EKG
147
EKG CARDIOVASCULAR ANATOMY & PHYSIOLOGY
description
EKG. Cardiovascular Anatomy & Physiology. Basic Heart Anatomy. The heart is a muscle made of 3 layers Pericardium aka = pericardial sac is a connective tissue layer around the heart Epicardium is the smooth outer surface of the heart - PowerPoint PPT Presentation
Transcript of EKG

EKG
CARDIOVASCULAR ANATOMY &
PHYSIOLOGY

Basic Heart Anatomy
▪ The heart is a muscle made of 3 layers
▪ Pericardium aka= pericardial sac is a connective tissue layer around the heart
1. Epicardium is the smooth outer surface of the heart
2. Myocardium is the muscular middle layer of heart tissue▪ It is made of cardiac muscle cells that give the heart the
ability to contracts to push out blood3. Endocardium is the innermost layer of the heart made up of smooth thin connective tissue This smooth layer allows blood to flow easily throughout the heart

Basic Heart Anatomy▪ The heart is a muscle
▪ Referred to as a 2 sided PUMP▪ Right side▪ Left side
▪ Each side has 2 hollow chambers ( total of 4 chambers▪ 2 upper chambers are called=Atrium ( singular) Atria ( plural)▪ 2 lower chambers are called = Ventricle(s)

Heart Anatomy- CONTINUED
▪ Both upper chambers receive blood back to the heart▪ RA- receives blood from the superior & inferior vena cava▪ LA- receives blood from the lungs
▪ Both lower chambers pump blood away from the heart▪ RV – pumps blood to the lungs for re-oxygenation▪ LV- pumps blood into the systemic circulation

Basic Heart Anatomy
▪ Valves of the Heart
♥The 4 valves of the heart allow blood to flow only in one direction
♥There are 2 sets of valves♥Atrioventricular valves
♥Are located between the atria and the ventricles♥Right sided valve is the tricuspid valve♥Left sided valve is the bicuspid valve or the mitral valve
♥Semilunar valves♥ Serve to prevent blood from flowing back into the ventricles
♥Right sided semilunar valve = Pulmonary valve is located between the right ventricle and the pulmonary artery
♥Left sided semilunar valve = Aortic valve is located between the left ventricle and the trunk of the aorta

Heart Anatomy-CONTINUED
AtriaAre the 2 upper chambers (LEFT & RIGHT)Upper chambers are located in what is called the BASE of the heart
VentriclesAre the 2 lower chambers (LEFT & RIGHT )Lower chamber are located in what is called the APEX of the heart

Heart Anatomy-
CONTINUED
• Blood flow through the heart
•Refer to handout on cardiac/pulmonary circulation
•Heart Blood Flow Animation

Basic Physiology
of the Heart
CARDIAC CYCLE
STROKE VOLUME
CARDIAC OUTPUT
AUTONOMIC NERVOUS SYSTEM

Cardiac Cycle♥ The heart functions as a unit:
♥ Both atria contract simultaneously then both ventricles contract♥ Blood is ejected into both the pulmonary and systemic circulation when the
ventricles contract♥ Both the tricuspid and mitral valves will also close during ventricular
contraction
♥ The cardiac cycle=Represents the time sequence between ventricular contraction and ventricular relaxation
♥ Systole is ventricular contraction
♥ Diastole is ventricular relaxation
♥ SO--- One cardiac cycle is equal to one systole and one diastole of the ventricle or one heart beat
♥ In a normal heart the cardiac cycle lasts for 0.8 seconds

Stroke Volume
♥ Stroke volume (SV)= is the amount or volume of blood pumped out of the one ventricle in a single beat or contraction♥ Normal SV is 70 cubic centimeters (cc) per beat
♥ The number of contractions or beats per minute is known as the heart rate
♥ The normal heat rate in an adult is 60-100 beats per minute

Cardiac Output
♥ Cardiac output is the amount of blood PUMPED by the LEFT VENTRICLE in ONE MINUTE
♥ The formula for Cardiac Output is:♥CARDIAC OUTPUT(CO) = STROKE VOLUME (SV) X HEART RATE (HR)
HR= 80SV= 70 cc
What is the Cardiac Output of this patient in cc’s_______ and in _______liters????

Cardiac Output
▪ Inadequate, CO will result in patients having any of the following symptoms:
▪Shortness of breath
▪Dizziness
▪Drop in blood pressure
▪Chest pain
▪Cool and clammy skin

PRELOAD and AFTERLOAD
♥ PRELOAD▪ Pre-load is the filling pressure of the heart, the
pressure the heart has when it is relaxing. (Volume- In)
♥ Afterload ▪ is the RESISTANCE against which the heart must
pump▪ After-load is the pressure of the contracting
heart. (Resistance-push- Out)▪ This pressure will greatly affect the stroke volume and
the cardiac output

Autonomic Nervous System
▪ ANS regulates functions of the body that are INVOLUNTARY
▪ Both HR and BP are regulated by this component of the nervous system
▪ There are 2 major divisions of the nervous system:
▪sympathetic and parasympathetic
▪ The major organs of the body are innervated by both systems with the exception of blood vessels which are only innervated by the sympathetic system

Sympathetic Nervous System
▪ Sympathetic nervous system (or Adrenergic)
▪ 1. Accelerates the heart
▪ 2. Two chemicals are influenced by the sympathetic system – ▪ epinephrine & norepinephrine
▪ 3. These chemicals increase heart rate, contractibility, automaticity, and AV conduction

Parasympathetic Nervous System
▪Parasympathetic nervous system ( or Cholinergic)
▪ 1. Slows the heart
▪ 2. The vagus nerve is one of this systems nerves, when stimulated slows heart rate and AV conduction.

