Diabetes Prevention for a Heterogeneous Population Richard Arakaki, M.D. Professor of Medicine and...
22
Diabetes Prevention for a Diabetes Prevention for a Heterogeneous Population Heterogeneous Population Richard Arakaki, M.D. Richard Arakaki, M.D. Professor of Medicine and Professor of Medicine and Chief, Division of Endocrinology and Chief, Division of Endocrinology and Metabolism Metabolism John A. Burns School of Medicine John A. Burns School of Medicine September 30, 2011 September 30, 2011
-
Upload
pamela-martin -
Category
Documents
-
view
214 -
download
0
Transcript of Diabetes Prevention for a Heterogeneous Population Richard Arakaki, M.D. Professor of Medicine and...
Diabetes Prevention for a Diabetes Prevention for a Heterogeneous PopulationHeterogeneous Population
Richard Arakaki, M.D.Richard Arakaki, M.D.
Professor of Medicine and Professor of Medicine and
Chief, Division of Endocrinology and MetabolismChief, Division of Endocrinology and Metabolism
John A. Burns School of MedicineJohn A. Burns School of Medicine
September 30, 2011September 30, 2011

Type 2 Diabetes Prevention: Type 2 Diabetes Prevention: A Few QuestionsA Few Questions
• UNEQUIVOCALLY SHOWN TO BE UNEQUIVOCALLY SHOWN TO BE PREVENTED AND/OR DELAYED!PREVENTED AND/OR DELAYED!
• How should we identify people at-risk?How should we identify people at-risk?
• What interventions are appropriate?What interventions are appropriate?
• How do we implement the interventions?How do we implement the interventions?
