Diabetic-foot-ulcer Presentation MUST 22

of 161
-
Upload
sedaka-donaldson -
Category
Documents
-
view
215 -
download
0
Transcript of Diabetic-foot-ulcer Presentation MUST 22
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
1/161
Pressure Ulcers
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
2/161
Pressure Ulcers
Definition and Location
Classification
Risk Factors
Prevention
Treatment
Pressure Ulcers treatment for each stage Complications
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
3/161
What is a Pressure Ulcer?
Definition: A pressure ulcer is a localized injuryto the skin or underlying tissue, usually over a bony
prominence, that is a result of pressure or of
pressure combined with shear or friction.
Reported prevalence rates have ranged
from 2.3 percent to 28 percent and reported
incidence rates from 2.2 percent to 23.9percent
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
4/161
What is a Pressure Ulcer?
95% of pressure ulcers develop on the lower body
(about 65% in the pelvic area and 30% in the lower
extremities) 2-6 times greater mortality risk
Effective pressure ulcer treatment best
achieved through interdisciplinary teamapproach
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
5/161
Pressure Ulcers
Location
Pressure ulcers commonly occur over the :
Sacrum
Greater trochanter Ischial tuberosity
Malleolus
Heel
Fibular head
Scapula
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
6/161
Areas of pressure
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
7/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
8/161
Pressure UlcersRisk Factors
Spinal cord injuries
Traumatic brain injury
Neuromuscular disorders Immobility
Malnutrition
Fecal and urinary
incontinence Altered level of
consciousness
Chronic systemic illness
Fractures
Aging skin decreased epidermal
turnover
dermoepidermal junction
flattens
fewer blood vessels
Decreased pain perception
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
9/161
Contributory factors:
Internal/patient-related factors: Systemic disease: metabolic, neurological,
vascular, terminal illness
Reduced mobility or immobility
Sensory impairment
Psychological e.g. depression
Anaemia
Malnutrition
Level of consciousness
Extremes of age
Previous history of pressure damage or poor
skin condition Acute or chronic oedema
Dehydration/fluid status- sweat, incontinence
External factors:Pressure - support surfaces, change of
position
Shear- positioning, mobility
Friction- moving and handling
techniques, patient education,
splinting, casts, positioning
Other factors
- Moisture - incontinence, sweating,
pyrexia, wound exudate
- Medication
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
10/161
Guidelines for Pressure Ulcers
Care
Recognition
Assessment Diagnosis Prevention and Treatment
Monitoring
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
11/161
Recognition Steps
Examine the patients skin thoroughly to
identify existing pressure ulcers
Identify risk factors for developing pressureulcers
Review records/resident interview to
identify previous history of pressure ulcers
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
12/161
Ulcer Type Pathophysiology Location
Diabetic Peripheral neuropathy secondary to
small or large vessel disease in
chronic, uncontrolled diabetes
Usually lower extremities
Ischemic Reduction in blood flow to tissuescaused by coronary artery
disease, diabetes mellitus,
hypertension, hyperlipidemia,
peripheral arterial disease, or
smoking
Usually distal lower extremitiesTips of toes
Pressure Unrelieved pressure resulting in
damage to skin or underlying
tissue
Usually over bony prominences (e.g.,
buttocks, elbows, heels, ischium,
medial and lateral malleolus,sacrum, trochanters)
Venous Venous hypertension resulting from
incompetence of venous valves, post-
phlebitic syndrome, or venous
insufficiency. Tend to be
irregularly shaped
Usually lower leg region
Distinguishing Features of Common
Types of Ulcers
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
13/161
Risk Assessment and Evaluation
Braden Scale
Push Tool
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
14/161
Braden Scale
Sensory Perception 1-4
Moisture 1-4
Physical Activity 1-4 Mobility 1-4
Nutrition 1-4
Friction & Shear 1-3 Score 18+ Low risk
15-18 Mild risk, 13-14 Moderate risk, 10-12
High risk, below 10 Very High Risk
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
15/161
Prevention
Aims
Reduce Pressure and Shearing effects
Reduce Moisture
General Skin Care
Nutrition Co-morbidities
Involve patient, family, caregivers
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
16/161
Prevention Daily skin inspection
Bathing and skin cleaning frequency
Moisturize skin; avoid hot water or harsh
solutions Assess and treat incontinence; use topical barriers
or absorbent padding when needed
Proper re-positioning frequently; q2hrly for thosebed-bound, q1hrly for those in wheelchairs; selfre-positioning every 15 minutes for those inwheelchairs
Avoid manipulating bony prominences
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
17/161
Prevention Practice proper positioning, transferring and turning
techniques to avoid friction and shearing forces; lift
dont shift
