Feasibility of continuous multiorgan variability analysis in the intensive care unit
12
Feasibility of continuous multiorgan variability analysis in the intensive care unit ☆,☆☆ Beverly Bradley MASc a , Geoffrey C. Green MASc a , Izmail Batkin PhD a , Andrew J.E. Seely MD, PhD a,b,c, ⁎ a Ottawa Hospital Research Institute, Ottawa, Ontario, Canada, K1H 8L6 b Division of Thoracic Surgery, University of Ottawa, Ottawa, Ontario, Canada, K1H 8L6 c Department of Critical Care Medicine, University of Ottawa, Ottawa, Ontario, Canada, K1H 8L6 Keywords: Heart rate variability; Respiratory rate variability; Continuous waveform monitoring; Multiorgan; Data loss; Data quality Abstract Purpose: The aim of the study was to evaluate the feasibility of continuous heart and respiratory rate variability (HRV and RRV, respectively) monitoring in critically ill patients derived from electrocardiogram (ECG) and end-tidal capnography (etCO 2 ) waveforms. Methods: Thirty-four patients (age, 56.5 ± 15.9 years; Acute Physiology and Chronic Health Evaluation II score, 22.8 ± 6.7) underwent continuous recording of ECG and etCO 2 waveforms from intensive care unit admission and intubation to discharge or maximum of 14 days. Overlapping 5-minute windows were analyzed with a wide range of variability measures (time, frequency, entropy, and scale-invariant and nonlinear domains). Waveform data quality, presence of disconnections and arrhythmias, quality of beat and breath detection, and subsequent variability computations were evaluated. Results: Patients were enrolled for 11.0 ± 3.6 days. The proportion of missing waveform data among all patients was (median [interquartile range, maximum]) 2.9% (1.3%-9.7%, 36.4%) for ECG and 3.1% (1.1%-11.4%, 84.5%) for etCO 2 . Heart rate variability data loss (ie, proportion of windows removed) was 1.3% (1.0%-2.1%, 5.9%) due to disconnection, 0.6% (0.1%-3.9%, 39.5%) due to atrial fibrillation, and 6.6% (1.4%-17.9%, 89.0%) due to data cleaning. Respiratory rate variability data loss was 7.3% (2.9%-11.6%, 47.7%) due to disconnection (or apnea) and 5.5% (2.9%-8.4%, 56.4%) due to cleaning. Continuous individualized multiorgan variability analysis processing resulted in HRV and RRV computations for 81.2% ± 25.0% and 87.5% ± 11.9% of available ECG and etCO 2 waveform data, respectively. Conclusions: The quality of continuously recorded ECG and etCO 2 waveforms in critically ill patients is adequate for subsequent continuous variability monitoring in this pilot study. The clinical utility of continuous variability analysis merits further investigation. © 2012 Elsevier Inc. All rights reserved. ☆ Institution at which the work was done: Ottawa Hospital Research Institute, Ottawa, Ontario, Canada. ☆☆ Competing interests: Andrew JE Seely founded Therapeutic Monitoring Systems (TMS), Inc. to commercialize patented Continuous Individualized Multiorgan Variability Analysis (CIMVA) technology with the objective of delivering variability-directed clinical decision support to improve quality and efficiency of care. All the other authors have no conflicts of interest to disclose. ⁎ Corresponding author. Divisions of Thoracic Surgery and Critical Care Medicine, Ottawa Hospital-General Campus, Box 708, Ottawa, Ontario, Canada K1H 8L6. Tel.: +1 613 737 8899x74892; fax: +1 613 737 8668. E-mail address: [email protected] (A.J.E. Seely). 0883-9441/$ – see front matter © 2012 Elsevier Inc. All rights reserved. doi:10.1016/j.jcrc.2011.09.009 Journal of Critical Care (2012) 27, 218.e9–218.e20
-
Upload
beverly-bradley -
Category
Documents
-
view
218 -
download
4
Transcript of Feasibility of continuous multiorgan variability analysis in the intensive care unit

Journal of Critical Care (2012) 27, 218.e9–218.e20
Feasibility of continuous multiorgan variability analysis inthe intensive care unit☆,☆☆
Beverly Bradley MASca, Geoffrey C. Green MASca,Izmail Batkin PhDa, Andrew J.E. Seely MD, PhDa,b,c,⁎
aOttawa Hospital Research Institute, Ottawa, Ontario, Canada, K1H 8L6bDivision of Thoracic Surgery, University of Ottawa, Ottawa, Ontario, Canada, K1H 8L6cDepartment of Critical Care Medicine, University of Ottawa, Ottawa, Ontario, Canada, K1H 8L6
Me
K
0d
Keywords:Heart rate variability;Respiratory rate variability;Continuous waveformmonitoring;Multiorgan;Data loss;Data quality
AbstractPurpose: The aim of the study was to evaluate the feasibility of continuous heart and respiratory ratevariability (HRV and RRV, respectively) monitoring in critically ill patients derived fromelectrocardiogram (ECG) and end-tidal capnography (etCO2) waveforms.Methods: Thirty-four patients (age, 56.5 ± 15.9 years; Acute Physiology and Chronic Health EvaluationII score, 22.8 ± 6.7) underwent continuous recording of ECG and etCO2 waveforms from intensive careunit admission and intubation to discharge or maximum of 14 days. Overlapping 5-minute windowswere analyzed with a wide range of variability measures (time, frequency, entropy, and scale-invariantand nonlinear domains). Waveform data quality, presence of disconnections and arrhythmias, quality ofbeat and breath detection, and subsequent variability computations were evaluated.Results: Patients were enrolled for 11.0 ± 3.6 days. The proportion of missing waveform data amongall patients was (median [interquartile range, maximum]) 2.9% (1.3%-9.7%, 36.4%) for ECG and3.1% (1.1%-11.4%, 84.5%) for etCO2. Heart rate variability data loss (ie, proportion of windowsremoved) was 1.3% (1.0%-2.1%, 5.9%) due to disconnection, 0.6% (0.1%-3.9%, 39.5%) due to atrialfibrillation, and 6.6% (1.4%-17.9%, 89.0%) due to data cleaning. Respiratory rate variability data losswas 7.3% (2.9%-11.6%, 47.7%) due to disconnection (or apnea) and 5.5% (2.9%-8.4%, 56.4%) dueto cleaning. Continuous individualized multiorgan variability analysis processing resulted in HRV andRRV computations for 81.2% ± 25.0% and 87.5% ± 11.9% of available ECG and etCO2 waveformdata, respectively.Conclusions: The quality of continuously recorded ECG and etCO2 waveforms in critically ill patientsis adequate for subsequent continuous variability monitoring in this pilot study. The clinical utility ofcontinuous variability analysis merits further investigation.© 2012 Elsevier Inc. All rights reserved.
