Female reproductive system (LO 66). Neuroendocrine control ... · response to the hormonal ......
19
2018. 03. 13. 1 Female reproductive system (LO 66). Neuroendocrine control of pregnancy (LO 67). Gabriella Kékesi Female reproductive system
Transcript of Female reproductive system (LO 66). Neuroendocrine control ... · response to the hormonal ......

2018. 03. 13.
1
Female reproductive system (LO 66).
Neuroendocrine control of pregnancy
(LO 67).
Gabriella Kékesi
Female reproductive system
2018. 03. 13.
2
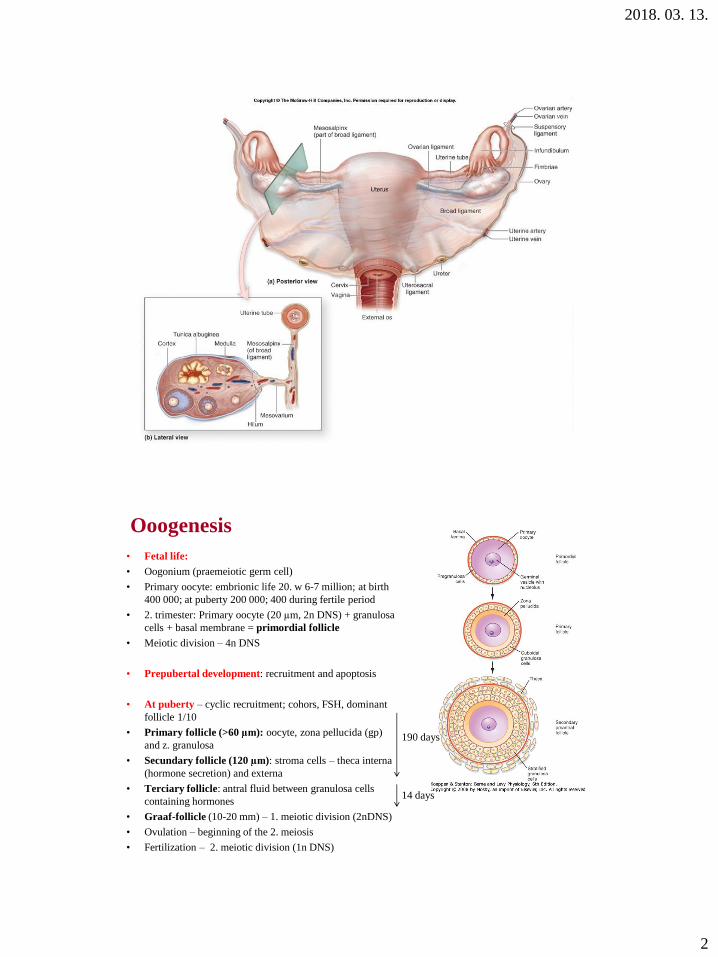
• Fetal life:
• Oogonium (praemeiotic germ cell)
• Primary oocyte: embrionic life 20. w 6-7 million; at birth
400 000; at puberty 200 000; 400 during fertile period
• 2. trimester: Primary oocyte (20 µm, 2n DNS) + granulosa
cells + basal membrane = primordial follicle
• Meiotic division – 4n DNS
• Prepubertal development: recruitment and apoptosis
• At puberty – cyclic recruitment; cohors, FSH, dominant
follicle 1/10
• Primary follicle (>60 µm): oocyte, zona pellucida (gp)
and z. granulosa
• Secundary follicle (120 µm): stroma cells – theca interna
(hormone secretion) and externa
• Terciary follicle: antral fluid between granulosa cells
containing hormones
• Graaf-follicle (10-20 mm) – 1. meiotic division (2nDNS)
• Ovulation – beginning of the 2. meiosis
• Fertilization – 2. meiotic division (1n DNS)
Ooogenesis
14 days
190 days
2018. 03. 13.
3
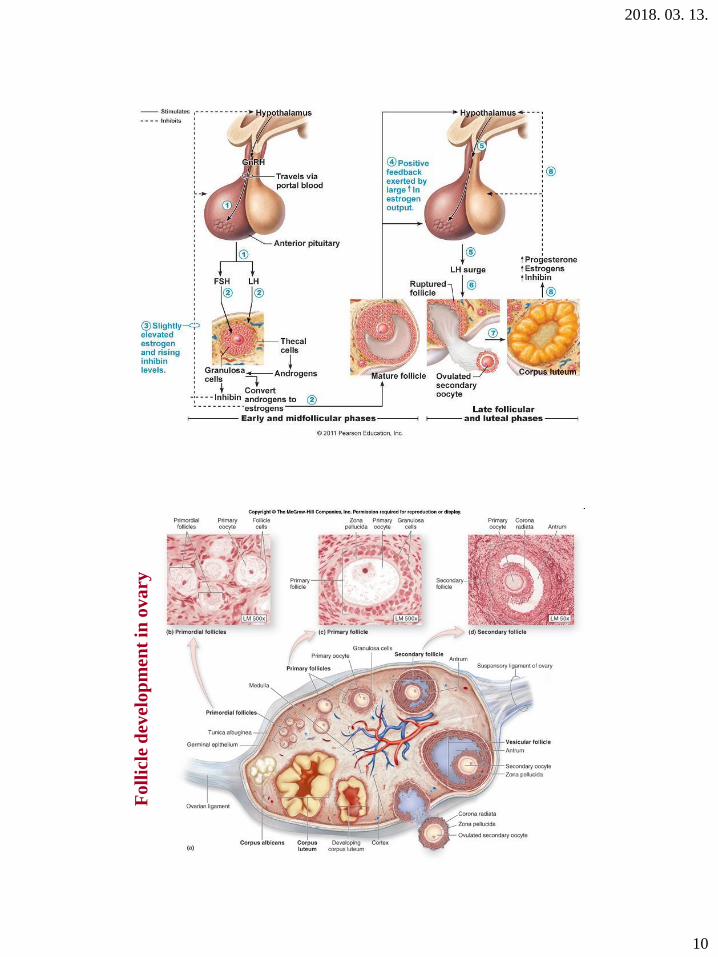
Fo
llic
le d
evel
op
men
t in
ov
ary
2018. 03. 13.
