Gastrointestinal bleeding definitions (I) -...
16
2010.10.14. 1 Gastrointestinal bleeding definitions (I) • Acute bleeding : vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often before proceeding to diagnosis • Chronic bleeding : repeated episodes of presence of occult blood in stool Gastrointestinal bleeding definitions (II) • Hematemesis : - fresh, red vomitus, containing hemoglobin (above lig. Treitz) suggesting acute bleeding - brown, containing digested blood (previous bleeding) • Melena : (min. 100 ml) digested blood in faeces • Hematochesia: fresh blood in the stool
Transcript of Gastrointestinal bleeding definitions (I) -...
2010.10.14.
1
Gastrointestinal bleedingdefinitions (I)
• Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often before proceeding to diagnosis
• Chronic bleeding: repeated episodes of presence of occult blood in stool
Gastrointestinal bleedingdefinitions (II)
• Hematemesis: - fresh, red vomitus, containing hemoglobin (above lig. Treitz) suggesting acute bleeding - brown, containing digested blood (previous bleeding)
• Melena: (min. 100 ml) digested blood in faeces
• Hematochesia:fresh blood in the stool
2010.10.14.
2
Gastrointestinal bleedingdefinitions (III)
• ESTIMATED CONSEQUENCES OF ACUTE BLOOD VOLUME LOST10% (500 ml) occasional vasovagal syncope 20% (1000 ml) exercise-induced tachycardia 30% (1500 ml) postural hypotension, pulse 40% (2000 ml) resting supine hypotension
and severe tachycardia 50% (2500 ml) severe shock and death
Main pathogenetic causes of gastrointestinal bleedings
I. Damage (disruption) of the continuity of vessel wall:
- ulcer bleeding, tumorous erosion, trauma
II. Alteration of circulation:
- portal hypertension, thrombosis etc.
III. Changes of haemostasis:
- thrombocytopenia - pathia, inferited of acquired factor deficiency
2010.10.14.
3
Gastrointestinal bleedingsymptoms
• MILD BLEEDING: ortostatic changes of pulse and RR
• CONTINUOUS BLEEDING: weakness, fatigue, dizziness, pallor, thrist, air hunger, cold extremities, diminished urinary output
• SEVERE BLOOD LOSS: signs of perturbed organ perfusion, hepatic encephalopathy, altered mental status, hepatorenal/ or renal insufficiency, metabolic acidosis, ischemic heart attack
Gastrointestinal bleedingmanagement of diagnosis (I)
• HISTORY- previous GI bleeding episodes, abdominal
surgery, known bleeding tendency, hematologic disorders, known severe liver, kidney or heart diseases
- current medication - aspirin, NSAIDs coumarol, habits of alcohol consumption
- onset, duration of present complains - form os bleeding, characteristics of stool
2010.10.14.
4
Gastrointestinal bleedingmanagement of diagnosis (II)
• Physical examination:pulse and RR in both supine and upright position, signs of hypovolemia, anemia and coagulopathy, abdominal status, ascites, bowel sounds, tongue, rectal digital examination etc.
• Initial laboratory studies: Hb, htc, WBC, platelet count, PT (INR), PTT, serum BUN and creatinine, liver function
Gastrointestinal bleedingmanagement of diagnosis (III)
• Stabilization of the patient´s condition:monitoring of ECG, RR, oxygen saturation, volume replacement (~300 ml/h saline), nasal oxygen, if necessary blood transfusion, FFP
• Insertion of nasogastric tube: (?)
• Endoscopy:emergency (<2 h) - urgent (within 12 h) - routine (next day) - diagnostic; therapeutic
• Angiography, Radionuclid scintigraphy (Tc99)
2010.10.14.
5
Gastrointestinal bleedingmain sources (I)
• OESOPHAGUS (~ 1/3 of all GI bleeding cases) variceal bleeding (portal hypertension) Mallory-Weiss tears
Reflux oesophagitis stage III-IV. Corrosive oesophagitis
hiatal herniatumoursperforation or rupture (traumatic,
iatrogenic..)
