EASING THE PATIENT BURDEN OF PSORIASIS AND … Psoriasis.pdf · EASING THE PATIENT BURDEN OF...
17
EASING THE PATIENT BURDEN OF PSORIASIS AND PSORIATIC ARTHRITIS: THE ROLE OF THE SPECIALTY PHARMACIST Claire Lee, PharmD, CSP, CPHQ Clinical Quality Improvement Supervisor Diplomat Flint, Michigan Pharmacy Accreditation Pharmacy Times Continuing Education is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education. This activity is approved for 1.0 contact hour (0.10 CEU) under the ACPE universal activity number 0290- 0000-16-022-L01-P. The activity is available for CE credit through May 3, 2016. Faculty Disclosure Claire Lee, PharmD, CSP, CPHQ, has the following relevant financial relationships with commercial interests to disclose. – Employee: Diplomat
Transcript of EASING THE PATIENT BURDEN OF PSORIASIS AND … Psoriasis.pdf · EASING THE PATIENT BURDEN OF...

EASING THE PATIENT
BURDEN OF PSORIASIS
AND PSORIATIC ARTHRITIS:
THE ROLE OF THE
SPECIALTY PHARMACIST
Claire Lee, PharmD, CSP, CPHQClinical Quality Improvement Supervisor
DiplomatFlint, Michigan
Pharmacy Accreditation
Pharmacy Times Continuing
Education is accredited by the
Accreditation Council for Pharmacy
Education (ACPE) as a provider of
continuing pharmacy education. This
activity is approved for 1.0 contact
hour (0.10 CEU) under the ACPE
universal activity number 0290-
0000-16-022-L01-P. The activity is
available for CE credit through May
3, 2016.
Faculty Disclosure
Claire Lee, PharmD, CSP, CPHQ, has the following relevant financial relationships with commercial interests to disclose.
– Employee: Diplomat

This activity is sponsored
by Pharmacy Times
Continuing Education and
supported by an educational
grant from Lilly.
Learning Objectives
• Explain the pathophysiology, etiology, prognosis, clinical presentation, and comorbidities associated with psoriasis and psoriatic arthritis
• Identify current and emerging treatment options for psoriasis
• Examine current and emerging treatment options for psoriatic arthritis
• Determine the role of the specialty pharmacist in supporting patient education and adherence for psoriasis and psoriatic arthritis
Overview• Psoriasis
– Chronic inflammatory disorder of the skin
– Affects approximately 3.2% of adults over the age of 20 in the US
• 7.4 million adults over the age of 20 (2013)
• Psoriatic Arthritis
– Chronic systemic inflammatory disease
– Affects between 6 and 42% of patients with psoriasis
– Appears before skin manifestations of psoriasis in approximately 10-15% of
patients
• Both diseases affect male and female patients equally
Rachakonda TD, et al. J Am Acad Dermatol. 2014;70(3):512-516.; Mease PJ, et al. Drugs.
2014;74(4):423-441.; Griffiths CEM, et al. Lancet. 2007;370(9583):263-271.

