Does witnessing resuscitation help parents come to terms with the death of their child? A review of...
10
Intensive and Critical Care Nursing (2011) 27, 253—262 available at www.sciencedirect.com journal homepage: www.elsevier.com/iccn REVIEW Does witnessing resuscitation help parents come to terms with the death of their child? A review of the literature Kathryn Shaw ∗ , Dawn Ritchie, Gary Adams Queens Medical Centre, Derby Road, Nottingham, United Kingdom Accepted 9 May 2011 KEYWORDS Paediatric; Witnessed; Resuscitation; Parents Summary The aim of this review is to determine if witnessed resuscitation helps parents come to terms with the death of their child. Witnessed resuscitation is a controversial subject. There is disagreement in the literature and the opinions of healthcare professionals, as to whether parents should be present during the resuscitation of their children. This is an international problem that occurs consistently, when caring for patients requiring resuscitation. Despite this, however, research indicates that the advantages of this form of resuscitation for parents far outweigh the disadvantages. Electronic searches of PubMed, CINAHL and OVID were performed, with a manual search of retrieved articles. Primary studies, which were included, examined parents’ views of witnessed resuscitation in children. Of 1038 articles, eight met the inclusion criteria. These included qualitative and quantitative studies, which explored whether parents wanted to be present. The benefits and detrimental effects were explored, in order to determine whether witnessed resuscitation helps parents come to terms with the death of their child. Of 1253 parents, 87.1% wanted to be present. All but one parent believed witnessing resus- citation should be the choice of the parent and all but one parent who was present would do so again indicating that witnessed resuscitation is beneficial to parents. Effective parental support is needed whatever their choice and policies need to be in place to support witnessed resuscitation. More research is required to establish the long term outcomes of witnessed resuscitation as no randomised controlled trials have yet been completed. © 2011 Elsevier Ltd. All rights reserved. Introduction Family-centred care is paramount in caring for the child in hospital, however debate continues as to whether parents ∗ Corresponding author. Tel.: +44 01159515151. E-mail address: kat [email protected] (K. Shaw). should be allowed into the resuscitation room. The Resus- citation Council state that parents should be allowed to remain with their child throughout the resuscitation, how- ever, this is not always adhered to and local policies are often not in place to support this (Resuscitation Council, 2005; Nottingham University Hospitals, 2008). There are many different views on witnessed resus- citation, both from healthcare professionals and family 0964-3397/$ — see front matter © 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.iccn.2011.05.001
-
Upload
kathryn-shaw -
Category
Documents
-
view
223 -
download
4
Transcript of Does witnessing resuscitation help parents come to terms with the death of their child? A review of...

Intensive and Critical Care Nursing (2011) 27, 253—262
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ iccn
REVIEW
Does witnessing resuscitation help parents come toterms with the death of their child? A review of theliterature
Kathryn Shaw ∗, Dawn Ritchie, Gary Adams
Queens Medical Centre, Derby Road, Nottingham, United Kingdom
Accepted 9 May 2011
KEYWORDSPaediatric;Witnessed;Resuscitation;Parents
Summary The aim of this review is to determine if witnessed resuscitation helps parents cometo terms with the death of their child. Witnessed resuscitation is a controversial subject. Thereis disagreement in the literature and the opinions of healthcare professionals, as to whetherparents should be present during the resuscitation of their children. This is an internationalproblem that occurs consistently, when caring for patients requiring resuscitation. Despite this,however, research indicates that the advantages of this form of resuscitation for parents faroutweigh the disadvantages.
Electronic searches of PubMed, CINAHL and OVID were performed, with a manual search ofretrieved articles. Primary studies, which were included, examined parents’ views of witnessedresuscitation in children. Of 1038 articles, eight met the inclusion criteria. These includedqualitative and quantitative studies, which explored whether parents wanted to be present.The benefits and detrimental effects were explored, in order to determine whether witnessedresuscitation helps parents come to terms with the death of their child.
