
Efficacy and safety of high-dose daptomycin for complicated Gram-positive infections
26
Efficacy and safety of high-dose daptomycin for complicated Gram- positive infections • Single-centre retrospective study (2009-2012): N=72 pts (median age: 67 yr) with severe/complicated infections caused by staphylococci/enterococci • Pts treated with high-dose daptomycin (>6 mg/kg) 1x/day as short infusion (renal insufficiency: dosing interval prolonged to 48h) • Median treatment duration: 17 days (range: 5-89 days) • Median follow-up: 21 months (range: 0 days- 3.5 yr) Steinrucken J. ECCMID 2013 abs. P857 1 of 2
-
Upload
stacy-armstrong -
Category
Documents
-
view
31 -
download
3
description
1 of 2. Efficacy and safety of high-dose daptomycin for complicated Gram-positive infections. Single-centre retrospective study (2009-2012) : N=72 pts (median age: 67 yr) with severe/complicated infections caused by staphylococci/enterococci - PowerPoint PPT Presentation
Transcript of Efficacy and safety of high-dose daptomycin for complicated Gram-positive infections

Efficacy and safety of high-dose daptomycin for complicated Gram-positive infections
• Single-centre retrospective study (2009-2012): N=72 pts (median age: 67 yr) with severe/complicated infections caused by staphylococci/enterococci
• Pts treated with high-dose daptomycin (>6 mg/kg) 1x/day as short infusion (renal insufficiency: dosing interval prolonged to 48h)
• Median treatment duration: 17 days (range: 5-89 days)
• Median follow-up: 21 months (range: 0 days- 3.5 yr)
Steinrucken J. ECCMID 2013 abs. P857
1 of 2

Efficacy: Clinical cure: 64 pts (89%)
Safety•Death during hospital stay: 5 pts (7%)
•All AEs resolved after discontinuation of daptomycin
•No correlation between daily or cumulative daptomycin dose and occurrence or severity of AEs
Efficacy and safety of high-dose daptomycin for complicated Gram-positive infections
High-dose daptomycin seems to be highly efficacious for treatment of complicated Gram-pos. infections, but may also cause severe AEs
Steinrucken J. ECCMID 2013 abs. P857
2 of 2
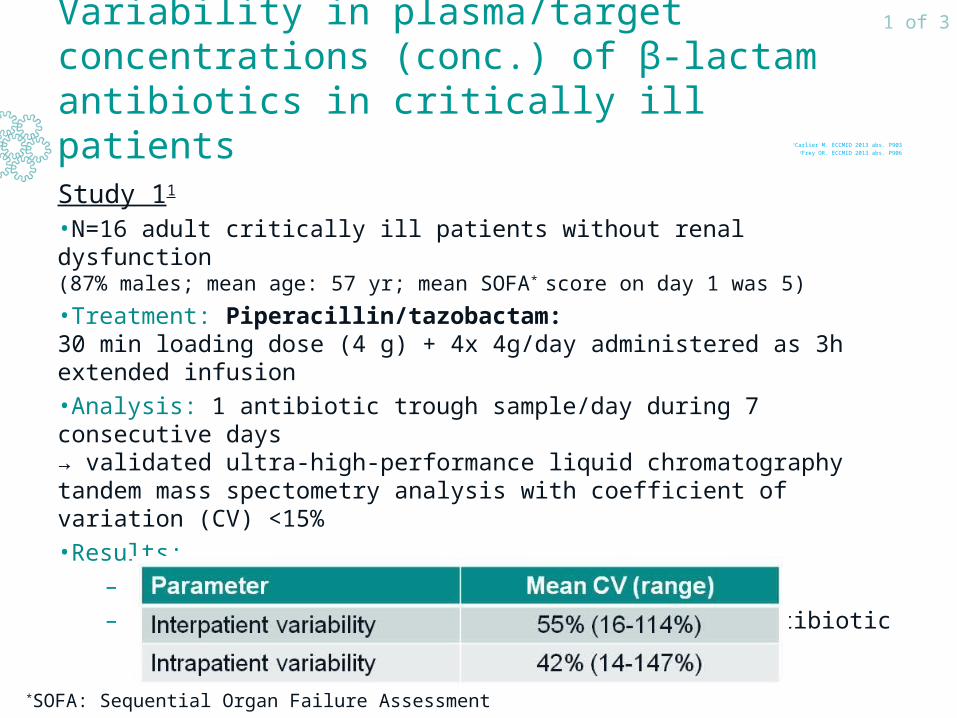
Variability in plasma/target concentrations (conc.) of β-lactam antibiotics in critically ill patients
Study 11
•N=16 adult critically ill patients without renal dysfunction (87% males; mean age: 57 yr; mean SOFA* score on day 1 was 5)
•Treatment: Piperacillin/tazobactam: 30 min loading dose (4 g) + 4x 4g/day administered as 3h extended infusion
•Analysis: 1 antibiotic trough sample/day during 7 consecutive days → validated ultra-high-performance liquid chromatography tandem mass spectometry analysis with coefficient of variation (CV) <15%
•Results:
– 82 antibiotic conc. available
– High intra- and interpatient variability in antibiotic trough conc.: Range: 4-155 mg/l
1Carlier M. ECCMID 2013 abs. P9032Frey OR. ECCMID 2013 abs. P906
1 of 3
*SOFA: Sequential Organ Failure Assessment

