EXTRAOCULAR MUSCLE TRANSPLANTATION* BYRogerL....
33
EXTRAOCULAR MUSCLE TRANSPLANTATION* BYRogerL. Hiatt, MD TRANSPLANTATION OF EXTRAOCULAR MUSCLES IS HAMPERED BY THE SAME factors of muscle transplantation elsewhere in the body; the blood and nerve supply to the muscle from the donor site must be transferred in- tact to the recipient site, while maintaining their functions. If the muscle tissue remains viable, however, there are then some benefits to be gained from transplantation even if the muscle tissue is not contractile. Trans- plantation in this study is defined as detachment of the tissue from the body and its placement in another site in the body. This is in contrast to transposition in which a portion of the tissue remains attached to the body while another portion is placed at a new site, such as in a pedicle skin flap. Transposition is often incorrectly called transplantation in the literature referring to ocular muscle transplantation. OCULAR MUSCLE TRANSPOSITION Numerous authors have described various methods of transferring one or more insertions of the six extraocular muscles to a new site. In general, if a tendon or muscle is moved in the natural line of action (as in a simple recession), this is then not called transplantation, transposition, or any special term. However, when a portion or all of the tendon is moved up or down, nasally or temporally, or in any other direction from the natural line of action, this is often called transplantation. In reality, this is trans- position of muscles and will be so treated in this study. Most of the procedures of transposition described in the literature are for paralytic strabismus of one or more of the extraocular muscles.1'16 From the University of Tennessee College of Medicine, Department of Ophthalmology, Memphis, Tennessee 38163. This study was supported in part by the Ophthalmology Education Fund. TR. AM. OPHTH. Soc., vol. LXXI, 1973
Transcript of EXTRAOCULAR MUSCLE TRANSPLANTATION* BYRogerL....

EXTRAOCULAR MUSCLETRANSPLANTATION*
BYRogerL. Hiatt, MD
TRANSPLANTATION OF EXTRAOCULAR MUSCLES IS HAMPERED BY THE SAMEfactors of muscle transplantation elsewhere in the body; the blood andnerve supply to the muscle from the donor site must be transferred in-tact to the recipient site, while maintaining their functions. If the muscletissue remains viable, however, there are then some benefits to be gainedfrom transplantation even if the muscle tissue is not contractile. Trans-plantation in this study is defined as detachment of the tissue from thebody and its placement in another site in the body. This is in contrast totransposition in which a portion of the tissue remains attached to thebody while another portion is placed at a new site, such as in a pedicleskin flap. Transposition is often incorrectly called transplantation in theliterature referring to ocular muscle transplantation.
OCULAR MUSCLE TRANSPOSITIONNumerous authors have described various methods of transferring one ormore insertions of the six extraocular muscles to a new site. In general,if a tendon or muscle is moved in the natural line of action (as in a simplerecession), this is then not called transplantation, transposition, or anyspecial term. However, when a portion or all of the tendon is moved upor down, nasally or temporally, or in any other direction from the naturalline of action, this is often called transplantation. In reality, this is trans-position of muscles and will be so treated in this study.Most of the procedures of transposition described in the literature are
for paralytic strabismus of one or more of the extraocular muscles.1'16
From the University of Tennessee College of Medicine, Department of Ophthalmology,Memphis, Tennessee 38163. This study was supported in part by the OphthalmologyEducation Fund.
TR. AM. OPHTH. Soc., vol. LXXI, 1973

Extraocular Muscle Transplantation
Since we are concerned with transplantation in this study, further dis-cussion of these procedures, in which suturing of the muscle to the globeis performed in only one place, will not be given.An unusual example of transposition is moving the insertions of the
muscles to the orbital wall in order to nullify their action in nystagmus.17The tendon transposition may be to some site other than the globe.
Motais'8 and Berke19 described moving the superior rectus to thelevator insertion for ptosis of the upper lid.
Other authors, such as Knapp20 and Moller,21 described movingthe site of insertion of muscles and tendons for treatment of the so-called"A and V" syndromes, or in special cases of palsy, as in double elevatorpalsy.22One fascinating transposition of muscles was an attempt to increase
the blood supply to a particular portion of the globe, by transposition ofthe inferior oblique to the macular region in senile maculardegeneration.23' 24And lastly, experimental work has been performed in which the inser-
tions of muscles have been exchanged in order to study the action. of suchmuscles and the innervational plasticity of the ocular motor system.25-28
OCULAR MUSCLE SUBSTITUTION EXPERIMENTATION
Interest in extraocular muscle transplantation has increased because ofthe need or desire to lengthen a muscle when all the other steps such asrecession and myotomy have been taken. Most work, however, has cen-tered around the substitution of other material, both foreign and auto-genous, to attach the muscle to be lengthened.
Jampolsky29 has suggested using a vein from the leg or the ante-cubital space, because of its elastic properties and its likelihood of re-maining not only viable, but also of retaining some of its naturalproperties.
Beisner30 was interested in preserving the natural insertion of anextraocular muscle by using a silicone tendon prosthesis. Silastic 372 andsilicone were calendered over dacron mesh, and a dacron suture wasused to anchor the material. A breakdown of Tenon's capsule occurredin 11 of 24 dogs in recessions of 5-15 mm from two weeks to nine monthsafter operation. A fibrous capsule around the implant was often adher-ent to the sclera.Bowen and Dyer3' lengthened the lateral rectus of 14 dogs and ob-
served them for 10-20 days. They performed the procedure with sili-cone that had been calendered over dacron mesh to prevent 5-0 blacksilk sutures from tearing out. Some adherence to the globe remained
427

even after long periods in vivo prohibiting the prosthesis from acting per-fectly as tendons.
Morales, Polack and Arata32 used 6-0 catgut and silk sutures onplain silicone sheeting to lengthen the superior rectus in 12 rabbits whichwere observed from one to five months. No breakdown occurred in therabbits, and the posterior portion of the implant was free from scar. Theprocedure was performed on two patients with large angle esotropia andamblyopia who maintained good motility and good tolerance to theimplant.Roman, Fazio, Brzezinski and Ferrarexi33 recessed the medial rec-
tus muscle and sutured it to an implant of silicone sheet the width of themuscle and in a plane with the muscle in order to lessen the action of themuscle. This procedure was performed to correct a large angle esotropiain 11 patients. In another group of 11 patients, the same procedure wasdone, plus a resection of the lateral rectus, with no significant differencein the amount of correction from the first group. In a group of patientswith esotropia, the medial rectus was recessed and the lateral rectus re-sected in 23 patients. In a second group of 14 patients, the medial rectusalone was recessed. The latter operation gave about one-half as muchcorrection as did the former operation.
Palmieri34 used lyophilized organic grafts to the extrinsic ocularmuscles in rabbits. In the first group, transplantation of human fascialata to the lateral rectus was accomplished. In the second group, animaltendon transplantation of the same species, but not the same animal, wasused. The tendon was lyophilized in glass and transplanted to the supe-rior rectus of the right eye and substituted between the cut ends of themuscle. Little reaction was found to occur in some, but the hyalinizationand fibrosis were more severe in the human transplanted fascia lata thanin autogenous tissue.
NONOCULAR MUSCLE TRANSPLANT EXPERIMENTATION
Significant information which should be considered in evaluatingocular muscle transplantation has come from efforts to transplant otherbody muscles. Carlson35 removed 50 pubo-ischio-tibialis muscles inmature axolotls. He mixed the fragments and replaced them into thesite from which the muscle was removed. Both gross and histological re-generation of the muscle was similar to that observed in frogs and rats.There was an initial period in which sarcoplasm formed from the mincedmuscle fragments. Following this, a population of myoblasts was estab-lished, and the regeneration of muscles from minced fragments could becompared with the formation of muscles in regenerating limbs.
428 Hiatt

