... 84
Summary Statement - the CRHVC 2005-2007 Postpartum Depression Research
Project ........................................................................................................................ 97
List of Figures
Figure 1. The Structure of the Calgary Regional Home Visitation Collaborative ..... 2 Figure 2. First Language of Mothers with Postpartum Depression who Screened
Positive on the First and Second Edinburgh Screen................................... 23 Figure 3. Educational Support Provided by Home Visitors to Mothers with
Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen........................................................................................... 25
Figure 4. Referrals Made by Home Visitors for Mothers with Postpartum
Depression who Screened Positive on the First and Second Edinburgh Screen .............................................................................................................. 26
Figure 5. Benefits of Home Visitation for Mothers with Postpartum Depression who
Screened Positive on the First and Second Edinburgh Screen .................. 27 Figure 6. Frequency of Risk Factors for Mothers with Postpartum Depression who
Screened Positive on the First and Second Edinburgh Screen .................. 29 Figure 7. Risk Factors for Individual Mothers with Postpartum Depression who
Screened Positive on the First and Second Edinburgh Screen .................. 30 Figure 8. First Language of Mothers with Postpartum Depression who Screened
Positive on the First and Negative on the Second Edinburgh Screen........ 31 Figure 9. Educational Support Provided by Home Visitors to Mothers with
Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen.................................................................. 32
Figure 10. Referrals Made by Home Visitors for Mothers with Postpartum
Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen........................................................................................... 34
Figure 11. Benefits of Home Visitation for Mothers with Postpartum Depression
who Screened Positive on the First and Negative on the Second Edinburgh Screen .............................................................................................................. 36
Figure 12. Frequency of Risk Factors Reported by Mothers with Postpartum
Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen........................................................................................... 37
Figure 13. Identified Risk Factors for Mothers who Screened Positive on the First
and Negative on the Second Edinburgh Screen........................................... 38
i
Figure 14. First Language of Mothers with Postpartum Depression who Screened
Negative on the First and Positive on the Second Edinburgh Screen........ 39 Figure 15. Referrals Made by Home Visitors for Mothers with Postpartum
Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen........................................................................................... 40
Figure 16. Benefits of Home Visitation for Mothers with Postpartum Depression
who Screened Negative on the First and Positive on the Second Edinburgh Screen .............................................................................................................. 41
Figure 17. Frequency of Risk Factors Reported by Mothers with Postpartum
Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen........................................................................................... 43
Figure 18. Identified Risk Factors for Mothers who Screened Negative on the First
and Positive on the Second Edinburgh Screen ............................................ 44 Figure 19. First Language of Mothers with Postpartum Depression who Screened
Positive on the First Edinburgh Screen and Closed Early ......................... 45 Figure 20. Educational Support Provided by Home Visitors to Mothers with
Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early................................................................................ 46
Figure 21. Referrals Made by Home Visitors for Mothers with Postpartum
Depression who Screened Positive on the First Edinburgh Screen and Closed Early.................................................................................................... 47
Figure 22. Benefits of Home Visitation for Mothers with Postpartum Depression
who Screened Positive on the First Edinburgh Screen and Closed Early 48 Figure 23. Frequency of Risk Factors Reported by Mothers with Postpartum
Depression who Screened Positive on the First Edinburgh Screen and Closed Early.................................................................................................... 50
Figure 24. Identified Risk Factors for Mothers who Screened Positive on the First
Edinburgh Screen and Closed Early ............................................................ 51 Figure 25. Early Closure Factors for Mothers with Postpartum Depression
Attending the CRHVC Healthy Families Program 2005-2007 .................. 52 Figure 26. Barriers to Attendance at all Community-based Programs and Resources
Offering Support to Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007........................................... 63
ii

Figure 27. Goal Statements Related to the Management of Postpartum Depression
for Mothers Attending the CRHVC Healthy Families Program 2005-2007.......................................................................................................................... 68
Figure 28. Risk Factors for Mothers with Postpartum Depression Attending the
CRHVC Healthy Families Program Identified at the Time of 2005-2006 Postpartum Screening.................................................................................... 72
iii

List of Tables Table 1. Reported Prevalence Rates of Postpartum Depression in Different
Populations of Mothers ...................................................................................... 9 Table 2 - Summary of Support and Interventions for Mothers with Postpartum
Depression Attending the CRHVC Healthy Families Program 2005-2007. 17 Table 3. Roles and Responsibilities and Time Frames for the CRHVC 2005-2007
Postpartum Depression Research Project ...................................................... 19 Table 4. Demographic Profile of Mothers with Postpartum Depression Attending the
CRHVC Healthy Families Program 2005-2007 and Support/Referrals Offered by Home Visitors ................................................................................ 53
Table 5. Benefits of Home Visitation as Mentioned by Mothers with Postpartum
Depression Attending the CRHVC Healthy Families Program 2005-2007 and Reported to Home Visitors ....................................................................... 57
Table 6. Risk Factors Identified by Home Visitors for Mothers with Postpartum
Depression Attending the CRHVC Healthy Families Program 2005-2007. 59 Table 7. Barriers Experienced by Mothers with Postpartum Depression Attending
the CRHVC Healthy Families Program 2005-2007 Relating to Attendance at Community-based Postpartum Depression Support Programs .............. 61
Table 8. Barriers Experienced by Mothers with Postpartum Depression Attending
the CRHVC Healthy Families Program 2005-2007 Relating to Attendance at the Family Doctor......................................................................................... 61
Table 9. Barriers Experienced by Mothers with Postpartum Depression Attending
the CRHVC Healthy Families Program 2005-2007 Relating to Attendance at Community-based Mental Health Programs............................................. 62
Table 10. Opinions of Mothers with Postpartum Depression Attending the CRHVC
Healthy Families Program 2005-2007 about Barriers to Attendance at all Community-based Postpartum Depression Support Programs and Resources ........................................................................................................... 66
Table 11. Goal Statements Relating to the Support and Management of Postpartum
Depression for Mothers Attending CRHVC Healthy Families Program 2005-2007 ........................................................................................................... 69
Table 12. Risk Factors Identified during Postpartum Screening for Mothers with
Postpartum Depression Attending CRHVC Healthy Families Program 2005-2006 ........................................................................................................... 71
iv

Table 13. Risk Factors Identified During Screening (N=408) using the CRHVC
Postpartum Screening Tool for Mothers Attending the CRHVC Healthy Families Program 2006-2007 ........................................................................... 75
Table 14. Benefits of Home Visitation Programs - Comparison of the Findings of the
CRHVC 2005-2007 Postpartum Depression Research Project with Benefits Reported in the Literature............................................................................... 77
Table 15. Barriers to Attendance at Community-based Postpartum Depression
Support Programs - Comparison of the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with Barriers Reported in the Literature........................................................................................................... 79
Table 16. Risk Factors for Mothers with Postpartum Depression - Comparison of
the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with Risk Factors Reported in the Literature .................................. 81
Table 17. Demographic Profile of Mothers with Postpartum Depression -
Comparison of the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with the Demographic Profiles Reported in the Literature .................................................................................................... 84
v

Appendices Appendix 1 - Data Collection Forms for the CRHVC 2005-2007 Postpartum Depression Research Project
vi

Executive Summary
Postpartum depression affects many new mothers and is known to have a
detrimental effect on the development of the mother-child relationship. The Calgary
Regional Home Visitation Collaborative (CRHVC) Healthy Families Program has
provided support and referral services for mothers with postpartum depression since its
inception in 2002. In 2004, the CRHVC found that over 35% of the mothers attending the
CRHVC Healthy Families Program screened positive for postpartum depression. The
CRHVC, given its commitment to research and evaluation, undertook the 2005-2007
Postpartum Depression Research Project to determine the demographic profile of mothers
with postpartum depression attending the CRHVC Healthy Families Program.
The average age of the 130 mothers with postpartum depression attending the
CRHVC Healthy Families Program was 30 (20-43) years; 81 (60%) of the mothers had
English as their first language. The CRHVC Home Visitors provided emotional support
for the mothers, arranged referrals to community-based postpartum depression support
programs and resources and provided various educational materials to the mothers. The
greatest barriers to mothers’ attendance at the community-based support programs to
which they were referred included transportation and child care issues and no perceived
benefit from attending the program. The greatest risk factors for the mothers were
financial and relationship difficulties, social isolation and current or past depression.
The CRHVC, given its commitment to research that advances support for mothers
with postpartum depression should consider additional studies, notably the development
of outcome-based best practice postpartum depression support guidelines for Home
Visitors and research to better understand mothers’ perceptions of postpartum depression.
vii

Acknowledgements
In submitting this Final Report, I would like to acknowledge the exceptional support
that I have received from the following people and organizations.
Funding Agencies
The ALVA Foundation, Toronto Ontario (majority of funding) Calgary and Area Child and Family Services Authority Calgary Children’s Initiative
The Calgary Regional Home Visitation Collaborative
Marianne Symons, Program Manager Amanda Robinson, Screener Nadine McClure Smith, Research Assistant Wichita Ferro, Screener, CRHVC Leadership Team Supervisors Team The Contracted Service Provider Agencies Home Visitors Mothers
Consultants and External Support
Dr. David Cawthorpe, Research and Evaluation Expert Petrina Hough, Evaluation Facilitator Calgary Health Region Public Health Nurses Members of the community with an interest in mother/child health
The Alberta Home Visitation Collaborative Network
Members of the Board Member organizations
viii

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
1. The Calgary Regional Home Visitation Collaborative (CRHVC) 1.1. History of the CRHVC
It is well-recognized that children who grow up in a home environment where there
are low levels of social support, a lack of parenting skills, insufficient funds for basic
necessities, alcohol or drug abuse concerns and/or mental health issues are susceptible to
neglect and abuse (Hough, 2004). These negative living circumstances are frequently
manifested in vulnerable children as delayed cognitive development, lifelong learning
difficulties, emotional problems or poor social adjustment.
In the early 2000’s, a number of Calgary-based organizations that served children
and families completed a comprehensive review that critically evaluated the availability
of community-based support services for vulnerable mothers and their babies/children.
This study clearly showed that the level of available support for at-risk mothers and their
families was minimal. In order to address this issue, a Steering Committee comprised of
representatives from local organizations with an interest in child and family services
responded to a provincial Request for Proposal for the creation of a Home Visitation
Program in Calgary. The Steering Committee’s efforts culminated in the creation of the
CRHVC in 2002. The mandate of the CRHVC was to oversee the development of a
comprehensive Home Visitation Program for new mothers and their babies/children who
were likely to be living in at-risk situations.
1.2. The Present Day CRHVC
Organizationally, the CRHVC includes a Leadership Team, an Administration
Team, Contracted Community Agencies, Home Visitors and a Supervisors Team. The
organizational structure of the CRHVC is depicted in Figure 1.
1

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 1. The Structure of the Calgary Regional Home Visitation Collaborative*
CALGARY CHILD AND FAMILY SERVICES (REGION 3)
CALGARY REGIONAL HOME VISITATION COLLABORATIVE
MANAGEMENT COMMITTEE (Leadership Team)
Screening, Research and Administrative Support (3FTE) Program Manager (Marianne Symons)
SERVICE
PROVIDER Calgary
Immigrant Women’s
Association
SERVICE PROVIDER Children’s
Cottage Society of Calgary
SERVICE PROVIDER
Salvation Army Children’s Village
SERVICE PROVIDER
Closer To Home
SERVICE PROVIDER Spectrum Youth and
Family Services Association Executive Director
SERVICE
PROVIDER Families Matter
Executive Director
Fiscal Agent Hull Child and Family Services
Program Supervisor
(0.4 FTE)
Program
Supervisor (1.4 FTE)
Program Supervisor
(1 FTE)
Program Supervisor
(0.4 FTE)
Program Supervisor
(0.6 FTE)
Program Supervisor
(1 FTE)
Home Visitors
(2 FTE) Four 0.5 positions
Home Visitors (7 FTE)
Home Visitors
(5 FTE)
Home Visitors (2 FTE)
Home Visitors
(3 FTE)
Home Visitors
(5 FTE)
* May 2007
A brief description of the roles and responsibilities of the CRHVC Leadership
Team, the CRHVC Administration Team, the Contracted Service Provider Agencies,
Home Visitors and the Supervisors Team follows.
2

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
1.2.1. The CRHVC Leadership Team
The CRHVC Leadership Team serves as a management committee for the
CRHVC and as such, sets the strategic direction and provides overall leadership of the
CRHVC. The Leadership Team is comprised of representatives from the fiscal agent
(Hull Child and Family Services), Calgary and Area Child and Family Services
Authority, Calgary Health Region, the CRHVC Project Manager, and sector
representatives (organizations offering home visitation services but who are not providing
services for the CRHVC Healthy Families Program and other institutions as deemed
appropriate). The Calgary Children’s Initiative served on the Leadership Team from the
inception of the CRHVC in 2002 until April 2007 at which time they determined that the
CRHVC was operating effectively and no longer required their assistance.
1.2.2. The CRHVC Administration Team
The CRHVC Administration Team hold degrees/diplomas in the Human Services
and includes a Program Manager (Marianne Symons) who coordinates and administers
the programs of the CRHVC, one fulltime Administrative Research Assistant (Nadine
McClure-Smith), one full-time Screener (Amanda Robinson) and a part-time Screener
(Wichita Ferro). The Administration Team also includes a Research Coordinator (Patricia
Hull) who oversees the design and evaluation of targeted research projects.
1.2.3. The CRHVC Contracted Service Provider Agencies
The Contracted Service Provider agencies provide Home Visitation services
through the CRHVC Healthy Families Program. The Contracted Service Provider
agencies of the CRHVC include: Closer to Home Community Services, Calgary
Immigrant Women’s Association (CIWA), Families Matter, Spectrum Youth and Family
3

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Services Association, Children’s Cottage Society of Calgary and the Salvation Army
Children’s Village (SACV). The staffing complement of each agency includes a Program
Supervisor and a specified number of Home Visitors; the standard ratio of Supervisor to
Home Visitor is 1:5. The Contracted Service Provider Agencies have established solid
working relationships and partnerships with the organizations in communities where they
provide services. These partner organizations provide community-based support services
that can be accessed by families participating in the Healthy Families Program. In order
to promote increased utilization of their services, the CRHVC has developed information
brochures, consent for service and assessment tools, many of which have been translated
into different languages including Chinese, Vietnamese, Punjabi, Arabic, and Spanish. In
addition, qualified Aboriginal Home Visitors are employed by the Closer to Home
agency and their involvement has increased the participation of Aboriginal families.
1.2.4. The CRHVC Home Visitors
The majority of the CRHVC Home Visitors have diplomas or degrees in the
human services fields and in general, their career experience exceeds two years. The
Home Visitors support the mothers attending the CRHVC Healthy Families Program by:
developing individualized service/goal plans/interventions based on family needs;
assessing progress towards those goals; teaching parenting skills to mothers; providing
emotional support for the mothers and; making referrals to community resources. Each
CRHVC Home Visitor has a caseload of between 15 and 20 families.
The CRHVC Home Visitors are committed to connecting families to needed
community-based postpartum depression support programs and specialized
services/resources. They make their first visit to the family within a week of referral and
4

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
depending on family needs (and the parents desire to remain in the CRHVC Healthy
Families Program) may continue to see the family until the child reaches age five.
1.2.5. The CRHVC Supervisors Team
The CRHVC Supervisors Team serves as an operations committee and facilitates
achievement of the CRHVC’s strategic directives. The Supervisors Team is comprised of
a Supervisor from each of the Contracted Service Provider agencies, the CRHVC
Program Manager and other members of the Administration Team as may be appropriate.
2. The 2004 CRHVC Evaluation Project - Link to the CRHVC 2005-2007 Postpartum Depression Research Project
In 2004, the CRHVC organized a review and evaluation of its operations. A
consultant, Petrina Hough coordinated this initiative and her findings are detailed in a
comprehensive report (Hough, 2004). One part of the evaluation focused on postpartum
depression in mothers attending the CRHVC Healthy Families Program. Hough (2004)
determined that:
Eighty-eight percent (n=129) of the mothers in the 2004 CRHVC evaluation sample completed the Edinburgh Postpartum Depression Screening Tool (EPDS)
The rate of postpartum depression at the time of the first EPDS was 35% (n= 42) The rate of postpartum depression at the time of the second EPDS was 21% (n= 17)
On the basis of her study findings, Hough (2004) concluded that:
The percentage of women in the 2004 CRHVC evaluation sample who screened positive for postpartum depression at either the first or second screen was significantly higher than that reported for the general population;
Given this, postpartum depression appeared to be an important issue for service delivery by the CRHVC;
The services to which mothers with postpartum depression are usually referred to are not ideal for many mothers due to the nature of the treatment offered (usually group work), the long waitlist for services, the logistics of getting there (transport, childcare), and because services are not available in languages other than English;
Given that the existing services are not meeting the identified need in the Healthy Families postpartum depression population, a coordinated effort to assist mothers suffering from postpartum depression needs to be defined and;
5
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
The profile of the mothers who are dealing with postpartum depression, notably their demographics and any relation to scores on screening tools needs to be explored in Calgary. The CRHVC fully endorsed the findings in Hough’s (2004) Report and, in 2004
sought funding to undertake a follow-up study to address her recommendations.
3. The ALVA Foundation - Funding Support for the CRHVC 2005-2007 Postpartum Depression Research Project
The CRHVC is committed to carrying out its mandate in the context of an
evaluation and research framework. Based on Hough’s (2004) recommendations, the
CRHVC made a decision to undertake a study that would describe the demographic
profile of mothers with postpartum depression attending the CRHVC Healthy Families
Program specifically, their use of community-based postpartum depression support
services and resources and the relation between their postpartum screening scores (with
the Parkyn Screen/Healthy Families America Screen) and postpartum depression. In
2004, the CRHVC requested and received majority funding from the ALVA Foundation
(Toronto, Ontario) to undertake the CRHVC 2005-2007 Postpartum Depression Research
Project, an exploratory evidence-based research initiative that would describe:
1) The demographic profile of mothers with postpartum depression attending the CRHVC Healthy Families Program
2) The relationship/frequency between risk factors identified on the postpartum screening tools (the Parkyn Screen and the Healthy Families America Screen) in mothers with postpartum depression attending the CRHVC Healthy Families Program
3) The community-based support services and resources accessed by mothers with postpartum depression and the barriers to accessing these programs
The Calgary and Area Child and Family Services Authority and the Calgary
Children’s Initiative provided additional funding support. Patricia Hull was hired as the
Research Coordinator in April 2005.
6

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
4. Literature Review - Postpartum Depression
4. 1. Overview of Postpartum Depression
Postpartum depression is a costly common major depressive disorder that affects
10-20% of women in their child-bearing years (Gjerdingen andYawn, 2007). According
to Beck (2006), its diagnosis is dependent on a mother having five or more of the
following symptoms for at least two weeks; insomnia or hypersomnia, psychomotor
agitation or retardation, fatigue, changes to appetite, feelings of worthlessness or guilt,
decreased concentration and suicidality and in addition; symptoms of one or both of
depressed mood or loss of pleasure. Baby blues, which manifest as anxiety, tearfulness
and mild irritability within several days after the baby’s birth (and tend to disappear
within several weeks of birth) affect 50-75% of new mothers (Beck, 2006). On the other
hand, postnatal psychosis is a rare but severe psychiatric disturbance where a mother
becomes "out of touch'' with reality after the birth of a baby (Ballard, Davis, Cullen,
Mohan and Dean, 1994; Seyfried and Marcus, 2003; Sit, Rothschild and Wisner, 2006).
Stewart, Robertson, Dennis, Grace and Wallington (2003) completed a
comprehensive literature review of postpartum depression with a particular focus on four
areas: risk factors for postpartum depression; detection, prevention and treatment of
postpartum depression; effects of the illness on the mother-infant relationship and; public
health interventions and strategies to mitigate the impact of postpartum depression. This
publication is an excellent resource and includes a comprehensive list of references.
4. 2. The Edinburgh Postnatal Depression Scale (EPDS)
The Edinburgh Postnatal Depression Scale (EPDS) is a ten-item self-reporting
measurement tool designed to identify postnatal depression in new mothers (Cox, Holden
7

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
and Sagovsky, 1987). The validity of the EPDS in terms of its ability to detect postnatal
depression has been widely reported (Boyce and Hickey, 2005; Dennis and Ross, 2006;
Sword, Watt and Kreuger, 2006). The EPDS questionnaire is the most frequently used
screening tool for detecting postpartum depression; a score of > 12 is indicative of
postpartum depression (Dennis 2005).
4. 3. Prevalence of Postpartum Depression
Various authors have noted that 60% of women experienced their first depression
after becoming a mother and that the presence of a pre-existing depressive disorder made
relapse more likely after the baby’s birth (Arnold, Baugh, Fisher, Brown and Stowe,
2002; Flores and Hendrick, 2002). Ramsay (1993) noted that 50% of cases of postpartum
depression were not detected, and hence not treated. At the same time, only 49% of
mothers who reported depression actually sought help and support (MacLennan, Wilson
and Taylor, 1996). Cooper and Murray (1998) noted that, over a five year period women
with postpartum depression were twice as likely to experience future episodes of
depression.
The prevalence rate of postpartum depression has been widely reported for
different populations of mothers in various countries. Overall, these studies concluded
that postpartum depression was a major public health issue/concern affecting mothers and
families from most cultures. The onset and duration of postpartum depression was
influenced by various medical/health and psychosocial factors in the mothers’ home
environment. A summary of the findings from various studies is detailed in Table 1.
8

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 1. Reported Prevalence Rates of Postpartum Depression in Different Populations of Mothers Prevalence - Postpartum Depression
Reference Comments
13% O’Hara & Swain (1996) Diverse population-based studies; summary results of 59 studies; rate in adolescent mothers was 25%
3-25% Dennis, Janssen & Singer (2004)
Rates fluctuated in relation to sample size, timing of the assessment, choice of diagnostic criteria, and whether the studies were retrospective or prospective
3.5- 40%
Inandi, Bugdayci, Sasmaz, Dunbar & Sumer (2005)
Rates varied depending on definition of postpartum depression, evaluation criteria and geographical location; (31% in Turkish mothers - the focus of their study)
1-5.9 % Beck (2006) Study focused on the first 12 months postpartum with the highest rates noted at two and six months postpartum; reference to mothers from different cultures
11.5% Fuggle, Glover, Khan & Haydon (2002)
Study focused on Bengali women in England and Bangledash x
10% Righhetti-Veltema, Conne-Perreard, Bousquet & Manzano (1998)
General population-based study
10-20% Surkan, Peterson, Hughes & Gottlieb (2006)
Reference to various literature studies
Variable (see comments)
Bloch, Rotenberg, Koren & Klein (2005)
Rates of 43.9%, 46.8% and 31.3 % found in African-American, Hispanic and white women respectively
23 % Baker, Cross, Greaver, Wei, Lewis, and the Healthy Start CORPS (2005)
Native population studies, authors noted that this rate of postpartum depression was significantly higher than that for other populations
35% Hough (2004) Mothers of different cultures attending CRHVC Healthy Families Program - mothers pre-screened by Calgary Health Region, thus accounting for the relatively high prevalence
9

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
4.4. Risk Factors for Postpartum Depression
Risk factors for postpartum depression have been extensively documented (Beck,
1998, 2001, 2006; Bernazzanni, Saucier and Borgeat, 1997; Boyce and Hickey, 2005;
Dennis et al., 2004; Misri, Kostaras, Fox, and Kostaras, 2000; Righhetti-Veltema et al.,
1998; Ryan, Milis and Misri, 2005; Seyfried and Marcus, 2003; Stewart et al., 2003;
Vasquez and Pitts, 2006). A summary of the most usual and important risk factors for
postpartum depression follows.
4.4.1. Risk Factors for Postpartum Depression that Relate to the Mother
The mother-related risk factors for postpartum depression that have been reported
in the literature include:
Prenatal depression, anxiety, panic, obsessive thoughts or behavior History of childhood abuse Psychiatric illness in other family members, notably partners Relationship difficulties Inadequate social support (family, friends and partners); loneliness Low level of education Socio-economic issues including unemployment Multiparity Inability to breastfeed; unhappiness with child feeding Stressful life events, particularly financial problems Marital conflict/domestic violence Low confidence as a parent Child care stress Low self-esteem Poor coping/stress management skills Maternal non-adjustment; negative attitude to the baby New immigrant status Single parent status inclusive of recent separation or divorce situations Super woman syndrome Perfectionist ideals and attitudes Hormonal risks (thyroid imbalance) or premenstrual dysmorphic disorder or
infertility issues) Reluctance to seek support for physical/mental health related concerns
10