Da Qing IGT and Diabetes StudyDa Qing IGT and Diabetes StudyDa Qing IGT and Diabetes StudyDa Qing IGT and Diabetes Study
• Screened 110,660 persons in Da Qing, China Screened 110,660 persons in Da Qing, China for IGT for IGT
• Randomized 577 persons with IGT at 33 local Randomized 577 persons with IGT at 33 local health centershealth centers
• Four arm study over 6 years (group Four arm study over 6 years (group intervention for weight loss)intervention for weight loss)– Diet (modest weight reduction due to low BMI)Diet (modest weight reduction due to low BMI)– ExerciseExercise
– Diet + Diet + Exercise– ControlControl
Pan et al. Diabetes Care 1997;20:537-44

Da Qing IGT and Diabetes StudyDa Qing IGT and Diabetes StudyDa Qing IGT and Diabetes StudyDa Qing IGT and Diabetes Study
a Adjusted for BMI and fasting glucosePan et al. Diabetes Care 1997;20:537-44
Intervention 6 yr Incidence of
NIDDM
% reduction from controla
Control 67.7 % - -
Diet 43.8 % 31 % (p<0.03)
Exercise 41.1 % 46 % (p<0.0005)
Diet + Exercise 46.0 % 42 % (p<0.005)
Mean change in BMI for intervention -0.69; Control -0.34
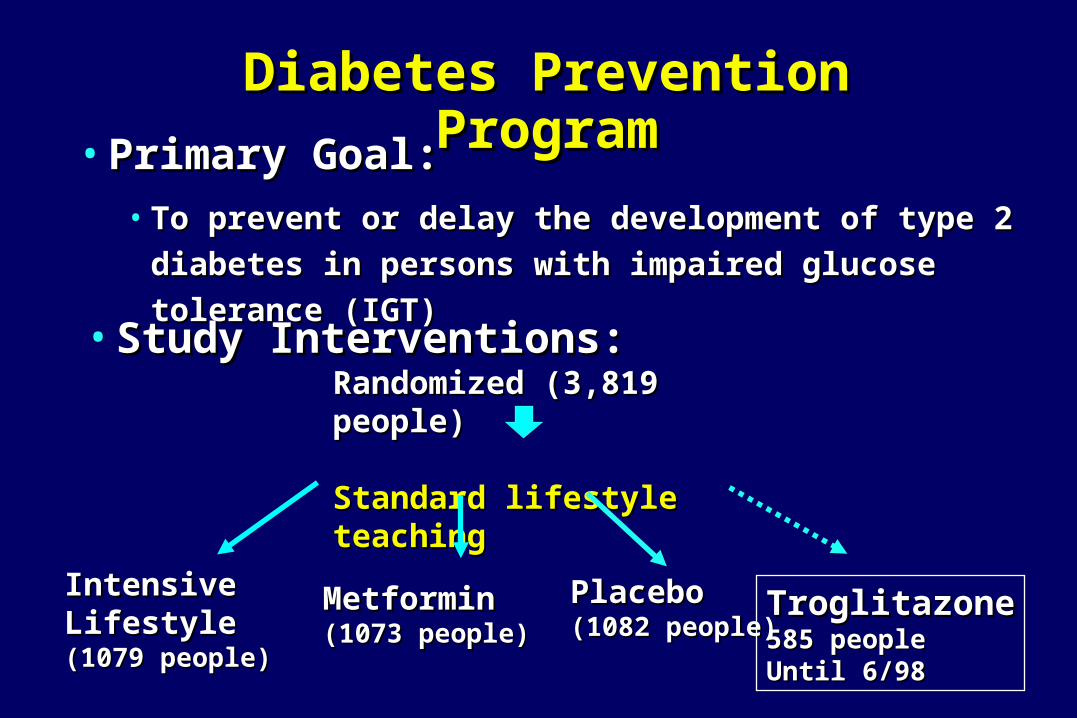
Diabetes Prevention ProgramDiabetes Prevention Program
• Primary Goal: Primary Goal: • To prevent or delay the development of type 2 diabetes in To prevent or delay the development of type 2 diabetes in
persons with impaired glucose tolerance (IGT)persons with impaired glucose tolerance (IGT)
Randomized (3,819 people)Randomized (3,819 people)
