Epidemiology and Geographical Variation of Myasthenia Gravis in the Province of Pavia, Italy
6
Fax +41 61 306 12 34 E-Mail [email protected] www.karger.com Original Paper Neuroepidemiology 2012;38:100–105 DOI: 10.1159/000336002 Epidemiology and Geographical Variation of Myasthenia Gravis in the Province of Pavia, Italy Cristina Montomoli a Antonietta Citterio b Giovanni Piccolo b Rita Cioccale a Virginia V. Ferretti a Cesare Fratti c Roberto Bergamaschi b Vittorio E. Cosi b a Section of Medical Statistics and Epidemiology, Department of Health Sciences, University of Pavia, b Neurological Institute ‘C. Mondino’ Foundation, and c Local Health Authority, Statistical Office, Pavia, Italy Introduction Myasthenia gravis (MG) is an autoimmune neuro- muscular disease caused by an antibody-mediated attack directed against acetylcholine receptors (AChR) at neu- romuscular junctions [1, 2]. A recent systematic review reported 3.0 per 100,000 inhabitants as the most accurate MG incidence estimate [3]. Although the disease can develop at any age, two peaks have been recognized in its incidence: the twenties in women and the over-fifties in men [2, 4]. In recent de- cades, however, several reports have noted that incidence of elderly-onset patients with MG has been increasing in the USA and in European countries [4–6]. Italian epidemiological studies, carried out in the 1980s and 1990s, reported prevalence rates of MG rang- ing from 7.7 to 11.1 per 100,000 inhabitants [7–11]. In the area under study, a previous analysis was carried out in 1984, reporting a prevalence of 6.2 per 100,000 inhabit- ants [12]. The analysis of the geographical distribution of a dis- ease is important as it can give clues to an etiological ex- planation and can test specific hypotheses about environ- mental risk factors. In recent years the Bayesian method- ology has been strongly encouraged as an alternative to the frequentist approach when dealing with epidemio- Key Words Myasthenia gravis Prevalence Bayesian mapping Italy Abstract Background and Aims: Previous studies have reported a prevalence estimate of myasthenia gravis (MG) from 7.7 to 11.1 per 100,000 inhabitants in Europe. Moreover, the study of the geographical distribution of MG should be useful to generate specific hypotheses. The aims are to estimate MG prevalence and to investigate its geographical variation in a delimited area in Northern Italy. Methods: The primary source of data was the MG database of the Neurological In- stitute of Pavia and all other sources of case collection in and outside the province. We adopted a Bayesian approach to analyze MG geographical variation within the finest geo- graphical grid. Results: We identified 119 live MG prevalent cases resident in the province of Pavia on December 31, 2008. The overall crude prevalence was 24 per 100,000 in- habitants. The Bayesian analysis identified a small cluster of higher MG prevalence in the northern area of the province. Conclusions: The estimated MG prevalence sets the prov- ince of Pavia among the high-risk areas. The identification of high/low MG risk areas deserves further investigation of ge- netic and environmental factors possibly related to a major risk of the disease in that area. Copyright © 2012 S. Karger AG, Basel Received: February 8, 2011 Accepted: December 12, 2011 Published online: February 24, 2012 Cristina Montomoli Section of Medical Statistics and Epidemiology, Department of Health Sciences University of Pavia, Via Bassi, 21 IT–27100 Pavia (Italy) Tel. +39 0382 987 533, E-Mail cristina.montomoli @ unipv.it © 2012 S. Karger AG, Basel 0251–5350/12/0382–0100$38.00/0 Accessible online at: www.karger.com/ned Downloaded by: Ondokuz Mayis Universitesi 193.140.28.22 - 4/29/2014 9:17:02 PM
-
Upload
vittorio-e -
Category
Documents
-
view
216 -
download
3
Transcript of Epidemiology and Geographical Variation of Myasthenia Gravis in the Province of Pavia, Italy

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Neuroepidemiology 2012;38:100–105 DOI: 10.1159/000336002
Epidemiology and Geographical Variation of Myasthenia Gravis in the Province of Pavia, Italy
Cristina Montomoli a Antonietta Citterio b Giovanni Piccolo b Rita Cioccale a
Virginia V. Ferretti a Cesare Fratti c Roberto Bergamaschi b Vittorio E. Cosi b
a Section of Medical Statistics and Epidemiology, Department of Health Sciences, University of Pavia, b Neurological Institute ‘C. Mondino’ Foundation, and c Local Health Authority, Statistical Office, Pavia , Italy
Introduction
Myasthenia gravis (MG) is an autoimmune neuro-muscular disease caused by an antibody-mediated attack directed against acetylcholine receptors (AChR) at neu-romuscular junctions [1, 2] .