Of 1253 parents, 87.1% wanted to be present. All but one parent believed witnessing resus-citation should be the choice of the parent and all but one parent who was present would do
so again indicating that witnessed resuscitation is beneficial to parents.Effective parental support is needed whatever their choice and policies need to be in place tosupport witnessed resuscitation. More research is required to establish the long term outcomesof witnessed resuscitation as no randomised controlled trials have yet been completed.
ts re
s
© 2011 Elsevier Ltd. All righ
Introduction
Family-centred care is paramount in caring for the child inhospital, however debate continues as to whether parents
∗ Corresponding author. Tel.: +44 01159515151.E-mail address: kat [email protected] (K. Shaw).
creo2
c
0964-3397/$ — see front matter © 2011 Elsevier Ltd. All rights reserved.doi:10.1016/j.iccn.2011.05.001
served.
hould be allowed into the resuscitation room. The Resus-itation Council state that parents should be allowed toemain with their child throughout the resuscitation, how-ver, this is not always adhered to and local policies are
ften not in place to support this (Resuscitation Council,005; Nottingham University Hospitals, 2008).There are many different views on witnessed resus-itation, both from healthcare professionals and family

2
memtvt
A
Trtpoti
bs
tw(1Epe
kadnipo
tm2elaasoU
L
Dswntto
R
Tt
puotT
H
SgsbcdagsowqipTdaesobadw
tistpppaipeHpTdcu
sdmhv
54
embers and deliberation is ongoing (Ardley, 2003; Boiet al., 1999; Madden and Condon, 2007). Part of this argu-ent is based on health professional’s views; however for
he purpose of this review the focus will be on the parents’iews on witnessed resuscitation and any benefits and riskshat this carries.
ims objectives and methology
he aim of this review is to determine whether witnessedesuscitation helps parents come to terms with the death ofheir child. The main objectives were to determine whetherarents wanted to be present during resuscitation attemptsn their child and to determine whether witnessing resusci-ation had any benefits or detrimental effects to the parentsf their child died.
For the purpose of this study, witnessed resuscitation wille defined as cardiopulmonary resuscitation (CPR) which iseen by family members in the acute hospital setting.
The studies retrieved by searching the literature werehe subject of strict inclusion and exclusion criteria andere, if applicable, included in the overview if they were:
1) unsuccessful resuscitation attempts in children in the0 years between 1999 and 2009; (2) were written in thenglish language and (3) the children were defined by therimary study. Studies in adults and pregnant women werexcluded.
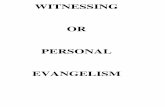
PubMed, CINAHL and OVID were searched with a range ofeywords; the results were then subject to a title, abstractnd full text review, as shown by Fig. 1. Due to the databaseifferences, it was found that differing search terms wereeeded for each to achieve the most results whilst remain-ng relevant. A manual search of reference lists was alsoerformed. Table 1 shows the search terms and the numberf relevant articles retrieved for each.
Whilst randomised controlled trials (RCTs) are seen to behe most rigorous form of research, they are not always theost appropriate (Centre for Reviews and Dissemination,
001). The only such study in the area was prematurelynded due to ethical concerns (Robinson et al., 1998). Thisack of research has meant that papers with both qualitativend quantitative methods have been included in this reviewnd have been critiqued accordingly. In addition, all of thetudies in this review were carried out in the United Statesr Australia and so are not fully relevant to practice in thenited Kingdom.
imitations
ue to the lack of research it has been necessary to includetudies with different methods and varying integrity. Thisas considered acceptable for this review due to the smallumber of relevant studies and the importance of quali-ative opinions. Another limitation is that differing searcherms were used, however this was deemed necessary inrder to find the relevant journal articles.
esults and discussion
he eight papers considered relevant are grouped in rela-ion to both type and location of research. The first three
ascm
K. Shaw et al.
apers explore parent’s views of witnessed resuscitationsing hypothetical scenarios, though using differing meth-ds. Looking at each in turn gives a better understanding ofheir relevance and integrity, the results are summarised inable 2.
ypothetical scenarios
tudies 1—3 utilised hypothetical scenarios, whilst these doive a good insight into the views of parents they lack thetress responses and reflexive decision making that woulde present in an actual resuscitation. Although study 1omprised 400 parents who presented to the emergencyepartment (ED) of a large teaching hospital over 10 weeksnd had a 98% completion rate, the study used only a sin-le interviewer, which could increase interviewer bias. Theurvey included written scenarios, with related questionsn whether the procedure had been witnessed before andhether parents would want to stay. This was in the form of auestionnaire filled in by the parent. The study did not spec-fy or ask for the ages of children, which could have led toarents’ of adult children being recruited (Boie et al., 1999).he ages of children were implied in the study through linerawings (Boie et al., 1999) and although this representsn alternative approach to data information, it could, how-ver, have been missed or misconstrued/misinterpreted byome. Therefore, a clear statement is needed about the agesf children at the start of the survey and additional mem-ers of the interviewing team could have been utilised. Inddition, the study did not record age or ethnicity of respon-ents, however their gender, education level and incomeere included (Boie et al., 1999).
