Development of the diagnostic ultrasound system LISENDO 880 · Tetsuo Watanabe 1) Masanori Hisatsu...
8
1 − − 〈MEDIX VOL.66〉 XX-E231 1. Introduction 1.1 Background to the development Since 2014, we have approached the cardiovascular field by diagnostic ultrasound system ProSound* 2 F75 PremierCV. Despite our continued efforts, we have encountered cases that cannot be explained with conventional cardiac functional measurements, such as patients with heart failure whose left ventricular ejection fraction (EF) is maintained. To provide solutions to clinical challenges such as these by visualization and quantification of cardiac hemodynamics, we have devel- oped “LISENDO 880” (Figure 1), a premium-class diagnostic ultrasound system dedicated to the cardiovascular field. 1.2 The origin of the name “LISENDO 880” The word “LISENDO” combines the English word listen as in “listen to the sound” and the Greek word endo mean- ing “inside,” to create “LISENDO”: “listening to the sound inside the body”. “LISENDO” is our brand name for diagnos- tic ultrasound systems dedicated to the cardiovascular field. Hitachi introduced the world’s first diagnostic ultrasound system equipped with Color Doppler in 1983, namely “SSD- 880”. By nurturing our original aims and reinvigorating our pursuit of the understanding of hemodynamics, we have used again the same number from “SSD-880” in the product name. 1.3 Product concepts The development of LISENDO 880 has been based on three main concepts – “Pure Image,” “Seamless Workflow,” and “Your Application” – to provide customer value as a pre- mium-class platform dedicated to the cardiovascular market providing “performance,” “usability,” and “application.” Development of the diagnostic ultrasound system LISENDO 880 1) Products R&D Division 1, Diagnostic R&D Division, Hitachi, Ltd. Healthcare Business Unit 2) Engineering R&D Division 1, Diagnostic R&D Division, Hitachi, Ltd. Healthcare Business Unit 3) Marketing Division, Diagnostic Systems Division, Hitachi, Ltd. Healthcare Business Unit Key Words: Cardiovascular, HI Framerate, “ Focusing”, VFM, Cardiac 3D e Tetsuo Watanabe 1) Masanori Hisatsu 1) Masato Eda 1) Takashi Fujii 2) Tomoaki Chono 2) Takashi Kayama 3) Hitachi, Ltd. Healthcare Business Unit (HHBU) was formed as the healthcare section of Hitachi group in April 2016. The premium ultrasound system, “LISENDO * 1 880”, is the first model to be marketed from HHBU. LISENDO 880 has been de- veloped to embrace the functions and performance dedicated to cardiovascular applications, establishing Hitachi’s reputation in this field. Figure 1: LISENDO 880 Technical Report
Transcript of Development of the diagnostic ultrasound system LISENDO 880 · Tetsuo Watanabe 1) Masanori Hisatsu...

1− − 〈MEDIX VOL.66〉 XX-E231
1. Introduction1.1 Background to the development
Since 2014, we have approached the cardiovascular field by diagnostic ultrasound system ProSound*2 F75 PremierCV.
Despite our continued efforts, we have encountered cases that cannot be explained with conventional cardiac functional measurements, such as patients with heart failure whose left ventricular ejection fraction (EF) is maintained. To provide solutions to clinical challenges such as these by visualization and quantification of cardiac hemodynamics, we have devel-oped “LISENDO 880” (Figure 1), a premium-class diagnostic ultrasound system dedicated to the cardiovascular field.
1.2 The origin of the name “LISENDO 880”
The word “LISENDO” combines the English word listen as in “listen to the sound” and the Greek word endo mean-ing “inside,” to create “LISENDO”: “listening to the sound inside the body”. “LISENDO” is our brand name for diagnos-tic ultrasound systems dedicated to the cardiovascular field.
Hitachi introduced the world’s first diagnostic ultrasound system equipped with Color Doppler in 1983, namely “SSD-880”. By nurturing our original aims and reinvigorating our pursuit of the understanding of hemodynamics, we have used again the same number from “SSD-880” in the product name.
1.3 Product concepts
The development of LISENDO 880 has been based on three main concepts – “Pure Image,” “Seamless Workflow,”
and “Your Application” – to provide customer value as a pre-mium-class platform dedicated to the cardiovascular market providing “performance,” “usability,” and “application.”
Development of the diagnostic ultrasound system LISENDO 880
1) Products R&D Division 1, Diagnostic R&D Division, Hitachi, Ltd. Healthcare Business Unit2) Engineering R&D Division 1, Diagnostic R&D Division, Hitachi, Ltd. Healthcare Business Unit
3) Marketing Division, Diagnostic Systems Division, Hitachi, Ltd. Healthcare Business Unit
Key Words: Cardiovascular, HI Framerate, “ Focusing”, VFM, Cardiac 3De
Tetsuo Watanabe1) Masanori Hisatsu1) Masato Eda1) Takashi Fujii2) Tomoaki Chono2) Takashi Kayama3)
Hitachi, Ltd. Healthcare Business Unit (HHBU) was formed as the healthcare section of Hitachi group in April 2016. The
premium ultrasound system, “LISENDO*1 880”, is the first model to be marketed from HHBU. LISENDO 880 has been de-
veloped to embrace the functions and performance dedicated to cardiovascular applications, establishing Hitachi’s reputation
in this field.
