Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy

of 26
Transcript of Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
1/26
5EMOTIONS AN DPERSONALITY DISORDERSTh e pain of acute or chronic negative affect lies at the heart of thosepatterns of emotionality now termed the affective and personalitydisorders. -M. J. Mahoney
According to the psychoevolutionary heory of emotion, and par-ticularly the derivatives model, personality disorders are extreme ex-pressions of certain personality traits. The eight primary emotions areassociated conceptually with certain families of personality traits(such as shyness, quarrelsomeness, and gloominess). When a traitis expressed in an extreme form, we tend to label the individual pos-sessing that trait by a diagnostic term (e.g., dependent, antisocial,ordysthymic).Other characteristics are also included in a diagnosis ofpersonality disorder, but extreme forms of emotions and traits are thebasic elements. The theory provides a series o hypotheses aboutthe connections among these three domains.If these hypotheses are plausible, then one might expect per-sonality disorders to have a circumplex structure similar to those thatapply to personality and emotions. This chapter provides a review ofthe empirical literature on the comorbidity of personality disorders,which suggests that a circumplex is an appropriate description of thesimilarity relations of such disorders. Research shows the applicabil-ity of the circumplex to personality disorders, and some of the impli-cations of this view are explored.
The psychoevolutionary theory of emotion makes a number of pre-dictions and generates a number of hypotheses. For example, the theory
81
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
2/26
predicts a circumplex or circular ordering of similarity of emotion concepts.This has been demonstrated empirically by Plutchik (1980a), Russell(1989),G. A. Fisher et al. (1989, and others.
One of the hypotheses generated by the theory is that personalitytraits should also have a circumplex structure, and there is much supportingevidence for this idea (see Plutchik Conte, 1997). Another derivativehypothesis is that personality disorders are extreme forms of certain per-sonality traits and should therefore have a similar circumplex structure.This hypothesis applies only to the personality disorders and not to psy-chiatric diagnoses in general.A number of studies have examined the degree to which personalitydisorder diagnoses can be related to one another by means of a circumplexstructure. In this chapter review some of those studies.
THE RELATION BETWEEN EMOTIONS ANDPERSONALITY DISORDERSThe 4th edition of the Diagnostic and Statistical Manual of Mental Dis-
orders (DSM-IV) identifies a personality disorder asan enduring pattern of inner experience and behavior that deviatesmarkedly from the expectations of the individuals culture, is pervasiveand inflexible, has an onset in adolescence or early adulthood, is stableover time, and leads to distress or impairment. (American PsychiatricAssociation, 1994, p. 629)
I hypothesize that the personality disorders that have been identified bypsychiatrists are extreme forms of personality traits, which are in turn re-lated to the basic emotions. An examination of several personality disordersillustrates these ideas.
The emotion of fear is a highly adaptive state that functions to protectan individual from danger by stimulating withdrawal and escape. Whenstates of fear are persistent in an individual, such patterns of behavior arerecognized as personality traits and are described with the labels shy, timid,withdrawn, or submissive. Labels of this sort do not necessarily imply ab-normality, but they are usually considered to be part of the broad spectrumof personality traits seen in any large population. If, however, such person-ality traits become extreme and function as a dominant aspect of a personsway of relating to other people, clinicians may be inclined to use a diag-nostic term taken from the system of personality disorders to describe thetrait. Such an individual might be diagnosed as dependent, avoidant, orpassive.Similarly, the emotion of anger is a highly adaptive state that func-tions to stimulate attacks on barriers to the satisfaction of an individuals82 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
3/26
TABLE 5.1Hypotheses About the Connections Between Emotional Feelings,Personality Traits, and Personality Disorder DiagnosisEmotion Personality trait Personality disorder
Fear Shy, timid, nervous Dependent, avoidantAnger Qu arre lsome, grouchy, critical, sarcastic Antisocial, narcissisticSadness Gloomy, apathetic, lonely DysthymiaJOY Sociable, generous, sympathetic Hypomania, maniaDisgust Hostile, scornful, rebellious, critical ParanoidAcceptance Trustful, tolerant, contented HistrionicExpectation Curious, orderly, controlling Obsessive-compulsiveSurprise Indecisive, impulsive Borderline
needs. When states of anger occur frequently in an individual, such pat-terns of behavior are recognized as personality traits and are described bysuch labels as quarrelsome, grouchy, critical, or sarcastic. Labels of this sortdo not necessarily imply abnormality, but they are considered to be part ofthe broad spectrum of personality traits seen in any large population. If,however, such personality traits become extreme and function as a domi-nant aspect of a persons way of relating to other people, clinicians tendto describe the state using a diagnostic term taken from the system ofpersonality disorders; in this case, such terms as antisocial or narcissisticmight seem appropriate.The same reasoning may be applied to each of the eight basic emo-tions. Sadness becomes associated with the traits of gloominess, apathy , orloneliness and in an extreme form with dysthymia. Joy is related to sociability,generosity, or sympathy and in an extreme form to hypomania or mania.Disgust is connected to the traits of hostility, sc m fd m s s, or dejknce and inan extreme form to the diagnosis of paranoia. Acceptance is associated withthe traits of trustfulness, tolerance, and gullibility, and in extreme forms it isrelated to the diagnosis of histrionic. The emotion of expectation or interestis related to the traits of curiosity, orderliness, and control, but in extremeform it may be diagnosed as obsessive-compulsive. Finally, the emotion ofsurgnse may be related to the personality traits of indecisiveness or impulsivityand to the diagnosis of borderline personality disorder. It should be noted thatthese suggestions are in the nature of hypotheses, and the reader may dis-agree with one or more of the proposed connections. One justification forthese suggestions is that they form part of a large nomological network,which taken together has good explanatory power and has implications forresearch and clinical theory. These hypotheses are summarized in Table5.1.
Similar ideas have been proposed by others. For example, Leary andCoffey (1955) have suggested that the traits of being cooperative andoverly agreeable are associated with the hysterical personality disorder; that
EMO TIONS AN D PERSONALITY DISORDERS 83
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
4/26
being trustful and dependent are associated with the phobic personalitydisorder; that modest, self-punishing traits are associated with the obsessivepersonality disorder; that skeptical, distrustful traits are connected with theschizoid personality disorder; and that critical, aggressive traits are part ofthe psychopathic personality disorder. In 1982, Wiggins suggested a similarset of relations between personality traits and personality disorders, andthese ideas were further elaborated by Kiesler (1986) and Benjamin (1993).Table 5.2 summarizes these ideas.