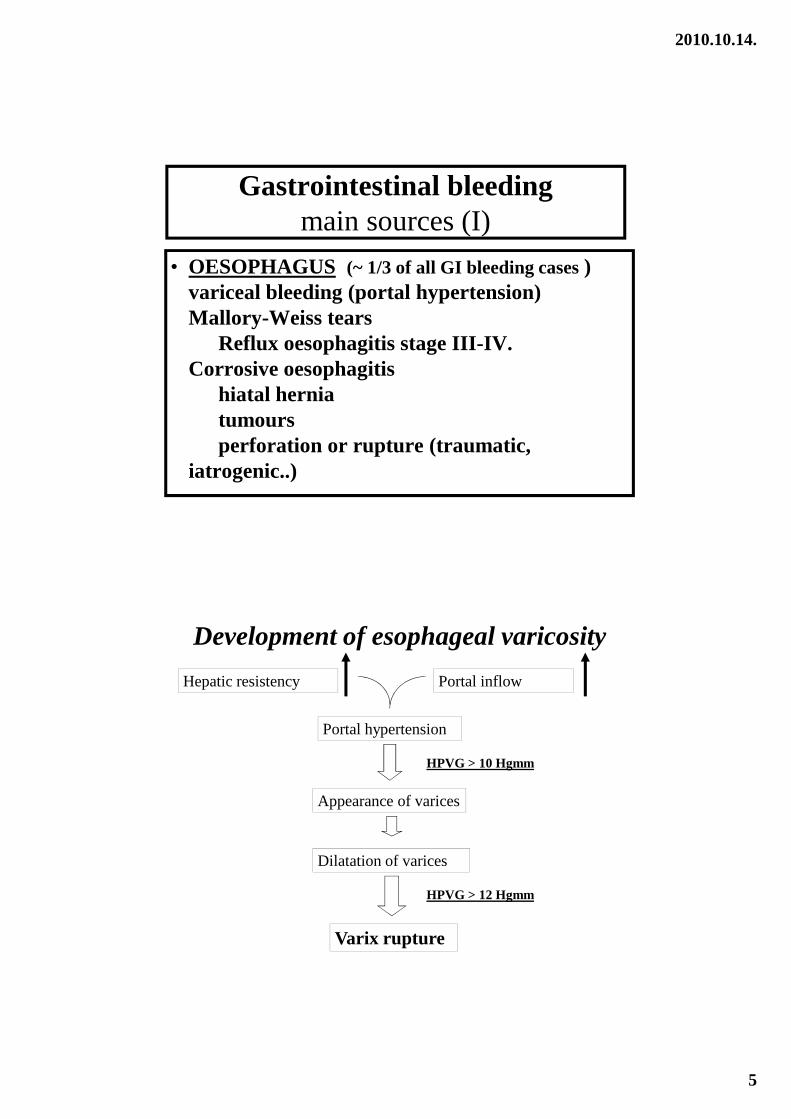
Development of esophageal varicosity
Hepatic resistency Portal inflow
Portal hypertension
Appearance of varices
Dilatation of varices
Varix rupture
HPVG > 10 Hgmm
HPVG > 12 Hgmm
2010.10.14.
6
Gastrointestinal bleedingmain sources (II)
• STOMACH AND DUODENUM (~ 1/2 of all) gastric and duodenal erosions (~ 30%)gastric ulcer and Dielaufoy lesion (~ 20%) duodenal ulcer (~ 30%)
tumours (also benign!) anastomositis, jejunal ulcer
