Diagnosis and Management of Endometrial Polyps: A Critical ...
13
Review Article Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature S. Salim, H. Won, MBBS, MM, MRANZCOG, E. Nesbitt-Hawes, B Med, N. Campbell, MBChB, FRANZCOG, and J. Abbott*, B Med (Hons), MRCOG, FRANZCOG, PhD From the University of New South Wales (all authors), and Royal Hospital for Women (Drs. Won, Nesbitt-Hawes, and Abbott), Randwick, New South Wales, Australia. ABSTRACT This review article summarizes the salient literature on the diagnosis and management of endometrial polyps. Electronic re- sources including Medline, PubMed, CINAHL, The Cochrane Library (including the Cochrane Database of Systematic Reviews), Current Contents, and EMBASE were searched with the MeSH terms including all subheadings and keywords endometrial polyps, abnormal uterine bleeding, polypectomy , polyp management, polyp and diagnosis, and polyp and malignancy . There is a paucity of level I evidence in the literature on the diagnosis and management of this common gynecologic disease. Nonin- vasive investigations such as transvaginal ultrasonography, with or without the use of 3-dimensional ultrasonography and contrast techniques remain the mainstay of first-line investigation. Hysteroscopic resection is the most effective management for endo- metrial polyps and allows histologic assessment, whereas blind biopsy or curettage has low diagnostic accuracy and should not be performed. This article will review the cause, epidemiology, clinical presentation, diagnostic investigations, and manage- ment of endometrial polyps. Journal of Minimally Invasive Gynecology (2011) 18, 569–581 Crown Copyright Ó 2011 Published by Elsevier Inc. on behalf of AAGL. All rights reserved. Keywords: Endometrial polyps; Abnormal uterine bleeding; Polypectomy; Hysteroscopic polypectomy; Infertility; Malignancy DISCUSS You can discuss this article with its authors and with other AAGL members at http://www.AAGL.org/jmig-18-5-1700 Use your Smartphone to scan this QR code and connect to the discussion forum for this article now* * Download a free QR Code scanner by searching for ‘‘QR scanner’’ in your smartphone’s app store or app marketplace. Endometrial polyps are a common gynecologic condition that are associated with clinical symptoms such as abnormal vaginal bleeding and infertility, as well as premalignant and malignant conditions. They may be found through specific investigation or as an incidental finding on imaging for another reason. This review will critically appraise the liter- ature regarding diagnosis and management of endometrial polyps and will review cause and epidemiology. Methods This review was produced by searching electronic resources including Medline (1950–2010), EMBASE (1980–2010), PubMed, CINAHL, The Cochrane Library (including the Cochrane Database of Systematic Reviews), Current Contents, as well as manual searching of bibliogra- phies of known primary research and review articles. These were searched with the MeSH terms including all subhead- ings and keywords endometrial polyps, abnormal uterine bleeding, polypectomy , polyp management, polyp and diagnosis and polyp and malignancy , as well as nonspecific keywords such as uterine diseases, polyps, and intrauterine were used to include a broad range of clinical studies and relevant publications. A total of 330 articles were identified, with 265 provision- ally included manuscripts retrieved, reviewed, and abstracted by team members, and with review and discussion of content The authors have no commercial, proprietary, or financial interest in the products or companies described in this article. Corresponding author: Jason Abbott, B Med(Hons), MRCOG, FRANZCOG, PhD, Royal Hospital for Women, University of New South Wales, Barker St, Randwick, New South Wales 2031, Australia. E-mail: [email protected] Submitted March 22, 2011. Accepted for publication May 26, 2011. Available at www.sciencedirect.com and www.jmig.org 1553-4650/$ - see front matter Crown Copyright Ó 2011 Published by Elsevier Inc. on behalf of AAGL. All rights reserved. doi:10.1016/j.jmig.2011.05.018
Transcript of Diagnosis and Management of Endometrial Polyps: A Critical ...
Review Article
Diagnosis and Management of Endometrial Polyps: A CriticalReview of the Literature
S. Salim, H. Won, MBBS, MM,MRANZCOG, E. Nesbitt-Hawes, BMed, N. Campbell, MBChB,FRANZCOG, and J. Abbott*, B Med (Hons), MRCOG, FRANZCOG, PhDFrom the University of New South Wales (all authors), and Royal Hospital for Women (Drs. Won, Nesbitt-Hawes, and Abbott), Randwick,
New South Wales, Australia.
ABSTRACT This review article summarizes the salient literature on the diagnosis and management of endometrial polyps. Electronic re-
The authors have
products or comp
Corresponding au
PhD, Royal Hosp
Randwick, New S
E-mail: j.abbott@
Submitted March
Available at www
1553-4650/$ - se
doi:10.1016/j.jmi
sources includingMedline, PubMed, CINAHL, The Cochrane Library (including the Cochrane Database of Systematic Reviews),Current Contents, and EMBASE were searched with the MeSH terms including all subheadings and keywords endometrialpolyps, abnormal uterine bleeding, polypectomy, polyp management, polyp and diagnosis, and polyp and malignancy. Thereis a paucity of level I evidence in the literature on the diagnosis and management of this common gynecologic disease. Nonin-vasive investigations such as transvaginal ultrasonography, with or without the use of 3-dimensional ultrasonography and contrasttechniques remain the mainstay of first-line investigation. Hysteroscopic resection is the most effective management for endo-metrial polyps and allows histologic assessment, whereas blind biopsy or curettage has low diagnostic accuracy and shouldnot be performed. This article will review the cause, epidemiology, clinical presentation, diagnostic investigations, and manage-ment of endometrial polyps. Journal of Minimally Invasive Gynecology (2011) 18, 569–581 Crown Copyright� 2011 Publishedby Elsevier Inc. on behalf of AAGL. All rights reserved.
Keywords: Endometrial polyps; Abnormal uterine bleeding; Polypectomy; Hysteroscopic polypectomy; Infertility; Malignancy
DISCUSS
You can discuss this article with its authors and with other AAGL members athttp://www.AAGL.org/jmig-18-5-1700no commercial, proprietary, or financial interest in the
anies described in this article.
thor: JasonAbbott, BMed(Hons),MRCOG, FRANZCOG,
ital for Women, University of New SouthWales, Barker St,
outh Wales 2031, Australia.
unsw.edu.au
22, 2011. Accepted for publication May 26, 2011.
.sciencedirect.com and www.jmig.org
e front matter Crown Copyright � 2011 Published by Elsevier Inc. on behalf of AAGL. All rights
g.2011.05.018
Utoadth
reserved.
se your Smartphonescan this QR code
nd connect to theiscussion forum foris article now*
* Download a free QR Code scanner by searching for ‘‘QRscanner’’ in your smartphone’s app store or app marketplace.
Endometrial polyps are a common gynecologic conditionthat are associated with clinical symptoms such as abnormalvaginal bleeding and infertility, as well as premalignant andmalignant conditions. They may be found through specificinvestigation or as an incidental finding on imaging foranother reason. This review will critically appraise the liter-ature regarding diagnosis and management of endometrialpolyps and will review cause and epidemiology.
Methods
This review was produced by searching electronicresources including Medline (1950–2010), EMBASE(1980–2010), PubMed, CINAHL, The Cochrane Library(including the Cochrane Database of Systematic Reviews),Current Contents, as well as manual searching of bibliogra-phies of known primary research and review articles. Thesewere searched with the MeSH terms including all subhead-ings and keywords endometrial polyps, abnormal uterinebleeding, polypectomy, polyp management, polyp anddiagnosis and polyp and malignancy, as well as nonspecifickeywords such as uterine diseases, polyps, and intrauterinewere used to include a broad range of clinical studies andrelevant publications.
A total of 330 articles were identified, with 265 provision-ally included manuscripts retrieved, reviewed, and abstractedby teammembers, and with review and discussion of content
570 Journal of Minimally Invasive Gynecology, Vol 18, No 5, September/October 2011
and relevance to the review. Most were Canadian Task ForceClassification II uncontrolled case series, with a considerablysmaller number of Canadian Task Force Classification Irandomized controlled trials. Final decisions regarding inclu-sion or exclusion were made on the basis of the methodologicquality, which involved relevant features of population,intervention, and outcome.
Cause
Endometrial polyps are a localized endometrial intrauter-ine overgrowth that may be single or multiple, measuringfrom a few millimeters to centimeters, and may be sessileor pedunculated [1]. Endometrial polyps consist of endome-trial glands, stroma, and blood vessels [2], with most polypsarising from the fundal region and extending toward the in-ternal os. Occasionally they project through the external cer-vical os and can be seen in the vagina. Risk factors for thedevelopment of endometrial polyps include age, hyperten-sion, obesity, and tamoxifen use [3–5].
Microscopically, endometrial polyps are typically a mix-ture of dense fibrous tissue (stroma), large and thick walledvascular channels, and glandular spaces of varying shapesand size, covered by a surface epithelium. Recent workdescribes the parallel arrangement of the endometrial glandslong axis to the surface epithelium as a histologic feature ofendometrial polyps. This feature, found in 80% of premeno-pausal women, was significantly less common in postmeno-pausal women (42%) (p 5.001) and did not occur at allin any of the 56 normal control subjects, suggesting that,when present, this is an important additional histologicfeature for diagnosis [1].
The exact cause of polyps is unknown, and their hetero-geneity makes identification of a single causative factorunlikely. Genetic factors may be contributory to the develop-ment of endometrial polyps, with reports identifying clustersof anomalies in chromosomes 6 and 12, which may alter theproliferative process, resulting in endometrial overgrowthand polyp formation [6]. Women with various intrauterinediseases (polyps, leiomyomata, adenomyosis) demonstratealterations in endometrial levels of matrix metalloprotei-nases and cytokines compared with control subjects [7]. Itis not yet known whether these changes produce the patho-logic processes or are a result of their development. Thesesame biochemical mediators are implicated in the role ofintrauterine disease causing fertility impairment. The pre-ponderance of polyps in the postmenopausal group maybe partly explained by an increase in a proliferation-regulating protein, p63, in this group. This protein is alsoa marker of reserve cells of the basalis layer, from whichpolyps are believed to arise [8].
Estrogen and progesterone regulate the balance of prolif-eration and apoptosis in normal endometrium, althoughconflict exists over the roles of hormonal receptors in thepathophysiology of endometrial polyps. It appears that bothestrogen and progesterone contribute to the elongation of en-
dometrial glands, stromal tissues, and spiral arteries that givethe characteristic polypoid appearance to these growths [9].In postmenopausal women, estrogen receptors are moreprevalent in polyps than in normal endometrium [10], withmore limited evidence showing progesterone receptors maycontribute to polyp development in some women [11].