Pathophysiology
From N Engl J Med, Nestle FO, Kaplan DH, Barker J. Psoriasis, 361(5):496-509.
Copyright © (2009) Massachusetts Medical Society. Reprinted with permission
from Massachusetts Medical Society.
Pathophysiology
Increased levels of pro-inflammatory
mediators
Secretion of inflammatory
cytokines
Long-term (ie, chronic)
disruption of immune cell
signaling
Lasting changes to
underlying cell mechanisms in
the skin and joints
Clinical presentation
Mease PJ, et al. Drugs. 2014;74(4):423-441.
Etiology
• Nine chromosomal loci have been associated with statistically significant linkage to psoriasis (PSORS1-PSORS9).
• Disease concordance studies among twins show that the risk of psoriasis is two-three times higher between monozygotic twins than it is among dizygotic twins.
Genetic Factors
• Infection (ie, streptococcal pharyngitis, HIV)
• Stress, trauma, smoking, cold weather, humidity, diet and obesity
• Drugs (ie, beta-blockers, lithium, anti-malarial, interferon)
Environmental Factors
Nestle FO, et al. NEJM. 2009;361(5):496-509.; Chandran V, et al. J Autoimmuni. 2010; 34(3):J314-321.
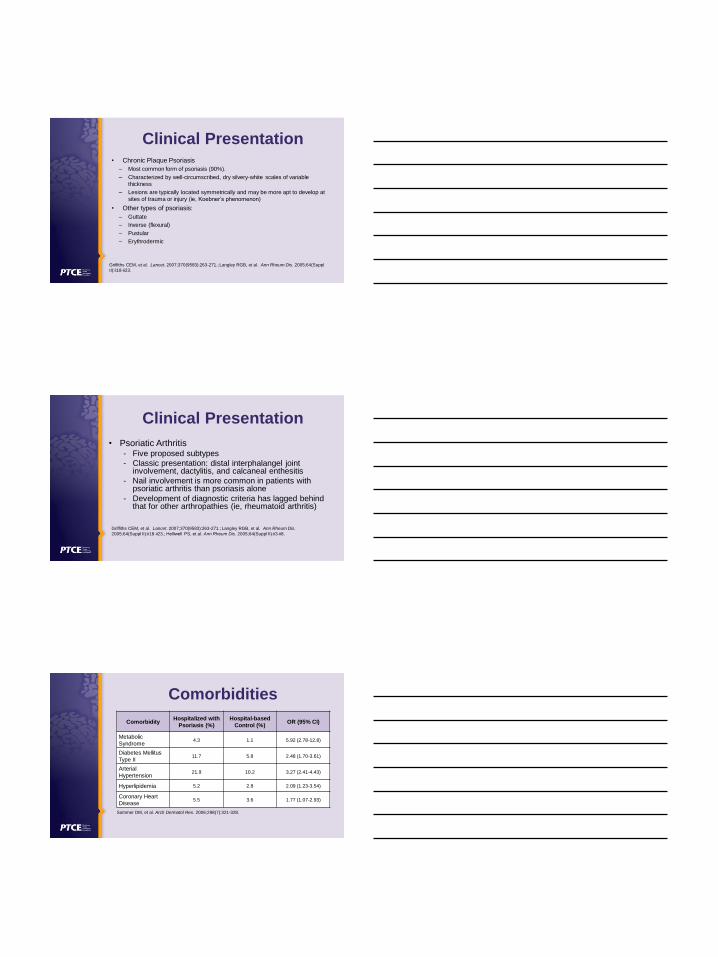
Clinical Presentation• Chronic Plaque Psoriasis
– Most common form of psoriasis (90%).
– Characterized by well-circumscribed, dry silvery-white scales of variable
thickness
– Lesions are typically located symmetrically and may be more apt to develop at
sites of trauma or injury (ie, Koebner’s phenomenon)
• Other types of psoriasis:
– Guttate
– Inverse (flexural)
– Pustular
– Erythrodermic
Griffiths CEM, et al. Lancet. 2007;370(9583):263-271.; Langley RGB, et al. Ann Rheum Dis. 2005;64(Suppl
II):ii18-ii23.
Clinical Presentation
• Psoriatic Arthritis- Five proposed subtypes
- Classic presentation: distal interphalangel joint involvement, dactylitis, and calcaneal enthesitis
- Nail involvement is more common in patients with psoriatic arthritis than psoriasis alone
- Development of diagnostic criteria has lagged behind that for other arthropathies (ie, rheumatoid arthritis)
Griffiths CEM, et al. Lancet. 2007;370(9583):263-271.; Langley RGB, et al. Ann Rheum Dis.
2005;64(Suppl II):ii18-ii23.; Helliwell PS, et al. Ann Rheum Dis. 2005;64(Suppl II):ii3-ii8.
Comorbidities
ComorbidityHospitalized with
Psoriasis (%)
Hospital-based
Control (%)OR (95% CI)
Metabolic
Syndrome4.3 1.1 5.92 (2.78-12.8)
Diabetes Mellitus
Type II11.7 5.8 2.48 (1.70-3.61)
Arterial
Hypertension21.9 10.2 3.27 (2.41-4.43)
Hyperlipidemia 5.2 2.8 2.09 (1.23-3.54)
Coronary Heart
Disease5.5 3.6 1.77 (1.07-2.93)
Sommer DM, et al. Arch Dermatol Res. 2006;298(7):321-328.
Comorbidities• Patients with psoriasis are at least 1.5 times more likely to experience
depression and use more anti-depressant medications than the general
population
• Psychological symptoms may not correlate with disease severity
• Psychosocial effects
– Shame and embarrassment (89%)
– Anxiety (58%)
– Lack of confidence (42%)
– Depression (24%)
– Family friction (26%)
– Reduction in participation in athletic activities (50%)
– Major difficulties at work (44%)
Dowlatshahi EA, et al. J Invest Dermat. 2014;134(6):1542-1551.; Perrott SB, et al. Physiol Behav.
2000;70(5):567-571.; Russo PAJ, et al. Australas J Dermatol. 2004;45(3):155-161.
Characterizing Disease Severity
• Body surface area affected:
• Patients generally categorized as mild-to-moderate or moderate-to-severe
• Moderate-to-severe typically defined as:– Involvement of more than 5% to 10% of body surface area (BSA)
– Involvement of face, palms, or soles of feet– Disease that is otherwise disabling
< 5%
5-10%
> 10%
Mild Psoriasis
Moderate Psoriasis
Severe Psoriasis
Menter A, et al. Lancet. 2007;370(9583):272-284.
Assessment and Prognosis
• Clinical Practice
– Patient interview
• Assessment Tools
– Psoriasis Area and Severity Index (PASI)
– Physician Global Assessment (PGA)
• Static form (standard)
• Dynamic form
– American College of Rheumatology (ACR) 20
• Quality of life assessment
Feldman SR, et al. Ann Rheum Dis. 2005;64(Suppl II):ii65-68.; Mease PJ, et al. Ann Rheum Dis.
2005;64(Suppl II):ii49-ii54.; Krueger GG, et al. J Am Acad Dermat. 2000;43(2 Pt 1):281-285.

