Fighting Against Ebola: Public Health and Nepal
41
- SHRADDHA ACHARYA
-
Upload
mmc-iom-nepal -
Category
Health & Medicine
-
view
101 -
download
0
Transcript of Fighting Against Ebola: Public Health and Nepal
- SHRADDHA ACHARYA
INTRODUCTION
Ebola virus disease (EVD), formerly known asEbola hemorrhagic fever, is a severe, oftenfatal illness in humans.
The average EVD case fatality rate is around50%. Case fatality rates have varied from 25%to 90% in past outbreaks.

HISTORY
Ebola virus disease (EVD) first appeared in 1976 in 2 simultaneous outbreaks, one in Sudan (Nzara), and the other in, Democratic Republic of Congo (Yambuku).
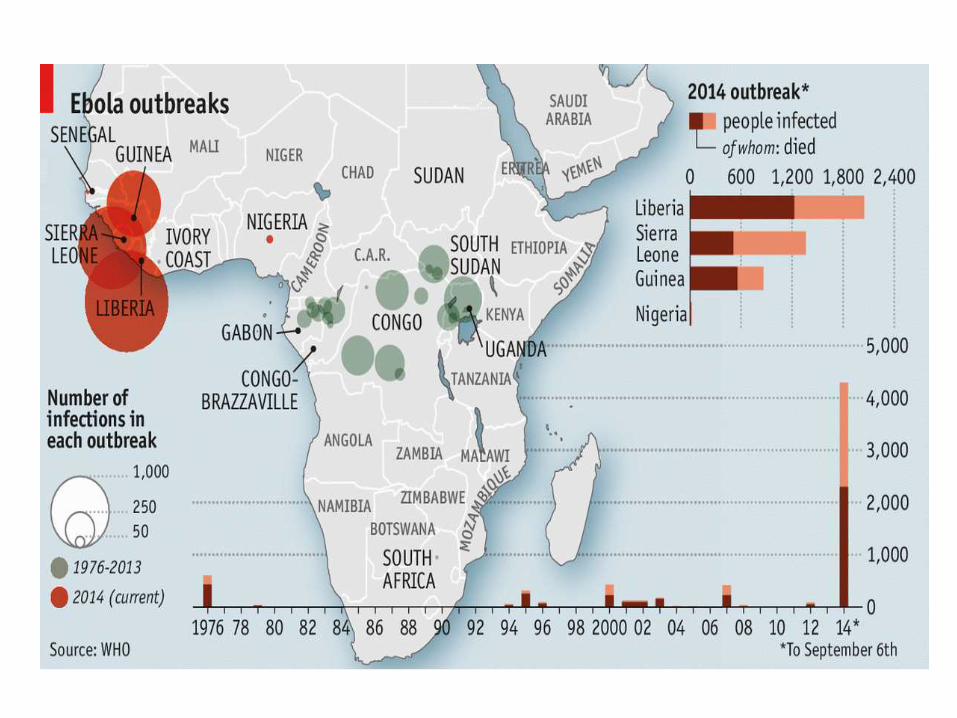
The current outbreak in west Africa, (first cases notified in March 2014), is the largest and most complex Ebola outbreak since the Ebola virus was first discovered in 1976.
HISTORY (…contd)
It has also spread between countries starting in Guinea then spreading across land borders to Sierra Leone and Liberia, Nigeria and Senegal.