☆ Institution at which the work was done: Ottawa Hospital Research Institute, Ottawa, Ontario, Canada.☆☆ Competing interests: Andrew JE Seely founded Therapeutic Monitoring Systems (TMS), Inc. to commercialize patented Continuous Individualized
ultiorgan Variability Analysis (CIMVA) technology with the objective of delivering variability-directed clinical decision support to improve quality andfficiency of care. All the other authors have no conflicts of interest to disclose.⁎ Corresponding author. Divisions of Thoracic Surgery and Critical Care Medicine, Ottawa Hospital-General Campus, Box 708, Ottawa, Ontario, Canada
1H 8L6. Tel.: +1 613 737 8899x74892; fax: +1 613 737 8668.E-mail address: [email protected] (A.J.E. Seely).
883-9441/$ – see front matter © 2012 Elsevier Inc. All rights reserved.oi:10.1016/j.jcrc.2011.09.009

218.e10 B. Bradley et al.
1. Introduction
Improving individualized patient monitoring is a criticalongoing objective in the intensive care unit (ICU); however,several barriers still exist to the effective management andextraction of useful information in this setting [1]. One majorchallenge is harvesting the physiologic data continuouslycollected at the bedside as per standard patient care.Enormous quantities of potentially useful data are discardedevery day largely because of technical barriers, such as theneed for specialized software and issues when interfacingbetween data acquisition, data analysis, and commercialmonitoring systems [2]. A survey of 50 ICUs in Ontario,Canada, reported that only 22% of sites had access to bedsidemonitor data outside the ICU (but within the hospital) and thatonly 7 sites (14%) had the ability to capture data directly frompatient monitors [3]. Several research platforms capable ofcontinuous long-term physiologic data acquisition in the ICUhave been introduced [2,4-9], and commercial products arestarting to appear on the market (eg, BedmasterEx [ExcelMedical Electronics, Jupiter, Florida], Capsule Technologies,Andover, Massachusetts, and iSirona, Panama City, Florida).However, continuous acquisition of bedside monitoring dataremains uncommon and of unproven clinical value.
As the technological barriers to harvesting ICU datacontinue to be surmounted, a second challenge is findingways to condense the plethora of data generated in an ICU(continuous streams of physiologic waveforms from severaldifferent monitors) into a comprehensive yet parsimonioussummary of useful information. Rather than monitoring vitalsigns individually, 1 approach is to treat the host's responseto disease processes as a complex system and to usevariability analysis to better characterize the system stateover time. In particular, the reduced degree and complexityof variability are thought to be indicative of stress andreduced adaptability [10,11]. Continuous patient monitoringin the ICU combined with variability analysis introduces thepossibility of analyzing the evolution of variability over time.
There is considerable evidence that heart rate variability(HRV) is altered in association with disease processes and maybe used to describe the status of critically ill patients [10,12-15].Heart rate variability analysis has also shown prognosticcapabilities in adult septic patients as an early marker of multipleorgan dysfunction syndrome (MODS) [16] and an earlypredictor of death in emergency departments [17]. Respiratoryrate variability (RRV), defined as the breath-to-breath changes inthe respiratory rate, was identified as a novel predictor ofsuccessful weaning of patients from mechanical ventilation [18-23]. These prior studies generally assess variability for shortisolated epochs. We hypothesize that a continuous approach toboth HRV and RRV analyses, which examine a wide panel ofHRV and RRV metrics, could provide a means to track thesystemic state of a complex human system. This technology iswell suited to the ICU, in which real-time, continuous, digitalphysiologic data acquisition (including waveform analysis) has
already been demonstrated [2,4-9]. Although many freelyavailable tools exist that facilitate variability analysis (eg,Physionet [24]), there exists no standardized comprehensivevariability analysis solution, nor does there exist ameans to trackmultiorgan variability continuously over time.
Continuous individualized multiorgan variability analysis(CIMVA) is a software tool that we have developed forcontinuous HRV and RRV monitoring to assess the potentialto improve care for patients at risk for or with existing criticalillness, such as sepsis [25] or risk of failed extubation. In thispilot study, our main objective was to explore the feasibility ofcontinuous automated HRV and RRV monitoring (usingCIMVA) derived from electrocardiogram (ECG) and end-tidalcapnogram (etCO2) waveforms harvested from critically illpatients in an ICU setting. This activity consisted of 4 phases:(1) developing a system to conveniently collect patientwaveform data (ECG and etCO2) from any ICU bed, (2)converting the waveform data into a time series of inter-beat/interbreath intervals, (3) using the CIMVA software tocalculate a wide panel of continuous HRV and RRV outputs toprovide information previously unavailable to the clinician,and (4) annotating the new data with data quality measures ateach stage. We assess the success of this endeavor bothqualitatively (by commenting on the setup and the system'sease of use) and quantitatively (by evaluating the amount ofmissing or rejected data vs. the remaining usable high-qualitydata collected for subsequent variability analysis).
2. Methods
2.1. Consent
This study was approved by the Ottawa Hospital ResearchEthics Board. Waived consent was obtained because thestudy was observational, data were deidentified, and wewished to eliminate the potential for bias and limitations toexternal validity.
2.2. Patient enrollment
Critically ill patients experiencing respiratory and/orcardiac failure were selected to have their ECG and etCO2
continuously recorded while in the ICU. Thirty-four patientswere enrolled between June 2009 and November 2009. Datacollection was initiated within 36 hours of admission to theICU, and patients were monitored for 14 days or until ICUdischarge, whichever came first.
2.2.1. Inclusion criteriaInclusion criteria were respiratory and/or cardiac failure,
enrollment in the study within 36 hours of ICU admission,and expected period on study greater than 72 hours. Re-spiratory failure is defined as the need for mechanicalventilation and a PaO2/FiO2 less than 300. Cardiac failure is

218.e11Continuous multiorgan variability analysis in the ICU
defined as hypotension requiring 2 or more consecutivehours of vasopressors (norepinephrine or epinepherineN5 μg/kg per minute, phenylephrine N50 μg/min, orvasopressin N0.03 U/min).
2.2.2. Exclusion criteriaExclusion criteria were chronic atrial fibrillation (a-fib)
(determined frommedical history reported by the patient/familyto the treating team) and/or being transferred from another ICU.
