f BioMedTracker Cancer Immunotherapies - · PDF fileBioMedTracker Cancer Immunotherapies MAY...
40
f WWW.BIOMEDTRACKER.COM BioMedTracker Cancer Immunotherapies MAY 2014
-
Upload
nguyenlien -
Category
Documents
-
view
219 -
download
2
Transcript of f BioMedTracker Cancer Immunotherapies - · PDF fileBioMedTracker Cancer Immunotherapies MAY...

f
W W W . B I O M E D T R A C K E R . C O M
BioMedTracker
Cancer Immunotherapies
MAY 2014

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
2
Summary
Perhaps no other recent topic in oncology has generated as much excitement as the immunotherapies.
PD-1s, checkpoint inhibitors, CAR-T, and DC therapies – all have become common fare for those
following cancer drug development. Indeed, “Cancer Immunotherapy” was voted the Science
Breakthrough of the Year for 2013 (Science, Vol. 342, no. 6165) and MD Anderson promoted
immunotherapies as part of their ambitious Moon Shots program. And attendees at the recent 2014
American Association for Cancer Research witnessed a flood of immunotherapy sessions first-hand.
Immunotherapies in oncology have actually been around for decades, including the use of cytokines and
immunomodulatory agents that had a general stimulatory effect on the immune system. Targeted
monoclonal antibodies also are technically immunotherapies. However, the renewed interest in
immunotherapies has primarily been driven by a few promising new classes that are the focus of this
report. Topics covered include:
Programmed-death (anti-PD-1 drugs) and other immune checkpoint inhibitors
Dendritic cell (DC) therapies
T-cell therapies (CAR-T)
Cancer vaccines
About the Author
BioMedTracker is an independent research service that offers proprietary clinical assessments and
patient-based revenue forecasts of developmental drugs within a comprehensive and intuitive drug
information database. Clients from the pharmaceutical, biotech, and investment industries rely on
BioMedTracker for its insight on the likelihood of approval, commercial potential, and future data and
regulatory catalysts for drugs within the competitive landscape of every important disease and
indication. Over the last several years, BioMedTracker has become the leader in providing objective
information alongside evidence based clinical assessments and investment research on pipeline drugs
worldwide. For more information on getting direct access to BioMedTracker, please visit
www.biomedtracker.com
Disclaimer
Copyright © 2014 Sagient Research, Inc.
This report is published by Sagient Research, Inc. (the Publisher). This report contains information from
reputable sources and although reasonable efforts have been made to publish accurate information,
you assume sole responsibility for the selection, suitability and use of this report and acknowledge that
the Publisher makes no warranties (either express or implied) as to, nor accepts liability for, the
accuracy or fitness for a particular purpose of the information or advice contained herein. The Publisher
wishes to make it clear that any views or opinions expressed in this report by individual authors or
contributors are their personal views and opinions and do not necessarily reflect the views/opinions of
the Publisher.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
3
Contents
Background .............................................................................................................. 4
Programmed Death (PD-1) Inhibitors ...................................................................... 6
Other Checkpoint Inhibitors ................................................................................... 18
Dendritic Cell Therapies ......................................................................................... 23
Chimeric Antigen Receptor T-Cell (CAR-T) Therapies ........................................... 27
Cancer Vaccines ..................................................................................................... 30
IDO Inhibitors ........................................................................................................ 35
Miscellaneous Immunotherapies ........................................................................... 35

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
4
Background
The immune system is a complex defense mechanism against foreign particles, but it often fails to
recognize cancer cells. Nevertheless, the idea of stimulating the immune system to better attack cancer
cells has long been attractive because of the special properties an immunotherapy could provide
including high specificity against tumor cells and a uniquely long-lasting response (immunologic
memory).
Figure 1. Idealized characteristics of traditional (blue) and immunotherapies (green). Immunotherapies
may show similar survival kinetics to traditional therapies as an immune response develops, but could
provide a much longer survival benefit for a subset of patients (long green tail). Combinations of
traditional and immunotherapies could combat the initial drop in survival while also providing the long-
term response (red). (Adapted from Perlmutter, AACR 2014)
Therapies that modulate the immune system have, of course, been common in other disease areas,
particularly autoimmune disorders. Even cancer immunotherapies in the broader sense have been
available for decades including general immunomodulators (e.g. cytokines), and targeted antibody
biologics that block specific oncogenic pathways but that also stimulate immune responses against the
targeted tumor cells (e.g. Avastin, Herceptin). Indeed, most therapies that result in lysed tumor cells
likely stimulate at least some immune response to tumor specific antigens that are released as a
secondary mechanism.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
5
However, the more recent identification of novel mechanisms that cancer cells use to actively avoid
immune detection (e.g. immune checkpoints) as well as emergence of new technologies to manipulate
immune cells have ignited a new wave of interest and drug development in immunotherapies. And, so
far, the early clinical signs are promising, particularly for PD-1s which are demonstrating the long
durability characteristic of an endogenous immune response in several tumor types.
Two next-generation immunotherapies have already reached the market with the FDA approval of
Provenge (sipuleucel-T; DNDN) for prostate cancer in 2010 marking the start of the current era of
immunotherapies. Provenge is a complex cell therapy that was remarkable as the first targeted prostate
cancer therapy in the castration-refractory setting to demonstrate a survival advantage (Jevtana
[cabazitaxel, SNY] also showed a survival benefit around the same time but is more similar to a
traditional chemotherapy). Although Provenge has achieved limited commercial success due to a variety
of factors (including the rapid arrival of strong traditional-drug competitors), its development did set the
stage for the current generation of immunotherapies, including addressing the issue of extending overall
survival (OS) without extending progression-free survival (PFS) that may be common to many
immunotherapies due to the lag time required for an immune response to develop.
Following Provenge was the approval of Yervoy (ipilimumab, BMY) for melanoma in 2011. Yervoy is an
inhibitor of the CTLA-4 immune checkpoint. Checkpoint inhibitors are some of the most promising
immunotherapies in development (especially PD-1s), with several large companies developing drugs in
this space including Bristol-Myers Squibb, Roche, and Merck. These inhibitors attack endogenous
immune controls that some tumors co-opt to suppress immune attacks against them. In addition to the
CTLA-4 checkpoint, other checkpoints have been identified including the Programmed Death checkpoint
(PD, or PD-1), TIM3 (T-cell Immunoglobulin and Mucin domain 3), and LAG3 (Lymphocyte-activation
gene or CD223).
It is worth noting that because of the broad definition of immunotherapies, some companies are trying
to inflate interest in their more traditional drugs by associating them with the more novel
immunotherapies. Thus, those following the field must be cautious about understanding the actual
mechanism behind new drugs in the space. One example is Provectus Biopharmaceuticals (PVCT). Its
lead drug, PV-10, is a formulation of the small molecule, rose bengal, which has been long been used as
a biological stain. Although the specific mechanism of action to kill tumor cells is not entirely clear, PV-
10 is believed to accumulate in the lysosomes of rapidly growing tumor cells and cause cell lysis.
However, more recently, the company has been promoting a tumor specific immune response
associated with PV-10 that is most likely a secondary effect of lysing tumor cells (see 2013 AACR poster
#1248 and 2013 PLOS One publication, DOI: 10.1371/journal.pone.0068561).
Another example is Peregrine Pharmaceuticals (PPHM) and its promotion of bavituximab. Early in its
development, the company described the mechanism of action primarily through targeting of exposed
phosphatidylserine (PS) on tumor cell surfaces. Now, however, the company is proposing a more
detailed mechanism involving immune signaling to macrophages by PS. While macrophage polarization
and tumor-specific immune response could very well be a part of PS signaling, it also could be an effect
of a more intense effort to measure immune responses which could likely be identified with many
oncotherapies.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
6
Programmed Death (PD-1) Inhibitors
Perhaps the most widely-anticipated immunotherapy class is the Programmed Death checkpoint
inhibitors, commonly referred to as anti-PD-1 therapies (although not technically accurate since this
includes anti-PD-L drugs against PD ligands). Programmed Death is one of several immune checkpoints
that are being actively explored for drug development (others include CTLA-4, TIM3, and LAG3). Each
checkpoint may have different endogenous functions, associated signaling pathways, and levels of
expression in diverse tumors. Thus, the inhibition of different checkpoints may result in different
efficacy across tumor types.
Currently, four PD-1 drugs are the most advanced in clinical development:
Nivolumab (BMY)
Lambrolizumab (MRK)
Pidilizumab (CureTech)
RG7446 (Roche)
Of the four leading drugs, only RG7446 targets a PD ligand while the other three target the PD-1
receptor. Thus, although both elements of the PD axis have six therapies in clinical stage development,
drugs targeting the PD-1 receptor are generally further along in development.
