Design criteria for a Total Knee prosthesis for the Indian population
92
Dr L.Prakash M.S. (orth), MCh (orth)
-
Upload
l-prakash -
Category
Healthcare
-
view
458 -
download
0
Transcript of Design criteria for a Total Knee prosthesis for the Indian population
Dr L.Prakash M.S.
(orth), MCh (orth)









Can this surgery be done in smaller district level hospitals??






Medial tibiofemoral
Lateral tibiofemoral
Patellofemoral













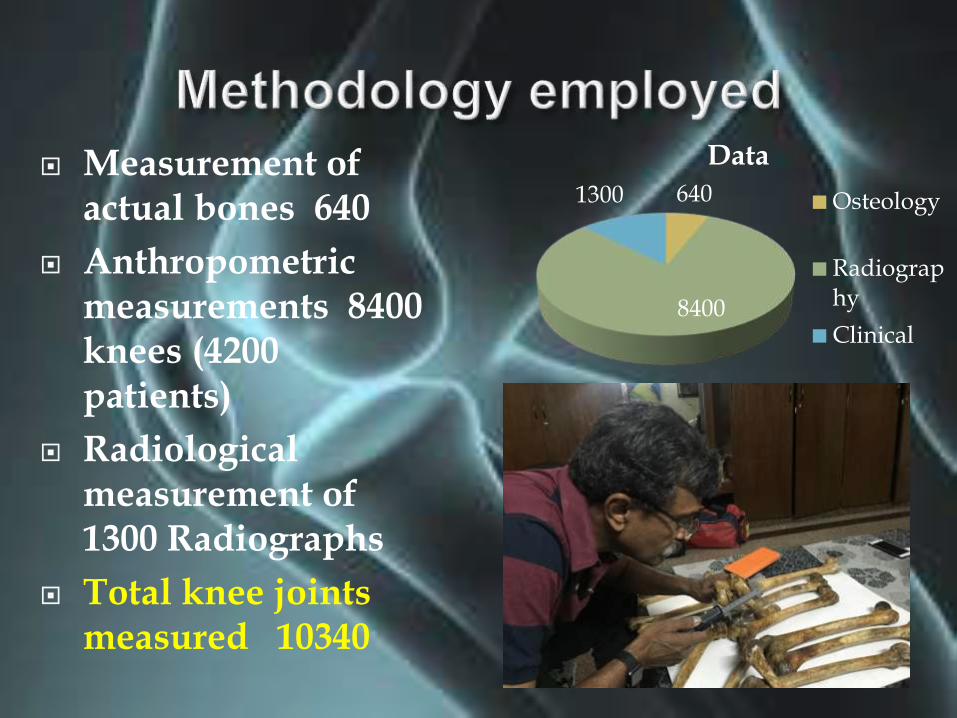
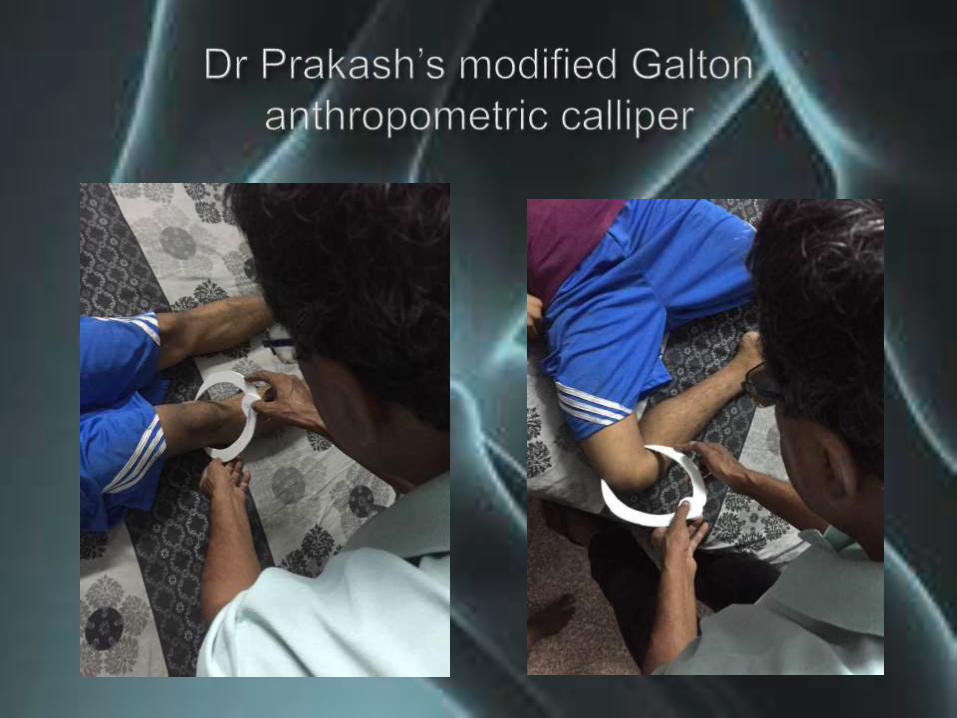
Measurement of actual bones 640
Anthropometric measurements 8400 knees (4200 patients)
Radiological measurement of 1300 Radiographs
Total knee joints measured 10340
