
Eye of the Eagle - The Carter Center | Waging Peace, Fighting Disease & Building … ·...
12
January 2006 Volume 7, Number 1 THE CARTER CENTER Eye of the Eagle Nigeria Hosts Fifth Annual Health Program Review President Carter Visits Ethiopia to See Trachoma Program Success continued on page 6 continued on page 2 What’s Inside T he fifth annual review of all Carter Center-assisted health programs in Nigeria took place Sept. 5–7, 2005, in Abuja. The health programs represented were the Guinea Worm Eradication Program, the River Blindness Program, the Trachoma Control Program, the Lymphatic Filariasis Elimination Program, and the Schistosomiasis Control Program. Some of the key updates presented in the three-day meeting included the following: Through September 2005, only 116 cases of Guinea worm disease had been reported in Nigeria, which is a reduction of 70 percent compared to the same period in 2004. During the same period, the River Blindness Program had assisted the Ministry of Health in providing health education to and treating nearly 3.3 million people with Mectizan ® (donated by Merck & Co.) in nine states, which is 68 percent of the 2005 ultimate treatment goal of 4.8 million people. The nine states contributed the equivalent of $125,000 USD to the program, led by Ebonyi (5 million of the Lions Club, The Carter Center, and the Ethiopian government to elim- inating blinding trachoma in Ethiopia. Before heading to Mosebo, the delegation was briefed on the Carter Center health programs by Teshome Gebre, country representative for The Carter Center in Addis Ababa, Ethiopia. In addition to President and Mrs. Carter, the delegation also included James Wagner, president of Emory University, and his wife, Debbie; John Moores, chairman of the Carter Center Board of Trustees; Richard Blum, member of the Carter Center Board of Trustees; John Hardman, executive director of The Carter Center; Joseph Feczko, vice president of Pfizer; Jacob Kumaresan, president of built. They visited families who constructed household latrines out of readily available materials and met children who demonstrated how their household latrines worked. Villagers in the assisted area of Amhara have built a total of 90,552 household latrines in 2004 and 122,832 and counting in 2005. A group of men and women who had received eyelid surgery welcomed the delegation by holding candles which represented their freedom from the misery of trichiasis. The historic visit showed the strong commitment I n September 2005, President and Mrs. Carter and a delegation of officials visited Ethiopia to see the accomplishments of the trachoma con- trol program in the Amhara region of the country. In the trachoma-endemic village of Mosebo, the delegation saw several households that have benefited from the Lions/Carter Center-supported latrine promotion activities, a virtual latrine revolution due to the fast pace at which household latrines have been Program Transfer in Sudan . . . . . . . . . . 3 Nigeria Promotes Cleanup . . . . . . . . . . 3 Mayor Aims for Latrines . . . . . . . . . . . . 4 Latrine Access in Ghana . . . . . . . . . . . 5 IACO 2005 Review . . . . . . . . . . . . . . . 8 Treatment in Mexico . . . . . . . . . . . . . 10 Drug Safety Study . . . . . . . . . . . . . . . . 11 Bed Net Recommendation . . . . . . . . . 12
Transcript of Eye of the Eagle - The Carter Center | Waging Peace, Fighting Disease & Building … ·...
January 2006Volume 7, Number 1 THE CARTER CENTER
Eye of the Eagle
Nigeria Hosts Fifth AnnualHealth Program Review
President Carter Visits Ethiopia toSee Trachoma Program Success
continued on page 6
continued on page 2What’s Inside
The fifth annual review of allCarter Center-assisted healthprograms in Nigeria took place
Sept. 5–7, 2005, in Abuja. The healthprograms represented were the GuineaWorm Eradication Program, the RiverBlindness Program, the TrachomaControl Program, the LymphaticFilariasis Elimination Program, and theSchistosomiasis Control Program.
Some of the key updates presentedin the three-day meeting included the following:
Through September 2005, only116 cases of Guinea worm disease had
been reported in Nigeria, which is areduction of 70 percent compared tothe same period in 2004.
During the same period, the River Blindness Program had assistedthe Ministry of Health in providing health education to and treating nearly3.3 million people with Mectizan®
(donated by Merck & Co.) in ninestates, which is 68 percent of the 2005ultimate treatment goal of 4.8 millionpeople. The nine states contributed theequivalent of $125,000 USD to theprogram, led by Ebonyi (5 million
of the Lions Club, The Carter Center,and the Ethiopian government to elim-inating blinding trachoma in Ethiopia.
Before heading to Mosebo, the delegation was briefed on the CarterCenter health programs by TeshomeGebre, country representative for The Carter Center in Addis Ababa,Ethiopia. In addition to President and Mrs. Carter, the delegation alsoincluded James Wagner, president ofEmory University, and his wife, Debbie;John Moores, chairman of the CarterCenter Board of Trustees; RichardBlum, member of the Carter CenterBoard of Trustees; John Hardman,executive director of The CarterCenter; Joseph Feczko, vice presidentof Pfizer; Jacob Kumaresan, president of
built. They visited families who constructed household latrines out of readily available materials and metchildren who demonstrated how theirhousehold latrines worked. Villagers in the assisted area of Amhara havebuilt a total of 90,552 householdlatrines in 2004 and 122,832 andcounting in 2005.
A group of men and women whohad received eyelid surgery welcomedthe delegation by holding candleswhich represented their freedom fromthe misery of trichiasis. The historicvisit showed the strong commitment
In September 2005, President andMrs. Carter and a delegation of officials visited Ethiopia to see the
accomplishments of the trachoma con-trol program in the Amhara region ofthe country. In the trachoma-endemic village of Mosebo, the delegation sawseveral households that have benefitedfrom the Lions/Carter Center-supportedlatrine promotion activities, a virtuallatrine revolution due to the fast paceat which household latrines have been
Program Transfer in Sudan . . . . . . . . . . 3
Nigeria Promotes Cleanup . . . . . . . . . . 3
Mayor Aims for Latrines . . . . . . . . . . . . 4
Latrine Access in Ghana . . . . . . . . . . . 5
IACO 2005 Review . . . . . . . . . . . . . . . 8
Treatment in Mexico . . . . . . . . . . . . . 10
Drug Safety Study . . . . . . . . . . . . . . . . 11
Bed Net Recommendation . . . . . . . . . 12
Trachoma
2
Ethiopia Visitcontinued from page 1
Waging Peace. Fighting Disease. Building Hope.