A separate, unrelated Ebola outbreak began in Boende, Equateur, an isolated part of the Democratic Republic of Congo.
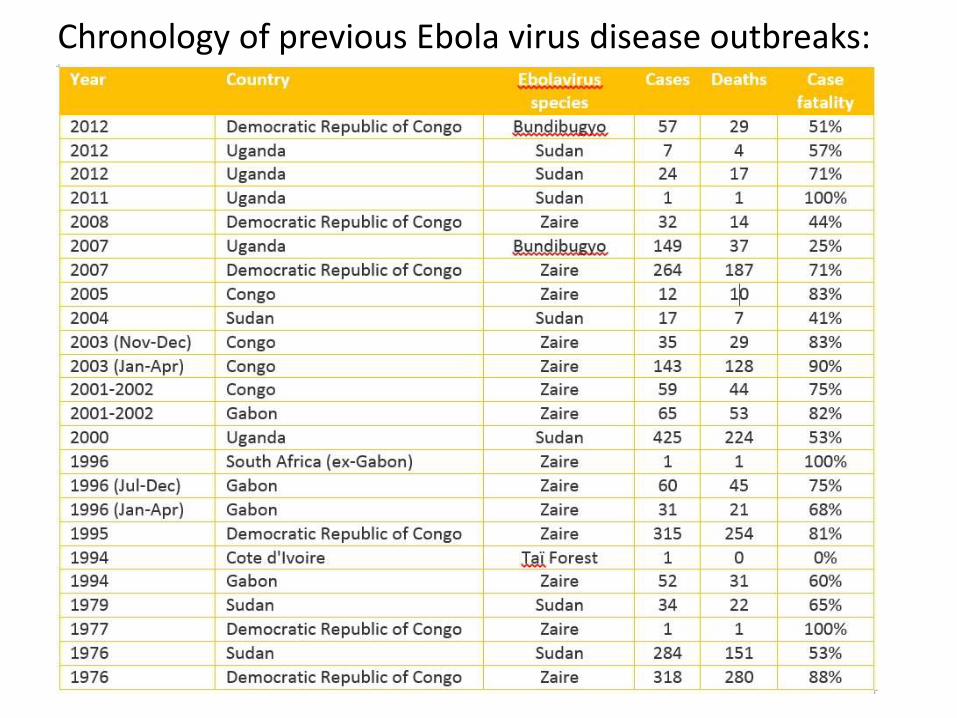
Chronology of previous Ebola virus disease outbreaks:
Ebola Virus
Family: Filoviridae
Genera: Cuevavirus, Marburgvirus, and Ebolavirus
Species: Zaire, Bundibugyo, Sudan, Reston and Tai Forest
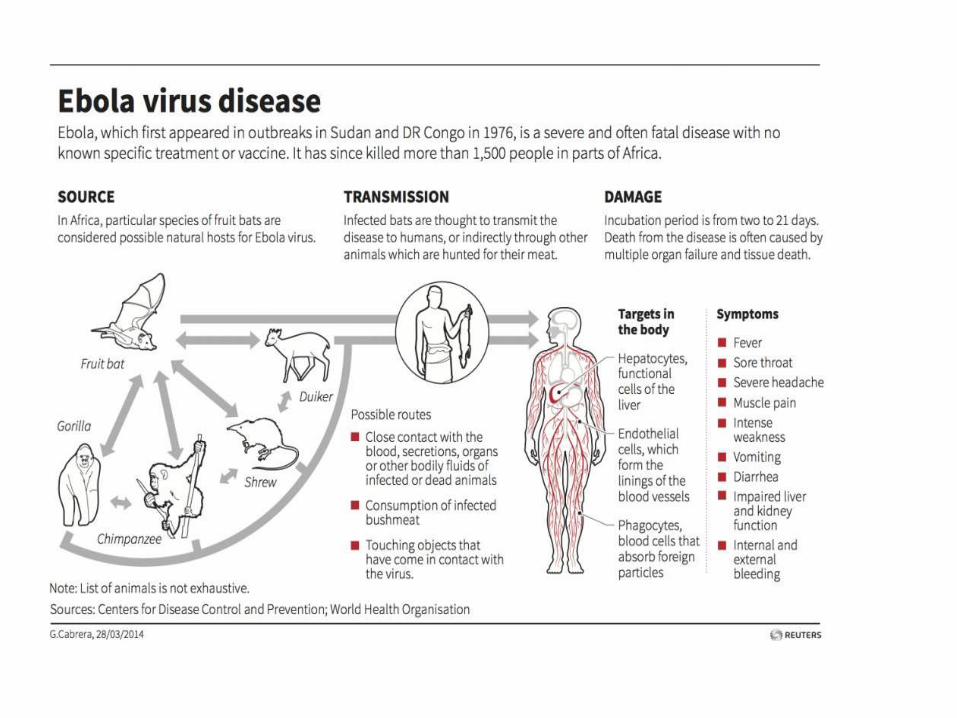
TRANSMISSION
Ebola spreads through human-to-human transmission via direct contact (through broken skin or mucous membranes in, for example, the eyes, nose, or mouth) with:blood or body fluids (including but not limited to urine, saliva, sweat, feces, vomit, breast milk, and semen) of a person who is sick with Ebola,objects (like needles and syringes) that have been contaminated with the virus, materials (e.g.bedding, clothing) contaminated with these fluids,infected fruit bats or primates (apes and monkeys)

