B. Keith English, M.D. Chair, Pediatrics & Human Development Departmental Update.

DEPARTMENT of HEALTH
and HUMAN SERVICES
Fiscal Year 2019
General Departmental Management Opioids Epidemic and Serious Mental Illness Initiative
Office of Medicare Hearings and Appeals Office for Civil Rights
National Coordinator for Health Information Technology Health Insurance Reform Implementation Fund
Nonrecurring Expenses Fund Service and Supply Fund
Retirement Pay & Medical Benefits for Commissioned Officers HHS General Provisions
Justification of Estimates for Appropriations Committees

Page 2
DEPARTMENT OF HEALTH AND HUMAN SERVICES DEPARTMENTAL MANAGEMENT
FY 2019
FTE Budget Authority
General Departmental Management 1,005
$289,545,000
PHS Evaluation Set‐Aside – Public Health Service Act
129 $53,445,000
Pregnancy Assistance Fund1
2 $25,000,000
HCFAC2
34 $10,000,000
Proposed Mandatory Funding – Departmental Appeals Board3 Proposed User Fee Collections – Departmental Appeals Board6
14
0
$2,000,000
$1,457,000
GDM Program Level4 1,184 $381,447,000
Office of Medicare Hearings and Appeals 705 $112,381,000
Proposed Mandatory Funding – Office of Medicare Hearings and Appeals Recovery Audit Collections – Office of Medicare Hearings and Appeals and Departmental Appeals Board5 Proposed User Fee Collections – Office of Medicare Hearings and Appeals6
200
45
0
$125,000,000
$10,000,000
$3,679,000
OMHA Program Level 950 $251,060,000
Office for Civil Rights
153
$30,904,000
Office of the National Coordinator for Health IT
164 $38,381,000
Service and Supply Fund Opioids Epidemic and Serious Mental Illness and Serious Emotional Disturbance Initiative
1,001
0
$0
$10,000,000,000
TOTAL, Departmental Management 3,452 $10,701,792,000
1 The Pregnancy Assistance Fund (PAF) is authorized and appropriated by the Patient Protection and Affordable Care Act (ACA) Public Law 111‐148. 2 The reimbursable program (HCFAC) in the General Department Management (GDM) account reflects estimates of the allocation account
for 2019. Actual allocation will be determined annually. 3 The proposed mandatory funding has a legislative proposal in place to transfer funds from the Federal Hospital Insurance and Federal
Supplementary Medical Insurance Trust Funds to the Departmental Appeals Board. 4 The GDM Program Level does not include either estimated reimbursable budget authority and associated FTE or Pregnancy Assistance Fund
and associated FTE, unless otherwise indicated. 5 Recovery Audit Collections reflect FY 2018 House and Senate Bills to address Medicare Appeals at OMHA and DAB. 6 The proposed user fee collections for OMHA and DAB represent a proposal that creates a post‐adjudication user fee applied to all unfavorable
appeals (other than beneficiary appeals) at the 3rd and 4th level of appeals.

Page 3
INTRODUCTION The FY 2019 Congressional Justification is one of several documents that fulfill the Department of Health and Human Services’ (HHS) performance planning and reporting requirements. HHS achieves full compliance with the Government Performance and Results Act of 1993 (GPRA) and Office of Management and Budget (OMB) Circulars A‐11 and A‐136 through the HHS agencies’ FY 2019 Congressional Justifications and Online Performance Appendices, the Agency Financial Report, and the HHS Citizens’ Report. These documents are available at http://www.hhs.gov/budget. The FY 2019 Congressional Justifications and accompanying Online Performance Appendices contain the updated FY 2019 Annual Performance Report and FY 2019 Annual Performance Plan. The Agency Financial Report provides fiscal and high‐level performance results. The Summary of Performance and Financial Information summarizes key past and planned performance and financial information.


Page 5
DEPARTMENT OF HEALTH AND HUMAN SERVICES OFFICE OF THE SECRETARY
Secretary Alex M. Azar II
Deputy Secretary Eric Hargan
Chief of Staff
E. Peter Urbanowicz
Inspector General Daniel R. Levinson
Director, Office for Civil Rights Roger Severino
Assistant Secretary for Preparedness and
Response Robert P. Kadlec, M.D.
Assistant Secretary for Public Affairs Judy Stecker
Assistant Secretary for Financial Resources
Vacant
General Counsel Robert Charrow
Director, Office of Global Affairs
Garrett Grigsby
Director, Office of Intergovernmental and
External Affairs Vacant
Chair, Departmental Appeals Board
Constance B. Tobias
Assistant Secretary for Administration
Vacant
Assistant Secretary for Health
Brett P. Giroir, M.D.
Assistant Secretary for Planning and Evaluation
Vacant
Assistant Secretary for Legislation
Matthew Bassett
Chief Administrative Law Judge
Office of Medicare Hearings and Appeals Nancy Griswold
National Coordinator for Health IT Don Rucker, M.D.

Page 6
ORGANIZATIONAL CHART: TEXT VERSION
Department of Health and Human Services o Alex M. Azar II
Deputy Secretary Eric Hargan
Chief of Staff E. Peter Urbanowicz The following offices report directly to the Secretary:
Inspector General o Daniel R. Levinson
Chief Administrative Law Judge of the Office of Medicare Hearings and Appeals o Nancy Griswold
Director of the Office for Civil Rights o Roger Severino
National Coordinator for Health Information Technology o Don Rucker, M.D.
Assistant Secretary for Administration o Vacant
Assistant Secretary for Health o Brett P. Giroir, M.D.
Assistant Secretary for Legislation o Matthew Bassett
Assistant Secretary for Planning and Evaluation o Vacant
Assistant Secretary for Preparedness and Response o Robert P. Kadlec, M.D., M.P.H.
Assistant Secretary for Public Affairs o Judy Stecker
Assistant Secretary for Financial Resources o Vacant
General Counsel o Robert Charrow
Director, Office of Global Affairs o Garrett Grigsby
Chief of the Departmental Appeals Board o Constance B. Tobias
Director of the Office of Intergovernmental and External Affairs o Vacant
Page 7
DEPARTMENTAL MANAGEMENT OVERVIEW
Departmental Management (DM) is a consolidated display that includes the Office of the Secretary (OS) activities funded under the following accounts:
General Departmental Management (appropriation);
Office of Medicare Hearings and Appeals (appropriation);
Office for Civil Rights (appropriation);
Office of the National Coordinator for Health Information Technology (appropriation);
Service and Supply Fund (revolving fund); and
Opioids Epidemic and Serious Mental Illness and Serious Emotional Disturbance Initiative. The mission of the OS is to provide support and assistance to the Secretary in administering and overseeing the organization, programs, and activities of the Department of Health and Human Services. The overall FY 2019 President’s Budget request for DM totals $10,701,792,000 in program level funding, including 3,452 full‐time equivalent (FTE) positions, an increase of $9,944,409,000 above the FY 2018 Annualized Continuing Resolution (CR) Level. The FY 2019 Budget will support ongoing and critical priorities including the Opioid Epidemic and Serious Mental Illness and Serious Emotional Disturbance, Global Health Security Agenda, the HHS Pain Management Task Force, religious freedom, and the Departmental Appeals Board. The General Departmental Management (GDM) appropriation supports the activities associated with the Secretary’s responsibilities as chief policy officer and general manager of the Department in administering and overseeing the organization, programs, and activities of HHS. These activities are carried out through eleven Staff Divisions (STAFFDIVs), including the Immediate Office of the Secretary, the Departmental Appeals Board, and the Offices of public affairs, legislation, planning and evaluation, financial resources, administration, intergovernmental and external affairs, general counsel, global affairs, and the assistant Secretary for Health. The FY 2019 President’s Budget program level request for GDM includes a total of $381,447,000 and 1,184 FTE. The Office of Medicare Hearings and Appeals (OMHA) was created pursuant to the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA). As mandated by MMA, OMHA opened its doors on July 1, 2005, to hear Medicare appeals at the Administrative Law Judge (ALJ) level, for cases under titles XVIII and XI of the Social Security Act. OMHA is funded from the Medicare Hospital Insurance and Supplemental Medical Insurance Trust Funds. The FY 2019 President’s Budget request for OMHA is $251,060,000 and 950 FTE. Of this amount, $125,000,000 and 200 FTE will be provided through proposed mandatory funding, $10,000,000 in Recovery Audit collections, and $3,679,000 in proposed user fee collections. The request will help support critical initiatives intended to improve the Medicare appeals process by allowing the addition of up to 106 ALJ teams. The budget will also allow OMHA to expand its alternative dispute resolution initiatives by allowing for the addition of attorney adjudicators and settlement conference facilitators who will increase the agency’s disposition capacity. The budget also proposes additional legislative authorities for OMHA to address the Medicare appeals backlog. The Office for Civil Rights (OCR) is the Department's chief law enforcer and regulator of civil rights, conscience, and religious freedom, and health information privacy and security. The FY 2019 President’s Budget request for OCR is $30,904,000 in budget authority and 153 FTE. The Budget supports OCR’s

Page 8
essential programmatic focus as the primary defender of the public’s right to nondiscriminatory access to, and receipt of, HHS‐funded health and human services, conscience and religious freedom protections, and access, privacy, and security protections for individually identifiable health information. To carry out these functions, OCR investigates complaints, enforces rights, develops policy, promulgates regulations, and provides technical assistance and public education to ensure understanding of, and compliance with, non‐discrimination and health information privacy laws. The Office of the National Coordinator for Health Information Technology (ONC) was established by Executive Order 13335 on April 27, 2004, and subsequently authorized by the Health Information Technology for Economic and Clinical Health Act on February 17, 2009. The FY 2019 President’s Budget request for ONC is $38,381,000 and 164 FTE, to coordinate national efforts related to the implementation and use of interoperable electronic health information exchange. The Office of the National Coordinator for Health Information Technology (ONC) leads the Government’s efforts to ensure that electronic health information is available and can be shared safely and securely to improve the health and care of all Americans and their communities. ONC’s work is pivotal to achieving interoperability, encouraging market competition, advancing patient access to their electronic records, combating information blocking, and bringing innovative easy‐to‐use products into the hands of users. The Service and Supply Fund (SSF), the HHS revolving fund, is composed of two components: the Program Support Center (PSC) and the Non‐PSC activities. For the FY 2019 President’s Budget request the SSF is projecting total revenue of $1,802,732,432 and usage of 1,001 FTE. The FY 2019 Budget proposes a $10 billion historic investment for Combatting Opioid Epidemic and Serious Mental Illness and Serious Emotional Disturbance. This investment supports department‐wide collaboration to address the opioids epidemic and focus on rural and underserved populations through evidence‐based approaches and establishes a new grant program for Certified Community Behavioral Health Clinics that provide services to individuals suffering from serious mental illness.
Page 9
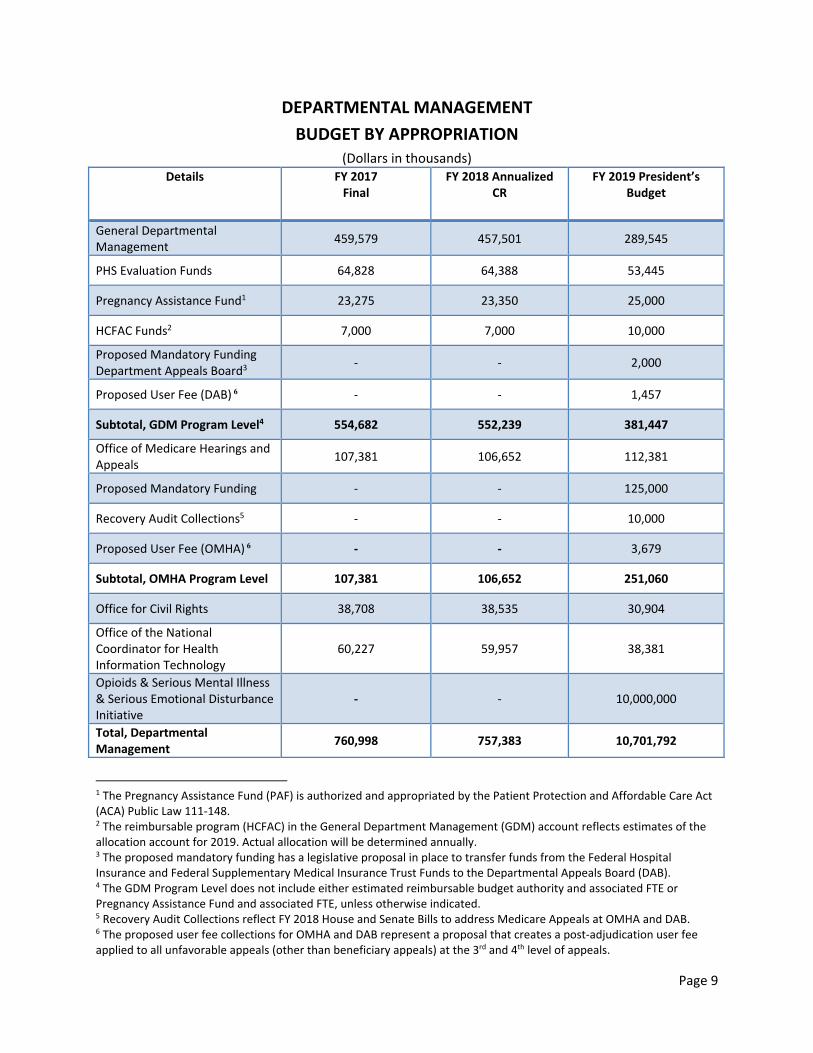
DEPARTMENTAL MANAGEMENT
BUDGET BY APPROPRIATION (Dollars in thousands)
Details
FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
General Departmental Management
459,579 457,501 289,545
PHS Evaluation Funds 64,828 64,388 53,445
Pregnancy Assistance Fund1 23,275 23,350 25,000
HCFAC Funds2 7,000 7,000 10,000
Proposed Mandatory Funding Department Appeals Board3
‐ ‐ 2,000
Proposed User Fee (DAB) 6 ‐ ‐ 1,457
Subtotal, GDM Program Level4 554,682 552,239 381,447
Office of Medicare Hearings and Appeals
107,381 106,652 112,381
Proposed Mandatory Funding ‐ ‐ 125,000
Recovery Audit Collections5 ‐ ‐ 10,000
Proposed User Fee (OMHA) 6 ‐ ‐ 3,679
Subtotal, OMHA Program Level 107,381 106,652 251,060
Office for Civil Rights 38,708 38,535 30,904
Office of the National Coordinator for Health Information Technology
60,227 59,957 38,381
Opioids & Serious Mental Illness & Serious Emotional Disturbance Initiative
‐ ‐ 10,000,000
Total, Departmental Management
760,998 757,383 10,701,792
1 The Pregnancy Assistance Fund (PAF) is authorized and appropriated by the Patient Protection and Affordable Care Act (ACA) Public Law 111‐148. 2 The reimbursable program (HCFAC) in the General Department Management (GDM) account reflects estimates of the allocation account for 2019. Actual allocation will be determined annually. 3 The proposed mandatory funding has a legislative proposal in place to transfer funds from the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds to the Departmental Appeals Board (DAB). 4 The GDM Program Level does not include either estimated reimbursable budget authority and associated FTE or Pregnancy Assistance Fund and associated FTE, unless otherwise indicated. 5 Recovery Audit Collections reflect FY 2018 House and Senate Bills to address Medicare Appeals at OMHA and DAB. 6 The proposed user fee collections for OMHA and DAB represent a proposal that creates a post‐adjudication user fee applied to all unfavorable appeals (other than beneficiary appeals) at the 3rd and 4th level of appeals.

General Departmental Management

Page 1
TABLEOFCONTENTS
Appropriations Language ................................................................................................................ 3
Language Analysis ........................................................................................................................... 4
Authorizing Legislation.................................................................................................................... 5
Amounts Available for Obligation ................................................................................................... 6
Summary of Changes ...................................................................................................................... 7
Budget Authority by Activity ‐ Direct .............................................................................................. 8
Budget Authority by Object Class ‐ Direct ...................................................................................... 9
Budget Authority by Object Class – Reimbursable ....................................................................... 10
Salary and Expenses ...................................................................................................................... 11
Appropriation History Table ......................................................................................................... 12
Overview of Performance ............................................................................................................. 13
Overview of Budget Request ........................................................................................................ 15
Narratives by Activity .................................................................................................................... 16
Immediate Office of the Secretary ................................................................................... 16
Secretarial Initiatives and Innovations ............................................................................. 21
Assistant Secretary for Administration ............................................................................. 22
Assistant Secretary for Financial Resources ..................................................................... 27
Acquisition Reform ........................................................................................................... 30
Assistant Secretary for Legislation .................................................................................... 31
Assistant Secretary for Public Affairs ................................................................................ 33
Office of the General Counsel ........................................................................................... 35
Departmental Appeals Board ........................................................................................... 38
Office of Global Affairs ...................................................................................................... 47
Office of Intergovernmental and External Affairs ............................................................ 50
Center for Faith‐Based and Neighborhood Partnerships ................................................. 52
Office of the Assistant Secretary for Health ..................................................................... 54
Executive Summary ............................................................................................ 54
Immediate Office of the Assistant Secretary for Health .................................... 56
Office of HIV/AIDS and Infectious Disease Policy .............................................. 64
Office of Disease Prevention and Health Promotion ......................................... 69

Page 2
President’s Council on Fitness, Sports and Nutrition ........................................ 74
Office of Human Research Protections .............................................................. 77
National Vaccine Program Office ....................................................................... 81
Office of Adolescent Health ............................................................................... 85
Public Health Reports ........................................................................................ 87
Teen Pregnancy Prevention ............................................................................... 90
Office of Minority Health ................................................................................... 91
Office on Women’s Health ............................................................................... 105
Office of Research Integrity ............................................................................. 113
Embryo Adoption Awareness Campaign ......................................................... 117
Sexual Risk Avoidance ...................................................................................... 119
Minority HIV/AIDS Initiative ............................................................................ 120
Rent, Operation, and Maintenance and Related Services .............................................. 121
Shared Operating Expenses ............................................................................................ 122
PHS Evaluation Funded Appropriations .......................................................................... 124
Assistant Secretary for Planning and Evaluation ............................................. 124
Health Care Evaluation .................................................................................... 131
Assistant Secretary for Financial Resources .................................................... 133
Office of the Assistant Secretary for Health .................................................... 134
Teen Pregnancy Prevention ............................................................................. 136
Pregnancy Assistance Fund .............................................................................. 137
Supporting Exhibits ..................................................................................................................... 140
Detail of Positions ........................................................................................................... 140
Detail of Full‐Time Equivalent (FTE) Employment .......................................................... 141
FTEs Funded by the Affordable Care Act ........................................................................ 142
Statement of Personnel Resources ................................................................................. 143
Rent and Common Expenses .......................................................................................... 144
Physicians’ Comparability Allowance (PCA) ................................................................................ 145
Grants.Gov .................................................................................................................................. 147
Centrally Managed Projects ........................................................................................................ 151
Significant Items in Conference, House, and Senate Appropriations Committees Report ........ 154

Page 3
APPROPRIATIONS LANGUAGE
GENERAL DEPARTMENTAL MANAGEMENT For necessary expenses, not otherwise provided for general departmental management, including hire of [six] passenger motor vehicles, and for carrying out titles III, XVII, XXI, and section 229 of the PHS Act, the United States‐Mexico Border Health Commission Act, and research studies under section 1110 of the Social Security Act, [$457,501,000]$289,545,000 together with [$64,388,000]$53,445,000 from the amounts available under section 241 of the PHS Act to carry out national health or human services research and evaluation activities: [Provided further, That of the funds made available under this heading, $10,000,000 shall be for making competitive grants which exclusively implement education in sexual risk avoidance (defined as voluntarily refraining from non‐marital sexual activity): Provided further, That funding for such competitive grants for sexual risk avoidance shall use medically accurate information referenced to peer‐reviewed publications by educational, scientific, governmental, or health organizations; implement an evidence‐based approach integrating research findings with practical implementation that aligns with the needs and desired outcomes for the intended audience; and teach the benefits associated with self‐regulation, success sequencing for poverty prevention, healthy relationships, goal setting, and resisting sexual coercion, dating violence, and other youth risk behaviors such as underage drinking or illicit drug use without normalizing teen sexual activity: Provided further, That no more than 10 percent of the funding for such competitive grants for sexual risk avoidance shall be available for technical assistance and administrative costs of such programs:] Provided further, That funds provided in this Act for embryo adoption activities may be used to provide to individuals adopting embryos, through grants and other mechanisms, medical and administrative services deemed necessary for such adoptions: Provided further, That such services shall be provided consistent with 42 CFR 59.5(a)(4).

Page 4
LANGUAGE ANALYSIS Language Provision Explanation [That of the funds made available under The President’s budget does not this heading, $10,000,000 shall be for request amounts available for making competitive grants which sexual risk avoidance activities in exclusively implement education in FY 2019. sexual risk avoidance… ]

Page 5
AUTHORIZING LEGISLATION (Dollars in Thousands)
Details 2018
Authorized
2018 Annualized
CR 2019
Authorized
2019 President’s Budget
General Departmental Management: except account below:
Indefinite 178,920 Indefinite 171,438
Reorganization Plan No. 1 of 1953 ‐ ‐ ‐ ‐
Office of the Assistant Secretary for Health: Public Health Service Act
‐ ‐ ‐ ‐
Title III, Section 301 Indefinite 175,905 Indefinite 22,208
Title, II Section 229 (OWH) 1 31,922 1 28,454
Title XVII Section 1701 (ODPHP) 2 6,680 2 6,726
Title XVII, Section 1707 (OMH) 3 56,285 3 53,956
Title XVII, Section 1708 (OAH) 4 1,432 4 200
Title XXI, Section 2101 (NVPO) 5 6,357 5 6,400
Subtotal ‐ 278,581 ‐ 117,944
Total GDM Appropriation ‐ 457,501 ‐ 289,545
1) Authorizing legislation under Section 229 of the PHS Act expires September 30, 2014 2) Authorizing legislation under Section 1701 of the PHS Act expired September 30, 2002. Reauthorization will be proposed. 3) Authorizing legislation under Section 1707 of the PHS Act expires September 30, 2016. 4) Authorizing legislation under Section 1708 of the PHS Act expired September 30, 2000. 5) Authorizing legislation under Section 2101 of the PHS Act expired September 30, 2005. Reauthorization will be proposed

Page 6
AMOUNTS AVAILABLE FOR OBLIGATION
Detail FY 2017 Final FY 2018
Annualized CR
FY 2019 President’s Budget
Annual appropriation $460,629,000 $460,629,000 $289,545,000
Rescission1 ‐ ‐$3,128,132 ‐
Transfer of Funds to ACF2 ‐$1,050,000 ‐ ‐
Subtotal, adjusted budget authority $459,579,000 $457,500,868 $289,545,000
Total Obligations $459,579,000 $456,782,983 $289,545,000
1 Continuing Appropriations Act, 2018 (Division D of P.L. 115‐56) 2 Consolidated Appropriations Act, 2017 (Division H of P.L. 115‐31)

Page 7
SUMMARY OF CHANGES
(Dollars in Thousands)
Budget Year and Type of Authority Dollars FTE
FY 2018 Annualized CR 457,501 992
Total Adjusted Budget Authority 457,501 992
FY 2019 Current Request 289,545 1,005
Total Estimated Budget Authority 289,545 1,005
Net Changes ‐167,956 +13
Increases FY 2018 Annualized CR
FY 2019 Request Change from Base
Immediate Office of the Secretary 13,210 +90
Assistant Secretary for Public Affairs 8,351 +57
Assistant Secretary for Legislation 4,072 +28
ASFR, Financial Systems Integration 30,237 +206
Assistant Secretary for Administration 17,339 +119
Office of Intergovernmental and External Affairs 10,553 +72
Center for Faith Based Neighborhood Partnerships 1,290 +36
Office of the General Counsel 30,889 +211
Departmental Appeals Board 10,925 +7,075
Office of Global Affairs 5,985 +41
Rent 15,980 +109
Shared Operating Services ‐ Enterprise IT, SSF Payments 11,466 +1,096
Office of the Assistant Secretary for Health* 34,102 +396
Embryo Adoption Awareness Campaign 993 +7
Total 195,392 +9,543
*OASH includes increases in the Immediate Office, OHAIDP, ODPHP, PCFSN, OHRP, NVP, and PHR
Decreases FY 2018 Annualized CR
FY 2019 Request Change from Base
Secretary’s Initiative/Innovations 1,986 ‐986
Acquisition Reform 1,738 ‐738
Office of the Assistant Secretary for Health – OAH 1,432 ‐1,232
Teen Pregnancy Prevention 100,314 ‐100,314
Office of Minority Health 56,285 ‐2,329
Office on Women’s Health 31,922 ‐3,468
Sexual Risk Avoidance 14,898 ‐14,898
Minority HIV/AIDS 53,534 ‐53,534
Total 262,109 ‐177,499
Total Changes FY 2018 Annualized
CR
FY 2018 FTE
FY 2018 Request Change from Base
FY 2019 FTE Change from Base
Total Increase Changes 195,392 ‐ 9,543 +13
Total Decrease Changes 262,109 ‐ ‐177,499
Total 457,501 992 ‐167,956 1,005

Page 8
BUDGET AUTHORITY BY ACTIVITY ‐ DIRECT (Dollars in Thousands)
Activity FY
2017 FTE
FY 2017 Final
FY 2018 FTE
FY 2018 Annualized
CR
FY 2019 FTE
FY 2019 President's Budget
Immediate Office of the Secretary 79 13,300 79 13,210 79 13,300
Secretarial Initiatives and Innovations ‐ 1,765 ‐ 1,986 ‐ 1,000
Assistant Secretary for Administration 114 17,458 114 17,339 114 17,458
Assistant Secretary for Financial Resources 149 30,444 149 30,237 149 30,444
Acquisition Reform 1 1,750 1 1,738 1 1,000
Assistant Secretary for Legislation 27 4,100 27 4,072 27 4,100
Assistant Secretary for Public Affairs 56 8,408 56 8,351 56 8,408
Office of the General Counsel 143 31,100 143 30,889 143 31,100
Departmental Appeals Board 70 11,000 70 10,925 103 18,000
Office of Global Affairs 22 6,026 22 5,985 22 6,026
Office of Intergovernmental and External Affairs 68 10,625 68 10,553 68 10,625
Center for Faith‐Based and Neighborhood Partnerships 7 1,299 7 1,290 7 1,326
Office of the Assistant Secretary for Health 255 225,154 255 224,054 236 116,944
Embryo Adoption Awareness Campaign ‐ 998 ‐ 993 ‐ 1,000
HIV‐AIDS in Minority Communities 1 53,777 1 53,534 ‐ ‐
Shared Operating Expenses ‐ 11,544 ‐ 11,466 ‐ 12,725
Rent, Operations, Maintenance and Related Services ‐ 15,866 ‐ 15,980 ‐ 16,089
Sexual Risk Avoidance ‐ 14,966 ‐ 14,898 ‐ ‐
Total, Budget Authority 992 459,579 992 457,501 1,005 289,545

Page 9
BUDGET AUTHORITY BY OBJECT CLASS – DIRECT (Dollars in Thousands)
Object Class Table
Description FY 2017 Final FY 2018
Annualized CR
FY 2019 President's Budget
FY 2019 +/‐
FY 2018
11.1 Full‐time permanent 86,475 87,035 88,625 +1,590
11.3 Other than full‐time permanent 9,626 9,672 9,732 +60
11.5 Other personnel compensation 1,958 1,973 1,984 +11
11.7 Military personnel 2,742 2,679 2,660 ‐19
Subtotal Personnel Compensation 100,802 101,359 103,001 +1,642
12.1 Civilian personnel benefits 28,448 28,632 29,377 +745
12.2 Military benefits 1,280 1,267 1,278 +11
13.0 Benefits for former personnel ‐ ‐
Total Pay Costs 130,530 131,258 133,656 +2,398
21.0 Travel and transportation of persons 4,293 4,232 3,789 ‐443
22.0 Transportation of things 187 187 189 +2
23.1 Rental payments to GSA 15,724 15,831 15,623 ‐208
23.3 Communications, utilities, and misc. charges 2,164 2,173 2,186 +13
24.0 Printing and reproduction 811 816 805 ‐11
25.1 Advisory and assistance services 22,137 21,951 15,701 ‐6,250
25.2 Other services from non‐Federal sources 45,645 45,055 28,081 ‐16,974
25.3 Other goods and services from Federal sources 69,045 67,105 31,023 ‐36,082
25.4 Operation and maintenance of facilities 5,484 5,536 5,595 +59
25.5 Research and development contracts ‐ ‐ ‐ ‐
25.6 Medical care ‐ ‐ ‐ ‐
25.7 Operation and maintenance of equipment 4,981 4,781 5,238 +457
25.8 Subsistence and support of persons 109 109 109 ‐
26.0 Supplies and materials 2,560 2,562 2,624 +62
31.0 Equipment 453 454 425 ‐29
32.0 Land and Structures ‐ ‐ ‐ ‐
41.0 Grants, subsidies, and contributions 155,456 155,449 44,499 ‐110,950
42.0 Insurance claims and indemnities ‐ ‐
44.0 Refunds ‐ ‐ ‐ ‐
Total Non‐Pay Costs 329,049 326,242 155,889 ‐170,354
Total Budget Authority by Object Class 459,579 457,500 289,545 ‐167,955