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
4.4.2. Risk Factors for Postpartum Depression that Relate to the Baby
The baby-related risk factors for postpartum depression that have been reported in
the literature include:
Obstetric complications; negative birth experience Unplanned pregnancy Inadequate prenatal care Early mother-child separation Young age of mother at the time of birth Having a baby of the non-desired sex Baby's personality, health or disability Difficult infant behavior; fussy, demanding, poor eating habits, poor sleeping
patterns
It is important to note that the literature generally indicated that these mother/child-
related risk factors did not actually cause postpartum depression; in fact many women
who had these risk factors never became depressed.
4. 5. The Impact of Postpartum Depression
The devastating effects of postpartum depression on the maternal-child/family
interactions have been reported in numerous studies. Beck (1998, 2002) and others
(Austin 2003; Benvenutti, Valooriani, Degl’Innocenti, Favinin, Hipwell and Pazzagli,
2001; Murray, Sinclair, Cooper, Ducournau and Turner, 1999; Stewart et al., 2003) have
noted that, in general mothers and children were likely to be living in at-risk
circumstances if postpartum depression was present and/or not adequately managed.
4. 5. 1. The Impact of Postpartum Depression on the Mother
In a study of 570 women, Righhetti-Veltema et al., (1998) found that the coping
abilities of depressed mother were decreased while their vulnerability to new stress
factors increased. Mothers with postpartum depression have been shown to display
flatness of affect with less affection shown to their infants (Beck, 2002). Dennis et al.,
11

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
(2004) noted that mothers with postpartum depression frequently exhibited symptoms of
dysphoria, emotional lability, insomnia, confusion, anxiety, guilt, and suicidal ideation;
poor ability to cope, low self-esteem, negative maternal attitudes and loneliness which
tended to exacerbate postpartum depression symptoms. According to Goldsmith (2007),
mothers with postpartum depression felt overwhelmed and were often unable to complete
basic activities such as self-care, caring for the baby and doing household chores.
Logsdon, Wisner and Pinto-Foltz (2006a) noted that mothers with postpartum depression
were less likely to comply with recommended preventative health interventions. Other
researchers have noted that mothers with postpartum depression were also more unlikely
to seek necessary treatment and help (Dennis and Chung-Lee 2006).
4. 5. 2. The Impact of Postpartum Depression on the Infant/Child
Beck (1995) noted that infants of mothers with postpartum depression were
fussier and made fewer positive facial expressions and vocalizations than infants of
mothers who were not depressed. Ryan et al., (2005) and Logsdon et al., (2006a) reported
that postpartum depression negatively affected infants with consequent deleterious effects
on the child’s cognitive and emotional development in the early years. Infants of mothers
with postpartum depression have also demonstrated an aversion to interaction and
communication, thus contributing to their mothers’ negative mood and depression (Cohn
and Tronick, 1983; Forbes, Cohn, Allen and Lewinsohn (2004); Murray et al., 1999;
Stewart et al., 2003). Other adverse effects of postpartum depression on infants/children
that have been reported include attachment insecurity, social difficulties and long-term
behavioral difficulties (Beck, 1999; Orvaschel, Walsh-Allis and Ye, 1988). Finally,
postpartum depression has also been shown to adversely affect family health (Beck,
12

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
2006, Stewart et al., 2003) and additionally, to compromise child safety (Rhodes and
Iwashyna, 2007).
4. 6. Onset and Duration of Postpartum Depression
The onset of postpartum depression has been reported to be greatest in the first 12
weeks postpartum (Cooper and Murray, 1998; Stewart et al., 2003). The duration of
postpartum depression generally depends on its severity and the mothers’ timeliness in
seeking and receiving appropriate treatment(s) and support.
4. 7. Treatment of Postpartum Depression
According to Dennis (2006), Highet and Drummond (2004), Holden, Sagovsky
and Cox (1989), Horowitz and Goodman (2005) and Stewart et al., (2003), a variety of
interventions have been used to treat postpartum depression; these interventions include:
Psychological interventions (interpersonal psychotherapy, cognitive behavioral therapy, psychological debriefing)
Psychosocial interventions (antenatal and postnatal classes, intrapartum support, supportive interactions)
Quality of care improvements (continuity of care, antenatal identification and notification, early postpartum follow-up by general practitioners, flexible postpartum care, education strategies, relaxation and guided imagery
Dennis (2006) and Cooper and Murray (1998) and Murray, Cooper, Wilson and
Romaniuk (2003) suggested that postpartum depression was a major health issue and as
such, there was a need for timely and effective preventive strategies. Studies completed
by Dennis and Ross (2006) noted that early screening in conjunction with an
understanding of new mothers’ biological and psychosocial risk factors for postpartum
depression could form a sound basis for its early identification and timely treatment.
Lumley (2005) concluded that psychosocial and psychological strategies or specific
interventions tested in trials have not effectively prevented postpartum depression and
13

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
advised that the use of mental health workers could be an important strategy for
preventing postpartum depression. Dennis (2005) proposed that intensive care and
support in the home for new mothers should be considered as a key intervention for
managing postpartum depression. According to Whitton and Appleby (1996), successful
therapy partly involved mothers addressing incorrect ideals (such as expecting too much
of themselves) and having some time to themselves a strategy that in turn, would
strengthen the mother-child relationship.
Charbrol, Teissdre, Armitage, Danel and Walburg (2004) and others (Boath,
Bradley and Henshaw, 2004; Malone, Papagni, Ramini and Keltner, 2004; Stewart et al,
2003) noted that antidepressant therapy was a successful option for treating postpartum
depression in some, though not all mothers.
4.8. The Role of Community Support/Home Visitation as an Intervention for Postpartum Depression Holden et al., (1989) determined that mothers who had regular visits (average of
nine visits over thirteen weeks) from Health Visitors (Home Visitors) showed a greater
improvement in maternal mood and the quality of mother-infant relationship compared to
women who were not visited, a finding supported by Seeley, Murray and Cooper (1996).
Matthey (2004), citing the results of various studies noted that home visiting did not
appear to have a lasting impact on mother’s mood or self-esteem; at the same time, and
depending on the study, he concluded that home visiting was associated with positive
gains in the mother-child interaction. Ray and Hodnett (2001) conducted a
comprehensive review of randomized and quasi-randomized trials wherein they assessed
the effect of additional professional caregiver and/or social support interventions on the
14

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
course of postpartum depression. They concluded that there is evidence to affirm the
positive effect of professional support on reducing postpartum depression.
Shaw, Levitt, Wong and Kaczorowski (2006) examined the effectiveness of
postpartum support programs in improving the mothers’ knowledge, attitudes and skills
relating to parenting, mental health status, maternal quality of life and physical health.
They concluded that home visitation or peer support could benefit high risk populations
and that scores on the Edinburgh Postnatal Depression Scale were significantly reduced
when mothers participated in home visitation programs.
Leahy-Warren and McCarthy (2007) reviewed the evidence relating to different
treatment options for postpartum depression and noted that there was: limited success
with antidepressant medications, some success with psychotherapeutic options and a
positive impact of professional home visits and social support networks for mothers with
postnatal depression. These authors, citing Dennis (2005) concluded that the only
intervention that demonstrated a clear preventative effect with vulnerable mothers was
individual intensive postpartum support in the guise of postnatal home visits provided by
professionals.
5. Detection of Postpartum Depression in the CRHVC Healthy Families Program The results of the EPDS are considered valid if the screen is administered six
weeks to twelve months postpartum. The CRHVC Home Visitors first offer the EPDS to
mothers at sixteen weeks postpartum and again at thirty-two weeks postpartum. As
deemed necessary, the CRHVC Home Visitors can offer the EDPS a third time if they
believe that the mother might have become depressed. The CRHVC Home Visitors may
15

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
also offer screening at eight weeks if professionals from other organizations had not
already offered the EDPS to mothers.
Mothers who score twelve on the English version of the EPDS and mothers who
score ten on the translated versions of the EPDS are considered to have screened
positively for postpartum depression. The CRHVC Home Visitors, in conjunction with
the mothers who have a positive EDPS score, develop individualized treatment plans and
goal statements to address the mothers’ postpartum depression. The goal statements and
plans for treating the mothers’ postpartum depression range from offering emotional
support and education about postpartum depression to making referrals/connections to
community-based postpartum depression support programs and resources.
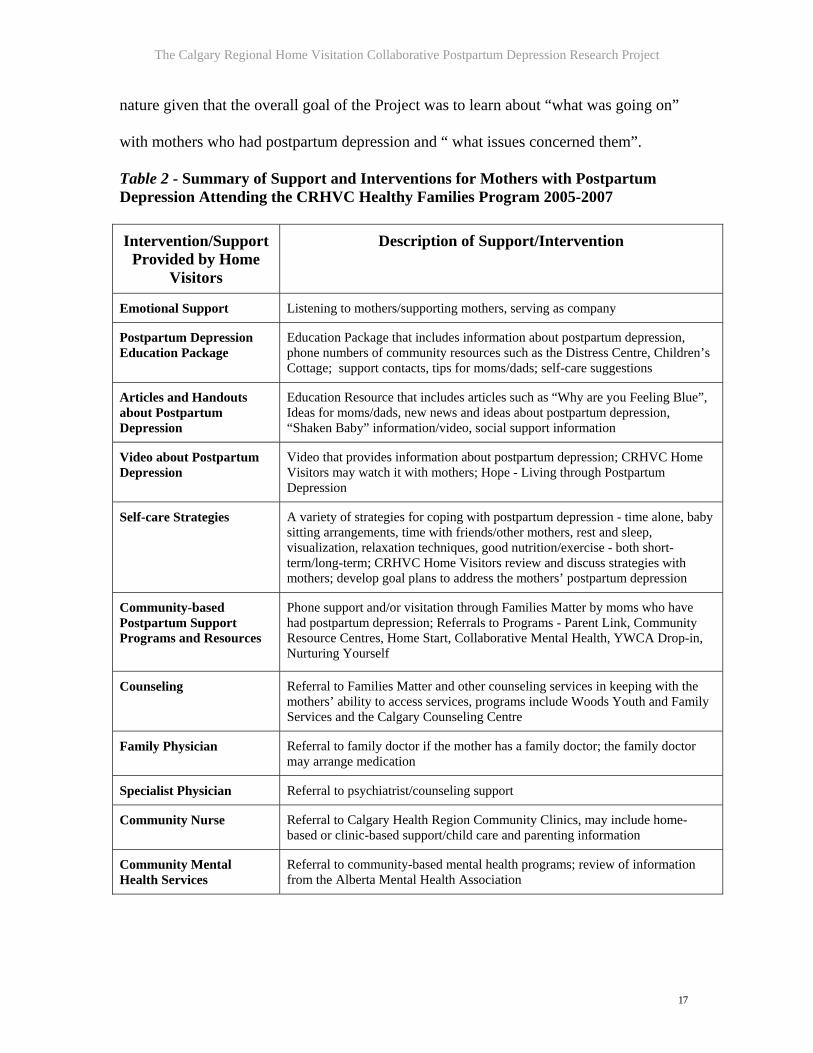
5.1. Overview of the Support and Interventions Provided for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program
The CRHVC Healthy Families Program provides support to mothers with
postpartum depression, part of which is referral to community-based postpartum
depression support programs and resources. Table 2 provides a summary of the support
that the CRHVC Home Visitors provide for mothers with postpartum depression.
6. The CRHVC 2005-2007 Postpartum Depression Research Project
The CRHVC is committed to the continual improvement of its programs and to
adding new knowledge about how Home Visitors can best serve vulnerable mothers with
postpartum depression and their families. As such, the CRHVC 2005-2007 Postpartum
Depression Research Project, with a mandate of addressing Hough’s (2004)
recommendations (p. 5 of this Report) was undertaken in 2005. The research approach
used for the CRHVC 2005-2007 Postpartum Depression Project was exploratory in
16
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
nature given that the overall goal of the Project was to learn about “what was going on”
with mothers who had postpartum depression and “ what issues concerned them”.
Table 2 - Summary of Support and Interventions for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 Intervention/Support
Provided by Home Visitors
Description of Support/Intervention
Emotional Support Listening to mothers/supporting mothers, serving as company
Postpartum Depression Education Package
Education Package that includes information about postpartum depression, phone numbers of community resources such as the Distress Centre, Children’s Cottage; support contacts, tips for moms/dads; self-care suggestions
Articles and Handouts about Postpartum Depression
Education Resource that includes articles such as “Why are you Feeling Blue”, Ideas for moms/dads, new news and ideas about postpartum depression, “Shaken Baby” information/video, social support information
Video about Postpartum Depression
Video that provides information about postpartum depression; CRHVC Home Visitors may watch it with mothers; Hope - Living through Postpartum Depression
Self-care Strategies A variety of strategies for coping with postpartum depression - time alone, baby sitting arrangements, time with friends/other mothers, rest and sleep, visualization, relaxation techniques, good nutrition/exercise - both short-term/long-term; CRHVC Home Visitors review and discuss strategies with mothers; develop goal plans to address the mothers’ postpartum depression
Community-based Postpartum Support Programs and Resources
Phone support and/or visitation through Families Matter by moms who have had postpartum depression; Referrals to Programs - Parent Link, Community Resource Centres, Home Start, Collaborative Mental Health, YWCA Drop-in, Nurturing Yourself
Counseling Referral to Families Matter and other counseling services in keeping with the mothers’ ability to access services, programs include Woods Youth and Family Services and the Calgary Counseling Centre
Family Physician Referral to family doctor if the mother has a family doctor; the family doctor may arrange medication
Specialist Physician Referral to psychiatrist/counseling support
Community Nurse Referral to Calgary Health Region Community Clinics, may include home-based or clinic-based support/child care and parenting information
Community Mental Health Services
Referral to community-based mental health programs; review of information from the Alberta Mental Health Association
17

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
6.1. Goals of the CRHVC 2005-2007 Postpartum Depression Research Project
The five goals of the 2005-2007 CRHVC Postpartum Depression Research
Project were to:
1) Determine and assess the demographic profile of mothers with postpartum depression attending the CRHVC Healthy Families Program;
2) Determine the community-based support services and resources that mothers with postpartum depression attending the CRHVC Healthy Families Program were referred to;
3) Determine and assess the factors that influenced the decisions of mothers with postpartum depression attending the CRHVC Healthy Families Program to participate/not participate in community-based support services and resources for postpartum depression;
4) Determine and assess the perceptions of mothers with postpartum depression attending the CRHVC Healthy Families Program about the support and services offered by their Home Visitors and;
5) Use the results of the CRHVC 2005-2007 Postpartum Depression Research Project as a source of input for recommending additional research studies and/or for strengthening the CRHVC’s postpartum depression support strategies
6.2. Schedule of Activities and Timeframes for the CRHVC 2005-2007 Postpartum Depression Research Project
The time frame for the CRHVC Postpartum Depression Research Project was
May 2005 to July 2007. The roles of the CRHVC Administration Team, Contracted
Service Agencies/Home Visitors and the Research Coordinator are detailed in Table 3.
6. 3. Guiding Principles for the CRHVC 2005-2007 Postpartum Depression Research Project
The CRHVC Postpartum Depression Research Project was undertaken in the
context of a research and evaluation framework. Its execution was guided by the
following principles: the use of evidence to support statements and conclusions; attention
to practical feasible recommendations to better understand and/or enhance the needs of
families served by the CRHVC Healthy Families Program; extensive involvement with
18

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
internal and external stakeholders and; the generation of new ideas for further study and
strengthening of the CRHVC Healthy Families Program.
Table 3. Roles and Responsibilities and Time Frames for the CRHVC 2005-2007 Postpartum Depression Research Project
Postpartum depression Project Activity
Roles and Responsibilities
Start Date Finish Date
Project Planning Phase: Design of data collection forms and procedures for the collection of postpartum depression data from the CRHVC Contracted Service agencies; development of guidelines for undertaking the pilot phase, implementation phase and close-out phase; confirmation of time frames for the different phases, design of guidelines for data analysis and final reporting
CRHVC Administration Staff, Research Coordinator
May 2005 August 2005
Pilot Phase: Review and revision of data collection forms; initial data collection from the CRHVC Home Visitors using the data collection forms
Project Coordinator, CRHVC Supervisors Team, CRHVC Healthy Families Staff
September 2005
October 2005
Implementation Phase: Continued data collection, analysis of the data collected during the implementation phase
Project Coordinator, CRHVC Administration Team, Supervisors Team
November 2005
February 2007
Close-out Phase: Data analysis, consolidation of findings and submission of the Final Report
Project Coordinator, CRHVC Administration Team, Supervisors Team; Healthy Families Staff
March 2007 July 2007
6.4. Project Planning Activities - The CRHVC 2005-2007 Postpartum Depression Research Project The following activities were completed during the project planning phase which
took place between May and October 2005.
6.4.1. Project Planning Phase - Design of the Pilot Phase, Implementation Phase and Close-out Phase The Research Coordinator and the CRHVC Administration Team developed a
framework for completing the Project in relation to specific criteria i.e. the CRHVC
2005-2007 Postpartum Depression Project had to:
Achieve the 5 stated goals Be completed by May 2007 Be literature-driven Provide recommendations for further study and research
19

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Use a participative approach and involve the CRHVC Administration Team, Supervisors and Home Visitors as well as external expert Consultants
In planning the CRHVC Postpartum Depression Research Project, the Research
Coordinator and the CRHVC Administration Team identified three distinct phases; the
pilot phase, the implementation phase and the post-pilot phase. The pilot phase was
scheduled for completion between August 2005 and December, 2005; its key activities
included the development and testing of the forms for collecting data about/from the
mothers with postpartum depression. The time frame for the implementation phase was
January 2006 until March 31, 2007. The key activities of the implementation phase
included continued data collection and an interim analysis of the findings. The main
activities of the post-pilot phase, which was scheduled for completion between April and
May, 2007 included a comprehensive analysis of the data and writing of the Final Report.
6.4.2. Project Pilot Phase - Design and Testing of the Data Collection Forms The Research Coordinator and the CRHVC Administration Team developed data
collection forms between May and August 2005. The forms were designed to capture
information about the mothers’ demographics, the nature of support/interventions
provided by the CRHVC Home Visitors, the type/nature of referrals made to community-
based postpartum depression support programs and resources (family doctor, specialist
physician, community health nurse and community-based postpartum depression support
programs) and the mothers’ perceptions about barriers to accessing these services.
The Supervisors Team reviewed the data collection forms and based on their
feedback, some changes were made. At the conclusion of the pilot phase, the Supervisors
as well as the CRHVC Administration Team completed a final review of the forms and
20

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
recommended several additional changes, primarily the clarification of several questions.
A copy of the data collection forms is included in Appendix 1.
For the purposes of data collection, the mothers with postpartum depression were
categorized as mothers who:
Screened positive on the first EDPS screen and positive on the second EDPS screen
Screened positive on the first EDPS screen and negative on the second EDPS screen
Screened negative on the first EDPS screen and positive on the second EDPS screen
Screened positive on the first EDPS screen and had early closure from the CRHVC Healthy Families Program
Mothers were included in the CRHVC 2005-2007 Postpartum Depression Research
Project if: they had attended the CRHVC Healthy Families Program in 2005-2007 and if;
the CRHVC Home Visitors could collect the information on the data collection forms.
6.4.3. Project Implementation Phase - Data Collection and Interim Analysis
The implementation phase of the Project took place between January 2006 and March
2007. During the implementation phase, the CRHVC Home Visitors continued to
complete and return the data collection forms to the CRHVC Research Assistant. As of
December 2006, data were available for 103 mothers attending the CRHVC Healthy
Families Program who had screened positive for postpartum depression. Overall, the
quality of the data collected/reported by the CRHVC Home Visitors was excellent.
An interim analysis of the data for mothers with postpartum depression was
completed in March 2006 and again in December 2006. The findings of the interim
analysis in December 2006 were as follows:
English was the first language of approximately half of the mothers with postpartum depression attending the CRHVC Healthy Families Program
21

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
The most usual forms of support offered to the mothers by the CRHVC Home Visitors were emotional support/company; the provision of education information packages about postpartum depression and; referrals to community-based postpartum depression support programs and resources
The most usual risk factors for postpartum depression identified by the CRHVC Home Visitors included financial difficulties (insufficient money for basic necessities), relationship difficulties, past/current depression and social isolation
Approximately 30% of the mothers with postpartum depression had early closure from the CRHVC Healthy Families Program
6.4.4. Project Close-out Phase - Data Analysis and Final Reporting
The implementation phase of the Project finished on March 31, 2007. During May,
June and July 2007 a comprehensive analysis of the data was completed and the Final
Report was written.
7. Findings and Results of the CRHVC 2005-2007 Postpartum Depression Research Project 7.1. Data Analysis and Overview of Findings
As noted earlier, the CRHVC 2005-2007 Postpartum Depression Research Project
categorized mothers with postpartum depression attending the CRHVC Healthy Families
Program into four distinct groups. Data were available for 130 mothers inclusive of:
34 (26%) of the 130 mothers who screened positive on the first EDPS and positive on the second screen
29 (22%) of the 130 mothers screened who positive on the first EDPS and negative on the second screen
15 (12%) of the 130 mothers who screened negative on the first EDPS and positive on the second screen
52 (40%) of the 130 mothers who screened positive on the first EDPS and had early closure from the CRHVC Healthy Families Program
The following sections of this Report summarize the findings for each of these
categories of mothers.
22

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
7.1.1. Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Positive on the Second Edinburgh Screen In this study, thirty-four (26%) of the 130 mothers with postpartum depression
attending the CRHVC Healthy Families Program screened positive on both the first and
second EDPS. The profile of these mothers is described below.
First Language of Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen The first language of mothers with postpartum depression attending the CRHVC
Healthy Families Program who screened positive on both the first and second EDPS is
depicted in Figure 2.
Figure 2. First Language of Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen
First Language of Mothers with Postpartum Depression (Positive 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (N=34)
Arabic, 3, 9%
Farsi, 2, 6%
Other*, 7, 21%
Spanish, 3, 9%
English, 19, 56%
EnglishSpanish
ArabicFarsi
Other*
* includes 1 mother whose first language/cultural background is Albanian, Cantonese, Hindi, Punjabi, Somalian, Tagalog and Vietnamese
23
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Findings and Conclusions
Nineteen (56%) of the 34 mothers with postpartum depression attending the
CRHVC Healthy Families Program who screened positive on both the first and second
EDPS had English as their first language; 15 (44%) of the mothers had a language other
than English as their first language.
Based on the results of this study, we suggest that postpartum depression occurred
in mothers from a wide variety of cultural backgrounds and that its likelihood was
relatively the same in mothers who had English as their first language and mothers
(collectively) whose first language was a language other than English.
Educational Support Provided by Home Visitors to Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen Figure 3 depicts the type/nature of educational support that Home Visitors
provided to mothers attending the CRHVC Healthy Families Program who screened
positive on both the first and second EDPS.
Findings and Conclusions
The Home Visitors provided various kinds of educational support to 28 of 34
(82%) of mothers with postpartum depression attending the CRHVC Healthy Families
Program who screened positive on both the first and second EDPS. The most usual form
of educational support that the CRHVC Home Visitors provided to these mothers was an
educational information package about postpartum depression. This education package
was given to 18 (64%) of the 28 mothers. The next most usual type of support that Home
Visitors gave mothers was educational handouts and articles about postpartum
depression. These materials were given to 6 (21%) of the 28 mothers. The mothers also
24

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
indicated that the CRHVC Home Visitors provided much-appreciated emotional support
and company while providing education and information about postpartum depression.
Figure 3. Educational Support Provided by Home Visitors to Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen
Educational Support Provided by Home Visitors to Mothers withPostpartum Depression (Positive 1st and Positive 2nd Edinburgh Screen)
Attending the CRHVC Healthy Families Program 2005-2007 (N=28)
Self-care Strategies,
1, 4%Video, 2, 7%
PPD Package, 18, 64%
Counseling Information,
1, 4%
Handouts, 6, 21%
Handouts
CounselingInformationPPD Package
Video
Self-careStrategies
Based on the results of this study, we suggest that the most usual type of
educational support that Home Visitors provided for mothers attending the CRHVC
Healthy Families Program who scored positive on both the first and second EDPS was
education and information about postpartum depression. The emotional support offered
by the CRHVC Home Visitors while providing this information was also highly valued
by the mothers.
Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen Figure 4 depicts the type/nature of referrals to community-based postpartum
depression support programs and resources that the Home Visitors made for mothers
25

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
attending the CRHVC Healthy Families Program who screened positive on both the first
and second EDPS.
Figure 4. Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen
Referrals Made by Home Visitors for Mothers with Postpartum Depression (Positive 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (N=53 Referrals for 34 Mothers)
Mental Health Services,
4, 8%
Community Health Nurse, 0, 0%
PPD Program, 36, 67%
Specialist Physician,
0, 0%
Family Doctor, 13, 25%
PPD Program
Family Doctor
Mental HealthServicesCommunityHealth Nurse SpecialistPhysician
Findings and Conclusions
The Home Visitors made 53 referrals to community-based postpartum depression
support programs and resources for the 34 mothers attending the CRHVC Healthy
Families Program who scored positive on the first and second EDPS. Thirty-six (67%) of
the 53 referrals were made to community-based postpartum depression support programs
and resources. Thirteen (25%) of the 53 referrals were made to family physicians.
Based on the results of this study, we suggest that the most usual type of referrals
that Home Visitors made for mothers attending the CRHVC Healthy Families Program
who scored positive on both the first and second EDPS were referrals to community-
based postpartum depression support programs and resources.
26

