Et. 2.Perdarhan Saluran Cerna

of 69
-
Upload
marpaung-liza -
Category
Documents
-
view
219 -
download
1
Transcript of Et. 2.Perdarhan Saluran Cerna
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
1/69
Dr. LEONARDO DAIRY, SpPD KGEH
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
2/69
INTRODUCTION
PSCBA (UGI BLEEDING)
PSCBB (LGI BLEEDING)
OCCULT BLEEDING
OBSCURE BLEEDING
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
3/69
Gastrointestinal (GI) bleeding is an extremely
common clinical problem
resulting in significant morbidity, mortality, and cost.There are over 300,000 hospitalizations annually in theUnited States for GI bleeding, accounting for 12% of
all hospital admissions. A conservative estimate of the overall annual cost of
hospital admissions for GI bleeding is $900 million, butthe true overall cost, including outpatient endoscopic
and radiologic investigations, clinic visits, and work dayslost, far exceeds.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
4/69
Upper GI bleeding (UGI) Incidence of UGI is approximately 100 cases per 100,000
population.Acid peptic disease (e.g., gastric,duodenal ulcers andgastritis) is the most common cause of upper GI bleeding,accounting for 5075% of all cases). Acid peptic disease isfollowed by variceal bleeding, gastric and duodenal erosivedisease, and Mallory-Weiss tears in prevalence. Furthermore, thepredominance of peptic ulcer bleeding has not been affected bythe advent of improved acid suppression with medical therapy.
The elderly appear to be at particular risk, as the proportion ofelderly patients who present with upper GI bleeding has steadily
increased, with persons older than age 60 years accounting for3545% of all cases. This increase cannot be explained bydemographics alone, as increasing age directly correlates with anincreased rate of hospitalization for upper gi bleeding.
.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
5/69
Lower GI bleeding less common, around 2027 per 100,000 .
80% of patients with GI bleeding pass heme per rectum as bright red blood,
maroon stools, or melena, only 24% of all GI bleeding is from a lower GI
source. The incidence of LGI bleeding is higher in men and elderly .
The rate of hospitalization for LGI bleeding increases more than 200-fold
from the third to the ninth decades, probably because of an increased
incidence of the most common etiologies; diverticulosis, angiodysplasia,
and neoplasia in the elderly. In most studies, diverticulosis is the most
common cause of acute LGI bleeding, accounting for 4255% of cases.
However, in one large series of patients with severe, persistent
hematochezia, angiodysplasia was the most common diagnosis, accounting
for 30%. Other, less common etiologies include colorectal neoplasia,
colonic ischemia, IBDi, infectious causes, radiation proctitis,, iatrageniccauses (e.g. postpolypectomy, endoscope trauma, and so on),
intussusception, solitary rectal ulcer syndrome, colonic varices, and
endometriosis .Hemorrhoidal bleeding is probably the most prevalent cause
of acute GI bleeding in the ambulatory setting, accounting for up to 76% of
cases, but it represents only 2
9% of admissions for lower GI bleeding.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
6/69
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
7/69
Definition
Bleeding derived from any sourceproximal to the Ligament of Treitz
1 in 1000 in us who
experienced upper GI
bleedingMen :women
2 : 1
Mortality rate 10%
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
8/69
PSCBA PERDARAHAN SEPANJANG SAL. CERNAPROK. DARI LIG.TREITZ.
KEGAWAT-DARURATAN
INSIDENS 50
100/100.000 PDDK (USA), 20.000KEMATIAN/TAHUN
TINGKAT MORTALITAS 10% - 36%, 33% (UK)
80% BERHENTI SPONTAN PERDARAHAN SALURAN CERNA ATAS
PERDARAHAN SALURAN CERNA ATAS
VARISESPERDARAHAN SALURAN CERNA ATAS
NON VARISES
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
9/69
Sebuah studi meta analisis terapi endoskopi
pada PSCBA secara bermakna mengurangifrekuensi perdarahan lanjut, pembedahan danmortalitas.
Angka morbiditas dan mortalitas juga sangatdipengaruhi oleh bagaimana optimalnyatatalaksana kasus dalam 24-48 jam pertama di
sarana pelayanan kesehatan.
