EUROLIVE Clinical Trials Operation Manual
50
1 THE EFFECT OF OLIVE OIL CONSUMPTION ON OXIDATIVE DAMAGE IN EUROPEAN POPULATIONS THE EUROLIVE STUDY PROJECT PROTOCOL OPERATION MANUAL FOR CLINICAL TRIALS
Transcript of EUROLIVE Clinical Trials Operation Manual
1
THE EFFECT OF OLIVE OIL CONSUMPTION ON
OXIDATIVE DAMAGE IN EUROPEAN
POPULATIONS
THE EUROLIVE STUDY
PROJECT PROTOCOL
OPERATION MANUAL
FOR CLINICAL TRIALS
2
RESEARCH TEAM Coordinator: Dr. M. Isabel Covas. Institut Municipal d’Investigació Mèdica (IMIM). Barcelona. Spain. Partner 1: Institut Municipal d’Investigació Mèdica (IMIM). Barcelona. Spain. Principal investigator (PI): Dr. M.I Covas. Partner 2:Department of Clinical Pharmacology. Rigshospitalet Copenhagen University Hospital. Denmark. PI: Prof. Henrik Poulsen. Partner 3: Research Institute of Public Health. University of Kuopio. Kuopio. Finland PI: Prof. Jukka Salonen.. Partner 4: Centro per lo Studio dell´Arteriosclerosi e delle Malattie Dismetaboliche “GC Descovich”. University of Bologna. Bologna. Italy. PI: Prof. Antonio Gaddi. Partner 5: German Institute of Human Nutrition (DifE). University of Postdam. Bergholz-Rehbrueke. Germany PI: Prof. Hans-J. Franz Zunft. Partner 6: .Institute of Transfusion Medicine. Charité. Humboldt University of Berlin. Germany PI: Prof. Holger Kiesewetter Partner 7: Nutrition and Bromatology Department. University of Barcelona. Spain PI: Prof. M. Carmen de la Torre. Partner 8: Oy Jurilab Ltd. Kuopio. Finland PI: Dr. Jari Kaikonnen. Partner 9: Principal Investigator: KEPKA. Consumers Protection Centre. Thessaloniki. Greece P.I.: Mr. Ioannis Sidiropoulos.
3
INDEX PAGE 1. INTRODUCTION
4
2. OBJECTIVES OF THE STUDY
5
3. PROCEDURES
3.1 Protocol of management for Olive oils
3.1.1 Characteristics of the olive oils
3.1.2 Distribution among Clinical Trial Centers.
3.1.3 Storage of the olive oils
3.1.4.Management of individual 25 ml containers
3.1.5 Control of stability
3.2 Protocol management for Clinical Trials
3.2.1 Study design
3.2.2 Study subjects
3.2.3 Sample size and power analysis
3.2.4 Olive oil administration
3.2.5 Methods
3.2.5.1 Recruitment of the participants in the study. Ethic aspects
3.2.5.2. Inclusion in the study: Identification Code
3.2.5.3 General measurements
3.2.5.4 Dietary control
3.2.5.5 Laboratory determinations
3.3. Protocol for Laboratoty samples handling
3.4. Data Base Management
3.5. Custody of the whole ensemble of each participant forms
6
6
6
6
7
7
7
7
7
8
8
9
9
9
10
10
11
11
12
21
21
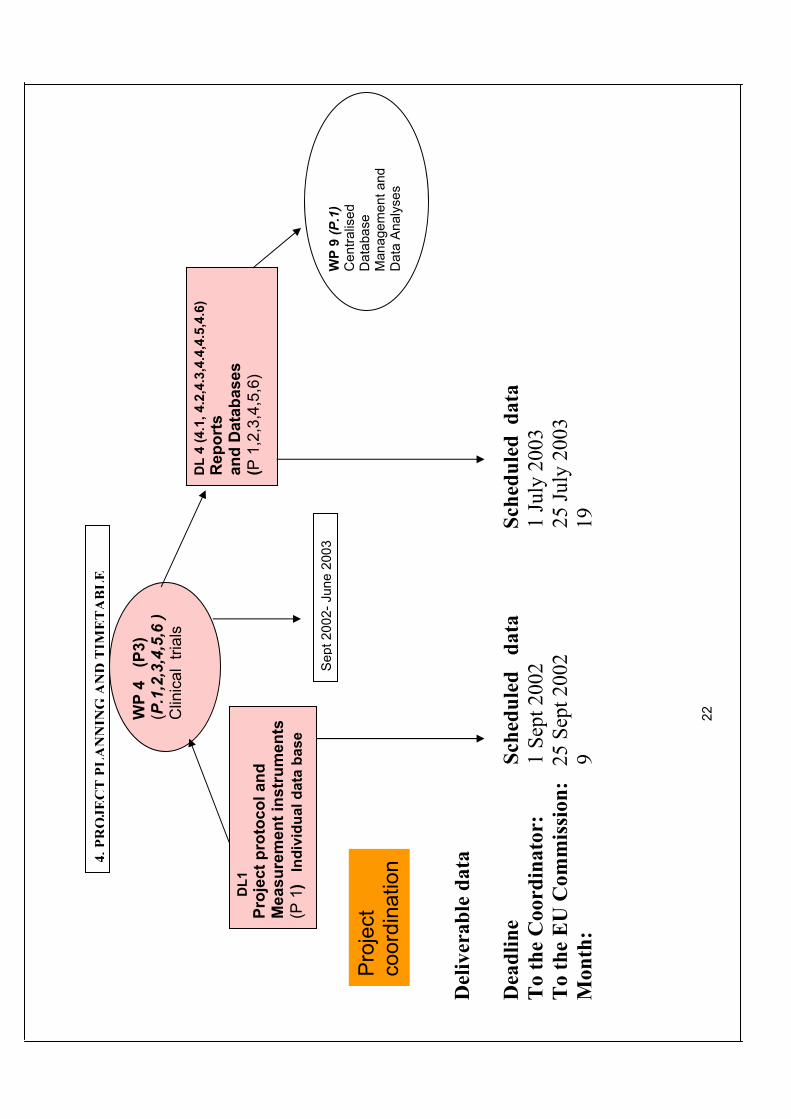
4. PROJECT PLANNING AND TIMETABLE
22
5. ANNEX 1. Participant Informative Signed form
23
6. ANNEX 2. Inclusion form
28
7. ANNEX 3. Randomization protocol
31
8. ANNEX 4. General Measurements
32
9. ANNEX 5. Physical activity assessment
36
10. ANNEX 6. 3-day-dietary record
37
11. ANNEX 7. Alcohol consumption assessment
40
12. ANNEX 8. Outline for laboratory samples handling
41
13. ANNEX 9. Shipment Document form
43
14. ANNEX 10. Laboratory Results form
46

4
1. INTRODUCTION There is growing epidemiological evidence supporting the idea that the Mediterranean diet has a beneficial
effect on diseases associated with oxidative damage, such as cardiovascular and neurodegenerative diseases,
cancer, and ageing.The Mediterranean diet has also been shown to be effective in secondary prevention of
CHD (4). The lower incidence of CHD in Mediterranean countries has been attributed to a diet rich in fruits,
vegetables, legumes, cereals, and to its major vegetable fat component, olive oil .
Olive oil is the only vegetable oil obtained from whole fruits rather than from seeds. Phenolic compounds are
responsible for the characteristic flavor and taste of common and virgin olive oil. Phenolic compounds are
lost in the olive oil refinement processes. However, unlike oils from other origins, extra-virgin olive oil of
high quality is consumed directly without refinement. Virgin olive oil phenolic compounds have been shown
to inhibit LDL oxidation metal-induced and peroxyl radical-dependent in vitro, and to inhibit the cytostatic
and cytotoxic activity of oxidized LDL on mucous intestinal cells .
A dietary antioxidant is a substance present in foods that significantly decreases the adverse effects of
reactive oxygen species, reactive nitrogen species, or both, on normal physiological function in humans.
Recommended daily intakes of beta-carotene and other carotenoids, vitamin C, vitamin E, and selenium are
currently under review. Other potentially beneficial antioxidants, such as phenolic compounds, could be
reviewed in the future when more substantial published information becomes available. Therefore, it is
imperative to undertake placebo-controlled, double blind, randomized, phenolic-rich food supplementation
trials to establish their effects on oxidative damage in humans.
The olive oils found in the market are:
1) Virgin olive oil: the direct product of milling and extraction by physical methods without any further
treatment. It is rich in phenolic content (from 150 to 600 mg/Kg of equivalents caffeic acid (CAE)). Extra-virgin
olive oil is a virgin olive oil with an acidity lesser than or equal to 1. Virgin olive oils with an acidity greater than
3.3 are refined. Phenolic compounds are lost in the virgin olive oil refinement processes.
2) Common Olive oil: (a mixture of refined and virgin olive oil with moderate phenolic content from 60 to 150
mg/Kg CAE).
3) Olive pomace oil: after virgin olive oil extraction the remains of the olive (called ”mark” or ”pomace”) is a
mixture of peels, parenchima, broken stone of the fruits and water. The extraction of oil from the pomace is done
by thermal dessication and with organic solvents. After refinement, some virgin olive oil is added for colour and
flavour purposes.
The market price of olive oils differs, common olive oils being cheaper than virgin ones. Thus, the nutritional
value of the different types of olive oils deserves to be investigated in order to inform both European
Consumers and the Olive Oil Industry of the nutritive characteristics of each type and their cost/benefit ratio.
Also, recomendations on the appropiate use of each type of olive oil for nutritional purposes could emerge from
the results of the project. An improved understanding of the interactions which exist between the phenolic
composition of olive oil and olive oil quality (flavour) is expected. People with low income should know if there
are other benefits than flavour, in order to invest in virgin olive oil instead of common olive oil. Also, a rationale
to include the nutritional facts, i.e. phenolic content, in labelling of olive oils is expected.
In this project, virgin, common, and refined (from virgin olive oil, not pomace oil) olive oil will be used.
5
2. OBJECTIVES
2.1. To compare the impact of olive oil, an antioxidant-rich foodstuff, on oxidative damage and low-
density lipoprotein (LDL) fatty-acid composition across selected European countries.
2.2. To investigate the bioavailability of olive oil phenolic compounds in humans.
2.3. To compare differences in the postprandial oxidative stress response as a function of the
phenolic content of olive oils.
2.4. To explore differences in lipid peroxidation and fatty acid composition of LDL among healthy men
from different European countries.
2.5. To determine whether the substitution of saturated by monounsaturated fat results in better LDL
fatty acid composition after three months of olive oil administration in Central and Northern
European participants.
2.6. To provide information to Olive oil Producers on the nutritive characteristics of the
different types of olive oil produced.
2.7. To actively disseminate the results of the project among European and non-European
consumers and the nutritional recommendations that stem from them.
6
3. PROCEDURES
3.1 Protocol of management for Olive oils
3.1.1 Characteristics of the olive oils
The olive oils selected for the study are from the cultivar “Picual” from Jaen (Andalucía, Spain). These oils
reflect the varieties of olive oils present in the market. As a previous step, determination of the total phenolic
content of several harvests of virgin olive oil was performed, and the virgin olive oil with higher phenolic
content (366 ppm) was selected. Fatty acids and vitamin E composition were also measured. This will be the
high phenolic content olive oil used in the study (Virgin). From the same cultivar and soil, harvests of virgin
olive oils which were submitted to refinement, were tested in order to select one with a similar fatty acid
profile to that of the virgin olive oil selected. The content of vitamin E in the refined olive oil was measured,
and an adjustment to similar values of that present in virgin olive oil was performed. The vitamin E
adjustment was performed for all the refined olive oil in a tank of 100 liters. Samples from the top, and
bottom of the tank were taken and the vitamin E concentration was tested in order to ensure the homogenity
of the adjustment. This will be the null phenolic content olive oil used in the study (Refined). By mixing, in
a tank, virgin and refined olive oil in a 1:2 parts ratio, respectively, a common olive oil (olive oil, UE 1991)
of 164 ppm of phenolic content was obtained. Samples from the top and bottom of the tank were taken and
the phenolic and vitamin E content and fatty acid profile were tested in order to ensure the homogenity of
the mixture. This will be the medium phenolic content olive oil used in the study (Common).
The required measurements of phenolic compounds, vitamin E and fatty acids were performed in the
Department of Nutrition and Bromatology (Partner 7). The adjustment of vitamin E levels in the refined
olive oil, the mixing of virgin and refined olive oils, and the distribution of olive oils in 5 L containers were
completed by the Department of Galenics of the Farmacia Faculty of Barcelona University, which has
industrial type installations. Nitrogen gas was put into the 5L containers. Olive oils were stored in the dark
in plastic containers of 5 liters at 4ºC.
The measured characteristics of the olive oils will be sent to the EU Commission as DL2. The following
measurements will be included: Quality parameters: (acidity and peroxide value), total phenolic compound
and vitamin E content, and fatty acid profile .
3.1.2 Distribution among Clinical Trial Centers.
Sets containing 4 containers of virgin (20 L), 4 containers of common (20 L), and 4 containers of refined
(20 L) olive oil will be sent from the Coordinating Centre, by courier mail, to each of the Clinical Trial
Centres participating in the Study (Partners 1-6). Codes (580, 430, 750) will be assigned to each type of
olive oil in order to blind the clinical trial.
3.1.3 Storage of the olive oils.
In the Clinical Centres, the 5-liter olive oil containers will be stored in darkness at 4ºC until the preparation
of 25-ml individual containers.
7
3.1.4 Management of individual 25 ml containers
At the end of each washout period, a set of portable containers with the corresponding 25 ml of olive oil for
each day of consumption will be prepared, and delivered to the participants at the beginning of each olive oil
administration period at the time of blood collection. After collection of the quantity of olive oil required to
prepare the 25-ml containers, nitrogen gas must be put in the 5-liter container. This prevents the contact of
the olive oil with oxygen in the remaining air layer.
Participants must be informed that individual containers must be stored in a dry, at room temperature (20-
25ºC) and relatively dark place at home. Participants must return the containers to the centre after the
corresponding olive oil consumption period in order to register the amount of olive oil consumed in this
period.
3.1.5 Control of stability
The Clinical Trial execution time has been estimated to be 9 months (Sept 2002-May 2003). Every 3
months, each participating center will send samples of the olive oils (50ml of each olive oil, with nitrogen
gas) to the Partner 7 Center in order to check the stability of the oils:
Dr. MC López-Sabater
Facultat de Farmàcia. Departament de Bromotologia I Nutrició.
Institut Municipal d'Investigació Mèdica (IMIM)
Av. Joan XXIII s/n
08029 Barcelona. SPAIN
Telephone: +34 93 4024508/ FAX: +34 93 4021896
E-mail: [email protected]
3.2 Protocol management for Clinical Trials
3.2.1 Study design
The study design is a cross-over clinical supplementation trial, in which 30 subjects in each centre (180
subjects in total) will be randomised for 3 periods of 3 weeks to receive 25 ml (as replacement of other raw
fats) of a raw:
- Virgin olive oil (High phenolic content)
- Common olive oil (Medium phenolic content)
- Refined olive oil (null/very low phenolic content)
Oils will be coded in order to perform the study in a blind manner. Before the assay and between olive oil
administration periods (25 ml per day during 3 weeks) wash-out periods of 2 weeks without olive oil
consumption, will be performed. The study will be done according the following protocol:
8
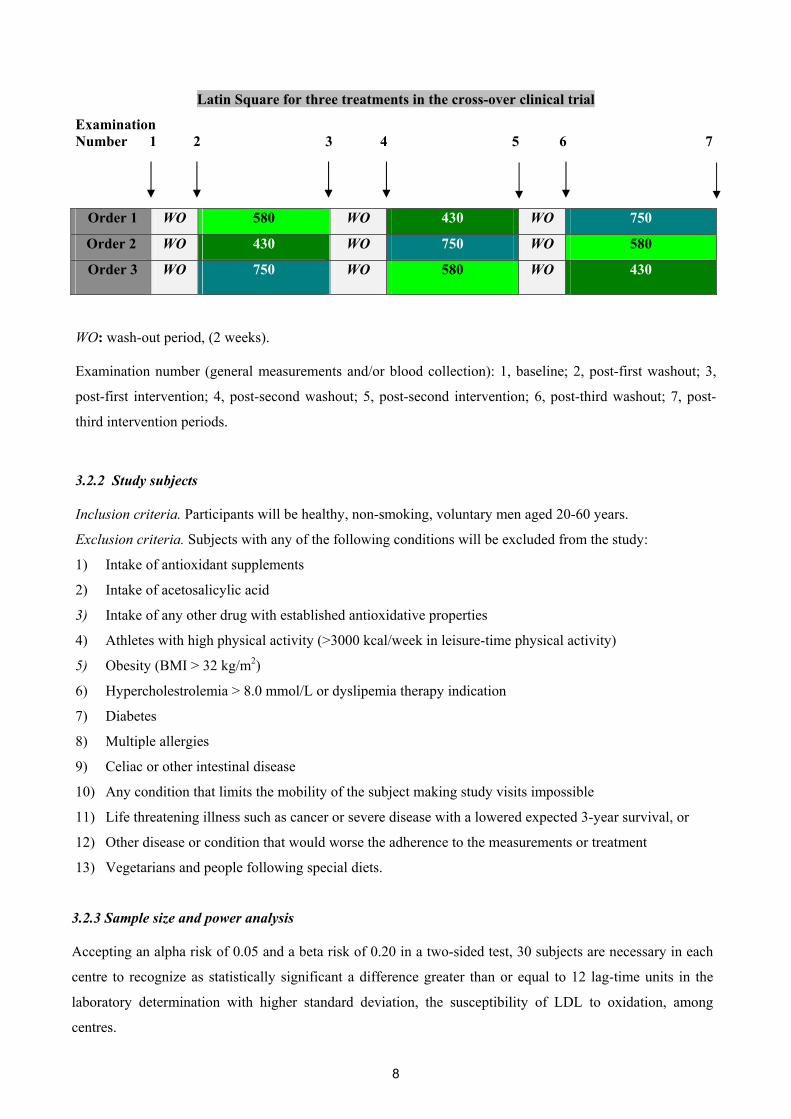
Latin Square for three treatments in the cross-over clinical trial
Examination Number 1 2 3 4 5 6 7
Order 1 WO 580 WO 430 WO 750
Order 2 WO 430 WO 750 WO 580
Order 3 WO 750 WO 580 WO 430
WO: wash-out period, (2 weeks).
