Fenótipos e biomarcadores na exacerbação da DPOC
10
Acute Exacerbations of Chronic Obstructive Pulmonary Disease Identification of Biologic Clusters and Their Biomarkers Mona Bafadhel 1,2 , Susan McKenna 1 , Sarah Terry 1 , Vijay Mistry 1,2 , Carlene Reid 1 , Pranabashis Haldar 2 , Margaret McCormick 3 , Koirobi Haldar 2 , Tatiana Kebadze 4 , Annelyse Duvoix 5 , Kerstin Lindblad 6 , Hemu Patel 7 , Paul Rugman 3 , Paul Dodson 3 , Martin Jenkins 3 , Michael Saunders 3 , Paul Newbold 3 , Ruth H. Green 1 , Per Venge 6 , David A. Lomas 5 , Michael R. Barer 2,7 , Sebastian L. Johnston 4 , Ian D. Pavord 1 , and Christopher E. Brightling 1,2 1 Institute for Lung Health, and 2 Department of Infection, Immunity and Inflammation, University of Leicester, Leicester, United Kingdom; 3 AstraZeneca R&D Charnwood, Loughborough, Leicestershire, United Kingdom; 4 Department of Respiratory Medicine, National Heart and Lung Institute, Centre for Respiratory Infections, Imperial College London, United Kingdom; 5 Cambridge Institute for Medical Research, University of Cambridge, Cambridge, United Kingdom; 6 Department of Medical Sciences, Clinical Chemistry, University of Uppsala, Uppsala, Sweden; and 7 Department of Clinical Microbiology, University Hospitals of Leicester NHS Trust, Leicester, United Kingdom Rationale: Exacerbations of chronic obstructive pulmonary disease (COPD) are heterogeneous with respect to inflammation and etiology. Objectives: Investigate biomarker expression in COPD exacerbations to identify biologic clusters and determine biomarkers that recog- nize clinical COPD exacerbation phenotypes, namely those associ- ated with bacteria, viruses, or eosinophilic airway inflammation. Methods: Patients with COPD were observed for 1 year at stable and exacerbation visits. Biomarkers were measured in sputum and serum. Viruses and selected bacteria were assessed in sputum by polymerase chain reaction and routine diagnostic bacterial culture. Biologic phenotypes were explored using unbiased cluster analysis and biomarkers that differentiated clinical exacerbation phenotypes were investigated. Measurements and Main Results: A total of 145 patients (101 men and 44 women) entered the study. A total of 182 exacerbations were captured from 86 patients. Four distinct biologic exacerbation clusters were identified. These were bacterial-, viral-, or eosinophilic- predominant, and a fourth associated with limited changes in the inflammatory profile termed “pauciinflammatory.” Of all exacerba- tions, 55%, 29%, and 28% were associated with bacteria, virus, or a sputum eosinophilia. The biomarkers that best identified these clinical phenotypes were sputum IL-1b, 0.89 (area under receiver operating characteristic curve) (95% confidence interval [CI], 0.83–0.95); serum CXCL10, 0.83 (95% CI, 0.70–0.96); and percentage peripheral eosino- phils, 0.85 (95% CI, 0.78–0.93), respectively. Conclusions: The heterogeneity of the biologic response of COPD exacerbations can be defined. Sputum IL-1b, serum CXCL10, and peripheral eosinophils are biomarkers of bacteria-, virus-, or eosinophil- associated exacerbations of COPD. Whether phenotype-specific bio- markers can be applied to direct therapy warrants further investigation. Keywords: chronic obstructive pulmonary disease; phenotypes; exac- erbations; airway inflammation; infection Acute exacerbations of chronic obstructive pulmonary disease (COPD) are associated with substantial morbidity and mortality (1, 2). Exacerbations are typically associated with increased neu- trophilic and to a lesser extent eosinophilic airway inflammation (3, 4). Respiratory viral and bacterial infections have been impli- cated in causing most exacerbations (5–7), but how these infec- tions alter lower airway inflammation and relate to treatment (Received in original form April 2, 2011; accepted in final form June 15, 2011) Supported by the Medical Research Council (United Kingdom) and AstraZeneca jointly as a “Biomarker Call Project”; C.E.B. is a Wellcome Trust Senior Clinical Fellow, and GlaxoSmithKline supported the measurement of surfactant protein D. The research was performed in laboratories partly funded by the European Regional Development Fund (ERDF 05567). The Medical Research Council, Well- come Trust, and the European Regional Development Fund had no involvement in the design of the study, data collection, analysis and interpretation of the data, in the writing of the manuscript, or in the decision to submit the manuscript. Author Contributions: S.M. and S.T. were involved in the recruitment of volunteers and in data collection. C.R., V.M., K.H., H.P., A.D., and K.L. were involved in data collection and interpretation. M.M., P.R., P.D., P.N., M.J., and M.S. were involved in study design, data collection, and interpretation. R.H.G. and P.H. were in- volved in study design and data interpretation. M.R.B., D.A.L., S.L.J., P.V., and I.D.P. were involved in the design of the study, data collection, and interpreta- tion. M.B. and C.E.B. were involved in the study design, volunteer recruitment, data collection, data interpretation, and data analysis, and had full access to the data and are responsible for the integrity of the data and final decision to submit. All authors contributed to the writing of the manuscript and have approved the final version for submission. Correspondence and requests for reprints should be addressed to Christopher E. Brightling, M.B.B.S., B.Sc. (Hons.), Ph.D., Institute for Lung Health, Clinical Sciences Wing, University Hospitals of Leicester, Leicester, LE3 9QP, UK. E-mail: [email protected] This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org Am J Respir Crit Care Med Vol 184. pp 662–671, 2011 Originally Published in Press as DOI: 10.1164/rccm.201104-0597OC on June 16, 2011 Internet address: www.atsjournals.org AT A GLANCE COMMENTARY Scientific Knowledge on the Subject Exacerbations of chronic obstructive pulmonary disease (COPD) are a major health burden worldwide, and affect a vulnerable population at risk of significant comorbidities. COPD exacerbations are heterogeneous with respect to etiology and inflammation and biomarkers are required to phenotype this heterogeneity. What This Study Adds to the Field We have shown that there are biologic COPD exacerbation clusters that are clinically indistinguishable, and that bio- markers can be used to identify specific clinical phenotypes during exacerbations of COPD (specifically those associ- ated with bacteria, virus, and sputum eosinophilia). Bac- terial and eosinophilic clinical exacerbation phenotypes can be identified from stable state. Our data further delineate the heterogeneity during COPD exacerbations and may identify populations that appropriately require cortico- steroids and antibiotics at the onset of an exacerbation.
