Diabetes in Pregnancy Guidelines: Maternal Aspects...1 Diabetes in Pregnancy Guidelines: Maternal...
36
1 Diabetes in Pregnancy Guidelines: Maternal Aspects The European Association of Perintal Medicince Working group on diabetes in pregnancy Eran Hadar 1 , MD. Eran Ashwal 1 , MD and Moshe Hod 1 , MD. 1. Helen Schneider Hospital for Women, Rabin Medical Center, Petach-Tiqva, Israel. Updated: 22.12.2013
Transcript of Diabetes in Pregnancy Guidelines: Maternal Aspects...1 Diabetes in Pregnancy Guidelines: Maternal...

1
Diabetes in Pregnancy Guidelines: Maternal Aspects
The European Association of Perintal Medicince
Working group on diabetes in pregnancy
Eran Hadar1, MD. Eran Ashwal1, MD and Moshe Hod1, MD.
1. Helen Schneider Hospital for Women, Rabin Medical Center, Petach-Tiqva, Israel.
Updated: 22.12.2013

2
Contents
1. Method of Development of Evidence-Based Clinical Practice Guidelines ............................3
2. Introduction and Background ...............................................................................................4
2.1. Types of Diabetes ..................................................................................................................... 4
2.2. Pathophysiology and Pathogenesis........................................................................................... 4
3. Gestational Diabetes Mellitus ...............................................................................................7
3.1. Epidemiology of GDM .............................................................................................................. 7
3.2. Fetal and Maternal Morbidity associated with GDM ................................................................. 7
3.3. Diagnosis of GDM ..................................................................................................................... 8
3.4. Classification of GDM ............................................................................................................. 11
4. Pre-gestational Diabetes Mellitus ....................................................................................... 12
4.1. Epidemiology of Pre-Gestational diabetes mellitus ................................................................. 12
4.2. Classification of Pre-Gestational diabetes mellitus.................................................................. 12
4.3. Pre-Pregnancy Evaluation for Women with Pre-Gestational Diabetes Mellitus ....................... 14
5. Prenatal care for women with diabetes during Pregnancy ................................................... 16
5.1. Glucose measurements .......................................................................................................... 16
5.2. Goals of treatment ................................................................................................................. 17
5.3. Fetal Growth Assesment ........................................................................................................ 18
5.4. Fetal Wellbeing ...................................................................................................................... 19
6. Treatment of hyperglycemia during pregnancy ................................................................... 20
6.1. Diet ........................................................................................................................................ 20
6.2. Glyburide ............................................................................................................................... 21
6.3. Insulin .................................................................................................................................... 22
7. Labor and Delivery ............................................................................................................ 23
7.1. Glucose monitoring during labor ............................................................................................ 23
7.2. Timing and Mode of delivery .................................................................................................. 24
8. Post Partum Care ............................................................................................................... 26
8.1. Post partum Glucose testing .................................................................................................. 26
8.2. Breastfeeting ......................................................................................................................... 27
8.3. Contraception ........................................................................................................................ 27
9. References ......................................................................................................................... 28

3
1. Method of Development of Evidence-Based Clinical Practice Guidelines
In updating the current version of these guidelines we followed the the proposed GRADE
system for Grading of Recommendations, Assessment, Development and Evaluation (1). This
system uses consistent language and graphical descriptions for the strength and quality of the
recommendations and the evidence on which it is based. Strong recommendations are
numbered as 1 and weak recommendations are numbered 2. For the quality of evidence, cross-
filled circles are used - OOO denotes very low quality evidence; OO low quality; O
moderate quality; and high quality of evidence.

4
2. Introduction and Background
Remarkable advances have been made in recent years, in clarifying the metabolic processes
that occur during pregnancy and their effect on intrauterine fetal development. Consequently,
clinicians have become increasingly aware of the compelling need to properly identify and
manage states associated with metabolic dysfunctions in pregnancy, the most important of
which is abbarant glucose metabolism, universly addressed as diabetes mellitus.
2.1. Types of Diabetes
Diabetes in pregnancy is divided into two types, the one that occurs during pregnancy and the
one that preceeds it. Distinguishing between those two types, is highly important as each has a
different impact on the course and outcome of pregnancy, as well as on maternal
consequences, fetal wellbing and development and long term consequences. Gestational
diabetes mellitus (GDM) usually appears in the second half of pregnancy and affects mainly
fetal growth rate, and may be associated with long-term effects, both for the newborn and the
mother. Pre-gestational diabetes mellitus (Pre-GDM or Overt Diabetes) includes Type 1, Type 2
or Maturity Onset Diabetes of the Young (MODY). It is potentially more serious, as it is present
before pregnancy, so that fetal effects begin already at fertilization and implantation, during
the embroyanl phase and continue throughout pregnancy. Hence, organogenesis may be
disrupted, leading to a high risk of early abortion, congenital anomalies as well as the smae
implications for abarrent growth and long term sequela. Maternal manifestations may also be
more hazardous, especially in the presence of vascular complications such as retinopathy or
nephropathy.
2.2. Pathophysiology and Pathogenesis
Pregnancy is a metabolic challenge that places considerable demands for insulin to meet the
increasing demands of maternal and fetal metabolism. If the threshold is surpassed maternal
hyperglycaemia may occur. In the mildest form - that of women with gestational diabetes and
normal fasting blood glucose - these changes arise predominantly in the “fed” state. During this
phase, postprandial fluctuations of virtually every maternal fuel are exaggerated. As the insulin

5
demands become progressively compromised, hyperglycaemia occurs in association with
further increases in postprandial fuel changes. At the extreme end of the spectrum of the
insulin deficiency effect are women with insulin-dependent diabetes and no insulin secretion,
who are totally dependent on exogenous insulin for metabolic control. Thus, the entire range of
maternal diabetes is expressed by quantitative and/or qualitative changes in the maternal fuel
mixer and reflecting upon the metabolic environment of the conceptus.
Fetal implications: Growth and development of the human conceptus occur within the
metabolic milieu provided by the mother and are ultimately dependent upon circulating
maternal fuels and tissue building blocks. An increasing body of evidence supports the
hypothesis that the abnormal gestational environment of the diabetic mother may imprint on
certain fetal developing tissues and organs, eventually leading to permanent long-term
implications for postnatal function. The fetal tissues most likely to be affected are neural cells,
adipocytes, muscle cells and pancreatic cells. Freinkel introduced the concept of pregnancy as
a “tissue culture experiment”, in which the placenta and the fetus develop in an “incubating
medium” totally derived from maternal fuels. All these fuels, glucose, amino acids, lipids, etc.,
traverse the placenta in a concentration-dependent fashion and thus contribute to the fetal
milieu. Since all these constituents are regulated by maternal insulin, disturbances in its supply
or actions will influence the whole nutritional content to which the fetus is exposed and,
eventually, lead to fetal hyperinsulinaemia. According to Freinkel’s hypothesis, the abnormal
maternal mixture of metabolites gains access to the developing fetus in utero, modifying the
phenotypic gene expression in newly-formed cells, which in turn may determine permanent,
short- and long-term effects in the offspring. Depending upon the time of embryo-fetus
exposure to the aberrant fuel mixture, different events may develop. Early in the first trimester,
intrauterine growth restriction and organ malformation, described by Freinkel as “fuel-
mediated teratogenesis” may happen. During the second trimester, at the time of brain
development and differentiation, behavioural, intellectual or psychological damage may occur.
During the third trimester, the abnormal proliferation of fetal adipocytes and muscle cells,