There is only limited agreement among these writers, but this maybe because our conceptions of personality disorders have changed consid-erably over the past 40 years. The key idea is that all schemas recognize aconnection between personality traits and personality disorders.
THE PROBLEM OF COMORBIDITYMany psychiatric patients appear to experience a number of psychi-
atric disorders simultaneously. The term comorbdty was introduced to char-acterize this situation.Empirical Studies
Many researchers have found evidence of such comorbidity. For ex-ample, in a study of 231 consecutive patient admissions, Herpertz, Stein-meyer, and Sass (1994) found that 41% had more than one personalitydisorder diagnosis according to DSM-III-R (American Psychiatric Asso-ciation, 1987). Labouvie, Miller, Langenbucher, and Morgenstern (1997)reported extensive overlap between Axis I and personality disorder diagnoses in a sample of 366 substance abusers. Marshall (1996) provided asummary of the literature showing comorbidity between panic disorder,social phobia, depression, and dependent and avoidant personality disor-ders.
In a study of 40 patients with obsessive-compulsive disorder, mostwere also found to have another Axis I diagnosis, but with an interestingvariation in the frequency of each personality disorder. The comorbidityfigures reported were as follows: avoidant (52%), dependent (40%), histri-onic (20%), paranoid (20 ) , narcissistic (8%), schizotypal (5 ) , andpassive-aggressive ( 5 ) . In addition, almost 6 out of 10 of the patientshad two or more personality disorder diagnoses (Rodriguez Torres DelPorto, 1995). These observations suggest that comorbidity is not an all-or-nothing phenomenon but can exist in degrees. The same point was madeby Corruble, Ginestet, and Guelfi (1996), who reported on the basis of anextensive review of the literature that 20-50% of inpatients and 50-85%of outpatients with a current major depressive disorder have an associatedpersonality disorder. Those with such personality disorders are likely to be84 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
5/26
TABLE 5.2Hypothesized Relations Between Personality Traits andPersonality DisordersTraits Personality Disorder
Leary and Coffey (1955)Cooperative, overly agreeableTrustful, dependentModest, self-punishingSkeptical, distrustfulCritical, aggressiveAmbitious, dominantWarm, agreeableUnassuming, ingeniousLazy, submissiveAloof, introvertedCold, quarrelsomeArrogant, calculatingDominant, assuredExhibitionistic, sociableFriendly, warmTrusting, deferentSubmissive, unassuredInhibited, detachedHostile, coldMistrusting, competitive
Benjamin (1993)Wall off, ignore, self-neglectSeparate, protect, blame, attackRecoil, self-neglectSeparate, blame, ignoreTrust, affirm, protect, blame, attack, self-attack,self-neglectTrust, wall off, protect, blame, self-attackSeparate, protect, blame, attack, ignore,self-blame, self-neglectSulk, recoil, wall off, blame, self-control,self-blameTrust, submit, sulk, self-blame, ignore,self-control, self-blame, self-neglect
Wiggins (1982)
Kiesler (1986)
HystericalPhobicObsessiveSchizoidPsychopathicCompulsiveHistrionicDependentPassive-aggressiveSchizoidParanoidNarcissisticNarcissisticHistrionic, narcissisticBorderlineBorderlineAvoidant, dependentSchizoid, schizotypalParanoid, antisocialParanoid, schizotypalSchizoidParanoidSchizotypalAntisocialBorderlineHistrionicNarcissisticAvoidantObsessive-compulsive
Note. From Personality Disorders and the Interpersonal Circumplex by T. A. Widiger and S.Hagemoser in Circumplex Models of Personalityand Emotions,edited by R Plutchik and H. R.Conte 1997, pp. 301. 303, 305, 310, Washington DC:American Psychological Association.Copyright 1997 by American Psychological Association. Reprinted by permission.
called borderline in about 30% of the cases, histrionic in about 20% of thecases, antisocial in about 10% of the cases, and narcissistic in less than5 . Again, comorbidity is a matter of degree.
In a study of 404 adult outpatients with major depression, Fava et al.(1996) found that most had one or more comorbid diagnoses of avoidant,histrionic, narcissistic, and borderline disorders. Klein, Lewinsohn, and
EMOTIONS AND PERSONALITY DISORDERS 85
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
6/26
Seeley (1996) studied a sample of 1,709adolescents and found that thosewith hypomanic traits were also more likely to attempt suicide, have re-current major depression, and show disruptive behavior. Spalletta, Troisi,Saracco, Ciani, and Pasini (1996) found that almost half of the patientswho had dysthymia also had a personality disorder.
Grilo, Becker, Fehon, Edell, and McGlashan (1996) reported thatadolescent patients with co-existing conduct and substance use disorderswere likely to have a comorbid borderline personality disorder as well.Okasha et al. (1996 reported comorbidity between borderline personalitydisorder and somatoform disorder, as well as between generalized anxietydisorder and avoidant personality disorder.
In a large group of outpatients, those with dependent personality dis-order were likely to have comorbid social phobia and borderline as well ashistrionic traits (Reich, 1996 . Similarly, Loranger (1996) reported thatdependent patients were more likely than those with other personalitydisorders to have major depression and bipolar disorder. In a sample of 200patients, Skodal et al. (1995) found that panic disorder was associated withdependent, borderline, and avoidant personality disorders and that socialphobia was associated with avoidant personality disorder.Implications
How should comorbidities be interpreted? Plutchik and Van Praag1998) have pointed out that anxiety, depression, aggression, impulsivity,and suicidality are not distinct and unrelated entities; there is considerablecomorbidity among these and other states. Of interest is that such com-orbidity shows a special pattern, one that might be called a similaritysmture. For example, anxiety and depression, whether considered as emotionsor as diagnoses, are often found together in the same individuals. Whenmedications reduce one of these symptoms in a patient, there is a highprobability that the other will also be reduced. Such high comorbidity isless likely to be found between anxiety and aggression or between depres-sion and impulsivity. The evidence suggests the existence of degrees ofcomorbidity and even the possibility of negative comorbidity. This wouldmean that having one particular personality disorder decreases the likeli-hood of having a different specific one.If the above conclusions are valid, then the idea of degrees of com-orbidity can be represented by a circumpkx-a circular order of elementsthat expresses certain types of relations. These include the relations ofsimilarity and polarity. If the elements being considered vary in degree ofsimilarity to one another (as do emotions, personality traits, and diagnoses)and show polarities (such as joy vs. sorrow, dominance vs. submission,antisocial vs. avoidant behavior), then a circle as an analog model may beused to represent these relations. Statistically, a set of correlations among86 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
7/26
these elements should show systematic increases and decreases in the de-gree of correlation between the elements, depending on their degree ofconceptual closeness (Plutchik, 1997).