Treatment
• Not a curable disease
• Goals of treatment:– Decrease lesion burden
– Improve quality of life
• Treatments categorized:– Topical
– Phototherapy
– Systemic
Menter A, et al. Lancet. 2007;370(9583):272-284.
Treatment
TNF – tumor necrosis factor; MTX - methotrexate
Menter A, et al. Lancet. 2007;370(9583):272-284.
Topical Therapy
• Used for the majority of patients with mild-to-moderate disease (80% of
patients with psoriasis)
• May be used as supportive therapy for resistant lesions in patients with
more extensive disease that are receiving other therapies
• Not recommended as monotherapy for patients with extensive disease
• High efficacy and safety
• Duration of therapy dependent on clinical goals and agent potency
• Adherence is generally poor
Menter A, et al. J Am Acad Dermatol. 2009;60(4):643-659.
Phototherapy
• Despite recent expansion in available
biologic options, it remains an essential
treatment option, Efficacious
– Cost effective
– No risk for systemic immunosuppressive
effects
Menter A, et al. J Am Acad Dermatol. 20010;62(1):114-135.
Traditional Systemic Therapy
• Used when disease is extensive, debilitating, or
severely impacts quality of life
• Continue to play an important role in treatment
• Benefits include ease of administration and low cost (as
compared to biologics)
• Challenges include toxicity and efficacy (as compared to
biologics)
Menter A, et al. J Am Acad Dermatol. 2009;61(3):451-485.
Traditional Systemic Therapy
Common
• Cyclosporine
• Methotrexate
• Acitretin
Less Common (off-label)
• Azathioprine
• Hydroxyurea
• Leflunamide
• Mycophenolate mofetil
• Sulfasalazine
• Tacrolimus
• 6-thioguanine
Menter A, et al. J Am Acad Dermatol. 2009;61(3):451-485.; Rosmarin DM, et al. J Am Acad Dermatol.
2010;62:838-53.; Jeffes EW III, et al. J Invest Dermatol. 1995;104:183-8.; Schiff MH, et al. Ann Rheum
Disease. 2014;73(8):1549-1551.; Soriatane [package insert]. Research Triangle Park, NC: Stiefel Laboratories,
Inc.; 2015.
Traditional Systemic Therapy• The role of methotrexate (MTX)
– Weekly dosages range from 7.5-25 mg
• Titration to optimal dose is recommended
• Consider intramuscular or subcutaneous injection for patients with adherence issues (equal efficacy)
• Patients not benefitting from oral MTX at doses ≥ 15 mg/week may benefit from subcutaneous administration
– Combination therapy
• For patients with psoriatic arthritis
• Evidence indicates combination therapy with etanercept or infliximab
results in better outcomes than biologic monotherapy for the treatment of psoriasis
Menter A, et al. J Am Acad Dermatol. 2009;61(3):451-485.; Jeffes EW III, et al. J Invest Dermatol
1995;104(2):183-188.; Menter A, et al. J Am Acad Dermatol. 2009;61(3):451- 485.; Schiff MH, et al. Ann
Rheum Disease. 2014;73(8):1549-1551.; Gottlieb AB, et al. British Journal of Dermatol. 2012;167(3): 649–
657.; Baranaskaite A, et al. Ann Rheum Disease. 2012;71(4):541-8.
Biologics
TNF-α inhibitors/ blockers
• Adalimumab
• Etanercept
• Golimumab
• Infliximab
IL-17A antagonist
• Ixekizumab
• Secukinumab
IL-12/23 antagonist
• Ustekinumab
Humira [package insert]. North Chicago, IL: AbbVie Inc; 2015.; Cimzia [package insert]. Smyrna, GA: UCB, Inc;
2013.; Enbrel [package insert]. Thousand Oaks, CA: Amgen Inc; 2013.; Simponi [package insert]. Horsham, PA:
Janssen Biotech, Inc; 2013.; Remicade [package insert]. Horsham, PA: Janssen Biotech, Inc; 2013.; Cosenty
[package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.; Stelara [package insert].
Horsham, PA: Janssen Biotech, Inc; 2012.
Pathophysiology Revisited
From N Engl J Med, Nestle FO, Kaplan DH, Barker J. Psoriasis, 361(5):496-509.
Copyright © (2009) Massachusetts Medical Society. Reprinted with permission
from Massachusetts Medical Society.