640
8400
1300
Data
Osteology
Radiography
Clinical
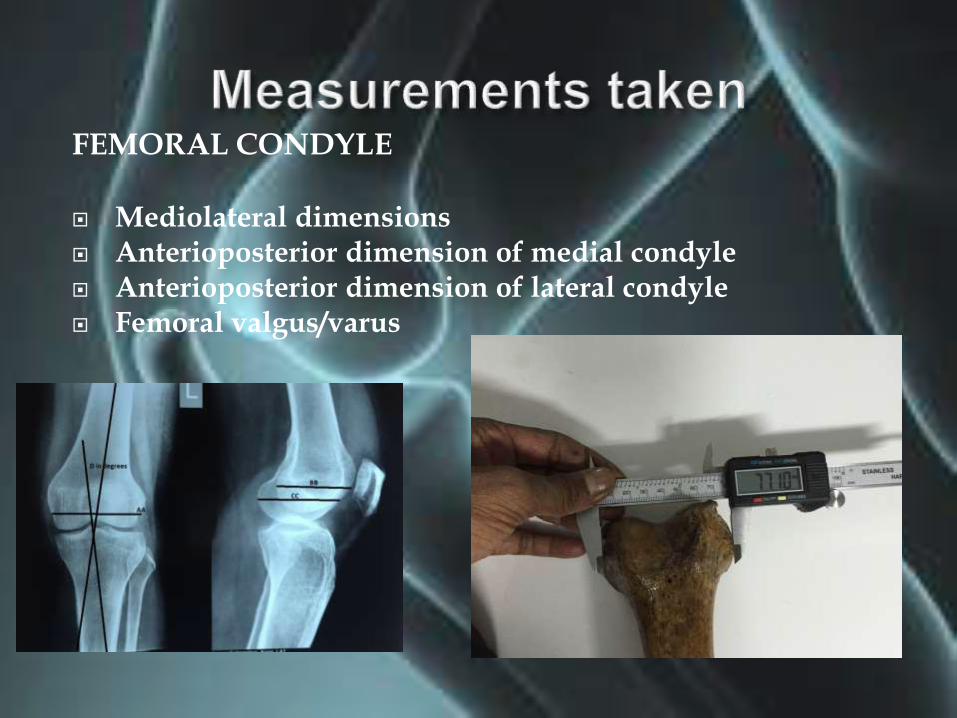
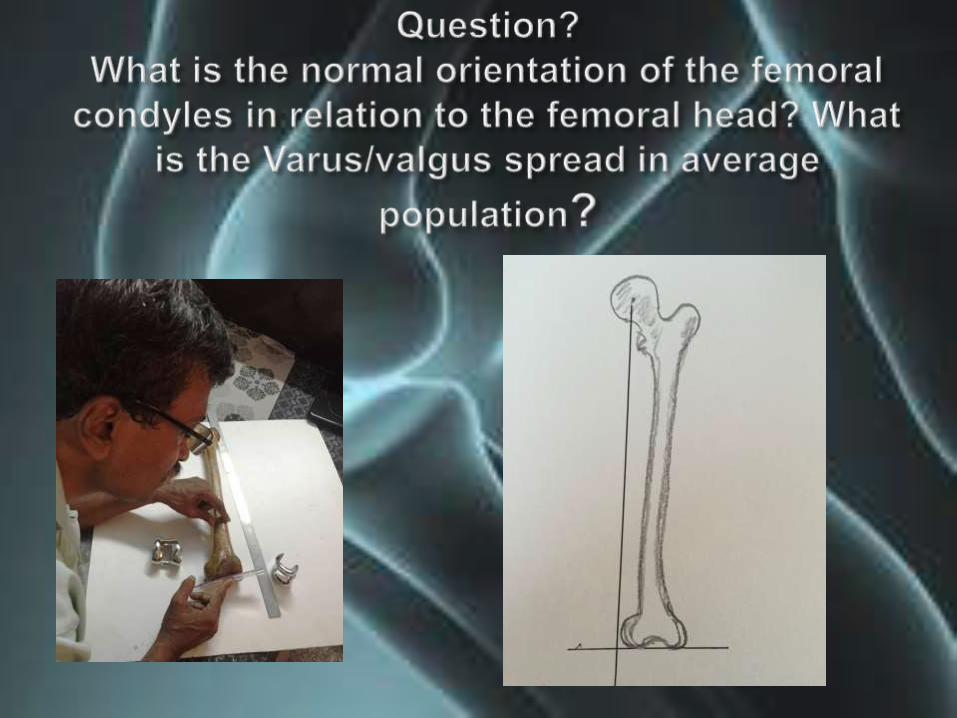
FEMORAL CONDYLE
Mediolateral dimensions Anterioposterior dimension of medial condyle Anterioposterior dimension of lateral condyle Femoral valgus/varus
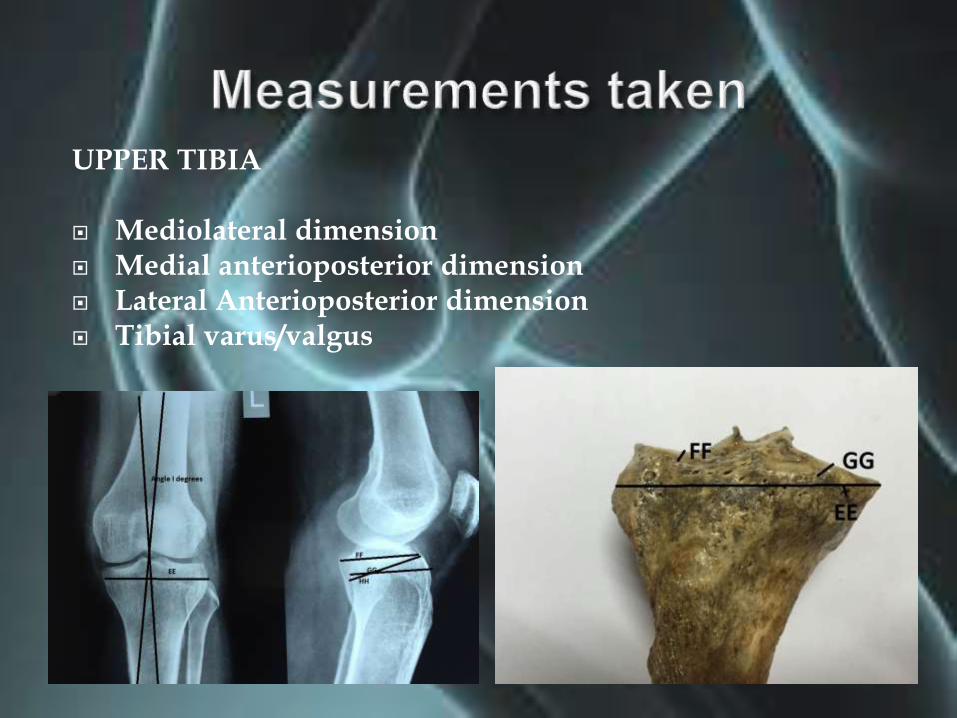
UPPER TIBIA
Mediolateral dimension Medial anterioposterior dimension Lateral Anterioposterior dimension Tibial varus/valgus
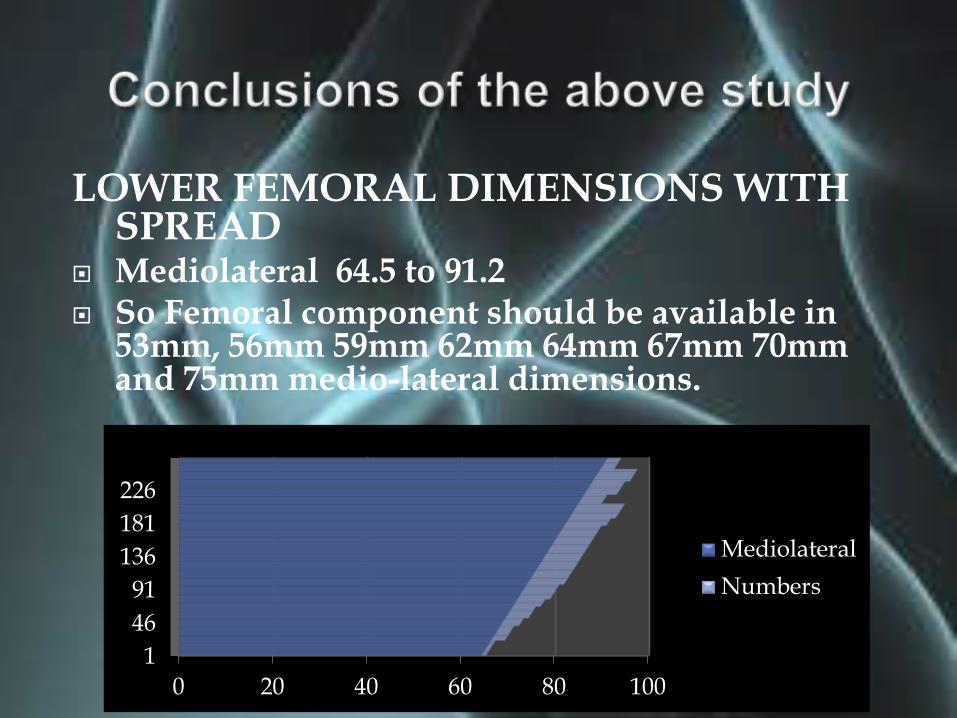
LOWER FEMORAL DIMENSIONS WITH SPREAD
Mediolateral 64.5 to 91.2 So Femoral component should be available in
53mm, 56mm 59mm 62mm 64mm 67mm 70mm and 75mm medio-lateral dimensions.