Variability in plasma/target concentrations (conc.) of β-lactam antibiotics in critically ill patients
Study 22
•N=238 critically ill pts with severe infections due to Gram-negative bacteria (mean age: 71 yr; mean creatinine clearance: 49 ml/min; mean meropenem clearance: 6.3
l/h; renal replacement therapy: 32% of pts; acute renal failure: 25% of pts)
•Treatment: Meropenem: 8 different dosing regimens; mean duration of therapy: 7.3 days (range: 2-23 days)
•Analysis: Steady state concentrations (Css) of meropenem in serum
•Definitions:
– Target conc.:
• Continuous infusion: Css 8-16 mg/l
• Intermittent bolus injection: drug conc. >8 mg/l for 40% of time – Overdose: AUC24h >768 mg.h/l
(reflecting meropenem dosage >12,000 mg/24h in normal subjects)
•Results: 557 serum levels measured
1Carlier M. ECCMID 2013 abs. P9032Frey OR. ECCMID 2013 abs. P906
2 of 3
Data from poster

Variability in plasma concentrations (conc.) of β-lactam antibiotics in critically ill patients
1Carlier M. ECCMID 2013 abs. P9032Frey OR. ECCMID 2013 abs. P906
3 of 3
Data from poster
Plasma antibiotic concentrations vary greatly within/between pts and also depend on the dosage regimen. Frequent therapeutic drug
monitoring may be warranted to prevent underdosing

Emergence of linezolid (LZD) resistance in coagulase-negative staphylococci (CNS) and Staphylococcus aureus
1Papadimitriou-Olivgeris M. ECCMID 2013 abs. O2782Cafini F. ECCMID 2013 abs. O279
3Grare M. ECCMID 2013 abs. O280
1 of 2

Emergence of linezolid (LZD) resistance in coagulase-negative staphylococci (CNS) and Staphylococcus aureus
• Multivariable analysis1:
1Papadimitriou-Olivgeris M. ECCMID 2013 abs. O2782Cafini F. ECCMID 2013 abs. O279
3Grare M. ECCMID 2013 abs. O280
2 of 2
The emergence of LZD-resistant S. aureus and CNS warrants cautious-ness about the use of LZD and the surveillance of LZD-treated pts

• Multi-centre retrospective study (2008-2011)
Impact of selective oropharyngeal/digestive tract decontamination (SOD/SDD) on antimicrobial resistance in intensive care units (ICUs)
Houben AJM. ECCMID 2013 abs. O344
1 of 2

Impact of selective oropharyngeal/digestive tract decontamination (SOD/SDD) on antimicrobial resistance in intensive care units (ICUs)
Use of SOD or SDD does not seem to increase resistance over time in ICUs. Resistance rates do not seem to differ between ICUs using
SOD, SDD or SC, except for resistance to colistin
Houben AJM. ECCMID 2013 abs. O344
• Average resistance rate per 100 beds per yr for gram-neg. bacteria:– All antimicrobial agents: decreasing time trend in rate of resistant
isolates for SOD, SDD and standard of care (SC) – Tobramycin, ciprofloxacin, ceftazidime, cefotaxime/ceftriaxone:
2008-2011: no significant ≠ between SOD, SDD and SC
– Colistin:• 2008-2011:
– SOD: 2.2x higher risk of resistance than SC(RR: 2.2; 95% CI: 1.4-3.5)
– SDD: 1.5x higher risk of resistance than SC(RR: 1.5; 95% CI: 1.0-2.4)
• 2011 only: no significant ≠ between SOD, SDD and SC
2 of 2