6
together with pancreatic cells and neuroendocrine cells hyperplasia may be responsible for
the development of obesity, hypertension and non-insulin diabetes mellitus later in life.
Maternal implications: Until the discovery of insulin by Banting and Best in 1921, very few
women with diabetes became pregnant spontaneously, and even fewer achieved a successful
pregnancy outcome. At that time, about 50% of women died during pregnancy from diabetes-
related complications (mainly ketoacidosis) and about 50% of the fetuses failed to develop in
utero. Diabetic women have a markedly higher risk for a number of pregnancy adverse events,
including spontaneous abortion, preterm labour, recurrent genital and urinary tract infections,
pyelonephritis, polyhydramnios, hypertensive disorders, traumatic birth and hyper- and hypo-
glycemic events. These complications, together with the increased rate of vascular alteration
(retinopathy and nephropathy), contribute to higher maternal morbidity and mortality among
diabetic patients. Also, hyperglycemia during pregnancy is associated with a high risk of
developing diabetes in later life. Currently, women with diabetic pregnancy today are enjoying
the benefits of the extraordinary progress made in all areas of medicine in general and in
obstetrics in particular. State-of the art tools have been developed for diagnosis, treatment
and follow-up of both mother and fetus, such as fetal heart rate monitors, ultrasonography,
glucose self-monitors and insulin pumps. As a result, leading medical centres worldwide report
a major reduction in maternal and fetal complications of diabetic pregnancy to levels similar to
those in normal pregnancy. Clinicians today recognize unequivocally that early diagnosis,
adequate treatment, and close follow-up are essential to eliminate most complications of
diabetic pregnancy and achieve a successful outcome.

7
3. Gestational Diabetes Mellitus
Untill recently, gestational Diabetes Mellitus (GDM) was defined as any carbohydrate
intolerance first diagnosed during pregnancy (2). This definition was altered in order to allow a
diagnosis of overt (or pregestational diabetes) to be made during pregnancy. Thus, the current
definition of GDM is: "Diabetes diagnosed during pregnancy that is not clearly overt
diabetes"(3).
3.1. Epidemiology of GDM
The estimated incidence of GDM in Europe ranges from 8% to 10%. The occurrence of GDM
parallels the prevalence of type 2 diabetes in a given population, both of which are in the rise
during recent years. The prevalence of GDM, and the occurrence of related complications,
depends upon the definition of normal glucose values during gestation (4).
3.2. Fetal and Maternal Morbidity associated with GDM
GDM is associated with a higher incidence of maternal morbidity, including - cesarean
deliveries, birth trauma and long term post partum type 2 Diabetes. Perinatal and neonatal
morbidity is also increased, with implications including: macrosomia, birth injury, shoulder
dystocia, hypoglycemia, polycythemia and bilirubinemia. Long term sequela of in utero
exposure to hyperglycemia may include a higher risk for obesity and diabetes later in life. Table
1 lists the implications of GDM for mother, fetus and the newborn as a child and adult (5-12).

8
Table 1: Fetal and Maternal morbidity
1. Fetal
a. Miscarriage
b. Fetal demise
c. Polyhydramnios
d. Preterm labor
2. Maternal
a. Hypertensive diseases
b. Recurrent genital and urinary tract infections
c. Traumatic labour
d. Instrumental delivery or caesarean section
e. Full blown diabetes in the future
3. Neonatal
a. Respiratory Distress Syndrome
b. Hypoglycemia
c. Hypocalcemia
d. Hyperbilirubinemia and Polycythemia
e. Cardiomyopathy
3.3. Diagnosis of GDM
The diagnostic criteria for GDM were first established more than 40 years ago by O’sullivan and
Mahan (13). These criteria were established using non-pregnant values and were designed to
predict the future occurrence of maternal type 2 diabetes. Since then, the classification,
diagnosis, and treatment of GDM have been based on the recommendations of the
International Workshop-Conference on Gestational Diabetes Mellitus (14). As of 2007, five such
international meetings had been held and their recommendations were adopted by major
medical institutions in Europe and America (American College of Obstetrics and Gynecology,
American Diabetes Association, European Association for the Study of Diabetes). These widely
used criteria are still controversial mainly because they lack correlation to perinatal outcome.
The other widely used set of criteria are those of the World Health Organization (WHO), which

9
are based on values of impaired glucose tolerance, also established for a non-pregnant
population (15). To resolve the above mentioned controversies, and set the evidence base for
GDM diagnosjs, the hyperglycemia and adverse pregnancy outcome study (HAPO) was
executed (16-18). Approximately 25,000 pregnant women at about 28 weeks of gestation were
tested for fasting plasma glucose, followed by a 75g oral glucose tolerance test (OGTT) and
glucose measurements at 1 and 2 hours post glucose intake. The results of the HAPO study
demonstrate a linear association between increasing levels of fasting, 1-hour and 2-hour
plasma glucose post a 75g OGTT, to birth weight above the 90th percentile, cord blood serum C-
peptide level above the 90th percentile, primary cesarean delivery, clinical neonatal
hypoglycemia, premature delivery, shoulder dystocia or birth injury, intensive neonatal care
admission, hyperbilirubinemia and pre-eclampsia.
Based on the realization that there is no apparent glucose cutoff, but rather a continuum of
glucose levels, these results were interperted to develop perinatal outcome based standards to
diagnose diabetes during pregnancy. The International Association of Diabetes and Pregnancy
Study Groups (IADPSG) has published the newest recommendations for the diagnosis of GDM
and Overt DM during pregnancy (19), which are partly based on the findings of the HAPO study.
These guidelines are summarized in table 2. Thresholds for diagnosis of overt diabetes during
pregnancy are summerized in Table 3, and threshold for GDM diagnosis in table 4. The novel
approach in the IADPSG suggested criteria is that overt diabetes can also be diagnosed during
pregnancy, and that the criteria are evidence based on the HAPO study results.

10
Table 2: Strategy for the detection and diagnosis of hyperglycemia disorder in pregnancy
In the First Prenatal Visit: Measure Fasting Plasma Glucose, Hemoglobin A1C or Random Plasma Glucose, on all
or high risk:
If results indicate overt diabetes as per table 5 Pre-existing diabetes
If results not diagnostic of overt diabetes as per table 5, and FPG 5.1-7.0 mmol/L (92-126mg/dl) GDM
If results not diagnostic of overt diabetes as per table 5 and fasting plasma glucose < 5.1mmol/L (92mg/dl)
Preform a 75g OGTT at 24-28 weeks of gestation
24-28 weeks of gestation: Perform a 75g OGTT on all women not previously diagnosed with overt diabetes or
GDM:
If fasting plasma glucose ≥ 7.0 mmol/L (126 mg/dl) Pre-existing diabetes
If one or more values equals or exceeds thresholds as per table 6 GDM
If all values less than thresholds indicated as per table 6 Normal
Table 3: Threshold Values for diagnosis of Overt diabetes in pregnancy
Measure of Glycemia Threshold Remarks
Fasting Plasma
Glucose
≥ 7.0 mmol/L ≥ 126 mg/dl
Hemoglobin A1C ≥ 6.5% DCCT/UKPDS Standardized
Random Plasma
Glucose
≥ 11.1
mmol/L
≥ 200 mg/dl Conform diadnosis of overt diabetes by FFPG or
hemoglobin A1C
Table 4: Threshold Values for diagnosis of GDM
Glucose Measure Glucose Threshold
Mmol/L mg/dl
Fasting Plasma Glucose 5.1 92
1 Hour Post 75g OGTT 10.0 180
1 Hour Post 75g OGTT 8.5 153