Standard lifestyle teachingStandard lifestyle teaching
Intensive Intensive LifestyleLifestyle(1079 people)(1079 people)
MetforminMetformin(1073 people)(1073 people)
PlaceboPlacebo(1082 people)(1082 people)
TroglitazoneTroglitazone585 people585 peopleUntil 6/98Until 6/98
• Study Interventions: Study Interventions:

0 1 2 3 4
0
10
20
30
40Placebo (n=1082)Metformin (n=1073, p<0.001 vs. Plac)Lifestyle (n=1079, p<0.001 vs. Met , p<0.001 vs. Plac )
Percent developing diabetes
All participants
All participants
Years from randomization
Cum
ula
tive in
cidence
(%
)
Placebo (n=1082)
Metformin (n=1073, p<0.001 vs. Placebo)
Lifestyle (n=1079, p<0.001 vs. Metformin , p<0.001 vs. Placebo)
Incidence of Diabetes Incidence of Diabetes
Risk reductionRisk reduction31% by metformin31% by metformin58% by lifestyle58% by lifestyle
N Engl J Med 346:393-403, 2002

Effect of Treatment on Incidence of DiabetesEffect of Treatment on Incidence of Diabetes
PlaceboPlacebo MetforminMetformin LifestyleLifestyle
IncidenceIncidence of diabetes 11.0% 7.8% of diabetes 11.0% 7.8% 4.8% 4.8%
(percent per year)(percent per year)
ReductionReduction in incidence in incidence -------- 31%31% 58%58%
compared with placebo/metformincompared with placebo/metformin 39%39%
Number needed to treatNumber needed to treat -------- 13.9 13.9 6.9 6.9
to prevent 1 case in 3 yearsto prevent 1 case in 3 years
N Engl J Med 346:393-403, 2002

Diabetes Incidence Rates by EthnicityDiabetes Incidence Rates by Ethnicity
0
4
8
12
Caucasian(n=1768)