2.3. Clinical data collection
The following parameters were recorded for each patientupon enrollment into the study: demographic information, ICUadmission diagnosis, comorbidities, andAcute Physiology andChronic Health Evaluation II score on the day of admission.Other parameters recorded throughout the study periodincluded date and time of extubation, total length of stay (ifwithin 30 days), survival status in ICUand at 30 days from ICUadmission, need for reintubation, and need for tracheotomy.These data were recorded on a clinical case report form (CRF)by a clinical research coordinator. Collection of the clinicaldata required a significant amount of effort, and, in particular,regular communication with nursing staff was required toensure that major interventions were not missed. The timing ofall clinical events (e.g, extubation time) was recorded based onthe displayed time on the Philips Intellivue patient monitors(Philips Healthcare, Andover, Massachusetts) to ensure thatthe time-stamped waveform data (and the resulting continuousHRV and RRV time series) were accurately aligned withactivities at the bedside.
ResearchNetwork
PhilipsNetwork
PhilipsInformCente
Intensive Care Unit
Intellivue monitors
Research Lab
CIMVA engine
Wav
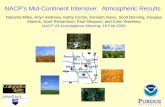
Fig. 1 Overview of data ha
The following parameters were recorded daily for eachpatient: MODS score and Sequential Organ Failure Assessmentscore, ventilator settings during the day and night (includinghighest level of ventilator support, maximum pressure support,level of positive end-expiratory pressure, and FiO2), presence anddosages of inotropes and/or vasopressors, presence and timing ofdialysis, timing of sedation interruptions, and patient rest periods.All major interventions performed (eg, central line, bronchos-copy, etc) were recorded as well as any new diagnoses.
2.4. Waveform collection and data harvest process
Continuous data collection was performed by harvesting theECG and etCO2 waveforms from Phillips Intellivue MP70bedside monitors. The ECG waveform is already monitored asper standard practice in the critical care environment. End-tidalcapnography monitoring requires a removable module thatinterfaces with the Philips Intellivue system and is used on an as-needed basis in the ICU. Electrocardiographic monitoring wasinitiated at time of ICU admission and continued until ICUdischarge or a maximum of 14 days; etCO2 monitoring wasinitiated when CO2 modules were applied at time of enrollmentand continued until extubation or a maximum of 14 days.Electrocardiogram and etCO2 (both sampled at 125 Hz; in thecase of etCO2, data were only collected while the patient wasintubated) were collected continuously for 24 hours a day anddownloaded manually on a per-patient basis using the PhilipsIntellivue Information Centre (PIIC) central station. Downloadswere done retrospectively on a daily basis.
The setup and process for harvesting patient waveformdata are shown in Fig. 1. When the download process is
Intellivue ationr (PIIC)
Holter Export
Hospital Network
Hospital Network
Philips Database Server
eformfile
Waveformfile
Patient IDfile
rvest setup and process.

218.e12 B. Bradley et al.
initiated at the PIIC station, patient data are transferred fromthe Philips Database Server over the hospital network to anOttawa Hospital Research Institute file server, accessibleonly by the research laboratory where CIMVA processingoccurs. The data are deidentified when it reaches the researchlaboratory. This download process uses the Philips IntellivueHolter Data Export software feature on the Philips DatabaseServer, which was installed by Philips for research purposes.With this feature enabled, the Philips Database Server is ableto transfer files containing physiologic waveforms from theICU to the hospital network.
2.5. Data processing steps andvariability computation
When the waveform data arrived at the research file serverafter the data harvest process, HRV and RRV analyses wereperformed for each patient using the CIMVA softwareengine. Continuous individualized multiorgan variabilityanalysis is currently implemented inMatlab (TheMathworks,Natick, Massachusetts), and data processing occurs on astandard PC (2 GB RAM, 2.20GHz processor speed). Thedata processing steps for both ECG and etCO2 waveform dataare shown in Fig. 2 and explained in more detail in AppendixE1 [26-28]. In this study, variability measures were calculatedusing sliding windows of 5-minute duration, with 50%overlap (2.5 minutes) between adjacent windows. Thisresulted in a complete set of variability and data qualitymeasures every 2.5 minutes. The output from the CIMVAdata processing engine is a matrix consisting of 1 row forevery input window (every 2.5 minutes in this study) and 1column for each of the data quality and HRV and RRVmeasures. The variability measures calculated by CIMVAhave been verified against surrogate data sets with knownproperties and, where possible, third-party software (eg,Kubios HRV (University of Eastern Finland) and Physionet).
ig. 2 The CIMVA data processing steps for both ECG and CO2
aveform data.
2.6. Analysis of data quality2.6.1. Missing data before CIMVA variability processingThe amount of missing data per patient was based on the
proportion of the total time for which data could have beencollected during that patient's ICU stay. Missing data consistof a complete disconnection of the monitoring device for anylength of time (ie, no signal present), a waveform segmentidentified by the Philips monitor as being erroneous (ie,signal is present, but sensor is disconnected), or corrupted ormissing data because of problems with the downloadprocess. Periods in which the patient was not intubated didnot count as missing etCO2 waveform data.
2.6.2. Data quality after CIMVA variability processingAfter CIMVA variability analysis of the waveform data,
the number of 5-minute variability windows filtered out
Fw
during the postprocessing stage was computed (for details,see step 7 in Appendix E1).
3. Results
3.1. Demographic data
Thirty-four patients were enrolled in the study. Only asingle patient (patient 7) was excluded because of chronic a-fib. Demographic information for the remaining 33 subjectsis shown in Table E1. Mean age was 56.5 years (±15.9); 39%were female, and 61%, male. The most common pattern oforgan failure was simultaneous respiratory and cardiacfailures (n = 23 patients) compared with just respiratory (n =

218.e13Continuous multiorgan variability analysis in the ICU
7) or just cardiac (n = 3) failure. On the day of admission, meanAcute Physiology and Chronic Health Evaluation II score was22.8 (±6.7), and mean MODS score was 6.8 (±2.9). Meannumber of days enrolled in the study was 11.0 days (±3.6days). Seven patients died within the 14-day monitoringperiod, and another 3 died within 30 days of enrollment(30-day mortality rate of 29.4%).
