I. General concepts in TB Epidemiology II. Epidemiological indicators of TB and their estimation
Upload
shyam-ashtekarCategory
view
545download
0
TB in India:
Epidemiology and
Public Health Aspects
DR Shyam Ashtekar
Asst Professor, Community Medicine
SMBT Medical college, Nashik
20 Nov 2015

Historical
• TB is a companion for humanity from times of hominid ancestors
• 1882, 24 March-Robert Koch found Mycobacteria TB
• Hence 24th March-World’s Stop TB Day
• 1890-Tuberculin Protein-diagnostic tool for TB infection
• 1895-X-ray invention made diagnostics easy

In 20th Century
• 1921-BCG vaccine
• 1944-Streptomycin
• 1960-National Tuberculosis Institute of India
• 1962- National Tuberculosis Control Program
(NTCP)
• 1992-NTCP review went negative
• 1993-WHO made a Global Emergency call for
STOP TB
• 1997-Revised NTCP (RNTCP)
• 2005 RNTCP-Part of NRHM/now NHM

EPIDEMIOLOGY OF TUBERCULOSIS
Distribution of TBWhere, when, whom
Analytical aspects
Why, How, What is to be done for control

The Global Burden• About 2 billion (200 crores) infected by TB
–world pop 7 billion (nearly 1/3rd pop
infected asymptomatically)
• 65 million people with disease
• About 8-10 million new cases
annually(about 14 per thousand pop)
• 1.3 million deaths annually
• Multi-Drug Resistance (MDR & XDR) and
HIV infection make a dangerous
complication

Global Map of TB

The global scene
• A global problem of poverty, poor living
conditions
• Dramatic control with improvement of living
conditions
• Control also helped by BCG and streptomycin
& INH
• But now a Reemergence-
• HIV & TB a dangerous combination.
• Resistance to ATT

Drastic reduction of TB in developed
nations, but India ….
• Even before advent of TB
drugs, TB vanished as a public
health problem from Europe
and US.. With better life and
nutrition, workplace
improvements.
• In India, TB still is a big public
health problem despite best
anti TB drugs and diagnostic
tools.

No significant decline in TB in India- See more at: http://www.tbfacts.org/tb-statistics-india/#sthash.B6wFATk6.dpuf

Burden of TB in India (2013 Park)
• All forms of TB, old and new: 2.1/1000 pop ( about 26
lakhs in India)
• Incidence of all TB cases annual: 1.7 cases/1000 pop
(about 21 lakhs in India)
• Prevalence of Infection (30% pop)
• Annual incidence of TB infection is 1.5% (ARTI)
• Incidence of new smear positive cases per anum is 0.75
per thousand pop (75 per lakh pop)
• Deaths due to TB-all India-2.4 lakh
• Total HIV cases with TB -8.87 lakh
• Case detection-all forms 58%
• BUT MOST OF THESE ARE UNDERESTIMATES

India-worries and concernsTB &
HIV link
dangerous
2% new cases are MDR (N=20000),
Old & new MDR is 1.37 lakh accumulated cases
High Economic loss (annual 15000cr)-
Afflicts and kills working age people-5 lakhs annually
Silent chronic, often asymptomatic,
Highly infective. One open case is a risk to 15 new people annually

Epidemiology Triad
Agent
Host Environment

Reservoir and Transmission
• Main reservoir is Human cases, perhaps some role of cattle
• Infective material is TB sputum/coughed out droplets. Case remains infective for long.
• Becomes non-infective in 2 to 15 days after Short course chemotherapy starts.
• Infection mainly through respiratory route (or GIT)
• Main spread is indoor-to close contacts, esp children
• Public spitting-dust particles inhaled-less important

Host (Person) factors
Poverty-undernutrition, crowded living
Smoking, silicosis
Diabetes, HIV
BCG gives selective partial immunity
Men>women
Main age groups-Childhood, Young Adult, old age
Possibly cattle handling exposes to some risk
Immunity –not all infections become disease (only10% become TB disease)
Close contact with open case

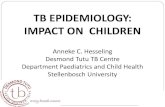
Age And TB prevalence
0
5
10
15
20
25
0-14 15-24 25-34 35-44 45-5455-64 65+
2
2123
20
16
11
7
Pe
rce
nta
ge
Age-wise TB cases -India 2006
% of TB cases

Agent factors
• Main type -Mycobacterium TB-Hominis
• Mycobacterium TB-Bovis- vet TB
• Atypical Mycobacteria-
• TB bacteria may be fast or slow growers-decides future course
of disease
• May be intra or extra cellular
• Take Zeihl Neelson stain (are basically Gram+ve)
• Hardy-against weather, chemicals. But killed in sunlight.
• Tend to stay dormant in human body.
• Indian TB is milder than European TB.

