
European Diagnostic Reference Levels in Paediatric Imaging Stephen Evans, Head of Medical Physics,...
50
European Diagnostic Reference Levels in Paediatric Imaging Stephen Evans, Head of Medical Physics, Northampton General Hospital, UK EFOMP Officer, Chair Projects
-
Upload
keyla-dunnell -
Category
Documents
-
view
255 -
download
2
Transcript of European Diagnostic Reference Levels in Paediatric Imaging Stephen Evans, Head of Medical Physics,...

European Diagnostic Reference Levels in Paediatric
Imaging
Stephen Evans, Head of Medical Physics, Northampton General
Hospital, UK
EFOMP Officer, Chair Projects

“Children are at a much higher risk compared to adults from developing cancer”

It’s not child’s play
• UNSCEAR (2010) estimates – 250 million paediatric radiological examinations (including
dental) per annum worldwide• Children may receive substantial radiation doses
– in early life– life-threatening disease
• Children may develop – childhood leukaemia– breast cancer or – thyroid cancer

It’s not child’s play
• Children need special attention: – diseases specific to childhood– additional risks
• Children need special care:– provided by parents and carers– from specially trained personnel
• Justification and optimization principles are even more important for children

• Higher sensitivity to radiation
• Longer life expectancy
• Paediatric doses will exceed adult doses if the same exposure settings are used
Why so high ?

Paediatric effective dose and risk
Examination Effective dose (mSv)
Lifetime risk of fatal cancer
Limbs <0.005 1/few million
Chest (PA) 0.01 1/million
Spine (AP, PA, Lat)
0.07 1/150,000
Pelvis 0.08 1/120,000
AXR 0.10 1/100,000
CT Head 2 1/5,000
CT Body 10 1/1,000
Cook JV, Imaging, 13 (2001), Number 4
? ? Twice the adult risk
i.e. 10% per Sv.
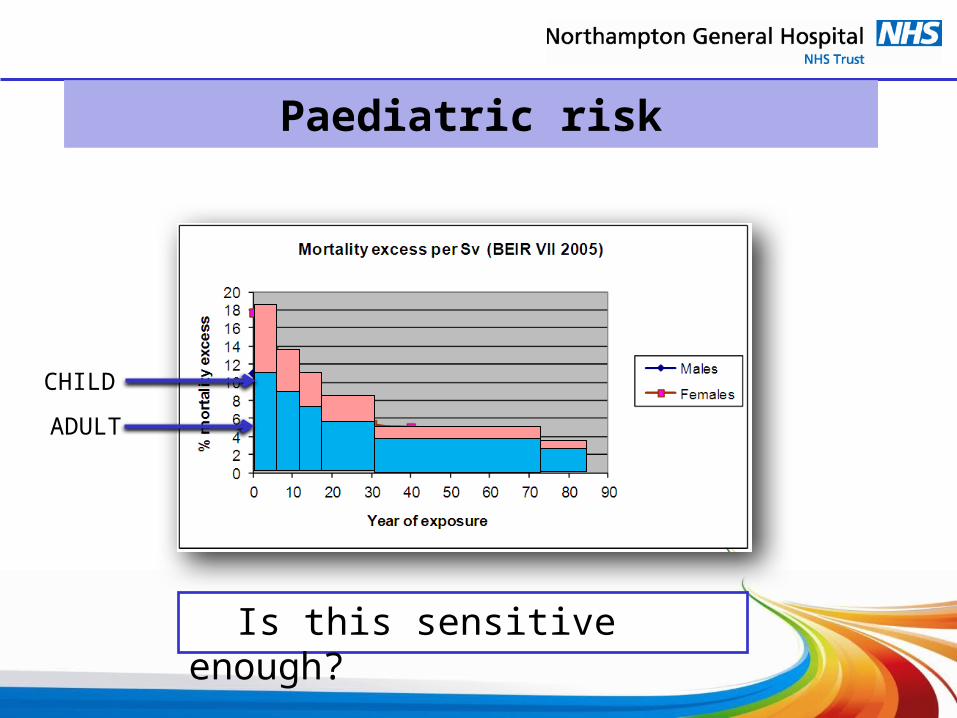
Paediatric risk
ADULT
CHILD
Is this sensitive enough?

