Development and Implementation of a Nurse Led Enteral ...
14
Development and Implementation of a Nurse Led Enteral Feeding Protocol Joanne Roddick Clinical Dietitian RBWH 1 AH-TRIP
Transcript of Development and Implementation of a Nurse Led Enteral ...

Development and Implementation of a Nurse Led Enteral Feeding Protocol
Joanne Roddick
Clinical Dietitian RBWH
1
AH-TRIP

What is the clinical problem?
2
7th most commonly diagnosed cancer in
Australia1
Head and Neck Cancer
RBWH (ENT/MaxFacs/Plastics) Data
➢ 20% increase in # surgeries, no change to Dietetic FTE
➢ 40% (n=29) of patients did not commence enteral feeds
within 24 hours of surgery
➢ Delays in achieving goal feeding rates
Surgery is often first line of treatment → many
patients require enteral feeding post-op2

What is the evidence?
3
COSA: Head and neck cancer nutrition
guidelines (2015):
Post operative tube feeding should commence
within 24 hours (Grade A)3
SCCM + A.S.P.E.N: Guidelines for the provision
and assessment of nutrition support therapy in
the adult critically ill patient (2016):
We recommend that enteral feeding protocols be
designed and implemented to increase the overall
percentage of goal calories provided.
(Moderate to High)4

What is the evidence?
4
➢ Provision of nutrition support in
immediate post operative period
improves healing and reduces
complications5-8
➢ In critical care setting,
standardised protocols provide a
standard to care to guide practice
to result in the provision of timely
nutrition support9-12

Implementation
5
Knowledge to Action
Framework
1. Identify problem and
review knowledge. Data
audited over 9 month
period
2. Adapt knowledge to
context by consulting
nursing staff and surgeons
during protocol
development
3. Assess barriers through
focus groups and one-on-
one interactions

Addressing Barriers to Implementation
6
1. Belief that initiation of enteral feeds is not part of nursing role.
➢ Nursing Champions identified to pilot and lead
implementation
➢ Education to address specific concerns raised in pre-
implementation discussions
2. Lack of knowledge around which enteral feed to use and
lack of clarity around enteral feed starting rates
➢ Revised enteral feed forms in line with protocol clearly
stating which enteral feed to use and starting rates made
easily available on ward
➢ Posters placed on ward for staff to refer to and increase
awareness


8
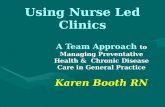
ROYAL BRISBANE AND WOMEN’S HOSPITAL DO NOT FILE IN MEDICAL NOTES
ENT/MaxFacs/Plastics
ENTERAL FEEDING REGIMEN
UR No: Surname: Given Name: Sex:
EN
TE
RA
L F
EE
DIN
G R
EG
IME
N
• ALLERGEN INFORMATION: This feed product contains milk protein and fish oil: it is not suitable for those with anaphylaxis to dairy or fish products. Please contact the dietitian for alternative options.
• Please record all feed and flushes delivered to the patient on the fluid balance chart.
• This order remains current until changed or ceased by the Dietitian or Medical Team.
Feeding method: Continuous Weight: ____________
Please select one feeding regimen only
Refer to “ENT/MaxFacs/Plastics Enteral Nutrition Pathway”
Standard Feeding Regimen (Non-Refeeding Risk)
START DATE
TIME OF FEED
FEED
DURATION
RATE (ml/hr)
COMMENTS
On commencement Nutrison Protein Plus
Multifibre
4/24 40ml/hr If tolerated increase to goal until 2200hrs
0600-2200 Nutrison Protein Plus
Multifibre
16/24 GOAL
____mL/hr
Refer to Dietitian
Refeeding Risk Regimen
On commencement Nutrison
Multifibre 16/24 40ml/hr Refer to Dietitian
FLUSHES: Continuous Feeds flush:
If on IV fluids: 60ml q4/24 If nil IV fluids: 120ml q4/24 Always give a water flush:
- whenever feeding is temporarily stopped (minimum of 40ml) or at least daily if not being used for feeds
- 30ml before medications, 5ml between each medication and 30ml after all medications given via tube
Total fluid volume = ________ml/ day (Feed = ________ml/ day ; Flush = ________ml/ day)
NOTE:
• Confirm tube placement before commencing feeds and document in medical chart using Enteral Nutrition insertion sticker
• Ensure the head of bed is elevated during gastric feeding and for at least 30 minutes after feeding
• Ready to hang bottles and giving sets can hang for no longer than 24 hours
• Record the time feeding was commenced on label on Ready to hang bottle
• If oral Phenytoin or Ciprofloxacin is administered, cease feeds 2 hours prior & recommence feeds 2 hours post administration and extend feeds for an extra 4hours and request dietitian review of feed times.
• Ensure the patient has a medication review by the ward pharmacist
• If there is pain on feeding or flushing of feeding tubes, stop feed/medication immediately and refer to the treating team.
Completed by _________________ Contact__________

Monitoring
9
➢August 2017-August 2018
➢Comparison of time to
commencing enteral feeds and
time to goal rate to baseline data
➢Survey to be conducted with
MDT to determine gaps in
knowledge and awareness of
protocol.

