Does Housing Mobility Policy Improve Health? · between housing and health and briefly discuss...
50
Does Housing Mobility Policy Improve Health? Dolores Acevedo-Garcia, Theresa L. Osypuk, and Rebecca E. Werbel Harvard School of Public Health Ellen R. Meara Harvard Medical School David M. Cutler Harvard University Lisa F. Berkman Harvard School of Public Health Abstract This article summarizes the empirical evidence for the effect of housing mobility poli- cies on health outcomes. Our focus derived from our interest in housing policies that might help reduce health disparities and our finding that, excluding policies concerned with the physical characteristics of housing (e.g., exposure to lead), only housing mobil- ity has been evaluated for its effects on health. We reviewed 13 articles covering five housing mobility studies and ranked them accord- ing to their methodological strength. Although health data have been collected in just a few studies, our review finds that this policy may potentially contribute to improving the health of both adults and children. Yet the empirical evidence is sparse, and only a handful of studies are methodologically sound. To date, the strongest evi- dence derives from the Moving to Opportunity (MTO) demonstration and from the Yonkers evaluation of scattered-site public housing. Keywords: Low-income housing; Neighborhood; Urban policy Introduction The aim of this article is to summarize the research evidence that U.S. housing mobility policies may help improve health outcomes. First, we present a conceptual framework to distinguish various pathways between housing and health and briefly discuss several recent reviews that have examined some of these pathways. Second, we explain our focus on housing mobility policies by highlighting the role that such policies may play in reducing health disparities. Third, we review and assess the research on the health impact of housing mobility policies. Finally, we discuss the implications of our review for future research and data collection and call for expanded long-term follow-up of housing policy demonstrations to determine their health consequences and the mechanisms by which such housing policies could help improve health. Housing Policy Debate · Volume 15, Issue 1 49 © Fannie Mae Foundation 2004. All Rights Reserved. 49
Transcript of Does Housing Mobility Policy Improve Health? · between housing and health and briefly discuss...

Does Housing Mobility Policy Improve Health?
Dolores Acevedo-Garcia, Theresa L. Osypuk, and Rebecca E. WerbelHarvard School of Public Health
Ellen R. Meara Harvard Medical School
David M. CutlerHarvard University
Lisa F. Berkman Harvard School of Public Health
Abstract
This article summarizes the empirical evidence for the effect of housing mobility poli-cies on health outcomes. Our focus derived from our interest in housing policies thatmight help reduce health disparities and our finding that, excluding policies concernedwith the physical characteristics of housing (e.g., exposure to lead), only housing mobil-ity has been evaluated for its effects on health.
We reviewed 13 articles covering five housing mobility studies and ranked them accord-ing to their methodological strength. Although health data have been collected in just a few studies, our review finds that this policy may potentially contribute toimproving the health of both adults and children. Yet the empirical evidence is sparse,and only a handful of studies are methodologically sound. To date, the strongest evi-dence derives from the Moving to Opportunity (MTO) demonstration and from theYonkers evaluation of scattered-site public housing.
Keywords: Low-income housing; Neighborhood; Urban policy
Introduction
The aim of this article is to summarize the research evidence that U.S.housing mobility policies may help improve health outcomes. First, wepresent a conceptual framework to distinguish various pathwaysbetween housing and health and briefly discuss several recent reviewsthat have examined some of these pathways. Second, we explain ourfocus on housing mobility policies by highlighting the role that suchpolicies may play in reducing health disparities. Third, we review andassess the research on the health impact of housing mobility policies.Finally, we discuss the implications of our review for future researchand data collection and call for expanded long-term follow-up of housingpolicy demonstrations to determine their health consequences and themechanisms by which such housing policies could help improve health.
Housing Policy Debate · Volume 15, Issue 1 49© Fannie Mae Foundation 2004. All Rights Reserved. 49

Fannie Mae Foundation
50 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
Housing and health
Historically, housing settlement patterns and conditions have beenclosely linked to the health of the population. The urbanization processthat accompanied the Industrial Revolution in both the United Statesand Western Europe gave rise to an increase in mortality in urbanareas. Infectious disease (e.g., tuberculosis) rates soared because ofincreased population density and overcrowding (Preston and Haines1991). Until the 19th century, both housing policy and public healthpolicy in Britain and other European countries were the responsibilityof a single government entity: the Ministry of Health (Whitehead2000). Although these functions were later separated, it is still commonfor public health practitioners to regard housing as an area for publichealth advocacy and action (Freeman 2002; Krieger and Higgins 2002;Srinivasan, O’Fallon, and Dearry 2003; Thiele 2002).
Although housing has long been hypothesized to affect health, docu-menting this relationship has been challenging. Some authors haveargued that although the role of housing is part of the conventionalwisdom on public health and is presented as a “factual reality that (byimplication) precedes and/or transcends the epistemology of social sci-ence” (Allen 2000, 49), there is in fact limited research evidence thatbad housing causes illness. In an editorial summarizing the findings of a special issue of Housing Studies dedicated to housing and health,Whitehead concluded that “[the articles fell] short of proof, either ofthe cause and effect or of the value of particular interventions, but indoing so [reflected] the current state of understanding of the relation-ship between health and housing” (2000, 339).
Pathways between housing and health
Several recent (2000–2002) reviews have examined the empirical evi-dence that housing has an effect on health. The conclusions are mixed.While some argued that the relationship between housing and health isclearly established (Krieger and Higgins 2002), others found a lack ofevidence (Thomson, Petticrew, and Morrison 2001). Summarizing thesereviews is difficult, however, because they focused on different path-ways between housing and health.
The pathways proposed in the literature can be grouped into threecategories1:
1 This is only one possible framework. Alternatively, Dunn (2002) theorizes that hous-ing affects health via three pathways: material (the role of housing affordability and

Does Housing Mobility Policy Improve Health? 51
1. Housing units as an immediate living environment. Housing unitsmay be the source of exposure to dangerous physical (poorlydesigned stairs), chemical (lead), and biological (cockroach aller-gens) conditions. Most of the literature on housing and health hasfocused on the effect of this material aspect of housing on specificillnesses (Allen 2000; Dunn 2000).
2. Housing as an expression of socioeconomic status. Housing is oftenexamined as a socioeconomic factor, categorized as homelessnessand housing tenure (homeownership status). As suggested by Dunn(2000), the research on homelessness generally has a disease focusand emphasizes the gap between the homeless and the rest of soci-ety, thus ignoring the possibility of a monotonic housing gradient inhealth comprising various aspects of housing, such as tenure, hous-ing wealth, mortgage debt burden, and neighborhood quality. Likeother indicators of socioeconomic status, homeownership displaysan association with health: Namely, people with higher socio-economic status (homeowners) may have better health outcomesthan those with lower socioeconomic status (renters). Some studieshave explored the robustness of predicting health with homeowner-ship as a measure of individual socioeconomic advantage at differ-ent stages of life (Kuh et al. 2002; Robert and House 1996;Wadsworth, Montgomery, and Bartley 1999). The magnitude of thehomeownership effect could be modest at the individual level, aboveand beyond other socioeconomic characteristics. In some healthstudies that controlled for the characteristics of the unit, housingtenure was no longer significant (Allen 2000), suggesting thathomeownership may be better for health because of the better phys-ical condition of the unit. Others have hypothesized that the psy-chosocial benefits of homeownership may be mediated by housingand neighborhood conditions (Kearns et al. 2000). Dunn’s (2000)criticism of the literature on homelessness and health can beapplied to research on homeownership and health, since this bodyof work also tends to overlook the complexity of the housing gradi-ent in health.
3. Locational aspect of housing. The location of housing may influencehealth through access to adequate physical and social environments(safe areas for children to play, social support networks) and publicand private services (policing, transport) (Macintyre and Ellaway2000). A growing literature is documenting the health effects ofneighborhood environments (Ellen, Mijanovich, and Dillman 2001;
Housing Policy Debate
accumulation of wealth, as well as the physical conditions of housing), meaningful (howpeople perceive and internalize their housing circumstances), and spatial (the role ofhousehold location and neighborhood).

Fannie Mae Foundation
52 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
Ellen and Turner 1997; Kawachi and Berkman 2003b; Leventhaland Brooks-Gunn 2000) and segregated housing patterns (Acevedo-Garcia and Lochner 2003; Acevedo-Garcia et al. 2003; Ellen 2000;Williams and Collins 2001). In addition, some studies have tried todisentangle the effect of the quality of the housing unit from thequality of the neighborhood where the unit is located (Kearns et al.2000).
Next, we summarize the findings of some recent reviews of the empiri-cal evidence on the link between housing and health; we place ourreview in the context of other recent work that underscores a renewedinterest in housing issues in the public health field. However, we do notaim to provide a comprehensive meta-analysis of this literature.
In the British Medical Journal, Thomson, Petticrew, and Morrison(2001) examined housing interventions aimed at rehousing and improv-ing infrastructure, defined as heating, double-glazing, and generalrefurbishment.2 They found that although most studies demonstratedsome health gains, small samples and inadequate control for con-founders limited the ability to generalize the findings. In an issue of theAmerican Journal of Public Health dedicated to the built environmentand health, Saegert et al. (2003) reviewed U.S. interventions to improvehealth by modifying housing units from 1990 to 2001 and concluded(1) that most studies addressed a single condition (typically lead poison-ing, injuries, or asthma) and (2) that while most evaluations reportedstatistically significant improvements, only 14 percent were regarded as “extremely successful” (1471).
In an issue of the American Journal of Public Health dedicated to hous-ing, Krieger and Higgins (2002) concluded that “an increasing body ofevidence” (758) has shown that housing as a determinant of health isassociated with various conditions through material aspects of thehousing unit (such as crowding or dampness), socioeconomic aspects(such as housing deprivation and the availability of subsidies), and loca-tional aspects (such as air quality, noise, and fear of crime).
In a review of the North American and British literature in HousingStudies, Dunn (2000) identified three main areas of housing and healthresearch: housing as a social determinant of health (which has beenoften examined in relation to homelessness), the pathological effects ofinadequate housing, and the psychological distress associated with liv-ing in inadequate housing. There is sufficient evidence that homeless-ness is associated with poor physical and mental health and limited
2 These authors excluded interventions to address lead, urea formaldehyde foam, poorair quality, allergens, and radon. No rationale was provided for these exclusions.

Does Housing Mobility Policy Improve Health? 53
access to health care. The literature on the pathological effects of suchhousing attributes as high-rise housing, crowding, dampness, and coldis vast, although Dunn (2000) did not present an assessment of the evi-dence. Research on housing and stress is relatively recent, and the evi-dence is limited. Regarding housing policy, Dunn (2000) found thatthere is equivocal evidence on the effectiveness of British policies aimedat enhancing the health of individuals with medical problems by givingthem priority for public housing.
In 2002, the Centers for Disease Control and Prevention (CDC) TaskForce on Community Preventive Services published a series of litera-ture reviews on policy interventions that could help improve commu-nity health (Anderson et al. 2002). Mixed-income housing and housingvouchers were examined. The authors did not find studies of mixed-income housing that met their design criteria for inclusion in theirreview, but did find sufficient evidence that housing voucher (mobility)policies reduce crime victimization and thus can be recommended. Ourreview differs from the CDC study in four main respects:
1. We examine housing mobility policies in the context of other hous-ing and health research and other housing policies that might helpreduce health disparities.
2. We examine various U.S. housing mobility policies, not just theMoving to Opportunity (MTO) demonstration.
3. We focus on health outcomes, while the CDC also included broadindicators that could have health implications, such as housingquality and neighborhood conditions.
4. In addition to summarizing the evidence, we discuss the design andfindings of each study.3
Methodological challenges in housing and health research
Research on housing and health presents several methodological chal-lenges. First, although there have been important advances in concep-tualizing the relationship between housing and health—for example,Dunn’s (2002) work on the material, meaningful, and spatial dimen-sions of housing—for the most part, conceptual frameworks have yet
Housing Policy Debate
3 Our review is also different from the first cross-site analysis of MTO by Goering,Feins, and Richardson (2002), who focused only on MTO and discussed health as partof a series of MTO outcomes, including crime, education, employment, and reliance onpublic assistance.

to be incorporated into the design of empirical studies. In a review ofthe literature, Allen (2000) concluded that research on housing andhealth has been largely atheoretical. Macintyre and Ellaway (2003)similarly assert that neighborhood and health research lacks theoreti-cal development.
Second, it is difficult to establish whether bad housing leads to poorhealth or vice versa. Most research has focused on cross-sectional sta-tistical associations between housing and health variables. The selec-tion of individuals into housing and neighborhoods presents the largestpotential source of bias in nonexperimental studies (which to date con-stitute the bulk of research in this area), since those with better healthmay be able to settle in better homes and neighborhoods. Researcherstherefore need to construct rigorous research designs to simulate aplausible counterfactual scenario (what would have happened in theabsence of the policy) (Orr 1999) in the absence of randomized designs(e.g., quasi-experimental designs, time-series designs). Longitudinalresearch designs are required to explore the direction of the linkbetween housing and health, as well as to examine the temporal dimen-sions of these associations: that is, variation in housing/neighborhoodenvironment and accumulation of deprivation across the life course,susceptibility to illness during social or physiological critical periods,and latency periods for the development of illness (Bartley, Blane, andMontgomery 1997). However, few longitudinal studies have shown anassociation between housing conditions in childhood and adult health(Marsh et al. 2000).
Third, only a few empirical studies have carefully examined specificpathways between housing and health. It has been difficult to isolate agiven pathway from other possible mechanisms. For example, it may behard to separate poor housing conditions from other facets of socioeco-nomic deprivation such as poverty. Similarly, it may be difficult to dis-entangle the effect of a housing unit’s condition from locational effects,specifically neighborhood conditions. Multilevel research designs arebeing used to disentangle these effects (Acevedo-Garcia et al. 2003;Ellen et al. 2001; O’Campo 2003; Subramanian, Jones, and Duncan2003). Identifying mechanisms is especially important for tying any onespecific housing policy to health, since policy often occurs far upstreamof health problems in the causal chain of events: Specifically, Williamsand Collins (2001) point to such mediators as improved physical orsocial neighborhood environment.
Fourth, plausible biological pathways between housing and health arewell established for some exposure/outcome combinations (exposure tolead and cognitive function in children), but most research has not
Fannie Mae Foundation
54 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 55
addressed the biological links between housing and health. Biomarkers,which are objectively measured indicators of “normal biologic proc-esses, pathogenic processes, or pharmacologic responses” (De Gruttolaet al. 2001, 487), are commonly employed to gauge toxic exposure inoccupational and environmental health (lead and carbon monoxide), todocument smoking status and exposure to secondhand smoke (nicotinelevels), and to evaluate the effectiveness of pharmacologic interventions(to reduce blood pressure or to treat AIDS) (Christiani 1996; De Grut-tola et al. 2001). Yet the use of biomarkers in housing and health inter-ventions, aside from gauging toxic exposure, is incipient (Loucks et al.2002). Use of objective measures of physiologic responses to housingmay provide unbiased measures for outcomes subject to bias fromsocial desirability or recall or for outcomes that are imperceptible forself-report, such as blood pressure and immune response (Loucks et al.2002).
Housing and health disparities
Understanding the source of health disparities and addressing themalong racial/ethnic and socioeconomic lines has become an increasinglyimportant topic in public health research and practice (Geronimus2000; Williams 1997; Williams and Collins 2001; Williams and Harris-Reid 1999). Sociological research suggests that housing factors mayunderlie disparities in socioeconomic outcomes, which have been widelyrecognized as upstream determinants of health (Berkman and Kawachi2000). For example, at the household level, limited access to homeown-ership contributes to substantial differences in wealth and its intergen-erational accumulation across racial/ethnic groups. In turn, wealthdisparities are linked to educational and labor market disparities (Con-ley 1999). There is also concern that housing segregation along raciallines and the spatial concentration of poverty separate racial/ethnicgroups into vastly different neighborhood environments. In turn, thenegative effects imposed on individuals living in highly disadvantagedneighborhoods are the source of disparities in socioeconomic outcomes(Altshuler et al. 1999; Iannotta, Ross, and the National ResearchCouncil 2002). Disparities in both individual-level and neighborhood-level socioeconomic outcomes may underlie health disparities alongracial/ethnic lines (Williams 1996, 1997; Williams and Collins 2001).
Social epidemiology research is beginning to show the effect of neigh-borhood characteristics independent of individual-level socioeconomicfactors on racial/ethnic disparities in health outcomes—for example, low birth weight (Buka et al. 2003). Research has also documented a
Housing Policy Debate
Fannie Mae Foundation
56 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
positive association between housing segregation and mortality andmorbidity among blacks. Although most of these studies have somemethodological weaknesses, the evidence to date consistently suggeststhat blacks in urban areas characterized by higher levels of housing seg-regation experience higher mortality and morbidity (Acevedo-Garciaand Lochner 2003; Acevedo-Garcia et al. 2003; Williams and Collins2001). However, research on both neighborhoods and segregation inrelation to health outcomes has been atheoretical, and the identificationof causal mechanisms has only recently become an area of exploration(Acevedo-Garcia and Lochner 2003; Acevedo-Garcia et al. 2003;O’Campo 2003). As noted by O’Campo, “We still lack a clear picture ofthe intervention and policy implications of this body of work” (2003, 9).4
In this article, we focus on the evidence that housing mobility policymay serve as a tool to improve health outcomes. Our previous work hasfocused on the locational aspects of housing—segregation and neighbor-hood environment—as a social determinant of health disparities.Therefore, we are particularly interested in whether housing policyinterventions could help address health disparities. Most of the empiri-cal evidence to date addresses the physical condition of units, and hous-ing interventions and policies aimed at improving those conditions arewidely recognized as tools to protect public health (Mood 1986). How-ever, while policies that address the locational aspects of housing arejust beginning to be recognized as public health tools, in the past threedecades housing policy has been increasingly informed by concernsabout racial and income segregation. We set out to examine theresearch evidence that public policies that have influenced or tried tocorrect the spatial and social isolation of low-income and racial/ethnicminority groups have also had an impact on their health outcomes.Recent social policy experiments have begun to document how, byenhancing people’s neighborhood environment, housing mobility policymight benefit health.
Housing policy and health
Housing is an important social policy domain. It represents one of the largest monthly costs for many Americans, and equity from
4 Although public health research has recognized a possible link between segregation,disadvantaged neighborhood environments, and ill health, health research is onlybeginning to address the role of public policy in health inequalities. For example, Hartet al. (1998) showed that metropolitan areas characterized by metropolitan governancehad lower black mortality rates than areas characterized by municipal fragmentationand that housing segregation mediated the effect of metropolitan governance on blackmale mortality.

