Factors that may cause Bleeding with Enoxaparin Factors that may cause Bleeding with Enoxaparin...
41
Factors that may cause Bleeding with Enoxaparin Ohoud Alarfaj MS Candidate Supervised by : Dr. Hisham S. Abou-Auda Dr. Mohammad H. Daba Dr. Ahmad Al-Barraq
-
date post
20-Dec-2015 -
Category
Documents
-
view
220 -
download
3
Transcript of Factors that may cause Bleeding with Enoxaparin Factors that may cause Bleeding with Enoxaparin...

Factors that may causeBleeding with EnoxaparinFactors that may cause
Bleeding with Enoxaparin
Ohoud AlarfajOhoud AlarfajMS CandidateMS Candidate
Supervised by:Supervised by:
Dr. Hisham S. Abou-AudaDr. Hisham S. Abou-Auda
Dr. Mohammad H. DabaDr. Mohammad H. Daba
Dr. Ahmad Al-BarraqDr. Ahmad Al-Barraq

IntroductionObjectiveMethodologyResultsConclusion
IntroductionObjectiveMethodologyResultsConclusion

Enoxaparin is in a class of medications called low molecular weight heparins (LMWH).
Enoxaparin is in a class of medications called low molecular weight heparins (LMWH).
LMWH is a class of medication used as an anticoagulant in diseases that cause thrombosis, as well as prophylaxis in situations that lead to a high risk of thrombosis.
LMWH is a class of medication used as an anticoagulant in diseases that cause thrombosis, as well as prophylaxis in situations that lead to a high risk of thrombosis.

LMWH is the product of enzymatic or chemical degradation of unfractionated heparin (UFH).
LMWH is the product of enzymatic or chemical degradation of unfractionated heparin (UFH).
LMWH results from studies in late 1970s to developing other safer form from heparin.
LMWH results from studies in late 1970s to developing other safer form from heparin.
In 1982 Kakkar et al was the first one who evaluates LMWH in humansIn 1982 Kakkar et al was the first one who evaluates LMWH in humans
Enoxaparin used to prevent blood clots.Enoxaparin used to prevent blood clots.
Used for several days after hip or knee replacement surgery , and in some cases following abdominal surgery, while you are unable to walk.
Used for several days after hip or knee replacement surgery , and in some cases following abdominal surgery, while you are unable to walk.
Also used if you are unable to get out of bed because of a serious illness.
Also used if you are unable to get out of bed because of a serious illness.
In addition, enoxaparin is used to prevent blood clots from forming in the arteries of the heart during certain types of chest pain and heart attacks.
In addition, enoxaparin is used to prevent blood clots from forming in the arteries of the heart during certain types of chest pain and heart attacks.
May be used for other conditions as determined by physician.May be used for other conditions as determined by physician.

Most of the available data comes from pharmacokinetic or population pharmacodynamic studies or clinical reports. Results in patients with renal impairment suggest that a reduction in calculated creatinine clearance levels is associated with an increased risk of accumulation of anti-Xa activity.
Most of the available data comes from pharmacokinetic or population pharmacodynamic studies or clinical reports. Results in patients with renal impairment suggest that a reduction in calculated creatinine clearance levels is associated with an increased risk of accumulation of anti-Xa activity.

The initial dose of enoxaparin: 1.5 mg/kg once daily or 1 mg/kg twice daily.
The initial dose of enoxaparin: 1.5 mg/kg once daily or 1 mg/kg twice daily.
Participants on dialysis were given 75% of the other subjects’ recommended initial dosage, i.e., 1.125 mg/kg once daily or 0.75 mg/kg twice daily.
Participants on dialysis were given 75% of the other subjects’ recommended initial dosage, i.e., 1.125 mg/kg once daily or 0.75 mg/kg twice daily.
DosageDosage

Due to the hydrophilic disposition of enoxaparin, accumulation is likely in patients with renal dysfunction, thereby increasing the risk of hemorrhagic complications if standard weight adjusted treatment doses are used.
Due to the hydrophilic disposition of enoxaparin, accumulation is likely in patients with renal dysfunction, thereby increasing the risk of hemorrhagic complications if standard weight adjusted treatment doses are used.
Enoxaparin treatment doses are calculated in terms of actual patient weight, but, because the drug is not distributed in fat, there is a possibility of excessive drug exposure in obese patients.
Enoxaparin treatment doses are calculated in terms of actual patient weight, but, because the drug is not distributed in fat, there is a possibility of excessive drug exposure in obese patients.