Page 10
BUDGET AUTHORITY BY OBJECT CLASS – REIMBURSABLE (Dollars in Thousands)
Object Class Code
Description FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
11.1 Full‐time permanent 57,403 56,016 52,495 ‐3,520
11.3 Other than full‐time permanent 3,296 3,278 3,278 ‐
11.5 Other personnel compensation 788 787 784 ‐3
11.7 Military personnel 1,675 1,691 1,691 ‐
Subtotal Personnel Compensation 63,162 61,772 58,249 ‐3,523
12.1 Civilian personnel benefits 19,096 18,604 18,610 +6
12.2 Military benefits 557 557 557 ‐
13.0 Benefits for former personnel ‐ ‐ ‐ ‐
Total Pay Costs 82,815 80,933 77,415 ‐3,517
21.0 Travel and transportation of persons 1,114 1,125 1,125 ‐
22.0 Transportation of things 100 100 100 ‐
23.1 Rental payments to GSA 6,411 6,494 6,516 +22
23.3 Communications, utilities, and misc. charges 146 147 147 ‐
24.0 Printing and reproduction 34 34 34 ‐
25.1 Advisory and assistance services 29,251 28,610 27,902 ‐708
25.2 Other services from non‐Federal sources 25,677 18,824 18,809 ‐15
25.3 Other goods and services from Federal sources 103,678 112,508 98,614 ‐13,893
25.4 Operation and maintenance of facilities 2,613 2,619 5,619 +3,000
25.5 Research and development contracts ‐ ‐ ‐ ‐
25.6 Medical care ‐ ‐ ‐ ‐
25.7 Operation and maintenance of equipment 4,485 4,489 4,489 ‐
25.8 Subsistence and support of persons ‐ ‐ ‐ ‐
26.0 Supplies and materials 396 396 388 ‐8
31.0 Equipment 311 312 315 +3
32.0 Land and Structures 56 56 56 ‐
41.0 Grants, subsidies, and contributions 3,172 3,172 3,172 ‐
42.0 Insurance claims and indemnities ‐ ‐ ‐ ‐
44.0 Refunds ‐ ‐ ‐ ‐
Total Non‐Pay Costs 177,444 178,886 167,287 ‐11,600
Total Budget Authority by Object Class 260,259 259,819 244,702 ‐15,117

Page 11
SALARY & EXPENSES (Dollars in Thousands)
Object Class Code
Description FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
11.1 Full‐time permanent 86,475 87,035 88,625 +1,590
11.3 Other than full‐time permanent 9,626 9,672 9,732 +60
11.5 Other personnel compensation 1,958 1,973 1,984 +11
11.7 CC personnel 2,742 2,679 2,660 ‐19
Subtotal Personnel Compensation 100,802 101,359 103,001 +1,642
12.1 Civilian personnel benefits 28,448 28,632 29,377 +745
12.2 CC benefits 1,280 1,267 1,278 +11
13.0 Benefits for former personnel ‐ ‐ ‐ ‐
Total Pay Costs 130,530 131,258 133,656 +2,398
21.0 Travel and transportation of persons 4,293 4,232 3,789 ‐443
22.0 Transportation of things 187 187 189 +2
23.3 Communications, utilities, and misc. charges 2,164 2,173 2,186 +13
24.0 Printing and reproduction 811 816 805 ‐11
25.1 Advisory and assistance services 22,137 21,951 15,701 ‐6,250
25.2 Other services from non‐Federal sources 45,645 45,055 28,081 ‐16,974
25.3 Other goods and services from Federal sources 69,045 67,105 31,023 ‐36,082
25.4 Operation and maintenance of facilities 5,484 5,536 5,595 +59
25.5 Research and development contracts ‐ ‐ ‐ ‐
25.6 Medical care ‐ ‐ ‐ ‐
25.7 Operation and maintenance of equipment 4,981 4,781 5,238 +457
25.8 Subsistence and support of persons 109 109 109 ‐
Subtotal Other Contractual Services 154,856 151,946 92,717 ‐59,229
26.0 Supplies and materials 2,560 2,562 2,624 +62
Subtotal Non‐Pay Costs 157,416 154,508 95,342 ‐59,166
Total Salary and Expenses 287,946 285,766 228,998 ‐56,768
23.1 Rental payments to GSA 15,724 15,831 15,623 ‐208
Total Salaries, Expenses, and Rent 303,670 301,597 244,621 ‐56,976
Total Direct FTE 992 992 1,005 +13

Page 12
APPROPRIATION HISTORY TABLE
Details
Budget Estimates to Congress
House Allowance
Senate Allowance
Appropriations
2009 ‐ ‐ ‐ ‐ Appropriation $374,013,000 $361,825,000 $361,764,000 $391,496,000
Transfers ‐ ‐$1,000,000 ‐$1,000,000 ‐$2,571,000 Trust Funds $5,851,000 $5,851,000 $5,851,000 $5,851,000 2010 ‐ ‐ ‐ ‐ Appropriation $403,698,000 $397,601,000 $477,928,000 $493,377,000 Transfers ‐ ‐$1,000,000 ‐$1,000,000 ‐$1,074,000 Trust Funds $5,851,000 $5,851,000 $5,851,000 $5,851,000 2011 ‐ ‐ ‐ ‐ Appropriation $490,439,000 $651,786,000 ‐ $651,786,000 Rescission ‐ ‐$1,315,000 ‐ ‐$1,316,000 Transfers ‐ ‐$176,551,000 ‐ ‐$176,551,000 Trust Funds ‐ $5,851,000 ‐ $5,851,000 2012 ‐ ‐ ‐ ‐ Appropriation $363,644,000 $343,280,000 $476,221,000 $475,221,000 Rescission ‐ ‐ ‐ ‐$898,000 Transfers ‐ ‐ ‐ ‐$70,000 2013 ‐ ‐ ‐ ‐ Appropriation $306,320,000 ‐ $466,428,000 $474,323,000 Rescission ‐ ‐ ‐ ‐$949,000 Sequestration ‐ ‐ ‐ ‐$23,861,000 Transfers ‐ ‐ ‐ ‐$2,112,000 2014 ‐ ‐ ‐ ‐ Appropriation $301,435,000 ‐ $477,208,000 $458,056,000 Transfers ‐ ‐ ‐ ‐$1,344,000 2015 ‐ ‐ ‐ ‐ Appropriation $278,800,000 ‐ $442,698,000 $448,034,000 2016 ‐ ‐ ‐ ‐ Appropriation $286,204,000 $361,394,000 $301,500,000 $456,009,000 Transfer ‐ ‐ ‐ ‐$516,000 2017 ‐ ‐ ‐ ‐ Appropriation $478,812,000 $365,009,000 $444,919,000 $460,629,000 Transfers ‐ ‐ ‐ ‐$1,050,000 2018 ‐ ‐ ‐ ‐ Appropriation $304,501,000 $292,881,000 $470,629,000 ‐ Rescission ‐ ‐ ‐ ‐$3,128,000

Page 13
General Departmental Management
All Purpose Table (Dollars in Thousands)
GDM FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 459,579 457,501 289,545 ‐167,956
Related Funding
PHS Evaluation Set‐Aside – Public Health Service Act 64,828 64,388 53,445 ‐10,943
Pregnancy Assistance Fund P.L. 111‐148 1 23,275 23,350 25,000 +1,650
HCFAC2 7,000 7,000 10,000 +3,000
Proposed Mandatory Funding (DAB)3 ‐ ‐ $2,000 +$2,000
Proposed User Fee Collections (DAB) 6 $1,457 +$1,457
Base Program Level 554,682 552,239 381,447 ‐170,792
FTE 1,169 1,157 1,184 +27
1 The Pregnancy Assistance Fund (PAF) is authorized and appropriated by the Patient Protection and Affordable Care Act (ACA) Public Law 111‐148. 2 The reimbursable program (HCFAC) in the General Department Management (GDM) account reflects estimates of the allocation account for 2019. Actual allocation will be determined annually. 3 The proposed mandatory funding has a legislative proposal in place to transfer funds from the Federal Hospital Insurance and General Supplementary Medical Insurance Trust Funds to the Departmental Appeals Board. 6 The proposed user fee collections for OMHA and DAB represent a proposal that creates a post‐adjudication user fee applied to all unfavorable appeals (other than beneficiary appeals) at the 3rd and 4th level of appeals.
GENERAL DEPARTMENTAL MANAGEMENT
Overview of Performance The General Departmental Management (GDM) supports the Secretary in his role as chief policy officer and general manager of HHS in administering and overseeing the organizations, programs and activities of the Department. The FY 2019 President’s Budget reflects decisions to streamline performance reporting and improve HHS performance‐based management. In accordance with this process GDM STAFFDIVs have focused on revising measures that depict the main impact or benefit of the program and support the rationale articulated in the budget request. This approach is reflected in the Department’s Online Performance Appendix (OPA). The OPA focus on key HHS activities, and includes performance measures that link to

Page 14
the HHS Strategic Plan for three GDM offices. They are: Immediate Office of the Secretary (IOS), Office of the Assistant Secretary for Administration (ASA), and OASH. The Office of the Assistant Secretary for Health (OASH) is the largest single STAFFDIV within GDM, managing thirteen cross‐cutting program offices, coordinating public health policy and programs across HHS operating and staff divisions (OPDIVs/STAFFDIVs), and ensuring the health and well‐being of Americans. This Justification includes individual program narratives that describe accomplishments, for all of the GDM components.

Page 15
OVERVIEW OF BUDGET REQUEST The FY 2019 President’s Budget for General Departmental Management (GDM) includes $289,545,000 in appropriated funds and 1,005 full‐time equivalent (FTE) positions. This request is ‐$167,956 below the FY 2018 Annualized CR. The GDM appropriation supports those activities associated with the Secretary’s roles as chief policy officer and general manager of the Department. This justification includes narrative sections describing the activities of each STAFFDIV funded under the GDM account, including the Rent and Common Expenses accounts. This justification also includes selected performance information. Secretary’s Initiatives and Innovation (‐$986,000) – The FY 2019 President’s Budget allows the Secretary to continue implementation of programs intended to improve and ensure the health and welfare of Americans. Acquisition Reform (‐$738,000) – The FY 2019 President’s Budget includes funding to continue improvements to acquisition practices and performance by maximizing competition and value, minimizing risk, and review of the acquisition workforce to develop, manage, and oversee acquisitions appropriately. Departmental Appeals Board (+$10,532,000) – The increase is composed of $18,000,000 in discretionary budget authority and $2,000,000 in proposed mandatory funding, and $1,457,000 in proposed user fee collections. The request supports DAB’s efforts, providing funding for additional employees needed to address the backlog of Medicare appeals. Office of Adolescent Health (‐$1,232,000) – The FY 2019 President’s Budget proposes eliminating this office and provides for funding to close out the program office. Teen Pregnancy Prevention (‐$100,314,000) – The FY 2019 President’s Budget does not include funds for this program. Minority Health (‐$2,329,000) – The FY 2019 President’s Budget enables OMH to continue to provide leadership in coordinating policies, programs, and resources to support implementation and monitoring of both the HHS Disparities Action Plan and the National Partnership for Action to End Health Disparities. Women’s Health (‐$3,468,000) – The FY 2019 President’s Budget allows OWH to continue the coordination of policies, programs, and information across HHS to support the OWH strategic plan. Sexual Risk Avoidance (‐$14,898,000) – The FY 2019 President’s Budget does not include funds for this program. Minority HIV/AIDS Initiative (‐$53,900,000) – The FY 2019 President’s Budget does not include funds for this program.

Page 16
IMMEDIATE OFFICE OF THE SECRETARY Budget Summary
(Dollars in Thousands)
Immediate Office of the Secretary
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 13,300 13,210 13,300 +90
FTE 79 79 79 ‐
Authorizing Legislation………….……………………………………………..........…..………….……………………….…Title III of the PHS Act FY 2018 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The Immediate Office of the Secretary (IOS) provides leadership, direction, policy, and management guidance to HHS, and supports the Secretary and Deputy Secretary in their roles as representatives of both the Administration and HHS. IOS serves as the nucleus for all HHS activities and shepherds the Department’s mission of enhancing the health and well‐being of Americans. The IOS mission involves coordinating all HHS documents, developing regulations requiring Secretarial action, mediating issues among Departmental components, communicating Secretarial decisions, and ensuring the implementation of those decisions. IOS achieves these objectives by ensuring key issues are brought to the Department’s attention in a timely manner, and facilitating discussions on policy issues. Documents requiring Secretarial action are reviewed for policy consistency with that of the Secretary and the Administration. IOS works with other Departments to coordinate analysis of, and input on, healthcare policy decisions impacting all HHS activities. IOS supports efforts to reform health care across HHS by improving the quality of the health care system and lowering its costs, computerizing all medical records, and protecting the privacy of patients. The Chief Technology Officer (CTO) drives and sustains innovation efforts at HHS, enabling Operating and Staff Divisions to deliver more efficient and effective services to the American people. CTO does this by establishing internal innovation programs and external partnerships to identify cross‐cutting program, process or technology issues at HHS and providing direction and technical support in solving these issues. CTO applies proven private sector techniques like design thinking, user‐centered design, and lean and agile approaches. This approach has empowered HHS agencies to test and develop ideas in an entrepreneurial environment that minimizes risk and improves performance. For example, these efforts have resulted in service improvements at HHS ranging from automating HRSA’s organ procurement and transplant process to enabling CMS to accelerate its clinical quality measures process from a 3‐5 year timeframe to 1 year. Along with other HHS officials, the CTO serves as a liaison to the White House Office of American Innovation, and represents the Department by engaging with public and private stakeholder organizations on efforts to modernize HHS by use of technology and accelerate IT innovation in the healthcare sector. The CTO also advises agencies on key technology policies and programs, open government practices, and applications of data to improve health and health care. The CTO collaborates with various HHS

Page 17
agencies responsible for developing health information technology policy in order to coordinate a cohesive IT strategy on behalf of the Department. The IOS Executive Secretariat works with pertinent components to develop comprehensive briefing documents, facilitates discussions among staff and operating divisions, and ensures final products reflect HHS policy decisions. IOS provides assistance, direction, and coordination to the White House and other Cabinet agencies regarding HHS issues. IOS sets the HHS regulatory agenda and reviews all new regulations and regulatory changes to be issued by the Secretary and/or the various components of the Department. The Executive Secretariat performs on‐going reviews of regulations which have already been published, with particular emphasis on reducing regulatory burden.
Funding History Fiscal Year Amount
FY 2014 $10,995,000
FY 2015 $13,300,000
FY 2016 $13,300,000
FY 2017 $13,300,000
FY 2018 Annualized CR $13,210,000
Budget Request The FY 2019 President’s Budget request for IOS is $13,300,000; an increase of $90,000 over the FY 2018 annualized CR level of $13,210,000. The increase will partially support pay and non‐pay inflationary costs. Funding will support personnel costs and maintain innovation initiatives and other services to achieve the Department’s Health Care, Human Services, Scientific Research, Health Data, Health Reform, and Workforce Development Strategic Goals. The funding will assist with development of tracking and coordination of Departmental correspondence and inquiries at a strategic level in regards to implementation and review of new and proposed laws. The request will allow the CTO to support the Secretary’s priorities for improving the efficiency, effectiveness, and accountability of HHS programs and services to meet requirements of Executive Order on a Comprehensive Plan for Reorganizing the Executive Branch (EO 13781) and OMB Memorandum M‐17‐22. CTO will continue its stakeholder engagement activities, providing guidance on HHS data and modernization priorities, establishing public/private partnerships to advance Secretarial priorities, and piloting new innovative health solutions with state and local governments. Along with other HHS officials, CTO will coordinate and harmonize health information technology strategy with various agencies within HHS and across the federal government to advance health and healthcare priority areas. Activities include reviewing policy and coordinating cross government feedback to ensure timely and effective IT policy. CTO will advance internal innovation programs and external partnerships to identify cross‐cutting process or technology issues at HHS and will provide direction and technical support in solving those issues. These programs will train HHS staff in employing
Page 18
user‐centered design, design thinking and user‐centered design techniques to improve services to the American public.
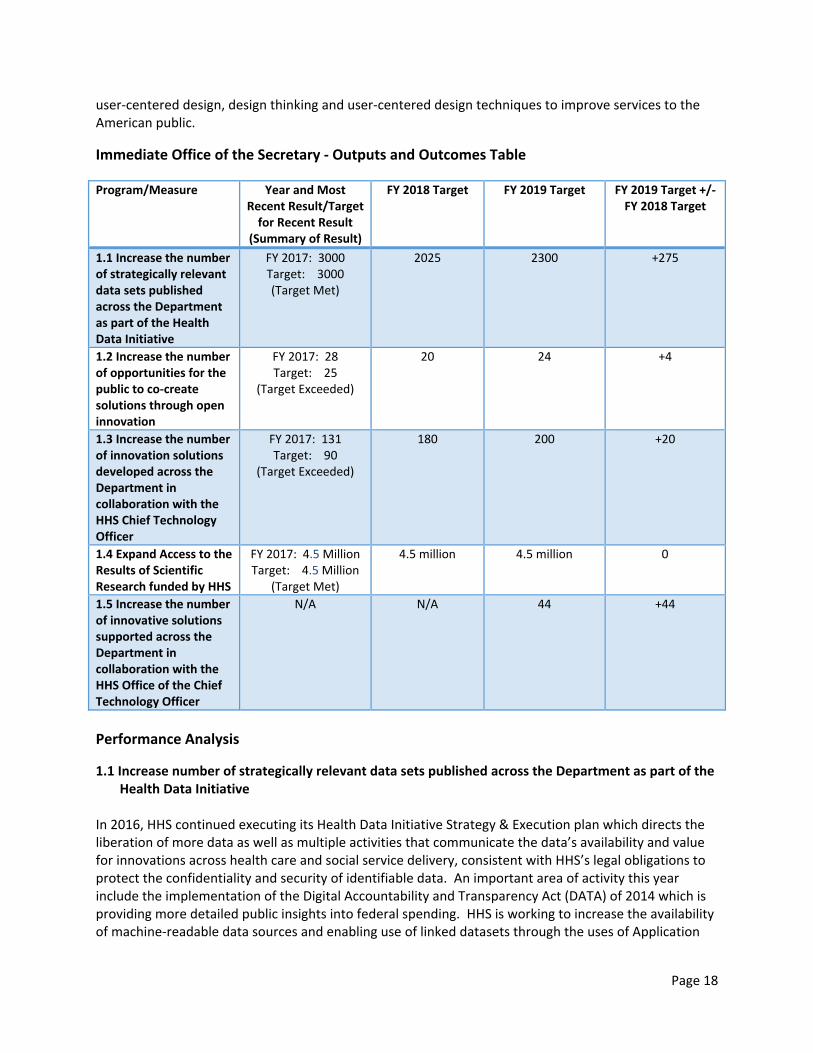
Immediate Office of the Secretary ‐ Outputs and Outcomes Table Program/Measure Year and Most
Recent Result/Target for Recent Result
(Summary of Result)
FY 2018 Target FY 2019 Target FY 2019 Target +/‐ FY 2018 Target
1.1 Increase the number of strategically relevant data sets published across the Department as part of the Health Data Initiative
FY 2017: 3000 Target: 3000 (Target Met)
2025 2300 +275
1.2 Increase the number of opportunities for the public to co‐create solutions through open innovation
FY 2017: 28 Target: 25
(Target Exceeded)
20 24 +4
1.3 Increase the number of innovation solutions developed across the Department in collaboration with the HHS Chief Technology Officer
FY 2017: 131 Target: 90
(Target Exceeded)
180 200 +20
1.4 Expand Access to the Results of Scientific Research funded by HHS
FY 2017: 4.5 Million Target: 4.5 Million
(Target Met)
4.5 million 4.5 million 0
1.5 Increase the number of innovative solutions supported across the Department in collaboration with the HHS Office of the Chief Technology Officer
N/A N/A 44 +44
Performance Analysis
1.1 Increase number of strategically relevant data sets published across the Department as part of the Health Data Initiative
In 2016, HHS continued executing its Health Data Initiative Strategy & Execution plan which directs the liberation of more data as well as multiple activities that communicate the data’s availability and value for innovations across health care and social service delivery, consistent with HHS’s legal obligations to protect the confidentiality and security of identifiable data. An important area of activity this year include the implementation of the Digital Accountability and Transparency Act (DATA) of 2014 which is providing more detailed public insights into federal spending. HHS is working to increase the availability of machine‐readable data sources and enabling use of linked datasets through the uses of Application

Page 19
Programming (APIs) interfaces. The APIs support machine‐to‐machine interactions that automate the supply of data to analytic tools, consumer platforms, and other forms electronic commerce and health care. These technology solutions and other advocacy efforts have led to an increase in number of datasets in 2016 at a faster rate of growth than previously imagined. Data inputs to healthdata.gov have steadily increased during this fiscal year. As of July 2016, there are 2,818 data sets from HHS and federated sources. Two examples of new resources include enhanced numbers of biomedical research databases published by the National Institutes of Health, and an online, cloud‐based, portal developed by the Food and Drug Administration that will allow scientists from industry, academia, government, and other partners to come together to foster innovation and develop the science behind a method of “reading” DNA known as next‐generation sequencing. In April 2017, HHS hosted the eighth Health Datapalooza, to showcase new products and services being developed with HHS data. HHS continues to expand its health data outreach efforts, particularly with its international partners. 1.2 Increase the number of opportunities for the public to co‐create solutions through open
innovation HHS has used innovation in a wide array of business areas and research fields to spur new ideas and concepts to be tested. HHS sees positive benefits to its education, training, and mentoring programs to help build a cadre of challenge managers across the operating divisions. HHS launched a $20 Million prize challenge for addressing antimicrobial resistance – a key problem that is in need of new solutions. 1.3 Increase the number of innovative solutions identified across the Department in collaboration
with the Chief Technology Officer CTO continued to encourage the development of innovative solutions across the Department during FY 2016. A primary focus used to enhance outreach capabilities and increase knowledge of programs across the Department. In FY 2017, CTO launched two rounds of the Ignite Accelerator program. In FY 2017, it also received 203 submissions through this program, of which 43 were selected for piloting and participated in the training “boot camp.” Two HHS operating divisions (HRSA and CDC) started their own incubator programs aimed at expanding the scope of the early stage solution development phase of innovation allowing more participants to learn. 1.4 Expand Access to the Results of Scientific Research In February 2015, HHS released the HHS Public Access Plans, which provide an outline of the Department’s efforts to increase access to the results of its scientific research, as appropriate. These plans now apply to research funded by six of its key scientific agencies: NIH, CDC, FDA, AHRQ, ACL, and ASPR. The HHS public access plans build on an existing infrastructure, the NIH’s National Library of Medicine’s (NLM) Pub Med Central, for the storing and sharing of publications of publications with the public. Thus far, NLM’s PubMed Central Database includes over 3.8 million journal articles. The rate of growth of the number of publications submitted since 2016 will continue to grow as the CDC, FDA, AHRQ and ASPR begin to include their funded journal articles in the PubMed Repository. As the contents of the

Page 20
database grow and diversify, HHS anticipates that it will create yet more opportunities for new connections to be made among disparate fields of scientific inquiry, and new types of knowledge and insights that can benefit health and healthcare. HHS expects it will allow for faster dissemination of research results into products, services and clinical practices that can improve healthcare. 1.5 Increase the number of innovative solutions supported across the Department in collaboration
with the HHS Office of the Chief Technology Officer This measure represents the number of projects developed at HHS that the CTO supports through dedicated staff time. This can include projects where CTO support was initiated in previous fiscal years and whose support continues in the fiscal year of question. This does not include projects that are captured in Measure 1.2 “opportunities for the public to co‐create solutions through open innovation.”

Page 21
SECRETARIAL INITIATIVES AND INNOVATIONS Budget Summary (Dollars in Thousands)
Secretarial Initiatives and Innovations
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 1,765 1,986 1,000 ‐986
FTE ‐ ‐ ‐ ‐
Authorizing Legislation: …………….......................................................................................Title III of the PHS Act FY 2018 Authorization……………….……………………………………………….....................………………………………………Indefinite Allocation Method…………………………………………………………….…………………………………………..………………Direct Federal
Program Description and Accomplishments The Secretarial Initiatives and Innovations request supports the Secretary in effectively responding to emerging Administration priorities, while supporting the missions of HHS Operating Divisions (OPDIVs) and Staff Divisions (STAFFDIVs). The funding allows the Secretary the necessary flexibility to identify, refine, and implement programmatic and organizational goals in response to evolving business needs and legislative requirements. Secretarial Initiatives and Innovations allows the Secretary to promote and foster innovative, high‐impact, collaborative, and sustainable initiatives that target HHS priorities and address intradepartmental gaps.
Funding History
Fiscal Year Amount
FY 2014 $2,735,000
FY 2015 $2,629,000
FY 2016 $2,000,000
FY 2017 $1,765,000
FY 2018 Annualized CR $1,986,000
Budget Request The FY 2018 President’s Budget request of $1,000,000 is $986,000 below the FY 2018 Annualized CR level of $1,986,000. The FY 2019 request will allow the Secretary to proactively respond to the needs of the Office of the Secretary as it continues to implement programs intended to improve and ensure the health and welfare of Americans. These funds will be directed to the Secretary's highest priorities and are implemented and monitored judiciously. The impact of these resources will be monitored based on the Secretary's stated goals and objectives for their use.

Page 22
ASSISTANT SECRETARY FOR ADMINISTRATION Budget Summary
(Dollars in Thousands)
Assistant Secretary for Administration
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 17,458 17,339 17,458 +119
FTE 114 114 114 ‐
Authorizing Legislation………….……………………………….......…………………………..…………….……Title III of the PHS Act FY2019 Authorization……………….…………………..........…..………….……………………………..….…………….......……Indefinite Allocation Method………………………………………….……………………………….……………………………..………..Direct Federal
Program Description and Accomplishments The Office of the Assistant Secretary for Administration (ASA) advises the Secretary on all aspects of administration; provides leadership, policy, oversight, supervision, and coordination of long and short‐range planning for HHS with respect to internal administration; and supports the agency’s strategic goals and objectives. ASA also provides critical Departmental policy and oversight in the following major areas through eight ASA components; five are GDM funded entities, and include the Immediate Office of the Assistant Secretary, Office of Human Resources, Equal Employment Opportunity Compliance and Operations Division, Office of the Chief Information Officer and the Office of Business Management and Transformation. The Office of Security and Strategic Information, which has been moved from ASA to the IOS, and the Program Support Center are funded through other sources and are not included in this request. Office of Human Resources (OHR) OHR provides leadership in the planning and development of personnel policies and human resource programs that support and enhance the Department's mission. OHR also provides technical assistance to the HHS Operating Divisions (OPDIVs) to accomplish each OPDIV’s mission through improved planning and recruitment of human resources, and serves as the Departmental liaison to central management agencies on related matters. OHR provides leadership in creating and sustaining a diverse workforce and an environment free of discrimination at HHS. OHR works proactively to enhance the employment of women, minorities, veterans, and people with disabilities, consistent with the law, through efforts that include policy development, oversight, complaint prevention, investigations and processing, outreach, commemorative events, and standardized education and training programs. Equal Employment Opportunity Compliance and Operations Division (EEOCO) EEOCO provides services to every HHS employee and applicant, ensuring equal access to EEO services and timely resolution of complaints, as well as equitable remedies. The Compliance Team provides leadership, oversight, technical guidance and engages in policy development for the complaint processing units in the HHS OPDIV EEO Offices including processing Remands, Appeals, and Conflict Cases. In addition, the team writes Commission Corp decisions, Final Orders, and Final Agency Decisions. Further, EEOCO serves as HHS’s liaison with lead agencies such as Equal Employment Opportunity Commission, Merit Systems Protection Board (MSPB), and Office of Personnel Management (OPM) in matters involving EEO complaint processing.