Figure 1: LISENDO 880
Technical Report

2− − 〈MEDIX VOL.66〉 XX-E231
Pure Image: Premium image quality with a wide range of parameter adjustment to meet the individual needs of examin-ers and patients
Seamless Workflow: Workflow streamlined to reduce the burden on examiners and patients
Your Application: Unique and distinctive applications that fulfill clinical goals and offer re-search opportunities
2. Pure Image
Returning to the basics of diagnostic ultrasound, we have sought improved performance in the three major imaging areas – spatial, contrast, and temporal resolution – advanc-ing performance using the Pure Symphonic Architecture technology (Figure 2).
Probes / Frontend
Variable Beamformer
Active Backend
OLEDMonitor
OLED Monitor: Organic Light Emitting Diode Monitor
Figure 2: Pure Symphonic Architecture technology
2.1 Electronic sector transducer “S121”
We have developed a new electronic sector transducer, “S121”, to meet users’ requirements for usability and high performance (Figure 3).
With a compact shape, the boot section can be held com-fortably and firmly in a variety of different ways. The small foot print of the acoustic lens and well-considered shape of the edge allow the operator to use different windows whilst reducing discomfort to the patient. Care has also been taken in the choice of diameter and weight of the cable so as not to impact on the examination.
For performance, consideration has been given to the probe’s frequency characteristics (Figure 4) to strike a balance between a broad bandwidth contributing to spatial resolution, and the high sensitivity required in the Doppler mode. To achieve this balance i.e., effective transmission and reception over a wide range from low to high frequen-cies, a single-crystal piezoelectric material with an electro-mechanical coupling coefficient of more than 90% is used.
2.2 “HI Framerate” and “eFocusing” realized by the Variable Beamformer “HI Framerate”
To improve the frame rate, conventional models employ multidirectional simultaneous reception technology to obtain multiple reception beams from a single transmission. Due to limitations imposed by the hardware, however, the simultane-ous reception of multidirectional beams is possible only from two to four directions. In this simple model, furthermore, the higher frame rate is a tradeoff with reduced lateral resolution.
As shown in Figure 5, LISENDO 880 is equipped with “HI Framerate,” a multidirectional simultaneous reception technology that can generate multiple reception beams from one transmission. This strikes a balance between high spa-tial resolution and high temporal resolution in B-mode and Color Doppler imaging (Figure 6), and also contributes to improved detection for generation of Doppler waveforms. Any regurgitant flows will move spatially in synchronization with the beating of the heart. It is often required to measure a regurgitation only several millimeters in size, located at a depth of 10 cm from the body surface. To capture such a regurgitation and display the Doppler waveforms with high sensitivity, first it is required to set the position and angle of the transducer so that the regurgitant jet remains within the scanning plane. Secondly, the Doppler sample gate must be set precisely over the regurgitation (Figure 7). The operator receives assistance for both these tasks in the Color Doppler images created by “HI Framerate” that strike a balance be-tween high spatial resolution and high temporal resolution.
Frequency [MHz]
Am
plitu
de [d
B]
New transducer (S121) Conventional transducer AConventional transducer B
Transducer elements
Reception beams
Transmission beam shape
Figure 4: Frequency characteristics of S121 transducer
Figure 5: Multidirectional simultaneous reception tech-nology “HI Framerate”
Figure 3: The electronic sector transducer S121

3− − 〈MEDIX VOL.66〉 XX-E231
As a result, improved Pulse Wave (PW) and Continuous Wave (CW) Doppler waveforms can be detected.
“eFocusing”
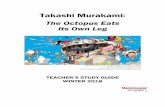
In beam forming during reception for diagnostic ultra-sound systems, the signals received by the transducer from each sample point along the reception beam are given a delay time before being phased and summed, so that the resulting reception signals are focused for all sample points. This is dynamic focus technology on reception. In transmis-sion beam forming on the other hand, a single transmission focus point is set, and the transmission beam is formed by giving a delay time to each transducer element at the time of transmission. Consequently, as shown in Figure 8, the transmission beam width is narrow and the lateral resolu-tion good at a depth near the transmission focus point, but at other depths away from the focus point, lateral resolution deteriorates.
“eFocusing” reduces transmission focus dependency using “HI Framerate,” a multidirectional simultaneous recep-tion technology. As shown in Figure 9 (a), the position of the transmission beam is shifted such that the reception beam fields resulting from each single transmission overlap, with the result that a synthetic reception beam can be created. This effect can be described taking scattering point ● as an example. In conventional transmission beam forming, if B-mode images are created from simultaneous multidirec-tional reception signals obtained from a single transmission, the lateral resolution of the image of point ● is low from each transmission wavefront as shown in Figure 9 (b), in the same manner as the lateral resolution deteriorates at a depth
away from the transmission focus point. However, by syn-thesizing the reception signals using the phase information from each transmission, the phases will match at the position of point ● . In other positions, the signal components attrib-utable to this scatterer are canceled out through the process of synthesis and result in B-mode images with improved lateral resolution as shown in Figure 9 (c). This process of synthesis can be interpreted as transmission beam focusing for sample points at every depth, i.e., realizing dynamic transmission focusing. Since reception also uses dynamic fo-cusing as in the conventional models, “eFocusing” achieves dynamic focusing in both transmission and reception. Fur-thermore, the reception signals synthesized from multiple transmissions contribute to an improved signal-to-noise ratio and thus improved penetration. Examples of B-mode images obtained by “eFocusing” are shown in Figure 10.