Extraocular Muscle TransplantationTamai36 performed a successful transplantation of an isolated mus-
cle using microsurgical technique. The rectus femoris muscle, attachedby a neurovascular bundle, was freed from a canine thigh and auto-transplanted orthotopically and heterotopically. He evaluated thegrafted muscles with light microscopy, electron microscopy, and electro-myography. He found the muscle to be viable and functional and sug-gested this operation in conditions such as Volkmann's contracture.
Allbrook37 did a study of skeletal muscle autotransplantation andregeneration in adult rats. He suggested that when small fragments ofstriated fibers are transplanted, rather complete reorganization and re-constitution of the muscle belly results.
Zhenevaskaya38 showed that transplanted muscles in rats, rabbits,and dogs tend to undergo complete restructuring which he called "trans-plantation regeneration".Mepomnyashchikh39 did autotransplantation of somatic muscle in
the myocardium of dogs and found replacement of the defect by connec-tive tissue in 20-25 days. Autografts of minced cardiac and somatic mus-cle tissue transplanted to the myocardium of dogs developed myogenicelements. The somatic muscle fragments formed muscle bands withmyoblasts, myosymplasts, and muscle tubes. Histochemical evaluationof the newly formed myogenic elements showed that they contain largeamounts of RNA, indicating an increase of protein synthesis in regen-erating tissue. The transplanted muscle was completely filled with con-nective tissue in 20-22 days.
WOUND REPAIR
The repair of the wound between muscle and muscle, and between mus-cle and sclera, must be considered in any discussion of ocular muscletransplantation.
Carroll and Blake40 studied the repair of extraocular muscles in rab-bits, both grossly and histologically. In the recession operation, even bythe 11th postoperative day, there was organized mature granulation tis-sue. In the eyes in which a complete tenotomy was done, a normalmuscle was found bound to the sclera by closely interwoven connectivetissue by the 21st postoperative day. By the 40th postoperative day,dense fibrous tissue became interwoven between the muscle fibers andheld the muscle firmly together.
In 1945, Chouke41 reported the gross and histologic changes fol-lowing a tucking operation. In 1963, Carusillo42 described the healingfollowing disinsertion and reattachment of muscles in rabbit eyes. In1965, Truhlsen43 reported his extensive histopathological study of the
429

recession operation including a study of various kinds of gut suture re-actions and absorption. He performed 72 recession operations in 34white rabbits followed by enucleations at intervals of 1, 3, 5, 7, 14, 21,28, and 60 days. Three human patients were studied on whom the reces-sion was done on a lateral rectus of eyes scheduled for enucleation thatwas performed at 1, 2, and 4 weeks after the recessions. In the rabbits,the exudative reaction was predominant, but fibroplasia began soon afterthe operation. Both humans and rabbits showed a proliferation responseand formation of new collagen by the seventh day. The human eye show-ed firm adherence by 28 days following surgery. It is interesting that hefound the new insertion site was wide, and the posterior line was a mini-mum of 1 mm, and the maximum of 4 mm behind the point of surgicalplacement.
Ingram44 45, 46 reported his extensive work on wound healing follow-ing extraocular muscle surgery in 1965 and 1966. He compared catgutand silk in recession and resection operations on rabbits. Inflammatoryreaction was found to be most severe two to four days postoperatively.Growth of fibrous tissue began on the third day, and by the fifth daymuscles were reattached and became very firmly reattached on the 10thday. From 10-28 days, regeneration of the muscle took place. He alsonoted that the catgut, when compared to silk, showed no significant dif-ference in the amount of reaction and the final reattachment of themuscle. In his second article he described the rate of muscle attachmentto the sclera following the recession and resection operations in rabbits.He showed that the muscle becomes united to fibrous tissue at the samerate as a muscle wound heals. The rate at which both of these woundsattained the strength of the normal unoperated muscle-to-sclera junctionwas 10-14 days after operation irrespective of whether catgut or silksutures were used. The rate of healing was determined by the depositionof fibrous tissue, and the tensile strength of the wound was considereda valid measure of the amount of fibrous tissue present. The tensilestrength was determined by using the Scott Thread testing machine. Healso determined that 5-0 chromic and 4-0 silk sutures provided the moststrength for muscle surgery, and that no wound strength increases be-fore the fourth postoperative day.
Ingram's third report described the healing after recessions, tenoto-mies, reattachments, and reefings in monkeys. He performed 24 lateralrectus recessions and 24 medial rectus tenotomies and reattachments,and did 11 medial rectus muscle recessions combined with excision ofTenon's capsule, and 11 lateral rectus reefings. He felt that the reactionin rabbit eyes is not entirely comparable with reactions in man because
Hiatt430

Extraocular Muscle Transplantation
of dissimilarities in the muscle insertions. He concluded that injury to theperitendon seems to be a more likely cause of adhesions between tendonand sclera then bleeding. Muscle tissue, in his opinion, was the sourceof fibroblasts, and adhesions were more likely to be the result of repairof trauma than the result of cautery. He also stresses that Tenon's capsulewas not necessary in the union of muscle to sclera, and he regards the in-cision in Tenon's capsule as another wound distinct from the underlyingtendon to sclera wound. He further concludes that there was no logicalmethod of restricting the forward extension of fibrous tissue at the re-attachment site, and the suture position does not affect this "pseudo-tendon" development. His last major point is that meticulous wound clos-ing can help prevent unnecessary adhesions.
SYNTHETIC AND ORGANIC SHEETING AND ADHESIVES
In the substitution operation on the extraocular muscles, adherence tothe sclera has been of concern to all workers in this field. Dunlap,47 hasdescribed the use of tubes and sheets of Silastic 372 and other plasticmaterials in managing extraocular muscle restrictions. Gelfilm, Mylar,Saran, medical Silastic 372, and Supramid were all tested. He concludedthat the site of placement makes no difference in the success of the ex-perimental surgery. The polyfilament cable type sheeting was noted toproduce the least amount of reaction. Rabbits were used, and the materi-al was put under, over, and around muscles. When he used Gelfilm undersimilar circumstances, it absorbed in approximately sixteen weeks.
Berens48 49 used Tenon's capsule as a transplant under the musclethat had become scarred to the sclera in the eyes of three patients. Hefelt this was helpful, but not curative, and needed more study.
Dunlap50' 5 did an evaluation of the synthetic cyanoacrylate adhe-sives as a possible replacement for muscle sutures in rabbits. He foundthat there was an inadequate bond formed and thought extension ofmuscle tissue in front of the adhesion with the sclera negated the maxi-mum measured placement of the muscle. Because of the small musclesand tendons of the dog and rabbit and the difficulty of suturing them, theadvantages of sutureless surgery in transplantation becomes evident.
METHODS AND MATERIALS
The basic design of our experimental procedure was to resect or excisea portion of one extraocular muscle, suture it to the disinserted end of asecond extraocular muscle, and then to reattach the free distal end of thetransplanted muscle to the sclera. Numerous variations of the standard
431