0 20 40 60 80 100
1
46
91
136
181
226
Mediolateral
Numbers
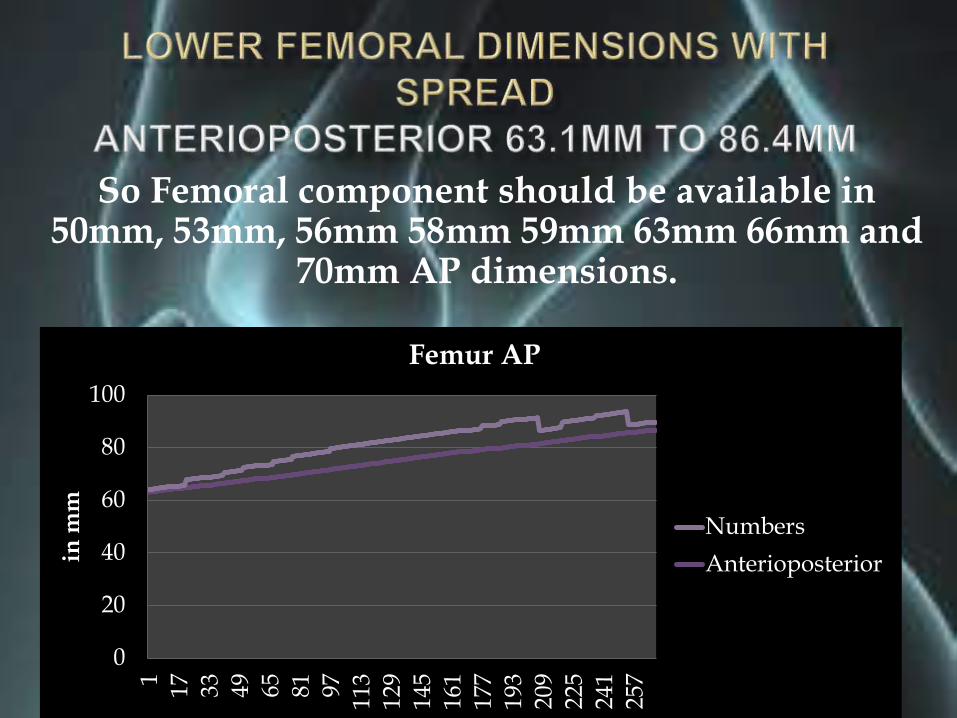
So Femoral component should be available in 50mm, 53mm, 56mm 58mm 59mm 63mm 66mm and
70mm AP dimensions.
0
20
40
60
80
100
1 17 33 49 65 81 97 113
129
145
161
177
193
209
225
241
257
in m
m
Femur AP
Numbers
Anterioposterior

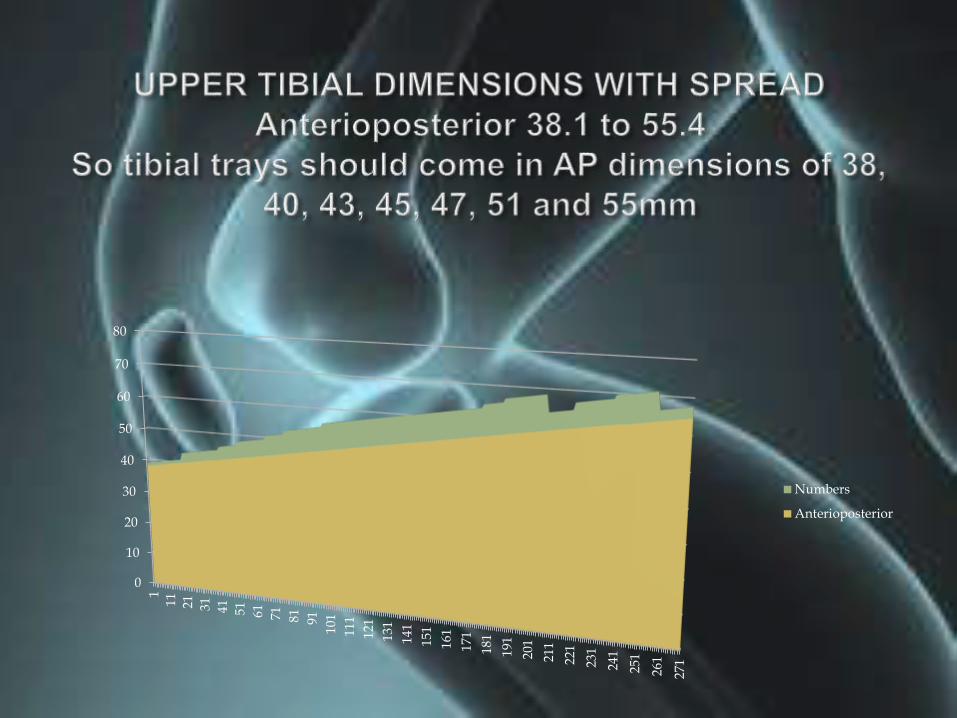
UPPER TIBIAL DIMENSIONS WITH SPREAD
Mediolateral 54.2 to 81.2mm and thus the tibial trays should be available in 55mm, 60mm, 63mm, 66mm, 71mm, 75mm and 81mm
0
20
40
60
80
100
1 13 25 37 49 61 73 85 97 109
121
133
145
157
169
181
193
205
217
229
241
253
265
M-L
dim
en
sio
n