TRANSMISSION (….contd)
People remain infectious as long as their blood and body fluids, including semen and breast milk, contain the virus.
People who have recovered from the disease can still transmit the virus through their semen for up to 7 weeks after recovery from illness.
SYMPTOMS • Fever
• Severe headache
• Muscle pain
• Weakness
• Fatigue
• Diarrhea
• Vomiting
• Abdominal (stomach) pain
• Unexplained hemorrhage (bleeding or bruising)
*The incubation period of Ebola is 2 to 21 days.

DIAGNOSIS
Confirmation that symptoms are caused by Ebola virus infection are made using the following investigations:
• antibody-capture enzyme-linked immuno sorbent assay (ELISA)
• antigen-capture detection tests• serum neutralization test• reverse transcriptase polymerase chain reaction
(RT-PCR) assay• electron microscopy• virus isolation by cell culture.

Prevention and controlGood outbreak control relies on:
- applying a package of interventions/case management
- surveillance and contact tracing- a good laboratory service,- safe burials- social mobilization.
Risk reduction:• Reducing the risk of wildlife-to-human
transmission• Reducing the risk of human-to-human
transmission• Outbreak containment measures
Treatment and vaccines
• Yet no proven treatment available for EVD.
• But, supportive care-rehydration with oral or intravenous fluids, maintaining oxygen status and blood pressure and treatment of specific symptoms, improves survival.
• No licensed vaccines are available yet.
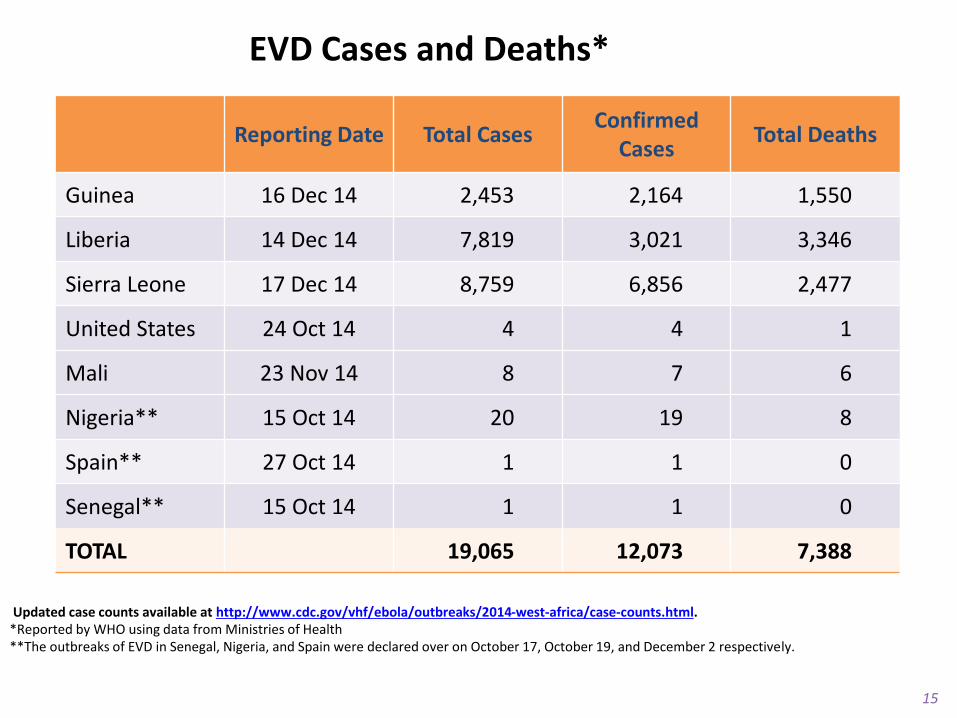
