Extraoral drilling for zygoma implants
42
-
Upload
luc-vrielinck -
Category
Documents
-
view
231 -
download
2
description
Decription of a modification of the surgical technique for placing zygoma implants
Transcript of Extraoral drilling for zygoma implants

Rationale for modification of the
zygoma implant drilling technique
• The patient presented with a combination of:
– Hemimaxillectomy situation
– Reduced bone volume in the regio of the zygomatic bone
– Limited mouth opening
• When drilling from intraorally it is very easy to miss the
remaining bone volume in the zygomatic bone
• When drilling from extraorally, the bone volume can be
evaluated under direct vision
• It appears to be easier to assure that the implant will be
in as much remaining bone as possible
Indications of the extraoral
drilling technique• Limited mouth opening
• Reduced bone volume in zygomatic bone
• When the implant needs to be anchored in
the lateral orbital rim eventually crossing
the orbital floor
Case 1
• Extraoral drilling for zygomatic implant due to :
– Limited bone volume
– Limited mouth opening
Situation
• Situation after right hemimaxillectomy and
broad irradiation of maxilla and skull base
2005
• Tumor free
• Loss of a zygoma implant right
• Severely limited mouth opening 1 cm
• Postradiotherapy fibrosis and retraction of
the upper lip and cheek
Preoperative view
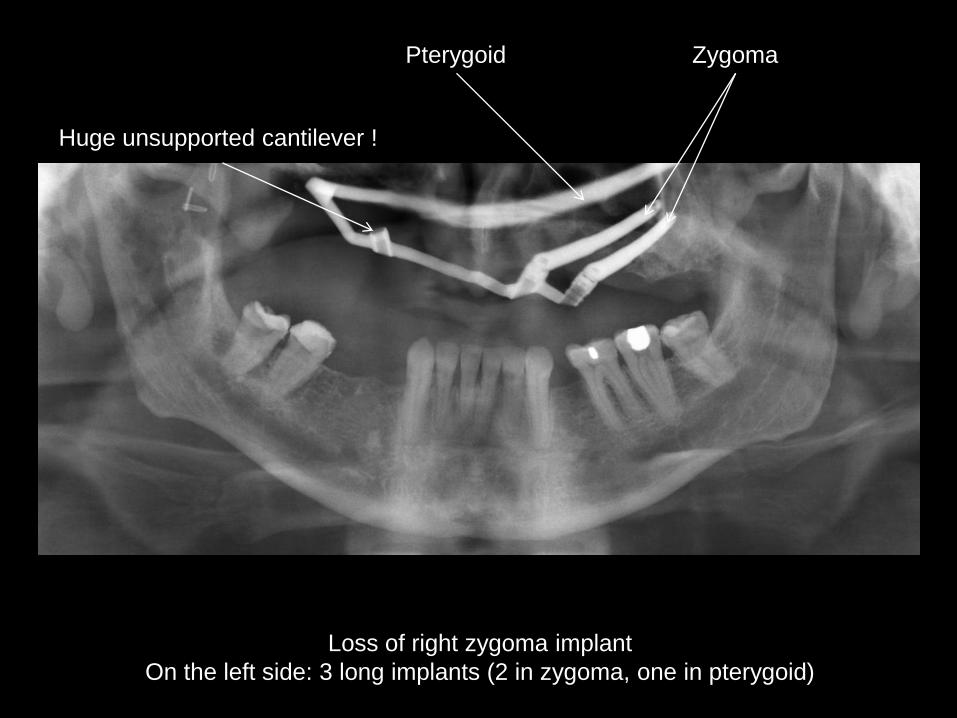
Loss of right zygoma implant
On the left side: 3 long implants (2 in zygoma, one in pterygoid)
Pterygoid Zygoma
Huge unsupported cantilever !
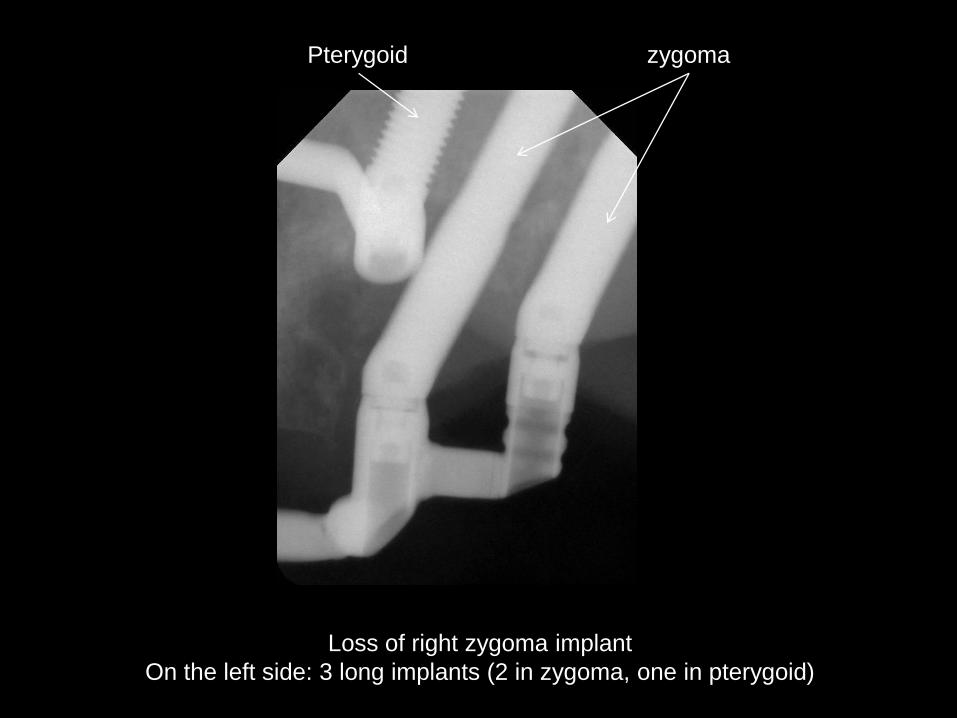
Loss of right zygoma implant
On the left side: 3 long implants (2 in zygoma, one in pterygoid)
Pterygoid zygoma
Preoperatieve view

Preoperatieve view