Basic Electrophysiology Basic Cell Groups
▪ The heart is made up of thousands of myocardial cells
▪ There are 2 basic myocardial cell groups: ▪ myocardial working cells ▪ pacemaker cells of the electrical conduction system
▪ MYOCARDIAL CELLS responsible for generating the physical contraction an d relaxation of the heart muscle
▪ PACEMAKER CELLS ▪ do not contain contractile fragment and can not contract▪ Responsible for controlling the rate & rhythm of the heart by
regulating depolarization

Characteristics of Cardiac Cells
Cardiac cells possess primary cell characteristics:
Extensibility Ability to be stretched
▪ Excitability▪ Ability of cardiac cells to respond to electrical stimulation
▪ Conductivity▪ Ability of cardiac cells to receive electrical stimulation and transmit the
stimulus to other cells
▪ Contractility▪ Ability of cells to shorten and cause a muscle contraction
▪ Automaticity ▪ Ability of cardiac pacemaker cells to make their own electrical impulses

ELECTRICAL CELLS OF THE HEART
▪ Electrical cells
▪ a) Make up the conduction system of the heart
▪ b) Are distributed in an orderly fashion through the heart
▪ c) Possess specific properties
▪ (1) automaticity – the ability to spontaneously generate and discharge an electrical impulse
▪ (2) excitability – the ability of the cell to respond to an electrical impulse
▪ (3) conductivity – the ability to transmit an electrical impulse from one cell to the next

MYOCARDIAL CELLS
▪ Myocardial cells
▪ a) Make up the muscular walls of the atrium and ventricles of the heart
▪ b) Possess specific properties
▪ (1) contractility – the ability of the cell to shorten and lengthen its fibers
▪ (2) extensibility – the ability of the cell to stretch

Major Electrolytes that Affect Cardiac Function
An electrolyte is a substance with charged components producing positive and negative charged ions ▪ a positive ion is called a cation ▪ a negative ion is called a anion
3 major cations that affect heart muscle are:Potassium K+Sodium Na+Calcium Ca+
Magnesium Mg

DEPOLARIZATION & REPOLARIZATION
▪ Depolarization and Repolarization
▪ 1. Cardiac cells at rest are considered polarized, meaning no electrical activity takes place
▪ 2. The cell membrane of the cardiac muscle cell separates different concentrations of ions, such as sodium, potassium, and calcium. This is called the resting potential
▪ 3. Electrical impulses are generated by automaticity of specialized cardiac cells
▪ 4. Once an electrical cell generates an electrical impulse, this electrical impulse causes the ions (Na+ rush into the cell making inside more +) cross the cell membrane and causes the action potential, also called depolarization

Depolarization & Repolarization Continued
▪ 5. The movement of ions across the cell membrane through sodium, potassium and calcium channels, is the drive that causes contraction of the cardiac cells/muscle
▪ 6. Depolarization with corresponding contraction of myocardial muscle moves as a wave through the heart
▪ 7. Repolarization is the return of the ions to their previous resting state, which corresponds with relaxation of the myocardial muscle
▪ 8. Depolarization and repolarization are electrical activities which cause muscular activity
▪ 9. This electrical activity is what is detected on ECG, not the muscular activity

Conduction System THE PATH OF AN ELECTRICAL SIGNAL
▪ Step One: The S-A node creates an electrical signal▪ The S-A node controls your heart rate, it is called your heart's "natural pacemaker." Electrical
signals created by the S-A node travel down pathways to the A-V node creating the P WAVE▪ It has as inherent rate of 60-100 bpm
▪ Step Two: The signal follows natural pathways through both atria. This causes the blood to contract, pushing blood into the ventricles
▪ Step Three: The signal reaches the A-V node. There, the signal pauses very briefly to give the ventricles time to fill with blood. ▪ This delay is seen as the PR interval
▪ Step Four: The signal spreads through the His-Purkinje system. This makes the ventricles contract, pushing blood out to your lungs and body. ▪ This generates the QRS complex▪ Bundle of His have pacemaker cells that can self-initiate a rate of 40-60 bpm ▪ Purkinje pacemaker fibers are normally within 20-40 bpm

Electrical Conduction VIDEO
▪Electrical Flow in the Heart

EKG Conduction Animation
▪ Conduction and EKG Waveform Animation

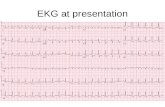
The ElectrocardiogramEKG or ECG
▪Graphic representation of the electrical activity of the heart
▪ It is a tracing of the electrical activity of the heart NOT the mechanical activity
▪ The machine used to record the activity is called an: electrocardiograph
▪ It is a diagnostic tool

Information Obtainable from EKG RHYTHM ANALYSIS
▪ Heart Rate
▪ Rhythm & regularity
▪ Impulse conduction time intervals
▪ Abnormal conduction pathways
▪ WE CANNOT HOWEVER determine:▪ Pumping action▪ Cardiac output▪ Blood pressure
▪ Cardiac muscle hypertrophy

EKG Machine
▪ An EKG machine is a voltmeter– it reads electrical energy from the body
▪ The heart uses electrical energy to contract muscles

