Fever in Infants and Children: Sepsis, Meningitis, and Occult Bacteremia Rashmi Srivastava, MD...
33
Fever in Infants and Children: Sepsis, Meningitis, and Occult Bacteremia Rashmi Srivastava, MD Department of Child Health
-
Upload
greta-abney -
Category
Documents
-
view
224 -
download
0
Transcript of Fever in Infants and Children: Sepsis, Meningitis, and Occult Bacteremia Rashmi Srivastava, MD...

Fever in Infants and Children:Sepsis, Meningitis, and Occult
Bacteremia
Rashmi Srivastava, MD
Department of Child Health

Fever Phobia• Fever is the most common pediatric complaint, second only to
routine care for clinic visits, and the most common reason kids are brought to the ER.
• In the Middle Ages, fever was felt to be a marker of death or divine punishment.
• Some feel true fever is harmful: 1/3 parents thought 38-40ºC(100.4-104ºF), 2/3 40-41ºC(104-106ºF), and all thought brain damage >41ºC(106ºF).
• 5-20% have no localizing signs on PE with no history to explain the fever.
• The majority of kids with fever do not have a serious illness, although a small percentage harbor or may develop a serious bacterial infection.

‘True’ Fever
• Occurs when IL-1, IL-6, TNF-ά or other cytokines are released from monocytes and macrophages in response to infection, tissue injury, drugs, and other inflammatory processes, increasing the body’s set point. The anterior hypothalamus maintains an inherent set point near 36ºC(98.6ºF).
• Normal circadian rhythm, which is highest(up to 2ºC, 3ºF) ~6pm and lowest at 6am. This accounts for increased volume of ER visits that peaks in the evening. Most true fevers follow this diurnal pattern.

‘False’ fever, aka hyperthermia• Does not directly increase the body’s set point.
• CNS disease that directly affects the hypothalamus--ICH, infection.
• Diseases that increase the body’s production of heat--hyperthyroidism, malignant hyperthermia, salicylate overdose.
• Excess heat load--child left in a car or left next to a heater for too long.
• Defective heat loss mechanisms--burns, heat stroke, drugs that compromise blood flow and sweating mechanisms.
• Normal causes of temperature elevation include physical activity, ovulation, and environmental temperature.

Reliable Temperature Measurement
• All measurements are estimates of the body’s true core temp—central circulation=aorta and pulmonary artery.
• RECTAL—gold standard
• Esophageal—accurate but impractical
• Tactile and axillary—inaccurate, varies considerably with environmental temperature
• Tympanic—inaccurate in age <3 years

Benefits of fever
• The hypothalamus will not allow the temp to rise above 41.5ºC(107ºF).
• WBCs work best and kill the most bacteria at 38-40ºC(100.4-104ºF).
• Neutrophils make more superoxide anion, and there is more and increased activity of interferon.
• Coxsackie and polio virus replication is directly inhibited.

Fever without a source(FWS)
• 5 to 20% of febrile children have no localizing signs on PE and nothing in the history to explain the fever. By definition, less than 7 days.
• FWS(like fever) is most common in children younger than age 5, with a peak prevalence between 6 and 24 months of age.• Those <6 months retain protective maternal antibodies
against common organisms, while those 18-24 months old are more immune competent, and are at a lower risk of developing bacteremia

Diagnostic Assessment in Children
• Age is important as 1) etiologic pathogens, 2) clinical exam, and 3) immune system capacity changes as the newborn ages.
• Most break them into the first 2-4 weeks of life(neonatal), 1-3 months, and 3 to 36 months.

Neonatal• PE is felt to be unreliable in detecting many serious bacterial
infections. Meningitis should always be considered—up to 10% appear well, only 15% have a bulging fontanelle, and 10-15% have nuchal rigidity. So, a high index of suspicion is important!!! ~20% will not have fever initially.• Hyperthermia or hypothermia• Lethargy or irritability• Poor feeding or vomiting• Apnea• Dyspnea• Jaundice• Hypotension• Diarrhea or abdominal distension• Bulging fontanelle• seizures

Neonates
• The majority of febrile neonates presenting to the ED have a nonspecific viral illness
• 12% have serious bacterial infections (SBI)• Infected by more virulent bacteria• More likely to develop serious sequelae from viral
infections• GBBS is associated with high rates of meningitis(39%),
non-meningeal foci(10%), and sepsis(7%)• The most common bacterial infections are UTI and occult
bacteremia