3.2. Missing data before CIMVA processing
3.2.1. ElectrocardiogramIn total, there were approximately 359 patient-days of
ECG monitoring time. As shown in Table 1, averageper-patient ECG monitoring time was 246 hours 33minutes (±102 hours 33 minutes) or 10.27 days. The
Table 1 Summary of collected and missing ECG waveform data bef
Patient ECG start(time of ICU admission)
ECG end(last recorded time)
ToEChh
2 June 21, 2009, 16:05 July 6, 2009, 13:47 353 June 22, 2009, 21:25 July 2, 2009, 09:21 224 June 23, 2009, 03:45 July 3, 2009, 09:52 245 a July 7, 2009, 09:45 July 16, 2009, 10:21 216 a July 7, 2009, 12:10 July 19, 2009, 18:06 298 July 13, 2009, 14:50 July 20, 2009, 20:18 179 July 16, 2009, 00:00 July 30, 2009, 11:54 3410 July 16, 2009, 18:00 July 31, 2009, 08:51 3511 July 17, 2009 02:10 July 22, 2009, 18:59 1312 July 23, 2009, 04:25 August 6, 2009, 12:43 3413 August 2, 2009, 12:20 August 17, 2009, 12:28 3614 August 4, 2009, 01:05 August 13, 2009, 19:30 2315 August 6, 2009, 08:45 August 7, 2009, 21:45 316 August 11, 2009, 11:15 August 26, 2009, 09:43 3517 August 11, 2009, 11:53 August 26, 2009, 09:38 3518 August 13, 2009, 15:00 August 28, 2009, 08:51 3519 August 16, 2009, 01:20 August 28, 2009, 09:00 2920 August 30, 2009, 23:55 September 9, 2009, 16:39 2321 September 1, 2009, 12:10 September 4, 2009, 13:06 722 September 10, 2009, 23:20 September 25, 2009, 08:59 3423 September 10, 2009, 18:46 September 15, 2009, 09:12 1124 September 15, 2009, 05:20 September 25, 2009, 09:00 2425 September 23, 2009, 20:30 October 1, 2009, 10:02 1826 October 1, 2009, 21:50 October 16, 2009, 08:44 3427 October 18, 2009, 20:45 October 30, 2009, 09:07 2728 October 20, 2009, 11:10 October 30, 2009, 13:04 2429 October 23, 2009, 15:05 November 3, 2009, 01:00 2430 October 27, 2009, 11:50 November 10, 2009, 10:43 3331 October 29, 2009, 02:45 November 13, 2009, 09:19 3632 November 3, 2009, 12:50 November 18, 2009, 10:01 3533 November 4, 2009, 02:00 November 5, 2009, 18:15 434 November 9, 2009, 03:50 November 16, 2009, 09:43 1735 November 10, 2009, 15:30 November 25, 2009, 09:48 35
Mean 26SD 10Median 27IQR (Q1-Q3)
a Information Technology (IT) IT maintenance on monitoring network duri
proportion of missing data (among all patients) was(median [interquartile range {IQR}, maximum]) 2.9%(1.3%-9.7%, 36.4%). Two patients (5 and 6) had greaterthan 25% of their data missing; this was because of ascheduled maintenance activity on the Philips clinicalnetwork (see Discussion).
3.2.2. End-tidal capnographyThere were approximately 296 patient-days of etCO2
monitoring time. As shown in Table 2, average per-patient etCO2 monitoring time was 195 hours 52 minutes(±117 hours 23 minutes) or 8.16 days. The proportion ofmissing data (among all patients) was 3.1% (1.1%-11.4%,84.5%). Four patients (3, 5, 6, and 25) had greater than25% of their data missing; for patients 5 and 6, this was
ore CIMVA processing
tal (possible)G (hh:mm),=hour, mm=min
Time missing(hh:mm)
% missing Time remaining(hh:mm)
7:42 01:50 0.51 355:517:56 10:45 4.72 217:116:07 14:48 6.02 231:186:36 78:51 36.41 137:443:56 97:53 33.30 196:033:28 09:06 5.25 164:217:54 06:07 1.76 341:460:51 09:31 2.72 341:196:49 00:07 0.09 136:414:18 05:01 1.46 339:160:08 12:15 3.41 347:524:25 01:23 0.59 233:017:00 04:57 13.40 32:038:28 10:22 2.89 348:067:45 01:39 0.47 356:053:51 04:03 1.15 349:475:40 31:21 10.61 264:182:44 27:58 12.02 204:452:56 00:02 0.06 72:535:39 09:18 2.69 336:210:26 26:33 24.05 83:533:40 06:55 2.85 236:441:32 01:37 0.89 179:556:54 09:04 2.62 337:496:22 25:56 9.38 250:261:54 03:15 1.35 238:399:55 17:01 6.81 232:544:53 13:36 4.07 321:166:34 10:32 2.87 356:027:11 00:12 0.06 356:580:15 08:26 20.98 31:483:53 18:22 10.57 155:304:18 06:38 1.87 347:391:16 14:43 6.91 246:330:03 20:52 9.25 102:336:22 09:06 2.9 238:39
1.3-9.7
ng patient stay.

Table 2 Summary of collected and missing etCO2 waveform data before CIMVA processing
Patient etCO2 start(tube connection time)
etCO2 end(last extubation orlast recorded time)
Total (possible)etCO2 (hh:mm)hh=hour, mm=min
Time missing a
(hh:mm)% missing Time remaining
(hh:mm)
2 June 22, 2009, 10:40 July 5, 2009, 17:20 318:40 24:47 7.78 293:523 June 24, 2009, 12:06 June 30, 2009, 05:05 136:59 115:47 84.53 21:114 June 24, 2009, 10:39 June 28, 2009, 11:00 96:21 00:22 0.39 95:585 b July 7, 2009 11:40 July 15, 2009, 11:15 191:35 77:06 40.24 114:296 b July 8, 2009, 11:15 July 14, 2009, 11:28 144:13 72:16 50.12 71:568 July 14, 2009, 15:18 July 16, 2009, 14:25 47:07 00:40 1.42 46:279 July 16, 2009, 11:19 July 30, 2009, 11:54 336:35 10:28 3.11 326:0610 July 17, 2009, 11:43 July 31, 2009, 08:51 333:08 03:30 1.05 329:3711 July 17, 2009, 12:02 July 20, 2009, 14:38 74:36 00:06 0.14 74:2912 July 23, 2009, 14:08 August 6, 2009, 12:40 334:32 04:32 1.36 329:5913 August 3, 2009, 09:47 August 17, 2009, 12:25 338:38 04:19 1.28 334:1814 August 4, 2009, 14:20 August 11, 2009, 13:10 166:50 00:09 0.10 166:4015 August 6, 2009, 13:37 August 7, 2009, 05:25 15:48 00:07 0.79 15:4016 August 12, 2009, 10:24 August 25, 2009, 02:30 294:06 10:51 3.69 283:1417 August 12, 2009, 10:45 August 26, 2009, 09:35 334:50 01:42 0.51 333:0718 August 14, 2009, 09:04 August 28, 2009, 08:48 335:44 06:29 1.93 329:1419 August 17, 2009, 13:05 August 26, 2009, 13:55 146:45 15:56 10.86 130:4820 August 31, 2009, 11:15 September 7, 2009, 13:05 169:50 21:49 12.85 148:0021 September 2, 2009, 10:10 September 4, 2009, 13:02 50:52 00:02 0.07 50:5022 September 11, 2009, 09:39 September 25, 2009, 16:10 342:31 09:45 2.85 332:4523 September 11, 2009, 14:11 September 13, 2009, 06:45 40:34 00:00 0.00 40:3424 September 15, 2009, 10:25 September 22, 2009, 10:50 168:25 04:03 2.41 164:2125 September 24, 2009, 09:50 September 30, 2009, 16:00 150:10 63:34 42.34 86:3526 October 2, 2009, 09:40 October 18, 2009, 16:00 390:20 63:48 16.35 326:3127 October 19, 2009, 09:50 October 29, 2009, 13:55 244:05 15:48 6.47 228:1628 October 21, 2009, 09:30 October 29, 2009, 13:50 196:20 03:19 1.70 193:0029 October 23, 2009, 16:00 November 2, 2009, 16:00 240:00 13:45 5.73 226:1430 October 28, 2009, 11:15 November 10, 2009, 08:00 308:45 11:01 3.57 297:4331 October 30, 2009, 11:50 November 13, 2009, 08:15 329:25 10:29 3.19 318:5532 November 4, 2009, 11:00 November 18, 2009, 08:57 325:12 12:03 3.71 313:0933 November 4, 2009, 11:00 November 5, 2009, 17:22 30:22 00:20 1.10 30:0234 November 9, 2009, 10:00 November 15, 2009, 15:10 149:10 24:41 16.56 124:2835 November 11, 2009, 13:15 November 25, 2009, 08:45 331:30 46:24 14.00 285:05
Mean 215:34 19:42 10.37 195:52SD 115:15 28:05 18.34 117:23Median 196:20 10:28 3.1 193:00IQR (Q1-Q3) 1.1-11.4
a Periods when the patient was extubated do not count as missing data and were deducted from the total possible etCO2 time.b IT maintenance on monitoring network during patient stay.