Carson (1996) proposed a similar view of the circumplex as a seamlessset of elements in a circle whose borders blend and interpenetrate. Hequestioned the persistent tendency to reify the DSM taxonomic system incategorical terms and suggested that the categories reflect a desire for aprecision we do not have and cannot get (p. 243).
Carson cited the chairperson and research coordinator of the DSM-IV Task Force (Frances, Widiger, Fyer, 1990), who have noted that theoccurrence of comorbidities is largely a function of the number of diag-nostic categories that are assumed to exist. A large number of diagnosticcategories leads to a large number of comorbidities, many of which areartifacts of the system. An example that Carson cited is the proposed di-agnosis of double depression, which refers to the co-occurrence of mildchronic plus major depressive features (Keller Shapiro, 1982). He con-cluded that clinical practice is not helped by placing patients into arbitraryand overlapping diagnostic categories.
Beginning in the 1970s, researchers have attempted to apply the cir-cumplex concept to a variety of domains including emotions, personalitytraits, and personality disorders. Much of this work is reviewed in the bookCircumplex Models of Personality nd Emotions (Plutchik Conte, 1997).
AN EMPIRICAL CIRCUMPLEX OF PERSONALITY DISORDERSDiagnostic Clusters
Over the years a number of attempts have been made to describe therelations among the personality disorders by means of a circumplex. Oneof the problems has been the lack of a consistent terminology for person-ality disorders as described in the DSM series. For example, DSM-11 (1968)listed 10 personality disorders;3 of them explosive, asthenic, and inadequate)were later dropped. Plutchik and Platman (1977) studied the remaining 7-compulsive, cyclothymic, hysterical, paranoid, passive-aggressive, schizoid,andsociopathic-for degree of similarity. To these they added one more term:well-djusted.
Twenty psychiatrists were asked to think of patients who had beendiagnosed with each of the labels and to select emotion words (such asgloomy, sociable or impulsive) that described each patient. The psychiatristschoices were scored in terms of the eight basic affect dimensions of theEmotions Profile Index (Plutchik Kellerman, 1974). This procedure pro-vided an emotion profile for each diagnosis.
EMOTIONS AND PERSONALITYDISORDERS 87
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
8/26
II FACTOR IIII
Paranoid
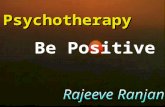
figure 5.1. Factor Analysis Based on Psychiatrists Definitions of DiagnosticTerms. From Personality Connotations of Psychiatric Diagnoses, by R.Plutchik and S. R Platman, Journal of Nervous and Mental Disease, 165, p.421. Copyright 1977 by Lippincott, Williams, Wilkins. Reprinted by permission.
These profiles were then intercorrelated for all possible pairs of di-agnoses. The matrix of intercorrelations was then factor analyzed using theprincipal-components method, and it was found that the first two factorsaccounted for 91% of the variance. The factor loadings for each diagnosiswere plotted using the first two axes, which resulted in the circumplexshown in Figure 5.1.
This figure indicates that personality disorders fit into a circumplexstructure, with cyclothymic opposite compulsive, hysterical opposite schizoidand well-adjustedopposite paranoid. Some spaces are found that could rep-resent other personality disorders, not defined in DSM-11 but which appearin the third edition of the DSM (DSM-III; American Psychiatric Asso-ciation, 1980) and DSM-IV. I t is important to emphasize that this circular88 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
9/26
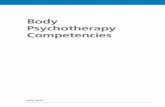
AMBITIOUS-DOMINANT
SchizoidNTROVERTED Dependent UNASSUMING-INGENUOUSassive-AggressiveAZY-
SUBMISSIVEfigure 5.2. Wigginss 1982 Interpersonal Types Outside Perimeter) andCorresponding Diagnoses Inside Perimeter). From Structural Approaches toClassification, by R. K. Blashfield, in Contemporary Directions inPsychopathology: Toward the DSM-IV p. 334), dited by T. Millon and G. L.Klerman, New York: Guilford Press. Copyright 1986 by the Guilford Press.Adapted with permission.
configuration of diagnostic labels is not a sign of psychiatrists fuzzy ideasabout diagnoses; it reflects instead the clear recognition of the overlap oftraits associated with each diagnosis. Another way to conceptualize thisidea is that diagnostic labels represent implicit probability estimates of thelikelihood of observing certain clusters of traits.
Another early attempt to provide a circumplex structure for thepersonality disorders was made by Blashfield (1986) and was based onWigginss (1982) interpersonal types. This is shown in Figure 5.2. Wigginslisted eight personality disorders and arranged them at equal distancesaround the perimeter of a circle on theoretical (rather than empirical)grounds. In this circumplex, histrionic is opposite paranoid, narcissistic isopposite dependent, and schizoid is opposite hypomanic. The term hypo-mnic was not listed in DSM-II or DSM-III, but Wiggins believed thatthe gregarious-extraverted personality dimension in its extreme form shouldlead to the hypomanic personality disorder.