11
Shortly, at the first prenatal visit, all or only high-risk women (based on the background
frequency of abnormal glucose metabolism in the population and on local circumstances)
should undergo testing for fasting plasma glucose (FPG), hemoglobin A1C, or random plasma
glucose (RPG). Criteria for low risk include: Absence of diabetes in first-degree relatives, Age<25
years, Normal pre-pregnancy weight, No history of poor carbohydrate metabolism, No history
of adverse pregnancy outcome. Criteria for high risk women for diabetes include: Pre-
pregnancy obesity, Family history of type 2 diabetes mellitus, GDM in a past pregnancy and
Known carbohydrate intolerance or glycosuria. If testing is negative for both GDM and overt
diabtets, a 75g OGTT should be performed after overnight fast at 24-28 weeks of gestation.
Recomendation (1): Diagnosis of GDM Strength & Quality
In the first prenatal visit, universal or risk based testing for diabetes should be
preformed with either: FPG, HbA1C or RPG (Diagnostic values are depicted in table 5) 1|OOO
If GDM or Overt diabtes have not been diagnosed at the first prenatal visit, a 2 hour 75g
OGTT should be performed at 24-28 weeks (Diagnostic values are depicted in table 6) 1|O
3.4. Classification of GDM
GDM is grouped on the basis of the fasting blood glucose level and mode of treatment (Table
6). A fasting level below 95 mg/dl (5.3 mmol/l) requires only dietary management and is
designated A1, and if above it is treated with diet and oral medication or insulin and is
designated A2 (20).
Table 5: Classification of GDM
Group Fasting Glucose 2-hr Postprandial glucose Treatment
A1 <95 mg/dl (5.3 mmol/l) <120 mg/dl (<6.7 mmol/l) Diet only
A2 >95 mg/dl (5.3 mmol/l) >120 mg/dl (6.7 mmol/l) Diet and oral hypoglyecmics or insulin

12
4. Pre-gestational Diabetes Mellitus
Metabolic changes in the pregnant mother also affect her child – in utero and thereafter, in
infancy, childhood and even adulthood. Many researchers are attempting to define and
describe the known obstetric risks and complications associated with maternal diabetes, the
underlying pathophysiology of the disease, and the manner in which hyperglycemia affects
these processes. Some of the recent improvement noted in the health of infants of diabetic
women derives from the advances made in the understanding of the disease, in monitoring
techniques, and in neonatal and paediatric medicine. However, for the most part it is due to
prevention by means of good maternal metabolic regulation. Careful control of glucose levels
for several months before conception can usually lower the risk of complications during
pregnancy and delivery, in some cases to within the range of the normal population. Today,
glucose analyzers are available for home use to enable self-regulation by women at risk.
Clinicians can then combine these daily measures with monthly measurement of glycosylated
haemoglobin (HbA1c) levels for precise and continuous surveillance. Together, the physician-
patient team can achieve maximum balance and lower fetal and neonatal morbidity and
mortality rates. It is essential to bring these issues to the awareness of all physicians so that
diabetic women of reproductive age will be referred to the appropriate clinics before
pregnancy. There, they will learn about the importance of glucose regulation already before
conception, and during pregnancy and delivery.
4.1. Epidemiology of Pre-Gestational diabetes mellitus
About 10% of all diabetic women have PreDM, that is, about 0.3 to 0.5% of all pregnant
women.
4.2. Classification of Pre-Gestational diabetes mellitus
In 1997, the American Diabetes Association (ADA) published new criteria for the classification
and diagnosis of diabetes mellitus to replace those in effect since 1979. The terms insulin-
dependent diabetes mellitus (IDDM) and non-insulin dependent diabetes (NIDDM) were
eliminated because they often led to misclassifications on the basis of the treatment

13
administered rather than the underlying cause. The new ADA classification differentiates four
clinical groups of diabetes mellitus: Type 1 diabetes, Type 2 diabetes, other specific types and
Gestational diabetes mellitus. Also, intermediate states, which are characterized by glucose
levels ranging between normal to the lower limit of diabetic values, are divided into two types:
Impaired fasting glucose (IFG) and impaired glucose tolerance (IGT)
PreGDM is also grouped on the basis of age at onset, duration of disease, and presence of
vascular complications – all direct prognostic factors for mother and fetus in the course of
pregnancy.
Table 6: Classification of Pre-GDM
Group Age at onset (yr) Duration of disease (yr) Vascular complication Treatment
B Over 20 Less than 10 None Diet-insulin
C Less than 10 and/or 10-19 None Diet-insulin
D Less than 10 and/or over 20 Backround Retinopathy Diet-insulin
F All ages Any duration Nephropathy Diet-insulin
R All ages Any duration Proliferative Retinopathy Diet-insulin
H All ages Any duration Cardiac disease Diet-insulin
T All ages Any duration After organ transplant Diet-insulin
Type 1 diabetes mellitus - In type 1 diabetes, which accounts for about 10% of all cases of
diabetes, beta cell destruction leads to insulin deficiency and the risk of ketoacidosis. There are
three forms. Immune-mediated type 1 diabetes is the most common form, and its diagnosis can
be confirmed by the presence of antibodies against the islet cells (ICA) or their components,
such as GAD, IAA, and ICA5/2. Idiopathic type 1 diabetes, which is less well-defined, includes
cases in which signs of autoimmune processes are absent. The third form, latent autoimmune
diabetes in adults (LADA), is apparently more prevalent than previously thought, accounting for
5-10% of all cases of diabetes diagnosed in adults (21-23).
Type 2 diabetes mellitus - Type 2 diabetes includes most forms of diabetes that derive from
combined insulin resistance and imbalance of insulin secretion. 90% of all diabetics have this

14
type. Over recent years, in developed countries, contrary to a decade or so ago, type 2 diabetes
has accounted for up to almost 1/3 of all PreDM (21-25).
Other specific types - About 3% of all cases of diabetes are of other specific types. The many
states that fall into this category, albeit relatively rare, include proven genetic defects in beta
cell function, genetic defects in insulin activity, exocrine pancreatic diseases, endocrinopathies,
diabetes due to medications or chemicals, infections, and the rare autoimmune diabetes and
genetic syndromes that involve diabetes. One of the genetic defects in beta cell function is
maturity onset diabetes of the young (MODY) (21).
Intermediate states - Impaired Fasting Glucose (IFG) is a relatively new concept that defines
individuals with fasting glucose levels of 110-125 mg/dl [6.1-7.0 mmol/l]. Impaired Glucose
Tolerance (IGT) has long been recognized and defines individuals with glucose levels of 140- 199
mg/dl [7.8-11.0 mmol/l] two hours after a 75g OGTT (26,27). The intermediate states are risk
factors for both diabetes mellitus (one-third of individuals with IGT will develop diabetes within
10 years) and macrovascular disease. They are usually not associated with the development of
microvascular complications unless the blood glucose reaches levels diagnostic of full-blown
diabetes (thereby changing the classification).
4.3. Pre-Pregnancy Evaluation for Women with Pre-GDM
Metabolic balance before and at the time of conception is crucial to prevent congenital
anomalies. Therefore, pregnancy planning and proper pre-pregnancy counseling is necessary
for all women with all subtypes of pregestational diabetets. The incidence of congenital
malformations is 3 times higher in women with diabetes than in healthy women, compared to a
backround malformation rated of 2-4%. It is still a major contributor to perinatal mortality in
the diabetic population. Appropriate planning and metabolic preparation can drastically
decrease congenital anomalies, to rates almost equal to those in the general population (28-32).