4
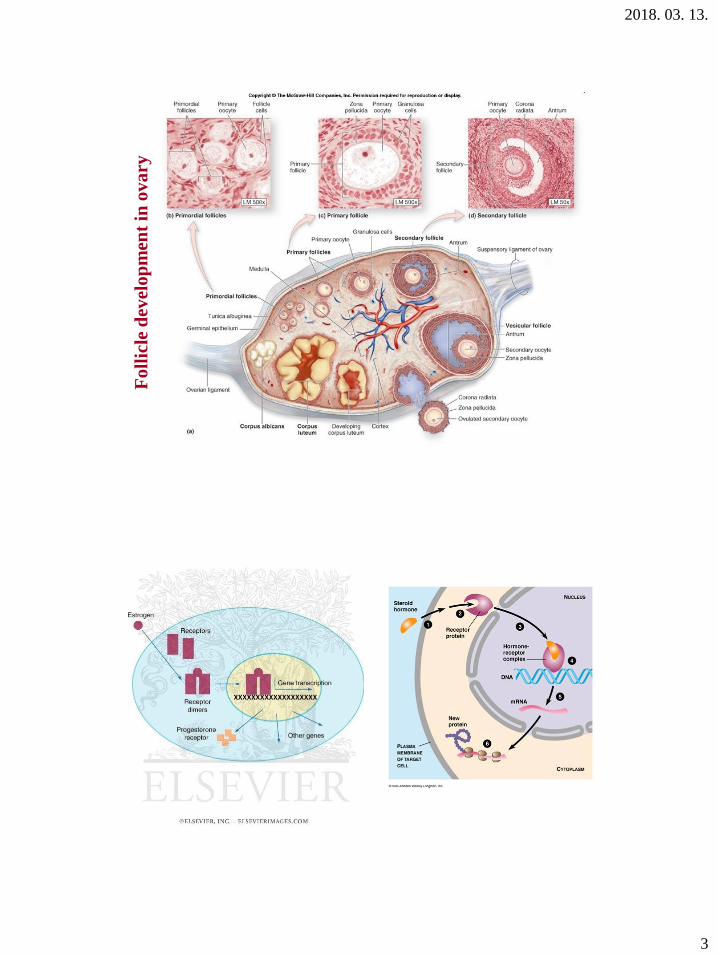
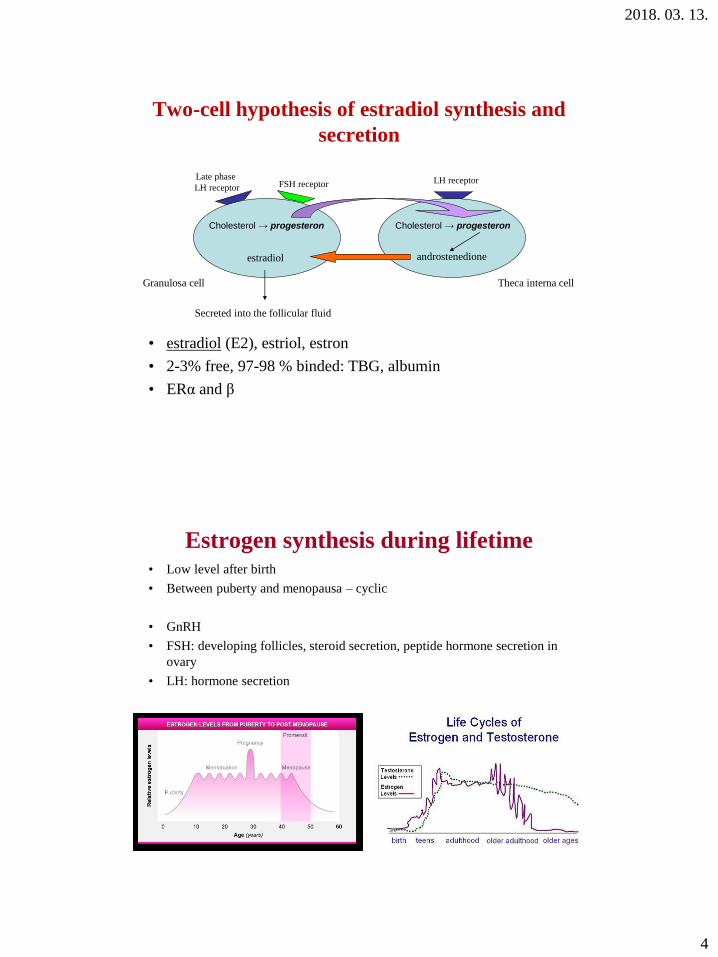
Two-cell hypothesis of estradiol synthesis and
secretion
• estradiol (E2), estriol, estron
• 2-3% free, 97-98 % binded: TBG, albumin
• ERα and β
Granulosa cell Theca interna cell
Late phase
LH receptorLH receptorFSH receptor
Cholesterol → progesteron Cholesterol → progesteron
androstenedioneestradiol
Secreted into the follicular fluid
Estrogen synthesis during lifetime• Low level after birth
• Between puberty and menopausa – cyclic
• GnRH
• FSH: developing follicles, steroid secretion, peptide hormone secretion in
ovary
• LH: hormone secretion
2018. 03. 13.