As stated earlier, one of the problems involved in studying personalityEMOTIONS AND PERSONALZTY DISORDERS 89
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
10/26
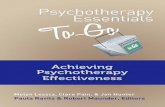
disorders is the changing terminology from one DSM edition to another.In addition, children have been labeled with somewhat different terms thanhave adults. In DSM-111, for example, children are said to have schizoid,awoidunt, conduct, oppositional,or identity disorders, whereas adults may haveany one or more of the 11 personality disorders: paranoid, schizoid, schizo-typal, histrionic, narcissistic, antisocial, borderline, awoidunt, dependent, compul-siwe, or pussiwe-aggressiwe.A study carried out with one of my colleagues provided data thatcould be used to establish an initial approximation to a circumplex orderfor diagnoses in preadolescent psychiatric patients (Pfeffer Plutchik,1989). We obtained DSM-111-R diagnoses for 106 preadolescent psychi-atric inpatients, 101 preadolescent psychiatric outpatients, and 101 non-patient preadolescents. We found that children with a diagnosis such asconduct disorder were also given other diagnoses with varying frequencies.For example, of those 66 children who were diagnosed as having a conductdisorder, 51%were also diagnosed as having a borderline personality dis-order, 39% as having a specific development disorder, 23% as having anattention deficit disorder, and 21 as having a dysthymic disorder. Thesame type of overlap analyses was done for each disorder. The approxi-mation to a circumplex structure is shown in Figure 5.3. This model ismeant to represent the relative, not absolute, positions on a similarity scaleof the different diagnoses. Such a circumplex reveals which diagnoses aremost difficult to differentiate from one another, as well as those that areeasy to distinguish.In another study designed to apply the circumplex idea to personalitydisorders, Plutchik and Conte (1997) used a modified paired comparisonprocedure. We asked 16 experienced clinicians to rate the degree of simi-larity or dissimilarity of the 11 DSM-111-R Axis I1 personality disorders.To this list we added three other categories: sadistic, self-defeating, anddysthymic personality disorders. (This latter disorder simply represents anexpression of the idea that many patients have pervasive patterns of de-pressive cognitions and behaviors that are, in fact, personality traits. Ben-jamin, 1993, agreed with this idea and has described the characteristics ofa new category, which she called depressive personality disorder.
When the clinicians made their similarity-dissimilarity judgments,they were not given single diagnostic labels (e.g., histrionic, paranoid, ornarcissistic because of the ambiguities associated with such labels. Insteada brief descriptive paragraph was written for each personality diagnosisbased explicitly on the criteria given in DSM-111-R. A separate group ofclinicians rated the adequacy of the descriptions, and a few changes weremade to increase the validity of the descriptions. The judges were askedto compare the written descriptions of the personality disorders for simi-larity on a scale ranging from +3 (the two descriptions are identical inmeaning) to -3 (the two descriptions are opposite in meaning), with 090 EMOTIONS IN THE PR CTICE O PSYCHOTHER PY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
11/26
Conduct DisorderI Specific Developmental Disorder
Deficit Disorder
Adjustment DisorderMajor DepressiveDisorder
Anxiety DisorderFigure 5.3. An Approximation to a Circumplex for Preadolescent PsychiatricDisorders Based on a Confusion Matrix. From Co-Occurrence of PsychiatricDisorders in Child Psychiatric Patients and Nonpatients: A Circumplex Mo del,by C. R. Pfeffer and R. Plutchik, 1989 , Comprehensive Psychiatry, 30 p. 280.Copyright 1 98 9 by W. B. Saunders Company. Reprinted with permission.
indicating that there is no relation between the descriptions. The ratingswere transformed into angular placements on a circle, with results as shownin Figure 5.4 (the method of transformation is described in detail in Conte
Plutchik, 1981).The locations of the diagnoses around the circumplex may be com-
pared to the traditional but arbitrary clusters that have been proposed inDSM-III. The first cluster includes paranoid schizoid and schizotypical di-agnoses, applied to individuals who often appear odd or eccentric. Thesecond cluster includes borderline mn3ssistic, histrionic and antisocial diag-noses. Individuals with such diagnoses are said to appear dramatic or erratic.The third cluster includes dependent compulsive avoidant and passive-aggressive diagnoses. Individuals with these disorders often appear anxious.As a convenient shorthand, these clusters have been referred to as theeccentric the erratic and the anxious groups.
Examination of Figure 5.4 shows that paranoid schirotypicd and schizoidare sequential and clearly form the eccentric cluster, although compulsive-obsessive appears to be also part of the eccentric cluster and has featuresE M O T I O N S A N D P E R S O N A L T Y D IS OR D ER S 91
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
12/26
BORDERLINE
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
13/26
that are similar to those of the paranoid diagnoses. The second cluster, thedramatic grouping, is not confirmed empirically. Narcissistic and antisocialare found to be similar and are related to the proposed sadistic diagnosis.Passive-aggressive is also found to be part of this grouping. This clusterseems to be centered around aspects of aggression and might properly belabeled the aggressive cluster.
The traditional anxious cluster purportedly consisting of avoidant, de-pendent, obsessive-compulsive, and passive-aggressive is not confirmed. Theempirical locations suggest that the avoidant and dependent diagnoses arehighly similar to one another and are similar to the self-defeating and dys-thymic disorders. This modified version of the anxious cluster should becalled the anxious-depressed cluster instead.Of some interest is that the histrionic and borderline diagnoses are neareach other on the circumplex and are also near the dysthymic diagnosis.They probably could be fit into the anxious-depressed cluster. The presenceof strong features of both anxiety and depression in these two diagnosessupports this placement.
One may think of these findings shown in Figure 5.4 as providing ameasure of the degree of overlap of personality disorders. Diagnoses thatare close on the circumplex are likely to be confused, whereas those thatare further apart are rarely confused.
The modified method of paired comparisons used in this study hasrevealed an empirical circumplex for the personality disorders. It shows thetraditional clusters to some degree but with some important differences.The so-called erratic cluster seems clearly to be related to problems of han-dling aggression. The anxious cluster includes self-defeating persohality anddysthymic personality, even though dysthymic is not included in Axis 11.This cluster might be called the anxious-depressed cluster. Emotions appearto be related to all of the personality disorders.
These findings help demonstrate that some degree of comorbidity ex-ists for all personality disorders and that there is a gradual transition fromone personality disorder to another in terms of similarity. Strictly speaking,this implies that clusters are somewhat arbitrary and are based on arbitraryselection of boundaries. The circumplex concept implies that all person-ality disorders, those that are now recognized and those that may be clin-ically labeled in the future, can be represented by placements on a circlevarying in degree of closeness.