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen Figure 5 depicts the benefits of Home Visitation from the perspective of mothers
attending the CRHVC Healthy Families Program who screened positive on both the first
and second EDPS.
Figure 5. Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen
Benefits of Home Visitation for Mothers with Postpartum Depression (Positive 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy Families
Program as Reported by Home Visitors (84 Responses by 34 Mothers)
Parenting Skills, 3, 4%
Company, 6, 7%
Self-esteem, 4, 5%
Basic Needs, 4, 5%
Goal Setting, 3, 4%
Advice, 3, 4%
Provide Information***,
10, 12%
Community Referral, 16, 19%Listening,
12, 14%
Same Language, 2, 2%
Support**, 21, 24%
Support
CommunityReferralListening
ProvideInformationAdvice
Company
Self-esteem
Parenting Skills
Basic Needs
Goal Setting
Same Language
**Emotional support (encouragement, understanding and comfort) *** Information about postpartum depression, self-care, coping/stress management Findings and Conclusions
The 34 mothers with postpartum depression attending the CRHVC Healthy
Families Program who screened positive on both the first and second EDPS identified 84
benefits of Home Visitation. The benefit most frequently reported by the mothers was the
emotional support (encouragement, understanding and comfort) provided by the CRHVC
Home Visitors which was identified 21 times (24% of the 84 benefits mentioned).
27

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Mothers also indicated that they valued listening - 12 (14%) of the 84 benefits of Home
Visitation that were mentioned; the company of the CRHVC Home Visitors - 6 (7%) of
the 84 benefits of Home Visitation that were mentioned; and improved self-esteem - 4
(5%) of the 84 benefits of Home Visitation that were mentioned. Collectively, these
“emotional” support benefits provided by the CRHVC Home Visitors accounted for 43
(51%) of the 84 benefits of Home Visitation perceived by mothers.
Community-based referrals were identified 16 times and accounted for 19% of the
84 benefits mentioned. The provision of information (about postpartum depression, self-
care and stress management) was cited as a benefit of Home Visitation by 10 (12%) of
these mothers.
Based on the results of this study, we suggest that mothers with postpartum
depression attending the CRHVC Healthy Families Program who screened positive on
the first and second EDPS believed that the emotional support provided by the CRHVC
Home Visitors and referrals to community-based postpartum depression support
programs and resources were the greatest benefits of attending the CRHVC Healthy
Families Program.
Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen Figure 6 depicts the number of times/frequency of the different risk factors (as a
percentage of all risk factors) that the Home Visitors identified/assessed for mothers
attending the CRHVC Healthy Families Program who screened positive on both the first
and second EDPS.
28

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 6. Frequency of Risk Factors for Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen
Frequency of Risk Factors for Mothers with Postpartum Depression (Positive 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy Families
Program 2005-2007 (60 Risks for 27 Mothers)
Relationship Diff iculties, 14, 23%
Social Isolation, 14, 23%Financial Diff iculties,
6, 10%
Having Other Children, 6, 10%
Health Concerns, 6, 10%
Other*, 5, 8%
Mental Health, Father 2, 3%
Diff icult Baby, 3, 5%
Life Stress, 4, 7%
Relationship Diff iculties
Social Isolation
Financial Diff iculties
Health Concerns
Having Other Children
Life Stress
Diff icult Baby
Mental Health - Father
Other*
* the following risk factors were mentioned 1 time each - 1st time, young mother, legal issues, homeless, past postpartum depression/depression and lack of sleep Findings and Conclusions
The Home Visitors identified/assessed risk factors for 27 (79%) of the 34 mothers
with postpartum depression attending the CRHVC Healthy Families Program who
screened positive on both the first and second EDPS. Sixty risk factors were identified.
Relationship difficulties and social isolation were the most frequently identified risk
factors; each of these risk factors was noted 14 times (23% of the 60 risks mentioned).
Figure 7 depicts the number and percent of the 27 mothers with postpartum
depression who were assessed as having each of the individual risk factors.
29

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 7. Risk Factors for Individual Mothers with Postpartum Depression who Screened Positive on the First and Second Edinburgh Screen
Risk Factors for Individual Mothers with Postpartum Depression (Positive 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy Families
Program 2005-2007 (27 Mothers)
Life Stress, 4, 15%
Difficult Baby, 3, 11%
Mental Health, Father 2, 7%
Other*, 5, 19%
Health Concerns, 6, 22%
Having Other Children, 6, 22%
Financial Difficulties, 6, 22%
Social Isolation, 14, 52%
Relationship Difficulties, 14, 52%
Relationship Difficulties
Social Isolation
Financial Difficulties
Health Concerns
Having Other Children
Life Stress
Difficult Baby
Mental Health - Father
Other*
* the following risk factors were mentioned 1 time each - 1st time, young mother, legal issues, homeless, past postpartum depression/depression and lack of sleep
The CRHVC Home Visitors identified that 14 (52%) of the 27 mothers had risks
relating to each of relationship difficulties and social isolation. Each of financial
difficulties and family health problems were risk factors for 6 (22%) of the 27 mothers.
Based on the results of this study, we suggest that the most usual risks for mothers
with postpartum depression attending the CRHVC Healthy Families Program who scored
positive on both the first and second EDPS were relationship difficulties, social isolation,
financial difficulties and family health problems.
7.1.2. Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Negative on the Second Edinburgh Screen In this study, twenty-nine (22%) of the 130 mothers with postpartum depression
attending the CRHVC Healthy Families Program screened positive on the first and
negative on the second EDPS. The profile of these mothers is described below.
30

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
First Language of Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen The first languages of mothers with postpartum depression attending the CRHVC
Healthy Families Program who screened positive on the first and negative on the second
EDPS are depicted in Figure 8.
Figure 8. First Language of Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen
First Language of Mothers with Postpartum Depression (Positive 1st and Negative 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (N=29)
Amharic, 2, 7%
Other*, 4, 14%
English, 23, 79%
English
Amharic
Other*
* includes 1 mother whose first language/cultural background is Arabic, Afghan, Chinese and Spanish Findings and Conclusions
Twenty-three (79%) of the 29 mothers with postpartum depression attending the
CRHVC Healthy Families Program who screened positive on the first and negative on the
second EDPS had English as their first language; 6 (21%) of the 29 mothers had a
language other than English as their first language.
Based on the results of this study, we suggest that postpartum depression occurred
in mothers from a wide variety of cultural backgrounds and that its likelihood was greater
31
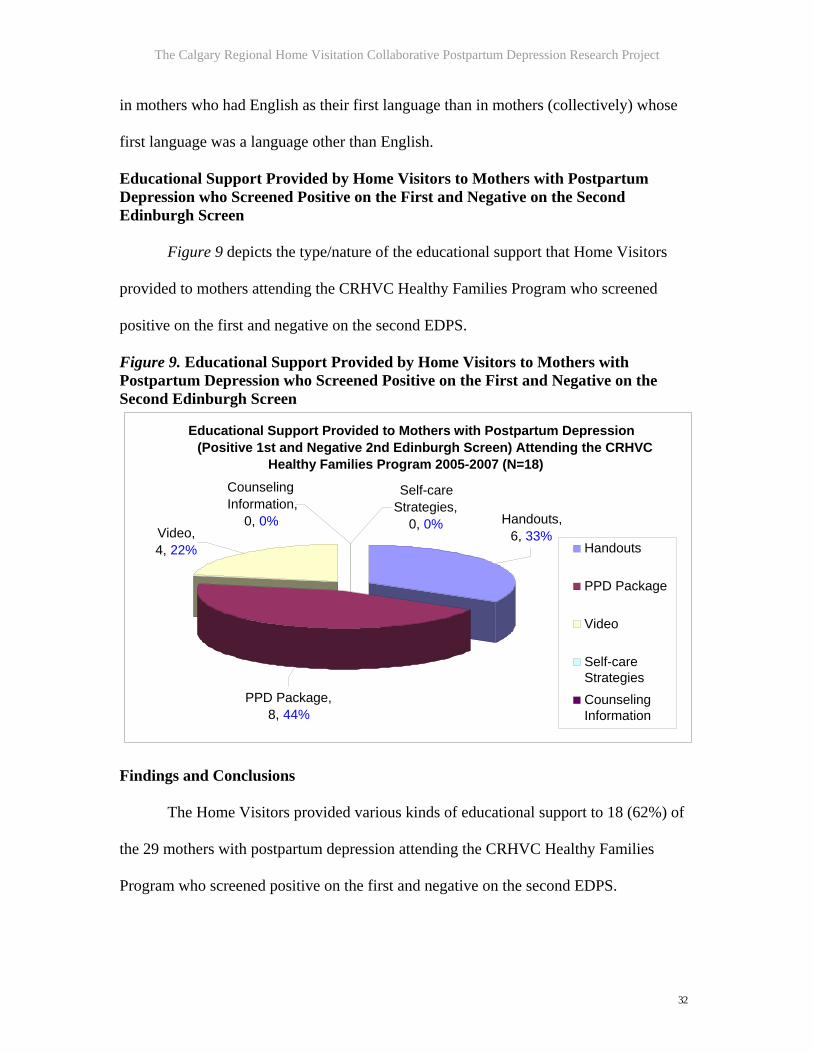
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
in mothers who had English as their first language than in mothers (collectively) whose
first language was a language other than English.
Educational Support Provided by Home Visitors to Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen Figure 9 depicts the type/nature of the educational support that Home Visitors
provided to mothers attending the CRHVC Healthy Families Program who screened
positive on the first and negative on the second EDPS.
Figure 9. Educational Support Provided by Home Visitors to Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen
Educational Support Provided to Mothers with Postpartum Depression (Positive 1st and Negative 2nd Edinburgh Screen) Attending the CRHVC
Healthy Families Program 2005-2007 (N=18)
Video, 4, 22%
PPD Package,8, 44%
Self-care Strategies,
0, 0%
Counseling Information,
0, 0% Handouts, 6, 33%
Handouts
PPD Package
Video
Self-careStrategiesCounselingInformation
Findings and Conclusions
The Home Visitors provided various kinds of educational support to 18 (62%) of
the 29 mothers with postpartum depression attending the CRHVC Healthy Families
Program who screened positive on the first and negative on the second EDPS.
32

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
The most usual form of educational support that the CRHVC Home Visitors
provided to these mothers was an information package about postpartum depression. This
package was given to 8 (44%) of the 18 mothers. The next most usual type of educational
support that Home Visitors provided was handouts and articles about postpartum
depression. These materials were given to 6 (33%) of the 18 mothers. The mothers also
indicated that the CRHVC Home Visitors provided much-appreciated emotional support
and company while providing education and information about postpartum depression.
Based on the results of this study, we suggest that the most usual type of support
that the CRHVC Home Visitors provided for mothers who scored positive on the first and
negative on the second EDPS was education and information about postpartum
depression. The emotional support offered by the CRHVC Home Visitors while
providing this information was also highly valued by the mothers.
Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen Figure 10 depicts the type/nature of referrals to community-based postpartum
depression support programs and resources that Home Visitors made for mothers
attending the CRHVC Healthy Families Program who screened positive on the first and
negative on the second EDPS.
Findings and Conclusions
The Home Visitors made 43 referrals to community-based postpartum depression
support programs and resources for the 29 mothers attending the CRHVC Healthy
Families Program who scored positive on the first and negative on the second EDPS.
Twenty-six (60%) of the 43 referrals were made to community-based postpartum
33

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
depression support programs and resources. Eleven (26%) of the 43 referrals were made
to family physicians.
Figure 10. Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen
Referrals Made by Home Visitors for Mothers with Postpartum Depression (Positive 1st and Negative 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (43 Referrals for 29 Mothers)
Mental Health Program, 5, 12%
Community Health Nurse, 1, 2%
Family Doctor, 11, 26%
Specialist Physician,
0, 0%PDD Program,
26, 60%
Family Doctor
SpecialistPhysicianPPD Program
Mental HealthProgramCommunityHealth Nurse
Based on the results of this study, we suggest that the most usual type of referrals
that the CRHVC Home Visitors made for mothers who scored positive on the first and
negative on the second EDPS were referrals to community-based postpartum depression
support programs and resources. All mothers received at least one referral.
Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen Figure 11 depicts the benefits of Home Visitation from the perspective of mothers
attending the CRHVC Healthy Families Program who screened positive on the first and
negative on the second EDPS.
34

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Findings and Conclusions
The 29 mothers with postpartum depression attending the CRHVC Healthy
Families Program who screened positive on the first and negative on the second EDPS
identified 63 benefits of Home Visitation. The benefit most frequently reported by the
mothers was the emotional support (encouragement, understanding and comfort)
provided by the CRHVC Home Visitors which was identified 27 times (43% of the 63
benefits mentioned). Mothers also indicated that they valued listening - 7 (11%) of the 63
benefits of Home Visitation that were mentioned; the company of the CRHVC Home
Visitors - 6 (10%) of the 63 benefits of Home Visitation that were mentioned; and
improved self-esteem - 3 (5%) of the 63 benefits of Home Visitation that were
mentioned. Collectively, these “emotional” support benefits provided by the CRHVC
Home Visitors accounted for 43 (68%) of the 63 benefits of Home Visitation as perceived
by the mothers. Community-based referrals were identified 8 times and accounted for
13% of the 63 benefits mentioned.
Based on the results of this study, we suggest that mothers with postpartum
depression who screened positive on the first and negative on the second EDPS believed
that the emotional support provided by the CRHVC Home Visitors and referrals to
community-based postpartum depression support programs and resources were the
greatest benefits provided by the CRHVC Healthy Families Program.
35

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 11. Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen
Benefits of Home Visitation for Mothers with Postpartum Depression (Positive 1st and Negative 2nd Edinburgh Screen) Attending the CRHVC Healthy Families
Program as Reported by Home Visitors (63 Responses by 29 Mothers)
Advice, 7, 11%
Other*, 2, 3%
Company, 6, 10%
Self-esteem,3, 5%
Listening, 7, 11%
Provide Information***,
3, 5%Community
Referral, 8, 13%
Support**,27, 43%
Support
Community ReferralListening
ProvideInformationAdvice
Company
Self-esteem
Other*
* Parenting skills and goal setting mentioned 1 time each **Emotional support (encouragement, understanding and comfort) *** Information about postpartum depression, self-care, coping/stress management Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen Figure 12 depicts the number of times/frequency of different risk factors (as a
percent of all risk factors) identified/assessed by Home Visitors for mothers attending the
CRHVC Healthy Families Program who screened positive on the first and negative on the
second EDPS.
Findings and Conclusions
The Home Visitors identified/assessed risk factors for 20 (69%) of the 29 mothers
with postpartum depression attending the CRHVC Healthy Families Program who
screened positive on the first and negative on the second EDPS. The mothers identified
44 risk factors. Relationship difficulties and life stress were the most frequently
36

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
mentioned risk factors; these risks were mentioned 8 times (18% of the 44 risks
mentioned) and 6 times (14% of the 44 risks mentioned) respectively.
Figure 12. Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Positive on the First and Negative on the Second Edinburgh Screen
Frequency of Risk Factors Reported for Mothers with Postpartum Depression (Positive 1st and Negative 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (44 Risks for 20 Mothers)
Difficulties with Baby, 3, 7%
Mental Health -Mother, 3, 7%
Other*,4, 9%
Life Stress, 7, 16%
1st Time young Mother, 3, 7%
Social Isolation, 6, 14%
Financial Difficulties,
4, 9%Health Concerns, 5, 11%
RelationshipDifficulties,
8, 18%Relationship Difficulties
Social Isolation
Financial Difficulties
Health Concerns
Life Stress
1st Time young Mother
Difficulties with Baby Mental Health-Mother Other*
* the following risk factors were mentioned 1 time each - young children, pregnant again and past postpartum depression/depression; involvement with Child Welfare was mentioned 2 times
Figure 13 depicts the number and percent of the 20 mothers who were assessed as
having the individual risk factors. The CRHVC Home Visitors indicated that 8 (40%) and
7 (35%) of the 20 mothers had risks relating to relationship difficulties and life stress
respectively. Social isolation was a risk factor for 6 (30%) mothers while family health
problems were a risk factor for 5 (25%) of the mothers.
Based on the results of this study, we suggest that the most usual risks for mothers
with postpartum depression who scored positive on the first and negative on the second
EDPS were relationship difficulties, life stress, social isolation and financial difficulties.
37

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 13. Identified Risk Factors for Mothers who Screened Positive on the First and Negative on the Second Edinburgh Screen
Identified Risk Factors Reported by Mothers with Postpartum Depression (Positive 1st and Negative 2nd Edinburgh Screen) Attending the CRHVC Healthy Families
Program 2005-2007 (20 Mothers)
Relationship Difficulties,
8, 40%
Health Concerns, 5, 25%
Financial Difficulties,
4, 20%
Social Isolation, 6, 30%
1st Time young Mother, 3, 15%
Life Stress, 7, 35%
Other*, 4, 20%
Mental Health - Mother, 3, 15% Difficulties with
Baby, 3, 15 %
Relationship Difficulties
Social Isolation Financial Difficulties
Health Concerns
Life Stress
1st Time young Mother
Difficulties with Baby Mental Health-Mother
Other*
* the following risk factors were mentioned 1 time each - young children, pregnant again and past postpartum depression/depression; involvement with Child Welfare was mentioned 2 times 7.1.3. Mothers with Postpartum Depression who Screened Negative on the First EDPS and Positive on the Second Edinburgh Screen In this study, fifteen (12%) of the 130 mothers with postpartum depression
attending the CRHVC Healthy Families Program screened negative on the first and
positive on the second EDPS. The demographic profile of these mothers is described
below.
First Language of Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second EDPS The first language of mothers with postpartum depression attending the CRHVC
Healthy Families Program who screened negative on the first and positive on the second
EDPS is depicted in Figure 14.
38

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 14. First Language of Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen
First Language of Mothers with Postpartum Depression (Negative 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (N=15)
Other*, 3, 20%
Urdu, 2, 13%
Arabic, 2, 13%
Punjabi, 2, 13%
English, 6, 41%
English PunjabiArabic UrduOther*
* includes 1 mother whose first language/cultural background is Cantonese, Korean and Mandarin Findings and Conclusions Six (41%) of the 15 mothers with postpartum depression attending the CRHVC
Healthy Families Program who screened negative on the first and positive on the second
EDPS had English as their first language; 9 (60%) of the 15 mothers had a language other
than English as their first language.
Based on the results of this study, we suggest that postpartum depression occurred
in mothers from a wide variety of cultural backgrounds and that it was somewhat less
likely to occur in mothers who had English as their first language than in mothers
(collectively) whose first language was a language other than English.
39

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen Figure 15 depicts the type/nature of referrals that Home Visitors made for
mothers attending the CRHVC Healthy Families Program who screened negative on the
first and positive on the second EDPS.
Figure 15. Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen
Referrals Made by Home Visitors for Mothers with Postpartum Depression (Negative 1st and Positive 2nd Edinburgh Screen) Attending
the CRHVC Healthy Families Program 2005-2007 (7 Referrals for 15 Mothers)
PDD Program, 5, 71%
Community HealthNurse, 0, 0%
Family Doctor, 1, 14%
Specialist Physician,
0, 0%Mental Health Service, 1, 14% Family Doctor
PPD Program
Mental Health Service
Community Health NurseSpecialist Physician
Findings and Conclusions
The Home Visitors made 7 referrals to community-based postpartum depression
support programs and resources for the 15 mothers with postpartum depression attending
the CRHVC Healthy Families Program who scored negative on the first and positive on
the second EDPS. Five (71%) of the 7 referrals were made to community-based
postpartum depression support programs and resources. One referral was made to a
family doctor and one referral was made to community mental health services.
40

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Based on the results of this study, we suggest that the CRHVC Home Visitors
were most likely to make referrals to community-based postpartum depression support
programs and resources for mothers who scored negative on the first and positive on the
second EDPS.
Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen Figure 16 depicts the benefits of Home Visitation from the perspective of mothers
attending the CRHVC Healthy Families Program who screened negative on the first and
positive on the second EDPS.
Figure 16. Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen
Benefits of Home Visititation for Mothers with Postpartum Depression (Negative 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy Families
Program 2005-2007 (29 Responses by 15 Mothers)
Listening, 7, 24%
Other*, 1, 3%
Company, 4, 14%
Goal Setting, 2, 7%
Provide Information***,
2, 7%
Community Referral, 2, 7%
Support**, 11, 38%
Support
CommunityReferralListening
ProvideInformationCompany
Goal Setting
Other
* Program in own language **Emotional support (encouragement, understanding and comfort) *** Information about postpartum depression, self-care, coping/stress management Findings and Conclusions
The 15 mothers with postpartum depression who screened negative on the first
and positive on the second EDPS identified 29 benefits of Home Visitation. The benefit
41

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
most frequently reported by the mothers was the emotional support (encouragement,
understanding and comfort) provided by the CRHVC Home Visitors which was identified
11 times (38% of the 29 benefits mentioned). Mothers also indicated that they valued
listening - 7 (24%) of the 29 benefits of Home Visitation that were mentioned; and the
company of the CRHVC Home Visitors - 4 (14%) of the 29 benefits of Home Visitation
that were mentioned. Collectively, these “emotional” support benefits provided by the
CRHVC Home Visitors accounted for 22 (76%) of the 29 benefits of Home Visitation as
perceived by mothers. Community-based referrals for postpartum depression support
were identified 2 times and accounted for 7% of the 29 benefits mentioned.
Based on the results of this study, we suggest that mothers with postpartum
depression attending the CRHVC Healthy Families Program who screened negative on
the first and positive on the second EDPS believed that the emotional support provided
by the CRHVC Home Visitors and referrals to community-based postpartum depression
support programs (as well as goal setting and the provision of educational materials) were
the greatest benefits of attending the CRHVC Healthy Families Program. Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen Figure 17 depicts the number of times/frequency of different risk factors that the
Home Visitors identified/assessed for mothers attending the CRHVC Healthy Families
Program who screened negative on the first and positive on the second EDPS.
Findings and Conclusions
The Home Visitors identified/assessed risk factors for 9 (60%) of the 15 mothers
with postpartum depression attending the CRHVC Healthy Families Program who
screened negative on the first and positive on the second EDPS. Financial difficulties and
42

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
relationship difficulties were the most usual risks; these were mentioned 4 times (24% of
the 17 risks mentioned) and 3 times (18% of the 17 risks mentioned) respectively.
Figure 17. Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Negative on the First and Positive on the Second Edinburgh Screen
Frequency of Risk Factors Reported by Mothers with Postpartum Depression (Negative 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC Healthy
Families Program 2005-2007 (17 Risks for 9 Mothers)
Social Isolation, 2, 12%
Financial Difficulties,
4, 24%
Having Other Children, 2, 12%
Other*, 6, 34%
Relationship Difficulties,
3, 18%
RelationshipDifficulties SocialIsolationFinancialDifficultiesHaving OtherChildrenOther*
* the following risk factors were mentioned 1 time each - health concerns for mother or baby, life stress, difficulties with infant, homeless, past postpartum depression/depression and Child Welfare involvement
Figure 18 depicts the number and percent of the 9 mothers who were assessed as
having the individual risk factors. The CRHVC Home Visitors identified that 4 (44%) of
the 9 mothers had risks relating to financial difficulties while 3 (33%) of the 9 mothers
had risk factors related to relationship difficulties.
Based on the results of this study, we suggest that the most usual risks for mothers
with postpartum depression attending the CRHVC Healthy Families Program who scored
negative on the first and positive on the second EDPS were financial difficulties and
relationship difficulties.
43
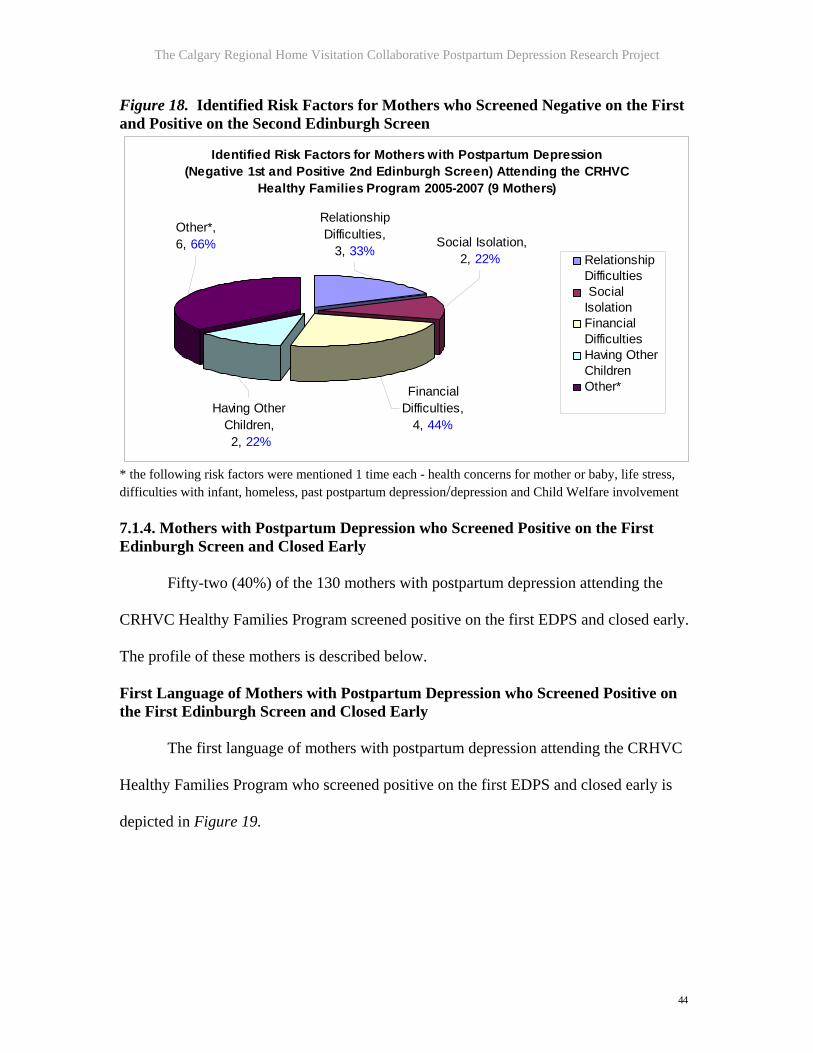
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 18. Identified Risk Factors for Mothers who Screened Negative on the First and Positive on the Second Edinburgh Screen
Identified Risk Factors for Mothers with Postpartum Depression (Negative 1st and Positive 2nd Edinburgh Screen) Attending the CRHVC
Healthy Families Program 2005-2007 (9 Mothers)
Relationship Difficulties,
3, 33%
Other*, 6, 66%
Having Other Children, 2, 22%
Financial Difficulties,
4, 44%
Social Isolation, 2, 22% Relationship
Difficulties SocialIsolationFinancialDifficultiesHaving OtherChildrenOther*
* the following risk factors were mentioned 1 time each - health concerns for mother or baby, life stress, difficulties with infant, homeless, past postpartum depression/depression and Child Welfare involvement 7.1.4. Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early Fifty-two (40%) of the 130 mothers with postpartum depression attending the
CRHVC Healthy Families Program screened positive on the first EDPS and closed early.
The profile of these mothers is described below.
First Language of Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early The first language of mothers with postpartum depression attending the CRHVC
Healthy Families Program who screened positive on the first EDPS and closed early is
depicted in Figure 19.
44