5
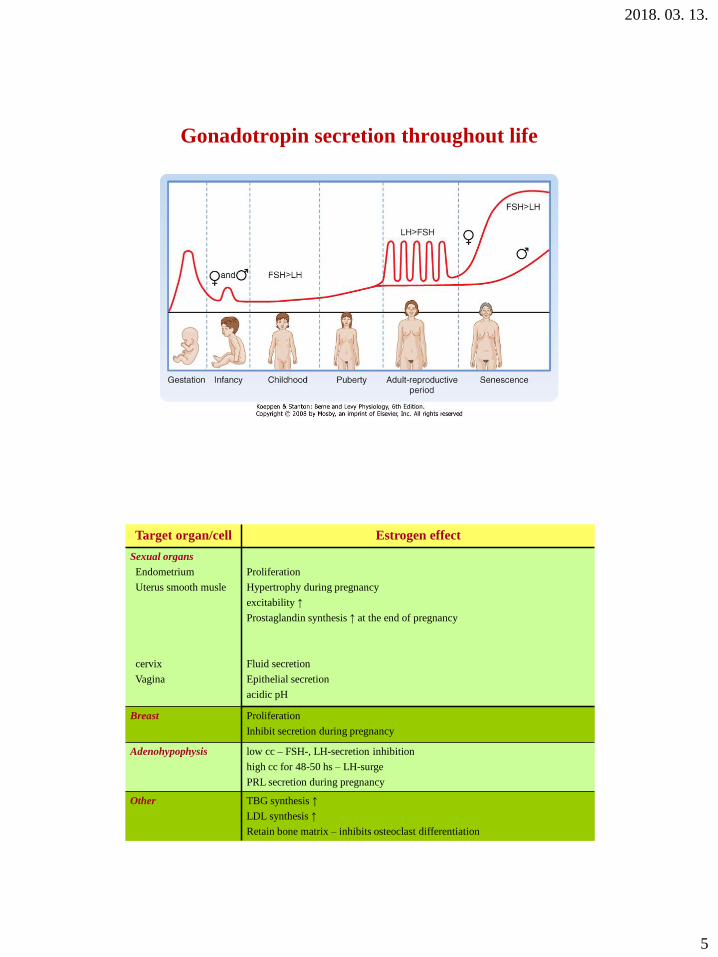
Gonadotropin secretion throughout life
Target organ/cell Estrogen effect
Sexual organs
Endometrium
Uterus smooth musle
cervix
Vagina
Proliferation
Hypertrophy during pregnancy
excitability ↑
Prostaglandin synthesis ↑ at the end of pregnancy
Fluid secretion
Epithelial secretion
acidic pH
Breast Proliferation
Inhibit secretion during pregnancy
Adenohypophysis low cc – FSH-, LH-secretion inhibition
high cc for 48-50 hs – LH-surge
PRL secretion during pregnancy
Other TBG synthesis ↑
LDL synthesis ↑
Retain bone matrix – inhibits osteoclast differentiation
2018. 03. 13.
6
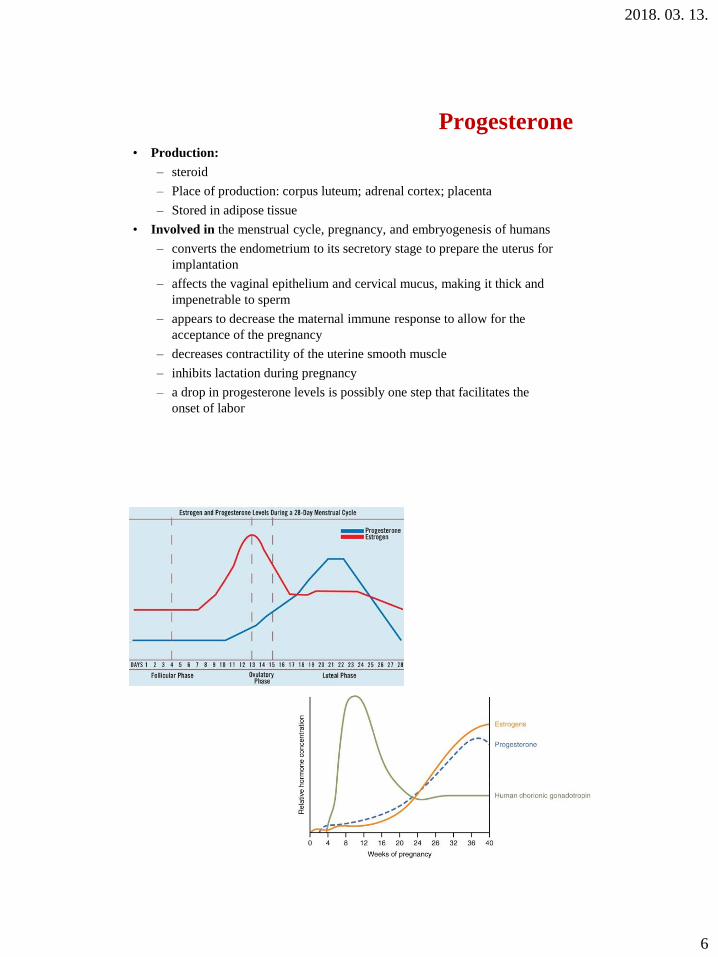
Progesterone
• Production:
– steroid
– Place of production: corpus luteum; adrenal cortex; placenta
– Stored in adipose tissue
• Involved in the menstrual cycle, pregnancy, and embryogenesis of humans
– converts the endometrium to its secretory stage to prepare the uterus for
implantation
– affects the vaginal epithelium and cervical mucus, making it thick and
impenetrable to sperm
– appears to decrease the maternal immune response to allow for the
acceptance of the pregnancy
– decreases contractility of the uterine smooth muscle
– inhibits lactation during pregnancy
– a drop in progesterone levels is possibly one step that facilitates the
onset of labor
2018. 03. 13.