angiodysplasiaforeign bodies in the stomachcancer of the head of the pancreas
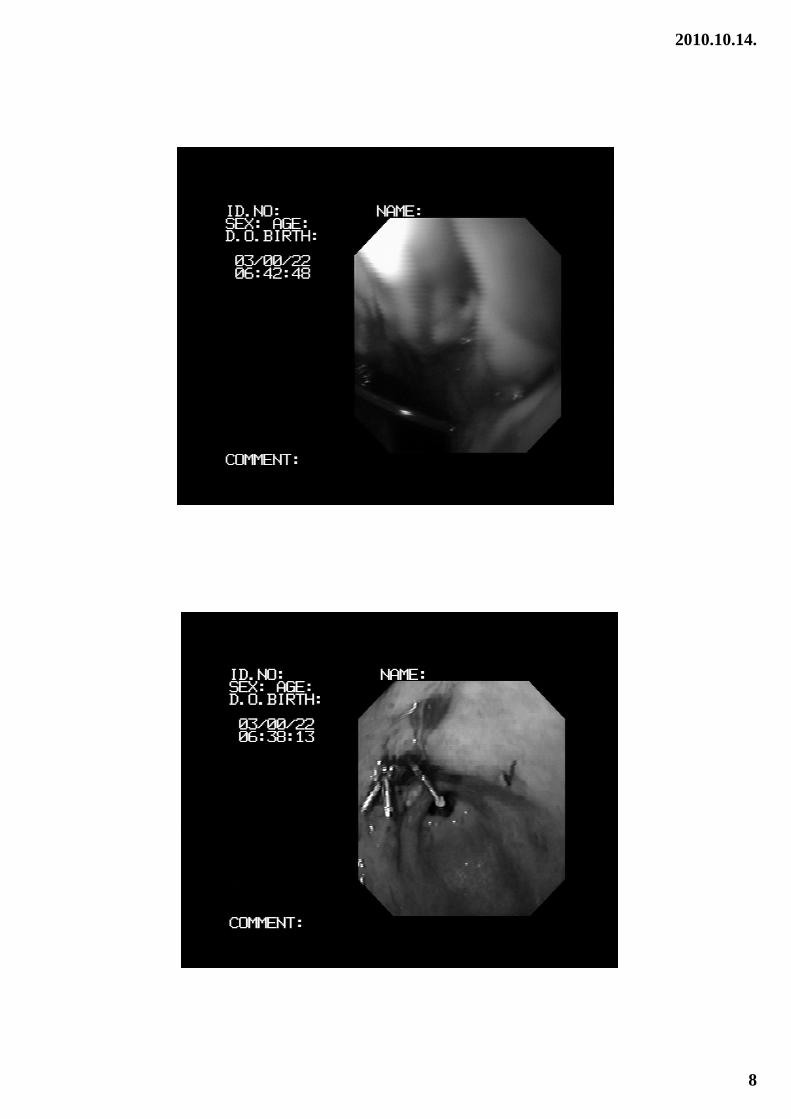
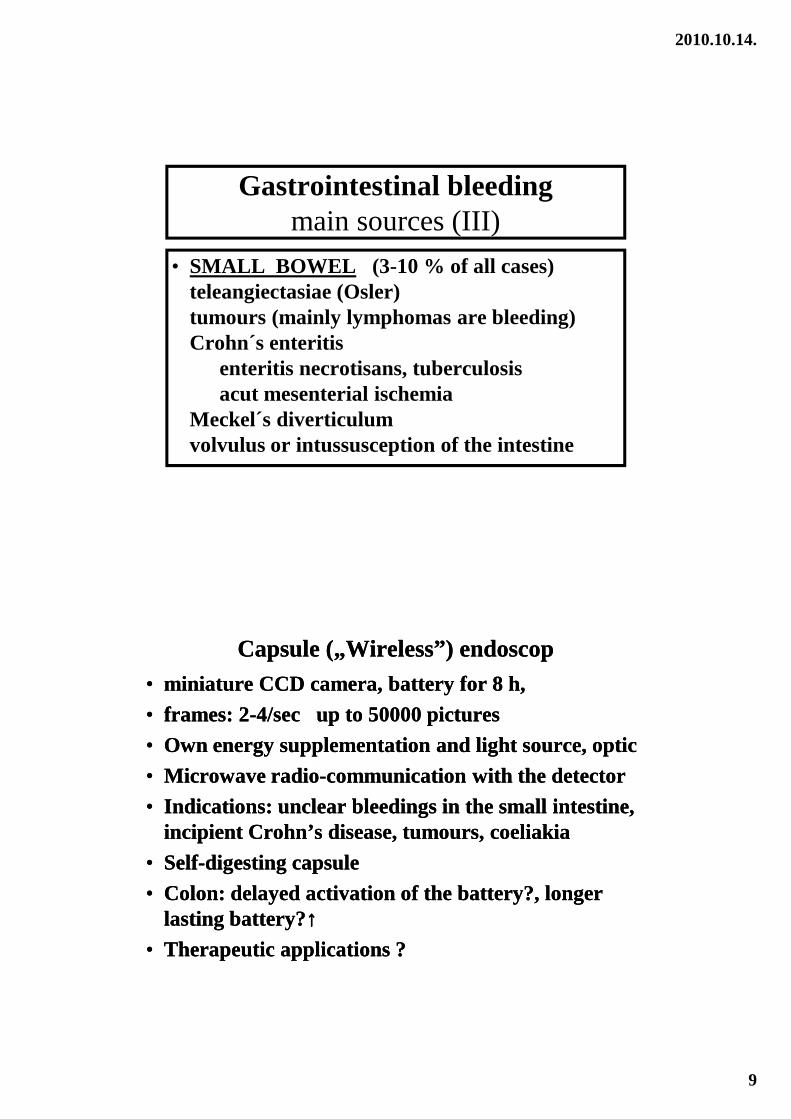
Classification of peptic ulcer bleeding according to Forrest
• Forrest I.: active bleeding seenI/A: spurting arterial bleedingI/B: oozing venous bleeding
• Forrest II.: stigmata of recent hemorrhageII/A: visible vessel, protuberance II/B: adherent clotII/C: ulcer base with digested Hb
• Forrest III: clean base, no stigmata of bleeding
2010.10.14.