Does Housing Mobility Policy Improve Health? 57
homeownership is the most common source of household wealth (U.S.Bureau of the Census and Economics and Statistics Administration2001). The government, at all levels, intervenes in the housing marketby providing, subsidizing, or constraining the purchase, location, orrental of housing in a variety of ways, including tax policy, zoning laws,and provision of housing for low-income residents.
In this literature review, we first sought to identify those federal hous-ing policies that appear to have the greatest potential for improving thehealth of low-income individuals and, thus, for reducing health dispari-ties.5 On the basis of empirical evidence for various aspects of housingas a social determinant and for racial/ethnic and socioeconomic dispari-ties in housing outcomes, we identified three such policies: homeowner-ship promotion, enforcement of antidiscrimination laws, and housingmobility. We then focused on housing mobility, since it appeared to bethe only one that has been empirically evaluated for its effects onhealth. Additionally, this focus is warranted because such policies areembedded in rental assistance programs, which constitute the largest(in monetary terms) and the most politically viable vehicle for address-ing the needs of the U.S. low-income population facing the most severehousing problems and concentration of poverty (Sard 2000).
Homeownership policy
There are several pathways through which homeownership may helpimprove health. First, homeownership is the main source of wealth formost American households. Access to home equity provides homeown-ing households with greater financial stability and enables them tobenefit from other investment opportunities. In 2001, the median netwealth for U.S. homeowner households was about $171,800, comparedwith only about $4,810 for renter households (Joint Center for HousingStudies 2003). Potentially, promoting homeownership and thus accu-mulation of wealth could be an effective way to enhance health.6 A vastbody of social epidemiology literature suggests an inverse gradient
Housing Policy Debate
5 Our focus does not derive from an assessment that federal policy is more influentialthan state or local housing policy, but rather from an organizing principle: We decidedto start our review work by focusing first on national policy. Future reviews mayaddress state and local housing policy. However, our examination of the literature sug-gests that there may be only limited instances of state and local policies that have beenevaluated for their effect on health with the criteria we established.
6 A related (and controversial) issue is whether redistribution of wealth could helpreduce health inequalities (Deaton 2002).

between socioeconomic status (income, education, and occupation) andphysical and mental health outcomes (Barker et al. 1993; Hattersley1999; Kaplan and Salonen 1990; Lundberg 1993; Marmot et al. 1991;Power et al. 1997; Syme 1987; Syme and Berkman 1976). Althoughstudies of the association between wealth, including homeownership,and health are relatively scarce because of lack of data on accumulationof wealth, the available evidence suggests a positive associationbetween wealth and health (Deaton 2002) and between homeownershipand health (Dunn 2000; Kuh et al. 2002). Some studies found thathomeownership is associated with a lower probability of limiting long-term illness (Wadsworth, Montgomery, and Bartley 1999); others foundthat children living in houses owned by their parents experienced lowerrates of behavioral, emotional, and cognitive problems and recom-mended promoting homeownership as a strategy for reducing suchproblems (Boyle 2002; Haurin, Parcel, and Haurin 2002).
Further, although the evidence is limited, homeownership may conferpsychological benefits (Dunn and Hayes 2000; U.S. Department ofHousing and Urban Development [HUD] 1995) and may contribute tobetter neighborhood physical and social environments (HUD 1995),which in turn may have health-promoting effects. However, the burdenof a home mortgage can also detrimentally influence health. Forinstance, in a nationally representative British panel study, Nettletonand Burrows (1998) documented that when homeowners experiencedproblems paying their mortgage or fell into arrears, their subjectivewell-being declined compared with those who had no mortgage prob-lems, even after adjusting for health problems, change in health status,income, and employment since baseline. Thus, the fear of losing one’shome results in worse health despite the fact that relatively few peopleactually experience repossession (Nettleton and Burrows 1998).
Although it would be important to incorporate health impact assess-ment into policy demonstrations aimed at promoting homeownershipamong racial/ethnic minority and low-income households, to our knowl-edge no such studies exist. Also, current policy goals assume that“homeownership is not an option for everyone”—that some low-incomehouseholds may be better served by rental assistance (HUD 2002, 7).
Fair housing policy
Enforcing antidiscrimination laws is another key component of housingpolicy. Housing discrimination and antidiscrimination policy could alsopotentially affect health outcomes through at least two mechanisms.First, since discrimination limits homeownership among minorities
Fannie Mae Foundation
58 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
Does Housing Mobility Policy Improve Health? 59
(Yinger 1995), antidiscrimination policy could enhance minority home-ownership and accumulation of wealth and, as a result, minorityhealth. Further, health research suggests that institutional housing dis-crimination (Gee 2002), as well as perceptions of racism and discrimi-nation, could have detrimental effects on cardiovascular and mentalhealth, for example (Harrell, Hall, and Taliaferro 2003; Jackson et al.1996; Krieger and Sidney 1996; Williams and Neighbors 2001;Williams, Neighbors, and Jackson 2003). However, to our knowledge,housing antidiscrimination policy has not been evaluated for its effectson health.
Housing mobility policy
In the United States, rental assistance is the main form of governmenthousing assistance for low-income households (HUD 2002). Moreover,rental assistance, in the form of housing vouchers, is increasingly beingexamined as a tool for deconcentrating poverty (Sard 2000). Besidesproviding income assistance to low-income households, the Section 8program by design could help reduce the concentration of poverty as itfacilitates housing mobility. Participants are free to choose any housingthat meets program requirements and are not limited to units in subsi-dized housing projects, which are generally located in distressed areas(Sard 2000; Turner, Popkin, and Cunningham 2000). Analyses of neigh-borhood characteristics of participants in different federal housing pro-grams have found that Section 8 certificates and vouchers “reduce theprobability that families live in the most economically and socially dis-tressed areas” (Newman and Schnare 1997, 703). Only about 15 per-cent of Section 8 recipients live in neighborhoods with poverty rates inexcess of 30 percent. By contrast, about 54 percent of public housingresidents live in such neighborhoods (Newman and Schnare 1997;Turner, Popkin, and Cunningham 2000). Therefore, the Section 8 pro-gram may benefit participants both through an effect on householdincome and through an effect on neighborhood quality. Both are likelyto have a beneficial effect on health outcomes.
Housing Policy Debate
Empirical evidence on housing mobility policy and health
Literature search methods
We began by casting a wide net for studies of any housing policies thatmight have been evaluated for health,7 but at the same time, we alsoimposed rigorous selection criteria. We searched eight medical, socialscience, policy, and housing databases for articles from 1974 throughApril 2002: MEDLINE, SocioFile, PsychINFO, the Social Sciences Cita-tion Index, the HUD USER Bibliographic Database, ProQuest, Policy-File, and JSTOR (which contains 35 journals for geography, populationstudies, and sociology). We used the following keywords in our search:public policy or policy, housing, and health. We also reviewed referenceswithin relevant articles, Internet sites, and housing journals: Health &Place (1995–2002); Housing Studies (1998–2002); Housing Theory andSociety (October 1999–August 2000); Urban Studies (1995–2002);Housing Policy Debate (1993–2002); Journal of Housing Research(1993–2002); Social Science and Medicine (1995–2002); and the Prince-ton Moving to Opportunity, HUD, and Urban Institute Web sites.
To be included in our review, studies must have fulfilled the followingconditions: (1) empirically evaluated a housing policy in the UnitedStates, (2) included at least one relevant health outcome, and (3) had acomparison group.
Relevant health outcomes were included as (1) direct health outcomes(individually measured mental or physical health, including experienceof violence), (2) hazardous health behaviors (substance abuse), and (3) medical care. Although several studies included indicators thatcould be proxies for health (number of school absences, unsafe housingor neighborhood conditions), we have not included such indirectoutcomes here.
We found three main bodies of research: housing mobility policy, hous-ing policy for the homeless/mentally ill, and lead standards policy. Wechose to focus on housing mobility as a potential tool for reducinghealth disparities. We did not find any studies on the health effects ofhomeownership promotion policy and antidiscrimination policy, the two
Fannie Mae Foundation
60 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
7 Some of the earliest work on the effect of housing mobility and health focused on thesevere distress that accompanied forced relocation because of urban renewal projects.For instance, 46 percent of women relocated from Boston’s West End experienced long-term grief reactions; 57 percent of these women reported that they continued to havesymptoms of depression two years after relocation (Fried 1963).