7
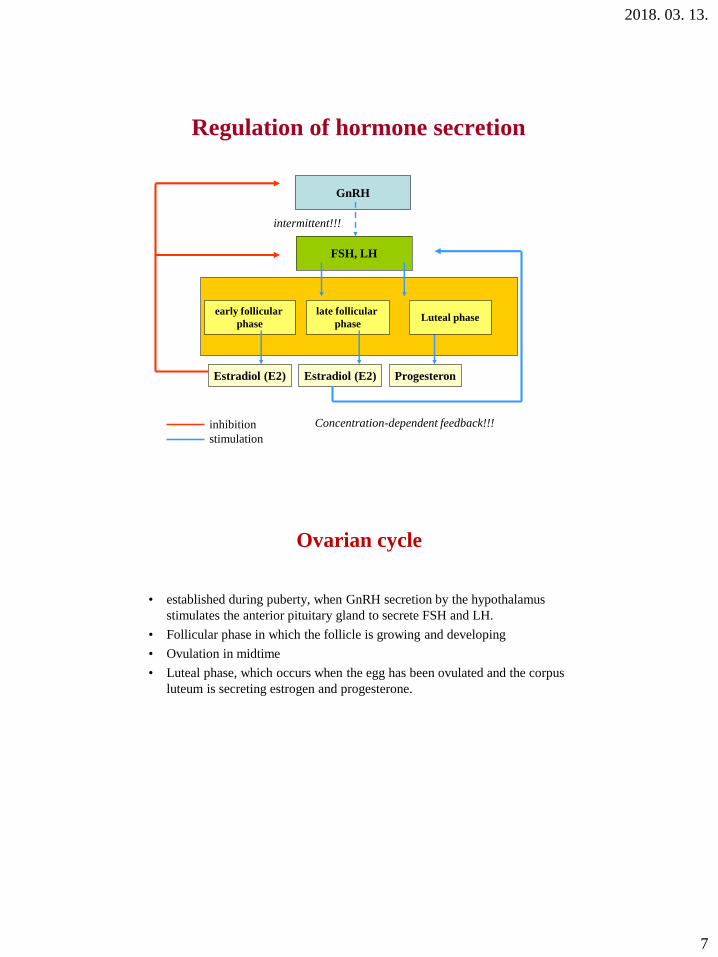
Regulation of hormone secretion
GnRH
FSH, LH
early follicular
phase
late follicular
phase
Estradiol (E2) Progesteron
inhibition
stimulation
intermittent!!!
Luteal phase
Estradiol (E2)
Concentration-dependent feedback!!!
Ovarian cycle
• established during puberty, when GnRH secretion by the hypothalamus
stimulates the anterior pituitary gland to secrete FSH and LH.
• Follicular phase in which the follicle is growing and developing
• Ovulation in midtime
• Luteal phase, which occurs when the egg has been ovulated and the corpus
luteum is secreting estrogen and progesterone.
2018. 03. 13.
8
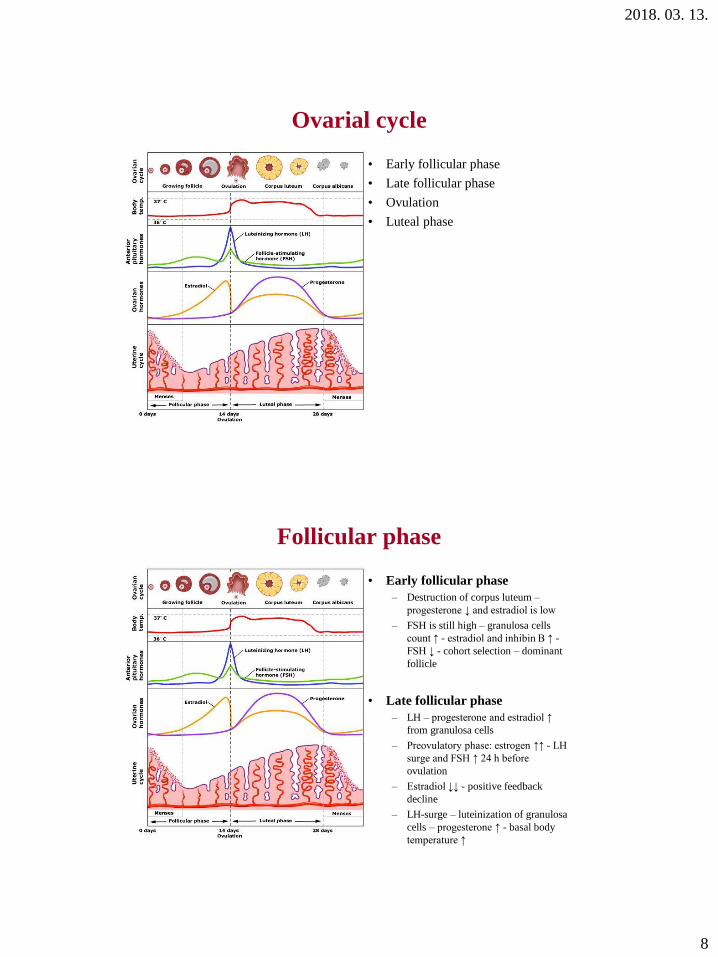
Ovarial cycle
• Early follicular phase
• Late follicular phase
• Ovulation
• Luteal phase
Follicular phase
• Early follicular phase
– Destruction of corpus luteum –
progesterone ↓ and estradiol is low
– FSH is still high – granulosa cells
count ↑ - estradiol and inhibin B ↑ -
FSH ↓ - cohort selection – dominant
follicle
• Late follicular phase
– LH – progesterone and estradiol ↑
from granulosa cells
– Preovulatory phase: estrogen ↑↑ - LH
surge and FSH ↑ 24 h before
ovulation
– Estradiol ↓↓ - positive feedback
decline
– LH-surge – luteinization of granulosa
cells – progesterone ↑ - basal body
temperature ↑
2018. 03. 13.