7
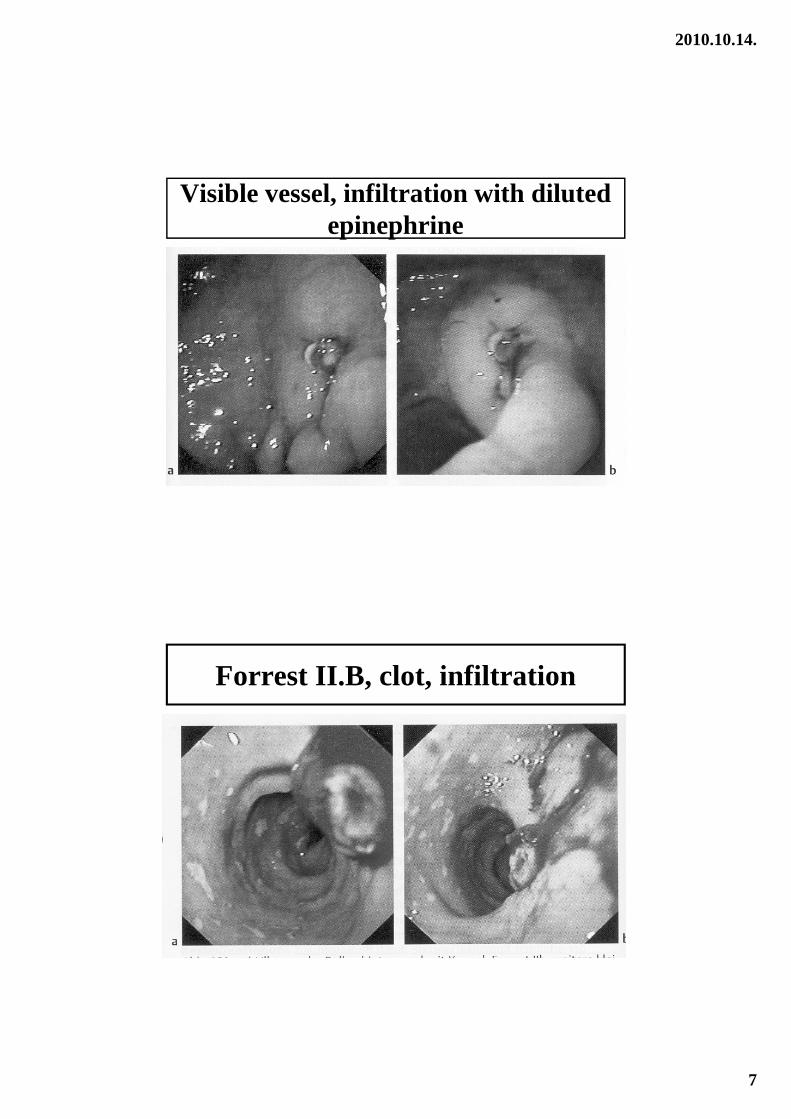
Visible vessel, infiltration with diluted epinephrine
Forrest II.B, clot, infiltration
2010.10.14.
8
2010.10.14.