Page 23
Office of the Chief Information Officer (OCIO) OCIO advises the Department on matters pertaining to the use of information and related technologies to accomplish Departmental goals and program objectives. OCIO establishes and provides assistance and guidance on the internal use of technology‐supported business process reengineering, investment analysis and performance measurement, while managing strategic development and application of information systems and infrastructure in compliance with the Clinger‐Cohen Act. OCIO promulgates internal HHS IT policies supporting enterprise architecture, capital planning and project management, and security. OCIO coordinates the implementation of IT policy from the Office of Management and Budget and guidance from the Government Accountability Office throughout HHS, and ensures the IT investments remain aligned with HHS strategic goals and objectives and the Enterprise Architecture. OCIO coordinates the HHS response to federal IT priorities including Data Center consolidation; cloud computing; information management, sharing, and dissemination; and shared services. OCIO is responsible for compliance, service level agreement management, delivery of services, service and access optimization, technology refreshment, interoperability and migration of new services. OCIO works to develop a coordinated view to ensure optimal value from IT investments by addressing key agency‐wide policy and architecture standards, maximizing smart sharing of knowledge, sharing best practices and capabilities to reduce duplication, and working with OPDIVs and STAFFDIVs on the implementation and execution of an expedited investment management process. Office of Business Management and Transformation (OBMT) OBMT provides results‐oriented strategic and analytical support for key management and various HHS components’ improvement initiatives and coordinates the business functions necessary to enable the supported initiatives and organizations to achieve desired objectives. OBMT also oversees Department‐wide multi‐sector workforce management activities. OBMT provides business process reengineering services, including the coordination of the review and approval process for reorganization and delegation of authority proposals that require the Secretary or designees’ signature. Finally, OBMT leads Departmental and cross‐government initiatives that promote innovation or implement effective management practices within the Department.
Funding History Fiscal Year Amount
FY 2014 $17,958,000
FY 2015 $17,458,000
FY 2016 $17,458,000
FY 2017 $17,458,000
FY 2018 Annualized CR $17,339,000
Budget Request The FY 2019 President’s Budget request for ASA is $17,458,000; an increase of $119,000 over the FY 2018 Annualized CR level of $17,339,000. The request will partially support pay and non‐pay inflationary increases; maintain current staffing levels; and continue its established mission of policy and oversight.
Page 24
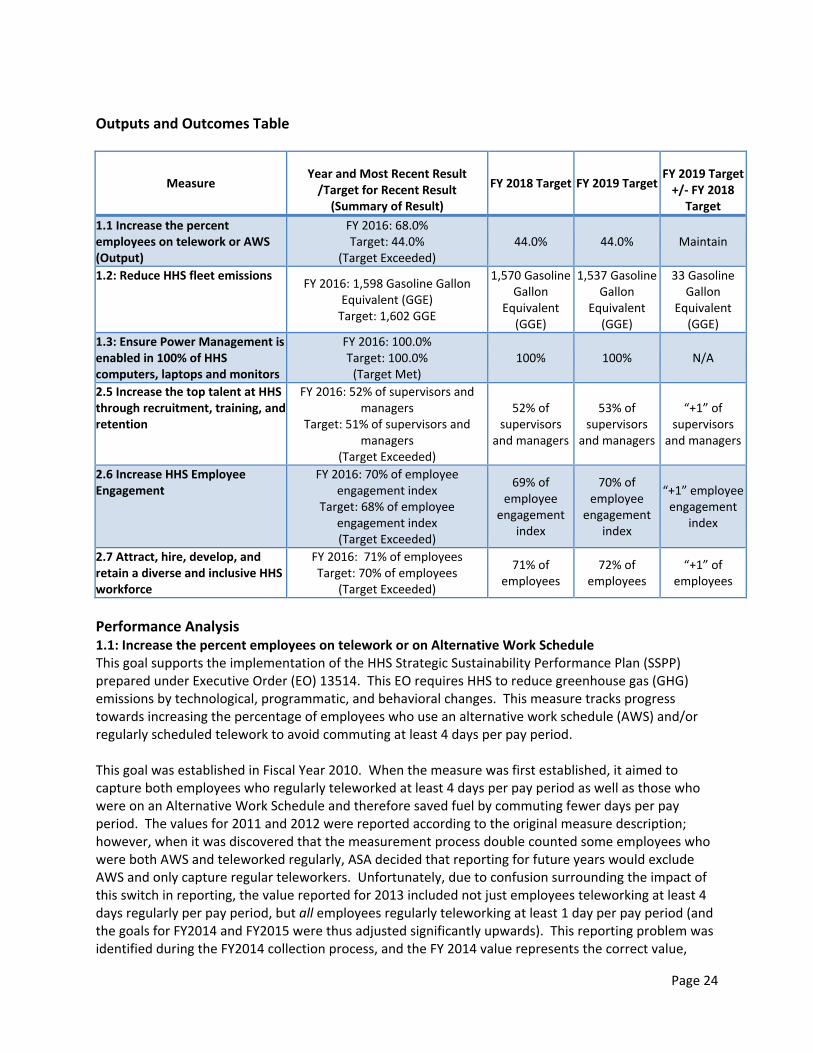
Outputs and Outcomes Table
Measure Year and Most Recent Result /Target for Recent Result
(Summary of Result)
FY 2018 Target FY 2019 Target FY 2019 Target +/‐ FY 2018
Target
1.1 Increase the percent employees on telework or AWS (Output)
FY 2016: 68.0% Target: 44.0%
(Target Exceeded) 44.0% 44.0% Maintain
1.2: Reduce HHS fleet emissions FY 2016: 1,598 Gasoline Gallon
Equivalent (GGE) Target: 1,602 GGE
1,570 Gasoline Gallon
Equivalent (GGE)
1,537 Gasoline Gallon
Equivalent (GGE)
33 Gasoline Gallon
Equivalent (GGE)
1.3: Ensure Power Management is enabled in 100% of HHS computers, laptops and monitors
FY 2016: 100.0% Target: 100.0% (Target Met)
100% 100% N/A
2.5 Increase the top talent at HHS through recruitment, training, and retention
FY 2016: 52% of supervisors and managers
Target: 51% of supervisors and managers
(Target Exceeded)
52% of supervisors
and managers
53% of supervisors
and managers
“+1” of supervisors
and managers
2.6 Increase HHS Employee Engagement
FY 2016: 70% of employee engagement index
Target: 68% of employee engagement index (Target Exceeded)
69% of employee
engagement index
70% of employee
engagement index
“+1” employee engagement
index
2.7 Attract, hire, develop, and retain a diverse and inclusive HHS workforce
FY 2016: 71% of employees Target: 70% of employees
(Target Exceeded)
71% of employees
72% of employees
“+1” of employees
Performance Analysis 1.1: Increase the percent employees on telework or on Alternative Work Schedule This goal supports the implementation of the HHS Strategic Sustainability Performance Plan (SSPP) prepared under Executive Order (EO) 13514. This EO requires HHS to reduce greenhouse gas (GHG) emissions by technological, programmatic, and behavioral changes. This measure tracks progress towards increasing the percentage of employees who use an alternative work schedule (AWS) and/or regularly scheduled telework to avoid commuting at least 4 days per pay period. This goal was established in Fiscal Year 2010. When the measure was first established, it aimed to capture both employees who regularly teleworked at least 4 days per pay period as well as those who were on an Alternative Work Schedule and therefore saved fuel by commuting fewer days per pay period. The values for 2011 and 2012 were reported according to the original measure description; however, when it was discovered that the measurement process double counted some employees who were both AWS and teleworked regularly, ASA decided that reporting for future years would exclude AWS and only capture regular teleworkers. Unfortunately, due to confusion surrounding the impact of this switch in reporting, the value reported for 2013 included not just employees teleworking at least 4 days regularly per pay period, but all employees regularly teleworking at least 1 day per pay period (and the goals for FY2014 and FY2015 were thus adjusted significantly upwards). This reporting problem was identified during the FY2014 collection process, and the FY 2014 value represents the correct value,

Page 25
percentage of employees regularly teleworking at least 4 days per pay period. Goals for the upcoming fiscal years have thus been adjusted appropriately for this metric. Increasing the percentage of teleworking/AWS employees reduces vehicle miles traveled. Widespread telework/AWS coupled with office sharing and swing space can reduce overall facilities costs in rents, waste removal, wastewater treatment, and energy use. 1.2: Reduce HHS fleet emissions HHS is committed to replacing gasoline‐powered vehicles with alternative fuel vehicles (AFV) in accordance with GSA acquisition guidelines. As a result, the fleet's petroleum consumption will decrease, as will the amount of carbon dioxide the fleet releases into the atmosphere. HHS is aiming to reduce fleet emissions by 2% annually. This measure uses Million Metric Tons of Carbon Dioxide equivalents, or MTCO2e, a standard measure of greenhouse gas emissions. In 2013, primarily through reducing its gasoline fuel use, HHS reduced its CO2e emissions substantially, bringing the number under the 2013 target, and 2014 saw another improvement in emissions levels. HHS CO2e emissions are expected to improve going forward. 1.3: Ensure Power Management is enabled in 100% of HHS computers, laptops and monitors HHS IT contracts have been revised to include power‐saving configuration requirements. HHS is measuring the percentage of eligible computers, laptops, and monitors with power management, including power‐saving protocols in the standard configuration for employee workstations. Consistent application of power management will decrease the electricity use of HHS facilities. This initiative supports the HHS strategic initiative to be a good steward of energy resources. The target for this measure is for 100% of HHS eligible computers, laptops, and monitors to have power management. HHS set aggressive goals to move from the 2010 level of 32% of devices with power management enabled to 100% of devices with power management by 2013 and to maintain that level continuing through 2015. In 2011, 85% of eligible devices were reported in compliance across the department, while in 2012 this increased to 94%. In 2013, an improved Department‐wide surveying showed that 97% of HHS laptops and computers had power management enabled (108,805 of 112,311 devices), while 89% of monitors were enabled across the Department (621,290 of 697,592 devices), for a total of 90% of devices covered by power management. The 2014 Electronic Stewardship Report showed this value increased to 99% with a breakdown of 98.44% or 107,622 eligible PCs & Laptops on power management, and 99.78% or 116,208 monitors on power management. HHS remains committed to meeting its power management target, and these numbers should continue to rise as HHS improves coordination between OCIO and OPDIV IT teams. 2.5: Increase the top talent at HHS through recruitment, training, and retention This performance metric has been added to the set of metrics ASA is tracking following a 2014 review of metrics by OHR. HHS is committed to recruiting and retaining top talent to meet America’s health and human service needs, and this metric allows measurement of progress towards this goal. This metric will be measured through responses to OPM Annual Employee Viewpoint survey of all full‐time and part‐time federal employees. Analysis will be conducted on the responses of HHS managers and supervisors to the question “My work unit is able to recruit people with the right skills.” The percentage will be tracked and reported annually. In FY 2014 49% of supervisors and managers answered the recruitment question positively.

Page 26
2.6: Increase HHS Employee Engagement This performance metric has been added to the set of metrics ASA is tracking following a 2014 review of metrics by OHR. Improving employee engagement within HHS is a vital method for promoting new and dynamic solutions to challenges facing the organization. This metric will be tracked using the employee engagement index, calculated from OPM Annual Employee Viewpoint survey. Specifically, the metric is derived from questions related to leadership, supervisor behaviors, and intrinsic experience. A successful agency fosters an engaged working environment to ensure each employee can reach their full potential and contribute to the success of their agency and the entire Federal Government. Historically, HHS has performed above the government norm, and future targets reflect HHS continuing efforts to improve employee engagement. In FY 2014, the HHS‐wide employee engagement index was 66%, while the government‐wide result was 63%. By increasing employee engagement, HHS can help create a workforce that is encouraged to provide for the health of all Americans. 2.7 Attract, hire, develop, and retain a diverse and inclusive HHS workforce This performance metric has been added to the set of metrics ASA is tracking following a 2014 review of metrics by OHR. HHS strives to have a workforce that reflects the population that it serves. A diverse workforce also introduces new and useful perspectives to issues that HHS must address. In order to gauge its success at hiring, developing, and retaining a diverse and inclusive workforce, HHS, in addition to using hiring and retention data, will look at the most recent results from OPM Annual Employee Viewpoint survey. Specifically, HHS will track the percentage of employees who positively report, “My supervisor is committed to a workforce representative of all segments of society.” In 2014, 68% of HHS respondents indicated their supervisors were committed to a diverse workforce. An analysis of this data as well as applicant and employee churn ratio analysis (not reported in this performance measure) will enable HHS leadership to drive further success in this area.

Page 27
ASSISTANT SECRETARY FOR FINANCIAL RESOURCES Budget Summary
(Dollars in Thousands)
Assistant Secretary for Financial Resources
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 30,444 30,238 30,444 +206
FTE 149 149 149 ‐
Authorizing Legislation: ……………........................................................................................Title III of the PHS Act FY 2017 Authorization……………….……………………………………………….....................…..…………………..………………Indefinite Allocation Method…………………………………………………………….……………………………………………………………Direct Federal
Program Description and Accomplishments Office of Budget (OB) – OB manages the performance budget and prepares the Secretary to present the budget to the Office of Management and Budget (OMB), the public, the media, and Congressional committees; serves as the HHS appropriations liaison; and manages HHS apportionment activities, which provide funding to the HHS Operating Divisions (OPDIVs) and Staff Divisions (STAFFDIVs). OB coordinates, oversees, and convenes resource managers and financial accountability officials within OS to update, share, and implement related HHS‐wide policies, procedures, operations, rules, regulations, recommendations, and priorities. Additionally, OB leads the Service and Supply Fund by providing budget process, formulation, and execution support, including budget analysis and presentation, account reconciliations, reporting, status of funds tracking, and certification of funds availability. OB manages the implementation of the Government Performance and Results Modernization Act and all phases of HHS performance budget improvement activities. Office of Finance (OF) – OF provides financial management leadership to the Secretary through the CFO and the Departmental CFO Community. The OF leads the HHS‐wide financial management efforts and prepares the Secretary to present the HHS Agency Financial Report to OMB, Treasury, GAO, Congressional committees, and the public, in coordination with HHS OPDIVs and STAFFDIVs. OF manages and directs the development and implementation of financial policies, standards, and internal control practices; and prepares the HHS annual consolidated financial and grant statements and audits, in accordance with the CFO Act, OMB Circulars, Federal Managers Financial Integrity Act, and the Federal Accounting Standards Advisory Board. OF provides Department‐wide leadership to implement new financial management requirements and other mandated reporting. OF oversees the HHS financial management systems portfolio, and is the business and systems owner of such systems. OF prepares the Agency Financial Report which includes the Department’s consolidated financial statements, the auditor’s opinion and other statutorily required annual financial reporting. For many years, HHS has earned an unmodified or “clean” opinion on the HHS audited Consolidated Balance Sheet, and Statements of Net Cost and Changes in Net Position, and Combined Statement of Budgetary Resources. OF successfully produced the Agency Financial Report on time in compliance with Federal requirements, and for the fourth year in a row, earned the prestigious Certificate of Excellence in Accountability Reporting Award for the FY 2016 HHS Agency Financial Report. OF leads the Department’s Enterprise Risk Management initiative. This work includes supporting the HHS ERM Council, to collaboratively identify, assess, and manage HHS’s risks. This also involves collaboratively engaging the OPDIVs and STAFFDIVs to establish, communicate, and implement HHS’s ERM vision, strategy, culture, and framework.

Page 28
OF manages HHS’s entire financial management systems environment, including projects to standardize financial accounting across the Department, implement government‐wide financial management requirements, address security and control weaknesses, and develop Financial Business Intelligence System to enhance Department‐wide analytic capabilities and support decision making. OF continues to progress on its strategic roadmap, manage programs to enhance system security, reliability, and availability; increase effectiveness and efficiency; and improve access to accurate, reliable, and timely information.
Office of Grants and Acquisition Policy and Accountability (OGAPA) – OGAPA provides HHS‐wide leadership, management, and strategy in grants, acquisitions, small business policy development, performance measurement, and oversight and workforce training. OGAPA also fosters collaboration, innovation, and accountability in the administration and management of the grants, acquisition, and small business functions throughout HHS. OGAPA also fulfills the HHS role as managing partner of GRANTS.gov, and supports the financial accountability and transparency initiatives such as those associated with the Federal Funding Accountability and Transparency Act, the DATA Act, and Open Government Directive, by maintaining and operating HHS Tracking Accountability in Government Grants System and Departmental Contract Information System. Since FY 2013, HHS has served as the co‐Chair for the Council on Financial Assistance Reform and OGAPA supported government‐wide grants policy initiatives through the Counsel on Financial Assistance Reform, including the development and implementation of the new uniform grants guidance at 2 CFR 200; the development and publication of HHS implementing regulation at 45 CFR 75; and the updating of internal policy guidance within the Grants Policy Statement and Grants Policy Administration Manual. OGAPA also led an initiative to update the HHS Acquisition Regulation; participated in acquisition rule making; made improvements to the HHS acquisition workforce training and certification programs; and began efforts to reform the HHS acquisition lifecycle framework to improve program management and acquisition outcomes across‐HHS. OGAPA established and monitored appropriate grant and acquisition related internal controls and performance measures; provided technical assistance and oversight to foster stewardship, transparency, and accountability in HHS grants and acquisition programs; responded to grants or acquisition‐oriented GAO and IG audits; and led the Department’s Strategic Sourcing, Green Procurement, and Government Purchase Card programs. OGAPA ensured that small businesses were given a fair opportunity to compete for HHS contracts; managed and tracked small business goal achievements; provided technical assistance and Small Business Program training to HHS contracting and program officials; conducted outreach and provided guidance to small businesses on doing business with HHS; and developed and implemented a new online tool to produce and publish HHS procurement forecast. Digital Accountability and Transparency (Data) Act Project Management Office ‐ The Digital Accountability and Transparency Act of 2014 (DATA Act) expands the Federal Funding Accountability and Transparency Act in an effort to improve the transparency of Federal spending. The HHS DATA Act Program Management Office is responsible for leading implementation of the DATA Act within HHS, and has been designated by OMB as the executing agent for the grants activities to be carried out under Section 5 of the statute. The Section 5 Pilot Program generated recommendations to standardize reporting elements, eliminate duplication and unnecessary reports, and reduce recipient compliance costs that were reported through OMB to Congress in August 2017.

Page 29
Funding History
Fiscal Year Amount
FY 2014 $28,974,000
FY 2015 $30,444,000
FY 2016 $30,444,000
FY 2017 $30,444,000
FY 2018 Annualized CR $30,238,000
Budget Request The FY 2019 President’s Budget request of $30,444,000 is $206,000 above the FY 2018 Annualized CR level of $30,238,000. The increase will partially support inflation costs and maintain ASFR responsibilities associated with financial management; program integrity; budget and performance analysis and support; grants and acquisition policies; grant transparency; acquisition workforce development; improving the use of program, performance, and financial data to inform business decisions and to offset salary increases. The Office of Budget will continue to meet its responsibilities for providing financial management leadership including preparation of HHS annual performance budget; production of budget and related policy analyses, options, and recommendations; management and support of program performance reviews, annual strategic plans, and agency priority goals; and development and implementation related to accountability and transparency priorities. The Office of Finance will continue to meet its responsibilities for providing financial management leadership including management, development, and implementation of HHS financial policies, standards and internal control practices; and preparing financial statements, financial audits, and other financial reports. OF will continue to modernize Department‐wide financial systems by enabling new functionality, standardizing and simplifying financial systems environment, strengthening internal controls, and improving financial reporting. This multi‐year modernization initiative will standardize financial management across HHS, modernize financial reporting to provide timely, reliable, and accurate information about HHS finances and enhance, standardize and simplify financial systems. OGAPA will continue to lead HHS to ensure that appropriate grant and acquisition related internal controls and policies are followed, provide technical assistance, policy advice, and training to HHS OPDIVs and STAFFDIVs to ensure stewardship of HHS grants, financial assistance, acquisition, and small business programs. The DATA Act PMO is expected to terminate operations on September 30, 2018. Funding is not requested in FY 2019.
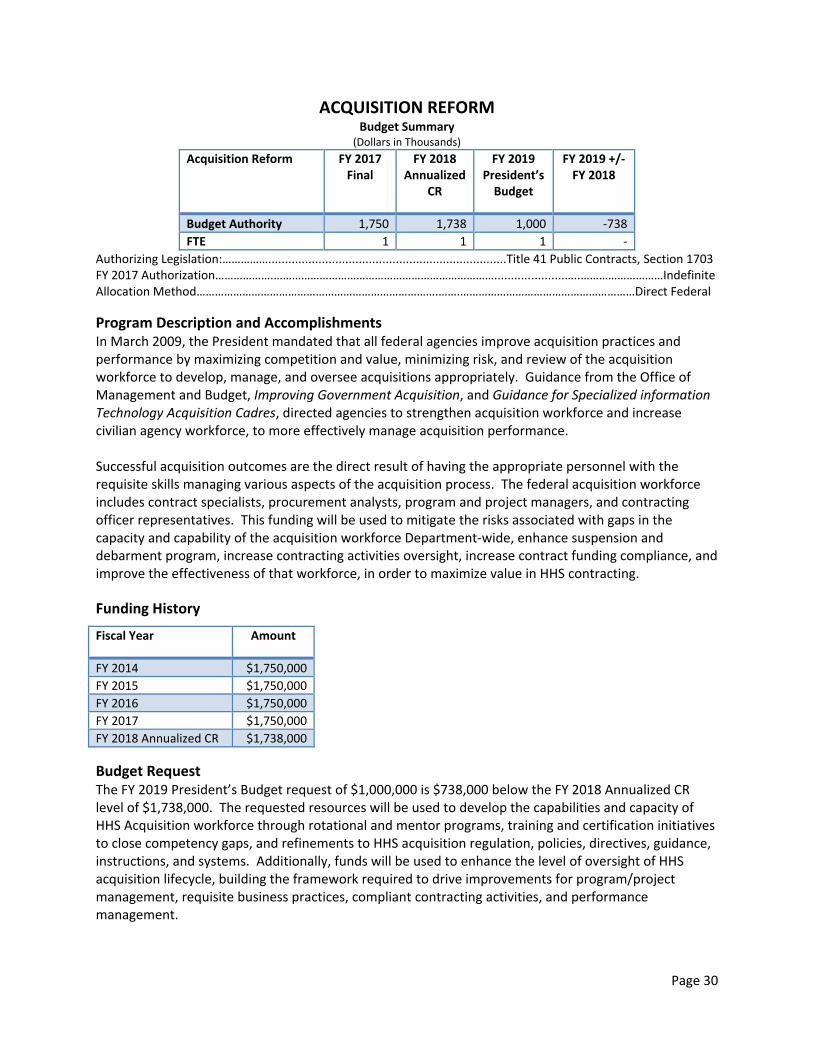
Page 30
ACQUISITION REFORM
Budget Summary (Dollars in Thousands)
Acquisition Reform FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 1,750 1,738 1,000 ‐738
FTE 1 1 1 ‐
Authorizing Legislation:…………….......................................................................Title 41 Public Contracts, Section 1703 FY 2017 Authorization……………….……………………………………………………………….....................…..………………………Indefinite Allocation Method…………………………………………………………………….…….…………………………………………………Direct Federal
Program Description and Accomplishments In March 2009, the President mandated that all federal agencies improve acquisition practices and performance by maximizing competition and value, minimizing risk, and review of the acquisition workforce to develop, manage, and oversee acquisitions appropriately. Guidance from the Office of Management and Budget, Improving Government Acquisition, and Guidance for Specialized information Technology Acquisition Cadres, directed agencies to strengthen acquisition workforce and increase civilian agency workforce, to more effectively manage acquisition performance. Successful acquisition outcomes are the direct result of having the appropriate personnel with the requisite skills managing various aspects of the acquisition process. The federal acquisition workforce includes contract specialists, procurement analysts, program and project managers, and contracting officer representatives. This funding will be used to mitigate the risks associated with gaps in the capacity and capability of the acquisition workforce Department‐wide, enhance suspension and debarment program, increase contracting activities oversight, increase contract funding compliance, and improve the effectiveness of that workforce, in order to maximize value in HHS contracting.
Funding History
Fiscal Year Amount
FY 2014 $1,750,000
FY 2015 $1,750,000
FY 2016 $1,750,000
FY 2017 $1,750,000
FY 2018 Annualized CR $1,738,000
Budget Request The FY 2019 President’s Budget request of $1,000,000 is $738,000 below the FY 2018 Annualized CR level of $1,738,000. The requested resources will be used to develop the capabilities and capacity of HHS Acquisition workforce through rotational and mentor programs, training and certification initiatives to close competency gaps, and refinements to HHS acquisition regulation, policies, directives, guidance, instructions, and systems. Additionally, funds will be used to enhance the level of oversight of HHS acquisition lifecycle, building the framework required to drive improvements for program/project management, requisite business practices, compliant contracting activities, and performance management.

Page 31
ASSISTANT SECRETARY FOR LEGISLATION Budget Summary
(Dollars in Thousands)
Assistant Secretary for Legislation
FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 4,100 4,072 4,100 +28
FTE 27 27 27 ‐
Authorizing Legislation:………….………………………………………………..........…..………….………………………Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The Office of the Assistant Secretary for Legislation (ASL), a staff division within the Office of the Secretary, serves as the principal advocate before Congress for the Administration’s health and human services initiatives; serves as chief HHS legislative liaison and principal advisor to the Secretary and the Department on Congressional activities; and maintains communications with executive officials of the White House, OMB, and other Executive Branch Departments on legislative matters, as well as with Members of Congress and their staffs, and the Government Accountability Office (GAO). ASL informs the Congress of the Department's views, priorities, actions, grants, contracts, and provides information and briefings that support the Administration’s priorities and the substantive informational needs of the Congress.
Immediate Office of the Assistant Secretary for Legislation ‐ Serves as principal advisor to the Secretary with respect to all aspects of the Department's legislative agenda and Congressional liaison activities. Examples of ASL activities include: working closely with the White House to advance Presidential initiatives relating to health and human services; managing the Senate confirmation process for the Secretary and the 19 other Presidential appointees requiring Senate confirmation; transmitting the Administration’s proposed legislation to the Congress; and working with Members of Congress and staff on legislation for consideration by appropriate Committees and by the full House and Senate.
Office of Health Legislation ‐ Assists in the legislative agenda and liaison for mandatory and discretionary health programs. This portfolio includes: health‐science‐oriented operating divisions, including SAMHSA, FDA, NIH, AHRQ, and CDC; medical literacy, quality, patient safety, privacy; bio‐defense and public health preparedness and response; health services and health care financing operating divisions, including CMS; Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP); private sector insurance; Continuity of Operations (COOP) activities.
Office of Human Services Legislation ‐ Assists in the legislative agenda and liaison for human services and income security policy. This portfolio includes: ACF, ACL, IHS, HRSA, and ONC; health IT; cyber security. These three offices develop and work to enact the Department's legislative and administrative agenda, coordinating meetings and communications of the Secretary and other Department officials with Members of Congress, and preparing witnesses and testimony for Congressional hearings. Congressional Liaison Office (CLO) – Assists in the legislative agenda and special projects. The office is the primary liaison to Members of Congress and serves as a clearing house for Member and

Page 32
Congressional staff questions and requests. This office maintains the Department’s program grant and contract notification system to inform Members of Congress and is responsible for notifying and coordinating with Congress regarding the Secretary’s travel and event schedule. Nearly 100,000 grant notifications are sent to Members of Congress annually. CLO is also responsible for processing correspondence from Members of Congress to the Assistant Secretary for Legislation and the Secretary. CLO provides staff support for the Assistant Secretary for Legislation, coordinating responsibilities to the HHS regional offices, and works with ASFR to coordinate budget distribution, briefings and hearings.
Office of Oversight and Investigations (O&I) ‐ Responsible for all matters related to Congressional audit and investigations of Departmental programs, including those performed by the Government Accountability Office (GAO). O&I serves as the central point of contact for the Department in handling congressional requests for oversight interviews, briefings, and documents; developing responses with agencies within the Department; consulting with other Executive Branch entities; and negotiating with congressional and GAO staff regarding investigations. HHS receives hundreds of oversight letters from Congressional Oversight Committees. HHS has received hundreds of new audit inquiries and over 400 recommendations that require corrective actions.
Funding History
Fiscal Year Amount
FY 2014 $3,791,000
FY 2015 $3,643,000
FY 2016 $4,100,000
FY 2017 $4,100,000
FY 2018 Annualized CR $4,072,000
Budget Request The FY 2019 President’s Budget request for ASL is $4,100,000; an increase of $28,000 over the FY 2018 Annualized CR level of $4,072,000. The Budget will allow ASL to continue to provide mission critical support to the legislative healthcare and human services agenda and continue to meet Congressional inquiries related to the broad range of HHS programs. In FY 2019, ASL will continue to facilitate the Secretary’s commitment to safeguard the health and well‐being of the American people, and advance positive changes to our health care system to improve its affordability, accessibility, quality, and responsiveness. The request for ASL will facilitate communication between the Department and Congress. This requires continued work on several mission critical areas with Members of Congress, Congressional Committees and staff, including: managing the Senate confirmation process for Department nominees; preparing witnesses and testimony for Congressional hearings; coordinating Department response to Congressional oversight and investigations as well as coordinating responses to GAO inquiries; improving Congressional awareness of issues relating to the programs and priorities of the Administration and advising Congress on the status of key HHS priority areas.

