Sales Management: 6 Strategies to Refocus Complainers and Improve Team Morale
Upload
marilyn-heathCategory
view
230download
0


Descriptors
• “frequent flyers”
• “help-rejecting complainers”


Descriptors
• “frequent flyers”• “help-rejecting complainers”
• emotional hypochondriacs (secondary gain)
• egocentric • irresponsible, fickle
• “love intoxicated”

Sources of Stigma
• Reaction to anger, neediness (countertransference)
• The perception of willful treatment resistance (“help rejecting complainers”)

“Negative Therapeutic Reactions”
a) Unconscious guilt
b) Unconscious envy – need to destroy
therapists offerings
c) Unconscious identification with a
sadistic object
Kernberg, OF 1977

Sources of Stigma
• BPDs self concept: “bad”, “evil”, “damaged”, “small child” (Zanarini et al. 2001)
• Reaction to anger, neediness (countertransference)
• The perception of willful treatment resistance (“help rejecting complainers”)
• Cross-sectional exposure (“frequent flyers”)
• Misinformation about heritability and prognosis
• Unrealistic expectations of competence

Consequences of Stigma
• avoidance and misinformation by professionals

“Despite its prevalence, enormous public health costs, and the devastating toll it takes on individuals, families, and communities, [borderline personality disorder] only recently has begun to command the attention it requires”.
House Resolution 1005, April 1, 2008

Consequences of Stigma
• an “unwanted diagnosis” by patients confirming their worst fears about themselves
• avoidance and misinformation by professionals
• under-utilization of the diagnosis (~ 2-6% in one OPC)
• failure to provide adequate didactic training or capable clinical supervision
• lack of parity; fair reimbursement

“I dread being diagnosed as borderline. It conveys that I’m malicious and manipulative.”

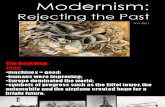
REPONSES TO DIAGNOSIS OF BPD(N = 30)
WORSE BETTER
Shame
Likability
Hope
Overall
Rubovszky et al.

Psychoeducation for BPD
- 30 with workshop about BPD vs. 20 wait listed- PE decreases impulsivity and unstable relations over next 12 weeks- “a useful and cost efficient form of pre-treatment”
Zanarini & Frankenburg, JPD 2008

Minimal BPD Didactic Training Objectives(? 6 Hours)
i) Knowledge of the DSM diagnostic criteria and their meaningii) Awareness of its prognosis and heritabilityiii) How to assess and manage deliberate self- harm and suicidal threatsiv) The role and liabilities of medicationv) The role and outcomes from BPD-specific therapies

Four Models About the Interface between MDD & BPD And their Implications about Course
BPD is Primary: BPD can cause 2 signs and symptoms of MDD; its improvements will be followed by a decrease in MDD
MDD is Primary: MDD can cause 2 BPD Phenomenology; its improvements will be followed by a decrease in BPD
BPD & MDD are Unrelated: Changes in the course in either disorder will not effect the other
Overlapping Etiology: Changes in either disorder will effect the course of the other disorder; but will do so weakly or inconsistently

AD COOCCURRENCE IN BPD
No. BPD % with AD % General
Type AD No. Studies Subjects All (CLPS****) Population*
MDD** 7 1122 44-53 (50%) 17%
Bipolar I*** 8 1006 9 (12%) 1.6%
Bipolar II*** 6 436 11 (8%) 2-3%
Cyclothymic*** 2 404 4% 1%
* Kessler et al., 1994 ** Koenigsberg et al. 1999; Gunderson et al. 2001 *** Paris et al. 2005* *** McGlashan et al. 2000

BPD COOCCURRENCE IN AD
No. AD Type AD No. Studies Subjects % with BPD
MDD* 6 1005 10-15%
Bipolar I** 12 830 11%
Bipolar II** 3 137 16%
* Koenigsberg et al. 1999; Gunderson et al. 2001** Paris et al., 2005

FAMILY STUDIES
Increased Prevalence in RelativesProbands MDD Bipolar I Bipolar II BPD
MDD YES* Yes* ? ?
Bipolar I Yes* YES* Yes* No
Bipolar II Yes Yes* YES ?
BPD ? No ? YES
*Replicated Family Study data

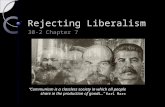
Cross-lagged Panel Analysis Relating Borderline and Depressive Psychopathology over 3 Years (N =
570)
BOR_B
DEP_B
BOR_6
DEP_6
BOR_12
DEP_12
BOR_24
DEP_24
BOR_36
DEP_36
.75*** .78*** .68*** .81***
-.08 .38*** .38*** .33***
.20*** .09* .17*** .11*
.01 .06 .04 .04
Note: BPD = Borderline features, assessed at Baseline (B) and 6, 12, 24 and 36 month follow- alongs; DEP = Depression diagnostic status assessed at these intervals. ***p <.001, **p <.01, *p <.05.

