Fiber Optic Monitoring for Spinal Cord Ischemia
13
Fiber Optic Monitoring for Spinal Cord Ischemia Thomas V. Bilfinger, MD 1 , ScD; Robert M. Galler, DO 2 ; Rickson Mesquita, PhD 3 ; Angela D’Souza, PhD 4 ; Asher Emanuel, MD 5 ; Arjun Yodh, PhD 3* ; Thomas F. Floyd, MD 4,5,6* . Stony Brook University, Department of Surgery 1 , Neurosurgery 2 , Biomedical Engineering 4 , Anesthesiology 5 University of Pennsylvania, Department of Physics and Astronomy 3 , Surgery 6 Principal Investigators*
description
Fiber Optic Monitoring for Spinal Cord Ischemia. Thomas V. Bilfinger, MD 1 , ScD; Robert M. Galler, DO 2 ; Rickson Mesquita, PhD 3 ; Angela D’Souza , PhD 4 ; Asher Emanuel, MD 5 ; Arjun Yodh, PhD 3* ; Thomas F. Floyd, MD 4,5,6* . - PowerPoint PPT Presentation
Transcript of Fiber Optic Monitoring for Spinal Cord Ischemia

Fiber Optic Monitoring for Spinal Cord
IschemiaThomas V. Bilfinger, MD1, ScD; Robert M. Galler, DO2; Rickson Mesquita, PhD3; Angela D’Souza, PhD4; Asher
Emanuel, MD5; Arjun Yodh, PhD3*; Thomas F. Floyd, MD4,5,6*.
Stony Brook University, Department of Surgery1, Neurosurgery2, Biomedical Engineering4, Anesthesiology5
University of Pennsylvania, Department of Physics and Astronomy3, Surgery6
Principal Investigators*

Aortic Surgery & Spinal Cord Ischemia
Frequency of spinal ischemia after aortic procedures varies between 0.2% in elective AAA to 40% in acute dissections requiring repair with Type 2 aneurysm-repairs having an up to 21% incidence.
Hypotension, hypoxia, vasospasm, inflammation and edema, and hemorrhage all propagate spinal ischemia after injury as well as the number of interrupted segmental arteries.
Prevention of secondary injury from ischemia may assist in limiting disability.

The TechnologyDiffuse Correlation Spectroscopy: Quantifies the fluctuations of
light scattered in tissues. Fluctuations in light scattering occur due to the motion of scatterers in tissue, mainly red blood cells. The greater the scattering, the greater the blood flow. Boas, D.A., L.E. Campbell, and A.G. Yodh, Scattering and Imaging with Diffusing Temporal Field Correlations. Phys Rev
Lett, 1995. 75(9): p. 1855-1858. Durduran, T., R. Choe, W.B. Baker, and A.G. Yodh, Diffuse optics for tissue monitoring and tomography. Rep. Prog. Phys.,
2010. 73: 076701.
Diffuse Optical Spectroscopy: Quantifies the reflectance or absorbance of light by tissue chromophores and fluctuations in these measurements. Oxy- and deoxy-hemoglobin concentrations (e.g. cHbO2, cHb respectively) are the most significant tissue absorbers in the NIR.

Experimental Design
Adult Dahl sheep underwent general anesthesia with controlled ventilation.
Arterial catheters placed in carotid and femoral arteries. Endo-aortic balloon placed via femoral artery and advanced to
proximal descending thoracic aorta. DCS/DOC probe was tested after placement in the mid-thoracic
region, after both open (laminectomy) and percutaneous approaches, and in intrathecal or epidural locations.
Spinal blood flow and oxygenation, along with mean arterial pressure (femoral & carotid) were measured during blood pressure manipulation via sodium nitroprusside, neosynephrine or vasopressin administration, and after intra-aortic balloon inflation in the superior descending thoracic aorta.

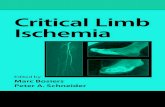
Spinal Cord Blood Supply
Nicholas Theodore, M.D., Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona

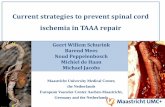
DCS/DOS Sensor
SD1
D2
Source wavelength may be switched between 685nm, 785nm, and 830 nm to effect DCS or DOS measurements
DCS/DOS Sensor: The current probe in has one source and two detectors. The source fiber is shared for both DCS and DOS through an optical switch. Each detector location has a pair of single mode and multimode fibers. The single mode fibers are used to detect the blood flow, as monitored by DCS, while the multimode fibers detect the blood oxygenation measured using DOS. The probe is very flexible and thin (less than 1 mm thick), and is about 3 m long, which permits flexibility in accommodating the instrument in the operating room. The source-detector separations are 1.0 cm and 2.0 cm, which allows the technique to interrogate to depths of approximately 0.0-1.0 cm.

Open Subdural Probe Placement

Percutaneous Subdural Placement

A bolus of 400 µg neosynephrine results in a parallel increase in Mean Arterial Pressure (MAP) and blood flow. A bolus of 4 units vasopressin also resulted in a parallel increase in MAP and blood flow. For vasopression, blood flow returns to baseline levels in spite of persistent elevation of MAP, likely the result of autoregulation.
Blood Flow-DCS

Repetitive boluses of sodium nitroprusside (400ug) cause parallel decreases in MAP and blood flow. Repetitive boluses of sodium nitroprusside (400ug) cause parallel decreases in MAP and blood flow. Repetitive boluses of sodium nitroprusside (400ug) cause parallel decreases in MAP and blood flow. Repetitive boluses of sodium nitroprusside (400ug) cause parallel decreases in MAP and blood flow.
Repetitive boluses of sodium nitroprusside (400ug) cause parallel decreases in MAP and blood flow.
Blood Flow-DCS

Repetitive boluses of sodium nitroprusside (400ug) cause parallel decreases in MAP and blood flow.
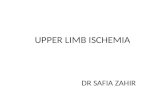
Balloon inflation in the proximal descending thoracic aorta results in a marked increase in MAP above the balloon, as measured by the carotid artery catheter, while pressure below the balloon, as measured by the femoral artery catheter, falls to near zero. Blood flow in the thoracic aorta dramatically increases in parallel with the carotid MAP, but falls back to baseline likely due to either autoregulation and or due to developing ischemia.
Percutaneous-Proximal Descending Aortic Balloon Inflation
Blood Flow-DCS

Tissue Oxygenation-DOSPercutaneous-Proximal Descending Aortic Balloon
Inflation
Following balloon inflation, tissue oxygenation remains steady or increases slightly.

Results SummaryBlood Flow data correlates well with changes in
MAPFiber-optic probe effectively measuring changes in
blood flow in the spinal cord in both subdural and epidural positions.
Probe can be placed via open and percutaneous approaches