Thanks to the effect of dynamic focusing in transmission and reception, “eFocusing” reduces the transmission focus dependency experienced in conventional models, and elimi-nates the need to set a transmission focus depth. Therefore, in addition to providing high-quality B-mode images with ex-cellent penetration, it also contributes to improved workflow by reducing examination time.
Transmission
Reception beam field
(b) B-mode images of scattering point ● formed by a single transmission
(a) Reception field and scattering point ●in each transmission
(c) B-mode image by “ Focusing”
Synthesis
e
Figure 6: “HI Framerate” Off (left) and On (right)
Figure 7: Anatomy of the heart with ultrasound scan-ning planes
Figure 9: Effects obtained by “eFocusing”
Figure 8: Conventional transmission beam
Transducer elements
Deterioration of lateral resolution
Transmission focus point
Transmission beam shape
〈MEDIX VOL.66〉 25
の高空間分解能と高時間分解能を両立(図6)し、さらにはドプラ波形の検出改善にも寄与する。ドプラ波形検出のターゲットとなる逆流血流は、心臓全体の拍動に合わせて空間的に動いている。また、体表から10cmの深い位置にある数mm
程度の広がりを持った軽度な逆流を計測する場合もある。ドプラ波形を感度よく計測するためには、まずスキャン断面に安定して逆流が表示されるように、つまりスキャン断面が逆流血流を安定して捉えるようにプローブの位置や角度を設定する必要がある。次に、スキャン断面に表示された逆流血流にドプラサンプルゲートを精度よく設定する必要がある(図7)。“HI Framerate”により高空間分解能と高時間分解能を両立したカラードプラ画像が、それらを良好にアシストする。その結果、PW(Pulse Wave)およびCW(Continuous wave)ドプラ波形の検出能力改善が見込まれる。
“eFocusing”超音波診断装置の受信ビームフォーミングでは、振動子で
受信した信号に対し、受信ビーム上の各サンプル点について所望の遅延時間を与えて整相加算するため、全サンプル点についてフォーカスされた受信信号が得られる。これが受信ダイナミックフォーカス技術である。一方、送信ビームフォーミングでは、一点の送信フォーカス点を設定し、送信時に各振動子に遅延時間を与えることで、送信ビームを形成している。このため、図8に示すように、送信フォーカス点に近い深度では送信ビーム幅が狭く方位分解能が良いが、フォーカス点から離れた深度では方位分解能が劣化する。
“eFocusing”は、多方向同時受信技術“HI Framerate”を用い、送信フォーカス依存性を低減する。図9(a)に示すように、1回の送信から得られる受信ビーム領域が重なるように送信ビーム位置をシフトし、位置が重複している受信ビームを合成する。この効果について、散乱点●の画像形成の例で説明する。従来の送信ビームフォーミングにおいて、送信フォーカス点から離れた深度で方位分解能が劣化するのと同様に、1回の送信で得られた多方向同時受信信号からBモード画像を形成すれば、図9(b)に示すように各送信波面にしたがって方位分解能が劣化した●の画像が得られる。しかし、各送信において、位相情報を持った受信信号を合成することにより、●の位置においてのみ位相が一致する。それ以外の位置では、この散乱体に起因する信号成分は合成によって打ち消され、結果として図9(c)のように方位分解能が向上したBモード画像が得られる。この合成は各深度のサンプル点に送信フォーカスしていることに相当し、つまり送信ダイナミックフォーカスを実現している。従来と同様に、受信もダイナミックフォーカスであるため、“eFocusing”では送受信ダイナミックフォーカスを実現している。また、複数の送信から得られた受
図6:“HI Framerate” Off(左)とOn(右)
図7:心臓の解剖図と超音波のスキャン断面
図8:従来の送信ビーム
振動子
送信フォーカス点
方位分解能劣化
送信ビーム形状
図9:“eFocusing”により得られる効果
合成
受信ビーム領域
送信
(a)各送信における受信領域と散乱点●
(b)1回の送信で散乱点●のBモード像を形成した場合
(c)“ Focusing”によるBモード像
e

4− − 〈MEDIX VOL.66〉 XX-E231
2.3 High quality imaging achieved by Active Backend with a wide range of image quality parameter adjustments to meet the individual needs of exam-iners and patients.
Ultrasound diagnostic imaging can be examiner-depen-dent in terms of differences in adjustment and preference. It can also be patient-dependent in terms of difference in body physique and constitution. This brings about the need for a wide range of image parameter adjustments.
LISENDO 880 is programmed with multiple image ad-justment parameters that have been refined through the development of our previous platform portfolio, including the ProSound, HI VISION and ARIETTA*3 series, and are thus capable of offering a wide range of image quality ad-justments to provide images suited to the various modes of diagnosis, ranging from quantitative to morphological (Fig-ure 11), and overcoming the long-held challenge of reducing examiner-and patient-dependency.
○ Qualitative diagnosis: Images with a wide dynam-ic range, capable of visualiz-ing the detailed information of the myocardium. Allows evaluation of the heart wall and assessment of its prop-erties.