9
Gastrointestinal bleedingmain sources (III)
• SMALL BOWEL (3-10 % of all cases) teleangiectasiae (Osler)tumours (mainly lymphomas are bleeding) Crohn´s enteritis
enteritis necrotisans, tuberculosisacut mesenterial ischemia
Meckel´s diverticulum volvulus or intussusception of the intestine
Capsule („Wireless”) endoscopCapsule („Wireless”) endoscop•• miniatureminiature CCD camera, CCD camera, batterybattery forfor 8 h, 8 h,
•• framesframes: 2: 2--4/sec 4/sec upup toto 50000 50000 picturespictures
•• OwnOwn energyenergy supplementationsupplementation and and lightlight sourcesource, , opticoptic
•• MicrowaveMicrowave radioradio--communicationcommunication withwith thethe detectordetector
•• IndicationsIndications: : unclearunclear bleedingsbleedings inin thethe smallsmall intestineintestine, , incipientincipient Crohn’sCrohn’s diseasedisease, , tumourstumours, , coeliakiacoeliakia
•• SelfSelf--digestingdigesting capsulecapsule
•• Colon: Colon: delayeddelayed activationactivation of of thethe batterybattery?, ?, longerlongerlastinglasting batterybattery??↑↑↑↑↑↑↑↑
•• TherapeuticTherapeutic applicationsapplications ??
2010.10.14.
10
Gastrointestinal bleedingmain sources (IV)