Examination number (general measurements and/or blood collection): 1, baseline; 2, post-first washout; 3,
post-first intervention; 4, post-second washout; 5, post-second intervention; 6, post-third washout; 7, post-
third intervention periods.
3.2.2 Study subjects
Inclusion criteria. Participants will be healthy, non-smoking, voluntary men aged 20-60 years.
Exclusion criteria. Subjects with any of the following conditions will be excluded from the study:
1) Intake of antioxidant supplements
2) Intake of acetosalicylic acid
3) Intake of any other drug with established antioxidative properties
4) Athletes with high physical activity (>3000 kcal/week in leisure-time physical activity)
5) Obesity (BMI > 32 kg/m2)
6) Hypercholestrolemia > 8.0 mmol/L or dyslipemia therapy indication
7) Diabetes
8) Multiple allergies
9) Celiac or other intestinal disease
10) Any condition that limits the mobility of the subject making study visits impossible
11) Life threatening illness such as cancer or severe disease with a lowered expected 3-year survival, or
12) Other disease or condition that would worse the adherence to the measurements or treatment
13) Vegetarians and people following special diets.
3.2.3 Sample size and power analysis
Accepting an alpha risk of 0.05 and a beta risk of 0.20 in a two-sided test, 30 subjects are necessary in each
centre to recognize as statistically significant a difference greater than or equal to 12 lag-time units in the
laboratory determination with higher standard deviation, the susceptibility of LDL to oxidation, among
centres.
9
The common standard deviation of the method is 15 min. A dropout rate of 15% has been anticipated. This
sample size will also permit us to show, as statistically significant with a power of 80 %, a difference of 10
lag-time units among treatments in the clinical trial which is designed as a cross-over with three types of
olive oil (one without, a second with low-content and a third with high-content of phenolic compounds), in
each centre. Drop-outs before the first intervention period will be replaced in order to avoid drop-outs greater
than 15%, It was recomended that all efforts should be made to ensure that volunteers are ready to complete
the RCT before randomization. Codes for 5 additional volunteers will be supplied (from 31 to 35) from the
coordinating centre
3.2.4 Olive oil administration
In the olive oil administration periods 25 ml of raw virgin, common or refined olive oil will be taken with
participant prefered foods. A set of portable containers with the corresponding 25 ml of olive oil for each day
of consumption will be delivered to the participants at the beginning of each olive oil administration period.
The nutritionists will assist by advising participants and their family members on the adequate foods to eat
using the raw olive oils in each specific country. Participants will be encouraged to consume all the olive oil
pouring it off from the 25 ml containers, absorbing the excess in the dish with bread and eat this bread.
The participants will be instructed to return the containers to the centre after the corresponding olive oil
consumption period in order to register the amount of olive oil consumed in the period.
3.2.5 Methods
3.2.5.1 Recruitment of the participants in the study. Ethic aspects.
At the first contact with the potential participant, an explanation of the study, its objectives, development,
confidentiality, as well as the required signed agreement, will be performed. A Participant Signed Consent
Form for the possible volunteers, recommendations (ANNEX 1) and the explanatory booklet of the study
(DL 24) will be delivered to the participants. If they wish participate, they must read carefully the
Participants Signed Consent Form (ANNEX 1) and if they agree with it, to sign the document. A general
questionnaire (ANNEX 2) will be administered in order to check whether there are criteria which preclude
participation of a candidate from the study. Volunteers will be selected when clinical history, physical
examination, blood pressure, and toxic habits do not show any exclusion criteria. Next a routine laboratory
analysis will be performed which will include: Biochemical tests (serum glucose, total cholesterol,
creatinine, GGT, alanine transaminase (GPT), triacylglycerols); Haematological tests (Haemogram: white
blood cells, haemoglobine, platelets); Urine (Stick: pH, glucose, ketones, bilirrubine, proteins, red blood
cells, leukocytes, and nitrates. Included subjects have to have analytical values within the reference range established for these parameters.
Concerning the borderline values, the criteria of the person in charge of the clinical trial will be applied on
10
the basis of the state of the art, clinical signification of the borderline value, risk prediction or interference in
the evaluation of the intervention.
The protocol must be approved by the Local Ethics Committee.
3.2.5.2. Inclusion in the study:
Olive Oil Administration Order.
Randomization of the participants will be performed in the Coordination Centre. At the time of the
participant’s inclusion in the study, each centre will send a fax (ANNEX 3) to the Coordinating Centre with
the participant’s internal identification (code given in the centre) and the initials of the participant’s name.
The Coordination Centre will send this fax back to the Clinical Trial centre with the random code (identifier
code) and the order of participant’s inclusion in the study.
Participants will be randomized into one of the following orders of olive oil administration :
Order 1: 580/430/750
Order 2: 430/750/580
Order 3:750/580/430
The questionnaires, records of blood pressure,blood collection tubes, and laboratory aliquots will be labeled
with the following Identification: Identifier Code-Number of examination (1-7)
Identifier code: Partner achronym : (IMIM-Spain= IMIM, RH-Denmark= RHC, University-Finland=
UKU, UNIBO-Italy= UBLG, DIFE-Bergholz-Rehbruecke-Germany= DIFE, CHARITE-Berlin-Germany=
UBER) + Volunteer number: number assigned to the volunteer after randomization in the Coordinating
Centre (from 01 to 35).
Examination number: 1 (baseline), 2 (first post-washout period), 3 (first post-intervention period), 4 (second
post-washout period), 5 (second post-intervention period), 6 (third post-washout period), 7 (third post-
intervention period).
3.2.5.3 General measurements
General measurements will be registered in a form common to all the participating Centres but adapted to the
local language if preferred (ANNEX 4).
The following variables will be recorded at the beginning of the study (ANNEX 4):
a) Educational factors
b) Family History of Disease
c) Height,waist/hip ratio
The following variables will be measured at the beginning at the end of the study:
11
a) Physical activity: Physical activity in the leisure time performed in the last year will be evaluated.
An adaptation of the Minnesota Leisure Time Questionnarie will be used (ANNEX 5).
The following variables will be recorded at baseline, and before and after olive oil intervention periods:
a) Weight, systolic and diastolic blood pressure (ANNEX 4)
3.2.5.4 Dietary control
Participants will record the quality and quantity of food ingested/day by means of a 3-day dietary record (see
model in ANNEX 6) at baseline (Exploration number 1) and during the last three days of each olive oil
administration periods (Exploration numbers:3, 5 and 7). On each ocasion, alcohol consumption in the last seven
days (in order to establish the mean daily intake including both working and week-end days) will be recorded in a
separate questionnaire (ANNEX 7).
-To avoid an excessive intake of antioxidants and phenolic compounds during the clinical trial period,
participants will be advised to limit the consumption of the followings foods to:
a) 2 servings of vegetables or pulses/day
b) 3 servings of fruits (this includes juices)
c) 3 cups of tea or coffee/day
d) 2 pieces of a bar of chocolate/day
e) 2 glasses of wine/day
f) <1 liter of beer/day
Participants will be personally advised by a nutritionist on how to record food consumption and complete the
above mentioned dietary recommendations.
Energy consumption and dietary intakes of macro- and micronutrients will be calculated from the 3-day
records using an appropriate software which should permit the introduction of new foods and nutrients
relevant for the adjustment of the effect of oil ingestion (i.e. phenolic compounds).
Nutrients selected to be included in the general data base will be:
Essencial
Energy, carbohydrate, protein, total fat, saturated fat, polyunsaturated fat,
monounsaturated fat, cholesterol, oleic acid, ascorbic acid, tocopherol, retinol,
folate, pyridoxine, cobalamin, beta-carotene, selenium, zinc, iron, total phenolic
compounds
Desirable
Alfa-carotene, lutein, lycopene, beta-cryptoxanthin, flavonoids, phenolic acids, tannins,
myristic acid, palmitic acid, linolenic acid, linoleic acid, arachidonic acid, dietary fiber,
soluble dietary fiber
Concerning phenolic compounds in food, given that information about their content in food is
scattered and scarce, a list of the phenolic compounds in foods will be constructed from data
collected by Kuopio University and IMIM. This list will be distributed to all participants .
12
3.2.5.5 Laboratory determinations
The following measurements will be carried out in samples drawn from the subjects at the
examinations done before the first wash-out period (1-basal), and before and at the end of the virgin ,
common and refined olive oil administration periods of the clinical supplementation trial:
- Measurement of phenolics:
- selected phenol as a marker of olive oil consumption
- Measures of lipid peroxidation:
- susceptibility of LDL to oxidation
- baseline uninduced LDL conjugated dienes
- hydroxy fatty acids in plasma
- plasma F2 isoprostanes
- oxidized LDL
- Measurements of DNA oxidation
- urinary 8-oxo deoxyguanosine (8-oxo dGuo)
- urinary 2,6-diamino-4-hydroxy formamidopyrimidine (FaPyGua)
- urinary 4,6-diamino-5-formamidopyrimidine (FaPyAde)
- Measurements of endogenous antioxidants
- whole blood superoxide dismutase, plasma glutathione reductase and peroxidase
activities
- serum glutathione (ox/redox) and paraoxonase activity
- Measurements of exogenous antioxidants
- plasma tocoferol, betacarotene, and lycopene
- plasma ascorbic (AA)´AA/DHA (dehydroascorbic) acid
- plasma enterolactone
- Other determinants of lipid peroxidation:
- serum lipids (cholesterol, LDL, HDL, triglycerides)
- fatty acids in LDL at the beginning and at the end of the study
The chemical tests will be performed in a single central laboratory from deep-frozen samples. Four
laboratories will act as central laboratories in the study
3.3. Protocol for laboratory sample handling in the Eurolive study. Randomized clinical trial
assay
3.3.1. Materials
It is recommended that the same materials are used by all participant centers to avoid differences in
the blood collection and sample conservation:
BD Vacutainer tubes. BD (Becton and Dickinson and Company) Vacutainer Systems,
Preanalytycal Solutions. Belliver Industrial Estate, Plymouth. PL6 7BP. UK.
13
1. Product number 366457: 16 x 75 mm x 10.0 ml BD Vacutainer™ glass whole
blood tube; Lavender conventional closure; Paper label; Additive: K3EDTA 15%
solution, 0.117 ml, 17.55 mg. (100/bx, 1000/ca).
2. Product number 366430: 16 x 100 mm x 10.0 ml BD Vacutainer™ glass serum
tube; Red conventional closure; Paper label; No additive, silicone coated. (100/bx,
1000/ca).
3. Product number 366485: 13 x 75 mm x 5.0 ml BD Vacutainer™ glass plasma tube;
Green conventional closure; Paper label; Additive: Lithium heparin (freeze-dried),
72 USP units. (100/bx, 1000/ca).
Nalge Nunc International. Kamstrupvej 90-PO box 280. DK-4000 Roskilde Denmark.
1. Cryotube 1.8mL SI, INT, STARFOOT, ROUND (50/bag, 450/cases) (ref 377267).
2. Nunc cryocolor code, blue (ref 354879).
3. Nunc cryocolor code, red (ref 354968).
4. Nunc cryocolor code, green (ref 355018).
D(+)-sucrose (Fluka Biochemika 84099, SIGMA-ALDRICH)
N-ethylmaleimide (NEM) (E-3876 SIGMA-ALDRICH)
Bathophenanthroline-disulfonic acid (BPDS) (B-1375 SIGMA-ALDRICH)
Sodium Bisulfite (S-9000 SIGMA-ALDRICH)
EDTA/ Titriplex III [1.08418 Merk)]
33.5% Metaphosphoric acid (M-6288 SIGMA-ALDRICH)
69% Perchloric acid-d (24,425-2 SIGMA-ALDRICH)
HCL 1M
25 mL flasks for olive oil
Cardboard containers of the cryotubes 13 x 13 x 5cm (378220 Nalge Nunc International)
10 mL tubes
3.3.2. Sample identification
Labels for primary tubes, cryotube aliquots, and cardboard boxes for cryotubes will be sent to all the
Clinical Trial Centres from the Coordinating center (IMIM). Samples from each type of byologic fluid
blood collection (serum, plasma, urine…) will be aliquoted in color-coded cryotubes depending on the use
or not of anticoagulant, and which anticoagulant has been used in each case. Furthermore, each cryotube must
have the IDENTIFICATION (or sample-code) (see below) and the PARAMETER-CODE (see below).
IDENTIFICATION: Identifier Code - Number of examination (1-7)
Identifier code: Partner achronym : (IMIM-Spain= IMIM, RH-Denmark= RHC, University-Finland=
UKU, UNIBO-Italy= UBLG, DIFE-Bergholz-Rehbruecke-Germany= DIFE, CHARITE-Berlin-Germany=
UBER) + Volunteer number: number assigned to the volunteer in the Coordinating Centre (from 01 to 35).

14
Number of examination: Number of examination/Blood collection number: 1 (baseline), 2 (first post-
washout period), 3 (first post-intervention period), 4 (second post-washout period), 5 (second post-
intervention period), 6 (third post-washout period), 7 (third post-intervention period).
PARAMETER-CODE:
EDTA whole blood Use Nunc cryocolor code blue: for EDTA whole blood:
SOD activity: SOD-EDTA whole blood; DNA extraction (Buffy coat): buffy-cells EDTA;
Oxidized glutathione from EDTA whole blood: GSSG-EDTA whole blood; Reduced
glutathione from EDTA whole blood: GSH-EDTA whole blood; RNA extraction from white
blood cells (leukocytes) pellet from EDTA whole blood: RNA-leukos EDTA.
EDTA Plasma Use Nunc cryocolor code blue: for
Phenolic compounds (tyrosol, hydroxytyrosol, metyl-hydroxytyrosol): PC-EDTA pl; Oxidized
LDL: oxLDL-EDTA pl; GSH-Px/GSSG-Rd: GSH Enz-EDTA pl; Lipid-soluble antioxidants:
LSA plasma-EDTA pl; hydroxy fatty acids: OH-FA-EDTA pl; Enterolactone: enter-EDTA
pl; Reserve: stock-EDTA pl.
Use 5mL plastic tube: for EDTA plasma:
Isoprostanes: Isoprostanes-EDTA pl; LDL isolation for CD: CD-EDTA pl; LDL isolation for
FA: FA/LDL-EDTA pl.
Serum
Use Nunc cryocolor code red: for serum:
Lipids: Lipids-s; paroxonase activity: PON-s; reserve: Stock-s.
Use 5mL plastic tube:
Uninduced dienes: UnCD-s
Lithium Heparin plasma
Use Nunc cryocolor code green: for LITHIUM HEPARIN plasma:
Ascorbic acid/dehydroascorbic acid: AA/DHAA Hep pl.
For example, the sample for isoprostanes for the third participant from Italy after the second
intervention period will be:
UBLG/03/5 Isoprostanes EDTA pl and the cryotube will wear a cryocolor code blue.
24h urine:
Use 10mL tubes for: 24h urine-DNA oxidation: DNAox-urine
Use 25mL containers for: Phenolic compounds in urine: PC-urine
15
IT MUST BE TAKEN INTO ACCOUNT THAT SOME DETERMINATIONS REQUIRE SPECIAL
SAMPLE HANDLING
3.3.3. Sample collection
Samples must be collected at fasting state of at least 10 hours .
Serum : One 10 mL tube (Blood collections from 1 to 7)
Serum tubes must be allowed to exactly clot for 30 minutes at room temperature. After
centrifugation (1000 x g, 15 minutes) serum must be stored at -80°. Samples for uninduced
dienes require special handling (Partner 8 and partner 1 protocols).
EDTA Whole blood/Buffy cells/ Plasma:
Blood collections 1 and 7: Six 10 mL tubes
Blood collections 2,3,4,5 and 6: Five 10 mL Tubes
Keep blood tubes in an ice bath at the time of blood collection. Take the quantity of whole
blood required to perform the aliquots for GSSG, GSH (Partner 1), SOD (Partner 8) and RNA
(optional). Centrifuge at +4°C (1000 x g, 15 minutes), and at the first blood collection buffy-coat
must be collected from the interphase layer. Then collect plasma and consider that some samples
require a special pre-analytical treatment (see partners 1, 7, and 8 protocols). Store aliquots at -
80°C as soon as possible after blood drawing.
Heparin Plasma : One 5mL tube (Blood collections from 1 to 7)
Take blood sample from freely running needle to ensure that haemolysis does not occur.