Page 33
ASSISTANT SECRETARY FOR PUBLIC AFFAIRS Budget Summary
(Dollars in Thousands)
Assistant Secretary for Public Affairs FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 8,408 8,351 8,408 +57
FTE 56 56 56 ‐
Authorizing Legislation:………….………………………………………………..........…..………….………………….…Title III of the PHS Act FY 2018 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………..……..………..Direct Federal
Program Description and Accomplishments The Office of the Assistant Secretary for Public Affairs (ASPA) serves as the Health and Human Services (HHS) principal Public Affairs office, leading HHS efforts to promote transparency, accountability, and access to critical public health and human services information for the American people. ASPA is also responsible for communicating the HHS mission, Secretarial initiatives, and other activities to the general public through various channels of communication. ASPA plays an important role by:
Overseeing efforts to expand HHS’s transparency and public accountability efforts through new and innovative communications tools and technology.
Providing timely, accurate, consistent and comprehensive public health information to the public, and ensuring the information is easy to find and understand.
Advising and preparing the Secretary for public communications, including communicating HHS strategic plans.
Coordinating public health and medical communications across all levels of government and with international and domestic partners.
Developing and managing strategic risk communications plans in response to national public health emergencies.
Serving as the central HHS press office handling media requests, developing press releases, and managing news issues that cut across HHS.
Overseeing the HHS flagship website, HHS.gov.
Developing Departmental protocols and strategies to utilize social media and the web.
Supporting television, web, and radio appearances for the Secretary and senior HHS officials; managing the HHS studio and providing photographic services; producing and distributing internet, radio, and television outreach materials.
Writing speeches, statements, articles, and related material for the Secretary, Deputy Secretary, Chief of Staff, and other senior HHS officials.
Overseeing HHS‐wide FOIA and Privacy Act program policy, implementation, compliance, and operations.
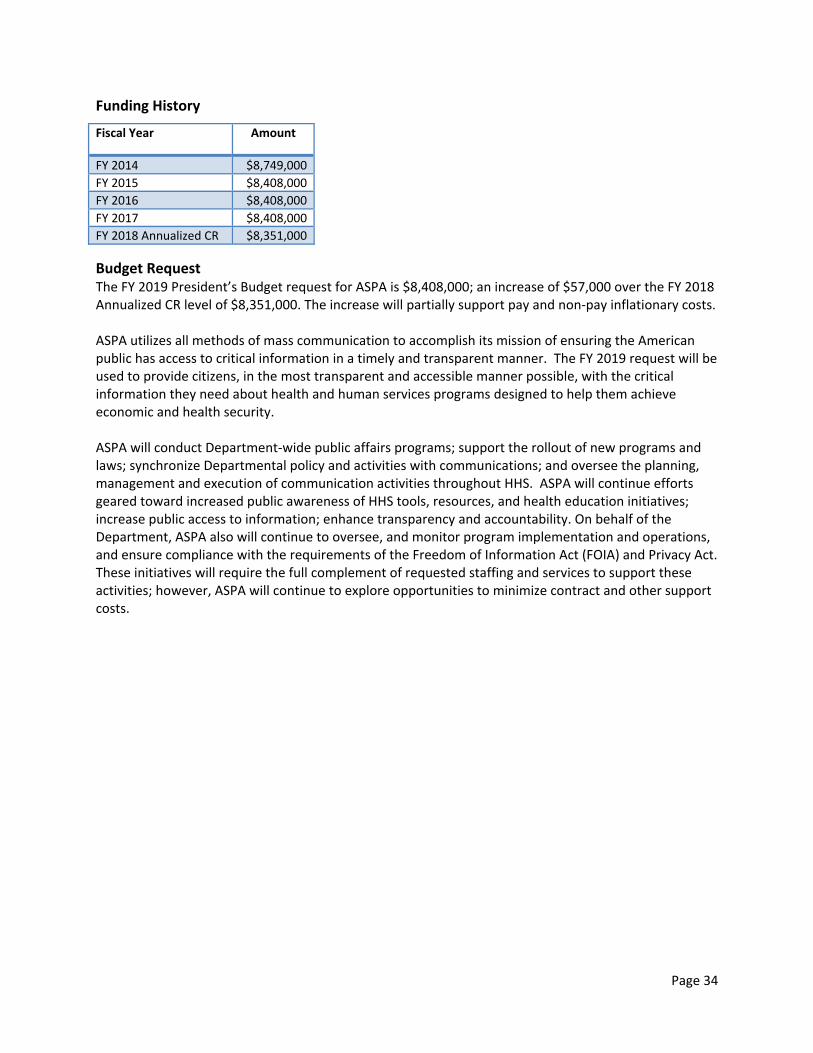
Page 34
Funding History
Fiscal Year Amount
FY 2014 $8,749,000
FY 2015 $8,408,000
FY 2016 $8,408,000
FY 2017 $8,408,000
FY 2018 Annualized CR $8,351,000
Budget Request The FY 2019 President’s Budget request for ASPA is $8,408,000; an increase of $57,000 over the FY 2018 Annualized CR level of $8,351,000. The increase will partially support pay and non‐pay inflationary costs. ASPA utilizes all methods of mass communication to accomplish its mission of ensuring the American public has access to critical information in a timely and transparent manner. The FY 2019 request will be used to provide citizens, in the most transparent and accessible manner possible, with the critical information they need about health and human services programs designed to help them achieve economic and health security. ASPA will conduct Department‐wide public affairs programs; support the rollout of new programs and laws; synchronize Departmental policy and activities with communications; and oversee the planning, management and execution of communication activities throughout HHS. ASPA will continue efforts geared toward increased public awareness of HHS tools, resources, and health education initiatives; increase public access to information; enhance transparency and accountability. On behalf of the Department, ASPA also will continue to oversee, and monitor program implementation and operations, and ensure compliance with the requirements of the Freedom of Information Act (FOIA) and Privacy Act. These initiatives will require the full complement of requested staffing and services to support these activities; however, ASPA will continue to explore opportunities to minimize contract and other support costs.

Page 35
OFFICE OF THE GENERAL COUNSEL Budget Summary (Dollars in Thousands)
Office of the General Counsel FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 31,100 30,889 31,100 +211
FTE 143 143 143 ‐
Authorizing Legislation:………….………………………………………………..........…..………….………………………Title III of the PHS Act FY 2018 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The Office of the General Counsel (OGC), with a team of over 400 attorneys and a comprehensive support staff, is one of the largest, most diverse, and talented law offices in the United States. It provides client agencies throughout HHS with representation and legal advice on a wide range of highly visible national issues. OGC’s goal is to support the strategic goals and initiatives of the Office of the Secretary of Health and Human Services, and HHS, by providing high quality legal services, including sound and timely legal advice and counsel. Accomplishments:
OGC has been working with the Department of Justice (DOJ) to defend litigation challenging the Secretary’s handling of the backlog of Medicare appeals pending before the Office of Medicare Hearings and Appeals (OMHA). HHS generally prevailed in such suits, as claimants have a right to escalate their claims when OMHA is not within statutory timelines, until the D.C. Circuit Court of Appeals overturned one such case brought by the American Hospital Association and remanded it to the District Court. On remand, the District Court issued a writ of mandamus requiring the Secretary to eliminate the backlog of Medicare claims appeals pending at OMHA on a fixed timetable to be cleared by December 31, 2020. The D.C. Circuit subsequently vacated the mandamus order and remanded the case back to the District Court to evaluate the merits of the Secretary’s claim that lawful compliance with the mandamus order’s timetable would be impossible. Following a brief discovery period during which plaintiffs deposed two HHS employees and the Secretary produced a limited number of documents, the parties are currently finishing summary judgment briefing before the District Court.
OGC’s Centers for Medicare & Medicaid Services Division (CMSD) provided advice on numerous legal issues that arose in launching the Medicare Quality Payment Program (QPP). The QPP is at the heart of the bipartisan Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) repeal of the much criticized sustainable growth rate formula for Medicare physician payment. The highly complex system of QPP provisions that took effect in FY 2017 permanently impacts Medicare physician payment. OGC helped the Centers for Medicare & Medicaid Services (CMS) to craft flexibility in the type and timing of clinician reporting for the Medicare Incentive Payment System (MIPS) and to maximize recognition of clinician participation in Alternative Payment Models (APMs), playing an instrumental role in achieving agency goals to substantially reduce burdens on clinicians while meeting statutory requirements. OGC also successfully defended cases challenging Medicare reimbursement to hospitals, helping to preserve the Medicare Trust Fund.
OGC’s General Law Division (GLD) has been instrumental in advising CMS regarding the administration of its core programs, including advising policy makers regarding relevant fiscal and

Page 36
procurement laws. In addition, GLD continues to have a lead role in providing advice regarding the Federal Advisory Committee Act (FACA), as well as providing advice on the disclosure, retention, and withholding of information requested through various mechanisms. Finally, GLD has provided employment and labor law advice to senior policy makers, and has represented the Department in related litigation matters.
OGC’s Public Health Division (PHD) spearheaded the efforts to resolve over $2 billion in contract support costs claims stemming from the multi‐year Indian Self‐Determination and Education Assistance Act (ISDEAA) contract litigation against the Indian Health Service. This effort has resulted in settling $1.8 billion in claims for $807 million, a savings of over $977 million. Additionally, PHD coordinated the Department's legal response to the Zika virus disease outbreak response on complex matters such as: ensuring that the department properly issued an assurance of confidentiality issued under section 308(d) of the PHS Act; advising on environmental and related issues associated with aerial spraying for mosquitoes; advising on the distribution of medical devices and preparedness kits to the population; negotiating the terms of multiple agreements for receiving and sharing Zika virus samples in a manner that allowed for widespread distribution of therapeutics, vaccines, and related products consistent with other countries’ intellectual property rights and related rights; and use of the Strategic National Stockpile.
Funding History
Fiscal Year Amount
FY 2014 $39,226,000
FY 2015 $31,100,000
FY 2016 $31,100,000
FY 2017 $31,100,000
FY 2018 Annualized CR $30,899,000
Budget Request The FY 2019 President’s Budget request for the Office of the General Counsel (OGC) is $31,100,000; an increase of $211,000 over the FY 2018 Annualized CR level of $30,899,000. The FY 2019 request of $31,100,000 will partially support pay and non‐pay inflationary costs incurred by OGC as a result of providing HHS with legal representation on key social, economic, and healthcare issues. In FY 2019, OGC will provide legal advice pertaining to fiscal law, grants, and procurements. OGC attorneys will be highly involved in rulemaking and will continue to assist and support CMS in its mission of making health insurance available, transforming the health care delivery system and the Medicaid program, and reducing fraud, waste and abuse in the federal health care systems. OGC will provide legal advice to clients seeking to revise and update regulations, such as those for the Health Resources Administration’s (HRSA) health professional shortage designation, Substance Abuse Mental Health Services Administration’s (SAMHSA) confidentiality of substance abuse patient records, and the 340B Drug Program. OGC will also advise and assist the National Institutes of Health (NIH) on many important and complex matters, including the agency’s large research grants portfolio, intellectual property, technology transfer, third‐party reimbursement at NIH’s Clinical Center, genomic data sharing, biodefense research, and diversity initiatives. OGC will advise on multiagency preparedness efforts related to pandemic influenza, MERS‐CoV and other chemical, biological, radiological, and nuclear threats. OGC will also coordinate and ensure

Page 37
consistency in the negotiation of over 300 Indian Self‐Determination and Education Assistance Act (ISDEAA) contracts and compacts, which transfer $2 billion annually to Tribes, and will handle approximately 1,500 contract dispute claims under ISDEAA. OGC will also be involved in the implementation of the 2007 Hague Convention on the International Recovery of Child Support and Other Forms of Family Maintenance. OGC will continue to assist in the finalization of major rulemaking efforts by the Office of Child Support Enforcement (OCSE) and the Office of Child Care. In addition, OGC will continue to provide defense of litigation challenging Designation Renewal System rules and re‐competition decisions for the Head Start program.

Page 38
DEPARTMENTAL APPEALS BOARD
Budget Summary (Dollars in Thousands)
Departmental Appeals Board FY 2017 Final FY 2018 Annualized CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 11,000 10,925 18,000 +7,075
Mandatory Funding ‐ ‐ 2,000 +2,000
Proposed User Fee Collections ‐ ‐ 1,457 +1,457
Total DAB Funding Level 11,000 10,925 21,457 +10,532
FTE 70 70 117 +47
* The FY 2019 President’s Budget provides $10,000,000 from Recovery Audit collections to address Medicare Appeals at OMHA and DAB. This amount is not displayed in this table. Authorizing Legislation………….……………………………………………..........…..………….………………………….Title III of the PHS Act FY 2018 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….…………………....………..Direct Federal
Program Description and Accomplishments The Departmental Appeals Board (DAB), a staff division within the Office of the Secretary, provides impartial, independent hearings and appellate reviews, and issues Federal agency decisions under more than 60 statutory provisions governing HHS programs. The DAB’s mission is to provide high‐quality adjudication and other conflict resolution services in administrative disputes involving HHS, and to maintain efficient and responsive business practices. Cases are initiated by outside parties who disagree with a determination made by an HHS agency or its contractor. Outside parties include states, universities, Head Start grantees, nursing homes, clinical laboratories, doctors, medical equipment suppliers, and Medicare beneficiaries. Disputes heard by the DAB may involve over $1 billion in federal funds in a single year. DAB decisions on certain cost allocation issues in grant programs have government‐wide impact because HHS decisions in this area legally bind other Federal agencies. The DAB is organized into four Divisions: Board Members – Appellate Division The Secretary appoints the DAB Board Members, including the Board Chair who serves as the executive for the DAB. Board Members, acting in panels of three, issue decisions with the support of Appellate Division staff. Board Members provide appellate review of decisions by DAB ALJs and Department of Interior ALJs (in certain Indian Health Service cases). In addition, Board Members provide de novo review of certain types of final decisions by HHS components, including ACF, CMS, HRSA, SAMHSA, ONC, and PSC, involving discretionary and mandatory grants and cooperative agreements. Board review ensures consistency of administrative decisions, as well as adequacy of the record and legal analysis before court review. For example, Board decisions in cases involving grant awards promote uniform application of OMB cost principles. Board decisions are posted on the DAB Website and provide precedential guidance on ambiguous or complex requirements. In FY 2017, the Board/Appellate Division received 126 cases; and closed 134 cases, of which 92 were by decision.

Page 39
Administrative Law Judges – Civil Remedies Division (CRD) CRD staff support DAB Administrative Law Judges (ALJs) who conduct adversarial hearings and issue decisions on the record in a wide variety of proceedings that are critical to HHS healthcare program integrity efforts to combat fraud, as well as quality of care concerns. Hearings in these cases may last a week or more. Cases may raise complex medical or clinical issues. Some cases require presentation of evidence to prove allegations of complicated fraudulent schemes. Cases may also raise legal issues of first impression, such as appeals of enforcement cases. DAB ALJs hear cases appealed from CMS or OIG determinations which exclude providers, suppliers, or other healthcare practitioners from participating in Medicare, Medicaid, and other Federal healthcare programs, or impose civil monetary penalties (CMPs) for fraud and abuse in such programs. CRD jurisdiction also includes appeals from Medicare providers or suppliers, including cases under the Clinical Laboratory Improvement Amendments of 1988 (CLIA). Expedited hearings are provided when requested in certain types of proceedings, such as provider terminations and certain nursing home penalty cases. These cases typically involve important quality of care issues. ALJs also hear cases which may require challenging testimony from independent medical/scientific experts (e.g., in appeals of Medicare Local Coverage Determinations (LCDs) or issues of research misconduct for the purposes of fraudulently obtaining federal grants in cases brought forth by the Office of Research Integrity (ORI)). Through reimbursable inter‐agency agreements, ALJs conduct hearings on CMPs imposed by the Inspector General of the Social Security Administration (SSA) and on certain debt collection cases brought by the SSA. ALJs also conduct hearings in certain regulatory actions brought by the Food and Drug Administration (FDA), including CMP determinations, No Tobacco Sale Orders (NTSOs), clinical investigator disqualifications, and other adverse actions. In FY 2017, CRD received 7,970 new cases and closed 7,514 (94%), 1,861 by decision. Medicare Appeals Council – Medicare Operations Division (MOD) The MOD provides staff support to the Administrative Appeals Judges (AAJs) and Appeals Officers (AOs) on the Medicare Appeals Council (Council). The Council provides the final administrative review within HHS of claims for entitlement to Medicare and individual claims for Medicare coverage and payment filed by beneficiaries or health care providers/suppliers. Council decisions are based on a de novo review of decisions issued by ALJs in the Office of Medicare Hearings and Appeals (OMHA). CMS (or one of its contractors) and SSA may also refer ALJ decisions to the Council for own‐motion review. In the majority of cases, the Council has a statutorily imposed 90‐day deadline by which it must issue a final decision. An appellant may file a request with the Council to escalate an appeal from the ALJ level because the ALJ has not completed his or her action on the request for hearing within the adjudication deadline. MOD has been receiving a greater number of these escalations as the caseload has been increasing at the OMHA level. The Council also reviews cases remanded back to the Secretary from Federal court; related to this workload, MOD is responsible for preparing and certifying administrative records to Federal court. Cases may involve complex issues of law, such as appeals arising from overpayment determinations, non‐sample audits, or statistical sampling extrapolations involving thousands of claims and high monetary amounts. Some cases, particularly those filed by enrollees in a Medicare Advantage plan, require an expedited review due to the pre‐service nature of the benefits at issue (e.g., pre‐service authorization for services or procedures or authorization for prescription drugs).

Page 40
Beginning in FY 2015, through a reimbursable agreement with CMS, MOD began adjudicating appeals filed under a CMS demonstration project with the state of New York. The demonstration project, called “Fully Integrated Duals Advantage” Plan (FIDA), offers an estimated 170,000 Medicare‐Medicaid enrollees in New York an opportunity for more coordinated care. FIDA will provide a streamlined appeals process which gives beneficiaries the opportunity to address denials of items and services through a unified system that includes all Medicare and Medicaid protections. These new FIDA cases are not included in the MOD workload Chart C below. DAB will incorporate them into its future workload projections after gaining an experience base from which to project annual FIDA case closures. In FY 2017, MOD received 9,396 appeals and closed 2,545. Note that case closures include 215 cases dismissed pursuant to administrative settlement agreements with certain hospitals for partial payment for eligible claims in exchange for withdrawing the associated appeals. Alternative Dispute Resolution (ADR) ‐ Alternative Dispute Resolution Division The ADR Division provides services in DAB cases and supports the Chair as the HHS Dispute Resolution Specialist. The ADR Division provides mediation in DAB cases; provides or arranges for mediation services in other HHS cases (including workplace disputes and claims of employment discrimination filed under the HHS Equal Employment Opportunity program); and provides policy guidance, training, and information on ADR techniques (including negotiated rulemaking – a collaborative process for developing regulations with interested stakeholders). Under the Administrative Dispute Resolution Act, each Federal agency must appoint a dispute resolution specialist and must engage in certain activities to resolve disputes by informal methods, such as mediation, that are alternatives to adjudication or litigation. The DAB Chair is the Dispute Resolution Specialist for HHS and oversees ADR activities pursuant to the HHS policy issued under the Act. Using ADR techniques decreases costs and improves program management by reducing conflict and preserving relationships that serve program goals (e.g., between program offices and grantees, or among program staff). In FY 2017, the ADR Division received 112 requests for ADR services, and closed 114, and conducted 12 conflict resolution seminars. Workload Statistics: Board Members – Appellate Division Chart A shows total historical and projected caseload data for the Appellate Division. FY 2018 and FY 2019 data are based on (1) CRD’s projections of the number of ALJ decisions to be issued in FYs 2018 and 2019 in both non‐FDA and FDA cases, and (2) the following assumptions:
Changes in Appellate staff, including retirement of long‐time Division Director in August 2017 and hiring one additional attorney in FY 2019; and
Increases in the number of appeals of ALJ decisions issued in FDA cases in FY 2018 and increases in the number of appeals of ALJ decisions issued in non‐FDA cases in FY 2019.

Page 41
APPELLATE DIVISION CASES – Chart A Cases FY 2017 FY 2018 FY 2019
Open/start of FY 78 70 80
Received 126 135 150
Decisions 92 90 100
Total Closed 134 125 125
Open/end of FY 70 80 105 Administrative Law Judges – Civil Remedies Division Chart B shows caseload data for CRD. FY 2018 and FY 2019 data are projected based on historical trends and certain assumptions, including:
The extension of the inter‐agency agreements in FY 2017 to hear FDA cases, an increase in the number of CMP complaints and NTSOs in 2017, and no significant changes in the number of CMP complaints and NTSOs in FYs 2018 and 2019;
CMS’s increased use of data analysis techniques to detect provider/supplier fraud and noncompliance;
A continued 20% increase each year in the number of provider/supplier cases (including a 20% increase in revocations each year resulting from a 2014 change in regulations governing revocations and a 35% increase in effective date cases each year resulting from 2016 changes in CMS program integrity policies);
New types of hearing requests, such as appeals pursuant to agreements under the Medicare Coverage Gap Discount Program;
The Inspector General’s increased focus on exclusion cases;
No major regulatory changes; and
Increases in personnel in FY 2019, including one ALJ, and three attorneys.
CIVIL REMEDIES DIVISION CASES – Chart B Cases FY 2017 FY 2018 FY 2019
Non‐
FDA FDA
Non‐
FDA FDA
Non‐
FDA FDA
Open/start of FY 420 808 669 1,015 1,182 1,195
Received 1,210 6,760 2,117 7,200 2,117 7,200
Decisions 221 1,640 221 1,800 300 1,800
Total Closed 961 6,553 1,604 7,020 2,176 7,020
Open/end of FY 669 1,015 1,182 1,195 1,123 1,375
The data in the preceding chart separates the FDA cases and non‐FDA cases, which is CRD’s core work. Medicare Appeals Council – Medicare Operations Division Chart C contains historical and projected caseload data for MOD. FY 2018 and FY 2019 data are based on information from the HHS Dashboard Report and Long‐Term Projections Report. Assumptions on which the data are based include:
In FY 2019, pursuant to the proposed legislation, change in the standard of review from “de novo” to “material error of law” and “substantial evidence,” increasing the Council’s current adjudicative capacity by approximately 30%;

Page 42
An additional 16,000 cases closed in FY 2018 pursuant to administrative settlements;
Increased case receipts in FY 2018 as OMHA’s disposition capacity increases with new ALJ teams and resources;
Increased overpayment cases (including Recovery Audit (RA) and statistical sampling cases); Increased CMS demonstration projects across the country;
Participation in Department‐wide administrative initiatives to improve efficiency within the Medicare appeals process and address appeals as early as possible; and
Increased requests for certified administrative records in cases appealed to Federal court.
MEDICARE OPERATIONS DIVISION CASES – Chart C Cases FY 2017 FY 2018 FY 2019
Open/start of FY 23,469 30,320 29,044
Received 9,396 17,044 26,412
Cases Closed 2,330 2,320 6,240
Administrative Settlements
215 16,000 ‐‐
Open/end of FY 30,320 29,044 49,216
Funding History
Budget Request The FY 2019 President’s Budget discretionary request for the DAB is $18,000,000; an increase of $9,075,000 over the FY 2018 annualized CR level of $10,925,000. The request also includes $2,000,000 in proposed mandatory funding, and $1,457,000 in proposed user fee collections. The budget increases will provide new funding above the FY 2018 level for 47 additional employees needed to address the backlog of Medicare appeals and to replenish staffing in all other Divisions. Since FY 2010, the Medicare Operations Division of the DAB has experienced a significant increase in the number of annual appeals. Because resources have remained relatively constant over this same period of time, the increase in appeals has led to a backlog of cases and an increase in average case processing times. With case receipts continuing to outpace staff resources, the backlog will continue to grow and hamper overall productivity. In addition, intensified efforts to increase the disposition of OMHA’s appeals backlog will result in an increase of appeals flowing to the DAB, further exacerbating the rate of increase in the MOD backlog. In addition to the increased volume of receipts, MOD faces a greater percentage of technically complex statistical sampling cases and multi‐claim overpayment cases. Further, MOD cases often generate voluminous administrative record; when cases are appealed to Federal court, MOD staff must prepare and certify the accuracy of the record for the court. The caseload data presented here fully justifies the DAB request. The Budget will allow the MOD to add 4 AAJs, 24 attorneys, and 3 legal support positions, increasing MOD’s overall staff size from 29 to 60. This increase, along with the proposed legislative change to the
Fiscal Year Amount
FY 2014 $10,450,000
FY 2015 $11,000,000
FY 2016 $11,000,000
FY 2017 $11,000,000
FY 2018 Annualized CR $10,925,000

Page 43
Council’s standard of review (addressed in detail below), would increase the Council’s adjudicative capacity to 6,240 cases, representing a 169% increase over the projected FY 2018 level adjudication capacity of 2,320 cases. As a result of the Medicare Appeals backlog, the DAB has had to shift resources to MOD from other Divisions. The Budget will right‐size staffing across DAB as well as address the increase in Civil Remedies Division pending appeals. One new attorney would be assigned to the Appellate Division, one to the ADR Division, and three to the CRD Division. Currently, all DAB policy, adjudicative oversight, and administrative operations are consolidated in the Immediate Office of the Chair and the Operations Division. This structure allows judges and legal staff to focus solely on legal work, ensuring maximum productivity. The FY 2019 request would allow the DAB to increase administrative efficiency, improve oversight in the DAB’s adjudicatory divisions, and focus more attention on organizational improvement and myriad operational challenges, driven by growing demands and a lack of specialized personnel dedicated to administrative support and IT development. Accordingly, the Immediate Office would add 5 new staff and the Operations Division would add 5 new staff. Legislative Proposal – Improving the Medicare Appeals Process As part of the Department’s FY 2019 budget process, the DAB submitted a legislative proposal to change the Medicare Appeals Council’s (Council) standard of review under Section 1869(d)(2)(B) of the Social Security Act from de novo to an appellate‐level standard of review. Under the proposed standard of review, the Council would be able to grant a request for review of a decision by an ALJ or other adjudicator of Medicare claims if: (1) there is an abuse of discretion; (2) there is an error of law material to the outcome of the case; (3) the findings of fact are not supported by substantial evidence; or (4) there is a need to clarify an important question of law, policy, or fact. The proposal would also clarify that the Council may deny a request for review.