• COLON AND RECTUM (~15-20 % of all) diverticulosis hemorrhoids, rectal fissures, ulcers and varicesneoplasms (cancer and polyps) arteriovenous malformations (right colon!) IBD (ulcerative colitis, Crohn´s colitis) Infectious colitis (Shigella, Salmonella, ameba) Ischemic colitis, radiation colitis
Gastrointestinal bleedingstrategy of treatment (I)
• Administration to intensive care unit, with permanent endoscopic, surgical, radiological consultation, laboratory, availability of blood products
• Proper assessment of the hemodynamic status, evaluation of prognostic factors, immediate volume replacement, laboratory studies, blood group determination, necessary supplementation
2010.10.14.
11
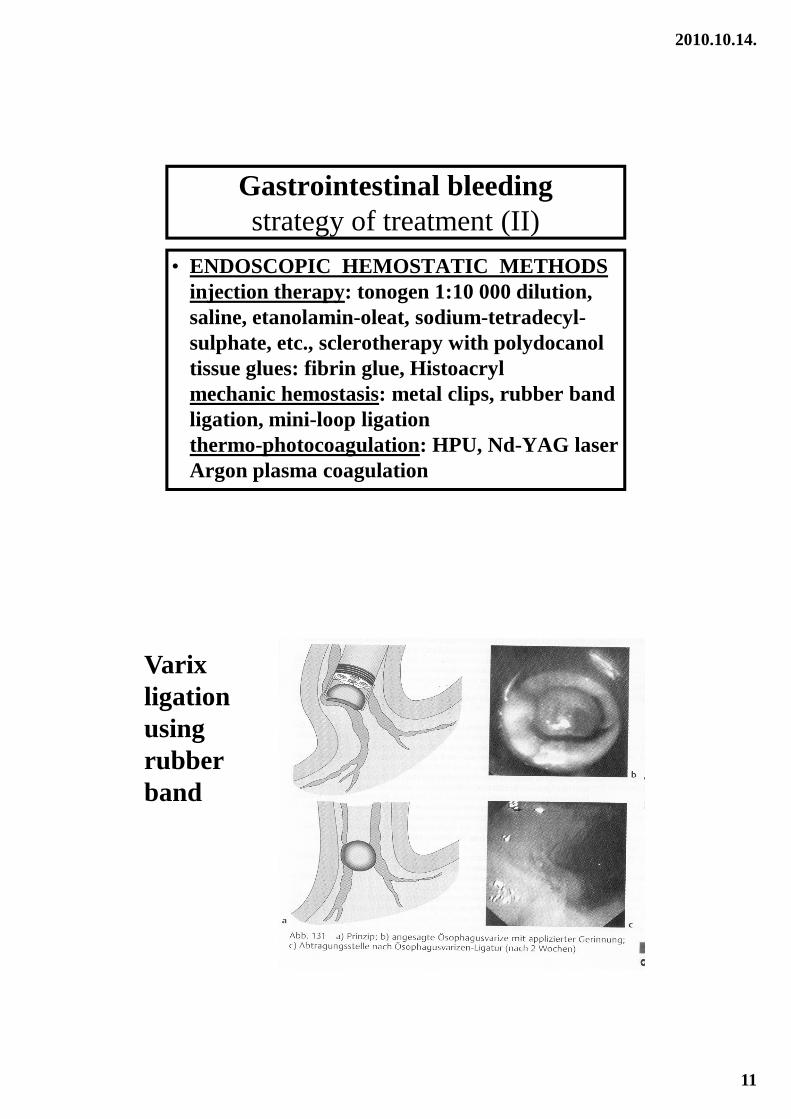
Gastrointestinal bleedingstrategy of treatment (II)
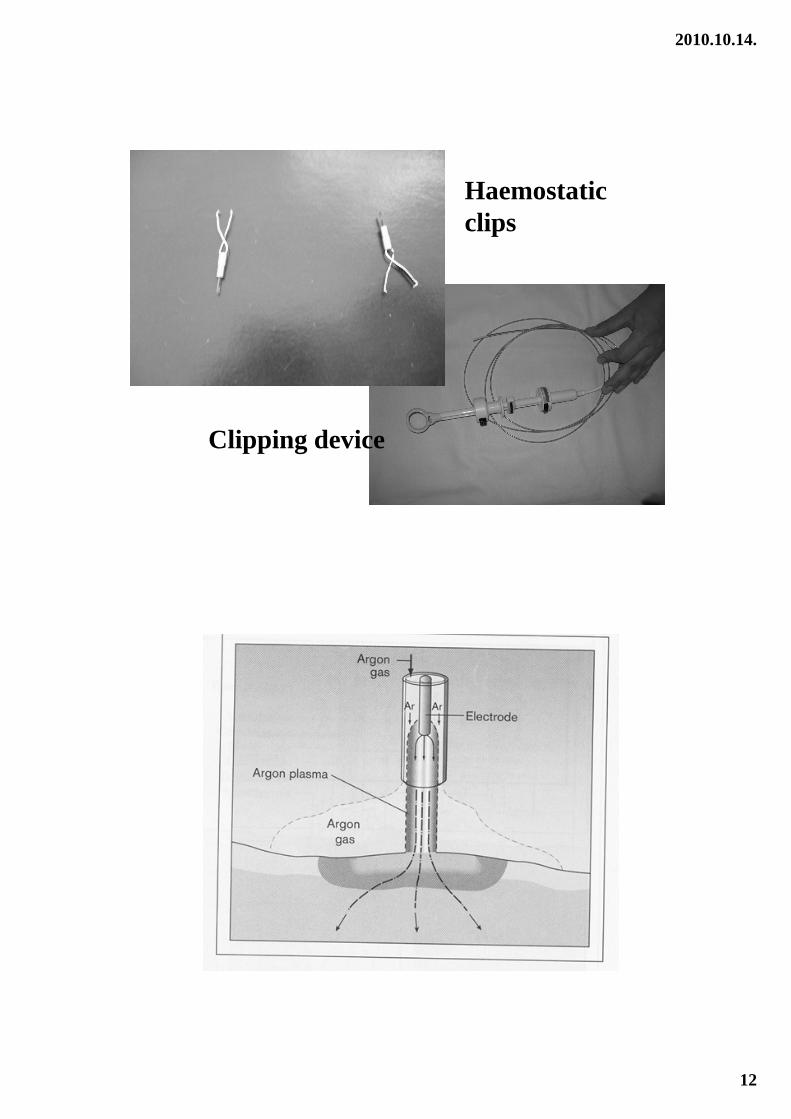
• ENDOSCOPIC HEMOSTATIC METHODSinjection therapy: tonogen 1:10 000 dilution, saline, etanolamin-oleat, sodium-tetradecyl-sulphate, etc., sclerotherapy with polydocanol tissue glues: fibrin glue, Histoacryl mechanic hemostasis: metal clips, rubber band ligation, mini-loop ligation thermo-photocoagulation: HPU, Nd-YAG laser Argon plasma coagulation
Varix ligation using rubber band
2010.10.14.
12
Haemostatic clips
Clipping device
2010.10.14.