15
Recomendation (2): Pre-Pregnancy Evaluation Strength & Quality
All diabetic women of reproductive age must be advised to avoid pregnancy without proper
counseling, planning and preperation 1|
Pre-pregnancy HbA1C should be be aimed below 6-7%, prior to becoming pregnant 1|O
Pre-Pregnancy counseling and planning should include the following:
5mg folic acid supplementation, 3 months prior to pregnancy to the end of 1st
trimester
Renal function assessment: 24hr urine collection, urine albumin/creatinine and creatinine
Ocular examination to diagnose diabetic retinopathy
Cardiac examination, depending upon concurrent vascular risk factors
Neurologic examination, depending upon neourological complaints
Discontinue teratogenic medication prior to pregnancy or immediately upon diagnosis
1|OO
Advise that pregnancy is contra-indicated in the following cases:
Severe nephropathy (Creatinine clearance <40 or Creatinine > 2.5mg/dl)
Uncontrolled hypertension
Unmanageable proliferative retinopathy
Active coronary disease
1|OO

16
5. Prenatal care for women with diabetes during Pregnancy
The ultimate goal for the management of pregnancies complicated by diabetes should be a
normal outcome for both mother and baby. Since maternal survival has been nearly uniform for
several decades, fetal and neonatal survival has, until recently, been the primary therapeutic
goal. With the advent of reliable techniques for outpatient assessment of fetal well-being and
for control of maternal diabetes, perinatal survival approaching that of the non-diabetic
population may now be achieved in many cases with a minimum of in-hospital care. Fetal and
maternal outcome is directly correlated with the degree of maternal metabolic derangement.
Examinations should be performed in a multidisciplinary clinic with professional expertise in
high-risk pregnancy (Table 7).
Table 7: Diabetes in Pregnancy Center
Staff Equipment
1. Perinatologist 1. Central Laboratory
2. Diabetologist-endocrinologist 2. Fetal heart rate monitors
3. Diabetic nurse-educator 3. Ultrasoound & Fetal Echocardiography
4. Dietician 5. Glucometers
Insulin Infusion Pumps (CSII)
Continuous glucose monitors (CGMS)
5. Social worker / psychologist 6. Insulin and Oral hypoglycemics
6. Secretary
7. Consultants: Ophthalmology, Nephrology, Cardiology
5.1. Glucose measurements
Blood glucose level can be measured in one of 3 ways: Glycosylated hemoglobin (HbA1C), Self
Monitoring of Plasma Glucose (SMBG) and continuos glucose monitoring (CGM).
HbA1C - This measure reflects the average level of glucose in the 3 months prior to
measerment. It is correlated to the risk of congenital malformations and not to other adverse
pregnancy outcome. It is best used during pregnancy planning and follow-up in pregestational
diabetes and not for GDM glycemic contol (33-37).

17
SMBG - Self monitoring is is achived by multiple daily fingerprcisk via a glucometer. It provides
only the glucose values upon the second of measurement, probably missing in between
hyper/hypo glycemic events. Multiple studies have shown the efficacy of tight glycemic control
in reducing pregnancy complications by utilizing proper and realiable use of SMBG in women
with gestational and pre-gestational diabetes (39-43).
CGM – The device is composed of a subcutaneous enzymatic sensor attached to a non-
implanted transmitter that sends readings to a receiver, providing numerous automated testing
of interstitial tissue glucose calibrated to reflect plasma glucose. The continuous measurement
enables the detection of virtually all glucose fluctuations and to modify treatment accordingly
(44-46). CGM may lead to a small reduction in A1C in non pregnant population (47,48) can detect
high postprandial blood glucose levels and nocturnal hypoglycemia (49-50), although no clear
maternal or neonatal benefit were found during pregnancy (46, 51).
Recomendation (3): Glucose measements Strength & Quality
SMBG is recomneded for all pregnant women with diabetes, timimg of measurments:
Preprandial - Before each meal
Postprandial - 1 or 2 hours after every meal
If nocturnal hypoglycemia is suspected - during night time
1|O
CGM may be used during pregnancy in women with overt dibatets 2|OO
5.2. Goals of treatment
The main goal of treatment is to prevent adverse effects to mother and infant. Normalization of
glucose levels is a proven factor in the attainment of this goal and should be achived without
hypoglycemic events.
Glucose Control - No controlled studies have established the optimal blood glucose level for
prevention of increased fetal risk. However, postprandial glucose levels are more closely
associated with macrosomia than fasting levels (16-18).

18
Prevention and treatment of hypoglycaemia - At every intensive intervention before and
during pregnancy, an increased prevalence of hypoglycaemic events may be expected,
especially in the first weeks of pregnancy as a result of oestrogen release.
Recomendation (4): Goals of treatment Strength & Quality
Goals of treatment in GDM and Overt diabetes are:
Fasting Glucose < 95mg/dl (5.3mmol/L)
1 hour post prandial < 140mg/dl (7.8 mmol/L)
2 hour post prandial < 120 mg/dl (6.7 mmol/L)
1|OO
Goals of treatmet in overt diabetes:
HbA1C < 7 % 1|OOO
Educate to recognise and treat signs of hypoglycemia:
Sugar, rapidly absorbed tablets, sweetened liquids and bread
Supply women with a glucagon injection, teach family members how to use it
1|
5.3. Fetal Growth Assesment
Monitoring fetal growth is both challenging and inaccurate, with a ±15% error. Since fetal
macrosomia is the most frequent complication of diabetes, a particular effort should be
directed toward its diagnosis and management. The macrosomic fetus, at some time will be
above the 95th percentile for one or more parameters, most frequently, the abdominal
circumference. The positive predictive value for the diagnosis of macrosomia exceeds 90%
when the abdominal circumference or the estimated fetal weight is above the 95th percentile.
In Type 1 diabetes, macrosomia is more apparent in some fetal structures: liver, subcutaneous
fat, soft tissues of arm, thigh and cheeks. These variables (selective organomegaly) are
measurable and may aid in predicting early development of macrosomia. IUGR is associated
with conditions that predispose to uteroplacental insufficiency, and therefore is most likely to
appear in DM complicated by severe vasculopathy.

19
5.4. Fetal Wellbeing
Fetal assessment of diabetic pregnancies is achived by Biophysical profile (BPP) including the
non stress test (NST). It serves as an important tool for fetal surveillance, especially in order to
prevent unnecessary early interventions, thereby allowing prolongation of pregnancy beyond
37 weeks (52).
Recomendation (5): Antenatal Follow Up Strength & Quality
Routine antenatal visits should include:
Perinatologist: at least once monthly
Diabetologist and diabetic nurse educator: 1-3 weeks as needed
Weight, blood pressure and urine protein: 1-2 weeks in the 2nd and 3rd trimesters
1|OOO
In Pre-GDM women routine examinations during pregnancy should include:
24hr urine protein: once a trimester
Retinal examination: once a trimester
HbA1c: Every 4-6 weeks
1|OOO
NST and / OR BPP should be preformed once weekly from 32-34 weeks until delivery
NST and / or BPP should be preformed twice weekly from 32 weeks until delivery, if
dibetes is poorly controlled
1|OOO
Ultrasound growth assessments every 2-4 weeks, starting at around 20 weeks of
pregnancy for preGDM’s and time of diagnosis for GDM’s, until delivery 1|OOO

