Epidemiology Epidemiology Incidence of malignancy age 0-14 and 0-19 years Total Leukemia Lymphoma...
33
Epidemiology Epidemiology Incidence of malignancy age 0-14 and 0-19 years • Total • Leukemia • Lymphoma • CNS • Neuroblastoma • Retinoblastoma • Kidney • Liver • Bone • Soft tissue sarcoma • Germ cell • Carcinoma • Other & unclassified 130.9 (%) 144.6 (%) 42.2 32.23 37.3 38.77 14 . 3 10.92 21 . 0 14.52 28.1 21.46 29.5 20.40 9.8 7,49 7,1 4,91 3.8 2.90 3.3 2.28 8.5 6.49 7.1 4.92 1.4 1.07 1.4 0.97 5.4 4.12 7.6 5.25 8.3 6.34 9.4 6.50 4.0 3.05 8.0 5.53 3.4 2.60 9.9 6.85 1.2 0.92 2.9 2.00 *per 1 000 000 children, ACCIS (Automated Childhood Cancer Information System ) 2
-
Upload
camron-lawrence -
Category
Documents
-
view
214 -
download
0
Transcript of Epidemiology Epidemiology Incidence of malignancy age 0-14 and 0-19 years Total Leukemia Lymphoma...

EpidemiologyEpidemiology Incidence of malignancy age 0-14 and 0-19 years
EpidemiologyEpidemiology Incidence of malignancy age 0-14 and 0-19 years
• Total
• Leukemia• Lymphoma• CNS• Neuroblastoma• Retinoblastoma• Kidney• Liver• Bone• Soft tissue sarcoma• Germ cell• Carcinoma• Other & unclassified
130.9 (%) 144.6 (%) 42.2 32.23 37.3 38.77 14.3 10.92 21.0 14.52 28.1 21.46 29.5 20.40 9.8 7,49 7,1 4,91 3.8 2.90 3.3 2.28 8.5 6.49 7.1 4.92 1.4 1.07 1.4 0.97 5.4 4.12 7.6 5.25 8.3 6.34 9.4 6.50 4.0 3.05 8.0 5.53 3.4 2.60 9.9 6.85 1.2 0.92 2.9 2.00
*per 1 000 000 children, ACCIS (Automated Childhood Cancer Information System ) 2006.

Classification and Incidence of Classification and Incidence of Lymphoma in Children of Age Lymphoma in Children of Age 0-19y
x106 %
• Hodgkin’s lymphoma (HLHL) 8.9 43.6
• Non-Hodgkin lymphoma (NHLNHL) 11.5 56.4
*WHO/REAL
**ACCIS 2006.

Hodgkin’s LymphomaHodgkin’s LymphomaHD→HL (RS and H cells are of lymphoid origin; RS of B cell lineage)

EpidemiologyEpidemiology• Developed countries 7/mil
– rare before 5y– 5.5/mil before 15y– 8.9/mil before 19y – 12.1/mil 15-20y
• Western Asia, all ages >7/mil
• 2 peaks: 20y and 55y, in underdeveloped countries a shift toward earlier age
• ♀:♂ = 3:1 in children under 10y
SUBTYPES• Lymphocyte predominance - more frequent in underdeveloped
countries, particularly in South Asia; also in younger children• Nodular sclerosis is the most frequent in developed countries

Etiology ofEtiology of HL HL Environmental, Genetic and Immunological Factors
• More frequent in certain families and ethnic gropus – genetic or common environmental factors
• Familial occurrence in 4.5% of all HL
• Association with EBV• Parents’ education and
income inversely correlate with HL
• More frequent with primary and secondary immunodeficiencies

Etiology ofEtiology of HL HL andand EBV EBV
• EBV genome more frequently found in children of 0-14y than of 15-39y with HL
• EBV+ HL of mixed cellularity
• Latent membrane protein-1 (LMP-1) expressed in EBV+ H/RS mimics activated CD40R→ activates the anti-apoptotic nuclear factor κB
*Nature Reviews Cancer 4, 757-768 (October 2004)

Clinical Features of HL
• Peripheral lymphadenopathy, painless, not responding to antibiotic therapy– Cervical 70-80%– Axillary 25%– Other localizations
• Mediastinal mass• Splenomegaly and/or hepatomegaly• Systemic symptoms, B symptoms

Diagnosis ofDiagnosis of HL – HL – laboratory laboratory analysesanalyses
• CBC– Hemolytic anemia
(Coombs+), anemia of chronic disease, bone marrow infiltration
– Leukocytosis, lymphopenia, eosinophilia and/or monocytosis
– Thrombocytopenia and/or ITP
• Urine (protenuria, nephrotic syndrome)
• ↑ Acute phase reactants (SE, CRP, Cu(S), ferritin, fibrinogen)
• Routine biochemical analyses (LDH – tumor mass, AP – bone involvement...)
• Patohistological findings