There are conflicting reports of increased estrogen andprogesterone receptor concentration in the glandular epithe-lium of polyps but not in the stroma when compared withnormal endometrium [12] and other work showing no differ-ence in the concentration of receptors in any area [13]. It ispossible that the timing in the cycle may be contributory,with endometrial staining demonstrating that estrogenreceptors are more prevalent during the secretory than theproliferative phase [14]. Regardless of the hormonal recep-tor status, functional similarities between endometrialpolyps and normal endometrium occur, with polyps under-going similar cyclic surface changes to those seen in normalendometrium [15].
Epidemiology and Clinical Presentation
The reported prevalence of endometrial polyps varieswidely and ranges from 7.8% to 34.9%, depending on thedefinition of a polyp, diagnostic method used, and thepopulation studied [16–19]. The prevalence of polypsappears to increase with age, and it is reported that morepostmenopausal (11.8%) than premenopausal women (5.8%)are affected (p ,.01). The association with menopause maybe a selection bias, given that postmenopausal women withany vaginal bleeding are more likely to be investigated[17]. There are conflicting reports of menopause being animportant etiologic factor, and this is an area for future re-search [17,19–23]. The incidence of endometrial polyps isunknown with several prospective studies demonstratingendometrial polyps in symptom-free women [24–27].
For both premenopausal and postmenopausal womenwith an endometrial polyp, abnormal vaginal bleeding oc-curs in approximately 68% of cases and is the most commonpresenting symptom for women with this disease [28]. Over-all, 64% to 88% of premenopausal women with endometrialpolyps have symptoms [28], most commonly presentingwith menorrhagia, irregular menses, postcoital bleeding, orintermenstrual bleeding. Endometrial polyps account for39% of all abnormal vaginal bleeding in premenopausalwomen [29], with this bleeding believed to be due to stromalcongestion within the polyp leading to venous stasis andapical necrosis [9].
Although bleeding is a common presentation, womenwith a polyp may remain symptom free and present withthis incidental finding on imaging for other indications[30]. It is important to note that symptoms do not correlatewith polyp number, diameter, and site [31]. In the postmen-opausal period, 56% of women with an endometrial polyppresent with symptoms such as postmenopausal bleeding[28,31]. Polyps account for only 21% to 28% of all causes
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
Salim et al. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature 571
of postmenopausal bleeding [21,28,29]. The presence ofa polyp does not always cause symptoms, with a class IIstudy of 686 women aged 20 to 74 years reporting thatabnormal uterine bleeding is significantly less frequent(p 5.015) among women with polyps compared withthose without [17]. Such data indicate that most postmeno-pausal women with polyps are symptom free, and abnormalbleeding is not commonly associated with polyps in premen-opausal women.
In premenopausal women, endometrial polyps are associ-ated with infertility, although the causal relationship remainsuncertain [32]. Hypotheses include mechanical obstructionhindering ostium function and affecting sperm migration[33], or biochemical effects of polyps on implantation orembryo development. The latter reflects the finding of in-creased levels of metalloproteinases and cytokines such asinterferon-gamma found in polyps when compared with nor-mal uterine tissue [7]. Women treated with gonadotropinsfor infertility are exposed to a higher level of estrogen, whichpredisposes them to development of endometrial polyps[34]. The incidence of polyps occurring in infertile womenis widely variable, ranging between 3.8% to 38.5% of womenwith primary infertility, 1.8% to 17% of women with second-ary infertility, and 1.9% to 24% of infertile women whencombined [32,35–37]. The specific subpopulation and thediagnostic voracity are factors that may lead to this widevariation.
Women using tamoxifen are at specific risk fordevelopment of polyps, with class II studies reporting upto 30% to 60% prevalence in this particular group[22,38–40]. Premenopausal women using the combinedoral contraceptives may be at reduced risk for developmentof polyps, with a large population study showing theoverall prevalence of polyps in premenopausal women tobe 5.8%, whereas users of combined oral contraceptiveshad a prevalence of 2.1% [17]. Other risk factors that maypredispose to endometrial polyps include hypertension andobesity [22]. Increased levels of estrone is the likely mecha-nism in obese women, although the link with hypertensionmay be a confounder of obesity, rather than a direct correla-tion to the causation of polyps.
Cervical polyps are associated with endometrial polypsin 24% to 27% of cases [23,41,42]. The frequency ofthe association increases with the presence of abnormalbleeding and advancing age (p ,.001), with up to 56.8% ofpostmenopausal women presenting with vaginal bleedinghaving both diseases [42]. Women who have atypical glandu-lar cells demonstrated on Pap smear may be diagnosed withan endometrial polyp in 3.4% to 5% of cases [30,43].
Tendency to Malignancy
Most endometrial polyps are benign; however they maybecome hyperplastic, with malignant transformation devel-oping in 0% to 12.9% of polyps in case series reported todate [3,19,44–48]. A recent meta-analysis has reviewed
malignant risk in detail, and the reader is directed to thisfor further information, with important findings in this areaincluded here [49]. The most salient fact from this reviewis that the risk of malignancy found in endometrial polypsis highest in postmenopausal women with symptoms. Thereported incidence of carcinoma confined to endometrialpolyps varies between 0% to 4.8%, depending on thepopulation studied and the diagnostic methods used [16].Although the risk of malignancy is low in premenopausalwomen [50], it has been significantly correlated with in-creasing age and menopausal status (p 5.03); polyps witha size greater than 1.5 cm (p ,.001) [45]; and hypertensionand tamoxifen use [4]. In a class II-3 study, the incidence ofendometrial hyperplasia and malignancy was similar andclinically relevant in patients with symptoms (3.2%) andsymptom-free patients (3.9%), suggesting that polyps shouldbe removed whenever identified [47]. The use of ultrasonog-raphy may aid in the diagnosis of neoplastic change withinendometrial polyps, with sensitivity of 67% to 100% andspecificity of 71% to 89% [51,52]. The variation in rangeis dependent on the endometrial thickness used as therequirement for further investigation by more invasivemethods. The data are limited in this area, and thedifferentiation of endometrium from endometrial polypssonographically with regard to possible neoplastic changeis a confounding factor.
Natural History
The spontaneous regression rates of incidentally detectedendometrial polyps at 1 year is estimated in one study to be27% [27]. In this class II-1 study, the size of polyps atdiagnosis correlated with their likelihood of persistence at12 months follow-up. Polyps with a mean length of 15.1 mmwere significantly less likely to have spontaneously re-gressed at follow-up compared with polyps that hada mean length of 10.7 mm (mean difference 4.4, 95% confi-dence interval [CI] 0.2-8.6, p 5.04) [27], suggesting thatsmaller polyps are more likely to regress spontaneously. Aseparate prospective study also demonstrated that smallerpolyps ,1 cm were more likely to regress spontaneously,whereas those .1 cm were more likely to persist and causeabnormal uterine bleeding, although the difference was notsignificant (p 5.16) [53]. Polyp regression may be associ-ated with isolated episodes of menorrhagia associated withcramping followed by resumption of normal menstruationpossibly related to the passage of endometrial polyps [53].
Diagnosis
Imaging
Transvaginal UltrasonographyOn transvaginal ultrasonography (TVUS), an endome-
trial polyp typically appears as a hyperechoic lesion withregular contours within the uterine lumen, outlining the
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
572 Journal of Minimally Invasive Gynecology, Vol 18, No 5, September/October 2011
endometrial walls on which it rests, surrounded by a thinhyperechoic halo [26]. Cystic spaces corresponding todilated glands filled with proteinaceous fluid may be seenwithin the polyp [54] or the polyp may appear as a nonspe-cific endometrial thickening or focal mass within the endo-metrial cavity [55]. Such sonographic findings are notspecific to polyps, and other endometrial abnormalitiessuch as submucosal fibroids may have the same features[56]. To aid in the diagnosis of an endometrial polyp,TVUS is best performed in premenopausal women beforeday 10 of the cycle when the endometrium is at its thinnestto minimize the risk of false-positive and -negativefindings [57].
Table 1 compares the diagnostic accuracy of various im-aging techniques for endometrial polyps. TVUS has reportedsensitivity of 19% to 96%, specificity of 53% to 100%, pos-itive predictive value (PPV) of 75% to 100%, and negativepredictive value (NPV) of 87% to 97%, when comparedwith hysteroscopy with guided biopsy. A paucity of level Ievidence may explain this wide range of data, as well asstudies describing a small number of patients. Withinsome of these studies the pathologic condition is heteroge-neous, with some combining both endometrial polyps andsubmucous fibroids as a diagnostic group, making exact fig-ures difficult to extract. In a single large prospective studyevaluating the causes of menorrhagia, the reported sensitiv-ity, specificity, PPV, and NPVof TVUS for the diagnosis ofendometrial polyps were 86%, 94%, 91%, and 90%, respec-tively [61].
There are limited data to support color-flow or powerDoppler aiding in the differentiation of hyperplasia and ma-lignancy in polyps [51,79,80]. A class II-2 study demon-strated specificity and NPV of 95% and 94% respectivelyin the diagnosis of endometrial polyps with the addition ofcolor-flow Doppler scanning to TVUS to identify a singlefeeding vessel [81], whereas others demonstrated addingcolor-flow Doppler scanning to have low specificity for en-dometrial cancer [51], with no difference in the histologiccondition of polyps on the basis of their resistive index, pul-satility index, or size [82].
The use of power Doppler sonography seems more prom-ising [79,83,84]. This technique offers some advantages overconventional color-flow Doppler sonography that makes ita better technique for depicting vascular networks. Thereis level II evidence demonstrating that the addition of powerDoppler sonography with identification of a single vesselpattern improves diagnostic sensitivity to 89% and specific-ity to 87% for an endometrial polyp [83], in comparison tothe multivessel or scattered vessel pattern seen in malignantlesions or endometrial hyperplasia [79]. This benefit wasseen in the diagnosis of endometrial polyps in symptom-free patients, whereas sensitivity in women with symptomsremained largely unchanged from gray-scale TVUS alone[83]. At this time, sonographic examination either with orwithout color-flow or power Doppler sonography is nota substitute for pathologic evaluation after surgical removal.