20
6. Treatment of hyperglycemia during pregnancy
6.1. Diet
Nutritional therapy is the cornerstone for diabetes, although no solid evidence prove its benefits during
pregnancy (53-58). Women with diabetes are recommended to follow an individually tailored diet that
aims to provide carbohydrate-controlled meals with appropriate weight gain, normoglycemia and the
absence of ketosis (26-34). Other aspects of such a dietary plan include healthy food, sized portions,
personal and cultural preferences, prepregnancy BMI, desired body weight, physical activity and blood
glucose levels. The diet should deliver the minimal nutritional requirements for all pregnant women, and
the caloric intake must be compatible with pregnancy and ensure the proper weight gain according to
the patient’s ideal weight before and during pregnancy. The distribution of caloric intake should be 35-
40% carbohydrates (complex carbohydrates are recommended), 20-25% protein, and 35-40% fat (10%
polyunsaturated).
Recomendation (6): Diet Strength & Quality
Daily caloric intake for diabetic patint is dependent upon pre-Pregnancy BMI:
BMI < 19.8 kg/m2: 35-40 KCalories/kg
BMI 19.8-29 kg/m2: 30-32 KCalories/kg
BMI >29 kg/m2: 24-25 Calories/kg
1|OO
Daily caloric intake included carbohydrate (35–45%), protein (20-25%), and fat (35-40%),
distributed as as follows::
8:00 (Breakfast): 10%
10:00 (Mid Morning): 5%
13:00 (Lunch): 30%
15:00 (Early Afternoon): 10%
17:00 (Late Afternoon): 5%
20:00 (Dinner): 30%
23:00 (Night / Bedtime): 10%
1| OO
For morbidly obese women, pre pregnancy caloric intake may be reduced by 30%, but not
below 1600-1800 Kcalories/d 2|OOO
In women with diabetic nephropathy, protein may be lowered to 0.6-0.8 g/kg ideal body
weight. 2|OOO

21
Weight Gain - There is no evidence regarding optimal weight gain for women with gestational or overt
diabetes (55). Maternal weight gain is associated wth adverse pregnancy outcome and limiting maternal
weight gain is not associated with a decrease in fetal birth weight (59). However, the institute of Medicine
does not recommend weight loss during pregnancy, even for morbidly obese women (60-61) (Table 8).
Some studies have addressed a posibilty of a severly caloric restricted diest, mainly for obese patients in
order to achive weight loss during pregnancy (60-61). However, weight reduction during pregnancy may be
associated with ketunoria (62-63) which has been associated with impaired fetal and neonatal
development (64, 65).
Table 8: Institute of Medicine - Recommendations for Weight Gain during Pregnancy
Total Weight Gain Rates of Weight Gain 2nd and 3rd Trimester
Prepregnancy BMI kg lbs Mean (range) in kg/week Mean (range) in lbs/week
Underweight (< 18.5 kg/m2) 12.5-18 28-40 0.51
(0.44-0.58) 1 (1-1.3)
Normal weight (18.5-24.9 kg/m2) 11.5-16 25-35
0.42 (0.35-0.50)
1 (0.8-1)
Overweight (25.0-29.9 kg/m2) 7-11.5 15-25 0.28
(0.23-0.33) 0.6 (0.5-0.7)
Obese (≥ 30.0 kg/m2) 5-9 11-20 0.22
(0.17-0.27) 0.5 (0.4-0.6)
6.2. Glyburide
Glyburide (Glybenclamide, Gluben) may be used as drug therpay in GDM, for those failing to
achieve glycemic control following a two week trial of diet. Evidence suggests that glyburide is
safe and effective during pregnancy. Some data exist as to the prediction of Glyburide
success/failure to achieve good metabolic control, where in such cases insulin should be
preferred as 1st line therapy.

22
Recomendation (7): Glyburide Strength & Quality
Glyburide may be used when diet treatment failes to achive glycemic goals within 2 weeks.
Exepct for the following, where insulin should be first line:
Diagnosis of diabetes < 20 weeks of gestation
Need for medical therapy > 30 weeks
Fasting plasma glucose levels > 110mg/dl
1hr post prandial glucose >140mg/dl
Pregnancy weight gain >12Kg
1|O
Glyburide should be started on a dosage of 2.5mg/d, with dosage elevated according to
glycemic control every 4-5 days, to a maximal dose of 20mg/d
1|O
6.3. Insulin
When glucose level cannot be maintained within limits by diet and/or glyburide, insulin is
required. There is no evidence supporting the advantages of any one dose or regimen over
another, thus, insulin programs should be personaly individualized (29, 56, 66-68).
Rapid-acting insulin analogues (Lispro, Aspart) can improve glycemic levels, although no
evidence suggests them to be superior to regular human insulin. For other analogues, insulin
Detemir was found safe and effective as long-acting human insulin. Paucity of data exists on
insulin glargine during pregnancy, and although it appears to be safe and well tolerated, data is
of low quality and fear of mitogenicity exists, due to high affinity to IGF receptors.
Recomendation (8): Insulin Strength & Quality
The following insulins may be used in pregnancy: Regular, NPH, Lispro, Aspart, Detemir 1| O O
Subcutaeous continuous insulin infusion may be continued during pregnancy and may be
initated if glycemic control is not achived by multiple daily injections 2| O O

23
7. Labor and Delivery
Labor and delivery is aimed to occur at term and vaginaly, or otherwise if indicated by maternal
or fetal compromise.
7.1. Glucose monitoring during labor
According to the Pedersen hypothesis, following birth, without continuous exposure to
sufficient levels of glucose, the newborn may become hypoglycemic. Maternal hyperglycemia
during labor is associated with Neonatal hyperglycemia, birth asphyxia and non-reassuring fetal
heart rate tracings (73-78). Targeting maternal glucose levels to values of 4-7mmol/L (72-
126mg/dl) during labor (Table 9), leads to a lower risk of maternal hypoglycemia than targeting
lower levels (79).
Table 9: Protocol to achieve glycemic control during labor and delivery
For women treated by nutritional medical therapy and oral hypoglycemic agents:
Glucose < 95mg/dl:
Non glucose IV solutions
Blood glucose should be monitored, by glucometer or sensor, at least every two hours.
Glucose > 95mg/dl:
IV Insulin should be initiated combined with 100ml/hr of IV glucose
Blood glucose levels should be monitored, by glucometer or sensor, every 15 minutes, until control is achieved.
For women treated with insulin:
Combined insulin and glucose containing solutions should be initiated
Glucose administration is maintained constant and insulin infusion is modified according to glucose levels:
Glucose Levels 95-150 mg/dl Insulin dose 1-2 Unit / Hour
Glucose Levels 151-180 mg/dl Insulin dose 2 Unit Push
Glucose Levels 181-220 mg/dl Insulin dose 3 Unit Push
Glucose Levels > 200 Insulin dose 4 Unit Push
Human short term insulin is recommended during labor and delivery and 10% dextrose.
Insulin infusion of over 16 hours, mandates monitoring of plasma potassium levels.