Biopsy inBiopsy in HL HL
• Tumor biopsy (morpology and immunohistochemistry)
• Bilateral bone marrow biopsy except CS Ia
• Not to be performed: – Needle biopsy of tumor– Staging laparotomy

bone marrow skinbone
biopsy needle

Classification ofClassification of HL (WHO) HL (WHO) andand incidence in childrenincidence in children
%
Children/ adolescents
Classical nodular sclerosis 45-50 44/77
Classical mixed cellularity 30-35 33/11
Classical lymphocyte predominance
7-14
Classical lymphocyte depletion 0.5-20
Nodular-lymphocyte predomination (NLP)
10-20

ImmunophenotypeImmunophenotype
CD15 CD30 CD20 CD45
Classical forms + + -/+ -
NLP - - + +

Ann Arbor Ann Arbor ClassificationClassification
• I (one lymph node or one extralymphatic localization)• II (2 or more lymph nodes on both sides of diaphragm)• III (2 or more lymph nodes on both sides of diaphragm)• IV (1 or more extralymphatic organs [liver, bone marrow,
lung] or tissues)
• Designations A and B
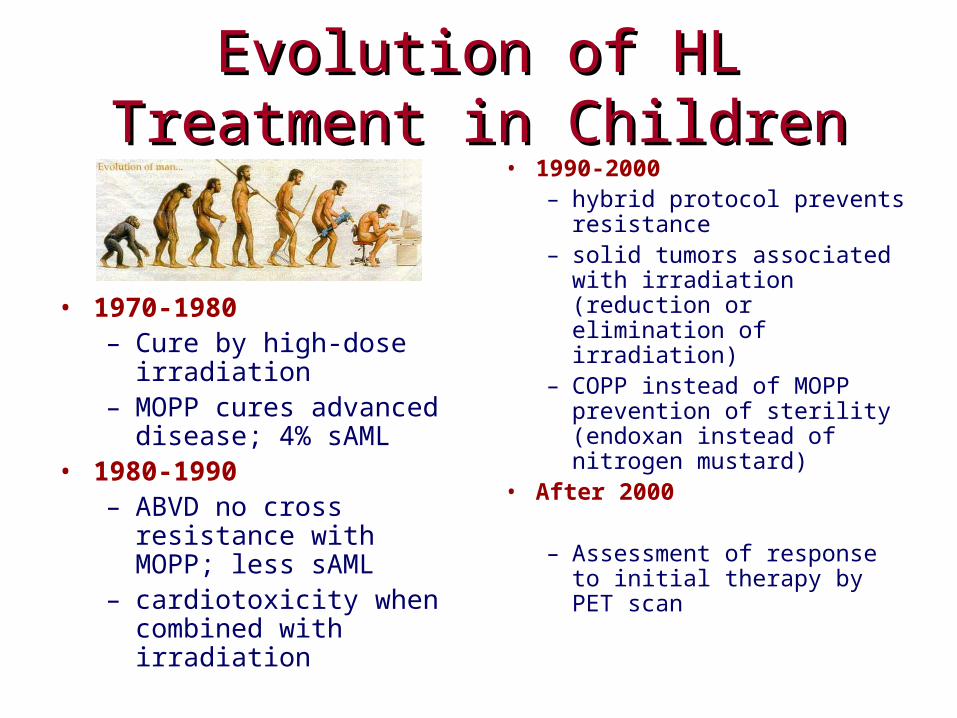
Evolution of HL Treatment in Evolution of HL Treatment in ChildrenChildren
• 1970-1980– Cure by high-dose
irradiation– MOPP cures advanced
disease; 4% sAML• 1980-1990
– ABVD no cross resistance with MOPP; less sAML
– cardiotoxicity when combined with irradiation
• 1990-2000– hybrid protocol prevents
resistance– solid tumors associated
with irradiation (reduction or elimination of irradiation)
– COPP instead of MOPP prevention of sterility (endoxan instead of nitrogen mustard)
• After 2000
– Assessment of response to initial therapy by PET scan

Late Complications of Late Complications of HLHL Treatment Treatment• Skeleton:
– sequelae of RT, 6-7x greater risk of avascular necrosis (cortico)
• Hypothyroidism: – 50% chidren after 10y of treatment
(especially girls)
• Sterility –RT, alkylating ag.– Infertility, reduced fertility, early
menopause (banks of sperm and ova)
– ♀ less gonadotoxicity of alkylating ag, as well as in younger ♀ than ♂ of same age
• Pluća:– RT and bleomycin: pneumonitis
and fibrosis, 3-5 toxicity in 5.1%
• Cardiovascular:– RT- dose, volume, fractions
(pericarditis, cardiomiopathy, CAD, valvular damage, conduction system, non-coronary VD- stroke
– anthracycline (dose)- (LV dysfunction, cardiomyopathy, CHF)
– host factors – severe damage <20g
• Secondary cancer: – in 30% od children after 30y from
HL diagnosis (thyroid Ca, breast Ca, non-melanoma skin cancer, NHL, AL)
Late toxicity ranking: 1=mild, 2=moderate, 3=severe, 4=life-threatening, 5=deadly
CAD =coronary artery disease, VD=valvular disease, LV= left ventricle, CHF= congestive heart failure

