
DEVELOPMENTAL DISTURBANCES OF ORAL TISSUES II- Developmental Disturbances Affecting the Oral Mucosa...
38
DEVELOPMENTAL DISTURBANCES OF ORAL TISSUES II- Developmental Disturbances Affecting the Oral Mucosa Prf. Dr. Gamal Fatah- ALLAH
-
Upload
amelia-barber -
Category
Documents
-
view
230 -
download
3
Transcript of DEVELOPMENTAL DISTURBANCES OF ORAL TISSUES II- Developmental Disturbances Affecting the Oral Mucosa...
DEVELOPMENTAL DISTURBANCES OF ORAL TISSUES
II- Developmental Disturbances Affecting the Oral Mucosa Prf. Dr. Gamal Fatah-ALLAH

Titles • I- Developmental Disturbances of The tongue. • II- Developmental Disturbances of The Oral mucosa • IV- Developmental Disturbances of The lip. • V- Developmental Disturbances of The Jaws.• VI- Developmental Disturbances of The Salivary glands.
• DEVELOPMENTAL DISTURBANCES OF THE FACE
• VIII- Syndromes associated with abnormalities of oral tissues:

DEVELOPMENTAL DISTURBANCES OF THE FACE
1. Microstomia. 2. Macrostomia. 3. Facial Hemihypertrophy. 4. Facial Hemiatrophy. 5. Facial Clefts.
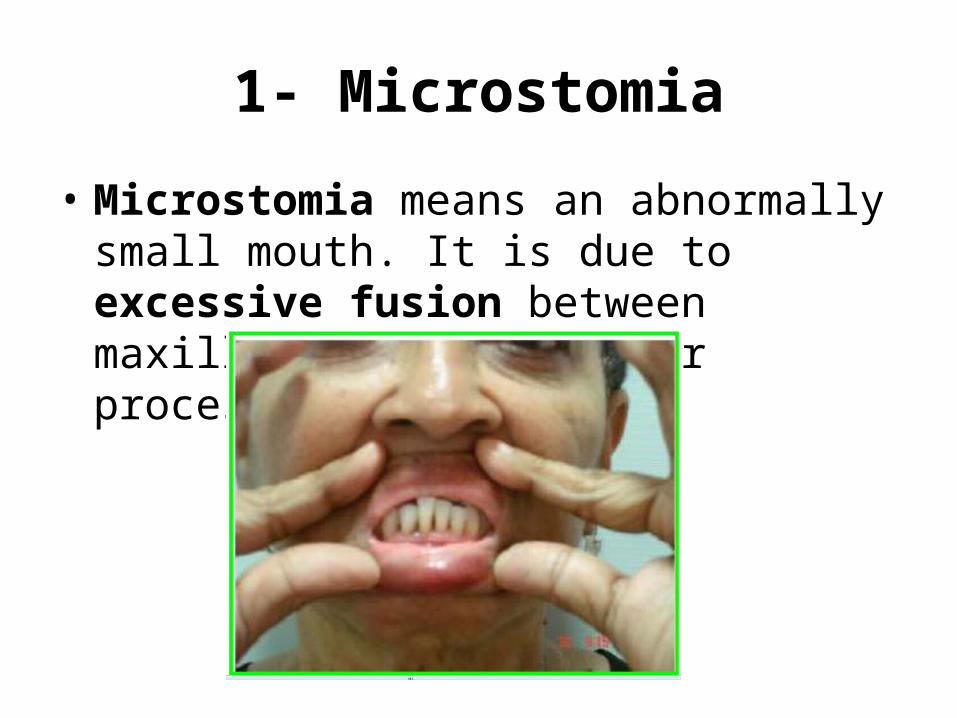
1- Microstomia
• Microstomia means an abnormally small mouth. It is due to excessive fusion between maxillary and mandibular processes.

2- Macrostomia Excessively large mouth. It is due to premature arrest of fusion between maxillary and mandibular processes bilaterally. •, Oral Pathology, •1•Oral Medicine •th Lect.•4•1

3- Facial Hemihypertrophy (Hemifacial Hypertrophy)
• Enlargement of half of the head with enlarged teeth on the involved side.
• Female predilection; 15-20% have mental retardation and seizures;
• Etiology: – Unknown. – Hormonal imbalance. – Incomplete twinning. – Chromosomal abnormalities. – Lymphatic or vascular or neurogenic abnormalities.
Facial Hemihypertrophy• Significant unilateral enlargement of the face
(frontal bone, maxilla, palate, mandible, alveolar process, condyle, and associated soft tissues); usually the right side
• Malocclusion due to enlarged teeth. Roots and crowns of the teeth are often enlarged and often erupt early.
• Unilateral macroglossia with increase size of fungiform papilla.