Tibial dimensions
0
10
20
30
40
50
60
70
80
1
11
21
31
41
51
61
71
81
91
101
111
121
131
141
151
161
171
181
191
201
211
221
231
241
251
261
271
Numbers
Anterioposterior

Should match dimensions of Indian Knees
Should be available in a wide range
Should be an anatomic model with separate left and right components
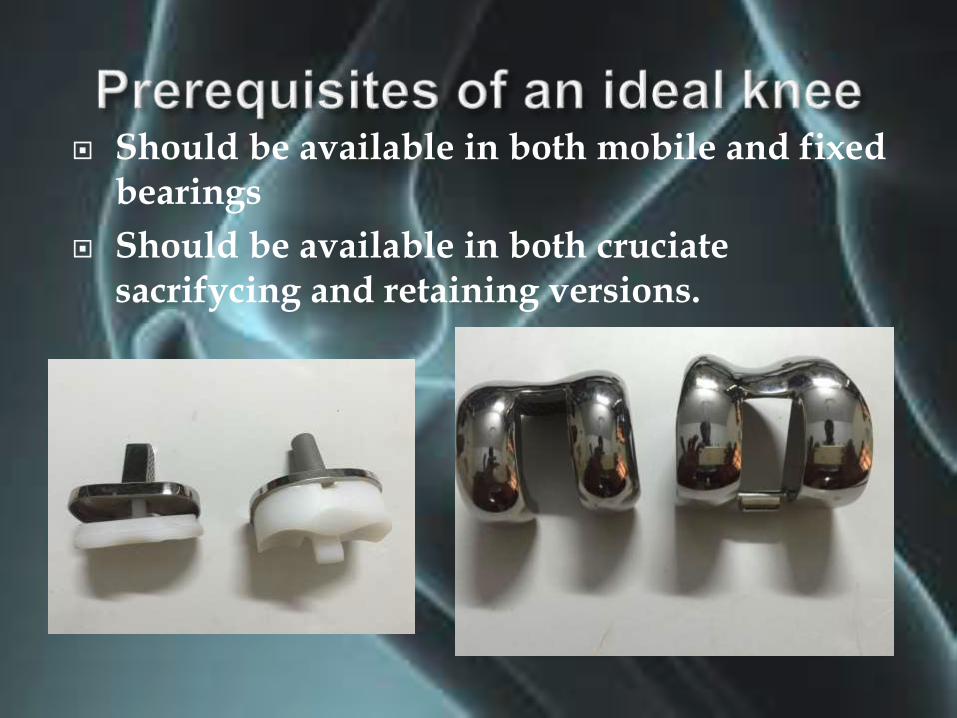
Should be available in both mobile and fixed bearings
Should be available in both cruciatesacrifycing and retaining versions.
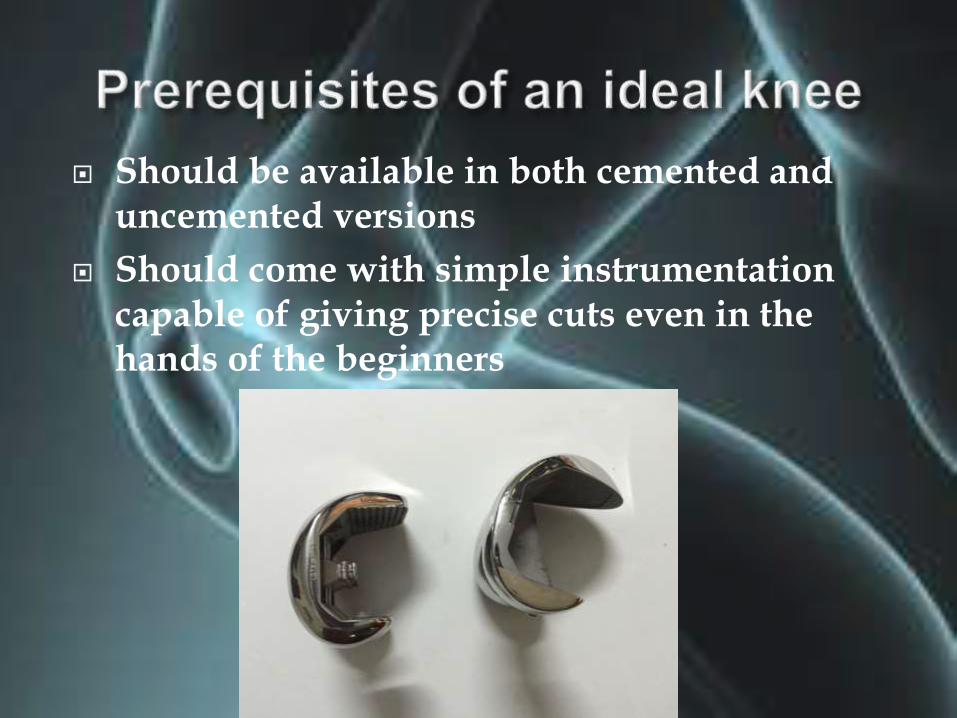
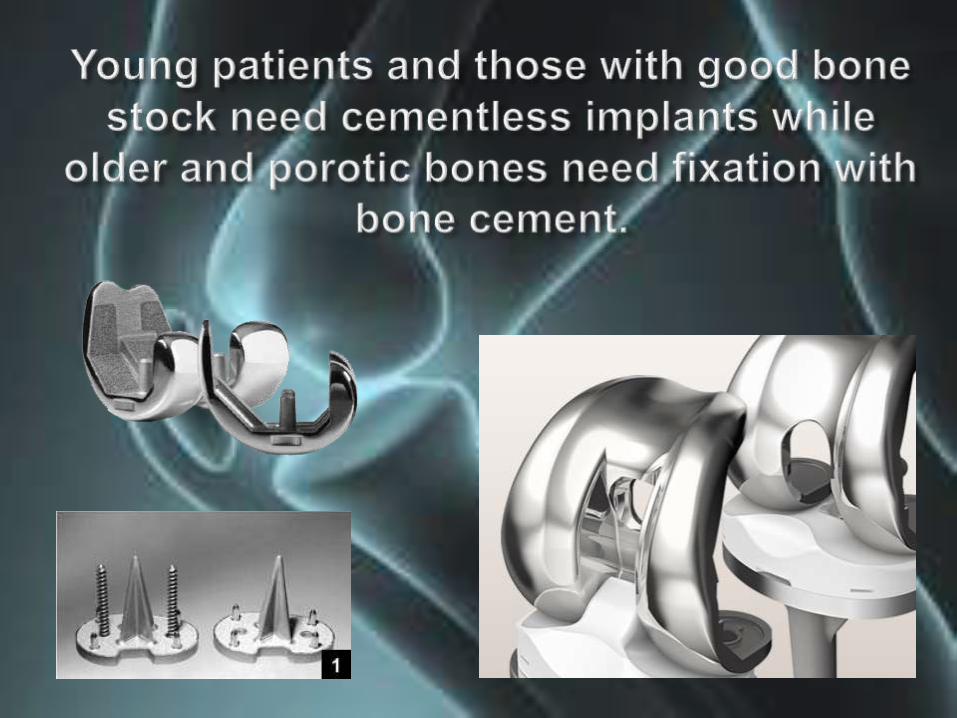
Should be available in both cemented and uncemented versions
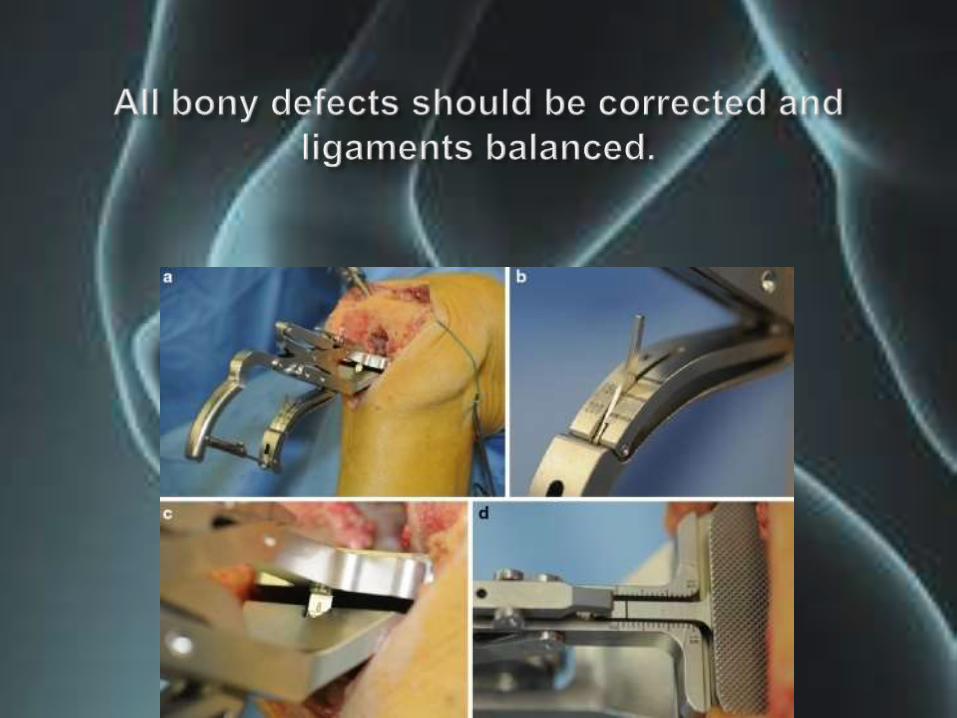