Page 44
DAB ‐ Outputs and Outcomes Table
Measure Year and Most Recent Result/Target for Recent Result
(Summary of Result)
FY 2018 Target
FY 2019 Target FY 2019 Request +/‐ FY 2018
1.1.1 Percentage of Board Decisions with net case age of six months or less
2017: 70% Target: 66%
(Target Exceeded)
50% 50% Maintain
1.2.1 Percentage of Board decisions meeting applicable statutory and regulatory deadlines for issuance of decisions.
FY 2017: 100% Target: 100% (Target Met)
90% 100% +10%
1.3.1 Percentage of decisions issued within 60 days of the close of the record in HHS OIG enforcement, fraud and exclusion cases.
FY 2017: 100% Target: 90%
(Target Exceeded)
90% 90% Maintain
1.3.2 Percentage of decisions issued within 60 days of the close of the record in SSA OIG CMP cases and other SSA OIG enforcement cases.
FY 2017: 100% Target: 90%
(Target Exceeded)
90% 90% Maintain
1.3.3 Percentage of decisions issued within 180 days from the date appeal was filed in provider/supplier enrollment cases.
FY 2017: 100% Target: 90%
(Target Exceeded)
90% 90% Maintain
1.4.1 Cases closed in a fiscal year as a percentage of total cases open in the fiscal year.
FY 2017: 81% Target: 50%
(Target Exceeded)
50% 50% Maintain
1.5.1 Number of conflict resolution seminars conducted for HHS employees.
FY 2017 12 Sessions Target: 12 Sessions
(Target Met)
10 10 Maintain
1.5.2 Number of DAB cases (those logged into ADR Division database) requesting facilitative ADR interventions prior to more directive adjudicative processes.
FY 2017: 112 Target: 110
(Target Exceeded)
110 110 Maintain
1.6.1 Average time to complete action on Requests for Review measured from receipt of the claim file.
FY 2017: 605 days Target: 576 days (Target Not Met)
1,229 days 798 days ‐431 days
1.7.1 Number of dispositions FY 2017: 2,330 +215 (CMS settlements)
Target: 2,320 (Target Exceeded)
2,320 6,240 +3,920

Page 45
Performance Analysis DAB has made measurable progress in the strategic management of human capital by reengineering its operations and improving its case management techniques. The DAB shifts resources across its Divisions as needed to meet changing caseloads, and targets mediation services to reduce pending workloads. Appellate Division In FY 2017, 70% of Appellate Division decisions had a net case age of six months or less, exceeding the Measure 1.1.1 target of 66%. In FY 2018 and FY 2019, the target for Measure 1.1.1 is reduced to 50%, due to the loss of productivity while the DAB fills the vacancy caused by the retirement of its long‐time Division Director in August 2017, and due to an increase in the number of appeals. The Appellate Division expects to meet the targets for Measure 1.1.1 in both fiscal years. In FY 2017, the Appellate Division met the target for Measure 1.2.1 by issuing decisions in 100% of appeals having a statutory or regulatory deadline. In FY 2018, the target for Measure 1.2.1 will decrease from 100% to 90% for the same reasons as for the reduction stated above. In FY 2019, the target will return to 100% as productivity normalizes and as a result of hiring one additional staff attorney. The Appellate Division expects to meet the target levels for Measure 1.2.1 in both FY 2018 and FY 2019. Civil Remedies Division For FY 2017, Measures 1.3.1, 1.3.2, and 1.3.3 relate to the percentage of cases in which CRD ALJs met the statutory or regulatory deadlines for rendering final decisions in particular types of cases (60 days from record closed date for OIG and SSA enforcement, fraud, or exclusion cases; 180 days for CMS provider/supplier enrollment cases). CRD exceeded its targets in all three Measures in FY 2017. For FY 2018 and FY 2019, the DAB proposes consolidating prior Measures 1.3.1, 1.3.2, and 1.3.3 into a single new Measure 1.3.1, which will track the percentage of all CRD decisions issued within all applicable statutory and regulatory deadlines. The target for Measure 1.3.1 will remain the same in FY 2018 and FY 2019, and CRD expects to meet that target in both fiscal years. Measure 1.4.1 tracks cases closed as a percentage of all cases open during the fiscal year. CRD exceeded its FY 2017 target by closing 81% of open cases. CRD closed 59% of non‐FDA cases and 86% of FDA cases. The FY 2018 and FY 2019 targets remain unchanged because non‐FDA cases are more complex, resulting in longer adjudication times, and because CRD projects the same number of receipts of FDA CMPs and NTSOs. CRD expects to meet Measure 1.4.1 in both of those years, but will be challenged to do so if it receives a significant increase in the number of FDA cases and new types of appeals through reimbursable inter‐agency agreements. Medicare Operations Division Target 1.6.1 measures how long it takes to close a case after MOD receives the claim file. However, the DAB does not request the claim file until staff is available to work on the case. Therefore, the measure only reflects how long it takes MOD to close a case after the claim file for the case is received, not how long it takes from the date the DAB receives the request for review to the date the Council issues a final decision. The larger the backlog, the longer it takes for MOD staff to be available to work on a new case and the longer the overall time for HHS to resolve Medicare claims. The average case age is projected to increase from 605 days in FY 2017 to 1,229 days in FY 2018, but decrease to 798 days in FY 2019. While the focus on closing high priority cases, including Part C and D pre‐service cases and beneficiary appeals, is designed to reduce the average case age, this effort is negated in FY 2018 by the consistent rate of
Page 46
growth of the Medicare appeals backlog. New staff, as well as the proposed legislative change in the standard of review, will increase the DAB’s ability to address that trend in FY 2019. Measure 1.7.1 tracks case closures, which are directly proportional to staffing. Case closures will remain relatively constant in FY 2018, and are expected to increase in FY 2019 due to an increase in staff. Alternative Dispute Resolution (ADR) Division In FY 2017, ADR met Measure 1.5.1 and exceeded Measure 1.5.2 by leveraging resources through a variety of means, including: using video teleconferencing technology to replace in‐person mediations, thereby reducing staff‐time otherwise needed for travel; using interagency partnerships to share scarce ADR training and mediation resources across Agency lines; and using unpaid legal interns. In FY 2017, caseload receipts increased modestly due to the FY 2016 initiatives to mediate Equal Employment Opportunity cases for the Office of the Secretary’s EEO Compliance and Operations Division and the Indian Health Service’s EEO Compliance and Operations Division. ADR projects no additional case increases for FY 2018 or FY 2019. ADR anticipates meeting its targets for Measures 1.5.1 and 1.5.2 in FY 2018 and FY 2019 by continuing to leverage resources through technology, interagency partnerships, and unpaid interns. ADR also plans to address backlogging by redirecting resources from conflict resolution seminars to mediations (decreasing Measure 1.5.1 from 12 to 10 seminars), and by increasing the number of cases mediated by free Federal Sharing Neutrals program mediators.

Page 47
OFFICE OF GLOBAL AFFAIRS Budget Summary
(Dollars in Thousands)
Office of Global Affairs FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 6,026 5,985 6,026 +41
FTE 22 22 22 ‐
Authorizing Legislation………….………………………………………………..........…..………….………………………Title III of the PHS Act Authorization Status……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The Office of Global Affairs (OGA) promotes and protects the health of US citizens, and works to improve global health and safety. It does so by advancing HHS's global strategies and partnerships, and by working with HHS divisions and other US Government (USG) agencies in the coordination of global health policy and international engagement. OGA develops policy recommendations and provides staff support to the Secretary and other HHS leaders on global health and social services issues. OGA coordinates these matters within HHS, across the government, and at multilateral institutions working on major crosscutting global health initiatives. OGA provides global health expertise on a range of policy issues, and identifies and uses capacities present in HHS to address needs and opportunities overseas, while providing knowledge and analysis of international developments for the benefit of the Secretary and HHS as a whole. Priority areas include global health security, antimicrobial resistance, infectious disease preparedness and response, multilateral and bilateral diplomacy and negotiations, international HIV/AIDS control through the President’s Emergency Plan for AIDS Relief (PEPFAR), health aspects of trade interests, polio eradication, increasing access to safe and effective medicines, and reducing barriers to care. HHS has a range of relationships with other USG departments as well as more than 190 national Ministries of Health. Multilateral partners include the World Health Organization (WHO); the Pan American Health Organization (PAHO) and other regional offices of the WHO; the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund); the UN Joint Program on HIV/AIDS (UNAIDS); the Organization for Economic Cooperation and Development (OECD); and the GAVI Alliance. Significant accomplishments include:
Led the Secretary’s effort to strengthen HHS’s and the USG’s critical strategic commitments to global health security and the Global Health Security Agenda, HHS work overseas, and strengthening the WHO.
Provided leadership on interagency team to identify and overcome obstacles within China to facilitate the sharing of Influenza H7N9 samples with National Influenza Collaborating Centers to support the US decision to produce an updated H7N9 vaccine.
Represented HHS equities in trade negotiations, served as a lead technical resource for the USG on all health‐related trade issues, including bilateral trade issues, and represented the government in multilateral negotiations and meetings related to health and trade.
Led government efforts in multilateral negotiations at WHO, PAHO, the Global Fund, and UNAIDS convenings, advancing many US global health priorities, and ensuring the world is better prepared

Page 48
to prevent, detect, and respond to, global infectious disease threats, protecting the people of the US and the world, and protecting and strengthening global health security.
Represented HHS at high‐level diplomatic forums globally, including bilateral health dialogues, government missions to address urgent global health issues (e.g., Zika, MERS, and Ebola)
Led USG engagement on health in the Group of Seven and Group of Twenty, Arctic Council, and OECD.
Collaborated with CDC, ASPR and other partners to advance Zika collaborations on the U.S. – Mexico border through binational case investigations, expansion of mosquito surveillance, and communications protocols.
Funding History
Fiscal Year Amount
FY 2014 $6,270,000
FY 2015 $6,270,000
FY 2016 $6,026,000
FY 2017 $6,026,000
FY 2018 Annualized CR $5,985,000
Budget Request The FY 2019 President’s Budget request for the Office of Global Affairs (OGA) is $6,026,000; an increase of $41,000 over the FY 2018 annualized CR level of $5,985,000. At this level, OGA will continue efforts to ensure the health and well‐being of Americans, and to improve health and safety across the globe, through leadership and collaboration with multilateral organizations including the World Health Organization, the Group of Seven (G7) and Group of Twenty (G20), the Food and Agriculture Organization, and the Organization for Animal Health, among others, and through efforts to coordinate government policy and programs for HHS through political and diplomatic channels. OGA will continue to coordinate and facilitate the involvement of OPDIVs and STAFFDIVs with these entities. OGA will maintain a leadership role on Global Health Security Agenda coordination for the US Government, and focus efforts on political, diplomatic, and coordination issues. OGA will champion efforts to prevent, detect, and control illness and death related to infections caused by antibiotic‐resistant bacteria. It will coordinate with government and international partners to implement measures to mitigate the emergence and spread of antibiotic resistance and ensure the continued availability of therapeutics for the treatment of bacterial infections. OGA will lead the Department’s negotiations on issues where trade and health intersect, ensuring that the Secretary’s directives are carried out, and representing HHS equities in health and trade settings where these issues arise. In South Africa, Brazil, China, India, Switzerland, and Mexico, OGA health attachés will continue to represent HHS as they work with other government agencies, NGOs, and industry on research, regulation, information sharing, and multilateral issues – important to pandemic preparedness, safety of products, intellectual property and clinical trials, among many other objectives. OGA will continue its oversight of the Border Health Commission’s work, in partnership with Mexican counterparts, to identify critical health problems affecting states along the United States’ southern border with Mexico, and identify opportunities for collaboration to address these problems.
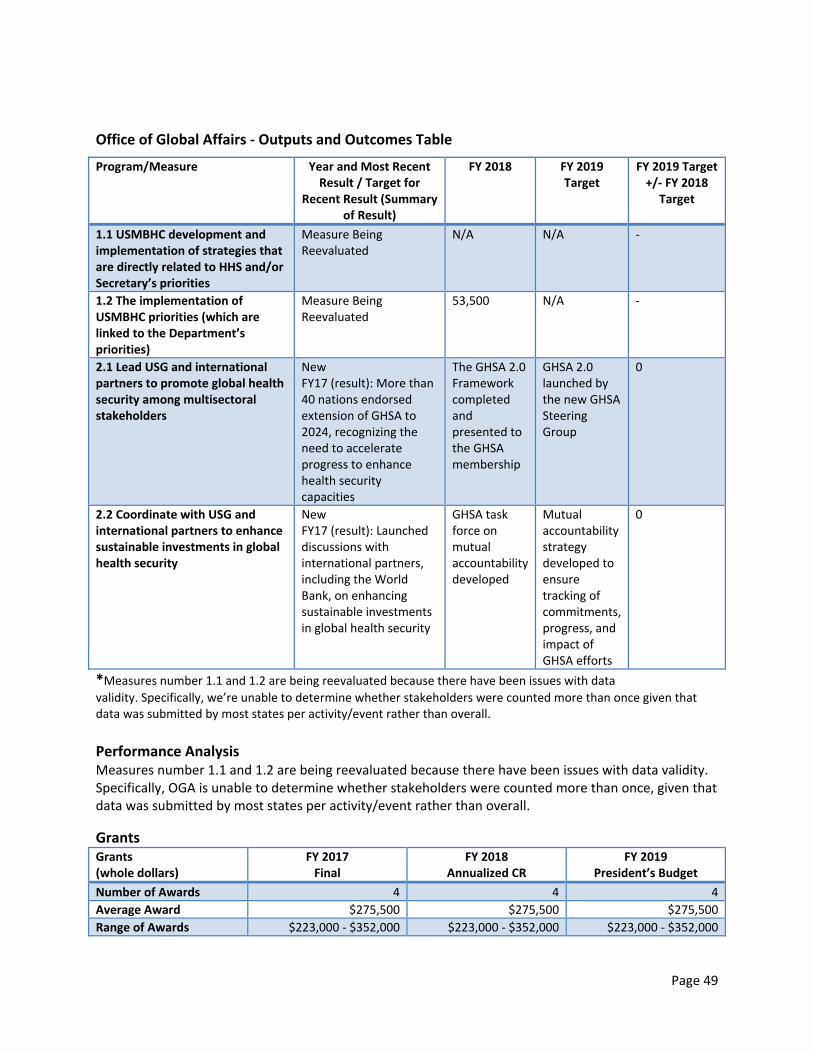
Page 49
Office of Global Affairs ‐ Outputs and Outcomes Table
Program/Measure Year and Most Recent Result / Target for
Recent Result (Summary of Result)
FY 2018
FY 2019 Target
FY 2019 Target +/‐ FY 2018
Target
1.1 USMBHC development and implementation of strategies that are directly related to HHS and/or Secretary’s priorities
Measure Being Reevaluated
N/A N/A ‐
1.2 The implementation of USMBHC priorities (which are linked to the Department’s priorities)
Measure Being Reevaluated
53,500 N/A ‐
2.1 Lead USG and international partners to promote global health security among multisectoral stakeholders
New FY17 (result): More than 40 nations endorsed extension of GHSA to 2024, recognizing the need to accelerate progress to enhance health security capacities
The GHSA 2.0 Framework completed and presented to the GHSA membership
GHSA 2.0 launched by the new GHSA Steering Group
0
2.2 Coordinate with USG and international partners to enhance sustainable investments in global health security
New FY17 (result): Launched discussions with international partners, including the World Bank, on enhancing sustainable investments in global health security
GHSA task force on mutual accountability developed
Mutual accountability strategy developed to ensure tracking of commitments, progress, and impact of GHSA efforts
0
*Measures number 1.1 and 1.2 are being reevaluated because there have been issues with data
validity. Specifically, we’re unable to determine whether stakeholders were counted more than once given that data was submitted by most states per activity/event rather than overall.
Performance Analysis Measures number 1.1 and 1.2 are being reevaluated because there have been issues with data validity. Specifically, OGA is unable to determine whether stakeholders were counted more than once, given that data was submitted by most states per activity/event rather than overall.
Grants Grants (whole dollars)
FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
Number of Awards 4 4 4
Average Award $275,500 $275,500 $275,500
Range of Awards $223,000 ‐ $352,000 $223,000 ‐ $352,000 $223,000 ‐ $352,000

Page 50
OFFICE OF INTERGOVERNMENTAL AND EXTERNAL AFFAIRS Budget Summary (Dollars in Thousands)
Office of Intergovernmental and External Affairs
FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
FY 2019 +/‐ FY2018
Budget Authority 10,625 10,553 10,625 +72
FTE 68 68 68 ‐
Authorizing Legislation:………….………………………………………………..........…..………….………………………Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The Office of Intergovernmental and External Affairs (IEA) serves the Secretary as the primary link between the HHS and state, local, territorial and tribal governments and non‐governmental organizations. Its mission is to facilitate communication related to HHS initiatives with these stakeholders. IEA not only communicates HHS positions to the stakeholders, but brings information back to the Secretary for use in the HHS policymaking process. The IEA is composed of a headquarters team that works on policy matters within HHS Operating and Staff Divisions. In addition to the Headquarters team, IEA has ten regional offices which include the Secretary’s Regional Directors, Executive Officer, Outreach Specialist and Intergovernmental Affairs Specialists responsible for public affairs, business outreach and media activities. The Regional Directors (RDs) coordinate the HHS Regional Offices in planning, development, and implementation of HHS policy. The Office of Tribal Affairs, in IEA, coordinates and manages tribal and native policy issues, assists tribes in navigating through HHS programs and services, and coordinates the Secretary’s policy development for Tribes and national Native American organizations. IEA is actively involved in leading the educational outreach and stakeholder engagement on the Secretary priorities related to Opioids Abuse, Childhood Obesity, and Serious Mental Illness initiatives. IEA efforts significantly increased the awareness and understanding of states, local, tribal and territorial governments; organizations, groups, private institutions, academia, private sector and labor unions of the various healthcare related programs. These efforts have proven to be hugely successful in improving the communication, and ultimately the relationships with stakeholders across the country. IEA accomplished the following goals in supporting the Secretary as the Department’s Chief Policy Officer:
Formulated and executed Secretary's engagement with a broad spectrum of stakeholders
Provided strategy, expert technical advice, and guidance on implications of policy options
Reviewed and analyzed draft regulations, releases, and policy documents to ensure stakeholder views/concerns/are considered
Promoted HHS announcements and releases to stakeholders
Supported WH initiatives‐ State Days, Tribal Leaders, Opioid listening sessions
Helped execute on RFIs, Executive Orders, and Roll‐outs Instituted quarterly meeting of external intergovernmental partners (NGA, ASTHO, NACo, NCSL, NASAD, NLC) to share information on priorities
Instituted quarterly meetings of HHS colleagues with intergovernmental and external affairs responsibilities to share information and maximize effectiveness

Page 51
Instituted weekly workgroup consisting of CMS, ASFR, ASL and ASPA to coordinate on waivers
Kept senior management informed of trends, evolving issues, controversial, and highly sensitive issues and recommended solutions/responses
Partnership Center’s goals, strategy, personnel, website was redirected to reflect current Administration’s priorities
1. Supported the Secretary’s Initiatives in the following manner: Formulated & executed the Secretary's engagement on:
healthcare reform
3 clinical priorities (childhood obesity, serious mental illness and opioids) formulated corresponding workgroups
drug pricing regulatory reform
quarterly STAC, Indian Country travel issued RFI to removing barriers for religious and faith‐based organizations to participate in HHS programs
responded to public health emergency declarations for hurricanes and wildfires by proactive outreach to affected Governors, Mayors, State Legislators and County Commissioners
hosted 3 faith‐based/community focused webinars and a livestream event with subject matter experts and tools for addressing the opioid epidemic
2. Supported ReImagine
Regional participation‐ Management & Stewardship Team
HQ participation‐ Transformation Lead; Healthcare System Team Optimizing Regional Performance
Funding History
Fiscal Year Amount
FY 2014 $9,576,000
FY 2015 $10,625,000
FY 2016 $10,625,000
FY 2017 $10,625,000
FY 2018 Annualized CR $10,553,000
Budget Request The FY 2019 President’s Budget request for IEA of $10,625,000 is $72,000 over the FY 2018 Annualized CR level of $10,553,000. The increase will partially support pay and non‐pay inflationary costs, continue coordination of a wide range of outreach activities, and facilitate cross‐cutting initiatives. IEA will continue mission critical activities via personnel who are knowledgeable about the complexity and sensitivity of various HHS programs, including health insurance marketplace, consumer/population distinctions, governmental organizations and external organizations, to ensure successful communication and coordination of healthcare and human services policy issues and other priority initiatives of the Department, Secretary and the Administration. IEA will continue to utilize electronic avenues to reduce travel costs, improve communication, timeliness, and relationships with stakeholders across the country.

Page 52
CENTER FOR FAITH‐BASED AND NEIGHBORHOOD PARTNERSHIPS Budget Summary (Dollars in Thousands)
Center for Faith‐Based and Neighborhood Partnerships
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 1,299 1,290 1,326 +36
FTE 7 7 7 ‐
FY 2019 Authorization………….………………………………………………..........…..……………………………...……Title III of the PHS Act Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments: Established in 2001, the Center for Faith‐based and Neighborhood Partnerships (HHS Partnership Center) supports the efforts of faith and community organizations in addressing national public health and human services issues. Additionally, the HHS Partnership Center is committed to the clinical priorities of the Secretary and the Administration, and the Secretary’s priority of finding, exposing, and removing every barrier to full and active engagement of the faith‐based community in the work of HHS.
While not a grant‐making office, the HHS Partnership Center is positioned to advance the Secretary’s priorities in faith‐based and community organizations through outreach, education, capacity building, and aligning community health and human services assets.
In 2014, the HHS Partnership Center was realigned within the Office of Intergovernmental and External Affairs (IEA), and now receives executive leadership and management direction from IEA. The HHS Partnership Center supports faith and community engagement with the public health and human services priorities of the Secretary and HHS by:
Serving as an open door for faith and community‐based partners to connect with and learn about the priorities of the Secretary and HHS,
Building and strengthening relationships between diverse sector partners,
Aligning community‐based resources and existing efforts toward shared goals,
Leveraging subject matter expertise of the agency and developing educational opportunities for community‐level health leaders,
Building regional and national coalitions of external stakeholders that advance HHS priorities, and
Communicating key messages, resources, grant opportunities and awards relevant to faith and community partners.
Accomplishments in 2017 include:
1. Supported the Secretary as the Department’s Chief Policy Officer
Formulated and executed Secretary's engagement with a broad spectrum of stakeholders
Promoted HHS announcements and releases to stakeholders
Helped execute on RFIs, Executive Orders, and Roll‐outs Kept senior management informed of trends, evolving issues, controversial, and highly sensitive issues and recommended solutions/responses
Aligned Partnership Center’s goals, strategy, personnel, and website to reflect current Administration’s priorities

Page 53
2. Supported the Secretary’s Initiatives Formulated & executed the Secretary's engagement on:
o healthcare reform o 3 clinical priorities (childhood obesity, serious mental illness and opioids) engagement
with corresponding workgroups o removing barriers for religious and faith‐based organizations to participate in HHS
programs o responding to public health emergency declarations for hurricanes and wildfires by
proactive outreach to faith‐based and community organizations o hosting 4 faith‐based/community focused webinars and a livestream event with subject
matter experts and tools for addressing the opioid epidemic
Funding History
Fiscal Year Amount
FY 2014 $1,299,000
FY 2015 $1,299,000
FY 2016 $1,299,000
FY 2017 $1,299,000
FY 2018 Annualized CR $1,290,000
Budget Request The FY 2019 President’s Budget request for CFBNP is $1,326,000; an increase of $36,000 over the FY 2018 Annualized CR level of $1,290,000. The budget increase will continue support for CFBNP’s mission to effectively administer federal programs that promote the economic and social well‐being of families, children, individuals, and communities.
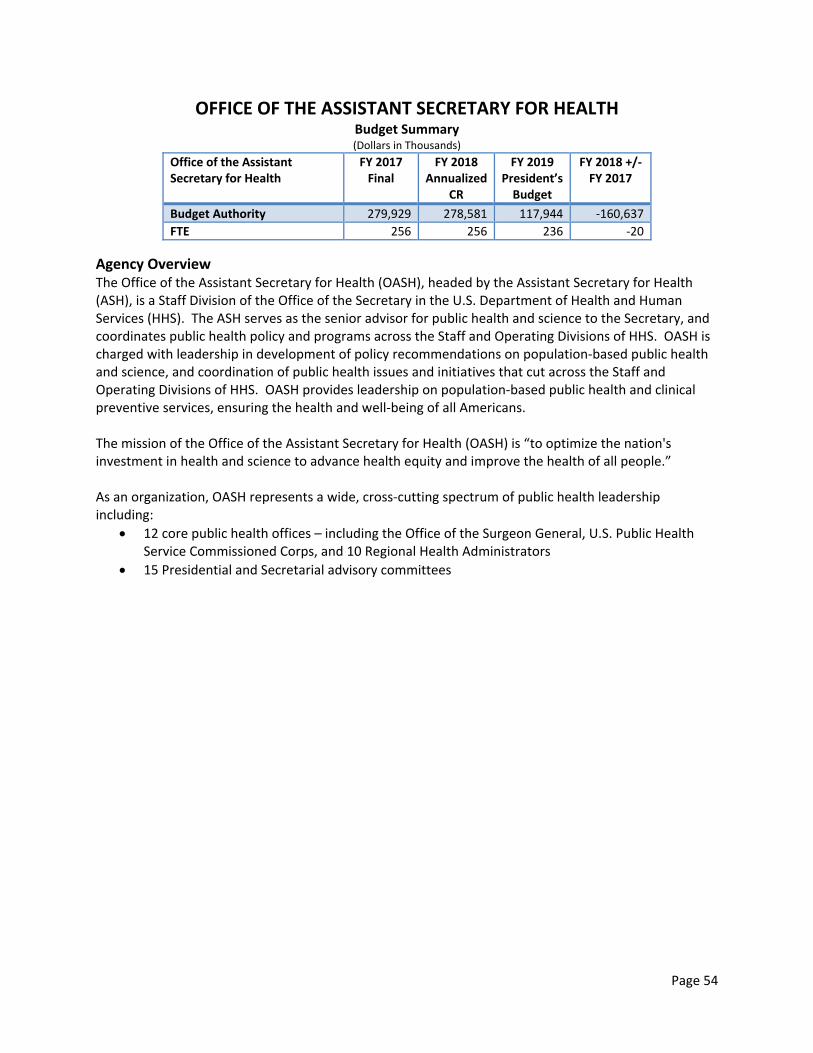
Page 54
OFFICE OF THE ASSISTANT SECRETARY FOR HEALTH Budget Summary (Dollars in Thousands)
Office of the Assistant Secretary for Health
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2018 +/‐ FY 2017
Budget Authority 279,929 278,581 117,944 ‐160,637
FTE 256 256 236 ‐20
Agency Overview The Office of the Assistant Secretary for Health (OASH), headed by the Assistant Secretary for Health (ASH), is a Staff Division of the Office of the Secretary in the U.S. Department of Health and Human Services (HHS). The ASH serves as the senior advisor for public health and science to the Secretary, and coordinates public health policy and programs across the Staff and Operating Divisions of HHS. OASH is charged with leadership in development of policy recommendations on population‐based public health and science, and coordination of public health issues and initiatives that cut across the Staff and Operating Divisions of HHS. OASH provides leadership on population‐based public health and clinical preventive services, ensuring the health and well‐being of all Americans. The mission of the Office of the Assistant Secretary for Health (OASH) is “to optimize the nation's investment in health and science to advance health equity and improve the health of all people.” As an organization, OASH represents a wide, cross‐cutting spectrum of public health leadership including:
12 core public health offices – including the Office of the Surgeon General, U.S. Public Health Service Commissioned Corps, and 10 Regional Health Administrators
15 Presidential and Secretarial advisory committees

