Drug Dosing in Renal Insufficiency - Philippine College of ... · Drug Dosing in Renal...
47
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
Transcript of Drug Dosing in Renal Insufficiency - Philippine College of ... · Drug Dosing in Renal...

Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila

Declaration of Conflict of Interest
For today’s lecture on Drug Dosing in Renal Insufficiency, I declare that I have no potential conflict of interest.

Objectives
Discuss the effects of impaired kidney function on drug pharmacokinetics
Describe the principles of pharmacotherapy in patients with renal disease
Calculate drug dosages for patients with renal insufficiency

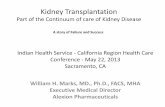
Oral absorption
Elimination
Parenteral drug administration
Tissue receptor action
Systemic Circulation
Protein-bound
Free
Liver First-pass effect
Bioavailability
Kidneys
Parent drug
Active / Inactive metabolites

Drug Pharmacokinetics
Bioavailability % of a drug dose that appears in the central
circulation after oral administration compared to the IV route
Drug distribution Drug metabolism Renal handling

Bioavailability in Renal Insufficiency
Decreased drug absorption Nausea and vomiting Alkalinizing effect of salivary urea Use of PPIs and H2-receptor blockers Use of phosphate binders Gut edema Bacterial colonization Altered intestinal motility
Altered hepatic first-pass metabolism

Bioavailability in CKD
Drug absorption Absolute bioavailability rarely altered
Reduced: furosemide, pindolol
Increased: Beta blockers, dihydrocodeine, dextropropoxyphene
Alterations in peak concentration (Cmax) and time at which peak concentration is attained (Tmax)
There is no quantitative strategy to predict changes for one drug based on data from
another in the same class

Drug Pharmacokinetics
Bioavailability Drug Distribution
Volume of distribution (Vd) ratio of administered dose to the resulting plasma
concentration in equilibrium Dose Blood concentration Useful for predicting loading doses
Plasma protein binding
Vd =

Volume of distribution (Vd) in CKD
Increased Vd
Edema and ascites Hypoalbuminemia Potentially decrease
plasma drug levels of water-soluble and protein-bound drugs
Decreased Vd
Muscle wasting Volume depletion Potentially increase
plasma drug levels of water-soluble drugs

Plasma protein binding in CKD Acidic drugs have reduced plasma protein
binding due to decreased albumin concentration and albumin affinity Unbound fractions may increase
Increased drug toxicity Increased drug metabolism
Lower drug plasma concentrations Altered protein binding may decrease T1/2

Drug Pharmacokinetics
Bioavailability Drug distribution Drug metabolism

Drug metabolism in CKD Slowing down of reduction and hydrolysis
reactions Normal rates of glucuronidation, sulfation,
conjugation and microsomal oxidation reactions Consider adverse effects of pharmacologically
active metabolites Seizures from meperidine Peripheral neuropathy from nitrofurantoin Respiratory depression from morphine
Since there is significant patient variation, no prior assumptions will substitute for careful
clinical evaluation.

Drug Pharmacokinetics
Bioavailability Drug distribution Drug metabolism Renal handling of drugs

Renal handling of drugs Renal excretion dependent on:
Glomerular filtration rate (GFR) Molecular size Protein binding
Tubular secretion May compensate for decreased protein binding
Tubular reabsoprtion
As rate of creatinine clearance (ClCr) decreases, drugs dependent on tubular secretion are also excreted more slowly.
The ClCr is a reasonable estimate of GFR and the tubular capacity for drug excretion.

Renal handling of drugs in CKD
Decreased drug clearance
Prolonged plasma half-life of drugs
Accumulation of ‘active’ drug metabolites
Decreases in renal drug metabolism
Changes in drug distribution: protein binding

Drug metabolism and drug handling in AKI Changes in metabolism
Delayed drug metabolism
Variable effect on hepatic metabolic activity
Reduced drug clearance Hypoxia
Decreased protein synthesis
Competitive inhibition from medications
Decreased hepatic perfusion
There are large gaps in knowledge of drug metabolism and disposition in
patients with multiorgan dysfunction syndrome, multisystem organ failure and AKI; thus, patients are at risk of
underdosing and overdosing.