218.e14 B. Bradley et al.
because of the Philips clinical network maintenancementioned above. For patient 3, data were intermittentlymissing on days 4 to 6 because of problems with theetCO2 tubing (excessive humidity). More frequent checksof the monitor and tubing changes (as the studyprogressed) helped to reduce these problems. Patient 25initially used an etCO2 unit that was found to be faulty;the unit was replaced on day 3.
3.3. Data processing time
Total data processing time varied per patient because ofdiffering lengths of ICU stay. Processing time was roughly 2
seconds per 5-minute window of input data (including bothECG and etCO2 processing). For a typical patient (with a 14-day ICU stay), retrospectively computing all CIMVA resultsfor HRV and RRV took about 4.5 hours.
3.4. Data quality after CIMVA processing
All patients had some degree of HRV and RRV data (ie,5-minute windows) removed because of disconnection,cleaning, or a-fib (in the case of HRV data), as shown inTables 3 and 4. Note that any window can meet 1 or more ofthese rejection criteria and, thus, may be represented multipletimes in the data presented. The presence of disconnection

Table 3 Summary of RRI data quality after CIMVA data processing of ECG waveform
Patient Total time(hh:mm)
Total no.of 5-minwindows
Proportion of 5-min windows containing: Totalwindowsremaining
Proportionof windowsremoved (%)
N0%disconnection
≥50% atrialfibrillation detected
N3% ofRRIs cleaned
% n % n % n
2 a 355:51 8515 1.0 82 39.5 3364 19.0 1617 3522 58.63 217:11 5197 0.4 20 0.2 9 2.3 118 5055 2.74 231:18 5532 1.5 82 2.3 129 11.4 633 4732 14.55 a 137:44 3307 2.4 80 28.8 954 35.5 1175 1178 64.46 196:03 4701 5.9 278 5.0 234 13.5 635 4022 14.48 164:21 3938 1.2 47 11.0 435 17.6 693 3210 18.59 a 341:46 8187 1.2 99 2.3 188 89.0 7290 889 89.110 341:19 8172 0.9 77 0.1 8 0.1 12 8090 1.011 136:41 3272 0.5 16 0.0 0 0.1 3 3253 0.612 339:16 8131 1.0 78 3.7 297 4.8 390 7675 5.613 a 347:52 8329 1.3 110 11.4 946 27.0 2251 5107 38.714 233:01 5607 1.5 82 0.1 8 1.4 80 5455 2.715 32:03 767 0.3 2 0.5 4 11.3 87 678 11.616 348:06 8331 1.5 128 0.1 5 0.2 14 8193 1.717 a 356:05 8522 1.4 122 0.1 11 20.3 1728 6699 21.418 a 349:47 8372 1.1 94 0.6 52 11.5 963 7276 13.119 a 264:18 6324 2.0 125 15.5 980 80.1 5066 388 93.920 204:45 4902 2.1 102 0.7 36 3.9 190 4650 5.121 72:53 1743 2.2 38 0.0 0 1.4 25 1680 3.622 336:21 8049 1.4 111 0.1 11 6.6 532 7424 7.823 83:53 2017 2.8 57 1.6 32 12.0 242 1749 13.324 a 236:44 5676 2.3 130 0.8 43 32.1 1824 3784 33.325 a 179:55 4308 1.3 58 6.1 263 15.9 687 3335 22.626 337:49 8091 1.1 87 0.2 16 0.3 25 7986 1.327 250:26 5994 3.2 189 2.3 140 4.6 278 5553 7.428 238:39 5619 2.1 116 0.6 35 0.7 38 5498 2.229 a 232:54 5554 2.3 128 1.9 104 45.8 2546 2990 46.230 321:16 7665 0.9 69 0.1 7 2.1 162 7443 2.931 356:02 8500 1.2 106 0.2 19 0.3 26 8384 1.432 356:58 8517 1.5 126 0.2 18 0.4 34 8376 1.733 31:48 742 1.1 8 4.6 34 6.6 49 662 10.834 155:30 3699 0.9 35 0.1 3 4.2 154 3513 5.035 347:39 8302 1.0 87 0.1 6 1.4 114 8107 2.3Mean 246:33 5896 1.6 90.0 4.3 254.3 14.7 899.4 4744.1 18.8SD 102:33 2454 1.0 53.3 8.7 623.6 21.4 1554.8 2614.9 25.0Median 238:39 5676 1.3 87 0.6 34 6.6 242 4732 7.8IQR (Q1-Q3) 4308-8187 1.0-2.1 0.1-3.9 1.4-17.9 3210-7424 2.7-21.4
a Denotes patients who experienced episodes of a-fib, bigeminy, trigeminy, or other arrhythmias or irregular sinus rhythm at some point during the study period.
