Diabetic foot & ankle
19
Diabetic Foot & Ankle Dr. Vijay Kumar Loya JR, JIPMER
-
Upload
vijay-loya -
Category
Health & Medicine
-
view
146 -
download
1
Transcript of Diabetic foot & ankle

Diabetic Foot & Ankle
Dr. Vijay Kumar Loya JR, JIPMER

EPIDEMOLOGY Diabetic foot ulcers were found in 4.54% newly diagnosed patients(Sinharay K et. al, 2012)
Prevalence of DFU is about 14.3% in Indian population (according to a study done in Northern India, Shahi SK et. al)

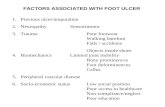
RISK FACTORS
NEUROPATHY
SENSORY
MOTOR
AUTONOMIC
PVD DELAYED BONE HEALING ALTERED IMMUNE FUNCTION

Large sensory fibres – protective sensation is lostSmall fibres can lead to increased pain sensation, allodynia.Sensory disturbances show a length related pattern with stocking & glove distribution due to dying back distal axonopathy Motor neuropathy can cause claw toes from intrinsic muscle weakness & equinus contracture of Achilles tendon→ stress on fore-foot→high focal pressure & skin breakdown.Sweat gland dysfunction allows the skin to dry & crack→microbe entry

DIAGNOSISPHYSICAL EXAMINATIONEMG/NCSLOSS OF PROTECTIVE SENSATION IS THRESHOLD AT WHICH NEUROPATHIC ULCERS/CHARCOT ARTHOPATHY OCCUR

PVD ABI is unreliable in diabetics as calcification can lead to high results masking the severity of disease.
Toe pressure or TcpO2 better indicator. Angiography is gold standard, but requires IV contrast infusion.
ABI >0.45 & TcpO2 >40mm Hg necessary for ulcer to heal.



vijay loya

TREATMENTNON-OPERATIVETCC – TOTAL CONTACT CASTINGREMOVABLE DIABETIC BOOTSNEGATIVE PRESSURE WOUND THERAPYHYPERBARIC WOUND THERAPYEXTRA CORPOREAL SHOCK WAVE TREATMENT



TCC is the gold standard for off-loading of plantar ulcerations.
ii. Patients with grade 3 or greater ulcers should undergo incision and drainage and antibiotic therapy, with wound improvement before TCC application.
iii. Casts should be changed every 2 to 4 weeks until erythema and edema have resolved and the temperature of the affected limb has decreased and become similar to that of the contralateral limb. Ulcers should be evaluated and debridement should be performed at the time of cast changes.
iv. Radiographs should be repeated every 4 to 6 weeks, or more often if there is an acute change.
v. TCC commonly continues for up to 4 months; when the active disease phase is complete, the patient can be fitted with a Charcot restraint orthotic walker, later followed by a custom shoe with orthoses.


OPERATIVE TREATMENT – URGENT SURGICAL INDICATION – NECROTISING FASCITTIS/ GANGRENE/ DEEP ABSCESSLESS URGENT INDICATIONS ARE - COMPROMISED SOFT TISSUE ENVELOPE
NEED TO AVOID PROLNGED ANTIBOTICS LOSS OF MECHANICAL FUNCTION BONE INVOLVEMENT THAT IS LIMB THREATENING

OPERATIVE TREATMENTDEBRIDEMENTEXOSECTOMY OR REALIGNMENT ARTHODESISAMPUTATION AT APPROPRIATE LEVELRESECTION ARTHOPLASTYACHILLES TENDON Z-PLASTY



THANK YOU