Saline Infusion SonographyThe use of saline infusion sonography (SIS) or sonohys-
terography (SHG) increases sonographic contrast of the en-dometrial cavity, enabling delineation of the size, locationand other features of an endometrial polyp. With SIS, polypsappear as echogenic, smooth, intracavitary masses with ei-ther broad bases or thin stalks outlined by fluid [55]. Thistechnique may outline small endometrial polyps missed ongray-scale TVUS and is likely improve diagnostic accuracy[60,85–89]. In a prospective comparative study, the use ofsaline solution as a contrast agent significantly enhancedthe sensitivity and specificity compared with TVUS alone,because it detected small lesions that were missed bynoncontrast sonography [60]. Differentiating endometrialpolyps from submucosal fibroids can be difficult, but exam-ination of lesion echotexture and identification of overlyingechogenic endometrium are useful features to distinguish thetwo [90].
When compared with hysteroscopy by use of guided bi-opsy for the identification of different endometrial diseases,SIS has sensitivity of 58% to 100%, specificity of 35% to100%, PPV of 70% to 100%, and NPV of 83% to 100%[37,56,59,60,62]. A number of prospective comparativestudies have reported no significant difference betweenSIS and diagnostic hysteroscopy in diagnosing endometrialpolyps [60,86,91].
When compared with hysteroscopy, SIS has the advan-tage of assessing both the uterine cavity and other uterineand pelvic structures and visualizing potential myometrialand adnexal abnormalities [91]. Previous work reports SISto be less painful than diagnostic hysteroscopy in the outpa-tient setting [92], although these studies were not performedwith the smaller-diameter hysteroscope in common use to-day, with both techniques requiring the cervix to be traversedand uterine distension to occur [93]. Disadvantages of SISinclude an inability to determine final endometrial disease[56], a longer learning curve compared with noncontrastTVUS [87], and patient discomfort caused by fluid leakageor pain with the use of a balloon catheter [94]. Gel instilla-tion sonohysterography may be an alternative solution tothis issue, although limited data are currently available onthis technique [94].
Three-dimensional TVUS and Three-dimensional SISThree-dimensional ultrasonography (3-D US) is a nonin-
vasive imaging technique with the ability to generate multi-planar reconstructed images through the uterus and itsexternal contours. One of the most useful scan planes ob-tained with the 3-D US is the coronal view which is usuallynot obtained by two-dimensional (2-D) ultrasound becauseof the limited mobility of the transvaginal transducer [95].Coronal views allow more accurate visualization betweenthe endometrium and myometrium at the fundus and cornualangles [96], providing superior diagnostic accuracy in de-tecting endometrial polyps compared to 2-D TVUS. A class
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
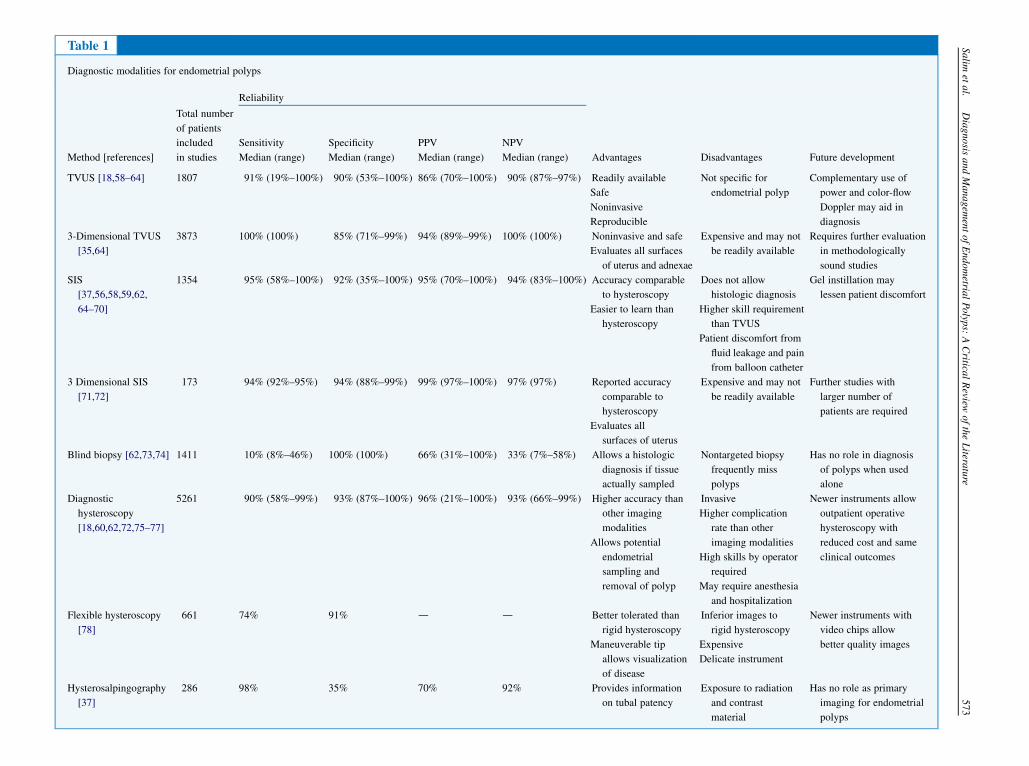
Table 1
Diagnostic modalities for endometrial polyps
Reliability
Method [references]
Total number
of patients
included
in studies
Sensitivity
Median (range)
Specificity
Median (range)
PPV
Median (range)
NPV
Median (range) Advantages Disadvantages Future development
TVUS [18,58–64] 1807 91% (19%–100%) 90% (53%–100%) 86% (70%–100%) 90% (87%–97%) Readily available
Safe
Noninvasive
Reproducible
Not specific for
endometrial polyp
Complementary use of
power and color-flow
Doppler may aid in
diagnosis
3-Dimensional TVUS
[35,64]
3873 100% (100%) 85% (71%–99%) 94% (89%–99%) 100% (100%) Noninvasive and safe
Evaluates all surfaces
of uterus and adnexae
Expensive and may not
be readily available
Requires further evaluation
in methodologically
sound studies
SIS
[37,56,58,59,62,
64–70]
1354 95% (58%–100%) 92% (35%–100%) 95% (70%–100%) 94% (83%–100%) Accuracy comparable
to hysteroscopy
Easier to learn than
hysteroscopy
Does not allow
histologic diagnosis
Higher skill requirement
than TVUS
Patient discomfort from
fluid leakage and pain
from balloon catheter
Gel instillation may
lessen patient discomfort
3 Dimensional SIS
[71,72]
173 94% (92%–95%) 94% (88%–99%) 99% (97%–100%) 97% (97%) Reported accuracy
comparable to
hysteroscopy
Evaluates all
surfaces of uterus
Expensive and may not
be readily available
Further studies with
larger number of
patients are required
Blind biopsy [62,73,74] 1411 10% (8%–46%) 100% (100%) 66% (31%–100%) 33% (7%–58%) Allows a histologic
diagnosis if tissue
actually sampled
Nontargeted biopsy
frequently miss
polyps
Has no role in diagnosis
of polyps when used
alone
Diagnostic
hysteroscopy
[18,60,62,72,75–77]
5261 90% (58%–99%) 93% (87%–100%) 96% (21%–100%) 93% (66%–99%) Higher accuracy than
other imaging
modalities
Allows potential
endometrial
sampling and
removal of polyp
Invasive
Higher complication
rate than other
imaging modalities
High skills by operator
required
May require anesthesia
and hospitalization
Newer instruments allow
outpatient operative
hysteroscopy with
reduced cost and same
clinical outcomes
Flexible hysteroscopy
[78]
661 74% 91% d d Better tolerated than
rigid hysteroscopy
Maneuverable tip
allows visualization
of disease
Inferior images to
rigid hysteroscopy
Expensive
Delicate instrument
Newer instruments with
video chips allow
better quality images
Hysterosalpingography
[37]
286 98% 35% 70% 92% Provides information
on tubal patency
Exposure to radiation
and contrast
material
Has no role as primary
imaging for endometrial
polyps
Salim
etal.
Diagnosis
andManagem
entofEndometria
lPolyp
s:ACritica
lReview
oftheLitera
ture
573
574 Journal of Minimally Invasive Gynecology, Vol 18, No 5, September/October 2011
II-2 study of 3850 consecutive 3-D US cases reported sensi-tivity of 100%, specificity of 99%, PPVof 99% and NPVof100% in diagnosing endometrial polyps when compared tohysteroscopy with biopsy [35]. These figures need to be in-terpreted with caution because only those with a suspectedpolyp on 3-D US subsequently underwent hysteroscopyand therefore do not include those women with endometrialpolyps who had negative 3-D US result. On reviewing thesedata, there is no capacity to provide NPV in this study.Smaller studies with this technique have reported more mod-est figures of 100% for sensitivity, 71% for specificity, 89%for PPV, and 100% for NPV [64].
Adding saline solution contrast into the endometrial cav-ity to perform 3-D SIS may provide additional informationin the diagnosis of endometrial polyps, because it combinesthe advantages of TVUS and SIS. However, studies reportonly slightly higher specificity (88% to 99%) and PPV(97% to 100%) for endometrial polyps than those of 3-DUS, with sensitivity of 92% to 95% and NPV of 97%[64,97]. Given these data, the greater expense of 3-Dsonography and its less-frequent availability, 2-D US withintrauterine contrast should be preferred as an effectiveand reliable noninvasive method to diagnose polyps.
Histologic Diagnosis
Blind BiopsyBlind dilation and curettage is inaccurate in diagnosing
endometrial polyps and should not be used as a diagnosticmethod [98]. Despite specificity and PPV of 100%, its useis limited by its low sensitivity of 8% to 46% and NPV of7% to 58% when compared with hysteroscopy and guidedbiopsy [62,73,74]. Use of an endometrial sampler ora curette can miss pedunculated polyps and fragmentationof sessile polyps may make histologic diagnosis difficult[99]. In postmenopausal women, this is particularly thecase for polyps, which tend to be broader based with an un-even surface caused by small translucent cysts covered byatrophic endometrium [99].