A recent systematic review reported 3.0 per 100,000 inhabitants as the most accurate MG incidence estimate [3] . Although the disease can develop at any age, two peaks have been recognized in its incidence: the twenties in women and the over-fifties in men [2, 4] . In recent de-cades, however, several reports have noted that incidence of elderly-onset patients with MG has been increasing in the USA and in European countries [4–6] .
Italian epidemiological studies, carried out in the 1980s and 1990s, reported prevalence rates of MG rang-ing from 7.7 to 11.1 per 100,000 inhabitants [7–11] . In the area under study, a previous analysis was carried out in 1984, reporting a prevalence of 6.2 per 100,000 inhabit-ants [12] .
The analysis of the geographical distribution of a dis-ease is important as it can give clues to an etiological ex-planation and can test specific hypotheses about environ-mental risk factors. In recent years the Bayesian method-ology has been strongly encouraged as an alternative to the frequentist approach when dealing with epidemio-
Key Words
Myasthenia gravis � Prevalence � Bayesian mapping � Italy
Abstract
Background and Aims: Previous studies have reported a prevalence estimate of myasthenia gravis (MG) from 7.7 to 11.1 per 100,000 inhabitants in Europe. Moreover, the study of the geographical distribution of MG should be useful to generate specific hypotheses. The aims are to estimate MG prevalence and to investigate its geographical variation ina delimited area in Northern Italy. Methods: The primary source of data was the MG database of the Neurological In-stitute of Pavia and all other sources of case collection in and outside the province. We adopted a Bayesian approach to analyze MG geographical variation within the finest geo-graphical grid. Results: We identified 119 live MG prevalent cases resident in the province of Pavia on December 31, 2008. The overall crude prevalence was 24 per 100,000 in-habitants. The Bayesian analysis identified a small cluster of higher MG prevalence in the northern area of the province. Conclusions: The estimated MG prevalence sets the prov-ince of Pavia among the high-risk areas. The identification of high/low MG risk areas deserves further investigation of ge-netic and environmental factors possibly related to a major risk of the disease in that area.
Copyright © 2012 S. Karger AG, Basel
Received: February 8, 2011 Accepted: December 12, 2011 Published online: February 24, 2012
Cristina Montomoli Section of Medical Statistics and Epidemiology, Department of Health Sciences University of Pavia, Via Bassi, 21IT–27100 Pavia (Italy) Tel. +39 0382 987 533, E-Mail cristina.montomoli @ unipv.it
© 2012 S. Karger AG, Basel0251–5350/12/0382–0100$38.00/0
Accessible online at:www.karger.com/ned
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 4/
29/2
014
9:17
:02
PM

Epidemiology of MG in Italy Neuroepidemiology 2012;38:100–105 101
logical data [13–15] and Bayesian mapping could be a bet-ter key to modeling the geographical distribution of a dis-ease [16–19] .
In the present study we update the prevalence estimate of MG in the province of Pavia, Northwestern Italy, and analyze the geographical distribution of MG prevalence across the finest administrative geographical areas by means of a Bayesian statistical approach.