Efficacy of fosfomycin in infections caused by extensively drug-resistant (XDR) and pan-drug-resistant (PDR) Gram-negative pathogens in critically ill ICU patients
• Multi-centre prospective observational study (Greece; 12 intensive care units (ICUs); 2010-2012)
• N=48 critically ill pts suffering from serious, microbiologically documented infections with XDR and PDR (but fosfomycin-susceptible) Gram-negative strains; treated with fosfomycin
• Fosfomycin treatment regimen:
– 6 g iv 2h infusion every 6h
– Median duration of treatment: 12 days
Pontikis K. ECCMID 2013 abs. P2112
1 of 2
Data from poster

Efficacy of fosfomycin in infections caused by extensively drug-resistant (XDR) and pan-drug-resistant (PDR) Gram-negative pathogens in critically ill ICU patients
As fosfomycin seems to have a considerable efficacy and acceptable safety, and development of resistance occurs infrequently, it may be
useful for treatment of PDR and XDR infections in critically ill pts
Pontikis K. ECCMID 2013 abs. P2112
Efficacy
14-day survival: 77.1% − 28-day survival: 62.5%
Microbiological outcomes
Safety
•Most frequent adverse event: Severe hypokalaemia (reversible): N=10
•Treatment termination due to adverse events: N=4
2 of 2
Data from poster
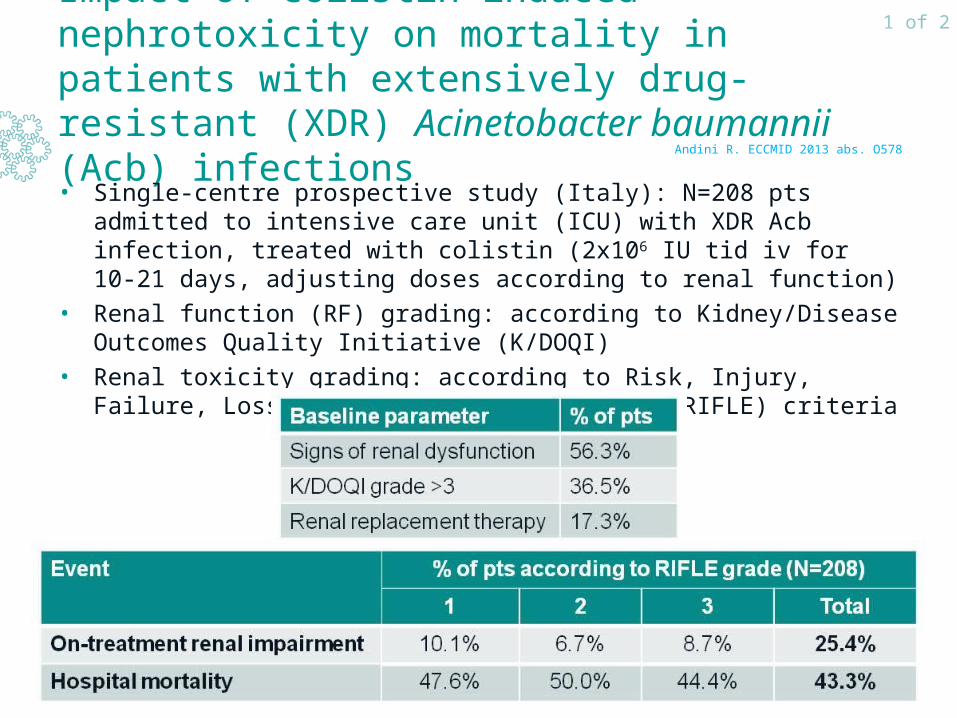
Impact of colistin-induced nephrotoxicity on mortality in patients with extensively drug-resistant (XDR) Acinetobacter baumannii (Acb) infections
• Single-centre prospective study (Italy): N=208 pts admitted to intensive care unit (ICU) with XDR Acb infection, treated with colistin (2x106 IU tid iv for 10-21 days, adjusting doses according to renal function)
• Renal function (RF) grading: according to Kidney/Disease Outcomes Quality Initiative (K/DOQI)
• Renal toxicity grading: according to Risk, Injury, Failure, Loss, End Stage Kidney Disease (RIFLE) criteria
Andini R. ECCMID 2013 abs. O578
1 of 2
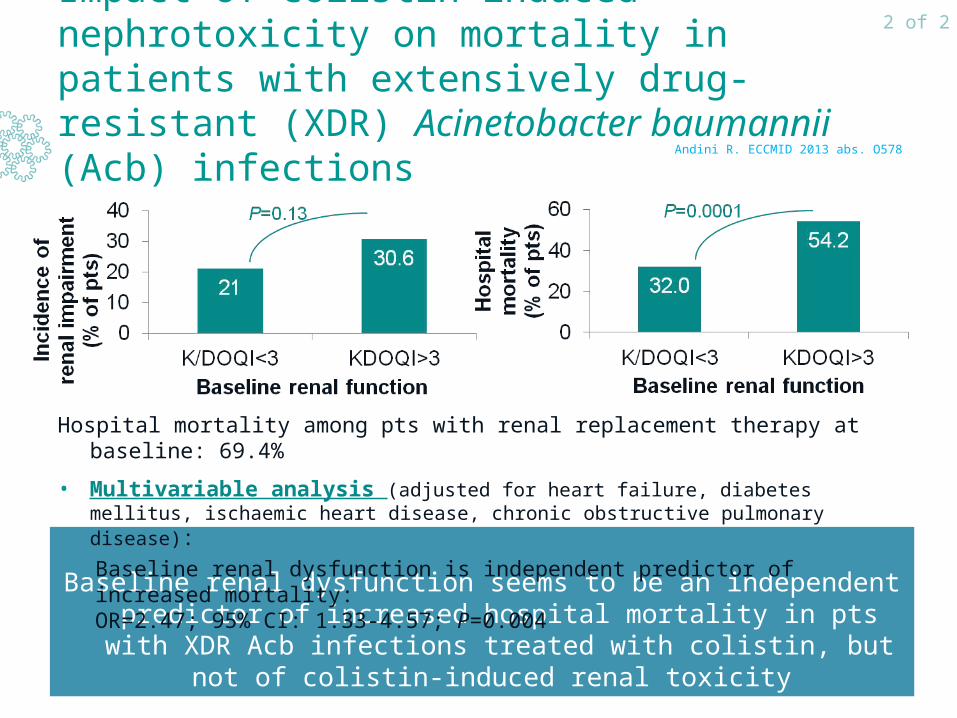
Impact of colistin-induced nephrotoxicity on mortality in patients with extensively drug-resistant (XDR) Acinetobacter baumannii (Acb) infections
Baseline renal dysfunction seems to be an independent predictor of increased hospital mortality in pts with XDR Acb infections treated
with colistin, but not of colistin-induced renal toxicity
Andini R. ECCMID 2013 abs. O578
Hospital mortality among pts with renal replacement therapy at baseline: 69.4%
• Multivariable analysis (adjusted for heart failure, diabetes mellitus, ischaemic heart disease, chronic obstructive pulmonary disease):
Baseline renal dysfunction is independent predictor of increased mortality:OR=2.47; 95% CI: 1.33-4.57; P=0.004
2 of 2