LMWHs have many adverse effects and the main one is bleedingLMWHs have many adverse effects and the main one is bleeding
Significant bleeding requires medical evaluation or is associated with at least a 3% reduction in hematocrit, or more than 12 g/L (1.2 g/dL) reduction in the hemoglobin level.
Significant bleeding requires medical evaluation or is associated with at least a 3% reduction in hematocrit, or more than 12 g/L (1.2 g/dL) reduction in the hemoglobin level.

Factors may affect bleeding riskFactors may affect bleeding risk
Concomitant drugs:warfarin, nonsteroidal anti-inflammatory, aspirin, ibuprofen, diclofenac, indomethacin, dipyredamole, digoxin, or clopidogrel.
Concomitant drugs:warfarin, nonsteroidal anti-inflammatory, aspirin, ibuprofen, diclofenac, indomethacin, dipyredamole, digoxin, or clopidogrel.
Concomitant disease:a history of gastrointestinal bleeding, Hypertension, diabetes mellitus, heart failure, pregnancy, anemia, SLE and kidney disease.
Concomitant disease:a history of gastrointestinal bleeding, Hypertension, diabetes mellitus, heart failure, pregnancy, anemia, SLE and kidney disease.
Other factors:Age.Obesity.
Other factors:Age.Obesity.

To determine the factors that may affect LMWH such as (age, weight, renal function, disease, drugs, etc.).
To determine the factors that may affect LMWH such as (age, weight, renal function, disease, drugs, etc.).
To check if there is any correlation between occurrence of bleeding and these factors among patients receiving LMWH.
To check if there is any correlation between occurrence of bleeding and these factors among patients receiving LMWH.

A retrospective trial, conducted in King Khalid University Hospital (KKUH).
A retrospective trial, conducted in King Khalid University Hospital (KKUH).
Study design:Study design:
The demographic data of patients: (age, sex, weight, height, BMI, Srcr). The demographic data of patients: (age, sex, weight, height, BMI, Srcr).
A special data collection form was used.A special data collection form was used.
Other concomitant drugs prescribed to the patient and concomitant diseases were also recorded.
Other concomitant drugs prescribed to the patient and concomitant diseases were also recorded.

Data Collection FormData Collection Form

Variables were coded individually, and data were analyzed using (SPSS) ver. 13.0 for Windows.
Variables were coded individually, and data were analyzed using (SPSS) ver. 13.0 for Windows.
Frequencies, Condescriptives, Parametric tests, Nonparametric testsFrequencies, Condescriptives, Parametric tests, Nonparametric tests
Logistic regression, Odds RatioLogistic regression, Odds Ratio
FemalesFemales
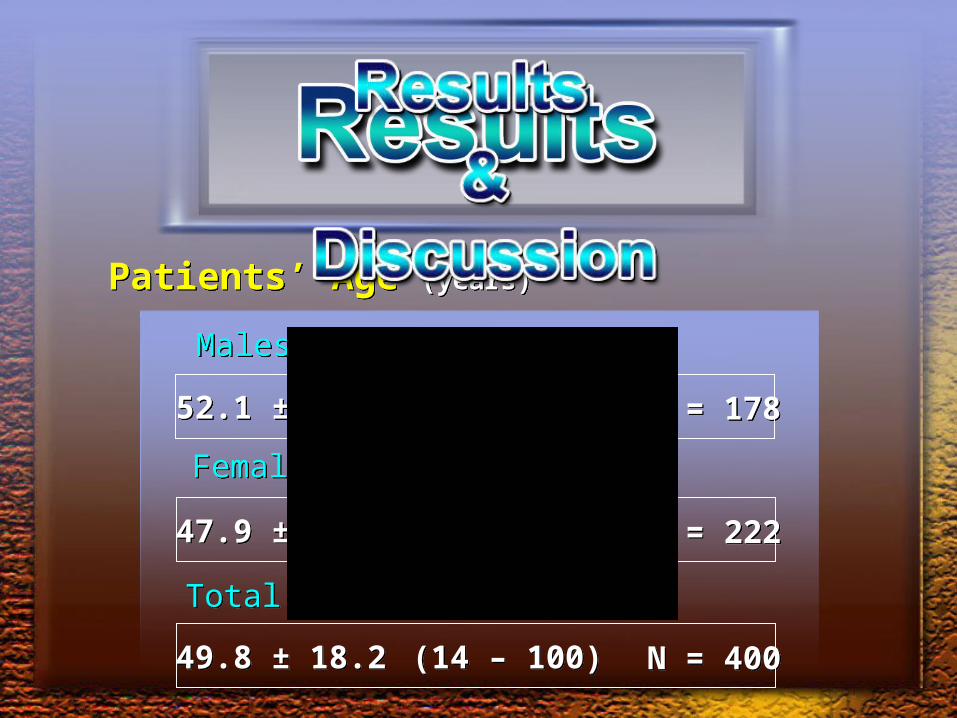
Patients’ Age (years)Patients’ Age (years)
52.1 ± 19.952.1 ± 19.9 (14 – 95)(14 – 95) N = 178N = 178
MalesMales
47.9 ± 16.647.9 ± 16.6 (14 – 100)(14 – 100) N = 222N = 222
TotalTotal
49.8 ± 18.249.8 ± 18.2 (14 – 100)(14 – 100) N = 400N = 400