Use dry lubricants (cornstarch) or protectivecoverings to reduce friction injury
Institute a rehabilitation program to maintain or
improve mobility/activity status
Consider nutritional supplementation/support for
nutritionally compromised persons
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
18/161
Prevention
Use adjunct devices (air mattresses, limb
padding) where necessary
Use pillows or padding to avoid bony
prominences such as knees from having direct
contact
Elevate the head of the bed no more than 30
unless absolutely necessary
Monitor and document interventions and
outcomes
Have a fixed re ositionin schedule
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
19/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
20/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
21/161
Staging of pressure ulcers
Suspected deep tissue injury Purple or maroon localized area of
discolored intact skin or blood-filled
blister due to damage of underlyingsoft tissue from pressure and/orshear*. The area may be preceded by
tissue that is painful, firm, mushy,boggy, warmer or cooler ascompared to adjacent tissue.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
22/161
Suspected Deep Tissue Injury
Purple or maroon localized area of discolored
intact skin or blood-filled blister due to
damage of underlying soft tissue from pressure
and/or shear.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
23/161
Deep Tissue Injury
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
24/161
Pressure Ulcers on Mucous
Membranes Pressure ulcers can develop on mucous
membranes from pressure exerted by a
medical device in use at the location of theulcer.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
25/161
LAYERS:
g = epitheliumf = lamina propria
e = muscularis mucosa
c = smooth muscle (location specific
presence )
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
26/161
Staging of pressure ulcers
Stage I
Intact skin with non blanchable
redness of a localized area, usuallyover a bony prominence. Darkly
pigmented skin may not have visible
blanching; its color may differ fromthe surrounding area.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
27/161
Stage 1
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
28/161
STAGE I
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
29/161
Stage 1 pressure ulcer on the
foot.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
30/161
Staging of pressure ulcers
Stage II
Partial thickness loss of dermis
presenting as a shallow open ulcer with ared pink ulcer bed, without slough*. May
also present as an intact or
open/ruptured serum-filled blister.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
31/161
STAGE II
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
32/161
Stage 2 pressure ulcer on the ear.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
33/161
Staging of pressure ulcersStage III
Full thickness tissue loss. Subcutaneous fat may be visible but bone,tendon or muscle are not exposed. Slough may be present but does notobscure the depth of tissue loss. May include undermining* andtunneling*.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
34/161
STAGE III
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
35/161
STAGE III
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
36/161
Staging of pressure ulcers
Stage IV
Full thickness tissue loss with
exposed bone, tendon or muscle.Slough or eschar may be presenton some parts of the ulcer bed.
Often include undermining andtunneling..
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
37/161
Grade 4
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
38/161
Staging of pressure ulcers
Unstageable
Full thickness tissue loss in which
the base of the ulcer is covered byslough (yellow, tan, gray, green or
brown) and/or eschar (tan, brown
or black) in the ulcer bed.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
39/161
UNSTAGEABLE
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
40/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
41/161
Pressure Ulcer Prevention Plan,
Documentation and Education of Patient
and CaregiversThe prevention of pressure ulcers incorporates
the interventions below:
I. Minimize or eliminate friction and shear
II. Minimize pressure (off-loading)
III.Support surfaces
IV.Manage moisture
V. Maintain adequate nutrition/hydration
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
42/161
Treatment
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
43/161
Assessment
History and Physical Examination
Assessing Complications
Nutritional Assessment and Management
Pain Assessment and Management
Psychosocial Assessment and Management
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
44/161
Pressure UlcersUlcer care
The four basic components
1. debridement of necrotic tissue as needed on initial and
subsequent assessments
2. cleansing the wound initially and with each dressingchange
3. prevention, diagnosis, and treatment of infection
4. using a dressing that keeps the ulcer bed moist andthe surrounding intact tissue dry
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
45/161
Debridement
Moist, devitalized tissue supports the growth of
pathological organisms.