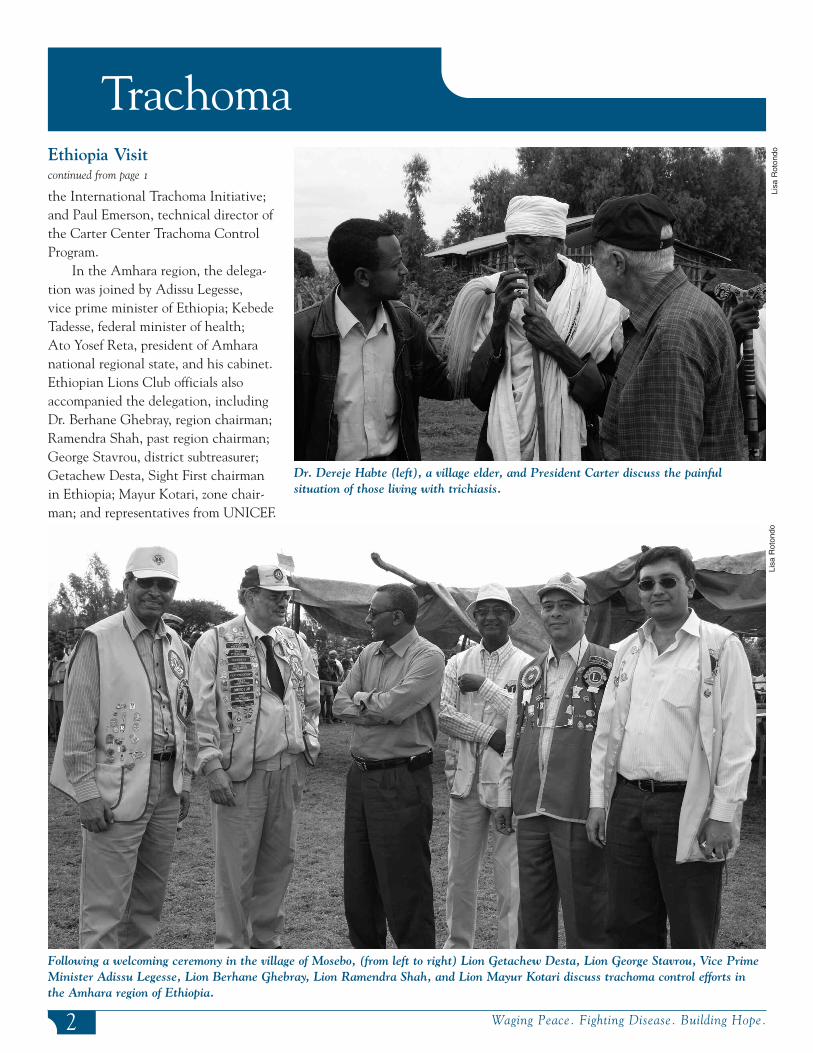
Dr. Dereje Habte (left), a village elder, and President Carter discuss the painful situation of those living with trichiasis.
Following a welcoming ceremony in the village of Mosebo, (from left to right) Lion Getachew Desta, Lion George Stavrou, Vice PrimeMinister Adissu Legesse, Lion Berhane Ghebray, Lion Ramendra Shah, and Lion Mayur Kotari discuss trachoma control efforts inthe Amhara region of Ethiopia.
Lisa
Rot
ondo
Lisa
Rot
ondo
the International Trachoma Initiative;and Paul Emerson, technical director ofthe Carter Center Trachoma ControlProgram.
In the Amhara region, the delega-tion was joined by Adissu Legesse, vice prime minister of Ethiopia; KebedeTadesse, federal minister of health; Ato Yosef Reta, president of Amharanational regional state, and his cabinet.Ethiopian Lions Club officials alsoaccompanied the delegation, includingDr. Berhane Ghebray, region chairman;Ramendra Shah, past region chairman;George Stavrou, district subtreasurer;Getachew Desta, Sight First chairmanin Ethiopia; Mayur Kotari, zone chair-man; and representatives from UNICEF.

Trachoma
3www.cartercenter.org
tools; participants use their own rakes,brushes, and machetes.
The scale of the benefit surprisesmany people who have individuallycontributed only a couple of hours ofwork. Community members are proudof the appearance of their villages, andthe reduction in flies and bad odors isimmediately apparent. Mr. and Mrs.Nanchang Chenko, residents of Yal village, said, “The village cleanup dayis a welcome development because,apart from helping us to keep our environment neat, it gives us somesense of unity as we come out to work together as a community.”
The Nigeria trachoma controlprogram encourages residents of trachoma-endemic areas to
clean up their villages to reduce thepopulation of flies and improve theenvironmental cleanliness. Currently,173 villages in Plateau and Nasarawastates participate in cleanup days,which are held on the last Saturday ofeach month and benefit more than100,000 people.
Each community forms a sanitationcommittee composed of people from allsections of society, including women,men, and children. The committeeorganizes community-wide participa-
Nigeria Promotes Village Cleanup Days
tion: Villagers are asked to first cleantheir own compounds and then cleancommunal areas such as roads, watersources, meeting points, and places of worship. The trachoma control program does not provide cleaning
Nigerians clean up their village.
N.
Jip
In March 2005, Sudan’s trachomacontrol program was moved fromthe Academy of Medical Sciences
and Technology to the Ministry ofHealth and its National Program forthe Prevention of Blindness. The transfer will help the program expandrapidly on a large scale in the wake of Sudan’s comprehensive peace agreement, benefiting thousands ofadditional Sudanese.
Since its transfer to the federalMinistry of Health, the program hascoordinated activities in Khartoum,Kassala, West Kordofan, and NorthernStates, establishing national and statetrachoma task forces, appointing stateblindness prevention coordinators, anddeveloping plans of action. The pro-gram is focusing on decentralizationand integration of program activities atthe state level and is enjoying unprece-
dented political support and awarenessthroughout the ministry.
The transition marks the end of a nascent period during which theAcademy advocated strongly for trachoma and onchocerciasis controlprograms and successfully launchedprogram activities. Federal trachomacontrol efforts are now directed by Dr. Kamal Hashim, coordinator of thePrevention of Blindness program, andDr. Awad Hassan, coordinator of theTrachoma Program.
An August 2005 visit to Sudan by Lisa Rotondo of The Carter Centerand Dr. Peter Kilima and Dr. SamAbbenyi, both of the InternationalTrachoma Initiative, laid the ground-work for future trachoma control activities in the country. Along withnational program staff, the group traveled to one of the priority states
Program Transfer AllowsSudan Activities to Grow Li
saR
oton
do
Peter Kilima of the InternationalTrachoma Initiative, Raymond Stewart of The Carter Center, and Mohib Aziz,site foreman, examine a window at theexpanded Prevention of Blindness programbuildings, which are being renovated byThe Carter Center.
in northern Sudan and met with leaders to assess trachoma controlefforts. Findings from this visit helpedin the formation of a five-year plan for Sudan’s program.
