Endocrine Glands Pathology
8
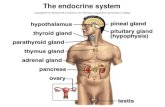
Eosinophilic pituitary adenoma (457) Pituitary gland ● Anterior lobe: ● Eosinophilic cell – adenomas secreting prolactin most common, then GH ● Excess GH in child → Gigantism. Adult → acromegaly. ● Slide: cells don't stick together (scattered cells), looks like cytology instead of tumor sample. Bright pink (eosinophilic) ● Basophilic cells (ACTH, MSH, TSH, FSH&LH) (tumors secreting those are rare) ● Chromophobic cells ● Posterior lobe: ● Modified glial cells (pituicytes) ● Axonal processes of hypothalamic nerve cells eosinophilic Scattered cells look like cytology Monomorphism ● Normal anterior pituitary contains different cell types for different hormones
description
Endocrine Glands Pathology
Transcript of Endocrine Glands Pathology

Eosinophilic pituitary adenoma (457)
Pituitary gland● Anterior lobe:
● Eosinophilic cell – adenomas secreting prolactin most common, then GH● Excess GH in child → Gigantism. Adult → acromegaly.● Slide: cells don't stick together (scattered cells), looks like cytology instead of
tumor sample. Bright pink (eosinophilic)● Basophilic cells (ACTH, MSH, TSH, FSH&LH) (tumors secreting those are rare)● Chromophobic cells
● Posterior lobe:● Modified glial cells (pituicytes)● Axonal processes of hypothalamic nerve cells
eosinophilic
Scattered cells look like cytology
Monomorphism● Normal anterior pituitary
contains different cell types for different hormones

Parathyroid adenoma (464)
● Usually unilateral● Produce PTH → hypercalcemia → symptoms
● Osteoporosis, depression, seizure, gallstone, nephrolithiasis● Benign tumor
Capsule between adenoma and normal tissue.
Some tendency to form follicles.Similar to normal parathyroid gland but more crowded.

Diffuse toxic hyperplasia of the thyroid (Graves disease) (452)● Autoimmune, more common in
female. Most common cause of hyperthyroidism.
● TSI (thyroid stimulating immunoglobulin) is main antibody. Acts as TSH.● Often autoantibodies cross react
with connective tissue around eye → exophthalmus
● Pretibial edema
Hyperthyroidism● Increase metabolic rate● Increased sympathetic activity● Sweating● Heat intolerance● Weight loss● Flushed skin (to increase heat loss)● Increased cardiac output● Tremor, hyperactivity, anxiety,
insomnia● Pretibial myxedema
Hypothyroidism● Decreased metabolism● Decreased sympathetic activity
○ Decreased sweating and constipation● Cold intolerance● Weight gain● Cold skin (decreased blood flow)● Decreased cardiac output
○ Shortness of breath○ Reduced exercise capacity
● Fatigue, slowed mental activity● Cretinism (in children)● Myxedema (in older children or adult)
● Plummer syndrome: multinodular goiter
● Diffuse, homogenous goiter:○ Grave's: hyperthyroidic goiter○ Lack of iodine: hypothyroidic
goiter
Scallop (or moth eaten) appearance. Adjacent parenchymal cells use colloid to produce thyroid hormone, producing empty space
Scattered follicles with a lot of parenchyma.Lymphocytes (dark purple cells in nodules)Parenchyma

Metastatic papillary carcinoma of the thyroid in the lymph node (461)
Malignant tumors of the thyroid:● Papillary – most common.
75% - 85%● Follicular – 10% - 20%● Medullary – 5%. Bad
prognosis, produces amyloid. Marker is calcitonin.● Scintigraphy with
radioactive iodine shows adenomas as cold areas.
● Anaplastic – <5%. Worst prognosis. Spreads viciously. Least common.
Slide:● small purple cells are
lymphocytes (they are present physiologically)
● cross section through papilla● nuclei appears pale (Orphan
Annie nuclei) (in cells lining the papillary)
● psammoma bodies (small calcification)● meningioma also has
psammoma bodies
Clear nuclei
Psammoma bodies
Cross section through papilla

Adrenal cortical adenoma (455)
● Adrenal cortical adenoma: incidentaloma, usually clinically silent
Slide:● Border is smooth (a thin layer)● Typical benign tumor.● Small islets (like normal
adrenal gland), but more crowded. Uniform nests. Dark pink cytoplasm. Small nuclei.
Intracytoplasmic lipid
Smooth border

Adrenal cortical carcinoma (456)
● Rare neoplasm. Large, invasive.● Hypercortisolemia → Cushing's● Might also cause Conn syndrome (too much aldosterone).● Usually asymptomatic until quite advanced (metastasis)
Slide● no uniform nests.● Sheets of solid cells not
forming structure● Atypia, Pleiomorphism
● some nuclei are much bigger, some with nucleoli. Dark nuclei.
● Mitosis.
mitosis

Pheochromocytoma (265)
● Stays within adrenal gland (medulla tumor). Produce norepinephrine and epinephrine (like normal medulla cells)● mostly benign, rarely malignant (atypical pheochromocytoma)
(metastasis)(10% malignant)● Symptoms related to sudden (or chronic) release of
catecholamines● Most common reason for secondary hypertension.● Catecholamine cardiomyopathy
● Fleshy appearance.
Slide:● Pale cells forming round nests
near border of tumor (“zellballen,” German for “cell balls”)
● Cells look paler than the ones from cortex.
Nuclei with “salt and pepper” chromatin typical for neuroendocrine tumors.

Well-differentiated neuroendocrine tumor (islet cell tumor, “APUD-oma”)(the pancreas) (458)
Well-differentiated neuroendocrine tumor● A lot of them comes from
Langerhans.● Gastrin, somatostatin, VIP
(vasoactive intestinal peptide), insulin, glucagon (rare). Neuroendocrine cells.
● Most islet cell tumors are small except gastrinoma, which grows aggressively.
Insulinoma● Β-cell tumors● Clinical triad of attack:
● Hypoglycemia when glucose level <50 mg/dL
● Confusion, stupor, loss of consciousness
● Precipitated by fasting or exercise, relieved by feeding or parenteral glucose
● Generally benign
Gastrinomas (Zollinger-Ellison syndrome)● Also likely in duodenum and
peripancreatic soft tissue (gastrinoma triangle)
● Extreme gastric acid secretion → peptic ulcer● Jejunal ulcers possible
VIPoma (Verner Morrison syndrome)● VIP (vasoactive intestinal
polypeptide)● Induces glycogenenolysis
→ hyperglycemia● Stimulate GI fluid secretion
→ secretory diarrhea
Pseudocapsule● Compressed parenchyma
of pancreas which became fibrotic
● Difficult to find on slide
Solid nest. Irregular.