Therefore, the removal of such tissue favorablyalters the healing environment of a wound.
Removal of devitalized tissue is considered
necessary for wound healing
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
46/161
Adjunctive Therapies
The therapies included :
electrical stimulation
hyperbaric oxygen infrared and ultraviolet light
low-energy laser irradiation
ultrasound
miscellaneous topical agents (including cytokinegrowth factors)
systemic drugs other than antibiotics
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
47/161
Wound Cleansing
Remove necrotic tissue, exudate, and metabolicwastes from the wound.
Minimum of chemical and mechanical trauma. .
Cleanse wounds initially and at each dressingchange
Do not clean ulcer wounds with skin cleansers or
antiseptics Use normal saline for cleansing
Consider whirlpool treatment for ulcers thatcontain thick exudate, slough, or necrotic tissue.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
48/161
Dressings
Keep the ulcer bed continuously moist.
Wet-to-dry dressings should be used only
for debridement
No differences in pressure ulcer healing
outcomes with diverse dressings
Keep the surrounding intact (periulcer) skindry while keeping the ulcer bed moist.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
49/161
Dressings
Control exudate but do not desiccate the
ulcer bed.
Consider caregiver time
Eliminate wound dead space by loosely
filling all cavities with dressing material.
Avoid overpacking the wound.
Monitor dressings applied near the anus
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
50/161
Pressure Ulcers
Treatment for each stage
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
51/161
Stage 1
Intensive implementation of preventive measuresas usual
Polyurethane dressings (transparent) applied every1 to 10 days (Tegaderm)
They are semipermeable films, permeable to watervapor, oxygen and other gases and impermeable towater and bacteria
Most lesions can be expected to heal by 2 weeks
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
52/161
Stage 2
The same as for stage I but
Wound should be inspected for signs of
infection Polyurethane dressings are more effective
and less costly than wet-to-dry dressings(Tegaderm or thin Duoderm )
Wet-to-dry dressings are rarely indicated atthis stage
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
53/161
Stage 3
Remove necrotic material
Small eschar:
Debridement by experienced PCP
Topical application of enzymatic debriding agents
Eschar should be scored
Enzymes must not touch surrounding areas
Large eschar: Surgical consultation
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
54/161
Stage 3
Loose material can be debrided with wet-to-dry
dressings every 8 hours
Polyurethane and hydrocolloid dressings(Duoderm) are more effective
Hydrocolloids are impermeable to gas and
moisture and are changed every 1-4 days
Deeper stage 3 or 4: Wounds need to be packed
with material depending on exudate
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
55/161
Stage 3
Hydrocolloid dressings are not appropriate
Dry wounds:less absorptive Hydrogels or
moist soaks with normal saline
Exudative wounds:Absorptive dressings such
as Hydrophilic foam alginates (Kaltostat ) or
saline impregnated gauze
Packings are changed daily
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
56/161
Stage 3
Consider specialized beds:
air fluidized beds
low-air-loss beds They should be used for at least 60 days
Patients with large defects: surgery consult
Patients with large defects in the sacral area and
urinary incontinence may require catheterization
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
57/161
Stage 4
They require surgical intervention for initialdebridement
Wet-to-dry dressings may help Whirlpool baths may facilitate debridement
Clean deep ulcers require packing
Consider grafting procedures Always keep in mind the goals of the
patient
D i
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
58/161
DressingsDressing Type Description Indication Brand Names
Transparent Film Adhesive, semi-
permeable, allows
vaporization
Stage I and II with
light or no exudates
Opsite, Tegaderm
Hydrogel Water/Glycerin based
gels on gauze ordressings
Stage II, III, IV; deep
ulcers; necrosis &slough
Acryderm, Flexigel,
Intrasite
Alginate From Seaweed Stage III, IV with
moderate to heavy
exudate
Algicell, Algisite,
Tegagen
Foam Moist, thermal
Insulation
Stage II to IV with
varying drainage
Hydrocell, Polyderm
Hydrocolloid Occlusive or
semiocclusive;
gelatin and pectin
Stage II to IV with
sough and necrosis
Dermafilm,
Tegaderm
Moistened Gauze Gauze in saline Stage III to IV
Managing Bacterial Colonization and
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
59/161
Managing Bacterial Colonization and
Infection
Stage 2, 3 and 4 pressure ulcers are invariably
colonized with bacteria.