Trachoma
4 Waging Peace. Fighting Disease. Building Hope.
In July 2005, Lisa Rotondo, ofCarter Center headquarters inAtlanta, visited Moussa Arimi,
mayor of N’Guigmi commune in theDiffa region of eastern Niger, about1,500 km east of the capital, Niamey.Arimi has been mayor for five monthsand actively supports latrine promotionin his commune of 30,000 people. Themayor spoke with Rotondo about hiscontribution to latrine constructionand the great demand for latrinesamong his constituents.
“Since I have been posted inN’Guigmi, improving the health sector has been one of my main priorities. United Nations MillenniumDevelopment Goals formed the basis ofmy five-year action plan, with healthconcerns being of utmost importance.When I first started working, I soughtout all the possible partnerships thatwould help me achieve these goals. Isoon learned about the Carter Center’ssupport of local community radio stations in broadcasting messages abouttrachoma. The hygiene and sanitationaspects really interested me, especiallythe emphasis on household latrines.
“After a few months, people startedcoming to me requesting support andtechnical advice on how to buildlatrines of their own. They had heardthe radio shows and wanted to find out more. The district health teamcontacted The Carter Center, and theytrained and equipped 10 village-basedmasons to build Sanplat latrine slabs.Fortunately, we do not have a problemgetting sand here in the desert, and we are not held back by a long rainy
season. The main assistance we need iswith cement, gravel, and iron rods forthe slab.
“From my commune’s yearly budget,I contributed 1 million CFA francs forthe purchase of gravel. Then I decidedto solicit the support of the localUnited Nations Development Programoffice, which matched my contribution.That gave us a total of 2 million francsto purchase the gravel (approximately$4,000 USD). Now, with the CarterCenter’s contribution of cement andiron rods, we are ready to start building.
“We already have an enormous list of people requesting support tobuild household latrines. After seriousreflection, I decided on the goal ofbuilding 5,000 household latrines overfive years for the commune. That will
give every one of our approximately5,000 households in N’Guigmi accessto a latrine. We’ve already built sixlatrines, and with everyone’s partici-pation and support from our partners, I am confident that we will reach our goal.”
This is the second in a series of articlesthat shows how the Carter Center Trachoma Control Program affects indi-viduals in the countries in which we work.The comments of the individuals are notreproduced word for word but reflect thespirit of our conversations with people inthe field. The authors try to be faithful tothe context, content, and tone of the peopledepicted. The Carter Center-assisted trachoma activities in Niger are supportedby the Conrad N. Hilton Foundation.
Series on the Human Face of the Trachoma Control Program
Mayor Aims for 5,000 Latrines in Niger Commune
Lisa
Rot
ondo
Moussa Arimi, mayor of N’Guigmi commune in Diffa, Niger
5www.cartercenter.org
Emerson PM, Simms VM, Mahalo P,Bailey RL. (2005). Household pit latrinesas a source of the fly Musca sorbens—a one year longitudinal study from TheGambia. Trop Med Int Health. 10: 706-9.
Kuper H, Solomon AW, Buchan JC,Zondervan M, Mabey D, Foster A.(2005). Participatory evaluations of trachoma control programmes in eight countries. Trop Med Int Health.10:764-72.
Melese M, Alemayehu W, Worku A.(2004). Trichiasis among close relatives,central Ethiopia. Ethiop Med J. 42:255-9.
Rabiu M, Alhassan M, Ejere H. (2005).Environmental sanitary interventions forpreventing active trachoma. CochraneDatabase Syst Rev. 18.
Simms VM, Makalo P, Bailey RL,Emerson PM. (2005). Sustainability and acceptability of latrine provision in The Gambia. Trans R Soc Trop MedHyg. 99:631-7.
Trachoma References
Trachoma
In conducting the survey, CarterCenter staff visited the 120 householdsthat had participated in the programs,inspected their latrines, and inter-viewed the nearest neighbor who didnot have a latrine. Almost everyoneinterviewed, whether they had latrinesor not, perceived latrine ownership as advantageous for convenience,cleanliness, and health. These resultsshow that heads of households wouldappreciate latrines if they could getthem and that there is an unmetdemand for latrines.
With this new evidence, TheCarter Center is working to help provide latrines for all households in villages with high trachoma endemicity and low levels of sanitationcoverage, as prioritized by the district assemblies. So far, the new priority approach to latrine provision isworking. In the four villages that havebeen selected to date, every householdnow has access to its own latrine.
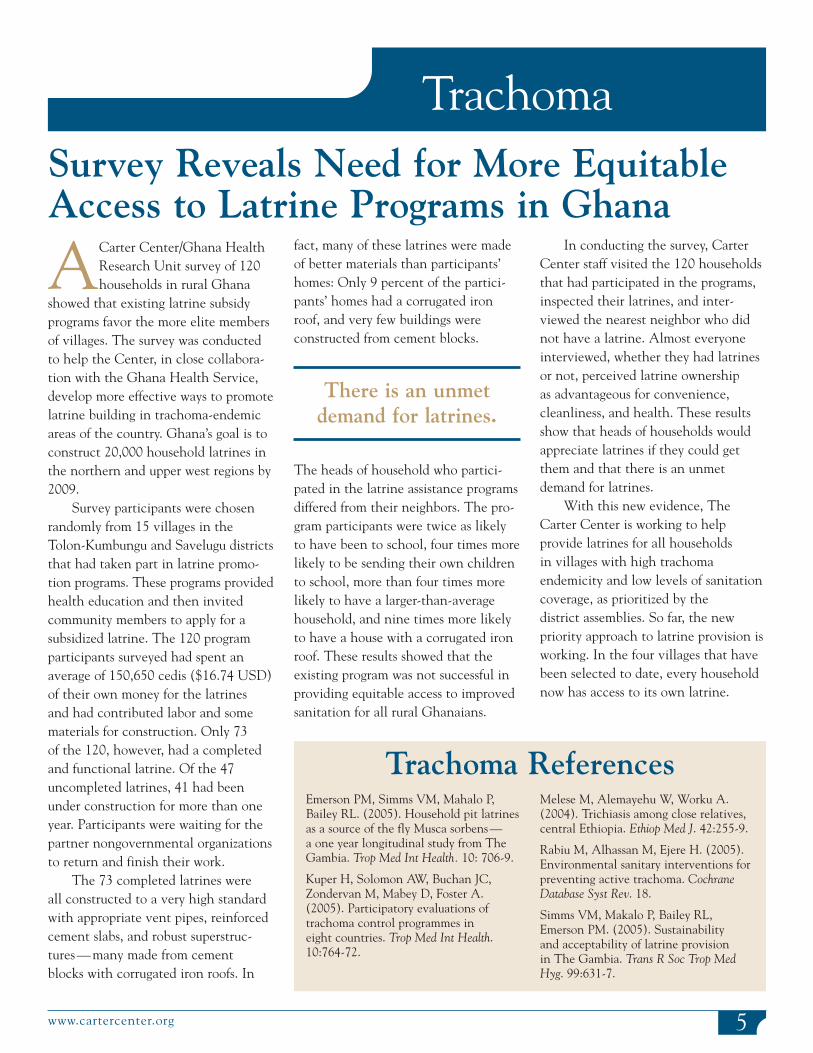
ACarter Center/Ghana HealthResearch Unit survey of 120households in rural Ghana
showed that existing latrine subsidyprograms favor the more elite membersof villages. The survey was conductedto help the Center, in close collabora-tion with the Ghana Health Service,develop more effective ways to promotelatrine building in trachoma-endemicareas of the country. Ghana’s goal is toconstruct 20,000 household latrines inthe northern and upper west regions by2009.