Immediately centrifuge, e.g. 2000-3000 rpm (700-1600 xg), for as short time as possible, about 1
min, just to make it possible to get 0.5mL of plasma from the sample. You will have to
experiment to get the required centrifugation time as short as possible (Partner 2 protocol).
24h Urine samples (Blood collections from 1 to 7)
The 24 hours urine containers will be handed to the volunteers before the study. A phone call will
be done two days before the basal examination to remind them to collect the 24 hours urine. When
collecting the 24 hours urine, the volunteer must discard the first morning urine on day 1, and
collect all the urine during this day, in a appropiate container , and including the first morning urine
of day 2. In order to ask if some urine has been thrown out of the 24 hours containers, the question:
“How much urine have you thrown” will be asked instead of: “Did you throw some urine?”.
Each aliquot of 24 hour urine samples, beside identification label, must have a label with the
total volume of 24-h urine collected during a day, both labels attached at the side of the
container. 24 hour-urine must be well mixed before performing the aliquots. The sample for
phenolic compounds (PC = Tyrosol, OHTyr and O-M-OHTyr) requires special handling (Partner
1 protocol).
Sample handling procedures are outlined in Annex 8

16
3.3.4. Sample requirements for partner 1 in the EUROLIVE study:
Sample (Label Code) Volume Nº aliquotes
Cryo-color
Serum LIPIDS (Lipids-s) 0.3mL 2 red
Serum STOCK (Stock-s) 0.5mL 2 red a EDTA DNA extraction (buffy-cells EDTA) 1.5mL 2 blue
EDTA plasma OxLDL (OxLDL-EDTA pl) 0.3mL 2 blue
EDTA plasma GSH ENZYMES (GSH enz-EDTA pl) 0.5mL 1 blue b EDTA plasma T, OHT, O-M-OHT (PC-EDTA pl) 2 mL 2 blue c EDTA plasma Conjugated Dienes (CD-EDTA pl) 4.5mL 2 5mL tube
EDTA plasma Stock (Stock-EDTA pl) 0.3mL 2 blue d EDTA whole blood GSSG (GSSG-whole blood EDTA) 0.5mL 1 blue d EDTA whole blood GSH (GSH-whole blood EDTA) 0.5mL 1 blue e EDTA blood leukos pellet-RNA extraction (RNA-leukos EDTA) From 0.5mL 1 blue f24h urine T, OHT, O-M-OHT (PC-urine) 25mL 2 container
a Buffy coat: Only at the beginning (1st collection) of the study. After centrifugation of the blood EDTA
tube, collect the interphase layer between the EDTA plasma and the cells phase, starting at the white
interphase using a sterile Pasteur pippette until 1,5mL has been collected.
b Plasma determination of PC (T, OHT, O-M-OHT):
0.5 M sodium bisulfite (Na2S2O5) preparation:
10.4g of sodium bisulfite/100mL of distilled water (3 month stability at 4ºC).
Add 50 µL of 0.5M sodium bisulfite to each 2 ml aliquot of EDTA plasma samples. Store samples at -80ºC
without delay.
c Isolation LDL particle by sequential flotation ultra centrifugation.:
18mM saccharose preparation:
1.5g of saccharose/250 mL of distilled water (store at 4ºC, stability 4 moths).
After centrifugation, EDTA plasma must be stored with saccharose. Add 45 µL of the 18mM saccharose
solution to each 4.5 ml plasma aliquot (use 5 ml polipropilene tubes with the corresponding caps). Store
samples at -80°C without delay. Send the plasma samples.Isolation of the LDL will be performed at the
IMIM.
d Glutathione determination:
Precaution measurements: It it important to prepare the following solutions in an extractor hood, pouring the
68% perchloric acid onto the distilled water.
17
12% perchloric acid (PCA), 2mM Bathophenanthroline-disulfonic acid (BPDA) preparation: (stability 9
months at room temperature)
412mL distilled water + 88mL 68% PCA + 0.5365g BPDA
12% PCA, 2mM BPDA, 40mM N-ethylmaleimide (NEM) preparation: (stability 9 months at room
temperature).
412mL distilled water + 88mL 68% PCA + 0.5365g BPDS + 2.502g NEM
EDTA whole blood sampling for GSSG determination:
1. Mix 0.5mL of EDTA whole blood with 0.5mL 12% PCA, 2mM BPDA.
2. Centrifuge for 5 min at 6160 x g (approximately 10000 rpm in an ependorf centrifuge) collect the
supernatant in a cryotube and store it at -80ºC withoth delay.
EDTA whole blood sampling for GSH determination:
1. Mix 0.5mL of EDTA whole blood with 0.5mL 12% PCA, 2mM BPDA, 40mM NEM.
2. Centrifuge for 5 min at 6160 x g collect the supernatant in a cryotube and store it at -80ºC withouth delay.
f Urinary determination of T, OHT, O-M-OHT: Put 0.5mL of 0.5 M sodium bisulfite (see plasma PC
protocol) into the 25 ml 24-h urine samples (see paragraph b). Write the total 24-hour urine volume on the
side of the container. Store samples at -80ºC without delay.
3.3.5. Sample requirements for partner 2 in the EUROLIVE study.
Sample Volume Nº of aliquotes Cryo-color a Hep plasma-AA/DHAA (AA/DHAA-hep pl) 0.5mL 1 green b 24h urine-DNA oxidation (DNAox-urine) 10mL 2 10 mL tube
a Plasma ascorbic acid (AA) and dehydroascorbic acid (DHAA):
10% Metaphosphoric acid (MPA), 2 mmol/L EDTA preparation: (stability of fresh solution 1 week. Aliquots
can be stored at -20ºC, for 3 more weeks).
351mL distilled water + 149g 33.5% MPA + 0.37224g EDTA
1. Take blood sample (5-10 mL depending on your standard heparin test tube) from freely running
needle to prevent haemolysis.
2. Centrifuge immediately at 2000-3000 rpm (716-1611 xg) for as short a time as possible (<1 min), just
to make it possible to get 0.5mL of plasma from the sample. (You may have to experiment with the
centrifuge to minimize the time between starting/stopping the centrifuge and getting the sample out).
The time from taking the blood sample to pipetting the 0.5mL plasma should be less than 2 min, and
should be the same for all samples.
3. Mix 0.5mL plasma (from above) with 0.5mL cold (ice cooled) 10% Metaphosphoric acid (MPA) in 2
mmol/L EDTA (the sample turns white).
18
4. Mix the sample in a vortex, centrifuge 3.000 rpm (1600 xg) for 5 min, and transfer the supernatant
(about 0.7-0.9mL) to a freezing tube and store at -80 C.
Regarding centrifugation steps: this depends mainly on the type of centrifuge you use. For the
initial centrifugation step, a centrifuge that starts and stops rapidly is a clear advantage. You
will have to experiment in order to get the necessary centrifugation time as short as possible.
REMEMBER: the ratio DHAA/AA will go up if you are not as fast as possible. From needle
puncture to obtaining plasma and addition of MPA, max 1-2 min.
b Urinary 8-oxodGuo, 8-oxoGuo, 8-oxoGua determination: 10mL tubes should not be filled more than 85%, or freezing pops off the top.
3.3.6 Sample requirements for partner 7 in the EUROLIVE study.
Sample Volume Nºaliquotes Cryo-color a EDTA plasma-fatty acid in LDL (FA/LDL-EDTA pl) 4.5mL 1 5 mL tube
a Isolation LDL particle by sequential flotation ultracentrifugation.: Only at the beginning and at the end of
the study (Blood collections 1 and 7). Add 45 µL of the 18mM saccharose solution to the 4.5 ml plasma
aliquot (Use 5 ml polipropilene tube with the corresponding caps) (see paragraph c of Sample Requirements
for Partner 1). Store samples at -80°C without delay.
3.3.7. Sample requirements for partner 8 in the EUROLIVE study.
Sample Volume Nº aliquotes
Cryo- color
Serum-Paroxonase (PON-s) 0.5mL 1 red a Serum-Uninduced Dienes (UnCD-s) 2.3mL 1 5mL tube
EDTA plasma-Lipid soluble antioxidants (LSA-EDTA pl) 0.5mL 1 blue
EDTA plasma-OH-FA (OHFA-EDTA pl) 1.3mL 1 blue
EDTA plasma-F2 Isoprostanes (Isoprostanes-EDTA pl) 2.3mL 2 5 mL tube
EDTA plasma-Enterolactone (Enter-EDTA pl) 2mL 1 blue
EDTA whole blood-superoxide dismut (SOD-EDTA
whole blood)
0.5mL 1 blue
a Serum for uninduced (baseline) dienes:
100 mg/ml EDTA solution preparation:
Add 10 mL of distilled water to 2,00g of EDTA, mix and adjust pH to 8.0 with 1M HCl (Without pH
adjustment, sometimes pH rises over 8, and only a part of EDTA is dissolved, then pH adjustment is carried
out to confirm dissolving of all the EDTA; However, if the pH does not rise over 8 during mixing (dissolving)
and all the EDTA is in the dissolved state, there is no need for the pH adjustment), fill with water to 20 ml.
The stability of the solution is 2 weeks.
19
Blood is allowed to clot 30-40 minutes at room temperature before centrifugation. (30 minutes is enough for
blood clotting. However, to prevent sample oxidation, the clotting time should not be over 40 minutes). After
centrifugation, EDTA is added to serum. Put exactly 23 µL of EDTA 100 mg/ml solution in a plastic tube and
add 2.3 mL of serum. The mixed EDTA containing serum is stored at -70°C without delay.
3.3.8. Shipment of samples.
The shipment of samples will be performed when a center had the complete number of samples from 5-10
volunteers. Place the frozen aliquots into pre-labeled storage boxes/bags. Put them in a box/bag with ice.
PLEASE WRITE ON BOTH BOXES/BAGS (storage and ice container): THE CENTRE, THE NAME AND
OF CONTACT PERSONS, ADDRESS, CITY, COUNTRY, PHONES, FAX AND E-MAILS.
When transferring the samples please notifiy in advance, by Fax or e-mail, that you will ship on the agreed
date. When shipping, please notify the receiver of the AWB number as soon as you get it, by Fax or e-mail.
Also, please, indicate the expected time of the arrival. It is best to ship samples on Monday to avoid delay due
to week-ends and holidays.
Toghether with the samples a Sent/Receiver Document Form (Annex 9) must be send to the Laboratory Centers
in which they will fill: data of shipment, code of sample, name of participant, observations and/or
problems during the extraction, collection, analysis, and storage of the samples. This filled document must be
included in the shipping boxes.
Samples for PARTNER 1 and 7, must be send to:
Dr Maria Isabel Covas/ Dr Montserrat Fitó/ Sra Yolanda Ferrer
Unitat de Lipids i Epidemiologia Cardiovascular (ULEC)
Institut Municipal d'Investigació Mèdica (IMIM)
Carrer Doctor Aiguader, 80
08003 Barcelona. SPAIN
Telephone: +34 93 2211009 / FAX: +34 93 2213237
E-mail: [email protected]
Samples for PARTNER 2, must be send to:
Prof. Henrik Poulsen
The Department of Clinical Pharmacology Q7642
Rigshospitalet, Copenhagen University Hospital,
20 Tagensvek,
KK-2200 Copenhagen N, DENMARK
Telephone: +45 (3545) 7671 / FAX: +45 3545 2745
E-mail: [email protected]
20
Samples for PARTNER 8, must be send to:
Dr. Jari Kaikkonen
Oy Jurilab Ltd. Neulaniementie 2L 12.
70210 Kuopio, FINLAND
Telephone: +358 (17) 4678000 / FAX: +358 (17) 467 8001
E-mail: [email protected]
3.3.9. Arrival of the samples to the partner laboratory
The Sent/Receiver Document Form (Annex 9) will be filled out by the Laboratory Centres. The following
information will be recorded: date of arrival (hour, day, month, year) and the condition of the sample. The
following codes will be used to describe the condition of sample after shipment: 00: arrived frozen and
unbroken, 01: arrived frozen, but vial is broken, 02: thawed in transit, but vial not broken, 03: thawed in
transit, and vial broken, and 04: does not exist.
Upon arrival, individual samples will be checked and deficiences with regard to volume, labeling or
temperature will be indicated to the Coordinator Centre and to the Centre of origin. Samples will be placed
immediately in the required conditions specified in the Laboratory protocol determinations. Then, the
Sent/Receiver Document Form must be filled out and sent by FAX to the sender Centre and to the
Coordinating Centre.
3.4. Data Base Management
The coordinating centre will send a draft of databases (for Clinical Trials and Laboratories) in MS Access in
order to standardize the data entry. However, if a centre prefers to use a different software this is acceptable
provided that the database structure exactly follows the sequence of variables of the official forms of the
study.
3.5. Custody of participant´s data
All the participant Centres must have Forms completed and under due custody by the Partners. Each Partner
involved in the clinical trial is responsible for the custody of the whole ensemble of each participant forms of
his/her center (i.e. basal data plus lab data).
According to standardized normatives for clinical assays in several countries, all the information from one
participant must remain available in an individualized manner (ANNEX 10). Each Laboratory partner
involved in the clinical trial will take care of the custody of this information. A copy of the laboratory data of
each participant will be sent to the corresponding Clinical Trial Centre.

