Facilities in Tuen Mun ~~ Investigation of people ~~ Conclusion ~~ Introduction ~~ Member list ~~
Upload
dina-harrellCategory
view
225download
1
Early Gastric CancerEarly Gastric Cancer
Dr. LF HungDr. LF Hung
Department of Surgery, Department of Surgery,
Tuen Mun Hospital, HKSARTuen Mun Hospital, HKSAR

BackgroundBackground
In 2005In 2005 1028 new cases of gastric cancer in 1028 new cases of gastric cancer in
Hong KongHong Kong 55thth commonest cancer commonest cancer 44thth major cause of cancer deaths major cause of cancer deaths
(635)(635)

Early Gastric Cancer Early Gastric Cancer (EGC)(EGC)
Definition:Definition: gastric cancer confined to the mucosa or gastric cancer confined to the mucosa or
submucosa, regardless of the presence or absence submucosa, regardless of the presence or absence of lymph node metastasis (T1)of lymph node metastasis (T1)
In JapanIn Japan ~50% patients with gastric cancer present as EGC~50% patients with gastric cancer present as EGC Mean age : 55Mean age : 55
In Western countries:In Western countries: ~ 15% patients with gastric cancer present as ~ 15% patients with gastric cancer present as
EGCEGC Mean age : 63Mean age : 63

Tuen Mun ExperienceTuen Mun Experience A retrospective study for the outcome of early A retrospective study for the outcome of early
gastric cancers from Jan 1999 to June 2006 in gastric cancers from Jan 1999 to June 2006 in TMHTMH
Data was collected from hospital computer Data was collected from hospital computer recordsrecords
All patients with operations done for gastric All patients with operations done for gastric cancers were includedcancers were included
Diagnosis of EGC was confirmed by histologyDiagnosis of EGC was confirmed by histology Survival was analyzed with Kaplan Meier CurvesSurvival was analyzed with Kaplan Meier Curves Cox regression was performed to analysis the Cox regression was performed to analysis the
predictive factors for survivalpredictive factors for survival

TMH figuresTMH figures
298 298 operations for gastric cancers from operations for gastric cancers from Jan 1999- June 2006 in TMHJan 1999- June 2006 in TMH
No. of operation per year
0
10
20
30
40
50
60
70
1999 2000 2001 2002 2003 2004 2005 2006
Year
No.
of
oper
atio
n

Early gastric cancersEarly gastric cancers
38 38 cases of early cases of early gastric cancergastric cancer
All operations for All operations for EGC were EGC were performed with performed with curative intention curative intention
87%
EGC13%
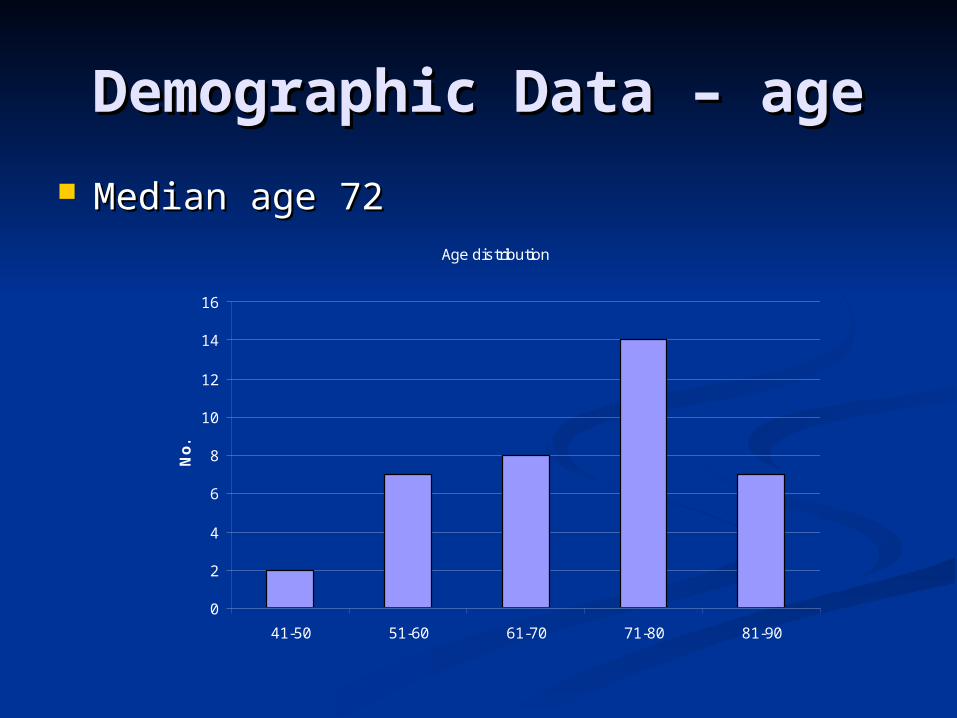
Demographic Data – ageDemographic Data – age
Median age 72Median age 72Age distribution
0
2
4
6
8
10
12
14
16
41-50 51-60 61-70 71-80 81-90
No
.