EKG LEADS and ELECTRODES
▪ ELECTRODE is the adhesive pad that contain conductive gel and is placed on the patients skin
▪ LEADS are the wires that are then connected to the electrode – they are color coded to be user-friendly
▪ In order for the machine to give a clear picture– there must be a positive, negative and ground lead
▪ EKG will look at the heart from the positive lead to the negative lead and gives a different view of the heart
▪ The exact portion of the heart being visualized depends on lead placement
▪ This allows for observation of electrical activity in many different parts of the heart

3 Lead EKG- Used for continuous patient monitoring
▪ A 3 lead ECG is considered non-diagnostic so it does not provide a clear view of the entire heart, but instead a basic view of the electrical pathway of the heart triangulated between the 3 leads.
▪ The 3 lead ECG is usually simple to use and most have standardized color coded placement of the 3 electrode leads. These are the most common 3 lead ECG placements:
▪ 3-electrode system - Uses 3 electrodes (RA, LA and LL).- Monitor displays the bipolar leads (I, II and III)- To get best results – Place electrodes on the chest wall equidistant from the heart
Will give us a view of the lateral, and inferior portion of the heart

AUGMENTED LEADS:PLEASE NOTE THE FOLLOWING:
▪ EKG Augmented Limb Leads
▪ The same three leads that form the standard leads also form the three unipolar leads known as the augmented leads. These three leads are referred to as aVR (right arm), aVL (left arm) and aVF (left leg) and also record a change in electric potential in the frontal plane.
▪ These leads are unipolar in that they measure the electric potential at one point
▪ We can get additional contiguous (adjoining) views of the heart:▪ aVL- Lateral▪ aVF- Inferior

5 Lead EKG
▪ This configuration refers to the standard Holter monitor or the 5 lead rhythm setup
White lead=right sternum/clavicle area
Black lead=left sternum/clavicle area
Red lead=left lower thoracic area
Green lead=right lower thoracic area
Brown lead= just below and to the right of the bottom of the sternum

12 LEAD EKG
▪ Definition- A representation of the heart’s electrical activity recorded from 10 electrodes placed in standard positions on the body surface.
▪ Analogy- Envision the heart as an object placed on a pedestal around which a person can move while taking photographs (different views) from all angles.

12 Lead EKG Provides a Cross Sectional View of the
Heart▪ 12-lead ECG
- 10 electrodes required to produce 12-lead ECG.- Electrodes on all 4 limbs (RA, LL, LA, RL)- Electrodes on precordium (V1–6)
V1 @4th IC right of sternum
V2 @ 4th IC left of sternum
V3@ between V2/V4
V4 @ 5th IC midclavicular
V5 5th IC between V4/V6
V6 @ 5th IC midaxillary
Leads I,II,II are bipolar= this means they have one positive and one negative electrode ( limb leads)
-Allows the best interpretation of specific areas of the heart
- Inferior (II, III, aVF)- High Lateral Wall(I, aVL)
-Lower Lateral Wall( V5, V6)
-Septal View (V1-V2)
-Anterior View (V3-V4)

Precordial LEAD Placement of the 12 lead EKG
V1 @4th IC right of sternumV2 @ 4th IC left of sternumV4 @ 5th IC midclavicular
V3 @ between V2/V4V6 @ 5th IC midaxillary V5 5th IC between V4/V6
Lead Placement Visual
12 LEAD EKG PLACEMENT VIDEO

EKG Graph Paper
▪ Arranged in a series of horizontal and vertical lines and squares
▪ Standard in all health care settings
▪ Moves at a constant speed of 25 millimeters per second
▪ Both time and amplitude are measured on EKG graph paper
▪ Time is measured on the HORIZONTAL line
▪ Amplitude is measured on the VERTICAL line
▪ Divided into small squares, each of which is 1 mm in width and equals a time interval of 0.04 second
▪ Darker lines further divide every 5th square, both vertically and horizontally▪ Each larger square measures 5 mm in height and 5 mm in
width and represents a time interval of 0.20 second

EKG Paper and Markings
▪ Divided into small squares, each of which is 1 mm in width and equals a time interval of 0.04 second
▪ Darker lines further divide every 5th square, both vertically and horizontally▪ Each larger square measures 5 mm in height and 5 mm in width and
represents a time interval of 0.20 second
▪ 5 of the large squares all equal one second noted by the small line on the very top of the paper
▪ Most practitioners will print a 6 second strip to interpret a patients rhythm
▪ The squares of on the EKG paper represent the measurement of the length of time required for the electrical impulse to traverse a specific time in the heart

EKG WaveformsP Wave
▪ P wave▪ Impulse fired by the SA node▪ The p wave is a smooth rounded upward deflection▪ Represents depolarization of the atria▪ It is 0.1 second in duration

PR Interval
Represents the time interval for the impulse to travel for the SA node through the internodal pathway toward the ventricle
Normal PR interval is 3-5 small boxes or 0.12 – 0.20 second in length

QRS Complex
▪ Represents the conduction of the impulse from the Bundle of His through the ventricle muscle or ventricle depolarization
▪ QRS measures less than 0.12 second or less than 3 small boxes on the EKG graph paper

ST Segment
▪ Represents the time interval which the ventricles are depolarized and ventricular repolarization
▪ ST segment is ISOELECTRIC or at baseline

T Wave
▪ Represents ventricular repolarization
▪ Resting phase of the cardiac cycle

U Wave
▪ The U wave is a wave on an electrocardiogram that is not always seen
▪ typically small, and, by definition, follows the T wave
▪ U waves are thought to represent repolarization of the Purkinje fibers.[1]

How is an EKG Interpreted?
▪ Read strip from left to right
▪ Apply the 5 step approach that you will learn
▪ Ask and answer each question in the 5 step approach
▪ You must master the accepted parameters for each dysrhythmia and then then apply those parameters to each of the 5 steps when analyzing the strip.