-
Upload
flavia-salame -
Category
Health & Medicine
-
view
1.238 -
download
1
Transcript of Fenótipos e biomarcadores na exacerbação da DPOC

Acute Exacerbations of Chronic ObstructivePulmonary DiseaseIdentification of Biologic Clusters and Their Biomarkers
Mona Bafadhel1,2, Susan McKenna1, Sarah Terry1, Vijay Mistry1,2, Carlene Reid1, Pranabashis Haldar2,Margaret McCormick3, Koirobi Haldar2, Tatiana Kebadze4, Annelyse Duvoix5, Kerstin Lindblad6,Hemu Patel7, Paul Rugman3, Paul Dodson3, Martin Jenkins3, Michael Saunders3, Paul Newbold3,Ruth H. Green1, Per Venge6, David A. Lomas5, Michael R. Barer2,7, Sebastian L. Johnston4,Ian D. Pavord1, and Christopher E. Brightling1,2
1Institute for Lung Health, and 2Department of Infection, Immunity and Inflammation, University of Leicester, Leicester, United Kingdom;3AstraZeneca R&D Charnwood, Loughborough, Leicestershire, United Kingdom; 4Department of Respiratory Medicine, National Heart and Lung
Institute, Centre for Respiratory Infections, Imperial College London, United Kingdom; 5Cambridge Institute for Medical Research, University ofCambridge, Cambridge, United Kingdom; 6Department of Medical Sciences, Clinical Chemistry, University of Uppsala, Uppsala, Sweden; and7Department of Clinical Microbiology, University Hospitals of Leicester NHS Trust, Leicester, United Kingdom
Rationale: Exacerbations of chronic obstructive pulmonary disease(COPD)areheterogeneouswith respect to inflammationandetiology.Objectives: Investigatebiomarkerexpression inCOPDexacerbationsto identify biologic clusters and determine biomarkers that recog-nize clinical COPD exacerbation phenotypes, namely those associ-ated with bacteria, viruses, or eosinophilic airway inflammation.Methods: Patientswith COPDwere observed for 1 year at stable andexacerbation visits. Biomarkers were measured in sputum andserum. Viruses and selected bacteria were assessed in sputum bypolymerase chain reaction and routine diagnostic bacterial culture.Biologic phenotypes were explored using unbiased cluster analysisandbiomarkers thatdifferentiated clinical exacerbationphenotypeswere investigated.Measurements and Main Results: A total of 145 patients (101 menand 44 women) entered the study. A total of 182 exacerbationswere captured from 86 patients. Four distinct biologic exacerbationclusters were identified. These were bacterial-, viral-, or eosinophilic-predominant, and a fourth associated with limited changes in theinflammatory profile termed “pauciinflammatory.” Of all exacerba-tions, 55%, 29%, and 28% were associated with bacteria, virus, or a
sputumeosinophilia.Thebiomarkersthatbest identifiedtheseclinicalphenotypes were sputum IL-1b, 0.89 (area under receiver operatingcharacteristic curve) (95%confidence interval [CI], 0.83–0.95); serumCXCL10, 0.83 (95%CI, 0.70–0.96); andpercentageperipheral eosino-phils, 0.85 (95%CI, 0.78–0.93), respectively.Conclusions: The heterogeneity of the biologic response of COPDexacerbations can be defined. Sputum IL-1b, serum CXCL10, andperipheral eosinophils are biomarkers of bacteria-, virus-, or eosinophil-associated exacerbations of COPD. Whether phenotype-specific bio-markers can be applied to direct therapywarrants further investigation.
Keywords: chronic obstructive pulmonary disease; phenotypes; exac-erbations; airway inflammation; infection
Acute exacerbations of chronic obstructive pulmonary disease(COPD) are associated with substantial morbidity and mortality(1, 2). Exacerbations are typically associated with increased neu-trophilic and to a lesser extent eosinophilic airway inflammation(3, 4). Respiratory viral and bacterial infections have been impli-cated in causing most exacerbations (5–7), but how these infec-tions alter lower airway inflammation and relate to treatment
(Received in original form April 2, 2011; accepted in final form June 15, 2011)
Supported by the Medical Research Council (United Kingdom) and AstraZeneca
jointly as a “Biomarker Call Project”; C.E.B. is a Wellcome Trust Senior Clinical
Fellow, and GlaxoSmithKline supported the measurement of surfactant protein
D. The research was performed in laboratories partly funded by the European
Regional Development Fund (ERDF 05567). The Medical Research Council, Well-
come Trust, and the European Regional Development Fund had no involvement
in the design of the study, data collection, analysis and interpretation of the data,
in the writing of the manuscript, or in the decision to submit the manuscript.
Author Contributions: S.M. and S.T. were involved in the recruitment of volunteers
and in data collection. C.R., V.M., K.H., H.P., A.D., and K.L. were involved in data
collection and interpretation. M.M., P.R., P.D., P.N., M.J., and M.S. were involved
in study design, data collection, and interpretation. R.H.G. and P.H. were in-
volved in study design and data interpretation. M.R.B., D.A.L., S.L.J., P.V., and
I.D.P. were involved in the design of the study, data collection, and interpreta-
tion. M.B. and C.E.B. were involved in the study design, volunteer recruitment,
data collection, data interpretation, and data analysis, and had full access to the
data and are responsible for the integrity of the data and final decision to submit.
All authors contributed to the writing of the manuscript and have approved the
final version for submission.
Correspondence and requests for reprints should be addressed to Christopher
E. Brightling, M.B.B.S., B.Sc. (Hons.), Ph.D., Institute for Lung Health, Clinical
Sciences Wing, University Hospitals of Leicester, Leicester, LE3 9QP, UK. E-mail:
This article has an online supplement, which is accessible from this issue’s table of
contents at www.atsjournals.org
Am J Respir Crit Care Med Vol 184. pp 662–671, 2011
Originally Published in Press as DOI: 10.1164/rccm.201104-0597OC on June 16, 2011
Internet address: www.atsjournals.org
AT A GLANCE COMMENTARY
Scientific Knowledge on the Subject
Exacerbations of chronic obstructive pulmonary disease(COPD) are a major health burden worldwide, and affecta vulnerable population at risk of significant comorbidities.COPD exacerbations are heterogeneous with respect toetiology and inflammation and biomarkers are required tophenotype this heterogeneity.
What This Study Adds to the Field
We have shown that there are biologic COPD exacerbationclusters that are clinically indistinguishable, and that bio-markers can be used to identify specific clinical phenotypesduring exacerbations of COPD (specifically those associ-ated with bacteria, virus, and sputum eosinophilia). Bac-terial and eosinophilic clinical exacerbation phenotypes canbe identified from stable state. Our data further delineatethe heterogeneity during COPD exacerbations and mayidentify populations that appropriately require cortico-steroids and antibiotics at the onset of an exacerbation.

response is not completely understood. This heterogeneity trans-lates that at present clinicians have limited tools to phenotypeexacerbations. During stable state a sputum eosinophilia is asso-ciated with corticosteroid responsiveness (8–10), whereas thepresence of a high bacterial load and sputum purulence has favor-able outcomes with antibiotics (11–15). These findings suggestthat it is possible to identify clinically important COPD exacer-bation phenotypes. This is crucial because systemic corticosteroidsand antibiotics have marginal efficacy (16–21) and the potential tocause adverse events in an already vulnerable population.
We hypothesize that approaches aimed at the identification ofCOPD exacerbation phenotypes may allow for better prognostic,therapeutic, and mechanistic applications (22–24). In this studywe investigated whether during exacerbations of COPD there are(1) definable biologic phenotypes using unbiased mathematicaltools (namely factor and cluster analysis); (2) identifiable bio-markers associated with clinical phenotypes, specifically thoseassociated with bacteria, viruses, or sputum eosinophilia; and(3) exacerbation phenotypes that can be predicted from stablestate.
METHODS
Patients
Patients with a physician diagnosis of COPD and a post-bronchodilatorFEV1/FVC ratio of less than 0.7 as per global initiative for chronicobstructive lung disease (GOLD) criteria (1) were recruited from theGlenfield Hospital, Leicester, United Kingdom, and through local ad-vertising. All patients fulfilled the inclusion criteria of age greater than40 years, GOLD stage I–IV, and greater than or equal to one exacer-bation in the preceding 12 months defined as the requirement of emer-gency health care (25). Patients were excluded if there was a documentedinability to produce sputum after the induced sputum procedure, a cur-rent or previous history of asthma, currently active pulmonary tubercu-losis, or any other clinically relevant lung disease other than COPD. Thepresence of comorbidity, reported atopy to common aeroallergens, orreversibility on lung function testing was not an exclusion criterion. Allpatients gave informed written consent and the study was approved bythe local ethics committee.