Biologics
Drug Chronic Plaque Psoriasis Psoriatic Arthritis
Adalimumab X X
Certolizumab pegol X
Etanercept X X
Golimumab X
Infliximab X X
Ixekizumab X
Secukinumab X X
Ustekinumab X X
Humira [package insert]. North Chicago, IL: AbbVie Inc; 2015.; Cimzia [package insert]. Smyrna, GA: UCB, Inc;
2013.; Enbrel [package insert]. Thousand Oaks, CA: Amgen Inc; 2013.; Simponi [package insert]. Horsham, PA:
Janssen Biotech, Inc; 2013.; Remicade [package insert]. Horsham, PA: Janssen Biotech, Inc; 2013.; Taltz [package
insert]. Indianapolis, IN: Eli Lilly and Company; 2016.; Cosenty [package insert]. East Hanover, NJ: Novartis
Pharmaceuticals Corporation; 2015.; Stelara [package insert]. Horsham, PA: Janssen Biotech, Inc; 2012.
Adalimumab
• TNF-α inhibitor
• Subcutaneous administration
• Moderate-to-severe chronic plaque psoriasis
– 80 mg at day 0, followed by 40 mg at day 7 and every other week
thereafter
• Psoriatic arthritis
– 40 mg every other week
• Loss of efficacy after restart; optimal treatment strategy is
continuous use
Humira [package insert]. North Chicago, IL: AbbVie Inc; 2015.; Menter A, et al. J Am Acad Dermatol.
2008;58(5):826-850.; Menter A, et al. J Am Acad Dermatol. 2008;58(1):106-115.
Certolizumab Pegol
• TNF-α blocker
• Subcutaneous administration
• Psoriatic arthritis
– 400 mg at weeks 0, 2, and 4, followed by 200 mg
every other week thereafter
• 400 mg every 4 weeks can be considered for
maintenance therapy
Cimzia [package insert]. Smyrna, GA: UCB, Inc; 2013.