PrognosisPrognosis
5y about 90%
• Localized: other forms= >90%:70%

Epidemiology ofEpidemiology of NHL NHL
• Rare before 3 y• Median 10 y• m:f = 2-3:1
Geographical differences: • rare in Japan• most frequent
malignancy in equatorial Africa and Brazil– Burkitt – most common
subtype,• Most common sites
abdomen and jaw• aberrations upstream of
cMYC gene

Lymphoma distribution in Lymphoma distribution in childrenchildren
%1. B cell precursor neoplasms 52. T cell precursor neoplasms 203. Mature B cell neoplasms
1. Burkitt lymphoma/leukemia 422. B-cell lymphoma unclassifable, with features intermediate 5
between DLBCL and BL
3. Diffuse large B cell lymphoma (DLBCL) with subgr. of 3 mediastinal (thymic) large B cell lymphoma 0,4
4. Mature large cell T and NK cell neoplasms – analplastic large-cell lymphoma (ALCL) *CD30+, non-T, non-B („null cell“) 15
Σ ~90

T NHLT NHL
• Mediastinal localization
• Superior vena cava syndrome or asphyxia
• Treatment and outcome same as T ALL

Superior Vena Cava Compression
• edema
• plethora and cyanosis of face, neck and upper extremities
• filled supraclavicular pits
• conjunctival bleeding,
• stridor, pulmonary obstruction
• pronounced chest venous vessels
• congested neck venous vessels
• profuse sweating

oliguria/anuriaoliguria/anuria
respiratory respiratory insufficiencyinsufficiency
fluid overloadfluid overload
cardiac failurecardiac failurearrhytmiasarrhytmias
cardiac arrestcardiac arrest pulmonary pulmonary edemaedema
↓↓CaCa
uric acid→ → → accumulation of crystals in the kidneys→
lactate → → → → → → → metabolic acidosis→ → → → →
vasoactive substances → vasoconstriction → → → → → →
phosphate → → → → → → →accumulation → → → → → →
K → → → → → → hyperkalemia
→
→
→
→
TUMOR LYSIS SYNDROMETUMOR LYSIS SYNDROMEacute renal acute renal
failurefailure

B NHLB NHL
Endemic in AfricaSporadic – abdominal site

Anaplastic large cell lymphoma (ALCL)
• Various localizations• Several morphological types:
– common type– small-cell variant– lymphohistiocytic– giant-cell – differential diagnosis Mb. Hodgkin– mixt– unclassifiable
• Immunohistochemistry: CD30 (Ki1), CD15, EMA, TIA-1, ALK (90%),
T/null cell markers (CD3, CD2, CD5, CD7, CD8, CD43 ili CD3 i CD45Ro)9-11% co-express B cell markers90-100% co-express myeloid markers
• t(2;5) - ALK/NPM fusion

Skin ALCL

ALCL of Chest and Abdomen

Types and Features of Types and Features of Childhood NHLChildhood NHL
Burkitt T lymphobl. ALCL
Immunohistochem. -IgM, rarely IgA or IgG
-CD19, CD20, CD22 and CD79a
-CD10 in 10%
-CD21, EBV antigen receptor, more frequently in the endemic form
Pan-T EMA, CD30 (Ki-1)
Genetic associations -t(8;14)(q24;q32) u 85% t(2;8)(p12;q24)
-t(8;22)(q24;q11) 15%.
cMyc sa hr.8
t(1;14)(p34;q11)
t(11;14)(p15;q11
t(11;14)(p13;q11)
t(10;14)(p24;q11)
t(2;5)(p23;q35)
ALK, NPM

Treatment ofTreatment of NHL NHL
• Always prevention of tumor lysis syndrome
• Chemotherapy only
• Extirpation is NOT to be performed

T NHLT NHL
Treatment protocol as for T ALL

UpdatesUpdates
• LOH 6q16 – factor of poor prognosis (pEFS 27 vs. 86%)
• NOTCH1/FBXW7 mutation – factor of favorable prognosis (pEFS 84 vs. 66%)
• New stratification
• Targeted treatment

Chemotherapy – Treatment ProtocolChemotherapy – Treatment Protocol
R1 resected
R2 not resectedstage I, II, II with LDH<500
R3 not resected, stage III, LDH>500,LDH<1000,st. IV, B-ALL, LDH<1000, CNS-
R4 not resected, stage III, IV, B-ALLLDH>1000, CNS+/-
Treatment courses
A B
A B A B
AA BB CC AA BB
AA BB CC AA BB CC
Protocol NHL-B/B-ALL - BFM 2000
Anaplastic large cell lymphoma (ALCL)
• ALCL 99 Protocol– Similar to B cell lymphoma protocols– LR 3 cycles of ABA– IR 6 cycles of ABABAB (1g/m MTX)– HR -II- (3g/m MTX)

UpdatesUpdates
• Crizotinib- ALK inhibitor
• Brentuximab vedotin- anti-CD30+vedotin (monomethyl auristatin E) conjugate
• Anti-ALK vaccine

PrognosisPrognosis
5y EFS
T NHL >80% B NHL
ALCL