Study Design
This was a prospective observational study. Patients were seen at stablestate and during exacerbations for the duration of 1 year. Stable visitsincluding the baseline visits were 8 weeks free from an exacerbation. Allpatients were given daily diary cards to complete, and asked to contactthe research team if there was an increase in symptoms of breathless-ness, sputum volume, and purulence. Exacerbations were definedaccording to Anthonisen criteria (14) and health care use (25). Exac-erbation data recording and sampling were only performed in patientswho had not received prior oral corticosteroids or antibiotics. Patientswere all clinically assessed (including chest radiograph, temperaturerecording, and blood gas analysis if clinically necessary) to excludeother causes of breathlessness. Patients with an exacerbation of COPDwere then treated according to guidelines (2).
Measurements
At all visits, patients underwent pre– and post–400-mg albuterol broncho-dilator spirometry (Vitalograph, Buckingham, Buckinghamshire, UK); in-duced or spontaneous sputum collection (26); and measurements ofsymptoms and health quality assessments using the Visual Analog Scale(27) and the Chronic Respiratory Disease Interviewer-Administered Stan-dardized Questionnaire (CRQ) (28). Sputum was collected and analyzedfor bacteria (29–31) (using standard routine culture, CFU, and real-timequantitative polymerase chain reaction [qPCR]), for viruses by PCR (32),and processed to produce cytospins for cell differential and supernatantfor fluid phase measurements (33). A broad panel of serum and sputumbiomarkers were measured using the Meso-Scale-Discovery (MSD,Gaithersburg, MD) platform standard preprepared plates (MSD, MD)
and single ELISA at stable and exacerbation visits (see Table E1 in theonline supplement).
Definition of Bacteria-, Virus-, and Sputum
Eosinophil–associated Exacerbations of COPD
Bacteria-associated exacerbations were defined as a positive bacterialpathogen on routine culture (Haemophilus influenzae, Moraxella catar-rhalis, Streptococcus pneumoniae, Staphylococcus aureus, or Pseudo-monas aeruginosa) or a total aerobic CFU count greater than orequal to 107 cells (12, 15). qPCR bacterial detection methods werenot used to define bacteria-associated exacerbations in this study.
A virus-associated exacerbation was defined as one that had a positivesputum viral PCR, whether in isolation or in combination with a positivebacterial pathogen on routine culture. A sputum eosinophil–associatedexacerbation was defined as the presence of more than 3% nonsquamouscells.
Statistical Analyses
Statistical analyses were performed using PRISM version 4 (Graph-PAD PRISM, La Jolla, CA) and SPSS version 16 (IBM, Chicago,IL). Parametric and nonparametric data are presented as mean(SEM) and median (interquartile range). Log transformed data arepresented as geometric mean (95% confidence interval [CI]). Multi-variate modeling using principal component analysis in sputum bio-markers was used to explore biomarker pattern expression atexacerbations. No adjustments for multiple comparisons have beenmade across biomarkers.
Factor analysis, a mathematical method that discovers patterns ofrelationships within large datasets, was used to identify factors in sputummediators at exacerbations thereby demonstrating biologic factors inde-pendent of each other and of any clinical expression. This method usingunsupervised principal component analysis demonstrated three factorsaccounting for 75% of the total variance (see Table E2). Cluster analysis,an unbiased mathematical method, allows one to classify groups onsimilar chosen characteristics alone. Thus, after demonstrating three bi-ologic factors, we used hierarchical cluster analysis to generate four bi-ologic clusters for exacerbation events and cases. Clinical characteristicsfor all exacerbation events were tabulated for each biologic cluster. One-way analysis of variance, Kruskal-Wallis test, and the chi-square testwere used to compare the clinical characteristics between cluster groups.
For comparison of clinical and biomarker changes between baselineand exacerbation visits the paired t test or Wilcoxon matched pairs testwas used. For comparison of exacerbations associated with or withoutbacteria, virus, and sputum eosinophilia the t test and Mann-Whitneytest were used, respectively. To determine suitable biomarkers, thereceiver operating characteristic curves were plotted for (1) exacerba-tion versus stable state; (2) bacteria- versus nonbacteria-associatedexacerbations; (3) virus- versus nonvirus-associated exacerbations;and (4) sputum eosinophilia– (. 3% nonsquamous cells) versus non-sputum eosinophilia–associated exacerbations.
Validation of the identified biomarkers for bacteria-, virus-, and spu-tum eosinophil–associated exacerbation was performed in a further 89exacerbation events from an independent cohort of subjects withCOPD. These subjects with COPD were recruited to enter a prospec-tive study with identical inclusion and exclusion criteria and study de-sign as the current study. Stable and exacerbation visits were treated inaccordance to the main study.
A P value of less than 0.05 was taken as the threshold of statisticalsignificance.
RESULTS
One hundred fifty-six patients were enrolled; 145 (101 men and44 women) completed the first visit and 115 completed 12months (Figure 1; see Figure E1). At baseline 3%, 48%,30%, and 19% had GOLD I, II, III, and IV, respectively. Mostpatients recruited were current or exsmokers (142 of 145),with a mean (range) pack-year history of 49 (10–153) withan absolute and percentage mean (SEM) reversibility to in-haled bronchodilator on study entry of 47 ml (11 patients) and
Bafadhel, McKenna, Terry, et al.: Biomarkers in COPD Exacerbations 663

4% (one patient), respectively. Skin prick testing or serum-specific IgE to a wide panel of aeroallergens confirmed that20% were atopic. Bacterial colonization, defined as the pres-ence of a potentially pathogenic microorganism (H. influen-zae,M. catarrhalis, S. pneumoniae, S. aureus, or P. aeruginosa)in a standard culture technique (29), was present in 28% ofpatients at baseline. Using qPCR a bacterial pathogen (H.influenzae, M. catarrhalis, S. pneumoniae, or S. aureus) wasdetected in 86% of patients at the baseline stable visit. A viruswas detected in 5% of subjects at study entry, whereas eosin-ophilic airway inflammation (. 3% nonsquamous cells) waspresent in 27% of patients. Baseline and exacerbation clinicalcharacteristics are shown in Table 1 (see Table E3).
Exacerbations
A total of 182 exacerbation events were captured from 86patients; of these 21 exacerbations warranted hospitalization.There was a reduction in the FEV1 and CRQ from baselineto exacerbation (FEV1 [L] 1.33 vs. 1.10; mean difference 0.24;95% CI, 0.12–0.36; P , 0.001) (CRQ [units] 4.11 vs. 3.12; meandifference 0.99; 95% CI, 0.74–1.23; P , 0.001). The magnitudeof these changes was independent of smoking status, sex,
GOLD severity (1), or Anthonisen criteria (14). Hospitalizedexacerbations were associated with a greater decline in lungfunction compared with exacerbations that were not hospital-ized (DFEV1 [ml]2355 vs.2131; mean difference 224; 95% CIof difference, 2356 to 292; P , 0.001), but not health statusdecline (DCRQ [units] 21.25 vs. 20.91; mean difference 0.34;95% CI of difference, 20.83 to 0.15; P ¼ 0.18).
Serum and sputum mediator data were available in 148 ex-acerbation events from 75 patients. Serum biomarkers that in-creased during an exacerbation were IL-6, tumor necrosisfactor (TNF) receptors I and II, serum amyloid-A, C-reactive pro-tein (CRP), procalcitonin, and serum eosinophil cationic protein(Table E4A). Sputum biomarkers that increased were IL-1b,TNF-a, TNFRI, TNFRII, IL6, CCL5, and CCL4 (Table E4B).No single biomarker had a receiver operating curve area underthe curve greater than 0.70 in determining an exacerbationfrom stable state (Figure E2). Of all sputum and serum bio-markers measured there was a significantly increased level ofserum TNF-a and CRP in patients who were hospitalized(CRP median [IQR] 56 (102) vs. 8 (14); P ¼ 0.002) (serumTNF-a geometric mean 4.3 [95% CI, 3.4–5.4] vs. 3.4 [95%CI, 3.2–3.6]; P ¼ 0.02).