Does Housing Mobility Policy Improve Health? 61
other areas we had identified as possible vehicles for reducing healthdisparities. We excluded housing standards on lead, because, unlikehousing mobility, they are already widely recognized as a tool forprotecting health, and housing policy for the homeless or mentally illpopulation, because this research overlooks the possibility of a morecomplex housing gradient in health (Dunn 2000).8
Housing mobility studies that met our inclusion criteria were docu-mented in an evaluation form developed at the CDC by Briss et al.(2000). Using the guidelines developed by these authors, we reviewedeach of the studies and ranked them by the strength of their studydesigns. Our evaluation was based on a number of criteria, includingstudy population and design, sampling methods, validity and reliabilityof exposure and outcome measures, data analysis, attrition, authors’interpretation of results, and presence of other major threats to validity.
Findings
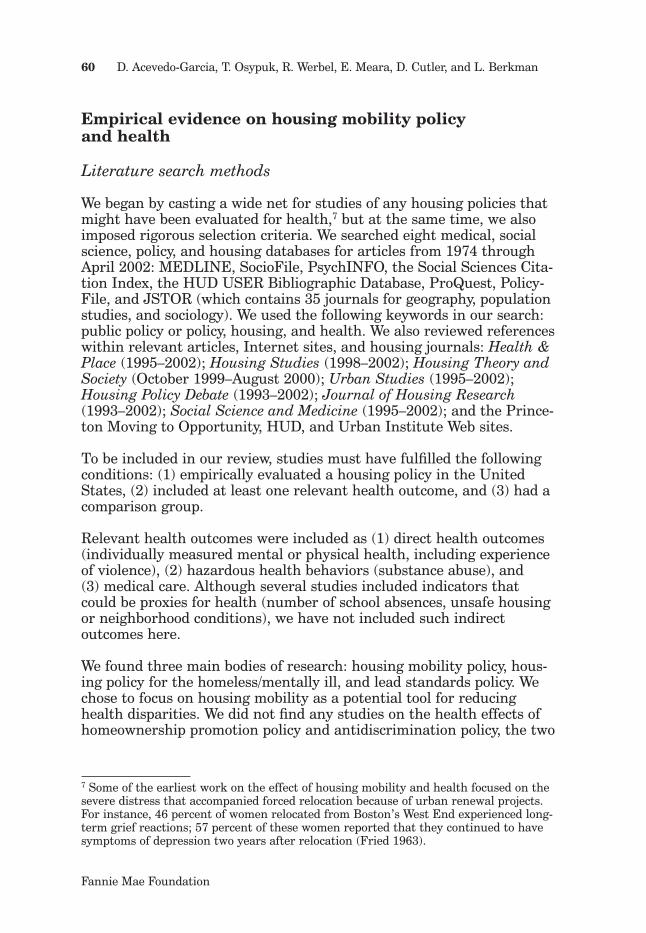
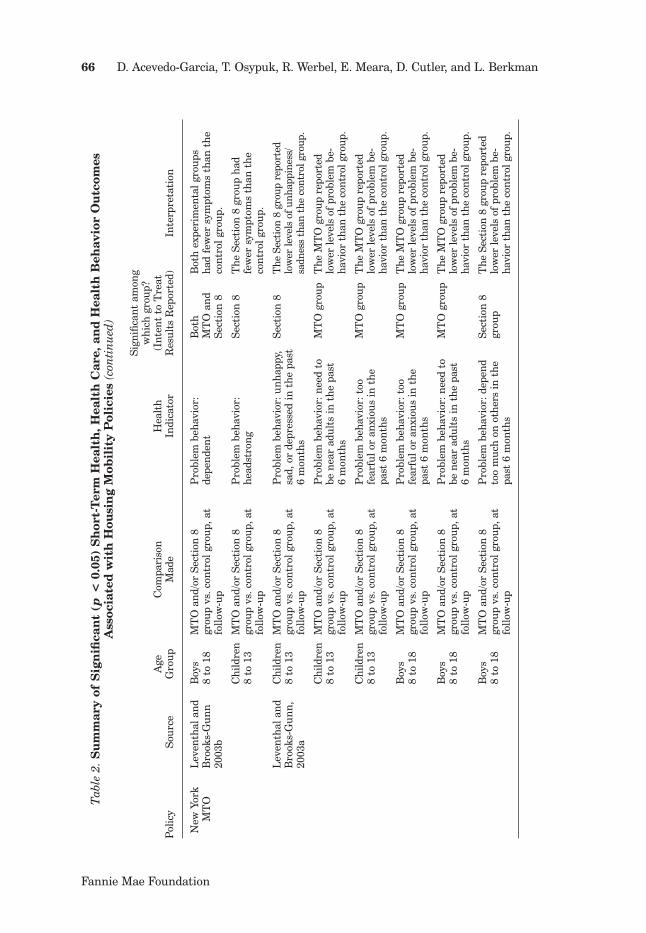
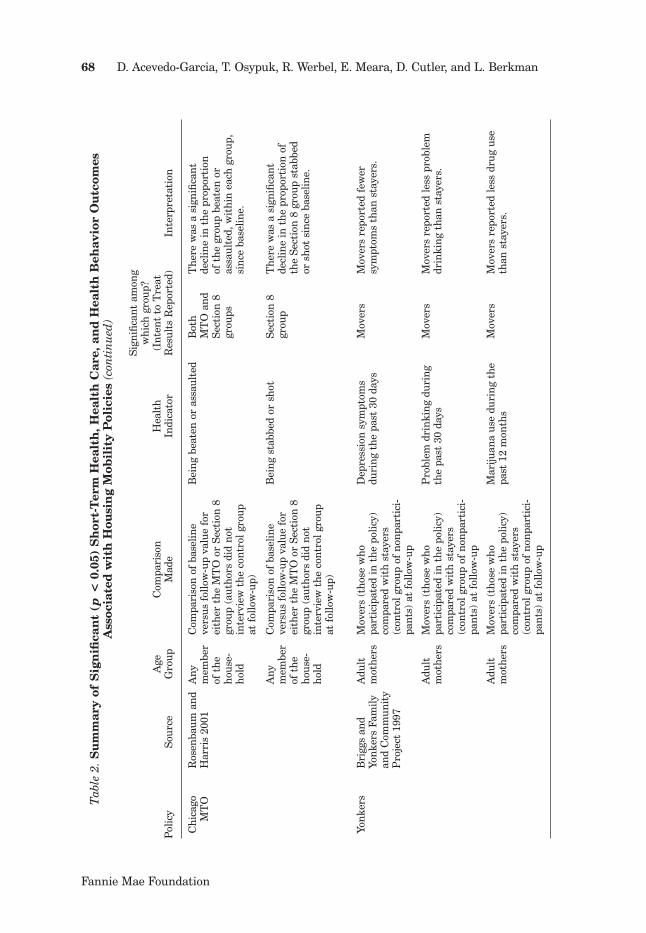
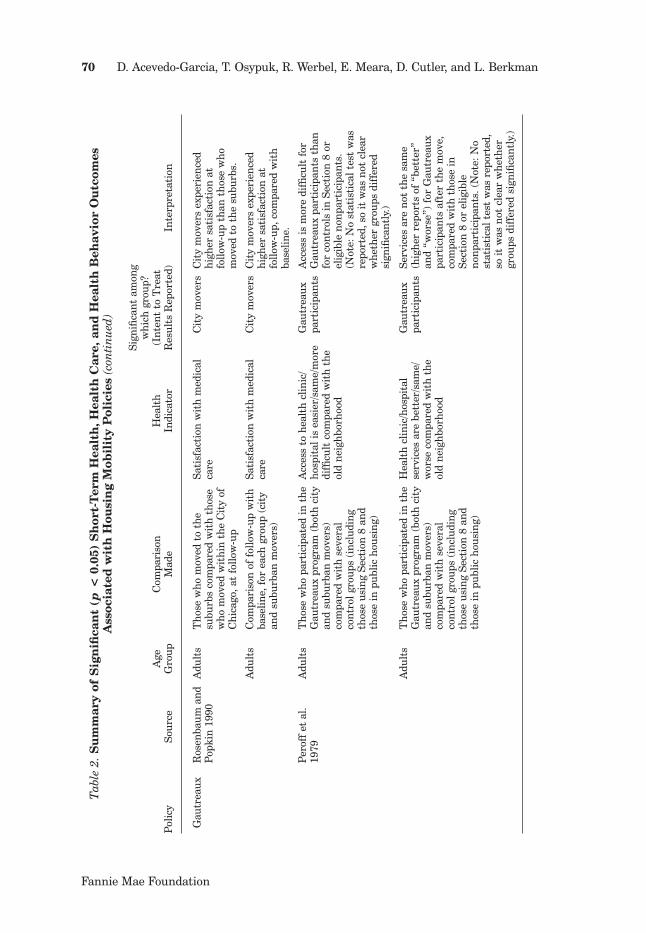
As shown in figure 1, our search yielded 479 citations, which werereviewed for relevance to our criteria. A total of 94 articles were keptfor closer inspection, and of these, 13 articles qualified for inclusion.These articles discussed five residential mobility policies: the MTOexperiment, the Gautreaux program, the Yonkers scattered-site publichousing program, the Section 8 program, and the Cincinnati SpecialMobility Program (table 1). We will first summarize the effects of eachpolicy on health (table 2) and then summarize the evidence.
Gautreaux program
The Gautreaux Assisted Housing Program, the first and best known ofthe litigation-initiated residential mobility housing programs, resultedfrom a lawsuit that was filed by Dorothy Gautreaux and other publichousing residents against HUD and alleged racial discrimination in theadministration of the Chicago public housing program. In 1976, theSupreme Court ordered the city of Chicago to racially desegregate itspublic housing and offer placements to black families in private unitslocated in other parts of the metropolitan area. Public housing resi-dents and those on the waiting list received Section 8 certificates andhousing counseling to move either within the city or to one of morethan 115 predominantly white suburbs.
Housing Policy Debate
8 Additionally, housing policy for the homeless/mentally ill population is a local policyarea, while our focus here is on federal policies.
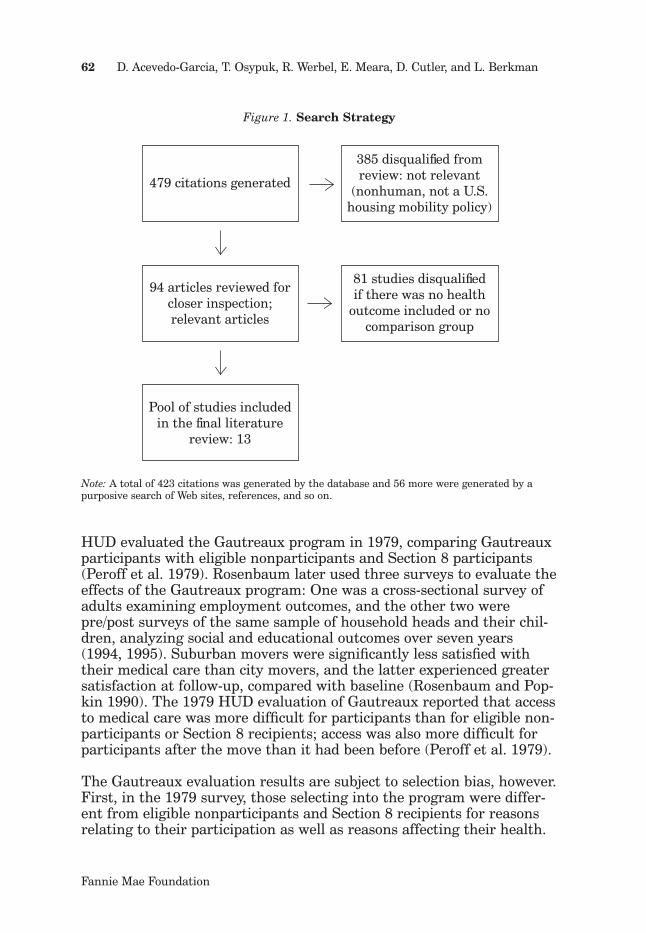
Figure 1. Search Strategy
Note: A total of 423 citations was generated by the database and 56 more were generated by apurposive search of Web sites, references, and so on.
HUD evaluated the Gautreaux program in 1979, comparing Gautreauxparticipants with eligible nonparticipants and Section 8 participants(Peroff et al. 1979). Rosenbaum later used three surveys to evaluate theeffects of the Gautreaux program: One was a cross-sectional survey ofadults examining employment outcomes, and the other two werepre/post surveys of the same sample of household heads and their chil-dren, analyzing social and educational outcomes over seven years(1994, 1995). Suburban movers were significantly less satisfied withtheir medical care than city movers, and the latter experienced greatersatisfaction at follow-up, compared with baseline (Rosenbaum and Pop-kin 1990). The 1979 HUD evaluation of Gautreaux reported that accessto medical care was more difficult for participants than for eligible non-participants or Section 8 recipients; access was also more difficult forparticipants after the move than it had been before (Peroff et al. 1979).
The Gautreaux evaluation results are subject to selection bias, however.First, in the 1979 survey, those selecting into the program were differ-ent from eligible nonparticipants and Section 8 recipients for reasonsrelating to their participation as well as reasons affecting their health.
479 citations generated
385 disqualified from review: not relevant
(nonhuman, not a U.S. housing mobility policy)
94 articles reviewed for closer inspection; relevant articles
Pool of studies included in the final literature
review: 13
81 studies disqualifiedif there was no health
outcome included or no comparison group
Fannie Mae Foundation
62 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 63
Tab
le 1
.Su
mm
ary
of H
ousi
ng
Mob
ilit
y S
tud
ies
wit
h H
ealt
h-R
elat
ed O
utc
omes
, Cla
ssifi
ed b
y M
eth
odol
ogic
al
Str
engt
h a
nd
Su
itab
ilit
y of
Stu
dy
Des
ign
Hea
lth-
Rel
ated
Out
com
es
Cla
ssifi
cati
on o
fM
etho
dolo
gica
lSu
itab
ility
of
Sour
ceP
olic
yIn
clud
ed in
the
Rev
iew
Out
com
e T
ype
Stre
ngt
h*St
udy
Des
ign
*
Kat
z, K
ling,
an
dL
iebm
an 2
001
MT
O B
osto
nC
rim
e vi
ctim
izat
ion
; in
juri
es, a
ccid
ents
, or
pois
onin
gs;
asth
ma
atta
ck r
equi
rin
g m
edic
al a
tten
tion
; 7-i
tem
par
ent
repo
rt o
f ch
ild b
ehav
ior
prob
lem
s; a
dult
sel
f-re
port
edhe
alth
; men
tal h
ealt
h (r
epor
ted
maj
or d
epre
ssiv
esy
mpt
om);
cal
m/p
eace
ful;
been
to
med
ical
car
e fo
r re
gula
rch
ecku
p or
imm
uniz
atio
n
Hea
lth,
men
tal
heal
th, c
rim
evi
ctim
izat
ion
,he
alth
car
eut
iliza
tion
1 (g
ood)
Gre
ates
t
Lev
enth
al a
nd
Bro
oks-
Gun
n20
03b
MT
O N
ew Y
ork
Men
tal h
ealt
h fo
r ch
ildre
n (
prob
lem
beh
avio
ral o
utco
mes
)an
d m
othe
rs
Men
tal h
ealt
h2
(fai
r)G
reat
est
Faut
h, L
even
thal
, an
d B
rook
s-G
unn
200
2
Yon
kers
A
dole
scen
t ex
posu
re t
o vi
olen
ce a
nd
acce
ss t
o ci
gare
ttes
and/
or a
lcoh
olC
rim
evi
ctim
izat
ion
and
acce
ss t
oill
egal
hea
lth-
harm
ing
subs
tan
ces
3 (f
air)
Gre
ates
t
Ros
enba
um a
nd
Pop
kin
199
0G
autr
eaux
Sati
sfac
tion
wit
h m
edic
al c
are
Hea
lth
care
3
(fai
r)G
reat
est
Lev
enth
al a
nd
Bro
oks-
Gun
n20
03a
MT
O N
ew Y
ork
Ado
lesc
ent
use
of c
igar
ette
s an
d al
coho
l; ch
ild m
enta
lhe
alth
; chi
ld h
ealt
h; e
xpos
ure
to v
iole
nce
Hea
lth,
hea
lth
beha
vior
/su
bsta
nce
abus
e, m
enta
lhe
alth
, cri
me
vict
imiz
atio
n
3 (f
air)
Gre
ates
t
Housing Policy Debate