In study 2 the respondents were parents presenting tohe ED with children, therefore eliminating the possibil-ty of them being of adult age (Isoardi et al., 2005). Thistudy examined the parent’s views of witnessed resuscita-ion under hypothetical scenarios, along with other invasiverocedures, and showed a high completion rate of 553 of aossible 573 (96.5%). The study did specifically ask whetherarents would want to be present and this selection couldlso increase parental anxiety even though parents of crit-cally ill children were excluded (Isoardi et al., 2005). Thisrospective written survey recorded the age and sex of par-nts showing that 79% of the 553 respondents were women.owever, it could be argued that this is representative ofarents likely to present with a child needing resuscitation.here is a higher representation of mothers being presenturing this stressful period and additional studies could bearried out, in future work, to establish why there is annder-representation of fathers at resuscitations.
Study 3 used interviewers to approach a convenienceample of 300 parents in the paediatric ED waiting room,uring the day, Monday to Friday (Jones et al., 2005). Theain criticism here stems from the fact that this could
ave introduced an increased bias on the part of the inter-iewer/investigator. In addition the study only includes
limited amount of qualitative information on the rea-ons parents would want to stay or leave. The informationollected by the study remains valuable and includes infor-ation on the parent’s age, gender, education level and

Does witnessing resuscitation help parents come to terms with the death of their child? A review of the literature 255
1,038 Articles found in
searches
937 excluded titles or
not English language
44 excluded abstracts
– adult focussed
- professional views
- not witnessed
resuscitation
101 included titles
57 included abstracts 49 excluded full texts
- adult focussed
- professional views
- literature reviews
8 included full texts
Excluded
Excluded
Excluded
Included
Included
Included
ram
masher
uh2bsa
Figure 1 Flow diag
previous experience of procedures on their child, as wellas the child’s age and gender (Jones et al., 2005).
Emergency department
These studies examined the parents’ responses to pro-cedures, successful or otherwise, carried out within theemergency department. Study 4 examined both resuscita-tion and other invasive procedures with 22 parents from apossible 66, where two witnessed resuscitation (Mangurtenet al., 2006). The survey was adapted from the validated‘Parkland Health and Hospital System’ and the time lag was
three months. This study examines a number of interven-tions, however its generalisability in terms of its findingsare limited, merely due to its small sample size (Mangurtenet al., 2006). The reasons given by parents are still valid andptiT
of included articles.
ay well mirror the thoughts and feelings of other parentsnd relatives in similar situations. Until additional in-depthtudies are carried out healthcare professionals will onlyave the findings of a select few. Whilst information on age,thnicity, education and gender of the parents was given theelevance was not explored.
Study 5 investigated the parents of children, who hadndergone failed resuscitation starting prior to arrival inospital over a year long period (McGahey-Oakland et al.,007). This resulted in ten parents of a possible 25 patientseing interviewed (McGahey-Oakland et al., 2007). Thistudy considered family members who were both presentnd absent, increasing the relevance to this review. The
arent’s age, gender and ethnicity were included, as well ashe child’s age and whether they had an acute life threaten-ng event or chronic illness (McGahey-Oakland et al., 2007).he Parkland survey was used, along with a modified ver-
256 K. Shaw et al.
Table 1 Relevant articles by database.
Database Keywordssearched
Results Relevant titles Relevant or noabstract
Relevant fulltext (unique)
Pubmed ‘Resuscitation’ + ‘families’ + ‘death’ + ‘child’ 89 10 9 2Medline ‘Resuscitation’ + ‘families’ + ‘death’ + ‘child’ 0 0 0 0Medline Resuscitation + child 803 33 23 5CINAHL ‘witnessed
resuscitation’OR‘resuscitation’AND ‘child’ OR‘paediatric’ OR‘paediatric’AND ‘families’OR ‘parent’AND ‘death’
46 27 16 0
10
spTaTaioivtti
P
St6a(hlvpbpstIehewwo1ifO
rwgvaimdei
titmeutbip
C
Sts2rGfar2
Manual search
ion, which had a 70% endorsement by reviewers, for thosearents who were absent (McGahey-Oakland et al., 2007).hree previously validated psychological and mental healthssessments were also used (McGahey-Oakland et al., 2007).his study had a one to two years time lag between the eventnd interview. This could have been minimised by access-ng information as it happened and following up the parentsver time. The use of semi structured interviews with onenterviewer for this study would have increased the internalalidity but could also introduce interviewer bias. In addi-ion the study only examined those parents who wantedo be present for the resuscitation and were happy to benterviewed about their experience.
