Endocrine
58
Endocrine BIOL 242
Transcript of Endocrine

Endocrine
BIOL 242

Hormones• Classes (Chemical)

Hormones• Classes (Chemical)
• Amines

Hormones• Classes (Chemical)
• Peptides /proteins

Hormones• Classes (Chemical)
• Lipid soluble/steroids

Hormones• Classes (Chemical)
Prostaglandins and leukotrines
Secreted by all cells except RBC’s

Hormones• Mechanisms of Action

Hormones• Mechanisms of Action
• Steroids and Thyroid Hormone

Hormones• Hormone receptors

Hormones• Hormonal Interactions

Hormones• Tropic hormones
• ANS input –
• Humoral input

Hormones• Glands have a large blood supply• Glands are surrounded by connective tissue • May be paired glands or single structures

Hormones• Pathologies
Describe 3 hormone pathologies….

Hormones• Overview of functions• regulate chemical composition and volume of
internal environment: water and electrolytes• regulate metabolism and energy balance• regulate contraction of smooth and cardiac
muscle fibers• regulate homeostasis despite disruptions• regulate activities of immune system• integration of growth and development• contribute to basic processes of reproduction

Pituitary - Hypophysis CerebriLocation
• hypophyseal fossa of the sella turcia, just above optic chiasma
• pathology: tumor may cause visual problems

Pituitary - Hypophysis CerebriParts
• pars distalis (anterior) - releases about 7 hormones
• pars intermedia - unknown function in humans
• pars nervosa (posterior) - releases but does not produce – ADH and oxytocin

Pituitary - Hypophysis Cerebri• Regulated by neuron impulses & releasing
factors originate in hypothalamus
• hypophysis may also influence the hypothalamus
• releasing factors (RF) - often tropins
• inhibiting hormones - from the hypothalamus stops


Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• hGH - human growth hormone = somatotropin
– not fetal and early postnatal - rather children– adult aids in maintenance– periods of fasting or starvation
• Functions - stimulate protein synthesis – inhibit protein breakdown– increases rate amino acids enter cell– stimulates triglycerides into fatty acids and glycerol– retards use glucose --> ATP production– structurally and functionally like insulin– causes the production of insulin -like growth factors (IGF’s)– formation of cartilage and bone -->epiphyseal plates– decreases fat production– hGH and IGF --> decrease glucose fro ATP in most cells– allows for neurons to use glucose in times of sparity– may stimulate liver to release glucose into blood = insulin antagonist
• Pathologies = hyperglycemia - excess GH --> diabetes effect: high blood sugar– diabetes mellitus - lack of insulin activity– Pituitary dwarfism - hyposecretion or lack of receptors– Giantism - hypersecretion or in adults acromegaly
• Controlled: – GH releasing hormone (GHRH) - low blood sugar – GHIH - inhibits GH, secreted w/high blood glucose
• growing children - cyclic secretions - peaks early hrs of sleep cycle

Human Growth Hormone

Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• TSH - thyroid stimulating hormone =
thyrotropin• Functions - stimulate secretion of T3 & T4
(produced by thyroid)• Controlled: by thyrotropin secreting
hormone TRH from hypothalamus– release of TRH depends upon blood levels of
TSH,T3 and blood glucose and metabolism - negative feed back system


Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• FSH – Follicle Stimulating Hormone
– from anterior pituitary to ovaries/testes
• Functions - initiates dev of egg-containing follicles– influences estrogen secretions– Males - stimulates sperm production in testes
• Controlled: Gonadotropin releasing hormone (GnRH) from hypothalamus FSH release– FSH release suppressed by estrogen and testosterone -
negative feed back system


Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• LH – Leutinizing Hormone• Functions - w/FSH estrogen and
releases 2nd oocyte: ovulation– Form of corpus luteum and secretion of
progesterone– Prepare uterus for egg implant and mammary
glands for milk production– Male interstitial cells --> testosterone
• Controlled: GnRH


Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• PRL - Prolactin• Functions - initiate and maintain milk production
– mammary glands are primed by estrogen, progesterone, glucocorticoids, hGH, T4, insulin
– not ejection which is oxytocin
• Controlled: hypothalamus - PIH or dopamine – as estrogen and progesterone fall --> dopamine secretion– just before menstruation– PRH - during pregnancy causes PRL release– nursing decreases PIH release
• Pathologies – females - too much = loss of menstruation– males - too much = impotence


Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• ACTH - adrenocorticotropic hormone• Functions - stimulates growth of adrenal cortex
– stimulates release of glucocorticoids by adrenal cortex
• Controlled: CRH - corticotropin releasing hormone from hypothalamus– stress related– low blood sugar, physical trauma, macrophage
interleukin release– also negative feedback from blood levels of
glucocorticoids


