Evidence in focus - Smith & Nephew and... · 2019-02-20 · NAVIO™ Surgical System design NAVIO...
20
Evidence in focus Compendium of evidence Summary of the current preclinical and clinical evidence on NAVIO February 2019 Supporting healthcare professionals Supporting healthcare NAVIO™ Surgical System
Transcript of Evidence in focus - Smith & Nephew and... · 2019-02-20 · NAVIO™ Surgical System design NAVIO...

Supporting healthcare professionals
Supporting healthcare professionals for over 150 yearsNAVIO™Surgical System
Supporting healthcare professionals for over 150 years
Evidence in focusCompendium of evidence
Summary of the current preclinical and clinical evidence on NAVIOFebruary 2019 Supporting healthcare professionals
Supporting healthcare professionals for over 150 yearsNAVIO™Surgical System

Purpose
To summarise the current preclinical and clinical evidence on NAVIO (Smith & Nephew Memphis, TN, USA).
Compendium of evidence
NAVIO™ Surgical System
22
studies reporting on NAVIO
Patient outcomes Accuracy
Total operative
time
Studies
Author/year Study title Study outcomes
Study type Page number
Why robotics? Conventional techniques versus robotics 4
NAVIO Surgical System design 4
Batailler C, et al. 2018
Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty
5
Battenberg A, et al. 2018
Early survivorship of robotic-assisted unicompartmental knee arthroplasty 6
Canetti R, et al. 2018
Faster return to sport after robotic-assisted lateral unicompartmental knee arthroplasty: a comparative study
7
Casper M, et al. 2018
Accuracy assessment of a novel image-free handheld robot for total knee arthroplasty in a cadaveric study
8
Gregori A, et al. 2013
Case study: totals aren’t always an inevitability 8
Gregori A, et al. 2014
Case study: first in man: using the NAVIO surgical system to implant a JOURNEY™ UNI knee 9
Gregori A, et al. 2014
Handheld precision sculpting tool for unicondylar knee arthroplasty. A clinical review 9
Gregori A, et al. 2015
Accuracy of imageless robotically assisted unicondylar knee arthroplasty 10
Gonzalez D, et al. 2014
Preliminary results of UKR implanted using an image free handheld robotic device 10
Preclinical
Key: Study outcomes Key: Study type
Clinical
Evidence in focus
page 2 of 20