Sass AD, Chopra KB. Portal hypertension and variceal hemorrhage. Med Clin N Am. 2009;93:83753.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
10/69
CAUSE OF GI BLEEDING
Common causesGastric ulcer, Duodenal ulcer
Esophageal varices
Mallory-Weiss tear
Rare causes
Esophageal ulcer, Erosive duodenitis
Aortoenteric fistula, Hemobilia
Pancreatic sources
Crohns disease
No lesion identified
Less Frequent Causes
Dieulafoys lesion
Vascular ectasia
Portal hypertensive gastropathy
Gastric antral vascular ectasiaGastric varices
Neoplasia
Esophagitis
Gastric erotions
Rare Causes
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
11/69
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
12/69
o
AINS
Aspirin
Gastric Acid
Helicobacter pylori Anti-koagulan
Anti-trombotik
Merokok
Alkohol
Penyakit hati kronik
Rockey DC. Gastrointestinal bleeding. Gastroenterol Clin N Am. 2005;34:5818.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
13/69
CLINICAL PRESENTATION
HEMATEMESIS :
MUNTAH DARAH WARNA MERAH KECOKLAT COKLATAN KEHITAM HITAMAN (CAFFEIN)
MELENA :
BAB WARNA HITAM (TERRY STOOL) >50CC DARAH
HAEMATOCHEZIA :
BAB WARNA MERAH TERANG GELAP
OCCULT BLEEDING :
TDK ADA PERUBAHAN WARNA BAB, NAMUN BENZIDINETEST (+)
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
14/69
1. PERDARAHAAN ANAMNESE RIWAYAT COMMON
VOMITING (MENTAL)MALLORYWEISS TEAR ?
HEARTBURN & REGURGITASI REFLUX ESOFAGITIS ?
DYSFAGIA & BBMALIGNANCY PD ESOFAGUS ?
MAKAN OBAT-OBATAN & ALKOHOLGASTRIC EROSIVE ?
ULKUS PEPTIKUM ?
LIVER STIGMATA (CH) VARICES BLEEDING ?
PENYAKIT BERAT (DI ICU) STRESS ULCER ?
DIAGNOSTIK
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
15/69
GAMBARAN KLINIK
Hematemesis + Melena PSCBA esofagus &gaster
Melena PSCBA duodenum
Berat ringannya perdarahan dinilai dari :
manifestasi klinik yang ada
derajat turunnya kadar hemoglobin, ada tidaknya manifestasi gangguan
hemodinamik.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
16/69
2. PEMERIKSAAN FISIK :
Penilaian status hemodinamik & resusitasi Jaundice & Tanda2 liver stigmata & HT portal
Bleeding diathesis : purpura, ekimosis, ptikiae
3. RADIOLOGI
Ba. Swallow, Ba. Follow Through, MDF double contras, Kolon in loop.
Upper & Lower Abdominal Scanning
4. ENDOSKOPI
Gastroduodenoskopi Sigmoidoskopi
Colonoskopi
Push Enteroskopi
Capsule Endoscopy
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
17/69
Historical Features Important in Assesing the
Etiology of Gastrointestinal Bleeding
Age
Prior Bleeding
Previous gastrointestinal disease
Previous surgery
Underlying medical disorder (especialy liver disease)
Nonsteroidal anti-inflammatory drugs/aspirin
Abdominal pain
Change in bowel habits
Weight loss/anorexia
History of oropharyngeal disease
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
18/69
Diagnosis
Pemeriksaan fisik
Tanda vital syok?