Demographic Data – sex Demographic Data – sex ratioratio
~ ¾ ~ ¾ of EGC patients are of EGC patients are malemale
female, 10, 26%
male, 28, 74%

Common Presenting Common Presenting symptomssymptoms
Epigastric pain 53%Epigastric pain 53% Upper GIB 34%Upper GIB 34% Anaemia 18%Anaemia 18% Weight loss 5% Weight loss 5%

Co-morbidityCo-morbidity
HypertensionHypertension 34%34%Diabetes MellitusDiabetes Mellitus 29%29%Ischaemic Heart DiseaseIschaemic Heart Disease 17%17%COPDCOPD 13%13%Cerebrovascular AccidentsCerebrovascular Accidents 5%5%Other malignancyOther malignancy 5%5%

EGC Tumor EGC Tumor characteristicscharacteristics
Tumor locationTumor location CardiaCardia 2 (5.2%)2 (5.2%)BodyBody 2 (5.2%)2 (5.2%)Lesser curveLesser curve 5 (13.4%)5 (13.4%)Greater curveGreater curve 2 (5.2%)2 (5.2%)IncisuraIncisura 10 (26.3%)10 (26.3%)AntrumAntrum 15 (39.5%)15 (39.5%)PylorusPylorus 2 (5.2%)2 (5.2%)
Types of operationTypes of operation Total gastrectomyTotal gastrectomy 6 (15.8%)6 (15.8%)Subtotal gastrectomySubtotal gastrectomy 7 (18.4%)7 (18.4%)Distal gastrectomyDistal gastrectomy 25(65.8%)25(65.8%)
All elective surgery with curative intentionAll elective surgery with curative intention

PathologyPathologyHistologyHistology All AdenocarcinomaAll Adenocarcinoma
StagingStaging T1 (mucosal)T1 (mucosal) 3030T1 (submucosal)T1 (submucosal) 88
N0N0 2828N1N1 88N2N2 22M1M1 00
DifferentiationDifferentiation WellWell 44
ModerateModerate 1818
PoorPoor 1616
Cell typeCell type IntestinalIntestinal 1717
DiffuseDiffuse 1515
MixedMixed 66

Cancer-specificCancer-specific survival survival
5 5 yr-survival 88.9%yr-survival 88.9%

Causes of deathsCauses of deaths
2 2 deaths due to tumor recurrencedeaths due to tumor recurrence 1 early post-operative deaths1 early post-operative deaths
Duodenal stump leakageDuodenal stump leakage

Potential predictive Potential predictive factorsfactors
AgeAge SexSex Tumor locationTumor location Type of operationType of operation T stageT stage N stageN stage No. of metastatic LNNo. of metastatic LN No. of LN yieldedNo. of LN yielded Cell typeCell type Degree of differentiationDegree of differentiation

Cox regression – EGC overall Cox regression – EGC overall survivalsurvival
Age is the only significant predictive Age is the only significant predictive factor ( p= 0.001)factor ( p= 0.001)
Other predictive factors are not Other predictive factors are not significantsignificant
Older ageOlder age is associated with medical is associated with medical co-morbiditiesco-morbidities
Japanese studyJapanese study
British Journal of Surgery 2004 4231 patients with EGC studied Overall survival rate and cause of
death analysed