Studies
Author/year Study title Study outcomes
Study type Page number
Herry Y, et al. 2017
Improved joint-line restitution in unicompartmental knee arthroplasty using a robotic-assisted surgical technique
11
Jamaraz B & Nikou C. 2012
Precision freehand sculpting for unicondylar knee replacement: design and experimental validation 12
Jaramaz B, et al. 2013
NAVIO™ PFS for unicondylar knee replacement: early cadaver validation 12
Jaramaz B, et al. 2015
Accuracy validation of semi-active robotic application for patellofemoral arthroplasty 13
Jamarmaz B, et al. 2018
Accuracy assessment of a novel image-free handheld robot for knee arthroplasty in bi-cruciate retaining total knee replacement
13
Khare R, et al. 2018
Implant orientation accuracy of a hand-held robotic partial knee replacement system over conventional technique in a cadaveric test
14
Lonner JH, et al. 2015
High degree of accuracy of a novel image-free handheld robot for unicondylar knee arthroplasty in a cadaveric study
14
Shah S, et al. 2018
Robotic assisted revision total knee replacement - early experience 15
Simons M & Riches P. 2014
The learning curve of robotically-assisted unicondylar knee arthroplasty 15
Smith JR, et al. 2013
Accuracy of a freehand sculpting tool for unicondylar knee replacement 16
Smith JR, et al. 2013
The accuracy of a robotically-controlled freehand sculpting tool for unicondylar knee arthroplasty 16
Vega Parra P, et al. 2017
Robotic-assisted unicompartmental knee replacement with NAVIO surigical system: Outcome evaluation using knee injury osteoarthritis outcome score
17
Wallace D, et al. 2014
The learning curve of a novel handheld robotic system for unicondylar knee arthroplasty 17
References 18
AbbreviationsUKA: unicondylar knee arthroplastyKOOS: knee injury and osteoarthritis scoreOKS: Oxford knee score
TKA: total knee arthroplastyRMS: Root mean square UKR: unicompartmental knee replacement
page 3 of 20
Why robotics?
Conventional techniques versus robotics
NAVIO™ Surgical System design
NAVIO is an image-free, freehand sculpting semi-active robotic tool, that allows for intraoperative patient-specific planning
The NAVIO system has two types of robotic control modes, Exposure Control and Speed Control. The surgeon can alternate between these two cutting control modes.
Conventional
Manual instruments include alignment rods that are intra- or extra-medullary that centralise and align the components according to the surgical plan.1
Conventional alignment guides:
• Lack precision1,2
• Are not tailored to each patient’s individual morphology
• Can result in inadvertent deviations from the surgical plan2
Exposure Control
Exposure Control adjusts the bur’s exposure with respect to a guard. If the surgeon encroaches on a portion of bone that is not to be cut, the NAVIO Surgical System retracts the spinning bur behind the guard, disabling cutting. The NAVIO Surgical System software adjusts the depth of the cut by adjusting the exposure of the bur outside of the guard.
During Exposure Control, the bur spins at full power (80,000 rpm), regardless of exposure level.
Robotics
Robotic systems include passive, semi-active, and active systems with a robotic arm, robotic guided cutting jigs, and robotic milling systems.
For total and partial knee replacement, robotic systems may:
• Help surgeons avoid surgical errors1, 3
• Decrease variability3
• Increase accuracy in mechanical alignment for more natural kinematics3-6
Speed Control
Speed Control regulates the speed of the bur, from 0 to 80,000 rpm, depending on its position. The control mode limits the speed of the spinning bur or disables bur motion entirely if the target surface has been reached. Bur motion is also disabled if the bur is moved outside of planned cutting boundaries.
“The current literature demonstrates that using computer navigation for UKA [compared to conventional techniques] results in better limb alignment and component positioning”2
The NAVIO handpiece accurately removes bone identified by the surgeon approved, patient-specific plan
page 4 of 20
Study overview
• Retrospective case-control study comparing implant position and revision rate for UKA performed with NAVIO™ robotics-assisted or conventional technique
− NAVIO group: 80 UKAs (lateral, 23; medial, 57; mean age, 69 years; mean length of follow-up; 19.7 months) − Conventional group: 80 UKAs (lateral, 23; medial, 57; mean age, 68 years; mean length of follow-up; 24.2 months)
• Implant position was assessed via radiographs at 1 year post-UKA
• Revision rate was calculated at the last follow up
Key results
• NAVIO group revision rate: 5% (lateral UKA, 0%; medial UKA; 7%)
− Reasons for revision: − Change to a thicker polyethylene due to persistent medial pain (1)
− Tibial plate subsidence (1) − Aseptic loosening of the tibial implant (1) − Unexplained pain, localised to the medial compartment (1)
• Conventional group revision rate: 9% (lateral UKA, 9%; medial UKA, 9%)
− Reasons for revision: − Malposition of the femoral implant (1) − Overcorrection (1) − Pain and tibial loosening (1) − Change to a thicker polyethylene due to persistent pain and hypocorrection (2) − Persistent pain without loosening (1) − Tibial loosening with varus alignment (1)
• The total reoperation rate was significantly lower in the NAVIO group compared to the conventional group for lateral UKAs (0 vs 22%; p=0.025) but there was no significant difference for medial UKAs (18 vs 14%)
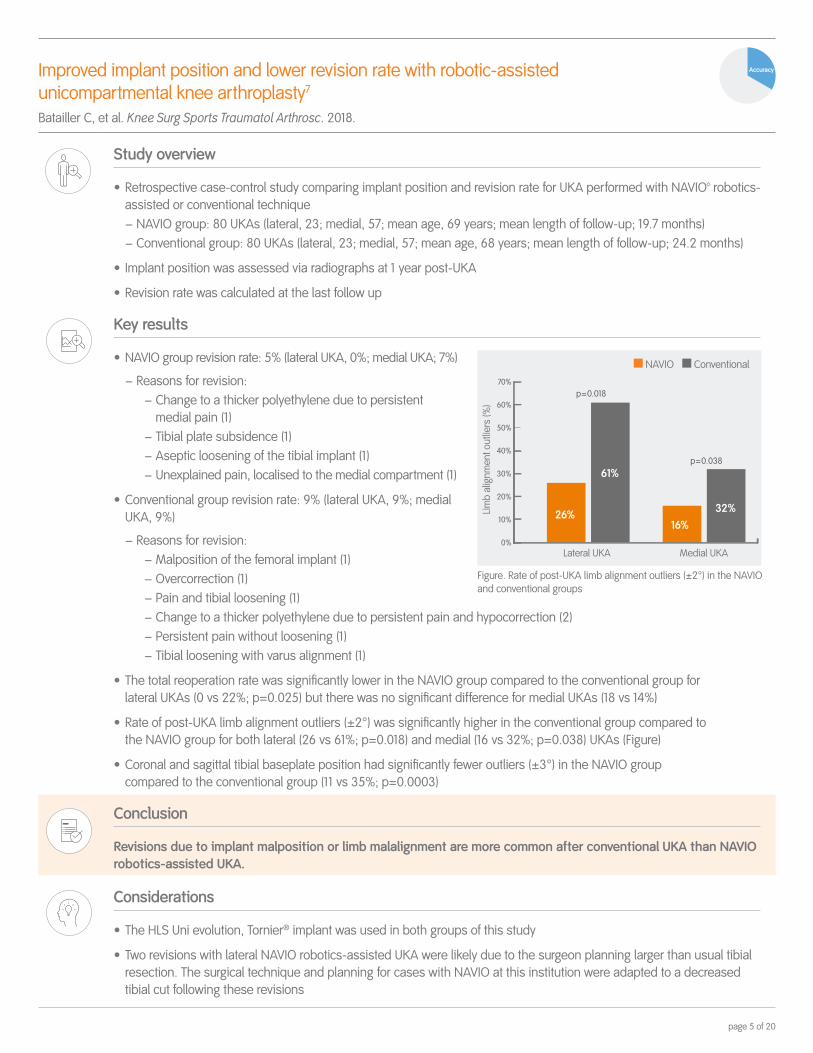
• Rate of post-UKA limb alignment outliers (±2°) was significantly higher in the conventional group compared to the NAVIO group for both lateral (26 vs 61%; p=0.018) and medial (16 vs 32%; p=0.038) UKAs (Figure)
• Coronal and sagittal tibial baseplate position had significantly fewer outliers (±3°) in the NAVIO group compared to the conventional group (11 vs 35%; p=0.0003)
Conclusion
Revisions due to implant malposition or limb malalignment are more common after conventional UKA than NAVIO robotics-assisted UKA.
Considerations
• The HLS Uni evolution, Tornier® implant was used in both groups of this study
• Two revisions with lateral NAVIO robotics-assisted UKA were likely due to the surgeon planning larger than usual tibial resection. The surgical technique and planning for cases with NAVIO at this institution were adapted to a decreased tibial cut following these revisions
Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty7 Batailler C, et al. Knee Surg Sports Traumatol Arthrosc. 2018.
Accuracy
Figure. Rate of post-UKA limb alignment outliers (±2°) in the NAVIO and conventional groups
Medial UKA
Limb
alig
nmen
t out
liers
(%)
Lateral UKA
32%16%
26%
61%
70%
60%
50%
40%
30%
20%
10%
0%
p = 0.038
p = 0.018
NAVIO Conventional
page 5 of 20