FIVE STEP APPROACH
▪Step 1: What is the rate?
▪Step 2: Is it regular?
▪Step 3 : Is the complex narrow?
▪ Step 4: Is there a P WAVE?
▪Step 5: Do all the complexes look the same?

STEP ONE & the 6 Second Method
▪What is the rate?▪Count the number of QRS complexes or number of ventricular beats in one minute -- ▪Normal heart rate is 60-100 bpm▪ 6 second method▪Simply count the number of QRS complexes in either 3 or 6 second strip▪ If a 3 second strip is used– X by 20▪ If a 6 second strip is used – X by 10

6 Second Strip

STEP 2
▪ Asks if the rhythm is regular?
▪ Rhythms that originate from the normal pacemakers in the heart will be regular
▪ IRREGULAR rhythms indicate extra or abnormal beats
▪ Looks at the patterns of your QRS complexes
▪ All heart rhythms are classified as regular or irregular
▪ You should use EKG calipers or use a piece of paper and mark r-r wave distance
1. Measure your R-R interval to determine Ventricular regularity
2. Measure your P-P waves for atrial regularity

STEP 3
▪ Is the complex narrow?
▪Narrow complexes are normal
▪Wide QRS complexes indicated a conduction abnormality
▪Normal QRS width is 0.12 second or less than 3 small boxes
▪ Wide QRS or greater than 0.12 second or more than 3 small boxes ( ventricular in origin)
▪Narrow QRS less than 0.12 second may indicate a supraventricular rhythm

Step 4
▪ ASK– IS THERE A P WAVE????????? Preceding the QRS complex?
▪ A P-wave before the QRS represent normal conduction from the atria to the ventricles
▪ If there is NO P wave---- the impulse is being generated from ELSEWHERE IN THE HEART AND IS NOT A SINUS RHYTHM

Step 5
▪ Do all the complexes look the same?

5 STEP APPROACH to EKG Interpretation
1.What is the rate?
2.Is it regular?
3.Are the QRS complexes narrow?
4.Is there a P WAVE? ( Is there a P WAVE before each complex?) Is the PRI normal ?
5.Do all the QRS complexes look the same?

Normal P wave, Absence of P wave, Abnormal P Wave

Step 5
▪Do all the complexes look the same?
▪Normal conductions follows the same pathway with each beat
▪Different looking complexes indicate that some impulses are following alternative or aberrant pathways

Conclusion of the 5 STEP METHOD
▪If you can answer affirmatively to all of the 5 steps then your patient has a Normal Sinus Rhythm or NSR

Normal Sinus RHYTHMS
▪Normal Sinus Rhythm or NSR ▪Rate 60-100
▪Sinus Bradycardia--- ▪Rate is LESS THAN 60
▪Sinus Tachycardia– ▪Rate is GREATER THAN 100 but not more than 140

Atrial RHYTHMS
ATRIAL FIBRILLATION
ATRIAL FLUTTER
SVT/PSVT

Rhythms That Originate in the Atria
▪Atrial Fibrillation
▪Atrial Fibrillation with Rapid Ventricular Response
▪Atrial Flutter
▪Supraventricular Tachycardia

EKG Findings Common to ATRIAL RHYTHMS
▪P wave absent or has an abnormal shape
▪Fibrillatory waves present– commonly called f waves
▪Flutter waves present
▪QRS is narrow

Atrial Fibrillation▪ Atrial fibrillation produces a rapid and irregular
heartbeat
▪ The atria (the upper two chambers of the heart that receive blood) quiver, or fibrillate, instead of beating normally
▪ impulses come from all over the atria, triggering 300 to 500 contractions per minute within the heart’s upper chambers
▪ the atrioventricular node becomes overwhelmed by impulses
▪ the result is an irregular and rapid heartbeat (80 to 160 beats per minute versus normal 60 to 100 beats per minute).
▪ Atrial Fibrillation

Atrial Fibrillation

Atrial Fibrillation
▪ P wave---none or fibrillation waves
▪ PR interval—none
▪ QRS—less than 0.12 seconds
▪ Ventricular rate—60-100 bpm
▪ Atrial rate( if different than the ventricular rate)– 300-600/min
▪ Complexes look similar
▪ RHYTHM__ IS IRREGULAR
▪ FYI- if the rate is less than 100 = controlled
▪ If the rate is greater than 100= rapid ventricular response or RVR

TREATMENT
▪Medications
▪Cardioversion
▪ Ablation surgical procedures

Atrial FLUTTER
▪ Typical atrial flutter results from a single “short-circuit” in the right atrium.
▪ This short-circuit causes the atria to beat at about 300 beats per minute while the lower chamber of the heart (the ventricles) beat at a slower rate (often 75 to 150 beats per minute
▪ Atrial flutter is similar to Atrial fibrillation
▪ It differs from atrial fibrillation (AF) in that the heartbeat is regular, not irregular.
▪ Will see characteristic FLUTTER waves that are saw-tooth in shape

Atrial Flutter
▪ P wave- none– Flutter waves
▪ PR interval– NONE
▪QRS -- less than 0.12 seconds
▪ Ventricular rate– 60-100 – but can be as high as 130-160
▪ Atrial rate– 240-320/ min
▪Complexes will look similar
▪ RHYTHM is REGULAR

Atrial Flutter

Atrial FLUTTER Treatment
▪Medications
▪ Ablation Therapy

Supraventricular Tachycardia - PSVT ( Paroxysmal SVT)
▪ Most episodes of SVT are caused by faulty
electrical connections in the heart
▪ Supraventricular tachycardia (SVT) is a rapid heart rhythm originating at or above the AV node.
▪ SVT rates are above 100 beats per minute and are typically 150-250 bpm.
▪ SVT’s rapid heart rate does not allow the ventricles to completely fill with blood, decreasing cardiac output.