Table 5.3 helps explain the partially arbitrary nature of the personalitydisorders; it compares the labels given for personality disorders in the dif-ferent DSM editions, as well as in a recent psychoanalytically orientedlisting. A number of the diagnostic labels have changed over time, and thedefinitions themselves have been modified as well. There is no reason tobelieve that this process of addition and subtraction of terms and redefi-nitions will not continue into the future. It is likely that this process is a
EMOTION S A N D PERSONALI7Y DISORDERS 93
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
14/26
TAE53
ifeenPo
dLssoPsotyisods
Phayc
DM-9
DM-9
DMR19
DMV19
Aha1
Pad
Pad
Pad
Pad
Pad
Shzod
Shzod
Shzod
Shzod
Shzod
Pveaeve
Shzoyp
Shzoyp
Shzoyp
Shzoyp
Cmpsve
Cmpsve
Obevecompsve
Obevecompsve
Obeve
Heca
Hsroc
Hsroc
Hsroc
Heca
Cohmic
Ncssc
Ncssc
Ncssc
Ncssc
Sohc
Asoa
Asoa
Asoa
Asoa
Epove
Aod
Aod
Aod
Ahc
D
D
D
Maohsc
In
e
Bdn
Bdn
Bdn
Bdn
Pveaeve
Pveaeve
Hpmac
P
c
Inae
Ssc
Sf-den
Af
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
15/26
reflection of the circumplex structure of personality disorders and the in-evitable overlaps of meaning that occur. Some version of a depressive ordysthymic personality disorder as well as a hypomanic disorder is likelyto be incorporated into the personality disorder circumplex.Table 5.4 represents a summary of nine circumplex models that havebeen applied to personality disorders. In each case, different methods ofdata acquisition and different analyses, judges, and patient samples wereused. The table lists the relative sequence of personality disorders aroundthe circumplex. The estimate of the exact angular location of each diag-nosis was based on the actual published figures.
Despite the differences in method, many commonalities may be seen.Starting with paranoid as an arbitrary reference point, almost all studieshave found that narcissistic and antisocial diagnoses are close to it on thecircumplex; borderline is usually found somewhere in the middle of thelist, whereas dependent, self-defeating, and avoidant are generally foundnear the schizoid or schizotypal diagnoses. For example, narcissistic has amean location of 45;histrionic has a mean location of 117; and schizoidhas a mean location of 295. Despite some differences among studies, thereappears to be good agreement on the sector of the circumplex in whicheach diagnosis is located. These findings support the value of a circumplexanalysis of personality disorder diagnoses and demonstrate both the simi-larity and polarity structure of such diagnoses.Implications
The following list summarizes some of the ideas that have been pre-
1. There is now considerable evidence based on different meth-ods and patient populations that personality disorders vary indegree of similarity to one another and show polarities aswell. These facts can be best described by means of a circum-plex.2. The exact number of personality disorders as well as the mostappropriate ways of labeling and defining them are still amatter of controversy. The controversies are largely a func-tion of how one chooses to group the elements of overlappingcategories. Changes will probably continue to be made in thefuture.3. The existence of overlapping categories is one of the reasonsthat most patients are given several personality disorder di-agnoses. This is also the reason for the relatively low relia-bility of diagnoses in the personality disorder domain.4 I t is evident that degree of conflict within the individual is
sented thus far concerning the circumplex for personality disorders:
EMOTIONS AND PERSONALITY DISORDERS 95
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
16/26
TABLE 5.4A Summary of Angular Circumplex Locations of Personality DisordersAngle AnglePlutchik and Platman 1977) degrees) Wiggins 1 982) (degrees)
ParanoidSociopathicCyclothymicHistrionicWell-adjustedCompulsivePassive-aggressiveSchizoid
082130156187283320340
ParanoidNarcissisticCompulsiveHypomanicHistrionicDependentPassive-aggressiveSchizoid
0459014018022027031 5Angle AnglePlutchik and Conte 1 985) (degrees) Millon 1 987) (degrees)
ParanoidAntisocialNarcissisticBorderlineHistrionicWell-adjustedDependentCompulsiveAvoidantPassive-aggressiveSchizotypalSchizoidAntisocial
040536511518021 6300327330333335335
ParanoidNarcissisticHistrionicPassive-aggressiveBorderlineSelf-defeatingDependentAvoidantSchizotypalSchizoidCompulsiveAggressive
027588110312815319322245275305Angle AngleRomney and Bynner 1989) (degrees) Pincus and Wiggins 1990) (degrees)
ParanoidNarcissisticCompulsiveHypomanicHistrionicDependentPassive-aggressiveSchizoid
0 Paranoid32 Antisocial90 Narcissistic147 Histrionic180 Dependent203 Avoidant270 Schizoid330
02278106236274310
Angle Strack, Lorr, and AngleSim and Romney 1 990) (degrees) Campbell 1 990) (degrees)ParanoidNarcissisticHistrionicHypomanicCompulsiveDependentBorderlineSch zotypalAvoidantSchizoidPassive-aggressiveAntisocialCompulsive
0124054112172185202233254281350306
ParanoidNarcissisticAggressiveHistrionicAntisocialPassive-aggressiveBorderlineSelf-defeatingAvoidantSch zotypalSchizoidDependent
03040607010415090210211232240
96 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
17/26
TABLE 5.4 Continued)AnglePlutchik and Conte 1994) degrees)
Paranoid 0Obsessive-com pulsive 20Antisocial 60Narcissistic 05Sadistic 102Passive-aggressive 117Histrionic 160Borderline 170Dysthymic 192Self-defeating 225Avoidant 240Schizoid 292Schizotypal 312
Dependent 210
From The Circumplex as a General Model of the Structure of Emotions and PersonaliGrby R.Plutchik in Cifcumplex Models of Personality and Emotions, edited by R. Plutchik and H. R. Conte1997 p. 36 Washington DC: American Psychological Association. Copyright 1997 by AmericanPsychological Association. Reprinted by permission.
a function of how diverse or opposed his personality diag-noses are. This may, in fact, be an indirect way of measuringconflict.5. I t is apparent that emotions are intimately involved in per-sonality disorders. Anger and aggression are central to suchdisorders as antisocial and paranoid personality disorders,whereas anxiety and depression are central to avoidant, de-pendent, and dysthymic disorders. I t is thus not surprisingthat a circular order of similarity applies to both emotionsand personality disorder diagnoses. Both these domains areessentially concerned with interpersonal relations.
A CIRCUMPLEX FOR IMPULSES TO ACTIONMost theories of emotion acknowledge the complex nature of the
emotional response. However, although considerable attention has beenpaid to the autonomic arousal aspect of emotion, relatively little attentionhas been paid to the issue of impulses to action that are implied by emo-tions. In other words, although feelings of fear and anger are often asso-ciated with the behaviors of flight or fight, such feelings need not neces-sarily result in such behaviors. This s simply because the situation mayprevent the carrying out in action of the feelings. The existence of a gate,a stockade, a rope, or a predator may prevent the behaviors of flight or
EMOTJONS AN D PERSONALlTY DISORDERS 97
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
18/26
fight from occurring. However, the impulse to run or the impulse to attackmay still be present. The combination of such impulses is what is usuallyreferred to as conflict.