Risk from single CT exam
Estimated Risks of Radiation-Induced Fatal Cancer from Pediatric CT
David J. Brenner1, Carl D. Elliston1, Eric J. Hall1 and Walter E. Berdon2,AJR February 2001, Volume 176, Number 2
Read More: http://www.ajronline.org/doi/full/10.2214/ajr.176.2.1760289
1 in 400Not1 in 1000
1 in 1000Not1 in 5000
Single CT exam

What’s the main issue?
• Estimated about – 85% paediatric dose from CT,
interventional fluoroscopy and cardiac nuclear medicine
– 15% paediatric dose from radiography and general fluoroscopy

So what have we done about it?

Well, we have our Directives…

COUNCIL DIRECTIVE 2013/59/EURATOM of 5 December 2013
laying down basic safety standards for protection against the dangers arising from exposure to ionising radiation, and repealing Directives 89/618/Euratom,
90/641/Euratom, 96/29/Euratom, 97/43/Euratom and 2003/122/Euratom
(28) …important technological and scientific developments have led to a notable increase in the exposure of patients. …Directive should emphasise the need for justification of medical exposure, … the use of diagnostic reference levels and the availability of dose-indicating devices.

COUNCIL DIRECTIVE 2013/59/EURATOM
Art 4 (20) "diagnostic reference levels" means dose levels in medical radiodiagnostic or interventional radiology practices, or, in the case of radio-pharmaceuticals, levels of activity, for typical examinations for groups of standard-sized patients or standard phantoms for broadly defined types of equipment;
Art 22 (iii) where practicable, specific diagnostic reference levels are put in place;
Art 56 2. Member States shall ensure the establishment, regular review and use of diagnostic reference levels for radiodiagnostic examinations, having regard to the recommended European diagnostic reference levels where available, and where appropriate, for interventional radiology procedures, and the availability of guidance for this purpose.
Art 58 (f) appropriate local reviews are undertaken whenever diagnostic reference levels are consistently exceeded and that appropriate corrective action is taken without undue delay.
Art 53 MPE (a) optimisation of the radiation protection of patients and other individuals subject to medical exposure, including the application and use of diagnostic reference levels;

And, we have many many scientific studies and Reports…
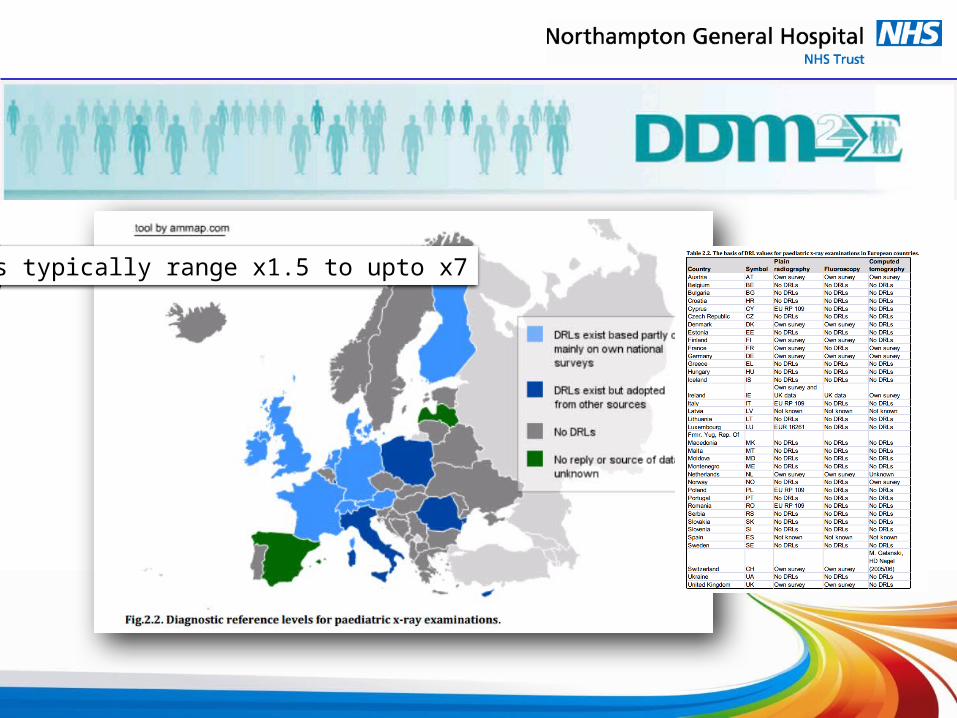
DRLs typically range x1.5 to upto x7
What does all this mean?