WeightWeight
FemalesFemales
80.2 ± 22.180.2 ± 22.1 (27.8 – 151)(27.8 – 151) N = 178N = 178
MalesMales
75.2 ± 19.175.2 ± 19.1 (38 – 186)(38 – 186)N = 222N = 222
TotalTotal77.4 ± 20.677.4 ± 20.6 (27.8 – 186)(27.8 – 186)
N = 400N = 400
(kg)
165.7 ± 9.0165.7 ± 9.0 (138 – 189)(138 – 189)HeightHeight(cm)
154.4 ± 6.4154.4 ± 6.4 (137 – 180)(137 – 180)
159.4 ± 9.5159.4 ± 9.5 (137 – 189)(137 – 189)

Dose 1Dose 1
Frequency 1Frequency 1
Dose 2Dose 2
n= 178
60.4 ± 25
(40-156)
n= 178
60.4 ± 25
(40-156)
(12-24) hr(12-24) hr
n= 3
60 ± 20
(40- 80)
n= 3
60 ± 20
(40- 80)
n= 222
56.5 ± 20.5
(30-120)
n= 222
56.5 ± 20.5
(30-120)
(12-24) hr(12-24) hr
n= 20
38 ± 11.05
(20- 60)
n= 20
38 ± 11.05
(20- 60)
MalesMales FemalesFemales
DOSES & FREQUENCY
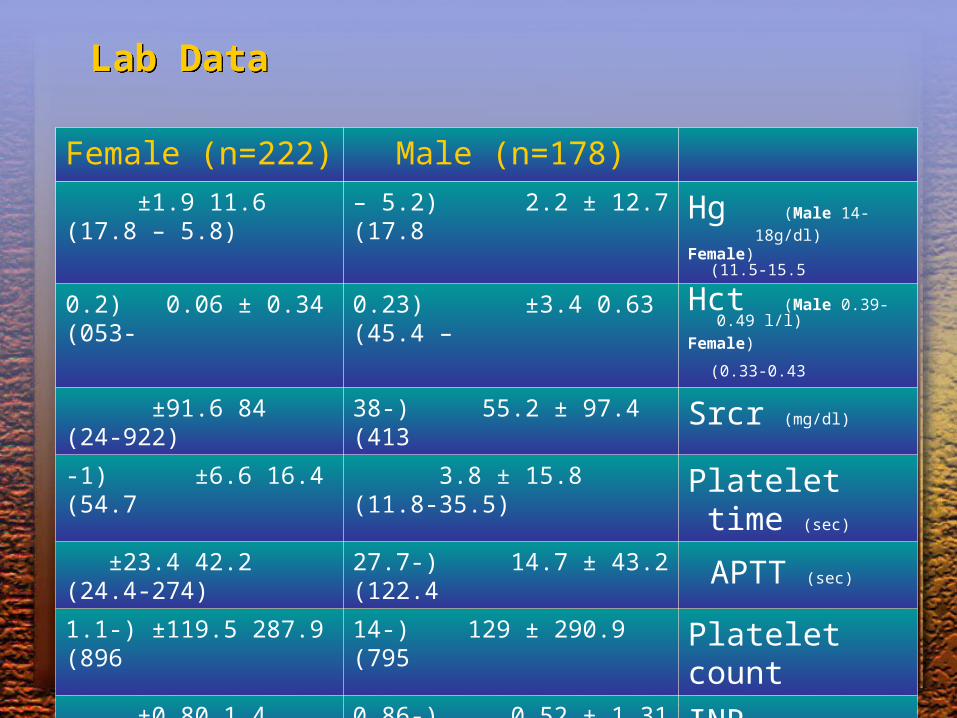
Lab DataLab Data
Male (n=178)Female (n=222)
Hg (Male 14-18g/dl)
) Female 11.5-15.5( 12.7 ± 2.2) 5.2 – 17.8(11.6 ±1.9) 5.8 – 17.8(
Hct (Male 0.39-0.49 l/l)
) Female 0.33-0.43( 0.63 ±3.4) 0.23 – 45.4(0.34 ± 0.06) 0.2- 053(
Srcr (mg/dl)97.4 ± 55.2) 38-413(84 ±91.6) 24-922(
Platelet time (sec) 15.8 ± 3.8) 11.8-35.5(16.4 ±6.6) 1 -54.7(
APTT (sec) 43.2 ± 14.7) 27.7-122.4(42.2 ±23.4) 24.4-274(
Platelet count290.9 ± 129) 14-795(287.9 ±119.5) 1.1-896(
INR1.31 ± 0.52) 0.86-4.10(1.4 ±0.80) 0.84-6.26(
CLcr (ml/min)91.75 ± 50.2) 12.6-293.9(117.6 ±58.8) 6-324.5(

ObeseObese
49 %49 %
OverweightOverweight 27 %27 %
UnderweightUnderweight
2 %2 %NormalNormal
22 %22 %

UnderweightUnderweight
NormalNormal
OverweightOverweight
Obesity (Class I)Obesity (Class I)
Obesity (Class II)Obesity (Class II)
Extreme ObesityExtreme Obesity
5 (2.8 %)5 (2.8 %)
46 (25.8 %)46 (25.8 %)
59 (33.1 %)59 (33.1 %)
40 (22.5 %)40 (22.5 %)
16 (9.0 %)16 (9.0 %)
12 (6.7 %)12 (6.7 %)
3 (1.4 %)3 (1.4 %)
42 (18.9 %)42 (18.9 %)
49 (22.1 %)49 (22.1 %)
60 (27.0 %)60 (27.0 %)
46 (20.7 %)46 (20.7 %)
22 (9.9 %)22 (9.9 %)
MalesMales FemalesFemales