Figure 2. PD-1 therapies targeting either the PD-L1/L2 ligand or PD-1 receptor.
Phase II or III studies have begun for all four leading drugs, but almost all of the clinical data to date
comes from large Phase I studies enrolling patients with many tumor types. Nevertheless, the most
promising tumor subgroups seem to be emerging as melanoma, NSCLC, and renal cell cancer.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
7
Nivolumab (BMY)
Figure 3. Key events and upcoming catalysts to watch in primary nivolumab indications.
Perhaps no company is pursuing immunotherapies more aggressively than Bristol-Myers Squibb—its
nivolumab has led the race among anti-PD-1 therapies for much of its short clinical history, although a
rolling BLA for Merck’s MK-3475 has recently been initiated, pushing it ahead of nivolumab for now. In
the last major data release at the 2013 ASCO meeting, positive survival data were presented from
expansion cohorts of three tumor subgroups from the Phase I solid tumor study.
Melanoma NSCLC RCC
OS (mo.) 16.8 9.6 22.0
ORR (%) 31 17 29
Table 1. Nivolumab efficacy from expansion cohorts of Study 003.
Melanoma
In treatment-refractory melanoma, the Phase I data are extremely promising. As is becoming a theme
with immunotherapies, the median PFS of 3.7 months from the expansion cohort is not impressive, but
the one- and two-year PFS rates are (36% and 27%, respectively), reflecting a sharp initial decline in the
Kaplan-Meier curve that eventually plateaus presumably as an immune response develops. Similarly, the
median OS of 16.8 months is positive, but the one- and two-year OS results (62% and 43%, respectively)
are even more impressive and surpass the 46 and 24% OS rates, respectively, of Yervoy, a different
checkpoint inhibitor (see CLTA-4 inhibitors below).

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
8
Figure 4. Nivolumab PFS data in melanoma (presented at ASCO 2013).
Also of note is the durability of response (24 months) which is an anticipated feature of
immunotherapies that makes them very attractive. Additionally, the safety profile appears very strong.
No deaths were reported since the presentation at the 2012 ASCO meeting. Finally, in a minor note, the
study showed remarkable response rates across a wide 100-fold range of doses, suggesting a lot of
flexibility in choosing an efficacious dose. Nevertheless, the 3mg/kg dose is being used for the Phase III
studies.
Multiple Phase III studies are ongoing, including a combination study with Bristol’s approved CTLA-4
checkpoint inhibitor, Yervoy. The CTLA-4 checkpoint plays a role earlier in T-cell activation as opposed
to the PD-1 checkpoint which functions more locally after T-cells have been activated, so there is a
potentially synergy to blocking both early and late checkpoints. Those trials are anticipated to be
completed in 2015. Early data from the Phase Ib study 004 suggests an estimated 82% one-year survival
rate.
Positive top-line data have also been released from a Japanese Phase II study in melanoma that showed
a median PFS of 172 days and supported a subsequent J-NDA filing in December 2013. Approval in Japan
for melanoma is estimated between 9/1/14-3/31/15.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
9
NSCLC
Nivolumab efficacy in treatment-refractory NSCLC patients has been striking, especially in heavily-
pretreated patients. Notably, a durable benefit has been observed in both squamous and non-squamous
NSCLC patients as the squamous cell population has been historically the most difficult to treat.
To date, four Phase III studies are ongoing or are planned, including the recent announcement of a
combination study with Yervoy that is expected to initiate by the end of 2014. Also in 2014, important
top-line data are anticipated from a Phase II study of squamous cell patients as well as from two Phase
III studies.
Renal Cell Cancer
Development of nivolumab is the least aggressive in RCC with only a single Phase III study ongoing
evaluating the drug post-anti-angiogenic therapy. This pivotal study against Afinitor (everolimus, NVS) is
not anticipated to complete until the first half of 2016.
Figure 5. Nivolumab trials in its three leading indications: NSCLC, melanoma, and renal cell cancer. The
most promising data released to date have come from the Phase I -003 study initially enrolling solid
tumor patients but has since continued in expansion arms for NSCLC, melanoma, and RCC.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
10
MK-3475 (pembrolizumab, MRK)
Figure 6. Key events and upcoming catalysts to watch in primary MK-3475 indications.
(Note: The generic name for MK-3475 was previously designated as lambrolizumab but was
subsequently changed to pembrolizumab. This report uses all three names interchangeably.)
MK-3475 is being developed most aggressively for melanoma and technically leads all anti-PD-1s with a
rolling BLA submitted in January 2014 for post-ipilimumab melanoma patients. Merck expects to
complete the BLA application in the first half of 2014.
In melanoma, the last major data release was at the 2013 ASCO meeting from the Phase I study and
revealed very impressive response rates of 38% and as high as 62% for the every two week dose, prior
ipilimumab treatment arm. The response rate did vary quite a bit across different dosing and pre-
treatment subgroups from 25-62%, but it did not correlate directly with prior ipilimumab exposure, and
all rates were still relatively high. Indeed, these response rates surpass what has been seen for the other
anti-PD drugs. However, comparisons should still be made cautiously as these data are from relatively
small studies (although this study did enroll 117 patients spread across 5 treatment arms).
More recently, updated data from the same study at the Society for Melanoma Research (SIMR)
meeting provided the first presentation of survival results. These initial survival data are very
encouraging with a 31 week mPFS and 81% one-year survival rate. The survival benefit for this
monotherapy appears to be relatively uniform across doses and dose schedules (79%-86%) and
compares favorably to nivolumab monotherapy (62% in Study 003) and an estimated 82% with the
nivolumab + ipilimumab combination therapy (Study 004). Also encouraging is the fact that response
rates were similar between groups with or without ipilimumab pretreatment affirming the value of
targeting multiple checkpoints.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
11
All Treatment Treatment Treatment Treatment
Treatment Description Lambrolizumab All
Monotherapy Lambrolizumab 10
mg/kg Q2W Lambrolizumab 10
mg/kg Q3W Lambrolizumab 2
mg/kg Q3W
Number of Patients 135 N/A N/A N/A
Overall survival - One year (Endpoint=Secondary)
81 % 82 % 79 % 86 %
Overall survival - 6 month (Endpoint=Primary)
89 % 86 % 93 % 91 %
Objective response rate - Central Review (Endpoint=Primary)
41 % N/A N/A N/A
Complete response rate - Central Review (Endpoint=Secondary)
9 % N/A N/A N/A
Progression free survival - 24 weeks (Endpoint=Secondary)
61 % 66 % N/A N/A
Progression free survival - median (Endpoint=Secondary)
31 weeks 61 weeks N/A N/A
Table 2. Phase I data of MK-3475 showing encouraging PFS and one-year OS results.
A Phase III study (006) vs Yervoy in melanoma and a pivotal Phase II/III study vs docetaxel in NSCLC are
ongoing, but combination studies are notably lacking. Combination studies are one of the most
promising avenues for the current wave of immunotherapies, and nivolumab (BMY) already has a Phase
III study initiated in combination with ipilimumab (BMY) for melanoma while RG7446 (Roche) is in
several early-stage combination studies with vemurafenib, erlotinib, and Avastin (Phase II), for example.
To address that deficiency, Merck recently announced three separate clinical collaboration agreements
through subsidiaries, with Amgen, Incyte, and Pfizer to evaluate novel combination regimens with MK-
3475. The financial terms of the agreements were not disclosed.
Planned investigations include:
Pfizer and Merck will evaluate in Phase I/II clinical studies the safety and efficacy of MK-3475 in combination with Pfizer’s small molecule kinase inhibitor axitinib (Inlyta) in patients with renal cell carcinoma. Additionally, they will assess MK-3475 plus PF-05082566 (PF-2566), an investigational immuno-oncology agent that targets the human 4-1BB receptor, in multiple cancer types.
Incyte and Merck will collaborate on a randomized, double-blind placebo controlled Phase I/II study to evaluate the safety and efficacy of a regimen combining MK-3475 with Incyte’s investigational immunotherapy agent, INCB24360, an indoleamine 2, 3-dioxygenase (IDO) inhibitor, in patients with previously treated metastatic and recurrent NSCLC, among other advanced or metastatic cancers. The Phase I portion of the trial is expected to establish a recommended dose regimen of INCB24360 and MK-3475. In the Phase II portion of the study, all patients receive MK-3475 and patients will be randomized to receive either INCB24360 or

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
12
matching placebo. The study is expected to begin in the first half of 2014 and will be co-funded by Incyte and Merck and conducted by Incyte.
