
EYE EXAM. How to approach the eye.. What do we need? Snellen chart Magnifier - preferably X8 Torch...
46
EYE EXAM
-
Upload
magdalen-glenn -
Category
Documents
-
view
218 -
download
0
Transcript of EYE EXAM. How to approach the eye.. What do we need? Snellen chart Magnifier - preferably X8 Torch...

EYE EXAM

How to approach the eye..
What do we need?
• Snellen chart • Magnifier - preferably X8 • Torch with a blue filter • Fluoroscine drops or paper • Topical anaesthesia • Topical short acting mydriatic preferably
tropicamide• Hand held ophthalmoscope • A Systematic approach
Two types
• Medical - red eye (infection, inflammation)
- loss of vision
• Trauma - penetrating
- blunt
- chemical
- thermal

History
• Main symptom(s)
• Pain
• Discharge
• Vision
• Any trauma
• PMH, PSH
• Medication

Examination
• Anatomical Lymphnodes Eye movements Lids and lashes Conjunctiva Cornea Anterior chamber Iris, Pupil & Lens Fundoscopy

Eye Movements

Ophthalmoscopy
• Dim room
• Approach from 15cm, “O” magnification
• Right to Right, Left to Left
• Red reflex
• Aim nasally, small aperture, low light
• Cornea
• Lens

Red Reflex

Fundoscopy 1
• Optic disk Swelling, cupping Colour Vessels, bleeds
• Macula Colour Exudates, abnormalities

Papilloedema

Fundoscopy 2
• Vessels New vessels Tortuousity, segmentation Colour
• Rest of retina Pallor Bleeds Pigmentation Retinopathy

Fundoscopy 3
• Tips
Both eyes open – yours and theirs!
Stand to side
Peripheral retina
Dilate pupils - if safe, after RAPD test and
VA test
Polarised filter

Rest of exam
• Visual acuity
• Visual fields
• RAPD
• “Digital” tonometry

VA – Pinhole

Rest of exam

Lids and Lashes

Lacrimal System

Dacryocystitis Treatment
• Acute - antibiotics
- I & D
• Chronic - DCR

Lids and lashes

Viral

Viral treatment
• Check Cornea!
• Symptomatic, supportive
• Chloramphenicol
• Refer if in doubt

Bacterial

Bacterial Treatment
• Simple - chloramphenicol - drops day, ointment nocte’• Gonococcal - admit - swabs - IV cefoxitin 1g QID - Topical Gentamycin• Neonatal - IV and topical Pen• Chlamydia - occ. Tetracycline QID four weeks - Oral doxycycline or erythromycin for six weeks

PKC
• HS reaction• Self resolving• ?Steroids
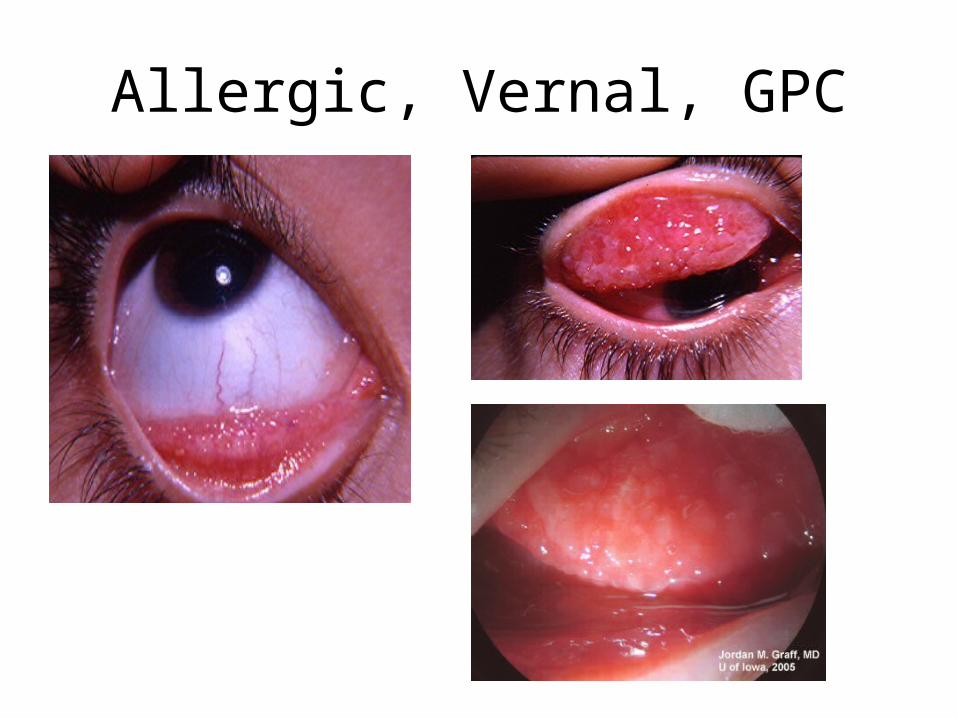
Allergic, Vernal, GPC