INTERACTIONS OF AXIS I WITH BPD
Effect Co-Occurring Axis I Disorder
↓ BPD Course
↓ Axis I Course
↑ Med Use
Subst Ab
NO
YES
?
MDD
?
YES
YES
Bipolar
NO
YES
YES
ED
NO
YES
?

MDD and BPD overlap descriptively, but when co-occurring BPD is primary


BPD & BIPOLAR DISORDERS
% BPD with Bipolar I & II 20%
% Bipolar I with BPD 11%
% Bipolar II with BPD 16%
% BPD who become bipolar 10%Gunderson et al. 2006

FAMILY STUDIES
Increased Prevalence in RelativesProbands MDD Bipolar I Bipolar II BPD
MDD YES* Yes* ? ?
Bipolar I Yes* YES* Yes* No
Bipolar II Yes Yes* YES ?
BPD ? No ? YES
*Replicated Family Study data

New Onsets of Bipolar I and II in Borderline and Other Personality Disorder Samples
BPD (N = 164) OPD (N = 401)
Bipolar I 7 (4.3%) 6 (1.8%)
Bipolar II 6 (3.7%) 6 (1.8%)
Bipolar I and II 13 (7.9%) 12 (3.1%)
* Two patients have onsets of both Bipolar I and II

INTERACTIONS OF AXIS I WITH BPD
Effect Co-Occurring Axis I Disorder
↓ BPD Course
↓ Axis I Course
↑ Med Use
Subst Ab
NO
YES
?
MDD
?
YES
YES
Bipolar
NO
YES
YES
ED
NO
YES
?

Bipolar D and BPD overlap descriptively, but not familiarly, and when co-occurring BPD is independent


BPD & Bipolar Disorder Diagnoses∙ Bipolar disorder is frequently overutilized (only 57% were confirmed with SCID)∙ 26% of false + Bipolar patients have BPD∙ 40% of BPD patients had false + Bipolar dx∙ Overuse of Bipolar dx is 2° to expected response to meds and the extensive marketing of mood stabilizers∙ Underuse of BPD is 2° to it’s lack of a medication–based therapy and its need for psychosocial treatment
Zimmerman et al. J Clin Psychiatry Jan 2010

Overview
• Treatment of BPD is not done
consistently or well
• Most clinicians don’t like treating
BPD patients
• There is a shortage of well-trained
BPD treaters

TRENDS IN TREATMENT OF BORDERLINE PERSONALITY DISORDER
• From Psychoanalytic Primacy to Multiple Modalities
(notably psychoeducation, cognitive/behavioral and psychopharmacological)


TRENDS IN TREATMENT OF BORDERLINE PERSONALITY DISORDER
• From Possible Improvement to Probable Remission
• From Psychoanalytic Primacy to Multiple Modalities
(notably psychoeducation, cognitive/behavioral and psychopharmacological)
• From Clinical Expertise to Evidence-based
• From Generic to Disorder-specific

THE FRAMEWORK FOR EXPECTABLE CHANGES
Areas of Relevant ExpectableDisturbance Interventions Time for ChangeSubjective state • Concerned attention, Hrs./Weeks Dysphoric feelings validation
• Reality testing • Problem solving
• MedicationBehavior • Clarification (esp. in-Rx months
examples) of defense purpose and maladapttive consequences
Interpersonal Style • Confrontation 6-18 months• Pattern recognition• Here-and-now interactional analysis
Intrapsychic • Defense and transference analysis >2 years Organization • Corrective experiences, real
relationships
From Gunderson, 2001

Behavioral PSA
DBT SFT MBT TFP


DBT
• Most influential
• Most validated
• Most understandable/learned
• Most accessible

DBT TFP MBT
Behavioral focus + - -
Cognitive focus - - +
Transference focus - + -
Interpretation - + -
Defense analyses - + +
Support + - +


Effective Manualized BPDTreatments Show:
1. They are better than TAU.
2. BPD patients require specifiably different and
disorder-specific interventions.
3. PSA therapy can be manualized –
standardized and replicated (up to a point)
4. Adherence and competence can be measured and
shown to correlate with effectiveness.

Mentalization: a common theme of all therapies for BPD
• All psychotherapies develop an interactional matrix in which the mind becomes a focus
• Therapists consider the patient by communicating their representations to them
• experience of patient is of another human having their mind in mind Process more important than content
Adapted from Bateman, 2004

Are EBT’s Worth Learning:
1. Will I do better by my next patient as a
result of the training?
2. Is the increment of increased
effectiveness worth the time and expense
of getting trained?

FIVE SHARED CHARACTERISTICS OF EFFECTIVE THERAPIES (DBT, TFP, MBT,
SFT) FOR BPD
- Structure (goals, roles)- Coherent theory with trained practitioners (self- selected)- Active: support and challenge- Focus on feelings recognition sources (chain analyses) experiencing
- Countertransference: recognition & management

WHY DO THIS WORK?
• Pride in skills (“If you can treat borderline patients, you can treat anyone”)• Personal growth• Having a highly personal, deeply appreciated, life-changing role