218.e15Continuous
multiorgan
variabilityanalysis
inthe
ICU

Table 4 Summary of IBI data quality after CIMVA data processing of etCO2 waveform
Patient Total time(hh:mm)
Total no.of 5-minwindows
Proportion of 5-min windows containing: Totalwindowsremaining
Proportionof windowsremoved (%)
N0%disconnection
≥5% ofIBIs cleaned
% n % n
2 293:52 7031 2.8 200 2.8 199 6639 5.63 21:11 1079 3.8 41 1.2 13 1037 3.94 95:58 2295 2.5 57 4.7 108 2130 7.25 114:29 2743 9.9 272 5.1 140 2361 13.96 71:56 1750 4.6 81 6.5 113 1589 9.28 46:27 1117 1.7 19 1.0 11 1087 2.79 326:06 7818 7.3 573 5.5 428 6950 11.110 329:37 7893 21.2 1673 56.4 4451 3226 59.111 74:29 1782 6.2 111 5.5 98 1654 7.212 329:59 7904 7.2 569 4.9 386 7047 10.813 334:18 8007 2.3 186 4.4 354 7515 6.114 166:40 3986 2.4 96 2.9 116 3810 4.415 15:40 374 8.8 33 9.6 36 331 11.516 283:14 6768 11.3 768 12.4 841 5671 16.217 333:07 7974 13.2 1056 5.5 438 6891 13.618 329:14 7885 8.2 647 7.1 559 7155 9.319 130:48 2946 47.7 1405 48.4 1427 1484 49.620 148:00 3545 5.6 200 2.1 74 3280 7.521 50:50 1218 4.4 54 1.6 20 1157 5.022 332:45 7963 6.5 517 5.3 423 7414 6.923 40:34 1138 17.8 203 17.8 202 909 20.124 164:21 3935 1.4 54 1.1 42 3839 2.425 86:35 2156 12.4 267 10.7 230 1845 14.426 326:31 7820 3.0 232 1.0 82 7529 3.727 228:16 5299 11.2 595 7.9 421 4640 12.428 193:00 4631 17.6 813 4.9 225 3752 19.029 226:14 5416 2.8 149 2.4 130 5151 4.930 297:43 7167 11.1 792 8.0 573 5917 17.431 318:55 7634 13.6 1035 12.9 981 6509 14.732 313:09 7499 7.3 544 5.8 432 6826 9.033 30:02 718 1.9 14 4.6 33 672 6.434 124:28 2977 16.3 486 10.3 307 2468 17.135 285:05 6838 7.4 504 7.7 525 6132 10.3MEAN 195:52 4706 9.1 431.7 8.7 436.9 4079.3 12.5SD 117:23 2779 8.7 417.7 11.9 784.7 2487.8 11.9MEDIAN 193:00 4631 7.3 267 5.5 225 3810 9.3IQR (Q1-Q3) 2156-7634 2.9-11.6 2.9-8.4 1654-6639 6.1-14.4
218.e16 B. Bradley et al.
indicates a period of poor signal quality, whereas a high levelof R-to-R intervals (RRIs) or inter-breath intervals (IBIs)removed in the cleaning process and/or the detection of a-fibdoes not necessarily imply poor quality waveform data. ForRRIs, this implies non–sinus heart rhythm, which confoundssubsequent variability analysis.
For HRV, among all patients, only 1.3% (1.0%-2.1%,5.9%) of variability windows had greater than 0% discon-nection present; 0.6% (0.1%-3.9%, 39.5%) of windows wasremoved because of detection of a-fib, and 6.6% (1.4%-17.9%, 89.0%) of windows were removed because of datacleaning. Patients 2, 5, and 19 had long intermittent periodsof a-fib as noted by bedside nursing staff on their ICU charts
and later recorded on their CRFs; CIMVA detected 39.5%,28.8%, and 15.5% of their windows, respectively, to have a-fib–like characteristics. Other patients with shorter intermit-tent a-fib episodes were 13, 17, 18, 25, and 29. Patient 9 hada bigeminy heart rhythm, and the cleaning algorithm filteredout most of this patient's data (89%). A similar result is seenfor patient 24 who had atrial bigeminy, which was notlabeled as a-fib but largely filtered by data cleaning. Ingeneral, of the 7 patients with more than 25% of theirwindows removed, all experienced a-fib or some other formof irregular sinus rhythm.
For RRV data, among all patients, 7.2% (2.9%-11.6%,47.7%) of windows had more than 0% disconnection

218.e17Continuous multiorgan variability analysis in the ICU
present, and 5.5% (2.9%-8.4%, 56.4%) of windows wereremoved because of cleaning. Two patients (10 and 19) hadmore than 25% of their RRV windows removed. For patient10, the breath-detection algorithm failed for a largeproportion of this patient's etCO2 data. For patient 19,there appeared to be a prolonged period of disconnection.Upon further review, however, the patient had already beenextubated at this time (the monitor may have been left oncollecting false data). Nevertheless, leaving this periodidentified as a disconnection allowed it to be properlyfiltered out from any variability analysis.
3.5. Illustration of continuous HRV/RRVmonitoring—case example
Fig. 3 shows an arbitrarily selected example of a smoothed14-day trajectory of HRV and RRV as measured with SD (forpatient 16). This patient had 2.9% of their ECG waveformdata missing and 1.7% of their HRV windows removed afterCIMVAprocessing; 3.7% of their etCO2waveform data weremissing, and 16.2% of their RRV windows were removed.Sections with prolonged disconnection or missing data arelabeled. The interpretation of these results (in particular, thecorrelation with clinical events) is beyond the scope of thisarticle and the subject of future work; however, they areshown as an example of the variability traces that can begenerated with the output of our system.
Fig. 3 Example of a 14-day trajectory of HRV (A) and RRV (B)(arbitrarily selected). Variability plotted as a moving average (2-hour slidon RRV plot is shown.
4. Discussion
The main objective of this study was to explore thefeasibility of continuous multiorgan variability monitoring forcritically ill patients in an ICU setting. We have implementedand evaluated a system that can successfully acquire and storemultiorgan waveform data from individual patients in the ICUfor continuous durations of up to 2weeks. There is no technicalreason why this time could not be extended for longer ICUstays. Data harvested from the bedside are automaticallydeidentified and transmitted over the hospital network to aresearch file server and integrated into the CIMVA dataprocessing software. The CIMVA software successfullycomputed variability data, where possible, for all patients inthe cohort. Although demonstrated with a Philips Intellivuepatient monitoring system, database server, and network, thegeneral setup presented is applicable to other monitoringvendors as well (eg, GE iCollect for data capture from Datex-Ohmeda monitors (GE Medical Systems, Waukesha, Wiscon-sin), BedmasterEx, etc), and work is ongoing to interfaceCIMVA with additional systems. Arterial blood pressure andoxygen saturation (SpO2) waveforms were also collected usingthe given setup; processing these with the CIMVA software isthe subject of future work.