○ Morphological diagnosis: High black and white con-
trast, structure-emphasized images. Main purpose is mor-phological understanding.
2.4 Improvement of contrast resolution by organic EL monitor
B mode, the abbreviation of Brightness mode, is the basic diagnostic ultrasound mode. The B-mode image depicts the internal structure of a biological tissue in shades of gray, or gradations of white and black. Among the important indica-tors for this gray scale performance is contrast resolution. If the monitor that displays ultrasound images has a poor gray scale – i.e., if the contrast ratio is low – the system cannot achieve high contrast resolution.
Organic Electro-luminescence (EL) monitors are made up of EL elements which emit light in a process known as electrophosphorescence. The display of black is clearly de-picted by controlling each element not to emit light, thereby achieving a high contrast ratio. Even in a high performance model, the contrast ratio of a liquid crystal monitor is rough-ly1000:1, compared to that of an organic EL monitor which achieves 250,000:1. It can be said to be the most suitable dis-play monitor for diagnostic ultrasound systems.
3. Seamless Work�ow3.1 Operating console
During an ultrasound examination, the examiner applies the transducer to the patient with one hand whilst manipu-lating the operating console with the other, and at the same time, observing ultrasound images displayed on the monitor. To stay focused on the examination, it is desirable not to take your eyes away from the monitor. An example of a rou-tine examination that requires continuous operation is Dop-pler waveform measurement. Firstly, on the real-time image, the position of the Doppler sample gate is adjusted using the “trackball (hereinafter referred to as T.B.)”, and secondly, when the desired image is obtained, the “Update” switch is pressed to start the Doppler scanning. The “Freeze” switch is pressed to stop updating, and finally, the “Store” switch is used to record the image. If it is necessary to look away from the monitor during the examination to check the loca-
26 〈MEDIX VOL.66〉
信信号を合成しているため、信号雑音比の向上効果も得られ、ペネトレーションが向上する。図10に“eFocusing”により得られたBモード画像の例を示す。このように、“eFocusing”では、送受信ダイナミックフォーカシング効果により、従来の問題点であった送信フォーカス依存が軽減され、送信フォーカス深度の設定が不要となる。また、高画質かつ高ペネトレーションなBモード画像の提供により、検査時間短縮などワークフローの改善にも貢献する。
2.3 Active Backendによる高画質化と、検査者および被検査者に合わせた画質調整幅の確保
超音波画像診断は、検査者による調整や好みの差など検査者依存性がある。また、被検査者の体質や体格による被検査者依存性もある。そのため、画像調整の幅の広さが求められる。
ALOKA LISENDO 880は、従来の製品ラインナップであるProSoundシリーズ、HI VISIONシリーズ、ARIETTA※4シリーズの開発で培った、超音波画像診断に特化したさまざまな画像調整パラメーターを兼ね備え、質的診断に適した画像から、形態診断に適した画像までを実現可能な画質調整の幅を持っている(図11)。その結果、課題となっていた検査者依存や被検査者依存の低減が可能になった。
○質的診断: ダイナミックレンジが広く、心筋のより詳細な情報を描出する画像。壁把握および性状評価が可能。
○形態診断: 白黒のメリハリを付け、構造物を強調した画像。形態把握を主目的とする。
2.4 有機ELモニターによるコントラスト分解能の向上超音波診断装置の基本モードであるBモードは、Bright-
nessモードの略で、白黒の階調性つまり白黒の濃淡のみで生体組織の内部構造を表現する。この濃淡表現の重要な性能指標として、コントラスト分解能が挙げられる。超音波画像を表示するモニターの白黒の階調表現が豊かでなければ、つまりコントラスト比が高くなければ、高コントラスト分解能は実現できない。有機EL(Electro-luminescence)モニターは、素子の自発
光であり、黒の映像を表現する際、各素子を発光させない制御をすることで黒が明確に表現でき、高コントラスト比を実現できる。液晶モニターのコントラスト比が、高性能な物でも1000:1程度であるのに対し、有機ELモニターは25万:1を達成している。超音波診断装置のモニターとして非常に適したデバイスと言える。
3.Seamless Workflow
3.1 操作パネル超音波検査は、1人の検査者が、片手でプローブを被検査
者に当て、モニターに表示された超音波画像を観察しつつ、もう片方の手で操作パネルを操作する。画像観察に集中するため、モニターから視線が移動しないことが望まれる。ルーチン検査において、超音波スキャン中の連続的な操作が必要な代表例として、ドプラ波形の計測が挙げられる。まず断層像がアクティブの状態において“トラックボール(以下T.B.)”でドプラサンプルゲート位置を合わせ、次に“Update”スイッチでドプラのスキャンをスタートし、所望の画像が得られたら“Freeze”スイッチで画像の更新を止め、最後にStoreスイッチで画像を保存する。途中で超音波画像を表示するモニターから目を離して操作パネルを確認すると、スキャン断面がずれて良好なドプラ波形が得られない場合がある。そこで、ALO-
KA LISENDO 880では、パームレスト付近をホームポジションとし、上記ドプラ波形の計測操作を、ホームポジションに掌の位置を固定したまま手元に視線を移すことなく操作で