In most cases, adequate cleansing and debridementprevent bacterial colonization from proceeding to
the point of clinical infection
If purulence or foul odor is present, more frequent
cleansing and possibly debridement are required.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
60/161
Infected Pressure Sore
Managing Bacterial Colonization and
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
61/161
Managing Bacterial Colonization and
Infection
Do not use swab cultures to diagnose woundinfection (colonization)
Consider 2-week trial of topical antibiotics forclean pressure ulcers that are not healing or
producing exudate
Effective against gram negative, positive, andanaerobes
Perform quantitative bacterial cultures of softtissue and evaluate for osteomyelitis when ulcerdoes not respond to topical antibiotic therapy.
Managing Bacterial Colonization and
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
62/161
Managing Bacterial Colonization and
Infection
Systemic antibiotic therapy for patients withbacteremia, sepsis, advancing cellulitis, orosteomyelitis.
Do not use topical antiseptics (povidone iodine,iodophor, Dakins solution, hydrogen peroxide,acetic acid) to reduce bacteria in wound tissue.
Systemic antibiotics are not required for pressureulcers with signs of local infection.
Protect pressure ulcers from exogenous sources ofcontamination
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
63/161
Infection Control
Follow body substance isolation precautions or anequivalent system.
Use clean gloves for each patient.
When treating multiple ulcers on the same patient,attend to the most contaminated ulcer last
Use sterile instruments to debride ulcers
Use clean dressings, rather than sterile ones, totreat pressure ulcers.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
64/161
Operative Repair of Pressure Ulcers
Operative procedures to repair pressureulcers include one or more of the following:
Direct closureSkin grafting
Skin flaps
Musculocutaneous flapsFree flaps.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
65/161
Operative Repair of Pressure Ulcers
Consider for operative repair when clean StageIII-IV do not respond to optimal patient care
Candidates are medically stable, well nourishedand can tolerate operative blood loss and postopimmobility.
Correct factors that may be associated withimpaired healing (smoking, spasticity, levels of
bacterial colonization, incontinence, and UTI)
Minimize pressure to the operative site by use ofspecial beds
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
66/161
Assessment of Ulcer Healing
Evaluate at least weekly
If general condition deteriorates, the ulcer shouldbe reassessed promptly
Evaluate using size, depth, presence of exudate,epithelialization, granulation tissue, necrotictissue, sinus tracts, undermining, tunneling,
purulent drainage or signs of infection.
A clean pressure ulcer with adequate innervationand blood supply should show progress towardhealing in 2 to 4 weeks
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
67/161
Monitoring
Healing ulcers should be assessed regularly
Monitor the individual's general health, nutritional
status, psychosocial support, pain level and bealert to signs of complications
The frequency of monitoring should be
determined by the clinician based on the condition
of the patient, ulcer, rate of healing, and the healthcare setting.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
68/161
Complications
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
69/161
Pressure Ulcers
Complications Amyloidosis
Endocarditis
Heterotopic bone
formation
Maggot infestation
Meningitis
Perineal-urethral fistula
Pseudoaneurysm
Septic arthritis
Sinus tract or abscess
Squamous cell carcinoma
in the ulcer
Systemic complications of
topical treatment
Osteomyelitis
Bacteremia
Advancing cellulitis
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
70/161
Case review
Adult male presented with a Sacral pressure
ulcer, bilateral superficial trochanteric ulcers.
he was manged in a single stage by ulcer
excision and bilateral superior gluteusmaximus V-Y advancement flap coverage. his
post operative period was uneventful.