Treatment
• Topical Antihistamines Spersallerge ®
• Topical Mast cell stabilisers Optichrom ®
• Topical Steroids
• Refer

Conjunctiva - other

Cornea

HZO
• Refer• Check immunity• Treat
Systemic antivirals
Topical antivirals
Analgesia

Glaucoma

Acute Angle Closure

Glaucoma Post - Surgery

Chronic OAG Cup/disk ratio

Acute Angle Closure Mx
• Recognise
• Risk or reality
• Meds - diamox 500mg stat, 250mg QID
- glycerine/mannitol 1-2g/kg
- pilocarpine 1-2% QID
- B-blockers BD
• Referral for Laser or Surgery

Diabetic retinopathy
• Background - dot and blot - hard exudates
• Pre-proliferative - cotton wool spots - IRMA - venous segmentation - large dark blots
• Proliferative - NVD or NVE - vitreous bleeds - fibrous proliferation and retinal detachment - neovascular glaucoma

Non Proliferative
• Background - dot and blot - hard exudates -micro aneurysms - macular oedema
• Pre-proliferative - cotton wool spots (soft) - IRMA - venous segmentation - large dark blots

Proliferative
• NVD• NVE• Fibrovascular
proliferation• Vitreous bleeds

Proliferative 2

FB, Blunt and Perforating Trauma
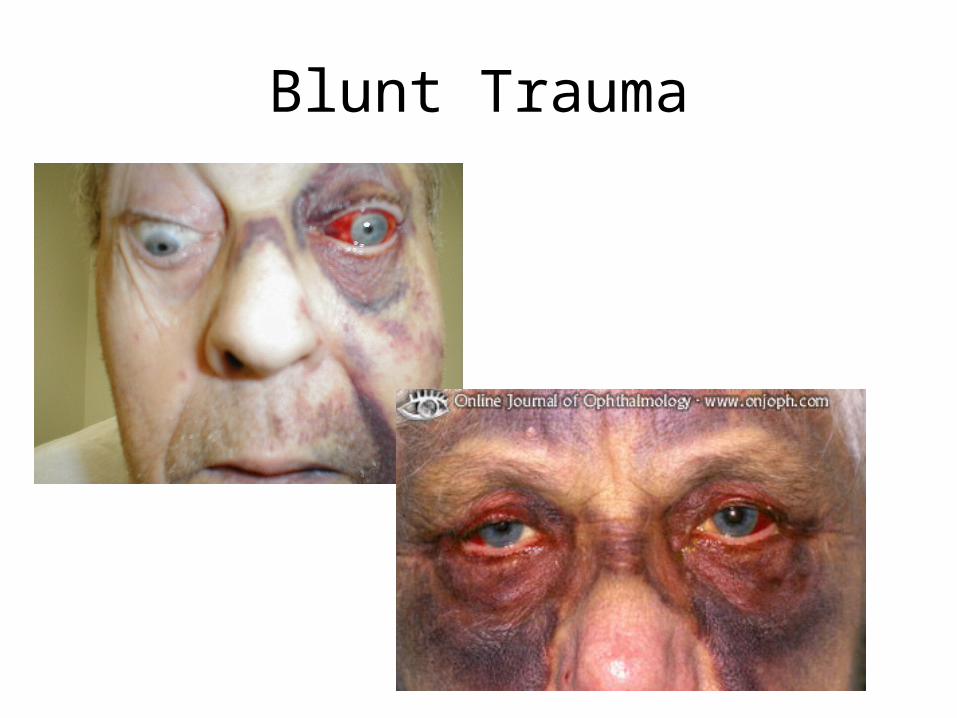
Blunt Trauma

Corneal Injury

Lens Injury
Other trauma
• Traumatic mydriasis
• Traumatic iritis
• Vitreous bleed
• Retinal detachment
• Macula oedema
• Optic neuropathy

Trauma management
• Analgesia
• Low light
• Gentle
• Same as all eyes
• X rays
• Topical antibiotics
• Tet Tox
References
• UCT Ophthalmology Lecture Notes
• www.trauma.org
• www.medicine.ucsd.edu/clinicalmed/eyes.htm
• www.atlasophthalmology.com
• www.eyecasualty.co.uk
• www.webeye.ophth.uiowa.edu/eyeforum


















