
Diet and dental caries edited
33
Welcome To All
-
Upload
raja-sekhar -
Category
Health & Medicine
-
view
74 -
download
1
Transcript of Diet and dental caries edited

Welcome To All
B. Sukanya
By
Presented
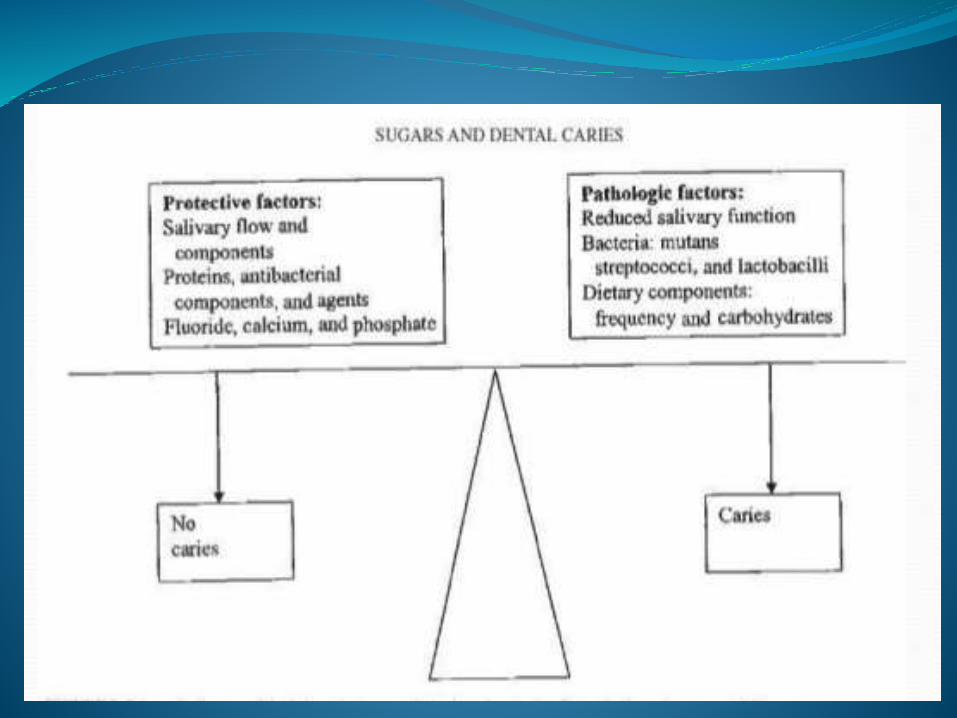
A dynamic relation exists between sugars and oral health. Diet affects the integrity of the teeth; quantity, pH, and composition of the saliva; and plaque pH. Sugars and other fermentable carbohydrates, after being hydrolyzed by salivary amylase, provide substrate for the actions of oral bacteria, which in turn lower plaque and salivary pH. The resultant action is the beginning of tooth demineralization.
The deciduous teeth erupt from 6 months and are lost by the
early teens. The permanent dentition replaces the deciduous
dentition from the age of 6 years and is complete by age 21.