図10:“eFocusing” Off(左)とOn(右)
図11:質的診断に適した画像(左)と形態診断に適した画像(右)
Figure 10: “eFocusing” Off (left) and On (right)
Figure 11: Image suited to qualitative diagnosis (left) and image suited to morphological diagnosis (right)
26 〈MEDIX VOL.66〉
信信号を合成しているため、信号雑音比の向上効果も得られ、ペネトレーションが向上する。図10に“eFocusing”により得られたBモード画像の例を示す。このように、“eFocusing”では、送受信ダイナミックフォーカシング効果により、従来の問題点であった送信フォーカス依存が軽減され、送信フォーカス深度の設定が不要となる。また、高画質かつ高ペネトレーションなBモード画像の提供により、検査時間短縮などワークフローの改善にも貢献する。
2.3 Active Backendによる高画質化と、検査者および被検査者に合わせた画質調整幅の確保
超音波画像診断は、検査者による調整や好みの差など検査者依存性がある。また、被検査者の体質や体格による被検査者依存性もある。そのため、画像調整の幅の広さが求められる。
ALOKA LISENDO 880は、従来の製品ラインナップであるProSoundシリーズ、HI VISIONシリーズ、ARIETTA※4シリーズの開発で培った、超音波画像診断に特化したさまざまな画像調整パラメーターを兼ね備え、質的診断に適した画像から、形態診断に適した画像までを実現可能な画質調整の幅を持っている(図11)。その結果、課題となっていた検査者依存や被検査者依存の低減が可能になった。
○質的診断: ダイナミックレンジが広く、心筋のより詳細な情報を描出する画像。壁把握および性状評価が可能。
○形態診断: 白黒のメリハリを付け、構造物を強調した画像。形態把握を主目的とする。
2.4 有機ELモニターによるコントラスト分解能の向上超音波診断装置の基本モードであるBモードは、Bright-
nessモードの略で、白黒の階調性つまり白黒の濃淡のみで生体組織の内部構造を表現する。この濃淡表現の重要な性能指標として、コントラスト分解能が挙げられる。超音波画像を表示するモニターの白黒の階調表現が豊かでなければ、つまりコントラスト比が高くなければ、高コントラスト分解能は実現できない。有機EL(Electro-luminescence)モニターは、素子の自発
光であり、黒の映像を表現する際、各素子を発光させない制御をすることで黒が明確に表現でき、高コントラスト比を実現できる。液晶モニターのコントラスト比が、高性能な物でも1000:1程度であるのに対し、有機ELモニターは25万:1を達成している。超音波診断装置のモニターとして非常に適したデバイスと言える。
3.Seamless Workflow
3.1 操作パネル超音波検査は、1人の検査者が、片手でプローブを被検査
者に当て、モニターに表示された超音波画像を観察しつつ、もう片方の手で操作パネルを操作する。画像観察に集中するため、モニターから視線が移動しないことが望まれる。ルーチン検査において、超音波スキャン中の連続的な操作が必要な代表例として、ドプラ波形の計測が挙げられる。まず断層像がアクティブの状態において“トラックボール(以下T.B.)”でドプラサンプルゲート位置を合わせ、次に“Update”スイッチでドプラのスキャンをスタートし、所望の画像が得られたら“Freeze”スイッチで画像の更新を止め、最後にStoreスイッチで画像を保存する。途中で超音波画像を表示するモニターから目を離して操作パネルを確認すると、スキャン断面がずれて良好なドプラ波形が得られない場合がある。そこで、ALO-
KA LISENDO 880では、パームレスト付近をホームポジションとし、上記ドプラ波形の計測操作を、ホームポジションに掌の位置を固定したまま手元に視線を移すことなく操作で
図10:“eFocusing” Off(左)とOn(右)
図11:質的診断に適した画像(左)と形態診断に適した画像(右)
26 〈MEDIX VOL.66〉
信信号を合成しているため、信号雑音比の向上効果も得られ、ペネトレーションが向上する。図10に“eFocusing”により得られたBモード画像の例を示す。このように、“eFocusing”では、送受信ダイナミックフォーカシング効果により、従来の問題点であった送信フォーカス依存が軽減され、送信フォーカス深度の設定が不要となる。また、高画質かつ高ペネトレーションなBモード画像の提供により、検査時間短縮などワークフローの改善にも貢献する。
2.3 Active Backendによる高画質化と、検査者および被検査者に合わせた画質調整幅の確保
超音波画像診断は、検査者による調整や好みの差など検査者依存性がある。また、被検査者の体質や体格による被検査者依存性もある。そのため、画像調整の幅の広さが求められる。
ALOKA LISENDO 880は、従来の製品ラインナップであるProSoundシリーズ、HI VISIONシリーズ、ARIETTA※4シリーズの開発で培った、超音波画像診断に特化したさまざまな画像調整パラメーターを兼ね備え、質的診断に適した画像から、形態診断に適した画像までを実現可能な画質調整の幅を持っている(図11)。その結果、課題となっていた検査者依存や被検査者依存の低減が可能になった。
○質的診断: ダイナミックレンジが広く、心筋のより詳細な情報を描出する画像。壁把握および性状評価が可能。
○形態診断: 白黒のメリハリを付け、構造物を強調した画像。形態把握を主目的とする。
2.4 有機ELモニターによるコントラスト分解能の向上超音波診断装置の基本モードであるBモードは、Bright-
nessモードの略で、白黒の階調性つまり白黒の濃淡のみで生体組織の内部構造を表現する。この濃淡表現の重要な性能指標として、コントラスト分解能が挙げられる。超音波画像を表示するモニターの白黒の階調表現が豊かでなければ、つまりコントラスト比が高くなければ、高コントラスト分解能は実現できない。有機EL(Electro-luminescence)モニターは、素子の自発
光であり、黒の映像を表現する際、各素子を発光させない制御をすることで黒が明確に表現でき、高コントラスト比を実現できる。液晶モニターのコントラスト比が、高性能な物でも1000:1程度であるのに対し、有機ELモニターは25万:1を達成している。超音波診断装置のモニターとして非常に適したデバイスと言える。
3.Seamless Workflow
3.1 操作パネル超音波検査は、1人の検査者が、片手でプローブを被検査
者に当て、モニターに表示された超音波画像を観察しつつ、もう片方の手で操作パネルを操作する。画像観察に集中するため、モニターから視線が移動しないことが望まれる。ルーチン検査において、超音波スキャン中の連続的な操作が必要な代表例として、ドプラ波形の計測が挙げられる。まず断層像がアクティブの状態において“トラックボール(以下T.B.)”でドプラサンプルゲート位置を合わせ、次に“Update”スイッチでドプラのスキャンをスタートし、所望の画像が得られたら“Freeze”スイッチで画像の更新を止め、最後にStoreスイッチで画像を保存する。途中で超音波画像を表示するモニターから目を離して操作パネルを確認すると、スキャン断面がずれて良好なドプラ波形が得られない場合がある。そこで、ALO-
KA LISENDO 880では、パームレスト付近をホームポジションとし、上記ドプラ波形の計測操作を、ホームポジションに掌の位置を固定したまま手元に視線を移すことなく操作で
図10:“eFocusing” Off(左)とOn(右)
図11:質的診断に適した画像(左)と形態診断に適した画像(右)

5− − 〈MEDIX VOL.66〉 XX-E231