Tab
le 1
.Su
mm
ary
of H
ousi
ng
Mob
ilit
y S
tud
ies
wit
h H
ealt
h-R
elat
ed O
utc
omes
, Cla
ssifi
ed b
y M
eth
odol
ogic
al
Str
engt
h a
nd
Su
itab
ilit
y of
Stu
dy
Des
ign
(co
nti
nu
ed)
Hea
lth-
Rel
ated
Out
com
es
Cla
ssifi
cati
on o
fM
etho
dolo
gica
lSu
itab
ility
of
Sour
ceP
olic
yIn
clud
ed in
the
Rev
iew
Out
com
e T
ype
Stre
ngt
h*St
udy
Des
ign
*
*So
urce
for
rat
ing
syst
em: B
riss
et
al. 2
000
Bri
ggs
1997
an
dth
e Yo
nke
rsFa
mily
an
dC
omm
unit
yP
roje
ct
Yon
kers
Scat
tere
d-Si
teP
ublic
Hou
sin
g
Mot
her’
s re
port
ed m
enta
l hea
lth
sym
ptom
s (d
epre
ssio
n,
anxi
ety)
, sub
stan
ce a
buse
(al
coho
l, dr
ugs)
, exp
erie
nce
of
viol
ence
dur
ing
the
past
12
mon
ths
Men
tal h
ealt
h,he
alth
beh
avio
r/su
bsta
nce
ab
use,
cri
me
vict
imiz
atio
n
4 (f
air)
Gre
ates
t
Mey
ers
et a
l. 19
95Se
ctio
n 8
Gro
wth
of
child
(he
ight
an
d w
eigh
t fo
r ag
e), a
s a
prox
yfo
r n
utri
tion
Hea
lth/
child
deve
lopm
ent
5 (l
imit
ed)
Lea
st
Ros
enba
um a
nd
Har
ris
2001
MT
O C
hica
goE
xper
ien
ce o
f vi
olen
ce o
r cr
ime
Cri
me
vict
imiz
atio
n5
(lim
ited
)G
reat
est
Per
off
et a
l. 19
79G
autr
eaux
Hea
lth
care
acc
ess
easy
or
diffi
cult
Hea
lth
care
5 (l
imit
ed)
Gre
ates
t
Han
ratt
y,M
cLan
ahan
,an
d P
etti
t 20
03
MT
OL
os A
nge
les
Med
ical
car
e ac
cess
, reg
ular
pla
ce f
or c
are
Hea
lth
care
5 (l
imit
ed)
Gre
ates
t
Ros
enba
um 1
994
Gau
trea
uxV
icti
miz
atio
n: W
heth
er y
outh
wer
e hu
rt b
y ot
her
stud
ents
in s
choo
lC
rim
evi
ctim
izat
ion
6 (l
imit
ed)
Gre
ates
t
Ros
enba
um 1
995
Gau
trea
uxV
icti
miz
atio
n: W
heth
er y
outh
wer
e hu
rt b
y ot
her
stud
ents
in s
choo
lC
rim
evi
ctim
izat
ion
6 (l
imit
ed)
Gre
ates
t
Fis
cher
199
1C
inci
nn
ati
Spec
ial M
obili
tyP
rogr
am
Bei
ng
atta
cked
/per
son
al e
xper
ien
ce o
f vi
olen
ce o
r ro
bber
yfo
r se
lf, c
hild
, or
nei
ghbo
r; r
ecei
pt o
f he
alth
car
e be
nefi
ts;
sati
sfac
tion
wit
h he
alth
car
e
Cri
me
vict
imiz
atio
n,
heal
th c
are
8 (l
imit
ed)
Lea
st
Fannie Mae Foundation
64 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 65
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
Bos
ton
M
TO
Kat
z, K
ling,
and
Lie
bman
2001
Chi
ldre
n6
to 1
5M
TO
gro
up (
also
kn
own
as
the
expe
rim
enta
l gro
up)
and/
or S
ecti
on 8
gro
up v
s.co
ntr
ol g
roup
, at
follo
w-u
p
An
y in
juri
es, a
ccid
ents
, or
pois
onin
gs o
ver
the
past
6
mon
ths
requ
irin
g m
edic
alat
ten
tion
MT
OT
he M
TO
gro
up h
ad f
ewer
inci
den
ts t
han
the
con
trol
grou
p.
Chi
ldre
n6
to 1
5M
TO
gro
up (
also
kn
own
as
the
expe
rim
enta
l gro
up)
and/
or S
ecti
on 8
gro
up v
s.co
ntr
ol g
roup
, at
follo
w-u
p
Fra
ctio
n o
f 7
beha
vior
pro
b-le
ms
amon
g bo
ysB
oth
MT
O a
nd
Sect
ion
8
Bot
h ex
peri
men
tal g
roup
sha
d fe
wer
beh
avio
r pr
oble
ms
than
the
con
trol
gro
up.
Adu
lts
MT
O g
roup
(al
so k
now
n a
sth
e ex
peri
men
tal g
roup
)an
d/or
Sec
tion
8 g
roup
vs.
con
trol
gro
up, a
t fo
llow
-up
Ove
rall
heal
th g
ood
or b
ette
rB
oth
MT
O a
nd
Sect
ion
8
Bot
h ex
peri
men
tal g
roup
sw
ere
heal
thie
r th
an t
heco
ntr
ol g
roup
.
Adu
lts
MT
O g
roup
(al
so k
now
n a
sth
e ex
peri
men
tal g
roup
)an
d/or
Sec
tion
8 g
roup
vs.
con
trol
gro
up, a
t fo
llow
-up
Cal
m a
nd
peac
eful
“a
good
bit
of t
he t
ime”
or
mor
eof
ten
in t
he p
ast
4 w
eeks
Bot
h M
TO
an
dSe
ctio
n 8
Bot
h ex
peri
men
tal g
roup
sw
ere
calm
er t
han
the
con
trol
grou
p.
New
Yor
k M
TO
Lev
enth
al a
nd
Bro
oks-
Gun
n20
03b
Adu
lts
MT
O a
nd/
or S
ecti
on 8
gr
oup
vs. c
ontr
ol g
roup
, at
follo
w-u
p
Dis
tres
s/an
xiet
y sy
mpt
oms
in t
he p
ast
mon
thM
TO
T
he M
TO
gro
up h
ad f
ewer
sym
ptom
s th
an t
he c
ontr
olgr
oup.
Chi
ldre
n8
to 1
8 M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r:
anxi
ous/
depr
esse
dM
TO
The
MT
O g
roup
had
few
ersy
mpt
oms
than
the
con
trol
grou
p.B
oys
8 to
18
MT
O a
nd/
or S
ecti
on 8
gr
oup
vs. c
ontr
ol g
roup
, at
follo
w-u
p
Pro
blem
beh
avio
r:
anxi
ous/
depr
esse
d M
TO
The
MT
O g
roup
had
few
ersy
mpt
oms
than
the
con
trol
grou
p.
Housing Policy Debate
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
New
Yor
k M
TO
Lev
enth
al a
nd
Bro
oks-
Gun
n20
03b
Boy
s 8
to 1
8M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r:
depe
nde
nt
Bot
h M
TO
an
dSe
ctio
n 8
Bot
h ex
peri
men
tal g
roup
sha
d fe
wer
sym
ptom
s th
an t
heco
ntr
ol g
roup
.
Chi
ldre
n8
to 1
3M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r:
head
stro
ng
Sect
ion
8T
he S
ecti
on 8
gro
up h
adfe
wer
sym
ptom
s th
an t
heco
ntr
ol g
roup
.
Lev
enth
al a
nd
Bro
oks-
Gun
n,
2003
a
Chi
ldre
n8
to 1
3M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r: u
nha
ppy,
sad,
or
depr
esse
d in
the
pas
t6
mon
ths
Sect
ion
8T
he S
ecti
on 8
gro
up r
epor
ted
low
er le
vels
of u
nhap
pine
ss/
sadn
ess
than
the
con
trol
gro
up.
Chi
ldre
n8
to 1
3M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r: n
eed
tobe
nea
r ad
ults
in t
he p
ast
6 m
onth
s
MT
O g
roup
The
MT
O g
roup
rep
orte
dlo
wer
leve
ls o
f pr
oble
m b
e-ha
vior
tha
n th
e co
ntro
l gro
up.
Chi
ldre
n8
to 1
3M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r: t
oo
fear
ful o
r an
xiou
s in
the
pa
st 6
mon
ths
MT
O g
roup
The
MT
O g
roup
rep
orte
dlo
wer
leve
ls o
f pr
oble
m b
e-ha
vior
tha
n th
e co
ntro
l gro
up.
Boy
s 8
to 1
8M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r: t
oo
fear
ful o
r an
xiou
s in
the
pa
st 6
mon
ths
MT
O g
roup
The
MT
O g
roup
rep
orte
dlo
wer
leve
ls o
f pr
oble
m b
e-ha
vior
tha
n th
e co
ntro
l gro
up.
Boy
s 8
to 1
8M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r: n
eed
tobe
nea
r ad
ults
in t
he p
ast
6 m
onth
s
MT
O g
roup
The
MT
O g
roup
rep
orte
dlo
wer
leve
ls o
f pr
oble
m b
e-ha
vior
tha
n th
e co
ntro
l gro
up.
Boy
s 8
to 1
8M
TO
an
d/or
Sec
tion
8
grou
p vs
. con
trol
gro
up, a
tfo
llow
-up
Pro
blem
beh
avio
r: d
epen
dto
o m
uch
on o
ther
s in
the
past
6 m
onth
s
Sect
ion
8gr
oup
The
Sec
tion
8 g
roup
rep
orte
dlo
wer
leve
ls o
f pr
oble
m b
e-ha
vior
tha
n th
e co
ntro
l gro
up.
Fannie Mae Foundation
66 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 67
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
New
Yor
k M
TO
Lev
enth
al a
nd
Bro
oks-
Gun
n,
2003
a
Gir
ls
11 t
o 18
M
TO
an
d/or
Sec
tion
8 g
roup
vs. c
ontr
ol g
roup
, at
follo
w-u
pT
een
gir
l her
self
use
d al
coho
l in
the
pas
t ye
ar
MT
O g
roup
T
he M
TO
gro
up r
epor
ted
high
er u
se o
f al
coho
l tha
n t
heco
ntr
ol g
roup
.
Boy
s 11
to
18M
TO
an
d/or
Sec
tion
8 g
roup
vs. c
ontr
ol g
roup
, at
follo
w-u
pT
een
rep
ort
that
pee
rs u
sed
ciga
rett
es in
the
pas
t ye
arM
TO
gro
up
The
MT
O g
roup
rep
orte
dpe
ers
used
cig
aret
tes
less
than
the
con
trol
gro
up.
Adu
lts
MT
O, S
ecti
on 8
, or
con
trol
grou
p, c
ompa
rin
g ba
selin
ew
ith
the
follo
w-u
p va
lue
Exp
osur
e to
vio
len
ce(m
ugge
d, t
hrea
ten
ed, b
eate
n,
or s
tabb
ed/s
hot)
All
thre
egr
oups
(MT
O,
Sect
ion
8,
and
con
trol
s)
Eac
h gr
oup
expe
rien
ced
ade
clin
e in
exp
osur
e to
vi
olen
ce f
rom
bas
elin
e to
fo
llow
-up.
Los
An
gele
s M
TO
H
anra
tty,
McL
anah
an,
and
Pet
tit
2003
Adu
lts
MT
O, S
ecti
on 8
, or
con
trol
grou
p, c
ompa
rin
g ba
selin
ew
ith
the
follo
w-u
p va
lue
No
sign
ifica
nt
resu
lts
repo
rted
——
Chi
cago
M
TO
R
osen
baum
an
dH
arri
s 20
01A
ny
mem
ber
of t
heho
use-
hold
Com
pari
son
of
base
line
vers
us f
ollo
w-u
p va
lue
for
eith
er t
he M
TO
or
Sect
ion
8gr
oup
(aut
hors
did
not
in
terv
iew
the
con
trol
gro
up
at f
ollo
w-u
p)
Bei
ng
thre
aten
ed w
ith
akn
ife
or g
un
Bot
h M
TO
an
dSe
ctio
n 8
grou
ps
The
re w
as a
sig
nifi
can
tde
clin
e in
the
pro
port
ion
of
the
grou
p th
reat
ened
wit
h a
knif
e or
gun
, wit
hin
eac
hgr
oup,
sin
ce b
asel
ine.
Housing Policy Debate
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
Chi
cago
M
TO
R
osen
baum
an
dH
arri
s 20
01
An
ym
embe
rof
the
hous
e-ho
ld
Com
pari
son
of
base
line
vers
us f
ollo
w-u
p va
lue
for
eith
er t
he M
TO
or
Sect
ion
8gr
oup
(aut
hors
did
not
in
terv
iew
the
con
trol
gro
up
at f
ollo
w-u
p)
Bei
ng
beat
en o
r as
saul
ted
Bot
h M
TO
an
dSe
ctio
n 8
grou
ps
The
re w
as a
sig
nifi
can
tde
clin
e in
the
pro
port
ion
of
the
gro
up b
eate
n o
ras
saul
ted,
wit
hin
eac
h gr
oup,
sin
ce b
asel
ine.
An
ym
embe
rof
the
hous
e-ho
ld
Com
pari
son
of
base
line
vers
us f
ollo
w-u
p va
lue
for
eith
er t
he M
TO
or
Sect
ion
8gr
oup
(aut
hors
did
not
in
terv
iew
the
con
trol
gro
up
at f
ollo
w-u
p)
Bei
ng
stab
bed
or s
hot
Sect
ion
8gr
oup
The
re w
as a
sig
nifi
can
tde
clin
e in
the
pro
port
ion
of
the
Sect
ion
8 g
roup
sta
bbed
or
sho
t si
nce
bas
elin
e.
Yon
kers
B
rigg
s an
dYo
nke
rs F
amily
and
Com
mun
ity
Pro
ject
199
7
Adu
ltm
othe
rsM
over
s (t
hose
who
pa
rtic
ipat
ed in
the
pol
icy)
com
pare
d w
ith
stay
ers
(con
trol
gro
up o
f n
onpa
rtic
i-pa
nts
) at
fol
low
-up
Dep
ress
ion
sym
ptom
s du
rin
g th
e pa
st 3
0 da
ysM
over
s M
over
s re
port
ed f
ewer
sy
mpt
oms
than
sta
yers
.
Adu
ltm
othe
rsM
over
s (t
hose
who
pa
rtic
ipat
ed in
the
pol
icy)
com
pare
d w
ith
stay
ers
(con
trol
gro
up o
f n
onpa
rtic
i-pa
nts
) at
fol
low
-up
Pro
blem
dri
nki
ng
duri
ng
the
past
30
days
Mov
ers
Mov
ers
repo
rted
less
pro
blem
drin
kin
g th
an s
taye
rs.
Adu
ltm
othe
rsM
over
s (t
hose
who
pa
rtic
ipat
ed in
the
pol
icy)
com
pare
d w
ith
stay
ers
(con
trol
gro
up o
f n
onpa
rtic
i-pa
nts
) at
fol
low
-up
Mar
ijuan
a us
e du
rin
g th
epa
st 1
2 m
onth
sM
over
sM
over
s re
port
ed le
ss d
rug
use
than
sta
yers
.
Fannie Mae Foundation
68 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 69
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
Yon
kers
B
rigg
s an
dYo
nke
rs F
amily
and
Com
mun
ity
Pro
ject
199
7
Adu
ltm
othe
rsM
over
s (t
hose
who
pa
rtic
ipat
ed in
the
pol
icy)
com
pare
d w
ith
stay
ers
(con
trol
gro
up o
f n
onpa
rtic
i-pa
nts
) at
fol
low
-up
Exp
erie
nce
of
a vi
olen
t or
trau
mat
ic e
ven
t du
rin
g th
epa
st 1
2 m
onth
s (v
icti
m o
fph
ysic
al a
ssau
lt/a
buse
, of
sexu
al a
ssau
lt/r
ape,
of
life-
thre
aten
ing
mug
gin
g, o
fla
rge
fire
or s
erio
us a
ccid
ent;
wit
nes
s to
ser
ious
ass
ault
or
viol
ent
deat
h; c
hild
or
spou
sedi
ed)
Mov
ers
Mov
ers
repo
rted
low
er le
vels
of v
iole
nt
or t
raum
atic
eve
nts
than
sta
yers
.
Yon
kers
Faut
h,
Lev
enth
al, a
nd
Bro
oks-
Gun
n20
02
Yout
h8
to 1
8M
over
s (t
hose
who
pa
rtic
ipat
ed in
the
pol
icy)
com
pare
d w
ith
stay
ers
(con
trol
gro
up o
f n
onpa
rtic
i-pa
nts
) at
fol
low
-up
Acc
ess
to c
igar
ette
s an
d al
coho
lM
over
sM
over
s ha
ve le
ss a
cces
s to
ciga
rett
es a
nd
alco
hol t
han
stay
ers
do.
Gau
trea
uxR
osen
baum
1994
Yout
hT
hose
who
mov
ed t
o th
e su
burb
s co
mpa
red
wit
h th
ose
who
mov
ed w
ithi
n t
he C
ity
ofC
hica
go, a
t fo
llow
-up
No
sign
ifica
nt
indi
cato
rsre
port
ed—
—
Ros
enba
um19
95Yo
uth
Tho
se w
ho m
oved
to
the
subu
rbs
com
pare
d w
ith
thos
ew
ho m
oved
wit
hin
the
Cit
y of
Chi
cago
, at
follo
w-u
p
No
sign
ifica
nt
indi
cato
rsre
port
ed—
—
Housing Policy Debate
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
Gau
trea
uxR
osen
baum
an
dP
opki
n 1
990
Adu
lts
Tho
se w
ho m
oved
to
the
subu
rbs
com
pare
d w
ith
thos
ew
ho m
oved
wit
hin
the
Cit
y of
Chi
cago
, at
follo
w-u
p
Sati
sfac
tion
wit
h m
edic
alca
reC
ity
mov
ers
Cit
y m
over
s ex
peri
ence
dhi
gher
sat
isfa
ctio
n a
t fo
llow
-up
than
tho
se w
hom
oved
to
the
subu
rbs.
Adu
lts
Com
pari
son
of
follo
w-u
p w
ith
base
line,
for
eac
h gr
oup
(cit
yan
d su
burb
an m
over
s)
Sati
sfac
tion
wit
h m
edic
alca
reC
ity
mov
ers
Cit
y m
over
s ex
peri
ence
dhi
gher
sat
isfa
ctio
n a
t fo
llow
-up,
com
pare
d w
ith
base
line.
Per
off
et a
l.19
79A
dult
sT
hose
who
par
tici
pate
d in
the
Gau
trea
ux p
rogr
am (
both
cit
yan
d su
burb
an m
over
s)
com
pare
d w
ith
seve
ral
con
trol
gro
ups
(in
clud
ing
thos
e us
ing
Sect
ion
8 a
nd
thos
e in
pub
lic h
ousi
ng)
Acc
ess
to h
ealt
h cl
inic
/ho
spit
al is
eas
ier/
sam
e/m
ore
diffi
cult
com
pare
d w
ith
the
old
nei
ghbo
rhoo
d
Gau
trea
uxpa
rtic
ipan
tsA
cces
s is
mor
e di
fficu
lt f
orG
autr
eaux
par
tici
pan
ts t
han
for
con
trol
s in
Sec
tion
8 o
rel
igib
le n
onpa
rtic
ipan
ts.
(Not
e: N
o st
atis
tica
l tes
t w
asre
port
ed, s
o it
was
not
cle
arw
heth
er g
roup
s di
ffer
ed
sign
ifica
ntl
y.)
Adu
lts
Tho
se w
ho p
arti
cipa
ted
in t
heG
autr
eaux
pro
gram
(bo
th c
ity
and
subu
rban
mov
ers)
co
mpa
red
wit
h se
vera
l co
ntr
ol g
roup
s (i
ncl
udin
gth
ose
usin
g Se
ctio
n 8
an
dth
ose
in p
ublic
hou
sin
g)
Hea
lth
clin
ic/h
ospi
tal
serv
ices
are
bet
ter/
sam
e/w
orse
com
pare
d w
ith
the
old
nei
ghbo
rhoo
d
Gau
trea
uxpa
rtic
ipan
tsSe
rvic
es a
re n
ot t
he s
ame
(hig
her
repo
rts
of “
bett
er”
and
“wor
se”)
for
Gau
trea
uxpa
rtic
ipan
ts a
fter
the
mov
e,co
mpa
red
wit
h th
ose
in
Sect
ion
8 o
r el
igib
le
non
part
icip
ants
. (N
ote:
No
stat
isti
cal t
est
was
rep
orte
d,so
it w
as n
ot c
lear
whe
ther
grou
ps d
iffe
red
sign
ifica
ntl
y.)
Fannie Mae Foundation
70 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 71
Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
Gau
trea
uxP
erof
f et
al.
1979
Adu
lts
Tho
se w
ho p
arti
cipa
ted
in t
heG
autr
eaux
pro
gram
(bo
th c
ity
and
subu
rban
mov
ers)
co
mpa
red
wit
h se
vera
l co
ntr
ol g
roup
s (i
ncl
udin
gth
ose
usin
g Se
ctio
n 8
an
dth
ose
in p
ublic
hou
sin
g)
Get
tin
g to
hea
lth
clin
ic/
hosp
ital
is e
asy/
fair
lyea
sy/d
iffic
ult
Gau
trea
uxpa
rtic
ipan
tsA
cces
s is
mor
e di
fficu
lt f
orG
autr
eaux
par
tici
pan
ts t
han
for
thos
e in
Sec
tion
8 o
r el
igib
le n
onpa
rtic
ipan
ts.
(Not
e: N
o st
atis
tica
l tes
t w
asre
port
ed, s
o it
was
not
cle
arw
heth
er g
roup
s di
ffer
ed
sign
ifica
ntl
y.)
Sect
ion
8M
eyer
s et
al.
1995
Chi
ldre
nle
ss t
han
3 ye
ars
old
Tho
se r
ecei
vin
g Se
ctio
n 8
vouc
hers
com
pare
d w
ith
thos
e w
ho w
ere
on t
he
Sect
ion
8 w
aiti
ng
list,
at
one
poin
t in
tim
e (c
ross
-sec
tion
al)
Low
chi
ld g
row
th (
mea
n
z-sc
ore
of w
eigh
t/ag
e ba
sed
on N
atio
nal
Cen
ter
for
Hea
lth
Stat
isti
cs g
row
th
refe
ren
ce n
orm
s)
Sect
ion
8
part
icip
ants
Chi
ldre
n o
f ad
ults
rec
eivi
ng
the
Sect
ion
8 s
ubsi
dyre
port
ed t
o ha
ve h
ighe
r m
ean
wei
ght/
age
grow
th r
atio
s (b
ette
r gr
owth
) th
an c
hild
ren
of a
dult
s on
the
wai
tin
g lis
tfo
r th
e su
bsid
y.
Cin
cin
nat
i Sp
ecia
l M
obili
ty
Pro
gram
(S
MP
)
Fis
cher
199
1A
dult
sB
efor
e ve
rsus
aft
er t
he m
ove,
amon
g th
ose
in t
he S
MP
pr
ogra
m
Bei
ng
atta
cked
/per
son
alex
peri
ence
of
viol
ence
or
robb
ery
for
self,
chi
ld, o
rn
eigh
bor
SMP
pa
rtic
ipan
tsM
over
s re
port
a r
educ
tion
invi
olen
ce s
ince
the
mov
e.
Housing Policy Debate