1996
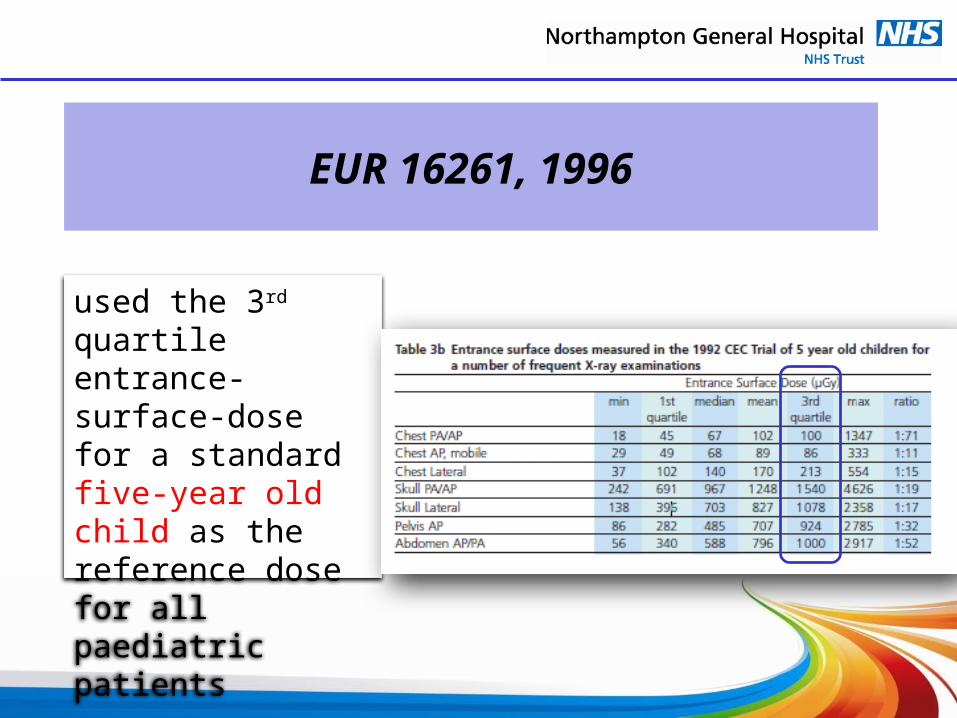
EUR 16261, 1996
used the 3rd quartile entrance-surface-dose for a standard five-year old child as the reference dose for all paediatric patients

• Good general principles– Patient identification!– Quality control of x-ray system– Use of low attenuation materials– Immobilisation
• Field size limitation– Good knowledge of paediatric
anatomy• Protective shielding
– Gonads, breast– Radiographic exposure factors– Number of exposures
EUR 16261, 1996
DRLs
NEVER EVENT
JUSTIFICATION
Good Radiographic Practice

Conclusions of EUR 16261
• Every effort should be made to reduce doses for children less than 5 years of age to below the values presented
• Strict adherence to all the radiographic technique factors recommended can lead to significant dose reduction
• X-ray generators employed in paediatric examinations should be capable of selecting the low mAs values required to ensure that the recommended kV values can be employed

1999

"Guidance on diagnostic reference levels DRLs for medical exposure", European Commission Radiation
Protection 109 (RP 109), 1999)
– exposures requiring the most attention and are of the most importance for the establishment of DRLs are the high-dose medical examinations, especially computed tomography (CT) and interventional procedures (IR)

RP 109
“DRLs should be set by Member States …………….. harmonised levels might be feasible and are certainly preferable.”

RP-109 - Factors affecting dose
• Equipment factors – inappropriate exposure protocols– deterioration of the image chain
• Human factors – inattention, indifference or too much work
pressure– individual reluctance to accept generally-
accepted standard procedures

DRLs in practice
• DRLs can be assessed using:– entrance surface doses, measured with TLD, or – DAP [Gy.cm2]
• DAP is more practical because
(i) the whole examination is recorded;
(ii) the position of the patient in the beam is less important
(iii) there is no need to disturb the patient• For CT
– Dose Length Product (DLP)

DAP DRL issues
• Disadvantages using DAP– absorbed organ dose needs to be measured
• not always a fixed relationship between the DAP and the absorbed dose
– where small areas are exposed, • the DAP can be low while the absorbed dose is
high– when a large area is exposed,
• the DAP can be high but the absorbed dose low– the field size is often changed during fluoroscopy
procedure

CT DRL issues
• Disadvantages of using DLP
DLP = scan length (cm) x CTDIvol (mGy)– Depends on height of patient
• Equipment characteristics– iterative reconstruction -50%– AEC variable mAs – ?%
• might be set too high • dose could be more