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
71/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
72/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
73/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
74/161
P Ul S i Q i
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
75/161
Pressure Ulcer Staging Quiz
The test is comprised of 12 pictures of pressure
ulcers.
Question 1
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
76/161
Question 1
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Question 2
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
77/161
Ques o
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 3
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
78/161
Question 3
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
79/161
Question 4
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 4
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
80/161
Question 4
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 5
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
81/161
Question 5
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 6
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
82/161
Question 6
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 7
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
83/161
Question 7
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 8
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
84/161
Question 8
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q ti 9
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
85/161
Question 9
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Q estion 10
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
86/161
Question 10
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Question 10
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
87/161
Question 10
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Question 11
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
88/161
Question 11
Category/Stage I
Category/Stage II
Category/Stage III
Category/Stage IV
Unstageable/Unclassified
Deep Tissue Injury
Question 12
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
89/161
Question 12
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
90/161
DIABETIC FOOT ULCERS
Dr Sedaka Donaldson
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
91/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
92/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
93/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
94/161
CASE M M C
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
95/161
CASE: Mr. M.C.
64 yr-old obese white male, not seen x 12 mo Type 2 DM (15 yrs)
BP (18 yrs)
Dyslipidemia (18 yrs)
CABG (10 yrs ago)
Claudication (today; 25 yds)
Insulin/Metformin/Statin/ARB/Hctz/CCB/ASA
Sore on my left foot, Doc
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
96/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
97/161
CASE: Mr. M.C.
Clinical evaluation of heel ulcer:
Probe reached bone
Extensive subcutaneous abscess
MRI: extensive osteomyelitis
ABI: 0.2
Angiography: severe infrapopliteal, suprapopliteal obstruction
Not amenable to revascularization Uncontrolled infection despite antibiotics/drainage
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
98/161
AMPUTATIONS IN DIABETES
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
99/161
AMPUTATIONS IN DIABETES
Common: Worldwideamputation 2to diabetes q 30 sec.
U.S.A.80,000 amputations/y (2002) Higher rates in men, racial/ethnic minorities
Costly:
$60,000/amputation
$2 billion/y total costs
Lancet 2005; 366:1719 Diabetes Care 2004; 27:1598 Diabetes Care 2003;26:495
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
100/161
AMPUTATIONS IN DIABETES
Tragic: Rule of 50
50% of amputations transfemoral/transtibial level
50% of patients 2ndamputation in 5y
50% of patients Die in
5y
Clinical Care of the Diabetic Foot, 2005
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
101/161
FOOT ULCERS IN DIABETES
Precipitate 85% of amputations: Rule of 15
15% of diabetes patients Foot ulcer in lifetime
15% of foot ulcers Osteomyelitis
15% of foot ulcers Amputation
Clinical Care of the Diabetic Foot, 2005
FOOT ULCERS IN DIABETES
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
102/161
FOOT ULCERS IN DIABETES
Costly: $30,000/ulcer
$9 billion/y total costs
Tragic:
Quality of life: ulcer patient amputation patient Burden of non-weight-bearing as ulcer heals
Lifetime behavioral adaptations to prevent recurrence Fear of recurrent ulcer/amputation
70% ulcer recurrence in 3y
Foot Ankle Int 2005; 26:32, 128 Clin Infect Dis 2004; 39(Suppl 2):S129
S i A i A
PATHOGENESIS OF DIABETIC FOOT ULCER AND AMPUTATION
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
103/161
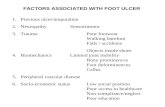
Sensory Joint Motor Autonomic PAD
Neuropathy Mobility Neuropathy Neuropathy
Protective Muscle atrophy and Sweating Ischemia
sensation 2foot deformities 2dry skin
Foot pressure Foot pressure Fissure Healing
Minor trauma esp. overrecognition bony prominences
Callus Pre-ulcer ULCER Infection AMPUTATION
Minor Trauma: Interdigital Maceration
Mechanical (Moisture, Fungus)
Chemical
Thermal
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
104/161
OTHER RISKS FOR ULCER/AMPUTATION
Failure to adequately care for the feet:
Inadequate patient education
Inadequate patient motivation
Depression, anxiety, anger more common in diabetes
Physical disability
Cannot see feet 2to retinopathy
Cannot reach feet 2to obesity, age (?50% of patients)Limited access to medical services
Age Ageing 1992; 21:333 Diabetes Care 2003; 29:495 Diab Metab Res Rev 2004; 20(Suppl 1):S13
CAUSAL PATHWAYS FOR FOOT ULCERS% Causal Pathways
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
105/161
% Causal Pathways
NEUROPATHY Neuropathy: 78%
Minor trauma: 79%DEFORMITY Deformity: 63%
Behavioral issues ?