21

DL1
Pr
ojec
t pro
toco
l and
M
easu
rem
ent i
nstr
umen
ts(P
1)
Indi
vidu
al d
ata
base
WP
9 (P
.1)
Cen
tralis
ed
Dat
abas
e M
anag
emen
t and
D
ata
Ana
lyse
s
WP
4 (
P3)
(P.1
,2,3
,4,5
,6 )
Clin
ical
tria
ls
DL
4 (4
.1, 4
.2,4
.3,4
.4,4
.5,4
.6)
Rep
orts
an
d D
atab
ases
(P
1,2
,3,4
,5,6
)
Del
iver
able
dat
a
D
eadl
ine
Sc
hedu
led
dat
a
Sche
dule
d d
ata
To
the
Coo
rdin
ator
:
1
Sept
200
2
1
July
200
3
To
the
EU
Com
mis
sion
: 2
5 Se
pt 2
002
25 Ju
ly 2
003
Mon
th:
9
19
Pro
ject
co
ordi
natio
n4.PR
OJE
CT
PLA
NN
ING
AN
DT
IME
TA
BL
E
Sept
200
2-Ju
ne 2
003
22
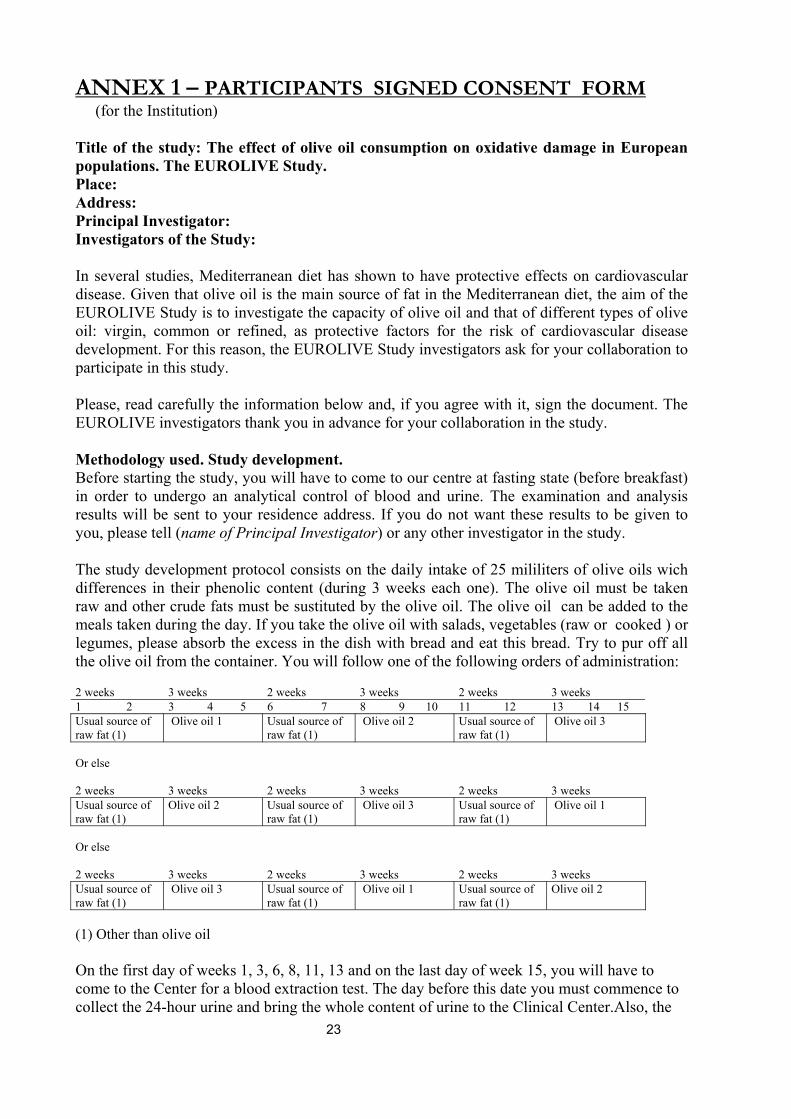
ANNEX 1 – PARTICIPANTS SIGNED CONSENT FORM (for the Institution) Title of the study: The effect of olive oil consumption on oxidative damage in European populations. The EUROLIVE Study. Place: Address: Principal Investigator: Investigators of the Study: In several studies, Mediterranean diet has shown to have protective effects on cardiovascular disease. Given that olive oil is the main source of fat in the Mediterranean diet, the aim of the EUROLIVE Study is to investigate the capacity of olive oil and that of different types of olive oil: virgin, common or refined, as protective factors for the risk of cardiovascular disease development. For this reason, the EUROLIVE Study investigators ask for your collaboration to participate in this study. Please, read carefully the information below and, if you agree with it, sign the document. The EUROLIVE investigators thank you in advance for your collaboration in the study. Methodology used. Study development. Before starting the study, you will have to come to our centre at fasting state (before breakfast) in order to undergo an analytical control of blood and urine. The examination and analysis results will be sent to your residence address. If you do not want these results to be given to you, please tell (name of Principal Investigator) or any other investigator in the study. The study development protocol consists on the daily intake of 25 mililiters of olive oils wich differences in their phenolic content (during 3 weeks each one). The olive oil must be taken raw and other crude fats must be sustituted by the olive oil. The olive oil can be added to the meals taken during the day. If you take the olive oil with salads, vegetables (raw or cooked ) or legumes, please absorb the excess in the dish with bread and eat this bread. Try to pur off all the olive oil from the container. You will follow one of the following orders of administration: 2 weeks 3 weeks 2 weeks 3 weeks 2 weeks 3 weeks 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Usual source of raw fat (1)
Olive oil 1 Usual source of raw fat (1)
Olive oil 2 Usual source of raw fat (1)
Olive oil 3
Or else
2 weeks 3 weeks 2 weeks 3 weeks 2 weeks 3 weeks Usual source of raw fat (1)
Olive oil 2 Usual source of raw fat (1)
Olive oil 3 Usual source of raw fat (1)
Olive oil 1
Or else
2 weeks 3 weeks 2 weeks 3 weeks 2 weeks 3 weeks Usual source of raw fat (1)
Olive oil 3 Usual source of raw fat (1)
Olive oil 1 Usual source of raw fat (1)
Olive oil 2
(1) Other than olive oil On the first day of weeks 1, 3, 6, 8, 11, 13 and on the last day of week 15, you will have to come to the Center for a blood extraction test. The day before this date you must commence to collect the 24-hour urine and bring the whole content of urine to the Clinical Center.Also, the 23
three days before the data of blood collection you must fill a 3-day dietary record and alcohol consumption records. On day 1 you will have to answer questionnaires of physical activity and smoking habits. Benefits and risks The benefit you will obtain from your participation in the study will be a better knowledge of your health, specially your cholesterol and other fats in blood. The study does not imply any risk for your health given that olive oil is a usual dietary product in Mediterranean countries. As for the quantity of blood obtained in each extraction, it does not exceed that collected in a routine laboratory analysis. Volunteerness Your participation in this study is voluntary so you can withdraw from it at any time. Confidentiality All the data related to your participation in this study will be considered confidential. In the working lists, it only will appear the number assigned to you in the study. In the study final report, or in case of communicating these results to the scientific community, your identity will be kept anonymous. Investigators of the study Should any doubt arise about any aspect of the study or should you wish to comment any part of this information form, please do not hesitate to inform the members of the investigating team (Name of the investigators and contact persons). You can communicate with them in a personal way (working days from X (hour) to Y (hour)) in the (Name of the Centre) (Phone: ----------) at the (Centre and adress).. At present, the research on cardiovascular diseases advances quickly and new tests to appear can be of great importance, being one of them genetic studes (DNA). If you give your consent, a part of the serum samples and DNA will remain frozen for future analysis, always related to the aim of the study, and you will always be informed if any new test needs to be undertaken. Consent After you have read this information and once we have clarified to you all the queries that may have appeared, if you decide to participate in the study, you will have to sign this “model of information”. I have read this information, I have been able to consult my queries, I understand the aims of the study and what its participation implies. ………………………………. ………………. ………… Participant Name and Surname Signature Date ………………………………. ………………. ………… Investigator Name and Surname Signature Date
24
ANNEX 1 – PARTICIPANTS SIGNED CONSENT FORM (for the participant) Title of the study: The effect of olive oil consumption on oxidative damage in European populations. The EUROLIVE Study. Place: Address: Principal Investigator: Investigators of the Study: In several studies, Mediterranean diet has shown to have protective effects on cardiovascular disease. Given that olive oil is the main source of fat in the Mediterranean diet, the aim of the EUROLIVE Study is to investigate the capacity of olive oil and that of different types of olive oil: virgin, common or refined, as protective factors for the risk of cardiovascular disease development. For this reason, the EUROLIVE Study investigators ask for your collaboration to participate in this study. Please, read carefully the information below and, if you agree with it, sign the document. The EUROLIVE investigators thank you in advance for your collaboration in the study. Methodology used. Study development. Before starting the study, you will have to come to our centre at fasting state (before breakfast) in order to undergo an analytical control of blood and urine. The examination and analysis results will be sent to your residence address. If you do not want these results to be given to you, please tell (name of Principal Investigator) or any other investigator in the study. The study development protocol consists on the daily intake of 25 mililiters of olive oils wich differences in their phenolic content (during 3 weeks each one). The olive oil must be taken raw and other crude fats must be sustituted by the olive oil. The olive oil can be added to the meals taken during the day. If you take the olive oil with salads, vegetables (raw or cooked ) or legumes, please absorb the excess in the dish with bread and eat this bread. Try to pur off all the olive oil from the container. You will follow one of the following orders of administration: 2 weeks 3 weeks 2 weeks 3 weeks 2 weeks 3 weeks 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Usual source of raw fat (1)
Olive oil 1 Usual source of raw fat (1)
Olive oil 2 Usual source of raw fat (1)
Olive oil 3
Or else
2 weeks 3 weeks 2 weeks 3 weeks 2 weeks 3 weeks Usual source of raw fat (1)
Olive oil 2 Usual source of raw fat (1)
Olive oil 3 Usual source of raw fat (1)
Olive oil 1
Or else
2 weeks 3 weeks 2 weeks 3 weeks 2 weeks 3 weeks Usual source of raw fat (1)
Olive oil 3 Usual source of raw fat (1)
Olive oil 1 Usual source of raw fat (1)
Olive oil 2
(1) Other than olive oil On the first day of weeks 1, 3, 6, 8, 11, 13 and on the last day of week 15, you will have to come to the Center for a blood extraction test. The day before this date you must commence to 25
collect the 24-hour urine and bring the whole content of urine to the Clinical Center.Also, the three days before the data of blood collection you must fill a 3-day dietary record and alcohol consumption records. On day 1 you will have to answer questionnaires of physical activity and smoking habits. Benefits and risks The benefit you will obtain from your participation in the study will be a better knowledge of your health, specially your cholesterol and other fats in blood. The study does not imply any risk for your health given that olive oil is a usual dietary product in Mediterranean countries. As for the quantity of blood obtained in each extraction, it does not exceed that collected in a routine laboratory analysis. Volunteerness Your participation in this study is voluntary so you can withdraw from it at any time. Confidentiality All the data related to your participation in this study will be considered confidential. In the working lists, it only will appear the number assigned to you in the study. In the study final report, or in case of communicating these results to the scientific community, your identity will be kept anonymous. Investigators of the study Should any doubt arise about any aspect of the study or should you wish to comment any part of this information form, please do not hesitate to inform the members of the investigating team (Name of the investigators and contact persons). You can communicate with them in a personal way (working days from X (hour) to Y (hour)) in the (Name of the Centre) (Phone: ----------) at the (Centre and adress).. At present, the research on cardiovascular diseases advances quickly and new tests to appear can be of great importance, being one of them genetic studes (DNA). If you give your consent, a part of the serum samples and DNA will remain frozen for future analysis, always related to the aim of the study, and you will always be informed if any new test needs to be undertaken. Consent After you have read this information and once we have clarified to you all the queries that may have appeared, if you decide to participate in the study, you will have to sign this “model of information”. I have read this information, I have been able to consult my queries, I understand the aims of the study and what its participation implies. ………………………………. ………………. ………… Participant Name and Surname Signature Date ………………………………. ………………. ………… Investigator Name and Surname Signature Date
26
ANNEX 1- Part B. Recommendations for the participants
Olive oil consumption
The containers must be stored in a dry, at 20-25ºC, and relatively dark place at home. Participants
must return the containers to the centre after the corresponding olive oil consumption period in
order to register the amount of olive oil consumed in this period.
The olive oil must be taken raw and other crude fats must be sustituted by the olive oil. The olive
oil can be added to the meals taken during the day. Please absorb the excessof olive oil in the dish
with bread and eat this bread. Try to pour off all the olive oil from the container.
Dietary control
To control an excessive intake of antioxidants and phenolic compounds during the clinical trial
period, participants will be allowed not to consume more than:
2 servings of vegetables or pulses/day
3 servings of fruits (this includes juices)
3 cups of tea or coffee/day
2 pieces of a bar of chocolate
2 glasses of red wine
<1 liter of beer
24 hours urine collection
On day 1 discard the first morning urine. Collect all the urine during this day, using an appropiate
container, and include the first morning urine of day 2.
27
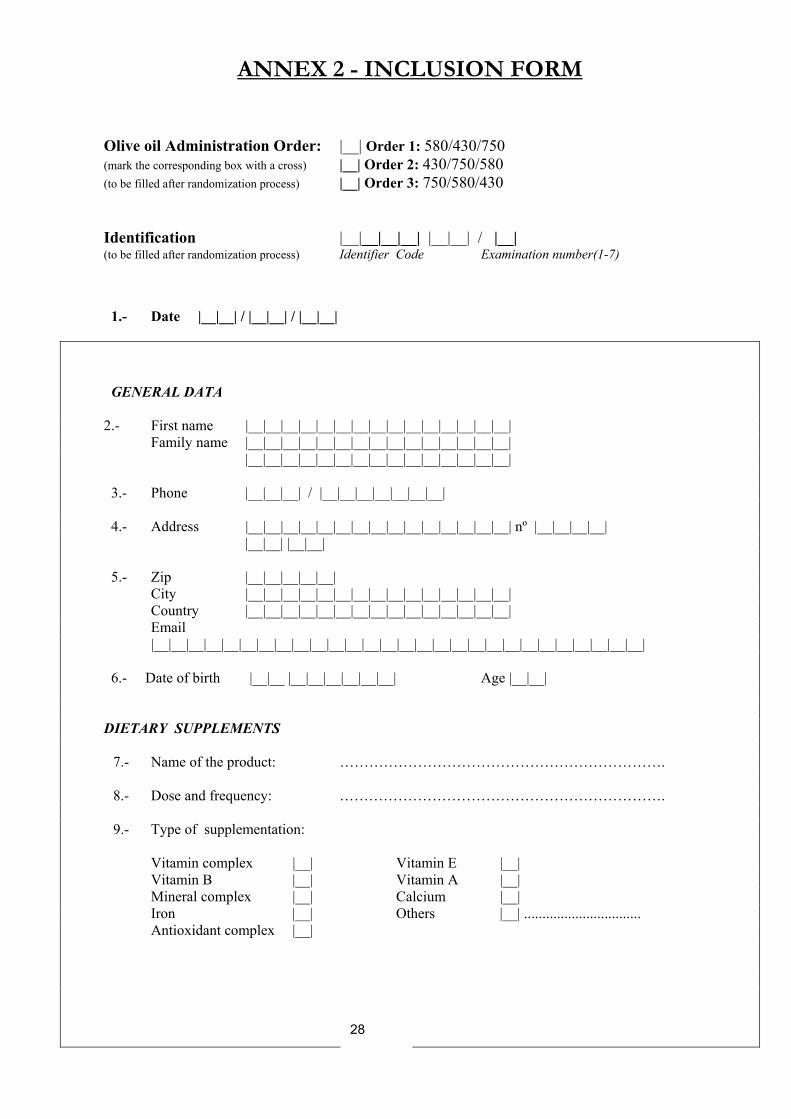
ANNEX 2 - INCLUSION FORM Olive oil Administration Order: |__| Order 1: 580/430/750 (mark the corresponding box with a cross) |__| Order 2: 430/750/580 (to be filled after randomization process) |__| Order 3: 750/580/430
Identification |__|__|__|__| |__|__| / |__| (to be filled after randomization process) Identifier Code Examination number(1-7)
1.- Date |__|__| / |__|__| / |__|__|
GENERAL DATA 2.- First name |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| Family name |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| 3.- Phone |__|__|__| / |__|__|__|__|__|__|__| 4.- Address |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| nº |__|__|__|__| |__|__| |__|__| 5.- Zip |__|__|__|__|__| City |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| Country |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| Email |__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__|__| 6.- Date of birth |__|__ |__|__|__|__|__|__| Age |__|__| DIETARY SUPPLEMENTS
7.- Name of the product: ………………………………………………………….
8.- Dose and frequency: …………………………………………………………. 9.- Type of supplementation: Vitamin complex |__| Vitamin E |__| Vitamin B |__| Vitamin A |__| Mineral complex |__| Calcium |__| Iron |__| Others |__| ................................ Antioxidant complex |__|
28
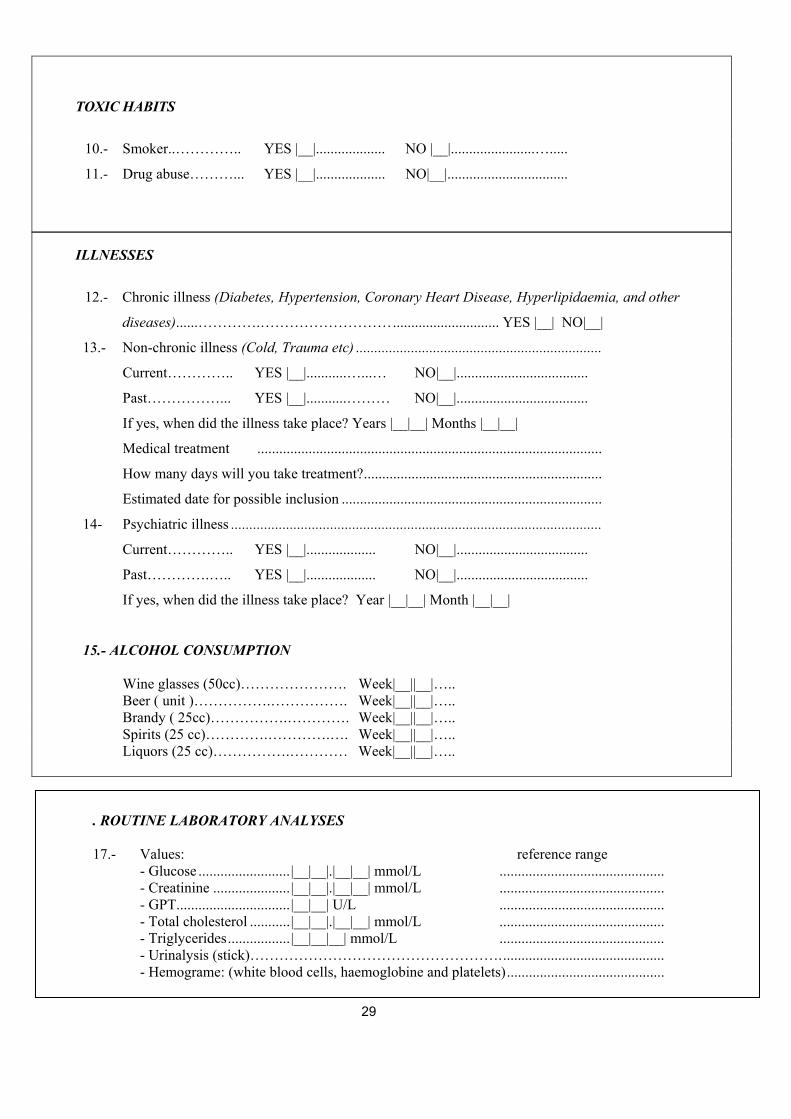
TOXIC HABITS
10.- Smoker..………….. YES |__|................... NO |__|.......................….....
11.- Drug abuse………... YES |__|................... NO|__|.................................
ILLNESSES
12.- Chronic illness (Diabetes, Hypertension, Coronary Heart Disease, Hyperlipidaemia, and other
diseases)......………….………………………............................. YES |__| NO|__|
13.- Non-chronic illness (Cold, Trauma etc) ...................................................................
Current………….. YES |__|...........…...… NO|__|....................................
Past……………... YES |__|...........……… NO|__|....................................
If yes, when did the illness take place? Years |__|__| Months |__|__|
Medical treatment ..............................................................................................
How many days will you take treatment?.................................................................
Estimated date for possible inclusion .......................................................................
14- Psychiatric illness .....................................................................................................
Current………….. YES |__|................... NO|__|....................................
Past………….….. YES |__|................... NO|__|....................................
If yes, when did the illness take place? Year |__|__| Month |__|__|
15.- ALCOHOL CONSUMPTION Wine glasses (50cc)…………………. Week|__||__|….. Beer ( unit )…………….……………. Week|__||__|….. Brandy ( 25cc)…………….…………. Week|__||__|….. Spirits (25 cc)………….………….…. Week|__||__|….. Liquors (25 cc)…………….………… Week|__||__|….. If the volunteer meet the inclusion criteria, routine laboratory analysis will be ordered:
. ROUTINE LABORATORY ANALYSES 17.- Values: reference range - Glucose .........................|__|__|.|__|__| mmol/L ............................................. - Creatinine .....................|__|__|.|__|__| mmol/L ............................................. - GPT...............................|__|__| U/L .............................................