Teeth are most susceptible to dental caries soon after they erupt;
therefore, the peak ages for dental caries are 2–5 years for the
deciduous dentition and early adolescence for the permanent
dentition. In developed countries, there is a trend for older adults
now to retain their teeth for longer, however, if the gums recede
with age the roots of the teeth become exposed, and, being
relatively less mineralized than the tooth crowns, are susceptible
to decay known as ‘root caries’
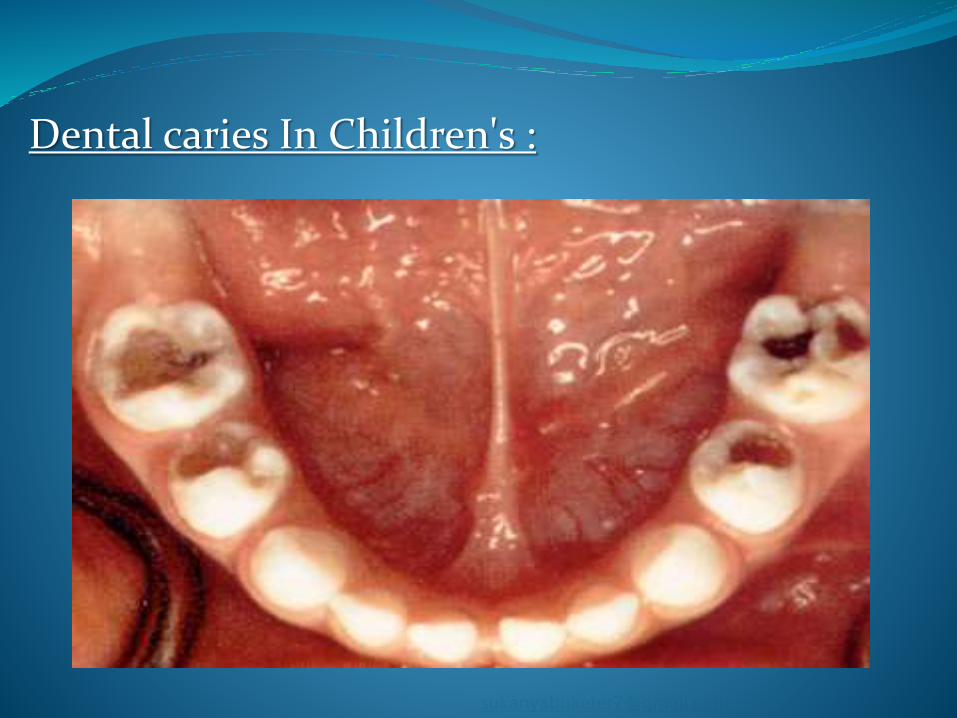
Dental caries In Children's :
The patient's diet and dental caries activity are related. From the
dietic viewpoint, dental caries is widely accepted as being
caused by the injestion of fermentable carbohydrates,
particularly Sucrose, fermentable carbohydrates and more
specifically sucrose are rarely eaten as such. They are eaten as
components of foods that contain other ingredients and have
different textures. the cariogenic potential of foods containing
sucrose depends on many variables such as the ability to
1. Be Retained by teeth
2. Form acids
3. Dissolve enamel
4. Neutralize or buffer acids.
Certain characteristics of sucrose-containing foods or conditions
surroundings their consumption are more important in terms of cariogenicity
than the amount of sugar they contain. Thus, Solid and retentive sucrose-
containing foods are more cariogenic than sugar-containing foods that are
liquid and non-retentive the frequency and the time of ingestion of foods are
also important. the sucrose-containing food becomes more dangerous if it is
eaten more frequently. food eaten at meals produces less caries than the same
eaten in between meals.
In decreasing order of cariogenicity, the food are grouped as:
-- Adherent, Sucrose-containing foods eaten frequently between meals.
-- Adherent, Sucrose-containing foods eaten during meals.
-- Non-retentive (liquid) Sucrose-containing beverages consumed frequently
between meals.
-- Non-retentive (liquid) Sucrose-containing foods consumed during meals.
1. the form of food or fluid
2. the duration of exposure
3. nutrient composition
4. sequence of eating
5. salivary flow
6. presence of buffers
7. and oral hygiene.
Dental caries was first described in Miller’s chemo parasitic theory in 1890. Caries is caused by the dissolution of the teeth by acid produced by the metabolism of dietary carbohydrates by oral bacteria. The 2 primary bacteria involved in caries formation are mutans streptococci and lactobacilli. In the 1960s the caries theory was depicted as 3 circles representing the3 prerequisites for dental caries: the tooth, the diet, and dental plaque
Mechanisms proposed to explain the anticariogenic effects of cheeses are as follows:
1-increased salivary flow and the
Subsequent buffering effect,
which can neutralize plaque acids
2-inhibition of plaque bacteria and the effect of that inhibition on reducing the amount of bacteria, thereby reducing acid production; and
3-intake of increased alkaline substances, calcium, inorganic phosphate, and casein, which decrease demineralization and enhance demineralization
When we say “sugar”, we usually mean granulated Table sugar. However there are so many kinds of sugars these days, we need to be very clear the word “sugar” includes these things ending in “ose”:
1. Sucrose (Table sugar) a simple sugar made from cane sugar or beets.
2. Fructose, a simple sugar in fruits, plants and honey.
3. Maltose, a complex sugar in barley and malt syrups.
4. Lactose, a complex sugar in milk.
5. Dextrose, a refined simple sugar from corn, sugar cane or beets.
6. Glucose, a simple sugar in fruits, vegetables and grains.

The recommended intake of non-milk extrinsic sugars is a maximum of 60g/day, which is about 10% of daily energy intake.