aediatric Intensive Care Unit
tudies 6 and 7 examined parent responses to resuscita-ion in the Paediatric Intensive Care Unit (PICU). Studyexamined both successful and unsuccessful resuscitation
ttempts, including parents who were present and absentMaxton, 2008). This study also uses a small sample size;owever the study is limited to resuscitation and has a timeag of just three months, using in-depth, unstructured inter-iews (Maxton, 2008). Interviewer bias could have been aroblem in this study as one interviewer appears to haveeen used for all interviews, though this aids continuity. Noarent details were shown; however these have not beenhown to be statistically significant in other studies althoughhese have not given values to show this (Boie et al., 1999;soardi et al., 2005; Jones et al., 2005; McGahey-Oaklandt al., 2007). Study 7 examined parents of children whoad died after resuscitation over a four-year period (Tinsleyt al., 2008). The study used a retrospective questionnaireith two interviewers to analyse parent feelings, location,hether it helped them grieve and whether they would rec-mmend being present to others (Tinsley et al., 2008). Of
15 eligible families, 33 participated, however this resultedn 41 interviews due to both the mother and father of someamilies participating, equating to a 34.8% response rate.f the 41 parents, 20 were not present for their child’sD
Tp
0 31 9 1
esuscitation; two having declined the opportunity and 21ere present (Tinsley et al., 2008). Information on parent’sender, child’s age and time between child’s death and inter-iew were recorded (Tinsley et al., 2008). This study givesgood insight into where parents want to be located dur-
ng their child’s resuscitation and the reasons for this. Theajor flaw in this study is that the interviews were con-ucted up to four years post-resuscitation attempt (Tinsleyt al., 2008); therefore increasing recall bias. However, thencreased sample size is a distinct advantage.
Recall bias may be increased by the stress and trauma ofhe event, as well as the time between the event and thenterview. However, ethically some time is needed to allowhe family to grieve, therefore, some studies allowed threeonths between the event and the interview (Mangurten
t al., 2006; Maxton, 2008). This is preferred to the gap ofp to four years by study 7 (Tinsley et al., 2008). Despitehis, the retrospective method only allows for a small num-er of respondents, therefore the hypothetical studies aremportant to gain the insight of a much larger group ofeople.
ase study
tudy 8 investigated the time spent by a nurse with a familyhrough a failed resuscitation and who met with them againix months later at their request (Dill and Gance-Cleveland,005). The parents were able to see their child undergoingesuscitation but left before the attempt stopped (Dill andance-Cleveland, 2005). Whilst study 8 shows the in-depth
eelings and emotions of one set of parents both during andfter the attempted resuscitation, it lacks the detail andigour to be used independently (Dill and Gance-Cleveland,005).
o parents want to be present?
he hypothetical studies show that out of a total of 1253arents, 87.1% wanted to be present during a resuscitation

Does
witnessing
resuscitationhelp
parentscom
eto
terms
with
thedeath
oftheir
child?A
reviewof
theliterature
257
Table 2 Studies 1—3 are hypothetical studies in the emergency department (ED); Studies 4 and 5 are retrospective studies based in the ED; Studies 6 and 7 are retrospectivestudies based in Paediatric Intensive Care Unit (PICU); Study 8 is a case study of one parent.
Study number Author Year Paper title How the study was carried out Findings of the study
1 Boie, Moore,Brummettand Nelson
1999 Do parents want to be presentduring invasive proceduresperformed on their children inthe emergency department? Asurvey of 400 parents
Prospective written surveywith a 98% response rate from407 potential participants overa 10-week period. Age of childnot specified and the child didnot have to be present in theED. Single research assistantused
83.4% (322 parents) wanted tobe present for resuscitation iftheir child required itBenefits: presence may aid inacceptance of deathDetrimental effects: someparents may want to remembertheir child well rather thanundergoing resuscitation
2 Isoardi,Slabbertand Treston
2005 Witnessing invasive paediatricprocedures, includingresuscitation, in theemergency department: aparental perspective
Prospective written survey with96.5% (553 parents) correctlycompleted. Carried out inpaediatric ED with child’s ageof 0—16 years. Quantitativequestions for whether parentswant to be present and reasons
85% (470) wanted to be presentfor resuscitationBenefits: 98% (542 parents)want to comfort their childDetrimental effects: 33% (181)parents did not want to get inthe way and 22% (122) did notwant to see their child in pain
3 Jones, Qaziand Young
2005 Ethnic differences in parentpreference to be present forpainful medical procedures
Prospective interviews of fourethnic groups. Conveniencesample with 300 parents fromthe paediatric ED waitingroom. Data on wanting to stay,reasons for this, anxiety atprocedures and whether thephysician should determinewhether they should stay
92% (277) wanted to be presentfor resuscitationBenefits: 82% (199 parents)who wanted to stay believedthat the child would wantthem and 57% (137) believedthey would soothe the childDetrimental effects: 77% (44not present parents) believedthey would be too nervous and26% (15) believed they wouldmake the doctor nervous

258K.