Mathematics of drug elimination Total body drug clearance = Drug dose AUC
Renal clearance = Total amount of drug in urine
Plasma drug concentration
Renal clearance rate = Clearance Sample collection time
T1/2 = Vd x 0.693 Drug clearance

Application of Pharmacokinetic Parameters
Parameter Clinical Application Bioavailability (F) Determines amount of drug
reaching systemic circulation and
amount at site of action
Volume of distribution (Vd) Determines size of a loading dose
Clearance (C) Determines maintenance dose
Half-life (T1/2) Determines amount of time
needed to reach steady-state
serum concentrations

Approach to adjust drug dosage
1. Obtain history and relevant clinical information.
2. Estimate GFR. 3. Review current medications. 4. Calculate individualized treatment
regimen. 5. Monitor. 6. Revise regimen.
KDIGO 2011

Assessment of kidney function
GFR should be standard measure to evaluate kidney function for drug dosing purposes
Clinicians should use the most accurate method/tool to assess kidney function for the individual patient
KDIGO 2011

Estimation of GFR and Creatinine Clearance Cockcroft and Gault
(140 – age) x Wt (kg) S Cr (mg/dl) x 72
MDRD Study Equation GFR = 175.6 x SCr -1.154 x Age-0.203 x 1.212 [black] x 0.742 [female]
ClCr = x 0.85 (F)

Estimation of GFR and Creatinine Clearance CKD-EPI formula GFR = 141 x min(SCr/κ,1)α x max(SCr/
κ,1)-1.209 x 0.993Age x 1.159 [black] x 1.018 [female]
κ = 0.7 [females], 0.9 [males] α = -0.329 [females], -0.411 [males] Min = minimum of SCr/κ or 1 Max = maximum of SCr/ κ or 1 Age = measured in years

Estimation of GFR in AKI
No estimating equations can provide an accurate estimate of GFR in AKI
Timed clearances of creatinine and urea may be particularly of value for AKI
Measure creatinine clearance with incorporation of mean of the beginning and ending serum creatinine value as an estimate of GFR
KDIGO 2011

Goals of therapy
Maintain efficacy while avoiding drug accumulation and associated adverse reactions. Maintain peak, trough or average
steady-state drug concentration
Optimize time above the MIC or ratio of AUC to MIC

Prescribing for a patient with renal dysfunction
Ascertain level of renal function (% normal ClCr)
Establish integrity of liver metabolism
Establish loading dose
Maintenance dose: dose reduction vs interval extension
Check for drug interactions
Decide on blood level monitoring

Calculating individualized regimen
Loading dose (LD) required if: drug has a long half-life there is need to rapidly achieve desired
steady-state concentration volume of distribution (VD) is significantly
increased
LDPt = Usual LD x VdPt Normal Vd

Calculating individualized regimen
Generally no change in LD EXCEPT for digoxin (50-75% of usual LD due to reduced Vd in renal failure)
With volume contraction, lower standard LD of aminoglycosides by 20-25% to avoid toxicity
In AKI, increased Vd of many drugs, especially hydrophilic antibiotics (Beta lactams, cephalosporins, penems) necessitates administration of aggressive loading doses (25-50% greater)

Calculating individualized regimen
Maintenance dose Prolonging dose interval and maintaining
same dose results in achievement of similar peak and trough concentrations and AUC
Adjust to patient’s renal function, as reflected by the drug’s T1/2
Initiate at normal or near-normal dosage regiments considering the positive fluid balance in early AKI

Calculating individualized regimen
Maintenance dose Changing dosing interval
Normal ClCr
Patient’s ClCr
Reducing dose given at standard intervals
Patient’s ClCr
Normal ClCr
Dosing interval = x Normal interval
Dose = x Normal dose