Should come with simple instrumentation capable of giving precise cuts even in the hands of the beginners
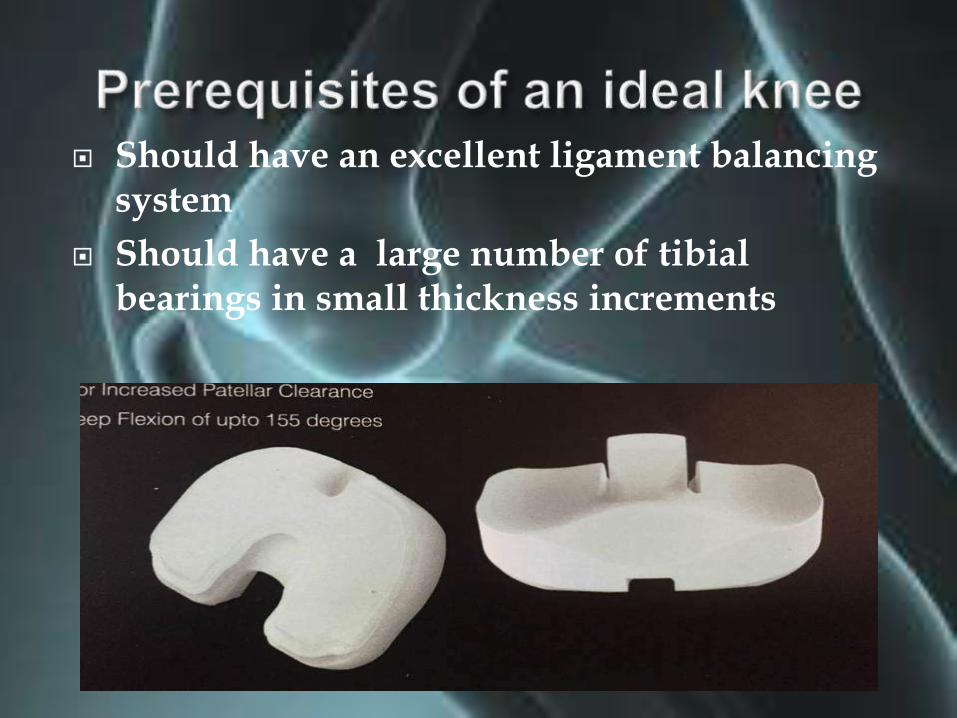
Should have an excellent ligament balancing system
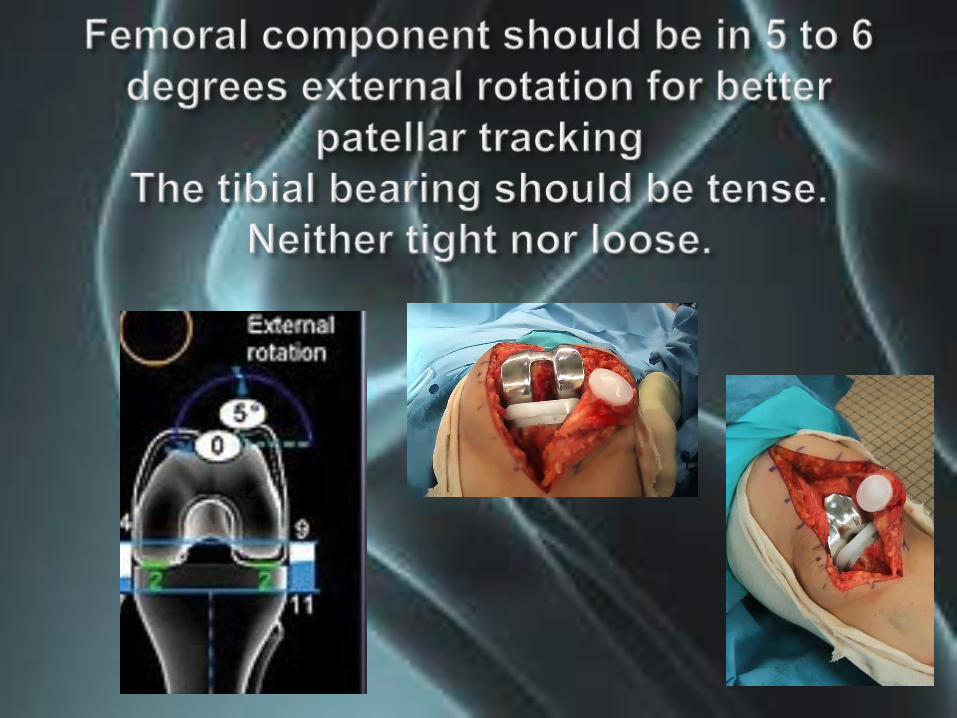
Should have a large number of tibialbearings in small thickness increments

The system should be modular with primary, revision and resection implants
Tibial metal-backs should come with medial and lateral wedges for bone defects

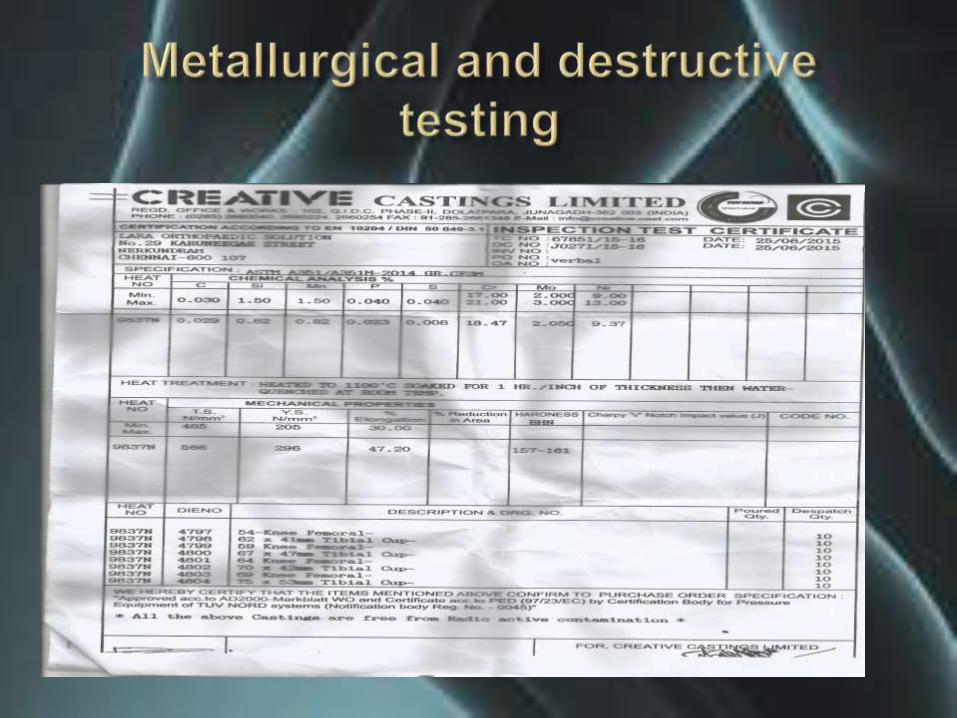
Should use ISO standard cobalt chrome castings and Virgin non irradiated UHMWUHDPE
Should be manufactured to ISO, USFDA and CE standards