MINOR TRAUMA
- Mechanical (shoes) POOR SELF-
- Thermal FOOT CARE
- Chemical
ULCER
Diabetes Care 1999; 22:157
DETECTING FEET-AT-RISK History:
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
106/161
History: Prior amputation
Prior foot ulcer PAD: known or claudication at < 1 block
Exam:
Insensate to 5.07/10g monofilament Major foot deformities
PAD Absent DP and PT pulses
Prolonged venous filling time Reduced Ankle-Brachial Index (ABI)
Pre-ulcerative cutaneous pathologyArch Intern Med 1998; 158:157
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
107/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
108/161
PHYSICAL EXAMINATION OF THE FEET
IN PERSONS WITH DIABETES
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
109/161
SENSORY NEUROPATHY IN DIABETES
Loss of protective sensation in feet
Sensory loss sufficient to allow painless skin injury
Major risk factor for foot ulcer in diabetes
Detect with 5.07/10g Semmes-Weinstein monofilament
Prevalence of insensate feet to 10g monofilament: Age > 40y: 30% of diabetic patients
Age > 60y: 50% of diabetic patients
Up to 50% have no neuropathic symptoms
Diabetes Care 2006; 29(Suppl 1):S24 Diabetes Care 2004; 27:1591
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
110/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
111/161
UTILITY OF MONOFILAMENT TESTING
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
112/161
UTILITY OF MONOFILAMENT TESTING
Predicts ulcer/amputation in 5 prospective studies:
NPV (normal sensing) = 90-98%
PPV (fail to sense) = 18-36%
Prospective 32 mo observational study: 80% of ulcers/100% of amputations in insensate feet
Superior predictive value to other tests: Pin prick, cotton wisp, symptoms
? 128 Hz tuning fork? ADA recommendation, 2006: also test vibration
Diabetes Care 2006; 29(Suppl 1):S25 J Fam Pract 2000; 49:S30 Diabetes Care 1992; 15:1386
USING THE 5.07/10gm MF (Tool-Kit)
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
113/161
Demonstrate sensation on
the forearm or hand Place monofilament
perpendicular to test site
Bow into C-shape for onesecond
Test four sites/foot: Predicts95% of ulcer formers vs. 8sites
Heel testing does not
discriminate ulcer formers Avoid calluses, scars, and
ulcers
USING THE 5.07/10g MF (Tool-Kit)
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
114/161
US G . 7/ g ( oo )
Minimize bias: Test sites in random sequences
Test each site X3, sham test as 1 of 3
Do you feel it? Yes or No?
Retest site if patient fails (misses 2/3 responses)
Insensate at 1 site = insensate feet
Falsely insensate with edema, cold feet
Test annually when sensation normal Use < 100x/d; replace if bent; replace q 3 mo.