Neonatal
Early Onset<7 DaysGroup B Strep
E. Coli
Listeria Monocytogenes
Enterobacteriaceae
Enterococcus
Strep viridans
Strep Pneumoniae
Hemophilus influenza nt
Herpes simplex
Later Onset>7 DaysGroup B Strep
Listeria Monocytogenes
Enterobacteriaceae
Strep Pneumoniae
Neisseria meningitidis
Herpes simplex

Neonatal
• Risk Factors• Preterm• Membrane rupture: before labor onset or prolonged>12
hours• Chorioamnionitis or maternal peripartum fever• UTI• Multiple pregnancy• Hypoxia or Apgar score <6• Poverty or age <20
• 1/3-1/2 neonatal sepsis will have no risk factors!

Neonatal• Screening tests: WBC<5000 or >20,000, PMN <4000,
I:T>.2, Plt<100,000, CRP>1, LFTs elevated(suggest HSV)• So, if <28 days of age and rectal temp> 38ºC
• Admit• Blood Culture• Urine Culture—cath specimen• Lumbar Puncture
• Cell count, protein, glucose, culture, PCR
• Parenteral Antibiotics• Ampicillin + Gentamicin(Cefotaxime), consider Acyclovir(primary
maternal infxn, esp if delivered vaginally, PROM, fetal scalp electrodes, skin eye or mouth lesions, seizures, CSF pleocytosis)

Infants 1 to 3 months• Causes
• HSV(17% are 15 days to 6 weeks of age)• Bacterial sepsis/meningitis
• Group B Strep, S. Pneumoniae, H. influenza, N. meningitidis, Enterobacteriaceae
• Bone and joint infections• UTI• Bacterial enteritis(esp Salmonella)• Pneumonia• Enterovirus sepsis/meningitis(July-October)
• The risk of bacteremia/meningitis is 3.3%, pneumonia, bone/joint infections and bacterial enteritis is 13.7%• 30-50% of those who are ultimately diagnosed with bacterial
meningitis have been seen by a physician within the prior week(usually 1-2 days before) and were diagnosed as having a trivial illness and discharged on oral antibiotics.



Infants 1 to 3 months
Infants who are toxic and febrile have a much higher risk of serious bacterial infection. They should be admitted, have a full sepsis workup, and given antibiotics/antiviralsAmpicillin and Cefotaxime.
Infants who are nontoxic and febrile who meet all Rochester criteria can ‘safely’ be treated as an outpatient. Generally, 1-2.9% of children meeting these criteria will develop a serious bacterial infection, 0.7% bacteremia, 0.14% meningitis.

Infants 1 to 3 months
• Rochester Criteria/Low Risk Criteria• Nontoxic—most critical and difficult• Previously healthy, not low birth weight• No focal bacterial infection on PE except Otitis Media• WBC 5,000-15,000/mm3 (normal)• Bands<1500/mm3 (normal)• Normal urinalysis, including gram stain• If diarrhea, must be non-bloody and WBC<5/hpf.• If respiratory symptoms present, normal CXR
• Negative predictive value 98.9%

Infants 1 to 3 months
• If all of the criteria are met, then there are 2 options for outpatient management:• 1) Blood, Urine Cultures, LP, Ceftriaxone 50mg/kg IM
(to 1g), and return for reevaluation within 24 hours.• 2) Blood, Urine Cultures and careful observation.
• Parents should have mature judgement, can return within 30 minutes and have a thermometer and a phone.
• IF NO LP IS DONE, DO NOT GIVE CEFTRIAXONE AS IT WILL COMPROMISE F/U IF THE PATIENT IS STILL FEBRILE

Infants 1 to 3 months
• Follow-up of low risk infants• If all cultures negative: afebrile, well
appearingCareful observation• Blood cultures negative: well appearing,
febrileCareful observation, may consider second dose of Ceftriaxone
• Blood culture positiveadmit for sepsis workup and parenteral antibiotics pending results
• Urine culture positive: if persistent feveradmit for sepsis workup, parenteral antibiotics pending results. If afebrile and welloutpatient antibiotics

Heptavalent pneumococcal conjugate vaccine, PCV7(Prevnar)• Licensed in February 2000• Routinely incorporated into the childhood
immunization schedule in mid-2000• 4, 6B, 9V, 14, 18C, 19F, 23F• Recommended for all children aged 2 to 23
months• Invasive pneumococcal disease in children
younger than 2 years has decreased by at least 60%.