Amgen and Merck will evaluate MK-3475 in combination with Amgen’s investigational oncolytic immunotherapy talimogene laherparepvec in a Phase Ib/II study in patients with mid- to late-stage melanoma.The multicenter, open-label clinical trial will be conducted in two parts and is planned to begin in the fall of 2014. Phase Ib is designed to determine the safety and tolerability of talimogene laherparepvec in combination with MK-3475 in patients with previously untreated, unresected, stage IIIB to IVM1a melanoma. The Phase II portion will evaluate efficacy, as assessed by the confirmed objective response rate (ORR), with talimogene laherparepvec in combination with MK-3475 versus MK-3475 alone in patients with previously untreated, unresected, stage IIIB to IVM1c melanoma. The study will also evaluate the efficacy of treatment with talimogene laherparepvec in combination with MK-3475 following disease progression on MK-3475 alone.
Separately, Merck announced it will start a new Phase I “signal finding” study to evaluate the safety and
efficacy of MK-3475 monotherapy in 20 different PD-L1-positive solid tumor types that have not been
studied previously.
Although a Phase I/II study (021) had already been initiated to evaluate MK-3475 in combination with a
variety of other therapies, these agreements greatly expand the push to develop a combination regimen
and bring MK-3475 closer to nivolumab and RG7446 combination development.
Figure 7. Key MK-3475 trials at a glance. MK-3475 is most advanced in NSCLC and melanoma. So far,
data have only been released from the Phase Ib solid tumors study which also included melanoma and
NSCLC arms.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
13
RG7446 (Roche)
Figure 8. Key events and upcoming catalysts to watch in primary RG7446 indications.
Of the four leading anti-PD-1 therapies, RG7446 is the only one targeting the PD-1 ligand rather than the
receptor. Also, unlike nivolumab (BMY) and MK-3475 (MRK), development is proceeding slightly faster in
NSCLC over melanoma and renal cell cancer with the Pivotal Phase III – OAK study (vs docetaxel, post-
platinum chemo) recently initiated in February 2014.
NSCLC
In NSCLC, efficacy has shown a strong correlation with PD-L1 positive tumor status, albeit from a small
sample size. Data at the 2013 ASCO revealed a 100% response rate in PD-L1 positive patients (n=4) vs
15% in negative patients.
Treatment Treatment Treatment
Treatment Description MPDL3280A
Squamous/non-squamous NSCLC MPDL3280A
PD-L1 tumor status-positive MPDL3280A
PD-L1 tumor status-negative
Number of Patients 37 4 26
ORR 24 % 100 % 15 %
24-week PFS 48 % N/A N/A
PD rate N/A 0 % 58 %
Table 3. Phase I data of RG7446 in NSCLC patients.
Renal Cell Cancer
Early RCC data have also been positive with activity in both ccRCC (clear cell) and nccRCC (non-clear cell)
which is impressive as nccRCC is historically very difficult to treat. While PD-L1+ predicted response
(with CRs only in this group) PD-L1 negative pts still showed some response. While a discussant at the
2013 ASCO presentation mentioned the need for an IHC assay, there is concern that this would
artificially narrow the patient population.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
14
Treatment Treatment Treatment Treatment
Treatment Description MPDL3280A 20mg/kg
Overall Population MPDL3280A 20mg/kg
RCC Patients
MPDL3280A 20mg/kg RCC Patients
Clear Cell
MPDL3280A 20mg/kg RCC Patients
Non-Clear Cell
Number of Patients 140 47 40 6
24-week PFS 45 % 53 % 57 % 20 %
SD of 24 weeks or longer 16 % 32 % 35 % 0 %
RECIST 1.1 ORR 21 % 13 % 13 % 17 %
Investigator-Assessed ORR PD-L1 Positive Patients
36 % 20 % N/A N/A
Investigator-Assessed ORR PD-L1 Negative Patients
13 % 10 % N/A N/A
Table 4. Phase I data at ASCO 2013 in RCC patients.
Notably, PD-L1 treatment showed no G3-5 pneumonitis which may be a concern with PD-1 targeted
treatment and has been observed with nivolumab and MK-3475. During the ASCO Q&A, a BMS scientist
asked why it looked like there was more stable disease with PD-L1 and a better response rate with PD-1
targeted compounds (ORR with nivolumab was 29%). The presenter commented that the final response
rate may not be 13% as patients are still on treatment.
Melanoma
In melanoma, data from the Phase I Solid Tumors study were recently updated at the Society for
Melanoma Research (SMR) meeting. This presentation showed slightly higher ORR than was last
presented at the 2013 ASCO meeting (32%, up from 29%), putting it at least on par with the other anti-
PD drugs at this early stage.
Treatment Treatment Treatment
Treatment Description MPDL3280A IV q3w
MPDL3280A IV q3w
PD-1 Positive pts MPDL3280A IV q3w PD-1 Negative pts
Number of Patients 44 15 15
Number of Evaluable Patients 34 N/A N/A
Overall response rate 32 % N/A N/A
24-week PFS 43 % N/A N/A
Disease control rate N/A 87 % 20 %
Table 5. Phase I melanoma data for RG7446 (presented at 2013 SMR).
The ongoing Phase Ib portion of the study is evaluating the drug in combination with vemurafenib. This
combination makes sense since PD-L1 expression is increased with vemurafenib treatment, but the
study is limited to a BRAF mutant population as vemurafenib is a B-Raf inhibitor.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
15
Figure 9. RG7446 Studies in lead indications NSCLC, melanoma, and renal cell cancer.
Pidilizumab (CureTech)
Of the four leading PD-1 drugs, the least has been revealed about pidilizumab, even as Phase II studies
have begun. Pidilizumab is notable for its development in hematological cancers along with solid
tumors.
Little data have been disclosed to date, although some Phase II data in DLBCL have been published
showing a promising 51% response rate in patients with measurable disease following stem cell
transplant.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
16
Treatment Treatment Treatment
Treatment Description Pidilizumab
All pts Pidilizumab
High-risk pts Pidilizumab
Pts with measurable disease
Number of Evaluable Patients 66 24 35
PFS at 16 months (Endpoint=Primary)
0.72 0.70 N/A
Overall response rate N/A N/A 51 %
Table 6. Published Phase II data in DLBCL.
In melanoma, positive Phase II data were also reported showing a low 10% response rate, but a more
encouraging 65% one-year survival rate.
Treatment
Treatment Description CT-011
Number of Patients 103
Objective response rate (Endpoint=Primary)
10 %
Survival rate at 12 months (Endpoint=Secondary)
65 %
Table 7. Phase II melanoma data for pidilizumab.
It was also reported late last year that a Phase II colorectal cancer study of pidilizumab in combination
with FOLFOX failed to meet its primary endpoint of an ORR and PFS benefit over FOLFOX alone.
Novartis and CoStim
Not to be left out of the race for PD-1 drugs, Novartis recently acquired CoStim, a private company
which is developing a PD-1 therapy as well. Little information is available on the PD-1 therapy or the rest
of the CoStim pipeline. Nevertheless, one likely rationale for the acquisition is to evaluate a combination
of a PD-1 inhibitor with the Novartis CAR T-cell therapy, CTL-019. This is a promising combination since
the removal of a checkpoint blockade is likely to enhance any therapy dependent on T-cell expansion.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
17
Figure 10. Overview of Anti-PD-1 Clinical Development

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
18
Other Checkpoint Inhibitors
Although PD-1 therapies have garnered the most attention, there are numerous other immune
checkpoints that function similarly. Indeed, the CTLA-4 inhibitor, Yervoy (ipilimumab, BMY), is the first
and only checkpoint inhibitor to gain FDA approval thus far. Other inhibitory immune checkpoint targets
under investigation in oncology include TIM3 and LAG3.
Figure 11. Multiple immune checkpoints exist and are possible therapeutic targets. Adapted from
Mellman et al.(2011) Nature 480.
Additionally, there are immune modulators that function on the opposite axis of checkpoints and
stimulate T-cell activation rather than inhibit it. CD28 has been identified as a primary early activator of
naïve T-cells. Other stimulators of activated T-cells include GITR and OX40 among others. Development
of these T-cell activators as oncology targets trails the inhibitory checkpoint targets with work primarily
still in preclinical stages, but one Phase II study of an anti-OX40 antibody has been initiated by
AstraZeneca and AgonOx in prostate cancer.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
19
Figure 12. Clinical development of CTLA-4, TIM3, and LAG3 checkpoint inhibitors.