Preoperatieve view
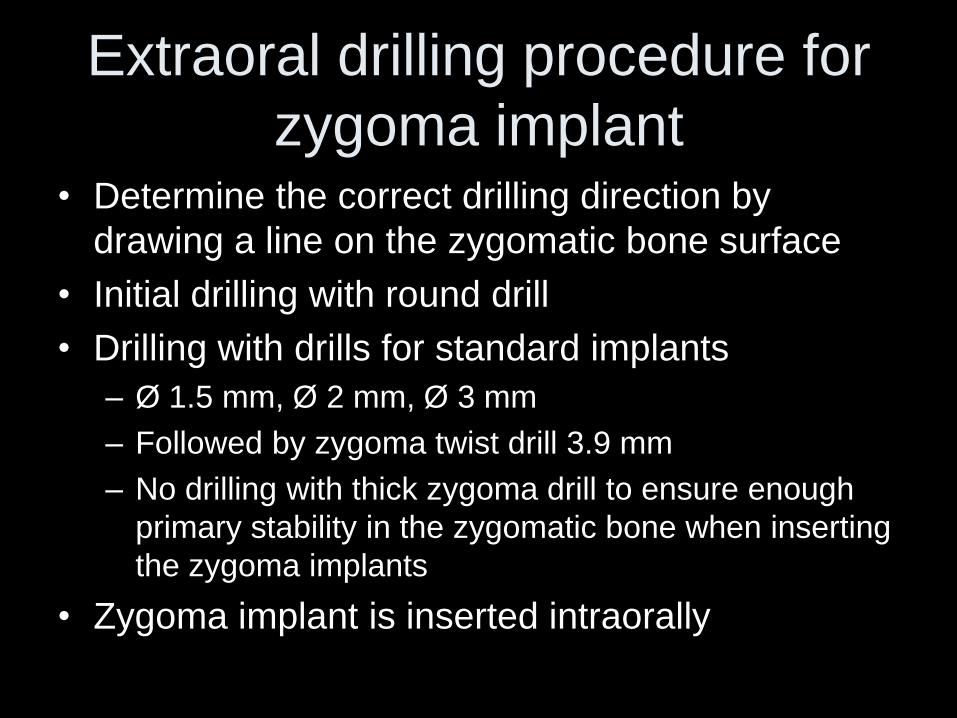
Extraoral drilling procedure for
zygoma implant • Determine the correct drilling direction by
drawing a line on the zygomatic bone surface
• Initial drilling with round drill
• Drilling with drills for standard implants
– Ø 1.5 mm, Ø 2 mm, Ø 3 mm
– Followed by zygoma twist drill 3.9 mm
– No drilling with thick zygoma drill to ensure enough
primary stability in the zygomatic bone when inserting
the zygoma implants
• Zygoma implant is inserted intraorally
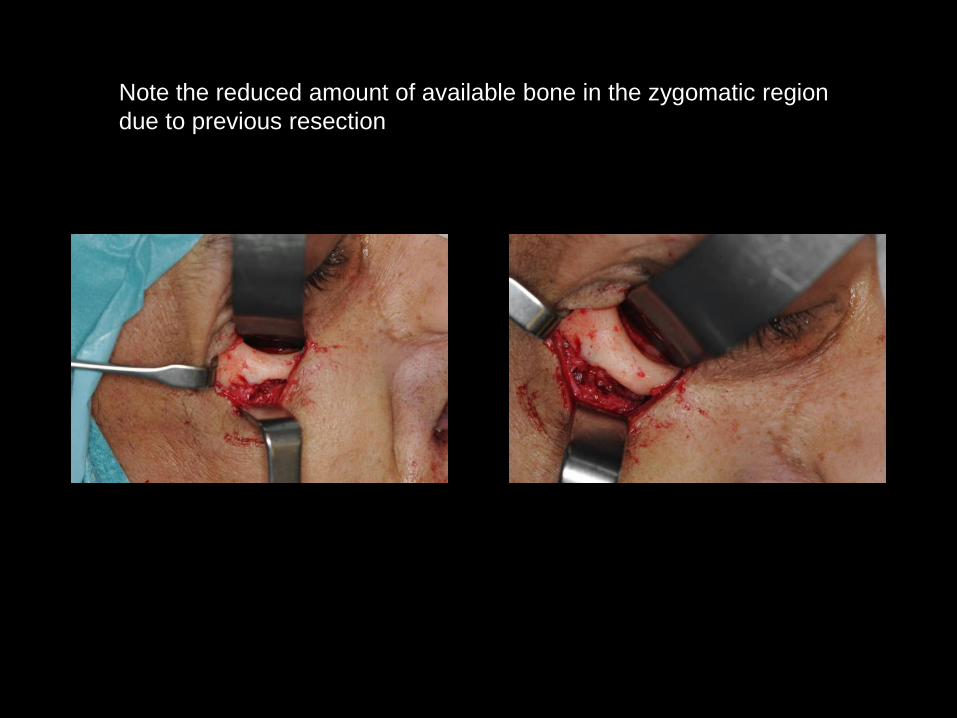