Hysteroscopy with Guided BiopsyHysteroscopy with guided biopsy is the gold standard in
the diagnosis of endometrial polyps [72]. The main advan-tage of hysteroscopy is the ability to visualize and removepolyps concurrently. Diagnostic hysteroscopy alone allowsonly subjective assessment of the size, location, andphysical properties of the lesion, with reported sensitivityof 58% to 99%, specificity of 87% to 100%, PPV of 21%to 100%, and NPVof 66% to 99% when compared with hys-teroscopy with guided biopsy [18,60,62,75,76,97]. Despitethe increasing popularity of office hysteroscopy, mostroutine diagnostic hysteroscopies are still performed in anoperating theater and require anesthesia and hospitalization[56,100]. This may be explained by the requirement ofa high level of expertise to perform hysteroscopy in an
ambulatory or office setting, especially if operativehysteroscopy is required concurrently. The evidence favorsoutpatient hysteroscopy for diagnosis, with 2 large-scalestudies reporting success rates of 92% to 96% in this setting,with no difference between premenopausal and postmeno-pausal women [21,76], and a class I study reporting lessexpense and greater patient preference for an outpatientprocedure [101]. The addition of polypectomy for smallpolyps is possible, and technological improvements andgreater surgeon skill should see increased uptake of outpa-tient procedures in the future.
Flexible hysteroscopy causes less pain for patients andallows an easier passage through the cervical canal whencompared with rigid hysteroscopy [102,103], making itmore suited for outpatient procedures. It is reported to havelower sensitivity of 74% for the diagnosis of endometrialpolyps when compared with rigid hysteroscopy [77,78].This may be explained by the lower quality image obtainedthrough the fiberoptic bundle that carries both light and theimages, although newer flexible hysteroscopy with videochips rather than the old fiberoptic image bundle allows animproved image quality [103]. Expense, delicacy of the in-strument with easy breakage, and more limited operative in-strumentation are disadvantages of flexible hysteroscopescompared with rigid hysteroscopes.
With continuing technological improvements producingnarrow diameter hysteroscopes, operative hysteroscopycan be readily performed in an outpatient setting [104]. Alarge-scale class II study reported 4863 consecutive opera-tive outpatient hysteroscopies including 2306 for endome-trial polyps, in which most small endometrial polyps wereremoved with minimal discomfort [104]. Polyps largerthan the diameter of the internal cervical os may be best re-moved with the patient under general anesthesia given theincreased patient discomfort and longer operating time.
Choice of distension medium is important when consider-ing patient comfort and improveddiagnostic accuracy.Normalsaline solution causes significantly less shoulder tip andlower abdominal pain compared with carbon dioxide [105],allowing clear, reliable imaging for accurate diagnosis [106]and is widely used in the outpatient setting [21,34,104,107].Although some patients may not require analgesia oranesthesia for office hysteroscopy, the use of paracervicalblock or intrauterine anesthetics, particularly if operativehysteroscopy isperformed subsequently,maybehelpful [108].
Complication rates at hysteroscopy are low, with a large-scale class II-1 study reporting an overall complication rateof 0.28% in 13 600 hysteroscopic procedures; the rate foroperative removal of an endometrial polyp in this study is0.4% [109]. Approximately half of the complications wereentry related, whereas the remainder were related to the sur-geon’s experience and type of procedure. Overall, hystero-scopic polypectomy has half the risk of complication whencompared with hysteroscopic myomectomy or endometrialablation and 1/10th the risk for complication comparedwith hysteroscopic synechiolysis [109].
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
Salim et al. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature 575
Other Diagnostic Tests
Hysterosalpingography may define endometrial polyps aspedunculated, nonspecific filling defects within the endome-trial cavity, with high sensitivity (98%) but low specificity(34.6%) compared with hysteroscopy [37]. It can be usedin infertile women to assess tubal patency, but, with disad-vantages including use of ionizing radiation, iodinated con-trast materials, and patient discomfort, routine use ofhysterosalpingography for diagnosis of an endometrialpolyp cannot be recommended.
Endometrial polyps can be identified on magnetic reso-nance imaging as low signal intensity intracavitary massessurrounded by high signal intensity fluid and endometriumby T2-weighted magnetic resonance imaging. Very highcost and limited availability, with limited advantages oversonography, preclude this technique from routine use. Com-puted tomography scanning has a limited role because of itscost, radiation exposure, and low sensitivity of 53% for en-dometrial thickness when compared with TVUS, even withcontrast enhancement [110]. Virtual hysterosalpingographywith 64-slice computed tomography scanning to assessthe uterine cavity has been described [111–113], althoughlimited data are currently available, and it should not beconsidered outside of a research protocol at this time.
ManagementFor women with endometrial polyps, management is
dependent on symptoms, risk of malignancy, fertility issues,and operator skills. Management options will be consideredunder the headings of conservative nonsurgical, conservativesurgical, and radical surgical approaches. Table 2 summa-rizes the management strategies for endometrial polyps.
Conservative Nonsurgical ManagementHaving diagnosed endometrial polyps, their removal ei-
ther in the office or with the patient under general anesthesiais considered a low-risk but not a no-risk procedure and therisk/benefit ratio must be discussed with the patient. In twoclass II-2 studies, it was found that polyps ,10 mm havea 27% chance of spontaneous regression over 12 monthsand a low chance of malignancy [27,53], indicating thatsymptom-free women with polyps ,10 mm in size couldbe managed conservatively.
Medical treatments may have some role in the manage-ment of endometrial polyps and GnRH agonists are reportedto give short-term symptomatic relief for endometrialpolyps, but symptom recurrence is common with treatmentcessation [125]. Although GnRH agonists could be used asan adjunctive treatment before hysteroscopic resection[125], this must be considered against the costs and side ef-fects of this medication and the comparative benefit fromsimple alternate extirpative treatments without the use ofthese medications.
In a class II study of 3 different hormone replacementtherapy types (2.5 mg with conjugated estrogen 0.625 mgand medroxyprogestorone 2.5 mg; estradiol 2 mg and nore-
thisterone 1 mg; tibolone 2.5 mg), the progestin with thehighest antiestrogenic activity (tibolone) is suggested to re-duce the development of endometrial polyps. Follow-up hys-teroscopic examination at 36 months after treatmentreported few polyps in any group (range 0–3), and theclinical superiority of any of these medications must beconsidered in a circumspect manner until class I studiesare undertaken. Importantly, the balance between diseasesuppression and other side effects of these medicationsmust be considered [126].
A randomized trial of LNG-IUS compared with observa-tion indicates that reduced endometrial thickness throughprogestogenic suppression may be a factor in reducing polypdevelopment. In the 4.5-year period of the study, 8 newpolyps were reported in the observation group comparedwith 3 in the LNG-IUS group (p 5.016). In this intentionto treat study, the 3 polyps in the LNG-IUS group occurredin 1 woman who did not have the LNG-IUS inserted and theremaining 2 in women who had it removed at 1 year becauseof side effects. Although these figures are encouraging, theuse of LNG-IUS for the treatment of polyps should becurrently limited to research protocols [127].
Conservative Surgical ManagementBlind dilation and curettage has been the standard man-
agement option for abnormal uterine bleeding and suspectedendometrial disease for many years and is still common prac-tice, with a survey from the United Kingdom in 2002reporting that 2% of gynecologists used blind dilation andcurettage for the management of endometrial polyps, and51% were performing blind curettage after hysteroscopyfor the removal of polyps [100]. Evidence suggests that thispractice is ineffective and has a significant complicationrate (1:100 perforation rate and 1:200 infection rate) associ-ated with its use. A class II study reports complete removal ofendometrial polyps by dilation and curettage alone in 8/51patients (4%), whereas the addition of polyp forceps in-creases complete extraction to 21/51 patients (41%). Theseclass II-2 and II-3 studies indicate that the endometrial dis-ease is removed less than 50% of the time, and in many casesremoval is incomplete [73,74,128–130]. Given the lowcomplication rate associated with hysteroscopic removal andits widespread availability, safety, and ability to be performedin an outpatient setting [76,105,109,131,132], blind dilationand curettage should be relegated to history and replacedby direct visualization and targeted disease removal.
TVUS-guided polypectomy has been suggested as a pos-sible improvement on the blind technique; however, after anearly feasibility study, there has been little further enthusi-asm for this technique [133]. The mean operating time forthe procedure was 8 minutes (95% CI, 5.9–10.4) and wassuccessful in 32/37 (86.5%) cases (95% CI, 75.5–97.5).In the failed cases, unsatisfactory imaging and failure tograsp the polyp were the causes. Two patients (5.4%) bledfrom the tenaculum insertion site, necessitating a suturefor hemostasis.