Stigmata penyakit hatikronik
Ikterus
Hepatomegali
Asites
Spider angioma
Palmar erythema
Pemeriksaan laboratorium
DPL
Prothrombin time
INR
Fungsi hati
Rockey DC. Gastrointestinal bleeding. Gastroenterol Clin N Am. 2005;34:5818.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
19/69
INITIAL PATIENT ASSESMENT
hemodynamics Blood loss (%) Severity of bleed
(vital signs) (fraction of
intravascularvolume)
Shock (Restinghypotension)
Postural(Orthostatictac
hycardia/hypotension)
Normal
20-25
10-20
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
20/69
HEMORRHAGIC I II III IV
CLASS 15% OR 20-25% OR 30-35% OR 40-50% OR
BLOOD LOSS 750 ML 1000-1250 ML 1500-1800ML 2000-2500 ML
HEART RATE 100 >120 >140
RESPIRATORY 14-19 20-29 30-40 >40
RATEARTERIAL NORMAL 110-80 70-60
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
21/69
Aspirasi nasogastrik
Membedakan perdarahan
saluran cerna atas danbawah
Sensitivitas 79%,spesifisitas 55%
Modalitas diagnostik danterapeutik
Townsend: Sabiston Textbook of Surgery, 18th ed. 2007.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
22/69
Diagnosis
Esofagogastroduodenoskopi (EGD)
Modalitas utama
Menentukan lokasi & penyebab perdarahan saluran
cerna atas: 90% - 95%
Rockey DC. Gastrointestinal bleeding. Gastroenterol Clin N Am. 2005;34:5818.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
23/69
Forrest class Type of lesion Risk of rebleed ifuntreated (%)
I a Arterial Spurting 100
I b Arterial Oozing 17-100
II a Visible Vessel 8-81
II b Sentinel Clot 14-36
II c Haematin covered flat spot 0-13
III No Stigmata 0-10
Tabel 2. KLASSIFIKASI FORRESTPSCBA
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
24/69
MANAGEMENT
RESUSCITATION
VASCULAR ACCESS
INTRAVENOUS FLUIDS BLOOD TESTS
TYPING & CROSS MATCHING
CORRECT COAGULOPATHY
BLOOD TRANSFUSION
Rockall scoring system for risk of
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
25/69
Rockall scoring system for risk ofrebleeding and death
Variable 0 point 1 point 2 points 3 points
Age (yrs) 80
Shock Systolic BP>100
Pulse 100
Pulse>100
Systolic BP100
Comorbidity None Cardiac failure
Coronary heart
disease
Other major co
morbidity
Renal failure
Hepatic Failure
Metastatic cancer
Diagnosis
Major
stigmata of
recent
bleeding
(SRH)
MW tear
No lesions
None
All other
diagnoses
Malignancy of
upper GI tract
Fresh blood
Ulcer with
adherent clot,
visible or
spurting vessel
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
26/69
Rockall score ranges 0-11
A total score30%
reeburg EM, Tarwee CB, Suel P, et al. Gut 1999;44:331-5
Rockall Score Clinical Implication
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
27/69
Prinsip Umum :1. Penilaian hemodinamik disertai resusitasi cairan dan
stabilisasi hemodinamik2. Penilaian onset dan derajat perdarahan
3. Usaha menghentikan perdarahan secara umum (stopgap treatment)4. Usaha identifikasi lokasi sumber perdarahan dengan
modalitas sarana penunjang yang tersedia
5. Mengatasi sumber perdarahan secara defenitif6. Minimalisasi komplikasi yang dapat terjadi7. Upaya pencegahan terjadinya perdarahan ulang dalam
jangka pendek maupun jangka panjang.
PENATALAKSANAAN
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
28/69
Penatalaksanaan
Penatalaksanaan pada PSCBA terbagi atas penatalaksanaanmedik dan penatalaksanaan bedah.
A. PENATALAKSAAN MEDIK1. Penatalaksanaan non-farmakologis : memperbaiki
keadaan umum, tanda vital, infus cairanparenteral/nutrisi, transfusi darah dan lain-lain.
2. Penatalaksanaan farmakologis : ARH2 atau PPI,sitoprotektor, antibiotika, obat hemostatik (tranexamicacid, adona AC dan somatostatin).
PENATALAKSANAAN
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
29/69
Mempertahankan pH lambung > 6
Proses koagulasi
Agregasi trombosit
Pembentukan fibrin
Dosis, Bolus 80 mg IV dilanjutkan dengan infus8 mg/jam selama 72 jam
Menurunkan angka kejadian perdarahanberulang
Menurunkan mortalitas
Barkun AN, Badou M, Kuipers EJ, Sung J, Hunt RH, et al. International consensus recommendations on the management ofpatients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2010;152:101-13.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
30/69
Seven-day intravenous low-dose omeprazole infusion
reduces peptic ulcer rebleeding for patients with
comorbiditiesCeng H, et al. Gastrointest Endosc 2009;70:433-
3 PENATALAKSANAAN KHUSUS
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
31/69
3. PENATALAKSANAAN KHUSUS
TOPICAL THERAPY
-Tissue adhesives
-Clotting factors
-Collagen
-Ferromagnetic tamponade
MECHANICAL THERAPY
-Snares
-Sutures
-Balloons
-Hemoclips
INJECTION THERAPY
-Variceal bleeding
-Non variceal bleeding
- Ethanol
- Other sclerosants
THERMAL THERAPY
-Electrocoagulation
- monopoloar
- electrohydrothermal
bipolar (multipolar)
-Heater probe
-Laser
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
32/69
Injeksi sklerosan seperti etanol, polidocanol, dan
etanolamin, dapat menyebabkan trombosispembuluh darah sehingga tercapai hemostasis.