9
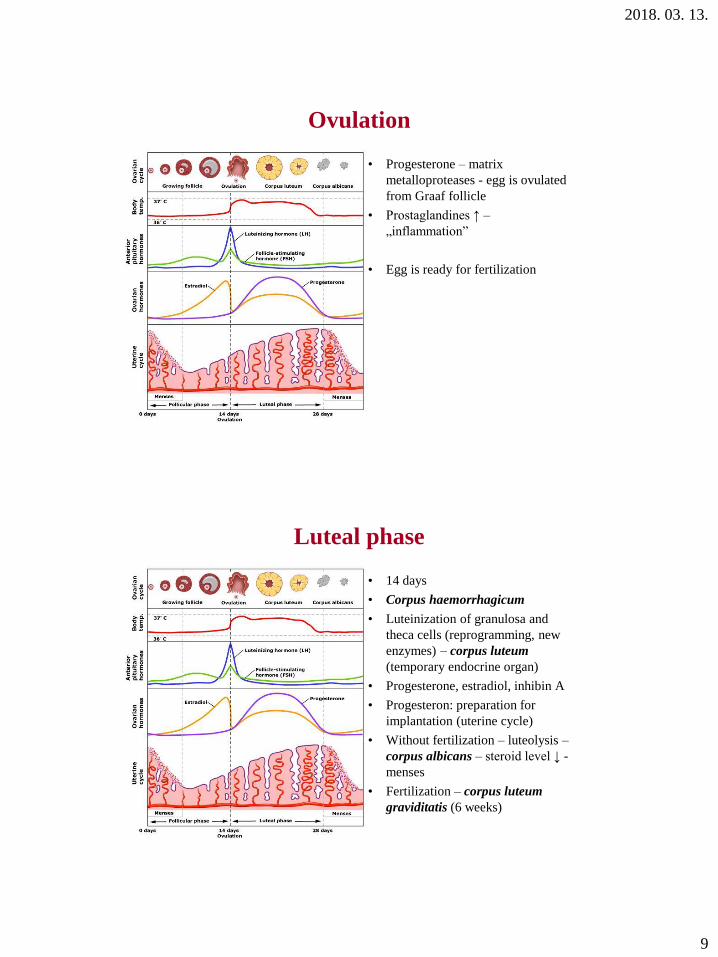
Ovulation
• Progesterone – matrix
metalloproteases - egg is ovulated
from Graaf follicle
• Prostaglandines ↑ –
„inflammation”
• Egg is ready for fertilization
Luteal phase
• 14 days
• Corpus haemorrhagicum
• Luteinization of granulosa and
theca cells (reprogramming, new
enzymes) – corpus luteum
(temporary endocrine organ)
• Progesterone, estradiol, inhibin A
• Progesteron: preparation for
implantation (uterine cycle)
• Without fertilization – luteolysis –
corpus albicans – steroid level ↓ -
menses
• Fertilization – corpus luteum
graviditatis (6 weeks)
2018. 03. 13.
10
Fo
llic
le d
evel
op
men
t in
ov
ary
2018. 03. 13.
11
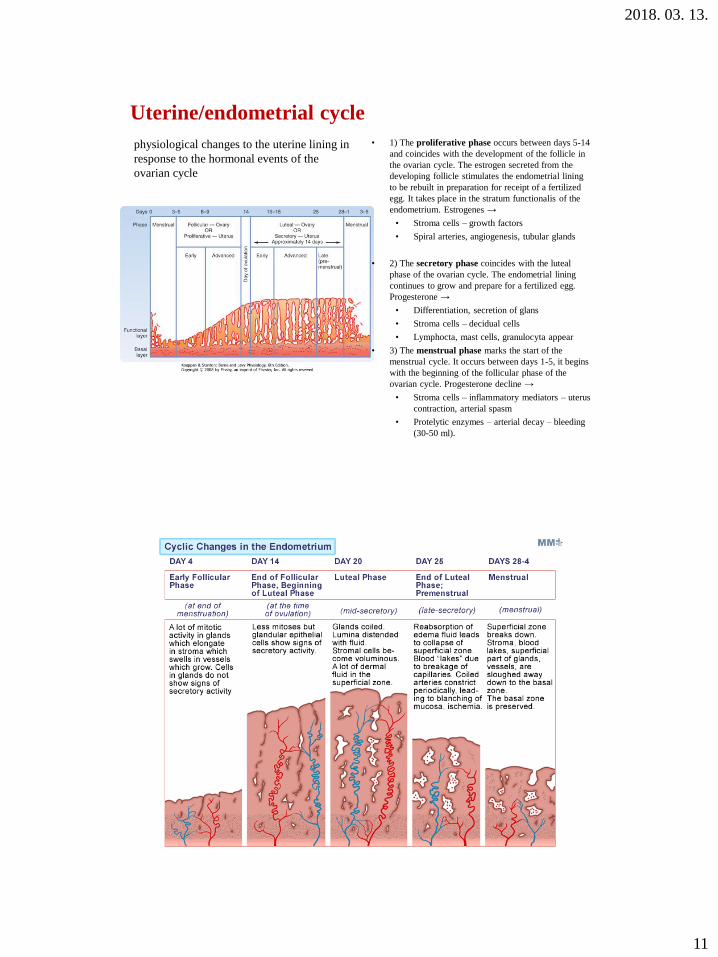
• 1) The proliferative phase occurs between days 5-14
and coincides with the development of the follicle in
the ovarian cycle. The estrogen secreted from the
developing follicle stimulates the endometrial lining
to be rebuilt in preparation for receipt of a fertilized
egg. It takes place in the stratum functionalis of the
endometrium. Estrogenes →
• Stroma cells – growth factors
• Spiral arteries, angiogenesis, tubular glands
• 2) The secretory phase coincides with the luteal
phase of the ovarian cycle. The endometrial lining
continues to grow and prepare for a fertilized egg.
Progesterone →
• Differentiation, secretion of glans
• Stroma cells – decidual cells
• Lymphocta, mast cells, granulocyta appear
• 3) The menstrual phase marks the start of the
menstrual cycle. It occurs between days 1-5, it begins
with the beginning of the follicular phase of the
ovarian cycle. Progesterone decline →
• Stroma cells – inflammatory mediators – uterus
contraction, arterial spasm
• Protelytic enzymes – arterial decay – bleeding
(30-50 ml).
Uterine/endometrial cycle
physiological changes to the uterine lining in
response to the hormonal events of the
ovarian cycle
2018. 03. 13.
12
Cervical cycle
• Follicular phase - estrogen – cervical mucus: thin, more, more
elastic secretion
• Luteal phase – progesterone – cervical mucus: thick, viscous
and less secretion
Neuroendocrine control of pregnancy
I. Sexual intercourse
II. Fertilization
III. Pregnancy
IV.Placenta
V. Child birth (delivery)
2018. 03. 13.