Should be affordable

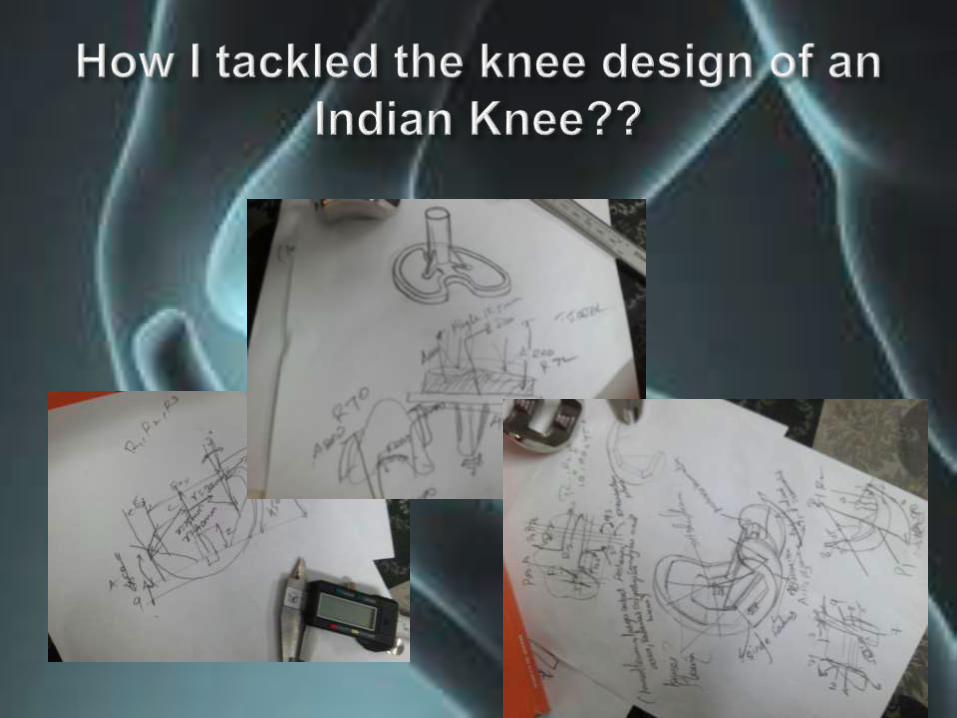
Dimensional studies followed by polymer clay models












8 left 8 right PCL sacrificing posterior stabilized femoral components
8 left and 8 right PCL retaining minimally constrained femoral components
( both of above in cemented and cementlessporous coated architecture)
7 tibial trays for fixed HDPE bearing
7 tibial trays for mobile bearing
Our knees will have 7 into 8 i.e. 56 HDPE inserts, either fixed or mobile, in small increments
Sizes will be 7,8,9,10.11.12.13.15,17mm
Patella, nonmetal backed will come in six sizes 26.29.32.35.38 and 41
1, Is it affordable?