Figure 1. Subject enrolment flow diagram for 12-monthobservational period.
664 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 184 2011

Factor and Cluster Analysis
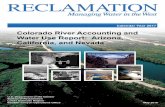
Factor analysis identified three biologic factors at exacerbationrepresenting proinflammatory, Th1, and Th2 factors as deter-mined by their cytokine expression profiles (Table E3). Clusteranalysis using the highest loading biomarker from each factor(TNFRII, CXCL11, and CCL17) revealed four biologic clusterpopulations for exacerbation events. Three clusters were termedas “bacteria-predominant,” “eosinophil-predominant,” and “virus-predominant.” A fourth cluster demonstrated low sputum medi-ator concentrations and had fewer events associated withknown etiology and was termed “pauciinflammatory.” Factormean scores were plotted for each cluster (Figures 2A, andE3A). Biologic cluster ellipsoids were calculated and plottedfor all exacerbation events to schematically represent biologicclusters of COPD exacerbations in three dimensions (Figure2B, Figure E3B). Exacerbation event characteristics of thesebiologic clusters are presented in Table 2 (Table E5). The base-line characteristics for each subject within each biologic clusterare shown in Tables 2 and E5. Cluster membership was deter-mined using either a patient’s first exacerbation event or thedominant cluster in patients with multiple exacerbations. Theintraclass correlation coefficient of the biologic clusters forpatients with repeated exacerbations was 0.73. Each biologiccluster was found to be differentially related to inflammationand etiology, but was otherwise clinically indistinguishable.
Exacerbations Associated with Bacteria
Fifty-five percent of exacerbations were bacteria-associatedexacerbations (positive bacterial pathogen on routine cultureor CFU > 107). Blood and sputum neutrophils were increased.Total bacterial load (16S) was higher in patients with a bacteria-associated exacerbation than those without (geometric mean7.67 [95% CI, 4.27 to 1.48] vs. 2.88 [95% CI, 1.78 to 4.78]; P ¼0.001). There was no difference in the 16S signal across exacer-bations of Anthonisen type (analysis of variance; P ¼ 0.64).Using qPCR, acquisition of a new species occurred in 15% ofexacerbations. Clinical assessments of change in FEV1, symp-toms of sputum production, and sputum purulence had an areaunder the receiver operating characteristic curve of 0.45 (95%CI, 0.35–0.55), 0.50 (95% CI, 0.40–0.60), and 0.58 (95% CI,0.48–0.68), respectively. The most suitable biomarker for deter-mining bacteria-associated exacerbations was sputum IL-1bwith an area under the receiver operating characteristic curveof 0.89 (95% CI, 0.83–0.95). A cutoff of 125 pg/ml had a
sensitivity of 90% and a specificity of 80% (Figures 3A andE4A). The best serum biomarker was CRP with an area underthe receiver operating characteristic curve of 0.65 (95% CI, 0.57–0.74). A serum CRP cutoff of 10 mg/L had a sensitivity of 60%and specificity of 70%.
Exacerbations Associated with Virus
Twenty-nine percent of exacerbations were associated with a vi-rus, most commonly rhinovirus. Virus-associated exacerbationshad a larger fall in % FEV1 compared with nonvirus-associatedexacerbations (217% vs. 29%; mean difference 28%; 95% CI,216 to 21; P ¼ 0.04). Clinical assessments of change in FEV1,symptoms of cough and breathlessness, had an area under thereceiver operating characteristic curve of 0.43 (95% CI, 0.32–0.53), 0.62 (95% CI, 0.52–0.72), and 0.51 (95% CI, 0.41–0.62),respectively. The best marker for distinguishing the presence ofa virus at exacerbation was serum CXCL10 (IP-10), with anarea under the receiver operating characteristic curve of 0.76(95% CI, 0.67–0.86). A serum CXCL10 cut off of 56 pg/ml gavea sensitivity of 75% and specificity of 65% (Figures 3B andE4B). For exacerbations associated with virus alone the areaunder the receiver operating characteristic curve for serumCXCL10 improved to 0.83 (95% CI, 0.70–0.96).
Exacerbations Associated with Sputum Eosinophilia
A sputum eosinophilia was observed in 28% of exacerbations.The most sensitive and specific measure to determine a sputumeosinophilia at exacerbation was the percentage peripheralblood eosinophil count with an area under the receiver operatingcharacteristic curve of 0.85 (95% CI, 0.78–0.93). A cutoff of 2%peripheral blood eosinophils had a sensitivity of 90% and spec-ificity of 60% for identifying a sputum eosinophilia of greaterthan 3% at exacerbation (Figure 3C, Figure E4C).
In summary, the etiologic and inflammatory causes of exacerba-tion events were as follows: bacteria alone 37%, virus alone 10%,sputum eosinophilia alone 17%, bacteria plus virus 12%, bacteriaplus sputum eosinophilia 6%, virus plus sputum eosinophilia 3%,bacteria plus virus plus sputum eosinophilia 1%, and none 14%.
Multivariate modeling using combinations of two or threebiomarkers for the detection of bacteria-, virus-, and eosinophil-associated exacerbations did not significantly improve on the singlemediators alone (data not shown). Differential clinical and bio-marker expression for exacerbations associated with bacteria,virus, and sputum eosinophilia are shown in Tables E4–E6.
TABLE 1. CLINICAL CHARACTERISTICS OF ALL PATIENTS AT ENTRY INTO THE STUDY AND CLINICAL FEATURES AT EXACERBATION
Study Entry Study Entry Exacerbation P Value
Male, n (%) 101 (70) FEV1,L† 1.33 (0.05) 1.10 (0.04) ,0.001
Age* 69 (43–88) FEV1% predicted† 52 (2) 42 (1) ,0.001
Age at diagnosis* 62 (38–83) Reversibility, ml 47 (11) 37 (11) 0.50
Current smokers, n (%) 42 (29) FEV1/FVC ratio, %† 52 (2) 50 (1) 0.65
Exsmokers, n (%) 100 (69) CRQTOTAL, units 4.11 (0.10) 3.12 (0.08) ,0.001
Pack-year history* 49 (10–153) VASTOTAL, mm 142 (6) 239 (6) ,0.001
Exacerbation rate in previous 12 mo 3 (0.2) Peripheral leukocyte count (3109 cells/L)‡ 8.2 (7.9–8.6) 9.3 (8.9–9.8) ,0.001
Maintenance prednisolone, n (%) 9 (6) Peripheral neutrophil count (3109 cells/L)‡ 5.3 (5–5.6) 6.3 (6–6.7) ,0.001
Prednisolone dosage, mg* 6 (4–10) Peripheral eosinophil count (3109 cells/L)‡ 0.21 (0.18–0.23) 0.19 (0.17–0.22) 0.84
Inhaled corticosteroid use, n (%) 125 (86) Total sputum cell count (3106 cells/g sputum)‡ 3.8 (3.1–4.7) 6.4 (5.2–7.8) ,0.001
Inhaled corticosteroid dose, mgx 1,540 (59) Sputum neutrophil count, % 68 (2) 74 (2) 0.02
Inhaled long-acting b agonist use, n (%) 110 (76) Sputum eosinophil count, %‡ 1.2 (1–1.6) 1.1 (0.9–1.5) 0.58
Definition of abbreviations: CRQ ¼ Chronic Respiratory Disease Questionnaire score; VAS ¼ visual analog score.