Yervoy (ipilimumab, BMY)
Yervoy became the first approved immune-checkpoint inhibitor in 2011 when it received FDA approval
for the second-line treatment of melanoma based on the Phase III – 020 Study. The study demonstrated
an approximately four-month median overall survival benefit over comparator (gp100, an experimental
peptide vaccine) and, along with Zelboraf (vemurafenib, Roche), led a wave of therapies that showed
overall survival benefits in advanced melanoma patients.
While there is a fairly low rate of grade 3/4 adverse events associated with ipilimumab treatment, there
have been some significant toxicities associated with treatment, now termed immune related adverse
events (IRAE). While the majority of these adverse events are mild in nature, severe cases of colitis and
bowel perforation have arisen. Physicians using ipilimumab must be aware of the possibility of
treatment emergent IRAEs and control them through the use of steroids, which do not affect the
response to ipilimumab. Although these IRAEs can be serious in nature, they also are indicative of a
highly active immune system and often go hand in hand with response to treatment.
Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
20
Comparator Treatment Treatment
Difference Between
Treatment and Comparator
Difference Between
Treatment and Comparator
Difference Between
Treatment and Comparator
Treatment Description GP100 + Placebo
Ipilimumab + Placebo
Ipilimumab + GP100
Ipilimumab + Placebo vs. GP100
+ Placebo
Ipilimumab + GP100 vs. GP100 +
Placebo
Ipilimumab + GP100 vs.
Ipilimumab + Placebo
Number of Patients 136 137 403 273 539 540
Median overall survival (Endpoint=Primary)
6.4000 Months
10.1000 Months
10.0000 Months
N/A (P=0.0026)
N/A (P=0.0004)
N/A (P=0.7575)
Median overall survival rate (12 months) (Endpoint=Secondary)
25.3000 % 45.6000 % 43.6000 % N/A N/A N/A
Median overall survival rate (18 months) (Endpoint=Secondary)
16.3000 % 33.2000 % 30.0000 % N/A N/A N/A
Median overall survival rate (24 months) (Endpoint=Secondary)
13.7000 % 23.5000 % 21.6000 % N/A N/A N/A
Median progression-free survival (Endpoint=Secondary)
2.7600 Months
2.8600 Months
2.7600 Months
N/A (P=0.0007)
N/A (P=0.0464)
N/A (P=0.0371)
Median progression-free survival rate (12 months) (Endpoint=Secondary)
48.5000 % 57.7000 % 49.1000 % N/A N/A N/A
Overall response rate (Endpoint=Secondary)
1.5000 % 10.9000 % 5.7000 % N/A
(P=0.0012) N/A
(P=0.0433) N/A
(P=0.0402)
Disease control rate (Endpoint=Secondary)
11.0000 % 28.5000 % 20.1000 % N/A
(P=0.0002) N/A
(P=0.0179) N/A
(P=0.0371)
Proportion of patients maintaining ORR for 2 years (Endpoint=Secondary)
0.0000 % 60.0000 % 17.4000 % N/A N/A N/A
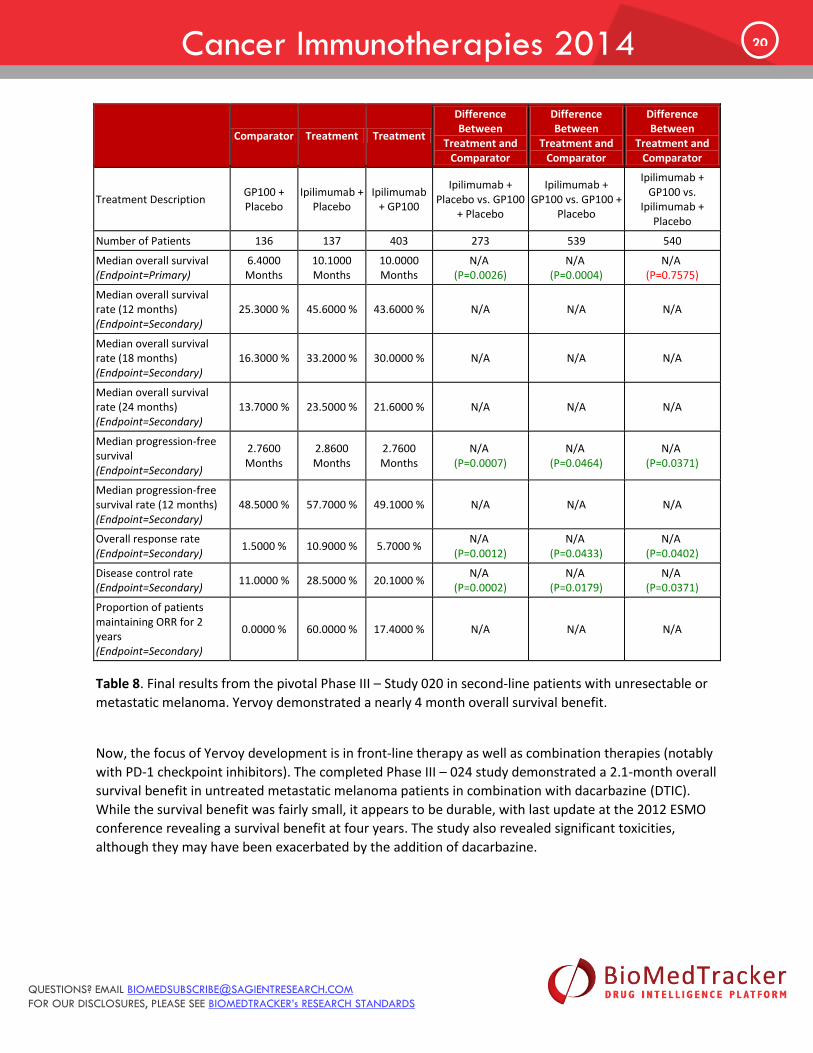
Table 8. Final results from the pivotal Phase III – Study 020 in second-line patients with unresectable or
metastatic melanoma. Yervoy demonstrated a nearly 4 month overall survival benefit.
Now, the focus of Yervoy development is in front-line therapy as well as combination therapies (notably
with PD-1 checkpoint inhibitors). The completed Phase III – 024 study demonstrated a 2.1-month overall
survival benefit in untreated metastatic melanoma patients in combination with dacarbazine (DTIC).
While the survival benefit was fairly small, it appears to be durable, with last update at the 2012 ESMO
conference revealing a survival benefit at four years. The study also revealed significant toxicities,
although they may have been exacerbated by the addition of dacarbazine.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
21
Placebo Treatment
Treatment Description Placebo + DTIC 850 mg/m2 Ipilimumab 10 mg/kg + DTIC 850 mg/m2
Number of Patients 252 250
Median OS (Endpoint=Primary)
9.1000 Months 11.2000 Months
OS - 1 yr 36.4000 % 47.5000 %
OS - 2 yr 17.8000 % 28.8000 %
OS - 3 yr 12.1000 % 21.2000 %
OS - 4 yr 9.6000 % 19.0000 %
Table 9. Updated data from Study 024 at the 2012 ESMO conference showing a survival benefit out to
four years.
Those positive results led to a recent European approval as a front-line treatment in November 2013. However, the company has yet to disclose the timing of any filing in the U.S. It is possible that the company is focusing its resources on the promising combination of Yervoy with its own PD-1 inhibitor, nivolumab; indeed, two Phase II studies (CheckMate 064 and 069) and a Phase III study (CheckMate 067) are underway.
Tremelimumab (AZN)
Tremelimumab is the only other CTLA-4 inhibitor in clinical development and has not met with the same
success as Yervoy, although it is not readily apparent why. Its pivotal Phase III study failed to show a
survival benefit over chemotherapy and development was ultimately suspended.
Tremelimumab has also posted negative data specifically in colorectal cancer, NSCLC, and HCC and been
suspended in numerous other originally-targeted indications. Now, development remains only for
mesothelioma with two Phase II studies ongoing. Neither study has posted data to date, although the
MESOT-TREM-2012 study should be nearing the final data collection date for its primary outcome of
objective reponse.