SVT/PSVT
▪P-wave- hard to find– if present there is one per QRS
▪PR interval-usually not measurable
▪QRS- 0.04-0.10 seconds NARROW
▪All complexes look the same
▪Ventricular rate- 150-240/min
▪RHYTHM is REGULAR

SVT/ PSVT

Treatments for SVT/PSVT
▪Carotid Massage
▪Vagal Maneuvers ▪ Valsalver maneuver & Holding breath, Cold immersion, coughing ▪ Innervated by parasympathetic NS
▪Medications
▪Synchronized Cardioversion
▪Ablation interventions

VIDEO on SVT/ A FIB & A Flutter
▪THE Atrial and SVT RHYTHMS

JUNCTIONAL RHYTHMS

Junctional RHYTHMS
▪ Junctional rhythms are named such because their impulse originates from the AV node (AV junction) instead of the SA node.
▪ ▪The SA node may be impaired secondary to drug toxicity or underlying cardiac disease.
▪ ▪When the AV node does not sense an impulse coming down from the SA node, it will become the pacemaker of the heart

Junctional RHYTHM
▪Rate- 40-60 bpm▪ RHYTHM is REGULAR
▪ P wave are ABSENT OR INVERTED
▪ ▪PR interval of <0.12 seconds (remember normal is 0.12-0.2)
▪Narrow complexes ( 0.06 seconds on average)
▪ All complexes look the same

Junctional RHYTHM

Junctional RHYTHM
▪ Junctional Bradycardia▪Rate=less than 40
▪Accelerated Junctional RHYTHM▪Rate=greater than 60
▪ Junctional Tachycardia ▪ rate= greater than 100

Junctional Treatment
▪ If the patient has NO symptoms--- they will just will observe the patient
▪ If symptomatic ----a permanent pacemaker may be needed
▪ If the junctional rhythm is due to digitalis toxicity, then the medication atropine, digoxin immune Fab (Digibind), or both may be necessary.

Heart BLOCKS
FIRST DEGREE
SECOND DEGREE
THIRD DEGREE

Heart Blocks
▪Heart blocks are arrhythmias caused by an interruption in the conduction of impulses between the atria and the ventricles.
▪♥The AV block can be total or partial or it may simply delay conduction.

The Heart Block Rhythms
First Degree AV Block ▪♥Second Degree AV Block ▪♥Type I (Wenckebach) -----also called Mobitz I▪♥Type II---- also called Mobitz II
▪♥Third Degree AV Block

First Degree Heart Block ▪ First Degree AV Block
▪ ♥Is the most common form of heart block
▪ ♥Looks similar to sinus rhythm
▪ ♥Impulse conduction between the atria and the Bundle of His is delayed at the level of the AV node
▪♥The PR interval will be prolonged (> 0.20)

5 STEPS to Interpret First Degree HB
▪ 1.What is the rate? 60-100 bpm
▪ 2. What is the rhythm? Usually regular
▪ 3. Is there a P wave before each QRS? YES Are P waves upright and uniform? Yes
▪ 4. What is the length of the PR interval? >0.20 seconds
▪ 5. Do all QRS complexes look alike? Yes
▪ What is the length of the QRS complexes? Less than 0.12 seconds (3 small squares)

Causes and S/S of First Degree AV Block
▪ ▪Can occur in healthy hearts
▪ ▪May be temporary
▪ ▪Myocardial infarction or ischemia
▪ ▪Medications – digitalis, calcium channel blockers, beta blockers
▪ ▪Myocarditis
▪ ▪Degenerative changes in the heart

Medical Tx of First Degree AV Block
▪ ▪No treatment is usually necessary if the patient is asymptomatic
▪ ▪Treat the underlying cause
▪ ▪Monitor closely to detect progression to a more serious form of block

2nd Degree AV Block Mobitz Type I (Wenckebach)
▪ ♥The delay of the electrical impulse at the AV node produces a progressive increase in the length of the PR interval (> 0.20 seconds)
▪ ♥The PR interval continues to increase in length until the impulse is not conducted or the QRS complex is “dropped”

2nd Degree AV Block Mobitz Type I (Wenckebach)
The PR interval continues to increase in length until the impulse is not conducted or
the QRS complex is “dropped”

5 Steps to Identify 2nd Degree AV Block Mobitz Type I (Wenckebach)
▪ 1. What is the rate? Varies
▪ 2. What is the rhythm? Ventricular: irregular
▪ 3. Is there a P wave before each QRS? ----------------------------Yes▪ Are P waves upright and uniform? ------------------------------- Yes, for
conducted beats
▪ 4. What is the length of the PR interval? ▪ Progressively prolongs until a QRS is not conducted
▪ 5. Do all QRS complexes look alike? ---------------------------------YES
▪ What is the length of the QRS complexes?▪ Less than 0.12 seconds (3 small squares)