1. reduces and inhibits demineralization.
2. Re-mineralization of enamel .
3. affects plaque :by inhibiting bacterial metabolism of sugar thus reducing acid production.
1. types of carbohydrate
2. physical form of food retention and oral clearance time
3. factor in the diet that protect against dental caries
4. intake frequency
5. nature of diet

CLASSIFICATION OF SUGARS FOR DENTAL HEALTH PURPOSES
Forms of sugars and starch in the diet
1. Sugars are a form of fermentable carbohydrate. Fermentable carbohydrates are carbohydrates (sugar sand starch) that begin digestion in the oral cavity via salivary amylase. Sugars enter the
2. diet in 2 forms: those found naturally in foods (e.g.,fruit, honey, and dairy products) and those that are added to foods during processing to alter the flavour, taste, or texture of the food
Prolonged oral retention of cariogenic components of food may lead to extended periods of acid production and demineralization and to shortened periods of re-mineralization. Retentiveness of foods is not the same as stickiness. A caramel or jellybean may be sticky, but its retentive properties are fairly low and they are cleared from the oral cavity faster than are retentive foods such as cookies or chips .
1. metabolism by microorganisms
2. adsorption onto oral surfaces
3. degradation by plaque and salivary enzymes
4. saliva flow, and
5. swallowing. Most carbohydrates will be cleared by these simultaneous mechanisms.
The frequency of consumption seems to be a significant contributor to the cariogenicity of the diet, although Bowen et al (10) concluded that it is not the frequency of ingestion per sec that is related to the development of caries but the time that sugars are available to microorganisms in the mouth caries is regarded as the outcome of the alternation of demineralization and re-mineralization. Higher frequency means more demineralization and less re-mineralization. The duration of the decrease in pH after intake of a cariogenic food is an importan tconfounder in this relation
Polyphenols
Polyphenols such as tannins in cocoa, coffee, tea, and many fruit juices may reduce the cariogenic potential of foods. In vitro experiments have shown that these polyphenolic compounds may interfere with glucosyltransferase activity of mutans streptococci, which may reduce plaq.ue formation. In rat experiments, tea polyphenols .
Sugar alcohol–based products Sugar-free gums can stimulate saliva, increasing the clearance of sugars and other fermentable carbohydrates from the teeth and the oral cavity and increasing buffer capacity. Tooth-friendly polyols include sorbitol, xylitol, mannitol, erythritol, and isomalt. However, xylitol carbon sugar that oral microflora cannot metabolize—has additional anti cariogenic effect sattributable to antimicrobial action, stimulation of saliva resulting in increased buffer activity and an increase in pH, and enhanced re-mineralization .Sorbitol-sweetened gums simulate saliva without causing a drop to the critical pH and have been shown to be equal to xylitol gum in terms of caries control
Tooth erosion is the progressive loss of dental hard tissue by acids in a process that does not involve bacteria or sugars. The intrinsic acids are from vomiting, gastroesophageal reflux, and regurgitation. Thee xtrinsic acids are from the diet [e.g. sports beverages and citrus products, including citrus fruit, juices, soft drinks, and citrus-flavored candies and lozenges]or from the occupational environment (e.g.,battery and galvanizing factories). Tooth erosion as a result of eating disorders (bulimia nervosa) and dietary practices involving frequent intake of acidic foods and beverages can weaken tooth integrity.