Note the reduced amount of available bone in the zygomatic region
due to previous resection
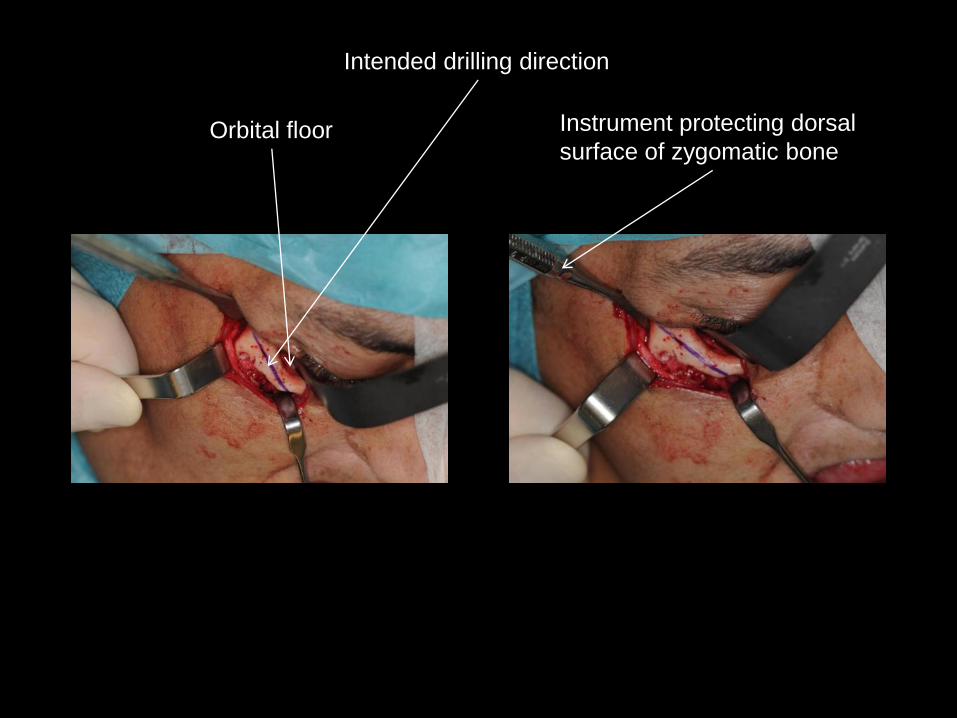
Intended drilling direction
Instrument protecting dorsal
surface of zygomatic boneOrbital floor
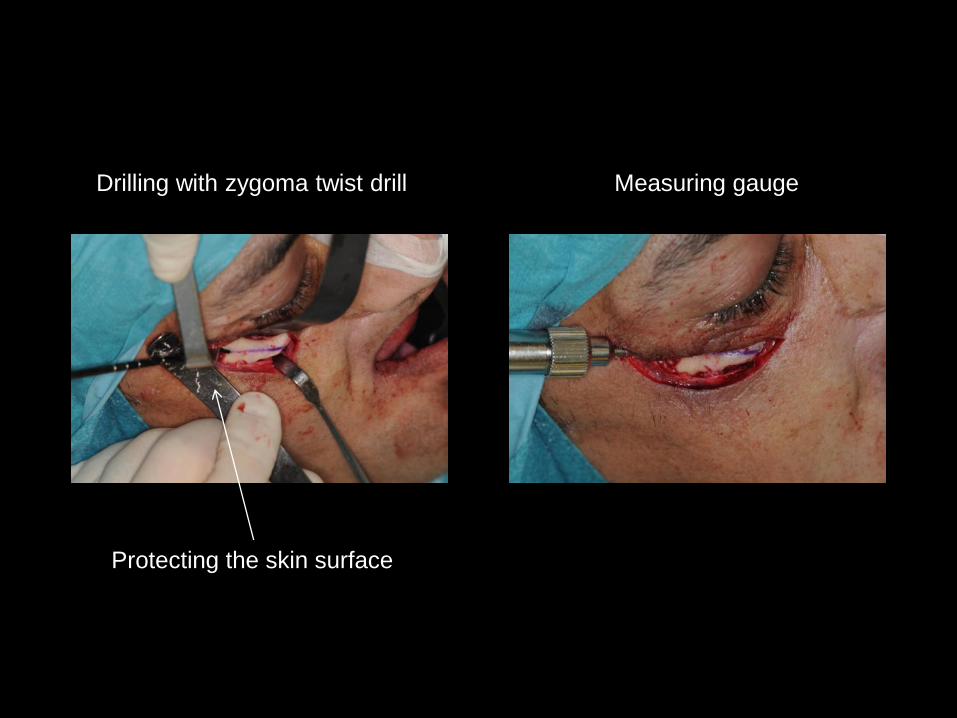
Drilling with zygoma twist drill Measuring gauge
Protecting the skin surface
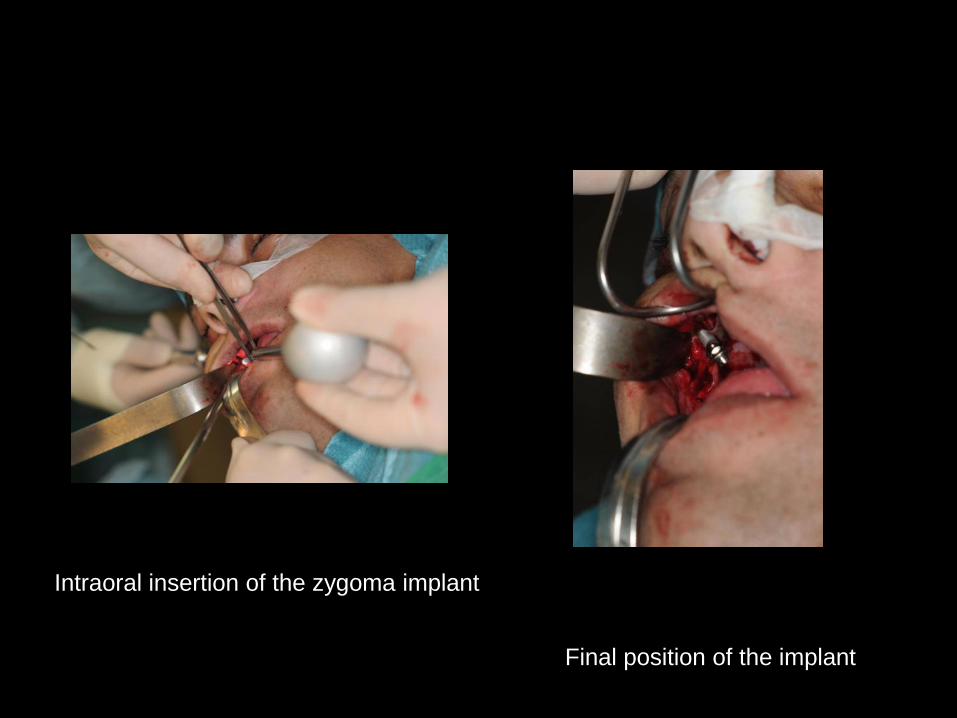
Intraoral insertion of the zygoma implant
Final position of the implant
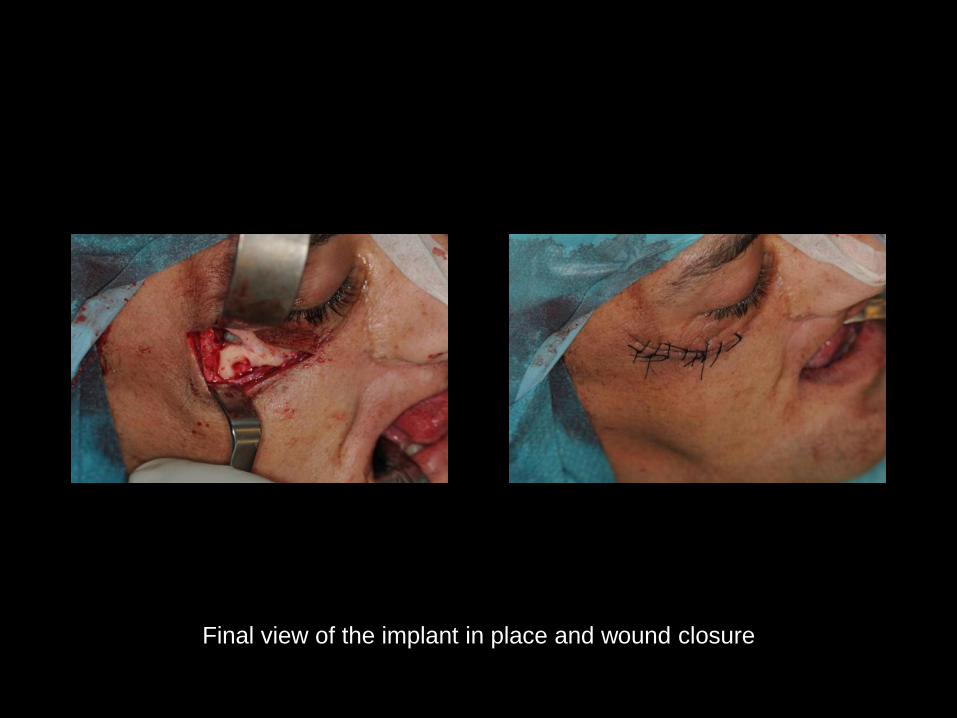
Final view of the implant in place and wound closure
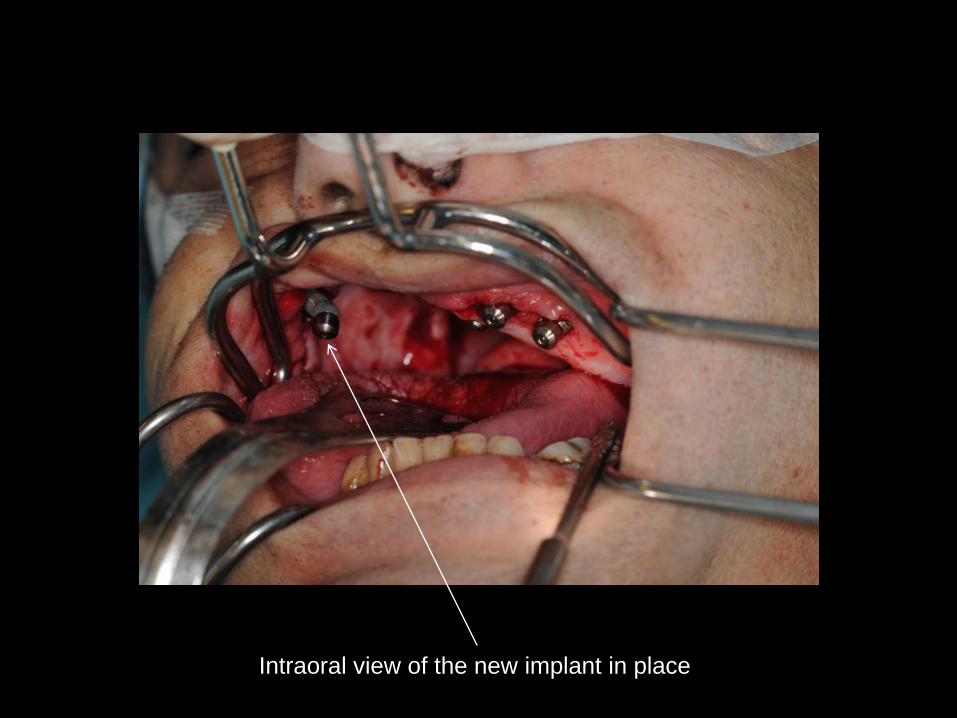