Data presented as mean (SEM) unless stated.
* Mean (range).y Post-bronchodilator.z Geometric mean (95% confidence interval).x Beclomethasone dipropionate equivalent.
Bafadhel, McKenna, Terry, et al.: Biomarkers in COPD Exacerbations 665

Predicting Bacteria-, Virus-, or
Sputum-associated Exacerbations
The odds ratio for a bacteria or an eosinophil-associated exac-erbation was 4.9 (95% CI, 2.4–9.9; P , 0.001) or 2.7 (95% CI,1.3–5.7; P ¼ 0.01) if the patient had a bacterial pathogen ondiagnostic routine culture or a sputum eosinophilia on greaterthan or equal to one occasion at stable state. The odds ratio fora virus-associated exacerbation if the patient had a virus atstable state was 0.5 (95% CI, 0.1–3.9; P ¼ 0.67).
Validation of the Biomarkers Peripheral Blood Eosinophils,
Sputum IL-1b, Serum CRP, and Serum CXCL10
In an independent study of COPD exacerbations, 89 subjects (57men and 32 women) with a mean (range) age of 68 (46–86) years
and mean (SEM) FEV1% predicted of 46 (2) percent sputumIL-1b and serum CXCL10 was measured using a commercialELISA (R&D Systems, Abingdon, UK). The area under thereceiver operating characteristic curve for percentage bloodeosinophils to identify a sputum eosinophil–associated exacer-bation was 0.95 (95% CI, 0.87–1.00) with a cutoff of 2% havinga sensitivity and specificity of 90% and 60%. The area underthe receiver operating characteristic curve for sputum IL-1band serum CRP to identify a bacteria-associated exacerbationwas 0.73 (95% CI, 0.61–0.85) and 0.70 (95% CI, 0.59–0.82);a sputum IL-1b cutoff of 130 pg/ml had a sensitivity and spec-ificity of 80% and 60%, and a serum CRP cutoff of 10 mg/Lhad sensitivity and specificity of 65%. The area under the re-ceiver operating characteristic curve for serum CXCL10 toidentify a virus-associated exacerbation was 0.65 (95% CI,
Figure 2. (A) Bar chart representing the
mean factor scores for the three identi-
fied biologic factors (proinflammatory,
Th1, and Th 2) categorized accordingto the four biologic clusters. (B) Propor-
tional representation of biologic chronic
obstructive pulmonary disease exacerba-tion clusters in three-dimensional ellip-
soids. Cluster 1 is termed “bacteria-
predominant” and is outlined in blue,
cluster 2 is termed “eosinophil-predomi-nant” and is outlined in green, cluster 3 is
termed “virus-predominant” and is out-
lined in red, and cluster 4 is termed “pau-
ciinflammatory” and is outlined in gray.
666 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 184 2011

0.52–0.78) with a cutoff of 145 pg/ml having a sensitivity andspecificity of 70% and 60%.
Further details and results are available in the online supplement.
DISCUSSION
In this study we have used two methods to investigate bio-markers in COPD. The first using unbiased statistical tools, freefrom bias and independent of clinical expression, identified bi-ologic COPD exacerbation phenotypes and characterized exac-erbations into four biologic clusters, The second method usedcurrent clinical exacerbation phenotypes of COPD related to po-tential etiology and inflammation, namely exacerbations that areassociated with bacteria, virus, or a sputum eosinophilia. Inter-estingly, we were unable to define biomarkers for exacerbationsper se, despite a generalized increase in systemic and airway in-flammation (34–36). The biologic exacerbation clusters were bac-terial-, viral-, or eosinophilic-predominant, and a fourth wasassociated with limited changes in the inflammatory profile andwas termed “pauciinflammatory.” These clusters were remark-ably similar to our clinical exacerbation phenotypes. We identi-fied biomarkers for our clinical exacerbation phenotypes thatwere then validated in an independent cohort. The bacteria-and sputum eosinophil–associated exacerbations rarely coexisted,and were reliably predicted from stable state suggesting funda-mental differences in their immunopathogenesis. Therefore, inaddition to identifying potential biomarkers to direct therapy,
these exacerbation clinical phenotypes are likely to represent dis-tinct pathophysiologic entities with specific biomarker signatures.
Biomarker profiling in COPD exacerbations has the potentialto further the understanding of disease mechanisms (22),whereas phenotypic approaches lend to prognostic and thera-peutic strategies (37, 38). Using factor and cluster analysis,a novel approach of characterizing COPD and exacerbations(23), we were able to reduce an extensive panel of measuredsputum biomarkers into three factors, from which we deter-mined four biologic clusters. This analytic strategy is free frominvestigator bias. These biologic clusters could not be distin-guished clinically or by Anthonisen criteria (14) and the exac-erbation severity was similar across the clusters. Importantly,using factor analysis we have shown differential inflammatoryprofiles between the bacteria-predominant, eosinophil-predominant,virus-predominant, and pauciinflammatory clusters. In patientswith multiple exacerbations the biologic clusters were repeat-able, and exacerbations associated with bacteria or a sputumeosinophilia but not viruses could be predicted from stable state.Therefore, our data are consistent with the view that bacterialand eosinophilic exacerbations may reflect instability withina complex and inherently unstable system, whereas viral exacer-bations are more likely to represent acquisition of a new patho-gen. It is likely both of these mechanisms drive exacerbations, butcritically we have determined biologic clusters and clinical phe-notypes that may respond to different management strategies,which can potentially be identified using biomarker profiles.
TABLE 2. BIOLOGIC CLUSTERS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE EXACERBATIONS, WITH CLINICALEXACERBATION AND BASELINE CHARACTERISTICS
Cluster 1:
Bacteria-predominant
Cluster 2:
Eosinophil-predominant
Cluster 3:
Virus-predominant
Cluster 4:
Pauciinflammatory P Value
Exacerbation characteristics
Number (%) 52 (35) 44 (30) 36 (24) 16 (11) —
Sputum TNFRII (pg/ml)* 1,722 (1,402–2,117) 353 (287–433) 1,254 (969–1,623) 77 (41–147) ,0.0001
Sputum CXCL11 (pg/ml)* 3.1 (2.2–4.3) 10.9 (7.7–15.5) 799 (415–1,539) 17.3 (5.6–53.1) ,0.0001
Sputum CCL17 (pg/ml)* 5.5 (4.5–6.7) 34.8 (27.3–44.5) 23.5 (16.2–34.1) 4.7 (3.5–6.3) ,0.0001
Bacterial exacerbation, % (95% CI) 86 (73–92) 29 (18–45) 44 (28–61) 31 (12–58) ,0.0001
Viral exacerbation, % (95% CI) 22 (13–35) 10 (3–23) 57 (39–73) 30 (10–61) ,0.0001
Eosinophilic exacerbation, % (95% CI) 6 (1–16) 60 (45–74) 28 (16–44) 27 (10–52) ,0.0001
D FEV1, ml† 2132 (2251 to 235) 2110 (2230 to 231) 2232 (2340 to 2124) 2280 (2524 to 236) 0.32
D CRQ, units † 20.9 (21.2 to 20.6) 20.9 (21.3 to 20.5) 20.9 (21.4 to 20.4) 21 (21.9 to 20.1) 0.99
D VASTOTAL, mm† 79 (42–116) 80 (41–119) 120 (86–154) 73 (38–108) 0.39
Baseline characteristics
Number, (%) 28 (37) 19 (25) 20 (27) 8 (11) —
Male, n (%) 18 (64) 14 (74) 14 (70) 7 (88) 0.63
Age, yrs‡ 69 (52–84) 68 (45–88) 70 (49–84) 69 (61–85) 0.62
Current smokers, n (%) 8 (29) 8 (42) 4 (20) 3 (38) 0.48
Pack-years smoked‡ 44 (10–122) 50 (20–106) 47 (10–134) 72 (23–120) 0.11
Exacerbation rate in previous 12 mo 3.8 (0.5) 4.3 (0.5) 4 (0.7) 4.9 (1.2) 0.58
Exacerbation rate during study 3.8 (0.3) 3.6 (0.4) 3.2 (0.3) 3.1 (0.5) 0.64
Inhaled corticosteroid dose, mgx 1,507 (147) 1,567 (133) 1,470 (160) 1,150 (188) 0.55
Residual volume, % 134 (8) 150 (9) 120 (8) 146 (23) 0.11
TLCO % predicted 56 (5) 59 (5) 57 (6) 46 (7) 0.62
FEV1% predicted, baseline 53 (3) 51 (5) 53 (5) 40 (7) 0.34
FEV1/FVC ratio (%) 51 (2) 47 (2) 50 (3) 47 (5) 0.67
CRQTOTAL , units 4.14 (0.20) 3.90 (0.22) 4.10 (0.26) 3.66 (0.50) 0.74
VASTOTAL , mm 178 (15) 142 (18) 124 (18) 147 (37) 0.14
Total sputum cell count (3106 cells/g)* 8.3 (5.5–12.5) 2.3 (1.6–3.2) 2.5 (1.2–5.3) 3.5 (1.2–10.7) 0.002
Sputum neutrophil count, % 75 (5) 53 (4) 68 (4) 81 (6) 0.003
Sputum eosinophil count, %* 1 (0.6–1.6) 3.1 (1.4–6.6) 1 (0.5–1.9) 0.5 (0.2–1) 0.012
Bacterial colonization, % (95% CI) 63 (48–77) 27 (15–43) 11 (3–29) 38 (18–61) 0.001
Definition of abbreviations: CCL ¼ ; CI ¼ confidence interval; CRQ ¼ Chronic Respiratory Disease Questionnaire score; CXCL ¼ ; TLCO ¼ carbon monoxide transfer
factor; TNF ¼ tumor necrosis factor; VAS ¼ visual analog score.