Pada perdarahan saluran cerna atas akibat non-
varises, efektivitas sklerosan sama dengan adrenalindalam mencapai hemostasis dan mencegahrekurensi.
Penggunaan sklerosan lebih terbatas karena dapatmengakibatkan ulkus atau striktur iatrogenik.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
33/69
Pemanasan menimbulkan penekanan pada arteri sehingga
perdarahan berhenti. Teknik pemanasan dibagi atas non-kontak dan kontak.
Pemanasan dengan teknik non-kontak menggunakan laser(neodymium:yttrium-aluminum-garnet) atau argon plasma
coagulation. Teknik pemanasan menggunakan laser kini jarang
digunakan.
Hemostasis pada pemanasan dengan argon tercapai pada
75,9% kasus dengan rekurensi pada 5,7% kasus.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
34/69
Pemanasan dengan teknik kontak menggunakanelektrokoagulasi bipolar dan heater probethermocoagulation.
Kombinasi elektrokoagulasi bipolar dan injeksiadrenalin dapat menurunkan risiko terjadinyarekurensi.
Kombinasi heater probe thermocoagulation dan injeksiadrenalin dapat mencapai hemostasis pada 98.6%kasus dengan angka rekurensi sebesar 8,2%.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
35/69
Endoloop, clip, dan rubber band ligation merupakanalat yang digunakan untuk menghentikanperdarahan secara mekanik.
Penggunaan clip dapat mencapai hemostasis pada100% kasus perdarahan saluran cerna atasdengan rekurensi yang lebih rendahdibandingkan injeksi adrenalin.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
36/69
Kombinasi penggunaanhemoclips dan endoloops Perdarahan berhenti
Racz I, et al. Endoscopic hemostasis of bleeding gastric ulcer with a combination of multiple hemoclips and endoloops. Gastrointest Endosc; 2009.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
37/69
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
38/69
Endoscopic clipping for acute nonvariceal upper-GI bleeding: a
meta-analysis and critical appraisal of randomized controlled trialsYuan Y, et al. Gastrointest Endosc 2008;68:339-51
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
39/69
Lo C, et al. Gastrointest Endosc 2006;63Comparison of hemostatic efficacy for
epinephrine injection
alone and injection combined with hemoclip therapyin treating high-risk bleeding ulcers:767-73
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
40/69
Penatalaksanaan
B.PENATALAKSAAN BEDAH,OPERASIdilakukan bila perdarahan tetap berlangsung atausudah masuk dalam keadaan gawat I s/d II makamerupakan indikasi operasi.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
41/69
Varices Esofagus
Ligasi banding
Skeleroterapi
Varices Gaster
Injeksi argon plasma
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
42/69
Toubia N, Sanyal AJ. Portal Hypertension and Variceal Hemorrhage. Med Clin N Am 92 (2008) 551574
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
43/69
Bendtsen F, Krag A, Moller S. Treatment of Acute Variceal Bleeding. Digestive and Liver Disease 40 ( 2008 ) 328-336
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
44/69
TERAPI FARMAKOLOGI1. TERLIPRESSIN
menurunkan tekanan portal sekitar 20 % setelah single dose
Dosis 2 mg/4 jam selama 48 jam pertama
Dapat dilanjutkan sampai 5 hari dengan dosis yang lebih rendah yaitu 1 mg/4 jam atau 12-24 jamsetelah perdarahan berkurang
2. SOMATOSTATIN DAN ANALOG
Somatostatin
Mengurangi tekanan portal sekitar 17 % tanpa mempengaruhi hemodinamik sistemik.
Diawali dengan 250 g bolus diikuti oleh infus 250 g/jam yang dapat dipertahankan sampai 24 jambebas perdarahan.10
Ocreotide
50 g diikuti oleh infus 25-50 g/jam
Menurunkan angka rebleeding
3. REKOMBINAN faktor VIIa
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
45/69
MANAJEMEN NON FARMAKOLOGI
ENDOSKOPI
1. EST ( Endoskopi Skleroterapi )
2. EVL ( Endoskopi Variceal Ligation)
TIPS ( Transjugular Intrahepatic Portosystemic
Shunts )
BALOON TAMPONADE
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
46/69
Endoscopic Sclerotherapy Endoscopic Band Ligation
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
47/69
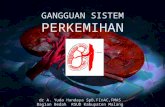
ENDOSCOPIC VARICEAL LIGATION (
EVL)
Endoscopy shows two
varices in the distal
esophagus that have
been banded. Thebands are indicated with
the green arrows. The
two strings in the rightof the field control the
trigger device used to
deploy the bands.