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
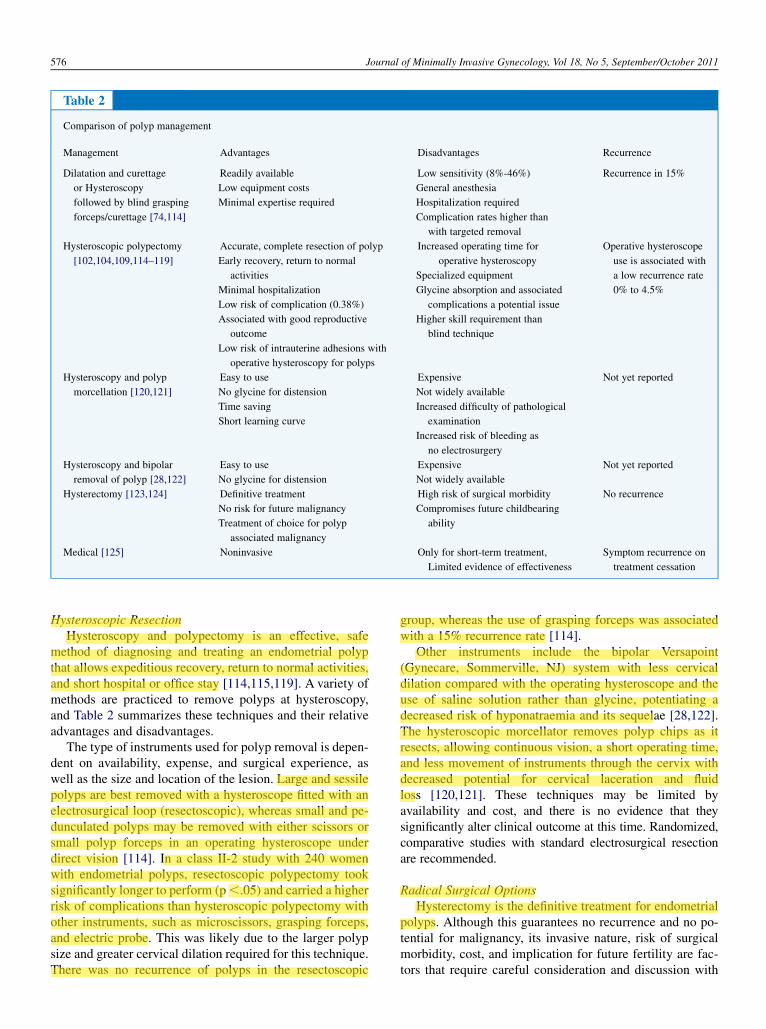
Table 2
Comparison of polyp management
Management Advantages Disadvantages Recurrence
Dilatation and curettage
or Hysteroscopy
followed by blind grasping
forceps/curettage [74,114]
Readily available
Low equipment costs
Minimal expertise required
Low sensitivity (8%-46%)
General anesthesia
Hospitalization required
Complication rates higher than
with targeted removal
Recurrence in 15%
Hysteroscopic polypectomy
[102,104,109,114–119]
Accurate, complete resection of polyp
Early recovery, return to normal
activities
Minimal hospitalization
Low risk of complication (0.38%)
Associated with good reproductive
outcome
Low risk of intrauterine adhesions with
operative hysteroscopy for polyps
Increased operating time for
operative hysteroscopy
Specialized equipment
Glycine absorption and associated
complications a potential issue
Higher skill requirement than
blind technique
Operative hysteroscope
use is associated with
a low recurrence rate
0% to 4.5%
Hysteroscopy and polyp
morcellation [120,121]
Easy to use
No glycine for distension
Time saving
Short learning curve
Expensive
Not widely available
Increased difficulty of pathological
examination
Increased risk of bleeding as
no electrosurgery
Not yet reported
Hysteroscopy and bipolar
removal of polyp [28,122]
Easy to use
No glycine for distension
Expensive
Not widely available
Not yet reported
Hysterectomy [123,124] Definitive treatment
No risk for future malignancy
Treatment of choice for polyp
associated malignancy
High risk of surgical morbidity
Compromises future childbearing
ability
No recurrence
Medical [125] Noninvasive Only for short-term treatment,
Limited evidence of effectiveness
Symptom recurrence on
treatment cessation
576 Journal of Minimally Invasive Gynecology, Vol 18, No 5, September/October 2011
Hysteroscopic ResectionHysteroscopy and polypectomy is an effective, safe
method of diagnosing and treating an endometrial polypthat allows expeditious recovery, return to normal activities,and short hospital or office stay [114,115,119]. A variety ofmethods are practiced to remove polyps at hysteroscopy,and Table 2 summarizes these techniques and their relativeadvantages and disadvantages.
The type of instruments used for polyp removal is depen-dent on availability, expense, and surgical experience, aswell as the size and location of the lesion. Large and sessilepolyps are best removed with a hysteroscope fitted with anelectrosurgical loop (resectoscopic), whereas small and pe-dunculated polyps may be removed with either scissors orsmall polyp forceps in an operating hysteroscope underdirect vision [114]. In a class II-2 study with 240 womenwith endometrial polyps, resectoscopic polypectomy tooksignificantly longer to perform (p,.05) and carried a higherrisk of complications than hysteroscopic polypectomy withother instruments, such as microscissors, grasping forceps,and electric probe. This was likely due to the larger polypsize and greater cervical dilation required for this technique.There was no recurrence of polyps in the resectoscopic
group, whereas the use of grasping forceps was associatedwith a 15% recurrence rate [114].
Other instruments include the bipolar Versapoint(Gynecare, Sommerville, NJ) system with less cervicaldilation compared with the operating hysteroscope and theuse of saline solution rather than glycine, potentiating adecreased risk of hyponatraemia and its sequelae [28,122].The hysteroscopic morcellator removes polyp chips as itresects, allowing continuous vision, a short operating time,and less movement of instruments through the cervix withdecreased potential for cervical laceration and fluidloss [120,121]. These techniques may be limited byavailability and cost, and there is no evidence that theysignificantly alter clinical outcome at this time. Randomized,comparative studies with standard electrosurgical resectionare recommended.
Radical Surgical OptionsHysterectomy is the definitive treatment for endometrial
polyps. Although this guarantees no recurrence and no po-tential for malignancy, its invasive nature, risk of surgicalmorbidity, cost, and implication for future fertility are fac-tors that require careful consideration and discussion with
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
Salim et al. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature 577
the patient [124]. There are no class I studies comparing hys-terectomy with conservative treatments for polyps; however,a pragmatic approach with the less-invasive treatment seemsappropriate in the absence of such evidence.
Clinical OutcomesClinical outcomesafter treatment of endometrial polyps are
generally good. In a randomized clinical trial of 150 womenwith an endometrial polyp allocated to hysteroscopic removalor observation, therewas nodifference identified in thevolumeofmenstrual loss between the groups, although the symptoms,such as intermenstrual bleeding, were significantly improvedby removal at follow-up (residual symptoms following polypremoval 7/75 vs conservative 28/75; p 5.001) [134]. Otherstudies report the symptomatic improvement to be verygood, with abnormal uterine bleeding resolved after hystero-scopic polypectomy in 75% to 100% of cases [135,136].
Adhesion risk is low after polypectomy, because themyometrium is not incised and the endometrium has anexcellent regenerative capacity [137]. A class I study with90 women reports no adhesions after hysteroscopic polypec-tomy, and routine antiadhesion treatments are unlikely tobe of benefit in this group of patients [116].
In a class II-3 retrospective study, recurrence of polypsafter 9 years of follow-up after hysteroscopic polypectomywas reported in 5 of 240 patients (3.7%), requiring repeathysteroscopic removal in 3 (1.7%) and subsequent hysterec-tomy in 2 (0.8%) [114]. This is in contrast to a class II-3study that reports recurrence of symptoms after polypec-tomy of 60% by survival curve analysis; however, only2/78 (2.5%) women were identified to have recurrent polyps,with many other diseases present in the remaining patientsincluding abnormal uterine bleeding [138]. This indicatesthat although recurrence of polyps is low, the presentingsymptoms leading to surgical removal are not always relatedto the presence of the polyp. It is therefore important to dif-ferentiate recurrence of disease with recurrence of symp-toms, and discussion of this fact with the patient beforeintervention is required.
Most of the data for polypectomy in subfertile patientssuggests that removal improves fertility, with reported preg-nancy rates varying between 43% to 80% [114,139,140].Both spontaneous pregnancy rates and those associatedwith assisted reproductive technology are reported to beincreased after polypectomy. In a class I study, polypectomybefore intrauterine insemination significantly increasedsubsequent pregnancy success (relative risk 2.1, 95% CI1.5-2.9, p ,.001). The rate of pregnancy in the study groupwas 51%, and of these, 65% had a spontaneous conceptionbefore the first intrauterine insemination, whereas allpregnancies in the control group were obtained during thefertility treatment [141].
There is conflict surrounding the size of polyp needed tobe removed to achieve an improvement in assisted reproduc-tive technology, with data suggesting that removal of polyps,2 cm has no impact on the outcome of fertility treatment
[142–144]. In contrast, a class II-2 study suggested that res-toration of fertility was not dependent on the size of lesionremoved (139) and a class II-3 study reported no significantdifference in the reproductive outcome for patients withpolyps %2.5 cm or .2.5cm [114].
Conclusion
Endometrial polyps are a common gynecologic diseasethat increases with age and are rarely associated with malig-nancy. Polyps may not be responsible for abnormal uterinebleeding symptoms in premenopausal women when theyare found, although, when diagnosed, removal seems pru-dent to exclude this as a simple causative factor. Noninvasivetechniques such as gray-scale TVUS are a reliable modalityfor diagnosis, with diagnostic improvement by use of con-trast techniques. In clinical practice, the choice of diagnosticmethod for endometrial polyps is dependent on the conditionof the patient, the facilities available, comparative costs, andthe physician’s experience with these modalities.
For management, hysteroscopic resection is safe and ef-fective and allows histologic assessment. Blind techniquesshould be avoided when visual techniques are available forexcision. Conservative treatment is a viable option pendingpatient preference and risk factors. For patients with infertil-ity and the presence of polyps, removal of disease is likely tobe helpful to subsequent pregnancy. Conservative treatmentsfor benign lesions should be favored over radical options.
References
1. Kim KR, Peng R, Ro JY, Robboy SJ. A diagnostically useful histo-
pathologic feature of endometrial polyp: the long axis of endometrial
glands arranged parallel to surface epithelium. Am J Surg Pathol.
2004;28:1057–1062.
2. PetersonWF, Novak ER. Endometrial polyps.Obstet Gynecol. 1956;
8:40–49.
3. Savelli L, De Iaco P, Santini D, et al. Histopathologic features and
risk factors for benignity, hyperplasia, and cancer in endometrial
polyps. Am J Obstet Gynecol. 2003;188:927–931.
4. Cohen I. Endometrial pathologies associated with postmenopausal
tamoxifen treatment. Gynecol Oncol. 2004;94:256–266.
5. Onalan R, Onalan G, Tonguc E, Ozdener T, Dogan M,
Mollamahmutoglu L. Body mass index is an independent risk factor
for the development of endometrial polyps in patients undergoing
in vitro fertilization. Fertil Steril. 2009;91:1056–1060.
6. Vanni R, Dal Cin P, Marras S, et al. Endometrial polyp: Another
benign tumor characterized by 12q13-q15 changes. Cancer Genet
Cytogenet. 1993;68:32–33.
7. Inagaki N, Ung L, Otani T, Wilkinson D, Lopata A. Uterine cavity
matrix metalloproteinases and cytokines in patients with leiomyoma,
adenomyosis or endometrial polyp. Eur J Obstet Gynecol Reproduct
Biol. 2003;111:197–203.
8. Nogueira AA, Sant’Ana de Almeida EC, Poli Neto OB, Zambelli
Ramalho LN, Rosa e Silva JC, Candido dos Reis FJ. Immunohisto-
chemicalexpressionofp63inendometrial polyps: evidence that abasal
cell immunophenotype is maintained.Menopause. 2006;13:826–830.
9. Jakab A, �Ov�ari L, Juh�asz B, Birinyi L, Bacsk�o G, T�oth Z. Detection
of feeding artery improves the ultrasound diagnosis of endometrial
polyps in asymptomatic patients. Eur J Obstet Gynecol Reproduct
Biol. 2005;119:103–107.