Data presented as mean (SEM), unless stated.
* Geometric mean (95% CI).y Mean change (95% CI) between exacerbation and baseline.z Mean (range).x Beclomethasone dipropionate equivalent.
Bafadhel, McKenna, Terry, et al.: Biomarkers in COPD Exacerbations 667

Figure 3. Receiver operating characteristic curve with
area under the curve (95% confidence interval) illustrating
biomarkers that positively predict (A) bacteria-, (B) virus-,and (C) eosinophil-associated exacerbations. Area under
the curve (95% confidence interval) is shown in the paren-
theses. CCL¼ ; CRP¼ C-reactive protein; CXCL¼ ; TNF¼tumor necrosis factor.
668 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 184 2011

The inflammatory profile of a COPD exacerbation is typicallyneutrophilic, but eosinophilic airway inflammation also exists,and is associated with a favorable response to corticosteroid ther-apy (8–10). Eosinophilia in inflammatory airways disease is as-sociated with increased all-cause mortality (39, 40) and mayhighlight different genetic, biologic, and pathologic disease pro-cesses. Importantly, the sputum differential rather than totaleosinophil count has consistently been shown to be associatedwith important clinical outcomes (9, 10). We found that theperipheral percentage eosinophil count was a sensitive biomarkerof a sputum eosinophilia. Current guidelines recommend the useof systemic corticosteroids for COPD exacerbations, although themagnitude of the benefit is marginal and their use associated withsignificant side effects (18). Our findings raise the possibility thattargeting corticosteroid therapy in a subgroup of exacerbationsdependent on the peripheral eosinophil count may reduce inap-propriate use of systemic corticosteroids.
Bacteria are considered to play a role in up to 50% of exac-erbations (7). Current guidelines propose sputum purulenceto guide antibiotic therapy (13). Sputum purulence is sensitivefor detecting bacterial culture or high bacterial yields at exac-erbation in COPD (12). However, the use of sputum purulencealone is confounded by its presence at stable state and chronicbacterial colonization (41), possibly as a consequence of poorbacterial clearance (42). Furthermore, the change in sputumpurulence or sputum production symptoms in our cohort wasnot sensitive or specific for identifying a bacteria-associatedexacerbation. The most sensitive and specific assay for deter-mining bacteria-associated exacerbations was sputum IL-1b.This extends previous findings that bronchoalveolar lavage IL-1b was a good biomarker for ventilator-associated pneumonia(43), and suggests that this airway marker may suitably deter-mine bacterial infections, above that of serum CRP or procalci-tonin whose use could not be demonstrated in this study or inothers (34, 35). Sputum IL-1b could thus be used as a biomarkerto correctly identify bacteria-associated exacerbations butwould require the development of a rapid near patient test tobe of use in clinical practice.
Viruses have been implicated as amajor cause of COPD exac-erbations and are detected in approximately half of severeCOPD exacerbations (5, 6). The total sputum eosinophil counthas been proposed as a potential biomarker of a viral exacerbation(5). Here we also found that the total absolute sputum eosino-phil count was increased in virus-associated exacerbations, butnot the differential sputum eosinophil count, suggesting theassociation was largely a consequence of a change in the total-cell count. The application of clinical symptoms in combinationwith serum CXCL10 (IP-10) has been proposed as a possiblebiomarker for rhinovirus infection at exacerbation (44). Thisstudy confirms that serum CXCL10 levels as a potential pre-dictor of a virus-associated exacerbation, independent of a re-quirement for symptom evaluation. Novel antiviral approachesare in development and CXCL10 is thus a promising biomarkerto direct future antiviral therapy.
One potential criticism is that this is a single-center study andtherefore our findings need to be replicated across multiple cen-ters, and validated prospectively to identify the biologic clustersand our proposed biomarkers for the clinical exacerbation phe-notypes; nonetheless, this approach may represent a new para-digm in the management of COPD exacerbations. Importantly,we have replicated the biomarkers peripheral blood eosinophils,sputum IL-1b, and serum CXCL10 in a validation cohort. Pe-ripheral blood eosinophils remained a strong marker of a sputumeosinophilia. Sputum IL-1b and serum CXCL10 were measuredusing a different platform but remained significant albeit weakerpredictive markers of identifying a bacteria- or virus-associated
exacerbation. In our study a statistical analytic limitation wasthat we did not correct for repeated measures and assessedchanges in biomarkers in paired or unpaired tests; however,we examined two methods to investigate biomarkers in COPDexacerbations, using unbiased statistical tools to demonstratefour biologic clusters and analysis of biomarkers to look at pre-defined clinical exacerbation subgroups, and further used multi-variate analysis to determine that combinations of markers didnot improve our predictive model. The presence of coinfectionwith virus and bacteria in our study was lower than that previ-ously reported (5), but may reflect differences in the severityof exacerbations. The relationship between virus and bacterialinfection in exacerbations, however, remains poorly understood(5, 45). We chose to define a bacteria-associated exacerbationbased on a positive routine culture or a high bacterial load;however, the causal links between the presence of bacteriaand exacerbations has not been rigorously confirmed, and evi-dence for efficacy of antibiotics in treatment is conflicting (13,19–21, 46). Developments in molecular bacterial identificationof bacteria (47) and emerging microbiomics (48) are beginningto redefine the microbiota of the airway in health and diseaseand will likely change the view of what defines a bacterial in-fection. Improvements in viral detection and the identificationof new respiratory viruses are also changing the understandingof the associations between exacerbations and these agents.Further work is required before therapeutic implications andinterpretative criteria can be established for these sensitive de-tection methods. Whether identification of a pauciinflammatorybiologic cluster and a proportion of subjects without clear evi-dence of a cause for their exacerbation reflect the insensitivityof our chosen cutoffs for definitions or a real entity requiresfurther clarifications.