* Sickle Cell, Autoimmune hemolytic, Iron Deficiency
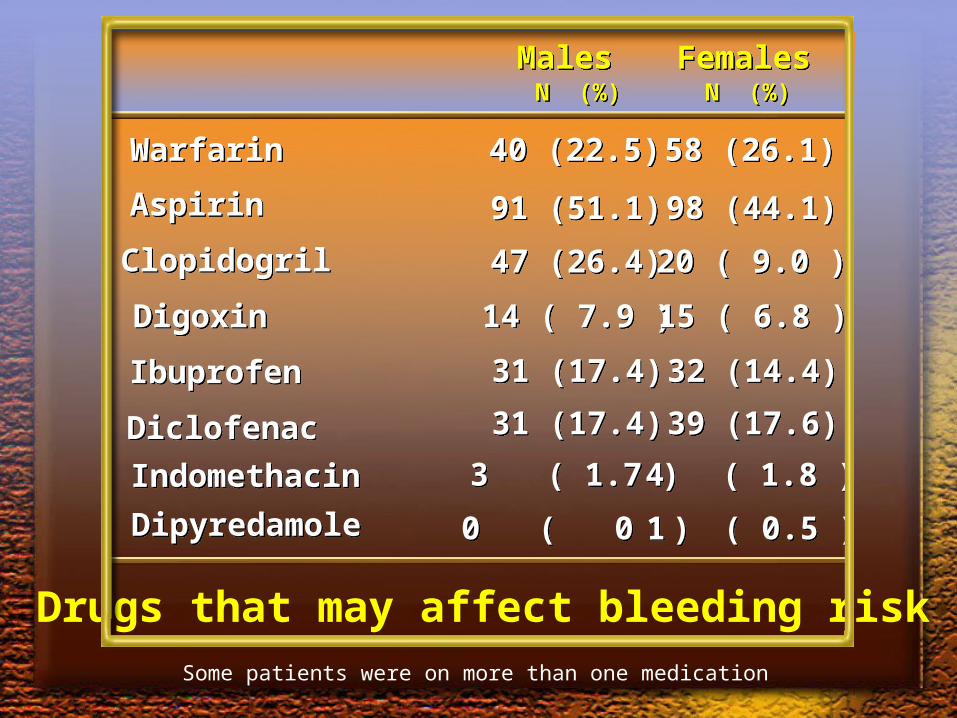
WarfarinWarfarin
AspirinAspirin
ClopidogrilClopidogril
DigoxinDigoxin
IbuprofenIbuprofen
DiclofenacDiclofenac
IndomethacinIndomethacin
DipyredamoleDipyredamole
40 (22.5)40 (22.5) 58 (26.1)58 (26.1)
91 (51.1)91 (51.1) 98 (44.1)98 (44.1)
47 (26.4)47 (26.4) 20 ( 9.0 )20 ( 9.0 )
14 ( 7.9 )14 ( 7.9 ) 15 ( 6.8 )15 ( 6.8 )
31 (17.4)31 (17.4) 32 (14.4)32 (14.4)
31 (17.4)31 (17.4) 39 (17.6)39 (17.6)
3 ( 1.7 )3 ( 1.7 ) 4 ( 1.8 )4 ( 1.8 )
0 ( 0 )0 ( 0 ) 1 ( 0.5 )1 ( 0.5 )
MalesMales FemalesFemalesN (%)N (%) N (%)N (%)
Drugs that may affect bleeding riskSome patients were on more than one medication

23.5 %23.5 %