techniques were planned to study the effect of various parameters onthe surgical procedure.The transplantation of a portion of extraocular muscle was first at-
tempted on three white albino rabbits weighing approximately sevenpounds each. The six eyes of the three rabbits were subjected to thesame procedure of transplanting a portion of the inferior rectus to thesuperior rectus. In each instance, cyanoacrylate adhesive was used in-stead of suturing. The rabbits were killed after three months and micro-scopic study of the tissue performed. The procedure was then abandonedon rabbits for two reasons: (1) The fragile tendonous-muscle was diffi-cult to handle and attach to another muscle because of its fragility andsmall size, and (2) After studying the microscopic tissue, it was foundthat there was fragmentation of the transplanted portion, and the diffi-culty of applying a minimal amount of "glue" made the specimen un-satisfactory for study. The recipient muscle also tended to fragment, andthere was an excessive amount of reaction around the adhesive. Thehealing, however, was complete and Tenon's capsule and the underlyingsclera were loosely adherent to the transplanted muscle.
Following the experimentation with the rabbits, a segment of the lat-eral rectus was transplanted to the medial rectus in five eyes of threedogs. Sutures of 5-0 mild chromic catgut were used. The muscles werestudied grossly and microscopically at the end of 4.5 months. The stan-dard protocol was then developed and extensive studies were done using27 dogs.
Table 1 lists the eyes of each animal studied, the surgical procedure,any special technique, the postoperative period before the animals werekilled, and the disposition made of the eyes. A number of procedureswere performed, including lateral rectus transplanted to medial rectus,superior rectus to inferior rectus, etc. before the standard procedure wasdeveloped.The standard procedure consisting of transplanting the inferior
oblique to the lateral rectus and was used for most of our comparativestudies. Certain special techniques were used to evaluate the changesproduced by variations of the standard procedure.Dogs weighing from 30-35 pounds were used. These animals were pre-
pared by the veterinarian who used dichlorvos (Task from Shell Chemi-cal Company) anthelmintic capsules in the recommended dosage, alongwith distemper-hepatitis (Affiliated Laboratories, Inc.) vaccine, and dio-xothion insecticide (Kem Dip from Vet-Kem Laboratories, Inc.). The dogswere debarked by sectioning of the vocal cords under anesthesia. Thispreparation required approximately three weeks.
432 Hiatt

000 0 0 0
00 00 00 00 co 00 00 00
eq eq eq eq
Ci Ci CiCi Ci Ci C] Ci >~~"0
33000
.40.2 'o.. .4z .4
~4.0--~4-
00 cn
0 r;
oo'.
9 ,o. B 10) ^0 0 WCEEv ~D
C Mc0 U0a0 M:00 0o 00 0o 00 00 0o 00 00 0o
eq c tL C - 00 0
z0
0
0
P:RU
0V)
Ut
aE
a)
WA
K C.Scn 9
W8 2u
a)
zz.49 .4
0." -S
m .4

00 0
00 00 00
*.S *.e .S
ci c] oci
N C4 CX
c04 E04
00
00
.2 40 0 0 0 .00.0 000~~~.20 0 00.2 .2o~~~~~~~~~~c CAtoo
00 c 00
C0 co c0i
0000--I
13"o
°22~~"0*sE 00 0000 00
00000 0 0 000co0 0 00
- o co o 4 LOO Oa- - - - -C - "
00
c0
- -0
tQ a.0

Obo bo Obo b N bo bo
C u) C u) C u)
) ()G() C) 0L) ) 0 L0) CL0 ) 0) 0
- . . . . . -9 - IP-4-A - .
w r.)
- CiC* -
co t~- tL- co LO~ OM - CO
cd
w 0
.240
k1
115-i..O
1.004
W; W
- 4= = tA
co cn0~~00 ' .0
00 ~0 00 00w --14m~-4-
00 000-0r; 1-4;
o!o4o
0: 00 00 0000 00 0 00 00)9co co oo co o oooo Coooo oo
00 0m C)- l co LO cor-4 r- cqi eli oli oi Cl 0 1
.,OZ.4&.4. -.0w0
. .--4
t-cq

SURGICAL PROCEDURE
1. AnesthesiaFifteen milligrams of morphine was given intramuscularly 45 minutespreoperatively, along with 0.5 mgm/lb of hydroxyzine (Vistaril). Intra-venous pentabarbital was given initially at the rate of 10 mgm/lb, withthe intravenous continued throughout the procedure using a drip of 5%odextrose and water and additional pentabarbital as needed. The prepara-tion and the draping consisted of clipping the hair around the eyes with abarber's clipper and using .25%o hexachlorophene and 90%o ethyl alcoholto dean the skin. A drop of argyrol was then instilled into the eye andthe eye was irrigated with saline until clear. Two drops of polymyxinB-bacitracin-neomycin (Neosporin) and two drops of 101o phenylephrinehydrochloride (Neo-Synephrine) were then placed in each eye.
2. Surgical TechniqueThe standard procedure which was developed consisted of transplantingthe inferior oblique to the lateral rectus and will be described in detail.A speculum was placed in the eye, and a 4-0 black silk suture was usedas a marking suture at the limbus, indicating the position of the lateralrectus. A lateral canthotomy was performed after clamping the lateralcanthus with a hemostat (Fig. 1, A). An opening was made horizontallyinto the conjunctiva by using an inferior cul-de-sac incision. A separateincision was made somewhat more vertically into Tenon's capsule. Asmall muscle hook was placed under the lateral rectus, and this was re-placed with a large muscle hook. The lateral rectus was then freed ofall connective tissue. (Fig. 1, B). A 6-0 black silk suture was then thread-ed through the insertion of the lateral rectus and double tied at both thesuperior and inferior borders. The lateral rectus was then freed from theglobe and retracted out of the way. The inferior oblique was likewisecleaned and freed, and a muscle clamp was placed near its insertion tothe globe. It was then freed from the globe, and approximately 15 mmof the muscle was resected allowing the remainder of the muscle to re-tract into the orbit. If technically easier, a suture was placed in each endof the inferior oblique (Figs. 1, c and D). The previously placed 6-0black silk suture in the lateral rectus was then brought through the mar-ginal tips of the former insertion of the inferior oblique held in the mus-cle clamp, then brought again through the center of the lateral rectus,and then finally through the center of the inferior oblique where it wastied. (Fig. 1, E). A 5-0 mild chromic catgut suture with a spatula needlewas then inserted into the other end of the inferior oblique in a similarmanner to the 6-0 black silk placed in the lateral rectus. This suture was
Hiatt436

Extraocular Muscle Transplantation. yS -_E M~~~~1
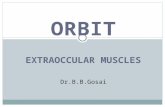
FIGURE 1
A: Dog 22 O.S., lateral canthotomy performed and incision in Tenon's capsule. Limbalmarking suture at the 3 o'clock position. B: Dog 10 O.D., lateral rectus and inferioroblique exposed with eye adducted and hooks under each muscle and forceps holdingTenon's away. c: Dog 10 O.D., suture placed at insertion of inferior oblique with hooksunder inferior oblique and lateral rectus. D: Dog 10 O.D., 5-0 black silk suture in distalend and 5-0 chromic catgut suture in proximal end of transplant of inferior oblique.E: Dog 21 O.S., transplanted inferior oblique attached to lateral rectus with 5-0 black
silk suture. F: Dog 21 0.S., inferior oblique sutured to former insertion of lateral rectus.
437

then placed in the sclera at the former insertion of the lateral rectus andtied (Fig. 1, F). Tenon's capsule was reapproximated over the trans-planted inferior oblique-lateral rectus muscle with 6-0 plain catgut su-ture, and the conjunctival incision was closed with the same suture. Thelateral canthotomy was closed using 6-0 black silk which was left inplace.
Postoperatively, two drops of polymyxin B-bacitracin-neomycin oph-thalmic solution were instilled into the eye, and the animal was giventhe same dosage of hydroxyzine hydrochloride as was given preoperative-ly. The only other medication given postoperatively at any time consistedof polymyxin B-bacitracin-neomycin ophthalmic solution if any infectionoccurred.
3. Modified Exenteration TechniqueThe dogs were killed by giving five cc of Barb-Euthol (veterinarian)intravenously until respiration and cardiovascular collapse occurred.The 4-0 black silk limbal marking suture was identified. The upper andlower lids were sutured together at the gray-line with 4-0 black silk su-tures which were left long. An incision was made down to the orbitalrim circumferentially around the entire orbit. An incision was then madethrough the fascia and the periosteum, and the globe was freed circum-ferentially from the orbit using curved blunt scissors being very carefulto avoid damage to Tenon's capsule. Using blunt dissection and spread-ing, the optic nerve and Tenon's capsule were cut as near to the apex ofthe orbit as possible, and the globe and contents were lifted from theorbit. The lids, skin, and fat were then dissected from the globe, withcare being taken not to distrub the underlying transplanted muscle asidentified by the limbal marking suture. Another 4-0 black silk markingsuture was placed into the cut end of the lateral rectus for identification.
4. Special Procedures(a) Isobutylcyanoacrylate adhesive: This was used in six dog eyes us-
ing the standard procedure as described previously. Instead ofusing sutures, a chromium plated spatula was used to apply thecyanoacrylate adhesive directly to the two adjoining portions oftissue to be joined. The two portions were brought together im-mediately, and instant adhesion occurred. The remainder of theprocedure was identical to the standard procedure.
(b) Supramid: In order to study the effect of the anticipated adhesionsbetween the transplanted muscle and other ocular structures,Supramid (superpolymid) was used in the standard procedure in
438 Hiatt