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 19. First Language of Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early
First Language of Mothers with Postpartum Depression (Positive 1st Screen and Early Closure) Attending the CRHVC Healthy Families
Program 2005-2007 (N=52)
Arabic, 8, 15%
Spanish, 3, 6%
Other*, 8, 15%
English, 33, 63%
English
Arabic
Spanish
Other*
* includes 1 mother whose first language/cultural background is Amharic, Hindi, Japanese, Korean, Nuer, Urdu, Other and Vietnamese Findings and Conclusions
Thirty-three (63%) of the 52 mothers attending the CRHVC Healthy Families
Program with postpartum depression who screened positive on the first EDPS and closed
early had English as their first language.
Based on the results of this study, we suggest that postpartum depression occurred
in mothers from a wide variety of cultural backgrounds and that its likelihood was
somewhat greater in mothers who had English as their first language than in mothers
(collectively) whose first language was a language other than English.
Educational Support Provided by Home Visitors to Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early Figure 20 depicts the type/nature of the educational support that the Home
Visitors provided to mothers attending the CRHVC Healthy Families Program who
screened positive on the first EDPS and closed early.
45

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 20. Educational Support Provided by Home Visitors to Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early
Educational Support Provided by Home Visitors to Mothers withPostpartum Depression (Positive 1st Screen and Early Closure)
Attending the CRHVC Healthy Families Program 2005-2007 (N=34)
Video, 6, 18%
Self-care Strategies,
0, 0%
Counseling Information,
0, 0%
Handouts, 6, 18% PPD Package,
22, 65%
PPD Package
Handouts
Video
Self-careStrategiesCounselingInformation
Findings and Conclusions
The Home Visitors provided various kinds of educational support to 34 (65%) of
the 52 mothers with postpartum depression attending the CRHVC Healthy Families
Program who screened positive on the first EDPS and closed early. The most usual form
of educational support was an information package about postpartum depression which
was given to 22 (65%) of the 34 mothers. Handouts about postpartum depression were
given to 6 (18%) of the mothers. In addition to these education materials, the mothers
also indicated that the CRHVC Home Visitors provided much-appreciated emotional
support and company at the time of visiting.
Based on the results of this study, we suggest that the provision of an information
package about postpartum depression was the most usual type of educational support that
the Home Visitors provided for mothers attending the CRHVC Healthy Families Program
46

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
who scored positive on the first EDPS and closed early. The emotional support offered by
the CRHVC Home Visitors while providing this information was also highly valued by
the mothers.
Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early Figure 21 depicts the type/nature of referrals to community-based postpartum
depression support programs and resources that the Home Visitors made for mothers
attending the CRHVC Healthy Families Program who screened positive on the first
EDPS and closed early.
Figure 21. Referrals Made by Home Visitors for Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early
Referrals Made by Home Visits for Mothers with Postpartum Depression (Positive 1st Screen and Early Closure) Attending the CRHVC Healthy
Families Programs 2005-2007 (N=73 Referrals for 52 Mothers)
Specialist Physician,
1, 1% Community
Health Nurse, 1, 1%
Mental Health Services,12, 16%
Family Doctor, 17, 23% PPD Program,
42, 58%
PPD Program
Family Doctor
Mental Health ServicesSpecialist Physician
Community HealthNurse
Findings and Conclusions
The Home Visitors made 73 referrals to community-based postpartum depression
support programs and resources for the 52 mothers with postpartum depression attending
the CRHVC Healthy Families Program who screened positive on the first EDPS and
47

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
closed early. Forty-two (58%) of the 73 referrals were made to community-based
postpartum depression support programs. Seventeen (23%) of the 73 referrals were made
to family doctors.
Based on the results of this study, we suggest that referrals to community-based
postpartum depression support programs and resources were the most likely type of
referral that the Home Visitors made for mothers attending the CRHVC Healthy Families
Program who screened positive on the first EDPS and closed early.
Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early Figure 22 depicts the benefits of Home Visitation programs from the perspective
of mothers attending the CRHVC Healthy Families Program who screened positive on
the first EDPS and closed early.
Figure 22. Benefits of Home Visitation for Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early
Benefits of Home Visitation for Mothers with Postpartum Depression (Positive 1st Screen and Early Closure) Attending the CRHVC Healthy Families Program
2005-2007 as Reported by Home Visitors (83 Responses by 34 Mothers)
Support**, 21, 26%
Community Referral, 15, 18%Listening,
10, 12%Provide Information***,
9, 11%
Advice, 7, 8%
Self-esteem, 4, 5%
Other*, 2, 2%
Basic Needs, 7, 8%
Company, 4, 5%
Parenting Skills, 4, 5%
Support
CommunityReferralListening
ProvideInformationAdvice
Basic Needs
Self-esteem
Parenting Skills
Company
Other*
…
* Planning/goal setting and service in same cultural background mentioned 1 time each **Emotional support (encouragement, understanding and comfort) *** Information about postpartum depression, self-care, coping/stress management
48

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Findings and Conclusions
The 34 mothers with postpartum depression attending the CRHVC Healthy
Families Program who screened positive on the first EDPS and closed early identified 83
benefits of Home Visitation. The benefit most frequently reported by the mothers was the
emotional support (encouragement, understanding and comfort) provided by the CRHVC
Home Visitors which was identified 21 times (26% of the 83 benefits mentioned)
Mothers also indicated that they valued listening - 10 (12%) of the 83 benefits of Home
Visitation that were mentioned; the company of the CRHVC Home Visitors - 4 (5%) of
the 83 benefits of Home Visitation that were mentioned; and improved self-esteem - 4
(5%) of the 83 benefits of Home Visitation that were mentioned. Collectively, these
“emotional” support benefits provided by the CRHVC Home Visitors accounted for 39
(47%) of the 83 benefits of Home Visitation as perceived by mothers. Community-based
referrals were identified 15 times and accounted for 18% of the 83 benefits mentioned.
Based on the results of this study, we suggest that mothers with postpartum
depression attending the CRHVC Healthy Families who screened positive on the first
EDPS and closed early believed that the emotional support provided by the CRHVC
Home Visitors and referrals to community-based support programs and resources were
the greatest benefits of attending the CRHVC Healthy Families Program.
Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early Figure 23 depicts the number of times/frequency of different risk factors that
Home Visitors identified/assessed for mothers attending the CRHVC Healthy Families
Program who screened positive on the first EDPS and closed early.
49

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 23. Frequency of Risk Factors Reported by Mothers with Postpartum Depression who Screened Positive on the First Edinburgh Screen and Closed Early
Frequency of Risk Factors Reported by Mothers with Postpartum Depression (Positive 1st Edinburgh Screen and Early Closure) Attending the CRHVC Healthy
Families Program 2005-2007 (55 Risks for 32 Mothers)
Other*, 3, 5%
Life Stress, 5, 9%
Past PPD Depression,
4, 7%
Financial Difficulties,
9, 16%
Health Concerns, 3, 5%
Relationship Difficulties,
13, 24%
Social Isolation, 15, 27%Mental Health -
Mother, 3, 5%
Social Isolation
RelationshipDifficultiesFinancialDifficultiesLife Stress
Past PPDDepression Health Concerns
Mental Health -MotherOther*
* the following risk factors mentioned 1 time each – young mother/pregnant again, homeless and Child Welfare involvement Findings and Conclusions The Home Visitors identified/assessed risk factors for 32 (62%) of the 52 mothers
with postpartum depression attending the CRHVC Healthy Families Program who
screened positive on the first EDPS and closed early. A total of 55 risk factors were
identified. Social isolation and relationship difficulties were the most frequently
mentioned risk factors; these risks were mentioned 15 times (27% of the 55 risks
mentioned) and 13 times (24% of the 55 risks mentioned) respectively. Financial
difficulties accounted for 9 (16%) of the mothers’ risk factors.
Figure 24 depicts the number and per cent of the 32 mothers who were assessed
as having the individual risk factors. Home Visitors identified that 15 (47%) of the 32
50

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
mothers had risks relating to social isolation. Relationship difficulties and financial
difficulties were risk factors for 13 (41%) and 9 (28%) of the 32 mothers respectively.
Figure 24. Identified Risk Factors for Mothers who Screened Positive on the First Edinburgh Screen and Closed Early
Identified Risk Factors Reported by Mothers with Postpartum Depression(Positive 1st Edinburgh Screen and Early Closure) Attending the CRHVC Healthy
Families Program 2005-2007 (55 Risks for 32 Mothers)
Mental Health -Mother,3, 9%
Social Isolation,15, 47%
Relationship Difficulties,
13, 41%
Health Concerns,3, 9%
Financial Difficulties,
9, 28%
Past PPD Depression,
4, 13%
Life Stress, 5, 16%
Other*, 3, 9%
Social Isolation
RelationshipDifficulties FinancialDifficultiesLife Stress
Past PPDDepression Health Concerns
Mental Health -MotherOther*
Based on the results of this study, we suggest that the most usual risks for mothers
with postpartum depression attending the CRHVC Healthy Families Program who scored
positive on the first EDPS and closed early were social isolation, relationship difficulties
and financial difficulties.
Early Closure Factors Figure 25 depicts the reasons for mothers’ early closure from the CRHVC
Healthy Families Program.
Findings and Conclusions
The Home Visitors assessed early closure factors for 9 (17%) of the 52 mothers
with postpartum depression attending the CRHVC Healthy Families Program who
screened positive on the first EDPS and closed early. Financial difficulties accounted for
51

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
3 (27%) of the early closure factors. Information was generally not available for the other
mothers primarily because of their early closure.
Figure 25. Early Closure Factors for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007
Early Closure Factors - Mothers with Postpartum Depression (Positive 1st Screen and Early Closure) Attending the CRHVC Healthy Families
Program 2005-2007 (N=9) Other*, 4, 37%
Moved, 2, 18%
No Support from Baby's Father,
2, 18%
Financial Difficulties,
3, 27%
Financial Difficulties
No Support fromBaby's Father
Moved
Other*
* Relationship difficulties, hospitalization, lost contact and lost custody were each mentioned 1 time
Based on the results of this study, we suggest that financial difficulties were the
most likely factors that caused mothers with postpartum depression to have early closure
from the CRHVC Healthy Families Program. Further targeted studies are suggested.
8. Consolidated Findings and Conclusions
The CRHVC Home Visitors took an active role in the CRHVC 2005-2007
Postpartum Research Project and returned the completed data sheets to the CRHVC
Research Assistant in a timely manner. In general, the quality and quantity of the
information that they were able to collect was excellent. Clearly, this finding is a
reflection of the trusting relationship that the CRHVC Home Visitors had established
with the mothers.
52

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
The findings of the CRHVC 2005-2007 Postpartum Depression Project as
depicted in Figures 2-24 are summarized in Tables 4, 5 and 6.
Table 4. Demographic Profile of Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 and Support/Referrals Offered by Home Visitors Categories
of Mothers
No. Mothers
Postpartum Support Prior to Home
Visitor*
First Language
of Mothers
Age of Mother
(Average/ Range)
Educational Support and Information Provided by
Home Visitors
Referrals Made by Home Visitors
Mothers with Positive 1st and Positive 2nd EDPS
34 Meds - 2 Counseling - 1 Both - 6
English -19 Arabic - 3 Spanish - 3 Farsi - 2 Other - 7 **
Average - 29 Range - 20-43
PPD Pack -18 Handouts - 6 Video - 2 Counseling Info -1 Self-care Info - 1
Family Doctor - 13 Specialist Physician - 0 Postpartum Support - 36 Mental Health Service - 4 Community Nurse - 0
Mothers with Positive 1st and Negative 2nd EDPS
29 Meds - 3 Counseling - 0 Both - 1
English - 23 Amharic - 2 Other - 4 ***
Average - 28 Range - 19-42
PPD Pack - 8 Handouts - 6 Video - 4 Counseling Info -0 Self-care Info - 0
Family Doctor - 11 Specialist Physician - 0 Postpartum Support - 26 Mental Health Service - 5 Community Nurse - 1
Mothers with Negative 1st and Positive 2nd EDPS
15 Information not available
English - 6 Arabic - 2 Punjabi - 2 Urdu - 2 Other - 3****
Average - 30 Range - 20-43
Information not available
Family Doctor - 1 Specialist Physician - 0 Postpartum Support - 5 Mental Health Service - 1 Community Nurse - 0
Mothers with Positive 1st Screen and Early Closure
52 Meds - 3 Counseling - 0Both - 1
English -33 Arabic - 8 Spanish - 3 Other - 8 *****
Average - 30 Range - 19-43
PPD Pack -22 Handouts - 6 Video - 6 Counseling Info - 0 Self-care Info - 0
Family Doctor - 17 Specialist Physician - 1 Postpartum Support - 42 Mental Health Service - 12 Community Nurse - 1
All Mothers with Postpartum Depression
130 Meds - 8 Counseling - 1 Both - 8*
English - 81 Arabic - 14 Spanish - 7 Amharic - 3 Urdu - 3 Punjabi -3 Other -19******
Average - 30 Range- 19-43
PPD Pack - 48 Handouts - 18 Video - 12 Counseling Info -1 Self-care Info - 1
Family Doctor - 42 Specialist Physician - 1 Postpartum Support - 109 Mental Health Service - 22 Community Nurse - 2
*Based on admission information for 67 mothers **Other - 1 mother with first language Albanian, Cantonese, Hindi, Punjabi, Somalian, Tagaloog, and Vietnamese *** Other – 1 mother with first language Arabic, Afhgan, Chinese and Spanish **** Other - 1 mother with first language Cantonese, Korean and Mandarin ***** Other - 1 mother with first language Amharic, Hindi, Japanese, Korean, Nuer, Urdu, Vietnamese and unknown ****** Other 19 mothers (2 mothers with first language Cantonese, Farsi, Vietnamese, Korean, Hindi, and 1 mother with first language Albanian, Somalian, Mandarin, Japanese, Nuer, Afhghan, Tagaloog and unknown)
53

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 4 summarizes the interventions used by other health professionals to treat
the mothers’ postpartum depression prior to their referral to the CRHVC Healthy
Families Program. The mothers provided this information to the CRHVC Home Visitors.
It was beyond the scope of the CRHVC 2005-2007 Postpartum Depression Research
Project to ascertain the duration of these treatments and/or their relative effectiveness in
decreasing the mothers’ postpartum depression.
Table 4 also summarizes: the demographic profile of mothers with postpartum
depression attending the CRHVC Healthy Families Program; the educational support
offered to the mothers by the CRHVC Home Visitors and; referrals made to community-
based postpartum depression support programs and resources for the mothers.
8.1 Interventions for Postpartum Depression Prior to the Mothers’ Admission to the CRHVC Healthy Families Program
Information regarding interventions used to treat mothers with postpartum
depression prior to their referral to the CRHVC Healthy Families Program was available
for 67 mothers (this information was not requested during the earlier part of the study
thus accounting for the lesser amount of information for this question). Seventeen (25%)
of the 67 mothers who screened positive for postpartum depression had received prior
treatment(s), most notably medication or a combination of medication and counseling.
Based on the results of this study, we suggest that approximately 25% of mothers
received treatment for postpartum depression prior to their admission to the CRHVC
Healthy Families Program and that the intervention was most likely to be medication
and/or counseling.
54

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
8.2. First Language of Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program As detailed in Table 4, 81 (62%) of the 130 mothers with postpartum depression
attending the CRHVC Healthy Families Program had English as their first language. The
next two most common first languages were Arabic, 14 (11%) and Spanish, 7 (5%) of the
130 mothers respectively.
Based on the results of this study, we suggest that postpartum depression affected
mothers from a wide variety of cultures and that approximately 60% of the mothers with
postpartum depression attending the CRHVC Healthy Families Program had English as
their first language with the remaining 40% of mothers having a variety of languages as
their first language.
8.3. Ages of Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program As detailed in Table 4, the average age of mothers with postpartum depression
attending the CRHVC Healthy Families Program was 30 years (range 19-43 years).
Based on the results of this study, we suggest that mothers of all ages attending
the CRHVC Healthy Families Program and notably women in their twenties and thirties
were susceptible to having postpartum depression. It is important to note that young
mothers (< 19 years of age) received support from other Calgary organizations that have
a mandate to help young mothers.
8.4. Educational Support and Information Provided by Home Visitors to Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program As detailed in Table 4, the CRHVC Home Visitors provided educational support
in the form of an information package or articles/handouts/video about postpartum
55

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
depression to 78 (60%) of the 130 mothers with postpartum depression. The level of
support with respect to counseling and self-care strategies was minimal.
Based on the results of this study, we suggest that 60% of the mothers attending
the CRHVC Healthy Families Program received some form of educational material about
postpartum depression. The most usual form of educational support that the CRHVC
Home Visitors provided to mothers was an information package about postpartum
depression.
8.5. Referrals Made by Home Visitors for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program As detailed in Table 4, the CRHVC Home Visitors made 176 referrals for the 130
mothers attending the CRHVC Healthy Families Program. The CRHVC Home Visitors
were most likely to make referrals to community-based postpartum depression support
programs and resources; 109 (62%) of the 176 referrals were made to these programs.
Forty-two (24%) of the 176 referrals were made to family physicians; twenty-two (13%)
of the referrals were made to community-based mental health programs. The number of
referrals to specialist physicians and community nurses was minimal.
Based on the results of this study, we suggest that the CRHVC Home Visitors
were most likely to refer mothers attending the CRHVC Healthy Families Program to
community-based postpartum depression support programs and resources.
9.0 Benefits of Home Visitation as Perceived by Mothers with Postpartum Depression Attending CRHVC Healthy Families Program 2005-2007 and Reported to Home Visitors The Home Visitors asked mothers with postpartum depression about the benefits
that they experienced from participating in the CRHVC Healthy Families Program. Table
56

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
5 summarizes the mothers’ perceptions about the benefits of attending the CRHVC
Healthy Families Program.
Table 5. Benefits of Home Visitation as Mentioned by Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 and Reported to Home Visitors Benefits of Home Visitation as Reported by Mothers to Home Visitors
Mothers with Positive 1st and
Positive 2nd EDPS (N=34 Mothers)
Mothers with Positive 1st and
Negative 2nd EDPS
(N=29 Mothers)
Mothers with Negative 1st and Positive
2nd EDPS (N=15
Mothers)
Mothers with Positive 1st Screen and
Early Closure (N=52
Mothers)
All Mothers with
Postpartum Depression
(N=130 Mothers)
Emotional Support and Encouragement*
21 (25%) 27 (42%) 11 (38%) 21 (25%) 80 (31%)
Referrals to Community Resources
16 (19%) 8 (13%) 2 (7%) 15 (18%) 41 (16%)
Opportunity to Speak with Home Visitor/Listening
12 (14%) 7 (11%) 7 (24%) 10 (12%) 36 (14%)
Provision of Information about Postpartum Depression
10 (12%) 3 (5%) 2 (7%) 9 (11%) 24 (9%)
Company of the CRHVC Home Visitor
6 (7%) 6 (10%) 4 (14%) 4 (5%) 20 (8%)
Increased Self-esteem/Confidence
4 (5%) 3 (5%) 0 (0%) 4 (5%) 11 (4%)
Basic Needs Support
4 (5%) 0 (0%) 0 (0%) 7 (8%) 11 (4%)
Support and Advice
3 (4%) 7 (11%) 0 (0%) 7 (8%) 17 (7%)
Learned Parenting Skills
3 (4%) 2 (3%) 0 (0%) 4 (5%) 8 (3%)
Support with Goal Setting
3 (4%) 0 (0%) 2 (7%) 1 (1%) 6 (2%)
Service in Mother’s First Language
2 (2%) 0 (0%) 1 (3%) 1 (1%) 4 (2%)
Total Number of Benefits Mentioned
84 63 29 83 258
**Emotional support (encouragement, understanding and comfort)
57

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Emotional Support Benefits of Participation in the CRHVC Healthy Families Program
The 130 mothers in this study attending the CRHVC Healthy Families Program
reported a variety of benefits that related to their interaction with the Home Visitors; the
support benefits relating to emotional support for the mothers included:
Emotional support (encouragement, understanding and comfort) accounted for 80 (31%) of the 258 benefits mentioned by the mothers
Listening accounted for 36 (14%) of the 258 benefits mentioned by the mothers Providing company accounted for 20 (8%) of the 258 benefits mentioned by the
mothers Improvement in self-esteem accounted for 11 (4%) of the 258 benefits
mentioned by the mothers
Collectively, these benefits, which, overall reflected the emotional support provided
by the CRHVC Home Visitors accounted for 147 (57%) of the 258 benefits identified by
mothers attending the CRHVC Healthy Families Program.
Other Benefits of Participation in the CRHVC Healthy Families Program
The 130 mothers in this study reported a variety of ways in which they benefited from
participating in the CRHVC Healthy Families Program; the benefits relating to
educational/information support, community-based referrals and other support included:
Referrals to community-based postpartum depression support programs and resources accounted for 41 (16%) of the 258 benefits mentioned by the mothers
Information relating to postpartum depression accounted for 24 (9%) of the 258 benefits mentioned by the mothers
Advice, parenting skills information, assistance with basic needs, help with goal setting and service in the same language accounted for 46 (18%) of the 258 benefits mentioned by the mothers
Based on the results of this study, we suggest that the greatest benefits
experienced by mothers attending the CRHVC Healthy Families Program were the
emotional support provided by the CRHVC Home Visitors and referrals to community-
based postpartum depression support programs and resources.
58