Survey participants were chosenrandomly from 15 villages in theTolon-Kumbungu and Savelugu districtsthat had taken part in latrine promo-tion programs. These programs providedhealth education and then invitedcommunity members to apply for a subsidized latrine. The 120 programparticipants surveyed had spent anaverage of 150,650 cedis ($16.74 USD)of their own money for the latrines and had contributed labor and somematerials for construction. Only 73 of the 120, however, had a completedand functional latrine. Of the 47uncompleted latrines, 41 had beenunder construction for more than oneyear. Participants were waiting for thepartner nongovernmental organizationsto return and finish their work.
The 73 completed latrines were all constructed to a very high standardwith appropriate vent pipes, reinforcedcement slabs, and robust superstruc-tures—many made from cement blocks with corrugated iron roofs. In
fact, many of these latrines were madeof better materials than participants’homes: Only 9 percent of the partici-pants’ homes had a corrugated ironroof, and very few buildings were constructed from cement blocks.
There is an unmetdemand for latrines.
The heads of household who partici-pated in the latrine assistance programsdiffered from their neighbors. The pro-gram participants were twice as likelyto have been to school, four times morelikely to be sending their own childrento school, more than four times morelikely to have a larger-than-averagehousehold, and nine times more likelyto have a house with a corrugated ironroof. These results showed that theexisting program was not successful inproviding equitable access to improvedsanitation for all rural Ghanaians.
Survey Reveals Need for More EquitableAccess to Latrine Programs in Ghana

education and provision of 57,551praziquantel treatments in three states(Plateau, Nasarawa, and Delta), whichis 36 percent of the 2005 annual treat-ment objective. The need to move toproviding “triple combination therapy”with Mectizan, albendazole, and prazi-quantel was noted as an important goalfor the near future.
The Trachoma Control Programassisted in the construction of 7,377
River Blindness
6 Waging Peace. Fighting Disease. Building Hope.
also considered the new collaboration with the Nigerian malaria program ininsecticide-treated net distribution.The lymphatic filariasis and malariaprograms jointly have distributed55,881 insecticide-treated nets since2004, with 17,261 from January throughSeptember 2005. Reimpregnation ofthese nets is a major challenge.
The Schistosomiasis ControlProgram had assisted in health
Program Reviewcontinued from page 1
naira), Nasarawa (6.5 million naira),and Delta (840,000 naira).
The River BlindnessProgram had assisted the Nigerian Ministry of Health in providing
health education to and treating nearly 3.3 million people.
In addition, the LymphaticFilariasis Elimination Program hadassisted the Ministry of Health in providing health education to andtreating 2.1 million people, which is 61percent of the 2005 ultimate treatmentgoal of 3.5 million people, in Plateauand Nasarwa states with combinationtherapy of Mectizan® and albendazole(donated by GlaxoSmithKline). Duringthe discussion, meeting participants
Lion Dr. Oluwasesan Onofowokan speaks at the review of Carter Center-assisted healthprograms in Abuja, Nigeria.
Fra
nkR
icha
rds
Table 1
River Blindness
7www.cartercenter.org
The following are the individualswho facilitated release of funds for the River Blindness Program in Nigeria.
Ebonyi StateState LevelHon. Dr. Henry AloHon. Commissioner for HealthHon. Collins AgboPersonal Assistant to the GovernorLinus NkwoAccountant General, Ebonyi State
LGA LevelLazarus E. OgbuzuruSecretary, LGA Joint AccountCommitteeEdwin IgbeleAccountant responsible for LGAfund release, Ministry of FinanceEbonyi
Nasarawa StateState LevelDr. John MammanPermanent Secretary, Ministry ofLocal Government and ChieftaincyAffairs, Nasarawa StateAlhaji Halilu Bala UsmanCommissioner, Ministry of LocalGovernment and ChieftaincyAffairs, Nasarawa State.
Delta StateState LevelDr. Okowa IfeanyiHon. Commissioner for HealthMinistry of Health AsabaDr. Ogaranya Tabs TaboweiPermanent Secretary, Ministry ofHealth, AsabaDr. Tobby MajerohDirector, Primary Health Care &Disease Control, Asaba
LGA LevelSonny OdigiriChairman, Ukwuani LGAChief Mary ChidiChairman, Ndokwa East LGAHon. F.P.C. AniamakaChairman, Aniocha North LGA
Figure 1
latrines and the provision of healtheducation in 173 intervention villages through September 2005.