Pituitary - Hypophysis CerebriAnterior Pituitary Hormones• MSH - melanocyte stimulating hormone• Functions - increase in skin pigment –
amphibians– humans - ? Appetite and sexual arousal?– does seem to darken human skin
• Controlled: CRH - corticotropin releasing hormone– dopamine inhibits


Pituitary - Hypophysis Cerebri• Posterior Pituitary Hormones - stores and releases does
not make– made in cell bodies of neurosecretory cells - moved to axon
terminals• ADH – antidiuretic hormone• Function - decreases urinary output, retain water
– raise BP - constriction of arterioles = vasopressin• Controlled: osmoreceptors in hypothalamus
– variety of factors affect blood levels of hormone– For example body level of hydration
• Pathologies = Diabetes insidus – hyposecretion of ADH or kidneys do not respond to ADH =
nephrogenic DI– treat with less salt in diet and some diuretics (?) work– large amount of urine, treat w/ADH


Pituitary - Hypophysis Cerebri• Posterior Pituitary Hormones - stores and releases does
not make– made in cell bodies of neurosecretory cells - moved to axon
terminals• Oxytocin - • Function - uterus and breasts during childbirth
– Contraction of smooth muscles: delivery and milk let-down– maternal instincts in males and nonpregnant females– sexual pleasure– inhibits release of prolactin inhibiting hormone
• Controlled– stretch receptors in cervix hypothalamus– nursing infant
• Given in synthetic form to induce labor or increase uterine tone


ThyroidLocation - neck between C5-C7Parts: a. Two lateral lobes with
a connecting isthmusRegulated by TSH from pars
distalis to produce thyroxinpathologies - malignant and
benign tumorsif removed need hormone supplements
Hormones - stored up in large amounts: up to a 100 day supply

• Formation - thyroid cells trap iodine– I binds to tyrosine of thyroglobulin molecule (TGB)– I'd TGB forms T3 and T4– T3 and T4 are lipid soluble and enter blood – T3 < T4, but T3 more potent– T4 may T3 (- one I)
Thyroid – thyroid hormones

Thyroid – thyoid hormonesFunctions
oxygen use and BMRproduction of ATP from O2
increases body temperaturecellular metabolism: protein synthesis, lipolysis, use of ATP glucos, lower cholesterolall lead to heat productiongrowth development and maturation
especially Nerve tissuemodulate NS - receptors of NE and epi
receptors in nuclei of cellsT3 more affinity than T4

Thyroid – thyroid hormones• Controlled: level of iodine, blood levels of T3 and T4
– negative feedback via hypothalamus and anterior pituitary– low T3 --> TRH secreted from ant pituitary --> TSH release
• Pathologies– Cretinism - hyposecretion of T's – dwarfism– Grave's - hypersecretion, enlarges thyroid– autoimmune: body makes Ab that mimic TSH edema behind eyes– Goiter - enlarged thyroid, symptoms of many thyroid problems– absence in early infancy under dev NS: mental retard– absence in adults --> decrease alertness
• Calcitonin - CT: produced by C cells• Functions - regulates calcium and
phosphate levels in blood• inhibits bone break down
and uptake of Ca in bones• limits action of osteoclasts
in bone•

Thyroid – calcitonin• produced by C cells
• Functions - regulates calcium and phosphate levels in blood– inhibits bone break down and uptake of Ca in
bones– limits action of osteoclasts in bone

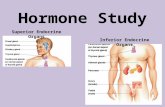
Parathyroid• = 4 glands• Location
– Within the fibrous capsule of the thyroid– Posterior surface of each lateral lobe - super and inferior parathyroid
gland• Hormone = PTH • Functions
– regulates calcium and phosphate levels– breakdown of Ca in bone and increases blood Ca– increases action of osteoclasts in bone– increases kidney release of Ca
• Controlled: blood levels of Ca• Pathologies
– Hyperparathyroidism - neurons depolarize w/o stimulus• due to Ca deficiency• causes tetany

Pancreas• Pancreas -exocrine and endocrine gland
• Location - flattened, posterior and inferior stomach– Parts
• Islets of Langerhans • Some cells in the parenchyma

PancreasHormones• Glucagon - produced by A cells or alpha cells
– post absorb state - prevents glu from falling too low
• Function - raises blood sugar - target = liver– glycogen glucose glycogenolysis– lactic acid and amino acids glucose– promote Fatty Acids as alternate Energy source– production of Acetyl CoA and ketones
• = glucose sparing• glucose --> blood
• Controlled– negative feedback from blood glucose levels– inhibited by glucose levels of absorb state and high PS activity– inhibited when beta cells are active