Intraoral view of the new implant in place

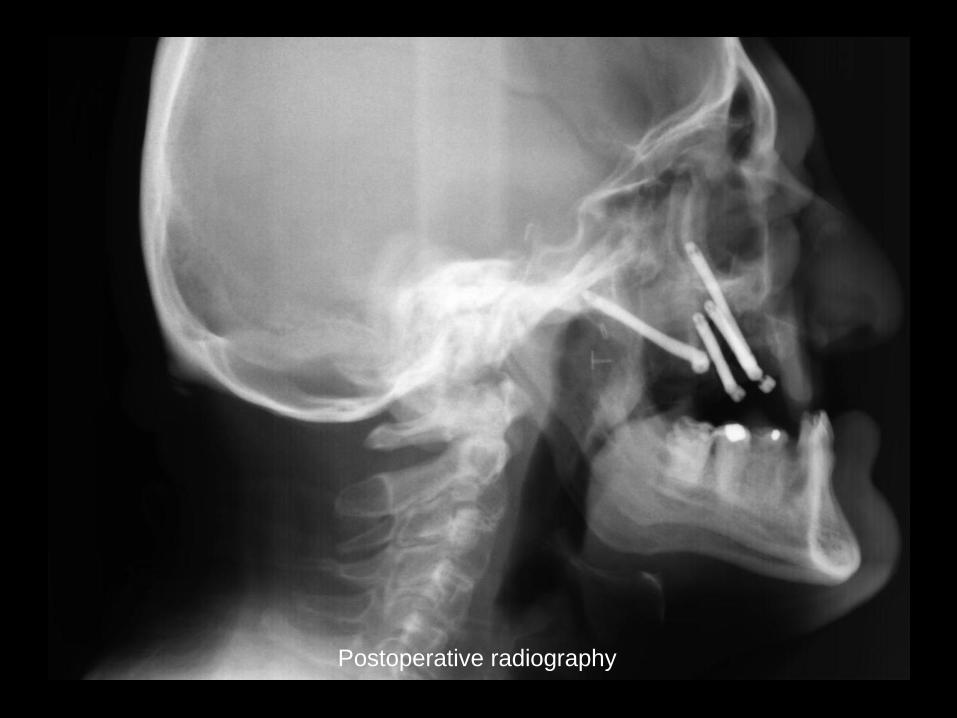
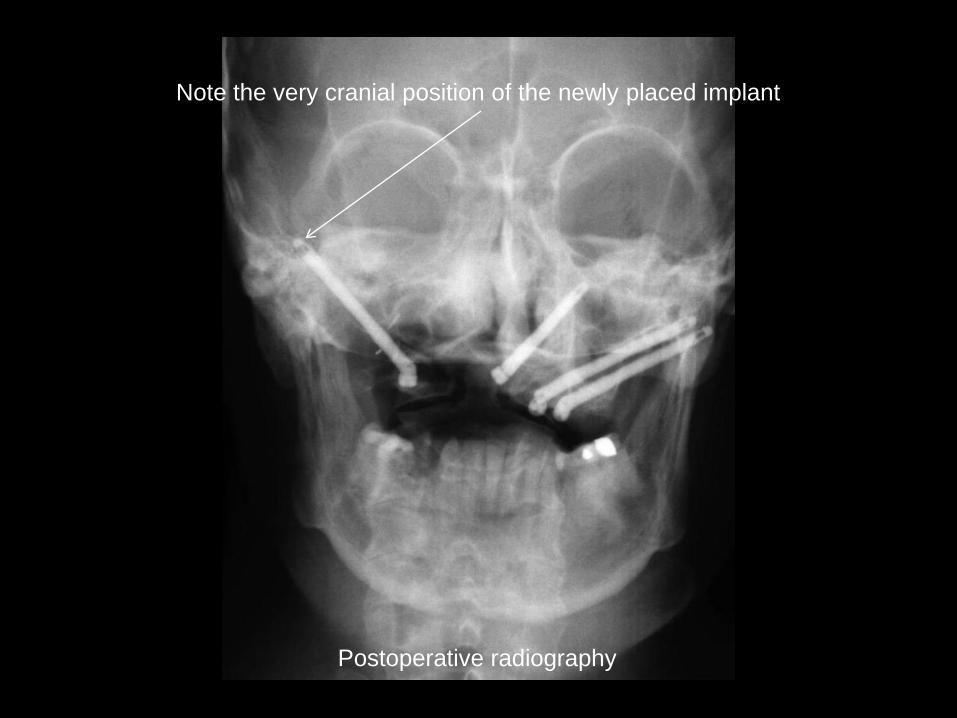
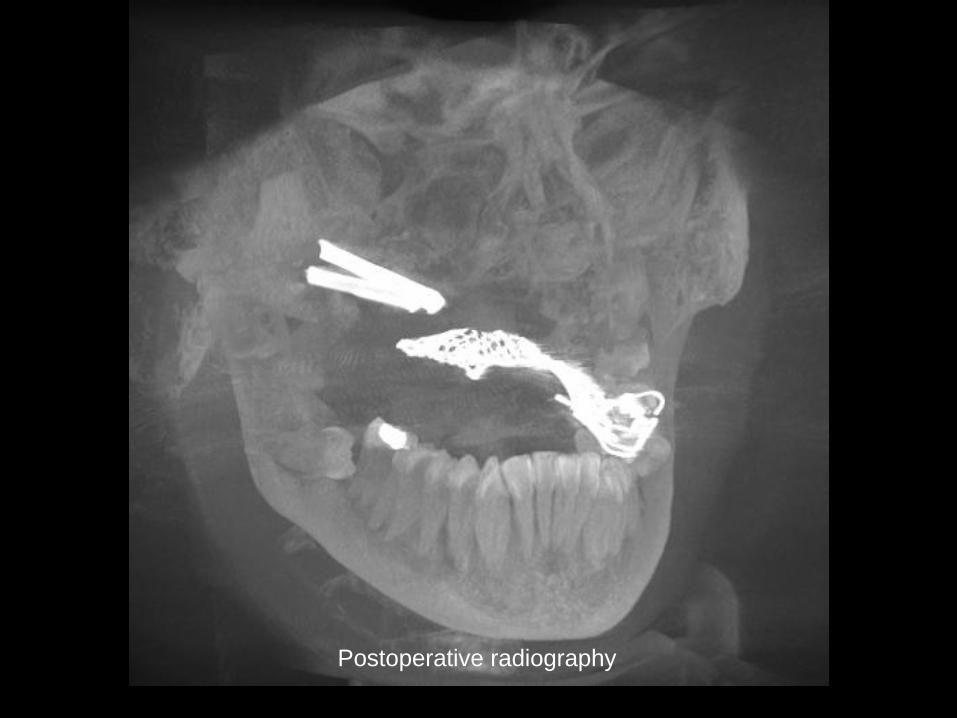
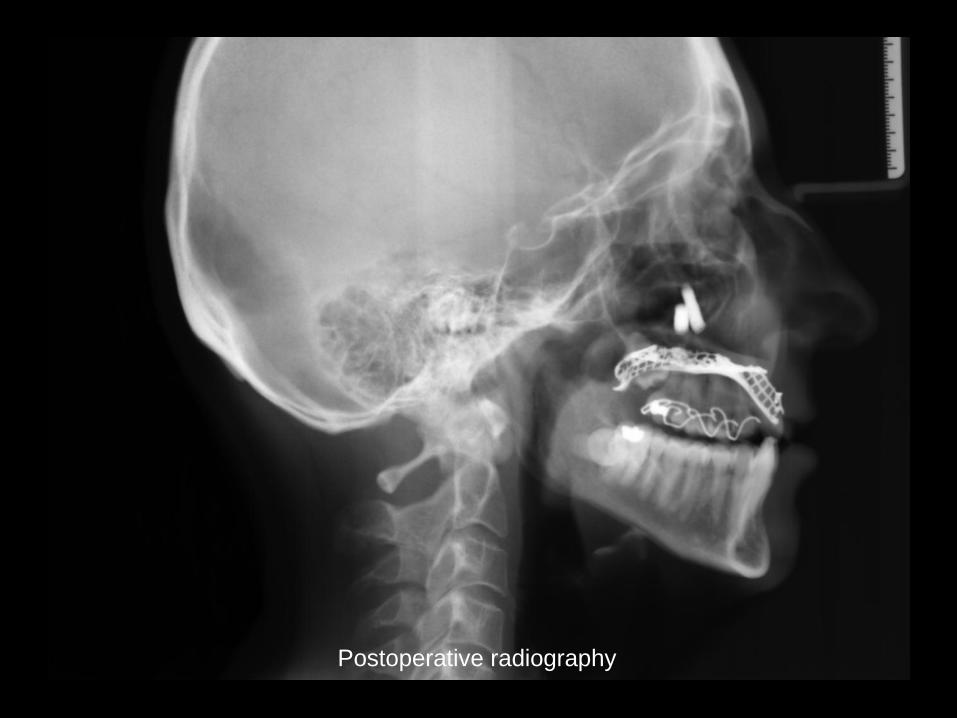
Postoperative radiography
Postoperative radiography
Postoperative radiography
Note the very cranial position of the newly placed implant
Case 2
• Situation after reight maxillectomy for
adenoid cystic carcinoma
• No radiotherapy
• Very limited bone volume due to resection
of large part of zygomatic bone
• Planning:
– 1 implant in zygomatic bone