1. Unilateral enlargement of the face. 2. Malocclusion due to enlarged teeth.3. Unilateral macroglossia with increase size of fungiform papilla.
4- Facial Hemiatrophy (Hemifacial Atrophy)
• Progressive atrophy of some or all of the tissues on one side of the face, occasionally extending to other parts of the body.
• Etiology: – Unknown– peripheral nerve dysfunction– Trauma– infection,– Heredity– unilateral progressive systemic sclerosis.
Clinical Appearance of Hemifacial Atrophy
• Onset in 1st or 2nd decade of life, the left side of the face is more commonly affected.
• Characteristic loss in the soft tissues (hollowing of cheek) below the skin, usually on one side of the face; in some severe cases, the underlying bone is also affected.
• Jaw bones and roots of teeth on affected side my exhibit delayed development and retarded tooth eruption.

Clinical Appearance of Hemifacial Atrophy
• Note, hollowing of the cheek & atrophy of jaw bones of the affected side.
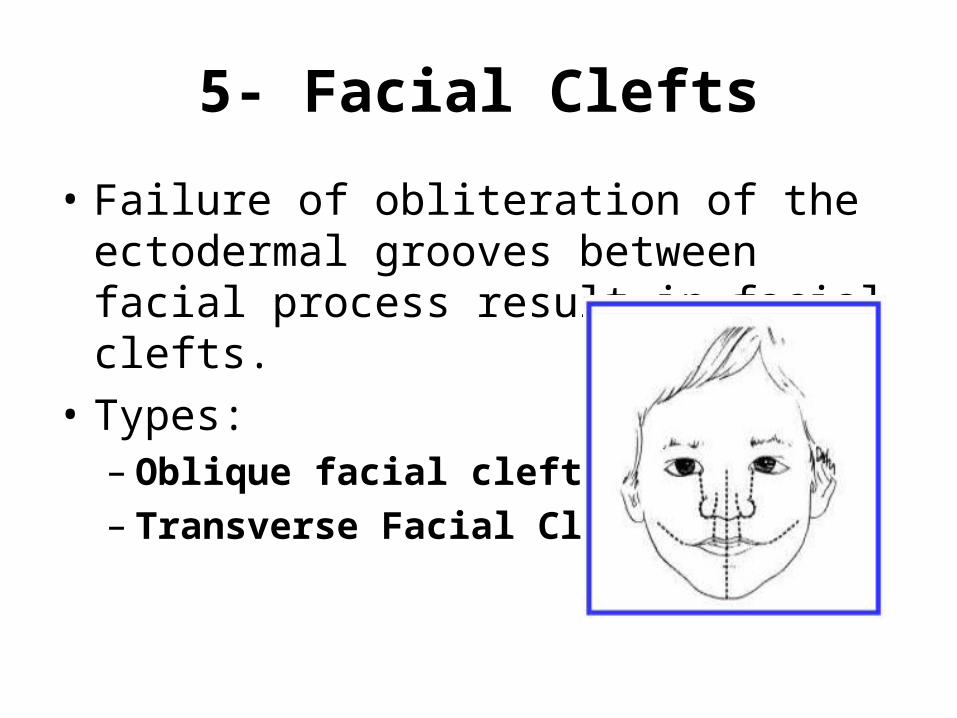
5- Facial Clefts
• Failure of obliteration of the ectodermal grooves between facial process result in facial clefts.
• Types:– Oblique facial cleft– Transverse Facial Cleft

A-Oblique facial cleft
• Rare developmental cleft runs from the inner canthus of the eye to the ala of the nose or upper lip (path of the nasolacrimal duct). – Failure of maxillary and lateral nasal processes
mesenchyme to obliterate the ectodermal groove between these processes.
• It is usually unilateral, but may be bilateral• Always associated with cleft lip and cleft
palate.

• Developmental cleft runs from the inner canthus of the eye to the ala of the nose or upper lip along the path of the nasolacrimal duct.