Impact of azithromycin on risk of cardiovascular (CV) death
• Retrospective cohort study (Tennessee Medicaid cohort; 1992-2006) in pts (30-74 yr) who had been prescribed azithromycin (excluding pts who had life-threatening non-CV illness, diagnosis of drug abuse, who were hospitalisated in prior 30 days or resided in nursing home during previous year)
• Study group: Azithromycin: N=347,795 prescriptions*
• Control groups:– No antibiotics: N=1,391,180 propensity-score-matched control periods
(of similar length to the courses of antibiotic therapy)
– Amoxicillin: N=1,348,672 prescriptions
• Primary endpoints:
– CV death
– Death from any cause
• Most common indications for azithromycin/amoxicillin prescription: infections of ear, nose, throat, bronchitis (62/63%)
• Amoxicillin vs no antibiotics: no significant ≠ in risk of (CV) death
Ray WA et al. N Engl J Med 2012;366:1881-90
1 of 2

Impact of azithromycin on risk of cardiovascular (CV) death
During the first 5 days of therapy, azithromycin seems to increase the risk of CV death compared with amoxicillin/no antibiotics, especially
in pts with a high baseline risk of CV disease
Ray WA et al. N Engl J Med 2012;366:1881-90
2 of 2

Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-Kp) during ICU stay
• Single-centre retrospective study (Greece; 2-year period): N=273 intensive care unit (ICU) pts
+ 5 extra pts admitted to ICU due to bacteraemia
→ 53 pts with KPC-Kp BSI: 30-day mortality: 43.4%
Predictors of KPC-KP BSI during ICU stay (multivariable logistic regression)
Papadimitriou-Olivgeris M. ECCMID 2013 abs. P1365
1 of 2
Data from poster

Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-Kp) during ICU stay
Septic shock, resistance to GENT/CS/TIG, high SAPS II score at onset and high age may predict higher 30-day mortality after KPC-Kp BSI,
while combination therapy may predict lower mortality
Papadimitriou-Olivgeris M. ECCMID 2013 abs. P1365
Independent predictors of 30-day mortality (multivariable logistic regression)
2 of 2
Data from poster

Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-Kp)
• Multi-centre retrospective cohort study (Italy; 2010-2011): N=125 pts with bloodstream infection (BSIs) caused by KPC-Kp isolates
• Primary outcome: Death within 30 days of 1st positive blood culture: 52/125 pts (41.6%)
Tumbarello M et al. Clin Infect Dis 2012;55:943-50
1 of 2

Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-Kp)
Tumbarello M et al. Clin Infect Dis 2012;55:943-50
• Multivariable logistic regression:
2 of 2
Septic shock at BSI onset, inadequate initial antimicrobial therapy and high APACHE III score may predict higher 30-day mortality after
KPC-Kp BSI, while combination therapy may predict lower mortality

Predictors of colonisation by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-Kp) resistant to colistin (CS) during ICU stay
• Single-centre retrospective study (Greece; 2-year period): N=254 intensive care unit (ICU) pts hospitalised for ≥6 days;
• Rectal samples taken upon ICU admission and 1x/week afterwards
• During 2-year period: 305 KPC-Kp isolates collected (Enterotube IITM BDTM BBLTM; presence of blaKPC gene confirmed by PCR)
Antibiotic susceptibility (agar diffusion method according to CLSI guidelines):
Papadimitriou-Olivgeris M. ECCMID 2013 abs. O343
1 of 2

Predictors of colonisation by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-Kp) resistant to colistin (CS) during ICU stay
The high rate of colonisation of ICU pts by KPC-Kp resistant to colistin warrants cautiousness about the surveillance of CS-treated pts, in
order to avoid patient-patient transmission via the staff
Papadimitriou-Olivgeris M. ECCMID 2013 abs. O343
Multivariable analysis:
2 of 2

Impact of chlorhexidine gluconate (CHG) patient bathing on hospital-acquired and healthcare-associated infections
1Climo MW et al. N Engl J Med 2013;368:533-422Rupp ME et al. Infect Control Hosp Epidemiol 2012;33:1094-100
1 of 3

Impact of chlorhexidine gluconate (CHG) patient bathing on hospital-acquired and healthcare-associated infections
Study 1
•Overall incidence of skin reactions: CHG bathing: 2.0% - control: 3.4%
•No skin reactions related to bathing; 85% of reactions: mild/moderate
1Climo MW et al. N Engl J Med 2013;368:533-422Rupp ME et al. Infect Control Hosp Epidemiol 2012;33:1094-100
2 of 3

Impact of chlorhexidine gluconate (CHG) patient bathing on hospital-acquired and healthcare-associated infections
Study 2•188,859 patient-days; 68,302 CHG baths
•Adherence to CHG bathing: adult critical care units: 90% > other units: 57.7%
•No consistent effect of CHG bathing on other healthcare-associated infections
•No adverse events related to CHG bathing reported
Patient bathing with CHG not only reduces the risk of MDROs and hospital-acquired bloodstream infections in ICU populations, but
may also reduce the risk of CDI in a broad range of hospitalised pts
1Climo MW et al. N Engl J Med 2013;368:533-422Rupp ME et al. Infect Control Hosp Epidemiol 2012;33:1094-100
3 of 3

• Retrospective analysis of 2 large registries: SEIFEM/Fungiscope (2007-2012)
• N=32 pts with haematological conditions (HC) and invasive mucormycosis (IM), treated with lipid formulations of amphotericin B + posaconazole (lip-AmB+POS)
Treatment response (after median follow-up of 3 months)
Response after combination antifungal therapy for invasive mucormycosis in pts with haematological diseases: data from SEIFEM and Fungiscope
Pagano L. ECCMID 2013 abs. P1006
1 of 2

Mortality (at day 90)
13 pts (41%) still alive 12 months after diagnosis without signs of active infection
Univariable logistic regression analysis
Response after combination antifungal therapy for invasive mucormycosis in pts with haematological diseases: data from SEIFEM and Fungiscope
Combination antifungal therapy with Lip-AmB+POS seems to be efficacious in the treatment of IM in pts with haematological diseases
Pagano L. ECCMID 2013 abs. P1006
Data from poster
2 of 2


