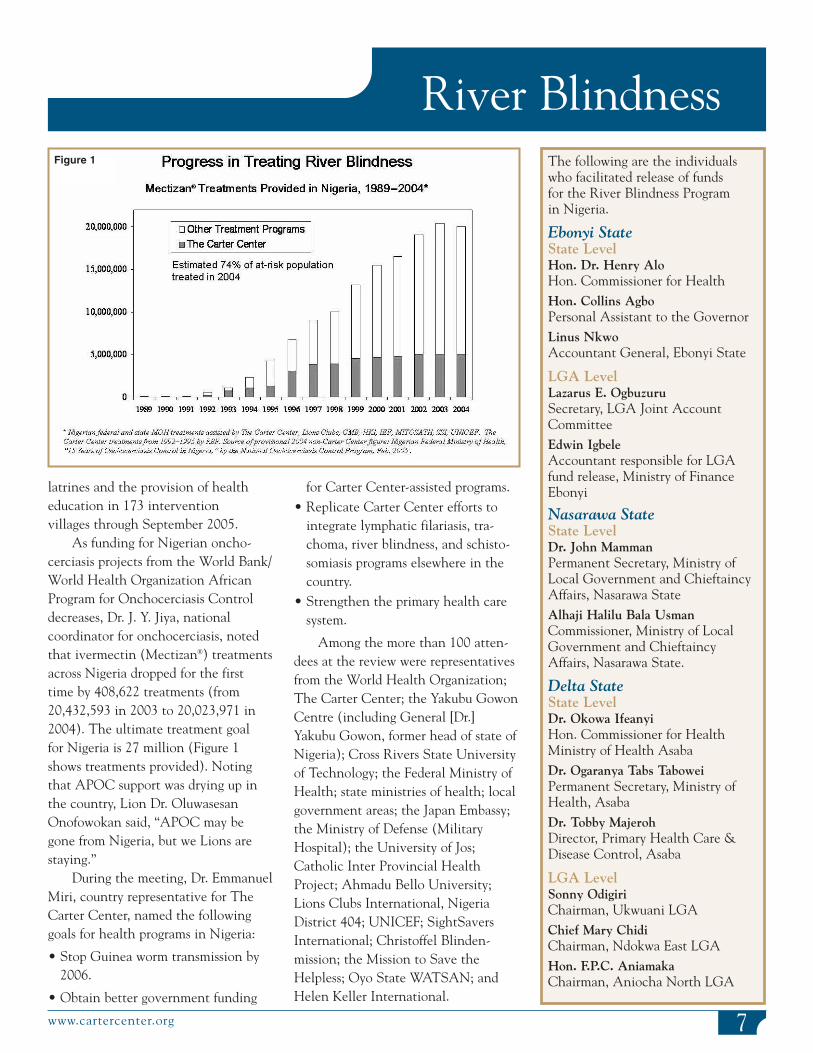
As funding for Nigerian oncho-cerciasis projects from the World Bank/World Health Organization AfricanProgram for Onchocerciasis Controldecreases, Dr. J. Y. Jiya, national coordinator for onchocerciasis, notedthat ivermectin (Mectizan®) treatmentsacross Nigeria dropped for the first time by 408,622 treatments (from20,432,593 in 2003 to 20,023,971 in2004). The ultimate treatment goal for Nigeria is 27 million (Figure 1shows treatments provided). Notingthat APOC support was drying up inthe country, Lion Dr. OluwasesanOnofowokan said, “APOC may begone from Nigeria, but we Lions arestaying.”
During the meeting, Dr. EmmanuelMiri, country representative for TheCarter Center, named the followinggoals for health programs in Nigeria:
• Stop Guinea worm transmission by2006.
• Obtain better government funding
for Carter Center-assisted programs.• Replicate Carter Center efforts to
integrate lymphatic filariasis, tra-choma, river blindness, and schisto-somiasis programs elsewhere in thecountry.
• Strengthen the primary health caresystem.
Among the more than 100 atten-dees at the review were representativesfrom the World Health Organization;The Carter Center; the Yakubu GowonCentre (including General [Dr.]Yakubu Gowon, former head of state ofNigeria); Cross Rivers State Universityof Technology; the Federal Ministry ofHealth; state ministries of health; localgovernment areas; the Japan Embassy;the Ministry of Defense (MilitaryHospital); the University of Jos;Catholic Inter Provincial HealthProject; Ahmadu Bello University;Lions Clubs International, NigeriaDistrict 404; UNICEF; SightSaversInternational; Christoffel Blinden-mission; the Mission to Save theHelpless; Oyo State WATSAN; andHelen Keller International.

River Blindness
8 Waging Peace. Fighting Disease. Building Hope.
The Onchoceriasis EradicationProgram for the Americas(OEPA) showed its progress
in fighting the disease at the fifteenthannual InterAmerican Conference on Onchoceriasis (IACO), held inCaracas, Venezuela, November 16–18,2005. The conference coveredadvancement made toward ultimatetreatment goals and impact of
eligible population covered by each ofthe 13 foci in round 1 and, so far, inround 2. The first round of treatmentsin 2005 reached 94 percent of the eligible population in the Americas.All but the southern Venezuela focussurpassed their 85 percent coveragegoal. A meeting was held to specificallyaddress the southern Venezuela focus in July 2005, and, perhaps as a result,treatments so far in round 2 for thatfocus (2,992) have already exceededthe treatments given in the entire first round (2,280), an increase of 31 percent.
Survey data on baseline and current eye disease from onchocerciasisfor each of the 13 foci were reviewed
IACO 2005 Shows Progress in Improving Visual Health in the Americas
Mectizan® treatments, among othertopics, and was convened by theMinistry of Health of Venezuela andOEPA. OEPA is funded by the Lions-Carter Center SightFirst Initiative, theBill & Melinda Gates Foundation,Merck & Co., and other donors.
For 2005, through October, a totalof 672,304 Mectizan treatments werereported in the 13 endemic foci of the
region, which is 74 percent of the 2005 ultimate treatment goal[UTG(2)] of 908,852.The first six months of2005 (round 1) yielded426,729 treatments, andin the second round,through October,245,575 treatments hadbeen reported. Figure 2shows the percent of the
There were 85 attendees at IACO2005. The Venezuela organizing
delegation included Dr. FranciscoArmada, Venezuelan Minister ofHealth; Dr. José Mendoza, VenezuelanViceminister of Health; Dr. RafaelBorges; Dr. Jacinto Convit; Dr. FátimaGarrido; Dr. Harland Schuler; and Dr. Carlos Botto. Two representativesfrom each of the nine endemic statesin Venezuela also attended.
The representatives from the other five endemic countries includedDr. Joao Batista Furtado Vieira, Dr. Claudete Schuertz and Dr. MarcosPellegrini (Brazil); Dr. SantiagoNicholls and Dr. Ivan Mejia(Colombia); Dr. Jose Rumbea and Dr. Juan Carlos Vieira (Ecuador); Dr. Edgar Mendez-Gordillo and
Dr. Eduardo Catú Rodríguez(Guatemala); and Dr. Miguel LutzowSteiner (Mexico).
Lions Clubs have been strong supporters of the OEPA initiative, and were represented at IACO by Dr. Libardo Bastidas Passos(Colombia); Ramiro Peña Constante(Ecuador); Dr. Carlos Samuel Arévalo(Guatemala); Dr. Florencio CabreraCoello (Mexico); Andrés Sánchez, Dr. Manuel Bautista Plaza, BlancaGarcía de Ortiz (Venezuela); andHolly Becker (United States).