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
10. Risk Factors Identified by Home Visitors for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007
Home Visitors identified 175 risk factors for 88 of the mothers with postpartum
depression attending the CRHVC Healthy Families Program. Table 6 summarizes the
number and percent of the mothers’ risk factors
Table 6. Risk Factors Identified by Home Visitors for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007
Postpartum Depression Risk Factor as
Identified by Mother to Home Visitor
Mothers with Positive 1st and
Positive 2nd EDPS (N=27
Mothers)
Mothers with Positive 1st and
Negative 2nd EDPS
(N=20 Mothers)
Mothers with Negative 1st
and Positive 2nd EDPS
(N=9 Mothers)
Mothers with Positive 1st and
EDPS and Early Closure
(N=32 Mothers)
All Mothers with
Postpartum Depression
(N=88 Mothers)
Relationship Difficulties 14 (23 %) 8 (19 %) 3 (18 %) 13 (25%) 38 (22 %) Social Isolation/Lack of Support
14 (23 %) 6 (14 %) 2 (12 %) 15 (28%) 37 (21 %)
Financial Difficulties 6 (10 %) 4 (9 %) 4 (24 %) 9 (16%) 23 (13 %) Health Concerns - Mother/ Baby
6 (10 %) 5 (12 %) 1 (6 %) 3 (5%) 15 (9 %)
Life Stress 4 (7 %) 7 (16 %) 1 (6 %) 5 (9%) 17 (10 %) Young Mother/Pregnant Again
6 (10 %) 1 (2 %) 2 (12 %) 1 (negligible) 10 (6 %)
Difficulties with Baby 3 (5 %) 3 (7 %) 1 (6 %) - 7 (4 %) 1st Time mother/Young Mother
1 (2 %) 3 (7 %) 0 (0 %) - 4 (2 %)
Past Postpartum Depression/Depression
1 (2 %) 1 (2 %) 1 (6 %) 4 (7%) 7 (4 %)
Mental Health Issues – Mother
0 (0 %) 3 (7 %) 0 (0 %) 3 (5%) 6 (3%)
Child Welfare Involvement
0 (0 %) 2 (5 %) 1 (6 %) 1 (negligible) 4 (2%)
Homeless 1 (2 %) 0 (0 %) 1 (6 %) 1 (negligible) 3 (2 %) Mental Health Issues – Father
2 (3 %) 0 (0 %) 0 (0 %) - 2 (0.5 %)
Lack of Sleep 1 (2 %) 0 (0 %) 0 (0 %) - 1 (0.5 %) Legal Issues 1 (2 %) 0 (0 %) 0 (0 %) - 1 (0.5 %) Total Risk Factors Mentioned
60 43 17 55 175
The most significant risk factor for mothers with postpartum depression attending
the CRHVC Healthy Families Program was relationship difficulties which accounted for
38 (22%) of the 175 risk factors. Social isolation and financial difficulties were the next
59

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
most frequently mentioned risk factors; these risks accounted for 37 (21%) and 23 (13%)
of the 175 risk factors respectively. The least mentioned risks for the mothers in this
study were the fathers’ mental health issues, homelessness, lack of sleep and legal issues.
Based on the results of this study, we suggest that the most usual risk factors for
mothers with postpartum depression attending the CRHVC Healthy Families Program
were relationship difficulties, financial difficulties and social isolation.
11. Barriers to Attendance at Community-Based Based Support Programs for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 The Home Visitors asked mothers attending the CRHVC Healthy Families
Program about various factors that influenced them to attend /not attend community-
based postpartum depression support programs and resources. The factors included
distance from the referral location, lack of transportation, program costs, language
concerns, lack of childcare, waitlist issues, type/nature of support provided by the
program or no perceived benefit of attending the program. The mothers were also asked
to identify additional factors which influenced their decision to attend/ not attend
community-based postpartum depression support programs and resources.
Tables 7 to 9 summarize the factors that were/were not barriers to the mothers’
attendance at community-based support services and resources. Table 7 deals with
mothers’ perceptions about barriers to their attendance at postpartum depression support
programs and resources. Tables 8 and 9 summarize mothers’ perceptions about barriers to
their attendance at the family doctor and community-based mental health programs
respectively.
60

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 7. Barriers Experienced by Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 Relating to Attendance at Community-based Postpartum Depression Support Programs
Barriers that Could Affect Mothers
Attendance
Positive 1st and Positive 2nd
EDPS*
Positive 1st and Negative 2nd EDPS **
Positive 1st EDPS and
Early Closure***
All Mothers (N=61 Mothers)
Barrier Barrier Barrier Barrier Yes No Yes No Yes No Yes No
Distance from Referral
7 6 3 2 10 5 20 13
Limited Transportation
5 6 6 1 11 5 22 12
Costs of Attending 2 8 - 2 4 9 6 19 Language Concerns 3 8 2 3 10 9 15 20 Lack of Childcare 8 6 3 2 7 4 18 12 Waitlist Issues 1 5 - 2 4 4 5 11 Type of Support 4 5 3 - 4 4 11 9 No Perceived Benefit 11 4 5 1 4 4 20 9 Other 7 - 4 - 8 - 19 0 Totals 48 48 26 13 62 44 136 105
* 21 Mothers ** 12 Mothers *** 28 Mothers Table 8. Barriers Experienced by Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 Relating to Attendance at the Family Doctor
Barriers that Could Affect Mothers
Attendance
Positive 1st and Positive 2nd EDPS*
Positive 1st and Negative 2nd EDPS**
Positive 1st EDPS and
Early Closure***
All Mothers (N=20 Mothers)
Barrier Barrier Barrier Barrier Yes No Yes No Yes No Yes No Distance from Referral 1 4 - 1 1 3 2 8 Limited Transportation 1 3 - 1 1 4 2 8 Costs of Attending - 4 - 1 - 4 0 9 Language Concerns 1 3 - 1 2 3 3 7 Lack of Childcare 3 2 2 - 2 3 7 5 Waitlist Issues 3 1 - - 1 3 4 4 Type of Support 1 2 - - 1 2 2 4 No Perceived Benefit 2 4 - 2 3 2 5 8 Other 1 - - - 1 1 2 1 Totals 13 23 2 6 12 25 27 54
* 8 Mothers ** 3 Mothers *** 9 Mothers
61

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 9. Barriers Experienced by Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 Relating to Attendance at Community-based Mental Health Programs
Barriers that Could
Affect Mothers Attendance
Positive 1st and Positive 2nd EDPS*
Positive 1st and Negative 2nd EDPS**
Positive 1st EDPS and
Early Closure***
All Mothers (N=9 Mothers)
Barrier Barrier Barrier Barrier Yes No Yes No Yes No Yes No Distance from Referral
2 - - - 1 1 3 1
Limited Transportation
1 - 1 - 1 2 3 2
Costs of Attending 1 1 - - 1 1 2 2 Language Concerns - 2 - - 1 1 1 3 Lack of Childcare 2 - 1 - 1 - 4 0 Waitlist Issues 1 - - - 2 1 3 1 Type of Support 2 - - - 1 1 3 1 No Perceived Benefit 1 1 - - - 2 1 3 Other - - - - 1 - 1 0 Totals 10 4 2 0 9 9 21 13
* 2 Mothers ** 1 Mother *** 6 Mothers Findings and Conclusions
Based on the information in Tables 7 to 9, we suggest that the most usual barriers
to mothers’ attendance at community-based postpartum depression programs and
resources for mothers with postpartum depression were lack of childcare, limited
transportation and no perceived benefit from attending the program. The factors least
likely to be barriers for the mothers with postpartum depression were program costs and
the language of the program.
Figure 26 provides a summary of the information detailed in Tables 7 to 9 with
respect to whether various factors were/were not barriers to attendance at community-
based postpartum support programs and resources, family doctors and mental health
services for mothers with postpartum depression attending the CRHVC Healthy Families
Program.
62

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 26. Barriers to Attendance at all Community-based Programs and Resources Offering Support to Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007
Barriers to Attendance at Community-Based Support Programs for Mothers with Postpartum Depression Attending the CRHVC
Healthy Families Program 2005-2007
2527
8
19
29
1216
26
2122 22
30 30
1614
20
1
17
0
5
10
15
20
25
30
35
Distance from Resource
Limited Transportation
Program Cost
Language of Program
Lack of Childcare
WaitlistedType of Support
No Perceived Benefit
Other
Barriers to Mothers' Attendance
Num
ber o
f Mot
hers
* Community-based postpartum depression support programs, family doctors and mental health services Consolidated Findings and Conclusions - Individual Barriers to Attendance at Community-based Postpartum Depression Support Programs and Resources The CRHVC Home Visitors asked the mothers if certain factors were/were not
barriers to their attendance at community-based postpartum depression support programs
and resources. The findings for these factors - distance from the resource, limited
transportation, program cost, language of program, lack of childcare, waitlist issues,
type/nature of support provided by the program, no perceived benefit of attending the
program or other factors are summarized in the following sections.
Distance from the Resource as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Forty-seven mothers provided information about whether distance from the
resource was/was not a barrier to attendance at support programs. Twenty-five (53%) of
63

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
the 47 mothers considered distance from the resource to be a barrier to attendance while
22 (47%) of the 47 mothers did not consider distance from the resource to be a barrier.
Limited Transportation as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Forty-nine mothers provided information about whether limited transportation
was/was not a barrier to attendance at support programs. Twenty-seven (55%) of the 49
mothers considered distance from the resource to be a barrier to attendance while 22
(45%) of the 49 mothers did not consider limited transportation to be a barrier.
Program Cost as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Thirty-eight mothers provided information about whether program cost was /was
not a barrier to attendance at support programs. Eight (21%) of the 38 mothers considered
program cost to be a barrier to attendance while 30 (79%) of the 38 mothers did not
consider program cost to be a barrier.
Language as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Forty-nine mothers provided information about whether language was /was not a
barrier to attendance at support programs. Nineteen (39%) of the 49 mothers considered
language to be a barrier to attendance while 30 (61%) of the 49 mothers did not consider
language to be a barrier.
Lack of Childcare as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Forty-four mothers provided information about whether lack of childcare was/was
not a barrier to attendance at support programs. Twenty-nine (63%) of the 46 mothers
64

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
considered lack of child care to be a barrier to attendance while 17 (37%) of the 46
mothers did not consider lack of child care to be a barrier.
Waitlist as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Twenty-eight mothers provided information about whether waitlist was /was not a
barrier to attendance at support programs. Twelve (43%) of the 28 mothers considered
waitlist to be a barrier to attendance while 16 (57%) of the 28 mothers did not consider
waitlist to be a barrier.
Type/Nature of Support as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Thirty mothers provided information about whether the type/nature of support
was/was not a barrier to attendance at support programs. Sixteen (53%) of the 30 mothers
considered the type/nature of support offered by the program to be a barrier to attendance
while 14 (47%) of the 30 mothers did not consider the type/nature of support to be a
barrier.
No Perceived Benefit of the Attending the Program as a Barrier to Attendance at Community-based Postpartum Depression Support Programs and Resources Forty-six mothers provided information about whether lack of a perceived benefit
of attending the program was/was not a barrier to attendance at support programs.
Twenty-six (57%) of the 46 mothers considered no perceived benefit of attending the
program to be a barrier to attendance while 20 (43%) of the 46 mothers did not consider
no perceived benefit of attending the program to be a barrier.
65

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Other Barriers to Attendance at Community-based Postpartum Depression Support Programs and Resources Twenty-three mothers provided information about other factors that were /were
not barriers to attendance at community-based postpartum depression support programs
and resources. Twenty-two (96%) of the 23 mothers identified an additional barrier to
attendance at community-based programs while 1 (4%) of the mothers did not identify
any other barriers. The mothers reported a wide variety of barriers and none of the
barriers was mentioned more than two times.
Table 10 ranks the individual factors in terms of whether they were/were not a
barrier to attendance at community-based postpartum depression support programs and
resources.
Table 10. Opinions of Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 about Barriers to Attendance at all Community-based Postpartum Depression Support Programs and Resources
Barriers that Could Affect Mothers
Attendance
Number of Mothers who Responded
Number and Percent of Mothers who Perceived the
Factor to be a Barrier*
Number and Percent of Mothers who Perceived the Factor Not to be a
Barrier Lack of Childcare 46 29(63%) 17(37%) No Perceived Benefit from Attending
46 26(57%) 20(43%)
Limited Transportation
49 27(55%) 22(45%)
Type of Support 30 16(53%) 14(49%) Distance from Referral 47 25(53%) 22(47%) Waitlist Issues 28 12(43%) 16(57%) Language Concerns 49 19(39%) 30(61%) Costs of Attending 38 8(21%) 30(79%) Other 23 22(96%) * 1(4%)
*19 different barriers mentioned 1-2 times each Based on the results of this study, we suggest that mothers with postpartum
depression attending the CRHVC Healthy Families Program experienced various barriers
to attendance at community-based postpartum depression support programs and
66

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
resources. Lack of a perceived benefit to attending the program and child care or
transportation issues were the most notable barriers for the mothers.
It was beyond the scope of the CRHVC 2005-2007 Postpartum Depression
Research Project to study: the benefits experienced by mothers from attending the
community-based postpartum depression support programs and resources; the duration of
their attendance at these programs and reasons for attrition and; the impact of attendance
on the course of the mothers’ postpartum depression.
It was also beyond the scope of the CRHVC 2005-2007 Postpartum Depression
Research Project to study the number of mothers in different groups (i.e. mothers who
had a positive first and second EDPS; mothers with a positive first and negative second
EDPS, mothers with a negative first and positive second EDPS and mothers with a
positive first EDPS and early closure) who actually attended the community-based
postpartum depression support programs and resources. Likewise, the CRHVC 2005-
2007 Postpartum Depression Research Project did not examine the relationship between
the mothers’ attendance at these programs and the mothers’ perceptions about the factors
that were/were not perceived to be barriers. These issues could be explored in future
targeted studies, particularly the attendance of mothers who perceived no barriers to
attending the programs.
12. Postpartum Depression Goal Statements for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007
The Home Visitors, in consultation with mothers developed goal statements for
mothers attending the CRHVC Healthy Families Program who screened positive for
postpartum depression. The CRHVC Home Visitors used the goal statements to develop
plans and strategies to address the mothers’ postpartum depression.
67

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Figure 27 summarizes/categorizes the mothers’ goal statements relating to the
management of the mothers’ postpartum depression as; goal statements related to plans
and strategies for self-care, stress management and coping, support/education for
postpartum depression, improved self-confidence and decreased social isolation.
Figure 27. Goal Statements Related to the Management of Postpartum Depression for Mothers Attending the CRHVC Healthy Families Program 2005-2007
Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program 2005-2007 - Goals Related to Postpartum Depression
(67 Goals for 39 Mothers)*
Stress Management and Coping Goals,
20, 30%
Self-care Goals, 22, 33%
Social Isolation Goals, 3, 4%
PPD Referral and Support Goals,
16, 24%
Self-esteem Goals, 6, 9%
Self-care Goals
Stress Managementand Coping GoalsPPD Referral andSupport GoalsSelf-esteem Goals
Social IsolationGoals
*39 (30%) of 130 mothers with postpartum depression had goal statements relating to postpartum depression
Table 11 categorizes the individual goal statements relating to postpartum
depression for mothers attending the CRHVC Healthy Families Program. It is important
to note that it was beyond the scope of the CRHVC 2005-2007 Postpartum Depression
Research Project to assess the extent to which mothers achieved/did not achieve their
goals and the impact of the postpartum depression strategies on decreasing the mothers’
postpartum depression.
68

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 11. Goal Statements Relating to the Support and Management of Postpartum Depression for Mothers Attending CRHVC Healthy Families Program 2005-2007 Mothers (N=130) 67 Goal Statements Referring to Postpartum Depression (PPD) Number/% of Goals
A. PPD Goals Relating to Mothers’ Self-care Multiple self care skills 16 Mother will address her PPD issues through self care strategies 1 Maintains own health/mother recognize importance of taking care of her health 2 Mother will focus some energy on herself so that she stays healthy 1 Home Visitor will encourage mother to follow through with counseling 1 Mother will follow through with doctor's appointments 1 Mother will ask for help/take time for herself to reduce feelings of depression Summary - total goals relating to self-care interventions for the mother 22 (33%) B. PPD Goals Relating to Mothers’ Stress Management and Coping Coping skills/Stress management 12 Home Visitor will assist mother to identify and implement support for PPD and stress 1 Financial management to reduce anxiety 1 mother will be open to discussing her anxiety 1 During home visits mother will talk about how she is feeling 1 mother will report that she has more energy and can do things during the day 1 Mother able to manage daily routines with family 1 Follow safety plan to keep herself and family safe 1 Mother will report she is no longer a threat to the family’s safety/ well-being 1 Summary – total goals relating to stress and coping interventions for the mother 20(30%) C. PPD Goals Relating to PPD Support (Education, Community Referrals) Home Visitor will offer support/encouragement as mother learns to cope with depression 1 Maintains own health/mother will be referred to Families Matter to address PPD 1 Mother will follow through with supports for PPD 1 Mother will watch a video about depression and how to cope with it 1 Mother will report a decreased level of depression 1 Home Visitor will give information & referrals about PPD & ways of coping 1 Mother will be connected to Families Matter 1 mother will contact services that can help her out with PPD 1 Mother will advise Home Visitor when she is feeling her 'waves' of depression 1 Home Visitor will give Healthy Families PPD package/ Families Matters referrals 1 Increase knowledge about mental health services 1 Home Visitor will connect mother with postpartum support group 1 Mother will access resources/ build a support system to help with the PPD 1 Professional referral for PPD 1 Home Visitor will connect mother with postpartum support group 1 Self monitoring skills - mother will monitor her PPD 1 Summary - total goals relating to PPD support for the mother 16 (24%) D. PPD Goals Relating to Self-Confidence Demonstrating good self-confidence 3 Mother suffers from depression/history of abuse - she will work on developing self-esteem 1 Mother will feel better about herself and feel that she is a 'person' again 1 Home Visitor will regularly check with mother regarding her emotional status 1 Summary - total goals relating to self-confidence for the mother 6 (9%) E. PPD Goals Relating to Social Isolation Mother will enjoy spending time away from the home/feel less isolated 1 Mother will report that she feels less isolated 1 Mother will call Home Visitor when she needs to talk with somebody 1 Summary - total goals relating to social isolation for the mother 3 (4%)
69

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Findings and Conclusions
Thirty-nine (30%) of the 130 mothers had 67 goal statements that were related to
the management of their postpartum depression. The goals relating to postpartum
depression fell into five distinct categories. Twenty-two (33%) of the 67 goal statements
were related to self-care strategies for the mothers; 20 (30%) of the goal statements
related to stress management and coping for the mothers; 16 (24%) of the goal statements
related to support and encouragement for the mothers’ postpartum depression; 6 (9%) of
the goal statements related to improving mothers’ self-confidence; and 3 (4%) of the goal
statements related to decreasing the mothers’ social isolation.
Based on the results of this study, we suggest that the most usual goal statements
that the CRHVC Home Visitors developed to strategically address the mothers’
postpartum depression were related to self-care, stress and coping and support and
encouragement. It was beyond the scope of the CRHVC 2005-2007 Postpartum
Depression Project to assess actual goal achievement/non-achievement for the individual
mothers and any related impact on decreasing the mothers’ postpartum depression.
The foregoing results suggest that goal statements relating to postpartum
depression were developed for only 30% of the mothers. It is important to note that the
CRHVC Home Visitors developed strategies to address postpartum depression for all
mothers; these strategies were detailed in the mothers’ files and had not yet recorded as
goal statements when the analysis for the CRHVC 2005-2007 Postpartum Depression
Research Project was completed. In essence, the goal statements detailed in Table 11
represent only part of the plans and strategies that were developed for mothers with
postpartum depression. This finding is further discussed in the conclusions of this Report.
70

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
13. Risk Factors Identified at the Time of Postpartum Screening for Mothers with Postpartum Depression Attending CRHVC Healthy Families Program 2005-2007
Table 12 depicts the risk factors identified at the time of postpartum screening for
125 mothers who screened positive on the EDPS during the CRHVC 2005-2007
Postpartum Depression Research Project. These mothers had been screened in 2005-2006
with one of two postpartum screens – either the Parkyn Screen or the Healthy Families
America Screen. No mother was screened with both screens.
Table 12. Risk Factors Identified during Postpartum Screening for Mothers with Postpartum Depression Attending CRHVC Healthy Families Program 2005-2006
Risk Factor Identified for the Mother at the Time of Postpartum Screening (with the Parkyn Screen or the Healthy Families America Postpartum Screen)
Number of Mothers Screening Positive for the Risk - Parkyn Screen (N=84)*
Number of Mothers Screening Positive for the Risk - Healthy Families America Screen (N=41)*
Total Number of Mothers Screening Positive for the Risk - Both Screens (N=125)*
Financial Difficulties 63 (75%) 35 (85%) 98 (78%) No Emergency Contacts/No Support (1 or 2 Parents)
49 (58%) 14 (34%) 63 (50%)
Mental Illness - History of Depression /Postpartum Depression
17 (20%) 36 (89%) 53 (42%)
Low Education - Grade School to Some High School
20 (24%) 17 (41%) 37 (30%)
Inadequate Prenatal Care 10 (12%) 5 (12%) 17 (14%) Marital Difficulties 5 (6%) 5 (12%) 10 (8%) Complications Pregnancy/Delivery 35 (42%) NA** - Abortion or Adoption Considered NA** 17 (42%) - History Substance Abuse NA** 13 (32%) - Unstable Housing NA** 11 (27%) - Partner Unemployed NA** 9 (22%) - Parenting Difficulties 16 (19%) NA** - Single (Level of Support not Stated) NA** 7 (17%) - Low Birth Weight 12 (14%) NA** - Family History of Genetic Challenges 12 (14%) NA** - Prolonged Maternal Separation With Infant Contact
9 (11%) NA** -
Single - with support 9 (11%) NA** - Age of Mother (15-19) 7 (8%) NA** - Mental Illness Mother/Father 7 (8%) NA** - Marital Difficulties 7 (8%) NA** - Congenital Health Challenges (Baby) 5 (6%) NA** - Assessed Lack of Bonding 2 (2%) NA** - Prolonged Maternal/Infant Separation 1 (1%) NA** - Other ***
*The percentages represent the percent of mothers from the total groups of mothers who screened positive for the risk factor; ** Screening factor not on the Screen; ***There were 63 “other reasons” of which 17 were low education, 16 were parenting difficulties and 7 were marital difficulties. Note: The Parkyn Screen was used in 2005 and 2006. The Healthy Families America Screen was used in 2006 when the Parkyn Screen was discontinued.
71
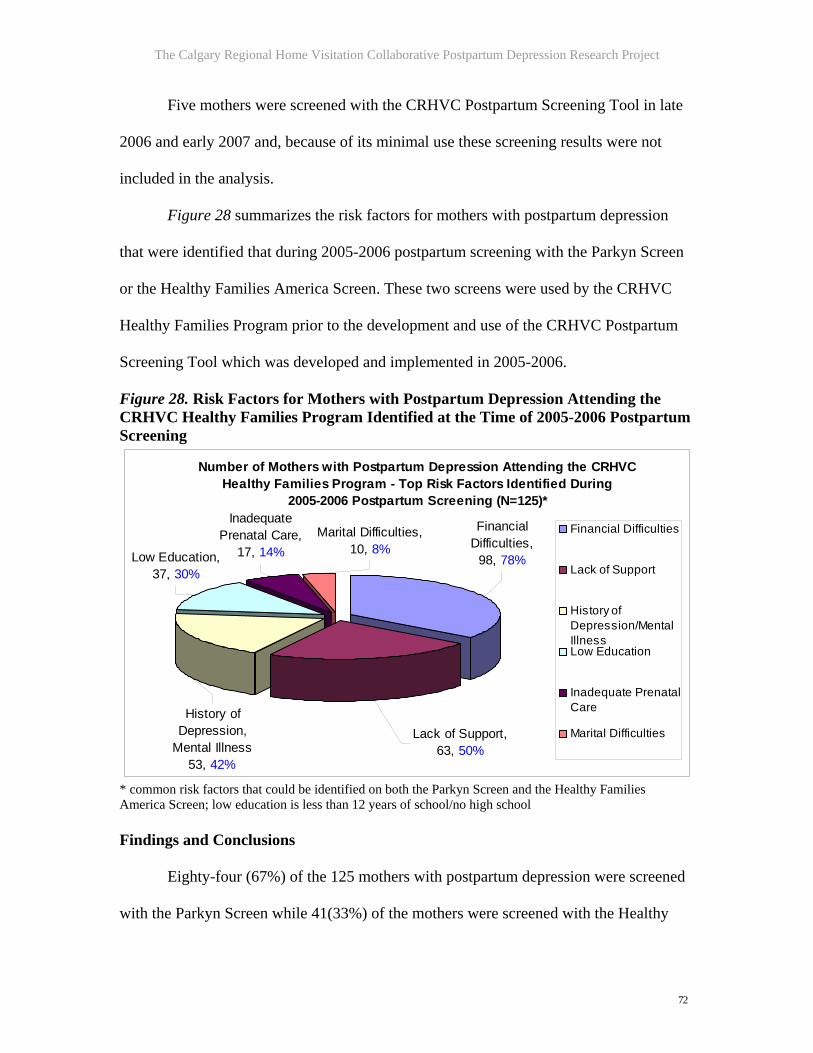
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Five mothers were screened with the CRHVC Postpartum Screening Tool in late
2006 and early 2007 and, because of its minimal use these screening results were not
included in the analysis.
Figure 28 summarizes the risk factors for mothers with postpartum depression
that were identified that during 2005-2006 postpartum screening with the Parkyn Screen
or the Healthy Families America Screen. These two screens were used by the CRHVC
Healthy Families Program prior to the development and use of the CRHVC Postpartum
Screening Tool which was developed and implemented in 2005-2006.
Figure 28. Risk Factors for Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program Identified at the Time of 2005-2006 Postpartum Screening
Number of Mothers with Postpartum Depression Attending the CRHVC Healthy Families Program - Top Risk Factors Identified During
2005-2006 Postpartum Screening (N=125)*
History of Depression,
Mental Illness 53, 42%
Lack of Support, 63, 50%
Financial Difficulties,
98, 78%
Inadequate Prenatal Care,
17, 14%Marital Difficulties,
10, 8%Low Education, 37, 30%
Financial Difficulties
Lack of Support
History ofDepression/MentalIllnessLow Education
Inadequate PrenatalCare
Marital Difficulties
* common risk factors that could be identified on both the Parkyn Screen and the Healthy Families America Screen; low education is less than 12 years of school/no high school Findings and Conclusions
Eighty-four (67%) of the 125 mothers with postpartum depression were screened
with the Parkyn Screen while 41(33%) of the mothers were screened with the Healthy
72