ResultsResults
5- and 10-year cancer-specific survival rates were 98.4 and 96.3
Overall survival rates were 90.2 and 80.9 %
The critical age for determining prognosis was 70 years for men and 75 years for women
Age identified as the most powerful prognostic indicator in EGC
Treatment for EGCTreatment for EGC
Traditionally:Traditionally: Radical surgery with extended Radical surgery with extended
lymphadenectomy (D2 dissection)lymphadenectomy (D2 dissection) Excellent 5 year survival, > 90%Excellent 5 year survival, > 90% Incidence of positive nodes in:Incidence of positive nodes in:
mucosal GC: 1.8% - 5%mucosal GC: 1.8% - 5% submucosal GC: 10%-25%submucosal GC: 10%-25%
EGC rarely spreads beyond the EGC rarely spreads beyond the perigastric nodesperigastric nodes
Question: Is uniform radical surgery and Question: Is uniform radical surgery and D2 dissection always necessary ?D2 dissection always necessary ?

Treatment for EGCTreatment for EGC
Post-gastrectomy morbidity:Post-gastrectomy morbidity: Early and late dumpling syndromeEarly and late dumpling syndrome Reflux esophagitisReflux esophagitis Alkaline regurgitationAlkaline regurgitation Weight lossWeight loss MalabsorptionMalabsorption Vitamin and mineral deficiencyVitamin and mineral deficiency AnaemiaAnaemia Metabolic bone diseaseMetabolic bone disease

Treatment for EGCTreatment for EGC
Current surgical trend:Current surgical trend: Extensive resection Extensive resection Tissue preservation Tissue preservation Uniform performance Uniform performance Individual basis Individual basis Minimizing morbidity and mortalityMinimizing morbidity and mortality Maximizing therapeutic effects and quality Maximizing therapeutic effects and quality
of lifeof life Tissue preservation:Tissue preservation:
““reduced” scope of lymphadenectomyreduced” scope of lymphadenectomy ““reduced” resection of the stomachreduced” resection of the stomach concept of : “less invasive” surgeryconcept of : “less invasive” surgery

Current Treatment Current Treatment StrategiesStrategies
Reduced resection of stomach:Reduced resection of stomach: Endoscopic resection (EMR/ESD) Endoscopic resection (EMR/ESD) Pylorus preserving gastrectomyPylorus preserving gastrectomy Proximal gastrectomyProximal gastrectomy Laparoscopic gastrectomyLaparoscopic gastrectomy
Reduced scope of lymphadenectomy:Reduced scope of lymphadenectomy: Modified D1 dissectionModified D1 dissection Modified D2 dissectionModified D2 dissection