In conclusion, COPD exacerbations are heterogeneous. Thisphenotypic heterogeneity can be defined. Using unbiased statis-tical tools we have determined four biologic exacerbation clus-ters that relate to identifiable patterns of inflammation andpotential causative pathogens. We have defined sensitive andspecific biomarkers to identify predefined clinical exacerbationphenotypes, which need to be tested in randomized prospectivestudies of targeted therapy. These subgroups are independentand suggest that the mechanisms driving their exacerbationsare distinct and may be amenable to more specific interventions,potentially moving the management of COPD exacerbations to-ward the realization of phenotype-specific management.
Author Disclosure: M.B. received grant support from the Medical Research Coun-cil (MRC). S.M. does not have a financial relationship with a commercial entitythat has an interest in the subject of this manuscript. S.T. does not have a financialrelationship with a commercial entity that has an interest in the subject of thismanuscript. V.M. does not have a financial relationship with a commercial entitythat has an interest in the subject of this manuscript. C.R. does not have a financialrelationship with a commercial entity that has an interest in the subject of thismanuscript. P.H. does not have a financial relationship with a commercial entitythat has an interest in the subject of this manuscript. M.M. is employed by andowns stocks in AstraZeneca (AZ). K.H. does not have a financial relationship witha commercial entity that has an interest in the subject of this manuscript. T.K.does not have a financial relationship with a commercial entity that has an in-terest in the subject of this manuscript. A.D. does not have a financial relationshipwith a commercial entity that has an interest in the subject of this manuscript.K.L. does not have a financial relationship with a commercial entity that has aninterest in the subject of this manuscript. H.P. does not have a financial relation-ship with a commercial entity that has an interest in the subject of this manu-script. P.R., P.D., and M.J. are employed by and own stocks in AZ. M.S. isemployed by AZ. P.N. was an employee of AZ at the time of conducting thisresearch and preparation of the manuscript. He is now an employee of MedI-mmune LLC, which is a subsidiary of AZ and owns stocks in AZ. R.H.G. wasa consultant for Nycomed and received travel accommodations from Chiesi.P.V. received institutional grant support from the Swedish Research Council.D.A.L. received institutional grant support and was a consultant for GlaxoSmithK-line (GSK). He is on the Advisory Board and received honorarium from GSK.M.R.B. received institutional grant support form the MRC. S.L.J. was a consultantfor AZ, Centocor, Sanofi-Pasteur, Synairgen, GSK, and Chiesi. He received
Bafadhel, McKenna, Terry, et al.: Biomarkers in COPD Exacerbations 669

institutional grant support from AZ, Centocor, Sanofi-Pasteur, Synairgen, and AZ.He received lecture fees from AZ, owns stocks in Synairgen, and received travelaccommodations from Pfizer. I.D.P. received institutional grant support from theMRC and received honorarium from GSK, AZ, Merck, and Novartis. He receivedtravel accommodations from Boehringer Ingelheim (BI). C.E.B. received institu-tional grant support from the MRC, AZ, MedImmune, and Roche. He receivedsupport for the development of SPD assays in Cambridge from GSK. He is on theAdvisory Board of GSK, AZ, Roche, Novartis, Genentech, and MedImmune andwas a consultant for MedImmune and Novartis. He received travel accommoda-tions from BI.
Acknowledgment: The authors thank all the research volunteers who participatedin the study, and also the following people for their valuable assistance throughoutthe study: J. Aniscenko, M. Bourne, R. Braithwaite, D. Burke, J. Footitt, E. Goldie,J. Goldie, N. Goodman, S. Gupta, B. Hargadon, I. Rushby,M. Shelley, A. Singapuri,D. Vara, R. Walton, and S. Winpress.
References
1. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P,
Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van Weel C, et al. Global
strategy for the diagnosis, management, and prevention of chronic
obstructive pulmonary disease: GOLD executive summary. Am J
Respir Crit Care Med 2007;176:532–555.
2. Halpin D. NICE guidance for COPD. Thorax 2004;59:181–182.
3. Bhowmik A, Seemungal TA, Sapsford RJ, Wedzicha JA. Relation of
sputum inflammatory markers to symptoms and lung function changes
in COPD exacerbations. Thorax 2000;55:114–120.
4. Saetta M, Di SA, Maestrelli P, Turato G, Ruggieri MP, Roggeri A,
Calcagni P, Mapp CE, Ciaccia A, Fabbri LM. Airway eosinophilia in
chronic bronchitis during exacerbations. Am J Respir Crit Care Med
1994;150:1646–1652.
5. Papi A, Bellettato CM, Braccioni F, Romagnoli M, Casolari P, Caramori
G, Fabbri LM, Johnston SL. Infections and airway inflammation in
chronic obstructive pulmonary disease severe exacerbations. Am J
Respir Crit Care Med 2006;173:1114–1121.
6. Seemungal T, Harper-Owen R, Bhowmik A, Moric I, Sanderson G,
Message S, Maccallum P, Meade TW, Jeffries DJ, Johnston SL.
Respiratory viruses, symptoms, and inflammatory markers in acute
exacerbations and stable chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 2001;164:1618–1623.
7. Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic
obstructive pulmonary disease. N Engl J Med 2008;359:2355–2365.
8. Shim C, Stover DE, Williams MH Jr. Response to corticosteroids in
chronic bronchitis. J Allergy Clin Immunol 1978;62:363–367.
9. Pizzichini E, Pizzichini MM, Gibson P, Parameswaran K, Gleich GJ,
Berman L, Dolovich J, Hargreave FE. Sputum eosinophilia predicts
benefit from prednisone in smokers with chronic obstructive bron-
chitis. Am J Respir Crit Care Med 1998;158:1511–1517.
10. Brightling CE, Monteiro W, Ward R, Parker D, Morgan MD, Wardlaw
AJ, Pavord ID. Sputum eosinophilia and short-term response to
prednisolone in chronic obstructive pulmonary disease: a randomised
controlled trial. Lancet 2000;356:1480–1485.
11. White AJ, Gompertz S, Bayley DL, Hill SL, O’Brien C, Unsal I,
Stockley RA. Resolution of bronchial inflammation is related to
bacterial eradication following treatment of exacerbations of chronic
bronchitis. Thorax 2003;58:680–685.
12. Stockley RA, O’Brien C, Pye A, Hill SL. Relationship of sputum color
to nature and outpatient management of acute exacerbations of
COPD. Chest 2000;117:1638–1645.
13. Ram FS, Rodriguez-Roisin R, Granados-Navarrete A, Garcia-Aymerich
J, Barnes NC. Antibiotics for exacerbations of chronic obstructive
pulmonary disease. Cochrane Database Syst Rev 2006;(2):CD004403.
14. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK,
Nelson NA. Antibiotic therapy in exacerbations of chronic obstruc-
tive pulmonary disease. Ann Intern Med 1987;106:196–204.
15. van d V, Monninkhof E, van der Palen J, Zielhuis G, van HC, Hendrix R.
Clinical predictors of bacterial involvement in exacerbations of chronic
obstructive pulmonary disease. Clin Infect Dis 2004;39:980–986.
16. Aaron SD, Vandemheen KL, Hebert P, Dales R, Stiell IG, Ahuja J,
Dickinson G, Brison R, Rowe BH, Dreyer J. Outpatient oral pred-
nisone after emergency treatment of chronic obstructive pulmonary
disease. N Engl J Med 2003;348:2618–2625.
17. Davies L, Angus RM, Calverley PM. Oral corticosteroids in patients
admitted to hospital with exacerbations of chronic obstructive
pulmonary disease: a prospective randomised controlled trial. Lancet
1999;354:456–460.
18. Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light
RW, Anderson P, Morgan NA. Effect of systemic glucocorticoids on
exacerbations of chronic obstructive pulmonary disease. Department
of Veterans Affairs Cooperative Study Group. N Engl J Med 1999;
340:1941–1947.
19. Puhan MA, Vollenweider D, Latshang T, Steurer J, Steurer-Stey C.
Exacerbations of chronic obstructive pulmonary disease: when are
antibiotics indicated? A systematic review. Respir Res 2007;8:30.
20. Puhan MA, Vollenweider D, Steurer J, Bossuyt PM, Ter RG. Where is
the supporting evidence for treating mild to moderate chronic ob-
structive pulmonary disease exacerbations with antibiotics? A sys-
tematic review. BMC Med 2008;6:28.
21. Rothberg MB, Pekow PS, Lahti M, Brody O, Skiest DJ, Lindenauer PK.
Antibiotic therapy and treatment failure in patients hospitalized for
acute exacerbations of chronic obstructive pulmonary disease. JAMA
2010;303:2035–2042.
22. Han MK, Agusti A, Calverley PM, Celli BR, Criner G, Curtis JL, Fabbri
LM, Goldin JG, Jones PW, Macnee W. Chronic obstructive pulmo-
nary disease phenotypes: the future of COPD. Am J Respir Crit Care
Med 2010;182:598–604.
23. Weatherall M, Shirtcliffe P, Travers J, Beasley R. Use of cluster analysis
to define COPD phenotypes. Eur Respir J 2010;36:472–474.
24. Tashkin DP. Frequent exacerbations of chronic obstructive pulmonary
disease: a distinct phenotype? N Engl J Med 2010;363:1183–1184.
25. Rodriguez-Roisin R. Toward a consensus definition for COPD exacer-
bations. Chest 2000; 117(5, Suppl 2)398S–401S.
26. Bhowmik A, Seemungal TA, Sapsford RJ, Devalia JL, Wedzicha JA.
Comparison of spontaneous and induced sputum for investigation of
airway inflammation in chronic obstructive pulmonary disease. Tho-
rax 1998;53:953–956.
27. Brightling CE, Monterio W, Green RH, Parker D, Morgan MD, Wardlaw
AJ, Pavord D. Induced sputum and other outcome measures in chronic
obstructive pulmonary disease: safety and repeatability. Respir Med
2001;95:999–1002.
28. Guyatt G. Measuring health status in chronic airflow limitation. Eur
Respir J 1988;1:560–564.
29. Health Protection Agency 2009. Investigation of bronchoalveolar lavage,
sputum and associated specimens. National Standard Method BSOP
2009;57:3.
30. Pye A, Stockley RA, Hill SL. Simple method for quantifying viable
bacterial numbers in sputum. J Clin Pathol 1995;48:719–724.
31. Creer DD, Dilworth JP, Gillespie SH, Johnston AR, Johnston SL, Ling
C, Patel S, Sanderson G, Wallace PG, McHugh TD. Aetiological role
of viral and bacterial infections in acute adult lower respiratory tract
infection (LRTI) in primary care. Thorax 2006;61:75–79.
32. Bisgaard H, Zielen S, Garcia-Garcia ML, Johnston SL, Gilles L, Menten
J, Tozzi CA, Polos P. Montelukast reduces asthma exacerbations in 2-
to 5-year-old children with intermittent asthma. Am J Respir Crit Care
Med 2005;171:315–322.
33. Kelly MM, Keatings V, Leigh R, Peterson C, Shute J, Venge P,
Djukanovic R. Analysis of fluid-phase mediators. Eur Respir J
Suppl 2002;37:24s–39s.
34. Hurst JR, Donaldson GC, Perera WR, Wilkinson TM, Bilello JA, Hagan
GW, Vessey RS,Wedzicha JA. Use of plasma biomarkers at exacerbation
of chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2006;174:867–874.
35. Bozinovski S, Hutchinson A, Thompson M, Macgregor L, Black J,
Giannakis E, Karlsson AS, Silvestrini R, Smallwood D, Vlahos R,
et al. Serum amyloid A is a biomarker of acute exacerbations of
chronic obstructive pulmonary disease. Am J Respir Crit Care Med
2008;177:269–278.
36. Hurst JR, Perera WR, Wilkinson TM, Donaldson GC, Wedzicha JA. Sys-
temic and upper and lower airway inflammation at exacerbation of chronic
obstructive pulmonary disease.Am J Respir Crit CareMed 2006;173:71–78.
37. Burgel PR, Paillasseur JL, Caillaud D, Tillie-Leblond I, Chanez P,
Escamilla R, Court-Fortune I, Perez T, Carre P, Roche N. Clinical
COPD phenotypes: a novel approach using principal component and
cluster analyses. Eur Respir J 2010;36:531–539.
38. Hurst JR, Vestbo J, Anzueto A, Locantore N, Mullerova H, Tal-Singer
R, Miller B, Lomas DA, Agusti A, Macnee W, et al. Susceptibility to
670 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 184 2011

exacerbation in chronic obstructive pulmonary disease. N Engl J Med
2010;363:1128–1138.
39. Hospers JJ, Schouten JP, Weiss ST, Postma DS, Rijcken B. Eosinophilia is
associated with increased all-cause mortality after a follow-up of 30
years in a general population sample. Epidemiology 2000;11:261–268.
40. Hospers JJ, Schouten JP, Weiss ST, Rijcken B, Postma DS. Asthma
attacks with eosinophilia predict mortality from chronic obstructive
pulmonary disease in a general population sample. Am J Respir Crit
Care Med 1999;160:1869–1874.
41. Rosell A, Monso E, Soler N, Torres F, Angrill J, Riise G, Zalacain R,Morera
J, Torres A. Microbiologic determinants of exacerbation in chronic ob-
structive pulmonary disease. Arch Intern Med 2005;165:891–897.
42. Taylor AE, Finney-Hayward TK, Quint JK, Thomas CM, Tudhope SJ,
Wedzicha JA, Barnes PJ, Donnelly LE. Defective macrophage
phagocytosis of bacteria in COPD. Eur Respir J 2010;35:1039–1047.
43. Conway MA, Kefala K, Wilkinson TS, Moncayo-Nieto OL, Dhaliwal
K, Farrell L, Walsh TS, Mackenzie SJ, Swann DG, Andrews PJ,
et al. Diagnostic importance of pulmonary interleukin-1beta and
interleukin-8 in ventilator-associated pneumonia. Thorax 2010;65:
201–207.
44. Quint JK, Donaldson GC, Goldring JJ, Baghai-Ravary R, Hurst JR,
Wedzicha JA. Serum IP-10 as a biomarker of human rhinovirus in-
fection at exacerbation of COPD. Chest 2010;137:812–822.
45. Sethi S. Coinfection in exacerbations of COPD: a new frontier. Chest
2006;129:223–224.
46. Sethi S. The problems of meta-analysis for antibiotic treatment of
chronic obstructive pulmonary disease, a heterogeneous disease:
a commentary on Puhan et al. BMC Med 2008;6:29.
47. Sethi S, Evans N, Grant BJ, Murphy TF. New strains of bacteria and
exacerbations of chronic obstructive pulmonary disease. N Engl J
Med 2002;347:465–471.
48. Hilty M, Burke C, Pedro H, Cardenas P, Bush A, Bossley C, Davies J,
Ervine A, Poulter L, Pachter L, et al. Disordered microbial commu-
nities in asthmatic airways. PLoS ONE 2010;5:e8578.
Bafadhel, McKenna, Terry, et al.: Biomarkers in COPD Exacerbations 671