Page 55
OASH SUMMARY TABLE ‐ DIRECT (Dollars in Thousands)
Office FY 2017 FTE
FY 2017 Final
FY 2018 FTE
FY 2018 Annualized
CR
FY 2019 FTE
FY 2019 President’s Budget
Immediate Office of the Assistant Secretary for Health 50 11,678 50 11,599 50 11,678
Office of HIV AIDS and Infectious Disease Policy 6 1,402 6 1,392 6 1,402
Office of Disease Prevention and Health Promotion 23 6,726 23 6,680 23 6,726
President’s Council on Fitness, Sports and Nutrition 6 1,168 6 1,160 6 1,168
Office for Human Research Protections 31 6,493 31 6,449 31 6,493
National Vaccine Program Office 17 6,400 17 6,357 17 6,400
Office of Adolescent Health 4 1,442 4 1,432 1 200
Public Health Reports 2 467 2 464 2 467
Teen Pregnancy Prevention 16 100,770 16 100,314 ‐ ‐
Office of Minority Health 57 56,541 57 56,285 57 53,956
Office on Women’s Health 43 32,067 43 31,922 43 28,454
Office of Research Integrity (Non‐Add) 28 8,558 28 8,558 28 8,558
HIV‐AIDS in Minority Communities 1 53,777 1 53,534 ‐ ‐
Embryo Adoption Awareness Campaign ‐ 998 ‐ 993 ‐ 1,000
Subtotal, GDM 256 279,929 256 278,581 236 117,944
‐ ‐ ‐ ‐ ‐ ‐
PHS Evaluation Set‐Aside ‐ ‐ ‐ ‐ ‐ ‐
OASH ‐ 4,285 ‐ 4,256 ‐ 4,285
Teen Pregnancy Prevention Initiative ‐ 6,800 ‐ 6,754 ‐ ‐
Subtotal, PHS Evaluations ‐ 11,085 ‐ 11,010 ‐ 4,285
‐ ‐ ‐ ‐ ‐ ‐
TOTAL OASH PROGRAM LEVEL 256 291,014 256 289,591 236 122,229

Page 56
IMMEDIATE OFFICE OF THE ASSISTANT SECRETARY FOR HEALTH Budget Summary
(Dollars in Thousands)
Immediate Office of the Assistant Secretary for Health
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 11,678 11,599 11,678 +79
FTE 50 50 50 ‐
Authorizing Legislation…………………………………………………………………………………………………………...Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………….……………………………….……………………..………..Direct Federal, contracts
Program Description and Accomplishments The Assistant Secretary for Health (ASH) and the Immediate Office of the Assistant Secretary for Health (OASH) serve in an advisory role to the Secretary on issues of public health and science. The Immediate Office of the ASH drives the OASH mission, “mobilizing leadership in science and prevention for a healthier Nation,” by providing leadership and coordination across the Department in public health and science, and advice and counsel to the Secretary and Administration on various priority initiatives such as the opioid epidemic and related behavioral health issues, immunization policy, autism, and emerging public health challenges related to infectious disease. OASH oversees 12 core public health offices — including the Office of the Surgeon General and the U.S. Public Health Service Commissioned Corps — as well as 10 regional health offices across the nation and 15 presidential and secretarial advisory committees. Senior public health officials within the Immediate Office work to ensure a public health and prevention perspective is addressed in Secretarial and Presidential priorities through effective networks, coalitions, working groups, and partnerships that identify public health concerns and undertake innovative projects. Three key priorities provide a framework for addressing public health needs:
Creating Better Systems of Prevention
Eliminating Health Disparities & Achieving Health Equity
Making Healthy People Come Alive for All Americans.
Creating Better Systems of Prevention Over the last 100 years, people in the US have gained another 30 years of life, with 25 of those years attributable to advances made in public health. The work of the Department and the public health system has expanded in that time, moving from basic public health initiatives to a focus on core functions of assessment, policy development, and assurances, as well as responding to challenges such as newly emerging infectious diseases, behavioral health, and non‐communicable diseases. OASH is addressing the enormous challenges presented by the opioid epidemic, which touches so many Americans, but especially those in rural and underserved populations. These challenges include opioid prescribing practices, increased rates of suicide and accidental opioid overdose, and persistent needs for comprehensive and science‐based pain treatment approaches. The first‐ever Surgeon General’s Report on Alcohol, Drugs, and Health was released in 2016 and reviews what is known about substance misuse and how to use that knowledge to address it and related challenges. Through its support, along with the

Page 57
Substance Abuse and Mental Health Services Administration (SAMHSA) on the Behavioral Health Coordinating Council, the work of the Surgeon General with health care providers, and coordination with OASH offices such as Women’s Health, Minority Health, and Office of HIV/AIDS and Infectious Disease Policy, this epidemic remains a priority issue for OASH and the entire Department. In addition, the Surgeon General (SG) provides Americans with practical scientific information on how to improve their health and reduce the risk of illness and injury. Recent priorities of the SG include activities around healthy aging, mental and emotional well‐being, and healthy eating. Eliminating Health Disparities and Achieving Health Equity The Immediate Office of the ASH provides leadership in the area of health equity by raising awareness and improving the health care and health system experience for populations disproportionally affected by health disparities. The Empowered Communities for a Healthier Nation Initiative supports the Secretary’s priority on addressing serious mental illness. Additionally, OASH relies on research and evaluation outcomes to further policy in adolescent health, addressing care and prevention across the life span, and using health information technology to reduce health disparities. Making Healthy People Come Alive for All Americans Healthy People 2020 established health goals for the nation, tracks progress toward meeting targets, and aligns national efforts to guide action for public health. In addition to continuing support for Healthy People 2020, OASH continues the Leading Health Indicators (LHI) initiative which identifies critical health priorities for the Nation. The LHI initiative also serves as an effective policy framework for policymakers and public health professionals at the local, state, and national level for tracking progress toward meeting key national health goals. LHIs assist in focusing efforts to reduce some of the leading causes of preventable deaths and major illnesses. OASH also has ten regional offices, led by Regional Health Administrators (RHAs). The RHAs serve as the lead federal official for public health and science in each region. Using their regional expertise and networks, RHAs catalyze public health action to impact leading health indicators by serving as extensions and spokespersons for OASH, as well as fostering coordination and collaboration around HHS priorities across Federal departments. The RHAs ensure that the priorities of the Department and OASH are better incorporated at the local, state, and national level.
Funding History
Fiscal Year Amount
FY 2014 $12,151,000
FY 2015 $11,678,000
FY 2016 $11,678,000
FY 2017 $11,678,000
FY 2018 Annualized CR $11,599,000
Budget Request The FY 2019 President’s Budget request for the Immediate Office of the Assistant Secretary for Health is $11,678,000; an increase of $79,000 over the FY 2018 Annualized CR level of $11,599,000. The increase will partially support pay and non‐pay inflationary increases. The FY 2019 request will maintain OASH’s baseline leadership in the Immediate Office of the ASH, the Office of the Surgeon General, and the

Page 58
regions. The Immediate Office line item will support Administration and Department initiatives, including reducing childhood obesity, addressing the Nation’s opioid epidemic and the misuse of pain medication, and re‐imagining OASH efforts.
U.S. Public Health Service Commissioned Corps The United States Public Health Service Commissioned Corps (Corps), which consists of over 6,500 uniformed public health professionals who work alongside their equivalent civilian counterparts performing the same day jobs but often receiving higher total compensation. The Commissioned Corps receives military‐like benefits, but has not been incorporated into the Armed Forces since 1952 and generally does not meet DOD’s criteria for the military compensation system. Further, the Corps’ mission assignments and functions have not evolved in step with the public health needs of the Nation. It is time for that to change. HHS is committed to providing the best public health services and emergency response at the lowest cost, and is undertaking a comprehensive look at how the Commissioned Corps is structured. The specific recommendations and plans resulting from this analysis will be released in the months to come, and could range from phasing out unnecessary Corps functions to reinventing the Corps into a smaller, more targeted cadre focused on providing the most vital public health services and emergency response. The goal of this proposal is to modernize how the Government employs public health professionals and how HHS responds to public health emergencies, saving Federal funds and reducing duplication while safeguarding the well‐being of the Nation.

Page 59
Immediate Office ‐ Outputs and Outcomes Table Long Term Objective: Creating Better Systems of Prevention Performance measures reflect previous administration priorities and will be updated for FY 2019 in the fall.
Program/Measure Year and Most Recent Result / Target for Recent Result / (Summary
of Result)
FY 2018 Target
FY 2019 Target
FY 2019 Target +/‐ FY 2018
Target
1.a: Shape policy at the local, State, national and international levels (Outcome) Measure 1: The number of communities, state and local agencies, Federal entities, NGOs or international organizations that adopt (or incorporate into programs) policies and recommendations generated or promoted by OASH through reports, committees, etc.
FY 2015: 881 Target: 312 (Target Exceeded)
530 530 ‐‐
1.b: Communicate strategically (Outcome)
Measure 1: The number of visitors to Websites and inquiries to clearinghouses;
Measure 2: Number of regional/national workshops/conferences, community based events, consultations with professional and institutional associations; Measure 3: new, targeted educational materials/campaigns; Measure 4: media coverage of OASH‐supported prevention efforts (including public affairs events).
FY 2015: 46,339,946 Target: 24,770,771 (Target Exceeded)
27,400,000 27,400,000 ‐‐
1.c: Promote effective partnerships (Outcome) Measure 1: Number of formal IAAs, MOUs, contracts, cooperative agreements, and community implementation grants with governmental and non‐governmental organizations that lead to prevention‐oriented changes in their agendas/efforts.
FY 2015: 759 Target: 355 (Target Exceeded)
330 330 ‐‐

Page 60
Program/Measure Year and Most Recent Result / Target for Recent Result / (Summary
of Result)
FY 2018 Target
FY 2019 Target
FY 2019 Target +/‐ FY 2018
Target
1.d: Strengthen the science base (Outcome) Measure 1: Number of peer‐reviewed texts (articles, reports, etc.) published by govt. or externally; Measure 2: number of research, demonstration, or evaluation studies completed and findings disseminated; Measure 3: the number of promising practices identified by research, demonstrations, evaluation, or other studies.
FY 2015: 221 Target: 68 (Target Exceeded)
80 80 ‐‐
1.e: Lead and coordinate key initiatives within and on behalf of the Department (Outcome) Measure 1: Number of prevention‐oriented initiatives/entities within HHS, across Federal agencies, and with private agencies, and with private organizations that are convened, chaired, or staffed by OASH; Measure 2: Number of outcomes from efforts in measure 1 that represent unique contributions, as measured by non‐duplicative programs, reports, services, events, etc.
FY 2015: 326 Target: 120 (Target Exceeded)
220 220 ‐‐
Long Term Objective: Eliminating Health Disparities and Achieving Health Equity
Program/Measure Most Recent Result
FY 2018 Target
FY 2019 Target
FY 2019 Target +/‐ FY 2018
Target
2.a: Shape policy at the local, State, national and international levels (Outcome) Measure 1: The number of communities, NGOs, state and local agencies, or Federal entities, that adopt (or incorporate into initiatives) policies and recommendations targeting health disparities that are generated or promoted by OASH through reports, committees, etc.
FY 2015: 444 Target: 152 (Target Exceeded)
300 300 ‐‐
2.b: Communicate strategically1 (Outcome) Measure 1: The number of visitors to Websites and inquiries to
FY 2015: 6,146,660 Target: 1,494,114 (Target Exceeded)
2,800,000 2,800,000 ‐‐

Page 61
clearinghouses; Measure 2: number of regional/national workshops/conferences or community based events; Measure 3: new, targeted educational materials/campaigns; Measure 4: media coverage of OASH‐supported disparities efforts (including public affairs events); and estimated number of broadcast media outlets airing Closing the Health Gap messages.
2.c: Promote Effective Partnerships (Outcome) Measure 1: Number of formal IAAs, MOUs, contracts, cooperative agreements and community implementation grants with governmental and non‐governmental organizations that lead to changes in their agendas/efforts to address health disparities.
FY 2015: 786 Target: 241 (Target Exceeded)
250 250 ‐‐
2.d: Strengthen the science base (Outcome) Measure 1: Number of peer‐reviewed texts (articles, reports, etc.) published by govt. or externally; Measure 2: number of research, demonstration, or evaluation studies completed and findings disseminated; Measure 3: number of promising practices identified in research, demonstration, evaluation, or other studies.
FY 2015: 188 Target: 39 (Target Exceeded)
50 50 ‐‐
2.e: Lead and coordinate key initiatives within and on behalf of the Department (Outcome) Measure 1: Number of prevention‐oriented initiatives/entities within HHS, across Federal agencies, and with private agencies, and with private organizations that are convened, chaired, or staffed by OASH; Measure 2: Number of outcomes from efforts in measure 1 that represent unique contributions, as measured by non‐duplicative programs, reports, services, events, etc.
FY 2015: 186 Target: 61 (Target Exceeded)
140 140 ‐‐

Page 62
Long Term Objective: Making Healthy People Come Alive for All Americans
Program/Measure Most Recent Result
FY 2018 Target
FY 2019 Target
FY 2019 Target +/‐ FY 2018
Target
3.a: Shape policy at the local, State, national and international levels (Outcome) Measure 1: The number of communities, NGOs, state and local agencies, Federal entities, or research organization that adopt (or incorporate into programs) policies, laws, regulations and recommendations promoted or overseen by OASH.
FY 2015: 365 Target: 153 (Target Exceeded)
220 220 ‐‐
3.b: Communicate strategically (Outcome) Measure 1: The number of visitors to Websites and inquiries to clearinghouses; Measure 2: number of regional/national workshops/conferences, community based events, and consultations with professional and institutional associations; Measure 3: new, targeted educational materials/campaigns.
FY 2015: 7,661,388 Target: 3,550,397 (Target Exceeded)
3,500,000 3,500,000 ‐‐
3.c: Promote Effective Partnerships (Outcome) Measure 1: Number of formal IAAs, MOUs, contracts, cooperative agreements and community implementation grants with governmental and non‐governmental organizations that lead to changes in their agendas/efforts related to the public health or research infrastructure.
FY 2015: 239 Target: 91 (Target Exceeded)
100 100 ‐‐
3.d: Strengthen the science base (Outcome) Measure 1: Number of peer‐reviewed texts (articles, reports, etc.) published by govt. or externally; Measure 2: number of research, demonstration, or evaluation studies completed and findings disseminated; Measure 3: number of public health data enhancements (e.g. filling developmental objectives or select population cells; development of state and community data) attributable to OASH leadership.
FY 2015: 68 Target: 67 (Target Exceeded)
55 55 ‐‐
3.e: Lead and coordinate key initiatives within and on behalf of the Department
FY 2015:64,679 Target: 6,436
6,400 6,400 ‐‐
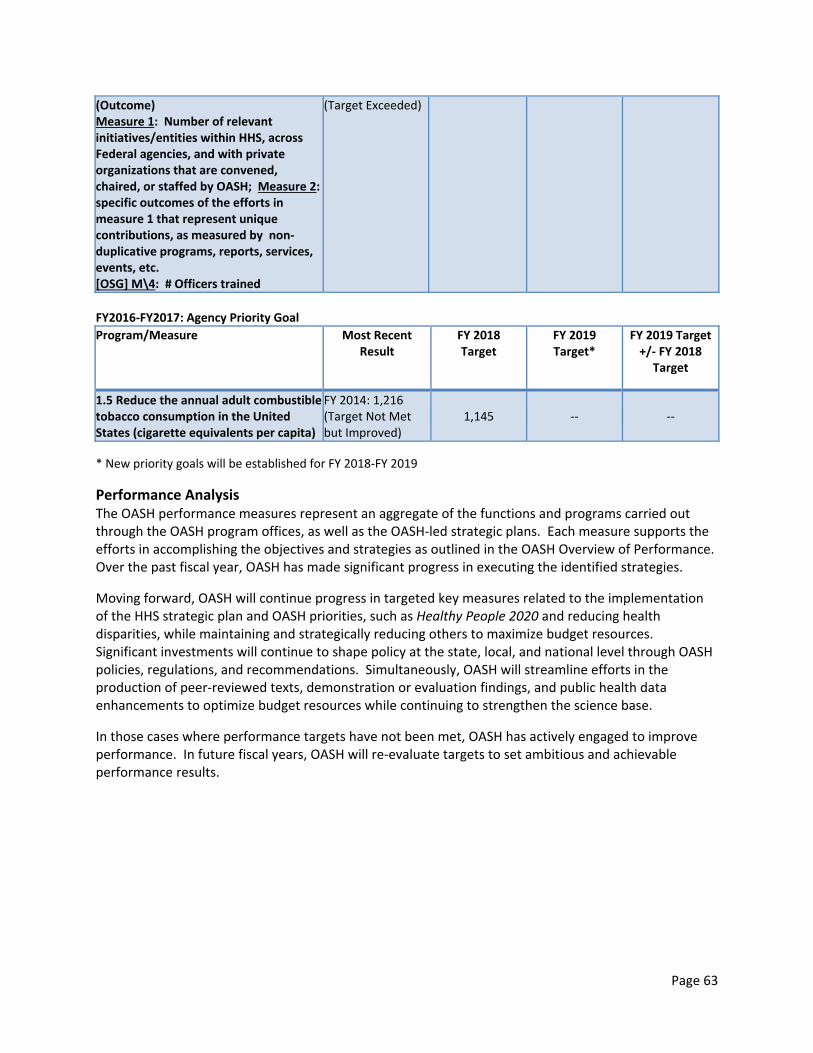
Page 63
(Outcome) Measure 1: Number of relevant initiatives/entities within HHS, across Federal agencies, and with private organizations that are convened, chaired, or staffed by OASH; Measure 2: specific outcomes of the efforts in measure 1 that represent unique contributions, as measured by non‐duplicative programs, reports, services, events, etc. [OSG] M\4: # Officers trained
(Target Exceeded)
FY2016‐FY2017: Agency Priority Goal
Program/Measure Most Recent Result
FY 2018 Target
FY 2019 Target*
FY 2019 Target +/‐ FY 2018
Target
1.5 Reduce the annual adult combustible tobacco consumption in the United States (cigarette equivalents per capita)
FY 2014: 1,216 (Target Not Met but Improved)
1,145 ‐‐ ‐‐
* New priority goals will be established for FY 2018‐FY 2019
Performance Analysis The OASH performance measures represent an aggregate of the functions and programs carried out through the OASH program offices, as well as the OASH‐led strategic plans. Each measure supports the efforts in accomplishing the objectives and strategies as outlined in the OASH Overview of Performance. Over the past fiscal year, OASH has made significant progress in executing the identified strategies.
Moving forward, OASH will continue progress in targeted key measures related to the implementation of the HHS strategic plan and OASH priorities, such as Healthy People 2020 and reducing health disparities, while maintaining and strategically reducing others to maximize budget resources. Significant investments will continue to shape policy at the state, local, and national level through OASH policies, regulations, and recommendations. Simultaneously, OASH will streamline efforts in the production of peer‐reviewed texts, demonstration or evaluation findings, and public health data enhancements to optimize budget resources while continuing to strengthen the science base.
In those cases where performance targets have not been met, OASH has actively engaged to improve performance. In future fiscal years, OASH will re‐evaluate targets to set ambitious and achievable performance results.

Page 64
OFFICE OF HIV/AIDS AND INFECTIOUS DISEASE POLICY Budget Summary
(Dollars in Thousands)
Office of HIV/AIDS and Infectious Disease Policy
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 1,402 1,392 1,402 +10
FTE 6 6 6 ‐
Authorizing Legislation…………………………………………………………………………………………………………...Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…..………………………………………………………….……………………………….…..………..Direct Federal, Contracts
Program Description and Accomplishments The Office of HIV/AIDS and Infectious Disease Policy (OHAIDP) is responsible for coordinating, integrating, and directing the HHS policies, programs, and activities related to infectious diseases of public health significance as delegated by the Secretary to the Assistant Secretary for Health (ASH). Currently the portfolio includes projects focused on HIV/AIDS, viral hepatitis, blood and tissue safety and availability (which are affected by infectious diseases), and tick‐borne diseases. OHAIDP supports these subject areas by undertaking department‐wide planning, internal assessments, and policy evaluations which identify opportunities to maximize collaboration, eliminate redundancy, and enhance resource alignment to address strategic priorities. OHAIDP develops and shares policy information and analyses with HHS OPDIVs and STAFFDIVs, and ensures that senior Department officials are fully briefed on ongoing and emerging issues pertaining to HIV/AIDS, viral hepatitis, and blood and tissue safety and availability. OHAIDP is in close communication with other federal and non‐federal stakeholders, community leaders, service providers, and other experts. OHAIDP maintains a high level of transparency by disseminating information about federal domestic programs, resources, and policies pertaining to HIV/AIDS and viral hepatitis on HIV.gov. OHAIDP manages three federal advisory committees:
Advisory Committee on Blood and Tissue Safety and Availability (ACBTSA) – provides advice and recommendations directly to the Secretary on issues pertaining to blood and tissue safety and availability as well as infectious disease concerns related to organ transplantation.
Presidential Advisory Council on HIV/AIDS (PACHA) – provides advice, information, and recommendations to the Secretary regarding programs, policies, and research to promote effective treatment, prevention and cure of HIV disease and AIDS, including considering common co‐morbidities of those infected with HIV. Throughout FY 2018, PACHA will continue to discuss critical issues such as HIV and the opioid epidemic, HIV incidence, HIV/AIDS research, and health outcomes and disparities.
Tick‐Borne Disease Working Group – provides advice and recommendations directly to the Secretary on how to improve the federal response to addressing tick‐borne diseases; coordinates among federal agencies, researchers, health care providers, and patient organizations to identify gaps in federal activities and research priorities; and helps ensure interagency coordination and minimize overlap (new in FY 2017).
HIV/AIDS Following the release of the National HIV/AIDS Strategy (NHAS) in 2010 and the updated NHAS in 2015, OHAIDP was delegated the responsibility for coordinating the response to NHAS across HHS and other federal departments. Up until January 2017, OHAIDP co‐chaired the federal interagency workgroup

Page 65
with the Director of the Office of the National AIDS Policy (ONAP). Since then, OHAIDP has been leading the efforts on the federal interagency workgroup (FIW). These efforts have focused on implementing and expanding efficient and effective efforts across the federal government to prevent new HIV infections, improve the health of people living with HIV, and reduce HIV‐related disparities. Further, OHAIDP continued to support the monitoring and reporting of the NHAS by developing, in collaboration with the FIW, the 2017 NHAS Progress Report, which will be disseminated in early 2018. OHAIDP’s efforts to improve coordination of HIV/AIDS programs across HHS include hosting regular meetings of senior HIV/AIDS leadership to discuss HIV/AIDS‐related activities and policies; reviewing all HIV/AIDS funding opportunity announcements for consistency with the goals/strategies of the NHAS; and technical consultations on strategic issues related to NHAS implementation. Throughout FY 2017, OHAIDP led a cross‐HHS effort to review evidence on the prevention benefit of HIV treatment and viral suppression, and to ensure that the findings are communicated consistently and accurately. In addition, in FY 2017, OHAIDP continued its series of quarterly training webinars for federal staff and the public to increase their ability to share and implement best practices and scientific advances in HIV prevention, care, and treatment. In FY 2018, OHAIDP plans to engage the Regional Resource Coordinators to adapt and implement the HIV pre‐exposure prophylaxis (PrEP) Framework across the HHS Regions as a resource to aid in scaling up PrEP. OHAIDP also plans to host, in collaboration with federal and non‐federal stakeholders, a workshop on improving outcomes along the HIV care continuum across the lifespan. AIDS.gov, the federal government’s leading source of information about HIV prevention and care and information on federal HIV policies, programs, and resources, was visited by more than 6 million users in 2016. In June 2017, AIDS.gov was rebranded to HIV.gov to reflect the advances in medical science and treatment of HIV, and to further improve the user experience through easier navigation to related content, enhanced search functionality, and ability to share specific pieces of content. In 2017, HIV.gov increased its use of Facebook Live to broadcast messages from senior leaders at key HIV‐related conferences. HIV.gov conducted 15 Facebook Live broadcasts, reaching about 50,000 confirmed users. Facebook Live is more cost efficient than producing video and allows for a greater reach to audiences who are unable to attend conferences in person. For World AIDS Day 2017, HIV.gov worked with the youth‐focused social media channel Snapchat to create a featured Snapchat story in observance of World AIDS Day and to encourage increased HIV testing by using the HIV.gov HIV Testing Sites and Care Services Locator, an interagency tool that compiles information from several HHS agencies and federal departments. Visits to the Locator increased by 600% on World AIDS Day – the highest single day usage in the Locator’s 9‐year history. According to metrics provided by Snapchat, OHAIDP reached between 1 to 2 million Snapchat users who opened the story, and that it was one of the most popular news stories of the year for Snapchat. OHAIDP enhanced its digital assistance efforts with new in‐depth and comprehensive blog posts on HIV.gov to align with the President’s May 2017 Executive Order on Technology. OHAIDP is responsible for overseeing and monitoring activities supported by the Secretary’s Minority AIDS Initiative Fund (SMAIF). In FY 2017, OHAIDP supported 30 projects that promote innovation, collaboration, and systems transformation across HHS to strengthen HIV prevention, care, and treatment among racial and ethnic minorities. Key FY 2017 projects included:

Page 66
THRIVE, a four year collaboration between OHAIDP and CDC, invested approximately $50 million to support innovative comprehensive models of HIV prevention and care for men who have sex with men (MSM) of color.
A molecular surveillance and data‐to‐care project for Hispanic/Latino MSM to envelop those networks in a combination of high‐impact public health prevention efforts such as the use of PrEP.
HIV.gov (formerly AIDS.gov), the federal government’s leading source of information about HIV prevention and care, is visited by more than 865,000 visitors each month. In the spring of FY 2017, AIDS.gov launched a major redesign and rebrand to HIV.gov to further improve users’ experiences, to optimize for a mobile environment, and to provide an even greater focus on racial and ethnic minorities and other populations at greatest risk for HIV.
A network of regional health advisors working in ten public health service regions to promote HIV prevention and the continuum of care, access to comprehensive PrEP services for high‐risk racial and ethnic minorities, and the Viral Hepatitis Action Plan.
A three‐year project, which leverages existing community health workers to link and retain racial and ethnic minorities living with HIV to HIV medical care so that they can access antiretroviral treatment to improve health outcomes and reduce the risk of HIV transmission to others.
A three‐year demonstration project to diagnose and cure hepatitis C virus (HCV) infection in Ryan White clinics servicing large numbers of racial and ethnic minorities living with HIV.
In an effort to increase awareness of the impact of HIV and AIDS on women and girls, in FY 2017, OHAIDP conducted an internal quality review assessment of the content and messages on HIV.gov that are specific to women and girls. The updated content will include effective prevention and care strategies that best reflect the science, experiences, and needs, of women and girls. Further, OHAIDP has partnered with the Office on Women’s Health (OWH) to develop Positive Spin Women, a digital tool that uses the power of personal storytelling to raise awareness of the HIV care continuum and encourage women living with HIV to get into treatment and achieve the goal of viral suppression. Positive Spin‐Women will be released on HIV.gov in early 2018, and will be promoted extensively through all HIV.gov social media tools. Viral Hepatitis OHAIDP has the lead role in coordinating national efforts and informing policies to prevent, diagnose, and treat viral hepatitis in the United States. The office convenes the Viral Hepatitis Implementation Group, which is comprised of representatives from more than 20 federal agencies and offices spanning the Departments of Health and Human Services, Housing and Urban Development, Justice, and Veterans Affairs. OHAIDP efforts include:
Leading the Group in developing and implementing the National Viral Hepatitis Action Plan, 2017 – 2020, which details four ambitious goals supported by strategies and recommended actions that could put the U.S. on a path to elimination of viral hepatitis, as well as 17 indicators that will be used to track progress and improve transparency and accountability for achieving results. The Action Plan is a framework for strengthening the collective national response to hepatitis B and C.
Convening a Hepatitis C Medicaid Affinity Group in collaboration with federal partners (CDC, CMS, HRSA, OMH and SAMHSA) and state Medicaid programs (nine states, IN, KY, LA, MA, MD, NY, VT, WA, WI). This groups aims to increase the number and percentage of Medicaid patients diagnosed with hepatitis C that are successfully treated and cured by identifying state‐led

Page 67
solutions and sharing promising strategies from states to encourage continuous quality improvement among participating states.
Providing technical information about the Action Plan, progress, policies, programs, and consultation within and outside of HHS on viral hepatitis prevention and treatment.
Developing and managing the viral hepatitis website at hhs.gov/hepatitis and supporting complementary efforts of partners outside of the federal government, including states, counties, cities, and nonprofit organizations.
Blood and Tissue Policy OHAIDP provides internal coordination of policies, programs, and resources, related to blood, organs, and tissues, through the Blood Organ and Tissue Senior Executive Council (BOTSEC), a cross‐departmental council comprising representatives from CDC, FDA, NIH, CMS, HRSA, ASPR, and ASPE. OHAIDP actively participates in the Department’s preparedness and response activities addressing the safety and availability of blood and tissues during national emergencies.
In response to the emerging threat of Zika in 2016, OHAIDP continues to monitor issues related to vector‐borne diseases, and works to ensure that safe blood and tissue products remain available in the United States and its territories. Most blood collection centers are financially unstable. This creates an enterprise rise to the blood supply system. Financial instability could lead to shortages across wide swaths of the country – and could result in localized shortages and force cancellations of elective surgeries, and reduced ability to respond to disasters. OHAIDP is leading the stress test efforts with FDA and ASPR to address the crisis in the sustainability of the U.S. Blood System. OHAIDP is responsible for coordinating cross‐governmental efforts to collect vital policy information such as recovery, distribution, and utilization, of allograft tissue from deceased and living donors. Additionally, OHAIDP is coordinating development of an emergency disaster plan with the American Association of Tissue Banks Emergency Preparedness Task Force with input from key HHS OpDivs and StaffDivs and the American Burn Association. Tissue products provide needed wound coverage for patients with thermal and chemical burns. OHAIDP’s blood and tissue portfolio is funded through a joint funding agreement with multiple HHS agencies (CDC, FDA, HRSA, NIH and CMS). Tick‐Borne Disease In June 2017, OHAIDP created the Tick‐Borne Disease Working Group, required by the 21st Century Cures Act. OHAIDP established the charter, and recruited and recommended voting members for final selection by the acting ASH and the Secretary. Of the 14 voting members, seven are federal employees representing CDC, NIH, FDA, and OASH. The seven remaining seats are public members representing diverse stakeholders, including physicians and other health care providers, researchers, people living with tick‐borne disease, and their families. The first two meetings of the working group were held in December 2017. Work is underway for the group to begin preparation of the Report to Congress required by the Act.
Funding History Fiscal Year Amount
FY 2014 $1,459,000
FY 2015 $1,402,000
FY 2016 $1,402,000
FY 2017 $1,402,000
FY 2018 Annualized CR $1,392,000

Page 68
Budget Request The FY 2019 President’s Budget request for OHAIDP is $1,402,000, an increase of $10,000 above the FY 2018 Annualized CR level of $1,392,000. The increase will allow OHAIDP to continue operations for HIV, blood and tissue policy, viral hepatitis policy activities, and the PACHA.

