
Drug-drug interactions management using...
38
Drug-drug interactions management using DDI-predictor Michel TOD University Hospital from Lyon, France
Transcript of Drug-drug interactions management using...

Drug-drug interactions management
using DDI-predictor
Michel TOD
University Hospital from Lyon, France

Disclosure
Nothing to disclose

Introduction
• DDIs may result in severe adverse events, lack
of efficacy, treatment delay or interruption, ...
• Anticancer drugs have a narrow safety margin
• Yet DDIs on / with anticancer drugs are poorly
documented
• Need for a predictive approach for DDIs

Motivating example (1)
Tamoxifen SPC:
“PK interaction with CYP2D6 inhibitors, showing a 65-75%
reduction in plasma levels of active forms of the drug, has been
reported. Reduced efficacy of tamoxifen has been reported with
concomitant usage of e.g. paroxetine. Co-administration with
potent CYP2D6 inhibitors (e.g. paroxetine, fluoxetine, quinidine,
cinacalcet or bupropion) should whenever possible be avoided.”
A women is treated by Tamoxifen. May Terbinafine be prescribed ?

Motivating example (2)
Terbinafine SPC:
“Terbinafine tablets inhibits the CYP2D6-mediated metabolism. This
finding may be of clinical relevance for compounds predominantly
metabolised by CYP2D6, e.g. tricyclic antidepressants, beta-
blockers, selective serotonine reuptake inhibitors, antiarrhythmics
and monoamine oxidase inhibitors.
Terbinafine tablets decreased the clearance of desipramine by 82%.”
A women is treated by Tamoxifen. May Terbinafine be prescribed ?
Motivating example
• Probably not.
A women is treated by Tamoxifen. May Terbinafine be prescribed ?
• But I am not shure: it depends on the magnitude of the
interaction.
• I need a tool to predict the magnitude of interactions.

Overview
1. Definitions and history
2. How to use DDI-predictor
3. Principle, validation and limits of the approach
4. Case studies

Definitions and history

Kinetics of a metabolic DDIProfile of the substrate average concentration
1: substrate alone
2: substrate + compet. inhibitor
3: substrate + suicide inhibitor
4: substrate + inductor
End of interactor administration
Substrate + interactor
Time (days)
Co
nce
ntr
atio
n

Magnitude of a DDI
10
The magnitude of a DDI is measured by the ratio of AUCs
at steady-state :
RAUC = AUC of the substrate administered with the interactor
AUC of the substrate alone

Interpretation of the AUC ratio
Lack of interaction: RAUC = 1
In case of inhibition: RAUC > 1
In case of induction: RAUC < 1
Dosing adaptation
Ajusted dose (mg/d) = Usual dose (mg/d) / RAUC

Brief History (1)
Since 2010, the IMSM was extended by our group :
• to other CYPs: 2D6, 2C9, 2C19, 1A2
• to CYP polymorphism
• to cirrhosis
• to DDIs in children and neonates
The In vivo Mechanistic Static Model (IMSM) for prediction
of CYP mediated DDIs was introduced in 2007 by Ohno et al.
• The substrate and the interactor are administered per os

Brief History (2)
Since 2013, the IMSM and the associated library is accessible
through a free academic website :
www.ddi-predictor.org
• Not a simple database !
• Makes predictions for undocumented DDIs (ca. 25000)
• Used for prescription analysis in hospital settings
• About 2000 connections / month worldwide

How to use the website to predict a DDI

Front page

Features

Choose a substrate

Choose e.g. an inhibitor
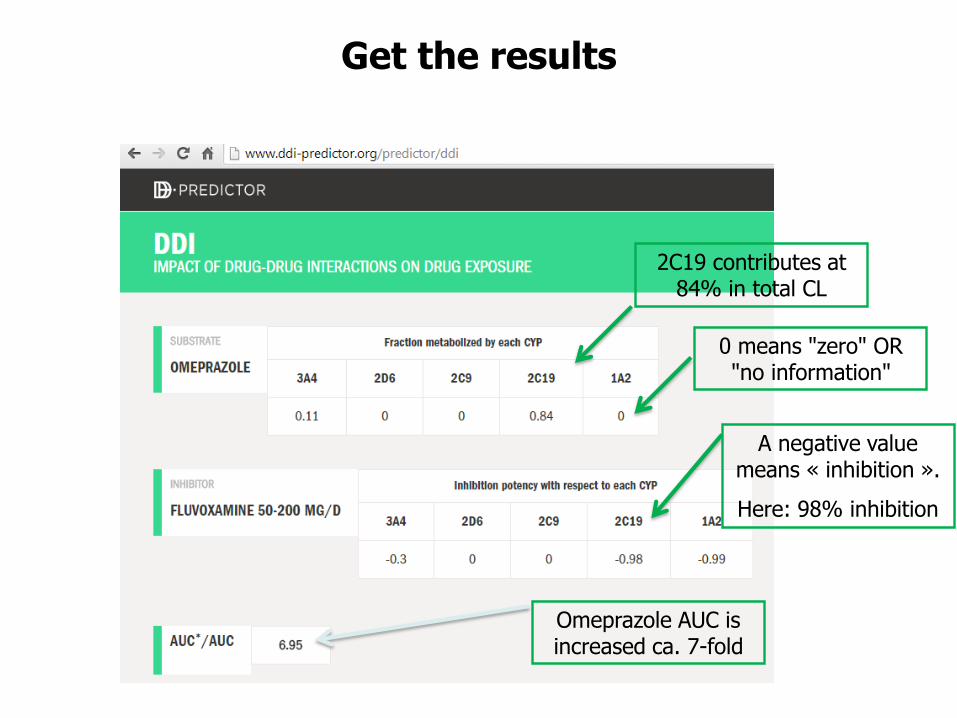
0 means "zero" OR "no information"
Get the results
A negative value means « inhibition ».
Here: 98% inhibition
2C19 contributes at 84% in total CL
Omeprazole AUC is increased ca. 7-fold