Study overview
• Retrospective study to assess revision rates of patients who received UKA with NAVIO™ Surgical System
• 128 UKA patients included who had undergone UKA with NAVIO at five US sites
• Surgeon adopter’s initial cases
Key results
• Mean follow up of 2.3 years
• Survivorship at 2 years with NAVIO: 99.2% (Figure)
− Greater than that reported in the Australian, New Zealand and Swedish registry
• One revision with NAVIO
− Due to hamstring irritation and ischial tuberosity bursitis in 60 year old male
Conclusion
High early implant survivorship rate for the NAVIO system that is higher than that presented in the literature for annual registries.
Early survivorship of robotic-assisted unicompartmental knee arthroplasty8
Battenberg A, et al. 35th Annual Meeting of SOA. July 11-14, 2018; Palm Beach, FL, USA.
93
94
95
96
97
98
99
100NAVIOSwedish registry
Australian registry New Zealand registry
Figure. Survivorship data from this study compared to annual registry data for conventional UKA reporting 2-year UKA survivorship
95.7% 96.3% 96.0%99.2%
Patient outcomes
page 6 of 20

Faster return to sport after robotic-assisted lateral unicompartmental knee arthroplasty: a comparative study9
Canetti R, et al. Arch Orthop Trauma Surg. 2018;138:1765-1771.
Patient outcomes
Study overview
• A retrospective analysis of lateral UKAs in patients with isolated osteoarthritis, performed by a single surgeon between April 2012 and December 2016 with either NAVIO™ handheld robotics technology or conventional techniques
− NAVIO: 11 UKAs (mean age, 66.5 years)
− Conventional surgery: 17 UKAs (mean age, 59.5 years)
− Mean follow-up of 37.2 months
• Return to sport (RTS) and knee function outcomes were compared
Key results
• NAVIO reduced mean time to RTS by 6.3 months compared to conventional surgery (4.2 vs 10.5 months; p<0.01; Figure)
• With NAVIO, by end of follow-up all patients returned to sport (100%) and the majority returned to their pre-symptomatic intensity level (91%); respective outcomes were 94% and 82% for conventional surgery
• NAVIO achieved favourable knee function outcomes compared to conventional surgery, as measured by the International Knee Society Score-Objective (IKSS-O):
− Significantly better postoperative IKSS-O (97.2 vs 91.2; p<0.05)
− Significantly greater IKSS-O improvement after surgery compared to preoperative scores (+30.9 vs +22.8; p<0.05)
• Results of the International Knee Society Score-Functional, Lysholm Knee Scale and Forgotten Joint Scale were similar with both procedures
Conclusion
Compared to conventional surgery, NAVIO robotics-assisted lateral UKA reduced time to RTS at pre-symptomatic levels. This could be attributed to the less invasive approach with NAVIO, limiting soft tissue damage and enabling faster muscle recovery, or better implant positioning. These results may help surgeons to inform patients in planning their anticipated level of postoperative activity following lateral UKA, especially young, active patients with high expectations.
Mea
n tim
e to
RTS
(mon
ths)
NAVIO Conventional surgery
121086420
∆6.3 months
p<0.01181614
20
4.2 10.5
Figure. Mean time to RTS after UKA with NAVIO versus conventional surgery. Error bars represent standard deviation
page 7 of 20

Study overview
• Eight experienced TKA surgeons carried out TKA using NAVIO™ Surgical System on 18 cadavers (2 or 3 per surgeon)
• JOURNEY™ II, GENESIS™ II and LEGION™ implants were used
• Conical divots were prepared at known positions on the implants to allow for accuracy assessment
Key results
• All (bur and cut-guide) absolute mean tibial and femoral errors were within 1mm/° of neutral
− Except for femoral flexion (with cut-guide) which was within 2° of neutral
Conclusion
NAVIO provides accurate implementation of the surgical plan with small errors in implant placement.
Accuracy assessment of a novel image-free handheld robot for total knee arthroplasty in a cadaveric study10
Casper M, et al. Comput Assist Surg. 2018;23:14-20.
Accuracy
Error type Total error
Femoral Tibial
Flexion/posterior slope -2±2.2° -0.2±1.3°Varus/valgus -0.1±0.9° -0.2±0.9°
Rotation -0.5±1.2° NR
Study overview
• Active, 53 year old male
• Satisfied with prior partial knee procedure in right knee, now severe pain in medial compartment with no lateral/anterior compartment pain in left knee
• Surgeon exploring partial knee replacement as first option but considering total due to extreme varus deformity of 12°
Key results
• At the planning stage, NAVIO allowed the surgeon to make an informed decision intraoperatively on best way to proceed
• NAVIO allowed the surgeon to plan an implant fit and position with minimal bone resection to balance knee and correct long leg alignment without over-correction
• Post-operative long leg alignment 2º varus (improvement of 10º)
Conclusion
NAVIO allows surgeons to confidently approach a challenging surgery with the knowledge that they can execute a predetermined plan accurately to get the best outcome for the patient.
Case study: totals aren’t always an inevitability11
Gregori A, et al. BLUE BELT Technologies Inc. 2013.
Pre-operative Post-operative
Patient outcomes
page 8 of 20