Etanercept
• TNF-α blocker
• Subcutaneous administration
• Plaque psoriasis
– 50 mg twice weekly for 3 months, followed by 50 mg once weekly thereafter
• Psoriatic arthritis
– 50 mg once weekly +/- methotrexate
• Anti-etanercept antibodies possible
– Do not appear to reduce efficacy
• Potential for loss of efficacy over time
Enbrel [package insert]. Thousand Oaks, CA: Amgen Inc; 2013.; Menter A, et al. J Am Acad Dermatol.
2008;58(5):826-850.
Golimumab
• TNF-α blocker
• Subcutaneous administration
• Psoriatic arthritis
– 50 mg once monthly +/- methotrexate
Simponi [package insert]. Horsham, PA: Janssen Biotech, Inc; 2013.
Infliximab
• TNF-α blocker
• Intravenous infusion
• Plaque psoriasis and psoriatic arthritis
– 5 mg/kg at weeks 0, 2, and 6, followed by every 8 wees
thereafter
• Antibodies possible and likely reduce efficacy
– More likely to develop with intermittent therapy
– Continuous therapy is recommended
Remicade [package insert]. Horsham, PA: Janssen Biotech, Inc; 2013.; Menter A, et al. J Am Acad Dermatol.
2008;58(5):826-850.

Ixekizumab
• IL-17A antagonist
• Subcutaneous administration
• Moderate-to-severe plaque psoriasis
– 160 mg at week 0, followed by 80 mg at weeks 2, 4, 6, 8, 10, and 12,
and then 80 mg every 4 weeks thereafter
• Shown to be more efficacious than etanercept in clinical trials
• High levels of response through 60 weeks of treatment
• Most common adverse events: nasopharyngitis, upper respiratory tract infection
Campa M, et al. Dermatol Ther (Heidelb). 2015 Dec 29.; Griffiths CEM, et al. Lancet. 2005;386(9993):541-551.;
Taltz [package insert]. Indianapolis, IN: Eli Lilly and Company; 2016.
Secukinumab• IL-17A antagonist
• Subcutaneous administration
• Moderate-to-severe plaque psoriasis– 300 mg at weeks 0, 1, 2, 3, and 4, followed by 300 mg
every 4 weeks thereafter• For some patients, 150 mg may be acceptable
• Psoriatic arthritis– When psoriasis also present, use plaque psoriasis
dosing
– Psoriatic arthritis only: 150 mg at weeks 0, 1, 2, 3, and 4, and every 4 weeks thereafter
• Shown to be more efficacious than etanercept in the treatment of moderate-to-severe plaque psoriasis
Cosenty [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2015.; Langley RG, et al.
NEJM. 2014;371(4):326-338.
Ustekinumab• IL-12 and IL-23 antagonist
• Subcutaneous administration
• Psoriasis
– Patients weighing ≤ 100 kg (220 lbs): 45 mg at weeks 0 and 4, followed by 45 mg every 12
weeks thereafter
– Patients weighing > 100 kg (220 lbs): 90 mg at weeks 0 and 4, followed by 90 mg every 12
weeks thereafter
• Psoriatic arthritis
– 45 mg at weeks 0 and 4, followed by 45 mg ever 12 weeks thereafter
– 90 mg dosing regimen should be given to patient with co-existent moderate-to-severe
plaque psoriasis weighing > 100 kg (220 lbs)
• Shown to be more effective than etanercept in treating moderate-to-severe
psoriasis
• Biologic least likely to be discontinued
Stelara [package insert]. Horsham, PA: Janssen Biotech, Inc; 2012.; Griffiths CEM, et al. NEJM.
2010;362(2):118-128.