– 1 implant in lateral orbital rim partially
crossing the orbital floor



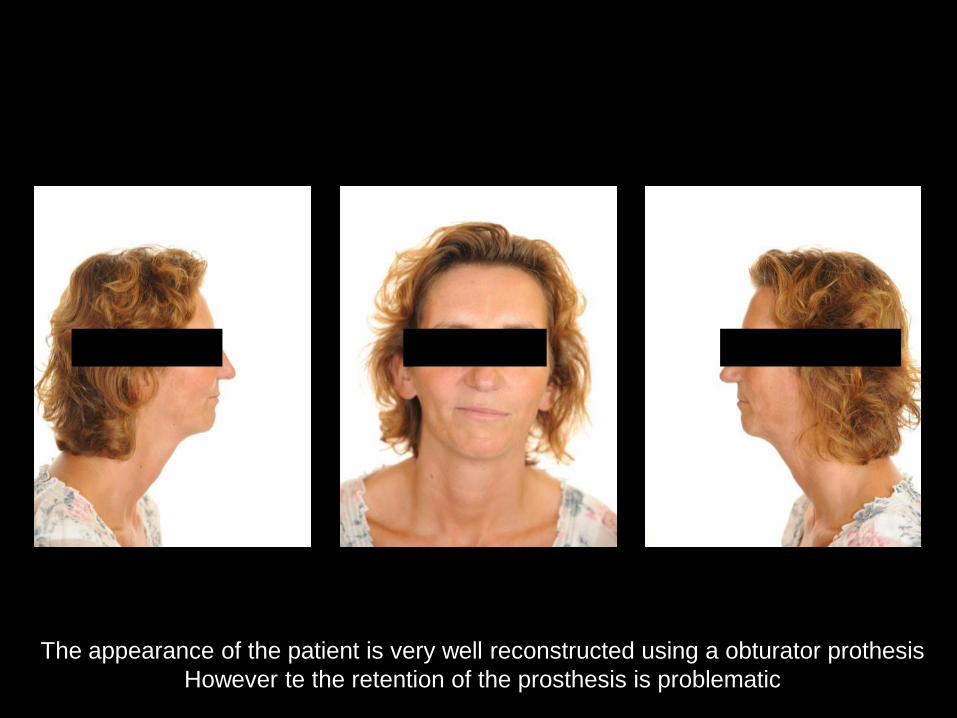
The appearance of the patient is very well reconstructed using a obturator prothesis
However te the retention of the prosthesis is problematic
The appearance of the patient is very well reconstructed using a obturator prothesis
However te the retention of the prosthesis is problematic

03/09/2011: Intake

03/09/2011: Intake
3D Treatment planning
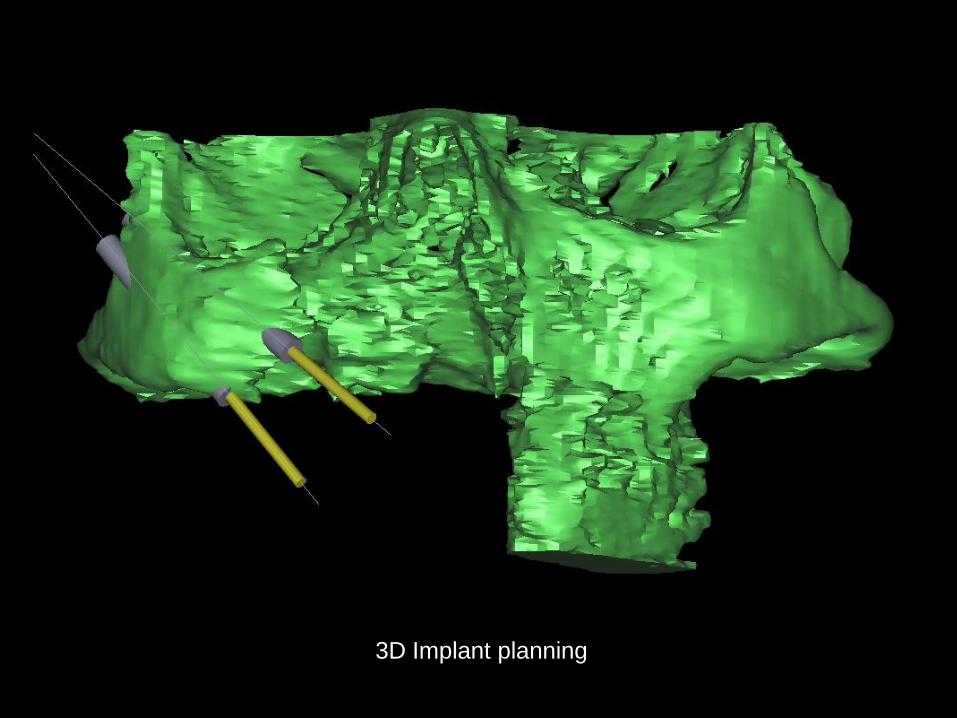
3D Implant planning
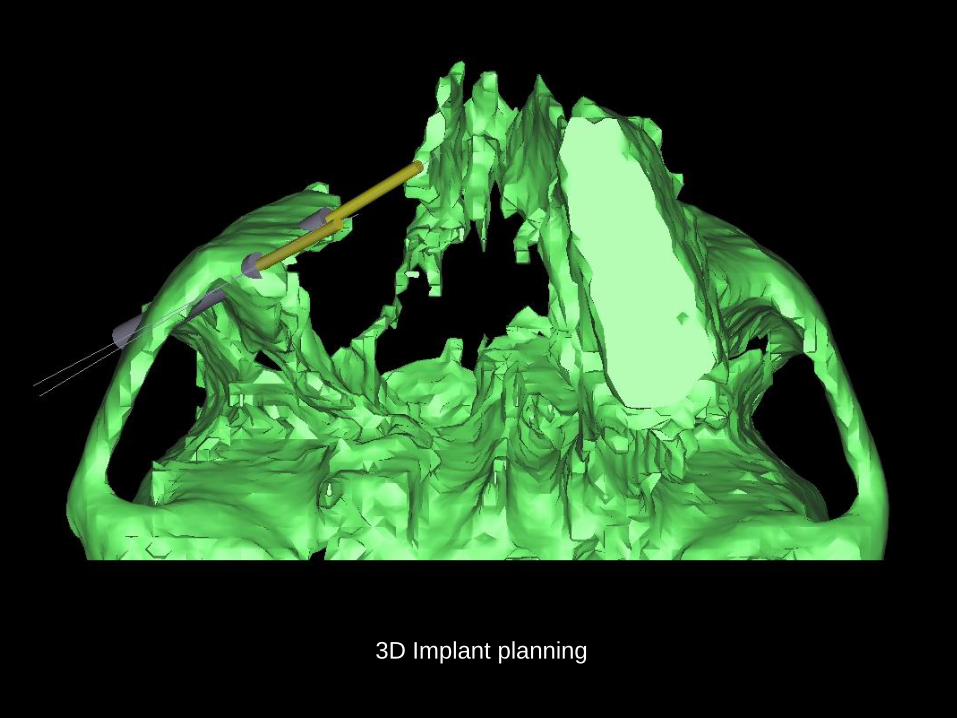
3D Implant planning
