Department of propede u ti cs of internal medicine Ass. Prof. N.Z. Yarema
48
Extrasystoly. Paroxismal tachycardia. Heart blocks. Atrial fibrillation. Etiology. Pathogenesis. Clinical pattern of an attack. ECG signs. Cardiac rrhythm disorders dangerous for patient’s life. Principles of treatment and prophylaxis Department of propedeutics of internal medicine Ass. Prof. N.Z. Yarema
-
Upload
ralph-travis -
Category
Documents
-
view
32 -
download
1
description
Cardiac Arrhythmias. Classification. Extrasystoly. Paroxismal tachycardia. Heart blocks. Atrial fibrillation. Etiology. Pathogenesis. Clinical pattern of an attack. ECG signs. Cardiac rrhythm disorders dangerous for patient’s life. Principles of treatment and prophylaxis. - PowerPoint PPT Presentation
Transcript of Department of propede u ti cs of internal medicine Ass. Prof. N.Z. Yarema

Cardiac Arrhythmias. Classification. Extrasystoly. Paroxismal tachycardia.
Heart blocks. Atrial fibrillation. Etiology. Pathogenesis. Clinical pattern of an attack. ECG signs. Cardiac rrhythm
disorders dangerous for patient’s life. Principles of treatment and prophylaxis
Department of propedeutics of internal medicine
Ass. Prof. N.Z. Yarema



Etiology.
• Violations of rhythm of cardiac activity cause such defeats of myocardium:
• organic: IHD,defects of heart, AH, myocarditis, cardiomyopathy;
• · toxic: medicines, alcohol;• · hormonal : thyrotoxicosis, myxedema,
pheochromocytoma, climax;• · functional : neurogenic, sporting;• · anomalies of development of heart - more
frequent all WPW.


Pathogenesis
• Theories of origin of arrhythmias:
• Pathological automatism (presence of ectopic focuses)
• Mechanism of re-entry
• trigern (starting) activity.

Classification of violations of rhythm and conductivity of heart
• I. Violations of formation of impulse• Sinus tachycardia
(more than 90 complexes are for a minute)
• Sinus bradycardia (less than 60 complexes are for a minute )
• Sinus arrhythmia • Stop (refuse) of sinus node• Migration of supraventricular driver of rhythm

• Extrasystolia (a synonym is premature depolarization):
• auricle (atrial)
• auricle-ventrical (atrioventricular)
• ventrical

• Tachycardia:
• supraventricular:
• sino - auricle
• (sinoatrial)
• auricle (atrial)
• auricle - ventrical
• (atrioventrical)
• ordinary (to 30 in a hour)
• frequent (30 and anymore in a hour)
• allorythmia (bi-, thre-, quadrigeminia)
• polymorphic
• twin
• early (R on T)
• chronic
• paroxysmal
• noudle

• ІІ. VIOLATION OF LEADTHROUGH OF IMPULSE
- Sinoauricular of blockade- Atrioventricular blockades:
• І st.
• ІІ st.
• ІІІ st.



Description of normal sinus rhythm
• correct rhythm with frequency of heartbeats 60-100 per 1 min.
• the P wave is positive in II, III, AVF leads, negative - in the AVR leads, permanent form of P wave
• a complex QRS follows by every P waveR (if there is not а-v-blockade).
• Interval of P-Q>0.12 (if there are not additional ways of leadthrough).

Sinus tachycardia
• ECG is criteria:• correct rhythm• sinus P waves are ordinary configuration.• 100-180 beats per 1 min.• gradual beginning and completion• Reasons: physical and emotional loading, pain,
fever, hypovolumia, hypotension, anaemia, thyrotoxicosis, action of certain matters (coffeine, alcohol)

Sinus bradycardia• ECG is criteria:• correct rhythm• less than 60 beats per 1 min• sinus P waves• interval of PQ >0,12 sec.• Reasons: increase of parasympatic tonus,
myocarditis, myxedema, hypothermia, mechanical icterus, syndrome of weakness of sinus knot.
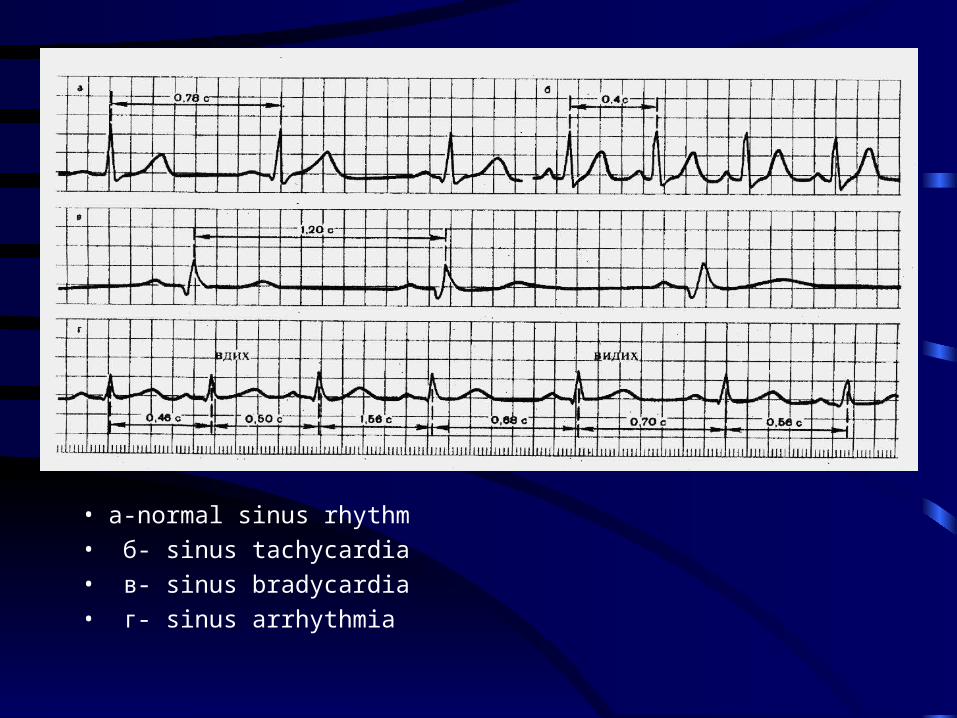
• a-normal sinus rhythm
• б- sinus tachycardia
• в- sinus bradycardia
• г- sinus arrhythmia