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Families America Screen in 2005-2006. As noted in Table 12, these two postpartum
screens also included other risk factors that were unique to the individual screens. The
common risk factors identified on the Parkyn Screen and the Healthy Families America
Postpartum Screen included financial difficulties, lack of support, depression/mental
illness, low education level, inadequate prenatal care and marital difficulties. Financial
difficulties, the most usual risk factor was identified as a risk factor for 98 (78%) of the
125 mothers; lack of available social support was a risk factor for 63 (50%) of the 125
mothers. Depression/mental illness were risk factors for 53 (19%) of the 125 mothers.
Thirty-seven (30%) of the 125 mothers had risks relating to a low level of education
(essentially no high school) and 10 (8%) of the mothers with postpartum depression had
risks associated with marital difficulties.
The Parkyn Postpartum Screen also identified complications of
pregnancy/delivery as a risk factor for 35 (42%) of the 84 mothers; parenting difficulties
as a risk factor for 16 (19%) of the 84 mothers; and low birth weight of the baby as a risk
factor for 12 (14%) of the 84 mothers. These findings likely reflected the medical/health
nature of the questions on the Parkyn Screen.
The Healthy Families America Postpartum Screen identified mothers’
consideration of adoption/abortion as a risk factor for 17 (42%) of the 41 the mothers;
unstable housing as a risk factor for 11 (27%) of the 41mothers and; history of substance
abuse as a risk factor for 13 (32%) of the 41mothers. These findings likely reflected the
psychosocial nature of the questions on the Healthy Families America Screen.
Based on the results of this study, we suggest that the most usual risk factors
identified at the time of postpartum screening that characterized mothers who later
73

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
screened positive for postpartum depression were financial difficulties, lack of
support/social isolation, depression/mental illness and low education (less than 12 years
of school.
The CRHVC 2005-2007 Screening Tool Project (completed concurrently with the
CRHVC Postpartum Depression Research Project) culminated in the development of a
standardized postpartum screening tool with demonstrated high validity and reliability.
Table 13 summarizes risk factors identified with the CRHVC Postpartum Screening Tool
during its early implementation in 2006-2007.
The most usual risk factors that were identified at the time of screening with the
CRHVC Postpartum Screening Tool included lack of sufficient money (i.e. correlates
with financial difficulties identified on the Parkyn and Healthy Families America
Screen); lack of confidence in caring for the baby (i.e. correlates with parenting
difficulties identified on the Parkyn and Healthy Families America Screen); mother
depressed/past depression (i.e. correlates with depression/mental difficulties identified on
the Parkyn and Healthy Families America Screen); social isolation (i.e. correlates with no
support/social isolation identified on the Parkyn and Healthy Families America Screen).
The three screens used during the time frame of the CRHVC 2005-2007
Postpartum Depression Research Project - the Parkyn Postpartum Screen, the Healthy
Families America Postpartum Screen and the CRHVC Postpartum Screening Tool -
consistently identified specific risk factors - financial difficulties, lack of confidence in
caring for the baby, social isolation and present/past depression/mental illness as common
risk factors at the time of postpartum screening. These risk factors have also been shown
to be risk factors for postpartum depression.
74

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 13. Risk Factors Identified During Screening (N=408) using the CRHVC Postpartum Screening Tool for Mothers Attending the CRHVC Healthy Families Program 2006-2007 Category of Risk for
Mothers with Positive Postpartum Screens
No. Mothers
Number of Mothers who had the Risk
Number of Mothers who did not have the Risk
Comments
Insufficient money for basic necessities/financial difficulties
408 222 (54%) 177 (43%) 9 (2%) of mothers didn’t know
Lack of confidence in caring for the baby
408 202 (49%) 206 (51%)
Social Isolation/lack of social support
408 202 (49%) 206 (51%) 2 mothers chose not to answer
Mother depressed since the baby’s birth (postpartum depression)
356 136 (38%) 220 (62%)
History of depression (mother) 290 57 (20%) 232 (80%) Presence of a medical health problem in the family that could interfere with caring for baby
408 36 (9%) 369 (90%) 3 (0.7%) of mothers didn’t know
Family involvement with Welfare Services during past 2 years
408 31 (8%) 376 (92%) 1 mother chose not to answer; 6 (1%) of mothers involved with Welfare more than 2 years earlier
Low level of education (no or some grade school)
408 27 (7%) 381 (93%)
Unsafe Home for baby/children 408 28 (7%) 372 (91%) 8 (2%) of mothers didn’t know
Mental health problem in the family that could interfere with caring for baby
408 25 (6%) 378 (93%) 5 (1%) of mothers didn’t know
Alcohol use in the home likely to make parenting difficult for mother
408 6 (1%) 92 (91%) 101 (25%) of homes had alcohol use
Emotional abuse in the home 408 11 (3 %) 396 (97%) 1 mother chose not to answer
Verbal abuse in the home 408 7 (2%) 400 (98%) 1 mother chose not to answer
Baby not wanted 408 8 (2%) 356 (87%) 42 (10%) of mothers would have preferred to have the baby earlier or later in life
No or minimal prenatal medical care
408 6 (1%) 402 (99%)
Drug use likely to make it difficult to care for baby
408 1 (0.02%) 407 (99.8%) 5 (1%) of homes had drug use
Physical abuse in the home 408 1 (0.02%) 407 (99.8%)
Further studies that could explore the extent to which any or all of these four risk
factors - financial difficulties, lack of confidence in caring for the baby, social isolation
75

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
and current/past depression/mental illness that were consistently identified at the time of
postpartum screening could be early predictors of postpartum depression in new mothers
- are suggested.
14. Discussion and Conclusions of the CRHVC 2005-2007 Postpartum Depression Research Project 14.1. Comparison of the Results of the CRHVC 2005-2007 Postpartum Depression Research Project with the Findings in the Literature The results of the CRHVC 2005-2007 Postpartum Depression Research Project
were compared with the findings in the literature. These comparisons are detailed in the
following sections.
14.1.1 Benefits of Participation in Home Visitation/CRHVC Healthy Families Programs
The 130 mothers participating in the CRHVC 2005-2007 Postpartum Depression
Research Project identified 258 benefits of Home Visitation Programs (Table 5). Eighty
(31%) of the 130 mothers stated that the most important benefit of attending the CRHVC
Healthy Families Program was the emotional support and encouragement offered by the
Home Visitors. Table 14 compares the benefits of attendance at the CRHVC Healthy
Families Program with benefits of Home Visitation that have been reported in the
literature.
Discussion and Conclusions
The benefits of participation in the CRHVC Healthy Families Program that were
identified in the CRHVC 2005-2007 Postpartum Depression Research Project reflected
the benefits that have been reported in peer-reviewed publications. In particular, the key
role of the emotional support that the CRHVC Home Visitors provided to mothers with
postpartum depression was noteworthy and it is likely that there is significant opportunity
76

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
to further develop the important role of the Home Visitor in treating postpartum
depression. The education support offered by the CRHVC Home Visitors consisted of
information packages/articles/videos about postpartum depression. The mothers also
considered referrals to community-based postpartum depression support programs and
resources as a key benefit of attending the CRHVC Healthy Families Program.
Table 14. Benefits of Home Visitation Programs - Comparison of the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with Benefits Reported in the Literature
Study/ Reference
Greatest Benefits of Home Visitation Programs
Comments
CRHVC 2005-2007 Postpartum Depression Research Project
>Support and encouragement of CRHVC Home Visitors (emotional support) >Referrals to community-based support resources > Provision of educational materials
130 mothers with postpartum depression
Sweet & Applebaum (2004)
>Parenting education >Parent social support > Parent counseling >Information on child development >Improved child-parent relationships >Improved child development screening >Provision of material goods >Referrals to social and health services
Overview of the effectiveness of home visiting
Shaw et al; (2006) >Home Visitation or peer support produced a statistically significant reduction in EDPS scores for mothers at high risk for postpartum depression >Home visitation may improve parent-infant interaction, maternal mental health
Literature search - 22 studies 1999/2003/2005
Ueda, Yamashita & Yoshida, (2006)
>Infant-related health problems requiring hospital care related to postnatal depression; Home Visitors provided emotional support
70 Japanese mothers, 19 of whom had postpartum depression
Logsdon et al., (2006a)
>Health care workers have responsibility to educate mothers about community support resources
Focus of article – impact of postpartum depression on mothering/need for mental health services
Dennis & Chung-Lee (2006)
>Opportunity for the mother to talk (develop a close working relationship with) with an empathetic non-judgmental health professional who listens - most desired treatment for postpartum depression
Consolidated findings of 40 articles (note - the opportunity to speak with a Home Visitor was listed as an important benefit in the CRHVC 2005-2007 postpartum depression study
Ray & Hodnett (2001)
>Professional and/or social support which may help in the treatment of postpartum depression
Review of 2 studies in the Cochrane database involving 137 mothers
77

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Discussions and Conclusions
The literature provides general and specific descriptions of the support that Home
Visitors provide for mothers with postpartum depression. The support offered by the
CRHVC Home Visitors mirrors the type of support reported in the literature.
14.1.2. Barriers to Attendance at Programs that Provide Support for Postpartum Depression
Sixty-one (47%) of the 130 mothers who participated in the CRHVC 2005-2007
Postpartum Depression Research Project provided feedback about whether certain factors
were/were not barriers to attendance at community-based postpartum depression support
programs and resources. As noted in Table 10, 29 (63%) of 46 mothers identified lack of
childcare as a barrier to attendance at community-based postpartum depression support
programs and resources. The next two most frequently mentioned barriers were no
perceived benefit of attending the program and limited transportation which were
identified by 26 (57%) of 46 mothers and 27 (55%) of 49 mothers respectively. Other
barriers to attendance were the type/nature of support offered by the program, distance
from the referral location, waitlist issues, language concerns and costs of attendance. At
the same time, many of the mothers confirmed that these factors were not barriers to
attendance.
Table 15 compares the barriers to attendance at community-based postpartum
depression support programs identified in the CRHVC 2005-2007 Postpartum Depression
Research Project with barriers reported in the literature.
Discussion and Conclusions
The barriers to participation in community-based postpartum depression support
programs and resources that were identified in the CRHVC 2005-2007 Postpartum
78

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Depression Research Project reflected the barriers that have been reported in peer-
reviewed publications, notably with respect to child care issues and transportation
concerns.
Table 15. Barriers to Attendance at Community-based Postpartum Depression Support Programs - Comparison of the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with Barriers Reported in the Literature
Study/ Reference
Greatest Barriers to Attendance at Community-based postpartum depression support programs
Comments
CRHVC 2005-2007 Postpartum Depression Research Project
>Lack of childcare >No perceived benefit of attendance at the support program >Limited transportation >Distance from referral >Type of support offered by the program
61 (of 130) mothers with postpartum depression
Teng, Blackmore & Stewart (2006)
>Practical barriers - not knowing how to and where to access services and language difficulties >Cultural barriers - fear of stigma and lack of validation of depressive symptoms by family and society
Study focused on immigrant women in Canada
Ross et al., (2006) >Transportation issues >Childcare issues
Literature review
Sword et al; (2006) >Reluctance to identify or acknowledge health concerns because of beliefs that depression is normal consequence of childbirth >Reluctance to get necessary help; therefore many unmet learning needs > Belief that postpartum depression is unacceptable, therefore not acknowledged >Language - unable to understand health information
Study focused on immigrant women in Canada
Gjerdingen & Yawn (2007)
> Cost-related issues >Time constraints >Lack of access >Lack of follow-through >Lack of childcare >Fear of referral to Child Protection Services > Fear of judgment
Comprehensive literature review
Dennis & Chung-Lee (2006)
>Mothers reluctant to seek support and to disclose their depressive state >Lack of awareness about support services >Lack of awareness of being depressed >Denial > Mothers’ concerns about postpartum depression not taken seriously by professionals (doctors); insufficient length of appointment; not referred to other services
Focus on mothers from different cultures; in-depth literature review
Murray, Woolgar, Murray & Cooper (2003)
>Self-exclusion from programs Case-control study; data from computerized health systems
79

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
The CRHVC Postpartum Depression Project identified two barriers - no perceived
benefit of attending the program and the type/nature of support offered by the support
program that to the best of this researcher’s (P. Hull) knowledge have not been previously
reported. We suggest that these two factors could be predictors of poor attendance and
early attrition from community-based support programs for postpartum depression, an
issue that has been well-documented in the literature. It is therefore important that Home
Visitation Programs ensure that mothers fully understand the type of/nature of support
offered by programs prior to recommending attendance; this will allow mothers to make
well-informed decisions about attendance. Home Visitors are in an ideal position to
provide this information and proactively support the mothers’ decision-making about
attendance at community-based postpartum depression support programs and resources.
It was beyond the scope of the CRHVC 2005-2007 Postpartum Depression
Research Project to study how these barriers actually impacted mothers’ attendance at
community-based postpartum depression support programs and resources and the
mothers’ perceptions about the benefits/lack of benefits of attendance.
14.1.3. Risk Factors Related to Postpartum Depression for Mothers Attending Home Visitation Programs
One hundred and twenty-five (96%) of the 130 mothers who participated in the
CRHVC 2005-2007 Postpartum Depression Research Project provided feedback to the
Home Visitors about personal and environmental risk factors identified at the time of
screening and/or that had become important after admission to the CRHVC Healthy
Families Program. As noted in Table 13, insufficient money for basic necessities was a
risk factor for 222 (54%) of the 408 mothers and lack of confidence in caring for the baby
was a risk factor for 202 (50%) of the 408 mothers. The next two most frequently
80

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
mentioned risk factors were social isolation and depression. Table 16 compares the risk
factors identified in the CRHVC 2005-2007 Postpartum Depression Research Project
with risk factors reported in the literature.
Table 16. Risk Factors for Mothers with Postpartum Depression - Comparison of the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with Risk Factors Reported in the Literature
Study/ Reference
Greatest Risks for Mothers with Postpartum Depression Comments
CRHVC 2005-2007 Postpartum Depression Research Project
>Insufficient money >Lack of confidence to care for baby >Mothers’ depression >Social isolation/lack of social support
408 mothers attending the Healthy Families Program
Webster, Pritchard, Creedy & East (2003)
>Previous postnatal depression (most significant risk); severe baby blues >Low social support >Dissatisfaction with the birth experience >Difficult infant temperament >Obstetric complications/satisfaction with labour/delivery >Infant feeding method (bottle-feeding)
Comparative study - antenatal and post natal risks
Horowitz & Goodman ( 2005)
> Prenatal depression or anxiety, history of depression > Inadequate social support > Poor relationship with partner >Life and child care stress
American study - focus timely intervention
Beck (2006) >Inadequate clinician support, caring, communication issues >Long painful labour; mother feels powerless > Unmet emotional needs >Prenatal depression > Anxiety >Low self-esteem >High stress level >Child care difficulties/ difficult infant temperament >Poor marital relationship >Maternity blues >Single marital status >Low socioeconomic status >Unplanned/unwanted pregnancy > Lack of social support
Review and summary article
Josefsson & Sydsjo (2007)
>Use of antidepressant medication and other medications >Presence of affective disorders
675 mothers; 221 with postpartum depression
Small, Lumley & Yelland (2006)
>Mothers under age 25 >Newcomers to the country, little or no English >No social support >Physical health problems >Baby with feeding problems >Homesickness (immigrants)
Australian study - 318 Vietnamese, Turkish and Filipino mothers
Sword et al., (2006)
>Low family income, need for financial assistance > New immigrants
Canadian study - 1,250 mothers,
81

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
> Low social support > Unmet learning needs (hospital)
31% new Canadians
Dennis et al., (2004)
>Immigration within the last 5 years >History of depression independent of childbirth >Diagnosis of pregnancy-induced hypertension >Vulnerable personality style >Stressful life events >Low social support/partner support >Lack of readiness for hospital discharge >Dissatisfaction - infant feeding method >Low maternal confidence in caring for infant
Canadian study - 594 mothers
Boyce & Hickey (2005)
>16 years of age or less >Having baby of non-desired sex >Past history of psychiatric illness >Experiencing stressful life events since conception >Marital dissatisfaction >Low social support >Vulnerable personality (vulnerability scale used) >Colicky baby > Early discharge from hospital
Australian study - convenience sample of 425 new mothers
Bloch et al., (2005)
>Past history of depression or the blues >Mood disorders during oral contraceptive use
Retrospective review 1800 mothers
Harvey & Pun (2007)
>Prenatal depression and related disorders Psychiatric patient clinical findings
Surkan et al., (2006)
>Number of children >Perceived discrimination >Lack of social support
Multiethnic urban population
Austin, Tulley & Park (2007)
>Prenatal anxiety Screening tool development study
Howell, Mora, Horowitz & Leventhal (2005)
>Lack of social support >Lack of self-efficacy >Skills in managing household and infants >Access and trust in support services
Telephone survey of 655 white, African-American and Hispanic women
Discussion and Conclusions
The risk factors identified for mothers who participated in the CRHVC 2005-2007
Postpartum Depression Research Project reflected the risks that have been reported in
peer-reviewed publications. In general, the most common risk factors identified in
studies (across cultures) for postpartum depression were insufficient income for basic
necessities, lack of confidence in caring for the baby, social isolation, new to the country
(thus language issues for many mothers), stressful life events and current/past depression.
82

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
One study (Boyce and Hickey, 2005) reported that 20 (25%) of the 80 mothers who had
infants of the non-desired sex developed postnatal depression while other investigators
(Webster et al., 2003) asserted that “postnatal highs” was a risk factor. Similarly,
mothers’ unmet learning needs (Sword et al., 2006) have been recently reported as a risk
factor. The impact/importance of risk factors could be further studied by the CRHVC.
14.1.4. Demographic Profile of Mothers with Postpartum Depression Attending Home Visitation/Healthy Families Programs
The CRHVC 2005-2007 Postpartum Depression Research Project assessed the
demographic profile of the 130 mothers with postpartum depression. Table 4 summarizes
these results. Table 17 compares the risk factors identified in the CRHVC 2005-2007
Postpartum Depression Research Project with the demographic profiles of mothers
reported in the literature.
Discussion and Conclusions
The demographic profile for the 130 mothers who participated in the CRHVC
2005-2007 Postpartum Depression Research Project reflected the mothers’ demographic
profiles that have been reported in peer-reviewed publications. In general, mothers with
postpartum depression tended to be 25-35 years old, predominantly white (English),
married and of middle to higher socioeconomic status. Much of the literature regarding
the demographic profile of mothers with postpartum depression is sketchy or inconsistent
(Ross et al., 2006). These authors completed an in-depth literature review and concluded
that only four variables - age, ethnicity, relationship status and socioeconomic status
could be assessed. Clearly, there is a need to further undertake studies of the demographic
profile of mothers with postpartum depression, particularly mothers from different
cultures.
83

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Table 17. Demographic Profile of Mothers with Postpartum Depression - Comparison of the Findings of the CRHVC 2005-2007 Postpartum Depression Research Project with the Demographic Profiles Reported in the Literature
Study/Reference Demographic Profile of Mothers Comments CRHVC 2005-2007 Postpartum Depression Research Project
> Average age 30 (19-43) > First language (English) - 81 (62%) >First language other than English - 49 (38%) > First language Arabic - 14 (11%) of mothers (7% of referred Arabic mothers)
130 mothers with postpartum depression - identified risks included insufficient income, minimal social support, past/current depression and life stress
Boyce & Hickey (2003)
>Average age - 26.9 years (no difference from study sample of 425 mothers) > Majority married
42 mothers with postpartum depression
Surkin et al., (2006) >Average age 29 > Mix of Black, Latina and English backgrounds; English - 40% range
Multiethnic study - comparative study
Josefsson & Sydsjo (2007)
>Average age - 33.5 (range of 5 years)
Comparative study - 675 mothers; 221 with postpartum depression
Ross et al., (2006) >Age predominantly 25-35 years > Predominantly white >Middle or higher socioeconomic status > Married or equivalent status
In-depth literature review; mothers a homogeneous group - not representative of general population
*660 mothers referred who had English as their first language; 406 mothers referred who had a language other than English as their first language; it was beyond the scope of this study to determine the percent of mothers from different cultures who had postpartum depression. The percent of mothers with postpartum depression in relation to all referred mothers is 25% (Marianne Symons, Program Manager). This higher percent of mothers with postpartum depression in the CRHVC (in comparison with the literature) is a reflection of the fact that the Calgary Health Region assesses mothers’ risks prior to referral to the CRHVC. 15. Conclusions and Recommendations of the CRHVC 2005-2007 Postpartum Depression Research Project On the basis of the findings of the CRHVC 2005-2007 Postpartum Depression
Research Project, a number of conclusions and recommendations can be made. These are
detailed in the following section.
84

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Conclusion and Recommendation 1 - Community-based Home Visitation Programs, notably the CRHVC Healthy Families Program Have the Capacity to Make Valuable Contributions to the Home Visitation Profession by adding new Knowledge and Ideas for Additional Studies Relating to the Management of Postpartum Depression
The CRHVC 2005-2007 Postpartum Depression Research Project made the
following contributions to the study of postpartum depression and Home Visitation.
Confirmation of Earlier Findings in the Literature
The findings of the CRHVC 2005-2007 Postpartum Depression Research Project
confirmed the findings of earlier studies; for example, the nature of the
psychosocial, environmental and medical/health-related risk factors that
characterized mothers with postpartum depression, the benefits afforded to
mothers who attended the CRHVC Healthy Families Program and the mothers’
demographic profile reflected the findings in the literature. This finding is
important for three reasons:
It suggests that the CRHVC focuses the service delivery of its Healthy Families Program appropriately.
It further suggests that other community-based Home Visitation Programs could use a research and evaluation framework to structure their Programs that would foster a greater use of evidence to plan and structure their programs
The CRHVC is well-positioned to take a leadership role in community-based Home Visitation research and ultimately influence the evolution of Home Visitation in Canada
Use of Different Study Methods/Approaches and the Addition of New Knowledge
The CRHVC 2005-2007 Postpartum Depression Research Project used an
approach that (to the best of this researcher’s knowledge) has not been reported in
the literature; for example; the Project categorized mothers who had been
screened using the EDPS for postpartum depression as mothers who:
85
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Screened positive on the first EDPS screen and positive on the second EDPS screen
Screened positive on the first EDPS screen and negative on the second EDPS screen
Screened negative on the first EDPS screen and positive on the second EDPS screen
Screened positive on the first EDPS screen and had early closure from the Program
The approach used in the CRHVC 2005-2007 Postpartum Depression Research
Project is important as it confirmed the changing status of mothers’ postpartum
depression and established/confirmed the importance of multiple screenings with the
EDPS. Future large-scale university-based studies (and/or community-based programs)
could undertake targeted studies to better know the course of postpartum depression and
the factors that cause changes in screening status for individual mothers. This is
important given that most studies appear to focus on screening (often one-time screening)
in the immediate postpartum period; it is clear that if additional screening is not
completed, at-risk mothers (those who screen positive and then negative on the EDPS)
could be missed.
The CRHVC 2005-2007 Postpartum Depression Research Project added new
knowledge that (to the best of this researcher’s knowledge) had not been reported
in the literature; for example; the Project identified two different barriers to
mothers’ attendance at community-based postpartum depression support programs
and resources. These barriers were - no perceived benefit from attending the
program and mothers’ concerns about the type/nature of the program not being
appropriate (for example, group vs. individual support programs).
Such barriers (and all other barriers) are important to study and understand. These
barriers could be contributing factors to the mothers’ poor attendance/early attrition or
86

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
self-exclusion from postpartum depression support programs, issues that are well-
documented in the literature.
The CRHVC 2005-2007 Postpartum Depression Research Project also explored
and quantified mothers’ perceptions with regard to the factors not being barriers
to attendance at community-based postpartum depression support programs and
resources. The results of this analysis indicated that almost half of the mothers did
not perceive these factors to be barriers to attendance.
It is important to further study mothers’ attendance at postpartum depression
support programs and resources. Targeted postpartum depression studies could address:
the benefits experienced by mothers who attended community-based postpartum
depression support programs and resources; attrition from these programs; duration of
attendance; the impact of attendance on the course of the mothers’ postpartum depression
and; attendance for those mothers who perceived no barriers to attendance.
Future studies could also explore the outcomes of Home Visitor support, notably from
the mothers’ perspectives, decreases in postpartum depression that are directly
attributable to Home Visitor support and the role of Home Visitors in the overall
continuum of care for mothers with postpartum depression.
Conclusion and Recommendation 2 - The CRHVC has Significant Opportunities to Partner with other Organizations to Study Postpartum Depression and Should Seek Funding to Undertake Future Research Projects Partnership/ Joint Studies with Other Organizations
The CRHVC has developed (and continues to enhance) solid databases of information
relating to its Healthy Families Program and to postpartum depression. There are likely
opportunities to partner with:
87