Subjects and Methods
Study Area The province of Pavia is located in Northwestern Italy and
covers 2,965 km 2 . The province is subdivided into 190 adminis-trative areas, called municipalities, and has 493,753 inhabitants (236,614 males and 257,139 females) according to the 2001 census [20] . It is a stable population: according to the previous census, the population in 1991 was 490,898 (234,428 males and 256,470 fe-males).
Case Ascertainment The primary source of case identification was the database of
the MG Center of the ‘C. Mondino’ Neurological Institute of Pa-via, which has been running since the early 1980s. Data were also drawn from the general hospitals in the province, from the neu-rological departments of the region and of the nearest provinces outside the region, from the most important neurological clinics, rehabilitation institutions, and hospitals in the rest of Lombardy, and from the registries of the local health unit (list of anticholin-esterase drug prescriptions, hospital discharge records, and mor-tality register). The clinical documents of the patients not pro-vided by our MG Center were reviewed by a senior neurologist of our group to verify the validity of the diagnosis.
The patients’ life status was checked through the mortality re-cords of the local health unit and through the municipality of-fices if patients had emigrated. Patients who had died before the prevalence day were excluded from the prevalence estimate.
We included all of the residents of the province of Pavia who were classified as MG according to the Osserman diagnostic cri-teria [21] for primary autoimmune disease. Secondary diseases were excluded. The study was approved by the local ethical com-mittee.
Statistical Analysis Descriptive statistics were used to describe collected variables.
The t test was used to compare quantitative variables. Prevalence rates were calculated per 100,000 inhabitants and
standardized to the Italian population using the direct method. Patients were considered prevalent if they were alive and resident in the area on December 31, 2008. We used as a denominator the population of the province of Pavia at the time of the 2001 census. The 95% confidence intervals (CI) were calculated from the Pois-son distribution approximation.
We analyzed the geographical variation of MG prevalence within the finest geographical grid for which the data were avail-able, that is 190 municipalities. We drew MG prevalence crude and Bayesian maps. The crude prevalence map was drawn calcu-
lating for each municipality the ratio between the area-specific number of MG resident cases and the resident population.
The Bayesian map was built using a hierarchical Bayesian model [22, 23] whose main idea is that each area-specific preva-lence is based on pooling information from neighboring areas to lower the uncertainty in sparsely populated areas. Methodologi-cal aspects of the Bayesian analysis applied to geographical map-ping are reported in previous articles [18, 19] . The Bayesian maps of prevalence were accompanied by a map of the posterior prob-ability (PP) that indicated whether the prevalence rate for each area was significantly lower or greater than a given reference val-ue [24] . The PP is the Bayesian equivalent of the p value [25] and is frequently used to measure the approximate level of confidence for a region to be a high- or a low-prevalence area. In our analysis, for example, we chose the median age-standardized MG preva-lence rate of the whole province of Pavia as a reference value to test whether each area-specific prevalence was different from the provincial values. We subdivided the range of PP (0–1) into five intervals ( ! 0.10, 0.10–0.25, 0.25–0.75, 0.75–0.90, and 1 0.90). A PP value higher than or equal to 0.90 strongly indicated that the area-specific risk was higher than the reference value, while a PP value less than or equal to 0.10 strongly indicated that the prevalence was lower than the reference value. In those areas where the PP value fell within the fourth interval (0.75–0.90), there was only an indication that the risk was higher than the reference value. Sim-ilarly, in those areas where the PP value belonged to the second interval (0.10–0.25), there was an indication that the prevalence was lower than the reference value. When the PP value fell within the central interval (0.25–0.75), there was not enough evidence to judge. In conclusion, the map of PP can be used to evaluate how confident we should be when we analyze a prevalence value that is much higher or lower than a reference value. We used Markov chain Monte Carlo techniques for computation implemented us-ing the WINBUGS software package [26, 27] .
Results
Clinical Characteristics In the period of 1985–2008, one hundred sixty MG-
affected individuals (94 females and 66 males) were resi-dent in the province of Pavia. 143 patients (89%) were followed by the MG Center of the Neurological Institute of Pavia.