Causes of 2nd Degree AV Block Mobitz Type I (Wenckebach)
▪ ▪May occur normally in an otherwise healthy person
▪ ▪Coronary artery disease
▪ ▪Inferior wall MI
▪ ▪Rheumatic fever
▪ ▪Medications – propanolol, digitalis, verapamil
▪ ▪Increased vagal stimulation

Medical Tx of 2nd Degree AV Block Mobitz Type I (Wenckebach)
No treatment is usually necessary if the patient is asymptomatic
▪ ▪Treat the underlying cause
▪ ▪Monitor closely to detect progression to a more serious form of block, especially if the block occurs during an MI
▪ ▪If symptomatic
▪ ▪Atropine may improve AV node conduction
▪ ▪Temporary pacemaker may help with symptom relief until the rhythm resolves itself

BIGGEST RISK WITH 2nd Degree AV Block Mobitz Type I (Wenckebach )
▪▪Reduced cardiac output, although this is uncommon ▪▪Progression to 3rd degree block

2nd Degree AV Block Mobitz Type II
▪Occurs when there is intermittent interruption of conduction
▪♥Less common that a 2nd Degree Type 1 block, but more dangerous
▪♥PR intervals are regular for conducted beats
▪♥The atrial rhythm is regular
▪♥The ventricular rhythm is irregular due to dropped or nonconducted (blocked) beats

2nd Degree AV Block Mobitz Type II
FIXED PR interval with randomly dropped QRS complexes

5 Steps to Identify 2nd Degree AV Block Mobitz Type II
▪ 1.What is the rate? Varies
▪ 2. What is the rhythm? Ventricular: irregular
▪ 3. Is there a P wave before each QRS? More than one can precede the QRS ▪ Are P waves upright and uniform? Yes, some not followed by a QRS -----Yes, for
conducted beats
▪ 4. What is the length of the PR interval? ------------ Constant for conducted beats
▪ 5. Do all QRS complexes look alike? -----------------------Yes, but may be intermittently absent
▪ What is the length of the QRS complexes? --------Less than or greater than 0.12 seconds

Causes and S/S of 2nd Degree AV Block Mobitz Type II
▪ Anterior wall MI
▪ ▪Degenerative changes in the conduction system
▪ ▪Severe coronary artery disease
▪ uses and S/S of 2nd Degree AV Block Mobitz Type II

Medical Tx of 2nd Degree AV Block Mobitz Type II
▪ May choose to just observe an asymptomatic patient
▪ ▪Bedrest to reduce myocardial oxygen demands
▪ ▪Oxygen therapy
▪ ▪Focus on raising the heart rate to improve cardiac output
▪ ▪Medication
▪ ▪Permanent pacemaker
▪ RISK:
▪ Reduced cardiac output
▪ ▪Progression to 3rd degree AV block (complete)

3rd Degree AV Block Complete heart block, AV dissociation
Is the most serious type of heart block
▪ ♥May progress to asystole, because ventricular rate is usually very slow and ineffective
▪ ♥Impulses from the atria are completely blocked at the AV node and can’t be conducted to the ventricles
▪ P waves are usually march consistently through….NO correlation between P’s & QRS’s
▪ Loss of all communcation between atria & ventricles

3rd Degree AV Block Complete heart block, AV dissociation
P waves are usually march consistently through….NO correlation between P’s & QRS’s

5 Steps to Identify 3rd Degree AV Block
1.What is the rate?----------------------less than 60
▪ 2. What is the rhythm?------------Regular
▪ 3. Is there a P wave before each QRS?--- NO --No relationship to QRS complexes ▪ Are P waves upright and uniform?----Yes What is the length of the
PR interval?-Totally variable, no pattern 4. Is the complex narrow?– No- they are WIDE
▪ 5. Do all QRS complexes look alike? -------------------Yes

Causes and S/S of 3rd Degree AV Block
▪ ▪Congenital condition
▪ ▪Coronary artery disease
▪ ▪Anterior or inferior wall MI
▪ ▪Degenerative changes in the heart
▪ ▪Digitalis toxicity
▪ ▪Surgical injury

Medical Tx of 3rd Degree AV Block
▪ ▪Aim to improve the ventricular rate ▪▪Atropine ▪ Isopreterenol
▪▪Permanent pacemaker

Heart Blocks Made EASY- GOLDEN RULES
▪ Perform a normal interpretation on the tracing
▪ If you find more P waves than QRS complexes do the following:
1. Measure your R-R interval
2. Measure your PR interval
If the R-R interval is CONSTANT, the block must be second degree type 2 or third degree. If the PR interval VARIES– HOW DOES IT VARY??
• If it elongates , the block must be second degree type 1
• If there is NO association, the block must be third degree

Ventricular Rhythms
▪ Objective
▪ Recognize ventricular dysrhythmias on EKG and relate cause, significance, symptoms, and treatment

Ventricular Rhythms ♥
▪ When the sinoatrial (SA) node and the AV Junctional tissues fails to generate an impulse the ventricles will assume the role of pacing the heart
▪ ♥ There is an absence of P waves because there is no atrial activity or depolarization
▪ ♥Ventricular rhythms will display QRS complexes that are wide (greater than or equal to 0.12 seconds) and bizarre in appearance