13
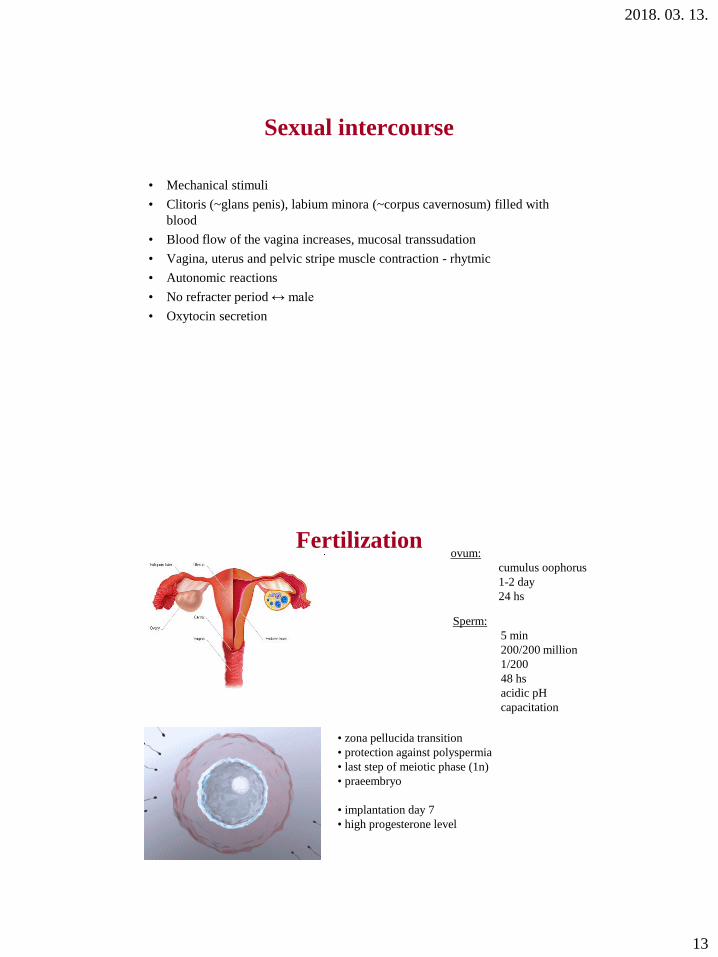
Sexual intercourse
• Mechanical stimuli
• Clitoris (~glans penis), labium minora (~corpus cavernosum) filled with
blood
• Blood flow of the vagina increases, mucosal transsudation
• Vagina, uterus and pelvic stripe muscle contraction - rhytmic
• Autonomic reactions
• No refracter period ↔ male
• Oxytocin secretion
Fertilization
Sperm:
5 min
200/200 million
1/200
48 hs
acidic pH
capacitation
ovum:
cumulus oophorus
1-2 day
24 hs
• zona pellucida transition
• protection against polyspermia
• last step of meiotic phase (1n)
• praeembryo
• implantation day 7
• high progesterone level
2018. 03. 13.
14
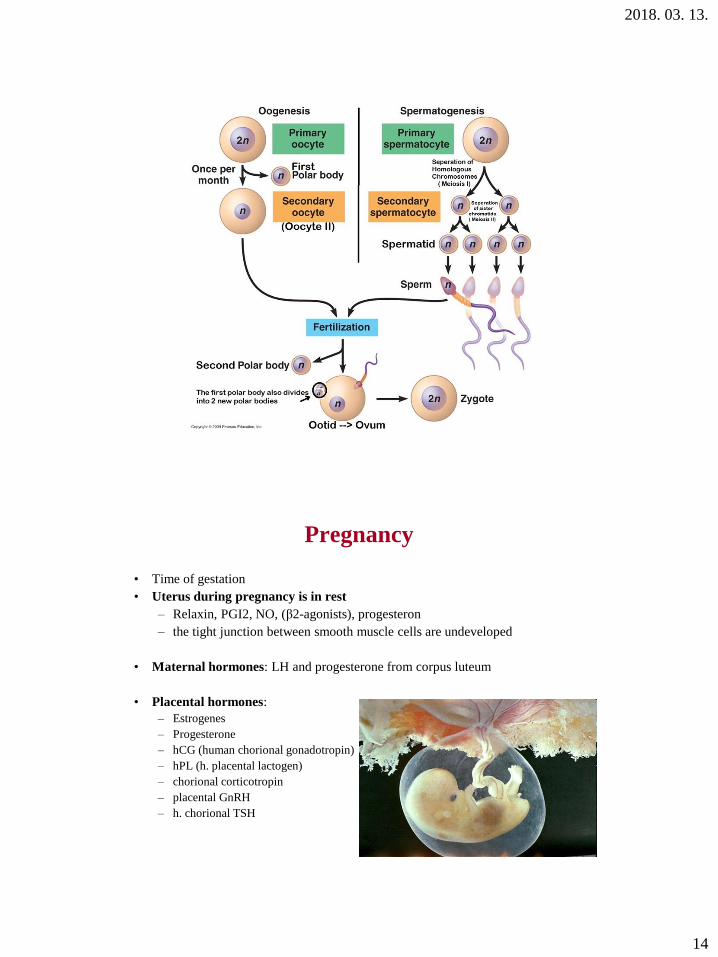
Pregnancy
• Time of gestation
• Uterus during pregnancy is in rest
– Relaxin, PGI2, NO, (β2-agonists), progesteron
– the tight junction between smooth muscle cells are undeveloped
• Maternal hormones: LH and progesterone from corpus luteum
• Placental hormones:
– Estrogenes
– Progesterone
– hCG (human chorional gonadotropin)
– hPL (h. placental lactogen)
– chorional corticotropin
– placental GnRH
– h. chorional TSH
2018. 03. 13.