24
Recomendation (9): Glucose monitoring durin labor Strength & Quality
Glucose values during labor should be maintained at 72–126 mg/dl (4.0 to 7.0 mmol/l)
The recomnded protocol is outlined in table 9.
1| O O
7.2. Timing and Mode of delivery
Due to an increased risk of Intra uterine fetal death, especially when hyperglycemic and
macrosomic, may trigger induction of labor, although there are no evidence to support any
such approach. Some guidelines suggest gestational diabetic pregnancies, with good control
and maybe appropriate for gesational age fetus ought to continue the pregnancy until 39-40
weeks at least (80-82). When diabetes is poorly controlled the timing of delivery should be
individualized to 34-39 weeks of gestation. Gestational diabetes is not an indication for
cesarean section, but it should be employed when estimated fetal weight is above 4000g (69-72).
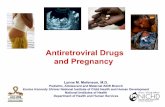
Recomendation (10):Timing and mode of delivery Strength & Quality
We recomned to follow the agoritm in figure 1 to decited the timing of delivery for
diabetic patients. 1| O O

25
Figure 1: Timing of delivery in GDM
37-38 WEEKS’
GESTATION
<3800 g
(AGA)
3800-4000 g
or/and
LGA
>4000 g
YES
Labor induction CS
40 weeks
Poor control?
Poor compliance?
Previous stillbirth?
Vascular disease?
NO

26
8. Post Partum Care
Women with GDM are at risk of developing type 2 diabetes mellitus, and sometimes type 1,
sometime after pregnancy, depending on risk factors such as: age at diagnosis of GDM, glucose
level on the first postpartum assessment, beta cell function, weight, and another pregnancy.
8.1. Post partum Glucose testing
All In women in whom glucose intolerance was diagnosed during pregnancy, the glycaemic
status should be re-evaluated at 6-12 weeks after delivery with a 75g glucose load (83). Diagnosis
is based on the currently recommended criteria, as presented in table 10. Women who do not
have diabetes according to these definitions should undergo repeated OGTT once yearly.
Women who had GDM should be advised to maintain a healthy life-style with regular exercise
and normal body weight for their habits and to seek consultation before their next pregnancy.
Table 10: Reclassification of disease after diabetic pregnancy by 75 g OGTT
Diagnosis Fasting blood glucose 2 hr blood glucose
Normal values <110 mg/dl (<6.1 mmol/l) <140 mg/dl (<7.8 mmol/l)
Interim state 110-125 mg/dl (6.1 - 7.0 mmol/l) 140-199 mg/dl (7.8 - 11.0 mmol/l)
Diabetes >126 mg/dl on two tests (>7.0 mmol/l) >200 mg/dl (> 11.1 mmol/l)
Recomendation (11): Post Partum Glucose Testing Strength & Quality
All In women with GDM, a 75g OGTT should be preformed 6-12 weeks after delivery 1| O O
Appropriate diet, physical exercise, weight loss and healthy lifestyle should be advised 1|
For GDM: Pharmacologicl treatment may be discontinued after delivry
FPG should be measured 24-48 hours post partum to rule out Overt diabetes 1|OO
For PreGDM: Insulin therapy should continute at 50% of predelivery dosage 1|OO

27
8.2. Breastfeeting
Infants of diabetic mothers are at an increased risk for future obesity and diabetes.
Breastfeeding has been shown as a protective factor for the occurrence of fetal and maternal
complications (84-85), including a reduction in childhood obesity, type 2 diabetes and even type 1
diabetes (86-89). Post partum lactation may be associated with post partum weight loss, and
lower rates of type 2 diabetes.
Recomendation (12):Breastfeeding Strength & Quality
Women with GDM or PreGDM, should be advied to breastfeed their baby 1|
8.3. Contraception
To properly plan her pregnancy, the diabetic woman must have access to effective
contraceptive methods. Thanks to advances in contraceptive technology, clinicians can now
offer their patients a relatively large range of options that meet medical criteria such as
effectiveness and efficiency and satisfy individual preferences.
Recomendation (13): Contraception Strength & Quality
Women with GDM or PreGDM, may use all available contraception 1|

28
9. References
1. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of
evidence and strength of recommendations. BMJ 2004 Jun 19;328(7454):1490.
2. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus.
Diabetes Care 1997 Jul;20(7):1183-97.
3. American Diabetes A. Standards of medical care in diabetes--2013. Diabetes Care 2013
Jan;36 Suppl 1:S11-66.
4. Jovanovic-Peterson L, Durak EP, Peterson CM. Randomized trial of diet versus diet plus
cardiovascular conditioning on glucose levels in gestational diabetes. Am J Obstet
Gynecol 1989 Aug;161(2):415-9.
5. Rudge MV, Calderon IM, Ramos MD, Peracoli JC, Pim A. Hypertensive disorders in
pregnant women with diabetes mellitus. Gynecol Obstet Invest 1997;44(1):11-5.
6. Yogev Y, Xenakis EM, Langer O. The association between preeclampsia and the severity
of gestational diabetes: the impact of glycemic control. Am J Obstet Gynecol 2004
Nov;191(5):1655-60.
7. Ehrenberg HM, Durnwald CP, Catalano P, Mercer BM. The influence of obesity and
diabetes on the risk of cesarean delivery. Am J Obstet Gynecol 2004 Sep;191(3):969-74.
8. Peters RK, Kjos SL, Xiang A, Buchanan TA. Long-term diabetogenic effect of single
pregnancy in women with previous gestational diabetes mellitus. Lancet 1996 Jan
27;347(8996):227-30.
9. Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2
diabetes: a systematic review. Diabetes Care 2002 Oct;25(10):1862-8.
10. Langer O, Rodriguez DA, Xenakis EM, McFarland MB, Berkus MD, Arrendondo F.
Intensified versus conventional management of gestational diabetes. Am J Obstet
Gynecol 1994 Apr;170(4):1036-46; discussion 46-7.
11. Modanlou HD, Komatsu G, Dorchester W, Freeman RK, Bosu SK. Large-for-gestational-
age neonates: anthropometric reasons for shoulder dystocia. Obstet Gynecol 1982
Oct;60(4):417-23.

29
12. McFarland MB, Trylovich CG, Langer O. Anthropometric differences in macrosomic
infants of diabetic and nondiabetic mothers. J Matern Fetal Med 1998 Nov-
Dec;7(6):292-5.
13. O'Sullivan JB, Mahan CM. Criteria for the Oral Glucose Tolerance Test in Pregnancy.
Diabetes 1964 May-Jun;13:278-85.
14. Metzger BE, Buchanan TA, Coustan DR, de Leiva A, Dunger DB, Hadden DR, et al.
Summary and recommendations of the Fifth International Workshop-Conference on
Gestational Diabetes Mellitus. Diabetes Care 2007 Jul;30 Suppl 2:S251-60.
15. Report of a WHO/IDF consultation 2006. Definition and diagnosis of diabetes mellitus
and intermediate hyperglycemia.
16. Group HSCR. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Int J
Gynaecol Obstet 2002 Jul;78(1):69-77.
17. Group HSCR, Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, et al.
Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008 May
8;358(19):1991-2002.
18. Group HSCR. Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study:
associations with neonatal anthropometrics. Diabetes 2009 Feb;58(2):453-9.
19. Hare JW WP. Gestational Diabetes and the white classification. . Diabetes Care 1980;
3:294-6.
20. White P. Pregnancy complicating diabetes. Am J Med 1949 Nov;7(5):609-16.
21. National Diabetes Data Group. Diabetes in America. 2d ed. Bethesda MNIoH, National
Institute of Diabetes and Digestive and Kidney Diseases, 1995; NIH publication no. 95-
1468.
22. Atkinson MA, Maclaren NK. The pathogenesis of insulin-dependent diabetes mellitus. N
Engl J Med 1994 Nov 24;331(21):1428-36.
23. Watanabe RM, Black MH, Xiang AH, Allayee H, Lawrence JM, Buchanan TA. Genetics of
gestational diabetes mellitus and type 2 diabetes. Diabetes Care 2007 Jul;30 Suppl
2:S134-40.