B- Transverse Facial Cleft
• Cleft running from the angle of the mouth toward the ear.
• Due to failure of migration and filling of ectomesenchyme along the line of fusion between the maxillary and mandibular processes.
• May be – unilateral or bilateral, – partial or complete,

• Cleft running from the angle of the mouth toward the ear.• Partial unilateral (A) bilateral complete(B) bilateral partial(C)
A BC

Titles • I- Developmental Disturbances of The tongue. • II- Developmental Disturbances of The Oral mucosa • IV- Developmental Disturbances of The lip. • V- Developmental Disturbances of The Jaws.• VI- Developmental Disturbances of The Salivary glands. • VII- DEVELOPMENTAL DISTURBANCES OF THE FACE
• VIII- Syndromes associated with abnormalities of oral tissues

• Treacher Collins syndrome. • Pierre Robin syndrome. • Peutz-Jegher syndrome. • Gardner's syndrome. • Mongolism. • Oxycephaly.
1- Treacher Collins syndrome
• Rare genetic disorder characterized by craniofacial deformities.
• May be inherited from a parent affected with the syndrome.
• This condition is a result of a defect of the first arch during development. Treacher Collins Syndrome also called mandibulofacial dysostosis.
Clinical Features of Treacher Collins syndrome
• Down-slanting eyes (antimongoloid eyes). • Notched lower eyelids (called a coloboma). • Underdevelopment or absence of cheekbones. • Lower jaw is small and sloping. • Underdeveloped, malformed ears, cause
hearing loss in about half of cases (congenital deafmutism).
• Cleft palate may be present.
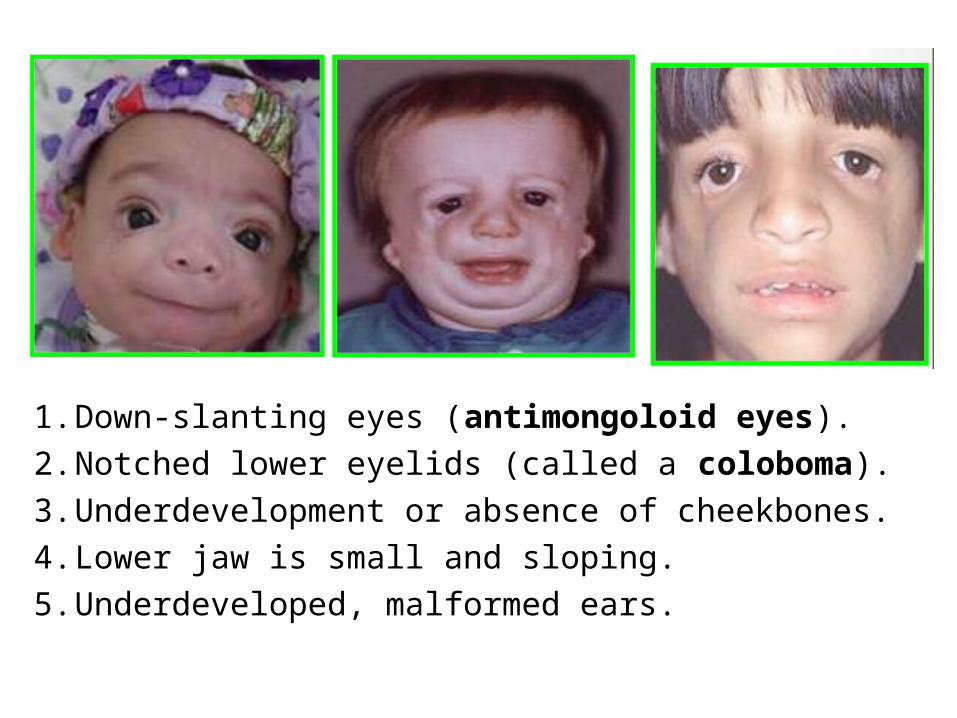
1. Down-slanting eyes (antimongoloid eyes). 2. Notched lower eyelids (called a coloboma). 3. Underdevelopment or absence of cheekbones. 4. Lower jaw is small and sloping. 5. Underdeveloped, malformed ears.