Shawet
al.
Table 2 (Continued)
Study number Author Year Paper title How the study was carried out Findings of the study
4 Mangurten,Scott,Guzzetta,Clarke,Vinson,Sperry,Hicks andVoelmeck
2007 Effects of family presenceduring resuscitation andinvasive procedures in apaediatric emergencydepartment
Phone interview of six parentsafter being present for aresuscitation intervention ontheir child, three months afterthe event. Some data includesa further 16 parents who werepresent for invasiveprocedures. This is a 34%response rate; however thesurvey used was adapted froma validated system
100% of parents would bepresent again if they were inthe same situation. Out ofthose who did not participatein the study only two declinedto be present for theinterventionBenefits: 95% of the 22 parentsbelieved that it helped themunderstand their child’scondition and helped thempersonally100% of parents believed ithelped them know everythingpossible had been done fortheir child86% of parents provided healthinformation which could assistin the resuscitationDetrimental effects: 77% of the22 parents asked questions andtwo parents felt faint
5 McGahey-Oakland,Lieder,Young andJefferson
2008 Family experiences duringresuscitation at a children’shospital emergencydepartment
Descriptive, retrospectivestudy interviewing 10 of apossible 25 parents of childrenwho died followingresuscitation which startedprior to arrival in hospital1—2 years between the eventand the interview. Quantitativestudies included a familypresence attitude scale andpsychological and mentalhealth measures. Qualitativequestions were used forinformation on parentexperiences
100% of seven parents presentwere positive about theexperience. No parent statedthat they would not want to bepresent. 100% of 10 parentsbelieved choice was veryimportant. Highlighted thatparents want to be with theirchild quickly and questionscould be asked laterBenefits: parents could seethat everything had been donefor their childHave closure from witnessingthe resuscitationDetrimental effects: stresslevels are higher than thegeneral population but nottraumatic

Does
witnessing
resuscitationhelp
parentscom
eto
terms
with
thedeath
oftheir
child?A
reviewof
theliterature
259
6 Maxton 2008 Parental presence duringresuscitation in the PICU: theparents’ experience
Hermeneuticphenomenological study ofeight parents who had beenpresent or absent duringresuscitation in a PICU. All fourchildren who had parentspresent died. Parents wereinterviewed three months afterthe event using in-depth,unstructured interviews
Study highlights that parentswant to be present during theirchild’s resuscitation. Parentsfocussed on their child ratherthan what was going on aroundthemBenefits: allows parents tounderstand the resuscitationand see that all has been done.Allows parents some sense ofcontrol and to feel they cancomfort their childDetrimental effects: someparents may feel that theyhave to remain when theycannot cope with the situation
7 Tinsley, Hill,Shah, Zim-merman,Wilson,Freier andAbd-Allah
2008 Experience of families duringcardiopulmonary resuscitationin a Paediatric Intensive CareUnit
Retrospective questionnaire toparents whose child died afterundergoing resuscitation inPICU34.8% response rate (41 out of115 parents)Time lag from event tointerview six months to fouryears21 parents were present and 20parents were not present.Included both quantitative andqualitative questions ininterviews with 2 researchers
Whilst 100% (7) of parents ofpreviously healthy childrenwanted to be present, only 47%(16) parents of chronically illchildren didBenefits: 67% (14) of parentswho were present thought ithelped them cope with thedeath as they could seeeverything possible had beendone. 35% (7) of the notpresent group thought it wouldhave made it easier to adjustDetrimental effects: 40% (8) ofparents who were not presentthought witnessing the eventwould have made it harder todeal with and 29% (6) ofparents who were present feltscared. One parent believed noparent should be present forresuscitation

260
Tabl
e2
(Con
tinu
ed)
Stud
ynu
mbe
rAu
thor
Year
Pape
rti
tle
How
the
stud
yw
asca
rrie
dou
tFi
ndin
gsof
the
stud
y
8D
illan
dG
ance
-Cl
evel
and
2005
Wit
hyo
uun
tilt
heen
d:fa
mily
pres
ence
duri
ngfa
iled
resu
scit
atio
n
Case
stud
yof
pare
nts
who
wit
ness
edpa
rtof
thei
rch
ild’s
resu
scit
atio
nat
thei
rre
ques
tan
dw
ere
follo
wed
upsi
xm
onth
sla
ter,
agai
nat
thei
rre
ques
t
Show
son
epa
rent
wan
ted
tobe
pres
ent
duri
ngth
eir
child
’sre
susc
itat
ion
Bene
fits:
allo
ws
the
pare
nts
tose
eth
atev
eryt
hing
isbe
ing
done
for
thei
rch
ildAr
gue
wit
ness
ing
resu
scit
atio
nca
nm
ake
grie
ving
easi
erN
ode
trim
enta
leff
ects
high
light
edin
this
pape
r
aeivwpeeGttsfit(5weot(‘ttlr
B
4im3(ergbserthveT
pspa2Ttopac
td
K. Shaw et al.
ttempt where death is likely (Boie et al., 1999; Isoardit al., 2005; Jones et al., 2005). The studies examin-ng actual resuscitation attempts support this hypotheticaliew that the majority of parents would like the choice ofhether to remain during the resuscitation, showing thatarents feel the need to be with their child in life threat-ning situations (Mangurten et al., 2006; McGahey-Oaklandt al., 2007; Maxton, 2008; Tinsley et al., 2008; Dill andance-Cleveland, 2005). This is shown in study 4 where onlywo of 69 parents declined to be present during interven-ions on their child (Mangurten et al., 2006). Choice washown as an important aspect as whilst some parents wouldnd it difficult to cope with the situation, others would wanto see that everything possible was being done for their childTinsley et al., 2008). All 10 parents interviewed in study
believed the choice was very important; regardless ofhether they were present themselves (McGahey-Oaklandt al., 2007). Choice is supported by study 7, as whilst 100%f the seven parents of previously healthy children wantedo be present, only 47% of the 34 chronically ill children didTinsley et al., 2008). One parent in study 1 highlights thatbecause I am the mother, I have the right to decide whethero leave or go’ (Boie et al., 1999, p. 72). Study 6 highlightedhat if parents choose not to remain then they must be regu-arly updated about the resuscitation as being in the waitingoom increases parental anxiety (Maxton, 2008).
enefits
0% of parents (eight parents) in study 7 believed that com-ng to terms with their child’s death would have been madeore difficult if the resuscitation had been witnessed whilst
5% (seven parents) believed it would have been made easierTinsley et al., 2008). Of those not present 100% (20 par-nts) believed all parents should have the choice, with halfecommending being present (Tinsley et al., 2008). In theroup that were present, 76% (16 parents) recommendedeing present, however one parent believed that parentshould not be present and not be given the choice (Tinsleyt al., 2008). The results support the view that witnessedesuscitation helps parents come to terms with the death ofheir child and seeing that everything possible has been doneelps parents cope, allows them to begin to grieve and pro-ides closure (Dill and Gance-Cleveland, 2005; Mangurtent al., 2006; McGahey-Oakland et al., 2007; Maxton, 2008;insley et al., 2008).
When asked about their activities at the bedside, 100% ofarents (22 parents) in study 4 stated that they emotionallyupported their child and 86% provided health information;arents believed that their presence comforted their childnd reduced their fear (Boie et al., 1999; Isoardi et al.,005; Mangurten et al., 2006; McGahey-Oakland et al., 2007;insley et al., 2008). Study 8 identifies how parents wantedheir child to hear them speak and were thankful for thepportunity (Dill and Gance-Cleveland, 2005). Of note is thatarents asserted that they would not have a problem beingsked to leave if their presence was detrimental to their
hild (McGahey-Oakland et al., 2007).In study 4, 100% (22 parents) ‘agreed or strongly agreedhat being at their child’s bedside was something they wouldo again’ and that it ‘helped them know everything possi-

ith t
scwla
I
Igbiweps2uTcbpvtte
C
Tfitabahac
tchetoptw
R
Irm
Does witnessing resuscitation help parents come to terms w
ble had been done for their child’ (Mangurten et al., 2006,p. 229). Parents who were present had reduced feelings of‘uncertainty, chaos and distress’ (Maxton, 2008, p. 3173).The idea that the witnessing of resuscitation can aid accep-tance of the death is supported by studies 1 and 8 as wellas 67% of the parents (14 parents) in study 7 (Boie et al.,1999; Dill and Gance-Cleveland, 2005; Tinsley et al., 2008).This is supported by one parent who states that ‘when youaren’t there, you don’t know if they did everything’ (Tinsleyet al., 2008, p. 800). Study 5 states that parents begin toaccept their child’s death during the resuscitation, whilststudy 6 highlights the importance to parents of being ableto say ‘goodbye’ (McGahey-Oakland et al., 2007; Maxton,2008).