30
24. Olefsky JM, Kolterman OG, Scarlett JA. Insulin action and resistance in obesity and
noninsulin-dependent type II diabetes mellitus. Am J Physiol 1982 Jul;243(1):E15-30.
25. Reaven GM, Bernstein R, Davis B, Olefsky JM. Nonketotic diabetes mellitus: insulin
deficiency or insulin resistance? Am J Med 1976 Jan;60(1):80-8.
26. Fuller JH, Shipley MJ, Rose G, Jarrett RJ, Keen H. Coronary-heart-disease risk and
impaired glucose tolerance. The Whitehall study. Lancet 1980 Jun 28;1(8183):1373-6.
27. Charles MA, Fontbonne A, Thibult N, Warnet JM, Rosselin GE, Eschwege E. Risk factors
for NIDDM in white population. Paris prospective study. Diabetes 1991 Jul;40(7):796-9.
28. Expert Committee on the D, Classification of Diabetes M. Report of the expert
committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2003
Jan;26 Suppl 1:S5-20.
29. American Diabetes Association. Preconception care of women with diabetes. Diabetes
Care 2002;25:S82–4.
30. White P. Classification of obstetric diabetes. Am J Obstet Gynecol 1978 Jan
15;130(2):228-30.
31. Sacks DA. Preconception care for diabetic women: background, barriers, and strategies
for effective implementation. Curr Diabetes Rev 2006 May;2(2):147-61.
32. Holing EV, Beyer CS, Brown ZA, Connell FA. Why don't women with diabetes plan their
pregnancies? Diabetes Care 1998 Jun;21(6):889-95.
33. Guerin A, Nisenbaum R, Ray JG. Use of maternal GHb concentration to estimate the risk
of congenital anomalies in the offspring of women with prepregnancy diabetes.
Diabetes Care 2007 Jul;30(7):1920-5.
34. Lapolla A, Dalfra MG, Bonomo M, Castiglioni MT, Di Cianni G, Masin M, et al. Can plasma
glucose and HbA1c predict fetal growth in mothers with different glucose tolerance
levels? Diabetes Res Clin Pract 2007 Sep;77(3):465-70.
35. Kernaghan D, Penney GC, Pearson DW, Scottish Diabetes in Pregnancy Study G. Birth
weight and maternal glycated haemoglobin in pregnancies complicated by type 1
diabetes. Scott Med J 2007 Feb;52(1):9-12.

31
36. Langer O MR. The relationship between glycosilated hemoglobins and verified self-
monitored blood glucose among pregnant and non-pregnant women with diabetes.
Practical Diabetes 1987;4:32-43.
37. Brustman L, Langer O, Engel S, Anyaegbunam A, Mazze R. Verified self-monitored blood
glucose data versus glycosylated hemoglobin and glycosylated serum protein as a means
of predicting short- and long-term metabolic control in gestational diabetes. Am J
Obstet Gynecol 1987 Sep;157(3):699-703.
38. Mazze RS, Shamoon H, Pasmantier R, Lucido D, Murphy J, Hartmann K, et al. Reliability
of blood glucose monitoring by patients with diabetes mellitus. Am J Med 1984
Aug;77(2):211-7.
39. Hawkins JS, Casey BM, Lo JY, Moss K, McIntire DD, Leveno KJ. Weekly compared with
daily blood glucose monitoring in women with diet-treated gestational diabetes. Obstet
Gynecol 2009 Jun;113(6):1307-12.
40. Siega-Riz AM, Viswanathan M, Moos MK, Deierlein A, Mumford S, Knaack J, et al. A
systematic review of outcomes of maternal weight gain according to the Institute of
Medicine recommendations: birthweight, fetal growth, and postpartum weight
retention. Am J Obstet Gynecol 2009 Oct;201(4):339 e1-14.
41. Jovanovic LG. Using meal-based self-monitoring of blood glucose as a tool to improve
outcomes in pregnancy complicated by diabetes. Endocr Pract 2008 Mar;14(2):239-47.
42. Cheng YW, Caughey AB. Gestational diabetes: diagnosis and management. J Perinatol
2008 Oct;28(10):657-64.
43. Wilson N, Ashawesh K, Kulambil Padinjakara RN, Anwar A. The multidisciplinary
diabetes-endocrinology clinic and postprandial blood glucose monitoring in the
management of gestational diabetes: impact on maternal and neonatal outcomes. Exp
Clin Endocrinol Diabetes 2009 Oct;117(9):486-9.
44. Yogev Y, Ben-Haroush A, Chen R, Kaplan B, Phillip M, Hod M. Continuous glucose
monitoring for treatment adjustment in diabetic pregnancies--a pilot study. Diabet Med
2003 Jul;20(7):558-62.

32
45. Garg S, Zisser H, Schwartz S, Bailey T, Kaplan R, Ellis S, et al. Improvement in glycemic
excursions with a transcutaneous, real-time continuous glucose sensor: a randomized
controlled trial. Diabetes Care 2006 Jan;29(1):44-50.
46. Kestila KK, Ekblad UU, Ronnemaa T. Continuous glucose monitoring versus self-
monitoring of blood glucose in the treatment of gestational diabetes mellitus. Diabetes
Res Clin Pract 2007 Aug;77(2):174-9.
47. Group JCS. JDRF randomized clinical trial to assess the efficacy of real-time continuous
glucose monitoring in the management of type 1 diabetes: research design and
methods. Diabetes Technol Ther 2008 Aug;10(4):310-21.
48. Deiss D, Bolinder J, Riveline JP, Battelino T, Bosi E, Tubiana-Rufi N, et al. Improved
glycemic control in poorly controlled patients with type 1 diabetes using real-time
continuous glucose monitoring. Diabetes Care 2006 Dec;29(12):2730-2.
49. Chen R, Yogev Y, Ben-Haroush A, Jovanovic L, Hod M, Phillip M. Continuous glucose
monitoring for the evaluation and improved control of gestational diabetes mellitus. J
Matern Fetal Neonatal Med 2003 Oct;14(4):256-60.
50. McLachlan K, Jenkins A, O'Neal D. The role of continuous glucose monitoring in clinical
decision-making in diabetes in pregnancy. Aust N Z J Obstet Gynaecol 2007
Jun;47(3):186-90.
51. Murphy HR, Rayman G, Lewis K, Kelly S, Johal B, Duffield K, et al. Effectiveness of
continuous glucose monitoring in pregnant women with diabetes: randomised clinical
trial. BMJ 2008;337:a1680.
52. American College of O, Gynecologists Committee on Practice B-O. ACOG Practice
Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 30,
September 2001 (replaces Technical Bulletin Number 200, December 1994). Gestational
diabetes. Obstet Gynecol 2001 Sep;98(3):525-38.
53. N. F. Summary and recommendations of the Second International Workshop-
Conference on Gestational Diabetes. Diabetes, 1985 ;35(Suppl 2):S123–S126.
54. Langer O. Maternal glycemic criteria for insulin therapy in gestational diabetes mellitus.
Diabetes Care 1998 Aug;21 Suppl 2:B91-8.