Tab
le 2
.Su
mm
ary
of S
ign
ifica
nt
(p<
0.0
5) S
hor
t-T
erm
Hea
lth
, Hea
lth
Car
e, a
nd
Hea
lth
Beh
avio
r O
utc
omes
A
ssoc
iate
d w
ith
Hou
sin
g M
obil
ity
Pol
icie
s (c
onti
nued
)
Sign
ifica
nt
amon
gw
hich
gro
up?
Age
Com
pari
son
Hea
lth
(In
ten
t to
Tre
atP
olic
ySo
urce
Gro
upM
ade
Indi
cato
rR
esul
ts R
epor
ted)
Inte
rpre
tati
on
Not
es:I
n t
his
tabl
e, w
e ap
plie
d th
e co
nve
nti
onal
sig
nifi
can
ce v
alue
p<
0.0
5 fo
r in
clus
ion
of
heal
th-r
elat
ed o
utco
mes
ass
ocia
ted
wit
h ho
usin
g m
obili
typo
licy,
so
that
we
coul
d be
con
sist
ent
acro
ss s
tudi
es b
y ap
plyi
ng
the
sam
e cu
toff
val
ue. M
any
stud
ies
repo
rted
sev
eral
val
ues
mor
e st
rin
gen
t th
an 0
.05,
alth
ough
on
ly a
few
rep
orte
d si
gnifi
can
ce v
alue
s at
p <
0.1
0. H
ousi
ng
mob
ility
was
ass
ocia
ted
wit
h se
vera
l hea
lth-
rela
ted
outc
omes
at
a p
valu
ebe
twee
n 0
.05
and
0.10
“m
argi
nal
ly s
ign
ifica
nt,
” fo
r al
l the
out
com
es t
hat
follo
w. I
n B
osto
n, M
TO
tre
atm
ent
child
ren
(ag
e 6
to 1
5) e
xhib
ited
mar
gin
ally
few
er a
sthm
a at
tack
s re
quir
ing
med
ical
att
enti
on in
the
pas
t 6
mon
ths
and
mar
gin
ally
few
er p
erso
nal
cri
mes
(pe
rson
al t
hrea
ts, r
obbe
ries
, or
atta
cks)
(Kat
z, K
ling,
an
d L
iebm
an 2
001)
. Res
pon
den
ts in
the
Chi
cago
MT
O t
reat
men
t gr
oup
expe
rien
ced
a re
duct
ion
in b
ein
g st
abbe
d or
sho
t in
the
ir n
eigh
-bo
rhoo
d fr
om b
asel
ine
to f
ollo
w-u
p (R
osen
baum
an
d H
arri
s 20
01).
You
th m
over
s in
the
Yon
kers
pro
gram
exp
erie
nce
d lo
wer
odd
s of
bei
ng
assa
ulte
d(F
auth
, Lev
enth
al, a
nd
Bro
oks-
Gun
n 2
002)
. You
ng
child
ren
who
se f
amily
rec
eive
d th
e Se
ctio
n 8
vou
cher
had
hig
her
stan
dard
ized
wei
ght/
heig
htgr
owth
rat
ios
than
chi
ldre
n w
hose
fam
ilies
wer
e on
the
Sec
tion
8 w
aiti
ng
list
(Mey
ers
et a
l. 19
95).
Par
ents
in t
he N
ew Y
ork
MT
O t
reat
men
t gr
oup
expe
rien
ced
low
er le
vels
of
depr
essi
ve s
ympt
oms
than
con
trol
s; M
TO
tre
atm
ent
child
ren
age
d 8
to 1
3 ex
peri
ence
d lo
wer
leve
ls o
f an
xiou
s/de
pres
sed
sym
ptom
s, a
nd
both
tre
atm
ent
grou
ps a
ged
8 to
13
disp
laye
d lo
wer
leve
ls o
f de
pen
den
t pr
oble
ms
than
con
trol
s; S
ecti
on 8
you
th a
ged
8 to
18
repo
rted
low
er le
vels
of
depe
nde
ncy
an
d he
adst
ron
g pr
oble
ms
than
con
trol
s (L
even
thal
an
d B
rook
s-G
unn
200
3b).
The
re w
ere
mar
gin
ally
sig
nifi
can
t lo
wer
lev-
els
of p
robl
em b
ehav
iors
/men
tal h
ealt
h fo
r th
ese
New
Yor
k gr
oups
: MT
O t
reat
men
t bo
ys 8
to
18 “
unha
ppy,
sad
, or
depr
esse
d”; M
TO
tre
atm
ent
boys
“dep
end
too
muc
h on
oth
ers”
; Sec
tion
8 b
oys
“nee
d to
be
nea
r ad
ults
”; S
ecti
on 8
you
nge
r ch
ildre
n (
8 to
13)
“n
eed
to b
e n
ear
adul
ts”;
Sec
tion
8 c
hil-
dren
(8
to 1
8) “
depe
nd
too
muc
h on
oth
ers”
(L
even
thal
an
d B
rook
s-G
unn
200
3a).
Cin
cin
nat
i Sp
ecia
l M
obili
ty
Pro
gram
(S
MP
)
Fis
cher
199
1A
dult
sB
efor
e ve
rsus
aft
er t
he m
ove,
amon
g th
ose
in t
he S
MP
pr
ogra
m
Job
prov
ides
med
ical
car
ebe
nefi
ts (
amon
g th
ose
empl
oyed
)
SMP
pa
rtic
ipan
tsM
over
s re
port
tha
t th
ey a
rem
ore
likel
y to
hav
e be
nefi
tsaf
ter
they
mov
ed (
com
pare
dw
ith
befo
re).
(N
ote:
No
stat
isti
cal t
est
was
rep
orte
d,so
it w
as n
ot c
lear
whe
ther
grou
ps d
iffe
red
sign
ifica
ntl
y.)
Adu
lts
Tho
se in
the
SM
P p
rogr
amco
mpa
red
wit
h co
ntr
ols
inpu
blic
hou
sin
g
Job
prov
ides
med
ical
car
ebe
nefi
ts (
amon
g th
ose
empl
oyed
)
SMP
pa
rtic
ipan
tsT
hose
in t
he S
MP
pro
gram
wer
e m
ore
likel
y to
hav
em
edic
al c
are
ben
efits
tha
n t
heco
ntr
ol g
roup
in p
ublic
hou
s-in
g. (
Not
e: N
o st
atis
tica
l tes
tw
as r
epor
ted,
so
it w
as n
otcl
ear
whe
ther
gro
ups
diff
ered
sign
ifica
ntl
y.)
Fannie Mae Foundation
72 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 73
Second, if relocation was not assigned randomly, agents’ perceptions orclients’ preferences introduced selection bias. Although researchersasserted that participants were assigned to their neighborhood regard-less of their locational preference (Rosenbaum 1995), other evidencesuggests that program managers may have screened families theybelieved were better suited for moving to the suburbs (Goering 2003).Third, the pre/post study of children experienced substantial loss tofollow-up (40 percent attrition). In addition to limiting the power todetect meaningful effects (since the sample size was only 114 to beginwith), the widely cited beneficial educational and social outcomes accru-ing to suburban children may have resulted from selection if those who dropped out of the study differed systematically from those whoremained (Briggs 1997). Fourth, the Gautreaux program did not includea control group (both groups did move), so we cannot glean what mighthave happened to participants in the absence of the policy. We concludetherefore that the Gautreaux studies have methodological problems.
Section 8
The Section 8 program gives qualified low-income participants a rentalsubsidy for use in private apartment units. The program has been eval-uated over the past 25 years in many comprehensive studies, includingseveral federally funded policy experiments (Kennedy and Leger 1990;Peroff et al. 1979). Yet most of these studies did not include outcomesrelevant to our literature review. We did, however, find one study thatmeasured health. Meyers et al. (1995) found that children under agethree from families on the Section 8 waiting list had decreased growth(weight for age) compared with children in families receiving vouchers,indicating that the Section 8 policy might prevent undernutrition.However, this study is subject to substantial validity threats because of its convenience sampling method and cross-sectional design.
Yonkers scattered-site public housing
In addition to tenant mobility programs, scattered-site public housingprograms have been implemented as a result of court decrees to raciallydesegregate concentrated areas of poverty in central cities. In 1986, theDistrict Court ordered Yonkers, N.Y., to racially desegregate its publichousing, since 26 of the city’s 27 public housing units were located inthe same high-poverty, racially isolated, southwest quadrant of the city.The court ordered the construction of 200 units of scattered-site publichousing in low-poverty areas, 7 of which were built between 1990 and1993 (Briggs and the Yonkers Family and Community Project 1997;
Housing Policy Debate

Peterson and Williams 1995). Tenants were selected by lottery oncefamilies met the qualification criteria.
The Yonkers research team plans a 15-year study, including measure-ment of physical and mental health effects. The team also created acomparison group through a snowball sampling method, beginningwith referrals from movers—they gave the team the names of acquain-tances who stayed behind in the public housing projects.9 Although theteam found few demographic differences between the movers and thestayers (Briggs and the Yonkers Family and Community Project 1997),this does not rule out selection bias resulting from an invalid compari-son, if the controls might not have qualified or might not have wantedto apply for scattered-site public housing for reasons that would makethem not comparable to those who applied.
Briggs and the Yonkers evaluation team documented recent violentvictimization, depression and anxiety symptoms, and substance abuseamong mothers (Briggs, Darden, and Aidala 1999; Briggs and theYonkers Family and Community Project 1997). Compared with stayers,the mover group reported a lower prevalence of depression symptoms,of problem drinking, of marijuana use, and of violent or traumaticevents (Briggs and the Yonkers Family and Community Project 1997).Among youth, movers reported lower access to alcohol and cigarettesthan stayers did (Fauth, Leventhal, and Brooks-Gunn 2002).
The strength of this study resides in its valid and reliable health meas-ures and its prospective design with a concurrent comparison group.Yet the uncertain appropriateness of the control group (and the result-ing selection bias introduced through creation of a snowball controlgroup) remains the largest threat to the study’s validity.
Other litigation studies
Several cities throughout the country are conducting household mobil-ity programs like the Gautreaux program or unit-based mobility pro-grams like the Yonkers scattered-site public housing, most initiated byracial discrimination litigation. Although these studies are rarely evalu-ated,10 we did find that one qualified for inclusion in our review. The
Fannie Mae Foundation
74 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
9 Originally, the Yonkers intervention would have exploited an experimental design,since a lottery was used, but there were too few lottery losers to create a large enoughcontrol group.
10 Some housing mobility programs, including those in Cleveland, Dallas, and Durham(N.C.), have been formally evaluated (Peterson and Williams 1995), but they are not

Does Housing Mobility Policy Improve Health? 75
evaluation of the Cincinnati Special Mobility Program measured violentvictimization and health care, although the study is methodologicallyvery weak. Fischer (1991) compared the intervention group before andafter the policy and also compared the intervention group with publichousing controls at follow-up. He found that moving out of concen-trated public housing was associated with fewer attacks or robberiesand with the receipt of employer-supplied health care benefits. How-ever, this was the weakest of all the studies included in our review. Thecontrol group was likely not comparable with the intervention group,and we could not assess the amount of bias, since the author did notreport any multivariate regressions or other analyses to control for con-founding. Moreover, he did not include any statistical tests of differenceor table of numerical results.
MTO
The federal government has implemented a randomized housing mobil-ity policy experiment in five U.S. metropolitan areas with the MTO pro-gram. Sponsored by HUD and begun in 1994, the experiment randomlyassigned selected participants from central-city public housing to one ofthree groups:
1. The treatment group (also referred to as the experimental or MTOgroup) was offered both a Section 8 housing voucher that could beredeemed only in a low-poverty neighborhood and housingcounseling.
2. The Section 8 group was offered a geographically unrestricted Sec-tion 8 housing voucher.
3. The in-place control group did not receive a voucher, but remainedeligible for public housing.
All of the participants consisted of low-income families, and most wereracial minorities (Goering et al. 1999). This review covers results fromthe first follow-up evaluation fielded in each city, which took placeapproximately two to three years after randomization and was releasedin 2002. The results from a more recent interim survey fielded in2001–2002 were released while this article was under review.
Housing Policy Debate
considered natural experiments because of their design and implementation. As aresult, conclusions drawn from favorable outcomes cannot be attributed to the policyitself unless a sound comparison group is found. Although we reviewed these studiesfor inclusion in this review, they did not qualify.

Two of the MTO sites have reported mental and physical health out-comes (Boston and New York), three have reported violent crime vic-timization (Boston, New York, and Chicago), two have reported medicalcare outcomes (Los Angeles and Boston), and one has reported health-behavior outcomes (New York) (Hanratty, McLanahan, and Pettit 2003;Katz, Kling, and Liebman 2001; Leventhal and Brooks-Gunn 2003a,2003b; Rosenbaum and Harris 2001).
As a result of the Boston MTO policy, children in treatment group fami-lies have experienced fewer injuries or accidents, and boys in the treat-ment and Section 8 groups both displayed fewer reported behaviorproblems than controls. Investigators reported a marginal reduction in the treatment of children’s asthma attacks and in personal crimevictimization (attacks, threats, or robberies). Boston treatment andSection 8 parents reported better overall health, as well as higher pro-portions of being calm and peaceful (Katz, Kling, and Liebman 2001).
Leventhal and Brooks-Gunn (2003a) provide evidence that moving tolow-poverty neighborhoods in New York resulted in large improve-ments in mental health for boys, especially among the treatment group.As table 2 illustrates, compared with controls, the New York experi-mental and Section 8 children, as well as subgroups (usually boys orthe younger children), reported significantly improved mental health,which manifested as fewer problem behaviors such as anxiety ordepression, dependency, fear, and the need to be near adults. In somecases, Section 8 children experienced lower levels of problem behavior(being headstrong, unhappy, sad, or depressed and depending too muchon others) than controls, when the experimental children did not (Lev-enthal and Brooks-Gunn 2003a, 2003b).
The New York MTO study found different significant effects for teenproblem health behaviors (using cigarettes or alcohol) by gender. Unex-pectedly, adolescent girls in the experimental group were significantlymore likely to have used alcohol in the past year than in-place controls,but teen boys in the experimental group reported fewer peers using cig-arettes. New York treatment group parents were significantly less likelyto report distress symptoms than controls and marginally less likely toreport depressive symptoms (Leventhal and Brooks-Gunn 2003a,2003b).
In terms of medical care, neither of the two sites that measured med-ical care found an effect (Hanratty, McLanahan, and Pettit 2003; Katz,Kling, and Liebman 2001). None of the three sites that measured expe-rience of violent crime found significant results between experimentaland control groups (p < 0.05), although the New York and Chicago
Fannie Mae Foundation
76 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 77
sites both found a reduction in crime from baseline to follow-up (Leven-thal and Brooks-Gunn 2003a; Rosenbaum and Harris 2001). This sug-gests that a secular decrease in crime may have occurred.
The design of the Chicago follow-up survey (investigators re-interviewed movers only, with no control group comparison) suggeststhat inferences from this site may be biased. The study may have expe-rienced secular effects without control group measurement at follow-up; for instance, if the participants were affected by an external factornot derived from the MTO study, such as economic changes, the studywould incorrectly infer an effect caused by MTO (Orr 1999).
While this article was under review, HUD released the MTO InterimImpacts Evaluation (Orr et al. 2003), which included detail of healthoutcomes resulting from relocation four to seven years after randomiza-tion. In that report, investigators did not report site-specific findings.Adults in the experimental and Section 8 groups experienced signifi-cantly lower obesity (measured as body mass index) than the controlgroup, and adults in the experimental group had a lower prevalence ofmental health problems (psychological distress and depression). Noeffects were observed among adults for asthma, self-reported health,high blood pressure, smoking, drinking alcohol, or activities of dailyliving. Among children, girls in both experimental groups reportedimproved mental health. Boys aged 12 to 19 in the Section 8 groupreported more injuries requiring medical attention. Aside from injuries,no physical health effects were observed for children or teens, andthere were no significant group differences in access to health care (Orr et al. 2003).
The MTO interim evaluation also measured risky health behaviorsamong adolescents. Teen girls in the experimental group reportedlower lifetime use of marijuana and of smoking tobacco. Teen boys inboth treatment groups unexpectedly reported significantly higher ratesof smoking tobacco than controls (Orr et al. 2003).
The health findings of the 2003 MTO interim report are somewhat con-sistent with the first follow-up study, indicating mainly mental healthbenefits, in addition to the lower levels of adult obesity, which had notbeen previously measured, among the experimental groups. This policymay differentially affect children by gender, as suggested by Leventhaland Brooks-Gunn (2003a), where girls’ mental health may benefit,whereas boys’ health may be harmed by smoking uptake and injuries inadolescence. The interim findings are also consistent for health careaccess, since neither evaluation found group differences.
Housing Policy Debate

Although the randomized design of the MTO study strengthens thecausal inferences drawn from the research, some threats to validityexist. If one analyzes only those who leased up (took advantage of thevoucher), MTO individuals are highly selected. The low lease-up ratescan be conceptualized as low treatment compliance and may reduce thestudy’s power to detect meaningful differences among groups.11 How-ever, researchers can use and have used an intent-to-treat (ITT) analy-sis to keep randomized groups intact in the analysis. If conductedcorrectly, ITT analysis should treat noncompliant subjects, in this casethose who were selected for the MTO experimental groups but did notuse the voucher, as treatment failures, since noncompliance may beassociated with “side effects” of the intervention. For instance, as sug-gested earlier, losing a regular source of medical care could be a signifi-cant side effect of moving to a new neighborhood. But if all originalstudy members are identified and if the effects of the treatment can beassumed as positive, then when analyzed as ITT, the effects should beunbiased by selection for the average effect on the group regardless ofcompliance (Greenland 2000). But the effect estimated by ITT is theeffect of being offered a housing voucher, not receiving one.
Furthermore, MTO researchers have conducted instrumental variableanalysis (IVA) that strengthens the conclusions that the policy mayimprove health. The authors estimated the effect of the treatment-on-treated (TOT) by using this technique, which corrects for bias thatwould usually arise if one applied an ITT analysis or directly comparedtreated with untreated individuals in a randomized trial. The techniqueuses a variable, “the instrument,” which is associated with the predic-tor and has no other influence on the outcome except that mediated bythe predictor, to estimate the causal effect of the treatment on thosewho were randomly assigned to treatment and actually received it. TheTOT analyses found significant results for some health outcomes thatwere not significant in the ITT analyses, suggesting that, as expected,
Fannie Mae Foundation
78 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
11 The experimental group actually used the low-poverty neighborhood voucher at a lowrate—48 percent across all five sites; see table 5 in Goering et al. (1999). Notably, thelease-up rate—hence selection into low-poverty neighborhoods—may be related tohealth. After conducting a multiple regression analysis predicting lease-up rates withbaseline information across all five sites, Shroder (2002) reported that families receiv-ing disability payments (supplemental security income/Social Security Disability Insur-ance/Social Security survivor benefits) were significantly less likely to lease up or takeadvantage of the housing voucher to move. Further, interviews with MTO mobilitycounselors revealed that many families that failed to use the voucher to move did sobecause they did not want to move farther away from the medical care that they ortheir children were receiving. These findings stimulated researchers to observe that“health care is perhaps the most important place-based service that these families relyon in their neighborhoods” (Kling, Liebman, and Katz 2001, 22). Thus, it is plausiblethat healthier individuals may have been selected into using the voucher.