Extraocular Muscle Transplantation
seven dog eyes. Supramid sheets 0.05 mm thick were placedunder the transplanted inferior oblique-lateral rectus and suturedto the sclera using 6-0 Supramid sutures at the four corners of thesheet of Supramid. The sheet of Supramid was made to extendtwo mm beyond the width and length of the transplanted inferioroblique. The remainder of the procedure was as described for thestandard procedure.
(c) Tenon's Capsule: In two eyes, a portion of Tenon's capsule wasused as a tongue flap and sutured under the transplanted inferioroblique-lateral rectus. The flap was anchored to the sclera with6-0 mild chromic catgut sutures and allowed to protrude a fewmillimeters beyond the border of the transplanted inferioroblique. In two dog eyes, a tongue of Tenon's capsule was suturedto the original stump of the lateral rectus after complete tenotomyof the lateral rectus was performed.
(d) Muscle Incisions: In the study of wound healing in normal mus-cles of two dog eyes, the medial and lateral rectus muscles wereincised seven mm posterior to the insertions and then resuturedwith 5-0 mild chromic catgut. In two dog eyes, the right lateralrectus was completely incised at both the insertion and seven mmposterior to the insertion, and was then resutured with 5-0 mildchromic catgut sutures.
EVALUATION OF TECHNIQUES
In order to evaluate the procedures, a protocol was followed to study thereactions of the eyes in the live animal, the gross and microscopic speci-men after modified exenteration, and the tensil strength. A scale of +1or excellent, +2 or good, +3 or fair, and +4 or poor was used. Pre-operatively, the animals were rated +1 to +4 for cooperation, excitabil-ity, general health of the dog, and overall suitability for the proce-dure. Likewise, the globes were rated +1 to +4 for factors such asinflammation and presence of deformity. If necessary, a loupe and hand-held slit lamp were used to study any type of gross abnormality detected.Preoperative photographs were taken for further study on all dogs, andoperative photographs were taken periodically to document the surgicalprocedure. Postoperatively, the animals were examined grossly andphotographs were taken (loupe and slit lamp examinations were done ifindicated) on at least the third, seventh, 14th, 21st, 28th, and 60th days.
Motility was also observed and rated +1 to +4. The overall grossreaction during the postoperative period was likewise evaluated. Whenthe animals were killed, the healing and gross reaction of the eye was
439

noted, and the modified exenterated specimen was likewise examinedgrossly and was evaluated for reaction, scarring, abnormalities, andother defects. Photographs were taken during the exenteration for il-lustration, along with photographs of the exenterated specimens beforethey were submitted for further study.1. Microscopic StudiesThe eyes for microscopic study were placed in 10%o formalin immediate-ly. After proper fixation and washing in 60%o alcohol, the globe wasopened with a flat razor blade and sectioned parallel to the transplantedmuscle and in the plane of the transplanted muscle as directed by thetwo marking sutures. After using alcohol and chloroform washings, itwas then fixed in paraffin for five hours with several changes and pre-pared for the microtome. Sections of eight microns were made at variousplanes through the transplanted muscle-globe structures. H & E, Mas-son's trichrome, and Mallory's PAH stain were used on all specimens.The slides were studied for evaluation of the following factors:
(a) General reaction from gross observations.(b) Evaluation of the muscle transplant itself as to viability and the
retention of muscle elements.(c) An evaluation of the muscle transplant reaction in the recipient
muscle especially at the junction site.(d) Tenon's capsule response to the surgery as to looseness or scar-
ring involving the transplanted recipient muscle.(e) The healing process between the transplanted muscle and the
scleral junction.(f) The reaction of the sclera and signs of adhesions between the
transplant and the recipient sclera along the body of the muscle.Blood vessel and inflammatory cell invasion was studied ifpresent.
(g) Suture reaction at the sites of muscle to muscle and muscle tosclera junctions.
2. Tensile StrengthThe muscles of 12 dog eyes were subjected to tests of tensile strength,three of which were the lateral rectus of unoperated eyes, and nine wereeyes that were operated upon using the standard procedure. The basictensilometer consisted of a custom-made device attached to a Hunter'sSpring Testing Gauge.# This instrument measures forces from zero to2220 gm at 10 gm intervals.
Hunter-Spring, a Division of Amtex Incorporated, Hartfield, Pennsylvania.
440 Hiatt

Extraocular Muscle Transplantation
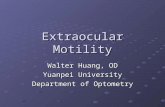
FIcuRE 2A: Tensilometer used to measure the tensile strength with spring gage at upper end ofmuscle clamp and screw device at lower end near base. B: Dog 25 O.S., clamps of tensilo-
meter on corneo-scleral junction and on tip of lateral rectus 20 mm apart.
A device constructed like a muscle clamp customarily used in musclesurgery was attached to the spring at the upper end. At the base of theinstrument was a similar clamp with a custom-made rotating screw-type wheel which allowed the instrument to produce one mm of separa-tion of the two muscle clamps for every one and one-half turns of thewheel (Fig. 2, A). When the tensile strength of the transplanted musclewas to be tested, the specimen was immediately placed in saline after themodified exenteration. It was then dissected, leaving a portion of thecornea near the limbal marking suture. The sclera was sectioned parallelto the transplanted muscle and back to the optic nerve. One muscleclamp of the Tensilometer was then clamped over the cornea-sclerajunction at the limbus, and the other was attached to the recipient lateralrectus-inferior oblique transplanted muscle, 20 mm from the other clamp
441

(Fig. 2, B). Thus the transplanted muscle to sclera and muscle to musclejunctions were between the two clamps. The force was then graduallyapplied at the rate of 10 gm/sec., and the observation was made as towhich portion of the tissue junction stretched and broke, and at whatlevel of force this occurred.
RESULTS
The results were recorded under the heading of general findings, micro-scopic studies, special techniques, and tensile strength studies.GENERAL FINDINGS
1. The general status of the animals was excellent except in two animalswhich were rated only fair in that the hyperactivity of the dogs prohibitedobtaining good cooperation for daily follow-up after the surgery. Theglobes were all of good or excellent quality with no abnormalities or in-fections that would prohibit judging the parameters of the study.
2. During the postoperative period the overall reaction produced by thesurgical procedure was rated excellent in all except three animals inwhich there was some minimal infection. The infection was treated withpolymyxin B-bacitracin-neomycin ophthalmic solution.The gross reaction to the surgical procedure as rated by loupe, gross
examination, photography, and slit lamp examinations was good to ex-cellent except in eight of the eyes in which there was considerable chem-osis and generalized swelling. In three of these eight eyes, the cantho-tomy had to be resutured during the postoperative period, but there wasno extrusion of sutures, transplanted muscle, Supramid, or any othermaterial.
3. MotilityMotility was difficult to judge. Some idea, however, could be obtainedduring the follow-up of the motility of the eye, and it was rated as good toexcellent in all eyes with none showing fair to poor motility.
4. External ExaminationThe gross examination at the time of the enucleation showed excellenthealing except in those dogs which were killed earlier than two weeks.By the end of two weeks, all eyes showed good to excellent healing withsubsiding edema, chemosis, and swelling, along with any signs of infec-tion that had been present.
Hiatt442