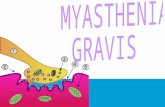
The mean age at onset was 49.4 8 20 years (range 3–85); it was significantly higher for men than for women (54 8 19 and 46 8 20 years, respectively, p ! 0.001). Among women, there was a clear peak of onset between the ages of 25 and 34 years. In men, there was evidence of a peak at 55–64 years ( fig. 1 ). The mean age at diagnosis was 50.0 8 20 years (range 11–85), suggesting a short de-lay between onset and MG diagnosis. The result is true for both sexes.
Forty-eight patients (30%) had one associated disease and 20 had two or more associated diseases (12.5%); 18
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 4/
29/2
014
9:17
:02
PM

Montomoli /Citterio /Piccolo /Cioccale /Ferretti /Fratti /Bergamaschi /Cosi
Neuroepidemiology 2012;38:100–105102
patients (11.2%) had an associated neoplasm and 15 (9%) had diabetes.
We found 49 MG cases with thymus abnormalities (32%), i.e. 16 males and 33 females. Histological analysis confirmed a diagnosis of thymoma in 41.5% of these cas-es. Most thymectomies have been performed in young patients, in particular from 25 to 44 years. No difference has been observed between thymectomy and sex.
Table 1 shows the distribution of the clinical classifica-tion of MG at onset and diagnosis. About 50% of patients show class I MG at disease onset, while at the time of di-agnosis the most frequent form is class IIb (42.2%).
Prevalence On prevalence day (December 31, 2008), we found 119
live MG patients in the province of Pavia, i.e. 46 males and 73 females. The crude prevalence was 24 per 100,000 inhabitants: 19 per 100,000 for males and 28 per 100,000 for females. The male-to-female sex ratio was 1: 1.6. Ta-ble 2 shows the distribution of MG prevalence by sex and age class. The Italian standardized prevalence rate was 22 per 100,000.
The mean age of prevalent patients was 58.3 8 17.0 years (range 18–89). Sixty-five patients (55%) were aged 50 years or younger at diagnosis (males 21/46, 46%; fe-males 44/73, 60%).
Mortality Forty-one patients (20 males and 21 females) died dur-
ing the study period (1985–2008). The crude death rate was 0.35 per 100,000. The final cause of death according to ICD IX was MG for 10 patients, malignant neoplasm for 13, diabetes for 4, cardiovascular diseases for 6, and other causes for the remaining 6 patients (cerebrovascu-lar disease, pneumonia, congenital hereditary muscular dystrophy, and other diseases of intestines).
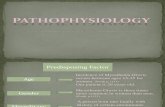
Geographical Distribution To analyze the geographical variations of MG preva-
lence across the 190 communes of the province, we built crude and Bayesian prevalence maps ( fig. 2 a, b, respec-tively). The maps had to be interpreted by considering that different shades of grey are proportional to the prev-alence value. Thus, the darker the area, the higher the prevalence of the disease estimated using patients resi-dent in each area. The crude prevalence map ranged from 0 to 258/100,000 inhabitants, while the Bayesian area-specific prevalence ranged from 20 to 46/100,000 inhab-itants. The comparison between the two maps shows that the crude map is extremely unhomogeneous and strong-
ly influenced by random variability ( fig. 2 a). This map was dominated by extreme prevalence values found in the areas with a scarce population. On the contrary, the Bayesian map ( fig. 2 b) was much smoother. The PP map ( fig. 2 c) revealed a northern area in the province where there is evidence (PP 1 0.90) and indication (0.75 ! PP ! 0.90) that the MG prevalence is greater than the median provincial rate while the risk is lower in the southern part.
Discussion
The present study has updated the MG prevalence in the province of Pavia compared to the findings obtained in the only previous epidemiological study carried out in 1984 in the same area, which reported an MG prevalence
0
5
10
15
20
25
30
35
40
10–14 15–24 25–34 35–44 45–54
Age (years)
55–64 65–74 >75
Pati
ents
(%)
Females
Males
Fig. 1. Distribution of age at onset in MG patients by sex.