BLEEDINGBLEEDINGVaginalVaginal
94 Patients94 Patients
GI bleedingGI bleeding
HematuriaHematuria
Gum bleedingGum bleeding
EpistaxisEpistaxis
HematomaHematoma
HemoptysisHemoptysis
MelenaMelena
33
1616
44
44
11
11
44
11
UnspecifiedUnspecified 6464
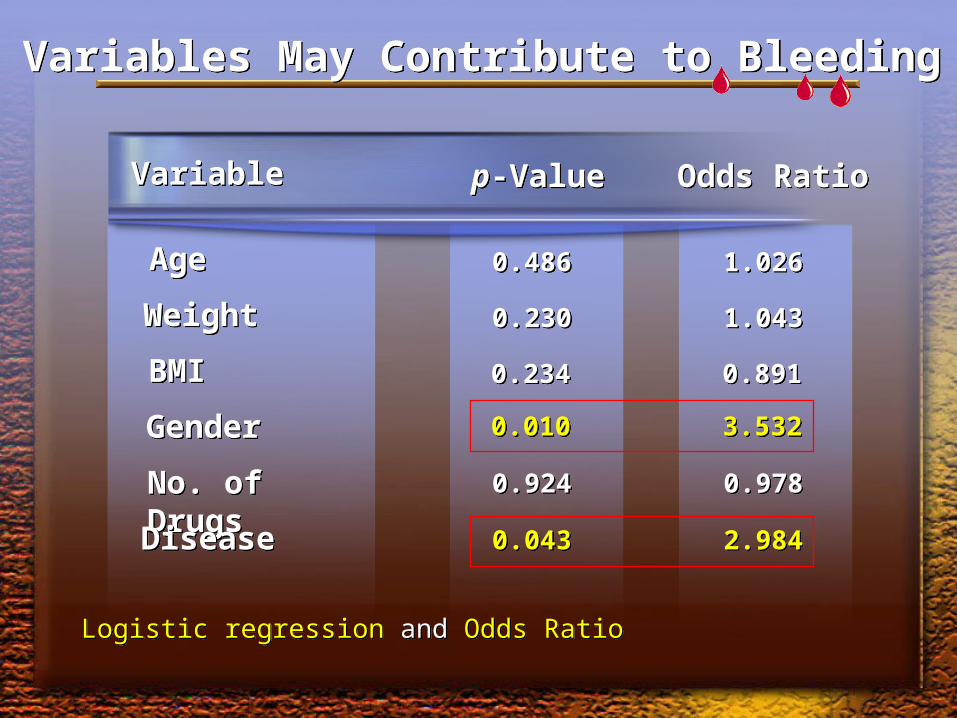
AgeAge
WeightWeight
BMIBMI
GenderGender
No. of DrugsNo. of Drugs
DiseaseDisease
Logistic regression and Odds RatioLogistic regression and Odds Ratio
0.4860.486 1.0261.026
0.2300.230 1.0431.043
0.2340.234 0.8910.891
0.0100.010 3.5323.532
0.9240.924 0.9780.978
0.0430.043 2.9842.984
VariableVariable p-Valuep-Value Odds RatioOdds Ratio
Variables May Contribute to BleedingVariables May Contribute to Bleeding