EVD Cases and Deaths*
Updated case counts available at http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html. *Reported by WHO using data from Ministries of Health **The outbreaks of EVD in Senegal, Nigeria, and Spain were declared over on October 17, October 19, and December 2 respectively.
15
Reporting Date Total CasesConfirmed
CasesTotal Deaths
Guinea 16 Dec 14 2,453 2,164 1,550
Liberia 14 Dec 14 7,819 3,021 3,346
Sierra Leone 17 Dec 14 8,759 6,856 2,477
United States 24 Oct 14 4 4 1
Mali 23 Nov 14 8 7 6
Nigeria** 15 Oct 14 20 19 8
Spain** 27 Oct 14 1 1 0
Senegal** 15 Oct 14 1 1 0
TOTAL 19,065 12,073 7,388
WHY US
PUBLIC HEALTH??
Firstly, Because
It’s a PUBLIC HEALTH ISSUE
• Outbreaks
• High case fatality
• No licensed vaccine for EVD
Secondly,
EBOLA : A GLOBAL RIGHTS INJUSTICE
WHY STILL NO
VACCINE FOR EBOLA?
EBOLA REALLY THAT DIFFICULT
VIRUS TO INTERVENE?
EBOLA: TERRIBLE BUSINESS TO
PHARMACEUTICAL COMPANIES?
OR
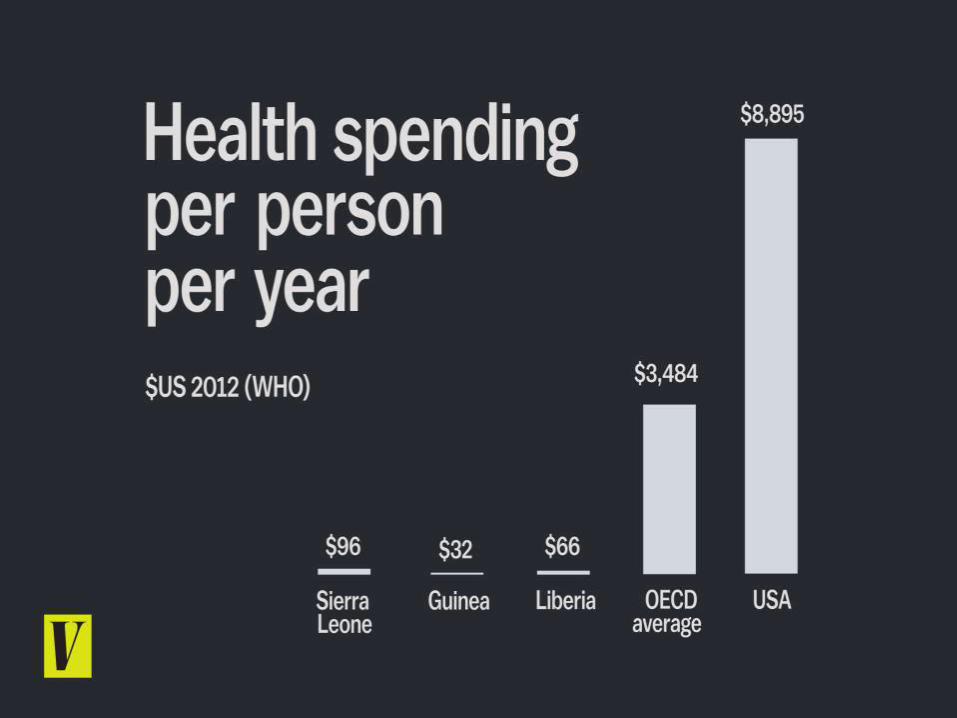
60 % of medical research is undertaken by private
pharmaceutical companies, who seek to obtain and exploit patents. This distorts medical priorities, as research is aimed at creating medications for which there is a stable demand from patients who have the capacity to pay. Chronic illnesses in high income countries are thus the research preference of these companies, as they involve patients that can pay for expensive medicine over the course of many years. -An article by John Rottingen and others, published in 2013 in The Lancet