The data presented here are a promising indication thatlong-term continuous waveform monitoring and interpreta-tion in the ICU are feasible without risk of excessive data
(standard deviation of RRI and IBI, respectively) for patient 16ing window) of 5-minute variability windows. Point of extubation

218.e18 B. Bradley et al.
loss. The patients with the most missing data were enrolled ata time when routine maintenance on the clinical network(software upgrade) had to be performed. Although mainte-nance and updates are unavoidable, data loss can be easilymitigated if given enough notice. Regular communicationwith ICU information technology personnel regardingmaintenance activities, upgrades, and other, is crucial forsuccessful continuous variability monitoring. The earlyproblems we encountered with the etCO2 tubing wererectified for patients enrolled later in the study. We arecurrently investigating ways of computing RRV in theabsence of etCO2 data (eg, using available ECG waveformdata [eg, chest impedance] as a surrogate for etCO2
waveform and identifying IBI time series from ECG [29])to further reduce the impact of data loss. The breath-detectionalgorithm occasionally fails in individual patients (eg, patient10) presumably because of inappropriate thresholds in therespiratory rate detection algorithm. Thus, there are numerousimprovements to be made to ensure robust waveforminterpretation in a diverse critically ill patient population.
In general, the amount of missing or incalculable data isfelt to be acceptable given the challenges of collecting datain this environment; however, what degree of missing HRVand RRV data are “too much” for a single patient issubjective and arbitrary, largely related to the timing of themissing data in association with clinical events. A systemthat is able to report HRV and RRV along with theunderlying waveform and a measure of its quality is ourobjective. We envision that future studies will ultimatelydetermine the utility of monitoring HRV and/or RRVpatterns in relation to clinical events.
We plotted individual patient variability over time forseveral patients in the study but found it challenging toassociate variability with specific clinical events in individualpatients because of overlapping or confounding events suchas sedation, ventilator setting changes, and other. In contrast,our previous work demonstrated continuous HRV monitoringto be useful in a pilot study of ambulatory bone marrowtransplant patients; significant alterations in HRV wereobserved before the clinical diagnosis and treatment ofsepsis [25]. Variability was reported in 12-hour increments,which was frequent enough to report clinically relevantalterations. Variability plotted over time in this study(illustrated in Fig. 3 for 1 arbitrary patient) shows that trendsin variability are evident on an even finer timescale. Afocused analysis of continuous variability monitoring inassociation with level of organ failure as well as its onset andresolution will be reported separately.
Data processing time is highly dependent on theprocessor used and the actual software implementationdetails. For this study, data were processed using acommodity PC using Matlab. The CIMVA data processingtime was small (relative to the length of the acquiredwaveforms) and not considered a prohibiting factor to thefeasibility of continuous variability analysis. This proces-sing time could be further decreased through optimization
of the Matlab code and by running the software on a serverwith more computational power. Despite this, the 2-secondprocessing time required for each 5-minute window fallswell within the update rate that would eventually berequired for real-time outputs (in which new HRV andRRV values are computed every 2.5 minutes assuming50% overlap between consecutive windows) even afteraccounting for multiple ICU beds running concurrently. Infact, the major technical challenge in providing real-timevariability results at the bedside is finding suitable dataharvest methods that allow access to the waveform data in acontinuous manner (the Philips Intellivue system describedherein is appropriate for retrospective analysis only). Workis underway to acquire real-time data from the clinicalnetwork using the BedmasterEx product (which allowsintegration with both Philips and GE products) and fromambulatory monitoring devices.
In the present work, we adopted a conservative approachin which any proportion of disconnection within a 5-minutewindow caused the rejection of that window from analysis.Further work is being done to assess how short disconnec-tions affect variability computations and how best to handledisconnection when it occurs. The amount of variability datalost because of disconnection was minimal in the HRV case.For RRV, disconnection percentages were higher than theywere for HRV but are still below 10%. This is likely becauseof very long breaths and/or apnea being detected asdisconnections. As the CIMVA software evolves, improvedhandling of artifacts (such as disconnection) will likelyreduce the proportion of data loss.
There was general agreement between those patients withreported a-fib on the CRF and a-fib detected by the CIMVAsoftware (data not shown). The manner in which a-fib dataare currently reported clinically (ie, only if/when a nursehappens to notice it, with onset/resolution times not alwaysnoted accurately) prevented us from performing a quantita-tive assessment of the accuracy of the a-fib detector. A moredetailed study using alarm data provided by the Philipsmonitor via the advanced arrhythmia option is planned.The data reported here do, however, provide insight intothe prevalence of a-fib in this critically ill population andthe degree to which data are potentially lost or unusable forvariability analysis of these patients.
There have been a few systems developed that arecapable of recording physiologic signals for researchpurposes [2,4-8]. Many of these use portable dataacquisition systems requiring local connections in theICU room close to the bedside and have had to overcomechallenges with communication interface protocols toaccess data through external ports on the monitors. Onekey advantage of the arrangement described in this article isthat there is no need for a portable bedside computer foreach patient (because the data export is requested at thecentral station), nor is there a need for additional hardwareat the bedside. The number of patients who can becontinuously monitored at any given time is limited only by

218.e19Continuous multiorgan variability analysis in the ICU
the number of etCO2 modules available. Last, the need forthe nursing staff to interact with the data collectionequipment is eliminated because the data downloading isperformed by a research coordinator at the PIIC station(although nursing or respiratory therapy staff could easilybe trained to do the download).
There are limitations to our system. First, manualcapture of clinical data and specific events or interventionson a paper CRF and subsequent translation to an electronicdatabase is a time-consuming, tedious, and error-proneprocess. The system presented by Vinecore et al [2] allowsfor synchronous recording of physiologic data and clinicalevents at the bedside. Having clinical and event dataentered electronically would facilitate subsequent variabil-ity analysis and correlation of variability with major eventsor interventions. Second, although CIMVA currentlyinterfaces with the Philips Intellivue patient monitoringsystem, in the future, it will also integrate with other vendorsystems (eg, GE, Capsule DataCaptor (Capsule Technolo-gies, Andover, Massachusetts), and BedmasterEx). For thePhilips Intellivue system, the sampling frequency of theECG waveform data at the patient monitor is 500 Hz.Unfortunately, the software feature that allowed us toconveniently perform remote downloads (Export Data toHolter) produced waveform data at a lower fidelity, 125Hz. However, this method also records beat annotationsbased on the native resolution (500 Hz), so the interbeatintervals used in our system have a precision of 2milliseconds, which is suitable for HRV analysis. The125-Hz sampling frequency is sufficient for RRV proces-sing based on the etCO2 waveform.