2, Can it be done in district hospitals?
3, Is it time tested with clinical data?
4, How soon will it be available and at what cost?
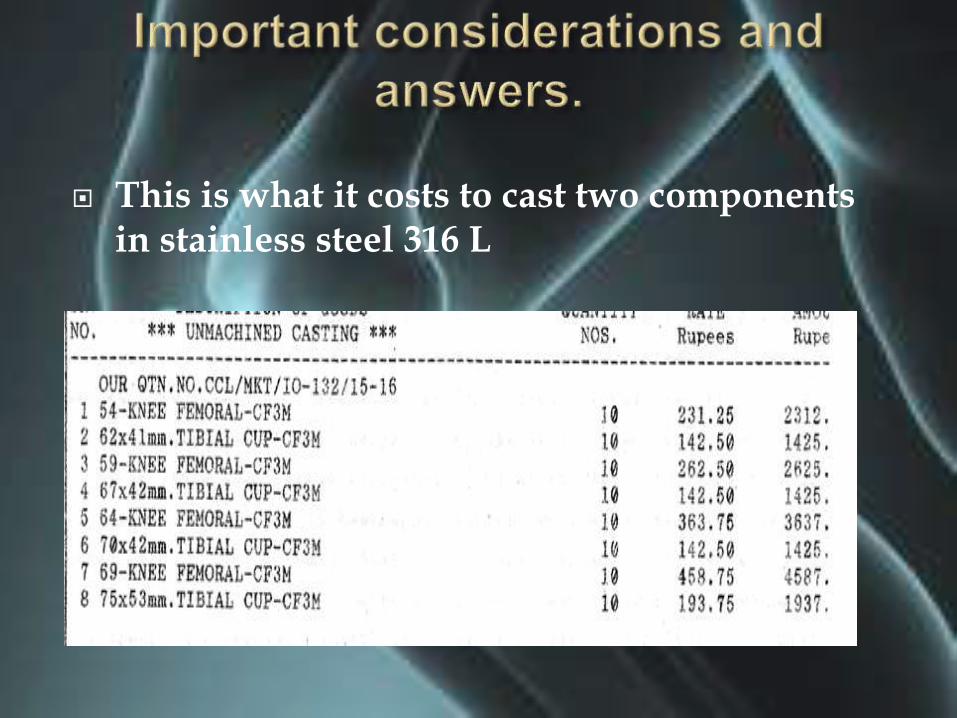
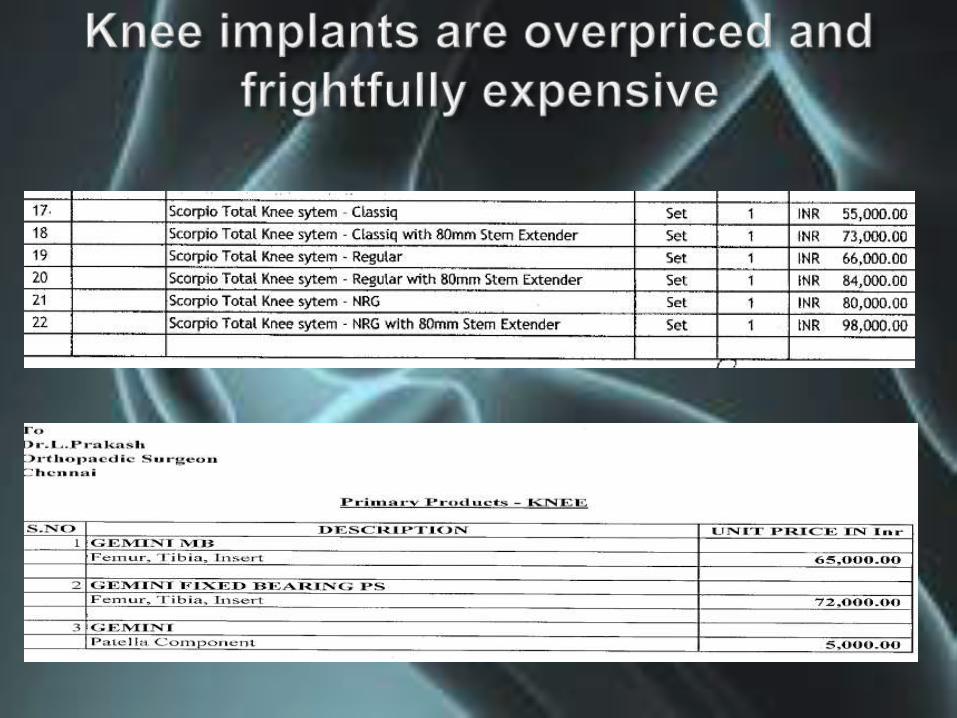
This is what it costs to cast two components in stainless steel 316 L
With HDPE components the production cost after QC, regulations, approvals and sterilization will be about Rs 10,000.00 Rs or $150 US
So the sale price would be about Rs 15000- or 225 US$
But will such a versatile knee sell at this ridiculous cost??

Even a poor patient does not want a cheap product
Cheap has become synonymous with sub standard.
Even today for our own use we buy branded medicines at four times, rather than risking the generic ones
So a cheap implant is not the answer.
Giving the best value for money to the surgeon and the best implant to the patient should be the key
The better the protocols, more stringent the quality control and better the implant tractability, more expensive the manufacturing process becomes.
So a good affordable Indian Knee with its versatile range should sell between 30K to 50K depending on type. Even at 50k (750$) a cementless knee is far far cheaper than it is in USA.
It certainly can be done in a simple AC clean theater with no infection risks, provided the OT is prepared properly and the correct protocol is followed.
It can certainly done in most district hospitals with a little extra care. ( after all I have operated in close to 89 operation theaters around the world without complications)
Pain and loss of function are the prime indications and thus patient selection is subjective.
In those below 55 with good bone stock, a cementless knee has to be used
Above this age, in view of bone stock and longevity, a cemented knee is preferred.