Does Housing Mobility Policy Improve Health? 79
the policy had stronger effects on those who actually relocated to low-poverty neighborhoods (Greenland 2000).12
The MTO research findings may also be biased by loss to follow-up.This threat presents itself especially in the New York study, where 31 percent of the participants were lost, and in Chicago, where only 51 percent—none of them controls—were interviewed at follow-up.
Although randomized trials eliminate many serious threats to internalvalidity, several remain. The most relevant for MTO are likely compen-satory rivalry and compensatory equalization, both of which occurwhen the treatment is perceived as desirable (Cook and Campbell1979). Compensatory rivalry, also called the John Henry effect, couldhave surfaced if MTO control group members felt cheated by not hav-ing received the treatment and worked harder than they would have inthe absence of this policy to seek some sort of substitute for the treat-ment, such as neighborhood mobility or homeownership. With compen-satory equalization, an administrative body that deems control statusless desirable than treatment steps in to offer a comparable treatmentas a sort of consolation. This could have happened in MTO, forinstance, if housing authorities provided vouchers to controls in a moreexpeditious manner than they would have without knowledge of thecontrol’s participation in the experiment. In both cases, the bias resultsin underestimating the treatment effect, because the controls are per-forming artificially better than they would have without the policy.
Assessment of the empirical evidence
The strongest studies had randomized designs using ITT analysesand/or valid and reliable measures of health. Our review methods gavethe Boston MTO study (Katz, Kling, and Liebman 2001) the strongestmethodological score because it was randomized and analyzed as ITT,used valid and reliable health measures, experienced very low attrition,
Housing Policy Debate
12 In general, IVA effect estimates for a trial will be further from the null than ITTestimates because many of those assigned to the treatment may not actually receive it. These individuals presumably dilute the estimated effect of the treatment in an ITTanalysis. The bias in the ITT effect estimates is proportional to the amount of noncom-pliance, so in experiments with substantial noncompliance, such as MTO, the differencebetween ITT and IVA estimates may be large. There is some criticism of using IVA esti-mates in this case, because people who did not adhere to the treatment/policy may bethose who could somehow have been harmed by it. For example, in MTO, it is plausiblethat people who did not use the vouchers were those who were afraid to lose their regu-lar source of medical care. In this case, the causal effect of the treatment on the treatedis not the same as the average causal effect of the treatment on the whole population.

used instrumental analysis to examine effects on movers, and exhibitedfew remaining threats to validity (table 1). It was the only study toattain “good” methodological rigor according to the Briss method (Brisset al. 2000). The New York MTO mental health study (Leventhal andBrooks-Gunn 2003b) ranked next highest because of its randomizeddesign, ITT and IVA, and valid and reliable health measures. Fourother studies fall in this same fairly strong category: the other NewYork MTO study (Leventhal and Brooks-Gunn 2003a), the two Yonkersstudies (Briggs and the Yonkers Family and Community Project 1997;Fauth, Leventhal, and Brooks-Gunn 2002), and one Gautreaux study(Rosenbaum and Popkin 1990). Despite its nonrandomized design, theYonkers study scored high because of its very low attrition rate; itsnumerous valid and reliable health measures; and its thorough policy,population, and methodological discussions (Briggs and the YonkersFamily and Community Project 1997).
We evaluated the rest of the studies as being of limited methodologicalstrength, because of five or more serious threats to validity. Falling inthis category were the Chicago (Rosenbaum and Harris 2001) and LosAngeles (Hanratty, McLanahan, and Pettit 2003) MTO studies, the Sec-tion 8 study assessing child growth/undernutrition (Meyers et al. 1995),and the original Gautreaux evaluation assessing health care satisfac-tion (Peroff et al. 1979). The Chicago MTO study experienced substan-tial attrition (50 percent) and did not interview controls at follow-up, sothe investigators could not conduct an ITT analysis. The Los Angelesstudy was ranked as limited because it was not clear how reliable orvalid the health care outcome was, and the researchers were notexplicit about their statistical and analytical methods. Two Gautreauxarticles using the same study data (Rosenbaum 1994, 1995) and theCincinnati litigation program (Fischer 1991) finished last in our analy-sis. These Gautreaux studies experienced substantial loss to follow-up(40 percent attrition), the author was not explicit about statisticalmethods used to account for confounding, and the validity and reliabil-ity of the victimization measure were not addressed. The Fischer(1991) study was methodologically weak because the author was notexplicit about the statistical methods used to control for confounding,and he did not present tests of statistical significance, numeric results,or validity/reliability of measures.
Overall, the evidence suggests that both tenant- and unit-based hous-ing mobility policies may contribute to improving child, adolescent, andadult health and health behaviors. However, this preliminary evidencecomes from a small number of studies, many of which have method-ological limitations associated with the lack of an experimental orquasi-experimental design.
Fannie Mae Foundation
80 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman
Does Housing Mobility Policy Improve Health? 81
Further, although there is some evidence that relocation to betterneighborhoods could lead to improved health among public housing res-idents, none of the studies reviewed explicitly tested the mechanismsthrough which housing mobility policies could impact health. As Briggsnotes, the literature on the neighborhood effects of housing mobilityprograms has not elucidated the mechanisms by which the observedoutcomes came to be, or the “how” of the processes involved (1997).Some mechanisms are being tested in the Yonkers study, but accordingto our review, very few of these have been tested thus far in the MTOexperiment. However, the potential exists to include such hypotheses inthe data collection for the 10-year MTO follow-up.
Discussion
The housing mobility policies described in this article were conceived as racial and economic desegregation policies. Although they were notintended to affect health, it appears that they may have. Indeed, Leven-thal and Brooks-Gunn claim that “the most significant benefits of theMTO program were noneconomic” (2003b, 1580). From a public healthperspective, the most important implication of the evidence on housingmobility is that housing policy has the potential to improve individualhealth. Mobility and other housing policies should continue to be evalu-ated for their impact on health. If the long-term benefits are positive,as suggested thus far by this limited research on housing mobility, suchpolicies may promise to improve individual health and quality of life, aswell as the health of the population as a whole. Because housing mobil-ity policies target very low-income families, these policies may also havethe potential to reduce health disparities by improving the health ofthese disadvantaged groups.
Generalizability
The available evidence suggests that housing mobility programs couldimprove health. However, there is strong empirical evidence from onlytwo MTO sites, Boston and perhaps New York, and from the Yonkersstudies. These results may not be generalizable to other cities with dif-ferent demographic and social characteristics. Moreover, as discussedearlier, MTO results could be generalizable by design only to familiesthat volunteer to leave public housing. At least in the MTO demonstra-tion, those families appear to be more disadvantaged than the generalpublic housing population and may have had strong, specific motives tomove. As summarized by Shroder (2002), “[W]ith this experiment wewill have a chance to evaluate without bias the benefit of moving out of
Housing Policy Debate

high poverty to those who want to move and are willing to keep search-ing until they succeed” (337, emphasis added). Accordingly, it is possiblethat MTO results overestimate the possible effects on health that theintervention could have on families that already are participating in theSection 8 program or families that could be transferred from publichousing to Section 8 without volunteering for it.
Effects on health outcomes
Before MTO, much of the evidence on health and housing mobility had little scientific weight because of the lack of experimental designsand the associated threat of selection bias. The evidence from MTO isstronger because of its experimental design, but since this policydemonstration was not designed to measure the effects of housingmobility on health, the range of health outcomes is limited for the mostpart to a few self-reported measures. Since none of the sites at the firstfollow-up study collected any physiological health measures or bloodsamples, there is no evidence of change in biological markers. However,the apparently positive effect on self-reported outcomes suggests that,at a minimum, psychological well-being improved.
Additionally, although the research teams at the various sites havespeculated about the possible mechanisms through which MTO mayimprove health, the demonstration was not designed to explore specificmechanisms. For example, Katz, Kling, and Liebman (2001) have pro-posed that the marginally significant reduction in the number of self-reported asthma attacks among children in experimental householdsmay be linked to the better air quality and the decreased stress, crowd-ing, lack of heat, or exposure to allergens from vermin that are associ-ated with living in better neighborhoods. Other questions forexploration include whether the housing units in the new neighbor-hoods contain less mold caused by aging or leaky pipes or whether win-dows are less likely to be nailed or painted shut, thus preventing airflow that could disperse indoor allergens or toxins that trigger asthma.In other words, the marginal reduction in asthma rates could be due toa neighborhood factor (safety, air quality) or a household factor (mold,allergens), or both. Given the present MTO data, it is not possible toelucidate the relative weight of these mechanisms.
Segregation, neighborhoods, and health
Although the MTO results may provide some indirect support for socialepidemiologic evidence that racial and economic residential segregation
Fannie Mae Foundation
82 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 83
could be positively associated with mortality and morbidity rates, theMTO’s scope is simply too small to alter racial segregation or povertyconcentration patterns at the metropolitan level. For example, the sizeof the black population in the Boston metropolitan area in 1990 wasapproximately 198,000. In the same year, the dissimilarity index forblacks in this metropolitan area was 69.6, indicating that nearly 70 per-cent of the black population—more than 138,000 individuals—wouldhave had to move to different neighborhoods to achieve an even distri-bution with respect to the non-Hispanic white population (Lewis Mum-ford Center for Comparative Urban and Regional Research 2001). Bycontrast, the MTO demonstration in Boston involved only about 135(mostly black) families.
In relation to the epidemiologic evidence on neighborhood effects onhealth, the randomization of study participants to the control group,the regular Section 8 group, or the MTO group means that it is safe toassume that any observed effects on health are not due to individual-level characteristics. That is, there is no threat of selection bias. How-ever, it is not clear that effects can be attributed to neighborhoodenvironment.
Future research and data
Conceptual frameworks. As discussed earlier, epidemiologic research onhousing and health has largely lacked a conceptual foundation. Hous-ing policy research constitutes a unique opportunity to explore variousneighborhood effects on health through experimental designs. Concep-tual frameworks should outline plausible mechanisms through whichneighborhood conditions could affect specific health outcomes. Thedevelopment of such conceptual frameworks will require multidiscipli-nary research teams that include housing policy and public healthexperts (Srinivasan, O’Fallon, and Dearry 2003). Public health researchcan help inform the selection of health outcomes that are more sensi-tive to certain neighborhood conditions at certain times in the lifecourse. For instance, Macintyre and Ellaway (2003) discuss the ideathat fear of crime or violence may influence women and elders morethan it does men or younger people, affecting mental but not physicalhealth. Conversely, children may be more sensitive than adults to mate-rial conditions like damp, which affects respiratory disease (Macintyreand Ellaway 2003). In the latest MTO report (Orr et al. 2003), theinvestigators found it difficult to interpret the lower rates of obesityamong experimental adults. However, public health research suggeststhat disadvantaged neighborhoods are associated with reduced access tohealthful foods because fewer grocery stores are available (Morland
Housing Policy Debate

et al. 2002) and with unsafe or “low-walkability” conditions that maynot be conducive to physical activity (Saelens et al. 2003). In turn,those factors may be linked to higher rates of obesity. Alternatively, the MTO interim finding that experimental families eat more mealstogether as a family may explain part of the obesity effect; for example,parents may be preparing healthier meals more frequently.
Since housing mobility programs have been introduced in part to helpremedy racial segregation, which originates in both institutional andinterpersonal racial discrimination, it is important to address discrimi-nation in the conceptual framework and variables measured in futurehousing mobility studies. The MTO team has taken a first step towardthis end by including an item in the interim report dealing withwhether participants faced housing discrimination during their lasthousing search (Orr et al. 2003). Yet the authors have not presentedthis information within a racial context. The MTO sites varied substan-tially in the racial makeup of their population, and different metropoli-tan areas display markedly different rates of housing discrimination(Acevedo-Garcia, Osypuk, and Krimgold 2003; Gabriel 1996), as doneighborhoods with different racial composition (Gabriel 1996). More-over, racial discrimination is experienced in many forms, across variouslife domains in addition to the housing domain, and many of these havebeen shown to affect health (Gee 2002; Krieger and Sidney 1996;Williams and Neighbors 2001; Williams, Neighbors, and Jackson 2003).Racial disparities in health are well-established (Williams 2001;Williams et al. 1997), but rarely do health investigators measure thesocial process of racism—that is, the mechanism by which race is mostlikely associated with health. Including a more comprehensive measureof racial discrimination, presenting racism experience by MTO site andby racial group, and analyzing data on discrimination by the racialcomposition of the census tract may be invaluable to better under-standing both housing-specific and non-housing-specific discriminationand its effects on health. Also, the Section 8 program faces importantchallenges, such as the negative reactions that some communities haveexpressed against the influx of families on housing assistance (Briggs1997, 1998; Rosenbaum 1995). Therefore, it would be important toassess the potentially negative effects—for example, stress and depres-sion—on the health of families moving into hostile communities.
Additionally, future research should explore whether improvements inhealth outcomes might eventually lead to long-term improvements ineconomic outcomes. For example, parents who receive public assistanceare more likely to have children with such chronic health conditions asasthma, which in turn limits their ability to work (Heymann and Earle1999). If housing mobility policies can effectively improve children’shealth, parents may be more likely to succeed in the labor force.
Fannie Mae Foundation
84 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 85
Multilevel data and analytic methods. Future research on housingmobility should include a larger sample of individuals, neighborhoods of origin, receiving neighborhoods, and metropolitan areas, as well asmore comprehensive data on unit characteristics. Many of the researchquestions that future studies should address are inherently multileveland thus will require multilevel analytic methods (Subramanian, Jones,and Duncan 2003). For instance, given that improvements in neighbor-hood quality that result from mobility policies are conceivably accompa-nied by improvements in the quality of housing units, it is important to determine whether mobility policies result in improved health out-comes because of housing unit effects, neighborhood effects, or both.Similarly, improvements in housing and neighborhood quality couldhave differential effects on individuals with various demographic andsocioeconomic characteristics. The health effects of improving theneighborhood environment may be greater for individuals/householdswith fewer coping resources, such as those with low socioeconomic sta-tus or single-headed households.
Multilevel methods may also allow us to assess whether there is signifi-cant variation in health outcomes across neighborhoods, includingacross experimental neighborhoods, and, if so, which factors couldexplain this variation. For instance, health effects may be greater if thereceiving neighborhoods have a low poverty rate (below 10 percent), asopposed to being simply less disadvantaged than the neighborhoods oforigin.
Further, to the extent that housing mobility demonstrations are con-ducted in a large cross-section of metropolitan areas, multilevel meth-ods may allow us to determine whether health outcomes are affected bymetropolitan area characteristics after we control for neighborhood orhousehold characteristics. For example, are health effects greater ifmobility policies are implemented in metropolitan areas with higherlevels of racial or economic segregation, since movers may have more togain than their counterparts in areas with lower levels of segregation?
Qualitative research methods. Our review focused on studies with anexperimental design, which social epidemiologists regard as a valuableyet often not feasible method of evaluating neighborhood effects (Oakes2004). The 2001 qualitative study of Boston’s MTO (Kling, Liebman,and Katz 2001), which brought the importance of health to the atten-tion of investigators, and the 2002 qualitative study of MTO (Popkin,Harris, and Cunningham 2002), as well as the qualitative neighborhoodand health studies of Boston by Gans and of Chicago by Raudenbushand Sampson (Kawachi and Berkman 2003a) suggest the potential ofsuch research methods for understanding the pathways through which
Housing Policy Debate