- Total cholesterol ...........|__|__|.|__|__| mmol/L ............................................. - Triglycerides.................|__|__|__| mmol/L ............................................. - Urinalysis (stick)…………………………………………….............................................
- Hemograme: (white blood cells, haemoglobine and platelets)...........................................
29
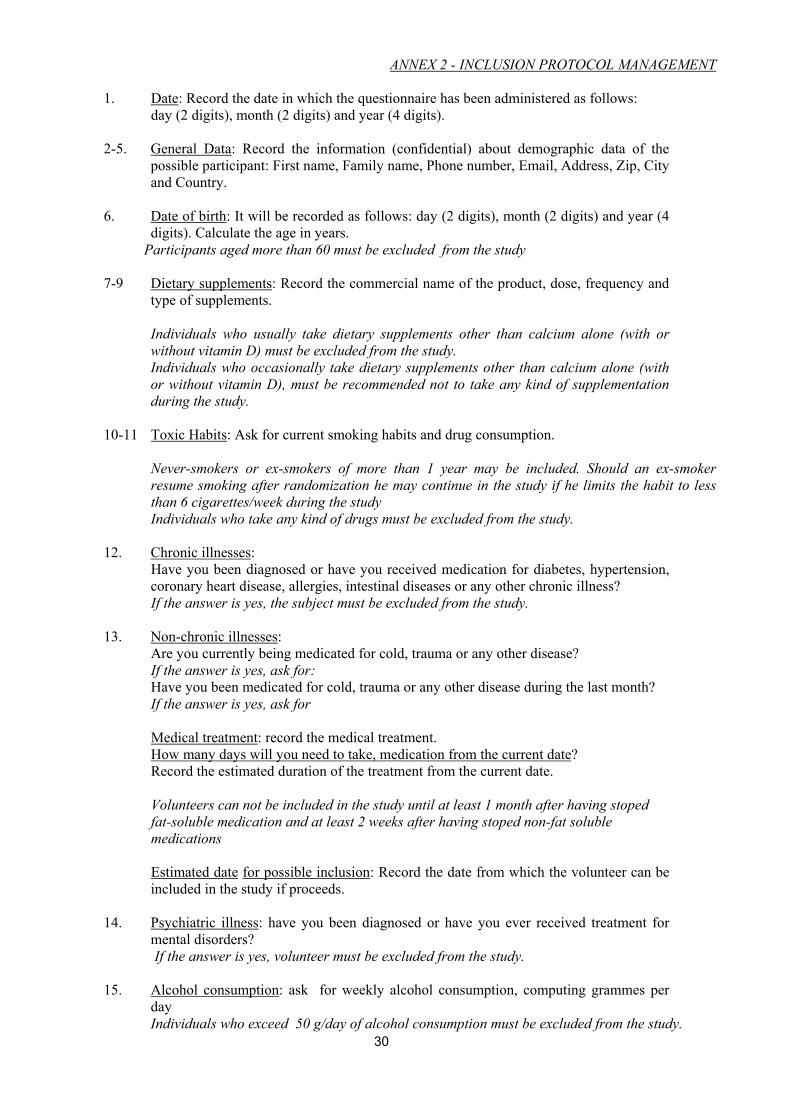
ANNEX 2 - INCLUSION PROTOCOL MANAGEMENT 1. Date: Record the date in which the questionnaire has been administered as follows: day (2 digits), month (2 digits) and year (4 digits). 2-5. General Data: Record the information (confidential) about demographic data of the
possible participant: First name, Family name, Phone number, Email, Address, Zip, City and Country.
6. Date of birth: It will be recorded as follows: day (2 digits), month (2 digits) and year (4
digits). Calculate the age in years. Participants aged more than 60 must be excluded from the study 7-9 Dietary supplements: Record the commercial name of the product, dose, frequency and
type of supplements. Individuals who usually take dietary supplements other than calcium alone (with or without vitamin D) must be excluded from the study. Individuals who occasionally take dietary supplements other than calcium alone (with or without vitamin D), must be recommended not to take any kind of supplementation during the study.
10-11 Toxic Habits: Ask for current smoking habits and drug consumption. Never-smokers or ex-smokers of more than 1 year may be included. Should an ex-smoker resume smoking after randomization he may continue in the study if he limits the habit to less than 6 cigarettes/week during the study Individuals who take any kind of drugs must be excluded from the study.
12. Chronic illnesses: Have you been diagnosed or have you received medication for diabetes, hypertension, coronary heart disease, allergies, intestinal diseases or any other chronic illness?
If the answer is yes, the subject must be excluded from the study.
13. Non-chronic illnesses: Are you currently being medicated for cold, trauma or any other disease? If the answer is yes, ask for: Have you been medicated for cold, trauma or any other disease during the last month? If the answer is yes, ask for
Medical treatment: record the medical treatment. How many days will you need to take, medication from the current date?
Record the estimated duration of the treatment from the current date. Volunteers can not be included in the study until at least 1 month after having stoped fat-soluble medication and at least 2 weeks after having stoped non-fat soluble medications Estimated date for possible inclusion: Record the date from which the volunteer can be included in the study if proceeds.
14. Psychiatric illness: have you been diagnosed or have you ever received treatment for
mental disorders? If the answer is yes, volunteer must be excluded from the study. 15. Alcohol consumption: ask for weekly alcohol consumption, computing grammes per
day Individuals who exceed 50 g/day of alcohol consumption must be excluded from the study.
30
2nd Letter 1st Surname**
1* Letter 1st Name*
1st Letter 1st Surname**
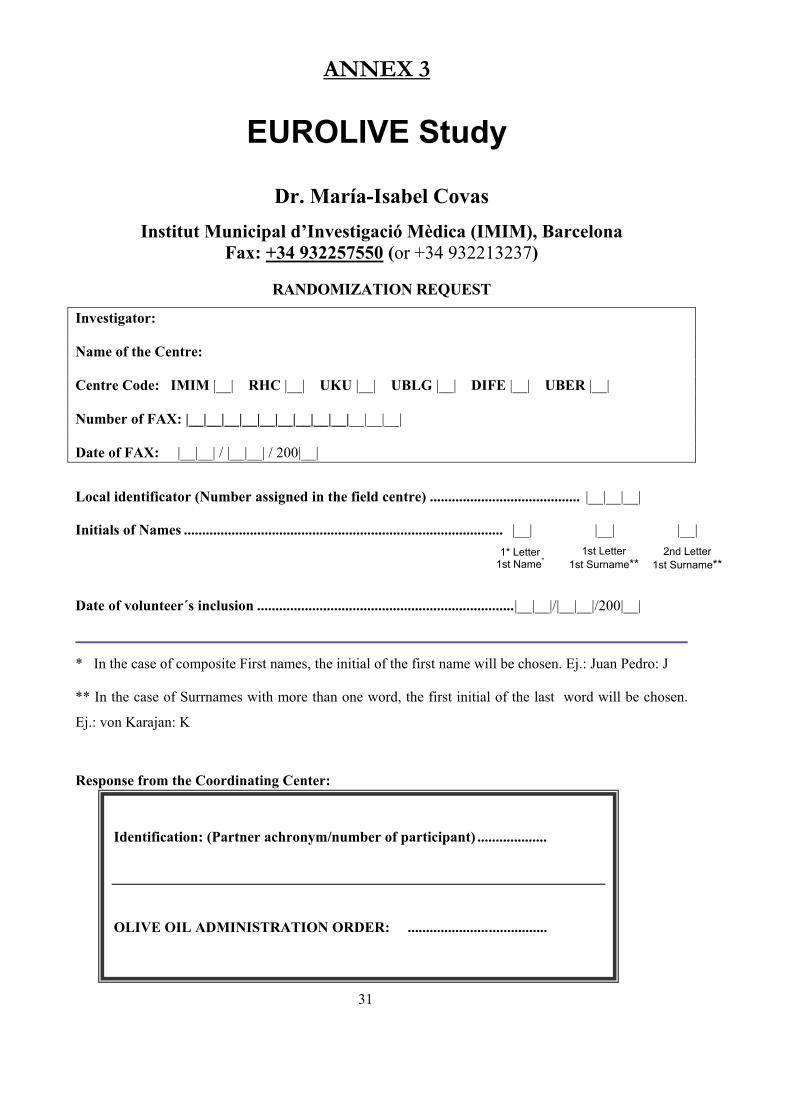
ANNEX 3
EUROLIVE Study
Dr. María-Isabel Covas Institut Municipal d’Investigació Mèdica (IMIM), Barcelona
Fax: +34 932257550 (or +34 932213237)
RANDOMIZATION REQUEST
Investigator: Name of the Centre: Centre Code: IMIM |__| RHC |__| UKU |__| UBLG |__| DIFE |__| UBER |__| Number of FAX: |__|__|__|__|__|__|__|__|__|__|__|__| Date of FAX: |__|__| / |__|__| / 200|__|
Local identificator (Number assigned in the field centre) ......................................... |__|__|__|
Initials of Names ....................................................................................... |__| |__| |__|
Date of volunteer´s inclusion ......................................................................|__|__|/|__|__|/200|__|
* In the case of composite First names, the initial of the first name will be chosen. Ej.: Juan Pedro: J
** In the case of Surrnames with more than one word, the first initial of the last word will be chosen.
Ej.: von Karajan: K
Response from the Coordinating Center:
31
Identification: (Partner achronym/number of participant) ................... OLIVE OIL ADMINISTRATION ORDER: ......................................
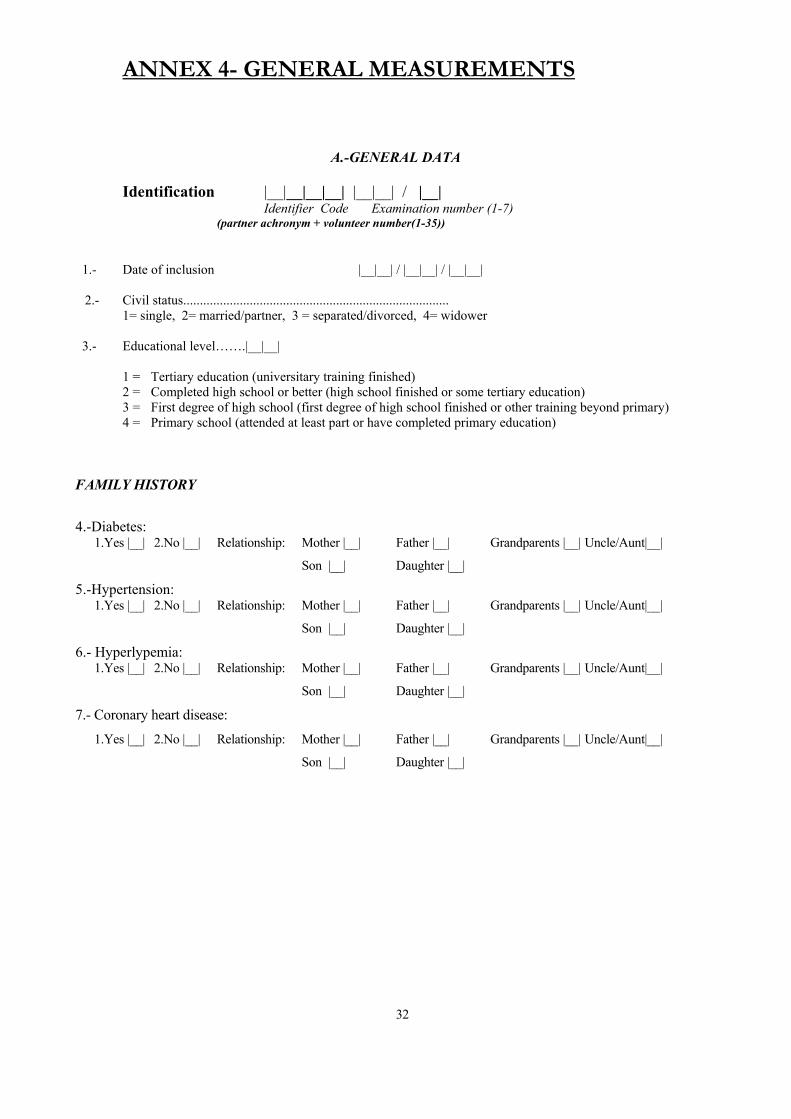
ANNEX 4- GENERAL MEASUREMENTS
A.-GENERAL DATA
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number (1-7) (partner achronym + volunteer number(1-35))
1.- Date of inclusion |__|__| / |__|__| / |__|__| 2.- Civil status................................................................................ 1= single, 2= married/partner, 3 = separated/divorced, 4= widower 3.- Educational level…….|__|__| 1 = Tertiary education (universitary training finished) 2 = Completed high school or better (high school finished or some tertiary education) 3 = First degree of high school (first degree of high school finished or other training beyond primary) 4 = Primary school (attended at least part or have completed primary education) FAMILY HISTORY
4.-Diabetes: 1.Yes |__| 2.No |__| Relationship: Mother |__| Father |__| Grandparents |__| Uncle/Aunt|__|
Son |__| Daughter |__|
5.-Hypertension: 1.Yes |__| 2.No |__| Relationship: Mother |__| Father |__| Grandparents |__| Uncle/Aunt|__|
Son |__| Daughter |__|
6.- Hyperlypemia: 1.Yes |__| 2.No |__| Relationship: Mother |__| Father |__| Grandparents |__| Uncle/Aunt|__|
Son |__| Daughter |__|
7.- Coronary heart disease: 1.Yes |__| 2.No |__| Relationship: Mother |__| Father |__| Grandparents |__| Uncle/Aunt|__|
Son |__| Daughter |__|
32

ANNEX 4- GENERAL MEASUREMENTS (2)
B. ANTHROPOMETRIC AND BLOOD PRESSURE MEASUREMENTS
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number(1-7) (partner achronym + volunteer number(1-35))
Date |__|__| / |__|__| / |__|__| 1.- Height (cm)…………….|__|__|__| 2.- Waist/Hip ratio )……………..|__|__|__| 3.- Weight ( kg. ) |__|__|.|__| |__|__|.|__| |__|__|.|__| |__|__|.|__| |__|__|.|__| |__|__|.|__| |__|__|.|__| 1st exam 2nd exam 3rd exam 4th exam 5th exam 6th exam 7th exam 4.- Systolic blood pressure |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| Diastolic blood pressure |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| / |__|__|__| 1st exam 2nd exam 3rd exam 4th exam 5th exam 6th exam 7th exam 33
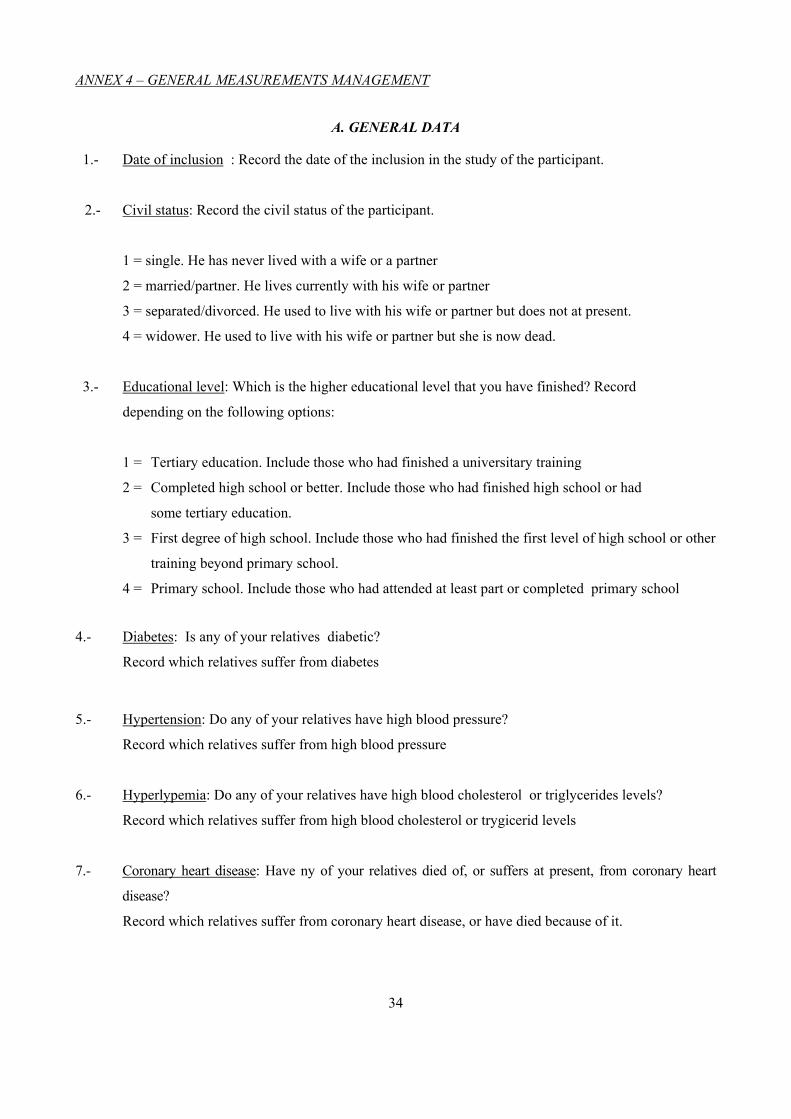
ANNEX 4 – GENERAL MEASUREMENTS MANAGEMENT
A. GENERAL DATA 1.- Date of inclusion : Record the date of the inclusion in the study of the participant.
2.- Civil status: Record the civil status of the participant.