PancreasHormones• Insulin - produced by B cells or beta cells
– absorptive state• Function - lowers blood sugar
– transport of glucose from blood into cells especially muscles– glucose --> glycogen for storage– "hormone of abundance"– amino acids --> cells and protein synthesis– glucose --> fatty acids– slows gluconeogenesis– glucose into all cells except liver, brain, RBC's & renal medulla
• Controlled: negative feedback from blood glucose– < 50 mg/dl --> stop insulin production– > 300 mg/dl = max secretion of insulin– release depends upon glucose receptors on beta cells– increase carbohydrates diet --> more glucose receptors on beta cells– decrease carbohydrate diet --> less glucose receptors– beta cells also stimulate by AA, gastric inhibiting hormone, cholecystokinin
(CCK), and increase PS activity


PancreasHormones• Somatostatin (GHIH) - produced by Delta cells or D cells• Function - inhibits release of insulin and glucagon
– decrease GI motility and secretion– decrease pancreatic secretion– slows all aspects of digestion and absorption– prolongs absorption - more time for body to handle incoming
nutrients• Controlled
– release increased by increase glucose and amino acids in plasma
– inhibited by pancreatic polypeptide• Pathology
– Hypersecretion --> diabetes mellitus eventually

PancreasHormones• Pancreatic polypeptide
– produced by F cells
• Function– regulates release of pancreatic digestive enzymes– decreases somatostatin
• Controlled– release: meals w/protein, fasting, exercise,
hypoglycemi– inhibited: somatostatin, elevated blood glucose

Pancreas• Diabetes Mellitus - hormonal deficiency of the B cells to produce
insulin• Cellular famine in the midst of plenty
– blindness, atherosclerosis, poor circulation (gangrene)– glucose enters urine because too much, also urea and ketones
• Type I - absolute deficiency of insulin - insulin dependent– 20% of infected autoimmune disorder– no glucose allowed to enter cells
• ketoacidosis from fatty acids --> ATP• Type II - less sensitive to insulin - not insulin dependent
– fewer receptors or receptors no longer sensitive– Juvenile or Adult onset 80% affected– Hyperglycemia
• Gestational diabetes - gone after delivery– due to changes in glucose metabolism during pregnancy– may be hazardous to the fetus

Adrenal• Location:
– above kidneys - no connection between kidneys and glands
• Parts
– Cortex - produces corticosteroids, small amts of male sex hormone
• hormones are essential for life

AdrenalHormones - cortex• Mineralcorticoids - or Aldosterone is the main
one• Functions - control water and electrolyte
homeostasis (Na+ & K+)– reabsorption of Na+ in kidney, and K+ release in urine– --> more Na+ in blood --> water retention– also prevents acidosis by releasing H+ into urine
• Controlled: renin-angiotensin pathway - detects decrease in blood volume from dehydration– concentration K+ increases --> aldosterone secreted
•

AdrenalHormones - cortex• Glucocorticoids - cortisol (mostly),
corticosterone, and cortisone• Functions - regulate metabolism and resistance
to stress– protein catabolism, lipolysis– make enough ATP – gluconeogenesis– anti-inflammatory, inhibit cells that aid immune
responses– maintain blood glucose levels
• Controlled - corticotropin releasing hormoneAdrenocorticotropic Hormone (ACTH)– released from anterior pituitary

AdrenalHormones - cortex
• Gonadocorticoids - estrogens and androgens (testosterone)
• Steroids are regulated by ACTH from the pars distalis

AdrenalParts: Medulla
produces catecholamines
epi and norepi
Sympthetic end organ w/sympathetic impulses cause release of hormones

GonadsLocations
ovariestestes
Hormones• Ovaries: estrogen and progesterones influenced by pars
distalis– Functions - develop and maintain female sex characteristics– reproductive cycle, maintain preg, prepare lactation
• Testes: testosterone an androgen– Functions - develop and maintain male sex characteristics– production of sperm

Pineal - epiphysis cerebriLocation - roof of third ventricle
covered w/pia mater and masses of neuroglia
Hormones• Melatonin - produced during darkness =
biogenic amine– Functions: lack of sleepiness
• diurnal: day/night cycle
– Controlled: stops when light hits retina hypothalamus superior cervical ganglion
• sympathetic postganglionic fibers end here
– Pathologies - Seasonal affective disorder

Thymus• Hormones: thymosin, thymic humoral
factor, thymic factor, thymopoietin
• Functions: immunity T cells and B cells/lymphocytes