neighborhood conditions might affect health. Qualitative investigationprovides a historical context and also communicates the reciprocal anddynamic process of how people shape their neighborhoods (Macintyreand Ellaway 2003). Qualitative research methods could also be used toinform the design of the quantitative data collection and help explainthe results from quantitative analyses (Popkin, Harris, and Cunning-ham 2002).
Better health, housing, and neighborhood data. Future studies shouldalso include better measurement of health outcomes, including baselineand follow-up measurements and triangulation of methods—biologicalmeasures, self-reported health measures, and validated scales (forexample, depression). Given proper ethical and confidentiality protec-tions, it would also be important to link participant data to healthinsurance claims or medical records, especially for diagnostic-specificinformation. Such linking may be feasible for policies such as MTO ifsubstantial proportions of participants were enrolled in Medicaid orstate children’s health insurance programs. Linking to administrativehealth data seems feasible, since the MTO follow-up study plans to link to other administrative data systems, such as welfare, arrestrecords, and schools (Orr et al. 2003). In addition to being uniformacross all the study sites (the original survey instruments were not),the 2001–2002 follow-up MTO household survey prepared by AbtAssociates, Inc., partially addressed some of these issues. Namely, itincluded detailed sections on injuries, asthma symptoms, body massindex, and blood pressure measurement. Yet additional measures mayinclude other health outcomes that could be associated with neighbor-hood conditions, for example, intimate partner violence and infectiousdiseases such as tuberculosis, HIV, and sexually transmitted diseases(Acevedo-Garcia 2000; Fullilove 2003; Kawachi and Berkman 2003b;O’Campo et al. 1995).
Biomarkers can be employed to test specific physiologic mechanisms ofhousing or neighborhood effects on health. For instance, the physiologi-cal stress response can be tested by measuring the stress hormone cor-tisol in saliva samples. Several biomarkers are available for asthma(Christiani 1996; Loucks 2003) (i.e., inflammatory markers), as well asfor immune function (Kiecolt-Glaser et al. 2002), both of which can beaffected by stress. If we hypothesize that housing mobility affects nutri-tional intake in the form of increased access to higher-quality super-markets in low-poverty neighborhoods or reduced access to fast food inhigh-poverty neighborhoods, we can measure serum fasting glucose orserum cholesterol. Biomarkers are useful for valid measurement of out-comes that may be influenced by cognitive status or by social desirabil-ity (such as smoking, intake of fruits and vegetables, or weight) or for
Fannie Mae Foundation
86 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 87
intermediate outcomes for chronic diseases that take a long time todevelop (such as blood pressure or cholesterol for heart disease) (DeGruttola et al. 2001; Loucks 2003).
To date, few social epidemiologic studies have progressed beyonddemonstrating that certain structural characteristics of neighborhoods,such as poverty or disadvantage, appear to exert a contextual influenceon health after taking into account compositional characteristics suchas the socioeconomic status of residents. Few attempts have been madeto characterize and measure the social, physical, and service aspects ofneighborhood environments and to test the causal mechanisms under-lying the influences of these aspects of neighborhood environments onhealth outcomes. Social epidemiologists concur that future research onneighborhood effects should incorporate the development of valid, reli-able measures and scales of various aspects of neighborhood environ-ments (Morland et al. 2002; O’Campo 2003; Saelens et al. 2003). Forexample, assessing whether a neighborhood is conducive to physicalactivity could involve gathering data on sidewalks, bicycle lanes,shared-used paths, work sites, green ways, or recreational facilities(Librett, Yore, and Schmid 2003). Recent work by the Urban Instituteunder the National Neighborhood Indicator Partnership project (Pettitet al. 2003) constitutes an example of the types of specific neighborhoodindicators that could be useful in future health research on neighbor-hood effects.
Moreover, subjective and objective neighborhood data may tap differenthealth mechanisms. For instance, subjective rating of crime may bemore inhibiting for exercise than objective crime rates; alternatively,subjective reports may introduce reporting bias. For instance, someonewith respiratory problems reports that his or her home is dampbecause this person believes it contributes to his or her illness. Further,subjective reports may empirically demonstrate less variation thanobjective assessments (Kawachi and Berkman 2003a; Macintyre andEllaway 2003).
Evaluation of other housing policies. Given that they target low-incomeand very low-income families, housing vouchers and mobility initiativesshould continue to be evaluated for their impact on the health of disad-vantaged groups and their contribution to reducing health disparities.Housing vouchers are becoming the dominant strategy for providinghousing assistance, with the potential for reaching approximately 5.4 million households—the estimated worst-case housing needs popu-lation (HUD, Office of Policy Development and Research 2000). As apolicy demonstration, MTO has been very limited in scope (about 1,800experimental families), and its political viability as a large-scale pro-gram is not certain. Therefore, it will be important to further evaluate
Housing Policy Debate

the health impact of Section 8 and some of its politically viable varia-tions—such as regional, as opposed to local, administration of the pro-gram, which has been proposed as a way to enhance its housingmobility potential (Katz and Turner 2001; Turner 1998).
Although the evidence from the housing mobility studies is not defini-tive, it will be important to put the magnitude of these results into per-spective. How big are the health effects of housing policy comparedwith the effects measured for explicit health interventions? Forinstance, are the effects on asthma from housing mobility large com-pared with the effects from health education programs specificallytargeting asthma? A closely related issue is the approximate cost ofhousing mobility programs. We should take the relative effects of hous-ing interventions and explicit health interventions on health outcomesin the context of their relative costs. A crude comparison shows thatthe total annual HUD budget for rental assistance is approximately$17.5 billion, compared with more than $140 billion annually for Med-icaid. Incorporating more specific cost-benefit considerations into ouranalyses could inform considerations of the specific health outcomes ofhousing mobility policies.
During the 1990s, under the HOPE (Home Ownership for PeopleEverywhere) VI program, the federal government changed its housingpolicy toward low-income households and moved away from project-based assistance (public housing projects) toward an increased use ofhousing vouchers and mixed-income housing developments (Buron etal. 2002; Sard 2000). The nature and scale of such policy changes war-rant an examination of their possible health effects, especially on fami-lies that have been displaced and unable to find affordable housing. Ina tracking study of HOPE VI, the Urban Institute has identified healthproblems as a major issue for former residents of distressed publichousing (Buron et al. 2002).
Earlier, we identified promotion of homeownership among low-incomehouseholds and antidiscrimination policy as two strategies that, likehousing mobility policy, could potentially mitigate health disparities. Inthe future, health research may identify quasi-experimental or experi-mental policy demonstrations in those two areas, where health out-comes could be incorporated into the evaluation. Further, otherimportant housing policies, such as federal tax deductions to promotehomeownership, policies to promote homeownership among low-incomehouseholds, and fair housing policies, should be evaluated for theireffect on health outcomes. For instance, in terms of health impactamong low-income groups, does homeownership have a larger positivehealth influence than housing mobility?
Fannie Mae Foundation
88 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 89
The evidence from Yonkers and MTO suggests that housing mobilitypolicy could have positive and, ironically, largely unintended effects onhealth. HUD has a strong, long-standing tradition aimed at conductinghousing policy demonstrations with an experimental design (Shroder2000). Therefore, there is already a good infrastructure for carrying outhousing policy demonstrations with attention to health outcomes. Intheir vision for housing policy in the new millennium, policy makersbelieve that “housing policy must be linked to other social policies”(Wachter 2000, 1). Integrating better health as an explicitly desirableoutcome of housing policy could help fulfill this vision.
Authors
Dolores Acevedo-Garcia is an Assistant Professor in the Department of Society, HumanDevelopment, and Health at the Harvard School of Public Health. Theresa L. Osypukis a doctoral student in the Department of Society, Human Development, and Health atthe Harvard School of Public Health. At the time of this writing, Rebecca E. Werbelwas a graduate student in the Department of Society, Human Development, and Healthat the Harvard School of Public Health. Ellen R. Meara is an Assistant Professor in theDepartment of Health Care Policy at Harvard Medical School. David M. Cutler is a Pro-fessor in the Department of Economics at Harvard University. Lisa F. Berkman is theThomas D. Cabot Professor of Public Policy in the Department of Society, HumanDevelopment, and Health at the Harvard School of Public Health.
References
Acevedo-Garcia, Dolores. 2000. Residential Segregation and the Epidemiology of Infec-tious Diseases. Social Science and Medicine 51(8):1143–61.
Acevedo-Garcia, Dolores, and Kimberly A. Lochner. 2003. Residential Segregation andHealth. In Neighborhoods and Health, ed. Ichiro Kawachi and Lisa F. Berkman,265–87. New York: Oxford University Press.
Acevedo-Garcia, Dolores, Kimberly A. Lochner, Theresa L. Osypuk, and S.V. Subraman-ian. 2003. Future Directions in Residential Segregation and Health Research: A Multi-level Approach. American Journal of Public Health 93(2):215–21.
Acevedo-Garcia, Dolores, Theresa L. Osypuk, and Barbara Krimgold. 2003. Metropoli-tan Report Cards: How Well Are Different Urban Areas Providing Quality of Life forAmericans of Color? Presented at the Color Lines Conference, sponsored by the CivilRights Project at Harvard University, Cambridge, MA. August 29–September 1.
Allen, Chris. 2000. On the “Physiological Dope” Problematic in Housing and IllnessResearch: Towards a Critical Realism of Home and Health. Housing, Theory, and Soci-ety 17:49–67.
Housing Policy Debate

Altshuler, Alan, William Morrill, Harold Wolman, Faith Mitchell, and the Committee onImproving the Future of U.S. Cities through Improved Metropolitan Area Governance,eds. 1999. Governance and Opportunity in Metropolitan America. Washington, DC:National Academy Press.
Anderson, Laurie M., Carolynne Shinn, Joseph St. Charles, Mindy T. Fullilove, SusanC. Scrimshaw, Jonathan E. Fielding, Jacques Normand, Ruth Sanchez-Way, ToddRichardson, and the Centers for Disease Control and Prevention. 2002. CommunityInterventions to Promote Healthy Social Environments, Early Childhood Development,and Family Housing: A Report on Recommendations of the Task Force on CommunityPreventive Services. Morbidity and Mortality Weekly Report 51(RR01):1–8.
Barker, David J.P., Peter D. Gluckman, Keith M. Godfrey, Jane E. Harding, Julie A.Owens, and Jeffrey S. Robinson. 1993. Fetal Nutrition and Cardiovascular Disease inAdult Life. Lancet 341:938–41.
Bartley, Mel, David Blane, and Scott Montgomery. 1997. Health and the Lifecourse:Why Safety Nets Matter. BMJ 314:1194–96.
Berkman, Lisa F., and Ichiro Kawachi, eds. 2000. Social Epidemiology. New York:Oxford University Press.
Boyle, Michael H. 2002. Home Ownership and the Emotional and Behavioral Problemsof Children and Youth. Child Development 73(3):883–92.
Briggs, Xavier de Souza. 1997. Moving Up Versus Moving Out: Neighborhood Effects inHousing Mobility Programs. Housing Policy Debate 8(1):195–234.
Briggs, Xavier de Souza. 1998. Brown Kids in White Suburbs: Housing Mobility andthe Many Faces of Social Capital. Housing Policy Debate 9(1):177–221.
Briggs, Xavier de Souza, Joe T. Darden, and Angela A. Aidala. 1999. In the Wake ofDesegregation: Early Impacts of Scattered-Site Public Housing on Neighborhoods inYonkers, New York. Journal of the American Planning Association 65:27–49.
Briggs, Xavier de Souza, and the Yonkers Family and Community Project. 1997.Yonkers Revisited: The Early Impacts of Scattered-Site Public Housing on Families andNeighborhoods. A Report to the Ford Foundation. New York: Columbia UniversityTeachers College, Harvard University, and Michigan State University.
Briss, Peter A., Stephanie Zaza, Marguerite Pappaioanou, Jonathan Fielding, LindaWright-De Agüero, Benedict I. Truman, David P. Hopkins, Patricia Dolan Mullen,Robert S. Thompson, Steven H. Woolf, Vilma G. Carande-Kulis, Laurie Anderson, AlanR. Hinman, David V. McQueen, Steven M. Teutsch, Jeffrey R. Harris, and the TaskForce on Community Preventive Services. 2000. Developing an Evidence-Based Guideto Community Preventative Services—Methods. American Journal of Preventive Medi-cine 18(1S):35–43.
Buka, Stephen L., Robert T. Brennan, Janet W. Rich-Edwards, Stephen W. Raudenbush,and Felton Earls. 2003. Neighborhood Support and the Birth Weight of Urban Infants.American Journal of Epidemiology 157(1):1–8.
Fannie Mae Foundation
90 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 91
Buron, Larry, Susan J. Popkin, Diane Levy, Laura E. Harris, Jill Khadduri, Abt Associ-ates, Inc., the Urban Institute, and the Office of Public Housing Investments. 2002.The HOPE VI Resident Tracking Study. Prepared for the U.S. Department of Housingand Urban Development. Washington, DC: Urban Institute.
Christiani, David C. 1996. Utilization of Biomarker Data for Clinical and Environmen-tal Intervention. Environmental Health Perspectives 104(suppl 5):921–25.
Conley, Dalton. 1999. Being Black, Living in the Red: Race, Wealth, and Social Policy inAmerica. Berkeley, CA: University of California Press.
Cook, Thomas D., and Donald T. Campbell. 1979. Validity. In Quasi-Experimentation:Design and Analysis Issues for Field Settings, 37–94. Boston: Houghton Mifflin.
Deaton, Angus. 2002. Policy Implications of the Gradient of Health and Wealth. HealthAffairs March-April, pp. 13–30.
De Gruttola, Victor G., Pamela Clax, David L. DeMets, Gregory J. Downing, Susan S.Ellenberg, Lawrence Friedman, Mitchell H. Gail, Ross Prentice, Janet Wittes, andScott L. Zeger. 2001. Considerations in the Evaluation of Surrogate Endpoints in Clini-cal Trials: Summary of a National Institutes of Health Workshop. Controlled ClinicalTrials 22:485–502.
Dunn, James R. 2000. Housing and Health Inequalities: Review and Prospects forResearch. Housing Studies 15(3):341–66.
Dunn, James R. 2002. A Population Health Approach to Housing: A Framework forResearch. Ottawa, Ontario, Canada: National Housing Research Committee andCanada Mortgage and Housing Corporation.
Dunn, James R., and Michael V. Hayes. 2000. Social Inequality, Population Health, andHousing: A Study of Two Vancouver Neighborhoods. Social Science and Medicine51:563–87.
Ellen, Ingrid Gould. 2000. Is Segregation Bad for Your Health? The Case of Low BirthWeight. In Papers on Urban Affairs, ed. William G. Gale and Janet Rothenberg Pack,203–38. Washington, DC: Brookings Institution Press.
Ellen, Ingrid Gould, Tod Mijanovich, and Keri-Nicole Dillman. 2001. NeighborhoodEffects on Health: Exploring the Links and Assessing the Evidence. Journal of UrbanAffairs 23(3–4):391–408.
Ellen, Ingrid Gould, and Margery Austin Turner. 1997. Does Neighborhood Matter?Assessing Recent Evidence. Housing Policy Debate 8(4):833–66.
Fauth, Rebecca C., Tama Leventhal, and Jeanne Brooks-Gunn. 2002. They’re MovingOut; Are They Moving Up? Early Impacts of Moving to Low-Poverty Neighborhoods onLow-Income Youth. New York: Columbia University, Teachers College, National Centerfor Children and Families.
Fischer, Paul B. 1991. Is Housing Mobility an Effective Anti-Poverty Strategy? AnExamination of the Cincinnati Experience. Lake Forest, IL: Lake Forest College,Stephen H. Wilder Foundation.
Housing Policy Debate

Freeman, Lance. 2002. America’s Affordable Housing Crisis: A Contract Unfulfilled.American Journal of Public Health 92(5):709–12.
Fried, Marc. 1963. Grieving for a Lost Home. In The Urban Condition: People and Pol-icy in the Metropolis, ed. Leonard J. Duhl, 151–71. New York: Simon & Schuster.
Fullilove, Mindy Thompson. 2003. Neighborhoods and Infectious Diseases. In Neigh-borhoods and Health, ed. Ichiro Kawachi and Lisa F. Berkman, 211–22. New York:Oxford University Press.
Gabriel, Stuart A. 1996. The Role of FHA in the Provision of Credit to Minorities. InMortgage Lending, Racial Discrimination, and Federal Policy, ed. John Goering andRon Wienk, 183–250. Washington, DC: Urban Institute Press.
Gee, Gilbert C. 2002. A Multilevel Analysis of the Relationship between Institutionaland Individual Racial Discrimination and Health Status. American Journal of PublicHealth 92(4):615–23.
Geronimus, Arline T. 2000. To Mitigate, Resist, or Undo: Addressing Structural Influ-ences on the Health of Urban Populations. American Journal of Public Health90(6):867–72.
Goering, John. 2003. The Impacts of New Neighborhoods on Poor Families: Evaluatingthe Policy Implications of the Moving to Opportunity Demonstration. FRBNY Eco-nomic Policy Review, June, pp. 113–40.
Goering, John, Judith D. Feins, and Todd M. Richardson. 2002. A Cross-Site Analysis ofInitial Moving to Opportunity Demonstration Results. Journal of Housing Research13(1):1–30.
Goering, John, Joan Kraft, Judith Feins, Debra McInnis, Mary Joel Holin, and HudaElhassan. 1999. Moving to Opportunity for Fair Housing Demonstration Program: Cur-rent Status and Initial Findings. Washington, DC: U.S. Department of Housing andUrban Development.
Greenland, Sander. 2000. An Introduction to Instrumental Variables for Epidemiolo-gists. International Journal of Epidemiology 29(4):722–29.
Hanratty, Maria H., Sara A. McLanahan, and Becky Pettit. 2003. Los Angeles SiteFindings. In Choosing a Better Life? Evaluating the Moving to Opportunity SocialExperiment, ed. John Goering and Judith D. Feins, 245–74. Washington, DC: UrbanInstitute Press.
Harrell, Jules P., Sadiki Hall, and James Taliaferro. 2003. Physiological Responses toRacism and Discrimination: An Assessment of the Evidence. American Journal of Pub-lic Health 93(2):243–48.
Hart, Kevin D., Stephen J. Kunitz, Ralph R. Sell, and Dana B. Mukamel. 1998. Metro-politan Governance, Residential Segregation, and Mortality among African Americans.American Journal of Public Health 88(3):434–38.
Hattersley, Lin. 1999. Trends in Life Expectancy by Social Class—An Update. HealthStatistics Quarterly 2:16–24.
Fannie Mae Foundation
92 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 93
Haurin, Donald R., Toby L. Parcel, and R. Jean Haurin. 2002. Impact of Homeowner-ship on Child Outcomes. In Low-Income Homeownership: Examining the UnexaminedGoal, ed. Nicolas P. Retsinas and Eric S. Belsky, 427–46. Washington, DC: Joint Centerfor Housing Studies, Harvard University, and Brookings Institution Press.
Heymann, S. Jody, and Alison Earle. 1999. The Impact of Welfare Reform on Parents’Ability to Care for Their Children’s Health. American Journal of Public Health89(4):502–05.
Iannotta, Joah G., Jane L. Ross, and the National Research Council. 2002. Equality ofOpportunity and the Importance of Place: Summary of a Workshop. Washington, DC:National Academy Press.
Jackson, James S., Tony N. Brown, David R. Williams, Myriam Torres, Sherrill L. Sell-ers, and Kendrick Brown. 1996. Racism and the Physical and Mental Health Status ofAfrican Americans: A Thirteen-Year National Panel Study. Ethnicity & Disease6(1–2):132–47.
Joint Center for Housing Studies. 2003. The State of the Nation’s Housing: 2003. Cam-bridge, MA: Harvard University.
Kaplan, George A., and Jukka T. Salonen. 1990. Socioeconomic Conditions in Childhoodand Ischaemic Heart Disease during Middle Age. British Medical Journal 301:1121–23.
Katz, Bruce J., and Margery Austin Turner. 2001. Who Should Run the HousingVoucher Program? A Reform Proposal. Housing Policy Debate 12(2):239–62.
Katz, Lawrence F., Jeffrey R. Kling, and Jeffrey B. Liebman. 2001. Moving to Opportu-nity in Boston: Early Results of a Randomized Mobility Experiment. Quarterly Journalof Economics 116(2):607–54.
Kawachi, Ichiro, and Lisa F. Berkman. 2003a. Introduction. In Neighborhoods andHealth, ed. Ichiro Kawachi and Lisa F. Berkman, 1–19. New York: Oxford UniversityPress.
Kawachi, Ichiro, and Lisa F. Berkman, eds. 2003b. Neighborhoods and Health. NewYork: Oxford University Press.
Kearns, Ade, Rosemary Hiscock, Anne Ellaway, and Sally Macintyre. 2000. “BeyondFour Walls”: The Psychosocial Benefits of Home. Evidence from West Central Scotland.Housing Studies 15(3):387–410.
Kennedy, Stephen D., and Mireille L. Leger. 1990. Final Comprehensive Report of theFreestanding Housing Voucher Demonstration. Washington, DC: U.S. Department ofHousing and Urban Development.
Kiecolt-Glaser, Janice K., Lynanne McGuire, Theodore F. Robles, and Ronald Glaser.2002. Emotions, Morbidity, and Mortality: New Perspectives from Psychoneuroim-munology. Annual Review of Psychology 53:83–107.
Kling, Jeffrey R., Jeffrey B. Liebman, and Lawrence F. Katz. 2001. Bullets Don’t GotNo Name: Consequences of Fear in the Ghetto. Working Paper 225. Joint Center forPoverty Research.
Housing Policy Debate