MDR(multi Drug Resistant) &
XDR (Extensively Drug Resistant)• Drug resistant TB is a
new problem
• MDR is INH & Rifampicin
resistance
• XDR is Extensively Drug
Resistant TB--Resistant
to INH+R and also
second-line drugs.
• Diagnosis is by
sputum
microscopy that
continues to be
positive even
after 4 months of
SCC.
• DOTS+ Regimen

Global picture of MDR

Environmental factors
• Crowded habitations
• Poor localities, with poor
sanitation
• Indoor transmission to
contacts is most
important
• Public spitting is a lesser
threat

Larger Socio-Economic
Determinants (Risk Factors)
• Poverty, poor housing
• Urbanization, population
density
• Malnutrition
• Low-education

Disease forms
Pulmonary (PTB)
• Primary lung disease with regional
lymph nodes-(most children used to
get before BCG)-called PRIMAY
COMPLEX
• POST-PRIMARY PULMONARY TB-
Most common, usually a flare up of
primary complex or new infection in
adult life
• One third cases of PTB are infective
(lesion is open to bronchi)
Extra pulmonary
• Uncommon after
BCG coverage
• All organs were
affected-
meninges, Ovary,
uterus, spine,
bones, kidneys,
intestines, lymph
nodes, skin, joints

Clinical picture of PTB
Common/main features
• Cough for >2 weeks
• Fever-low grade
• Pain in Chest
• Hemoptysis (blood in
spit)
Other features
• Loss of appetite
• Loss of weight-otherwise
unexplained
• Breathlessness
• Weakness
• Malaise

Childhood TB
• About 10-20% total TB is childhood TB
• Age 1-4 years
• Often due to close contacts with TB patients
• Usually Pulmonary now, less of other organs
• But no sputum, hence difficult to diagnose
• Hence also does not transmit TB like adults
• Failure to thrive, Malnutrition-both underlying
cause and effect of TB
• Childhood PTB may spread to other organs
• Tuberculin test usually clueless because of prior
BCG vaccine, But a Mantoux test >10 mm is
assumed as diagnostic

TB & HIV-Lethal partnership• HIV depletes immunity, hence-
• People with HIV & TB INFECTION have 30% chance of developing opportunistic TB DISEASE.
• HIV invites TB infection and flares up old TB -10% of them in first year.
• (Otherwise for PTB a lifetime chance of 10% relapse)
• Reinfection is common
• HIV-PTB is often sputum negative-hence difficult to diagnose, TT, Xray Chest often fails. Sputum culture called for.
• Spread of TB is faster in community.
• TB disease high in HIV prevalence areas, hence should get HIV test.

Diabetes and TB
• Diabetes patients account for
15-20% of PTB cases, because
immunity weakening
• All TB patients should get
screening for TB-sputum test

TB CONTROL PROGRAM-RNTCP
Public Health measures

What is Public Health..
It is the art and science of ..preventing disease, promoting health
and Prolonging life, through organized efforts of
community/society

Five levels of Prevention
5 Rehabilitation
4 Disability Limitation
3 EDPT( Early Diagnosis & Prompt Treatment)
2 Specific Protection
1 Health Promotion

Strategy in TB control
5 Rehabilitation
4 Disability Limitation (mainly by timely and complete treatment)
3 EDPT (mainly sputum microscopy for
symptomatic persons)
2 Specific Protection-mainly BCG (partial success)
1 Health Promotion-through socio-economics, nutrition-RNTCP can not do much effort here

WHO’s Stop TB strategy
• Pursue high quality DOTS expansion & enhancement
• Address HIV related TB, MDR, high risk groups
• Health system strengthening
• Engage all health care providers
• Empower people with TB, and communities
• Enable and promote research

RNTCP (Revised NTCP)
Objectives
• 70% of cases should be
detected (4per 1000) by
RNTCP with sputum
microscopy
• 85% of detected cases
must be cured.
Strategies
• BCG at birth
• Passive detection with
sputum microscopy
• DOTS therapy
• IEC-(Information,
education
communication )

BCG vaccination
• High protection level for TB health workers with BCG vaccination is proven
• Protects for 15-20 years, or even longer
• 0-80% of vaccinated community protected, esp against childhood TB, but not so much for adult PTB
• BCG offers only partial protection
• Can not be given in HIV cases

Clinical Detection is unreliable-PTB

Diagnostics in RNTCP
Clinically suspected
• Chronic cough>2
weeks in adults
• Blood spit-
hemoptysis
Investigations
• Sputum microscopy-Usually Direct-detects 80% cases in first test, 93% in second test, 100% by third test
• (Unusually concentrated sputum needs to be tested)
• If necessary Culture (for HIV cases or Drug sensitivity)
• Xray Chest (has only additional value)
• TT-Tuberculin Test, for child<2Y, or any person with >20mm induration

Short Course
Chemotherapy (SCC)Evidence
• Domiciliary treatment is equally or more effective than hospital based treatment (Chennai study)
• Isolation (to protect the family) is not required with SCC, and is fruitless by the time of detection
• Peru and China have demonstrated success with DOTS approach

What defines ‘Control’ of TB
Infection Prevalence Rate
• When prevalence of
INFECTION in children
below 14Y is brought
under 1 (now 40)
To do this..
• Reduce human reservoir
(cattle reservoir?)
• Cut transmission by
improvement of living,
control spitting
• Protect susceptible with
BCG, (also better
nutrition)

The Indian Challenge of TB
• TB is a barometer of Socio-economic situation -malnutrition, poor living conditions
• High burden of chronic cases, high infection rate, deaths, loss of work and wages
• Targets of reducing TB burden not achieved
• MDR, XDR, HIV are additional challenges
• Childhood TB needs attention.

The Global challenges for
elimination of TB by 2050
• Supply of funds for TB control at global/national levels (nearly 60% shortfall)
• Need for revolutionary technology for new medicines, vaccines, diagnostic tests (espfor latent infection),
• Genome research on TB may provide new tools.
• Long way to go for elimination

ThanksDr Shyam Ashtekar
SMBT Medical College, Dt Nashik
20 Nov 2015
This PowerPoint is available on slideshare.com
http://www.slideshare.net/ShyamAshtekar/epidemiology-and-public-
health-aspects-of-tb-in-india