Comparator Treatment
Treatment Description Chemotherapy Tremelimumab 15mg/kg
Number of Patients 327 328
Median overall survival (ITT) (Endpoint=Primary)
10.7000 Months 11.7600 Months
Overall Survival - Hazard Ratio N/A 1.0400
(P=0.7290)
Complete response rate (ITT) 1.8000 % 1.5000 %
Partial response rate (ITT) 8.3000 % 7.6000 %
Objective response rate (ITT) 10.1000 % 9.1000 %
6-month progression-free survival 14.1000 % 18.6000 %
Table 10. Data from the failed Phase III study of tremelimumab pivotal melanoma study.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
22
KAHR-102 (KAHR Medical)
One other anti-CTLA-4 therapy to note is KAHR-102, currently being developed by the Israeli company,
KAHR Medical. Unlike Yervoy and tremelimumab, which are both antibodies, KAHR-102 is a fusion
protein of CTLA-4 and FasL. The CTLA-4 portion binds to B7 ligands on lymphatic cancer cells which
should block their binding to endogenous CTLA-4 receptors. The FasL portion binds to the Fas receptor
that may be overexpressed on tumor cells and induces their apoptosis (cell death).
Although the drug is still in preclinical development, KAHR expects to initiate Phase I/II clinical trials in
2014.
TIM3 Antibody (Cellerant Therapeutics)
TIM3 (T-cell Immunoglobulin and Mucin domain 3) is another immune checkpoint that functions
similarly to other checkpoints. Cellerant Therapeutics has filed a patent application (#20130022623)
entitled “Antibodies that specifically bind to TIM3.” However, the company has not released any details
about the antibody.
BMS-986016 (BMY)
Along with its CTLA-4 and PD-1 antibodies, BMY is developing an anti-LAG3 antibody and has already
initiated a Phase I dose escalation and cohort expansion study. That study is evaluating the LAG-3
antibody alone and in combination with nivolumab, BMY’s anti-PD-1 antibody in solid tumors.
ImmuTune IMP701 and ImmuFact IMP321(Immutep)
Immutep is a French company developing the anti-LAG3 antibody, ImmuTune IMP701. The antibody is
still in preclinical testing for cancer as well as for chronic infectious diseases, and little information has
been released to date. Immutep had another anti-LAG3 antibody, ImmuTune IMP731, but that drug has
already been suspended.
Immutep is also developing ImmuFact IMP321 which is a soluble form of LAG-3 that binds to MHC
receptors on dendritic cells and leads to their stimulation. IMP321 has already reached clinical trials with
a Phase IIb/III study in breast cancer planned to initiate in 2015.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
23
Dendritic Cell Therapies
Dendritic cells (DCs) are immune cells that mediate innate and adaptive immunity. In general, they are
antigen-presenting cells that process pieces of foreign substances (antigens) and stimulate T-cells to
initiate an immune response against those specific elements. Consequently, the idea of forcing dendritic
cells to present any antigen of choice has been an attractive therapeutic idea.
One major DC therapy, Provenge (see below) achieved a landmark approval as the first DC therapy in
oncology in 2010. Indeed, the development and approval of Provenge can be viewed as the beginning of
the current generation of immunotherapies. However, Provenge has suffered from some inherent
difficulties associated with cellular therapies (e.g. complex production, route of administration), so it
remains to be seen whether other DC therapies can compete commercially against the emergence of
other, more traditional immunotherapies (e.g. small molecule, antibody).
Perhaps one route to commercial success will be their ability to carve out unique therapeutic settings.
Provenge, for example, received approval in a metastatic, but pre-symptomatic/minimally symptomatic
castration-resistant prostate cancer (CRPC) setting which, at the time, was a novel treatment setting
(most other therapies were being evaluated for symptomatic CRPC). While this approach has not been
entirely successful for Provenge, in part due to the untimely arrival of traditional drug competitors, it
could be a route with other therapies in the right competitive landscape.
Another approach may be in the development of allogeneic (non-patient specific) DC treatments that
would allow off-the-shelf convenience. These allogeneic therapies, however, may suffer from adverse
events related to rejection of foreign cells and perhaps lower efficacy. Thus, they might have more
success as treatments for aggressive hematologic malignancies for which patients are managed by bone
marrow transplant specialists who are already familiar with these issues.
Other Dendritic Cell Therapies
Despite the market struggles of Provenge, numerous other similar dendritic cell therapies are still in
development given the potential efficacy of these therapies. Some of these therapies are remarkably
similar to Provenge while others are slightly less logistically complex and may resemble more of an off-
the-shelf type therapy.
Note that many general immune stimulators affect dendritic cells indirectly, for example by targeting
cytokines that signal to dendritic cells and are not that novel. The table below only lists treatments
involving direct manipulation of DCs.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
24
Table 13. Dendritic cell therapies (involving direct manipulation of cells).

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
25
Provenge (sipuleucel-T, DNDN)
Provenge is a complex therapy by which autologous dendritic cells from patients are processed and
antigen loaded with prostatic acid phosphatase (PAP) fused to GMCSF. PAP is highly expressed prostate
cancer cells, and Provenge is designed to stimulate an immune response against PAP.
The clinical and regulatory success of Provenge has been well-documented. In addition to laying the
foundation for a new generation of immunotherapies, Provenge also led a wave of new prostate cancer
therapies providing survival benefits in the castration-resistant prostate cancer (CRPC) setting. In doing
so, the developmental path foreshadowed some common issues to immunotherapies, especially the
demonstration of an overall survival (OS) benefit without a progression-free survival (PFS) benefit.
Presumably, this is common to immunotherapies due to the lag time to develop an immune response.
Unlike its regulatory success, Provenge has not met with similar commercial success despite its
developmental lead over its competitors. In 2013, Provenge garnered only $265m in the U.S. market
compared to the blockbuster non-immunotherapies Zytiga (JNJ) and Xtandi (Astellas) which earned
$749m and $360m respectively, with projections for each topping $1b in the next few years. Provenge
has had trouble gaining traction in part due to its logistically complicated dosing scheme which requires
the collection and shipment of blood samples from patients to a central processing facility and then back
to the physician for infusion into the patient on three separate occasions. This dosing also requires the
establishment of infusion centers which are not as prevalent in smaller community urology settings.
The other major element that has hampered Provenge uptake is its pricing scheme. Because treatment
is only three infusions over six weeks, the entire $93,000 cost of the therapy is essentially covered
upfront by physicians who must assume the risk of subsequent reimbursement. This reimbursement
issue on top of the need for infusion centers has greatly hampered the adoption of Provenge among
smaller community urologists. And with the migration of Zytiga and Xtandi into the pre-chemotherapy
setting Provenge may never achieve a larger market share.
AGS-003 (ARGS)
AGS-003 uses dendritic cells loaded with RNA amplified from a patient’s tumor to generate tumor
specific antigens. A Phase II study in combination with Sunitinib in renal cell cancer patients
demonstrated reasonable survival results, and suggested that efficacy may be higher in intermediate
risk patients, although this result could also likely be a function of the small sample size.
The Phase III – ADAPT study in renal cell cancer (RCC) is currently underway in a similar patient
population to the Phase II study and is expected to complete enrollment in the second half of 2014.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
26
Treatment Treatment Treatment
Treatment Description AGS-003 + Sunitinib AGS-003 + Sunitinib Poor Risk Patients
AGS-003 + Sunitinib Intermediate Risk Patients
Number of Patients 21 10 11
Median Overall Survival 39.5 Months 9.1000 Months N/A
Patients Still Living > 4 Years Following Study Registration 33.0000 % N/A N/A
Median Progression Free Survival 11.2000 Months 5.8000 Months 19.4000 Months
Table 11. Phase II results of AGS-003 in combination with Sunitinib.
DCP-001 (DCPrime)
Unlike the other DC therapies, DCP-001 is an allogeneic therapy that does not require additional antigen
loading, and thus has the potential to be an off-the-shelf product. DCP-001 is based on DCOne, a
proprietary immortalized dendritic cell precursor cell line derived from a single individual with acute
myeloid leukemia (AML). The precursor cells are stimulated through an undisclosed process to
differentiate into functional DC that express multiple AML-specific antigens.
Currently, development is proceeding outside the U.S. with an ongoing Phase I/II study in the
Netherlands. Some positive qualitative information has been disclosed from the study (DCOne-1), but no
quantitative results. A Phase II study could begin in 2014.
DC-Vax (NWBO)
Northwest Biotherapeutics is developing a dendritic cell therapy (DCAX) that is unique in using a
spectrum of antigens derived from the lysate from the patients surgically resected tumor tissue rather
than priming dendritic cells with a single antigen (e.g. Provenge). Theoretically, this has the advantage of
both targeting multiple antigens and creating more personalized therapies that are matched to the
specific tumor expression profile of each patient. However, this technology could also have drawbacks
including a more variable response as some patients may have a few more highly expressed antigens
that stimulate a stronger immune response. The less-specific nature of the therapy could also lead to a
more variable safety profile as some preparations could generate immune responses against antigens
present on normal cells.