13
Gastrointestinal bleedingstrategy of treatment (III)
• MEDICAL THERAPY- acid suppression (PPI or H2RA infusion i.v.) - vasoactive drugs for the reduction of portal pressure: 1. octreotid (somatostatin) infusion: 100 µg i.v. bolus, 25 µg/h infusion for 48-96 h. 2. terlipressin (triglycil-lysin vasopressin) - lactulose, 3 x 20-40 ml/day, sucralphate, - Helicobacter pylori eradication therapy - propranolol, neomycin, ISMN, DDAVP etc.
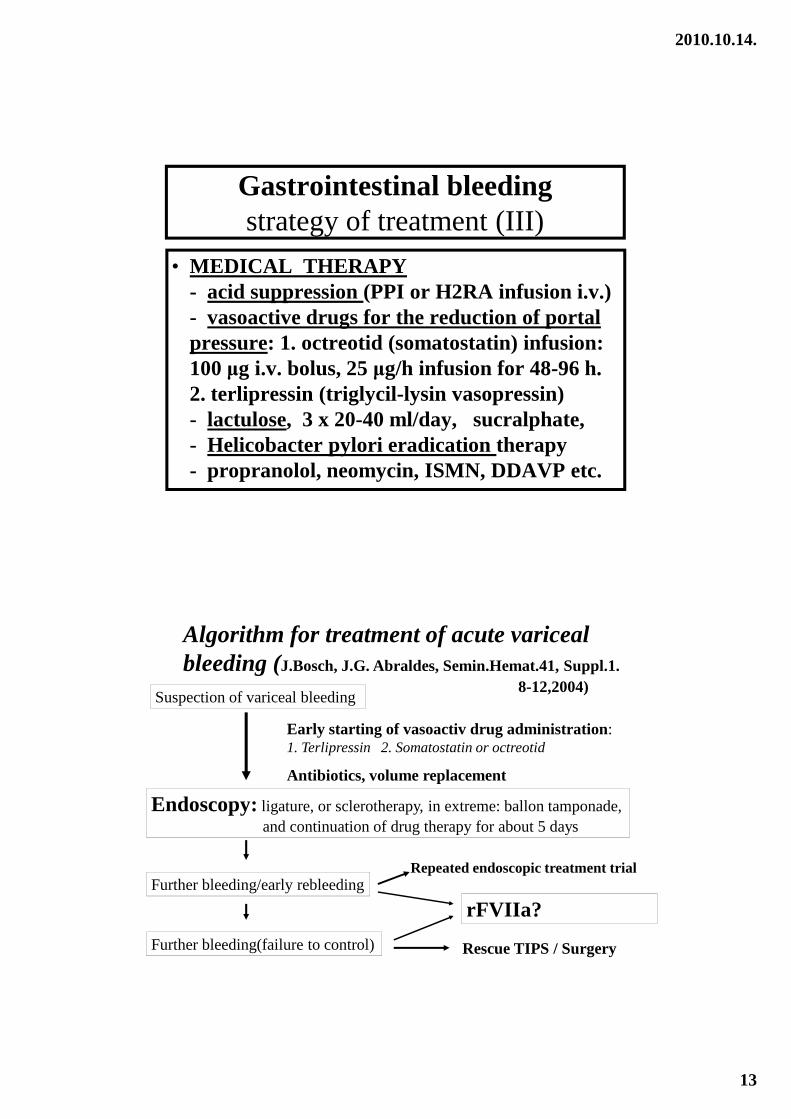
Algorithm for treatment of acute variceal bleeding (J.Bosch, J.G. Abraldes, Semin.Hemat.41, Suppl.1.
8-12,2004)Suspection of variceal bleeding
Endoscopy:ligature, or sclerotherapy, in extreme: ballon tamponade, and continuation of drug therapy for about 5 days
Further bleeding/early rebleeding
Further bleeding(failure to control)
Early starting of vasoactiv drug administration: 1. Terlipressin 2. Somatostatin or octreotid
Antibiotics, volume replacement
Repeated endoscopic treatment trial
Rescue TIPS / Surgery
rFVIIa?
2010.10.14.
14
Further treatment options
human albumin infusion,
in case of severe haemostatic disturbance fresh frozen plasma, eventually platelet suspension, especially of hugh amount of transfusions was given, - consider dilution and Ca supplementation!