AfricanAmerican(n=645)
Hispanic(n=508)
AmericanIndian
(n=171)
Asian/PI(n=142)
Cases/1
00 p
ers
on
-yr
Lifestyle Metformin Placebo
N Engl J Med 346:393-403, 2002
71%
51%
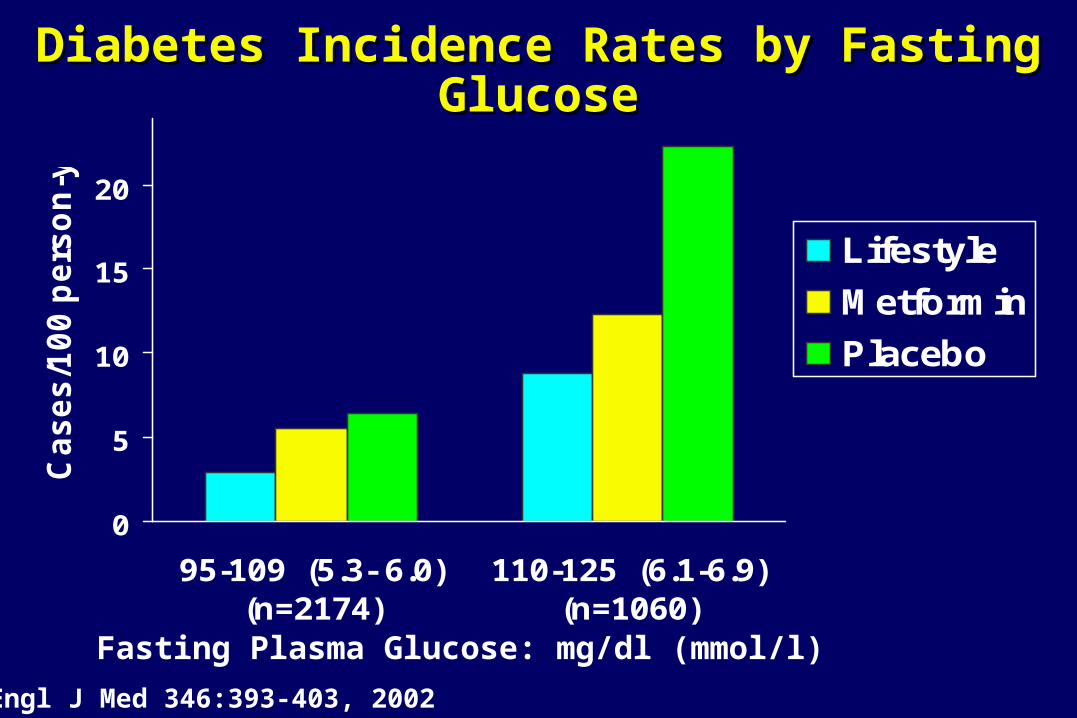
0
5
10
15
20
95-109 (5.3- 6.0)(n=2174)
110-125 (6.1-6.9)(n=1060)
Ca
se
s/1
00
pe
rso
n-y
r
Lifestyle
Metformin
Placebo
Diabetes Incidence Rates by Fasting GlucoseDiabetes Incidence Rates by Fasting Glucose
Fasting Plasma Glucose: mg/dl (mmol/l)
N Engl J Med 346:393-403, 2002

0
4
8
12
16
140-153(n=1049)
154-172(n=1103)
173-199(n=1082)
Ca
se
s/1
00
pe
rso
n-y
r
Lifestyle Metformin Placebo
Diabetes Incidence Rates by 2-hr GlucoseDiabetes Incidence Rates by 2-hr Glucose
2-Hour Plasma Glucose (mg/dl)
N Engl J Med 346:393-403, 2002
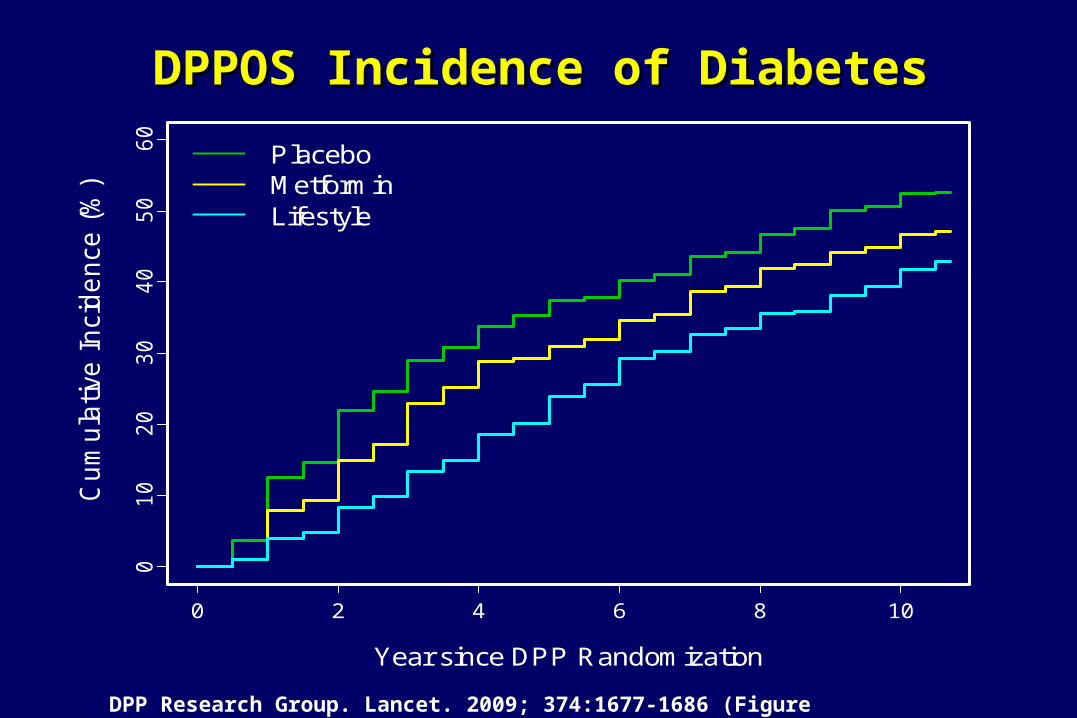
DPPOS Incidence of DiabetesDPPOS Incidence of Diabetes
0 2 4 6 8 10
01
02
03
04
05
06
0
Year since DPP Randomization
Cu
mu
lativ
e I
nci
de
nce
(%
)A. All Participants
PlaceboMetforminLifestyle
DPP Research Group. Lancet. 2009; 374:1677-1686 (Figure 4)

DPPOS Diabetes Risk Reduction
• Delay in diabetes onset after 10 years follow-up:–4 years for Lifestyle; 34% lower risk–2 years for Metformin; 18% lower risk
• The key factors for lower rate of diabetes development for lifestyle and metformin.
–Weight loss is the predominant factor; 16% RR per kg weight loss
–Metformin compliance

Summary of Treatment EffectsSummary of Treatment Effects
• Lifestyle intervention was beneficial regardless of ethnicity, age, BMI, or sex