33
55. Gunderson EP. Gestational diabetes and nutritional recommendations. Curr Diab Rep
2004 Oct;4(5):377-86.
56. Association AD. Gestational diabetes mellitus. Diabetes Care 2004 Jan;27 Suppl 1:S88-
90.
57. Kulkarni K, Castle G, Gregory R, Holmes A, Leontos C, Powers M, et al. Nutrition Practice
Guidelines for Type 1 Diabetes Mellitus positively affect dietitian practices and patient
outcomes. The Diabetes Care and Education Dietetic Practice Group. J Am Diet Assoc
1998 Jan;98(1):62-70; quiz 1-2.
58. Reader D, Splett P, Gunderson EP, Diabetes C, Education Dietetic Practice G. Impact of
gestational diabetes mellitus nutrition practice guidelines implemented by registered
dietitians on pregnancy outcomes. J Am Diet Assoc 2006 Sep;106(9):1426-33.
59. Magee MS, Knopp RH, Benedetti TJ. Metabolic effects of 1200-kcal diet in obese
pregnant women with gestational diabetes. Diabetes 1990 Feb;39(2):234-40.
60. Pettitt DJ, Bennett PH, Saad MF, Charles MA, Nelson RG, Knowler WC. Abnormal glucose
tolerance during pregnancy in Pima Indian women. Long-term effects on offspring.
Diabetes 1991 Dec;40 Suppl 2:126-30.
61. IOM of the National Academies. Weight gain during pregnancy: reexamining the
guidelines. http://iom.edu/Reports/2009/Weight-Gain-During-Pregnancy-Reexamining-
the-Guidelines.aspx (Accessed January 2013)
62. Dornhorst A, Nicholls JS, Probst F, Paterson CM, Hollier KL, Elkeles RS, et al. Calorie
restriction for treatment of gestational diabetes. Diabetes 1991 Dec;40 Suppl 2:161-4.
63. Knopp RH, Magee MS, Raisys V, Benedetti T, Bonet B. Hypocaloric diets and ketogenesis
in the management of obese gestational diabetic women. J Am Coll Nutr 1991
Dec;10(6):649-67.
64. Rizzo T, Metzger BE, Burns WJ, Burns K. Correlations between antepartum maternal
metabolism and child intelligence. N Engl J Med 1991 Sep 26;325(13):911-6.
65. Rizzo TA, Dooley SL, Metzger BE, Cho NH, Ogata ES, Silverman BL. Prenatal and perinatal
influences on long-term psychomotor development in offspring of diabetic mothers. Am
J Obstet Gynecol 1995 Dec;173(6):1753-8.

34
66. Buchanan TA, Kjos SL, Schafer U, Peters RK, Xiang A, Byrne J, et al. Utility of fetal
measurements in the management of gestational diabetes mellitus. Diabetes Care 1998
Aug;21 Suppl 2:B99-106.
67. Di Cianni G, Torlone E, Lencioni C, Bonomo M, Di Benedetto A, Napoli A, et al. Perinatal
outcomes associated with the use of glargine during pregnancy. Diabet Med 2008
Aug;25(8):993-6.
68. Langer O, Anyaegbunam A, Brustman L, Guidetti D, Levy J, Mazze R. Pregestational
diabetes: insulin requirements throughout pregnancy. Am J Obstet Gynecol 1988
Sep;159(3):616-21.
69. Chen R, Ben-Haroush A, Weismann-Brenner A, Melamed N, Hod M, Yogev Y. Level of
glycemic control and pregnancy outcome in type 1 diabetes: a comparison between
multiple daily insulin injections and continuous subcutaneous insulin infusions. Am J
Obstet Gynecol 2007 Oct;197(4):404 e1-5.
70. Kjos SL, Henry OA, Montoro M, Buchanan TA, Mestman JH. Insulin-requiring diabetes in
pregnancy: a randomized trial of active induction of labor and expectant management.
Am J Obstet Gynecol 1993 Sep;169(3):611-5.
71. Rouse DJ, Owen J, Goldenberg RL, Cliver SP. The effectiveness and costs of elective
cesarean delivery for fetal macrosomia diagnosed by ultrasound. JAMA 1996 Nov
13;276(18):1480-6.
72. Nachum Z, Ben-Shlomo I, Weiner E, Shalev E. Twice daily versus four times daily insulin
dose regimens for diabetes in pregnancy: randomised controlled trial. BMJ 1999 Nov
6;319(7219):1223-7.
73. Balsells M, Corcoy R, Adelantado JM, Garcia-Patterson A, Altirriba O, de Leiva A.
Gestational diabetes mellitus: metabolic control during labour. Diabetes Nutr Metab
2000 Oct;13(5):257-62.
74. Andersen O, Hertel J, Schmolker L, Kuhl C. Influence of the maternal plasma glucose
concentration at delivery on the risk of hypoglycaemia in infants of insulin-dependent
diabetic mothers. Acta Paediatr Scand 1985 Mar;74(2):268-73.

35
75. Curet LB, Izquierdo LA, Gilson GJ, Schneider JM, Perelman R, Converse J. Relative effects
of antepartum and intrapartum maternal blood glucose levels on incidence of neonatal
hypoglycemia. J Perinatol 1997 Mar-Apr;17(2):113-5.
76. Lean ME, Pearson DW, Sutherland HW. Insulin management during labour and delivery
in mothers with diabetes. Diabet Med 1990 Feb;7(2):162-4.
77. Miodovnik M, Mimouni F, Tsang RC, Skillman C, Siddiqi TA, Butler JB, et al. Management
of the insulin-dependent diabetic during labor and delivery. Influences on neonatal
outcome. Am J Perinatol 1987 Apr;4(2):106-14.
78. Feldberg D, Dicker D, Samuel N, Peleg D, Karp M, Goldman JA. Intrapartum management
of insulin-dependent diabetes mellitus (IDDM) gestants. A comparative study of
constant intravenous insulin infusion and continuous subcutaneous insulin infusion
pump (CSIIP). Acta Obstet Gynecol Scand 1988;67(4):333-8.
79. Carron Brown S, Kyne-Grzebalski D, Mwangi B, Taylor R. Effect of management policy
upon 120 Type 1 diabetic pregnancies: policy decisions in practice. Diabet Med 1999
Jul;16(7):573-8.
80. Tita AT, Landon MB, Spong CY, Lai Y, Leveno KJ, Varner MW, et al. Timing of elective
repeat cesarean delivery at term and neonatal outcomes. N Engl J Med 2009 Jan
8;360(2):111-20.
81. Rosenstein MG, Cheng YW, Snowden JM, Nicholson JM, Doss AE, Caughey AB. The risk
of stillbirth and infant death stratified by gestational age in women with gestational
diabetes. Am J Obstet Gynecol 2012 Apr;206(4):309 e1-7.
82. Spong CY, Mercer BM, D'Alton M, Kilpatrick S, Blackwell S, Saade G. Timing of indicated
late-preterm and early-term birth. Obstet Gynecol 2011 Aug;118(2 Pt 1):323-33.
83. Yogev Y, Ben-Haroush A, Chen R, Glickman H, Kaplan B, Hod M. Active induction
management of labor for diabetic pregnancies at term; mode of delivery and fetal
outcome--a single center experience. Eur J Obstet Gynecol Reprod Biol 2004 Jun
15;114(2):166-70.
84. Mayer-Davis EJ R-SS, Hu F, Colditz G, Gilman M. Breast feeding and risk for childhood
obesity: does diabetes or obesity status matter? Pediatr Res 2005;58:1027-8.

36
85. Mayer-Davis EJ, Rifas-Shiman SL, Zhou L, Hu FB, Colditz GA, Gillman MW. Breast-feeding
and risk for childhood obesity: does maternal diabetes or obesity status matter?
Diabetes Care 2006 Oct;29(10):2231-7.
86. O'Reilly M, Avalos G, Dennedy MC, O'Sullivan EP, Dunne FP. Breast-feeding is associated
with reduced postpartum maternal glucose intolerance after gestational diabetes. Ir
Med J 2012 May;105(5 Suppl):31-6.
87. Owen CG, Martin RM, Whincup PH, Smith GD, Cook DG. Does breastfeeding influence
risk of type 2 diabetes in later life? A quantitative analysis of published evidence. Am J
Clin Nutr 2006 Nov;84(5):1043-54.
88. Gunderson EP. Breastfeeding after gestational diabetes pregnancy: subsequent obesity
and type 2 diabetes in women and their offspring. Diabetes Care 2007 Jul;30 Suppl
2:S161-8.
89. Plagemann A, Harder T, Franke K, Kohlhoff R. Long-term impact of neonatal breast-
feeding on body weight and glucose tolerance in children of diabetic mothers. Diabetes
Care 2002 Jan;25(1):16-22.