2- Pierre Robin Syndrome
• Condition present at birth in which an infant has – a very small lower jaw,– Tongue tends to fall back and downward– A cleft palate.
• Etiology : – Unknown– or genetic.
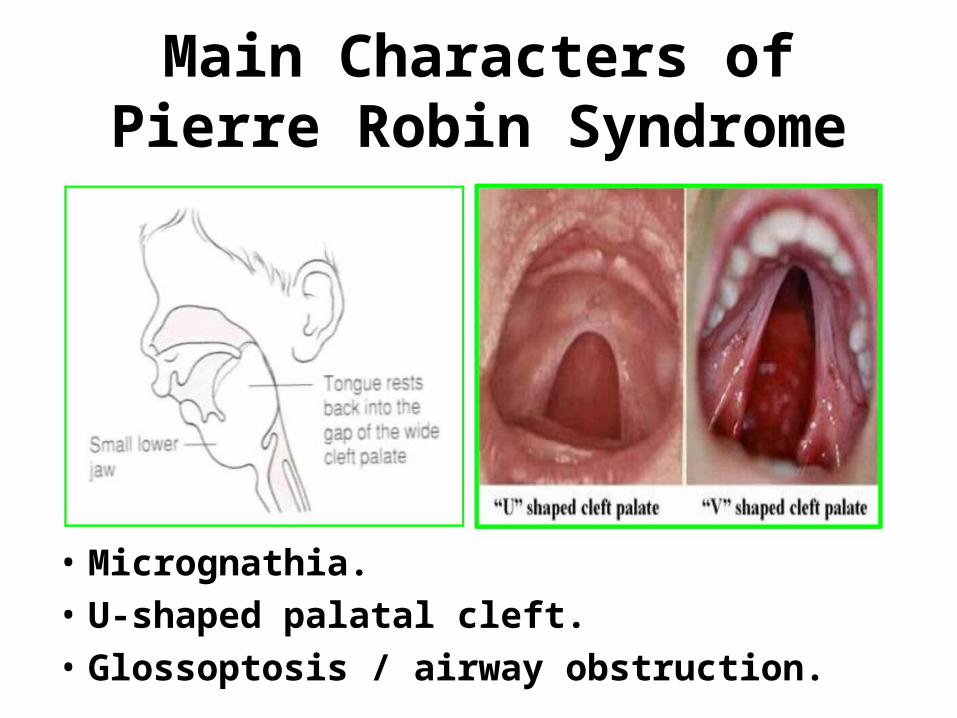
Main Characters of Pierre Robin Syndrome
• Micrognathia.• U-shaped palatal cleft. • Glossoptosis / airway obstruction.

3- Peutz-Jeghers syndrome
• Rare autosomal dominant. • Clinical Features:
1. The freckles; The freckles are usually present in infancy or childhood and may fade with age.• Lips or in the mouth & around the eyes and nose
(around facial openings). • May be around the hands and feet.
2. Hamartomatous polyps, multiple, usually in the small intestine. They may eads to abdominal pain and intestinal obstruction.

• Note, The freckles occur around facial openings.

Clinical Pictures of Peutz-Jeghers syndrome
• Freckles are also can be seen around the hands and feet.
• Freckles on the oral mucosa: buccal mucosa& inner side of lips
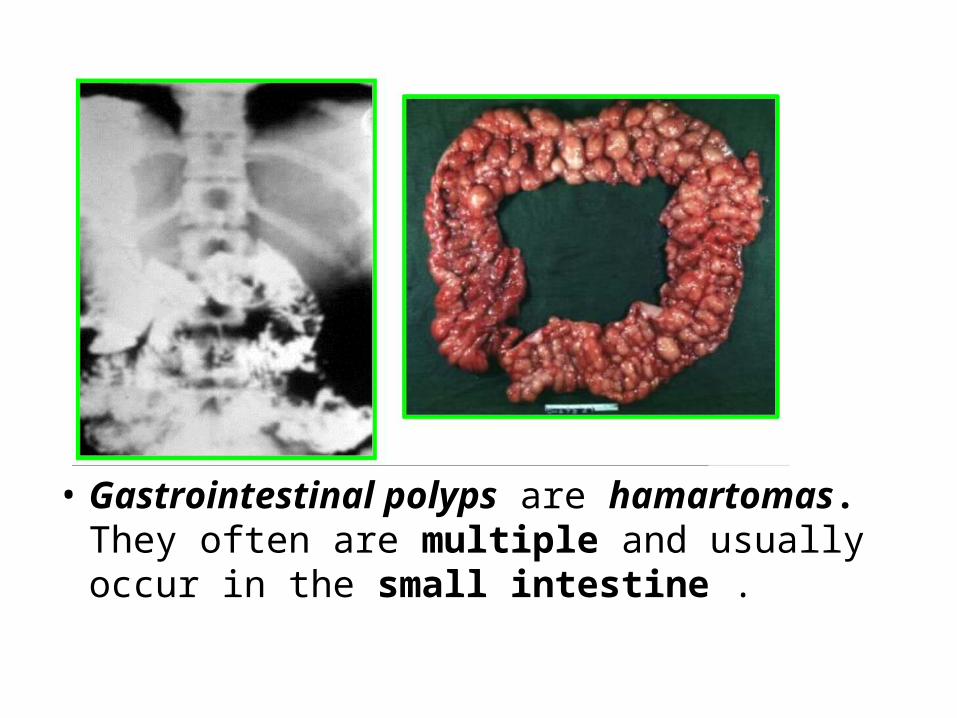
• Gastrointestinal polyps are hamartomas. They often are multiple and usually occur in the small intestine .