Extraocular Muscle Transplantation
5. Gross SpecimensThe gross specimens were all examined before any tests were performedeither for histologic study or tensile strength. Care was taken not to dis-turb the site of the transplanted muscle by paying particular attention tothe limbal suture which had been placed at the time of the initial opera-tion, and by the marking suture which was placed on the cut end of theextraocular muscle which received the transplant. The gross reaction ofthe conjunctiva, Tenon's capsule, the sclera, and the eye in general to thetransplanted muscle was rate +1 to +2 in all eyes (or excellent togood), with many of them showing only minimal signs of hyperemia andthickening of Tenon's capsule indicating that surgery had been per-formed. Special care was taken not to disturb the capsule, conjunctiva,sclera, etc. so that further analysis could be as accurate as possible.
MICROSCOPIC
Thirty-three eyes were subjected to transplants of one or more musclesand to histologic study with seven factors being evaluated.1. General reactionThe general reaction was rated good to excellent in all eyes except thatthere was a nodular reaction of (+3) rating in eight eyes.
2. The fate of the transplanted muscleIn all eyes, by the 28th day, the transplanted muscle had gone throughvarious phases of necrosis and replacement by fibrous tissue with oblit-eration of the capillaries in the transplanted muscle. However, an occa-sional muscle fiber could be identified even at the 28th day. A few moreremnants of muscle fibers could be seen up to 14 days than could be seenat 28 days. In the nine day eye, there were a few more muscle fibers re-maining. In the seven day eye, however, there was a nest of muscle fibersin various stages of necrosis and fibrous replacement. In the five day eye,it was estimated that about one-half of the muscle fibers were stillidentifiable (Fig. 3, A). In the three day eye, there were even moreidentifiable muscle fibers than in the five day animal.
3. The recipient muscleThe recipient muscle showed little reaction except at the junction pointbetween the recipient and the donor (Fig. 3, B). In the eyes that wereonly three to five days postoperatively, there were a considerable num-ber of red blood cells present at the junction between the transplant andthe recipient.
443

Hiatt
S. V i.,Ye:;::. i ,,
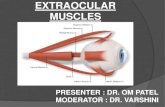
FIGURE 3
A: Dog 24 O.S., cross section of globe and photomicrograph (Masson's trichrome, XIOOtaken from region of arrow) showing suture reaction and necrosis of some muscle fibers andothers appear viable in portion of inferior oblique transplanted to lateral rectus. B: Dog17 O.S., cross section of globe and photomicrograph, (hematoxylin-eosin, X 100 takenfrom region of arrow) showing junction between recipient lateral rectus and transplanted
inferior oblique with suture reaction.
4. Tenon's capsule reactionSpecial attention was given not only to the reaction of Tenon's capsule,but also to the adherence of the capsule to the transplanted portion.Tenon's capsule remained thin generally, but the capsule became thick-ened and scarred in three of the eyes. The overall reaction of Tenon'scapsule was moderate with loose adherence to the underlying trans-planted muscle.
444

Extraocular Muscle Transplantation
5. Wound healingSpecial attention was given to the study of the healing of the transplantto the sclera anteriorly and to the recipient muscle posteriorly, particu-larly in eyes which were studied less than 14 days following surgery. Inall eyes after 14 days, there appeared to be a strong fibrous bond be-tween the transplanted tissue and the sclera, and between the trans-planted tissue and the recipient muscle. In the seven-day eye, there wasa considerable number of fibers formed, but in the five-day eye, therewere many red blood cells present, and fewer signs of fibrous tissue ap-peared at the junction site.
6. ScleraThe reaction of the sclera to the transplant was particularly noted alongthe extent of the transplant. In general, there were loose attachmentsbetween the sclera and transplanted muscles. In three instances, therewas some cellular reaction in the superficial layers and small vesselformation, particularly at the site of insertion of the transplanted muscle.
7. Suture reactionSutures were used in 28 eyes. The suture reaction around the silk wasgreater than around the catgut, the silk being used at the junction ofmuscle to muscle, and catgut at the junction of the sclera and muscle.The reaction was marked and nodular with granuloma formation in onlyfour of the 28 eyes.
SPECIAL TECHNIQUES
1. Isobutylcyanoacrylate adhesiveIsobutylcyanoacrylate adhesive was used in five eyes to anchor the trans-plant. The reaction of the sclera to the adhesive was very little more thanwith sutures. However, there was a moderate amount of spreading of theadhesive, prohibiting exact study of the healing process between thetransplant and its recipient, or between the transplant and the sclerawhere irregular healing was noted (Fig. 4, A). The general reaction tothe adhesive was moderate. Tenon's capsule was only moderatelyadherent.
2. SupramidSupramid was placed under the transplanted portion of muscle in fiveeyes. The generalized reaction was greater than in those eyes in which noSupramid was used. Specifically, there was a fibrous reaction around
445

446 Hiatt
.:....._|~~~~~.._ _ | ..::.: .:3- 8
M g~~~~LR
:st.*$ ..
*Sz
B +::: ... : . :. . . ..... ; , ............. .... .... . ......... ..... I
.r ..

Extraocular Muscle Transplantation
the Supramid which enclosed it almost in a sleevelike fashion. However,there was less adherence between the sclera and the transplanted musclethan in the eyes without the Supramid (Fig. 4, B). Tenon's capsule wasjudged to be somewhat more thickened when the Supramid was used.The Supramid tended to buckle and coil. In the later operations, carefulsuturing of the Supramid at all extremities resulted in less disturbanceto the overlying transplanted muscle.
3. Suturing of a tongue of Tenon's in place of horizontal muscleIn two eyes, a tongue of Tenon's capsule was formed and used to re-place the tenotomized right medial rectus on the right eye, and the leftlateral rectus on the left. The muscle that was tenotomized was found tobe retracted, but appeared to be normal otherwise. A few blood vesselsformed between the tongue of Tenon's capsule and the sclera where itwas sutured to the original muscle stump, but minimal cellular reactionwas seen. There was no adherence to the sclera underneath the tongueexcept at the site of the actual suturing. Tenon's itself was somewhatthickened, but loosely adherent to the sclera. There was little reactionof an inflammatory nature in the sclera, but there were a few inflam-matory cells around the sutures used to unite Tenon's to the globe.
4. Layer of Tenon's placed under the transplanted muscleIn two eyes, a portion of Tenon's capsule was excised and used as a"cushion" underneath the transplanted muscle (similar to the use ofSupramid) between the muscle and the sclera. The transplant itself didnot appear to be adversely affected by the presence of the capsule. Therewas a very loose adherence between the transplant and the Tenon's-sclera underneath. Tenon's capsule external to the transplanted musclewas loose.
5. Muscle incisions without transplantationIn order to study the effect of incisions into muscles without trans-plantation, five muscles were subjected to various incisions. In four of
FIGURE 4 (opposite)
A: Dog 11 O.S., cross section of globe and photomicrograph (Masson's trichrome, X25taken from region of arrow) with isobutylcyanoacrylate adhesive used to "glue" transplant-ed inferior oblique to sclera and lateral rectus. The high power shows clumping of adhesiveat the insertion. B: Dog 10 O.D., cross section of globe and photomicrograph (Masson'strichrome, X25). Supramid placed under transplanted inferior oblique to lateral rectus.The high magnification shows lack of adherence of transplant to sclera near insertion, but
some fibrous reaction around the Supramid. (See arrow.)
447