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
juanes
Highlight
578 Journal of Minimally Invasive Gynecology, Vol 18, No 5, September/October 2011
10. Sant’Ana de Almeida EC, Nogueira AA, Candido dos Reis FJ,
Zambelli Ramalho LN, Zucoloto S. Immunohistochemical expression
of estrogen and progesterone receptors in endometrial polyps and ad-
jacent endometrium in postmenopausal women. Maturitas. 2004;49:
229–233.
11. Liu Z, Kuokkanen S, Pal L. Steroid hormone receptor profile of pre-
menopausal endometrial polyps. Reprod Sci. 2010;17:377–383.
12. Lopes RGC, Baracat EC, de Albuquerque Neto LC, et al. Analysis of
estrogen- and progesterone-receptor expression in endometrial polyps.
J Minim Invasive Gynecol. 2007;14:300–303.
13. Mittal K, Schwartz L, Goswami S, Demopoulos R. Estrogen and pro-
gesterone receptor expression in endometrial polyps. Int J Gynecol
Pathol. 1996;15:345–348.
14. Taylor LJ, Jackson TL, Reid JG, Duffy SR. The differential expression
of oestrogen receptors, progesterone receptors, Bcl-2 and Ki67 in en-
dometrial polyps. Br J Obstet Gynaecol. 2003;110:794–798.
15. Maia H Jr, Maltez A, Studart E, Athayde C, Coutinho EM. Ki-67,
Bcl-2 and p53 expression in endometrial polyps and in the normal en-
dometrium during the menstrual cycle. Br J Obstet Gynaecol. 2004;
111:1242–1247.
16. Haimov-Kochman R, Deri-Hasid R, Hamani Y, Voss E. The natural
course of endometrial polyps: Could they vanish when left untreated?
Fertil Steril. 2009;92:828.e11–828.e12.
17. Dreisler E, Stampe Sorensen S, Ibsen PH, Lose G. Prevalence of endo-
metrial polyps and abnormal uterine bleeding in a Danish population
aged 20-74 years. Ultrasound Obstet Gynecol. 2009;33:102–108.
18. Fabres C, Alam V, Balmaceda J, Zegers-Hochschild F, Mackenna A,
Fernandez E. Comparison of ultrasonography and hysteroscopy in
the diagnosis of intrauterine lesions in infertile women. J Am Assoc
Gynecol Laparosc. 1998;5:375–378.
19. Anastasiadis PG, Koutlaki NG, Skaphida PG, Galazios GC,
Tsikouras PN, Liberis VA. Endometrial polyps: prevalence, detection,
and malignant potential in women with abnormal uterine bleeding.
Eur J Gynaecol Oncol. 2000;21:180–183.
20. Nappi L, Indraccolo U, Di Spiezio Sardo A, et al. Are diabetes,
hypertension, and obesity independent risk factors for endometrial
polyps? J Minim Invasive Gynecol. 2009;16:157–162.
21. Nagele F, O’Connor H, Davies A, Badawy A, Mohamed H, Magos A.
2500 Outpatient diagnostic hysteroscopies. Obstet Gynecol. 1996;88:
87–92.
22. Reslova T, Tosner J, ReslM, Kugler R, Vavrova I. Endometrial polyps:
a clinical study of 245 cases.ArchGynecol Obstet. 1999;262:133–139.
23. Vilodre LC, Bertat R, Petters R, Reis FM. Cervical polyp as risk factor
for hysteroscopically diagnosed endometrial polyps. Gynecol Obstet
Invest. 1997;44:191–195.
24. Fay TN, Khanem N, Hosking D. Out-patient hysteroscopy in asymp-
tomatic postmenopausal women. Climacteric. 1999;2:263–267.
25. de Ziegler D. Contrast ultrasound: a simple-to-use phase-shifting me-
dium offers saline infusion sonography-like images. Fertil Steril.
2009;92:369–373.
26. Martinez-Perez O, Perez-Medina T, Bajo-Arenas J. Ultrasonography
of endometrial polyps. Ultrasound Rev Obstet Gynecol. 2003;3:43.
27. Lieng M, Istre O, Sandvik L, Qvigstad E. Prevalence, 1-Year Regres-
sion Rate, and Clinical Significance of Asymptomatic Endometrial
Polyps: Cross-sectional Study. J Minim Invasive Gynecol. 2009;16:
465–471.
28. Golan A, Sagiv R, BerarM, Ginath S, GlezermanM. Bipolar electrical
energy in physiologic solutionda revolution in operative hystero-
scopy. J Am Assoc Gynecol Laparosc. 2001;8:252–258.
29. Valle RF. Hysteroscopy for gynecologic diagnosis. Clin Obstet
Gynecol. 1983;26:253–276.
30. Wu HH, Schuetz MJ 3rd, Cramer H. Significance of benign endome-
trial cells in Pap smears from postmenopausal women. J Reprod Med.
2001;46:795–798.
31. Hassa H, Tekin B, Senses T, KayaM, Karatas A. Are the site, diameter,
and number of endometrial polyps related with symptomatology? Am
J Obstet Gynecol. 2006;194:718–721.
32. Taylor P, Pattinson H, Kredenster J. Diagnostic hysteroscopy. In:
Hunt R, editor. Atlas of female infertility. Boston: Mosby–Year
Book; 1992. p. 200.
33. Shokeir TA, Shalan HM, El-Shafei MM. Significance of endometrial
polyps detected hysteroscopically in eumenorrheic infertile women.
J Obstet Gynaecol Res. 2004;30:84–89.
34. Hinckley MD, Milki AA. 1000 office-based hysteroscopies prior to
in vitro fertilization: feasibility and findings. JSLS. 2004;8:103–107.
35. Kupesic S, Kurjak A, Skenderovic S, Bjelos D. Screening for uterine
abnormalities by three-dimensional ultrasound improves perinatal
outcome. J Perinat Med. 2002;30:9–17.
36. Valle RF. Hysteroscopy in the evaluation of female infertility. Am J
Obstet Gynecol. 1980;137:425–431.
37. Preutthipan S, Linasmita V. A prospective comparative study between
hysterosalpingography and hysteroscopy in the detection of intrauter-
ine pathology in patients with infertility. J Obstet Gynaecol Res. 2003;
29:33–37.
38. Hann LE, Gretz EM, Bach AM, Francis SM. Sonohysterography for
evaluation of the endometrium in women treated with tamoxifen.
AJR Am J Roentgenol. 2001;177:337–342.
39. Cain J, ElMasriWM, Gregory T, Kohn EC. Chapter 41. Gynecology. In:
Brunicardi FC, Anderson D, Billiar TR, et al., editors. Schwartz’s prin-
ciples of surgery. 9th ed. New York: McGraw-Hill Professional; 2009.
40. Exacoustos C, Zupi E, Cangi B, Chiaretti M, Arduini D, Romanini C.
Endometrial evaluation in postmenopausal breast cancer patients re-
ceiving tamoxifen: an ultrasound, color flow Doppler, hysteroscopic
and histological study. Ultrasound Obstet Gynecol. 1995;6:435–442.
41. Spiewankiewicz B, Stelmachow J, Sawicki W, Cendrowski K,
Kuzlik R. Hysteroscopy in cases of cervical polyps. Eur J Gynaecol
Oncol. 2003;24:67–69.
42. Coeman D, Van Belle Y, Vanderick G, De Muylder X, De Muylder E,
Campo R. Hysteroscopic findings in patients with a cervical polyp.Am
J Obstet Gynecol. 1993;169:1563–1565.
43. Kim TJ, Kim HS, Park CT, Park IS, Hong SR, Park JS, et al. Clinical
evaluation of follow-up methods and results of atypical glandular cells
of undetermined significance (AGUS) detected on cervicovaginal Pap
smears. Gynecol Oncol. 1999;73:292–298.
44. Bakour SH, Khan KS, Gupta JK. The risk of premalignant and malig-
nant pathology in endometrial polyps. Acta Obstet Gynecol Scand.
2000;79:317–320.
45. Ben-Arie A, Goldchmit C, Laviv Y, Levy R, Caspi B, Huszar M, et al.
The malignant potential of endometrial polyps. Eur J Obstet Gynecol
Reprod Biol. 2004;115:206–210.
46. Ferrazzi E, Zupi E, Leone FP, et al. How often are endometrial polyps
malignant in asymptomatic postmenopausal women? A multicenter
study. Am J Obstet Gynecol. 2009;200:235e1–235e6.
47. Lieng M, Qvigstad E, Sandvik L, Jorgensen H, Langebrekke A,
Istre O. Hysteroscopic resection of symptomatic and asymptomatic
endometrial polyps. J Minim Invasive Gynecol. 2007;14:189–194.
48. Papadia A, Gerbaldo D, Fulcheri E, Ragni N, Menoni S, Zanardi S,
et al. The risk of premalignant andmalignant pathology in endometrial
polyps: should every polyp be resected?Minerva Ginecologica. 2007;
59:117–124.
49. Lieng M, Istre O, Qvigstad E. Treatment of endometrial polyps: a sys-
tematic review. Acta Obstet Gynecol Scand. 2010;89:992–1002.
50. Domingues A, Lopes H, Dias I, De Oliveria C. Endometrial polyps in
postmenopausal women. Acta Obstetrica Gynecologica Scandinav-
ica. 2009;88:618–620.
51. Vuento MH, Pirhonen JP, Makinen JI, Tyrkko JE, Laippala PJ,
Gronroos M, et al. Screening for endometrial cancer in asymptomatic
postmenopausal women with conventional and colour Doppler sonog-
raphy. Br J Obstet Gynaecol. 1999;106:14–20.
52. Perez-Medina T, Bajo J, Huertas MA, Rubio A. Predicting atypia in-
side endometrial polyps. J Ultrasound Med. 2002;21:125–128.
53. DeWaay DJ, Syrop CH, Nygaard IE, Davis WA, Van Voorhis BJ. Nat-
ural history of uterine polyps and leiomyomata.Obstet Gynecol. 2002;
100:3–7.
Salim et al. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature 579
54. Hulka CA, Hall DA, McCarthy K, Simeone JF. Endometrial polyps,
hyperplasia, and carcinoma in postmenopausal women: differentiation
with endovaginal sonography. Radiology. 1994;191:755–758.
55. Schorge J, Schaffer J, Halvorson L, Hoffman B, Bradshaw K,
Cunningham F. Chapter 8. Abnormal uterine bleeding. In: Schorge JO,
Schaffer JI, Halvorson LM, Hoffman BL, Bradshaw KD,
Cunningham FG, editors. Williams Gynecology. New York: McGraw-
Hill Professional; 2008.