Table 1. Classification of MG patients according to Osserman cri-teria at onset and diagnosis
Classification Onset Diagnosis
n % n %
I 75 46.6 47 29.2IIa 25 15.5 34 21.1IIb 53 33.5 67 42.2III – – – –IV – – 3 1.9Unknown 7 4.4 9 5.6
Total 160 100.00 160 100.00
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 4/
29/2
014
9:17
:02
PM

Epidemiology of MG in Italy Neuroepidemiology 2012;38:100–105 103
Table 2. M G prevalence (per 100,000) by age class and sex on December 31, 2008 (province of Pavia)
Age class Males Females T otal
cases prevalence 95% CI cases prevalence 95% CI cases prevalence 95% CI
15–24 years 1 4 1–32 1 5 1–33 2 5 1–1825–34 years 2 5 1–21 9 25 13–48 11 15 8–2735–44 years 6 15 7–34 10 26 14–49 16 21 13–3445–54 years 9 26 14–50 14 41 24–70 23 34 22–5155–64 years 5 16 7–39 11 33 19–60 16 25 15–4165–74 years 11 41 23–74 18 53 33–84 29 48 33–69>75 years 12 72 41–127 10 29 16–55 22 44 29–66
Total 46 19 14–26 73 28 22–36 119 24 20–29
0
0–6.5
6.5–13
13–19.5
>19.5a
<25
25–30
30–35
35–40
>40b
<0.10
0.10–0.25
0.25–0.75
0.75–0.90
>0.90c
Fig. 2. Map of the crude MG prevalence rate ( a ). Map of the Bayes-ian estimates of MG prevalence rates ( b ). Map of the Bayesian PP shows that each area-specific MG prevalence rate is higher than the median provincial MG rate ( c ).
Co
lor v
ersi
on
avai
lab
le o
nlin
e
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 4/
29/2
014
9:17
:02
PM

Montomoli /Citterio /Piccolo /Cioccale /Ferretti /Fratti /Bergamaschi /Cosi
Neuroepidemiology 2012;38:100–105104
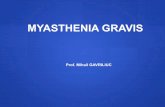
of 6.23 per 100,000 inhabitants [12] . The present estimate (24 per 100,000 inhabitants) is the highest reported to date [1–2, 4, 7–12, 28–32] ( fig. 3 ) and clearly indicates an increasing prevalence in the province of Pavia, in accor-dance with other studies showing that prevalence rates for MG have increased over time [32] . A possible explana-tion for the high prevalence we found with respect to oth-er studies is a greater reliability of the case-finding meth-od, which should allow the identification of almost all MG patients resident in the study area even if we cannot exclude that some patients remain unrecognized. More-over, the neurological Institute in Pavia has a long-stand-ing tradition in epidemiological surveys, and in particu-lar it is a referral center in Northern Italy for MG patients. This might have increased the likelihood of patients be-ing referred for observation.
The increased MG prevalence over time could be ex-plained by the improvement in the prognosis of the dis-
ease, by increased survival and better treatment, and by a higher detection rate due to the application of improved diagnostic tests and to the increased recognition of mild-er cases in which ocular symptoms predominate [2] . The low mortality rate (0.35 per 100,000) confirms the pro-gressively decreasing trend in the last decades, favored by the improvement of therapy and of respiratory intensive care, that allows MG patients to survive almost all epi-sodes of respiratory failure [2] .
The peculiarity of this study is the analysis of the geo-graphical distribution of the disease in small areas, as a map at a fine geographical grid can be more informative than a map at a coarser grid [33] . The geographical anal-ysis of the risk of disease is difficult, above all when the disease is rare and the area units are small. The use of a conventional statistical approach seems not to be suitable for this kind of analyses, as the map is strongly affected by random variation and is not interpretable from an ep-idemiological point of view. On the contrary, the Bayes-ian approach allows estimation of area-specific preva-lence rates and filtering out of the random variation from the estimated prevalence due to the small number of cas-es in each area, showing the true underlying variation of MG prevalence.