The Pan American HealthOrganization (PAHO) was representedby Dr. Celsa Sampson and Dr. MarioValcarcel. Ken Gustavsen (UnitedStates), José Francisco Gómez and
Elizabeth Sousa de Jesús (Venezuela)represented Merck, and Dr. MaryAlleman and Dr. Bjorn Thylefors represented the Mectizan® DonationProgram. Other participants and presenters included Dr. José AntonioKelly (Coordinator of the YanomamiHealth Plan), Dr. Tom Unnasch(University of Alabama atBirmingham), Dr. Ed Cupp (AuburnUniversity), Dr. Frank Richards (TheCarter Center), Dr. Richard Collins(University of Arizona), Dr. KevinWinthrop (Oregon Health andScience University), Dr. CarlosGonzales-Peralta (regional expert and former member of the Mectizan®
Expert Committee), and Dr. MarioAlberto Rodríguez (immunologist).
Figure 2
Lions Clubs. In addition, attendee Dr. Yankum Dadzie, chairman of theGlobal Alliance for LF EliminationExecutive Group, noted the desire ofhis group to assist in the scale up oflymphatic filariasis activities in Nigeria.
River Blindness
9www.cartercenter.org
In September 2005, NigeriaPresident Olusegun Obasanjopledged to fund $3 million of the
estimated $4.5 million needed by thecountry’s Ministry of Health to buildand sustain programs combatingGuinea worm, onchocerciasis, lymphatic filariasis, and schistosomiasis.The funding pledge came a day afterthe president met with a Carter Centerdelegation that included President andMrs. Carter; James Wagner, presidentof Emory University; John Moores,chairman of the Carter Center Boardof Trustees; and Richard Blum, memberof the Carter Center Board of Trustees.The group encouraged the Nigeriangovernment to invest in health programs assisted by The Carter Center and discussed the financialneeds of the Nigeria Ministry of Health for expanding programs that
fight the four parasitic diseases.
In the meet-ing where thefunding announce-ment was made,Dr. EyitayoLambo, federalminister of health,stressed the needto ensure funding for the programsin the years after PresidentObasanjo’s admin-istration ends.
Attendees at the September meetings included General Dr. YakubuGowon, U.S. and Canadian ambassa-dors, and representatives from theJapanese embassy, World HealthOrganization, UNICEF, UNDP, and
President Carter, Mrs. Carter, Dr. Eyitayo Lambo, and GeneralGowon listen as Dr. Donald Hopkins makes a point about CarterCenter-assisted health programs.
John
Moo
res
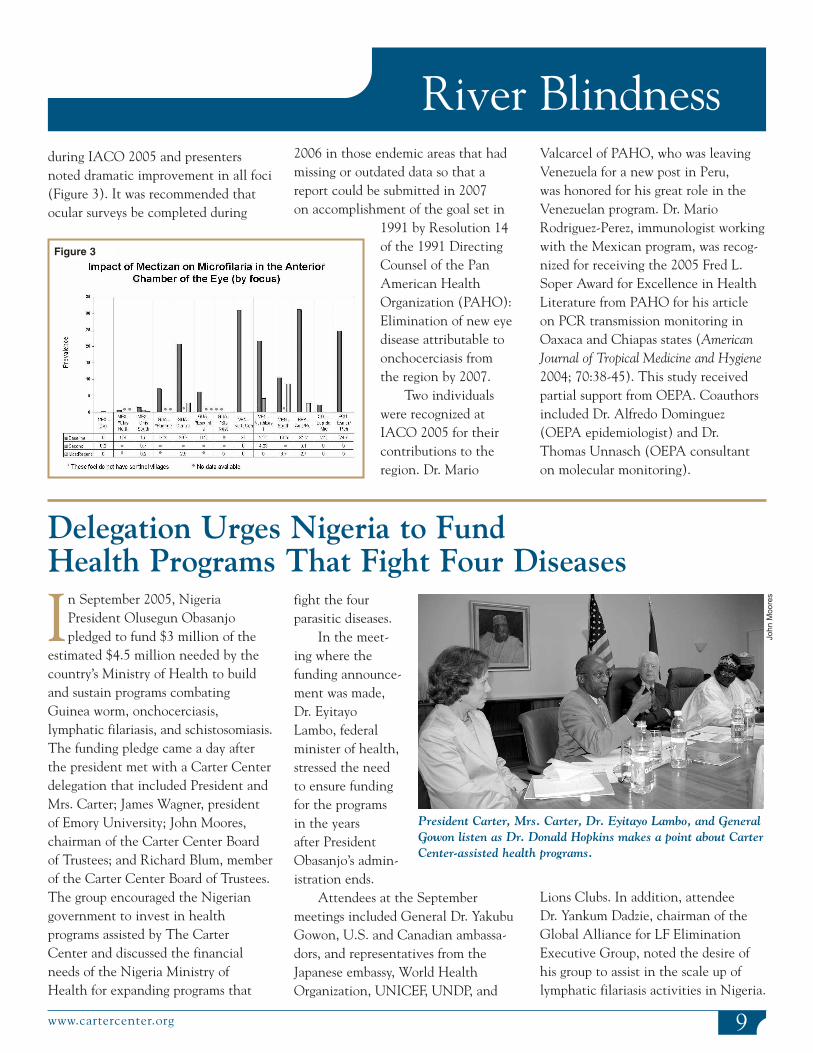
during IACO 2005 and presentersnoted dramatic improvement in all foci(Figure 3). It was recommended thatocular surveys be completed during
Delegation Urges Nigeria to Fund Health Programs That Fight Four Diseases
2006 in those endemic areas that hadmissing or outdated data so that areport could be submitted in 2007 on accomplishment of the goal set in
1991 by Resolution 14of the 1991 DirectingCounsel of the PanAmerican HealthOrganization (PAHO):Elimination of new eyedisease attributable toonchocerciasis from the region by 2007.
Two individualswere recognized atIACO 2005 for theircontributions to theregion. Dr. Mario
Valcarcel of PAHO, who was leavingVenezuela for a new post in Peru, was honored for his great role in theVenezuelan program. Dr. MarioRodriguez-Perez, immunologist workingwith the Mexican program, was recog-nized for receiving the 2005 Fred L.Soper Award for Excellence in HealthLiterature from PAHO for his articleon PCR transmission monitoring inOaxaca and Chiapas states (AmericanJournal of Tropical Medicine and Hygiene2004; 70:38-45). This study receivedpartial support from OEPA. Coauthorsincluded Dr. Alfredo Dominguez(OEPA epidemiologist) and Dr.Thomas Unnasch (OEPA consultanton molecular monitoring).