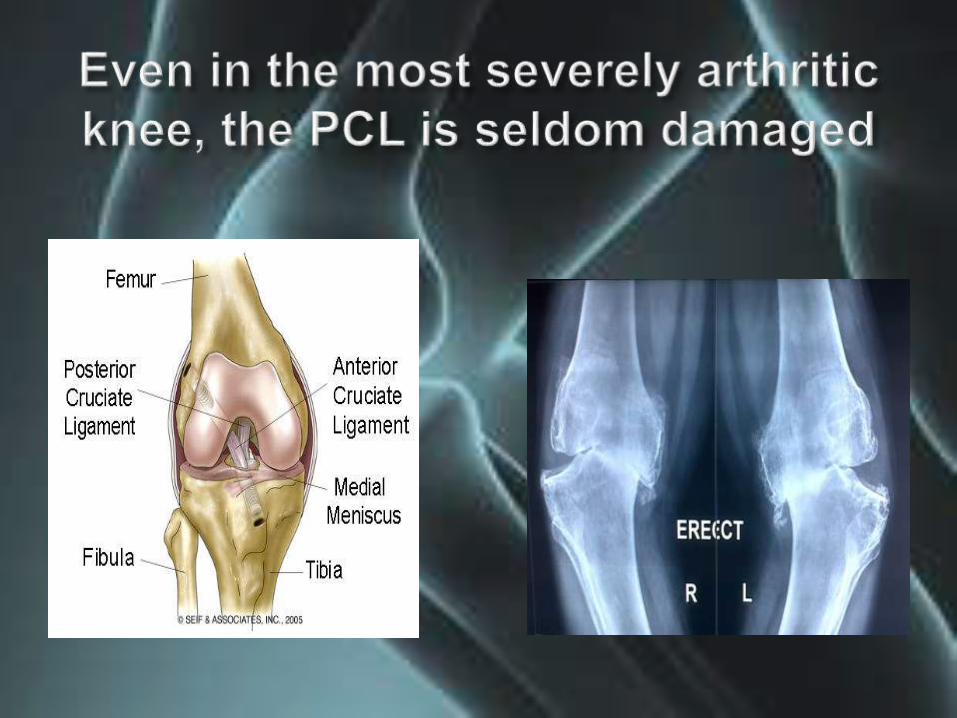
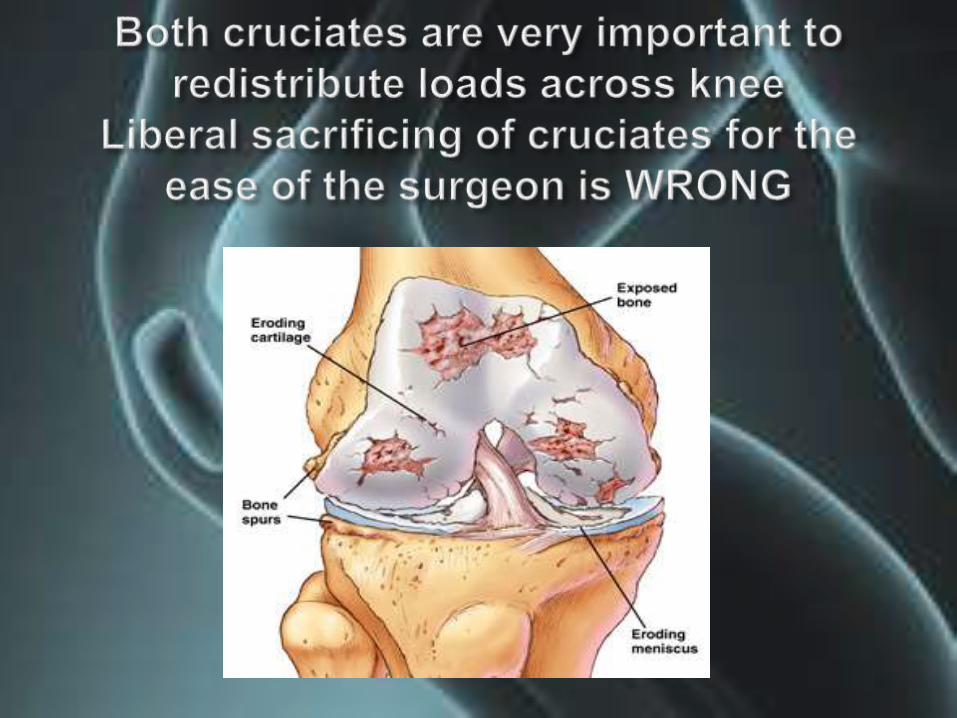
Unless the PCL is frayed or torn, retain it and use a CR component
Mobile bearings offer slightly better results than fixed bearings in the short term, but they have not been with us long enough for proper comparison.
Soft tissue releases and ligament balance is the most important factor for long term success of the operation
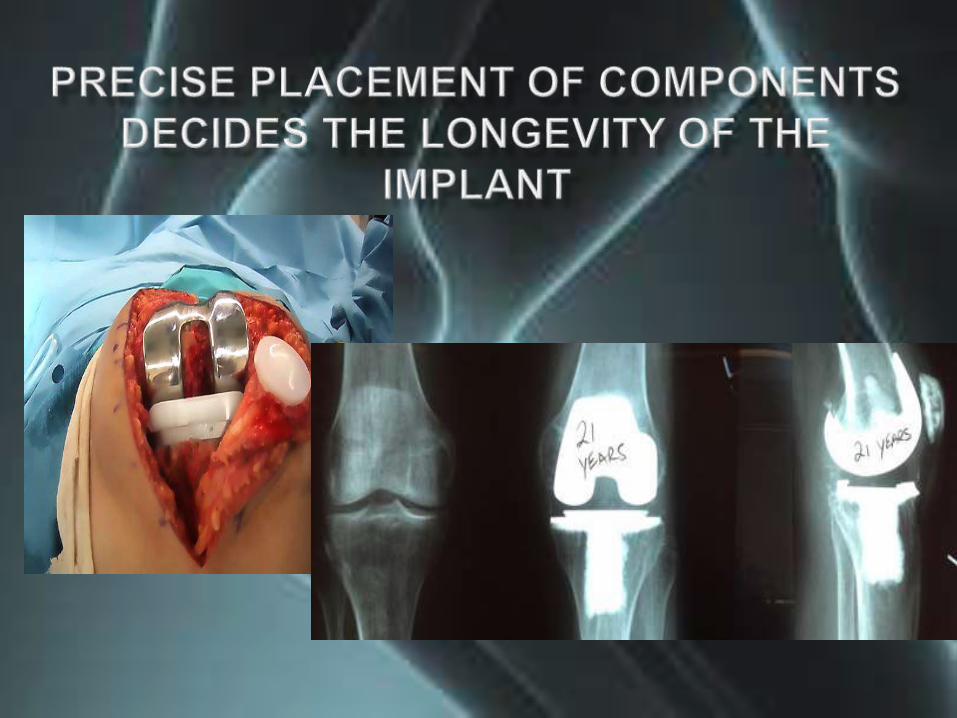
Perfect bone cuts and exact placement of the components is the key to long lasting success

Properly performed, TKR is one of the most satisfying surgical
procedures.

Choose the right patient, plan the surgery properly, be familiar with
the instruments
and have the complete range of
implants with you