The prospect of continuous multiorgan variability analysisin the ICU has widespread clinical and scientific significance,with potential to directly impact patient care, assistcomplexity science research in critical care and researchand development in monitoring technology. We have shownthat, from a technical perspective, continuously monitoringphysiologic signals and evaluating variability in an ICUsetting are feasible. Although variability measures werecomputed retrospectively for this observational study (ie,after the patients' ICU stay), the goal of CIMVA is to useHRV and RRV to improve prognostication (ability to detectseverity of illness and organ dysfunction in the present) andprediction (ability to predict clinical improvement ordeterioration in the future) in critically ill patients. Futureresearch will be focused on the direct evaluation of CIMVAto improve prognostication and prediction in the ICU. Theclinical significance of improved prognostication andprediction of clinical outcome is extensive and widespread.Potential applications include earlier diagnosis and interven-tion (ie, earlier detection and prediction of clinical deterio-ration), tailoring site of care (ie, outpatient vs ward vs ICUbed) to severity of illness, and the potential for directing carebased on real-time evaluation of prognosis.
Supplementary materials related to this article can befound online at doi:10.1016/j.jcrc.2011.09.009.
Acknowledgments
The authors acknowledge Philips Healthcare, who installedthe Holter Data Export feature as a courtesy to our researchgroup for research purposes. The authors gratefully acknowl-edge the support of the Ottawa Hospital Research Institute andthe Canadian Institutes of Health Research for this researchprogram. The study sponsors had no role in the design of thestudy or in the writing of this manuscript.
References
[1] Schenkman KA. Clinical data collection in the information era. PediatrCrit Care Med 2007;8:588-9.
[2] Vinecore K, et al. Design and implementation of a portablephysiologic data acquisition system. Pediatr Crit Care Med 2007;8:563-9.
[3] Lapinsky SE, Holt D, Hallett D, et al. Survey of informationtechnology in intensive care units in Ontario, Canada. BMC MedInform Decis Mak 2008;8:5.
[4] Siachalou EJ, Kitas IK, Panoulas KJ, et al. ICASP: an intensive-careacquisition and signal processing integrated framework. J Med Syst2005;29:633-46.
[5] Kropyvnytskyy I, Saunders F, Schierek P, et al. A computer system forcontinuous long-term recording, processing, and analysis of physio-logical data of brain injured patients in ICU settings. Brain Inj 2001;15:577-83.
[6] Saeed M, Lieu C, Raber G, et al. MIMIC II: a massive temporal ICUpatient database to support research in intelligent patient monitoring.Comput Cardiol 2002;29:64-644.
[7] Metnitz PGH, Laback P, Popow C, et al. Computer assisted dataanalysis in intensive care: the ICDEV project-development of ascientific database system for intensive care. Intl J Clin Monit Comput1995;12:147-59.
[8] Goldstein B, McNames J, McDonald BA, et al. Physiologic dataacquisition system and database for the study of disease dynamics inthe intensive care unit. Crit Care Med 2003;31:433-41.
[9] Norris PR, Dawant BM, Geissbuhler A. Web-based data integrationand annotation in the intensive care unit. Proc AMIA Annu Fall Symp1997:794-8.
[10] Seely AJ, Christou NV. Multiple organ dysfunction syndrome:exploring the paradigm of complex nonlinear systems. Crit CareMed 2000;28:2193-200.
[11] Seely AJ, Macklem PT. Complex systems and the technology ofvariability analysis. Crit Care 2004;8:R367-84.
[12] Buchman TG, Stein PK, Goldstein B. Heart rate variability in criticalillness and critical care. Curr Opin Crit Care 2002;8:311-5.
[13] Korach M, et al. Cardiac variability in critically ill adults: influence ofsepsis. Crit Care Med 2001;29:1380-5.
[14] Piepoli M, Garrard CS, Kontoyannis DA, Bernardi L. Autonomiccontrol of the heart and peripheral vessels in human septic shock.Intensive Care Med 1995;21:112-9.
[15] Annane D, et al. Inappropriate sympathetic activation at onset of septicshock: a spectral analysis approach. Am J Respir Crit Care Med1999;160:458-65.
[16] Pontet J, Contreras P, Curbelo A, et al. Heart rate variability as earlymarker of multiple organ dysfunction syndrome in septic patients.J Crit Care 2003;18:156-63.
[17] Chen WL, Chen JH, Huang CC, et al. Heart rate variability measuresas predictors of in-hospital mortality in ED patients with sepsis. Am JEmerg Med 2008;26:395-401.
[18] Papaioannou VE, Chouvarda I, Maglaveras N, Dragoumanis C,Pneumatikos I. Changes of heart and respiratory rate dynamics during

218.e20 B. Bradley et al.
weaning from mechanical ventilation: a study of physiologic complexityin surgical critically ill patients. J Crit Care 2011;26:262-72.
[19] Bien MY, Hseu SS, Yien HW, et al. Breathing pattern variability: aweaning predictor in postoperative patients recovering from systemicinflammatory response syndrome. Intensive Care Med 2004;30:241-7.
[20] El-Khatib M, Jamaleddine G, Soubra R, et al. Pattern of spontaneousbreathing: potential marker for weaning outcome. Intensive Care Med2001;27:52-8.
[21] Engoren M. Approximate entropy of respiratory rate and tidal volumeduring weaning from mechanical ventilation. Crit Care Med 1998;26:1817-23.
[22] Wysocki M, Cracco C, Teixeira A. Reduced breathing variability as apredictor of unsuccessful patient separation from mechanical ventila-tion. Crit Care Med 2006;34:2076-83.
[23] White CE, Batchinsky AI, Necsoiu C, et al. Lower interbreath intervalcomplexity is associatedwith extubation failure inmechanically ventilatedpatients during spontaneous breathing trials. J Trauma 2010;68:1310-6.
[24] Goldberger AL, Amaral LA, Glass L, et al. PhysioBank, Physio-Toolkit, and PhysioNet: Components of a new research resource forcomplex physiologic signals. Circulation 2000;101:e215-20.
[25] Ahmad S, Ramsay T, Huebsch L, et al. Continuous multi-parameterheart rate variability analysis heralds onset of sepsis in adults. PLoSONE 2009;4:e6642.
[26] Zhang Q, Manriquez A, Medigue C, Papelier Y, Sorine M. Robust andefficient location of T-wave ends in electrocardiogram. ComputCardiol 2005;32:711-4.
[27] ChenW, et al. Unconstrained detection of respiration rhythm and pulserate with one under-pillow sensor during sleep. Med Biol Eng Comput2005;43:306-12.
[28] Logan B, Healey J. Robust detection of atrial fibrillation for a longterm telemonitoring system. 32:(2005);619-22.
[29] Cysarz D, Zerm R, Bettermann H, et al. Comparison of respiratoryrates derived from heart rate variability, ECG amplitude, and nasal/oralairflow. Ann Biomed Eng 2008;36:2085-94.