these, the muscle was merely incised seven mm posterior to its insertionand then resutured. In the other eye, it was cut, not only seven mm fromthe limbus and resutured, but also it was cut at the sclera itself and re-sutured to the sclera. In the four eyes in which the incision was madeseven mm posterior to the insertion and resutured, the entire muscle,both distal and proximal to the incision, remained viable and retained allmuscle characteristics. There was considerable inflammatory reaction,particularly about the sutures and a few blood vessels about the cut mus-cle junction.
In the eye in which incisions were made both seven mm posterior tothe insertion and at the insertion, the result was similar to that foundwhen another portion of a muscle was transplanted to a similar site.Specifically, the result was similar to the standard procedure.
6. Tensile strengthTwelve specimens were subjected to tensile strength tests as outlined.Three unoperated eyes were tested using the lateral rectus. These threemuscles broke at 790, 820, and 830 gm with an average of 813 gm. Theother nine eyes tested had had the standard procedure (inferior obliqueto lateral rectus transplants) and were kept for three, five, seven, seven,seven, nine, nine, 21 and 32 days respectfully. The tensile strength wasabout 200 gm on the third to the fifth day, increased to 400 gm on theseventh day, to 550 to 600 gm on the ninth day, and by the 12th day hadreached the 750 gm range. The 21st-day eye and the 32nd-day eye ap-proached the normal muscle in tensile strength. All of the procedureswere of the standard procedures type with no special techniques exceptthat the three seven-day eyes included one each of the standard proced-ure, one in which Supramid was used, and one in which the adhesive wasused. They did not vary significantly from each other in tensile strength.All of the eyes under 12 days postoperative broke at the insertion of mus-cle to sclera, whereas all of those over 12 days broke by the musclestretching and breaking in the belly of the muscle.
PATIENTS
A. A 14-month-old white female was seen with a history of crossed eyessince birth. An older brother and a first-cousin also had crossed eyes.Examination revealed an alternating esotropia of 100 diopters. She wasfound to have a refractive error on the right of +2.00 D and on the left of
448 Hiatt

Extraocular Muscle Transplantation
+ 1.00 +.50 X 135 with good central vision in each eye. The eye exam-ination was otherwise normal. This prescription was used for a shorttime, but did not change the angle of the esotropia.At three years of age, she had a nine mm resection of the right lateral
rectus and a five mm recession of both medial recti. This reduced theangle of the esotropia to about 30 diopters, but in the ensuing monthsthis increased to 40 diopters. At age three, she had a resection of eightmm of the left lateral rectus and two marginal myotomies of the leftmedial rectus. The effect of this procedure was nil in that the esotropiaactually increased to 48 diopters. Three months later, a third operationwas performed and consisted of a recession of the right medial rectus toa point 13 mm from the limbus which was combined with a conjunctivalrecession. This reduced the esotropia to about 15 diopters only temporar-ily. Within a few weeks, it was back to 48 diopters. In the ensuingmonths, she varied between 40 and 60 diopters.At the age of four years, the fourth operation was performed on the
right eye. Forced ductions on the operating table showed a marked limit-ation of adduction of the right eye. An inferior cul-de-sac approach wasmade. The lateral rectus was exposed, resected eight mm, and advancedto its original insertion after excision of considerable scar tissues sur-rounding the lateral rectus. The inferior oblique had to be freed from thelateral rectus muscle. The medial rectus was exposed through an in-ferior cul-de-sac approach and considerable scar tissue removed. On ex-posure of the medial rectus, it was noted to be adherent to the sclera ap-proximately four to five mm along its secondary insertion. The resectedeightmm of the lateral rectus was sutured to the medial rectus. The com-bined muscle transplant was recessed to a point ten mm from the limbusand sutured to the sclera. Gelfilm was placed beneath the transplant ex-tending from the new insertion to posterior to the anastomosis. The con-junctiva was closed with running 5-0 plain catgut suture, neomycin sul-fate-hydrocortisone acetate (Neocortef) ointment was placed in the eye,and a firm bandage and head band were placed on the patient. Dex-amethasone neomycin methylcellulose (Maxitrol) l%o ointment was usedtopically twice a day, and oral systemic prednisolone 25 mgm per daywas administered postoperatively. The postoperative reaction was mark-ed, but subsided in about ten days. The position of her eyes subsequentto the surgery was approximately straight in the straight ahead positionand to the right. However, on gaze to the left, there was some under-action of the right medial rectus, and on attempt to converge, the nearpoint was somewhat remote.
449

450 Hiatt
F1GURE 5Patient B. A: Preoperative photograph of left esotropia of 80 diopters. B: Thirty diopters ofleft exotropia six weeks following the 10 mm transplant of left lateral rectus to left medialrectus for 80 diopters of left esotropia. c: Two days postoperative for correction of 30diopters of exotropia by resection of 2 mm of transplant-left medial rectus and advancing
it 5 mm to original stump of left medial rectus.
M.M."
.2,::,iw
:. Ik-.:

Extraocular Muscle Transplantation
B. A two year old male had a left esotropia measuring 70-80 diopterswithout correction (Fig. 5, A). There was a -2 underaction of the leftlateral rectus and +2 overaction of the left medial rectus. The atropinerefraction showed +3.50 O.D. and +5.50 - 1.00 X 90 O.S. with goodcentral vision in the right eye, and poor visual acuity in the left eye. Theeyes were otherwise normal. A transplant procedure was performed onthe left amblyopic eye. An inferior cul-de-sac approach was made. Theleft lateral rectus was cleaned and resected ten mm from its point ofinsertion to the globe posteriorly. The remainder of the lateral rectuswas then resutured to its original insertion with 5-0 mild chromic cat-gut suture.The medial rectus was exposed, and after it was disinserted from the
globe, the ten mm of lateral rectus was sutured to it with 5-0 chromiccatgut, and the other end of the transplanted lateral rectus was suturedto a point four mm posterior to the original insertion of the medial rectus.Gelfilm was placed under the transplant from the insertion to posteriorto the anastomosis. A running suture of plain catgut was used to closethe conjunctiva. At six weeks postoperatively, he continued to showovercorrection of 30 diopters, with the exotropia being fairly comitantwhen fixating with the right eye (Fig. 5, B). When the left eye fixed, thedeviation increased to approximately sixty diopters of exotropia. Thepatient was operated upon the following week, and the medial rectusmuscle which had first received the transplant of the lateral rectus mus-cle was examined. There were no adhesions between the posterior sur-face of the muscle and the sclera except at its secondary insertion site.The check ligaments were cleaned from the surrounding Tenon's cap-
sule and connective tissue, and fibrous tissue was cleaned from the medi-al rectus muscle. The muscle stump was found to be 9.5 mm from thelimbus which was approximately a millimeter greater than the distance ithad been placed at the original transplant surgery. Two millimetersof the transplanted lateral-medial rectus was then resected, and it wasadvanced five mm to a point 4.5 mm from the limbus, therefore placingthe muscle-transplant back to the original insertion of the medial rectus.The conjunctiva was closed with a running 5-0 plain catgut suture, andneomycin sulfate-hydrocortisone acetate ointment was placed in the eyeand patched. On the first postoperative day, he was cosmetically straightand has remained so since the operation. (Fig. 5, c).
C. A 15 year old black male with a history of crossed eyes since the ageof two had been treated only with glasses. He was found to have O.D.
451