Decomtamination of the intestine: lactulose, neomycin, rifaximin (Normix), SBP (spontaneous bacterial peritonitis) profilaxis: norfloxacin
adequat diet (low in fat, rich in carbohydrate and vitamines, less protein)
Gastrointestinal bleedingstrategy of treatment (IV)
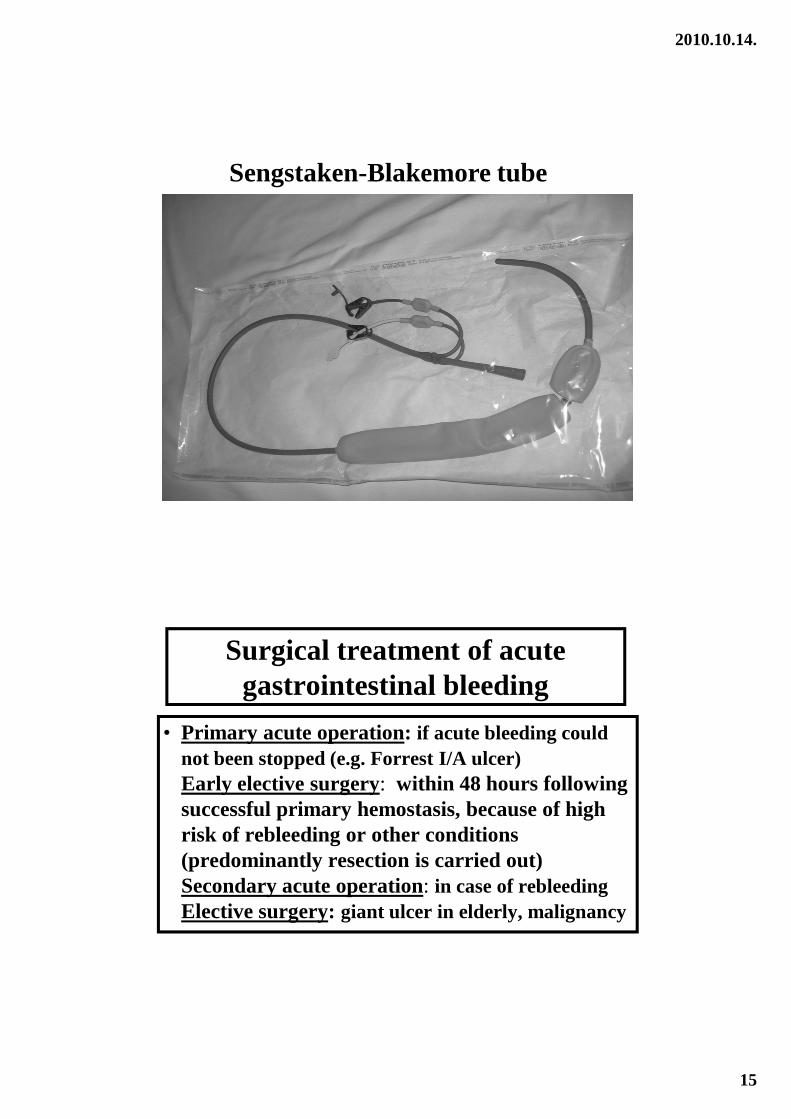
• OTHER THERAPEUTIC POSSIBILITIES -balloon tamponade (Sengstaken-Blakemore,
Linton tube, Minnesotta tube) -TIPS (transjugular intrahep. portosyst. shunt) -arterial embolisation during angiography -surgical intervention (suture, resection etc.) -tradition surgical shunt (porto-caval, spleno-renal) -liver transplantation
2010.10.14.
15
Sengstaken-Blakemore tube
Surgical treatment of acute gastrointestinal bleeding
• Primary acute operation: if acute bleeding could not been stopped (e.g. Forrest I/A ulcer)Early elective surgery: within 48 hours following successful primary hemostasis, because of high risk of rebleeding or other conditions (predominantly resection is carried out)Secondary acute operation: in case of rebleedingElective surgery: giant ulcer in elderly, malignancy
2010.10.14.
16
Further perspectives in GI bleeding
• SPONTANEOUSLY STOPS up to 80 % of all cases, if varix rupture is excluded
• SEVERE REBLEEDING (within 48 hours) upper GI tract: 15-20 % lower GI tract: < 10 %
• SURGICAL INTERVENTION : along with modern, GI intensive care unit 3-10 %
• OVERALL MORTALITY : 8-30 %