Because of the adaptability of the DCVAX platform, development is proceeding across a broad range of
tumor types (note: for easier tracking, BioMedTracker lists DCVax with a separate drug name for each of
its indications, e.g. DCVAX-Brain and DCVAX-Colon). Positive early data have been observed in glioma
brain cancer with DCVax brain nearly doubling overall survival over historical OS in a Phase I study of
newly diganosed GBM (with one one patient exceeding 10-year survival compared to a historical OS of
15 months). Of course, these are early data but prompted a jump directly to a pivotal Phase III study
which is expected to report top-line data by the end of 2014.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
27
Recently, Northwest also announced that it had already obtained a special hospital exemption to allow
drug sales in Germany, although this would seem to be a minor achievement relative to the impact of
the impending pivotal study data.
Chimeric Antigen Receptor T-Cell (CAR-T) Therapies
In addition to the manipulation of dendritic cells, another emerging approach is the application of gene
therapy technology in the modification of T-cells themselves to directly recognize tumor antigens. This
adoptive cell therapy (ACT) approach modifies T-cells to express surface receptors called chimeric
antigen receptors (CARs) that recognize antigens (motifs) on tumor cells.
CARs typically consist of a monoclonal antibody fragment, called a single-chain variable fragment (scFv),
that presents on the outside of T-cell membranes, and is fused to intraceullarly-facing stimulatory
molecules. The scFv portion recognizes the tumor target. Upon binding, the intracellular stimulatory
portions initiate a signal to activate the T cell.
Figure 14. Adapted from Sadelain et al., Nat. Rev. Cancer (2003).
As with dendritic cell therapies, CAR-T therapies require a fairly complex production and patient-
unfriendly ROA. Ultimately, though their success will depend on efficacy. To date, CAR-T therapies have
shown the most promise in hematologic cancers, especially B-cell malignancies like ALL and CLL. They
have also caused some concerning side effects, especially cytokine-release syndrome due to the
injection of cytokine-releasing T cells. Cytokine-release syndrome is characterized by high fevers and

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
28
sudden drops in blood pressure, and patients often require aggressive support in an intensive care unit
setting. It may be possible to counteract the massive cytokine release with IL-6-receptor blocking
antibodies like Actemra (tocilizumab, Roche), but it is unclear whether that would interfere with long-
term CAR T-cell function.
CTL019 (NVS)
CTL019 consists of CAR-T cells targeted to CD19, a common antigen on the surface of B-cells and current
target of more traditional antibody therapies in development as well. Novartis licensed the drug and
other CART therapies from the University of Pennsylvania. However, Penn and Novartis are now
engaged in a patent dispute over the CAR technology with Juno and St. Jude Children’s Hospital (see
Juno below) that could impact the development of CTL019.
In CLL, top-line results from the Phase II, dose-optimization study of CTL019 for CLL were released at the
2013 ASH meeting. Those early Phase II data included results from 10 patients who were treated with
CTL019. A total of 4 patients demonstrated a response, with 2 achieving CR and 2 achieving PR, though
the median follow-up was only 3 months. Updated results from a Phase I study in CLL were also
presented at that ASH. When those patients from the Phase I study are included, a total of 47%
responded to therapy (CR + PR), and transduced cells were still present in patients for up to 3 years.
In ALL, a recently published report in Science Translational Medicine (Vol. 6, 224, p. 224ra25) revealed
an 88% complete response rate in 16 B-cell ALL patients in a Phase I study. Despite the overall positive
signals, the ALL studies have also shown that patients who responded could still relapse with non-CD19-
expressing neoplasms. Furthermore, some patients have B cell aplasia requiring IVIG treatment –
perhaps not a scalable way to treat all relapsed leukemia patients, but possibly a treatment of last
resort.
Chimeric Antigen Receptors (CAR) Program (Juno)
Juno is a recently launched company formed from a partnership between the Fred Hutchinson Cancer
Research Center, Memorial Sloan-Kettering Cancer Center, and Seattle Children’s Research Institute. The
company made headlines in December 2013 when it secured a large initial Series A investment of
$120M with its launch.
Juno has two potential immunotherapy programs: one involving Chimeric Antigen Receptors (CARs) and
one involving T-Cell Receptors (TCRs). While the CART program appears to be similar to other CART
therapies in development, the TCR program is unique in targeting intracellelular tumor targets. The
program is developing T cells with modified TCR sequences to bind HLA to generate high-affinity TCRs.
Juno is initially developing high-affinity TCRs that interact with HLA-A2, which is common in half of the
U.S. population.
Despite the short history of the company, Juno is already entangled in a complex patent dispute with
Novartis. The disagreement originated as a charge by St. Jude Children’s Hospital that its patented anti-

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
29
CD19 CAR technology (patent No. 8,399,645) was shared with University of Pennsylvania researcher, Dr.
Carl June, under a materials transfer agreement (MTA), but U. Penn then tried to commercialize the
materials including a partnership with Novartis. Now, both Juno and Novartis have entered the litigation
to back their respective partners, and the outcome could have significant consequences on the race to
develop a CART therapy.
Chimeric Antigen Receptor (CAR) T-cell Program (BLUE/CELG)
bluebird bio (BLUE) entered into a collaboration with Celgene in early 2013 to develop CAR T-cell
therapies in oncology. Celgene has an option to license any products resulting from the collaboration
after the completion of a Phase I clinical study for each such product. bluebird bio will be responsible for
research and development activity through Phase I studies.
Celgene has also entered into a separate strategic collaboration in the CAR T-cell field with the Center
for Cell and Gene Therapy at Baylor College of Medicine, Texas Children’s Hospital and The Methodist
Hospital, Houston.
Financial terms of the agreement include an upfront payment and up to $225 million per product in
potential option fees and clinical and regulatory milestones. bluebird bio also has the right to participate
in the development and commercialization of any licensed products resulting from the collaboration
through a 50/50 co-development and profit share in the United States in exchange for a reduction of
milestones. Royalties would also be paid in regions where there is no profit share including in the United
States if bluebird bio declines to exercise their co-development and profit sharing rights.
UCART19 (Cellectis)
Cellectis is a French company specializing in genome manipulation via its nuclease technology
(meganucleases) and partners primarily in the discovery phase of research. However, the company is
also developing its own anti-CD19 CAR T-cell therapy similar to Novartis’ CTL019. Unlike CTL019,
however, UCART19 is an allogeneic therapy (not from same patient) which could allow for an off-the-
shelf CAR-T treatment. A press release from the company suggested that UCART19 performed as well as
traditional CAR T-cells in a mouse leukemia model although virtually no details were provided.
Recently, Cellectis entered a partnership with Servier. Cellectis will take UCART19 through the end of
Phase I studies after which Servier has the option to license the drug and take responsibility for further
clinical development.
Chimeric Immune Receptor (CIR) T cells (Abramson Cancer Center)
In addition to CTL019 which was licensed to Novartis, the Abramson Cancer Center at the University of
Pennsylvania is developing another type of CART therapy, termed chimeric immune receptor (CIR) T-cell

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
30
therapy, in which T-cells are transfected with mRNA to direct the transient expression of the CAR.
Currently, a Phase I study has initiated (NCT01355965) evaluating a CIRT with a CIR directed against
mesothelin for the treatment of mesothelioma. It should be noted, though, that mesothelin is highly
expressed in several other tumor types including pancreatic, ovarian, and lung.
CD19 eACT CAR-T Therapy (Kite Pharma)
At the 2013 ASH meeting, data were presented from a Phase I/IIa study being conducted by the National
Cancer Institute evaluating Kite Pharma’s CD19-directed CART therapy in advanced B-cell malignancies.
While a very small sample size, the trial did show a high response rate across B-cell malignancies
including PMBCL and DLBCL.
Treatment Treatment
Treatment Description eACT
Patients with PMBCL or DLBCL eACT
All Advanced B-cell Malignancies
Number of Patients 9 N/A
Number of Evaluable Patients 7 13
Overall Response (OR) 6 12
Complete Response (CR) 3 6
Partial Response (PR) 3 6
Table 12. Phase I/IIa results presented at the 2013 ASH showing a high response rate for Kite Pharma’s
CART therapy.
Autologous CAR-T Program for Breast Cancer (Adaptimmune)
Adaptimmune recently announced that it was awarded a grant of £2.1 million from the Biomedical
Catalyst Fund, managed by the UK’s innovation agency the Technology Strategy Board and the Medical
Research Council. The award will expedite the development of Adaptimmune’s second engineered T cell
therapy program with a new T cell receptor (TCR) into the clinic (UK) in triple negative breast cancer. The
award will support preclinical testing and regulatory approval for an initial pilot trial with a new TCR
targeting an undisclosed protein found to be highly expressed in some forms of breast cancer and other
cancer types. The trial is planned to start in 2015.