1 = single. He has never lived with a wife or a partner
2 = married/partner. He lives currently with his wife or partner
3 = separated/divorced. He used to live with his wife or partner but does not at present.
4 = widower. He used to live with his wife or partner but she is now dead.
3.- Educational level: Which is the higher educational level that you have finished? Record
depending on the following options:
1 = Tertiary education. Include those who had finished a universitary training
2 = Completed high school or better. Include those who had finished high school or had
some tertiary education.
3 = First degree of high school. Include those who had finished the first level of high school or other
training beyond primary school.
4 = Primary school. Include those who had attended at least part or completed primary school
4.- Diabetes: Is any of your relatives diabetic?
Record which relatives suffer from diabetes
5.- Hypertension: Do any of your relatives have high blood pressure?
Record which relatives suffer from high blood pressure
6.- Hyperlypemia: Do any of your relatives have high blood cholesterol or triglycerides levels?
Record which relatives suffer from high blood cholesterol or trygicerid levels
7.- Coronary heart disease: Have ny of your relatives died of, or suffers at present, from coronary heart
disease?
Record which relatives suffer from coronary heart disease, or have died because of it.
34
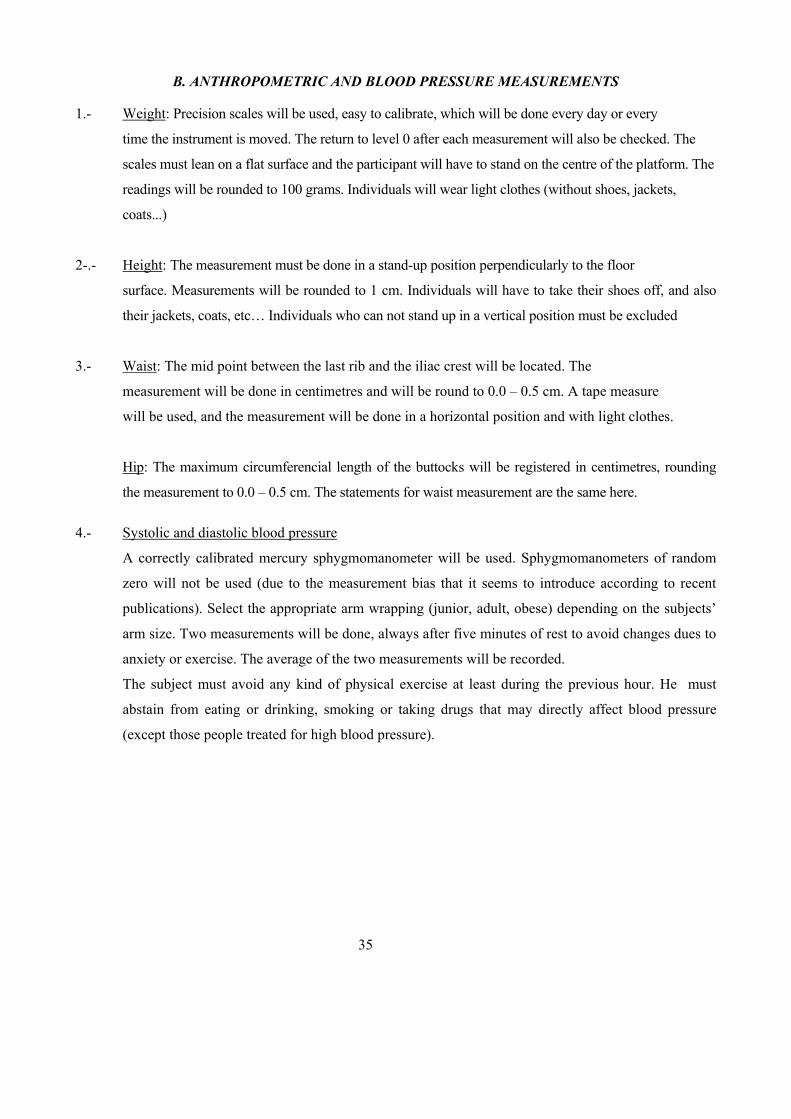
B. ANTHROPOMETRIC AND BLOOD PRESSURE MEASUREMENTS
1.- Weight: Precision scales will be used, easy to calibrate, which will be done every day or every
time the instrument is moved. The return to level 0 after each measurement will also be checked. The
scales must lean on a flat surface and the participant will have to stand on the centre of the platform. The
readings will be rounded to 100 grams. Individuals will wear light clothes (without shoes, jackets,
coats...)
2-.- Height: The measurement must be done in a stand-up position perpendicularly to the floor
surface. Measurements will be rounded to 1 cm. Individuals will have to take their shoes off, and also
their jackets, coats, etc… Individuals who can not stand up in a vertical position must be excluded
3.- Waist: The mid point between the last rib and the iliac crest will be located. The
measurement will be done in centimetres and will be round to 0.0 – 0.5 cm. A tape measure
will be used, and the measurement will be done in a horizontal position and with light clothes.
Hip: The maximum circumferencial length of the buttocks will be registered in centimetres, rounding
the measurement to 0.0 – 0.5 cm. The statements for waist measurement are the same here. 4.- Systolic and diastolic blood pressure
A correctly calibrated mercury sphygmomanometer will be used. Sphygmomanometers of random
zero will not be used (due to the measurement bias that it seems to introduce according to recent
publications). Select the appropriate arm wrapping (junior, adult, obese) depending on the subjects’
arm size. Two measurements will be done, always after five minutes of rest to avoid changes dues to
anxiety or exercise. The average of the two measurements will be recorded.
The subject must avoid any kind of physical exercise at least during the previous hour. He must
abstain from eating or drinking, smoking or taking drugs that may directly affect blood pressure
(except those people treated for high blood pressure).
35
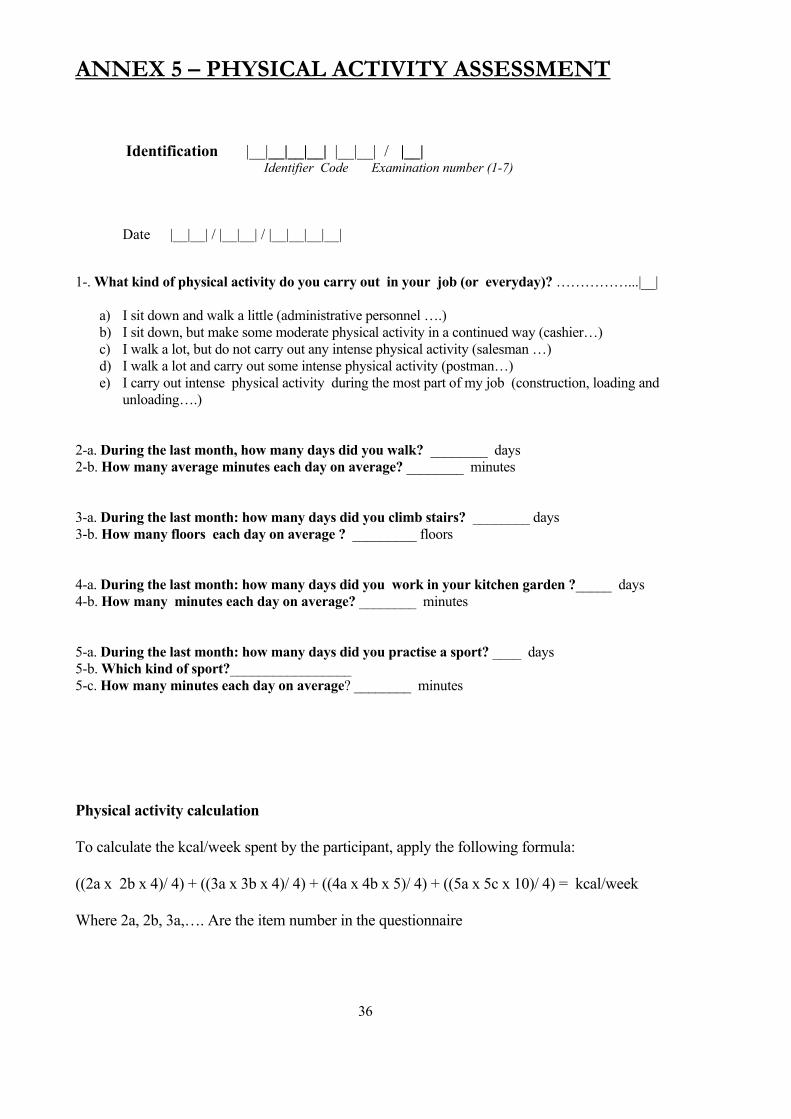
ANNEX 5 – PHYSICAL ACTIVITY ASSESSMENT
Identification |__|__|__|__| |__|__| / |__| Identifier Code Examination number (1-7)
Date |__|__| / |__|__| / |__|__|__|__| 1-. What kind of physical activity do you carry out in your job (or everyday)? ……………...|__|
a) I sit down and walk a little (administrative personnel ….) b) I sit down, but make some moderate physical activity in a continued way (cashier…) c) I walk a lot, but do not carry out any intense physical activity (salesman …) d) I walk a lot and carry out some intense physical activity (postman…) e) I carry out intense physical activity during the most part of my job (construction, loading and
unloading….)
2-a. During the last month, how many days did you walk? ________ days 2-b. How many average minutes each day on average? ________ minutes 3-a. During the last month: how many days did you climb stairs? ________ days 3-b. How many floors each day on average ? _________ floors 4-a. During the last month: how many days did you work in your kitchen garden ?_____ days 4-b. How many minutes each day on average? ________ minutes 5-a. During the last month: how many days did you practise a sport? ____ days 5-b. Which kind of sport?_________________ 5-c. How many minutes each day on average? ________ minutes Physical activity calculation To calculate the kcal/week spent by the participant, apply the following formula: ((2a x 2b x 4)/ 4) + ((3a x 3b x 4)/ 4) + ((4a x 4b x 5)/ 4) + ((5a x 5c x 10)/ 4) = kcal/week Where 2a, 2b, 3a,…. Are the item number in the questionnaire 36

ANNEX 6 3-DAY DIETARY RECORD. Day 1 Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number (1-7)
Date |__|__| / |__|__| / |__|__| BREAKFAST Type of food or beverage
Amount of consumption (in household measurements)
Dish preparation and meat/fish processing.
SNACK LUNCH SNACK DINNER
37
ANNEX 6 3-DAY DIETARY RECORD. Day 2
Identification |__|__|__|__| |__|__| / |__| Identifier Code Examination number (1-7)
Date |__|__| / |__|__| / |__|__|__|__| BREAKFAST Type of food or beverage
Amount of consumption (in household measurements)
Dish preparation and meat/fish processing.
SNACK LUNCH SNACK DINNER
38
ANNEX 6 3-DAY DIETARY RECORD. Day 3
Identification |__|__|__|__| |__|__| / |__| Identifier Code Examination number (1-7)
Date |__|__| / |__|__| / |__|__|__|__| BREAKFAST Type of food or beverage
Amount of consumption (in household measurements)
Dish preparation and meat/fish processing.
SNACK LUNCH SNACK DINNER 39
ANNEX 7 ALCOHOL CONSUMPTION QUESTIONNAIRE
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number (1-7) Date |__|__| / |__|__| / |__|__|__|__|
Wine glasses (100 cc) Red wine Young (of the year) ...................................................................................... |__| Old.................................................................................................................. |__| White wine .................................................................................................................. |__| Rosé wine..................................................................................................................... |__| Sparkling wine............................................................................................................ |__| Dessert wine (50cc)* Beer units (500 cc ?large’)…………………………………………………………………|__| Beer units (330 cc: "middle")................................................................................................. |__| Beer units (125 cc: "little") ..................................................................................................... |__| Cups of licor (50cc)* ................................................................................................................ |__| Destilates (whisky, vodka, brandy) (50 cc)* ..................................................................................................................................................... |__| ..................................................................................................................................................... |__| ..................................................................................................................................................... |__| Long drinks (rum with coke, gin and tonic… 25-50cc liquor) .......................................... |__| Others _____________________________________........................................................... |__| * Change units according to the local standard measures of beverages 40
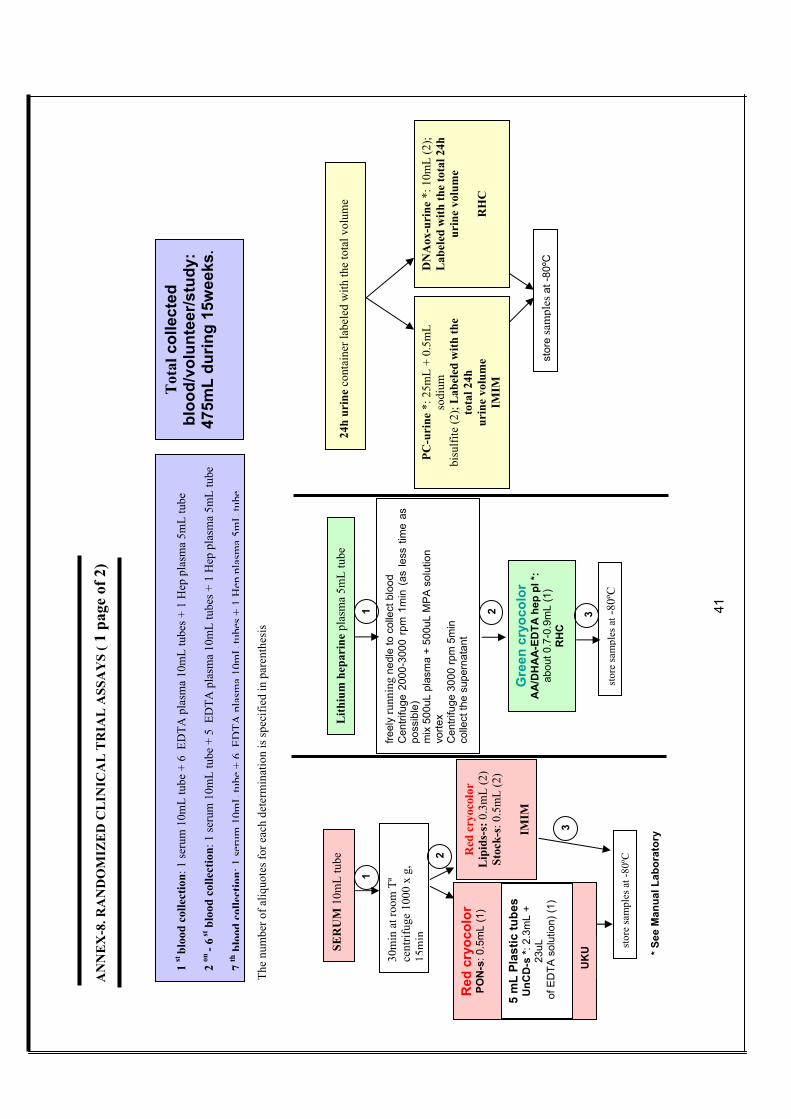
1 st
bloo
d co
llect
ion:
1 se
rum
10m
L tu
be +
6 E
DTA
pla
sma
10m
L tu
bes +
1 H
ep p
lasm
a 5m
L tu
be
2 on
- 6 st
blo
od c
olle
ctio
n: 1
seru
m 1
0mL
tube
+ 5
ED
TA p
lasm
a 10
mL
tube
s + 1
Hep
pla
sma
5mL
tube
7
thbl
ood
colle
ctio
n:1
seru
m10
mL
tube
+6
EDTA
plas
ma
10m
Ltu
bes+
1H
eppl
asm
a5m
Ltu
be
30m
in a
t roo
m T
ª ce
ntrif
uge
1000
x g
, 15
min
SER
UM
10m
L tu
be
stor
e sa
mpl
es a
t -80
ºC Red
cry
ocol
or
Lip
ids-
s: 0
.3m
L (2
)St
ock-
s: 0
.5m
L (2
)
IMIM
Red
cry
ocol
or
PON
-s: 0
.5m
L (1
)
1
2
3
Lith
ium
hep
arin
e pl
asm
a 5m
L tu
be
freel
y ru
nnin
g ne
dle
to c
olle
ct b
lood
C
entri
fuge
200
0-30
00 r
pm 1
min
(as
less
tim
e as
po
ssib
le)
mix
500
uL p
lasm
a +
500u
L M
PA
sol
utio
n vo
rtex
Cen
trifu
ge 3
000
rpm
5m
in
colle
ct th
e su
pern
atan
t
1 2
* See
Man
ual L
abor
ator
y
AN
NE
X-8
. RA
ND
OM
IZE
D C
LIN
ICA
L T
RIA
L A
SSA
YS
( 1 p
age
of 2
)
24h
urin
e co
ntai
ner l
abel
ed w
ith th
e to
tal v
olum
e
PC-u
rine
*: 2
5mL
+ 0.
5mL
sodi
um
bisu
lfite
(2);
Lab
eled
with
the
tota
l 24h
ur
ine
volu
me
IMIM
DN
Aox
-uri
ne *
: 10m
L (2
);
Lab
eled
with
the
tota
l 24h
ur
ine
volu
me
R
HC
stor
e sa
mpl
esat
-80º
C
3
Gre
en c
ryoc
olor
A
A/D
HA
A-E
DTA
hep
pl *
: ab
out 0
.7-0
.9m
L (1
) R
HC
stor
e sa
mpl
es a
t-80
ºC
The
num
ber o
f aliq
uote
s for
eac
h de
term
inat
ion
is sp
ecifi
ed in
par
enth
esis
Tot
al c
olle
cted
bl
ood/
volu
ntee
r/stu
dy:
475m
L du
ring
15w
eeks
.