VariableVariable p-Valuep-Value Odds RatioOdds Ratio
ObesityObesity
CLcrCLcr
Renal FunctionRenal Function
Total DoseTotal Dose
Age GroupAge Group
Old AgeOld Age
0.5000.500 1.7711.771
0.4960.496 1.0551.055
0.7220.722 0.7110.711
0.3110.311 1.0001.000
0.0120.012 2.6522.652
0.0860.086 1.5731.573
Variables May Contribute to BleedingVariables May Contribute to Bleeding
Logistic regression and Odds RatioLogistic regression and Odds Ratio

Males Females
Renal FunctionRenal Function
Normal Moderate Impairment Renal Failure
52.2%
7.2%
41%
6.7%
18.5%
74.3%

Statistically significant (X2 test=7.329) p=0.0256Statistically significant (X2 test=7.329) p=0.0256
Bleeding & Renal FunctionBleeding & Renal Function
Normal Moderate Failure258 114 28
20.5 % 25.4 % 42.9 %

AspirinAspirin 44 (46.8 %)44 (46.8 %)
WarfarinWarfarin 23 (24.5 %)23 (24.5 %)
ClopidogrilClopidogril 13 (13.8 %)13 (13.8 %)
DigoxinDigoxin 5 (5.3 %)5 (5.3 %)
IbuprofenIbuprofen 14 (14.9 %)14 (14.9 %)
DiclofenacDiclofenac 19 (20.2 %)19 (20.2 %)
Bleeding & DrugsBleeding & Drugs

Number of Concomitant Drugs & BleedingNumber of Concomitant Drugs & Bleeding
00 25 (26.6 %)25 (26.6 %)
11 34 (22.8 %)34 (22.8 %)
44 3 (42.9 %)3 (42.9 %)
5 - 65 - 6 0 (0 %)0 (0 %)
33 8 (20.0 %)8 (20.0 %)
22 24 (22.2 %)24 (22.2 %)
9494
149149
108108
4040
77
22
NumberNumber Bleeding [N (%)]Bleeding [N (%)]PatientsPatients
TotalTotal 94 (100%)94 (100%)400400