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
the Calgary Health Region (which has a well-documented interest in postpartum depression and an active Network framework)
the University of Calgary (or other universities) other Home Visitation Programs in Alberta (through AHVNA) other Home Visitation Programs in Canada (through proactive consultation with
other leaders/program managers
Such partnerships could require involvement in Ethics approval processes.
Ultimately, however, the benefits derived from such partnerships could increase the scope
of studies and highlight the role of Home Visitation in the continuum of care for
postpartum depression. The CRHVC has an opportunity to take a lead (or partnering) role
in establishing these research-based relationships. Such partnerships can lead to a more
strategic approach at the local level, a fact noted to be an important mechanism for
managing this major public health problem (Deave, 2002).
The CRHVC should also continue the data collection processes that were initiated
and used during the CRHVC 2005-2007 Postpartum Depression Research Project. It
would be important to evaluate whether additional information should be collected and as
necessary, to revise the data collection forms. Ultimately, this information could be used
for longitudinal studies about mothers with postpartum depression attending Healthy
Families Programs.
Role of Home Visitors in Research Studies
The CRHVC Supervisors and Home Visitors were actively involved throughout the
CRHVC 2005-2007 Postpartum Depression Research Project. They provided excellent
feedback with regard to the content and use of the data forms and collected and reported
the mothers’ information. The CRHVC Supervisors and Home Visitors were also active
participants in the CRHVC 2005-2007 Postpartum Screening Tool Project which was
88

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
completed concurrently. It is reasonable to assume that the CRHVC Healthy Families
staff would be willing and committed participants in future studies.
Potential Sources of Funding for Future Studies
The Alberta Centre for Child, Family and Community Research
www.research4children.com, which supports and encourages research in specific areas
(Early Childhood Development, Family Capacity Building, Community Capacity
Building, Successful Transitions to Youth and Tracking Long-term Outcomes) could be
approached to fund targeted studies.
Other potential sources of funding include the Burns Foundation, The United Way
and the Calgary Foundation. In addition, it may be feasible to approach ALVA, the
majority funder of the CRHVC 2005-2007 Postpartum Depression Project (and the
CRHVC Postpartum Screening Tool Project) to support a follow- up study. Such a study
could have national scope.
Conclusion and Recommendation 3 - The CRHVC has an Opportunity to Strengthen/Enhance its Service Delivery to Support Mothers with Postpartum Depression through Better Use of the Edinburgh Screening Tool Results and the Use of Goal Statements for Postpartum Depression The Development and Use of Goal Statements for Mothers with Postpartum Depression
The CRHVC Postpartum Depression Research Project confirmed the important
role that Home Visitors play in effectively supporting mothers with postpartum
depression: it quantified and categorized goal statements for mothers with postpartum
depression (Table 11) and as well, described the scope of services provided by Home
Visitors (Table 2), areas that have been generally reported in the literature.
89

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
An analysis of the number of goal statements and the format/way in which they
were written revealed the following:
Goals relating to postpartum depression were developed for only 39 (30%) of the 130 mothers with postpartum depression. It was beyond the scope of this Project to assess which mothers of the four categories had goal statements related to postpartum depression. Clearly, however, there is a need to develop relevant goal statements for all mothers with postpartum depression, specifically at the time of a positive screen
Many of the goal statements were not written in the context/terms of acceptable standards for goal statements (specific, measurable, actionable, relevant and time-bound)
Outcome measures were not reported (although this was beyond the scope of the Project) but is necessary to ascertain the effectiveness of Home Visitor interventions in impacting the course of postpartum depression, both in research studies and as an essential component of service delivery Discussion with Marianne Symons, CRHVC Program Manager revealed the
following practices of the CRHVC Healthy Families Program:
1) The Home Visitors write the first goal statement for mothers at 45-60 days after referral
2) The Home Visitors write the second goal statement for mothers (sometimes a review/modification of the first goal statement at 90 days
3) The Home Visitors administer the first EDPS at 16 weeks (112 days) 4) The Home Visitors write additional goal statements for mothers at 90 day
intervals 5) Home Visitors administer the second EDPS at 32 weeks (228 days)
When the mothers screen positive for postpartum depression (screening
completed at 112 days and/or 228 days), the Home Visitors immediately develop
strategies to address postpartum depression. These strategies are detailed in the mothers’
file notes at the time of the positive EDPS and subsequently added to the goal
statements/plans at the time of the next review (90 day intervals after the 112 day goal
plan is written). The CRHVC 2005-2007 Postpartum Depression Research Project was
limited in that it did not include a review of all goal statements and thus the Home
Visitors’ goals to address postpartum depression were not identified. In essence, goal
90

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
statements relating to postpartum depression had been developed (and were being
implemented) at the time of the CRHVC Postpartum Depression Research Project but
had not yet been added to the goal statements. This accounts for the relatively low level
of goal statements relating to postpartum depression that were identified in the CRHVC
2005-2007 Postpartum Depression Research Project. Marianne Symons, in consultation
with the CRHVC Supervisors Team, confirmed that all of the mothers with postpartum
depression had goal statements relating to postpartum depression.
At the same time, it recommended that the CRHVC reconsider the timing of
writing goal statements for mothers having positive EDPS screens. Ideally, the mothers’
goal statements should be modified in a timely manner if the EDPS is positive.
Targeted Training in Relation to the Use of EDPS Screening Results
Elliot, Ashton, Gerrard and Cox (2003) suggested that the screening for postnatal
depression should be grounded in the research process to ensure that Health Visitors
(Home Visitors) best use the results of screening to help mothers. These authors reported
the potential benefit of targeted screening tool training to assist Health Visitors.
Goldsmith (2007) reported the necessity for health professionals to have an excellent
understanding of postpartum depression in order for them to provide quality care.
Logsdon, Wisner and Shanahan (2006b) also noted the need to increase awareness about
postpartum depression for all primary care providers. Carter (2005) suggested that
postnatal visits by healthcare professionals showed promise in terms of preventing
postnatal depression. The CRHVC should seek an opportunity to undertake a three-part
postpartum depression training initiative that would:
1) Fully examine the current practices of the CRHVC Home Visitors with respect to their use of the results of the EDPS, their knowledge of best practices for
91
The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
postpartum depression and its management by Health Professionals, notably Home Visitors
2) Fully examine their existing goal statements for mothers with postpartum depression from the perspective of format, time of development and achievement of intended outcomes and explore Carter’s (2005) belief that postnatal visits can prevent postnatal depression and how this could be a component of the training program
3) Develop an evidence-based training program to address the findings in 1 and 2 and complete a follow-up study to evaluate the effectiveness (outcomes) of the training in terms of decreasing the mothers postpartum depression (and the impact on job satisfaction for the CRHVC Home Visitors)
Conclusion and Recommendation 4 - The CRHVC has an Opportunity to Take a Lead Role in Developing Best Practice Guidelines for Home Visitors who Support Mothers with Postpartum Depression Best Practice Home Visitation Guidelines for Home Visitors
McQueen and Dennis (2007) described a systematic process for developing
evidence-based best practice (clinical) postpartum depression guidelines for nurses. This
process incorporated the following steps:
Establishment of a multidisciplinary development team Identification of the scope of the guidelines and definition of outcomes Question formulation and search for evidence Appraisal of evidence Formulation of guideline recommendations and synthesis of the evidence Consultation and peer review, concensus conference and pilot testing Presentation of the Guidelines
The CRHVC has an opportunity to lead a similar initiative that would culminate in
the development of evidence-based practice guidelines for Home Visitors who support
mothers with postpartum depression. Such guidelines, which would encompass Home
Visitor interventions for screening, assessment and outcome evaluation, are not available
and if developed could foster more consistent outcomes-based management of
postpartum depression by Home Visitors. Downie, Wynaden, McGowan, Juliff, Axten,
Fitzpatrick, Ogilvie and Painter (2003) also reported guidelines for developing best
92

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
practices for postpartum depression; these could also serve as an important source of
information. Ingram and Taylor (2007) have suggested that Health Visitors (Home
Visitors) could play an important role in antenatal care, an opportunity that could also be
explored by the CRHVC, possibly in collaboration with the Calgary Health Region.
The CRHVC could collaborate with other Home Visitation Programs in Canada and
as such, take a lead (or partner) role in a study with national scope and relevance.
Conclusion and Recommendation 5 - The CRHVC has an Opportunity to Establish a Predictive Inventory of Risk Factors (as Part of the Postpartum Screening Process) that Could Foster Early Identification and Interventions for Mothers who are at Particular Risk for Developing Postpartum Depression The Development of a Predictive Inventory for Postpartum Depression
The CRHVC Postpartum Depression Research Project compared the risk factors
identified in postpartum screening (Table 13) with the risk factors identified following a
positive screen for postpartum depression (Table 12). Four risk factors - financial
difficulties, low maternal confidence in taking care of the baby, lack of social support and
depression/past depression - were identified as the most usual risk factors for postpartum
depression.
The CRHVC could undertake a targeted study that could be used to determine if
mothers who screen positively for these four risks at the time of postpartum screening
(with the CRHVC Postpartum Screening Tool) subsequently develop postpartum
depression and whether early intervention by the CRHVC Home Visitors could mitigate
the likelihood of postpartum depression. In essence, the CRHVC has an opportunity to
develop a succinct predictive postpartum depression screening tool within the context of
an existing postpartum screening tool. Such a predictive tool could effectively and
efficiently address the need for an easy-to-administer screening instrument for
93

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
postpartum depression. A number of investigators such as Austin et al. (2007) and Beck
(2002) have undertaken research in this area and have tested in-depth postpartum
depression screening tools. Larger-scale randomized trials could be undertaken by other
investigators.
Conclusion and Recommendation 6 - The CRHVC has an Opportunity to Initiate Comprehensive Community-based Postpartum Depression Support Programs (Emphasis - Strengthened Social Networks) for Mothers with Postpartum Depression The Importance of Social Networks for Mothers with Postpartum Depression
The importance of social networks as an important component of effective treatment
for postpartum depression is well-documented (Boyce and Hickey, 2005; Sword et al.
2006; Teng et al., 2007). Surkan et al., (2006) reported that mothers with two or more
people who provided consistent social support had less depressive symptoms.
The CRHVC could undertake focused studies that would engage mothers
(particularly those of the same culture and/or who are not able to readily make in-person
visits) in formal (or informal) social support networks. One possible initiative could
involve the development of telephone-based or internet-based support groups with the
involvement of a CRHVC Home Visitor and two or more mothers. Wroblewski and
Tallon (2004) described a comprehensive support program for mothers with postpartum
depression and their suggestions could be used as one source of input for structuring a
CRHVC Program.
Other Opportunities for Targeted CRHVC Studies
The CRHVC (within the context of available resources) could also lead/participate in
a wide variety of other studies related to:
94

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
The mothers (such as the perceptions about postpartum depression from the perspective of mothers from different cultures and translation of support information and reasons for early closure bearing in mind that the mothers’ participation in the Healthy Families Program is voluntary
Home Visitors, particularly from the perspective of strengthening their important professional role in addressing postpartum depression and understanding the challenges they face in their work; Sweet and Applebaum (2004) noted that Home Visitors often influence program success but that their contribution may go unmentioned. The CRHVC has an opportunity to address this finding and in essence, increase awareness of the professional role of Home Visitors
Program development and evaluation to address gaps in services particularly for immigrant women and to enhance a person-centred approach to support with special attention to the optimal amount of support needed by mothers; the CRHVC could continue to refine its postpartum depression database and link the information with the data in the postpartum screening database
Reasons for early closure from the CRHVC Healthy Families Program (bearing in mind that the mothers’ participation is voluntary) and self-exclusion from available support, an issue noted to be of importance in many studies (Murray, Woolgar, Murray and Cooper, (2003).
Outcomes studies (for children of mothers with postpartum depression); the CRHVC routinely assesses infant development and this data could be studied
Conclusion and Recommendation 7 - The CRHVC 2005-2007 Postpartum Depression Research Project has Limitations Limitations of the CRHVC 2005-2007 Postpartum Depression Research Project
The CRHVC 2005-2007 Postpartum Depression Research Project provided a
“snapshot” of the mothers with postpartum depression attending a community-based
Healthy Families Program and as such, has a number of limitations including:
The number of mothers (130) who were involved in the study is relatively small and it is therefore not possible to make definitive statements about the results and findings; as such the study must be considered exploratory in nature. It is important to note however that the results paralleled those in the literature thus demonstrating that the data collection methods and analysis were essentially sound
The study relied on self-reporting and there were no control participants
The 130 mothers in the Project may not represent the actual population of at-risk
mothers in Calgary (though there is little reason to support this suggestion)
95

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
At the same time, the study identified new ideas (such as the importance of no
perceived benefit from attendance at postpartum support programs and different ways of
assessing the course of postpartum depression) that could be further studied. Thus, it is
important for the CRHVC to continue its involvement in evaluation and research studies.
Conclusion and Recommendation 8 - The CRHVC has an Opportunity to Engage in Knowledge Mobilization and Share the findings of the CRHVC 2005-2007 Postpartum Depression
It is important that the CRHVC proactively disseminate the knowledge gained
from the CRHC Postpartum Depression Research Project through presentations and
publication of the findings. Some of the opportunities are detailed below.
Presentation of the Results of the CRHVC 2005-2007 Postpartum Depression Research Project
Opportunities include:
Contacting local and provincial practice-based (and academic) organizations which are involved with Home Visitation (through AHVNA) and requesting opportunities to make presentations that would highlight the relevance of this study
Seeking media coverage - newspaper and magazines that target mothers and children’s services
Making presentations to key stakeholders of the Government of Alberta Publication of the Results of the CRHVC 2005-2007 Postpartum Depression Research Project
Opportunities include:
Adding the study results to the CRHVC and AHVNA web sites and creating links with other organizations to ensure that the study results can be readily accessed
Submitting articles to journals and magazines for publication Sending the Final Report to other investigators who have/are undertaking studies
about postpartum depression in Canada (Teng et al.,2007; Dennis et al., 2004) and seeking their input and suggestions
96

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Summary Statement - the CRHVC 2005-2007 Postpartum Depression Research Project
Postpartum depression is a major public health concern in Canada that impacts at
least 10-20% of new mothers. Recent immigrants appear to be particularly vulnerable.
The sequelae of postpartum depression are devastating and negatively impact mothers,
children and their families. Leahy-Warren and McCarthy (2006, p 97) citing Dennis
(2005) who undertook a systematic review of postpartum depression in mothers noted
“the only intervention that had a clear preventative effect with vulnerable mothers was
individual intensive postpartum support in the guise of home visits provided by
professionals”. The CRHVC has a unique opportunity to confirm this finding and to
further strengthen the professional reputation of Home Visitors. This will require
initiation of targeted studies or involvement in collaborative studies.
The CRHVC 2005-2007 Postpartum Depression Research Project achieved its goals
and is well-positioned to participate in future studies given its strength-based philosophy,
the rigour of its Healthy Families and postpartum depression databases, commitment to
ongoing evaluation, cost-effective methods, use of evidence-based practices and its
dedicated professionals - the Leadership Team, Administration Team Supervisors Team
and, in particular the Home Visitors. The CRHVC should proactively seek funding to
continue its work and disseminate results.
Patricia Hull
M.Sc., M.Sc., EdD (candidate), PMP, CHE, CHRP, RD
July 30, 2007
97

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
References
Arnold, A.F., Baugh, C., Fisher, A., Brown, J., & Stowe, Z. N. (2002). Psychiatric aspects of the postpartum period. S.G. Kornstein & A.H. Clayton (eds). Women’s Mental Health, New York.
Austin, M.P. (2003). Targeted group antenatal prevention of postnatal depression: a
review. Acta Psychiatr Scand, 107(4), 244-250. Austin, M., Tully, L., & Parker, G. (2007). Examining the relationship between antenatal
anxiety and postnatal depression. Journal of Affective Disorders, 101 (1-3), 169- 174.
Baker, L., Cross, S., Greaver, L., Wei, G., Lewis, R., & Healthy Start CORPS. (2005). Prevalence of postpartum depression in a native American population. Maternal and Child Health Journal, 9 (1), 21-25. Ballard, C.G., Davis, R., Cullen, P.C., Mohan, R.N., & Dean, C. (1994). Prevalence of
postnatal psychiatric morbidity in mothers and fathers. British Journal of Psychiatry, 164, 782-788.
Beck, C.T. (1995). A meta-analysis of the relationship between postpartum depression
and infant temperament. Nursing Research, 45 (4), 225-30. Beck, C.T. (2006). Postpartum depression: it isn’t just the blues. American Journal of
Nursing, 106 (5), 40-50. Beck, C.T. (2002). Revision of the postpartum depression predictors inventory. Journal of Obstetric, Gynecological and Neonatal Nursing, 31(4), 394-402. Beck, C.T. (1998). The effects of postpartum depression on child development; A meta-
analysis. Archives of Psychiatric Nursing, 12, 20-20. Beck, C.T. (2001). Predictors of postpartum depression. An update. Nursing Research,
50 (5), 275-285.
Beck, C.T. (1999). Maternal depression and child behavior problems: a meta-analysis. Journal of Advanced Nursing, 29, 623-29.
Benvenuti, P., Valoriani, V., Degl’Innocenti, B.G., FAvini, I., Hipwell, A., & Pazzagli, A. (2001). Postnatal depression and the impact on infant-carrier attachment strategies: A case report. Archives of Women’s Mental Health, 3, 155-164.
Bernazzanni, O., Saucier, J.F., & Borgeat, F. (1997). Psychosocial predictors of
depressive symptomology level in postpartum women. Journal of Affective Disorders. 46, 39-49.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Bloch, M., Rotenberg, N., Koren, D., & Klein, E. (2005). Risk factors associated with the development of postpartum mood disorders. Journal of Affective Disorders, 88 (1), 9-18.
Boath, E., Bradley, E., & Henshaw, C (2004). Women’s view of antidepressants in the treatment of postnatal depression. Journal of Psychosomatic Obstetrics and Gynecology, 25, 221-233.
Boyce, P., & Hickey, A. (2005). Psychosocial risk factors to major depression after illness. Journal of Social Psychiatry and Psychiatric Epidemiology, 40, 605-612. Carter, F.A. (2005). Postnatal home visits from healthcare professionals show promise for
preventing postnatal depression. Evidence-based Mental Health, 8 (4), 108. Charbrol, H, Teissedre, F., Armitage, J., Danel, M., & Walburg, V. (2004). Acceptability
of psychotherapy and antidepressants for postnatal depression among newly delivered mothers. Journal of Reproductive and Infant Psychology, 22, 5-12.
Cohn, J.F., & Tronick, E.Z. (1983). Three-month old infants reaction to simulated
maternal depression. Child Development, 54, (1), 185-93. Cooper, P.J., & Murray, L. (1998). Postnatal depression. British Medical Journal, 316, (7148), 1884-1886. Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression:
Development of the Edinburgh Postnatal Depression Scale. British Journal of Psychiatry, 150, 782- 786.
Deave, T. (2002). Primary care research. Primary Health Care, 12 (9), 8. Dennis, C.E. (2006). Preventing postpartum depression part II: a critical review of
nonbiological interventions. Canadian Journal of Psychiatry, 49 (8), 526-538. Dennis, C.E. (2005). Psychosocial and psychological interventions for prevention of postnatal depression: systematic review. British Medical Journal, 331, 15-18. Dennis, C.E., & Chung-Lee (2006). Postpartum depression help-seeking barriers and
maternal treatrment of preferences: A qualitative systematic review. Birth. 33 (4), 323-321.
Dennis, C.E., Janssen, P.A., & Singer, J. (2004). Identifying women at-risk for
postpartum depression in the immediate postpartum period. Acta Psychiatrica Scandinavica, 110, 338-346.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Dennis, C.E., & Ross, L.E. (2006). Depressive symptomology in the immediate postnatal period: identifying maternal characteristics related to true-false and false-positive screening scores. The Canadian Journal of Psychiatry, 51, 265-273.
Downie, J., Wynaden, D., McGowan, S., Juliff, D., Axten, C., Fitzpatrick, L., Ogilvie, S.,
& Painter, S. (2003). Using the Edinburgh postnatal depression scale to achieve best practice standards. Nursing and Health Sciences, 5, 283-287.
Elliott, S.A., Ashton, C., Gerrard, J., & Cox. (2003). Is trainer training an effective
method for disseminating evidence-based practice for postnatal depression? Journal of Reproductive and Infant Psychology, 21 (3), 219-228.
Flores, D.L., & Hendrick, V.C. (2002). Etiology and treatment of postpartum depression.
Current Psychiatric Reports, 46 (6), 461-466.
Forbes, E.E., Cohn, J.F., Allen, N.B.; Lewinsohn, P.M. (2004). Infant affect during parent-infant interaction at 3 and 6 Months: Differences between mothers and fathers and influence of parent history of depression. Infancy, 5 (1), 61-84.
Fuggle, P., Glover, L., Khan., & Haydon. (2002). Screening for postnatal depression in
Bengali women: preliminary observations from using a translated version of the Edinburgh postnatal depression scale. Journal of Reproductive and Infant Psychology, 20 (2), 72-82.
Gjerdingen, D.K, & Yawn, B.P. (2007). Postpartum Depression Screening: Importance,
methods, barriers and recommendations for practice. Journal of the American Board of Family Medicine, 20, 280-288.
Goldsmith, M.E. (2007). Postpartum depression screening by family nurse practitioners. Journal of the American Academy of Nurse Practitioners. 19 (6), 321-327. Harvey, S.T., Pun, P. K. (2007). Analysis of positive Edinburgh depression scale referrals
to a consultation liaison psychiatry service in a two-year period. International Journal of Mental Health Nursing, 16 (3), 161-167.
Highet, N., & Drummond, P. (2004). A comparative evaluation of community treatments
for post-partum depression; implications for treatment and management practices. Australian and New Zealand Journal of Psychiatry, 38, 212-218.
Holden, J.M., Sagovsky, R., and Cox, J.L. (1989). Counseling of postnatal depression: a
controlled study of health visitor intervention in treatment of postnatal depression. British Medical Journal, 298, 223-226.
Horowitz, J.A., & Goodman, J.H., (2005). Identifying and treating postpartum
depression. Journal of Obstetric, Gynecological & Neonatal Nursing, 34 (2), 264-273.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Hough, P. (2004). Calgary Regional Home Visitation Collaborative Program Evaluation Report, the Calgary Regional Home Visitation Collaborative.
Howell, E.A., Mora, P.A., Horowitz, C.R., & Leventhal, H. (2005). Racial and ethnic differences in factors associated with early postpartum depressive symptoms. Obstetrics and Gynecology, 105, 1442-1450.
Inandi, T., Bugdayci, R., Sasmaz, T., Dunbar, P., & Sumer, H. (2005). Risk factors for depression in the first postnatal year: a Turkish study. Journal of Social Psychiatry and Psychiatric Epidemiology, 40, 725-730.
Ingram, J., & Taylor, J. (2007). Predictors of postnatal depression: using an antenatal needs assessment discussion tool. Journal of Reproductive and Infant Psychology, 25 (3), 210-222.
Josefsson, A., & Sydjo, G. (2007). A follow up study of postpartum depressed women:
recurrent maternal depressive symptoms and child behavior after four years. Archives of Womens Mental Health, 10, 141-145
Leahy-Warren, P. & McCarthy, G. (2007). Postnatal depression: prevalence, mothers’
perspectives, and treatments. Archives of Psychiatric Nursing, 21 (2), 91-100. Logsdon, C., Wisner, K.L., and Pinto-Folz. (2006a). The impact of postpartum
depression on Mothering. Journal of Obstetric, Gynecologic, & Neonatal Nursing. 35(5), 652-658.
Logsdon, M.C., Wisner, K., Billings, D.M., & Shanahan, B. (2006b). Raising the
awareness of primary care providers about postpartum depression. Issues in Mental Health Nursing, 27, 59-73.
Lumley, J. (2005). Attempts to prevent postnatal depression. British Medical Journal,
331, 5-6.
MacLennon, A., Wilson, D., & Taylor, A. (1996). The self-reported prevalence of postnatal depression in Australia and New Zealand. Journal of Obstetrics and Gynecology, 36, 313.
Malone, K., Papagni, K., Ramini, S., & Keltner, N. (2004). Antidepressants, antipsychotics, benzodiazepines and the breastfeeding dyad. Perspectives in Psychiatric Care, 40, 73-85. Matthey, S. (2004). Detection and treatment of postnatal depression (perinatal depression
or anxiety). Current Opinion in Psychiatry, 17, 21-29.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
McQueen, K., & Dennis, C. (2007). Development of a Postpartum Depression Best Practice Guideline: A Review of the Systematic Process. Journal of Nursing Care Quality. 22 (3), 199-204.
Misri, S., Kostaras, X., Fox, D., & Kostaras, D. (2000). The impact of partner support in
the treatment of postpartum depression. Canadian Journal of Psychiatry, 45, 554- 558.
Murray, L., Cooper, P.J., Wilson, A. & Romaniuk, H. (2003) Controlled trial of the short-
and long-term effect of psychological treatment of post-partum depression. British Journal of Psychiatry, 182, 420-427. Murray, L., Sinclair, D., Cooper, P., Ducournau, P., Turner, P., & Stein, A. (1999). The socioemotional development of 5 year-old children of postnatally depressed mothers. Journal of Child Psychology and Psychiatry, 40 (8), 1259-1271. Murray, L., Woolgar, M., Murray, J., & Cooper, P. (2003). Self-exclusion from health
care in women at high risk for postpartum depression. Journal of Public Health Medicine, 25 (2), 131-137.
O’Hara, M.W., & Swain, A.M. (1996). Rates and risks of postpartum depression- a meta-
analysis. International Review of Psychiatry, 8, 37-54 Orvaschel, H., Walsh-Allis, G., & Ye, W.J. (1988). Psychopathology in children of
parents with recurrent depression. Journal of Abnormal Child Psychology, 16 (1), 17-28
Ramsay, R. (1993). Postnatal depression. Lancet, 341, 1358. Ray, K.L., & Hodnett, E.D. (2001). Caregiver support for postpartum depression. Cochrane Database System Review, 3, CD000946. Rhodes, K.V., & Iwashhyna, T.J. (2007). Child injury risks are close to home: Parent
psychosocial factors associated with child safety. Maternal & Child Health Journal, 11 (3), 269-275.
Righhetti-Veltema, M., Conne-Perreard, E., Bousquet, A., & Manzano, J. (1998). Risk factors and predictive signs of postpartum depression. Journal of Affective Disorders, 49 (3), 167-80.
Ross, L.E., Campbell, V.L., Dennis, C., & Blackmore, E.R. (2006). Demographic characteristics of participants in studies of risk factors, prevention, and treatment of postpartum depression. Canadian Journal of Psychiatry, 51 (110), 704-710.
Ryan, D., Milis, L., & Misri, N. (2005). Depression during pregnancy. Canadian Family Physician, 51 (8), 1087-1093.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Seeley, S., Murray, L., & Cooper, P.J. (1996). Postnatal depression: the outcome for mothers and babies of health visitor intervention. Health Visitor, 69, 135-138.
Seyfried, L.S., & Marcus, S.M. (2003). Postpartum mood disorders. International Review of Psychiatry, 15, 231-242. Shaw, E., Levitt, C., Wong, S., & Kaczorowski, J. (2006). Systematic review of the literature on postpartum care: effectiveness of postpartum support to improve maternal parenting, mental health, quality of life, and physical health. Birth, 33 (3), 210-220. Sit, D., Rothschild, A. J., Wisner, K.L. (2006). A review of postpartum psychosis.
Journal of Women's Health, 15 (4), 352-368. Small, R., Lumley, J., and Yelland, J. (2003). Cross-cultural experiences of maternal depression: associations and contributing factors for Vietnamese, Turkish, and Filipino immigrant women in Victoria, Australia. Ethnicity and Health 8 (3), 189- 207. Stewart, D.E., Roberson, E., Dennis, C., Grace, M.A. & Wallington, T. (2003).
University Health Network Women’s Health Program. Postpartum depression: literature review of risk factors and interventions. www.toronto.ca/health/pdf/ppd_c_table.pdf
Surkan, P.J., Peterson, K.E., Hughes, M.D., & Gottlieb, B.R. (2006). The role of social
networks and support in postpartum women’s depression. Maternal and Child Health Journal. 10 (4), 375-383.
Sweet, M.A., & Applebaum, M.I. (2004). Is home visiting and effective strategy? Meta-
analytic review of home visiting programs for families with young children. Child Development, 75 (5), 1435-1456.
Sword, W., Watt, S., & Krueger, P. (2006). Postpartum health, service needs, and access
to care experiences of immigrant and Canadian women. Journal of Obstetrics and Gynecological and Neonatal Nurses, 35(6) 717-727.
Teng, L., Blackmore, E.R., Stewart, D.E. (2006). Healthcare worker’s perceptions of
barriers to care by immigrant women with postpartum depression: an exploratory qualitative study. Archives of Women’s Mental Health, 10 (3), 93-101.
Ueda, M., Yamashita, H., & Yoshida, K. (2006). Impact of infant health problems on
postnatal depression: Pilot study to evaluate a health visiting system. Psychiatry and Clinical Neurosciences, 60, (2) 182-189.
Vasquez, E. & Pitts, K. (2006). Red flags during home visitation: infants and toddlers.
Journal of Community Health Nursing, 23 (2), 123-131.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Webster, J., Pritchard, M.A., Creedy, D., and East, C. (2003). A simplified predictive index for the detection of women at risk for postnatal depression. Birth, 30 (2), 101-108.
Whitton, A., & Appleby, L. (1996). Maternal thinking and the treatment of postnatal
depression. International Review of Psychiatry, 8 (1), 73-78.
Wroblewski, M., & Tallon, D. (2004). Implementing a comprehensive postpartum depression support program. Association of Women’s Health, Obstetric and Neonatal Nurses Lifelines, 8 (3), 248-252.