5 m
L Pl
astic
tube
sU
nCD
-s *:
2.3
mL
+ 23
uL
of E
DTA
sol
utio
n) (1
)
UK
U
41
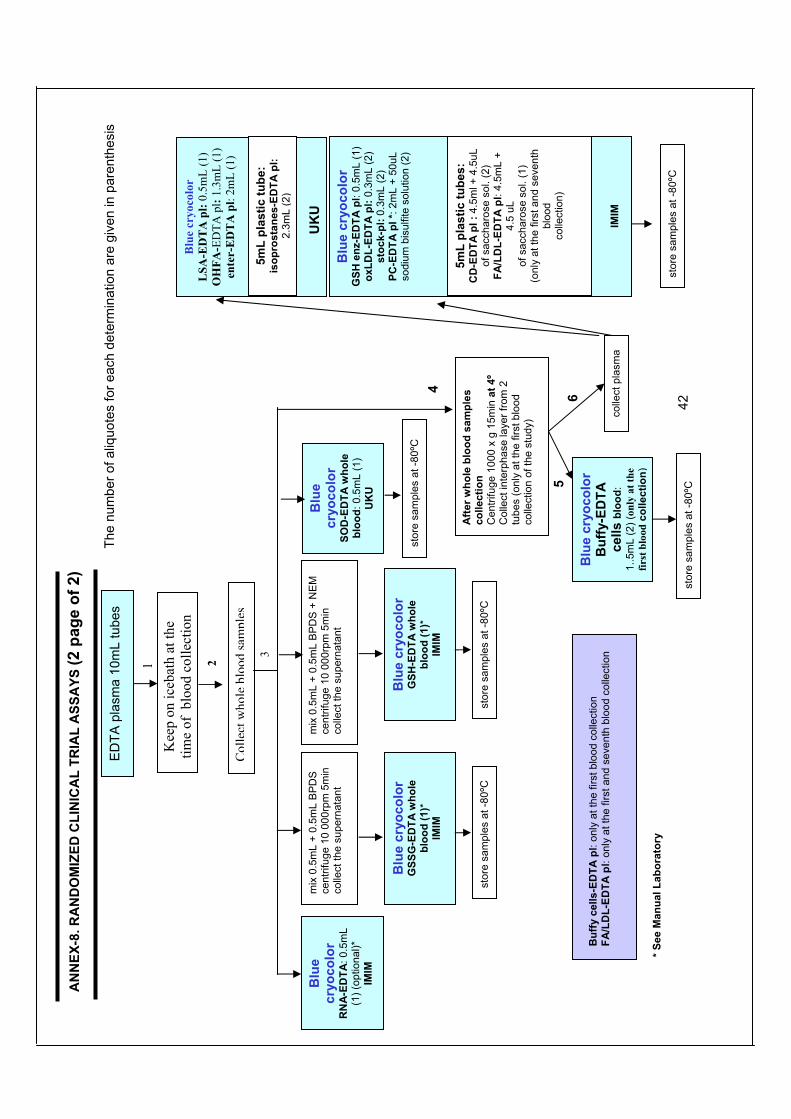
Afte
r who
le b
lood
sam
ples
co
llect
ion
Cen
trifu
ge 1
000
x g
15m
in a
t 4º
Col
lect
inte
rpha
se la
yer f
rom
2
tube
s (o
nly
at th
e fir
st b
lood
co
llect
ion
of th
e st
udy)
Blu
e cr
yoco
lor
Buf
fy-E
DTA
ce
lls b
lood
: 1.
.5m
L (2
) (on
ly a
t the
fir
st b
lood
colle
ctio
n)
colle
ct p
lasm
a
Blu
e cr
yoco
lor
SOD
-ED
TA w
hole
bl
ood:
0.5
mL
(1)
UK
U
stor
e sa
mpl
es a
t -80
ºC
Blu
e cr
yoco
lor
GSS
G-E
DTA
who
le
bloo
d (1
)*
IMIM
mix
0.5
mL
+ 0.
5mL
BP
DS
+ N
EM
ce
ntrif
uge
10 0
00rp
m 5
min
co
llect
the
supe
rnat
ant
Blu
e cr
yoco
lor
GSH
-ED
TA w
hole
bl
ood
(1)*
IM
IM
stor
e sa
mpl
es a
t -80
ºC
stor
e sa
mpl
es a
t -80
ºC
ED
TA p
lasm
a 10
mL
tube
s
Col
lect
who
lebl
ood
sam
ples
* S
ee M
anua
l Lab
orat
ory
stor
e sa
mpl
es a
t -80
ºC
stor
e sa
mpl
es a
t -80
ºC
Buf
fy c
ells
-ED
TA p
l: on
ly a
t the
firs
t blo
od c
olle
ctio
n FA
/LD
L-ED
TA p
l: on
ly a
t the
firs
t and
sev
enth
blo
od c
olle
ctio
n
Blu
e cr
yoco
lor
RN
A-E
DTA
: 0.5
mL
(1) (
optio
nal)*
IM
IM
mix
0.5
mL
+ 0.
5mL
BP
DS
ce
ntrif
uge
10 0
00rp
m 5
min
co
llect
the
supe
rnat
ant
Kee
p on
iceb
ath
at th
e tim
e of
blo
od c
olle
ctio
n
AN
NEX
-8. R
AN
DO
MIZ
ED C
LIN
ICA
L TR
IAL
ASS
AYS
(2 p
age
of 2
)
The
num
ber o
f aliq
uote
s fo
r eac
h de
term
inat
ion
are
give
n in
par
enth
esis
1 2
3
4
5 6
Blu
e cr
yoco
lor
GSH
enz
-ED
TA p
l: 0.
5mL
(1)
oxLD
L-ED
TA p
l: 0.
3mL
(2)
stoc
k-pl
: 0.3
mL
(2)
PC-E
DTA
pl *
: 2m
L +
50uL
so
dium
bis
ulfit
e so
lutio
n (2
)
Blu
e cr
yoco
lor
LSA
-ED
TA
pl:
0.5m
L (1
) O
HFA
-ED
TA p
l: 1.
3mL
(1)
ente
r-E
DT
A p
l: 2m
L (1
)
IMIM
5mL
plas
tic tu
be:
isop
rost
anes
-ED
TA p
l: 2.
3mL
(2)
5mL
plas
tic tu
bes:
C
D-E
DTA
pl :
4.5
ml +
4.5
uL
of s
acch
aros
e so
l. (2
) FA
/LD
L-ED
TA p
l: 4.
5mL
+ 4.
5 uL
of
sac
char
ose
sol.
(1)
(onl
y at
the
first
and
sev
enth
bl
ood
co
llect
ion)
UK
U
42
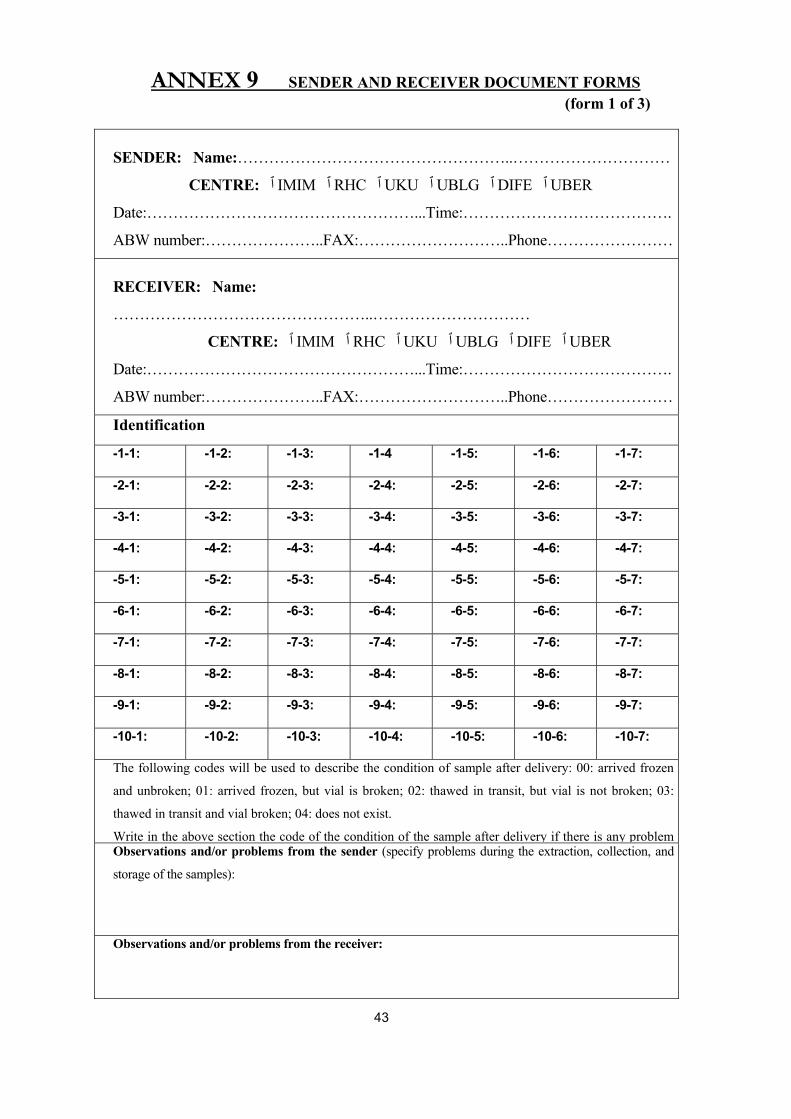
ANNEX 9 SENDER AND RECEIVER DOCUMENT FORMS (form 1 of 3)
SENDER: Name:……………………………………………..…………………………
CENTRE: ٱ IMIM ٱ RHC ٱ UKU ٱ UBLG ٱ DIFE ٱ UBER
Date:……………………………………………...Time:………………………………….
ABW number:…………………..FAX:………………………..Phone……………………
RECEIVER: Name:
…………………………………………..…………………………
CENTRE: ٱ IMIM ٱ RHC ٱ UKU ٱ UBLG ٱ DIFE ٱ UBER
Date:……………………………………………...Time:………………………………….
ABW number:…………………..FAX:………………………..Phone……………………
Identification
-1-1: -1-2: -1-3: -1-4 -1-5: -1-6: -1-7:
-2-1: -2-2: -2-3: -2-4: -2-5: -2-6: -2-7:
-3-1: -3-2: -3-3: -3-4: -3-5: -3-6: -3-7:
-4-1: -4-2: -4-3: -4-4: -4-5: -4-6: -4-7:
-5-1: -5-2: -5-3: -5-4: -5-5: -5-6: -5-7:
-6-1: -6-2: -6-3: -6-4: -6-5: -6-6: -6-7:
-7-1: -7-2: -7-3: -7-4: -7-5: -7-6: -7-7:
-8-1: -8-2: -8-3: -8-4: -8-5: -8-6: -8-7:
-9-1: -9-2: -9-3: -9-4: -9-5: -9-6: -9-7:
-10-1: -10-2: -10-3: -10-4: -10-5: -10-6: -10-7:
The following codes will be used to describe the condition of sample after delivery: 00: arrived frozen
and unbroken; 01: arrived frozen, but vial is broken; 02: thawed in transit, but vial is not broken; 03:
thawed in transit and vial broken; 04: does not exist.
Write in the above section the code of the condition of the sample after delivery if there is any problem Observations and/or problems from the sender (specify problems during the extraction, collection, and
storage of the samples):
Observations and/or problems from the receiver:
43
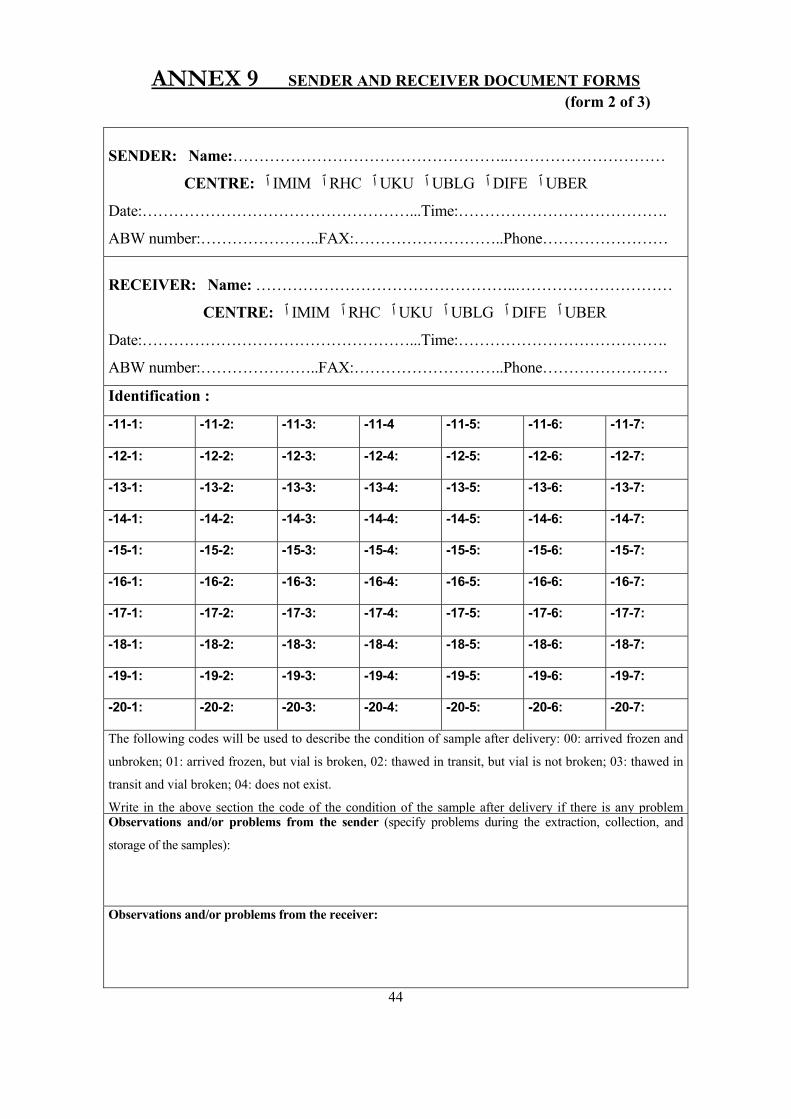
ANNEX 9 SENDER AND RECEIVER DOCUMENT FORMS (form 2 of 3)
SENDER: Name:……………………………………………..…………………………
CENTRE: ٱ IMIM ٱ RHC ٱ UKU ٱ UBLG ٱ DIFE ٱ UBER
Date:……………………………………………...Time:………………………………….
ABW number:…………………..FAX:………………………..Phone……………………
RECEIVER: Name: …………………………………………..…………………………
CENTRE: ٱ IMIM ٱ RHC ٱ UKU ٱ UBLG ٱ DIFE ٱ UBER
Date:……………………………………………...Time:………………………………….
ABW number:…………………..FAX:………………………..Phone……………………
Identification :
-11-1: -11-2: -11-3: -11-4 -11-5: -11-6: -11-7:
-12-1: -12-2: -12-3: -12-4: -12-5: -12-6: -12-7:
-13-1: -13-2: -13-3: -13-4: -13-5: -13-6: -13-7:
-14-1: -14-2: -14-3: -14-4: -14-5: -14-6: -14-7:
-15-1: -15-2: -15-3: -15-4: -15-5: -15-6: -15-7:
-16-1: -16-2: -16-3: -16-4: -16-5: -16-6: -16-7:
-17-1: -17-2: -17-3: -17-4: -17-5: -17-6: -17-7:
-18-1: -18-2: -18-3: -18-4: -18-5: -18-6: -18-7:
-19-1: -19-2: -19-3: -19-4: -19-5: -19-6: -19-7:
-20-1: -20-2: -20-3: -20-4: -20-5: -20-6: -20-7:
The following codes will be used to describe the condition of sample after delivery: 00: arrived frozen and
unbroken; 01: arrived frozen, but vial is broken, 02: thawed in transit, but vial is not broken; 03: thawed in
transit and vial broken; 04: does not exist.