Study overview
• 67 year old male with left knee osteoarthiritis
• Pain predominantly on medial side of knee
• Pre-operative deformity of 8° varus, medial compartmental cartilage thinning and joint space narrowing
• Previous right knee UKR
Key results
• Planned post-UKR alignment = 2° of varus
• Achieved post-UKR alignment = 3°
− The surgeon increased planned insert thickness during surgery, as NAVIO is a flexible platform
• Surgical time from tracker placement to trial acceptance: 50 minutes
• Total cutting time: 20 minutes
• Both patient and surgeon satisfied
• Patient discharged two days post-UKR with >90° knee flexion
Case study: first in man: using the NAVIO™ surgical system to implant a JOURNEY™ UNI knee12
Gregori A, et al. BLUE BELT Technologies Inc. 2014.
Post-operative frontal view Post-operative sagittal view
Patient outcomes
Study overview
• Clinical review
• Evaluation of the clinical and functional outcomes of the first 57 patients undergoing UKA with NAVIO Surgical System
Key results
• Post-UKA mechanical axis alignment within 1° of intra-operative NAVIO plan in 91% of cases (Figure)
• UKA reduced mean mechanical axis deformity from -6.2° pre-UKA to -3.4° six weeks post-UKA
• Mean NAVIO time (from tracker placement to implant trial acceptance) decreased from 69 to 54 minutes
• Cutting phase time decreased by 32.5 minutes from first to quickest procedure
• Mean Oxford Knee Score showed clinical improvement from 22 pre-UKA to 36 six weeks post-UKA
• All patients achieved full extension post-UKA
Conclusion
NAVIO allows surgeons to repeatedly precisely plan and execute highly accurate mechanical axis alignment. The learning curve of NAVIO is short, with mean NAVIO time reduced by 15 minutes after ten cases.
Handheld precision sculpting tool for unicondylar knee arthroplasty. A clinical review13
Gregori A, et al. 15th EFORT Congress. June 4-6, 2014; London, UK.
91%
Cases within 1° of intra-operative plan
Figure. Post-UKA mechanical axis alignment
Patient outcomes
Total operative
time
Accuracy
Accuracy
page 9 of 20

Study overview
• A single surgeon performed UKR on 18 patients with NAVIO Surgical System (2012 to 2013)
Key results
• OKS (old) improved from 38 pre-UKA to 23 six weeks post-UKA (22 to 37 new OKS*, respectively; Figure))
*To convert from the old OKS to the new OKS, the old OKS score is substracted from 60
Conclusion
Preliminary analysis shows satisfactory post-UKR outcome for UKR with NAVIO.
Preliminary results of UKR implanted using an image free handheld robotic device15
Gonzalez D, et al. BASK Annual Meeting. 8-9 April, 2014; Norwich, UK.
0
10
20
30
40
Pre-UKR Six weeks post-UKR
Oxf
ord
Knee
Sco
re (n
ew)
22
37
Patient outcomes
Accuracy of imageless robotically assisted unicondylar knee arthroplasty14
Gregori A, et al. 15th Annual meeting of CAOS. June 17-20, 2015; Vancouver, Canada.
Study overview
• Authors prospectively collected radiographic data on 92 patients who underwent medial UKA with NAVIO™ Surgical System at four centres (four surgeons)
Key results
• 89% of patients had post-UKA alignment within 3° of the planned coronal mechanical axis alignment (Figure)
• RMS error 1.98°
• RMS error between plan and post-UKA radiographic implant position:
− Femoral tibial alignment: 2.6°
− Tibial coronal alignment: 2.9°
− Tibial slope: 2.9°
Conclusion
Use of NAVIO can accurately prepare the bone surface of the tibia and femur; this allows for few errors resulting in high levels of accuracy in the planned coronal mechanical axis alignment when comparing planned versus achieved component placement.
89%
Post-UKA alignment within 3° of the planned coronal mechanical axis alignment
Accuracy
Figure. Percentage of patients with a post-UKA alignment within 3° of the planned coronal mechanical axis alignment
Figure. New OKS six weeks post-UKA
page 10 of 20