Page 69
OFFICE OF DISEASE PREVENTION AND HEALTH PROMOTION
Budget Summary (Dollars in Thousands)
Office of Disease Prevention and Health Promotion
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 6,726 6,680 6,726 +46
FTE 23 23 23 ‐
Authorizing Legislation:………….………………………………………………..........…..…….…Title XVII, Section 1701 of the PHS Act FY 2019 Authorization……………….………………………………………..........…..………….………………….….……......………Expired Allocation Method……………………………………………….………………………Direct Federal, Contract, Cooperative Agreement
Program Description and Accomplishments The Office of Disease Prevention and Health Promotion (ODPHP) provides leadership for a healthier America by initiating, coordinating, and supporting, disease prevention, health promotion, and healthcare quality activities, programs, policies, and information through collaboration with HHS and other federal agencies. Healthy People ODPHP meets its Congressional mandate to establish health goals for the Nation by leading the development and implementation of Healthy People. Healthy People provides science‐based, ten‐year national objectives for improving the health of all Americans at all stages of life, underpins HHS priorities and strategic initiatives, and provides a framework for prevention and wellness programs for a diverse array of federal and non‐federal stakeholders. In addition, many state and local health departments draw on Healthy People to develop their own health plans. The fourth iteration of the Healthy People objectives was released in 2010, as Healthy People 2020. In FY 2017, ODPHP continued to improve and expand the reach of its award winning Healthy People 2020 website (http://www.HealthyPeople.gov), which makes Healthy People 2020 information widely available and easily accessible. ODPHP continued its collaboration with the National Center for Health Statistics (NCHS) and other partners in updating a user‐centered, web‐based resource that expands the usefulness of the objectives’ data. This innovative web tool gives users a platform from which to learn, collaborate, plan, and implement objectives. Partnering with NCHS and the HHS Office of Minority Health, ODPHP increased accessibility and uptake of a disparities tool that allows users to easily see where disparities exist among population groups, and target their resources accordingly. In FY 2017, ODPHP continued a series of monthly public webinar‐based progress reviews of the Healthy People 2020 objectives and Leading Health Indicators (a subset of objectives representing high‐priority health issues), which allowed the Office of the Assistant Secretary for Health, in collaboration with the NCHS, the federal agencies that manage specific objectives, and community‐based organizations, to demonstrate progress toward achieving the ten‐year targets and identify areas needing additional work. On average, more than 1,000 sites registered to attend each webinar. In FY 2017, ODPHP, in partnership with NCHS, released a mid‐course review of progress in achieving the Healthy People 2020 objectives. In FY 2017, ODPHP continued the development of the next decade’s nation health objectives with the convening of the Secretary’s Advisory Committee on National Health Promotion and Disease Prevention Objectives for 2030, which are expected to be released in 2020.

Page 70
Dietary Guidelines for Americans ODPHP coordinates, on behalf of HHS, the development, review, and promotion of the recommendations of the Dietary Guidelines for Americans (DGA) as required by Congress (P.L. 101‐445). Published jointly every five years by HHS and the Department of Agriculture (USDA), the DGA is the basis of federal nutrition policy, programs, standards, and education for the general public. It also serves as the basis of the nutrition and food safety objectives in the Healthy People 2020. The process to develop the ninth edition began in FY2017 with much of the costs borne by USDA, the administrative lead for this next edition. Congress mandated in the 2014 Agricultural Act that the next, and future editions, of the DGA expand to provide guidance for children from birth to 2 years and for women who are pregnant. ODPHP leads the Federal Data Consortium on Pregnancy and Birth to 24 Months that currently has three projects: two adding to the National Health and Nutrition Examination Survey and one on the human milk composition database. Physical Activity Guidelines for Americans ODPHP, in collaboration with the President’s Council on Fitness, Sports, and Nutrition, NIH and CDC, led the Department’s development and release, in 2008, of the first federal Physical Activity Guidelines for Americans (PAG), a set of evidence‐based recommendations for physical activity for individuals six years and older to improve health and reduce disease. The PAG served as the primary basis for physical activity recommendations of the 2010 and 2015 DGA, and the physical activity objectives in Healthy People 2020. In FY 2016, a Physical Activity Guidelines Advisory Committee (PAGAC) was established to provide the scientific basis for the development of the next iteration of the PAG. ODPHP convened five meetings of the PAGAC in FY 2016, FY 2017, and FY 2018. The PAGAC’s report of recommendations is expected in February 2018, with release of the 2018 PAG in the first quarter of FY2019. healthfinder.gov ODPHP fulfills its congressional mandate to provide reliable prevention and wellness information to the public primarily with healthfinder.gov. Since 1997, healthfinder.gov has been a key resource for finding the best governmental and non‐profit online health information. The healthfinder.gov website provides over 100 featured topics and tools that use everyday language and examples to explain how taking small steps to improve health can lead to big benefits. The website also includes the myhealthfinder tool, developed in a joint effort with Agency on Health Research Quality, to provide personalized recommendations for clinical preventive services. In FY 2017, healthfinder.gov continued to extend the reach of actionable prevention information by disseminating content via the website, Facebook and Twitter, email newsletters, widgets, e‐cards, content syndication, and an Application Programming Interface (API). In addition, healthfinder.gov partnered with the American Academy of Family Physicians to explore ways family physicians can help: (1) provide feedback regarding how healthfinder.gov can be used to improve the patient’s experience and (2) encourage the use of healthfinder.gov’s personalized tool, myhealthfinder, to increase the use of recommended clinical preventive services. An outcomes study to answer this question is in the planning stage. Health Literacy ODPHP continues to play a leadership role in improving health literacy. In FY 2016, the HHS Health Literacy Workgroup established measures with targets for its biennial Health Literacy Action Plan. In FY

Page 71
2017, each agency in the workgroup collected sample health communication products which they will evaluate, using one of two HHS‐developed health communication evaluation tools. The results will inform the Second Health Literacy Action Plan. In FY 2017, FDA replaced CDC as co‐lead, along with ODPHP, of the workgroup.
Funding History
Fiscal Year Amount
FY 2014 $6,999,000
FY 2015 $6,726,000
FY 2016 $6,726,000
FY 2017 $6,726,000
FY 2018 Annualized CR $6,680,000
Budget Request The FY 2019 President’s Budget request for ODPHP is $6,726,000 an increase of $46,000 above the FY 2018 Annualized CR level of $6,680,000. The request will allow ODPHP to continue support for disease prevention and health promotion activities through: Healthy People, Dietary Guidelines for Americans, Physical Activity Guidelines for Americans, health literacy, and healthfinder.gov. Healthy People The FY 2019 request will support the development of the next decade’s objectives, Healthy People 2030, drawing on the input from the Secretary’s Advisory Committee for Health Promotion and Disease Prevention Objectives for 2030 and public comment. The development of Healthy People 2030 will be guided also by Departmental priorities to ensure alignment with key initiatives and to leverage existing resources. Additionally, the FY 2019 request will maintain the healthypeople.gov interactive tools and resources to facilitate communities’ use of evidence‐based practices to help move the nation toward achievement of the Healthy People 2020 goals and objectives. These activities will be supported through an ongoing collaboration with NCHS, other HHS agencies, and other federal Departments that manage Healthy People, including the Departments of Agriculture and Education. Dietary Guidelines for Americans Funds in FY 2019 will provide support the 2020 Dietary Guidelines Advisory Committee in its review of the scientific literature and development of its report of recommendations for the next edition of the DGA. In addition, ODPHP will enhance its communication of the current (2015) DGAs to help ensure Americans have the information they need to maintain a healthful diet. Physical Activity Guidelines for Americans Funds in FY 2019 will be used for the release of the second edition of the Physical Activity Guidelines for Americans and an accompanying public information campaign with an icon and targeted messages for consumers. The campaign will leverage partnerships to raise awareness of and encourage consumers to meet the recommendations in the PAG. Healthfinder.gov and Health Literacy ODPHP will use FY 2019 funds to continue to implement its congressional mandate to provide health information to professionals and the public. ODPHP also will continue to improve its ability to translate

Page 72
evidence‐based health information into clear and actionable prevention guidance in English and in Spanish. Additionally, ODPHP will continue its outreach and partnership building around use of healthfinder.gov’s content syndication and API tools, making its content available to use for free.
ODPHP ‐ Outputs and Outcomes Table
Program/Measure Year and Most Recent Result / Target for Recent Result /
(Summary of Result)
FY 2018 Target FY 2019 Target FY 2019 Target +/‐ FY 2018 Target
I.b Visits to ODPHP‐supported websites (Output)
FY 2017:10.35 Million
Target: 7.28 Million (Target Exceeded)
7.28 Million 10.5 Million +3.22 Million
II.a Percentage of States that use the national disease prevention and health promotion objectives in their health planning process (Outcome)
FY 2017: 94% Target: 90% (Target Exceeded)
90% 94% 4%
Performance Analysis ODPHP has a congressional mandate to provide health information to professionals and the public alike. ODPHP continues to consolidate and move a substantial amount of program activities online, enhancing the value to the public and professionals. Healthy People, once a paper‐based initiative, is now essentially an online resource with multiple interactive tools for tracking and implementing national health objectives (HealthyPeople.gov). The Physical Activity Guidelines for Americans has established an online community for stakeholders. Outreach for the Dietary Guidelines for Americans is primarily web‐based as well. Healthfinder.gov, once a general health information portal, has been redesigned to provide prevention and wellness information. As the data reflect, ODPHP is increasing its reach and engagement with Americans and exceeding performance targets. As a result, the public and professionals have more evidence‐based tools, resources, and support for their prevention and wellness activities. ODPHP expects to continue to grow its online presence. The initiative will allow Americans to be more productive in their prevention and wellness activities by offering social media, interactive learning technologies, data visualization tools, content syndication of prevention and wellness information, and forums that have proven to increase public and professional engagement. It also allows ODPHP to continue developing user‐centered information and websites based on health literacy and plain language principles, extending the reach and impact to those who are not savvy users of health information or the internet. ODPHP will continue to offer online professional training, with free continuing education credit, to help participants explore the challenges, successes, and processes involved in creating and sustaining healthier people and communities. ODPHP expects State use of the national disease prevention and health promotion objectives to mirror the uptake seen with the previous decade’s objectives—Healthy People 2010. By the end of the last decade, 100% of states used Healthy People 2010 to inform their health planning processes.

Page 73
The FY 2019 request allows ODPHP to improve the resources provided to users of Healthy People 2020, provided primarily online via healthypeople.gov, and through other social media and electronic means. The online presence of Healthy People will provide real‐time access to the latest data for the more than 1,200 national health objectives, making demographic data collected via surveys and surveillance systems from across the Department and other agencies understandable and relevant to a larger number of users. It will also provide a relational database, integrating objectives with evidence‐based practices and demographic data, which will make implementation significantly more targeted and actionable.

Page 74
PRESIDENT’S COUNCIL ON FITNESS, SPORTS AND NUTRITION Budget Summary
(Dollars in Thousands)
President’s Council on Fitness, Sports and Nutrition
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 1,168 1,160 1,168 +8
FTE 6 6 6 ‐
Authorizing Legislation:………….………………………………………………..........…..………….………………………Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The President’s Council on Fitness, Sports and Nutrition (The Council) (PCFSN) was originally established as the President’s Council on Youth Fitness by President Eisenhower, under Executive Order 13545 in 1956. PCFSN’s mission is to engage, educate, and empower Americans of all ages, socio‐economic backgrounds and abilities to adopt a healthy lifestyle that includes regular physical activity and good nutrition. The Council is a federal advisory committee of up to 25 volunteer citizens who serve at the discretion of the President. PCFSN advises the President, through the Secretary of Health and Human Services (HHS), on programs, partnerships and initiatives that increase access to opportunities for all Americans to lead active, healthy lives. PCFSN coordinates programmatic and health communication activities in consultation with offices within HHS and across the Federal government, as well as the private and non‐profit sectors to educate the public about the health benefits associated with regular physical activity and healthy eating. PCFSN activities include:
I Can Do It, You Can Do It!
Presidential Active Lifestyle Award
Sport for All Initiative
Physical Activity Guidelines for Americans In FY 2017, PCFSN collaborated with the HHS Office on Women’s Health to increase opportunities for girls and women with disabilities to be active and eat healthy through I Can Do It, You Can Do It!. This collaboration will undertake a process and impact evaluation of I Can Do It, You Can Do It! to determine how the program influences girls and women with disabilities to engage in physical activity and healthy eating behaviors and knowledge. PCFSN also initiated a collaboration with the HHS Regional Health Administrators in FY 2017, to expand the program’s reach to every state in the nation by May 2018.
Funding History
Fiscal Year Amount
FY 2014 $1,215,000
FY 2015 $1,168,000
FY 2016 $1,168,000
FY 2017 $1,168,000
FY 2018 Annualized CR $1,160,000

Page 75
Budget Request The FY 2019 President’s Budget request for PCFSN of $1,168,000 is an increase of $8,000 over the FY 2018 Annualized CR level of $1,160,000. The FY 2019 request will enable PCFSN to continue promoting national programs and initiatives that serve all Americans. The FY 2019 request will also enable PCFSN to support the secretary’s priority on Childhood Obesity Prevention. Childhood Obesity Prevention Programs/Initiatives The FY 2019 request will support PCFSN’s efforts to reduce childhood obesity, in particular, through the enhancement and promotion of new and existing physical activity and nutrition programs, including: Presidential Youth Fitness Program (PYFP); I Can Do It, You Can Do It! (ICDI); the Sport for All Initiative; Presidential Active Lifestyle Award (PALA+); and Presidential Champions. In FY 2019, PCFSN will continue its efforts to educate, engage, and empower all Americans, especially youth in the school and community settings, to lead an active, healthy lifestyle. Below are some of the Council’s obesity prevention efforts underway:
I Can Do It, You Can Do It! (ICDI) is a health promotion program that partners with K‐12 schools and school districts, colleges and universities, and community‐based organizations to provide access and opportunities for children and adults with disabilities to be healthy and active.
Sport for All Initiative is PCFSN’s national engagement effort to educate all Americans on the social and health benefits associated with sport participation. This effort emphasizes the core theme, “sport for all, play for life” by: (1) encouraging people of all ages, genders, ability levels and backgrounds to participate in sports; (2) uplifting the benefits associated with sports participation; and (3) sharing strategies that can help increase access to sports for youth. In FY 2019, the focus of this initiative with be on youth participation in sports, especially in distressed communities. PCFSN will also increase its partnerships with federal and non‐federal stakeholders to develop educational tools and resources targeting youth athletes, parents/caregivers, coaches, educators, and other key audiences about important safety and injury prevention protocols and practices.
Presidential Active Lifestyle Award (PALA+) is an eight‐week physical activity and nutrition program for anyone age 6 and older who wants to establish healthy habits and earn Presidential recognition at the end of the program. Participation in PALA+ is one way to move toward the recommendations in HHS’s Physical Activity Guidelines for Americans and Dietary Guidelines for Americans.
Public Engagement Activities In FY 2019, PCFSN will continue to deploy Council members to events across the nation and utilize traditional and social media to amplify childhood obesity prevention efforts undertaken by the Council and across the Department. In addition, PCFSN will support local, state and regional efforts to create active, healthy communities. Physical Activity Guidelines for Americans PCFSN will continue to serve on the Federal Steering Committee with the Office of Disease Prevention and Health Promotion and the Centers for Disease Control and Prevention to support the development of the second edition of the Physical Activity Guidelines for Americans (PAG). There will also be a national public engagement campaign will include the development and execution of a communication strategy to promote the PAG, which will include the promotion of a physical activity icon to accompany the Guidelines report and collateral materials. PCFSN will encourage the wide‐spread adoption of the PAG when released in later 2018 through its various communication channels, and will leverage Council members as message multipliers to reach target audiences.

Page 76
PCFSN ‐ Outputs and Outcomes Table
Program/Measure FY 2017 Target FY 2018 Target FY 2019 Target FY 2019 Target +/‐ FY 2018 Target
1.1 Number of partners supporting I Can Do It, You Can Do It!
FY17: 131 Target: 140 (Target Not Met)
150 155 +5
1.2 Number of website visits to the PAG or PAG Midcourse Report including downloads of collateral material
FY17: 380,534 Target: 300,000 (Target Exceeded)
400,000 450,000 +50,000
1.3 Number of social media impressions promoting the PAG or PAG Midcourse Report (e.g., Twitter)
FY17: 1 million Target: 1 million (Target Met)*
1.1 million 1.3 million +200,000
Performance Analysis Measure 1.1 enables PCFSN to accurately capture its level of engagement in improving access and opportunities for children and adults with disability to be healthy and active through the ICDI program. ICDI is the only federal initiative that facilitates physical activity and sports participation, through public and private partnerships, for Americans with disabilities. The FY 2019 target represents an increase of 5 sites over the FY 2018 target of 150 sites nationwide. Measures 1.2 and 1.3 track the national engagement strategy to promote and ensure the widespread adoption of HHS’s Physical Activity Guidelines for Americans (PAG). The target increases to measures 1.2 and 1.3 represent the expectation that website visits and social media impressions will increase during the development of, and following the release of, the 2018 PAG.
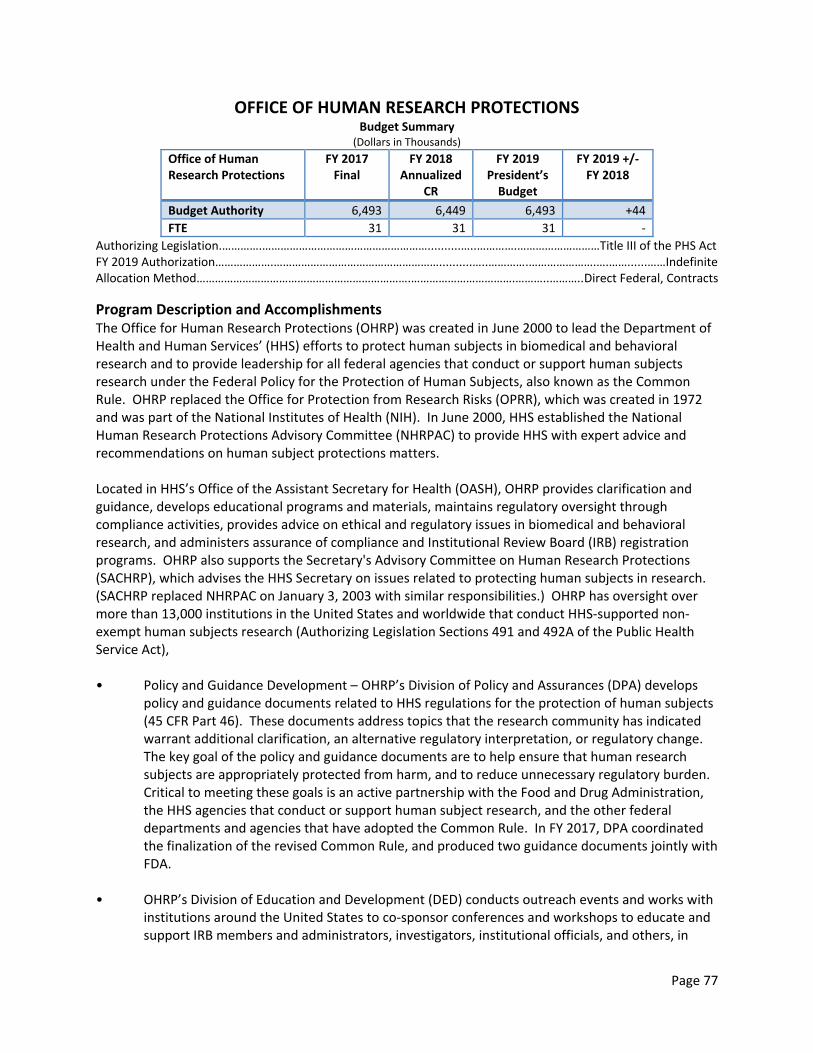
Page 77
OFFICE OF HUMAN RESEARCH PROTECTIONS Budget Summary
(Dollars in Thousands)
Office of Human Research Protections
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 6,493 6,449 6,493 +44
FTE 31 31 31 ‐
Authorizing Legislation.………….………………………………………………..........…..………….………………………Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….…………………………….………..………..Direct Federal, Contracts
Program Description and Accomplishments The Office for Human Research Protections (OHRP) was created in June 2000 to lead the Department of Health and Human Services’ (HHS) efforts to protect human subjects in biomedical and behavioral research and to provide leadership for all federal agencies that conduct or support human subjects research under the Federal Policy for the Protection of Human Subjects, also known as the Common Rule. OHRP replaced the Office for Protection from Research Risks (OPRR), which was created in 1972 and was part of the National Institutes of Health (NIH). In June 2000, HHS established the National Human Research Protections Advisory Committee (NHRPAC) to provide HHS with expert advice and recommendations on human subject protections matters. Located in HHS’s Office of the Assistant Secretary for Health (OASH), OHRP provides clarification and guidance, develops educational programs and materials, maintains regulatory oversight through compliance activities, provides advice on ethical and regulatory issues in biomedical and behavioral research, and administers assurance of compliance and Institutional Review Board (IRB) registration programs. OHRP also supports the Secretary's Advisory Committee on Human Research Protections (SACHRP), which advises the HHS Secretary on issues related to protecting human subjects in research. (SACHRP replaced NHRPAC on January 3, 2003 with similar responsibilities.) OHRP has oversight over more than 13,000 institutions in the United States and worldwide that conduct HHS‐supported non‐exempt human subjects research (Authorizing Legislation Sections 491 and 492A of the Public Health Service Act), • Policy and Guidance Development – OHRP’s Division of Policy and Assurances (DPA) develops
policy and guidance documents related to HHS regulations for the protection of human subjects (45 CFR Part 46). These documents address topics that the research community has indicated warrant additional clarification, an alternative regulatory interpretation, or regulatory change. The key goal of the policy and guidance documents are to help ensure that human research subjects are appropriately protected from harm, and to reduce unnecessary regulatory burden. Critical to meeting these goals is an active partnership with the Food and Drug Administration, the HHS agencies that conduct or support human subject research, and the other federal departments and agencies that have adopted the Common Rule. In FY 2017, DPA coordinated the finalization of the revised Common Rule, and produced two guidance documents jointly with FDA.
• OHRP’s Division of Education and Development (DED) conducts outreach events and works with institutions around the United States to co‐sponsor conferences and workshops to educate and support IRB members and administrators, investigators, institutional officials, and others, in

Page 78
their efforts to protect human subjects in research. The OHRP Research Community Forum (RCF) is the flagship DED education and outreach activity. RCFs are collaboratively planned events that typically have a one‐day workshop focused on applying the HHS regulations followed by a one‐day conference with keynote, plenary, and break‐out sessions around one or more themes related to research and human subjects protections. DED sponsors approximately three RCFs a year. DED also accepts between three to six institutional requests a year to support full or half‐day Educational Workshops. Furthermore, DED develops online educational materials including videos, webinars and infographics, for both the general public to educate them about research participation, and the research community to educate them about regulatory protections of human research subjects. In FY 2019, OHRP plans to sponsor up to three RCFs, co‐host six one‐day educational workshops, host one exploratory workshop, and speak at numerous events, successfully reaching as many as 6,800 participants in person. In addition, OHRP plans to conduct webcast presentations to various groups in the regulated community as needed. OHRP plans to post at least five new educational webinars and videos in FY 2019. So far in FY 2018, OHRP has conducted 3 OHRP‐sponsored full day educational workshops in University Park, IL, Memphis, TN, and Baltimore, MD; sent staff to speak at six different meetings, including the Fellowship Course on Comparative Effectiveness Research hosted by the Association of Health Care Journalists, and the annual conference of the Public Responsibility in Medicine and Research (PRIM&R), reaching as many as 3,000 attendees. OHRP’s public outreach website, About Research Participation, officially launched on January 9, 2017, and OHRP has added an educational video on Randomization and a set of infographics providing general information on how participants are protected in research. All materials were created in both English and Spanish. Since October 1, 2017, OHRP has posted 4 additional education videos for the research community on OHRP’s website.
• For‐Cause Compliance Evaluations – OHRP’s Division of Compliance Oversight (DCO) conducts inquiries and investigations into alleged noncompliance with HHS regulations for the protection of human subjects. These activities include conducting compliance inquiries, investigations, and preparing investigative reports, making determinations of noncompliance when appropriate, and requiring or recommending remedial or corrective action plans, as necessary.
• Not‐for‐Cause Compliance Site Visits ‐ DCO conducts a program of not‐for‐cause surveillance evaluations of institutions. These evaluations, when conducted on site by several OHRP staff and expert consultants, involve an extensive review of IRB records and resources, review of a sample of IRB‐approved protocols, and interviews with institutional officials, IRB administrators or human subject protections administrators, IRB members, IRB staff, and investigators. In FY 2017, DCO has opened one not‐for‐cause evaluation, and opened three investigations.
• Incident report review and follow‐up – DCO reviews incident reports submitted by institutions, and acknowledges or requests additional information from institutions, when needed. HHS regulations, at 45 CFR § 46.103(a) and (b)(5), require that institutions engaged in HHS‐conducted or ‐supported human subjects research have written procedures, to ensure that they promptly submit, to OHRP, reports on incidents related to unanticipated problems involving risks to subjects or others, any serious or continuing noncompliance with HHS regulations or IRB determinations, or any suspension or termination of an IRB approval. In 2017, DCO reviewed and processed 223 incident reports. So far in FY 2018, DCO has reviewed and processed 200 incident reports.