One of the few attempts to incorporate the concept of impulse intoa theory of emotion was made by Nina Bull almost 50 years ago. Sheproposed her attitude theory of emotion, which she described (1952) inthe following terms:
Emotion is conceived of as a sequence of neuromuscular events inwhich a postural set or preparatory motor attitude is the initial step.This preparatory attitude is both involuntary and instinctive and is theend result of a slight, tentative movement which gives a new orien-tation to the individual, but does not immediately go into the con-summatory stage of action. (p. 217)In two ingenious studies using hypnotized participants, Bull and her
collaborators (Bull Gidro-Frank, 1950; Pasquarelli Bull, 1951 foundconsistent bodily postures reported when certain emotion words (e.g., fear,anger, disgust, triumph, depression) were suggested. When other hypnotizedparticipants were asked to lock their bodies into these defined postures,they could not change their emotional feelings even when suggested bythe hypnotist unless they were allowed to change their postures. On thebasis of these results, Bull drew two important conclusions: (a) Both skel-etal muscle activity and visceral activity are involved in emotional feelingsand (b) different emotions have different postures or impulses to actionassociated with them.
Action impulses associated with emotions can be studied in severalways. One preliminary attempt to identify such impulses was described byPlutchik (1980b). A summary of this study is presented below.A list of 142 emotion words was arranged in random order and pre-sented to 15 judges. The judges were given the following instructions:
On the following pages there is a list of emotions. When we thinkabout each one, we can usually recognize that it implies an urge to actin some particular way. For example, when we think of anger, we usu-ally recognize an urge to attack or hurt someone. When we think ofsadness, we usually recognize an urge to cry or mourn for someone.
Please read the list, and give your opinion about what urges or im-pulses to action are implied by each emotion. Please make a first choiceand a second choice from the list of eight types of impulses presentedbelow. Place the numbers of your choices in the appropriate spaces.The Eight Impulses to Action
(1) to attack or hurt2) to cry or mourn3) to embrace or mate4) to explore or search5) to stop activity
98 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
19/26
( 6 ) to reject or get rid of7 ) to welcome or be with(8) t withdraw or get away p. 355)Table 5.5 (see p. 104)presents a summary of the judgments based onthe relative frequencies of first and second choices for each emotion. In
some cases there was almost complete agreement on these choices. In othercases there was much less agreement. The table presents first and secondchoices for each emotion term, although in many cases a third choicehelped to distinguish among the emotions. Emotions printed in bold lettersexpress the primary emotions most clearly.
In Table 5.5 the emotion words have been listed in the circumplexorder obtained on the basis of a direct similarity scaling method. The an-gular location of each emotion on a circle is listed alongside the emotionterm and the impulse to action that the judges have identified.
Examination of the table reveals clusters of emotions that show asystematic progression around the circle. The first cluster consists of a seriesof terms such as accepting, agreeable, calm, and obliging, all of which haveto welcome or be with as a major component impulse. All these termsand impulses imply an act of affiliation or incorporation. In most cases thesecond impulse consists of an urge to embrace or mate; other impulses mayalso be present.
The second group of emotions has as a primary impulse the urge towithdraw or get away and includes such terms as timid, panicky, embar-rassed, self-conscious, and nervous. The second impulse, in most cases, is anurge to stop activity. The differences between the different emotions arerelated in part to the relative magnitude of the primary and secondaryimpulses and in part to the presence of additional impulses, such as anurge to cry or to reject.
The third group of emotions consists of terms such as sad depressed,unhappy, and despairing. Most of these terms have as a primary impulse tocry or mourn and as a secondary impulse to withdraw or get away.
The fourth group of emotions, the orientation emotions, includessuch terms as vmillating, puzzled, confused, and surprised. The primary im-pulse in most of these emotions is to stop activity, and the secondaryone is to explore or search. A third impulse judged to exist in several ofthese emotions is to withdraw or get away.
The fifth grouping of emotions consists of those that have the feelingof rejection as a major component. Emotions such as disgusted, resentfulrevolted, and displeased all have as their primary impulse to reject or getrid of, and all have either withdrawal or attack as a secondary impulse.
The sixth group of emotions consists of those that have as their pri-mary impulse the urge to attack or hurt. Examples of such emotions arefurious, qwtrrelsome, aggressive, and sarcastic. The secondary impulse in mostcases is to reject or get rid of.
EMOTIONS AND PERSONALITY DISORDERS 99
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
20/26
The seventh group of emotions contains such terms as impulsive ex-pectant curious and planful. Most have as a primary emotion the urge toexplore or search. The secondary emotion in most cases is the urge towelcome or be with.Finally, the eighth major cluster of emotions that completes the circleis mostly concerned with sociability and includes such terms as eager de-lighted happy, and cooperative. The secondary impulse in almost all cases isthe urge to embrace or mate, and in many cases a third impulse is alsopresent. It should be mentioned that the first grouping and the last containmost of the same component impulses. This suggests that there is no sharpline of distinction between the emotions of joy and acceptance and theirderivatives, at least as measured by these impulses.
f great interest is that the judgments of impulses associated withemotions tend to cluster emotions in very much the same way as do thedirect judgments of similarity. The results support the concept that emo-tions are complex sequences of events that include impulses to action asan important part of the sequences. They also provide still another lan-guage to describe an important aspect of emotions, a language that is likelyto have particular value in the clinical context. Although patients maynot always be able to describe the emotions they feel in clear, subjectiveterms, they are likely to be able to describe the impulses to action that aremixed up in their internal conflicts.
THE QUESTION OF AXESA question that sometimes arises when considering circumplex mod-
els involves the underlying dimensions that give rise to the circumplex. Ithas been assumed by many investigators that in a two-dimensional surfaceas is the case with the circumplex), there are two independent axes that
are basic and that their interaction accounts for all the terms of the cir-cumplex. Using factor analytic studies of personality, different investigatorshave proposed such axes as dominance-submission, love-hate, emotionalstability-neuroticism, extroverted-introverted, or conservative-radical.The identification of such axes is somewhat arbitrary and depends on theinitial choices and sampling of items and on the assumptions and prefer-ences of the investigators.