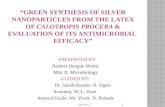
Rates of Invasive Pneumococcal Disease by Age Group and Year

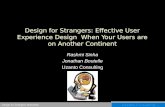
Rates of Invasive Pneumococcal Disease Caused by PCV7 and Non-PCV7 Serotypes in Neonates and Young Infants Aged 0 to 90 Days by Study Year

So what?
• This data is the first to suggest that neonates and infants too young to receive PCV7 are benefiting from herd immunity.
• One hypothesis is that vaccinated children are less likely to have nasal carriage of pneumococcus.

Infants 3 to 36 months• Infant sepsis syndrome:
• Age 3-36 months• Fever>39ºC• ANC>10,000
• If a child meets all 3 criteria, he has a 3% risk for pneumococcemia. If untreated, 3% will progress to meningitis.• Bacteremia risk peaks at 8-12 months• Pneumococcal sepsis peaks at 1 year, then drops off• Pneumococcal meningitis peaks at 3-5 months• OM, sinusitis, pneumonia, response to antipyretics, and social
status do not significantly alter risk.
• Other causes: HHV6(15%), UTI(girls 3%, boys 0.6%), menigococcemia(0.1%), Salmonella(0.2%), H. influenza(0.05%), Enterovirus(JulyOctober).

Infants 3 to 36 months• UA with micro, CBC with differential, Blood Cultures• LP if meningeal signs, not wanting to be held or moved,
petechiae, purpura or toxic.
• Antimicrobials:• OM or pneumonia: cover for pneumococcus, non-typable H. flu
and Moraxella: amoxicillin+augmentin, ceftriaxone• URI or no focus: cover for pneumococcus and menigococcus:
amoxicillin(80-100mg/dg/day), ceftriaxone• Pneumococcemia: promptly reassess, if well, should at least treat
with 1 dose ceftriaxone.
• PCV-7 >97% protection, thus all pneumococcal sepsis will decrease by 90%. So CBC and antimicrobials for this age group is becoming less critical.

Occult Bacteremia
5% of children with FWS have OCCULT BACTEREMIA• The presence of a positive blood culture in kids
who look well enough to be treated as outpatients and in whom the positive results are not anticipated.

Occult Bacteremia
• Streptococcus pneumonia is responsible for 2/3 to ¾ of all cases.• Peak prevalence between 6 and 24 months
• Association with high fever(39.4ºC or 103ºF)
• High WBC count(>15,000)
• Absence of evident focal soft tissue infection.
• Neisseria meningitidis, Haemophilus influenzae type b, and salmonellae account for most of the remaining cases.

Risk of Occult Bacteremia
OB has a low prevalence, so even though WBC is a sensitive and specific screening test, it has a low PPV. So the test does not discriminate between children who have FWS who are bacteremic and those who are not.
Therefore, blood culture is the gold standardstill has a high number of false positives, take 24-48hrs, and most cases of occult pneumococcal bacteremia clear without treatment.
Low Risk
Age >3yr
Temp <39.4ºC
WBC >5000 and
<15,000
High Risk
<2yr
>40ºC(104ºF)
<5000 or >15,000
Hx of contact with H. Flu or N. meningitidis

Occult Bacteremia
• Empiric antibiotics should be targeted against S. pneumoniae, N. meningitidis, and H. influenza• Amoxicillin
• Augmentin, Bactrim, 2nd or 3rd gen Cephalosporins
• Single dose Ceftriaxone 50-75mg/kg
• Followup is essential!

• Oski’s Pediatrics, 3rd edition
• Harriet Lane, 16th edition
• FWS in Children 0-36 months of age. TCNA 53(2006)167-194
• The Febrile Child. Emergency Medicine Reports. September 1995.
• Antibiotic Choices: The critical first hour. Pediatric Annals. June 1996.
• Evidence based approach to the febrile infant/child. Handout from Dr. Michael Cooperstock, MD. May 2000.
• Advisory Committee on Immunization Practices. Preventing pneumococcal disease among infants and young children: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2000;49(RR-9):1-35
• AAP; Committee on Infectious Disease. Policy statement: recommendations for the prevention of pneumococcal infections, including the use of pneumococcal conjugate vaccine, pneumococcal polysaccharide vaccine, and antibiotic porphylaxis/ Pediatrics. 2000;106:362-366.
• Whitney CG, FarleyMM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide vaccine. NEnglJMed. 2003;348:1737-1746.
• Poehling KA etal. Invasive Pneumococcal Disease Among Infants before and after Introductions of Pneumococcal Conjugate Vaccine. JAMA Apr 12, 2006,295:1668-74.