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project
Appendices
Appendix 1 - Data Collection Forms used in the CRHVC 2005-2007 Postpartum Depression Research Project

#138, 1830 – 52nd Street SE Calgary, Alberta T2B 1N1
Ph: (403) 204-0800 Fax: (403) 204-0829
HOME VISITOR-CLIENT POSTPARTUM DEPRESSION
SUPPORT SURVEY INTENT: The purpose of this survey is to collect data about the supports and services
accessed by mothers who have screened positive for postpartum depression. Information obtained from this questionnaire will be used to better understand the services and supports accessed by these mothers.
TO COMPLETE: Supervisors are to distribute the packages to the Home Visitor (as indicated below),
who are to complete the forms in keeping with the time frames as specified below.
Mother’s Name:_____________________________ CID #:_______________________ Baby’s Name:____________________________________ Baby’s DOB:_____________ Home Visitor that Completed Screen: ________________________________
1st Screen Date:
Closure Date:
This package is to reflect postpartum care and service that were provided to the mother between ________________ (date) and ________________ (date).
Time frame covered for the Client Postpartum Depression Screen:
After the first positive screen and before client closure x

Prior Diagnosis / Treatment for Postpartum Depression To the best of your knowledge, has your client been diagnosed with Postpartum Depression by a Physician, Psychiatrist or Psychologist prior to the completion of the first positive Edinburgh Screen? □ Yes □ No □ Unknown If yes, did the professional make a referral to treat her postpartum depression? □ Yes □ No □ Unknown If yes, was the referral / treatment in the form of:
□ Medication □ Counseling and/or Personal Support □ Both At the time of the first positive Edinburgh Screen, was the mother accessing services for her postpartum depression? □ Yes □ No □ Unknown Referrals / Support Offered by the Home Visitor □ No referral was made to a Support Service because the mother was already accessing treatment or support. □ Additional supports or referrals for postpartum depression were offered in conjunction with those already being accessed (detail below if applicable). □ Home Visitor offered initial supports and/or services for postpartum depression (detail below).
Postpartum Depression Information Offered to the Mother This survey is to be completed by the Home Visitor who completed the Postpartum Depression Screens with the client.
Please indicate information offered for postpartum depression. Visit Date:
(DD/MM/YY) Describe PPD Information Given to Client (Handout, Article, Video, Etc): Additional Comments:
Postpartum Depression Supports / Services Offered to the Mother This survey is to be completed by the Home Visitor who completed the Postpartum Depression Screens with the client.
Please indicate supports/services that were/are beyond the general emotional supports offered for postpartum depression.
Visit Date: (DD/MM/YY)
Specify Referrals Made to Community Resources: (F) Family Dr; (S) Specialist Physician; (P) Postpartum Program;
(M) Mental Health Services; (C) Community Health Nurse
Did MOB Access Community Resource? (Check if applicable)
Additional Comments:
YES NO DON’T KNOW
CID #:_______________________ 2

Home Visitor Referrals for Postpartum Depression Please complete the following chart(s) IF a community resource referral for postpartum depression was made by the Home Visitor. Please complete one chart for each referral made. If no referrals were made by Home Visitor, proceed to Additional Questions on page #4.
Client Access or Non-Access of Postpartum Depression Community Resources Please Check Applicable Columns Below
Referral #1: Specify Community Resource Referral:__________________________ Factors that Influenced Client Attendance: Positively Influenced Decision to
Attend Negatively Influenced Decision to
Attend Unknown
Distance from Client’s Home Availability of Transportation Cost of Attending Resource Ability to Understand Language at Resource Ability to Make Childcare Arrangements Resource had Waitlist Family Support to Attend Resource Client’s Perceived Benefit of Resource Attendance Other Reasons (Please Specify)
Client Access or Non-Access of Postpartum Depression Community Resources Please Check Applicable Columns Below
Referral #1: Specify Community Resource Referral:__________________________ Factors that Influenced Client Attendance: Positively Influenced Decision to
Attend Negatively Influenced Decision to
Attend Unknown
Distance from Client’s Home Availability of Transportation Cost of Attending Resource Ability to Understand Language at Resource Ability to Make Childcare Arrangements Resource had Waitlist Family Support to Attend Resource Client’s Perceived Benefit of Resource Attendance Other Reasons (Please Specify)
CID #:_______________________ 3

Additional Questions 1) In your opinion, was the mom’s post partum depression a contributing factor to closure?
□ Yes □ No □ Unknown If yes, please comment: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 2) In your opinion, were there any other factors or issues that contributed to the mother’s postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 3) In your opinion, what was the greatest benefit that the Healthy Families Program had for your client? __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ 4) In your opinion, were there any other interventions that could have been undertaken to help your client address her postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ 5) If you have any other comments that you feel are important, please indicate them here: _________________________________________________________________________________________________ _________________________________________________________________________________________________ Completed By: _______________________ Date Completed: _________________
CID #:_______________________ 4

#138, 1830 – 52nd Street SE Calgary, Alberta T2B 1N1
Ph: (403) 204-0800 Fax: (403) 204-0829
HOME VISITOR-CLIENT POSTPARTUM DEPRESSION SUPPORT SURVEY
INTENT: The purpose of this survey is to collect data about the supports and services
accessed by mothers who have screened positive for postpartum depression. Information obtained from this questionnaire will be used to better understand the services and supports accessed by these mothers.
TO COMPLETE: Supervisors are to distribute the packages to the Home Visitor (as indicated below),
who are to complete the forms in keeping with the time frames as specified below.
Mother’s Name:_____________________________ CID #:_______________________ Baby’s Name:____________________________________ Baby’s DOB:_____________ Home Visitor that Completed Screens: ________________________________
Screen Dates (as applicable) 1st Screen:_________ 2nd Screen:_________ 3rd Screen:_________
This package is to reflect postpartum care and service that were provided to the mother between ________________ (date) and ________________ (date).
Time frame covered for the Client Postpartum Depression Screen:
1. 2. 3. 4. 5. 6.
After the first positive screen and before the second screen where the second screen was positive □ After the first positive screen and before the second screen where the second screen was negative x After the first negative screen and before the second screen where the second screen was positive □ After the second positive screen and before the third screen where the third screen was positive □ After the second positive screen and before the third screen where the third screen was negative □ After the third positive screen to present □

Prior Diagnosis / Treatment for Postpartum Depression To the best of your knowledge, has your client been diagnosed with Postpartum Depression by a Physician, Psychiatrist or Psychologist prior to the completion of the first positive Edinburgh Screen? □ Yes □ No □ Unknown If yes, did the professional make a referral to treat her postpartum depression? □ Yes □ No □ Unknown If yes, was the referral / treatment in the form of:
□ Medication □ Counseling and/or Personal Support □ Both At the time of the first positive Edinburgh Screen, was the mother accessing services for her postpartum depression? □ Yes □ No □ Unknown Referrals / Support Offered by the Home Visitor □ No referral was made to a Support Service because the mother was already accessing treatment or support. □ Additional supports or referrals for postpartum depression were offered in conjunction with those already being accessed (detail below if applicable). □ Home Visitor offered initial supports and/or services for postpartum depression (detail below).
Postpartum Depression Information Offered to the Mother This survey is to be completed by the Home Visitor who completed the Postpartum Depression Screens with the client.
Please indicate information offered for postpartum depression. Visit Date:
(DD/MM/YY) Describe PPD Information Given to Client (Handout, Article, Video, Etc): Additional Comments:
Postpartum Depression Supports / Services Offered to the Mother This survey is to be completed by the Home Visitor who completed the Postpartum Depression Screens with the client.
Please indicate supports/services that were/are beyond the general emotional supports offered for postpartum depression.
Visit Date: (DD/MM/YY)
Specify Referrals Made to Community Resources: (F) Family Dr; (S) Specialist Physician; (P) Postpartum Program;
(M) Mental Health Services; (C) Community Health Nurse
Did MOB Access Community Resource? (Check if applicable)
Additional Comments:
YES NO DON’T KNOW
CID #:_______________________ 2

Home Visitor Referrals for Postpartum Depression Please complete the following chart(s) IF a community resource referral for postpartum depression was made by the Home Visitor. Please complete one chart for each referral made. If no referrals were made by Home Visitor, proceed to Additional Questions on page #4.
Client Access or Non-Access of Postpartum Depression Community Resources Please Check Applicable Columns Below
Referral #1: Specify Community Resource Referral:__________________________ Factors that Influenced Client Attendance: Positively Influenced Decision to
Attend Negatively Influenced Decision to
Attend Unknown
Distance from Client’s Home Availability of Transportation Cost of Attending Resource Ability to Understand Language at Resource Ability to Make Childcare Arrangements Resource had Waitlist Family Support to Attend Resource Client’s Perceived Benefit of Resource Attendance Other Reasons (Please Specify)
Client Access or Non-Access of Postpartum Depression Community Resources Please Check Applicable Columns Below
Referral #1: Specify Community Resource Referral:__________________________ Factors that Influenced Client Attendance: Positively Influenced Decision to
Attend Negatively Influenced Decision to
Attend Unknown
Distance from Client’s Home Availability of Transportation Cost of Attending Resource Ability to Understand Language at Resource Ability to Make Childcare Arrangements Resource had Waitlist Family Support to Attend Resource Client’s Perceived Benefit of Resource Attendance Other Reasons (Please Specify)
CID #:_______________________ 3

Additional Questions 1) In your opinion, were there any other factors or issues that contributed to the mother’s postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 2) In your opinion, if there was a change in the results of the first and second Edinburgh Screen, were there any specific events or circumstances that influenced this change?
□ Yes □ No □ Unknown If yes, please comment: __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ 3) In your opinion, what was the greatest benefit that the Healthy Families Program had for your client? __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ 4) In your opinion, were there any other interventions that could have been undertaken to help your client address her postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ 5) If you have any other comments that you feel are important, please indicate them here: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ Completed By: _______________________ Date Completed: _________________
CID #:_______________________ 4

#138, 1830 – 52nd Street SE Calgary, Alberta T2B 1N1
Ph: (403) 204-0800 Fax: (403) 204-0829
HOME VISITOR-CLIENT POSTPARTUM DEPRESSION SUPPORT SURVEY
INTENT: The purpose of this survey is to collect data about the supports and services
accessed by mothers who have screened positive for postpartum depression. Information obtained from this questionnaire will be used to better understand the services and supports accessed by these mothers.
TO COMPLETE: Supervisors are to distribute the packages to the Home Visitor (as indicated below),
who are to complete the forms in keeping with the time frames as specified below.
Mother’s Name:_____________________________ CID #:_______________________ Baby’s Name:____________________________________ Baby’s DOB:_____________ Home Visitor that Completed Screens: ________________________________
Screen Dates (as applicable) 1st Screen:_________ 2nd Screen:_________ 3rd Screen:_________
This package is to reflect postpartum care and service that were provided to the mother between ________________ (date) and ________________ (date).
Time frame covered for the Client Postpartum Depression Screen:
1. 2. 3. 4. 5. 6.
After the first positive screen and before the second screen where the second screen was positive x After the first positive screen and before the second screen where the second screen was negative □ After the first negative screen and before the second screen where the second screen was positive □ After the second positive screen and before the third screen where the third screen was positive □ After the second positive screen and before the third screen where the third screen was negative □ After the third positive screen to present □

Prior Diagnosis / Treatment for Postpartum Depression To the best of your knowledge, has your client been diagnosed with Postpartum Depression by a Physician, Psychiatrist or Psychologist prior to the completion of the first positive Edinburgh Screen? □ Yes □ No □ Unknown If yes, did the professional make a referral to treat her postpartum depression? □ Yes □ No □ Unknown If yes, was the referral / treatment in the form of:
□ Medication □ Counseling and/or Personal Support □ Both At the time of the first positive Edinburgh Screen, was the mother accessing services for her postpartum depression? □ Yes □ No □ Unknown Referrals / Support Offered by the Home Visitor □ No referral was made to a Support Service because the mother was already accessing treatment or support. □ Additional supports or referrals for postpartum depression were offered in conjunction with those already being accessed (detail below if applicable). □ Home Visitor offered initial supports and/or services for postpartum depression (detail below).
Postpartum Depression Information Offered to the Mother This survey is to be completed by the Home Visitor who completed the Postpartum Depression Screens with the client.
Please indicate information offered for postpartum depression. Visit Date:
(DD/MM/YY) Describe PPD Information Given to Client (Handout, Article, Video, Etc): Additional Comments:
Postpartum Depression Supports / Services Offered to the Mother This survey is to be completed by the Home Visitor who completed the Postpartum Depression Screens with the client.
Please indicate supports/services that were/are beyond the general emotional supports offered for postpartum depression.
Visit Date: (DD/MM/YY)
Specify Referrals Made to Community Resources: (F) Family Dr; (S) Specialist Physician; (P) Postpartum Program;
(M) Mental Health Services; (C) Community Health Nurse
Did MOB Access Community Resource? (Check if applicable)
Additional Comments:
YES NO DON’T KNOW
CID #:_______________________ 2

Home Visitor Referrals for Postpartum Depression Please complete the following chart(s) IF a community resource referral for postpartum depression was made by the Home Visitor. Please complete one chart for each referral made. If no referrals were made by Home Visitor, proceed to Additional Questions on page #4.
Client Access or Non-Access of Postpartum Depression Community Resources Please Check Applicable Columns Below
Referral #1: Specify Community Resource Referral:__________________________ Factors that Influenced Client Attendance: Positively Influenced Decision to
Attend Negatively Influenced Decision to
Attend Unknown
Distance from Client’s Home Availability of Transportation Cost of Attending Resource Ability to Understand Language at Resource Ability to Make Childcare Arrangements Resource had Waitlist Family Support to Attend Resource Client’s Perceived Benefit of Resource Attendance Other Reasons (Please Specify)
Client Access or Non-Access of Postpartum Depression Community Resources Please Check Applicable Columns Below
Referral #1: Specify Community Resource Referral:__________________________ Factors that Influenced Client Attendance: Positively Influenced Decision to
Attend Negatively Influenced Decision to
Attend Unknown
Distance from Client’s Home Availability of Transportation Cost of Attending Resource Ability to Understand Language at Resource Ability to Make Childcare Arrangements Resource had Waitlist Family Support to Attend Resource Client’s Perceived Benefit of Resource Attendance Other Reasons (Please Specify)
CID #:_______________________ 3

Additional Questions 1) In your opinion, were there any other factors or issues that contributed to the mother’s postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 2) In your opinion, if there was a change in the results of the first and second Edinburgh Screen, were there any specific events or circumstances that influenced this change?
□ Yes □ No □ Unknown If yes, please comment: __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ 3) In your opinion, what was the greatest benefit that the Healthy Families Program had for your client? __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ 4) In your opinion, were there any other interventions that could have been undertaken to help your client address her postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ 5) If you have any other comments that you feel are important, please indicate them here: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ Completed By: _______________________ Date Completed: _________________
CID #:_______________________ 4

#138, 1830 – 52nd Street SE Calgary, Alberta T2B 1N1
Ph: (403) 204-0800 Fax: (403) 204-0829
HOME VISITOR-CLIENT POSTPARTUM DEPRESSION SUPPORT SURVEY
INTENT: The purpose of this survey is to collect data about the supports
and services accessed by mothers who have screened positive for postpartum depression. Information obtained from this questionnaire will be used to better understand the services and supports accessed by these mothers.
TO COMPLETE: Supervisors are to distribute the packages to the Home Visitor (as
indicated below), who are to complete the forms in keeping with the time frames as specified below.
Mother’s Name:_____________________________ CID #:_______________________ Baby’s Name:____________________________________ Baby’s DOB:_____________ Home Visitor that Completed Screens: ________________________________
Screen Dates (as applicable) 1st Screen:_________ 2nd Screen:_________ 3rd Screen:_________
This package is to reflect postpartum care and service that were provided to the mother between ________________ (date) and ________________ (date).
Time frame covered for the Client Postpartum Depression Screen:
1. 2. 3. 4. 5. 6.
After the first positive screen and before the second screen where the second screen was positive □ After the first positive screen and before the second screen where the second screen was negative □ After the first negative screen and before the second screen where the second screen was positive x After the second positive screen and before the third screen where the third screen was positive □ After the second positive screen and before the third screen where the third screen was negative □ After the third positive screen to present □
1
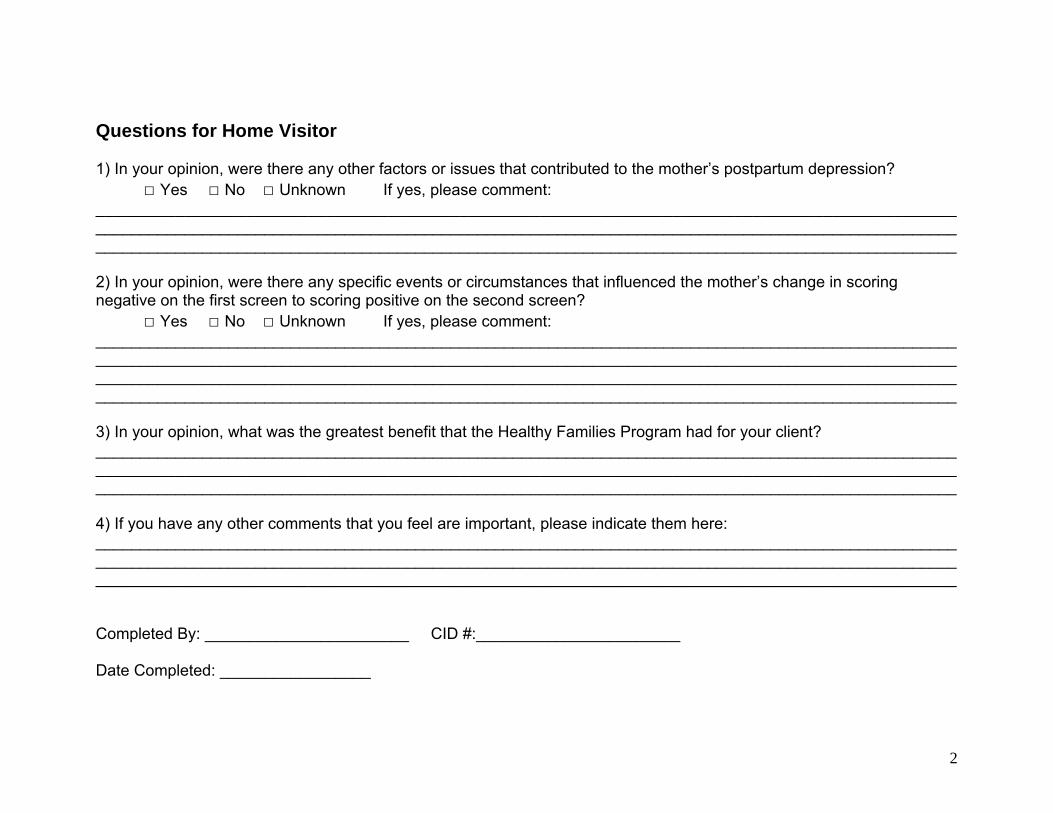
Questions for Home Visitor 1) In your opinion, were there any other factors or issues that contributed to the mother’s postpartum depression?
□ Yes □ No □ Unknown If yes, please comment: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 2) In your opinion, were there any specific events or circumstances that influenced the mother’s change in scoring negative on the first screen to scoring positive on the second screen?
□ Yes □ No □ Unknown If yes, please comment: __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ 3) In your opinion, what was the greatest benefit that the Healthy Families Program had for your client? __________________________________________________________________________________________________________________________________________________________________________________________________ _________________________________________________________________________________________________ 4) If you have any other comments that you feel are important, please indicate them here: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ Completed By: _______________________ CID #:_______________________ Date Completed: _________________
2

The Calgary Regional Home Visitation Collaborative Postpartum Depression Research Project