15
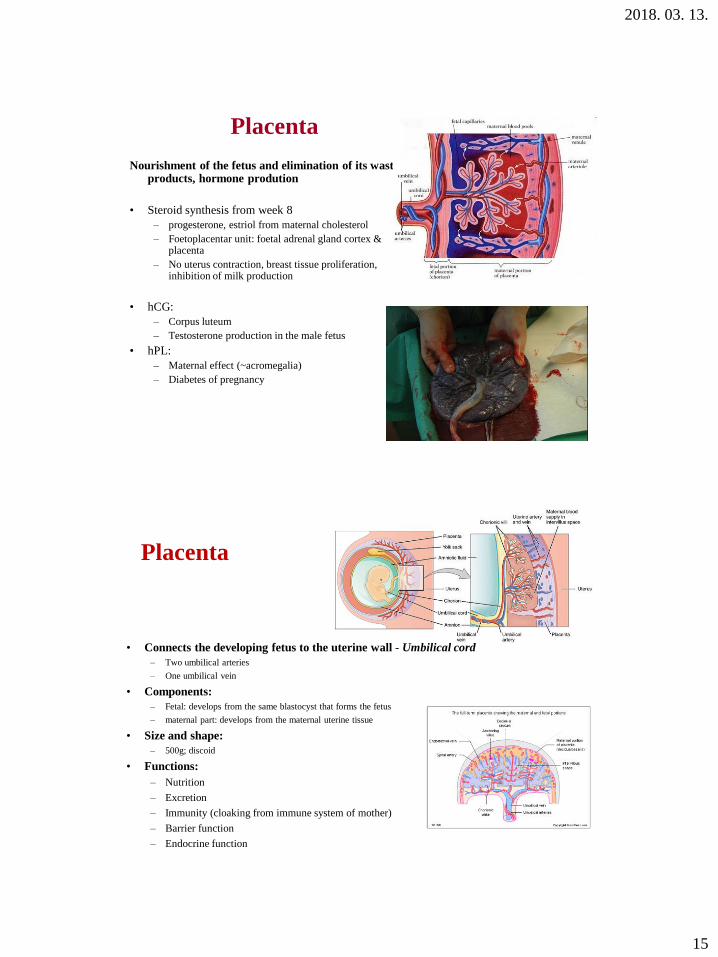
Placenta
Nourishment of the fetus and elimination of its waste products, hormone prodution
• Steroid synthesis from week 8
– progesterone, estriol from maternal cholesterol
– Foetoplacentar unit: foetal adrenal gland cortex & placenta
– No uterus contraction, breast tissue proliferation, inhibition of milk production
• hCG:
– Corpus luteum
– Testosterone production in the male fetus
• hPL:
– Maternal effect (~acromegalia)
– Diabetes of pregnancy
Placenta
• Connects the developing fetus to the uterine wall - Umbilical cord
– Two umbilical arteries
– One umbilical vein
• Components:
– Fetal: develops from the same blastocyst that forms the fetus
– maternal part: develops from the maternal uterine tissue
• Size and shape:
– 500g; discoid
• Functions:
– Nutrition
– Excretion
– Immunity (cloaking from immune system of mother)
– Barrier function
– Endocrine function

2018. 03. 13.
16
Protective (barrier) functions … BUT …• against infectious agents (IgG)
• there are some microbes that can cross this barrier, occasionally following placental lesions
and can lead to a miscarriage or leave behind congenital abnormalities. Transmission
possibilities:
– the transplacental infection during or shortly before birth
– the passage of the child through the maternal birth canal (HIV in the cervix mucus).
• Sexually transmitted diseases:
– treponema pallidum; HIV (15-20%) ; Gonorrhea (blennorrhoea neonatorum)
• Fetotoxic infections: rubella virus; toxoplasmosis; listeriosis; cytomegalovirus
• Medications:
– antibiotics and corticoids can pass through the placental barrier.
– certain steroid hormones get through as well (depending on their size).
• medications with well-documented teratogenic effects: e.g., Thalidomide (tranquillizer,
Contergan scandal), Roaccutane
• Barbiturates, alcohol… (abuse, addiction)
Endocrine function
• Before implantation hormone production is ensured through ovarian and
hypophyseal hormones
• During the pregnancy the hormone concentration in the maternal blood is
regulated by the cooperation of the placental, hypophyseal and fetal
suprarenal hormones as well as hormones from the gonads:
– The activity of the corpus luteum decreases progressively with the beginning of the 8th
week
– Replaced by the placenta at the end of the 1st trimester
At the beginning of the pregnancy the
syncytiotrophoblast produces the HCG
that has effects at both the level of the
infantile suprarenal glands (induces
DHEA) and the maternal corpus luteum
(induced secretion of E2 and P).
2018. 03. 13.
17
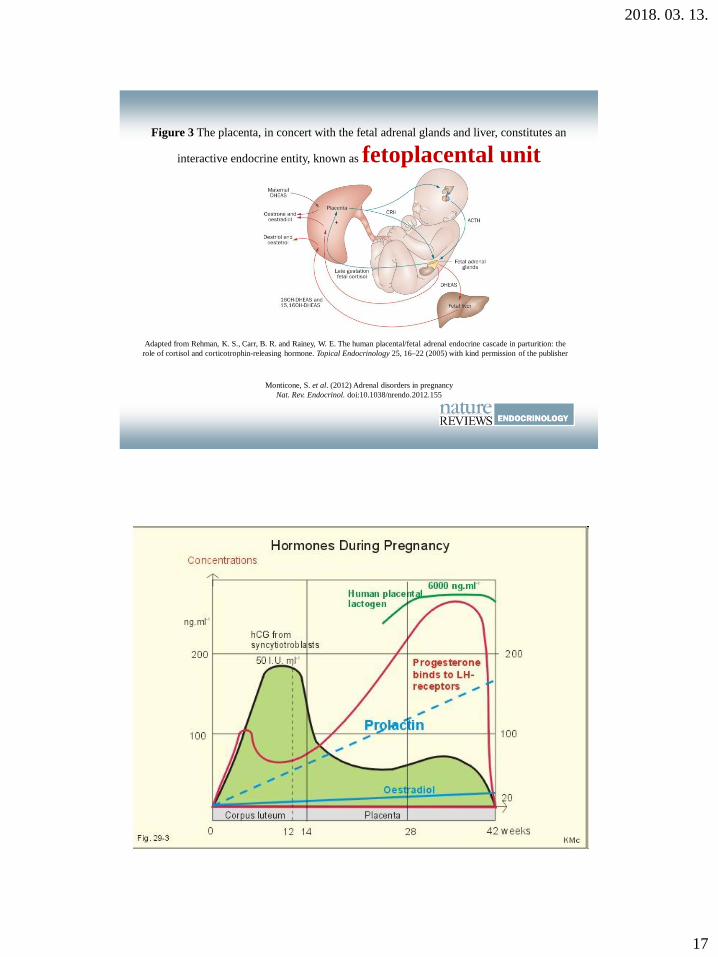
Figure 3 The placenta, in concert with the fetal adrenal glands and liver, constitutes an
interactive endocrine entity, known as fetoplacental unit
Monticone, S. et al. (2012) Adrenal disorders in pregnancy
Nat. Rev. Endocrinol. doi:10.1038/nrendo.2012.155
Adapted from Rehman, K. S., Carr, B. R. and Rainey, W. E. The human placental/fetal adrenal endocrine cascade in parturition: the
role of cortisol and corticotrophin-releasing hormone. Topical Endocrinology 25, 16–22 (2005) with kind permission of the publisher
2018. 03. 13.