Bayesian disease-mapping models are essentially con-servative, with high specificity but low sensitivity [24] . This conservatism can be viewed as a positive feature, avoiding ‘false positives’ in the identification of risk ar-eas. As a consequence, we can be reasonably confident in the high risk cluster of MG showed by the PP map. We argue that the north/south difference in disease preva-lence could be related to the disparity between a very in-dustrialized area in the north and an agricultural setting in the south of the province.
These findings would suggest specific analytical stud-ies intended to detect genetic and environmental factors possibly related to a major risk of disease in some areas.
0
5
10
15
20
25
30
Cambrid
geshire
Stockholm
Estonia
Norway
Croatia
Denmark
Greece
Pavia
Trento
Sassari
Reggio Em
ilia
Ferrara
Prev
alen
ce p
er 1
00,0
00
Fig. 3. Comparison of prevalence estimates in European and Ital-ian areas.
References
1 Thanvi BR, Lo TC: Update on myasthenia gravis. Postgrad Med J 2004; 80: 690–700.
2 Grob D, Brunner N, Namba T, Pagala M: Lifetime course of myasthenia gravis. Mus-cle Nerve 2008; 37: 141–149.
3 McGrogan A, Sneddon S, de Vries CS: The incidence of myasthenia gravis: a systematic literature review. Neuroepidemiology 2010; 34: 171–183.
4 Robertson NP, Deans J, Compston DA: My-asthenia gravis: a population based epidemi-
ological study in Cambridgeshire, England. J Neurol Neurosurg Psychiatry 1998; 65: 492–496.
5 Casetta I, Groppo E, De Gennaro R, et al: Myasthenia gravis: a changing pattern of in-cidence. J Neurol 2010; 257: 2015–2019.
6 Schon F, Drayson M, Thompson RA: Myas-thenia gravis and elderly people. Age Ageing 1996; 25: 56–58.
7 Tola MR, Granieri E, Paolino E, et al: Epide-miological study of myasthenia gravis in the
province of Ferrara, Italy. J Neurol 1989; 236: 388–390.
8 D’Alessandro R, Granieri E, Benassi G, et al: Comparative study on the prevalence of my-asthenia gravis in the provinces of Bologna and Ferrara, Italy. Acta Neurol Scand 1991; 83: 83–88.
9 Ferrari G, Lovaste MG: Epidemiology of myasthenia gravis in the province of Trento (Northern Italy). Neuroepidemiology 1992; 11: 135–142.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 4/
29/2
014
9:17
:02
PM

Epidemiology of MG in Italy Neuroepidemiology 2012;38:100–105 105
10 Aiello I, Pastorino M, Sotgiu S, et al: Epide-miology of myasthenia gravis in Northwest-ern Sardinia. Neuroepidemiology 1997; 16: 199–206.
11 Guidetti D, Sabadini R, Bondavalli M, et al: Epidemiological study of myasthenia gravis in the province of Reggio Emilia, Italy. Eur J Epidemiol 1998; 14: 381–387.
12 Citterio A, Lombardi M, Vercesi S, Cosi V: La prevalenza della miastenia gravis in provin-cia di Pavia; in Cosi V, Citterio A (eds): Proc 5th Natl Neuroepidemiology Congr, Pavia, 1984, pp 157–159.
13 Bland JM, Altman DG: Bayesian and fre-quentists. BMJ 1998; 317: 1151.
14 Dunson DB: Commentary: practical advan-tages of Bayesian analysis of epidemiological data. Am J Epidemiol 2001; 153: 1222–1226.
15 Weinshenker BG: Bayesian analysis: what does it add to studies of the natural history of MS? J Neurol Sci 2001; 189: 1–2.