• The efficacy of lifestyle relative to metformin was greater in older persons and in those with lower BMI
• The efficacy of metformin relative to placebo was greater in those with higher baseline fasting glucose and BMI

Li et al. Lancet 2008;317:1783-89
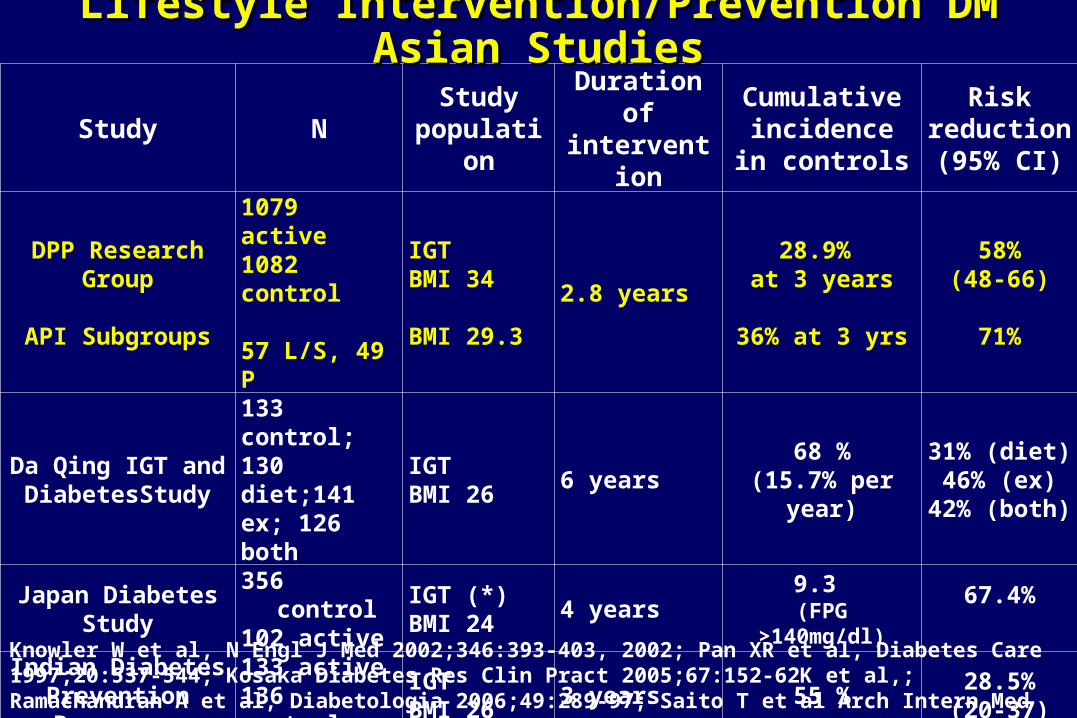
Cumulative incidence of DM during follow-up in Cumulative incidence of DM during follow-up in China Da Qing Diabetes Prevention Outcome StudyChina Da Qing Diabetes Prevention Outcome Study
Study NStudy
populationDuration of intervention
Cumulative incidence in
controls
Risk reduction(95% CI)
DPP Research Group
API Subgroups
1079 active1082 control
57 L/S, 49 P
IGTBMI 34
BMI 29.3
2.8 years
28.9% at 3 years
36% at 3 yrs
58%(48-66)
71%
Da Qing IGT and DiabetesStudy
133 control;130 diet;141 ex; 126 both
IGT BMI 26
6 years68 %
(15.7% per year)
31% (diet)46% (ex)
42% (both)
Japan Diabetes Study
356 control102 active
IGT (*)BMI 24
4 years 9.3 (FPG >140mg/dl)
67.4%
Indian Diabetes Prevention Programme
133 active136 control
IGTBMI 26
3 years 55 %28.5%(20-37)
Zensharen Study330 control311 active
IFG, IGTBMI 27
3 years 16.6 % 44%
Lifestyle Intervention/Prevention DM Asian StudiesLifestyle Intervention/Prevention DM Asian Studies
Knowler W et al, N Engl J Med 2002;346:393-403, 2002; Pan XR et al, Diabetes Care 1997;20:537-544; Kosaka Diabetes Res Clin Pract 2005;67:152-62K et al,; Ramachandran A et al, Diabetologia 2006;49:289-97; Saito T et al Arch Intern Med 2011;171:1352-60.