56. Bernard JP, Rizk E, Camatte S, Robin F, Taurelle R, Lecuru F. Saline
contrast sonohysterography in the preoperative assessment of benign
intrauterine disorders. Ultrasound Obstet Gynecol. 2001;17:145–149.
57. Nalaboff KM, Pellerito JS, Ben-Levi E. Imaging the endometrium:
disease and normal variants. Radiographics. 2001;21:1409–1424.
58. Ragni G, Diaferia D, Vegetti W, Colombo M, Arnoldi M,
Crosignani PG. Effectiveness of sonohysterography in infertile patient
work-up: a comparison with transvaginal ultrasonography and hys-
teroscopy. Gynecol Obstet Invest. 2005;59:184–188.
59. Valenzano MM, Lijoi D, Mistrangelo E, Fortunato T, Costantini S,
Ragni N. The value of sonohysterography in detecting intracavitary
benign abnormalities. Arch Gynecol Obstet. 2005;272:265–268.
60. Schw€arzler P, Concin H, B€osch H, et al. An evaluation of sono-
hysterography and diagnostic hysteroscopy for the assessment of
intrauterine pathology. Ultrasound Obstet Gynecol. 1998;11:
337–342.
61. Vercellini P, Cortesi I, Oldani S, Moschetta M, De Giorgi O,
Crosignani PG. The role of transvaginal ultrasonography and outpa-
tient diagnostic hysteroscopy in the evaluation of patients with menor-
rhagia. Hum Reprod. 1997;12:1768–1771.
62. Pasqualotto EB, Margossian H, Price LL, Bradley LD. Accuracy of
preoperative diagnostic tools and outcome of hysteroscopic manage-
ment of menstrual dysfunction. J Am Assoc Gynecol Laparosc.
2000;7:201–209.
63. Indman PD. Abnormal uterine bleeding. Accuracy of vaginal probe
ultrasound in predicting abnormal hysteroscopic findings. J Reprod
Med. 1995;40:545–548.
64. La Torre R, De Felice C, De Angelis C, Coacci F, Mastrone M,
Cosmi EV. Transvaginal sonographic evaluation of endometrial
polyps: a comparison with two dimensional and three dimensional
contrast sonography. Clin Exp Obstet Gynecol. 1999;26:171–173.
65. Rogerson L, Bates J, Weston M, Duffy S. A comparison of outpatient
hysteroscopy with saline infusion hysterosonography. BJOG. 2002;
109:800–804.
66. Chittacharoen A, Theppisai U, Linasmita V, Manonai J. Sonohyster-
ography in the diagnosis of abnormal uterine bleeding. J Obstet Gy-
naecol Res. 2000;26:277–281.
67. Kamel HS, Darwish AM, Mohamed SA. Comparison of transvaginal
ultrasonography and vaginal sonohysterography in the detection of en-
dometrial polyps. Acta Obstetricia et Gynecologica Scandinavica.
2000;79:60–64.
68. Gronlund L, Hertz J, Helm P, Colov NP. Transvaginal sonohysterogra-
phy and hysteroscopy in the evaluation of female infertility, habitual
abortion or metrorrhagia. A comparative study. Acta Obstetricia et
Gynecologica Scandinavica. 1999;78:415–418.
69. Cicinelli E, Romano F, Anastasio PS, Blasi N, Parisi C. Sonohysterog-
raphy versus hysteroscopy in the diagnosis of endouterine polyps.
Gynecol Obstet Invest. 1994;38:266–271.
70. Soares SR, Barbosa dos Reis MM, Camargos AF. Diagnostic accuracy
of sonohysterography, transvaginal sonography, and hysterosalpin-
gography in patients with uterine cavity diseases. Fertil Steril. 2000;
73:406–411.
71. de Kroon CD, Louwe LA, Trimbos JB, Jansen FW. The clinical value
of 3-dimensional saline infusion sonography in addition to 2-
dimensional saline infusion sonography in women with abnormal
uterine bleeding: work in progress. J Ultrasound Med. 2004;23:
1433–1440.
72. Makris N, Kalmantis K, Skartados N, Papadimitriou A, Mantzaris G,
Antsaklis A. Three-dimensional hysterosonography versus hystero-
scopy for the detection of intracavitary uterine abnormalities. Int J
Gynecol Obstet. 2007;97:6–9.
73. Svirsky R, Smorgick N, Rozowski U, et al. Can we rely on blind en-
dometrial biopsy for detection of focal intrauterine pathology? Am J
Obstet Gynecol. 2008;199:115e1–115e3.
74. Bettocchi S, Ceci O, Vicino M, Marello F, Impedovo L, Selvaggi L.
Diagnostic inadequacy of dilatation and curettage. Fertil Steril.
2001;75:803–805.
75. Birinyi L, Darago P, Torok P, et al. Predictive value of hysteroscopic
examination in intrauterine abnormalities. Eur J Obstet Gynecol
Reprod Biol. 2004;115:75–79.
76. Lo KW, Yuen PM. The role of outpatient diagnostic hysteroscopy in
identifying anatomic pathology and histopathology in the endometrial
cavity. J Am Assoc Gynecol Laparosc. 2000;7:381–385.
77. Chang CC. Efficacy of office diagnostic hysterofibroscopy. J Minim
Invasive Gynecol. 2007;14:172–175.
78. Zlatkov V, Kostova P, Barzakov G, et al. Flexible hysteroscopy in
irregular uterine bleeding. J BUON. 2007;12:53–56.
79. Alcazar JL, Castillo G, Minguez JA, Galan MJ. Endometrial blood
flow mapping using transvaginal power Doppler sonography in
women with postmenopausal bleeding and thickened endometrium.
Ultrasound Obstet Gynecol. 2003;21:583–588.
80. de Kroon C. Power Doppler area in the diagnosis of endometrial
cancer. Int J Gynecol Cancer. 2010;20:1160–1165.
81. TimmermanD, Verguts J, KonstantinovicML, et al. The pedicle artery
sign based on sonography with color Doppler imaging can replace
second-stage tests in women with abnormal vaginal bleeding. Ultra-
sound Obstet Gynecol. 2003;22:166–171.
82. Goldstein SR, Monteagudo A, Popiolek D, Mayberry P,
Timor-Tritsch I. Evaluation of endometrial polyps. Am J Obstet
Gynecol. 2002;186:669–674.
83. Jakab A, Ovari L, Juhasz B, Birinyi L, Bacsko G, Toth Z. Detection of
feeding artery improves the ultrasound diagnosis of endometrial
polyps in asymptomatic patients. Eur J Obstet Gynecol Reprod Biol.
2005;119:103–107.
84. Odeh M, Vainerovsky I, Grinin V, Kais M, Ophir E, Bornstein J.
Three-dimensional endometrial volume and 3-dimensional power
Doppler analysis in predicting endometrial carcinoma and hyperpla-
sia. Gynecol Oncol. 2007;106:348–353.
85. Anastasiadis PG, Koutlaki NG, Skaphida PG, Galazios GC,
Tsikouras PN, Liberis VA. Endometrial polyps: prevalence, detection,
and malignant potential in women with abnormal uterine bleeding.
Eur J Gynaecol Oncol. 2000;21:180–183.
86. Jansen FW, de Kroon CD, van Dongen H, Grooters C, Louwe L,
Trimbos-Kemper T. Diagnostic hysteroscopy and saline infusion
sonography: prediction of intrauterine polyps and myomas. J Minim
Invasive Gynecol. 2006;13:320–324.
87. Syrop CH, Sahakian V. Transvaginal sonographic detection of endo-
metrial polyps with fluid contrast augmentation. Obstet Gynecol.
1992;79:1041–1043.
88. Guven MA, Bese T, Demirkiran F. Comparison of hydrosonography
and transvaginal ultrasonography in the detection of intracavitary pa-
thologies in women with abnormal uterine bleeding. Int J Gynecol
Cancer. 2004;14:57–63.
89. Dijkhuizen FP, De Vries LD, Mol BW, Brolmann HA, Peters HM,
Moret E, et al. Comparison of transvaginal ultrasonography and saline
infusion sonography for the detection of intracavitary abnormalities in
premenopausal women. Ultrasound Obstet Gynecol. 2000;15:
372–376.
90. Richenberg J. Ultrasound of the uterus. In: Callen O, editor. Ultraso-
nography in obstetrics and gynecology. Philadelphia: WB Saunders;
2000: 837.
91. Widrich T, Bradley LD, Mitchinson AR, Collins RL. Comparison
of saline infusion sonography with office hysteroscopy for the evalua-
tion of the endometrium. Am J Obstet Gynecol. 1996;174:1327–1334.
92. O’Connell LP, Fries MH, Zeringue E, Brehm W. Triage of abnormal
postmenopausal bleeding: a comparison of endometrial biopsy and
580 Journal of Minimally Invasive Gynecology, Vol 18, No 5, September/October 2011
transvaginal sonohysterography versus fractional curettage with
hysteroscopy. Am J Obstet Gynecol. 1998;178:956–961.
93. Bettocchi S, Nappi L, Ceci O, Selvaggi L. What does ‘‘diagnostic hys-
teroscopy’’ mean today? The role of the new techniques. Curr Opin
Obstet Gynecol. 2003;15:303–308.
94. Exalto N, Stappers C, van Raamsdonk LAM, Emanuel MH. Gel instil-
lation sonohysterography: first experiencewith a new technique. Fertil
Steril. 2007;87:152–155.
95. Kupesic S, Kurjak A. Septate uterus: detection and prediction of
obstetrical complications by different forms of ultrasonography.
J Ultrasound Med. 1998;17:631–636.
96. Ayida G, Kennedy S, Barlow D, Chamberlain P. Contrast sonography
for uterine cavity assessment: a comparison of conventional two-
dimensional with three-dimensional transvaginal ultrasound; a pilot
study. Fertil Steril. 1996;66:848–850.
97. Makris N, Skartados N, Kalmantis K, Mantzaris G, Papadimitriou A,
Antsaklis A. Evaluation of abnormal uterine bleeding by transvaginal
3-D hysterosonography and diagnostic hysteroscopy. Eur J Gynaecol
Oncol. 2007;28:39–42.
98. Gimpelson RJ, Rappold HO. A comparative study between panoramic
hysteroscopy with directed biopsies and dilatation and curettage. A re-
view of 276 cases. Am J Obstet Gynecol. 1988;158(Pt 1):489–492.