Phosphodiesterase 4 (PDE4)
Inhibition
Schett G, Sloan VS, Stevens RM, Schafer P. Ther Adv Musculoskel Dis.
2010;2(5):271-78. copyright © 2010 by the authors. Reprinted by Permission of
SAGE Publications, Ltd.
Apremilast
• PDE4 inhibitor
• Oral administration
• Moderate-to-severe psoriasis and psoriatic arthritis
– 5 day titration, followed by 30
mg twice daily thereafter
(purpose is to reduce
gastrointestinal adverse effects)
Otezla [package insert]. Summit, NJ: Celgene Corporation; 2014.
Day AM Dose PM Dose
Day 1 10 mg --
Day 2 10 mg 10 mg
Day 3 10 mg 20 mg
Day 4 20 mg 20 mg
Day 5 20 mg 30 mg
Day 6 and
thereafter30 mg 30 mg
Clinical EndpointsDrug PASI 75 ACR 20
Adalimumab 71%-78% 58%
Certolizumab pegol N/A 52-58%
Etanercept 34%-49% 50%
Golimumab N/A 51%
Infliximab 75-88% 58%
Ixekizumab 87-90% N/A
Ustekinumab 65%-78% 42%-50%
Secukinumab 67%-87% 38-42%
Apremilast 29%-33% 32%-41%
Humira [package insert]. North Chicago, IL: AbbVie Inc; 2015.; Cimzia [package insert]. Smyrna,
GA: UCB, Inc; 2013.; Kircik LH, et al. J Drugs Dermatol. 2009;8(6):546-559.; Enbrel [package
insert]. Thousand Oaks, CA: Amgen Inc; 2013.; Simponi [package insert]. Horsham, PA: Janssen
Biotech, Inc; 2013.; Taltz [package insert]. Indianapolis, IN: Eli Lilly and Company; 2016.;
Remicade [package insert]. Horsham, PA: Janssen Biotech, Inc; 2013.; Stelara [package insert].
Horsham, PA: Janssen Biotech, Inc; 2012.; Cosentyx [package insert]. East Hanover, NJ: Novartis
Pharmaceuticals Corporation; 2015.; Otezla [package insert]. Summit, NJ: Celgene Corporation;
2014.

Emerging Therapies
• Agents targeting IL-23– BI-655066
– Guselumab
– Tildrakizumab
• Agents targeting IL-17– Brodalumab
Campa M, et al. Dermatol Ther (Heidelb). 2015 Dec 29.
BI-655066
• Targets IL-23
• Phase II trial (n=166)
– Patients with moderate-to-severely active psoriasis randomly assigned
to receive BI-655066 (18/0, 90/90, or 180/189 mg) or ustekinumab (45
or 90 mg, per weight), subcutaneously, at weeks 0 and 4
– 77.1% of patients receiving BI-655066 achieved PASI 90 after 12
weeks (compared to 40% with ustekinumab)
– Most common adverse effects: runny nose, sore throat, headache
• Trials ongoing
Campa M, et al. Dermatol Ther (Heidelb). 2015 Dec 29.; Papp K, et al. [abstract]. American Academy of
Dermatology; 2015 Mar 20-24; San Francisco, CA.
Guselkumab (CNTO-1959)• Targets IL-23
• Phase II trial (n = 293)
– Double-blind, randomized,
placebo-controlled, dose-
ranging, active-comparator
study
– Results
– Proportion of patients
achieving PGA score of 0 or 1
was significantly higher in the 50, 100, and 200 mg
guselkumab groups than in
the adalimumab group
• Phase III trials ongoing
Treatment
PGA Score of 0
(clear) or 1
(almost Clear at
16 Weeks
PASI 75 at 16
Weeks
Guselkumab 5 mg 34% 44%
Guselkumab 15
mg61% 76%
Guselkumab 50
mg79% 81%
Guselkumab 100
mg86% 79%
Guselkumab 200
mg83% 81%
Adalimumab† 58% 70%
Placebo 7% 5%
† 80 mg at week 0, 40 mg at week 1 and every other week thereafter.
Campa M, et al. Dermatol Ther (Heidelb). 2015 Dec 29.; Gordon KB, et al. NEJM. 2015;373(2):136-144.