tion of the various switches, the scanning plane can easily shift, and good Doppler waveforms may not be obtained. To avoid such errors with LISENDO 880, the area around the palm rest is designated as the home position, with the “T.B.,” “Update,” “Freeze & Gain,” and “Store” switches positioned so that the user can obtain the Doppler waveform with the palm of his hand fixed, without the need to look down (Fig-ure 12 (a)). By ensuring the depth of the palm rest, twisting of the wrist can be reduced when the palm is fixed on the home position, such as when measuring Doppler waveforms as described above (Figure 12 (a)).
In LISENDO 880, the “L” and “R” switches have been added to “Enter” and “Undo” to be also operable with the palm resting in the home position (Figure 12 (b)). With an increasing number of short-cuts added, complicated func-tions such as Cardiac 3D and cardiac function analysis, in-creasingly used in routine examinations, will be made easier and more intuitive.
Moreover, in cardiovascular ultrasound, the frequent-ly-used Time Gain Control (TGC) has been positioned on the lower left side of the operating console (Figure 12 (b)) for the first time in a Hitachi product. The arrangement of the frequently used B Gain and TGC in the front, combined with the easy-to-access position of the operating console, streamline workflow during the examination.
3.2 Automatic setting of the Doppler sample gate
The setting of a sample gate for Doppler measurement requires the examiner to operate the T.B. while applying the transducer to the patient. To reduce the burden, an automatic function to set the sample gate position has been developed.
Firstly, the system performs image recognition of the B-mode to determine the type of the section that is being dis-played. Next, on the same image, it automatically estimates the position of the sample gate. The automation of these tasks has been made possible through machine learning techniques where a large number of images and gate posi-
tions set by technologists have been collected and analyzed by the algorithms of machine learning to create a database. This is incorporated into the system and referenced as need-ed to perform the automatic setting (Figure 13). The use of machine learning is intended to improve accuracy and versa-tility, automatically selecting the same sample gate position as the examiner would do manually.
This function performs the recognition processing in transition to Doppler mode and allows the sample gate to be automatically set in the left ventricular inflow tract. In Dual Gate Doppler mode, furthermore, the sample gate for Tissue Doppler Imaging (TDI) is automatically set in the wall adja-cent to the left ventricular annulus as well (Figure 14). This function should popularize the usage of Dual Gate Doppler, which, although of clinical benefit, involves the complicated procedure of setting sample gates in two different locations.
3.3 Automatic detection of end-diastole (Ed) and end-systole (Es)
In Simpson’s measurement and others, analysis using B-mode images obtained in end-diastole (Ed) and end-sys-tole (Es) are an essential part of the routine examination. LISENDO 880 automatically detects Ed (R wave) and Es (T-wave end) by analyzing the ECG signals when the “Freeze” is selected and instantaneously displays images at
Figure 12: Operating console
Figure 13: Automatic recognition processing using machine learning
Figure 14: Automatic setting of sample gates in Dual Gate Doppler
(a) Home position
(b) From the left, TGC, “L” switch, and “R” switch
Extracted image Automatic recognition / measurement results
Machine-learned cross-sections, trace lines, measurement points, and sample gate locations are incorporated into a database which is imported into the diagnostic ultrasound system.