Endoscopic mucosal Endoscopic mucosal resectionresection
Endoscopic mucosal resection (EMR) for EGC: currently standard practice in Japan less invasive and more economical cure can be accomplished by local treatment in
selected cases allows complete pathological staging of the
cancer Accepted indications for EMR are:
(1) well-differentiated elevated cancers less than 2 cm in diameter
(2) small depressed lesions (<1cm) without ulceration
Indication for EMRIndication for EMR
Prediction of lymph node metastasis:Prediction of lymph node metastasis: Lesion < 2 cm sizeLesion < 2 cm size Well or moderately differentiated histologyWell or moderately differentiated histology No macroscopic ulcerationNo macroscopic ulceration Invasive disease limited to mucosa and not Invasive disease limited to mucosa and not
deeper than superficial submucosadeeper than superficial submucosa No lymphovascular invasionNo lymphovascular invasion
If criteria are met: lymph node If criteria are met: lymph node metastasis exist in only 0-4% of metastasis exist in only 0-4% of patientspatients
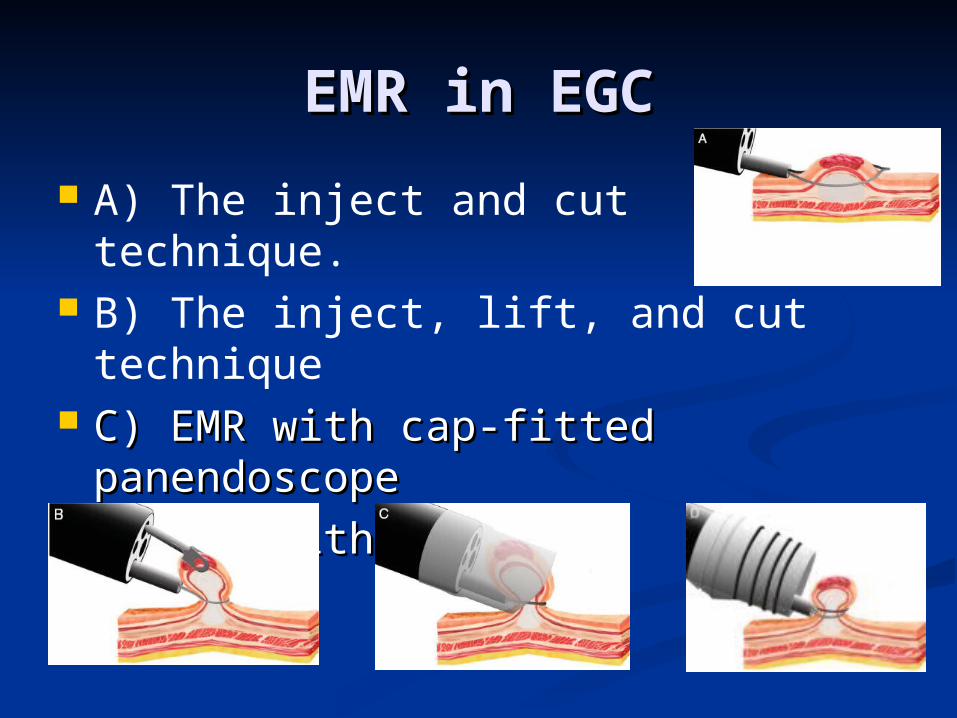
EMR in EGCEMR in EGC
A) The inject and cut technique. B) The inject, lift, and cut technique C) EMR with cap-fitted C) EMR with cap-fitted
panendoscopepanendoscope D) EMR with ligationD) EMR with ligation

EMR in EGCEMR in EGC
Limitation of EMR: Limitation of EMR: cannot be used to resect lesions > 15 mm
in one piece piecemeal resection specimen are difficult
for pathological analysis, causing inadequate staging
high risk of recurrence (up to 35%) Endoscopic submucosal dissection
(ESD), method of en-bloc resection developed

Endoscopic Submucosal Endoscopic Submucosal Dissection Dissection
provides en-bloc specimens precise histological staging and may
prevent disease recurrence requiring significant additional
technical skills longer procedure time