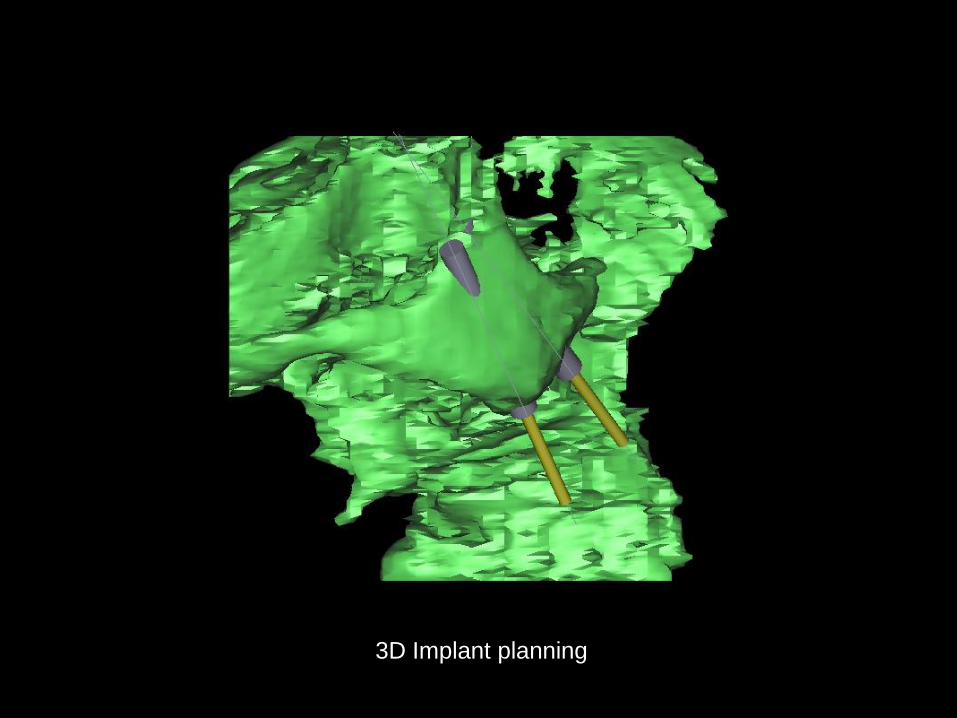
3D Implant planning
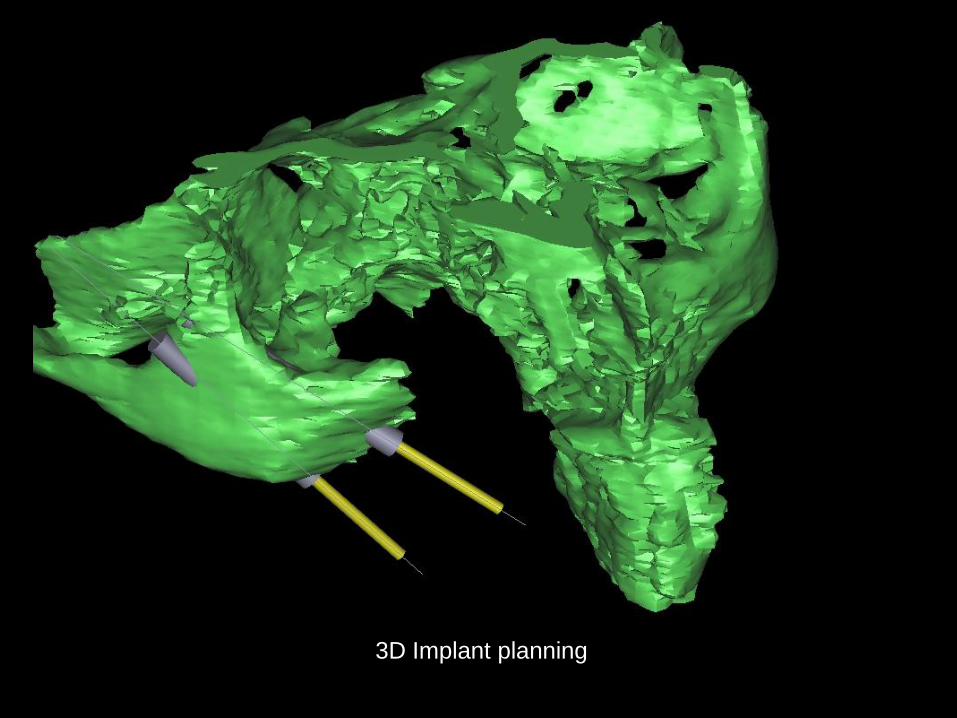
3D Implant planning
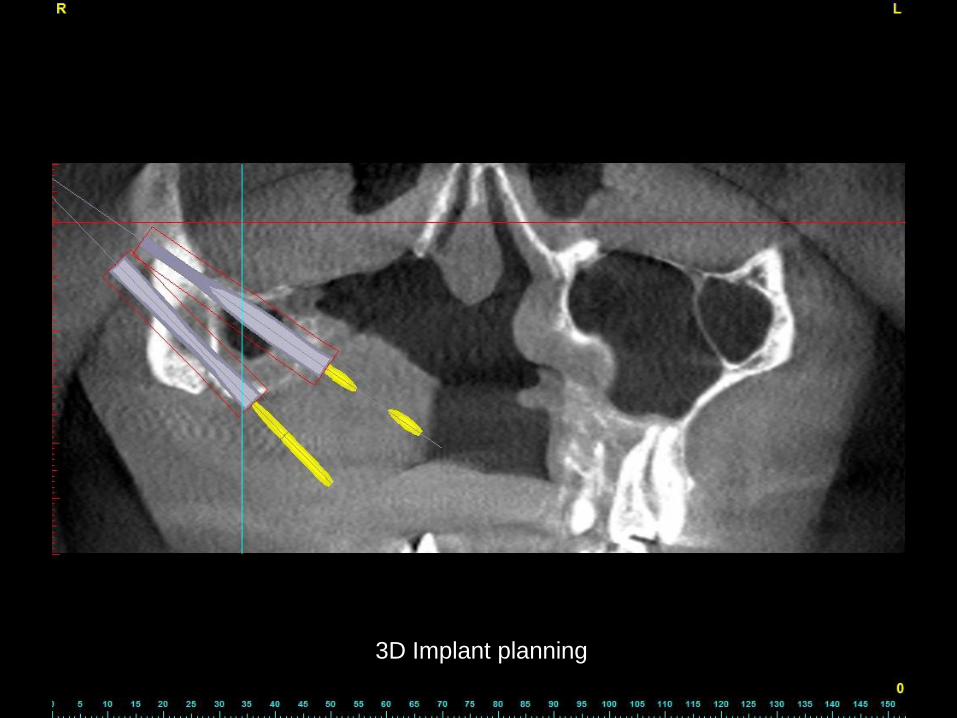
3D Implant planning
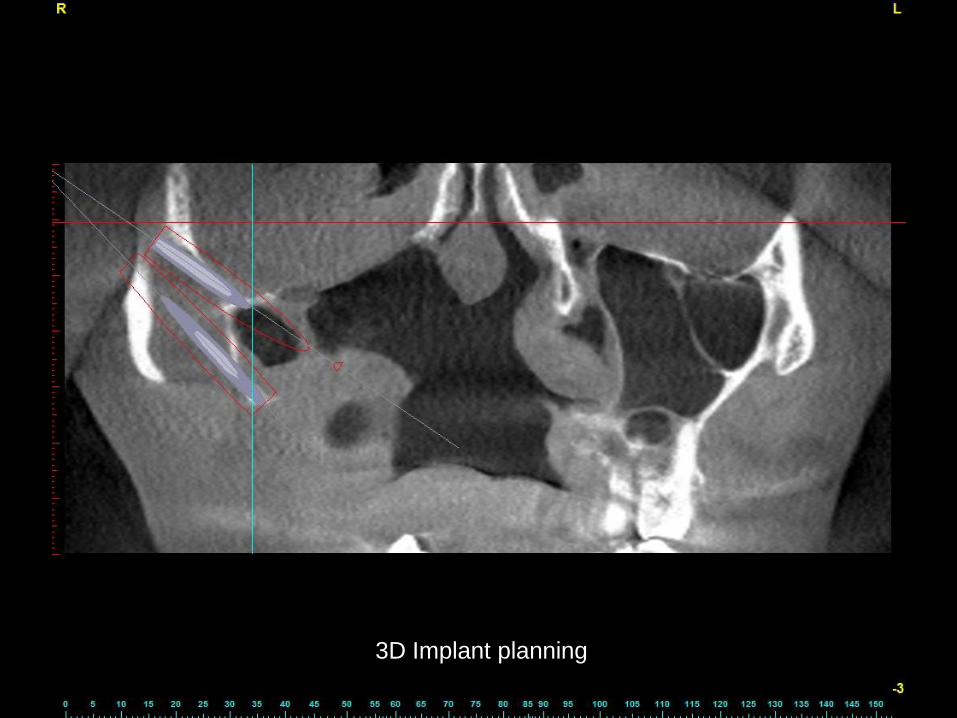
3D Implant planning

Exposed outer surface of zygomatic bone with initial drilling
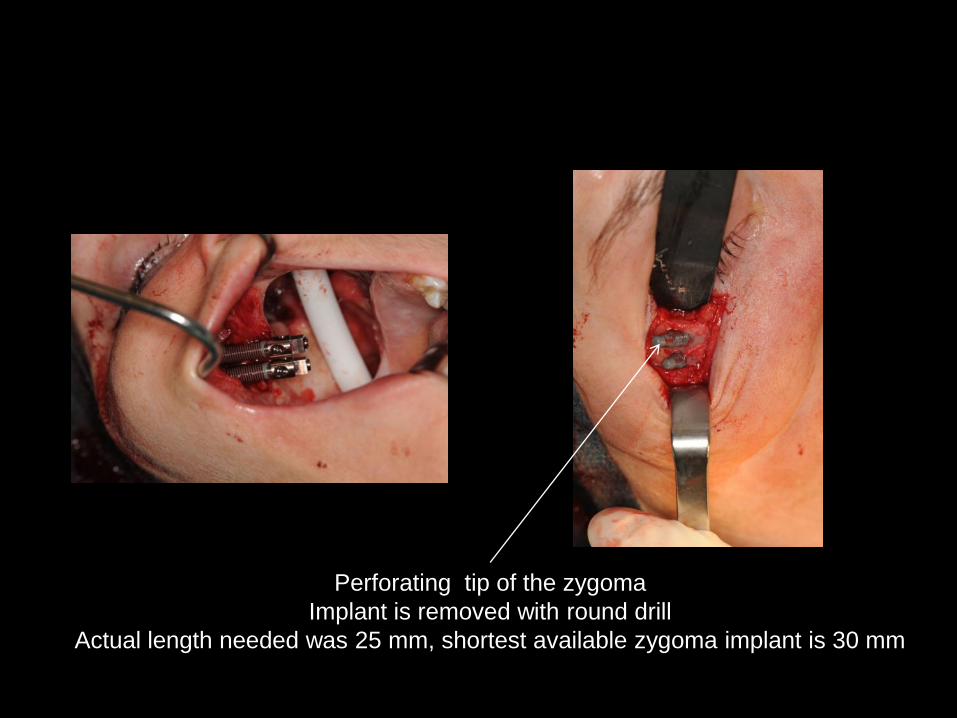
Perforating tip of the zygoma
Implant is removed with round drill
Actual length needed was 25 mm, shortest available zygoma implant is 30 mm

Postoperative radiography
Postoperative radiography
Postoperative radiography

Postoperative radiography