3.00 with 20/20 vision and O.S. +6.00 with 20/80 vision. He had ap-proximately 80 diopters of left esotropia with poor fixation, and the rota-tions were full. Fixation was eccentric being two degrees nasal from thefovea with a visuscope. The right eye was dominate, and the head posi-tion was straight. The eyes were otherwise normal.At surgery, an inferior cul-de-sac approach was made. The lateral
rectus was resected eight mm and the remaining lateral rectus was re-sutured to the original insertion with 5-0 chromic catgut. The medialrectus was exposed and disinserted from the globe, and the eight mmof lateral rectus was sutured to it with 5-0 mild chromic catgut. It wasthen sutured to the sclera at a point four mm posterior to the originalinsertion of the medial rectus with a similar suture. A thin piece of Gel-film was placed under the transplant, and the conjunctiva was closedwith a running 6-0 plain catgut suture. Bacitracin neomycin sulfatepolymixin B sulfate (Mycitracin) ointment was placed in the eye. Thereaction on the first day was moderate, and the ocular position in theprimary was excellent (Fig. 6, A). One week postoperatively, thepatient was thought to be having difficulty in abducting the left eye,but had an excellent cosmetic appearance in the straight ahead anddownward position (Fig. 6, B). By the end of the third week, there wasgood abduction in the left eye, and the reaction had become minimal.The convergence was good with full rotations of the extraocular muscles.At the end of six months, he was cosmetically straight at distance andnear with full rotations and was discharged from care at that time.
DISCUSSION
It has been shown that extraocular muscle tissue can be transplanted,survive, and remain viable. However, it has also been shown that it doesnot maintain its normal muscular characteristics. The operation on dogsand in humans produces no extensive reaction postoperatively. In view ofthe gross, microscopic, and tensile strength studies, we can conclude thatthe rate of healing of extraocular muscles as shown by Ingram43'44'46and others closely parallels the rate of replacement of transplanted extra-ocular muscle by fibrous tissue. Whereas, in eyes examined three daysafter transplant there was a large number of normal muscle fibers stillviable, by the 14th day there were few muscle fibers still present. Therecipient muscle reacted to the surgery with minimal reaction. Further-more, the general reaction of Tenon's capsule in most cases was mildwith some gross and microscopic adherence to the underlying transplant,but not enough to produce marked restrictions. The clinical reaction and
452 Hiatt

Extraocular Muscle Transplantation 453
FIGuRE 6
Patient C. A: Eighteen hours postoperative for left esotropia with 8 mm of lateral rectussutured to the medial rectus. B: One week postoperative for left esotropia with 8 mm of
lateral rectus sutured to the medial rectus.
gross reaction to the transplant was mild to moderate in most cases. Theadjacent sciera showed invasion with inflammatory cells and blood ves-sels in few instances, but the suture reaction was greater than that whichwas anticipated. The healing of the muscle to the sclera and muscle tomuscle was far advanced by the 14th day. As far as could be determined,the motility of the globe was not affected by the transplant procedure bygross examination.The study of the tensile strength closely correlates with that which
would be expected from an evaluation of the normal healing of extra-ocular muscle wounds and the microscopic reaction which was found intransplanted extraocular muscles. The tensile strength fairly well paral-leled the fibrous replacement of the transplanted extraocular muscle andthe healing of the muscle to sclera and muscle to muscle wounds. In threedays following surgery, those eyes which were tested underwent break-age after approximately 200 gmn of pressure were applied, whereas those

tested at 14 days withstood 800 gm of stretch before they were severed.It is also interesting that after 12 days, all of the eyes which underwenttensile strength testing broke by the actual muscle tissue stretching, andin no instance was there breaking of the muscle to transplant junction orthe transplant to sclera junction. Whereas, those under 12 days whichshowed a separation, separated not between muscle to muscle junction,but between the muscle to sclera junction. This is evidence that theunion of the transplanted tissue to sclera and to muscle is good after 14days.
In the special techniques used, it was shown that the Supramid result-ed in less adhesion between the muscle and sclera. However, this wascounteracted by the considerable reaction around the Supramid itselfwhich tended to nullify some of the advantages expected. When theisobutylcyanoacrylate adhesive was used, there was considerable cellularreaction about it, but it did result in a tight wound, and the ultimate fateof the transplant was the same as when sutures were used. When a sheetof Tenon's was placed under the transplanted muscle instead of Supra-mid, it did not result in fewer adhesions between the transplant and thesclera, but did result in additional fibrosis. When Tenon's was sutured tothe muscle stump in place of the muscle itself, some adhesions did occurbetween Tenon's capsule and the underlying sclera. The overall reactionof the sclera was similar to Tenon's placed under the transplanted mus-cle. When a muscle not undergoing transplantation was cut posterior toits insertion and then resutured, the wound healed with complete survi-val of both ends of the muscle. However, when the muscle was incised,both at the insertion and posterior to the insertion and then resutured,the result was similar to that found when another portion of muscle wastransplanted to an extraocular muscle in our standard procedure.
The use of autogenous tissue, namely, another extraocular muscle, tolengthen the action of another muscle by transplantation is a feasibleprocedure. When this technique was used in the three patients, it didnot result in extensive restriction of motion in the direction opposite theaction of the muscle receiving the transplant, nor did it result in any un-expected tissue reaction. Furthermore, in the eye on which the explora-tion was done, there was little adherence between the transplanted ex-traocular muscle and the underlying sclera. A satisfactory end result wasobtained in all three patients. It would seem that for a clinical and ex-perimental procedure, this tissue is at least as good as synthetic materials,such as silicone, that have been used in the past. It has a marked ad-vantage in that it is not a foreign material and subject to foreign body
Hiatt454

Extraocular Muscle Transplantation
reaction, and in no case was there extrusion, marked external reaction,or other problems encountered when artifical materials were used.
Obviously, the ideal goal has not yet been reached in which one couldtransplant the extraocular muscle, along with its fibrovascular sheathand neuromuscular apparatus intact. But with the evidence of con-tinued viability and integrity of muscle fibers transplanted elsewhere inthe body, it is possible that eventually such a micro technique could bedeveloped in the transplantation of extraocular muscles. Such a tech-nique would have many applications. Heterotransplantation of extra-ocular muscles could be used to treat paralyzed extraocular muscles.Heterotransplant or homotransplant to a fibrotic site, such as occurs afterthyroidopathy, would also be another obvious application. The most obvi-ous clinical use of the procedure outlined in this study with presenttechniques available is in a large-angle deviation in an amblyopic eye andthe use of either the medial rectus or lateral rectus portion which is re-sected and transplanted to the opposing muscle in order to lengthen arecession. A second application is in the often "available" and "dispos-able" inferior oblique be used to extend the recession of a medial orlateral rectus.
SUMMARY
1. The transplantation of extraocular homografts in rabbits, dogs, andhumans has been described.2. The extraocular muscle tissue transplanted remains viable, but losesits characteristics of muscle tissue during the period of the normal heal-ing process following extraocular muscle surgery.3. Autogenous homografts of extraocular muscles have an advantageover artificial synthetic material with the absence of extrusion and lessreaction.4. This is a clinically usable procedure today, especially in the amblyopiceye with high deviation to accomplish an additional lengthening of oneextraocular muscle, particularly if extraocular muscle surgery haspreviously been performed.
ACKNOWLEDGMENTS
I wish to thank Doctors William Austin and Robert Houk, veterinarians,for their assistance with the animal experiments, along with DoctorFederico Fuste, pathologist, for his assistance with preparation of the
455