Tildrakizumab (MK-3222)
• Targets IL-23
• Phase IIb trial (n = 355)
– Patients randomized to receive
tildrakizumab at a dose of 5, 25,
100, or 200 mg or placebo,
subcutaneously at weeks 0, 4, and
every 12 weeks thereafter
– After 16 weeks, the proportion of
patients achieving PASI 75 was significantly higher, when compared
to placebo, for all doses
– Low relapse rate after cessation of
therapy
• Phase III trials are ongoing
Treatments PASI 75
Tildrakizumab 5 mg 33.3%
Tildrakizumab 25 mg 64.4%
Tildrakizumab 100 mg 66.3%
Tildrakizumab 200 mg 74.4%
Placebo 4.4%
Campa M, et al. Dermatol Ther (Heidelb). 2015 Dec 29.
Brodalumab
• Targets IL-17
• Initially showed very promising results for moderate-to-severe
plaque psoriasis in phase III trials
– PASI 75 in 83-86% of patients after 12 weeks (210 mg dose)
• Phase III trials were halted in May 2015 due to “events of suicidal
ideation and behavior in the brodalumab program, which…likely
would necessitate restrictive labeling”
– Importance of context
• Further development to be determined
Campa M, et al. Dermatol Ther (Heidelb). 2015 Dec 29.; Danesh MJ, et al. JAAD. 2016;74(1):190-192.
Role of the Specialty Pharmacist
• Promote adherence
– Extent to which patients take medications as
prescribed by their health care providers
– Types of adherence
• Intentional (ie, skipping doses, changing the dose,
self-discontinuation)
• Unintentional (ie, forgetfulness, running out,
carelessness)
Cramer J, et al. Value Health. 2008;11(1):44‐7.; Gadkari A , et al. BMC Health Serv Res. 2012;12:98‐110.

Role of the Specialty Pharmacist
• Poor adherence rates– Up to half of patients do not adhere to
treatment
– Most commonly reported reasons:• Lack of efficacy/frustration
• Forgetting
• Too busy
• Regimen too time consuming or inconvenient
Richards HL, et al. J Eur Acad Dermatol Venereol. 2006;20(4):370-9.
Role of the Specialty Pharmacist
• Memory aids
– Pill boxes/dose packaging
• Studies demonstrating impact also utilized educational
interventions
• Motivational interviewing
– Studies in psoriasis significantly demonstrate:
• Reductions in disease severity
• Improvements in psoriasis self-management levels
Lee JK, et al. JAMA. 2006;296(21):2563-71.; Larsen MH, et al. Br J Dermatol. 2014;171(6):1458-69.
Role of the Specialty Pharmacist
• Technology
– Text message interventions in psoriasis
• Included reminders (3x/week) and educational tools (4x/week)
• Significant improvements seen in adherence and disease severity
• Patient access support
– Higher costs are correlated with lower adherence
– Copay assistance helps lower patient cost-share
• Copay cards
• Foundational assistance
Balato N, et al. Br J Dermatol 2013; 168(1):201-205.; Eaddy MT, et al. PT. 2012;37(1):45-55.

Role of the Specialty Pharmacist
• Injection technique
– Patients may be new to injectable medications
– Coach on:
• Storage
• Proper injection sites and rotation
• Injection preparation
• Injection technique
• Proper disposal
Humira [package insert]. North Chicago, IL: AbbVie Inc; 2015.
Role of the Specialty Pharmacist
• Adverse event counseling– Expectation setting
– Adverse event mitigation strategies
• Pharmacists often get questions related to injection site reactions and pain– Symptoms should go away within a few days
– Follow up with provider if persistent
– Review injection technique
• Infections– Follow up with provider; patient may need to interrupt
therapy
Humira [package insert]. North Chicago, IL: AbbVie Inc; 2015.
• Lifestyle modification
– Up-to-date vaccinations
– Healthy diet
– Avoid smoking, minimize alcohol
– Patient must know how to care for their skin
• Hygiene
• Clothing types
• Sun exposure
• Moisturizing
Balato N, et al. Br J Dermatol. 2013; 168(1):201-205.
Role of the Specialty Pharmacist

Additional Resources
• The American Academy of
Dermatology (AAD)
• The National Psoriasis Foundation