Figure 3
10 Waging Peace. Fighting Disease. Building Hope.
River Blindness
On a visit to Mexico in August2005, a group of health workersand others traveled muddy
mountain roads to visit the remotecommunities of Brasil and Estrella Roja in Chiapas. The visitors, whoincluded Becky Brookshire of TheCarter Center and public health workersfrom the Mexican Ministry of HealthOnchocerciasis Program and localLions Clubs, met Señora PitasiaGonzales, a 78-year-old blind woman,who lives with her daughters Marquinaand Manuela. Gonzales said that shewas once a strong and capable providerfor her family, but, due to the damageto her eyes caused years ago byonchocerciasis, she has lost her sight.She said her blindness has made herdependent on her daughters to help herclean and dress herself and navigatetheir small property. She expressedconfidence, however, that her grand-children will not go blind because theyare given free Mectizan® treatmentseach year.
Her confidence is well placed.Those in Chiapas who are blind from
onchocerciasis are all elderly, a sign of the success of the Mexican program,which has treated more than 85 percent of its eligible population semiannually for the last four years,preventing fur-ther visualdamage.Despite theprogram’sachievements,however, trans-mission ofonchocerciasisin Chiapas hasnot yet beenstopped. Someof the youngchildren exam-ined during the visit hadonchocercalskin nodules,indicating thatthey wererecentlyexposed to theO. volvulusparasite byinfected blackfly bites.However, aslong as thesechildren andthe others in the community continueto receive treatment, their symptomswill not advance, and eventually riverblindness will be history.
The effort to stop the disease is ongoing for the Ochocerciasis
Rural Mexican CommunitiesBenefit from Treatment
Elimination Program for the Americas.The same day the health workers met Señora Gonzales, they set up aMectizan distribution center in a smallschoolhouse in Brasil, where local residents receive tablets twice a year.Lions Club members helped hand out Mectizan and provided health education to the community members lined up at the door. To help people
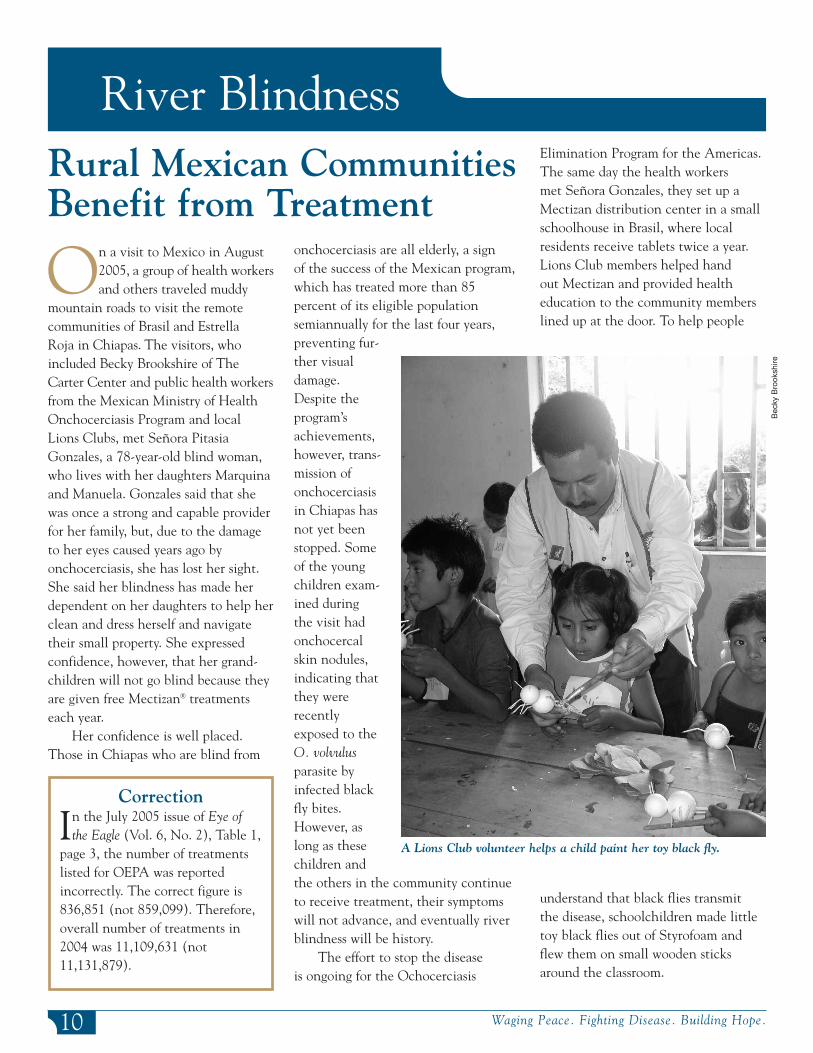
understand that black flies transmit the disease, schoolchildren made littletoy black flies out of Styrofoam andflew them on small wooden sticksaround the classroom.
Correction
In the July 2005 issue of Eye of the Eagle (Vol. 6, No. 2), Table 1,
page 3, the number of treatmentslisted for OEPA was reportedincorrectly. The correct figure is836,851 (not 859,099). Therefore,overall number of treatments in2004 was 11,109,631 (not11,131,879).
A Lions Club volunteer helps a child paint her toy black fly.
Bec
kyB
rook
shire

Duke BO (2005). Evidence for macro-filaricidal activity of ivermectin againstfemale Onchocerca volvulus: furtheranalysis of a clinical trial in the Republicof Cameroon indicating two distinctkilling mechanisms. Parasitology. 2005Apr; 130(Pt 4): 447-53.
Egbert PR, Jacobson DW, Fiadoyor S,Dadzie P, Ellingson KD (2005).Onchocerciasis: a potential risk factor for glaucoma. Br J Ophthalmol. 2005 Jul; 89(7): 796-8.
Molyneux DH (2005). Onchocerciasiscontrol and elimination: coming of age
in resource-constrained health systems.Trends Parasitol. 2005 Nov; 21(11): 525-9.
Nuwaha F, Okware J, Ndyomugyenyi R(2005). Predictors of compliance withcommunity-directed ivermectin treatmentin Uganda: quantitative results. Trop MedInt Health. 2005 Jul; 10(7): 659-67.
Renz A, Tanya VN, Trees AJ (2005).Antibiotic chemotherapy of onchocercia-sis: in a bovine model, killing of adult parasites requires a sustained depletion of endosymbiotic bacteria (wolbachiaspecies). J Infect Dis. 2005 Oct 15; 192(8):1483-93.
Richards FO Jr, Eigege A, Pam D, Kal A,Lenhart A, Oneyka JO, Jinadu MY, MiriES (2005). Mass ivermectin treatment for onchocerciasis: lack of evidence for collateral impact on transmission of Wuchereria bancrofti in areas of co-endemicity. Filaria J. 2005 Jul 15; 4:6.