Outcomes
10
➢100% (n=9) of patients have had enteral feeds initiated within
24 hours and achieved goal rate within average of 2 days.
ANECDOTALLY:
➢ Reduced pressure on Dietetic
workload
➢Nurses report high levels of
autonomy
➢‘We love being able to start
patient feeds as soon as
possible’
➢‘Very easy to use protocol’
➢We love having our own
enteral feed protocol’

Looking Forward
11
➢Development of Work Unit Guideline (WUG)
➢Enteral feeding form to be uploaded to intranet for easier
access by staff
➢Exploring how to embed protocol into standard practice for
sustainability

References
12
1. Australian Institute of Health and Welfare. Head and neck cancers in Australia [Internet] 2014 [cited October 18th 2017]. Available
from http://www.aihw.gov.au/publication-detail/?id=60129547291
2. Australian Government Cancer Australia. Head and Neck Cancer. Treatment Options [Intenet] 2015 [cited October 18th 2017].
Available from
http://headandneckcancerguide.org/adults/cancer-diagnosis-treatments/surgery-and-rehabilitation/cancer-removal-surgeries/
3. Findlay, M., Bauer, J., & Brown, T. (2015). Evidence-based practice guidelines for the nutritional management of adult patients with
head and neck cancer-Cancer guidelines Wiki. Wikicancerorgau. 2015. wiki. cancer. org. au/australia/COSA:
Head_and_neck_cancer_nutrition_guidelines. Accessed, 20th June 2017
4. McClave, S. A., Martindale, R. G., Vanek, V. W., McCarthy, M., Roberts, P., Taylor, B., ... & American College of Critical Care
Medicine. (2009). Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of
Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN). Journal of Parenteral and Enteral
Nutrition, 33(3), 277-316.
5. Abunnaja, S., Cuviello, A., & Sanchez, J. A. (2013). Enteral and parenteral nutrition in the perioperative period: state of the art.
Nutrients, 5(2), 608-623.
6. Kratzing, C. (2011). Pre-operative nutrition and carbohydrate loading. Proceedings of the Nutrition Society, 70(3), 311-315.
7. Stoppe, C., Goetzenich, A., Whitman, G., Ohkuma, R., Brown, T., Hatzakorzian, R., ... & Yeh, D. (2017). Role of nutrition support in
adult cardiac surgery: a consensus statement from an International Multidisciplinary Expert Group on Nutrition in Cardiac Surgery.
Critical Care, 21(1), 131.
8. Weimann, A., Braga, M., Carli, F., Higashiguchi, T., Hübner, M., Klek, S., ... & Waitzberg, D. L. (2017). ESPEN guideline: Clinical
nutrition in surgery. Clinical Nutrition, 36(3), 623-650.
9. Stewart, M. L. (2014). Interruptions in enteral nutrition delivery in critically ill patients and recommendations for clinical practice.
Critical care nurse, 34(4), 14-22.
10. Friesecke, S., Schwabe, A., Stecher, S. S., & Abel, P. (2014). Improvement of enteral nutrition in intensive care unit patients by a
nurse‐driven feeding protocol. Nursing in critical care, 19(4), 204-210.
11. Compton, F., Bojarski, C., Siegmund, B., & van der Giet, M. (2014). Use of a nutrition support protocol to increase enteral nutrition
delivery in critically ill patients. American Journal of Critical Care, 23(5), 396-403.
12. Mackenzie, S. L., Zygun, D. A., Whitmore, B. L., Doig, C. J., & Hameed, S. M. (2005). Implementation of a nutrition support protocol
increases the proportion of mechanically ventilated patients reaching enteral nutrition targets in the adult intensive care unit. Journal
of Parenteral and Enteral Nutrition, 29(2), 74-80.
13. Straus, S. E., Tetroe, J., & Graham, I. (2009). Defining knowledge translation. Canadian Medical Association Journal, 181(3-4), 165-
168.

13
➢ Ward 8AN
➢ Claire Blake
➢ Adrienne Young
➢ Nutrition and Dietetics
Department RBWH

14
Produced by Allied Health
Metro North and Metro South Hospital and Health Service
http://qheps.health.qld.gov.au/TRIP
State of Queensland (Metro North and Metro South Hospital and Health Service) 2018