There is, however, another way to consider the question of axes. Inany circular configuration it is unnecessary to consider any particular pairof axes as more basic than any other pair. The axes are arbitrary referencepoints that simply enable one to plot the positions of variables relative toone another. The axes may be removed or ignored, and all relationshipsamong the variables remain unchanged.
An important feature of a circular structure is that it may reveal100 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
21/26
empty sectors that might be filled systematically in subsequent research. Intheory, adding variables (e.g., traits, diagnoses) should not change the rel-ative configuration of the original ones but would result in a more completemapping of the universe being studied. The goal of a circumplex analysisis to sample all sectors of an interpersonal domain equally.
An alternative way of saying this is that in any true or nearly truecircle, the positions of all points (or elements) on the circle relative toone another are invariant irrespective of the coordinates used to locatethem. Assumed underlying dimensions cannot explain the circumplex be-cause any particular set of axes is arbitrary and no more basic than anyother. In a relatively seamless circle of elements, any rotation of axes doesnot change the relations among the elements. From a descriptive point ofview, it is inappropriate to reify certain axes as more fundamental thanothers.
THE APPLICATION OF CIRCUMPLEX MODELS TOCLINICAL PRACTICE
Three brief examples demonstrate the application of circumplex ideasto clinical practice.
In 1983, Kiesler described what he called the interpersonalcircle, whichis a circumplex of interpersonal behaviors. These include such behaviorsas dominant, submissive, hostile, and friendly. One of the offshoots of thismodel is the theory of complementarity. This theory hypothesizes thatdominant behaviors tend to elicit friendly ones, and hostile behaviors tendto elicit hostile ones.
In a further development of these ideas, Kiesler, Schmidt, and Wagner(1997) have used the theory to develop an Impact Message Inventory de-signed to measure the typical automatic, relatively preconscious sets ofemotional reactions each person has to others. Such reactions include feel-ings, action tendencies, and fantasies. The impact messages imply claimsof one person on another that relate to issues of control and affiliation.Factor analysis of the Impact Message Inventory reveals that the Inventoryhas a circumplex structure. The authors concluded that impact messagesare best understood in terms of emotions.
Horowitz and his colleagues (Horowitz, Rosenberg, Baer, Ureno,Villasenor, 1988) have developed an Inventory of Interpersonal Problems(IIP) based on a large sample of initial interviews of people starting psy-chotherapy. The IIP contains 127 statements of problems (e.g., It is hardfor me to say no to other people) and has been factor analyzed to ex-amine the relationships among the items. Results of this analysis revealsthat the items, which essentially refer to different aspects of interpersonalrelations, form a circumplex. The eight sectors of the circumplex have been
EMO TIONS AND PERSONALIT( DISORDERS 101
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
22/26
called by Horowitz et al. (in order) domineering, intrusive, overly nurturant,expbirable, no wsertiv e, socially avoidant, cold, and vindictive, and the test hasbeen widely used in clinical research.
In a follow-up to this work, Horowitz, Dryer, and Krasnoperova(1997)presented a model of interpersonal behavior that contains four prin-cipal postulates: (a) interpersonal behaviors can be described in terms ofthe two dimensions of affiliation, ranging from hostile to friendly behavior,and dominance, ranging from yielding to dominating behaviors; (b) aninterpersonal behavior invites a complementary reaction, and the relation-ship between the two is also characterized in terms of the circumplex; (c)noncomplementarity creates an interpersonal tension between partners;and (d) people learn complete interpersonal sequences rather than isolated,individual responses to particular stimuli. Empirical evidence is providedto illustrate each of these postulates.
In the final section of their chapter, the authors examined the natureof interpersonal goals. They emphasized that interpersonal problems are afunction of frustrated interpersonal goals. To understand a persons inter-personal problems, they maintained, it is necessary first to assess that per-sons interpersonal goals and wishes and to determine whether his or herpartners behavior is in accordance with them. The IIP fulfills this function.The authors discussed its construction, development, and application andprovide evidence to show that like interpersonal behaviors and problems,interpersonal goals can be described in terms of a two-dimensional circum-plex.
The third example is taken from the work of Henry (1997).His clin-ical research is based on Benjamins (1993) Structural Analysis of SocialBehavior, which is a kind of tripartite circumplex system. One circumplexmeasures interpersonal actions toward another person, a second circumplexmeasures interpersonal actions that are received from another person, andthe third measures behavior by the self toward the self.
Henry described a method for using the Structural Analysis of SocialBehavior model in the description of the dynamics of a patients interper-sonal problems and in the subsequent measurement of the outcome oftreatment. He went on to show how the use of this model has enabledhim, along with Benjamin, to generate a theoretical model of abnormalpersonality that proposes a qualitative definition for differentiating abnor-mal from normal personality. This is in contrast to earlier definitions inwhich pathology was seen quantitatively as a matter of degree of the ex-pression of certain traits. Further uses of this circumplex model are de-scribed. These include the development of new instruments to test theunderlying theory and to assess current interpersonal wishes, fears, andpower tactics. That all these instruments yield data in the same metricfacilitates the integration of diverse clinical information and provides forcongruence of problem, treatment, and outcome data. Henry concluded by102 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
23/26
demonstrating ways in which he believed the circumplex provides a basisfor the integration of theories of psychopathology and psychotherapy thatare as diverse as the cognitive, behavioral, and psychodynamic theories.
These examples suggest the potential power of the circumplex modelsof emotions, personality, and personality disorders to stimulate research, toguide the development of measuring instruments, and to help explain clin-ical problems.