Study overview
• Single-surgeon retrospective, case-controlled study comparing joint-line height following UKA using NAVIO™ robotics-assisted (40 patients; mean age, 69 years) or conventional technique (40 patients; mean age, 68 years)
• Weight-bearing radiographs were taken pre-UKA and 2 months post-UKA
Key results
• The joint-line was distalised significantly more following UKA in the conventional group than in the NAVIO Surgical System group when assessed using two methods (p<0.05; Figure)
− Method 1: angle between joint-line and lateral femoral cortex
− Method 2: angle between joint-line and femoral intramedullary axis
Conclusion
NAVIO robotics-assisted UKA allows for intraoperative planning of implant position and highly accurate bone resection, resulting in improved joint-line restitution when compared with a conventional technique. Furthermore, NAVIO Surgical System may avoid creating femoral superstructures, thereby reducing tibial resection and helping to prevent pain and other post-UKA complications. Further studies should be undertaken to assess long-term outcomes.
Improved joint-line restitution in unicompartmental knee arthroplasty using a robotic-assisted surgical technique16
Herry Y, et al. Int Orthop. 2017;41:2265-2271.
Accuracy
0
1
2
3
4
5
Method 1 Method 2
Mea
n jo
int-
line
heig
ht d
iffer
ence
af
ter s
urge
ry (m
m)
NAVIO Conventional
1.4
4.7
1.5
4.6
p<0.05 p<0.05
Figure. Mean joint-line height difference (mm) following UKA using robotics-assisted or conventional techniques, as analysed by two methods
page 11 of 20

Study overview
• Three operators performed medial UKR surgery with NAVIO Surgical System on two cadaver specimens (four knees)
• Each component included a set of eight conical divots in predetermined locations to allow for measurement of the position
Key results
• All NAVIO-assisted implants were within 1.5mm of the target in all directions
Conclusion
Use of NAVIO shows high levels of accuracy comparable to other robotics-assisted devices.
NAVIO PFS for unicondylar knee replacement: early cadaver validation18
Jaramaz B, et al. 13th annual meeting CAOS. June 13-15, 2013; Orlando, FL, USA.
Error type Mean total error
Maximum translation error 1.31mm
Maximum rotational error (femoral) 1.90°
Maximum rotational error (tibial) 3.26°
RMS error over all components 0.69mm/1.23°
Accuracy
Study overview
• Evaluation of NAVIO™ Surgical System performance for UKR in terms of implant fit and cutting time
− Three users with different levels of experience
− Five sawbone specimens
Key results
• Total cutting time: 6.5 to 9.5 minutes
• Mean cut time: 8.01 minutes
• Average distance from the planned implant position was 0.54mm
• Average total error: 0.54mm/1.08° (Figure 1)
Conclusion
NAVIO achieves high levels of accuracy, adequate for joint replacement surgery, with low levels of error.
Precision freehand sculpting for unicondylar knee replacement: design and experimental validation17 Jaramaz B & Nikou C. Biomed Tech. 2012;57:293-299.
Accuracy
Total operative
time
0
0.5
1
1.5
1.08
0.54
2
Rotational Translational
Plac
emen
t erro
r (°
/mm
)
5
6
7
8
9
10 8:16
7:408:14
User 1 User 2
Tim
e (m
inut
es)
User 3
Figure 1. Mean (range) component placement accuracy Figure 2. Mean (range) bone preparation time
page 12 of 20

Study overview
• Tests were performed (n=24) for four different implant designs, with a minimum of five cases per implant design
• NAVIO™ surgery was simulated with four implant designs (two ‘inlay’ and two ‘onlay’)
• Minimum of three synthetic bones and two cadavers were used for each design
• Fiducial markers establish a reference frame to determine the accuracy of prosthesis placement
• Final implant position and planned position were compared
Key results
Conclusion
The high levels of accuracy demonstrated by NAVIO are in accordance with those reported for UKR surgery. The results of this study are based on using the NAVIO Surgical System with the bur and saw function.
Accuracy validation of semi-active robotic application for patellofemoral arthroplasty19
Jaramaz B, et al. 15th Annual meeting of CAOS. June 17-20, 2015; Vancouver, Canada.
Error type Mean total error
Maximum RMS error 0.87mm
Maximum rotational error 1.2°
Accuracy
Study overview
• The study compared the planned and final implant placement using the JOURNEY™ II XR bi-cruciate retaining knee implant with NAVIO Surgical System
• TKA was performed on 24 cadaveric femurs, eight synthetic femurs, two cadaveric tibias, 10 synthetic tibias
• Final implant position was measured and compared to the surgical plan using a separate position tracking camera and analysis software
• A quantitative analysis was performed to determine the translational, angular, and rotational differences between the planned and achieved positions of the implant
Key results
Conclusion
NAVIO allows for high levels of accuracy in the implementation of the planned procedure for JOURNEY II XR placement.
Accuracy assessment of a novel image-free handheld robot for knee arthroplasty in bi-cruciate retaining total knee replacement20
Jaramaz B, et al. Health Sciences. 2018;2:98-101.
Error type Mean RMS error
Femoral implant Tibial implant
Varus/valgus 0.7° 0.69°Rotation (femoral)/posterior slope (tibial) 0.7° 0.88°
Distal resection 0.86mm 0.68mm
Accuracy
page 13 of 20