Ebola is a poor person’s disease, which does not threaten the
public health of rich countries, as previous outbreaks had affected a
few hundred people and had been confined to specific areas of
Africa.
90 percent of medical research is undertaken with resources from rich countries, it is not surprising that public financing to confront Ebola has also been scarce.
Patents create a disincentive for research on products that permit an immediate cure or prevent illness in poor people. Research to cure Ebola falls into the latter category, as the vaccine would be applied only one or two times, and treatments would be short-term. And, even worse, potential clients would be in Africa.
HENCE,
A TERRIBLE BUSINESS
!!!

• The patent system and the choices of rich countries have led to tropical contagious diseases, such as Ebola or malaria, being ignored by medical research, which dedicates only 1% of worldwide research funds to these illnesses and funds only appear when these illnesses get close to Europe and North America
ARE THESE ONLY THE SOLUTIONS?
• Find patients
• Isolate them
• Contact the patients
• Educate them
• Strictly follow the treatment
Why don’t states or philanthropic organizations
work for the outbreak, which are not guided by profitability concerns?

WHY A CONCERN TO NEPAL?

3,000-5,000 Nepalese in Ebola zone


According to Statistics from the Department of Foreign Employment, 2014:
• Around 200 Nepalese people went to West African countries in the past year.
• Eighty Nepalese got permits to work in Liberia, around 35 in Guinea and 100 in Nigeria, 500 work permits for Congo.
• As many as 25,000 Nepalese are believed to be working in Africa.
• Half the 3,000 workforce in the epidemic-hit West African countries is in Nigeria alone.

• Non-resident Nepalese in Africa say there could be some 200 compatriots in Guinea and 1,000 in Kenya.
• Hundreds of its security officers and personnel are deployed under the UN peacekeeping missions in West African nations, Liberia (20 personnel), Congo(1049).
• Cross Border with India and China

Is Nepal prepared for the possible Ebola
outbreak?
Although there are two private-run healthcenters inside the TIA, the country’s soleinternational airport, exposing the nation tocommunicable diseases confronting the worldincluding the EVD, for emergency treatment ofpassengers, they do not screen passengers.
MoHP has also decided to manage treatment ofEbola virus at Bir Hospital and Sukraraj Tropicaland Infectious Disease Hospital (STIDH) inKathmandu but they neither have diagnostic kits,ICUs nor separate wards to quarantine patients,or other resources to deal with a possibleepidemic.
Government decided to apply precautionarymeasures with immediate effects, settingquarantine health desks border checkpoints (asKodari- Tatopani, Mechi-Kakadvitta, Birgunj,Bhairahawa, Nepalgunj, Dhangadhi andMahendranagar) as the World HealthOrganization (WHO) declared Ebola threat asinternational health emergency.
But, is it possible that the border check posts canbe equipped with resources to deal with Ebolacases when the center lacks any such facility?
TIA Health desk

Seen As:
A problem of developing countries

SO, IS EBOLA JUST A CLINICAL
MANIFESTATION TO YOU?
ORYOU SEE SOMETHING
MORE TO IT?
REFERENCES
www.who.int/mediacentre/factsheets/fs103/en/ www.cdc.gov/vhf/ebola/about.html Ebola Virus- CIWEC Clinic “The Nepalese Army in UN Peace Support Operations”,
BPOTC “Nepal defenceless against Ebola risk” , Manish Gautam
www.ekantipur.com/2014/08/10/top-story/nepal...ebola.../
“Ebola: Tragedy or Injustice?”, Rodrigo Uprimny “Nepal ill-prepared for possible Ebola outbreak”, Arjun
Poudel

FINALLY,