Cancer Vaccines
Somewhat like traditional vaccines, cancer vaccines induce an immune response by presenting antigens
specific to tumor cells. Because many general immune therapies may stimulate similar immune

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
31
responses (simply due to cell lysis, for example), the cancer vaccine term is fairly imprecise.
Nevertheless, we have listed some drugs below that are typically considered vaccines (dendritic cell
therapies are also considered vaccines, but are detailed separately above).
Table 15. Cancer vaccines in development. Note that many therapies that lyse tumor cells as a
secondary mechanism are not listed.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
32
HyperAcute (NLNK)
The HyperAcute platform is based on tumor-specific, whole cancer cells that have been genetically
modified to express alpha-gal. Alpha-gal is a carbohydrate expressed on the cell surface and is predicted
to facilitate the lysing of tumor cells via complement-mediated lysis and lead to a subsequent immune
response against the array of tumor epitopes from that specific tumor type. HyperAcute therapies use
allogeneic (not from individual patient) cells, so this platform has the advantage of potentially being an
off-the-shelf product. However, it would also seem to suffer from a general lack of specificity that could
lead to unexpected side effects from immune responses against an entire cell lysate.
Currently, HyperAcute cell therapies are being developed for a range of tumor types, with develoment
most advanced in lung, melanoma, and pancreatic cancers. Interesting data were presented at the 2013
ASCO from a Phase II pancreatic cancer study suggesting that HyperAcute Pancreas may work better in
patients with elevated levels of anti-mesothelin antibodies which could be a potential biomarker.
However, the Phase III IMPRESS study in pancreatic cancer patients did not stratify for mesothelin
antibody levels.
Treatment Treatment Treatment
Treatment Description algenpantucel-L plus standard-
of-care adjuvant therapy
algenpantucel-L plus standard-of-care adjuvant therapy
patients with elevated levels of anti-mesothelin antibodies
algenpantucel-L plus standard-of-care adjuvant therapy
patients without elevated levels of anti-mesothelin antibodies
Number of Patients 69 N/A N/A
Disease Free Survival One Year (Endpoint=Primary)
62 % N/A N/A
Disease Free Survival Three Years (Endpoint=Secondary)
26 % N/A N/A
Overall Survival One Year (Endpoint=Secondary)
86 % N/A N/A
Overall Survival Three Years (Endpoint=Secondary)
39 % N/A N/A
Median Overall Survival (Endpoint=Secondary)
N/A 42 Months 20 Months
Table 13. HyperAcute Phase II pancreatic cancer data from ASCO 2013.
MAGE-A3 Antigen Specific Cancer Immunotherapeutic (GSK)
This therapy is based on the introduction of a recombinant tumor-specific antigen, melanoma-
associated antigen (MAGE-A3), in combination with a proprietary adjuvant system. So far, the data from

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
33
both NSCLC and melanoma trials has been fairly negative, including a recent disclosure that the Phase III
– MAGRIT study in NSCLC failed to meet two of its co-primary endpoints.
Difference Between Treatment and
Placebo Difference Between Treatment and Placebo
Treatment Description
MAGE-A3 ASCI vs. Placebo MAGE-A3 positive population
MAGE-A3 ASCI vs. Placebo MAGE-A3-positive patients who did not receive
chemotherapy
Number of Patients 2,312 N/A
Disease free survival (Endpoint=Primary)
N/A (P>0.005)
N/A (P>0.005)
Table 14. Phase III data showing the MAGRIT study in NSCLC failed to meet two primary endpoints.
Now, in both NSCLC and melanoma, the fate of MAGE-A3 rests on the ability to develop a biomarker
that can prospectively identify patients likely to benefit from the therapy. MAGRIT does have a third
prespecified endpoint stratifying patients using a gene signature for which details have not been
disclosed. Final results from MAGRIT are expected in 2015.
Advaxis
Advaxis is developing cancer vaccines based on the bacterium, Listeria, which is engineered to express a
fusion of various proteins with LLO sequences that cause rapid proteolysis of the fused protein to
generate an immune response.
Its lead drug, ADXS-HPV has posted somewhat unclear Phase II results in cervical cancer, although top-
line results are expected from a Phase II investigator-initiated trial (GOG/NCI) at the upcoming ASCO
2014. The effect of ADXS-HPV on 18-month survival was modest in this advanced, pre-treated patient
population. Without a comparator arm, it is difficult to determine whether the survival and stable
disease rates are favorable compared to standard of care. Since survival was not improved in patients
treated with ADXS-HPV+cisplatin vs. ADXS-HPV alone, this immunostimulatory drug has promise as a
standalone therapy, especially since the safety/tolerability profile of ADXS-HPV is favorable. Thus, ADXS-
HPV may find initial use in patients who cannot tolerate cisplatin treatment or are platinum resistant.
Advaxis believes that higher doses and more cycles of ADXS-HPV may provide even better results in
subsequent trials; patients in this India trial were given 1 billion CFUs in each vaccine. Since the highest
dose planned for the US, dose-finding Phase II study was 1 billion CFUs, it is unclear what these higher-
dose plans would entail. If ADXS-HPV has positive US trial results, Phase III trials may involve multiple
courses of treatment beyond the 12-week paradigm.
The favorable safety profile of ADXS-HPV is a positive for patients in this extremely difficult-to-treat
population, but the survival results in this trial are questionable as far as efficacy is concerned.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
34
All Treatment
Treatment Description ADXS-HPV +/- Cisplatin
Number of Patients 110
Number of Evaluable Patients 110
Overall survival (At 18 months) (Endpoint=Primary)
28 %
Stable disease (>3 months) 35 Patients
Disease control rate 43 %
Table 15. Results from Phase II study of cervical cancer patients in India.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
35
IDO Inhibitors
Indoleamine 2,3-dioxygenase (IDO) is a novel oncology pathway being targeted by a handful of drugs in
development. IDO is an enzyme that degrades the essential amino acid tryptophan, and some tumors
overexpress IDO resulting in tryptophan depletion in the local microenvironment leading to subsequent
T-cell inactivation.
Like other immunotherapies, combination therapies may hold the most promise for IDO, and some have
suggested a unique interaction with CTLA-4. Indeed, a Phase I/II combination study of INCB24360 with
Yervoy (ipilimumab, BMY) is ongoing in the treatment of melanoma.
Indoximod and NLG-919 (NLNK)
Indoximod is a small molecule inhibitor of IDO in Phase II development for breast cancer, and in Phase
I/II for brain cancer, melanoma, and pancreatic cancer. Two IDO variants exist, and there has been some
indication that indoximod is more of an IDO2 inhibitor than IDO1 suggesting that IDO inhibition may not
be the sole mechanism of action of the drug (although potentially different roles of each IDO variant are
not entirely clear). Regardless, no clinical data have been released in any indication, so a Phase II breast
cancer study is being closely watched for its anticipated top-line data release expected in Q4 2014/Q1
2015.
NLG-919 is another IDO inhibitor from NewLink that has just entered Phase I clinical trials. Fairly minor
preclinical data were presented at the 2014 AACR meeting showing signs of synergy with NLG-919 or
indoximod in combination with PD-1 therapies in a mouse melanoma model.
INCB24360 (INCY)
Some positive data have already been released for this small molecule IDO inhibitor which is in Phase II
trials for ovarian cancer and Phase I/II development for melanoma. An investigator-initiated study has
also begun in myelodysplastic syndromes. At the 2013 ASCO meeting, positive signals were reported in
colorectal cancer patients in a Phase I study, but the company has not revealed any plans to pursue
development in that indication.
Perhaps most important for INCB24360 is an ongoing Phase I/II study of the drug in combination with
the CTLA-4 checkpoint inhibitor, ipilimumab. Top-line data from that study is expected to be presented
at the 2014 ASCO meeting.
dCellVax (BMSN)
dCellVax is a dendritic cell (DC) therapy in which DCs are genetically modified to inhibit IDO signaling.
The precise molecular mechanism of IDO inhibition has not been disclosed, and the therapy is still in
preclinical development. An IND is expected soon and development will likely be in breast cancer
initially.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
36
Miscellaneous Immunotherapies
Contego (LBIO)
Contego is an autologous cell therapy containing tumor-infiltrating lymphocytes (TILs) obtained from a
patient’s tumor (melanoma currently). These extracted TILs are expanded in vitro and then infused back
into the patient.
Data from a Phase II study in melanoma were reported at the recent 2014 AACR meeting showing a
reasonable ORR in late-stage metastatic melanoma patients.