Study overview
• Two surgeons each carried out medial bilateral UKA on six cadavers − Equal number of UKAs were carried out with NAVIO™ Surgical System used on one knee and conventional methods for the other knee
• Conical divots were prepared at known positions on the implants to allow for accuracy assessment
• CT scans were obtained pre and post-UKA to identify final implant position, which was then compared to the planned position
Key results
• Maximum RMS femoral implant orientation error:
− NAVIO = ≤2.81° − Conventional = ≤7.52°
• Maximum RMS tibia implant orientation error:
− NAVIO = ≤2.96° − Conventional = ≤4.06°
Conclusion
NAVIO provides improved implant alignment accuracy over conventional approaches to UKA.
Implant orientation accuracy of a hand-held robotic partial knee replacement system over conventional technique in a cadaveric test21
Khare R, et al. Computer Assisted Surgery. 2018;23:8-13.
0
1
2
3
4
5
6
7
8
Femoral Tibial
Max
imum
RM
S im
plan
t or
ient
atio
n er
ror (
°)
NAVIOConventional
2.81
7.52
2.964.06
Accuracy
Study overview
• Four individuals carried out medial UKA on 25 cadavers with NAVIO Surgical System• Planned implant orientation and actual implant orientation were compared
Key results
• Bone preparation and implant position were within the range of 0.8 to 1.3mm and 1 to 2° of the planned implant position (Figure 1 and 2)
Conclusion
NAVIO provides accurate implementation of the surgical plan, with low levels of error, and is comparable to other semi-autonomous robotic orthopaedic devices.
High degree of accuracy of a novel image-free handheld robot for unicondylar knee arthroplasty in a cadaveric study22
Lonner JH, et al. Clin Orthop Relat Res. 2015;473:206-212.
Accuracy
0.0
0.5
1.0
1.5
2.0
Angular Transitional
Erro
r (°/
mm
*) 1.04 – 1.88 (degrees)
0.72 – 1.29 (mm)
0.0
0.5
1.0
1.5
2.0
Angular Transitional
Erro
r (°/
mm
*)
1.48 – 1.98 (degrees)
0.79 – 1.27 (mm)
*Figures show °/mm absolute means errors across three planes Figure 2. Tibial component accuracy Figure 1. Femoral component accuracy
Figure. Maximum RMS femoral and tibial orientation error NAVIO robotics-assisted or conventional technique
page 14 of 20

The learning curve of robotically-assisted unicondylar knee arthroplasty24
Simons M & Riches P. Bone Joint J. 2014;96B:SUPP11.
Study overview
• Five junior orthopaedic trainees all underwent initial NAVIO Surgical System UKA training and performed five UKAs with NAVIO on left-sided synthetic femurs and tibiae
• Each procedure was video recorded and timed• A ballpoint probe with four reflective spherical markers attached was used to record the position of prepared divots on
the implant to allow the 3D position of the implant to be compared to the planned position
Key results
• Total surgical time decreased significantly from 85 to 48 minutes after five surgeries
• All stages, except cutting tool set up, demonstrated a significant difference in operative time with increasing number of surgeries performed (p<0.05)
− Cutting phase decreased from 41 to 23 minutes (Figure)
• Translational and rotational accuracy of the implants did not significantly vary with surgery number
• Adequate accuracy was achieved from the first surgery
Conclusion
NAVIO achieves high levels of accuracy from the first procedure, with up to 44% reduction in time after five procedures.
44%reductionin operative
time after five surgeries
Accuracy
Total operative
time
Study overview
• Single-centre prospective study recruiting patients for revision TKA with NAVIO™ Surgical System (Aug 2017 to Jan 2018)
− Ten patients were included (females, 6; males, 4; mean age, 67.5 years)
• Preoperative and postoperative ROM, OKS, KSS and leg alignment were recorded
Key results
• Mean length of stay: 4.5 days
• Mean operating time: 92 minutes
• Improvements in ROM, OKS (Figure) and KSS and leg alignment compared to preoperative values
• No mechanical axis outliers
Conclusion
NAVIO is safe and capable of producing consistent coronal mechanical alignment in revision TKA.
Robotic assisted revision total knee replacement - early experience23
Shah S, et al. 19th Annual Scientific Meeting for APAS. September 6-8, 2018; Bangkok, Thailand.
Patient outcomes Accuracy
0
10
20
30
40
50
60
70
80
Preoperative Postoperative
Oxf
ord
Knee
Sco
re
33.4
68.8
Figure. Oxford Knee Score pre- and post-NAVIO
Figure. Reducation (%) in operative time after five surgeries
page 15 of 20

0.0
0.5
1.0
1.5
0.420.32
Femur Tibia
Rota
tiona
l erro
r (°)
Figure 1. Component placement accuracy (translational errors)
Study overview
• A single-surgeon tested precision of NAVIO™ Surgical System
• Carried out UKA with 20 identical femur and tibia synthetic bone pairs
• Four fidicular markers drilled in each femur and tibia sawbones were used to measure pre- and post-UKA position
Key results
• Fidicular marker analysis:
− Minimal movement of the arrays
• Mean cut surface data:
− Slight undercut of 0.14mm for femur and 0.21mm for tibia
• All implant positions compared favourably to the plan and were within the expected target zone with low errors in rotational and translational placement (Figure 1 and 2)
Conclusion
NAVIO implant positions are accurate to plan, with low levels of error in rotational and translational placement.
Accuracy of a freehand sculpting tool for unicondylar knee replacement25
Smith JR, et al. Int J Med Robotics Comput Assist Surg. 2013;10:162-169.
Accuracy
Study overview
• Two users trained with the NAVIO Surgical System, performed UKA on nine cadavers
− Consultant orthopaedic surgeon performed four implants
− Research associate performed five implants
• 3D image of the actual implant position was overlaid on the planned implant image to quantify differences in planned and achieved cuts in three planes and three rotations
Key results
Conclusion
NAVIO offers optimal positioning and sizing of implants, and the freehand sculpting tool produces high levels of accuracy in implant placement with low levels of error.
The accuracy of a robotically-controlled freehand sculpting tool for unicondylar knee arthroplasty26
Smith JR, et al. Congress of ISB. 4-9 August, 2013. Natal, Brazil.
Error type Mean total error
Femoral Tibial
Maximum implant rotational error 3.7° 4.1°
Maximum implant translational error 2.6mm 2.7mm
Maximum RMS angular error 2.0° 2.6°
RMS translational error across all directions 1.1mm 2.0mm
Accuracy
0
1
2
3
1.0 0.82
4
Femur Tibia
Tran
sitio
nal e
rror (
mm
)
Figure 2. Planned versus achieved rotation
page 16 of 20