Extrasystolia
premature excitation and reduction of heart or his separate parts is as a result of increase of activity of hearths of ectopic automatism.

Auricle extrasystolia
ECG of sign:
• premature reduction after which incomplete scray pause
• the P wave is changed, negative
• a complex QRS is not changed or aberrant.

• a- from the overhead departments of auricle
• б- from the middle departments of auricle
• в- from the lower departments of auricle
• г- is blocked auricle extrasystole

А-V- extrasystoles
• with simultaneous excitation of atriums and ventricles.
• EKG-signs:
• the P wave is not determined
• an extraordinary complex QRS is not extended
• incomplete scray pause

With previous excitation of ventricles
EKG-signs:
• an extraordinary complex QRS is not extended
• P wave is after QRS
• complete scray pause

Ventrical extrasystolia
• EKG of sign:
• complex QRS wide without a previous P wave
• complete scray pause
• Treatments need frequent monotopic, politopic, group and early as R/T extrasystoles.

• a- sinistroventrical extrasystole
• b- dextraventrical extrasystole

Paroxysmal tachycardia Supraventricular
tachycardia• EKG is signs:
• frequency of reductions of atriums - 120-250 per 1 min.
• auricle complexes are preceded the complexes of QRS
• the complexes of QRS are not changed

Atrioventricular tachycardia
• EKG-signs:
• 150-200 heart beats per 1 min.
• retrograde P wave (negative) after QRS or accumulates on him

• a- auricle paroxysmal tachycardia• б - atrioventricular tachycardia with previous excitation of
ventricles• в - atrioventricular tachycardia with simultaneous excitation of
atriums and ventricles

Ventrical tachycardia
• EKG is criteria: - >140 hearts beats per 1 min.
- the complexes of QRS are extended

EKG is at paroxysmal ventrical tachycardia


Trembling and fibrilation of atriums
• EKG is criteria of trembling:
• frequency of auricle waves 250-350 per 1 min. ( waves of f)
• EKG is criteria of fibrilation:
• waves of f
• wrong rhythm (different R-R)
• absence of P wave



Trembling and fibrilation of ventricles
• EKG is criteria:• Sinus wave curve with frequent, rhythmic, wide
and high waves, excitation of ventricles with frequency 200-300 per 1 min.
• it is not possible to distinguish the elements of ventrical complex
• Treatment:• electric cardioversion 200-300 Dzh. At
unefficiency the repeated cardioversion

• a- trembling of ventricles
• b- blinking and fibrilation of ventricles


Sinoauricular blockade
• EKG is criteria:
• periodic fall of cardiac cycles
• increase of pause between the waves of Р-Р in 2 times


Atrioventricular blockade Іst
• permanent lengthening of interval of P-Q anymore as on 0,20s• a- auricle form• б- key form• в- distal form blockade

А-v blockade ІІ ст • the periodic stopping of leadthrough of impulse is
from an auricle to the ventricles. There are three types:
• I type (Mobit I) is the gradual lengthening of interval of P-Q with the subsequent fall of QRST ( periods of Samoylov-Venkenbach)
• ІІ type (Mobit ІІ) is a fall of complexes of QRST without the gradual lengthening of interval of P-Q
• ІІІ type (Mobit ІІІ) of fall every second, or 2 and more complexes successively


А-v blockade ІІІ ст
complete autonomy of reduction of auricle and ventricles.The intervals of P-P and R-R are permanent, but R-R>P-P.

EKG is at the complete blockade of right bundle of bunch of Hiss

EKG is at the complete blockade of left bundle of bunch of Hiss


Syndrome of Wolf-Parkinson-White
• reduction of interval of P-Q (R)• a presence in composition a complex QRS
of additional wave of excitation is d-wave• deformation and increase of duration of
complex QRS• discordant displacement of RS-T and
change of polarity of wave T (inconstant sign)

EKG is at the syndrome of WPW

Conclusions• It is necessary to know for successful diagnostics
and treatment of arrhythmias:• basic nosotropic mechanisms of their development• · to own the methods of diagnostics of
arrhythmias• · to distinguish of high quality, potentially
malignant and malignant arrhythmias• · to understand algorithms diagnostic at the
therapeutic going near the different types of arrhythmias

Thank Thank youyou