16 Olsen SF, Marcuzzi M, Elliott P: Cluster analysis and disease mapping – why, when and how? A step by step guide. BMJ 1996; 313: 863–866.
17 Elliot P, Wakefield JC, Best NG, Briggs DJ: Spatial Epidemiology – Methods and Appli-cations. Oxford University Press, 2000.
18 Montomoli C, Allemani C, Solinas G, et al: An ecologic study of geographical variation in multiple sclerosis risk in central Sardinia, Italy. Neuroepidemiology 2002; 21: 187–193.
19 Bergamaschi R, Montomoli C, Candeloro E, et al: Bayesian mapping of multiple sclerosis prevalence in the province of Pavia, North-ern Italy. J Neurol Sci 2006; 244: 127–131.
20 ISTAT: Pavia 14 Censimento generale della popolazione e delle abitazioni. 2001. http://www.istat.it/censimenti/popolazione (ac-cessed April 20, 2010).
21 Osserman KE, Genkins G: Studies in myas-thenia gravis: review of a twenty-year experi-ence in over 1,200 patients. Mt Sinai J Med 1971; 38: 497–537.
22 Besag J, York J, Mollié A: Bayesian image-restoration, with applications in spatial sta-tistics. Ann Inst Stat Math 1991; 43: 1–20.
23 Bernardinelli L, Montomoli C: Empirical Bayes versus fully Bayesian analysis of geo-graphical variation in disease risk. Stat Med 1992; 11: 983–1007.
24 Richardson S, Thomson A, Best N, Elliott P: Interpreting posterior relative risk estimates in disease-mapping studies. Environ Health Perspect 2004; 112: 1016–1025.
25 Meng CY, Dempster AP: A Bayesian ap-proach to the multiplicity problem for sig-nificance testing with binomial data. Bio-metrics 1987; 43: 301–311.
26 Gilks WR, Richardson S, Spiegelhalter D: Markov chain Monte Carlo in Practice. Lon-don, Chapman and Hall, 1996.
27 Lunn DJ, Thomas A, Best N, Spiegelhalter D: WinBUGS – a Bayesian modelling frame-work: concepts, structure, and extensibility. Stat Comput 2000; 10: 325–337.
28 Storm-Mathisen A: Epidemiology of myas-thenia gravis in Norway. Acta Neurol Scand 1984; 70: 274–284.
29 Christensen PB, Jensen TS, Tsiropoulos I, et al: Incidence and prevalence of myasthenia gravis in western Denmark: 1975 to 1989. Neurology 1993; 43: 1779–1783.
30 Zivadinov R, Jurjevic A, Willheim K, Cazza-to G, Zorzon M: Incidence and prevalence of myasthenia gravis in the county of the coast and Gorski kotar, Croatia, 1976 through 1996. Neuroepidemiology 1998; 17: 265–272.
31 Poulas K, Tsibri E, Kokla A, et al: Epidemiol-ogy of seropositive myasthenia gravis in Greece. J Neurol Neurosurg Psychiatry 2001; 71: 352–356.
32 Kalb B, Matell G, Pirskanen R, Lambe M: Epidemiology of myasthenia gravis: a popu-lation-based study in Stockholm, Sweden. Neuroepidemiology 2002; 21: 221–225.
33 Oöpik M, Puksa L, Lüüs SM, Kaasik AE, Jakobsen J: Clinical and laboratory-recon-firmed myasthenia gravis: a population-based study. Eur J Neurol 2008; 15: 246–252.
34 Phillips LH: The epidemiology of myasthe-nia gravis. Semin Neurol 2004; 24: 17–20.
35 Walter SD: The ecologic method in the study of environmental health. 1. Overview of the method. Environ Health Persp 1991; 94: 61–65.
Dow
nloa
ded
by:
Ond
okuz
May
is U
nive
rsite
si
19
3.14
0.28
.22
- 4/
29/2
014
9:17
:02
PM