18
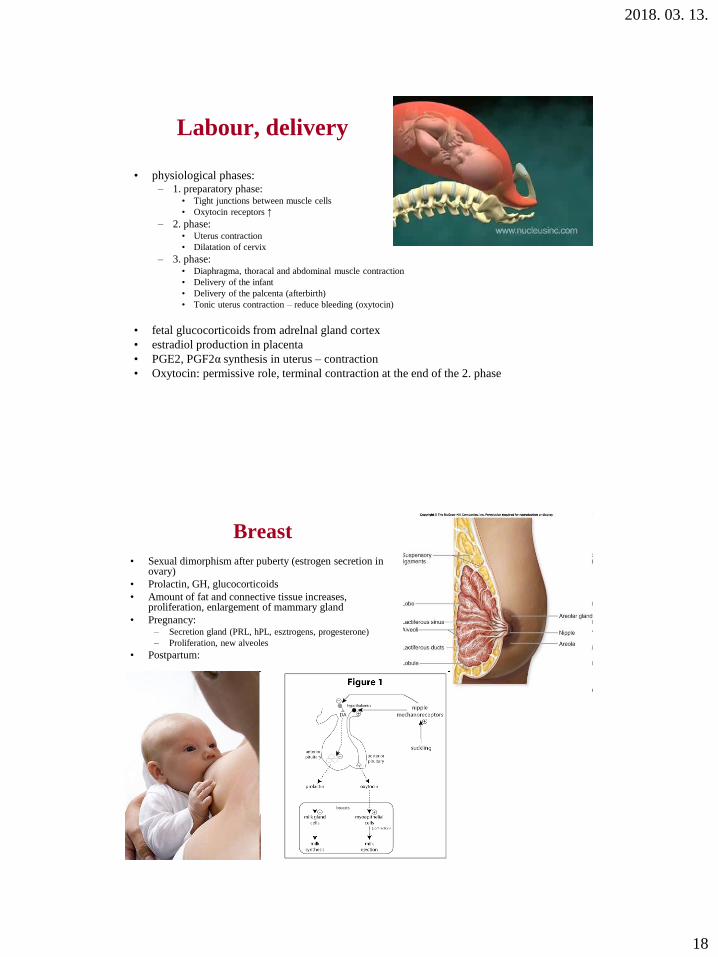
Labour, delivery
• physiological phases:– 1. preparatory phase:
• Tight junctions between muscle cells
• Oxytocin receptors ↑
– 2. phase:• Uterus contraction
• Dilatation of cervix
– 3. phase:• Diaphragma, thoracal and abdominal muscle contraction
• Delivery of the infant
• Delivery of the palcenta (afterbirth)
• Tonic uterus contraction – reduce bleeding (oxytocin)
• fetal glucocorticoids from adrelnal gland cortex
• estradiol production in placenta
• PGE2, PGF2α synthesis in uterus – contraction
• Oxytocin: permissive role, terminal contraction at the end of the 2. phase
Breast
• Sexual dimorphism after puberty (estrogen secretion in ovary)
• Prolactin, GH, glucocorticoids
• Amount of fat and connective tissue increases, proliferation, enlargement of mammary gland
• Pregnancy:– Secretion gland (PRL, hPL, esztrogens, progesterone)
– Proliferation, new alveoles
• Postpartum:
2018. 03. 13.
19
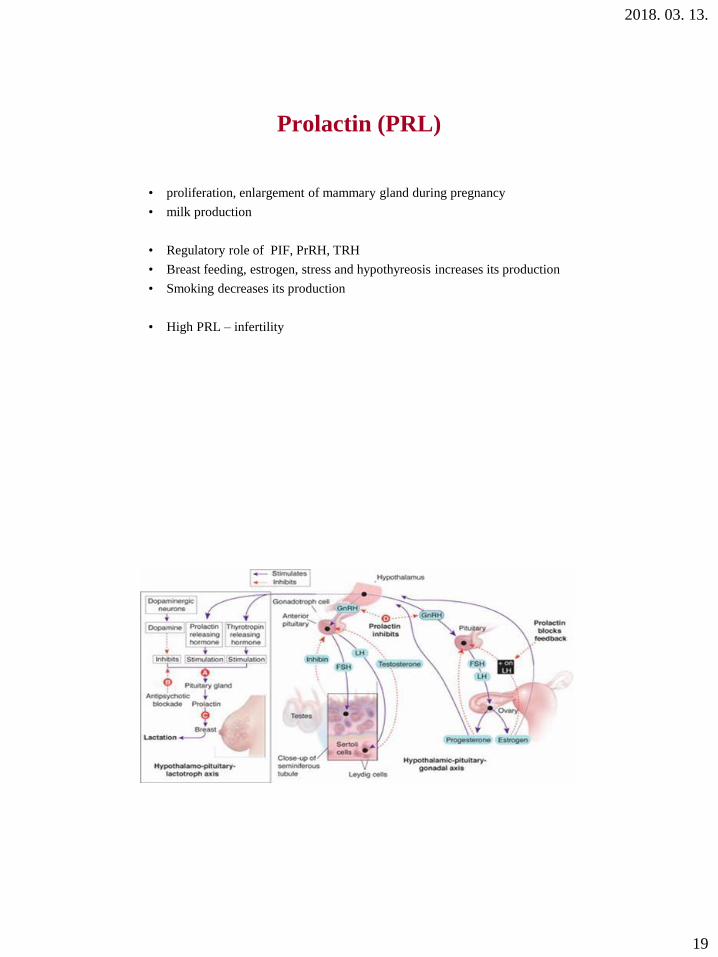
Prolactin (PRL)
• proliferation, enlargement of mammary gland during pregnancy
• milk production
• Regulatory role of PIF, PrRH, TRH
• Breast feeding, estrogen, stress and hypothyreosis increases its production
• Smoking decreases its production
• High PRL – infertility