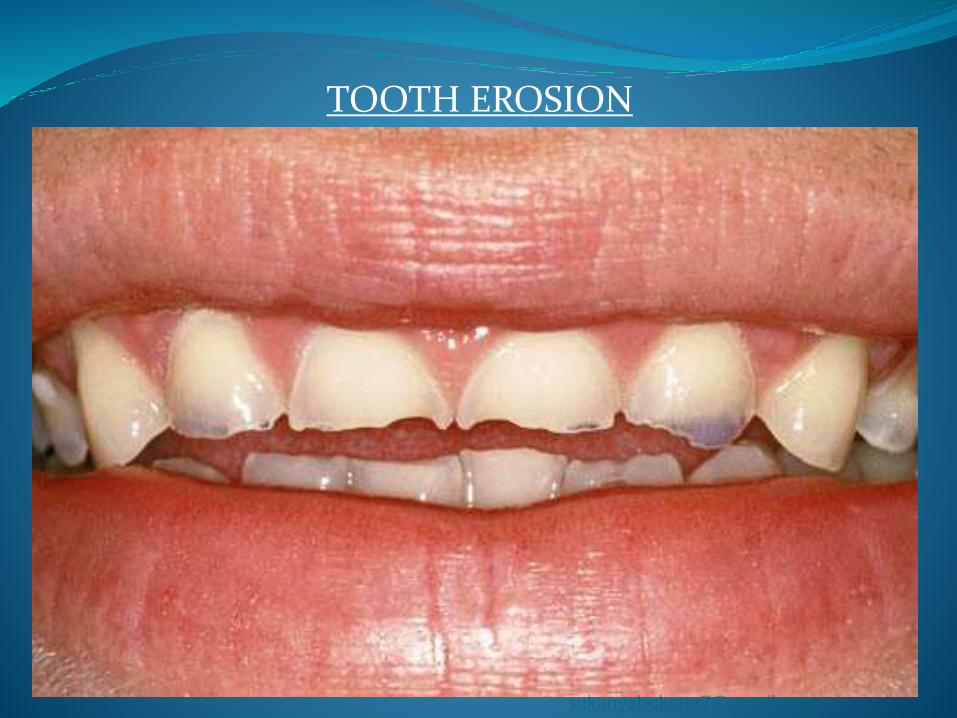
TOOTH EROSION
1. Infants and toddlers with prolonged breast-feeding on demand Infants and toddlers provided with a feeding bottle at bed time, or bottle suspended in the cot for use during the night, with sugar containing liquid
2. People with increased frequency of eating because of a medical problem, e.g., gastrointestinal disease, eating disorders, uncontrolled diabetes.
3. Those with an increased carbohydrate intake due to a medical problem e.g., Crohn’s disease, chronic renal failure, or other chronic illness, malnutrition or failure to thrive.
4. Those with reduced salivary secretion. Sjogren’s syndrome, irradiation in the region of the salivary glands.
5. Athletes taking sugar-containing sport supplement drinks.
6. Workers subject to occupational hazards such as food sampling and those on a monotonous job such as a nightshift.
7. Drug abusers who have a craving for sugar and a prolonged clearance rate as a result of reduced salivary secretion.
8. People of any age, on long term and/or multiple medications. Are these sugar-based and/or do they cause a dry mouth?
9. Any sugary bedtime snacks or drinks.
1. eat a balanced diet rich in whole grains, fruit, and vegetables and practice good oral hygiene—particularly the use of fluoridated toothpastes—to maximize oral and systemic health and reduce caries risk.
2. eat a combination of foods to reduce the risk of caries and erosion; include dairy products with fermentable carbohydrates and other sugars and consume these food swith, instead of, between meals; add raw fruit or vegetables to meals to increase salivary flow; drink sweetened and acidic beverages with meals, including foods that can buffer the acid ogenic effects
4. chew sugarless gum between meals and snacks to increase salivary flow.
5. rinse mouth with water, chew sugarless gum (particularly those containing sugar alcohols, which stimulates re-mineralization), and eat dairy product such as cheese after the consumption of fermentable carbohydrates.
6. drink, rather than sip, sweetened and acidic beverages.
7. moderate eating frequency to reduce repeated exposure to sugars, other fermentable carbohydrates, and acids.
8. avoid putting an infant or child to bed with a bottle of milk, juice, or other sugar-containing beverage.
1. Bread (sandwiches, toast, crumpets, pitta bread).
2. Pasta, rice, starchy staple foods
3. Cheese
4. Fibrous foods (e.g. raw vegetables)
5. Low sugar breakfast cereals (e.g. shredded wheat)
6. Fresh fruit (whole and not juices)
7. Peanuts (not for children under 5 years)
8. Sugar-free chewing gum
9. Sugar-free confectionery
10. Water, Milk, Sugar-free drinks, Tea and coffee (unsweetened)
B. Sukanya
By
Query's Section
..with the strength and resources we have,
we must think how we would conquer them..but
not lose hope due to the lack of resources.
A Simple Quote,
Thank You..


