Krieger, James, and Donna L. Higgins. 2002. Housing and Health: Time Again for Pub-lic Health Action. American Journal of Public Health 92(5):758–68.
Krieger, Nancy, and Steve Sidney. 1996. Racial Discrimination and Blood Pressure: TheCARDIA Study of Young Black and White Adults. American Journal of Public Health86(10):1370–78.
Kuh, Diana, Rebecca Hardy, Claudia Langenberg, Marcus Richards, and Michael E. J.Wadsworth. 2002. Mortality in Adults Aged 26–54 Years Related to Socioeconomic Con-ditions in Childhood and Adulthood: Post War Birth Cohort Study. British MedicalJournal 325(7372):1076–80.
Leventhal, Tama, and Jeanne Brooks-Gunn. 2000. The Neighborhoods They Live In:The Effects of Neighborhood Residence on Child and Adolescent Outcomes. Psychologi-cal Bulletin 126(2):309–37.
Leventhal, Tama, and Jeanne Brooks-Gunn. 2003a. The Early Impacts of Moving toOpportunity on Children and Youth in New York City. In Choosing a Better Life: Evalu-ating the Moving to Opportunity Social Experiment, ed. John Goering and Judith Feins,213–44. Washington, DC: Urban Institute Press.
Leventhal, Tama, and Jeanne Brooks-Gunn. 2003b. Moving to Opportunity: An Experi-mental Study of Neighborhood Effects on Mental Health. American Journal of PublicHealth 93(9):1576–82.
Lewis Mumford Center for Comparative Urban and Regional Research. 2001. 2000Census Data: Whole Population Public Use Data. State University of New York–Albany.World Wide Web page <http://mumford1.dyndns.org/cen2000/WholePop/WPSegdata/1120msa.htm> (accessed February 19, 2003).
Librett, John J., Michelle M. Yore, and Thomas L. Schmid. 2003. Local OrdinancesThat Promote Physical Activity: A Survey of Municipal Policies. American Journal ofPublic Health 93(9):1399–1403.
Loucks, Eric. 2003. Biological Markers in Housing–Health Research. Presented at theHarvard School of Public Health Symposium on Housing, Neighborhoods, and Health:State of the Evidence, Boston. June 26.
Loucks, Eric B., Jerry M. Spiegel, Carlos Barcelo, Annalee Yassi, Alfredo Aldama, andJames R. Dunn. 2002. Using Biomarkers for Measurement of the Health Effects ofHousing Conditions: Practical Guidelines. Presented at the 5th Pan American HealthOrganization Inter-American Health and Housing Conference, Havana, Cuba. May.
Lundberg, Olle. 1993. The Impact of Childhood Living Conditions on Illness and Mor-tality in Adulthood. Social Science and Medicine 36:1047–52.
Macintyre, Sally, and Anne Ellaway. 2000. Ecological Approaches: Rediscovering theRole of the Physical and Social Environment. In Social Epidemiology, ed. Lisa F. Berk-man and Ichiro Kawachi, 332–48. New York: Oxford University Press.
Macintyre, Sally, and Anne Ellaway. 2003. Neighborhoods and Health: An Overview. InNeighborhoods and Health, ed. Ichiro Kawachi and Lisa F. Berkman, 20–42. New York:Oxford University Press.
Fannie Mae Foundation
94 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 95
Marmot, Michael G., George Davey Smith, Stephen Stansfeld, Chandra Patel, FionaNorth, Jenny Head, Ian White, Eric Brunner, and Amanda Feeney. 1991. HealthInequalities among British Civil Servants—The Whitehall-II Study. Lancet337(8754):1387–93.
Marsh, Alex, David Gordon, Pauline Heslop, and Christina Pantazis. 2000. HousingDeprivation and Health: A Longitudinal Analysis. Housing Studies 15(3):411–42.
Meyers, Alan, Deborah Frank, Nicole Roos, Karen E. Peterson, Virginia A. Casey, L.Adrienne Cupples, and Suzette M. Levenson. 1995. Housing Subsidies and PediatricUndernutrition. Archives of Pediatrics and Adolescent Medicine 149(10):1079–84.
Mood, Eric W. 1986. Housing and Health: APHA–CDC Recommended Minimum Hous-ing Standards. Washington, DC: American Public Health Association.
Morland, Kimberly, Steve Wing, Ana Diez-Roux, and Charles Poole. 2002. Neighbor-hood Characteristics Associated with the Location of Food Stores and Food ServicePlaces. American Journal of Preventive Medicine 22(1):23–29.
Nettleton, Sarah, and Roger Burrows. 1998. Mortgage Debt, Insecure Homeownership,and Health: An Exploratory Analysis. Sociology of Health and Illness 20(5):731–53.
Newman, Sandra J., and Ann B. Schnare. 1997. “...And a Suitable Living Environ-ment”: The Failure of Housing Programs to Deliver on Neighborhood Quality. HousingPolicy Debate 8(4):703–41.
Oakes, J. Michael. 2004. The (Mis)Estimation of Neighborhood Effects: Causal Infer-ence for a Practicable Social Epidemiology. Social Science and Medicine58(10):1929–52.
O’Campo, Patricia. 2003. Advancing Theory and Methods for Multilevel Models of Resi-dential Neighborhoods and Health. American Journal of Epidemiology 157(1):9–13.
O’Campo, Patricia, Andrea C. Gielen, Ruth R. Faden, Xiaonan Xue, Nancy Kass, andMei-Cheng Wang. 1995. Violence by Male Partners against Women during the Child-bearing Years: A Contextual Analysis. American Journal of Public Health 85(8, part1):1092–97.
Orr, Larry L. 1999. Social Experiments: Evaluating Public Programs with ExperimentalMethods. Thousand Oaks, CA: Sage.
Orr, Larry, Judith D. Feins, Robin Jacob, Erik Beecroft, Lisa Sanbonmatsu, Lawrence F.Katz, Jeffrey B. Liebman, and Jeffrey R. Kling. 2003. Moving to Opportunity for FairHousing Demonstration Program. Interim Impacts Evaluation. Washington, DC: U.S.Department of Housing and Urban Development.
Peroff, Kathleen A., Cloteal L. Davis, Ronald Jones, and U.S. Department of Housingand Urban Development, Office of Policy Development and Research. 1979. GautreauxHousing Demonstration: An Evaluation of Its Impact on Participating Households.Washington, DC: U.S. General Accounting Office.
Peterson, George E., and Kale Williams. 1995. Housing Mobility: What Has It Accom-plished and What Is Its Promise? In Housing Mobility: Promise or Illusion? ed. Alexan-der Polikoff, 7–101. Washington, DC: Urban Institute.
Housing Policy Debate

Pettit, Kathryn L. S., G. Thomas Kingsley, Claudia J. Coulton, and Jessica Cigna. 2003.Neighborhoods and Health: Building Evidence for Local Policy. Washington, DC: UrbanInstitute.
Popkin, Susan J., Laura E. Harris, and Mary K. Cunningham. 2002. Families in Tran-sition: A Qualitative Analysis of the MTO Experience. Prepared for the U.S. Depart-ment of Housing and Urban Development, Office of Policy Development and Research,under a subcontract with Abt Associates, Inc. Washington, DC: Urban Institute.
Power, Chris, Clyde Hertzman, Sharon Matthews, and Orly Manor. 1997. Social Differ-ences in Health: Life Cycle Effects between Ages 23 and 33 in the 1958 British BirthCohort. American Journal of Public Health 87:1499–503.
Preston, Samuel H., and Michael R. Haines. 1991. Fatal Years: Child Mortality in LateNineteenth-Century America. Princeton, NJ: Princeton University Press.
Robert, Stephanie, and James S. House. 1996. SES Differentials in Health by Age andAlternative Indicators of SES. Journal of Aging and Health 8(3):359–88.
Rosenbaum, Emily, and Laura E. Harris. 2001. Low-Income Families in Their NewNeighborhoods: The Short-Term Effects of Moving from Chicago’s Public Housing.Journal of Family Issues 22(3):183–210.
Rosenbaum, James E. 1994. Housing Mobility Strategies for Changing the Geographyof Opportunity. Working paper. Northwestern University, Institute for Policy Research.
Rosenbaum, James E. 1995. Changing the Geography of Opportunity by ExpandingResidential Choice: Lessons from the Gautreaux Program. Housing Policy Debate6(1):231–69.
Rosenbaum, James E., and Susan J. Popkin. 1990. Economic and Social Impacts ofHousing Integration. Evanston, IL: Northwestern University, Center for Urban Affairsand Policy Research.
Saegert, Susan C., Susan Klitzman, Nicholas Freudenberg, Jana Cooperman-Mroczek,and Salwa Nassar. 2003. Healthy Housing: A Structured Review of Published Evalua-tions of U.S. Interventions to Improve Health by Modifying Housing in the UnitedStates, 1990–2001. American Journal of Public Health 93(9):1471–77.
Saelens, Brian E., James F. Sallis, Jennifer B. Black, and Diana Chen. 2003. Neighbor-hood-Based Differences in Physical Activity: An Environment Scale Evaluation. Ameri-can Journal of Public Health 93(9):1552–58.
Sard, Barbara. 2000. Housing Vouchers Should Be a Major Component of Future Hous-ing Policy for the Lowest-Income Families. Housing Policy in the New Millennium: Pro-ceedings, ed. Susan M. Wachter and R. Leo Penne, 291–318. Washington, DC: U.S.Department of Housing and Urban Development. World Wide Web page <http://www.huduser.org/publications/polleg/hpcproceedings.html> (accessed February 17, 2003).
Shroder, Mark. 2000. Social Experiments in Housing. Cityscape: A Journal of PolicyDevelopment and Research 5(1):237–59.
Shroder, Mark. 2002. Locational Constraint, Housing Counseling, and Successful Lease-Up in a Randomized Housing Voucher Experiment. Journal of Urban Economics51(2):315–38.
Fannie Mae Foundation
96 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman

Does Housing Mobility Policy Improve Health? 97
Srinivasan, Shobha, Liam R. O’Fallon, and Allen Dearry. 2003. Creating Healthy Com-munities, Healthy Homes, Healthy People: Initiating a Research Agenda on the BuiltEnvironment and Public Health. American Journal of Public Health 93(9):1446–50.
Subramanian, S. V., Kelvyn Jones, and Craig Duncan. 2003. Multilevel Methods forPublic Health Research. In Neighborhoods and Health, ed. Ichiro Kawachi and Lisa F.Berkman, 65–111. New York: Oxford University Press.
Syme, S. Leonard. 1987. Social Determinants of Disease. Annals of Clinical Research19(2):44–52.
Syme, S. Leonard, and Lisa F. Berkman. 1976. Social Class, Susceptibility, and Sickness.American Journal of Epidemiology 104(1):1–8.
Thiele, Bret. 2002. The Human Right to Adequate Housing: A Tool for Promoting andProtecting Individual and Community Health. American Journal of Public Health92(5):712–15.
Thomson, Hilary, Mark Petticrew, and David Morrison. 2001. Health Effects of HousingImprovement: Systematic Review of Intervention Studies. British Medical Journal323(7306):187–90.
Turner, Margery Austin. 1998. Moving Out of Poverty: Expanding Mobility and Choicethrough Tenant-Based Housing Assistance. Housing Policy Debate 9(2):373–94.
Turner, Margery Austin, Susan Popkin, and Mary Cunningham. 2000. Section 8 Mobil-ity and Neighborhood Health: Emerging Issues and Policy Challenges. Washington, DC:Urban Institute.
U.S. Bureau of the Census and Economics and Statistics Administration. 2001. NetWorth of Nation’s Households Unchanged, Census Bureau Reports. Press release. WorldWide Web page <http://www.census.gov/Press-Release/www/2001/cb01-33.html>(accessed May 2002).
U.S. Department of Housing and Urban Development. 1995. Homeownership and ItsBenefits. Urban Policy Brief. Washington, DC.
U.S. Department of Housing and Urban Development. 2002. Fiscal Year 2003 BudgetSummary. Washington, DC.
U.S. Department of Housing and Urban Development, Office of Policy Developmentand Research. 2000. Rental Housing Assistance—The Worsening Crisis. A Report toCongress on Worst-Case Housing Needs. Washington, DC.
Wachter, Susan M. 2000. Introduction. Housing Policy in the New Millennium: Proceed-ings, ed. Susan M. Wachter and R. Leo Penne, 1–12. Washington, DC: U.S. Departmentof Housing and Urban Development. World Wide Web page <http://www.huduser.org/publications/polleg/hpcproceedings.html> (accessed February 17, 2003).
Wadsworth, Michael E. J., Scott M. Montgomery, and Mel J. Bartley. 1999. The Persist-ing Effect of Unemployment on Health and Social Well-Being in Men Early in WorkingLife. Social Science and Medicine 48(10):1491–99.
Housing Policy Debate

Whitehead, Christine. 2000. Editorial. Housing Studies 15(3):339–40.
Williams, David R. 1996. Racism and Health: A Research Agenda. Ethnicity & Disease6(1–2):1–8.
Williams, David R. 1997. Race and Health: Basic Questions, Emerging Directions.Annals of Epidemiology 7:322–33.
Williams, David R. 2001. Racial Variations in Adult Health Status: Patterns, Paradoxes,and Prospects. In America Becoming: Racial Trends and Their Consequences. Vol. II,ed. Neil J. Smelser, William Julius Wilson, Faith Mitchell, and the National ResearchCouncil. Washington, DC: National Academy Press.
Williams, David R., and Chiquita Collins. 2001. Racial Residential Segregation: A Fun-damental Cause of Racial Disparities in Health. Public Health Reports 116(5):404–16.
Williams, David R., and Michelle Harris-Reid. 1999. Race and Mental Health: EmergingPatterns and Promising Approaches. In A Handbook for the Study of Mental Health:Social Context, Theories, and Systems, ed. Allan V. Horwitz and Teresa L. Scheid,295–314. Cambridge, England: Cambridge University Press.
Williams, David R., and Harold Neighbors. 2001. Racism, Discrimination, and Hyper-tension: Evidence and Needed Research. Ethnicity & Disease 11(4):800–16.
Williams, David R., Harold W. Neighbors, and James S. Jackson. 2003. Racial/EthnicDiscrimination and Health: Findings from Community Studies. American Journal ofPublic Health 93(2):200–08.
Williams, David R., Yan Yu, James S. Jackson, and Norman B. Anderson. 1997. RacialDifferences in Physical and Mental Health: Socioeconomic Status, Stress, and Discrimi-nation. Journal of Health Psychology 2(3):335–51.
Yinger, John. 1995. Closed Doors, Opportunities Lost: The Continuing Costs of HousingDiscrimination. New York: Russell Sage Foundation.
Fannie Mae Foundation
98 D. Acevedo-Garcia, T. Osypuk, R. Werbel, E. Meara, D. Cutler, and L. Berkman