Purchase calibrated MF (See Tool-Kit)
PAD IN DIABETES
P l (ABI < 0 9) 20 30%
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
115/161
Prevalence(ABI < 0.9): 20-30%
10-20% in type 2 diabetes at Dx
30% in diabetics age 50y
40-60% in diabetics with foot ulcer
Complications: Claudication and functional disability
Increases risk for concurrent CAD and CVD
Delays ulcer healing
Increases amputation risk
Not increase foot ulcer risk
JACC 2006; 47:921 Diabet Med 2005; 22:1310 Diabetes Care 2003; 26:3333
HX TO DETECT PAD IN DIABETES
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
116/161
HX TO DETECT PAD IN DIABETES
Claudication at < 1 block suggests severe ischemiaVascular Level Site of Pain
Aorto-iliac Buttocks/Thigh
Femoral CalfTibioperoneal Foot/Ankle
Rest pain indicates critical ischemia
Toes and forefoot
Difficult to distinguish from neuropathic pain
INTERPRETATION OF THE ABI
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
117/161
ABINormal 0.91-1.30
Mild obstruction 0.71-0.90
*Moderate obstruction 0.41-0.70
*Severe obstruction 0.40
**Poorly compressible >1.30
2to medial Ca++
*Poor ulcer healing with ABI 0.50
**Further vascular evaluation needed
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
118/161
MOTOR NEUROPATHY AND FOOT DEFORMITIES
Hammer toes
Claw toes
Prominent metatarsal heads
Hallux valgus
Collapsed plantar arch
Hammer
Toes
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
119/161
From Levin and Pfeifer, The Uncomplicated Guide
to Diabetes Complications, 2002
Toes
Claw Toes
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
120/161
From Levin and Pfeifer, The Uncomplicated
Guide to Diabetes Complications, 2002
HalluxValgus
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
121/161
From Boulton, et al Diabetic Medicine 1998, 15:508
PRE-ULCER CUTANEOUS PATHOLOGY
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
122/161
PRE ULCER CUTANEOUS PATHOLOGY
Neuropathy inappropriate footwear: Persistent erythema after shoe removal
Callus
Callus with subcutaneous hemorrhage: pre-ulcer
Autonomic neuropathy and secondary dry skin:
Fissure ulceration
Augment callus formation
Poor self-care of the feet:
Interdigital maceration with fungal infection
Nail pathology
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
123/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
124/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
125/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
126/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
127/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
128/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
129/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
130/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
131/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
132/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
133/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
134/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
135/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
136/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
137/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
138/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
139/161
RISK-STRATIFIED FOOTCARE
MANAGEMENT FOR DIABETES PATIENTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
140/161
HIGH RISK: CATEGORY 1-3 PATIENTS
A l h i f t
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
141/161
Annual comprehensive foot exam
Inspect feet at every office visit
Podiatry care stratified to risk level
Intensive patient education
Detect/manage barriers to foot care
Therapeutic footwear, if needed
HIGH RISK: CATEGORY 1 3 PATIENTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
142/161
HIGH RISK: CATEGORY 1-3 PATIENTS
Nursing tasks to facilitate foot exams:
High Risk Feet stickers to each chart (Tool-Kit)
Remove patients shoes/socks
Increases % of foot exams in observational studies
Determine that patient can reach/see soles of feet
Stock 10g monofilament in each room
Consider training to perform 10g monofilament exam
Provide patient education forms
Literacy/language appropriate
Diabetes Care 1983; 6:499 J Gen Intern Med 2003; 18:258
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
143/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
144/161
HIGH RISK: CATEGORY 1-3 PATIENTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
145/161
HIGH RISK: CATEGORY 1-3 PATIENTS
Regular prophylactic podiatry care:
Provide nail and skin care
Assess footwear needs
RCT: 48% RRR for recurrent ulceration
Optimal visit frequency not evidence-based:
Category 1 q 3-6 mo
Category 2 q 2-3 mo
Category 3 q 1-2 mo
Diabetes Care 2003; 26:1691 J Fam Practice 2000; 49(Suppl):S30
HIGH RISK: CATEGORY 1-3 PATIENTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
146/161
HIGH RISK: CATEGORY 1-3 PATIENTS
Intensive patient education:
1care clinician, podiatrist, educator contribute
Reinforce frequentlylow retention documentedPatient to demonstrate self-care knowledge
Questionnaires, tests are available (see Tool-Kit)
Utility:
? Reduced foot ulcer/amputation rates?