Calculating individualized regimen
Maintenance dose Changing dosing interval
100
20
Reducing dose given at standard intervals
20
100
Dosing interval = x 8 hours = 40 hrs.
Dose = x 1000 mg = 200 mg

Dtsch Arztebl Int 2010; 107(37): 647–56
ke = 0.693 / T1/2

Calculating individualized regimen
Dettli’s proportionality rules: Rule 1: Dose of a drug must be reduced in
inverse proportion to the T1/2
Rule 2: The interval (Tau) between doses must be prolonged proportionally to the T1/2
D Dnorm T1/2 norm
Tau Taunorm T1/2 = .

Calculating individualized regimen
Dettli’s proportionality rules: If dosing interval unchanged, AUC same but
with higher trough values—may prompt physician to wrongly lower the dose
Implies absurdly low doses or wide intervals between doses

Calculating individualized regimen
Halving rule of Kunin: Starting dose should be the same as the
normal dose, and thereafter half the starting dose should be given at intervals equal to one half-life.
If the half-life is shorter than the dosing interval, dose adjustment is usually unnecessary.
Achieves effective peak levels but markedly higher trough levels more adverse effects.

Dtsch Arztebl Int 2010; 107(37): 647–56

“Go fast, start high”
Calculating individualized regimen
“Start low, go slow”
vs.


Drug dosing considerations for CKD
Drug dosing recommendations may be different from original pharmacokinetic study due to variability in serum creatinine determinations
Use the most appropriate tool to assess kidney function
Drug dosages should be adjusted according to FDA or EMA approved product labeling
KDIGO 2011

Drug dosing considerations for CKD
Peer-reviewed literature recommendations should be used to guide drug-dosage adjustments
Obese CKD patients with large variations in protein levels should have drug dosage individualized based on best available evidence.
KDIGO 2011

Drug level monitoring
Ensures therapeutic levels while avoiding toxicity Measurement of serum drug concentrations
should be done especially for drugs with a narrow therapeutic range
Drug assays only measure total blood concentrations and may underestimate plasma levels or the active or free form of the drug
If not possible, dosage adjustments should be done in the presence of excessive pharmacologic effects or toxicity

Drug dosing considerations for HD
Dose should be given post-HD. Consider supplementary dose in addition to the dose adjusted to kidney failure after HD.
Supplementary dose derived from studies of low-flux membranes should be empirically increased by 50% when using hi-flux dialyzers.
Extended dialysis regimens with high diffusive membranes increase drug clearance and supplementary dose may need to be increased.
KDIGO 2011

Drug dosing considerations for PD
Perform antibiotic loading by an extended cycle in CAPD and APD
Transperitoneal drug movement may be less effective in the acute phase of peritoneal infection when inflammation-related capillary hyperperfusion subsides
Short dwell times in APD may prevent accumulation of antibiotic in the peritoneal cavity.
Monitoring of drug blood levels is advocated.
KDIGO 2011
For most drugs in clinical use, there is little evidence of significant drug removal during
chronic PD.

Key points
Renal dysfunction may result in altered pharmacokinetics and pharmacodynamics of individual drugs.
The goal of therapy is to maintain efficacy while avoiding drug accumulation and associated adverse effects.
An individualized approach is recommended, taking into consideration the integrity of other organ systems and potential drug interactions.

Key points
Monitoring drug levels may be necessary to ensure therapeutic levels while avoiding toxicity.
Physicians should be vigilant in recognizing adverse events.
In the intensive care unit, a “Go fast, start high” policy avoids subtherapeutic blood levels.

Key points
Consider giving scheduled doses after HD sessions OR give supplemental doses immediately post HD
For most drugs in clinical use, there is little evidence of significant drug removal during chronic PD.

References
Am Fam Physician 2007; 75:1487-96