Principle, validation and limits

10
Metabolic CL by CYP2D6
10
45
A alone A + B
CYP inhibition = 50%
Renal CL
90
10
A + C
CYP inhibitio
n = 100%
Total CL of A
AUC ratio
100
-
55
100/55
10
100/10
A
Contribution of CYP2D6 in
CL of A
= CR2D6
B C
Fraction of 2D6 inhibited
by B or C
= IX2D6
DDI-predictor Principle Two parameters are needed to predict Rauc

DDI-predictor Principle Substrate: Fraction Metabolised by a CYP
• using the AUC ratio of a DDI study with an inhibitor whose
IR is known
• using the AUC ratio of a pharmacogenetic study in poor
metabolizers
fm
(determined in vitro)
where CR is
CLCYP / CLtotal
CR
(determined in vivo)
replaced by
CR may be estimated:

DDI-predictor Principle Inhibitor: Inhibition Potency IR
• It may be shown that: ( ),
,
/
1 /
h u
h u
I KiIR
I Ki=
+
• IR ranges from 0 to 1 (in absolute value).
Ih,u / Ki
(determined in vitro)
Inhibitor potency IR
(determined in vivo)
replaced by
• IR is estimated using the AUC ratio of a DDI study with a substrate whose CR is known

DDI-predictor Principle
The Static Mechanistic Model of DDI-predictor
1
1 .=
−AUCR
CR IR
• Prediction of an AUC ratio knowing CR and IR (simplest
case):
• Similar approach for induction: inductive capacity IC,
ranging from 0 to infinity (actually, 10).
• Extension to multiple DDIs (= involving several CYPs)

The 3-step Approach:Learning, Confirming, Predicting
Drug 1
Drug 2
Drug
3
Drug 4
Drug 5
Inh. 1
Inh. 2
Inh. 3
Inh. 4
Learning data
Validation data
Unknown data, to be predicted

Estimating Parameters In Vivo Versus In Vitro : What Does It Change?
Alleviate the issues of in vitro-in vivo extrapolation :
• metabolites, enantiomers are not accounted for in vitro
• non metabolic pathways are not accounted for in vitro
• uncertainties on Ki, Ih,u, kinact, etc
• PBPK: scaling factors !! no longer required
BUT cannot be used at the preclinical stage of development

Substrates Inhibitors Inducers
200 100 25
Current state ofthe DDI-Predictor database
Genotypes:
5 genotypes ou groups of genotype
for each of CYP 2D6, 2C9, 2C19

External Validation on 643 Examples
The line is the y = x line. The dashed lines represent the 50–200%interval. Values above x = 1 represent DDIs by inhibition. Valuesbelow x = 1 represents DDIs by induction

Limits of DDI-predictor
• Limited to CYP3A4, 2D6, 2C9, 2C19, 1A2
• Drugs are administered per os
• Substrate PK must be linear (ex: phenytoïn)
• Predictions for a single dose level of the interactor
• Transporters are not explicitly considered : inaccurate
predictions in case of mixed mechanism
• Only two-drug interactions are handled
Temporary

Case studies

Ranking of TKIs by magnitude of interactions mediated by CYP3A4
Substrates CR3A4 Magnitude
Bosu, Dasa, Ibru, Evero > 0.80 +++
Apa, Axi, Crizo, Dabra, Erlo, Gefi, Idela, Ima, Lapa, Nilo, Ola, Palbo, Pazo, Pona, Ruxi, Suni
> 0.3 < 0.8
++
Cabosan, Regora, Vande < 0.3 +
Sorafenib 0.0 0

Undocumented interactions (1)
Back to Tamoxifene + Terbinafine
Active metabolites are decreased 3.2 fold …

Undocumented interactions (2)

Case report : ibrutinib - voricoHistory
• Man 71 years (67 kg), CLL since 2012.
• Prescription of VFEND 250 mg bid for aspergillosis
(liver function is normal).
• Several comedications, no DDI expected.
• Physicians wish to introduce ibrutinib (usual dose in
CLL : 3 capsules at 140 mg per day).

Case report : ibrutinib - vorico Management
How would you manage this treatment?
A. Ibrutinib standard dose 3 x 140 mg / day
B. Ibrutinib à 140 mg once per week
C. Ibrutinib standard dose but switch voriconazole to
itraconazole
D. Ibrutinib standard dose but switch voriconazole to
caspofungine
E. Something else

Case report : ibrutinib - vorico Ask DDI-predictor

• One capsule per week = dose reduction by a factor
3*7 = 21
• BUT ibrutinib peak concentration will still be 8 fold
(25/3) greater than the usual peak ….
• Propose to change antifungal treatment:
caspofungin, ou caspo + 5-flucytosine ?
Case report : ibrutinib - vorico Tentative answer

Conclusion
• DDI-predictor may help to manage some DDIs on
/with anticancer drugs
• Requires however some skills in pharmacokinetics
• IV interactions will also be handled in future
versions


