Bleeding and Co-morbiditiesBleeding and Co-morbidities
HTNHTN
DMDM
Heart FailureHeart Failure
PregnancyPregnancy
Renal FailureRenal Failure
AnemiaAnemia
IHDIHD
CADCAD
SLESLE
39 (41.5 %)39 (41.5 %)
40 (42.6 %)40 (42.6 %)
5 ( 5.3 % )5 ( 5.3 % )
19 (20.2 %)19 (20.2 %)
9 (20.2 %)9 (20.2 %)
3 ( 3.3 % )3 ( 3.3 % )
19 (20.2 %)19 (20.2 %)
2 ( 2.1 % )2 ( 2.1 % )
4 ( 4.3 % )4 ( 4.3 % )
DiseaseDisease Bleeding [ N (%) ]Bleeding [ N (%) ] OR (95% CI)OR (95% CI)
0.98 (0.61 – 1.56)0.98 (0.61 – 1.56)
1.42 (0.88 – 2.27)1.42 (0.88 – 2.27)
0.80 (0.29 – 2.20)0.80 (0.29 – 2.20)
2.62 (1.38 – 4.96)2.62 (1.38 – 4.96)
1.69 (0.73 – 3.91)1.69 (0.73 – 3.91)
1.11 (0.62 – 1.98)1.11 (0.62 – 1.98)
0.81 (0.17 – 3.88)0.81 (0.17 – 3.88)
1.90 (0.54 – 6.63)1.90 (0.54 – 6.63)
1.09 (0.11 – 10.57)1.09 (0.11 – 10.57)

Number Patients Bleeding [N (%)]
Number of Concomitant Disease & Bleeding
0 132 23) 17.4%(
1 102 29) 28.4%(
2 89 21) 23.6%(
3 61 15) 24.6%(
4 15 6 )40.0%(
Total 399 94

Bleeding and Lab Parameters
Hg (g/dL)Hg (g/dL) 12.55 ± 2.0512.55 ± 2.05 10.84 ± 2.0510.84 ± 2.05 13.6 %13.6 %
No BleedingNo Bleeding BleedingBleeding %▲%▲ Sig***Sig***
p<0.0001 (S)p<0.0001 (S)
HctHct 0.37 ± 0.060.37 ± 0.06 0.32 ± 0.050.32 ± 0.05 13.5 %13.5 % p<0.0001 (S)p<0.0001 (S)
Platelet Time(sec)Platelet Time(sec)
16.1 ± 5.916.1 ± 5.9 16.2 ± 4.316.2 ± 4.3 0.6 %0.6 % P=0.892 (NS)P=0.892 (NS)
Platelet CountPlatelet Count 294.7 ± 124.1294.7 ± 124.1 271.2 ± 121.6 271.2 ± 121.6 8.0 %8.0 % p=0.1076 (NS)p=0.1076 (NS)
APTT (sec)APTT (sec) 42.5 ± 21.142.5 ± 21.1 43.0 ± 15.943.0 ± 15.9 1.18 %1.18 % P=0.892 (NS)P=0.892 (NS)
)N = 306( )N = 94(

INRINR 1.37 ± 0.741.37 ± 0.74 1.35 ± 0.511.35 ± 0.51 1.5 %1.5 % p=0.822 (NS)p=0.822 (NS)
SCrSCr 84.5 ± 52.184.5 ± 52.1 108.1 ± 129. 5108.1 ± 129. 5 27.9 %27.9 % p=0.0104 (S)p=0.0104 (S)
CLCr**
(ml/min)CLCr**
(ml/min) 107.0 ± 54.7107.0 ± 54.7 103.2 ± 62.5103.2 ± 62.5 3.55 %3.55 % p=0.5677 (NS)p=0.5677 (NS)
No BleedingNo Bleeding BleedingBleeding %▲%▲ Sig***Sig***
Bleeding and Lab Parameters
*** T-Test or Wilcoxon Rank Sum Test
** Calculated by Cockroft & Gault equation
*** Normality or NonNormality was ascertained by Shapiro Wilks Test

1) Bazinet et al.
Thrombosis Research
2005
Discussion
Study Authors Year Conclusion
No dose adjustments are required in obese patients .
but in renally impaired patients adjustments may be necessary.
2 (Green et al. J Clin Pharmacol
2003 Dose adjustments of enoxaparin are required in obese patients to
reduce risk of bleeding .
3 (Ellis et al. Thrombosis/Hemostasis
2006 They suggest that in patients with high risk of bleeding such as old age, obese, renal failure, special care should be taken when LMWH is used. And monitoring should be considered.

Is laboratory monitoring of LMWH necessary?
Bounameaux et al.(2004) NO
Harenberg et al.(2004) YES
But i think from my results that the monitoring is important in high risk patients such as (old age- obese- renal failure).
• Because if patients have risks for bleeding this may lead to
increase bleeding when use LMWH.
Discussion