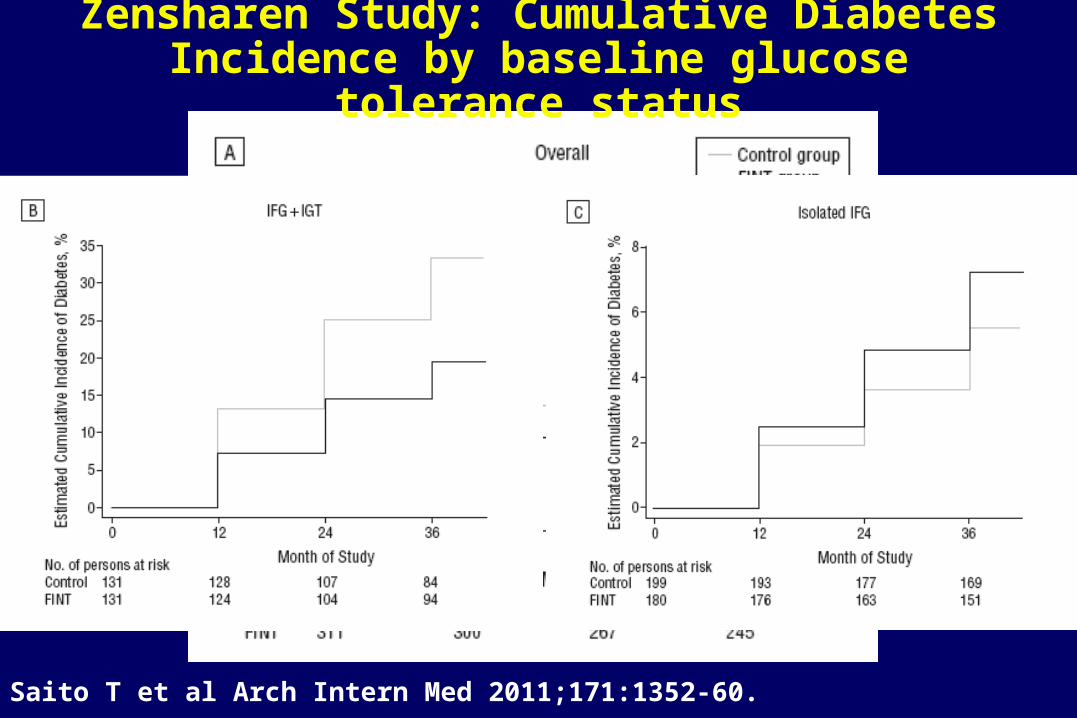
Saito T et al Arch Intern Med 2011;171:1352-60.
Zensharen Study: Cumulative Diabetes Incidence by baseline glucose tolerance status
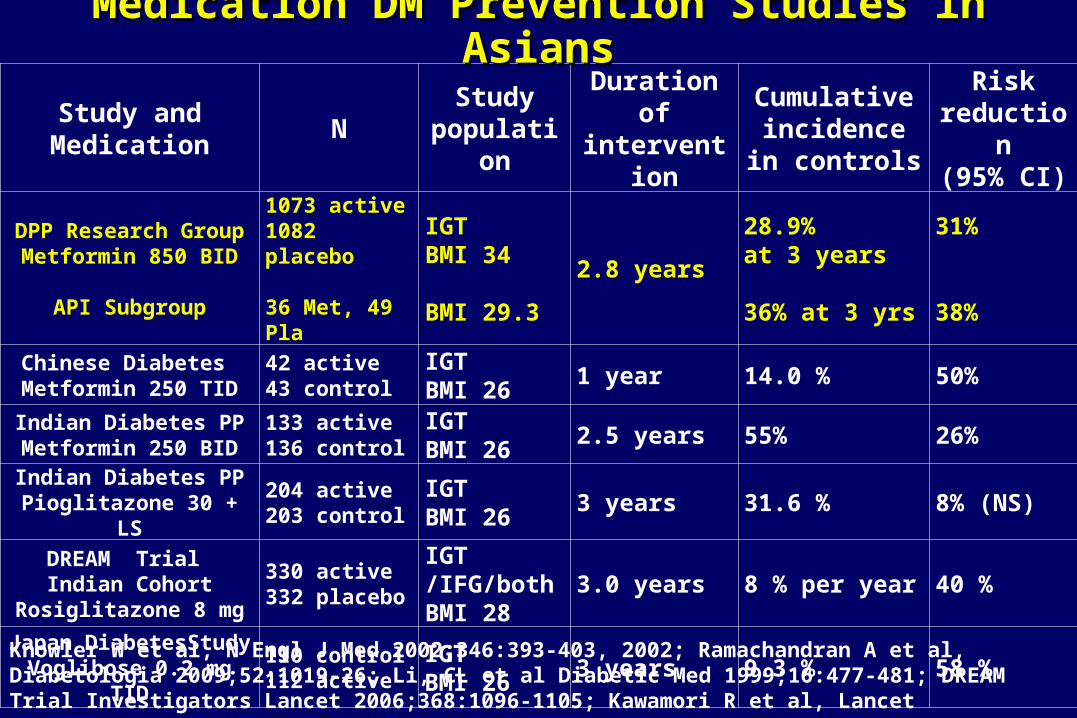
Study and Medication
NStudy
populationDuration of intervention
Cumulative incidence in
controls
Risk reduction(95% CI)
DPP Research GroupMetformin 850 BID
API Subgroup
1073 active1082 placebo
36 Met, 49 Pla
IGTBMI 34
BMI 29.3
2.8 years
28.9% at 3 years
36% at 3 yrs
31%
38%Chinese Diabetes Metformin 250 TID
42 active43 control
IGTBMI 26
1 year 14.0 % 50%
Indian Diabetes PPMetformin 250 BID
133 active136 control
IGTBMI 26
2.5 years 55% 26%
Indian Diabetes PPPioglitazone 30 + LS
204 active203 control
IGTBMI 26
3 years 31.6 % 8% (NS)
DREAM Trial Indian Cohort
Rosiglitazone 8 mg
330 active332 placebo
IGT /IFG/bothBMI 28
3.0 years 8 % per year 40 %
Japan DiabetesStudyVoglibose 0.2 mg TID
110 control112 active
IGTBMI 26
3 years 9.3 % 58 %
Knowler W et al, N Engl J Med 2002;346:393-403, 2002; Ramachandran A et al, Diabetologia 2009;52:1019-26; Li, CL et al Diabetic Med 1999;16:477-481; DREAM Trial Investigators Lancet 2006;368:1096-1105; Kawamori R et al, Lancet 2009;373:1607-14.
Medication DM Prevention Studies in AsiansMedication DM Prevention Studies in Asians

10% Estimate of diabetes associated with known genetic risk (Jablonski K et al Diabetes 2010)Primarily related to beta-cell function
Overall genetic markers (SNPs by GWAS) associated with increased rates of DM are similar across all ethnic groups (Europeans, Asians, etc; Tan JT et al, J Clin Endocrinol Metab 2010;95:390-397).