Performs automatic recognition processing with reference to the learned database.・Sample gate location detection processing ・Cross-section type determination processing ・Trace line extraction processing ・Measurement point setting processing

6− − 〈MEDIX VOL.66〉 XX-E231
these phases side by side in dual screen mode (Figure 15). This functionality significantly reduces examination time re-moving the need to search for Ed and Es frames when using measurements such as Simpson’s method.
3.4 Automated Cardiac Measurement
Automation of measurements such as heart function mea-surement, Simpson’s measurement (Disc method in the LV, LA, and RA), FAC measurement, Teichholz measurement, and LA/AO (M-mode) measurement1) has made the exam-ination more efficient. Conventionally, these measurements involve a cumbersome number of tasks that include image (phase) selection, measurement cursor setting, and trace line setting, increasing the challenge of quantification. The measurement cursor is automatically set in an optimal posi-tion by an automatic recognition process similar to the auto-matic setting of the Doppler sample gate described earlier (Figure 13).
In Simpson’s measurement, B-mode images in Ed and Es obtained by the above-mentioned automatic Ed/Es detection are displayed on the screen side by side, and the endocardi-al lining is traced by the same function, resulting in a great synergistic effect (Figure 15).
4. Your Application4.1 VFM (Vector Flow Mapping)
It is predicted that myocardial wall motion causes com-plicated hemodynamics in the heart chambers, such as turbulence and vortices, that has an effect on systematic hemodynamics, myocardial walls, and so on. To date, this phenomenon has only been assessed from the myocardial wall motion as visualized by conventional Color Doppler and B-mode imaging. VFM is a technology that visualizes hemodynamics taking into consideration myocardial wall motion, and facilitating evaluation of blood flow functions. It can provide displays of Shear Stress on the cardiac wall and Relative Pressures in the heart chamber (Figure 16) 2)
3). VFM requires high temporal resolution for Color Doppler
analysis, and therefore in conventional systems, the VFM images display poorer spatial resolution than those used in the routine examination because priority is given to tempo-ral resolution. This has hampered the adoption of VFM anal-ysis. The “HI Framerate” capability of LISENDO 880 strikes a balance between high spatial resolution and high temporal resolution in Color Doppler imaging, allowing VFM analysis to have the same feel as the routine examination. What can be expected in the future includes a new perspective on car-diac evaluation, such as the use of the Energy Loss function4) in the prognosis of heart failure, and clinical usefulness of the relative pressure difference, which changes with deterio-rating left ventricular function.
4.2 Heart failure diagnostic package (VFM, Dual Gate Doppler and R-R Navigation)
With the current globally aging population, the incidence of heart failure is increasing. As roughly half of the patients will have atrial fibrillation (AF) and the other half have heart failure with a preserved ejection fraction (HFpEF) where the left ventricular ejection fraction (LVEF) is preserved, pa-tients with AF and HFpEF are also on the rise5) 6).
In patients with HFpEF, a diagnostic index that replaces LVEF is required. LISENDO 880 comes equipped with VFM, a function capable of visualizing hemodynamics as described in section 4.1. Intracardiac hemodynamics are expected to stagnate in patients with a myocardial wall abnormality. In such a case, the heart muscle acting as a pump responds by bringing hemodynamics back to normal with the resultant overload on the myocardium. This overload results in de-creased myocardial motion and leads to heart failure. VFM can capture early changes in the hemodynamics by Energy loss, Relative pressure, and other parameters.
What can be expected from this capability is that a car-diac overload can be predicted based on the hemodynamic state even in the case of diastolic heart failure.
In the case of atrial fibrillation, on the other hand, mea-surements should be made in the correct phase to factor in the effect of coexisting arrhythmia. Especially in the case of HFpEF in which the possibility of congenital heart dis-ease is excluded, diastolic function index E/e’ is crucial in determining whether or not it is treatable. LISENDO 880 is equipped with R-R Navigation – a function that can instanta-
�15�Ed����Es����������������2� �����Simpson�������������
�15�Ed����Es����������������2� �����Simpson�������������
Figure 15: Ed (purple) and Es (orange) are automatical-ly detected and displayed side by side on the screen (below), and Simpson Auto Tracing is performed (above)
Figure 16: VFM (Relative Pressure) function

7− − 〈MEDIX VOL.66〉 XX-E231
neously search out a phase in which the R-R interval is the same as in the previous 2 waveforms – to help as a navigator in determining the correct phase in the event of arrhythmia. Furthermore, it is not always possible to obtain the optimal phase because in Doppler mode the optimal heart rate is de-termined from a spectrum of several heart beats, although B-mode images can provide abundant information on heart rate that is used by the navigator for phase determination. In such a case, the combined use with Dual Gate Doppler is expected to be beneficial so that the left ventricular inflow velocity waveform obtained by PW mode and the left ven-tricular annulus velocity waveform obtained TDI PW mode can be displayed in the same phase to calculate E/e’ (Figure 17)7)-9).
5. Ergonomic design5.1 System design to prevent Visual Display Terminals
(VDT) syndrome
In ultrasound examinations, the operator applies the transducer to the patient with one hand and manipulates the operating console with the other while observing the ultrasound images displayed on the monitor. Depending on the region being examined or the examination environment, the examiner often needs to twist his body position in an un-natural way during the examination which can place a large physical burden on him 10).