Parents in the studies did comment that the scene wastraumatic in the short term, but that they focussed ontheir child rather than the resuscitation attempt (Mangurtenet al., 2006; Maxton, 2008). Whilst the stress levels of par-ents were measured in one study, without a greater samplesize and a control group these results cannot be used withconfidence (McGahey-Oakland et al., 2007).
In addition offering witnessed resuscitation allows par-ents to make their own decisions about whether to bepresent and assisting in deciding when to stop a futileattempt can give parents some sense of control (Mangurtenet al., 2006; Maxton, 2008). No parents showed concernabout the resuscitation attempt being too short (McGahey-Oakland et al., 2007); instead parents were more likely toask to stop a futile resuscitation, acting as an advocate fortheir child (Maxton, 2008).
Detrimental effects
The disadvantages of witnessed resuscitation received muchlower response rates than the reasons for staying. Whilstsome parents may want their last memory of their childto be when they were well, as shown in study 2 only 1%of parents (seven parents) believed that their attendancewas not important (Isoardi et al., 2005). Two parents feelingfaint and parents asking questions during the resuscitationwere noted as they could have a direct detrimental effecton the child if they were to distract the resuscitation team(Mangurten et al., 2006). In relation to the parents, 77% (44parents) in study 3 reported feeling too nervous to witnessthe resuscitation (Jones et al., 2005). In addition to this, instudy 7, 29% (six parents) believed that witnessing the resus-citation did not help them cope with their child’s death andone parent suggested that parents should not be allowed towatch their child’s resuscitation in the same way they can-not watch an operation, making it less likely to be beneficialto this individual (Tinsley et al., 2008). Study 7 also reportsthat 40% of the 20 parents who were not present for theirchild’s attempted resuscitation believed that being therewould have made coming to terms with the death more dif-ficult (Tinsley et al., 2008). In addition, parents remainingwith their child as they believe that it to be their respon-sibility, rather than as their choice may have a detrimental
effect on the parents (McGahey-Oakland et al., 2007). Staffcoping mechanisms, such as humour are also challenged withparental presence as it can cause offence if used in front ofparents (Tinsley et al., 2008).nppr
he death of their child? A review of the literature 261
Study 6 highlights that parents need to be appropriatelyupported whether or not they are present for the resus-itation, as well as being able to leave and return as theyish (Maxton, 2008). Incidentally, social workers and chap-
ains are seen to be detrimental by parents as they cannotnswer technical questions (Maxton, 2008).
mprovements
mprovements put forward by parents include: (1) beingiven the choice of whether to stay with their child andeing supported, whatever their decision; (2) being givennformation when in the room or afterwards as they did notant to be delayed in seeing their child (McGahey-Oaklandt al., 2007; Tinsley et al., 2008). The information relayed toarents needs to be frequent, up-to-date and accurate, withimple explanations and straightforward language (Maxton,008; Tinsley et al., 2008). Resuscitation training using sim-lated family members may help with this (Pye et al., 2010).his may influence a hospitals support for witnessed resus-itation as it could be argued that a support person coulde better utilised during the resuscitation and therefore thearents should not be present. However, it is the authors’iew that parents should be supported during the resusci-ation whether at the bedside or in a separate room andherefore the number of staff required should be no differ-nt.
onclusion
he Resuscitation Council have acknowledged the bene-ts of witnessed resuscitation in paediatrics and supporthe practice. However, it is not policy in all paediatricreas and there is still debate surrounding whether it iseneficial (Resuscitation Council, 2005). In order to gainbetter understanding of whether witnessed resuscitation
elps parents come to terms with the death of their childn examination of published studies on resuscitation wasarried out.