Study overview
• Five surgeons performed UKA on at least 15 patients with NAVIO Surgical System − Two surgeons had experience with robotic devices for UKA − All surgeons had experience with conventional UKA and navigation for other knee procedures
• The number of surgeries to reach ‘steady state’ surgical time was calculated as the point at which two consecutive cases were completed within the 95% confidence interval of the surgeon’s ‘steady state’ time
Key results
• Average surgical time for the first 15 cases was 56.8 minutes
• Average improvement from slowest to quickest surgical time was 46 minutes
• Average of eight procedures to steady state
• Average steady state surgical time was 50 minutes (Figure)
Conclusion
NAVIO has a comparable learning curve to other robotics-assisted devices on the market.
The learning curve of a novel handheld robotic system for unicondylar knee arthroplasty28
Wallace D, et al. Bone Joint J. 2014;96B:SUPP16.
50 minaverage steady state
surgical time
Total operative
time
Robotic-assisted unicompartmental knee replacement with NAVIO™ surigical system: Outcome evaluation using knee injury osteoarthritis outcome score27
Vega Parra P, et al. Rev Chil Ortop Traumatol. 2017;58:7-12.
Study overview
• Single-surgeon case series of 47 patients (mean age, 67 years; females, 49%; males, 51%) who underwent UKA with NAVIO Surgical System using the STRIDE™ UNI prosthesis (November 5, 2013 to February 30, 2014)
• KOOS was recorded pre-UKA and 12 months post-UKA
Key results
• All categories of KOOS were improved significantly at 12 months post-UKA following NAVIO UKA compared to pre-UKA (p<0.001; Figure)
− Symptoms: 33.11 to 70.79 (p<0.001)
− Pain: 35.30 to 71.62 (p<0.001)
− Daily activities: 28.51 to 63.62 (p<0.001)
− Quality of life: 31.15 to 72.98 (p<0.001)
Conclusion
NAVIO robotics-assisted UKA with STRIDE UNI demonstrated a substantial improvement in patients’ quality of life, reducing pain and improving function during sports and recreational activities.
Patient outcomes
Figure. KOOS scores pre- and post- NAVIO robotics-assisted UKA
0
10
20
30
40
50
60
70
80
Symptoms Pain Daily activity
Quality of life
Sports and recreational
activities
Mea
n KO
OS
scor
e
p<0.001 p<0.001 p<0.001
p<0.001
p<0.001 Pre-UKA
Post-UKA
Figure. Average steady state surgical time
page 17 of 20