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
48/69
BALOON TAMPONADE
Linton tube dan Sengstaken-Blakemore
Tube
Algorithm for cirrhosis Without Bleeding
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
49/69
Algorithm for cirrhosis Without Bleeding
Algorithm For
Cirrhosis Without
Bleeding
Cirrhosis
Established
Reguler Interval
Usually one week
Upper Endoscopy
No varices Small or Medium
Varices
Large Varices
Observe Observe
(1
2 years Evaluation)
Primary Bleeding
Prophylaxis
Non Selectne Blockers
(and /or Nitrates)
Ligation
(2
3 years Evaluation)
Algorithm For
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
50/69
Algorithm For
Bleeding Cirrhoti
Algorithm For
Bleeding CirrhotisResuscitae
Begin Octreotide
(or Vasopressin)
Early endoscopy
Non-Portal
HypertensiveCause
Gastric Varices Esophagel
VaricesPortal
Hypertensive
Gastropathy
Treat appropriatelyContinue octreotide 5 daysBegin beta-blocker when stable
Band ligation or injectionSclerotheraphy
Ballon Tamponade
Rebleeding No rebleeding
Shunt (Child A)
TiPSS. or
Liver transplantation (Child B or C)
Continue treatment
Preventation of Rebleeding Pharmacological Treatment
Ligation /SclerotheraphyReguler Interval
Usually one week
Repeated Endoscopy
3 6 month
Eradication
Shunt (Child A)
TIPSS Or OLT (Child B or C)
Rebleeding
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
51/69
Peptic ulcer hemorrhage
Surgical intervention Only 10% of patients
Indications Failure of endoscopy Significant rebleeding after 1st endoscopy
Ongoing transfusion requirement
Need for >6 units over 24 hours
Earlier for elderly, multiple co-morbidities
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
52/69
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
53/69
Ulcus Pepticum Bleeding
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
54/69
Peptic ulcer hemorrhage
Gastric ulcer 10% are maliganant
30% will rebleed with simple ligation
Need Resection
Distal gastrectomy with Bilroth I or II Subtotal gastrectomy for 10% high on lesser curve
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
55/69
Peptic ulcer hemorrhage
Doudenal ulcer Expose ulcer with duodenotomy or duodenopyloromyotomy
Direct suture ligation, four quadrent ligation, ligation ofgastroduodenal artery
Anti-secretory procedure Truncal, parietal cell vagotomy
If unstable can use meds
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
56/69
Tatalaksana Perdarahan Saluran Cerna Atas
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
57/69
Rumah Sakit Tipe A dan BAnamnesis
Pemeriksaan tanda vitalPasang IV line, NGT
Periksa DPL, hemostasis
Hemodinamik tidak stabil,perdarahan aktif
Resusitasi
Kristaloid; koloid
Transfusi darahKoreksi faktor koagulasi
Terapi Empirik
Hemodinamik stabil, tidakada perdarahan aktif
Hemodinamik stabil,perdarahan berhenti
Hemodinamik tidak stabil,perdarahan tidak berhenti
Emergency endoscopy
Perdarahan berhenti
Elective endoscopy
Terapi definitif
Varises esofagus Ulkus
Bleeding site non-visualized
EVL, ES, SB tube
Bedah
Injeksihemostasis
Interventional diagnostic &therapeutic radiology
Obat vasoaktifOcreotide, somatostatin,
vasopressin
Konsensus Nasional Perkumpulan Gastroenterologi Indonesia 2007
Tatalaksana Perdarahan Saluran Cerna Atas
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
58/69
Rumah Sakit Tipe CAnamnesis
Pemeriksaan tanda vitalPasang IV line, NGT
Periksa DPL, hemostasis
Hemodinamik tidak stabil,perdarahan aktif
Resusitasi
Kristaloid; koloid
Transfusi darahKoreksi faktor koagulasi
Terapi Empirik
Hemodinamik stabil, tidakada perdarahan aktif
Hemodinamik stabil,perdarahan berhenti
Hemodinamik tidak stabil,perdarahan tidak berhenti
Perdarahan berhenti
Foto abdomen dg kontras Baatau
Rujuk untuk Endoskopi
Terapi definitif
Obat vasoaktifOcreotide, somatostatin,
vasopressin
Konsensus Nasional Perkumpulan Gastroenterologi Indonesia 2007
Perdarahan tidak berhenti
Balloon tamponadeSB tube
Perdarahan berhenti
Perdarahan tidak berhenti Bedah
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
59/69
Summary of consensus Recommendation Management
patients with non variceal UGI Bleeding
a. Resusitasi, risk assesment, and pre endoscopic management1. Immediately evaluate and initiate appropriate resusitation.