Overall, most parents believed that they should be givenhe choice of whether to witness resuscitation, with a signifi-ant majority wanting to be present throughout. However, itas been acknowledged that it would be acceptable for par-nts to be asked to leave if their presence was detrimentalo their child (McGahey-Oakland et al., 2007). The benefitsf offering witnessed resuscitation seem to outweigh theotential risks, with the evidence supporting the argumenthat witnessed resuscitation helps parents come to termsith the death of their child.
ecommendations
n order for all parents to have the choice, witnessedesuscitation needs to be a part of hospital policy. The imple-entation may be argued to increase the staff numbers
eeded for the resuscitation, however the parents are ariority. Support should be from a suitably trained supporterson, knowledgeable about the technical aspects of theesuscitation.

2
itswdhm2
C
N
R
A
B
B
C
D
I
J
M
M
M
M
M
N
P
R
R
62
More research is required in this critical area and thisncludes carrying out randomised clinical trials even thoughhis may be ethically difficult to achieve as RCT’s may beeen as preventing some parents from benefiting. However,ithout this there will be a large number of parents who areenied access to the resuscitation room due to the views ofealthcare professionals who believe that it will have detri-ental effects (Beckman et al., 2002; McClenathan et al.,
002).
onflict of interest statement
o conflicts of interest to disclose.
eferences
rdley C. Should relatives be denied access to the resuscitationroom? Intensive Crit Care Nurs 2003;19:1—10.
eckman A, Sloan B, Moore G, Cordell W, Brizendine E, Boie E, et al.Should parents be present during emergency department proce-dures on children, and who should make that decision? A surveyof emergency physician and nurse attitudes. Acad Emerg Med2002;9(2):154—8.
oie E, Moore G, Brummett C, Nelson D. Do parents want to bepresent during invasive procedures performed on their childrenin the emergency department? A survey of 400 parents. AnnEmerg Med 1999;34(1):70—4.
entre for Reviews and Dissemination. Undertaking SystematicReviews of Research on Effectiveness, 2nd edn. University ofYork; 2001, CRD.
ill K, Gance-Cleveland B. With you until the end: family
presence during failed resuscitation. J Spec Paediatr Nurs2005;10(4):204—7.soardi J, Slabbert N, Treston G. Witnessing invasive paediatricprocedures, including resuscitation, in the emergency depart-
T
K. Shaw et al.
ment: a parental perspective. Paediatr Emerg Med 2005;17:244—8.
ones M, Qazi M, Young K. Ethnic differences in parent prefer-ence to be present for painful medical procedures. Pediatrics2005;116(2):191—7.
adden E, Condon C. Emergency nurses’ current practices andunderstanding of family presence during CPR. J Emerg Nurs2007;33(5):433—40.
angurten J, Scott S, Guzzetta C, Clarke A, Vinson L, Sperry J,et al. Effects of family presence during resuscitation and invasiveprocedures in a pediatric emergency department. J Emerg Nurs2006;32(3):225—33.
axton F. Parental presence during resuscitation in the PICU: theparents’ experience. J Clin Nurs 2008;17:3168—76.
cClenathan B, Torrington K, Uyehara C. Family member presenceduring cardiopulmonary resuscitation: a survey of US and Inter-national critical care professionals. Chest 2002;122(6):2204—11.
cGahey-Oakland P, Lieder H, Young A, Jefferson L. Family expe-riences during resuscitation at a children’s hospital emergencydepartment. J Pediatr Health Care 2007;21(4):217—25.
ottingham University Hospitals. Resuscitation Policy; 2008.http://66.102.9.132/custom?q=cache:bJdJq2ScxQcJ:www.nuh.nhs.uk/about/foi/policies and procedures/clinicalpolices/clinical governance and practice/CLCGP001Resuscitation Policy.pdf+resuscitation+policy&cd=1&hl=en&ct=clnk&client=google-coop-np [accessed 14.1.10].
ye S, Kane J, Jones A. Parental presence during pediatric resusci-tation: the use of simulation training for cardiac intensive carenurses. J Spec Pediatr Nurs 2010;15(2):172—5.
esuscitation Council. Paediatric Advanced Life Support; 2005.http://www.resus.org.uk/pages/pals.pdf [accessed 29.12.09].
obinson S, Mackenzie-Ross S, Campbell Hewson G, Egleston C,Prevost A. Psychological effect of witnessed resuscitation onbereaved relatives. Lancet 1998;352:614—7.
insley C, Hill B, Shah J, Zimmerman G, Wilson M, Freier K, et al.Experience of families during cardiopulmonary resuscitation ina Paediatric Intensive Care Unit. Pediatrics 2008;122(4):799—804.