Notes
page 18 of 20

Notes
page 19 of 20

15298 V2 0219. Published February 2019, ©2019 Smith & Nephew. Smith & Nephew, Inc, 1450 Brooks Road, Memphis, TN 38116, USA ™Trademark of Smith & Nephew. All rights reserved. All trademarks acknowledged. www.smith-nephew.com
page 20 of 20
Disclaimer Great care has been taken to maintain the accuracy of the information contained in the publication. However, neither Smith & Nephew, nor the authors can be held responsible for errors or any consequences arising from the use of the information contained in this publication. The statements or opinions contained in editorials and articles in this journal are solely those of the authors thereof and not of Smith & Nephew. The products, procedures, and therapies described are only to be applied by certified and trained medical professionals in environments specially designed for such procedures. No suggested test or procedure should be carried out unless, in the reader’s professional judgment, its risk is justified. Because of rapid advances in the medical sciences, we recommend that independent verification of diagnosis, drugs dosages, and operating methods should be made before any action is taken. Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its manufacturer. Some of the products, names, instruments, treatments, logos, designs, etc. referred to in this journal are also protected by patents and trademarks or by other intellectual property protection laws even though specific reference to this fact is not always made in the text. Therefore, the appearance of a name, instrument, etc. without designation as proprietary is not to be construed as a representation by the publisher that it is in the public domain. This publication, including all parts thereof, is legally protected by copyright. Any use, exploitation or commercialisation outside the narrow limits of copyrights legislation, without the publisher’s consent, is illegal and liable to prosecution. This applies in particular to photostat reproduction, copying, scanning or duplication of any kind, translating, preparation of microfilms and electronic data processing and storage. Institutions’ subscriptions allow to reproduce tables of content or prepare lists of articles including abstracts for internal circulation within the institutions concerned. Permission of the publisher is required for resale or distribution outside the institutions. Permission of the publisher is required for all other derivative works, including compilations and translations. Permission of the publisher is required to store or use electronically any material contained in this journal, including any article or part of an article. For inquiries contact the publisher at the address indicated.
References
1. Pastides P, Nathwani D. The role of newer technologies in knee arthroplasty. Orthopaedics and Trauma. 2017;31:47-52. 2. Nair R, Tripathy G, Deysine GR. Computer navigation systems in unicompartmental knee arthroplasty: a systematic review. Am J Orthop. 2014;43:256-261. 3. Jacofsky DJ, Allen M. Robotics in arthroplasty: a comprehensive review. J Arthroplasty. 2016;31:2353-2363. 4. Lonner JH. Robotically assisted unicompartmental knee arthroplasty with a handheld image-free sculpting tool. Orthop Clin North Am. 2016;47:29-40. 5. Roche M. Robotic-assisted unicompartmental knee arthroplasty. The MAKO experience. Orthop Clin North Am. 2015;46:125-131. 6. Lonner JH, Moretti VM. The evolution of image-free robotic assistance in unicompartmental knee arthroplasty. Am J Orthop. 2016;45:249-254. 7. Batailler C, White N, Ranaldi FM, Neyret P, Servien E, Lustig S. Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc.
2018 Jul 31. [Epub ahead of print]8. Battenberg A, Netravali NA, Lonner JH. Early survivorship of robotic-assisted unicompartmental knee arthroplasty. Poster presented at: Southern Orthopaedic Association 35th Annual Meeting; July 11-14, 2018.
Palm Beach; Florida, USA. 9. Canetti R, Batailler C, Bankhead C, Neyret P, Servien E, Lustig S. Faster return to sport after robotic-assisted lateral unicompartmental knee arthroplasty: a comparative study. Arch Orthop Trauma Surg.
2018;138:1765-1771.10. Casper M, Mitra R, Khare R, et al. Accuracy assessment of a novel image-free handheld robot for total knee arthroplasty in a cadaveric study. Comput Assist Surg (Abingdon). 2018;23:14-20.11. Gregori A, Lethbridge R, Simone A. Case study: totals aren’t always an inevitability. BLUE BELT Technologies Inc. 2013. 12. Gregori A, Smith J, Simone A. Case study: First in man: using the NAVIO surgical system to implant a JOURNEY UNI knee. BLUE BELT Technologies Inc. 2014. 13. Gregori A, Picard F, Bellemans J, Smith J, Simone A. Handheld precision sculpting tool for unicondylar knee arthroplasty. A clinical review. Abstract presented at: 15th EFORT Congress; June 4-6, 2014; London, UK.14. Gregori A, Picard F, Lonner J, Smith J, Jaramaz B. Accuracy of imageless robotically assisted unicondylar knee arthroplasty. Paper presented at: International Society for Computer Assisted Orthopaedic Surgery;
June 17-20, 2015; Vancover, Canada. 15. Gonzalez D, Deakin AH, Picard F. Preliminary results of UKR implanted using an image free handheld robotic device. Poster presented at: Annual Meeting of the British Association for Surgery of the Knee; 8-9
April, 2014; Norwich, UK.16. Herry Y, Batailler C, Lording T, Servien E, Neyret P, Lustig S. Improved joint-line restitution in unicompartmental knee arthroplasty using a robotic-assisted surgical technique. Int Orthop. 2017;41:2265-2271. 17. Jaramaz B, Nikou C. Precision freehand sculpting for unicondylar knee replacement: design and experimental validation. Biomed Tech (Berl). 2012;57:293-299. 18. Jaramaz B, Nikou C, Simone A. NAVIO PFS for unicondylar knee replacement: early cadaver validation. Abstract presented at: International Society for Computer Assisted Orthopaedic Surgery; June 12-15, 2013;
Florida, USA.19. Jaramaz B, Noickou C, Casper M, Grosse S, Mitra R. Accuracy validation of semi-active robotic application for patellofemoral arthroplasty. Paper presented at: International Society for Computer Assisted
Orthopaedic Surgery; June 17-20, 2015; Vancover, Canada. 20. Jaramaz B, Mitra R, Nikou C, Kung C. Accuracy assessment of a novel image-free handheld robot for knee arthroplasty in bi-cruciate retaining total knee replacement. Health Sciences. 2018;2:98-101.21. Khare R, Jaramaz B, Hamlin B, Urish KL. Implant orientation accuracy of a hand-held robotic partial knee replacement system over conventional technique in a cadaveric test. Computer Assisted Surgery.
2018;23:8-13. 22. Lonner JH, Smith JR, Picard F, Hamlin B, Rowe PJ, Riches PE. High degree of accuracy of a novel image-free handheld robot for unicondylar knee arthroplasty in a cadaveric study. Clin Orthop Relat Res.
2015;473:206-212. 23. Shah S, Fick D, Khan R, De Cruz P. Robotic assisted revision total knee replacement- early experience. Abstract presented at: 19th Annual Scientific Meeting for APAS. September 6-8, 2018; Bangkok, Thailand.24. Simons M, Riches P. The learning curve of robotically-assisted unicondylar knee arthroplasty. Bone Joint J. 2014;96B:SUPP11.25. Smith JR, Picard F, Lonner J, Hamlin B, Rowe P, Riches P, Deakin A. The accuracy of a robotically-controlled freehand sculpting tool for unicondylar knee arthroplasty. Congress of the International Society of
Biomechanics. 4-9 August, 2013. Natal, Brazil. 26. Smith JR, Riches PE, Rowe PJ. Accuracy of a freehand sculpting tool for unicondylar knee replacement. Int J Med Robot. 2014;10:162-169. 27. Vega Parra PD, Dionisio Palacios Barajas J, Marquez Ambrosi RA, Duarte JR. Robotic-assisted unicompartmental knee replacement with NAVIO surigical system: Outcome evaluation using knee injury
osteoarthritis outcome score. Rev Chil Ortop Traumatol. 2017;58:7-12. 28. Wallace D, Gregori A, Picard F, et al. The learning curve of a novel handheld robotic system for unicondylar knee arthroplasty. Bone Joint J. 2014;96B:SUPP16.