Cochrane Database Syst Rev 2005 Jan 25;(1)CD001488 Foot Ankle Int 2005; 26:38
BASIC FOOT CARE CONCEPTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
147/161
BASIC FOOT CARE CONCEPTS
Daily foot inspection
May require mirror, magnification, or caregiver
Educate patient to recognize/report ASAP: Persistent erythema
Enlarging callus
Pre-ulcer (callus with hemorrhage)
BASIC FOOT CARE CONCEPTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
148/161
BASIC FOOT CARE CONCEPTS
Commitment to self-care:
Wash/dry daily
Avoid hot water; dry thoroughly between toes
Lubricate daily (not between toes)
Debride callus/corn to reduce plantar pressure 25%
Avoid sharp instruments, corn plasters
No self-cutting of nails if:
Neuropathy, PAD, poor vision
BASIC FOOT CARE CONCEPTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
149/161
BASIC FOOT CARE CONCEPTS
Protective behaviors:
Avoid temperature extremes
No walking barefoot/stocking-footedAppropriate exercise if sensory neuropathy
Bicycle/swim > walking/treadmill
Inspect shoes for foreign objects
Optimal footwear at all times
FOOT CARE EDUCATION TOOLS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
150/161
FOOT CARE EDUCATION TOOLS
Diabetic Foot Care
American Orthopedic Foot and Ankle Society
Multilingual translation Available in 20 languages
Reference:
EDUCATIONAL DEFICIENCIES:HIGH RISK PATIENTS
558 high risk patients:
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
151/161
558 high risk patients:
Deficiency % DeficientNot inspect feet regularly 50%
Walk barefoot/stockings 62%
Seldom/never test water temp. 40%Trim callus with sharp object 48%
Not know to call ASAP for foot ulcer 58%
Not know how to select footwear 57%
From GE Reiber, 2003
BASIC FOOTWEAR EDUCATION
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
152/161
Avoid:Pointed-toes
Slip-ons
Open-toes
High heels
Plastic
Black color
Too small
Favor:Broad-round toes
Adjustable (laces, buckles,Velcro)
Athletic shoes, walking shoesLeather, canvas
White/light colors
between longest toe and
end of shoe
Diabetes Self-Management 2005; 22:33
THERAPEUTIC FOOTWEAR: GOALS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
153/161
THERAPEUTIC FOOTWEAR: GOALS
Inappropriate footwear:
Contributes to 21-76% of ulcers/amputations
Optimal footwear should:
Protect feet from external injury
Reduce plantar pressure, shock and shear forces
Accommodate, stabilize, support deformities
Suitable for occupation, home, leisure
Diabetes Care 2004; 27:1832 Diab Metab Res Rev 2004; 20(Suppl1):S51
THERAPEUTIC FOOTWEAR: COMPONENTS
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
154/161
Padded socks(eg. CoolMax, Duraspun, others)
Cushion metatarsal heads, heels, and decrease plantarpressure
White, seamless, absorbent acrylic fibers
Shoe inserts/insoles(closed-cell foam, viscoelastic)
Off-the-shelf
Custom-molded
Therapeutic shoes
Extra-depth extra-width
Rigid rocker outsoles
Custom-molded
FOOTWEAR RECOMMENDATIONS BY RISK LEVEL
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
155/161
Low Risk (0) Proper style/fit, cushioned stock shoes
Sensation (1) Deep toe box shoes, cushioned insoles
Callosities, ulcer Hx Extra-depth stock shoes, custom-molded insole
Severe deformities Custom-molded extra-depth shoes and insoles,
rigid rocker outsoles
Modified from The Foot in Diabetes, 2000, p.136
THERAPEUTIC FOOTWEAR: EFFICACY
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
156/161
THERAPEUTIC FOOTWEAR: EFFICACY
Decreases plantar pressure 50-70%
Uncertain reduction in ulcer rate:
1prevention: no data
2prevention: controversial reduction of ulcer recurrence
Analytic/descriptive studies decreases ulcers 50-75%
2 RCTs no benefit
Benefits vary with footwear use, risk level?
Severe foot deformity, prior toe/ray amputation?
Diabetes Care 2004; 27:1774
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
157/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
158/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
159/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
160/161
-
8/13/2019 Diabetic-foot-ulcer Presentation MUST 22
161/161
THANK YOU