DLP - Dose
no AEC AEC
DL
P
no AEC AEC
Do
se
(S
ize
sp
ec
ific
)

“Image Gently”
“One size does not fit all...so when we image, let's image gently!“
Alliance for Radiation Safety in Pediatric Imaging


IAEA No. 24, 2013
“… standardized methodologies to determine paediatric dose for all major modalities, such as general radiography, fluoroscopy and computed tomography.”
“children can receive doses in excess of those delivered to Adults”

CENTRE FOR DISEASE CONTROL AND PREVENTION, 2000 CDC Growth Charts for the United States: Methods and Development, Vital and Health Statistics, Department of Health and Human Services, Rep. (PHS) 2002-1696, Hyattsville, MD (2002).
IAEA No. 24, 2013
5y old
Weight?
25 kgto15 kg
5y old
Height?
115 cmto100 cm
IAEA No. 24 – Patient size
• Options– Age (v. Poor)– Patient thickness
• good for projection radiography• not so good for CT• how to measure?
– Equivalent Cylindrical Diameter (ECD)
W is weight in gms and H is height
in cm

Equivalent Cylindrical Diameter
ECD
H2O
ECD
H2O

2011

Size-Specific Dose Estimate - SSDE
CTDIvol for 32 or 16 diameter phantom
SSDE = f32/16 x x CTDIvol
x depends on projection


Effective Diameter
A A
LAT
AP
Circle of same area

SSDE
Effective diameter for typical 5 year old = 18.5 cm
Conversion Factor for 5 year old (32 cm phantom) ~ 1.9
This means for a given CTDIvol the dose will be twice as much for a typical 5 year old compared to an adult.
Q: Can these factors be used to define the required exposure conditions or do we need equivalent cylindrical diameter ?

Interventional Fluoroscopy
• Equipment should be appropriately designed. Consider: – Beam filter– Beam area– Minimum tube currents– Reduced exposure pulse (need fast for heart)– Removal of the anti-scatter grid– Decreased magnification – Appropriate exposure levels - programming
• RIS – PACS, Repeat procedures– Any repeat exposure within the last 60 days should be
considered additive

Fluoroscopy
• What DRLs do we need?– Incident air kerma Ki (mGy)
Ki = Y(d)Pit(d/dFSD)2 Y(d) – output at distance d
Pit -- tube loading (mAs)
dFSD – focus to skin distance
– Entrance Surface Air Kerma (ESAK) Ke (mGy) Ke = Ki.B (Backscatter factor)
– Kerma-area-product (PKA) (mGy.cm2)
• KAP or DAP meter
IAEA No. 24

Possibilities
• Is it possible to have DRLs for fluoroscopy?– Probably yes
• Skin dose ?– Would not expect for small patients to be high– Obese older patients!!
• DAP ?– Field size varies– Sometime bigger (field) is better (visualisation)
• Monitor fluoroscopy exposure time + acquisitions runs (images) per procedure ?– May be our best indicator for Optimised systems!– TIME – Timely Intervention of Monitored Event

DRLs
• DRLs – show what should be possible– encourage changes in working procedures
• DRLs– Need to be tailored or take account of
• Equipment performance• Patient demographics

So what more do we need to do?
• Identify Equipment factors• Sort out Human factors• Extend the range of DRLs• Base DRLs on individuals
– do we use Equivalent Cylindrical Diameter ? or – effective diameter ? or– something else ?
Planar CT Floro ?DAP DLP TIME
EE o
Base DRLs on individuals

So what are we going to do?
PiDRL - consortium
• European Society of Radiology, ESR• European Society of Paediatric Radiology, ESPR • European Federation of Radiographer Societies, EFRS• European Federation of Organisations for Medical Physics,
EFOMP• Finnish Radiation and Nuclear Safety Authority, STUK with two
sub-contractors: – Helsinki University Hospital, HUS, and – Public Research Centre Henri Tudor

PiDRL - objectives
• Agree on a methodology for establishing and using DRLs for paediatric imaging, and
• Update and extend the European DRLs to
cover more procedures and a wider patient age / weight range.

PiDRL – Work packages
• WP0 - management and general coordination of the project
• WP1 - methodology for DRLs, and producing European
guidelines
• WP2 updating and extending the existing European DRLs
• WP 3 organize the European workshop

THE END
Diagnostic procedures saves children’s lives
but remember
the effects of radiation lasts their lifetime
We all have a duty as professionals
to make it safer for the children
It’s TIME for a change


