Allele frequency may reduce usefulness of SNPs for screening at-risk individuals
TCF7L2 Polymorphisms and progression to diabetes in the Diabetes Prevention Program (N Engl J Med, July 2006); high risk SNP but still responsive to lifestyle
intervention
Genetics Risk for Diabetes
Type 2 Diabetes Prevention: Type 2 Diabetes Prevention: A Few Answers?A Few Answers?
• How should we identify people at-risk?How should we identify people at-risk?
• Pathophysiologic and physical characteristics • low insulinogenic index (beta cell function) • high HOMA IR (insulin resistance)• higher BS levels; fasting > 110 mg/dl;
A1c>6.0%• Zensharen Study- need for OGTT
• GWAS; look for multiple SNPs, additive risk

Type 2 Diabetes Prevention: Type 2 Diabetes Prevention: A Few Answers?A Few Answers?
• What interventions are appropriate?What interventions are appropriate?• ANY effective Weight loss interventions
• Lower BMI group• More weight loss-greater effect
• Effective Exercise interventions• 150 min/week or more?
• Medications • Metformin 250 BID/TID (lower doses)• TZDs at high dose• Alpha-glucosidase inhibitors-preferred?Alpha-glucosidase inhibitors-preferred?
Type 2 Diabetes Prevention: Type 2 Diabetes Prevention: A Few Answers?A Few Answers?
• How do we implement the interventions?How do we implement the interventions?
• Community-Based Interventions• Physicians/physician’s groups• Medicare/ Other Insurers• Government-Federal/State
• Are we even there yet?

Thank you for your attentionThank you for your attention