2. Prognostic scales
3. Consider placement of NGT
4. Blood transfution
5. Correction of coagulopathy
6. Promotility agents should not be used7. Preendoscopic PPI therapy
b. Endoscopic management
1. Early endoscopy
2. Endoscopic therapeutic not indicated with low risk stigmata
3. Endoscopic therapy for ulcer with cloth is kontroversial.
4. Endoscopic therapy with high risk stigmata
5. Epinephrine injection sub optimal
6. No single endoscopic thermal is superior
7. Clips thermocoagulation or sclerosan injection alone or combination
8. Endoscopic therapy recommended in rebleeding
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
60/69
c. Pharmacologic management
1. H2 RA are not recommended
2. Somatostatin and ocretide are not routine recommended
3. IV bolus followed continuous infusion should be use to the decrease rebleeding
and mortality.
d. Non endoscopic and non pharmacologic in hospital management
1. Patients with endoscopic therapy should be hospitalized at least 72 hours
2. Surgical consultation if endoscopic therapy failed
3. Percutaneus embolisation can be consider4. Peptic ulcer bleeding with HP (+) be should eradication therapy
5. HP (-) diagnostic test should be repeat
e. Postdischarge, ASA, and NSAID
1. Previous PUB with NSAID, combination PPI and Cox-2 is recommended
2. Previous PUB with NSAID, NSAID plus PPI or cox-2 alone
3. PUB with low dose ASA, ASA therapy ???
4. Previous PUB who require cardiovascular prophylaxis, clopidogrel alone higherrisk than ASA with PPI
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
61/69
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
62/69
LGI hemorrhage
Sites Colon 95-97%
Small bowel 3-5%
Only 15% of massive GI bleeding Finding the site
Intermittent bleeding common
Up to 42% have multiple sites
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
63/69
Bleeding
diverticulosis
Colonic angiodysplasia
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
64/69
LGI hemorrhage diagnostics
Colonoscopy Within 12 hours in stable patients without large
amounts of bleeding
Selective viseral angiography Need >0.5 ml/min bleeding
40-75% sensitive if bleeding at time of exam
Tagged RBC scan
Can detect bleeding at 0.1 ml/min 85% sensitive if bleeding at time of exam
Not accurate in defining left vs right colon
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
65/69
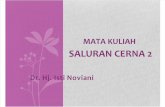
Meckels Diverticulum
Cecal angiodysplasia
with extravasation
Small bowel ulceration
due to NSAIDS
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
66/69
LGI hemorrhage treatment
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
67/69
LGI hemorrhage treatment
Endoscopy Great for angiodysplasia and polypectomy sites
Angiographic
Selective embolization for poor surgical
candidates Surgery
Ongoing hemorrhage >6 units or ongoing
transfusion requirement
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
68/69
Hemodynamic instability despitevigorous resuscitation (>6 unitstransfusion)
Failure of endoscopictechniques to arrest
hemorrhage Recurrent hemorrhage after
initial stabilization (with up to twoattempts at obtainingendoscopic hemostasis)
Shock associated with recurrenthemorrhage
Continued slow bleeding with atransfusion requirementexceeding 3 units/day
One of the criteria used to determine the need for surgical intervention isthe number of units of transfused blood required to resuscitate the patient.The more units required, the higher the mortality rate (Larson, 1986).Operative intervention is indicated once the blood transfusion numberreaches more than 5 units, as noted in the following table (Larson, 1986).
Number of UnitsTransfused
Need forSurgery, %
MortalityRate, %
0 4 4
1-3 6 14
4-5 17 28
>5 57 43
-
7/28/2019 Et. 2.Perdarhan Saluran Cerna
69/69