Ventricular Rhythms
▪ These 8 rhythms are the lethal ones: KNOW THESE
▪ ♥Idioventricular rhythm (ventricular escape rhythm; rate usually >20 – <40 bpm)
▪ ♥Accelerated Idioventricular rhythm (>40 bpm)
▪ ♥Agonal rhythm (20 or less bpm)
▪ ♥Ventricular tachycardia (>150 bpm)
▪ ♥Ventricular fibrillation
▪ ♥Torsades de Pointes
▪ ♥Pulseless Electrical Activity (PEA)
▪ ♥Asystole - Cardiac Standstill

Ventricular Rhythms
Premature Ventricular Contractions
▪ A PVC is not a rhythm, but an ectopic beat that arises from an irritable site in the ventricles.
▪ ▪PVCs appear in many different patterns and shapes, but are always wide and bizarre compared to a “normal” beat

PVC Patterns Ventricular
▪ Ventricular bigeminy PVC occurs every other beat
▪ Ventricular trigeminy PVC occurs every third beat
▪ Ventricular quadrigeminy PVC occurs every fourth beat
▪ Couplets Two PVC’s together
▪ Runs of ventricular tachycardia (VT) Three or more PVC’s in a row

Causes and S/S of PVC’s
▪ Causes
▪ ▪Exercise
▪ ▪Stress
▪ ▪Caffeine
▪ ▪Heart disease: MI, CHF, Cardiomyopathy, Mitral valve prolapse
▪ ▪Electrolyte imbalances
▪ ▪Hypoxia
▪ ▪Tricyclic antidepressants
▪ ▪Digitalis toxicity

Idioventricular Rhythm
Idioventricular arrhythmia is also termed ventricular escape rhythm. It is considered a last-ditch effort of the ventricles to try to prevent cardiac standstill.
▪ ▪The SA node and AV node have failed
▪ ▪Rate usually between 20 to 40 beats per minute (bpm)
▪ ▪Cardiac output is compromised!!
Keys to identifying: rhythm is SLOW, no P wave, wide & bizarre QRS!

5 Steps to Identify Idioventricular Rhythm
▪ What is the rate? Ventricular: 20-40 bpm
▪ 2. What is the rhythm? Usually regular
▪ 3. Is there a P wave before each QRS? Absent
▪ Are P waves upright and uniform? Absent
▪ 4. What is the length of the PR interval? Not measureable
▪ 5. Do all QRS complexes look alike?
▪ What is the length of the QRS complexes? Wide and bizarre (>0.12 sec), with T wave deflection

Causes and S/S of Idioventricular Rhythm Causes •
▪ Causes
▪ •Drugs- Digitalis
▪ •MI
▪ •Metabolic imbalances
▪ •Hyperkalemia
▪ •Cardiomyopathy

Treatment
▪ Medical Treatment
▪ ▪Atropine
▪ ▪Pacing
▪ ▪Dopamine when hypotensive
▪ ▪CPR

Agonal Rhythm
Agonal rhythm is when the Idioventricular rhythm is 20 beats or less per minute. Frequently is seen as the last-ordered semblance of a heart rhythm when resuscitation efforts are unsuccessful

5 Steps to Identify an Agonal Rhythm
▪ What is the rate? Ventricular: <20 bpm VERY SLOW!!
▪ 2. What is the rhythm? Usually regular
▪ 3. Is there a P wave before each QRS? Absent
▪ Are P waves upright and uniform? Absent
▪ 4. What is the length of the PR interval? Not measureable
▪ 5. Do all QRS complexes look alike?
▪ What is the length of the QRS complexes? Wide and bizarre (>0.12 sec), with T wave deflection

Signs and TX of Agonal Rhythm
▪ Signs and Symptoms
▪ ▪Loss of consciousness
▪ ▪No palpable pulse or measurable BP
▪ Medical Treatment
▪ ▪CPR/ACLS Protocol
▪ ▪If life saving efforts have already been attempted no further treatment

Ventricular Tachycardia ▪
▪ Ventricular tachycardia almost always occurs in diseased hearts.
▪ ▪Rhythm in which three or more PVCs arise in sequence at a rate greater than 100 beats per minute.
▪ ▪V-tach can occur in short bursts lasting less than 30 seconds, causing few or no symptoms.
▪ ▪Sustained v-tach lasts for more than 30 seconds and requires immediate treatment to prevent death.
▪ ▪V-tach can quickly deteriorate into ventricular fibrillation.

Ventricular Tachycardia

5 Steps to Identify Ventricular Tachycardia (V-Tach)
▪ 1. What is the rate? 101-250 bpm
▪ 2. What is the rhythm? Atrial rhythm not distinguishable
Ventricular rhythm usually regular
▪ 3. Is there a P wave before each QRS? No
▪ 4. What is the length of the PR interval? Not measureable
▪ 5. Do all QRS complexes look alike?
▪ What is the length of the QRS complexes? Wide and bizarre (>0.12 sec)

Causes of V TACH
▪ Causes
▪ ▪Usually occurs with underlying heart disease
▪ ▪Commonly occurs with myocardial ischemia or infarction
▪ ▪Certain medications may prolong the QT interval predisposing the patient to ventricular tachycardia
▪ ▪Electrolyte imbalance
▪ ▪Digitalis toxicity
▪ ▪Congestive heart failure

Medical Treatment of V Tach
▪ ▪If there is no pulse, begin CPR and follow ACLS protocol
▪ ▪If there is a pulse and the patient is unstable - cardiovert and begin drug therapy
▪ ▪Amiodarone
▪ ▪Lidocaine
▪ ▪With chronic or recurrent VT
▪ ▪Give antiarrhythmics
▪ ▪Ablation may be used for reentry