EMOTIONS A N D PERSONALITY DISORDERS 103
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
24/26
Impulses TABLE 5.5Arranged in a Circumplexto Action Associated With a Large Sample of EmotionsAngle(degrees) Emotion First choice Second choice
05122632374043526567687072737575767778
58
78a0a3a3a3a4a5aa869091102108
113120123125125126127127129133133133134134136136
AcceptingAgreeableSereneCheerfulReceptiveCalmPatientObligingAffectionateObedientTimidScaredPanickyAfraidSubmissiveBashfulEmbarrassedTerrifiedPensiveCautiousAnxiousHelplessApprehensiveSelf-consciousAshamedHumiliatedForlornNervousLonelyApatheticMeekGuiltySadSorrowfulRemorsefulHopelessDepressedWorriedDisinterestedGrief-strickenUnhappyGloomyDespairingWatchfulHesitantIndecisiveRejectedBored
Shy
Empty
To welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo embraceormateTo welcome or be withTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo welcome or be withTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo explore or searchTo explore or searchTo explore or searchTo cry or mournTo explore or searchTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo cry or mournTo withdraw or get awayTo cry or mournTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo cry or mournTo cry or mournTo cry or mournTo cry or mournTo cry or mournTo cry or mournTo explore or searchTo reject or get rid ofTo cry or mournTo cry or mournTo cry or mournTo cry or mournTo explore or searchTo stop activityTo stop activityTo cry or mournTo stop activity
To embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo welcome or be withTo stop activityTo stop activityTo cry or mournTo stop activityTo stop activityTo stop activityTo stop activityTo stop activityTo stop activityTo stop activityTo welcome or be withTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo stop activityTo reject or get rid ofTo reject or get rid ofTo withdraw or get awayTo stop activityTo withdraw or get awayTo stop activityTo stop activityTo cry or mournTo withdraw or get awayTo withdraw or get awayTo stop activityTo withdraw or get awayTo stop activityTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo stop activityTo explore or searchTo withdraw or get awayTo withdraw or get awayTo reject or get rid of
104 EMOTIONS IN THE PRACTICE OF PSYCHOTHERAPY
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
25/26
TABLE 5.5 Continued)Angle(degrees) Emotion First choice Second choice13713713813813914014114214514714815215716016116617017517617718118218318318418518518518618618819019219219319420120221 222022 1222225227227230230230231232235
Disappointed To cry or mournVacillating To stop activityDiscouraged To stop activityPuzzled To explore or searchUncertain To explore or searchBewildered To explore or searchConfused To stop activityPerplexed To explore or searchAmbivalent To stop activitySurprised To stop activityAstonished To stop activityAmazed To stop activityAwed To stop activityEnvious To attack or hurtDisgusted To reject or get rid ofUnsympathetic To reject or get rid ofUnreceptive To reject or get rid ofIndignant To reject or get rid ofDisagreeable To reject or get rid ofResentful To reject or get ridofRevolted To reject or get rid ofDispleased To reject or get rid ofSuspicious To explore or searchDissatisfied To reject or get rid ofContrary To reject or get rid ofJealous To attack or hurtIntolerant To reject or get rid ofDistrustful To withdraw or get awayVengeful To attack or hurtBitter To attack or hurtUnfriendly To reject or get rid ofStubborn To reject or get rid ofUncooperative To reject or get rid ofContemptuous To attack or hurtLoathful To attack or hurtCritical To reject or get rid ofAnnoyed To reject or get rid ofIrritated To reject or get rid ofAngry To attack or hurtAntagonistic To attack or hurtFurious To attack or hurtHostile To attack or hurtOutraged To attack or hurtScornful To reject or get rid ofUnaffectionate To reject or get rid ofQuarrelsome To attack or hurtImpatient To explore or searchGrouchy To reject or get rid ofDefiant To attack or hurtAggressive To attack or hurtSarcastic To attack or hurt
To withdraw or get awayTo explore or searchTo withdraw or get awayTo stop activityTo stop activityTo withdraw or get awayTo explore or searchTo stop activityTo explore or searchTo explore or searchTo explore or searchTo explore or searchTo explore or searchTo reject or get rid ofTo withdraw or get awayTo withdraw or get awayTo withdraw or get awayTo attack or hurtTo attack or hurtTo attack or hurtTo withdraw or get awayTo withdraw or get awayTo reject or get rid ofTo withdraw or get awayTo attack or hurtTo reject or get rid ofTo reject or get rid ofTo reject or get rid ofTo reject or get rid ofTo reject or get rid ofTo attack or hurtTo stop activityTo stop activityTo reject or get rid ofTo reject or get rid ofTo attack or hurtTo attack or hurtTo attack or hurtTo reject or get rid ofTo reject or get rid ofTo reject or get rid ofTo reject or get rid ofTo reject or get rid ofTo withdraw or get awayTo withdraw or get awayTo reject or get rid ofTo attack or hurtTo withdraw or get awayTo reject or get rid ofTo reject or get rid ofTo reject or get rid of
EMOTIONS AND PERSONALITY DISORDERS 105
-
8/12/2019 Emotions and Personality Disorders, Lib Emotions in the Practice of Psychotherapy
26/26
TABLE 5 5 Continued)Angle(degrees) Emotion First choice Second choice237240243244248249250255257257257260261261262268270271286297298307313131 431 531 932322323324326327328329331338341345351
RebelliousExasperatedDisobedientDemandingPossessiveGreedyWonderingImpulsiveAnticipatoryBoastfulExpectantDaringCuriousRecklessProudInquisitivePlanfulAdventurousEcstaticSociableHopefulG eefuElatedEagerInterestedEnthusiasticDelightedAmusedAttentiveJoyfulHappySelf-controlledSatisfiedPleasedReadySympatheticContentCooperativeTrustingTolerant
To attack or hurtTo reject or get rid ofTo reject or get rid ofTo attack or hurtTo embrace or mateTo attack or hurtTo explore or searchTo explore or searchTo welcome or be withTo welcome or be withTo welcome or be withTo explore or searchTo explore or searchTo attack or hurtTo welcome or be withTo explore or searchTo explore or searchTo explore or searchTo embrace or mateTo welcome or be withTo welcome or be withTo welcome or be withTo embrace or mateTo welcome or be withTo explore or searchTo welcome or be withTo welcome or be withTo welcome or be withTo explore or searchTo embrace or mateTo welcome or be withTo stop activityTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be with
To reject or get rid ofTo stop activityTo withdraw or get awayTo welcome or be withTo welcome or be withTo reject or get rid ofTo welcome or be withTo welcome or be withTo explore or searchTo reject or get rid ofTo explore or searchTo welcome or be withTo welcome or be withTo reject or get rid ofTo embrace or mateTo welcome or be withTo welcome or be withTo welcome or be withTo welcome or be withTo embrace or mateTo explore or searchTo embrace or mateTo welcome or be withTo embrace or mateTo welcome or be withTo embrace or mateTo embrace or mateTo embrace or mateTo welcome or be withTo welcome or be withTo embrace or mateTo welcome or be withTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mateTo embrace or mate
~ ~~Note. From Emotions:A Psychoevolutionary Synthesis (pp. 356-358), y R. Plutchik, 1980,NewYork: Harper Row. Copyright 1980 by Harper 8 Row. Reprinted by permission.
EMOTlONS IN THE PRACTICE OF PSYCHOTHERAPY