4- Gardner's syndrome
• Inherited autosomal dominant• characterized by: – Osteomas of the skull– Supernumerary teeth– Odontomas– Epidermoid cysts, fibromas and sebaceous cysts. – Adenomatous polyps in the colon predispose to
the development of colon cancer.

Manifestations of Gardner's Syndrome
1. Supernumerary teeth & odontomas. 2. Osteomas of the skull, 3. Epidermoid cysts, fibromas &
sebaceous cysts. 4. Polyps in the colon.

5- Down Syndrome (Mongolism, Trisomy 21)
• Trisomy 21 is a chromosomal disorder caused by the presence of all or part of an extra 21st chromosome.
• Clinical Features: – Mental retardation (Mild to severe).– Characteristic head:
• Small head (brachycephaly)• Flat facies with increased interocular distance (hypertelorism), • Depressed nasal bridge.
– Single transverse palmar crease (a single instead of a double crease) across one or both palms (Simian crease).
• 1- Small mouth (relatively) with protrusion of the tongue (macroglossia) and difficulty in eating and speaking. 2- Hypoplasia of the maxilla. 3- Delayed tooth eruption. 4- Hypodontia. 5- Juvenile periodontitis. 6- Cleft lip or palate (rare). 7- Fissured and geographic tongue. 8- Fissuring and thickening of the lips and angular cheilitis are frequent and increase in incidence and severity with age.

• 1-Characteristic small head (brachycephaly), flat facies with increased interocular distance (hypertelorism), depressed nasal bridge. 2- Single transverse palmar crease.
6- Oxycephaly
• Rare hereditary disease of the skull; the top of the skull assumes a cone shape.
• Caused by premature closure of the coronal & lambdoid sutures.
• Clinical Features: – Signs of intracranial pressure such as headache and optic
atrophy may be present.– The maxilla is small, narrow, retruded with crowding of
teeth. Radiographic appearance: Arcuate convolutions (copper beaten appearance) markings are seen as a result of intracranial pressure.

• Note, top of the skull assumes a cone shape, The maxilla is small, narrow, retruded & copper beaten appearance in radiograph.
Pathogenesis:
• To explain the 3 main features of the syndrome (Cleft palate, micrognathia & glossoptosis) during early stage of the formation of jaw bones, arrest of mandibular development occurred. Therefore the tongue remain high in its position preventing the 2 palatine processes of the maxilla from fusion causing cleft palate which is U-shaped coinciding with the shape of the tongue borders.

Main Points Discussed in this Lecture
• 1.Pathogenesis transeverse). 2.Differences between microstomia & macrostomia. 3.Etiology & clinical features of facial hemiatrophy & facial hemihypertrophy. 4.Etiology & clinical features for 6 syndromes: Treacher Collins syndrome- Pierre Robin Syndrome- Peutz-Jeghers syndrome- Gardner’s syndrome- Down syndrome- Oxycephaly.
• Session ID34








![ORAL ~RADIOLOGY - dent.zaums.ac.irdent.zaums.ac.ir/uploads/1_296_chapter1.pdf · tal Disturbances of the Face and Jaws. ... 19 Inflammatory l esions of the Jaws, ]66 ... 29 Developmental](https://static.fdocuments.us/doc/165x107/5a97a0aa7f8b9ab6188ced90/oral-radiology-dentzaumsac-disturbances-of-the-face-and-jaws-19-inflammatory.jpg)