WHO Report (2005). Onchocerciasis(river blindness). Report from theFourteenth InterAmerican Conference on Onchocerciasis, Atlanta, Georgia,United States. Wkly Epidemiol Rec. 2005Jul 29; 80(30): 257-60.
River Blindness References
11www.cartercenter.org
River Blindness
The Pan-American Health andEducation Foundation presented
its 2005 Fred L. Soper Award forExcellence in Health Literature to Dr.Mario Rodriguez-Perez and colleaguesfor the article “Polymerase ChainReaction Monitoring of Transmissionof Onchocerca volvulus in TwoEndemic States in Mexico,” publishedin the American Journal of TropicalMedicine and Hygiene (2004, 70: 38-45).This study received partial supportfrom the Onchocerciasis EliminationProgram for the Americas (OEPA),which is funded by the Lions–CarterCenter SightFirst Initiative, the Bill & Melinda Gates Foundation, Merck& Co., and other donors. Dr. AlfredoDominguez, an epidemiologist withOEPA, was coauthor of the study, and the senior author was Dr. ThomasUnnasch of the University of Alabama,a frequent participant in Carter CenterRiver Blindness Program reviews.
OEPA-SupportedStudy ReceivesSoper AwardArandomized study from
Thammasat University inThailand shows that a single,
combined dose of ivermectin (200micrograms/kg), praziquantel (40mg/kg), and albendazole (400 mg) in23 volunteers resulted in no clinicallyrelevant differences as compared to the drugs being given individually atdifferent times. The study looked forpharmacokinetic changes or adverse reactions between thesingle, combined doseand the individualdoses, using U.S. Food and DrugAdministration criteria.The study was con-ducted by Dr. KesaraNa-Bangchang and his colleagues and willsoon be reported in thejournal Transactions of the Royal Society of Tropical Medicine and Hygiene.
Study Shows Safety of CombiningThree Drugs in Single Dose
These results were reported to theJoint Action Forum (JAF) of AfricanProgramme for Onchocerciasis Control(APOC) in December 2004, and JAFnoted: “…This was operationally signif-icant for the integration of the treat-ment of onchocerciasis, lymphatic filar-iasis, and other helminths.” (Tenth ses-sion of the Joint Action Forum, APOC,Kinshasa, DRC, 7-9 December 2004)
A health worker gives a Nigerian boy praziquantel.
Em
ilyS
taub
THE CARTER CENTER
THE CARTER CENTER
THE CARTER CENTER
T
Global Health News
For up-to-the-minute news from The Carter Center, visit our Web site: www. cartercenter.org.
One Copenhill453 Freedom ParkwayAtlanta, GA 30307
This issue is made possible in part thanks to the Michael G. DeGroote Health Program Publications Fund.
The International Task Force forDisease Eradication met in
October 2005 at The Carter Center toreview the use of insecticide-treatedbed nets (ITNs). The task force notedthat the nets are very effective forfighting malaria and recommended thattheir use be widened as soon as possible.
Some of the group’s recommen-dations included the following:
• Use of ITNs could potentially prevent almost half a million deathsof African children per year.
• Initial priority should be given topregnant women and children under
5 years of age, but targeting entire at-risk populations is more effectivefor reducing transmission.
• Current use of ITNs is much lessthan it should be.
• Mass ITN distribution could affecttransmission of other vector-bornediseases, such as lymphatic filariasis.
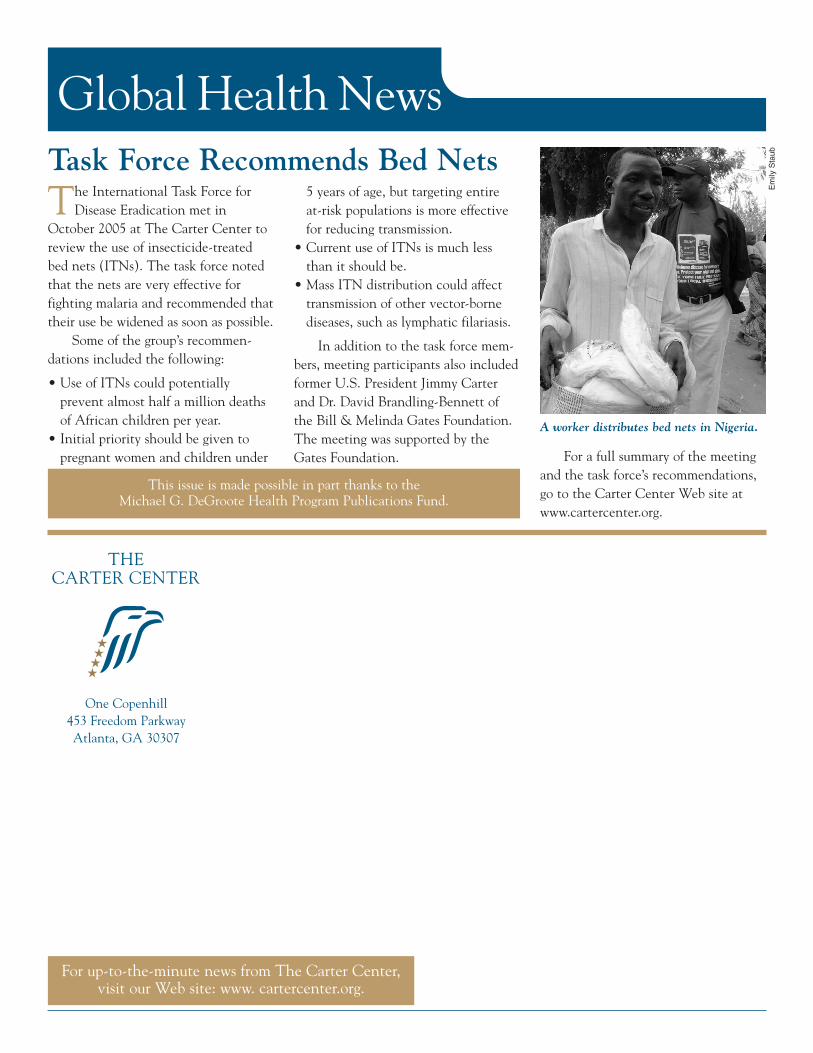
In addition to the task force mem-bers, meeting participants also includedformer U.S. President Jimmy Carterand Dr. David Brandling-Bennett ofthe Bill & Melinda Gates Foundation.The meeting was supported by theGates Foundation.
Task Force Recommends Bed Nets
For a full summary of the meetingand the task force’s recommendations,go to the Carter Center Web site atwww.cartercenter.org.
A worker distributes bed nets in Nigeria.
Em
ilyS
taub


