99. Hamou J. Hysteroscopy and micro-colopo-hysteroscopy: text and
atlas. Norwalk: Appleton & Lange; 1991.
100. Clark TJ, Khan KS, Gupta JK. Current practice for the treatment of
benign intrauterine polyps: a national questionnaire survey of consul-
tant gynaecologists in UK. Eur J Obstet Gynecol Reprod Biol. 2002;
103:65–67.
101. Kremer C, Duffy S. A randomised controlled trial comparing transva-
ginal ultrasound, outpatient hysteroscopy and endometrial biopsy with
inpatient hysteroscopy and curettage. BJOG. 2000;107:1058–1059.
102. Agostini A, Bretelle F, Cravello L, Maisonneuve AS, Roger V,
Blanc B. Acceptance of outpatient flexible hysteroscopy by premeno-
pausal and postmenopausal women. J Reproduct Med. 2003;48:
441–443.
103. Kremer C, Barik S, Duffy S. Flexible outpatient hysteroscopy without
anaesthesia: a safe, successful and well tolerated procedure. Br J
Obstet Gynaecol. 1998;105:672–676.
104. Bettocchi S, Ceci O, Nappi L, et al. Operative office hysteroscopy
without anesthesia: analysis of 4863 cases performed with mechanical
instruments. J Am Assoc Gynecol Laparosc. 2004;11:59–61.
105. Nagele F, Bournas N, O’Connor H, Broadbent M, Richardson R,
Magos A. Comparison of carbon dioxide and normal saline for
uterine distension in outpatient hysteroscopy. Fertil Steril. 1996;65:
305–309.
106. Goldfarb HA. Comparison of carbon dioxide with continuous-flow
technique for office hysteroscopy. J Am Assoc Gynecol Laparosc.
1996;3:571–574.
107. van Trotsenburg M, Wieser F, Nagele F. Diagnostic hysteroscopy for
the investigation of abnormal uterine bleeding in premenopausal
patients. Contrib Gynecol Obstet. 2000;20:21–26.
108. Valle RF. Office Hysteroscopy. Clin Obstet Gynecol. 1999;42:
276–289.
109. Jansen FW, Vredevoogd CB, Van Ulzen K, Hermans J, Trimbos JB,
Trimbos-Kemper TCM.Complications of hysteroscopy: a prospective,
multicenter study. Obstet Gynecol. 2000;96:266–270.
110. Grossman J, Ricci ZJ, Rozenblit A, Freeman K, Mazzariol F,
SteinMW. Efficacy of contrast-enhanced CT in assessing the endome-
trium. AJR Am J Roentgenol. 2008;191:664–669.
111. Celik O, Karakas HM, Hascalik S, Tagluk ME. Virtual hysterosalpin-
gography and hysteroscopy: assessment of uterine cavity and fallopian
tubes using 64-detector computed tomography data sets. Fertil Steril.
2010;93:2383–2384.
112. Carrascosa P, Baronio M, Capunay C, et al. Multidetector computed
tomography virtual hysterosalpingography in the investigation of the
uterus and fallopian tubes. Eur J Radiol. 2008;67:531–535.
113. Carrascosa P, Capunay C, Baronio M, et al. 64-Row multidetector
CT virtual hysterosalpingography. Abdominal Imaging. 2009;34:
121–133.
114. Preutthipan S, Herabutya Y. Hysteroscopic polypectomy in 240 pre-
menopausal and postmenopausal women. Fertil Steril. 2005;83:
705–709.
115. Bacsko G,Major T, Csiszar P, Borsos A. Operative hysteroscopy: min-
imally invasive surgery to control of menorrhagia. Acta Chir Hung.
1997;36:7–8.
116. Taskin O, Sadik S, Onoglu A, et al. Role of endometrial suppression on
the frequency of intrauterine adhesions after resectoscopic surgery. J
Am Assoc Gynecol Laparosc. 2000;7:351–354.
117. Henriquez DD, van Dongen H, Wolterbeek R, Jansen FW. Polypec-
tomy in premenopausal women with abnormal uterine bleeding: effec-
tiveness of hysteroscopic removal. J Minim Invasive Gynecol. 2007;
14:59–63.
118. Cravello L, Stolla V, Bretelle F, Roger V, Blanc B. Hysteroscopic
resection of endometrial polyps: a study of 195 cases. Eur J Obstet
Gynecol Reprod Biol. 2000;93:131–134.
119. Stamatellos I, Koutsougeras G, Karamanidis D, Stamatopoulos P,
Timpanidis I, Bontis J. Results after hysteroscopic management of
premenopausal patients with dysfunctional uterine bleeding or intra-
uterine lesions. Clin Exp Obstet Gynecol. 2007;34:35–38.
120. van Dongen H, Emanuel MH, Wolterbeek R, Trimbos JB, Jansen FW.
Hysteroscopic morcellator for removal of intrauterine polyps and my-
omas: a randomized controlled pilot study among residents in training.
J Minim Invasive Gynecol. 2008;15:466–471.
121. Emanuel MH, Wamsteker K. The Intra Uterine Morcellator: a new
hysteroscopic operating technique to remove intrauterine polyps and
myomas. J Minim Invasive Gynecol. 2005;12:62–66.
122. Vilos GA. Intrauterine surgery using a new coaxial bipolar electrode in
normal saline solution (Versapoint): a pilot study. Fertil Steril. 1999;
72:740–743.
123. Mousa HA, Senoun GMSAE, Mahmood TA. Medium-term clini-
cal outcome of women with menorrhagia treated by rollerball
endometrial ablation versus abdominal hysterectomy with conser-
vation of at least one ovary. Acta Obstet Gynecol Scand. 2001;80:
442–446.
124. Apgar BS, Kaufman AH, George-Nwogu U, Kittendorf A. Treatment
of menorrhagia. Am Fam Physician. 2007;75:1813–1819.
125. Vercellini P, Trespidi L, Bramante T, Panazza S, Mauro F,
Crosignani PG. Gonadotropin releasing hormone agonist treatment
before hysteroscopic endometrial resection. Int J Gynecol Obstet.
1994;45:235–239.
126. Oguz S, Sargin A, Kelekci S, Aytan H, Tapisiz OL,
Mollamahmutoglu L. The role of hormone replacement therapy in
endometrial polyp formation. Maturitas. 2005;50:231–236.
127. Gardner FJ, Konje JC, Bell SC, Abrams KR, Brown LJ, Taylor DJ,
et al. Prevention of tamoxifen induced endometrial polyps using
a levonorgestrel releasing intrauterine system long-term follow-up
of a randomised control trial. Gynecol Oncol. 2009;114:452–456.
128. Moghal N. Diagnostic value of endometrial curettage in abnormal
uterine bleedingda histopathological study. J Pak Med Assoc. 1997;
47:295–299.
129. Gebauer G, Hafner A, Siebzehnr€ubl E, Lang N. Role of hysteroscopy
in detection and extraction of endometrial polyps: Results of a prospec-
tive study. Am J Obstet Gynecol. 2001;184:59–63.
130. Loffer FD. Hysteroscopy with selective endometrial sampling com-
pared with D&C for abnormal uterine bleeding: the value of a negative
hysteroscopic view. Obstet Gynecol. 1989;73:16–20.
131. Bettocchi S, Ceci O, Di Venere R, Pansini MV, Pellegrino A,
Marello F, et al. Advanced operative office hysteroscopy without an-
aesthesia: analysis of 501 cases treated with a 5 Fr. bipolar electrode.
Hum Reprod. 2002;17:2435–2438.
132. Sciarra JJ, Valle RF. Hysteroscopy: a clinical experience with 320
patients. Am J Obstet Gynecol. 1977;127:340–348.

Salim et al. Diagnosis and Management of Endometrial Polyps: A Critical Review of the Literature 581
133. Lee C, Ben-Nagi J, Ofili-Yebovi D, Yazbek J, Davies A,
Jurkovic D. A new method of transvaginal ultrasound-guided poly-
pectomy: a feasibility study. Ultrasound Obstet Gynecol. 2006;27:
198–201.
134. Lieng M, Istre O, Sandvik L, Engh V, Qvigstad E. Clinical effective-
ness of transcervical polyp resection in women with endometrial
polyps: randomized controlled trial. J Minim Invasive Gynecol.
2010;17:351–357.
135. Brooks PG, Loffer FD, Serden SP. Resectoscopic removal of symp-
tomatic intrauterine lesions. J Reprod Med. 1989;34:435–437.
136. Nathani F, Clark TJ. Uterine polypectomy in the management of
abnormal uterine bleeding: a systematic review. J Minim Invasive
Gynecol. 2006;13:260–268.
137. Deans R, Abbott J. Review of intrauterine adhesions. J Minim Invasive
Gynecol. 2010;17:555–569.
138. Henriquez DDCA, van Dongen H, Wolterbeek R, Jansen FW. Poly-
pectomy in premenopausal women with abnormal uterine bleeding:
effectiveness of hysteroscopic removal. J Minim Invasive Gynecol.
2007;14:59–63.
139. Spiewankiewicz B, Stelmachow J, Sawicki W, Cendrowski K,
Wypych P, Swiderska K. The effectiveness of hysteroscopic polypec-
tomy in cases of female infertility. Clin Exp Obstet Gynecol. 2003;30:
23–25.
140. Valle RF. Therapeutic hysteroscopy in infertility. Int J Fertil. 1984;29:
143–148.
141. Perez-Medina T, Bajo-Arenas J, Salazar F, Redondo T, Sanfrutos L,
Alvarez P, et al. Endometrial polyps and their implication in the
pregnancy rates of patients undergoing intrauterine insemination:
a prospective, randomized study. Hum Reprod. 2005;20:1632–1635.
142. Hereter L, Carreras O, Pasciial M. Repercusion de la presencia de
polipos endometriales en un cicio de FIV [Spanish]. Prog Obstet
Ginecol. 1998;41:5–7.
143. Isikoglu M, Berkkanoglu M, Senturk Z, Coetzee K, Ozgur K. Endo-
metrial polyps smaller than 1.5 cm do not affect ICSI outcome. Reprod
Biomed Online. 2006;12:199–204.
144. Lass A,Williams G, Abusheikha N, Brinsden P. The effect of endome-
trial polyps on outcomes of in vitro fertilization (IVF) cycles. J Assist
Reprod Genet. 1999;16:410–415.