ESD in EGCESD in EGC
Commonly used devices: insulation-tipped diathermy knife (IT
knife) hook knife flex knife
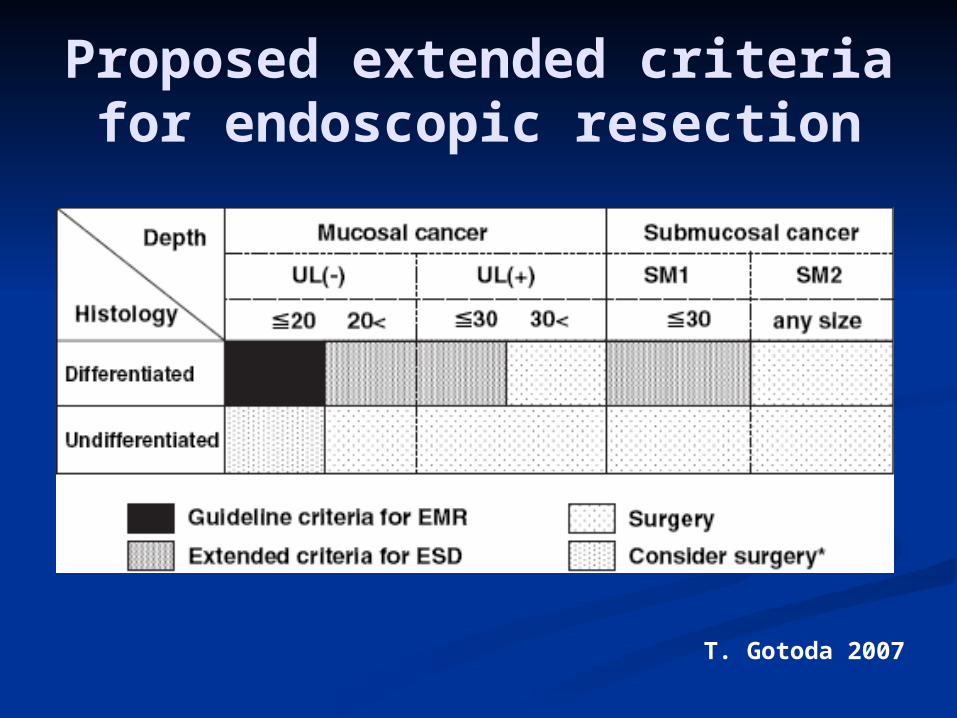
Proposed extended criteria for endoscopic resection
T. Gotoda 2007

Complications of endoscopic Complications of endoscopic resectionresection
PainPain Bleeding:Bleeding:
EMR: 8%EMR: 8% ESD: 7%ESD: 7% Managed by hot biopsy forceps or bipolar Managed by hot biopsy forceps or bipolar
haemostatic forcepshaemostatic forceps Perforation:Perforation:
Uncommon in EMRUncommon in EMR ESD: 4%ESD: 4% Closed with endoclipsClosed with endoclips
Local resection Local resection (EMR/ESD)(EMR/ESD)
Advantage:Advantage: Offer best quality of lifeOffer best quality of life Excellent disease specific survivalExcellent disease specific survival
Disadvantage:Disadvantage: Local recurrence when resection Local recurrence when resection
margin not clearmargin not clear

Current Treatment Current Treatment StrategiesStrategies
Reduced resection of stomach:Reduced resection of stomach: Local resection Local resection Pylorus preserving gastrectomyPylorus preserving gastrectomy Proximal gastrectomyProximal gastrectomy Laparoscopic gastrectomyLaparoscopic gastrectomy
Reduced scope of lymphadenectomy:Reduced scope of lymphadenectomy: Modified D1 dissectionModified D1 dissection Modified D2 dissectionModified D2 dissection

Laparoscopic Laparoscopic gastrectomygastrectomy
Laparoscopic assisted Billroth I Laparoscopic assisted Billroth I Gastrectomy (Kitano 1991)Gastrectomy (Kitano 1991)
Total laparoscopic, laparoscopic Total laparoscopic, laparoscopic assisted, hand-assisted gastrectomyassisted, hand-assisted gastrectomy
Standard D2 LN dissection is Standard D2 LN dissection is technically feasibletechnically feasible

Laparoscopic Laparoscopic gastrectomygastrectomy
Better short term outcome Better short term outcome compared with open gastrectomy :compared with open gastrectomy : decreased paindecreased pain improved pulmonary functionimproved pulmonary function early recovery of bowel functionearly recovery of bowel function shorter hospital stayshorter hospital stay
Comparable oncological clearanceComparable oncological clearance Comparable long term survivalComparable long term survival

Laparoscopic Laparoscopic gastrectomygastrectomy
Technically demandingTechnically demanding Need multicenter RCT to validate Need multicenter RCT to validate
the short term and long term the short term and long term outcome resultsoutcome results

ConclusionConclusion
Routine radical surgery + Routine radical surgery + lymphadenectomy in early gastric lymphadenectomy in early gastric cancer may carry significant cancer may carry significant morbidity and possible mortalitymorbidity and possible mortality
Practice of “less invasive” procedure Practice of “less invasive” procedure can:can: Maintain same therapeutic efficacy Maintain same therapeutic efficacy Improve patient quality of lifeImprove patient quality of life

The EndThe End