LISENDO 880 has been designed with a focus on reduc-ing the burden on the examiner’s neck and shoulders to prevent VDT syndrome. The console panel arm and monitor arm have a large range of motion to allow the examiner to maintain the optimal working posture either in the seated or standing position (Figures 18 (a) and 18 (b)).
Operating console: Moves up and down by 700-1000 mm and swivels by 25 degrees
Monitor: Moves up and down by 172 mm, swiv-els 360 degrees, and slides back and forth by 224 mm
As a result, the line of sight in the seated position falls about 10 degrees below the horizontal, as recommended by the Japan Society of Ultrasonics in Medicine 11). Further-more, another joint is added to the monitor arm so that the monitor can move smoothly back and forth in parallel to make it easy to adjust to the optimal distance for each ex-aminer (Figure 18(c)). Although such measures would be likely to increase the size of the system, a compact body size is realized as well.
5.2 Cable management
Challenges in the design of the body of the diagnostic ultrasound system include measures against VDT syndrome and improved management of transducer cables. In conven-tional models, transducer cables can get entangled when-ever the examiner switches transducers during or between examinations.
LISENDO 880 has multiple side hooks on both sides of the operating console, one dedicated to each probe holder.
The side hook is designed for the cable to be rolled up in a way such that when the probe is held in the holder the direction of the cable is horizontal to the direction in which the transducer is removed from the holder (Figure 19 (a)). As a result, when removed, the cable does not easily get en-tangled with the cable of other transducers. (Figure 19 (b)).
Consideration has also been given to the form, material and processing so that the cable can be pulled out smoothly, but is also held securely on the hook.
To be easily located, the hooks are designed to protrude from the sides of the console, at an angle against the root
Figure 17: Combined use of R-R Navigation and Dual Gate Doppler
Figure 18: Range of motion of the operating console and monitor
(a) Range of motion of the body (horizontal)
(c) Back and forth move-ment of the monitor
(b) Range of motion of the body (vertical)

8− − 〈MEDIX VOL.66〉 XX-E231
(a) Cables cannot be entangled
(c) Retractable hooks
(b) Cables do not entangle when the transducer is tak-en out
of the cable so that it is easily pulled out through the hook. They are also designed to retract under the console with a single touch so they can be folded away when the system is used in a small examination room or being moved to another place. Even in the retracted position, the hooks are designed to allow cables to be pulled out smoothly or held firmly (Fig-ure 19 (c)).
6. Conclusion
“LISENDO 880” provides more accurate “understanding of hemodynamics,” the basis of cardiovascular evaluation. With detailed analysis, it also provides information on the “efficient motion and pressure distribution of blood flow,” which has not been possible to investigate in the past. For all to live in safety and security in a society filled with smiles, we move forward with innovation in healthcare global team work.
*1 LISENDO, *2 Prosound, and *3 ARIETTA are registered trademarks of Hitachi, Ltd.
References
1) RM Lang, et al.: Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults. Journal of the American Society of Echocardiography, 28: 1-39, 2016.
2) Keiichi Itatani, et al.: The novel Insights into Cardiovas-cular Imaging Techniques with the Flow Visualization Method:The present conditions and the prospects of the Echocardiography Flow Visualization Method named VFM (Vector Flow Mapping). MEDIX VOL.60: 17-21.
3) Itatani K, et al.: Intraventricular Flow Velocity Visualiza-tion Based on the Continuity Equation and Measurements of Vorticity and Wall Shear Stress. Japanese Journal of Applied Physics 52(2013): 07HF16-1-6.
4) Damien G, et al.: Assessment of Aortic Valve Stenosis Se-verity. A New Index Based on the Energy Loss Concept. Circulation. 2000; 101: 765-771.
5) Sherif N, et al.: Recommendation for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiogra-
phy and European Association of Cardiovascular Imaging. J Am Soc Echocardiography 2016; 29: 277-314.
6) Hiroyuki I, et al.: Altered Spatial Distribution of the Dia-stolic Left Ventricular Pressure Difference in Heart Fail-ure: J Am Soc Echocardiography 2015; 28: 597-605.
7) Kusunose K, et al.: Clinical Utility of Single-Beat E/e’ Obtained by Simultaneous Recording of Flow and Tissue Doppler Velocities in Atrial Fibrillation With Preserved Systolic Function. JACC VOL.2, NO.10, 2009OCTO-BER2009: 1147-56
8) Hirotsugu Yamada, et al.: Evaluation of Left Ventricle Diastolic Function using Dual Doppler Method. Rad Fan Vol.6 No.3 (2008): 1-4.
9) Wada Y, et al.: Simultaneous Doppler Tracing of Transmi-tral Inflow and Mitral Annular Velocity as an Estimate of Elevated Left Ventricular Filling Pressure in Patients with Atrial Fibrillation. Circulation Journal Vol.76, March 2012: 675-681.
10) Masaru Maruyama, et al.: Does the Changing position at Abdominal Ultrasonography Reduce the Physical Load on the Ultrasonographer? – Second Report –.
11) Ultrasound Equipment and Safety Committee, The Japan Society of Ultrasonics in Medicine. Recommendations for Sonographers to Work Safely, Comfor tably and Healthfully – Equipment and working environment to prevent work-related musculoskeletal disorders and eye disorders –. 2012.
Figure 19: Cable management