All Treatment Treatment Treatment
Treatment Description Tumor Infiltrating Lymphocytes
(TILs) All Patients
Tumor Infiltrating Lymphocytes (TILs)
Ipilimumab Refractory Patients
Tumor Infiltrating Lymphocytes (TILs)
Pts Previously Progressed on anti-PD1
Number of Patients 101 45 10
Objective Response Rate (ORR)
54 % 42 % 50 %
Complete Response (CR) 11 Patients N/A N/A
Partial Response (PR) 44 Patients N/A N/A
Table 16. Phase II data presented at the 2014 AACR meeting.
TG4010 (Transgene)
TG4010 is a recombinant vaccinia virus vector directing expression of human MUC1 antigen and the
human cytokine, IL-2. Although normally expressed on the surface of epithelial cells, some tumors
overexpress MUC1 and may cause them to be more sensitive to an anti-MUC1 immune response.
Data from the Phase IIb portion of the Phase IIb/III – TIME study for NSCLC were released in January and
did not show a statistically significant PFS benefit using the ULN threshold. However, the company did
explore a potential biomarker to stratify patients.
Ultimately, few quantitative details were actually released to support the company's stance that these
results are positive enough to support the start of the Phase III portion of the study. As an exploratory
part of the study to find the correct level of their biomarker (TrPAL), the Phase IIb portion could be
viewed as successful. However, the company provided only vague statements on the "clinically
meaningful improvements" in PFS, which also suggest the lack of statistically significant benefit by either
biomarker measure (ULN or the quartile method). The post-hoc subgroup analysis for the non-
squamous, bevacizumab-naive patients is also somewhat dubious.
Recently, Novartis announced that it would not exercise its option to continue partnering on the drug,
returning all rights to Transgene. Transgene officials are expressing confidence that a partner can be

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
37
found by the end of 2014 allowing progression the Phase III portion of the trial. At minimum, more data
could be available at ESMO in September 2014 to further assess the potential of the drug in Phase III.
Treatment
Treatment Description TG4010
ULN Threshold
Improvement in PFS (Endpoint=Primary)
N/A (P>0.05)
Table 17. Phase IIb/III – TIME study in NSCLC did not show a PFS benefit using ULN threshold.
Bavituximab (PPHM)
Bavituximab is an antibody against phosphatidylserine (PS), a component of cell membranes that is
typically on the cytosolic face of membranes but is flipped to the extracellular surface of apoptosing or
stressed cells. Peregrine (PPHM) originally touted a mechanism for the drug in which tumors had more
exposed PS and PS could thus be a specific cancer target.
However, following mixed results in NSCLC and pancreatic cancer, including a high-profile discrepency in
patient records in its Phase IIb lung cancer study, the company has struggled to maintain confidence in
its lead drug candidate. It has since trumpeted a new immunotherapy mechanism of action for
bavituximab in which exposed PS actively suppresses immune signaling (much like a checkpoint
inhibitor), and bavituximab blocks PS to allow an anti-tumor immune response. While this PS
“checkpoint” may be valid, the change in proposed drug mechanism late in its development is curious
and warrants further mechanistic validation. One possibility that PS blockade causes some measurable
immune response, but probably not much different from immune responses that are associated with
many older oncology treatments.
Nevertheless, a Phase III study in combination with docetaxel has commenced. In the similarly designed
Phase IIb study, the combination showed a non-significant trend towards an OS improvement, but the
data were not as convincing as previously released data which showed a 13.1 vs 5.6 month increase OS.
Given a discrepancy in the placebo arm which led to an adjustment narrowing the efficacy gap, we are
less confident in the observed benefit.
Comparator Treatment
Treatment Description Docetaxel Bavituximab 3 mg/kg + Docetaxel
Median Overall Survival (Endpoint=Secondary)
7.3000 Months 11.7000 Months
(P=0.2170)
Table 18. Phase IIb OS data of bavituximab in NSCLC.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
38
T-VEC (talimogene laherparepvec, AMGN)
T-VEC is a virus injected directly into tumors that both selectively replicates in tumor cells and also
expresses the immune stimulant, GM-CSF. Positive melanoma interim results were released from the
OPTiM study at the last ASCO. The key issue from that presentation was the disclosure of overall survival
data which were not yet mature at the interim analysis and were not significant over the GM-CSF
comparator but did show a numerical advantage (23.3 mo. vs 19.0 mo. comparator). Additionally, the
Kaplan-Meier curves showed a late separation (around 15 mo.) which is actually consistent with the
predictions of an immunotherapy that is expected to have a relatively slow therapeutic response but
long durability (as is evidenced by the DRR). If the curves continue along the same trajectory, the study
is likely to show an overall survival benefit at least as large as Yervoy (ipilimumab, BMY). The study also
showed a significant benefit in time to treatment failure which, in this case, is really standard PFS (as
pointed out by a post-presentation discussant).
A fairly minor update since ASCO did not provide new OS numbers for the overall study population, but
a new subgroup analysis suggests that patients with less advanced disease or receiving T-VEC as a first-
line treatment experienced an even greater survival benefit. However, we caution against placing too
much emphasis on these subgroup results as these strong survival numbers are likely to be at least
partially the result of the weak CM-CSF comparator (which was highlighted as an issue at ASCO). It is
unlikely that T-VEC would fare so well in early or first-line therapy against a more effective comparator
such as DTIC.
In the end, we will have to await more mature survival data which are expected in the first half of 2014.
Even with a positive OS result, T-VEC does not necessarily have a clear path to approval. One major issue
for regulators could be the GM-CSF comparator rather than a more widely used therapy like DTIC.
Additionally, the study was necessarily open label given the unique nature of the T-VEC viral therapy
which must be injected intratumorally. Safety was satisfactory, but there were 10 deaths in the
treatment arm (although none were deemed treatment related).
Even if T-VEC does win FDA approval, the real issue for T-VEC could be its ability to compete against
already-approved therapies (like Yervoy) as well as the slew of anti-PD (Programmed Death) inhibitors
rapidly moving through clinical trials. The post-presentation discussant (Dr. Kim Margolin, Seattle Cancer
Care Alliance) went as far as to declare that T-VEC “is not ready for primetime” given its limitations, such
as injection only to accessible tumors (although there was an effect on distal tumors as well).
In the end, we continue to believe that T-VEC has an above average chance of getting approved if it
eventually meets its OS endpoint.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
39
Comparator Treatment
Difference Between Treatment and
Comparator
Difference Between Treatment and
Comparator
Difference Between Treatment and
Comparator
Treatment Description
GM-CSF Investigator
Assessed
Talimogene Laherparepvec
Investigator Assessed
Talimogene Laherparepvec vs. GM-
CSF All Patients
Talimogene Laherparepvec vs. GM-
CSF Pts with Stage III or IV
M1a Disease
Talimogene Laherparepvec vs. GM-
CSF First-Line Treatment
Median Overall Survival
19 Months 23.3 Months N/A N/A N/A
Hazard Ratio: Median Overall Survival
N/A N/A 0.79
(P=0.0746) 0.56 0.49
Hazard Ratio: Quality of Life Deterioration
N/A N/A 0.68
(P=0.0005) N/A N/A
Deterioration-Free Probability at 3 Months
22 % 42 % N/A N/A N/A
Table 19. Updated Phase III – OPTiM data for T-VEC in melanoma.

Cancer Immunotherapies 2014
QUESTIONS? EMAIL [email protected]
FOR OUR DISCLOSURES, PLEASE SEE BIOMEDTRACKER’s RESEARCH STANDARDS
40
Other BioMedTracker reports that may be of interest:
2014 ASCO Planner
This pre-meeting planner lists relevant talks and posters based on
presentation titles that were released on April 21, 2014. Included
with purchase is a supplementary Excel version that lets you view
sessions by Drug, Company, Authors and more.
View BioMedTracker’s 2014 ASCO Planner for more information
and a free look at some of the meeting highlights.
Ovarian Cancer Pulse Survey
A 5-question survey of 18 medical oncologists in the US about
current prescribing practices for ovarian cancer treatments and
diagnostics that can be used to gauge interest in new drug
candidates for the treatment of ovarian cancer.
To see drugs, drug candidates, and diagnostic techniques discussed,
view BioMedTracker’s Ovarian Cancer Pulse Survey.
Breast Cancer KOL Insight Interview
A Key Opinion Leader (KOL) interview with a medical oncologist in
the New York metropolitan area regarding breast cancer.
For a look at the free highlights and information on purchasing the
full transcript, visit BioMedTracker’s Breast Cancer KOL Insight
Interview