microscopic material. I would also like to thank Doctor Charles Robbinsand students Lee Smalley and Anthony Aspero, Jr for their assistancewith the surgery. Doctor James Rayner deserves special thanks for hisinspiration to do the study.
REFERENCES
1. Gifford SR: Muscle transplantation for paralytic strabismus. Arch Ophthalmol 2:651-657, 1929.
2. Uribe LE: Muscle transplantation in ocular paralysis. Am I Ophthalmol 65:600-607,1968.
3. Jackson E: Operation on the tendon of the superior rectus muscle for paresis ofsuperior oblique. Ophthalmological Review 22:61, 1903.
4. Forbes SB: Muscle transplantation for external rectus paralysis - Report of case withunusual complications. Am I Ophthalmol 48:248-251, 1959.
5. Krewson WE: Ocular tendon transplantation - Indications, variations and technic. IInternat Coll Surgeons 27:731-737, 1957.
6. Schillinger RJ: A new type of tendon transplant operation for abducens paralysis. IInternat Coll Surgeons 31:593-600, 1959.
7. O'Connor R: Tendon transplantation in ocular-muscle paralysis. Am I Ophthalmol 18:813-820, 1935.
8. Berens C, Girard LJ: Transplantation of the superior and inferior rectus muscles forparalysis of the lateral rectus. Am I Ophthalmol 33:1041-1049, 1950.
9. Orlowski N, Saba V: Un caso di atrofia segmentaria dell' iride consequente ad inter-vento di trapianto muscolare secondo O'Connor. Boll Oculist 45:871-878, 1966.
10. Meesmann A: Uber die Trochlearisuberpflanzung bei totaler ange borener okulo-motoriusparalyse. Klin Monatsbl Augenheilkd 135:247-252, 1959.
11. Hummelsheim E: Weitere Erfahrungen mit partieller Schnenuberpflanzung an denAugenmuskeln. Archiv Augenheilkd 62:71-74, 1909.
12. Hummelsheim E: Uber Sehnentransplantation am Auge. Ber Dtsch Ophthalmol Ges34:248-260, 1907.
13. Barthelmess G: Indikation und Komplikationen der Augenmuskel transplantation.Ber Dtsch Ophthalmol Ges 67:110-113, 1966.
14. Hildreth HR: The tendon-transplanting operation. Am I Ophthalmol 36:1267-1270,1963.
15. Peter LC: The use of the superior oblique as an internal rotator in third nerve paralysis.Trans Am Ophthalmol Soc 31:232-237, 1933.
16. Jensen CDF: Rectus muscle union - A new operation for paralysis of the rectus mus-cle. Trans Pac Coast Otoophthalmol Soc 45:359-387, 1964.
17. McKinney JW: Surgical treatment of ocular nystagmus. South Med 1 58:1546-1548,1965.
18. Motais A: Operation du ptosis par le greffe tardienne d'une laguette dutendon du mus-cle droit superior. Ann Ocul (Paris) 68:5, 1897.
19. Berke RN: An operation for ptosis utilizing the superior rectus muscle. Arch Ophthal-mol 42:685-708, 1949.
20. Knapp P: Vertically incomitant horizontal strabismus - The so-called "A" and "V"syndromes. Trans Am Ophthalmol Soc 57:666-669, 1959.
21. Moller DE: Vertikale transposition der horizontalen Musculi Recti zur beseitigung desHohenschielens. Monatsblat Augenheilkd 155:539-542, 1969.
22. Knapp P: The surgical treatment of double-elevator paralysis. Trans Am OphthalmolSoc 67:304-323, 1969.
23. Westsmith R, Demorest B, Flocks M: Muscle transplants to sclera in animals. Am I
456 Hiatt

Extraocular Muscle TransplantationOphthalmol 48:228-233, 1959.
24. Espiritu RB, Caparas MP, Puzon BQ: Suprachoroidal implantation. Phillipine I SurgObstet Gyn 17:246-265, 1962.
25. Chamberlain W: Ocular motility in the horizontal plane - An experimental study ofthe primary and secondary horizontal rotations of the rhesus monkey. Trans Ophthal-mol Soc 52:751, 1954.
26. Metz HS, Scott AB: Innervational plasticity of the oculomotor system. Arch Ophthal-mol 84:86-91, 1970.
27. Jampel RS: The fundamental principle of the action of the oblique ocular muscles.Am I Ophthalmol 69:623-638, 1970.
28. Leinfelder PJ, Black NM Jr: Experimental transposition of the extraocular musclesin monkeys. Am I Ophthalmol 24:1115-1120, 1941.
29. Jampolsky A: Personal communication.30. Beisner DH: Extraocular muscle recessions utilizing silicone tendon prostheses. Arch
Ophthalmol 83:195-204, 1970.31. Bowen SF Jr, Dyer JA: A silicone rubber tendon for extraocular muscles - As ex-
perimental study. Invest Ophthalmol 1:579-585, 1962.32. Morales AG, Polack FM, Arata AF: Silicone implant to extraocular muscles. Brit
Ophthalmol 50:235-244, 1966.33. Roman E, Fazio CM, Estupinan B, Jacobo A, Ferrarexi ER: Implante de silicon en
estropias de gran angulo. Arch Oftal (Buenos Aires) 44 :276-281, 1969.34. Palmieri L: Imnesti organici liofilizzatl su muscoli oculari estrinseci. Ann Ottalmol
Clin Oculist 94:1099-1107, 1968.35. Carlson BM: The regeneration of a limb muscle in the axolotl from minced fragments.
Anat Rec 166:423436, 1970.36. Tamai S, Komatsu S, Sakamoto H: Free muscle transplants in dogs, with microsurgical
neurovascular anastomoses. Plast Reconstr Surg 46:219-225, 1970.37. Allbrook D: Skeletal musde autotransplantation and regeneration, I Anat 106:195,
1970.38. Zhenevaskyo RP: Transplantatsiya skeletnykh myshts u zhivotaykh. Usp Sovrem Biol
65:133-143, 1968.39. Mepomnyashchikh GI: A morphological study of the cardiac and somatic muscle fol-
lowing autotransplantation into the myocardium of the dog. Translated from Byul-leten Eksperimental noi Biologii i Meditsiny 61:109-113, 1966.
40. Carroll FD, Blake EM: Repair following operations on the extraocular muscles. ArchOphthalmol 8:711-726, 1932.
41. Chouke KS: Repair following tucking operations on the extraocular muscles. Am JOphthalmol 28:50, 1945.
42. Carusillo M: Particolare innesto muscolo-tendineo in aftalmoplegia estrinseca dell'oculomotore comune, Ann Ottalmol Clin Oculist 93:1061-1066, 1967.
43. Truhlsen SM: The recession operation - Histopathologic response, and suture re-action and absorption. Trans Am Ophthalmol Soc 63:626-677, 1965.
44. Ingram RM: Tissue repair after the operations of recession and resection. Brit I Oph-thalmol 49:18-28, 1965.
45. Ingram RM: Rate at which muscle becomes joined to sclera after operations of reces-sion and resection. Brit I Ophthalmol 48:235-245, 1965.
46. Ingram RM: Wound healing after operations on the extraocular muscles on monkeys.Brit I Ophthalmol 50:186-208, 1966.
47. Dunlap EA: Plastic implants in muscle surgery - A study of the possible use of plasticmaterials in the management of extraocular motility restrictions. Trans Am Ophthal-mol Soc 65:393470, 1967.
48. Berens C: Tenon's capsule transplants in surgery of the ocular muscles, with especialreference to postoperative deviations with adhesions between the muscles and theeyeball. Trans Am Ophthalmol Soc 35:173, 1937.
457

458 Hiatt
49. Berens C, Romaine HH: Postoperative cicatricial strabismus, results of transplanta-tion of Tenon's capsule. TransAm Acad Ophthalmol Otolaryngol47 :103, 1942-1943.
50. Dunlap EA, Dunn M, Rossomondo R: Adhesives for sutureless muscle surgery. ArchOphthalmol 82:751-755, 1969.
51. Dunlap EA, Dunn M, Rossomonda R: Observations on the use of plastic adhesives inmuscle surgery with two new potential applications. Trans Am Ophthalmol Soc 67:283-303, 1969.