Write in the above section the code of the condition of the sample after delivery if there is any problem Observations and/or problems from the sender (specify problems during the extraction, collection, and
storage of the samples):
Observations and/or problems from the receiver:
44
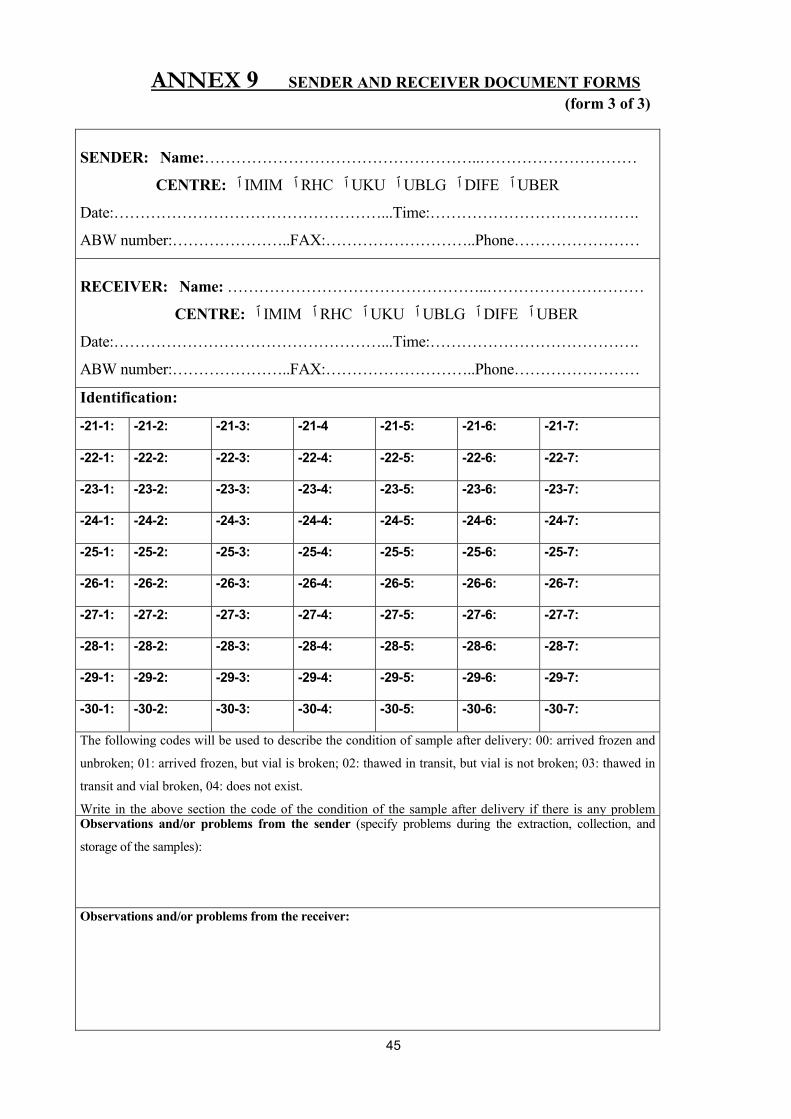
ANNEX 9 SENDER AND RECEIVER DOCUMENT FORMS (form 3 of 3)
SENDER: Name:……………………………………………..…………………………
CENTRE: ٱ IMIM ٱ RHC ٱ UKU ٱ UBLG ٱ DIFE ٱ UBER
Date:……………………………………………...Time:………………………………….
ABW number:…………………..FAX:………………………..Phone……………………
RECEIVER: Name: …………………………………………..…………………………
CENTRE: ٱ IMIM ٱ RHC ٱ UKU ٱ UBLG ٱ DIFE ٱ UBER
Date:……………………………………………...Time:………………………………….
ABW number:…………………..FAX:………………………..Phone……………………
Identification:
-21-1: -21-2: -21-3: -21-4 -21-5: -21-6: -21-7:
-22-1: -22-2: -22-3: -22-4: -22-5: -22-6: -22-7:
-23-1: -23-2: -23-3: -23-4: -23-5: -23-6: -23-7:
-24-1: -24-2: -24-3: -24-4: -24-5: -24-6: -24-7:
-25-1: -25-2: -25-3: -25-4: -25-5: -25-6: -25-7:
-26-1: -26-2: -26-3: -26-4: -26-5: -26-6: -26-7:
-27-1: -27-2: -27-3: -27-4: -27-5: -27-6: -27-7:
-28-1: -28-2: -28-3: -28-4: -28-5: -28-6: -28-7:
-29-1: -29-2: -29-3: -29-4: -29-5: -29-6: -29-7:
-30-1: -30-2: -30-3: -30-4: -30-5: -30-6: -30-7:
The following codes will be used to describe the condition of sample after delivery: 00: arrived frozen and
unbroken; 01: arrived frozen, but vial is broken; 02: thawed in transit, but vial is not broken; 03: thawed in
transit and vial broken, 04: does not exist.
Write in the above section the code of the condition of the sample after delivery if there is any problem Observations and/or problems from the sender (specify problems during the extraction, collection, and
storage of the samples):
Observations and/or problems from the receiver:
45
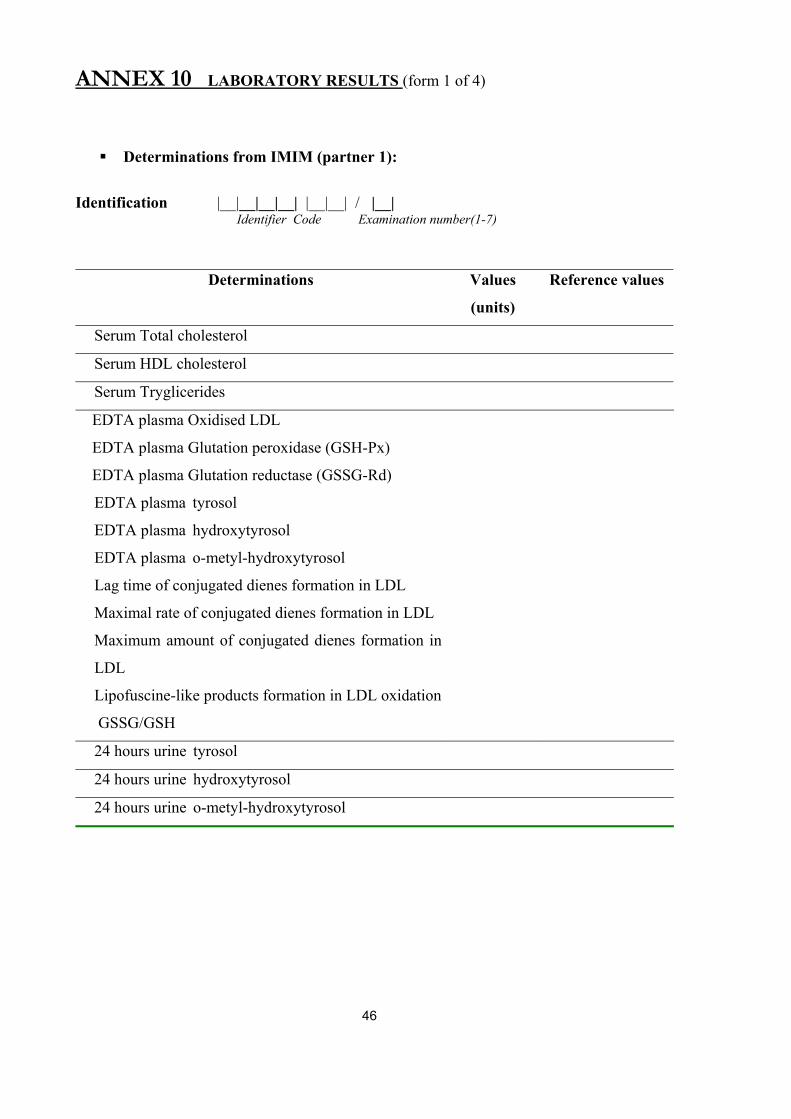
ANNEX 10 LABORATORY RESULTS (form 1 of 4)
Determinations from IMIM (partner 1):
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number(1-7)
Determinations Values
(units)
Reference values
Serum Total cholesterol
Serum HDL cholesterol
Serum Tryglicerides
EDTA plasma Oxidised LDL
EDTA plasma Glutation peroxidase (GSH-Px)
EDTA plasma Glutation reductase (GSSG-Rd)
EDTA plasma tyrosol
EDTA plasma hydroxytyrosol
EDTA plasma o-metyl-hydroxytyrosol
Lag time of conjugated dienes formation in LDL
Maximal rate of conjugated dienes formation in LDL
Maximum amount of conjugated dienes formation in
LDL
Lipofuscine-like products formation in LDL oxidation
GSSG/GSH
24 hours urine tyrosol
24 hours urine hydroxytyrosol
24 hours urine o-metyl-hydroxytyrosol
46
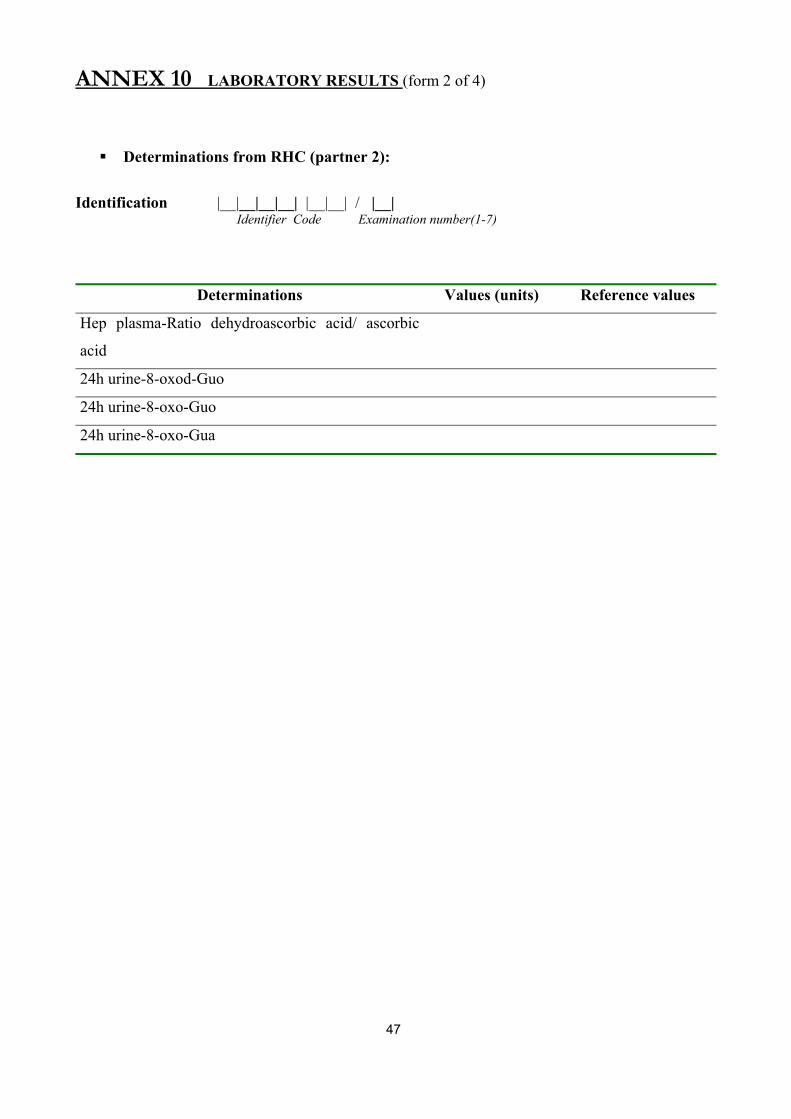
ANNEX 10 LABORATORY RESULTS (form 2 of 4)
Determinations from RHC (partner 2):
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number(1-7)
Determinations Values (units) Reference values
Hep plasma-Ratio dehydroascorbic acid/ ascorbic
acid
24h urine-8-oxod-Guo
24h urine-8-oxo-Guo
24h urine-8-oxo-Gua
47
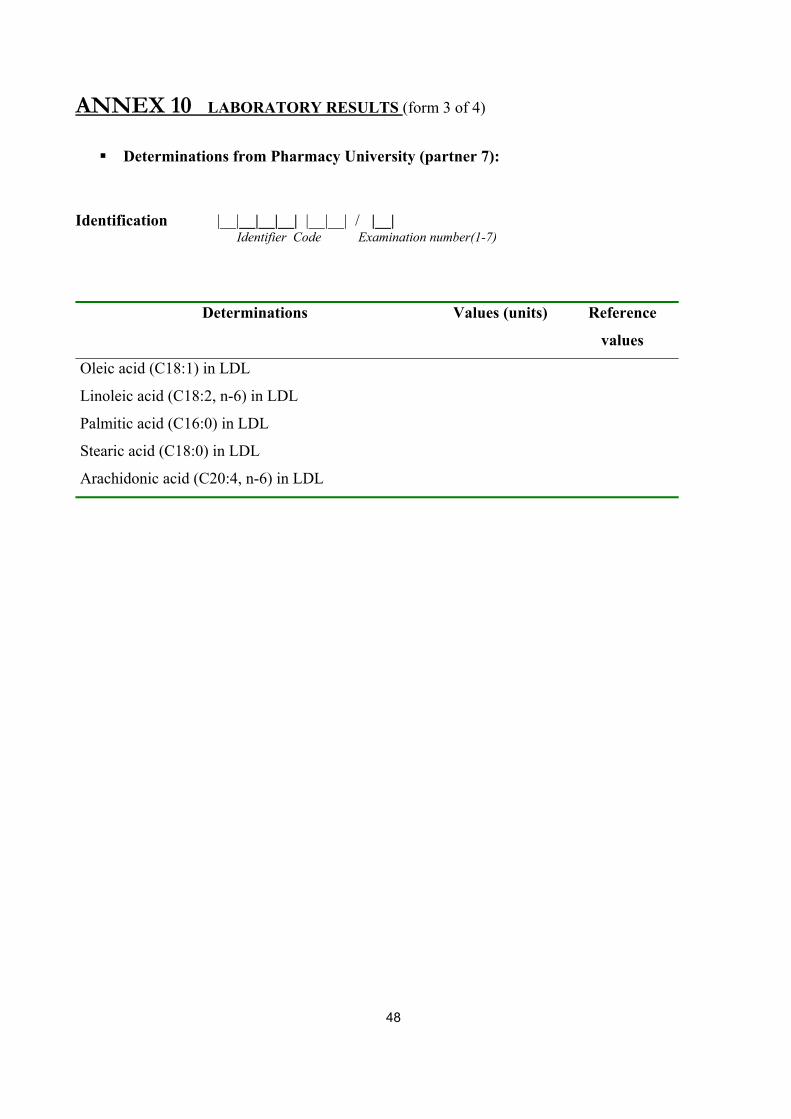
ANNEX 10 LABORATORY RESULTS (form 3 of 4)
Determinations from Pharmacy University (partner 7):
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number(1-7)
Determinations Values (units) Reference
values
Oleic acid (C18:1) in LDL
Linoleic acid (C18:2, n-6) in LDL
Palmitic acid (C16:0) in LDL
Stearic acid (C18:0) in LDL
Arachidonic acid (C20:4, n-6) in LDL
48
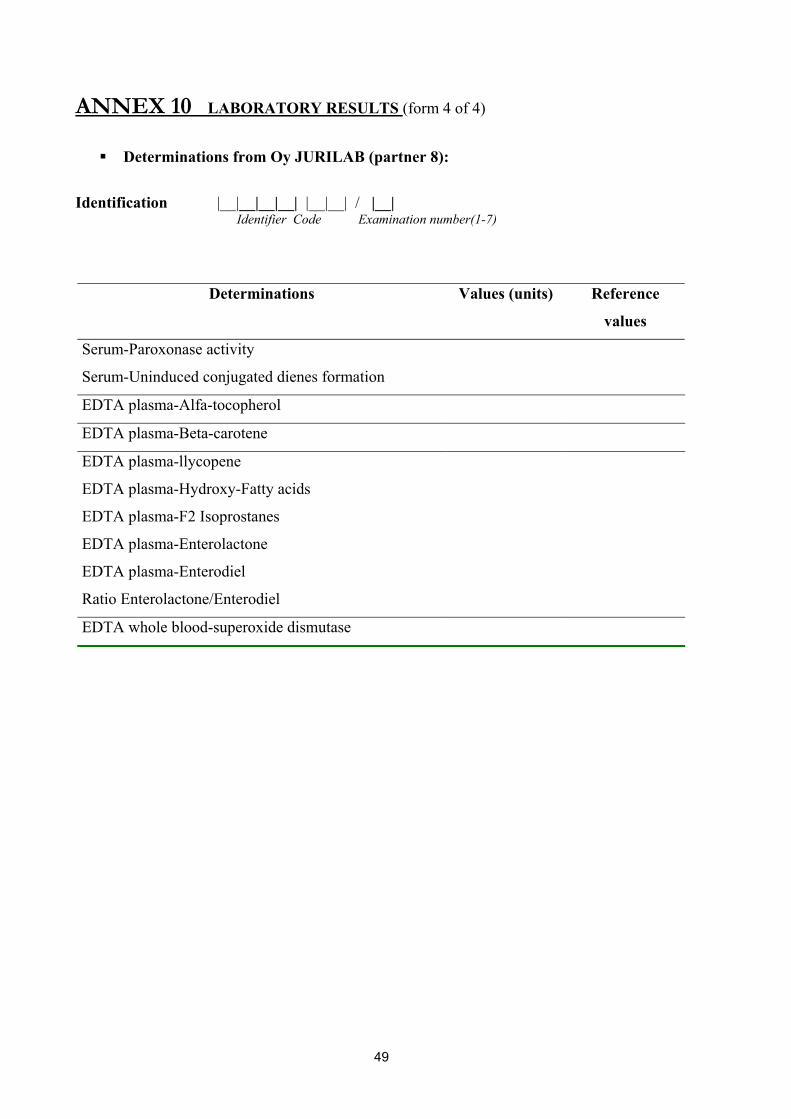
ANNEX 10 LABORATORY RESULTS (form 4 of 4)
Determinations from Oy JURILAB (partner 8):
Identification |__|__|__|__| |__|__| / |__|
Identifier Code Examination number(1-7)
Determinations Values (units) Reference
values
Serum-Paroxonase activity
Serum-Uninduced conjugated dienes formation
EDTA plasma-Alfa-tocopherol
EDTA plasma-Beta-carotene
EDTA plasma-llycopene
EDTA plasma-Hydroxy-Fatty acids
EDTA plasma-F2 Isoprostanes
EDTA plasma-Enterolactone
EDTA plasma-Enterodiel
Ratio Enterolactone/Enterodiel
EDTA whole blood-superoxide dismutase
49