Ventricular Fibrillation
▪ V-Fib (coarse and fine)
▪ ♥Occurs as a result of multiple weak ectopic foci in the ventricles
▪ ♥No coordinated atrial or ventricular contraction
▪ ♥Electrical impulses initiated by multiple ventricular sites; impulses are not transmitted through normal conduction pathway

Course and Fine V. FIB

5 Steps to Identify Ventricular Fibrillation
▪ 1. What is the rate? Not discernible
▪ 2. What is the rhythm? Rapid, unorganized, not discernable
▪ 3. Is there a P wave before each QRS? No
▪ Are P waves upright and uniform? No
▪ 4. What is the length of the PR interval? None
▪ 5. Do all QRS complexes look alike?
▪ What is the length of the QRS complexes? None

Causes of V FIB
▪ ▪AMI
▪ ▪Untreated VT
▪ ▪Electrolyte imbalance
▪ ▪Hypothermia
▪ ▪Myocardial ischemia
▪ ▪Drug toxicity or overdose
▪ ▪Trauma

Medical treatment
▪ ▪CPR with immediate defibrillation
▪ ▪Initiate ACLS algorithm
▪ IF not patient will DIE

Torsades de Pointes Rhythm ▪
▪ Torsades de pointes is associated with a prolonged QT interval. Torsades usually terminates spontaneously but frequently recurs and may degenerate into ventricular fibrillation.
▪ ▪The hallmark of this rhythm is the upward and downward deflection of the QRS complexes around the baseline. The term Torsades de Pointes means “twisting about the points.”

Torsades Rhythms

5 Steps to Identify Torsades de Pointes
▪ 1. What is the rate? Ventricular: 150-250 bpm
▪ 2. What is the rhythm? Regular or irregular
▪ 3. Is there a P wave before each QRS? No
▪ 4. What is the length of the PR interval? Not measurable
▪ 5. Do all QRS complexes look alike?
▪ What is the length of the QRS complexes? Wide and bizarre, some deflecting downward and some deflecting upward

Medical Treatment for Torsades
▪ Treatment
▪ ▪Begin CPR and other code measures
▪ ▪Eliminate predisposing factors - rhythm has tendency to recur unless precipitating factors are eliminated
▪ ▪Administrate magnesium sulfate bolus
▪ ▪Synchronized cardioversion is indicated when the patient in unstable if possible or defibrillate

Asystole
Ventricular standstill

5 Steps to Identify Asystole
▪ 1. What is the rate? none
▪ 2. What is the rhythm? none
▪ 3. Is there a P wave before each QRS?
▪ Are P waves upright and uniform? none
▪ 4. What is the length of the PR interval? none
▪ 5. Do all QRS complexes look alike?
▪ What is the length of the QRS complexes? none

Treatment of Aysytole
▪▪CPR
▪▪ACLS protocol

Pulseless Electrical Activity (PEA)
Electricity is working, but the mechanics and plumbing are not. ▪The absence of a palpable pulse and absence of myocardial muscle activity with presence of organized electrical activity on the cardiac monitor. The patient is clinically dead despite some type of organized rhythm on monitor.

The H’s
▪ •Hypovolemia #1 cause
▪ •Hypoxia
▪ •Hydrogen ions (acidosis)
▪ •Hypo / Hyperkalemia
▪ •Hypothermia
▪ •

The T’s
▪ •Toxins
▪ •Tamponade (cardiac)
▪ •Tension pneumothorax
▪ •Thrombosis (coronary or pulmonary)
▪ •Trauma
▪ •Massive MI
▪ •Overdose of tricyclic antidepressants

Medical Treatment
▪▪Determine cause & treat
▪▪CPR
▪▪Initiate ACLS protocol

Ectopic and Escape Beats

Ectopic Beats ----aka Ectopy or Arrhythmias
▪ A. Any cardiac impulse originating outside the SA node is considered abnormal and is referred to as an ectopic beat- WILL OCCUR EARLIER DUE TO INCREASE AUTOMATICITY
▪ B. Ectopic beats can originate in the atria, the AV junction, or the ventricles, and are named according to their point of origin
▪ Ectopic beat (or cardiac ectopy) is a disturbance of the cardiac rhythm frequently related to the electrical conduction system of the heart, in which beats arise from fiber or group of fibers outside the region in the heart muscle ordinarily responsible for impulse formation (i.e., the sinoatrial node). Depending upon the origins of the ectopic beat within the myocardium, an ectopic beat can be further classified as either:
▪ a premature ventricular contraction, or
▪ a premature atrial contraction

Causes for ectopic beats include:
▪ 1. Failure or excessive slowing of the SA node
▪ 2. Premature activation of another cardiac site
▪ 3. Abnormal conduction system

Escape Beats
▪ An escape beat is a heart beat arising from an ectopic focus in the atria, the AV junction, or the ventricles – WILL OCCUR LATER DUE TO DELAYED SA NODE FIRING
▪ The usual pacemaker fails, so a slower pacemaker fires at its inherent rate.
▪ Causes:▪ sinus node fails in its role as a pacemaker ▪ when the sinus impulse fails to be conducted to the ventricles as in
complete heart block ▪ The ectopic impulse in this instance is always late, appearing only after the
next anticipated sinus beat fails to materialize

Videos of Heart Rhythms
▪ Heart Rhythms