Page 79
• Secretary’s Advisory Committee on Human Research Protections (SACHRP) ‐ SACHRP consists of eleven members that provide expert advice and recommendations to the Secretary and the ASH on issues relating to the protection of human research subjects, with particular emphasis on special populations, such as neonates and children, prisoners and the decisionally impaired; pregnant women, embryos, and fetuses; individuals and populations in international studies; populations in which there are individually identifiable samples, data, or information; and investigator conflicts of interest. Examples of recent issues discussed include the expedited review list under the Revised Final Rule; and exemption §_.104(d)(4)(iii), the “HIPAA Exemption,” under the Revised Final Rule. To date SACHRP has approved ten sets of recommendations.
• Assurances of Compliance and Registering Institutional Review Boards – DPA administers the assurances of compliance with HHS protection of human subjects regulations and registrations of institutional review boards (IRB). These activities include processing more than 4,000 Federal‐wide Assurances (FWA) and more than 3,000 IRB registrations each fiscal year. In FY 2017, DPA processed 3,786 FWA approvals, and 3,286 IRB registrations. So far in FY 2018, DPA has processed 791 FWA approvals, and 732 IRB registrations.
• The HHS Strategic Plan highlights how HHS “works closely with…international partners to coordinate its efforts to ensure the maximum impact for the public.” To this end, OHRP maintains oversight responsibility for over 3,800 institutions located outside the United States which conduct HHS‐funded research. In support of this responsibility, OHRP publishes the International Compilation of Human Research Standards, coordinates a federal‐wide International Working Group, serves as a resource to other federal agencies and to researchers conducting research in other countries, provides technical advice on draft international documents, and hosts international delegations.
Key Priority ‐ In January 2017, HHS and 15 other Common Rule departments and agencies published a final revised Common Rule. The revised final rule becomes effective on July 19, 2018, represents the first major change to the human subjects protection system in over 20 years. OHRP will be developing new guidance and educational materials for the regulated community. OHRP supports the OASH/HHS strategic goals by contributing to the following measures: • Increase the number of local, state, and national health policies, programs, and services that
strengthen the public health infrastructure, and the number of policies in research institutions that improve the research enterprise.
• Increase the reach and impact of OASH communications related to strengthening the public health and research infrastructures.
• Increase the number of substantive commitments to strengthening the public health and research infrastructure on the part of governmental and non‐governmental organizations.
• Increase knowledge about the public health and research infrastructure, including research needs, and improve data collection needed to support public health decisions.

Page 80
Funding History Fiscal Year Amount
FY 2014 $6,756,000
FY 2015 $6,493,000
FY 2016 $6,493,000
FY 2017 $6,493,000
FY 2018 Annualized CR $6,449,000
Budget Request The FY 2019 request of $6,493,000 is $44,000 above the FY 2018 Annualized CR of $6,449,000. FY 2019 activities include:
Developing policies on the revised Common Rule, updating existing guidance and developing new guidance on the new regulations.
Sponsoring up to three OHRP‐sponsored Research Community Forums (a 2‐day event that incorporates a one day Educational Workshop and a 1‐day Conference) and one annual OHRP meeting; traveling support for staff to attend approximately 10 speaking invitations and OHRP co‐sponsored education activities, workshops and participation in other speaking invitations; support for program data analysis and reporting; development and maintenance of 508‐compliant online education and information resources including the development of transcripts for webinars and video recordings that are 508‐compliant and ready for online posting, recording and release of up to six 508‐compliant webinars online, video‐recording and release of up to six 508‐compliant lectures online, and the maintenance of a suitable webinar platform with a capacity for 1,000 participants together with service for live captioning, for conducting six or more educational webinars and update of the education webpages on the HHS/OHRP website.
Supporting the processing of more than 3,200 Institutional Review Board Registrations and approving over 3,700 Federal wide Assurances of Compliance.
Issuing up to two Guidance documents.
Opening four (one per quarter) Division of Compliance Oversight not‐for‐cause evaluations of institutions’ human subject protections programs, evaluating submitted complaints or allegations of noncompliance, and processing 600 to 800 incident reports from institutions, which include reports of any unanticipated problems involving risks to subjects or others, any serious or continuing noncompliance with the regulations or the requirements or determinations of the IRB, and any suspension or termination of IRB approval.
Supporting three SACHRP meetings and three to four joint meetings of SACHRP’s subcommittees.

Page 81
NATIONAL VACCINE PROGRAM OFFICE Budget Summary (Dollars in Thousands)
National Vaccine Program Office
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 6,400 6,357 6,400 +43
FTE 17 17 17 ‐
Authorizing Legislation:…………..………..…….……………………………………………....Title XXI of the Public Health Service Act FY 2019 Authorization………………….………….………………………………………………..........…..……………...……....…………..Expired Allocation Method………………….………………….…………………………………….……………………………….Direct Federal; Contracts
Program Description and Accomplishments In 1987, Congress created the National Vaccine Program Office (NVPO) to provide policy leadership and coordination on vaccine and immunization‐related activities among federal agencies and non‐federal stakeholders (state and local government, non‐governmental health groups, healthcare providers, health insurers, vaccine manufacturers and the public). This work is critical as it contributes to the control, and potential elimination, of vaccine‐preventable diseases, and improves the lives of many Americans – by reducing premature deaths, preventing illnesses, hospitalizations, and the long‐term consequences of these diseases, as well as curtailing lost work and school days in the United States and around the world – contributing to the nation’s productivity. One of NVPO’s core functions is to advance Departmental priorities on disease prevention – in this case by promoting health and wellness through immunization and optimization of the vaccine and immunization enterprise in the United States to accomplish that goal. NVPO leads the coordination of federal immunization activities to ensure they are carried out in an efficient and consistent manner, and also works with non‐federal stakeholders—domestic and international—to achieve the goals outlined in the 2010 National Vaccine Plan (NVP), that provides the framework—goals, objectives, and strategies—for pursuing the prevention of infectious diseases through immunizations. This includes federal government efforts towards vaccine research and development, vaccine safety, immunization coverage, supply, financing, education and communications, and global vaccine and immunization initiatives. NVPO also works with non‐federal partners to develop and implement strategies for achieving the highest reasonably possible level of prevention of vaccine‐preventable diseases. NVPO ensures coordination by taking a cross‐cutting view to identify and bridge research gaps in immunization activities through various projects. Manage National Vaccine Advisory Committee (NVAC) NVPO serves as Executive Secretariat for NVAC, which advises and makes vaccine‐related recommendations to the Assistant Secretary for Health (ASH), in his capacity as the Director of the National Vaccine Program. NVAC was established in 1987 to comply with Title XXI of the Public Health Service Act (P.L. 99‐660) (Section 2105). Specifically, the Committee was chartered with four main responsibilities:
1. Study and recommend ways to encourage the availability of an adequate supply of safe and effective vaccination products in the U.S.;
2. Recommend research priorities and other measures that should be taken to enhance the safety and efficacy of vaccines;

Page 82
3. Advise the Assistant Secretary for Health (ASH) on the implementation of the National Vaccine Program’s (NVP’s) responsibilities and the National Vaccine Plan, a coordinated, strategic framework established to achieve the vision of the NVP; and
4. Identify the most important areas of government and nongovernment cooperation that should be considered in implementing the NVP’s responsibilities and the National Vaccine Plan.
In the last year, NVPO convened two NVAC meetings, brought on a new Designated Federal Official (DFO), appointed 11 new voting members, and released one NVAC report. The report, published in the June 2017 issue of Public Health Reports, is called, Evaluation of the 2010 National Vaccine Plan Mid‐course Review: Recommendations from the National Vaccine Advisory Committee. This report provides the NVAC conclusions and recommendations to evaluate the progress on the goals of the National Vaccine Plan, and develop recommendations for consideration by the ASH. This NVAC review considers the findings of a parallel, separate mid‐course review of the status of the National Vaccine Plan commissioned by the National Vaccine Program Office (NVPO) in August 2015 that included a broad stakeholder engagement process. This report provides NVAC’s conclusions and recommendations, outlines their independent assessment of what would constitute near‐term success, and identifies indicators to use to measure success and monitor progress on the established target goals. Encouraging Adult Immunization Reducing vaccine‐preventable diseases in adults is a national health priority. Adult vaccination coverage rates remain low for most routinely recommended vaccines, and fall well below Healthy People 2020 targets. NVPO led the development of the National Adult Immunization Plan (NAIP), the nation’s first strategic plan focused on improving the use of vaccines by adults. The plan identifies four priority areas for program efforts and established baselines and targets for performance indicators to measure progress over time for each of these goals:
(1) Strengthen the Adult Immunization Infrastructure.
(2) Improve Access to Adult Vaccines.
(3) Increase Community Demand for Adult Immunizations.
(4) Foster Innovation in Adult Vaccine Development and Vaccination Related Technologies
In 2017, NVPO released a Path to Implementation for the NAIP, which focuses the efforts of federal and non‐federal partners in addressing the highest priority recommendations of the Plan. This plan operationalizes the NAIP and outlines discrete activities with measurable milestones to monitor progress on improving adult immunization. The plan also includes metrics and the priorities that will focus on areas with the greatest impact on improving adult immunization, such as improving the immunization information systems that are currently in use. Since 2012, NVPO has been co‐leading the NAIIS with CDC and the Immunization Action Coalition (IAC). This summit is dedicated to addressing and resolving adult and influenza immunization issues, and improving the use of vaccines recommended by CDC’s Advisory Committee on Immunization Practices. The NAIIS consists of over 700 partners, representing more than 130 public and private organizations. NVPO supports each of the NAIIS working groups, and leads the NAIIS quality and performance measure working group with the Indian Health Service and other non‐federal partners. In 2017, the group hosted a successful three‐day meeting, and planning is underway for a day‐long meeting in 2018.

Page 83
Spurring Vaccine Innovation Vaccine research and development, as well as the implementation of effective vaccine delivery programs, has led to the eradication and elimination of several once‐common serious infectious diseases. With further innovation and continued development, new and improved vaccines may have an even greater benefit to society. In the last year, NVPO has worked with partners to encourage vaccine innovation in the following ways:
21st Century Cures Act Report on Vaccine Innovation NVPO has led the interagency effort on behalf of the HHS Secretary, to coordinate the development of a congressional report on vaccine innovation and development, in compliance with the 21st Century Cures Act mandate. This report, Encouraging Vaccine Innovation: Promoting the Development of Vaccines that Minimize the Burden of Infectious Diseases in the 21st Century, examines U.S. vaccine development and innovation including the current landscape, existing challenges, and drivers and levers to incentivize development.
In December 2017, the report was delivered to Congress, and with the summary finding that the “U.S. vaccine enterprise is well established and has been successful at bringing innovative and new and improved vaccines to the market. However, the vaccine enterprise is at a turning point as challenges to innovation have increased for remaining infectious disease targets. Currently, HHS leads concerted and targeted efforts to address many of these challenges, spur continued innovation, and improve public health.”
SMART Vaccines Software Tool In an effort to support the prioritization of new vaccine targets, NVPO undertook the initiative to create the Strategic Multi‐Attribute Ranking Tool for vaccines (SMART Vaccines tool). As part of this effort, NVPO initiated and supported a multi‐phase study by the Institute of Medicine (IOM), now called the National Academies of Sciences, Engineering, and Medicine and the Fogarty International Center at NIH. The SMART Vaccines tool ranks vaccines in order of priority taking into consideration the most important attributes needed for a potential life‐saving preventive intervention. This decision‐support software tool is now publically available and can be downloaded for free; it had been previously only available in a testing phase. NVPO and NIH have recently focused on ensuring that the tool is adaptable and responsive for the intended decision‐making support, and to do so, advanced the project to an upgraded prototype for use in a real‐world setting this year with the Ugandan National Immunization Technical Advisory Group (UNITAG). This group was tasked by the Ugandan Ministry of Health to prioritize five vaccines to implement in country, and used the SMART Vaccines tool to organize the potential vaccines of interest into a prioritization list. The UNITAG pilot project served to initiate an important dialogue among members when deciding what attributes to consider in their decision making and provided an additional layer of transparency to the data used to arrive at the final ranking.

Page 84
Funding History
Fiscal Year Amount
FY 2014 $6,659,000
FY 2015 $6,400,000
FY 2016 $6,400,000
FY 2017 $6,400,000
FY 2018 Annualized CR $6,357,000
Budget Request The FY 2019 President’s Budget request for NVPO is $6,400,000; an increase of $43,000 above the FY 2018 Annualized CR level of $6,357,000. The FY 2019 budget request allows NVPO to continue to maximize the impact of vaccines on the health of the United States population, address gaps with a particular focus on high‐priority strategies, as identified in the 21st Century Cures Act Report on Vaccine Innovation, and meet the objectives of the HHS Strategic Plan to reduce the occurrence of infectious diseases, which include vaccine‐preventable diseases.
In FY 2019, NVPO’s planned activities include projects to improve uptake of flu vaccine, improve uptake of all ACIP recommended vaccinations in adults, increase coverage rates of HPV vaccination among adolescents and young adults, create opportunities to expand vaccine innovation efforts, and reduce racial and ethnic disparities in immunization coverage rates. The Budget does not include funding for new grants in the National Vaccine Program Office.

Page 85
OFFICE OF ADOLESCENT HEALTH Budget Summary
(Dollars in Thousands)
Office of Adolescent Health
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 1,442 1,432 200 ‐1,232
FTE 4 4 1 ‐3
Authorizing Legislation: ……………….…..…….………………………………………..Section 1708 of the Public Health Service Act FY 2019 Authorization……………………………...…………………………………….………………..........…..……………...……....……Expired Allocation Method…………………………,………………………………………………..Direct Federal, Competitive Grants, Contracts
Program Description and Accomplishments The Office of Adolescent Health (OAH) is dedicated to improving the health and well‐being of adolescents. OAH leads through promoting strength‐based approaches, bolstering multi‐sector engagement, and bringing in youth voices to support healthy development and transitions to productive adulthood. Authorized by the Public Health Service Act, OAH supports research, services, prevention and health promotion activities, training, education, partnership engagement, national planning, and information dissemination activities. OAH engages national partners from health care, public health, education, workforce development, community and out‐of‐school time programs, faith‐based groups, and the social services sector in efforts to put adolescent health firmly on the nation’s agenda, to prevent risky behavior and disease, and to promote health and healthy development. OAH’s Strategic Plan for FY 2016 – 2021 identifies strategies to improve adolescents’ health and well‐being, and continues work with professionals and communities serving young people. The strategic framework informs decisions to ensure talents and resources are aligned to achieve OAH’s mission. OAH administers the Pregnancy Assistance Fund (PAF) and the Teen Pregnancy Prevention Program (TPP). PAF is a grant program that funds states and Tribal entities to provide a seamless network of support services to expectant and parenting teens, women, fathers, and their families. TPP is a national, evidence‐based grant program that funds diverse organizations that work to prevent teen pregnancy across the nation. In 2015, OAH launched its call to action, Adolescent Health: Think, Act, Grow® (TAG), which provides a framework for youth‐serving professionals and organizations, families, and teens to promote the healthy and healthy development of young people. TAG provides free tools and resources – including the TAG Playbook, successful program strategies, research reviews, social media content, webinars, and videos featuring adolescent health experts – on the OAH website and through multiple communications and dissemination channels. OAH also leads the HHS Adolescent Health Work Group, which brings together representatives from across the Department to strategically plan across adolescent health and related programs, and participates in the federal Interagency Working Group on Youth Programs.

Page 86
Funding History
Fiscal Year Amount
FY 2014 $1,500,000
FY 2015 $1,442,000
FY 2016 $1,442,000
FY 2017 $1,442,000
FY 2018 Annualized CR $1,432,000
Budget Request The FY 2019 President’s Budget request for OAH of $200,000 is $1,232,000 below the FY 2018 Annualized CR level of $1,432,000. This level will support close out of OAH program office activities no longer needed to support the Teen Pregnancy Prevention Program.

Page 87
PUBLIC HEALTH REPORTS Budget Summary (Dollars in Thousands)
Public Health Reports FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 467 464 467 +3
FTE 2 2 2 ‐
Authorizing Legislation:….……….…………….................................................................................Title III of the PHS Act FY 2019 Authorization……………………………..……………………………………………….....................…..………………………Indefinite Allocation Method………………………………………………..……………………Direct Federal Contract; Cooperative Agreement
Program Description and Accomplishments Public Health Reports (PHR) is the official, peer‐reviewed scientific journal of the Office of the U.S. Surgeon General and U.S. Public Health Service. PHR is the only general public health journal in the federal government. It has been published since 1878, making it one of the oldest journals of public health in the U.S. The journal is published through an official agreement with the Associations of Schools and Programs of Public Health (ASPPH) and SAGE, one of the largest scholarly publishing houses in the world, through an agreement with ASPPH. PHR has been a key resource for those working in the field of public health. PHR is published bi‐monthly with a minimum of six regular print and online issues, plus three or four topic‐specific supplement issues annually. All are published electronically and in print, and are widely distributed through several scholarly channels. The entire set of PHR journal articles from 1878 has been digitized and is available at: http://www.ncbi.nlm.nih.gov/pmc/journals/333/. The journal’s impact factor has significantly increased in the last few years; its 2016 impact factor is 1.867. PHR offers articles in three main areas: public health practice, research, and viewpoints/commentaries. PHR’s mission is:
To facilitate the movement of science into public health practice and policy, to positively affect the health and wellness of the American public.
To publish scholarly manuscripts that describe new and innovative ways to deliver essential services, leading to improved quality, enhanced efficiency, and reduced costs.
To publish evaluations of public health programs that describe models of practice that can be replicated by others and that describe lessons learned.
The target audience for PHR is the broad public health community, including public health practitioners at the local, state, federal, and international levels, practice‐based academia, and policy makers at all levels of the government. Examples of topics PHR publishes on include addiction, tobacco control, infectious diseases, disease surveillance, teenage violence, occupational disease and injury, immunization, drug policy, lead screening, health disparities, and many other key and emerging public health issues. The types of articles published by PHR include original research, public health evaluation, case study/practice, brief report, reports and recommendations, systematic review, Surgeon General’s perspective, and HHS Executive perspective.
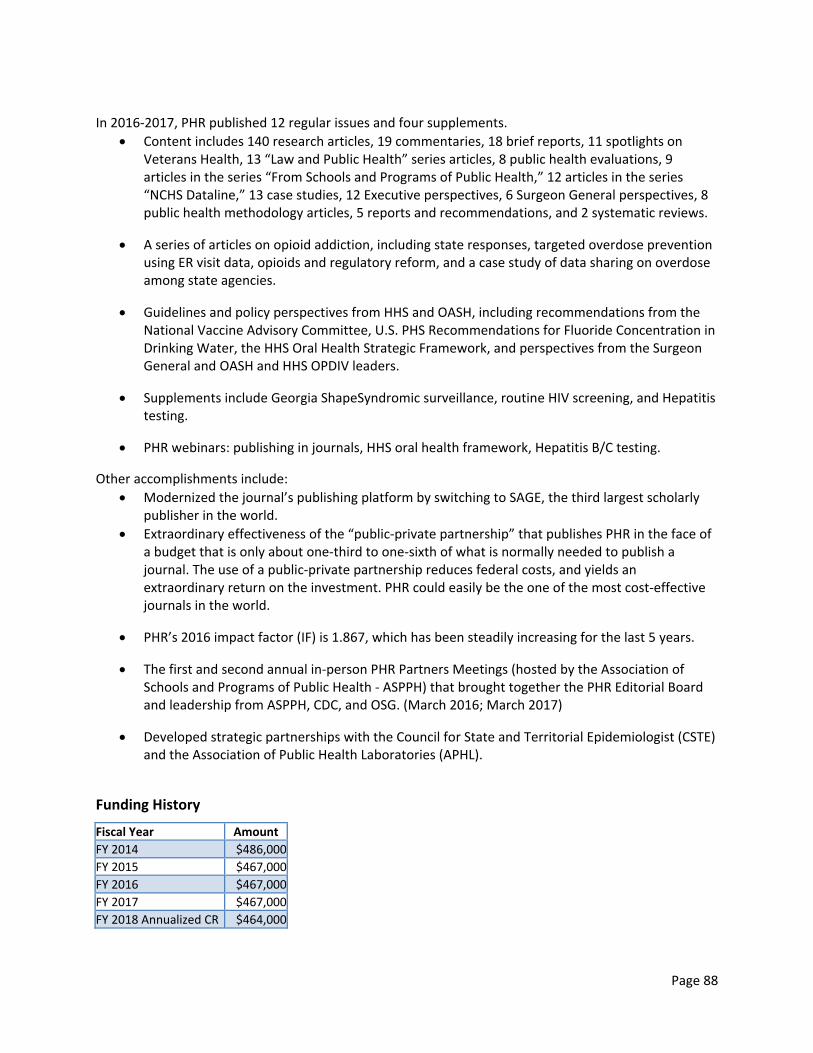
Page 88
In 2016‐2017, PHR published 12 regular issues and four supplements.
Content includes 140 research articles, 19 commentaries, 18 brief reports, 11 spotlights on Veterans Health, 13 “Law and Public Health” series articles, 8 public health evaluations, 9 articles in the series “From Schools and Programs of Public Health,” 12 articles in the series “NCHS Dataline,” 13 case studies, 12 Executive perspectives, 6 Surgeon General perspectives, 8 public health methodology articles, 5 reports and recommendations, and 2 systematic reviews.
A series of articles on opioid addiction, including state responses, targeted overdose prevention using ER visit data, opioids and regulatory reform, and a case study of data sharing on overdose among state agencies.
Guidelines and policy perspectives from HHS and OASH, including recommendations from the National Vaccine Advisory Committee, U.S. PHS Recommendations for Fluoride Concentration in Drinking Water, the HHS Oral Health Strategic Framework, and perspectives from the Surgeon General and OASH and HHS OPDIV leaders.
Supplements include Georgia ShapeSyndromic surveillance, routine HIV screening, and Hepatitis testing.
PHR webinars: publishing in journals, HHS oral health framework, Hepatitis B/C testing.
Other accomplishments include:
Modernized the journal’s publishing platform by switching to SAGE, the third largest scholarly publisher in the world.
Extraordinary effectiveness of the “public‐private partnership” that publishes PHR in the face of a budget that is only about one‐third to one‐sixth of what is normally needed to publish a journal. The use of a public‐private partnership reduces federal costs, and yields an extraordinary return on the investment. PHR could easily be the one of the most cost‐effective journals in the world.
PHR’s 2016 impact factor (IF) is 1.867, which has been steadily increasing for the last 5 years.
The first and second annual in‐person PHR Partners Meetings (hosted by the Association of Schools and Programs of Public Health ‐ ASPPH) that brought together the PHR Editorial Board and leadership from ASPPH, CDC, and OSG. (March 2016; March 2017)
Developed strategic partnerships with the Council for State and Territorial Epidemiologist (CSTE) and the Association of Public Health Laboratories (APHL).
Funding History
Fiscal Year Amount
FY 2014 $486,000
FY 2015 $467,000
FY 2016 $467,000
FY 2017 $467,000
FY 2018 Annualized CR $464,000
Page 89
Budget Request The FY 2019 President’s Budget request for Public Health Reports is $467,000, an increase of $3,000 over the FY 2018 Annualized CR level of $464,000.

Page 90
TEEN PREGNANCY PREVENTION Budget Summary
(Dollars in Thousands)
Teen Pregnancy Prevention
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 100,770 100,314 ‐ ‐100,314
FTE 16 16 ‐ ‐16
Authorizing Legislation: ………………………..………………Division H, Title II of the Consolidated Appropriations Act, 2016 FY 2019 Authorization……………….………………………….…………………………………..................................................Indefinite Allocation Method………………………………………………………………………….……………………..Direct federal, Contract, Grants
Program Description and Accomplishments The Teen Pregnancy Prevention (TPP) program is a discretionary grant program to support evidence‐based and innovative approaches to teen pregnancy prevention. It is administered by the Office of Adolescent Health (OAH) within the Office of the Assistant Secretary for Health. OAH leads coordination of program activities focused on adolescent health among the Department of Health and Human Services (HHS) offices and operating divisions. OAH provides ongoing training and technical assistance to its TPP grantees to ensure programming and evaluation.
Funding History
Fiscal Year Amount FY 2014 $100,762,000
FY 2015 $101,000,000
FY 2016 $101,000,000
FY 2017 $101,000,000
FY 2018 Annualized CR $100,314,000
Budget Request The FY 2019 President’s Budget request does not include funds for this program. Teenage pregnancy rates have declined precipitously over recent decades. The pregnancy rate for 15‐19 year‐olds has declined by nearly two thirds from its peak rate in 19901. This trend in declining pregnancy rates existed before the TPP program. TPP does not appear to have been a major driver in teenage pregnancy reductions. TPP serves less than one percent of teenagers in the United States.
1 Guttmacher Institute: National and State Trends by Age, Race and Ethnicity. September 2017. https://www.guttmacher.org/report/us-adolescent-pregnancy-trends-2013#figure1

Page 91
OFFICE OF MINORITY HEALTH Budget Summary
(Dollars in Thousands)
Office of Minority Health
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 56,541 56,285 53,956 ‐2,329
FTE 57 57 57 ‐
Authorizing Legislation………….………………………………………………...........…..…………Title XVII, Section 1707 of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….……………………………….…P.L. 111‐148 Allocation Method…………………………………….Direct federal, Competitive Grant and Cooperative Agreement, Contract
Program Description and Accomplishments The Office of Minority Health (OMH) was created in 1986, as one of the most significant outcomes of the 1985 Secretary’s Task Force Report on Black and Minority Health. OMH was subsequently established in statute by the Disadvantaged Minority Health Improvement Act of 1990 (PL 101‐527), re‐authorized under the Health Professions Education Partnerships Act of 1998 (PL 105‐392), and most recently re‐authorized under the Affordable Care Act of 2010 (PL 111‐148). OMH’s statutory authority requires that OMH work to improve the health of racial and ethnic minority groups including through coordination of the Department’s work in this area; supporting research, demonstrations and evaluations to test new and innovative models; increasing knowledge, information dissemination, education, prevention and service delivery to individuals from disadvantaged backgrounds; entering into contracts to increase access to primary health services providers for individuals who lack proficiency in English; and supporting a national minority health resource center.
OMH Mission and Vision
OMH’s mission is to improve the health of racial and ethnic minority populations through the development of policies and programs that help eliminate disparities.
OMH’s vision is to improve the health of racial and ethnic minority communities by focusing on prevention, putting people and communities at the center of its work, leadership that strengthens coordination and impact of HHS programs and actions of communities of stakeholders across the United States, and through partnerships with community‐ and faith‐based organizations.
OMH serves as the lead agency for coordinating efforts across the government to address and to eliminate health disparities. OMH convenes, and provides guidance to, HHS operating and staff divisions and other Federal departments, to identify health disparity and health equity policy and programmatic actions. This targeted leadership improves performance through better coordination on cross‐cutting initiatives, minimizes programmatic duplication, and leverages funds to reduce health disparities. OMH Strategic Priorities OMH focuses on translating core minority health and health disparity programs into strategic activities and policies at the federal, state, tribal, territorial, and local levels. OMH’s three strategic priorities are:
Lead implementation of the HHS Action Plan to Reduce Racial and Ethnic Health Disparities;
Coordinate the National Partnership for Action to End Health Disparities (NPA); Support Departmental initiatives and programs that provide access to quality health care; and
The Department’s strategic priorities: the opioid epidemic; childhood obesity; and serious mental illness.

Page 92
In addition, OMH plays a critical role in helping the Department respond effectively to public health crises, which often disproportionately affect OMH’s statutorily mandated populations of focus. OMH plays a critical role in supporting and implementing initiatives and programs that provide access to quality health care, address health disparities, and improve equity. Racial and ethnic minorities are less likely to receive preventive care, have higher rates of many chronic conditions, have fewer treatment options, have the highest rates of uninsured, and are less likely to receive quality health care. OMH does this through educational outreach and collaboration with strategic partners and stakeholders to increase these populations’ understanding of health coverage, health care, and how to effectively and efficiently use the health care system to improve their health. OMH also leads and coordinates the implementation of the National Partnership for Action to End Health Disparities (NPA), whose mission is to increase the effectiveness of programs that target the elimination of health disparities through the coordination of partners, leaders, and stakeholders committed to action. The NPA promotes cross‐cutting, multi‐sector, and systems‐oriented approaches to eliminate health disparities by coordinating the efforts of the four NPA implementation arms: the Federal Interagency Health Equity Team (FIHET); the 10 Regional Health Equity Councils (RHECs); the State and Territorial Offices of Minority Health; and National Partners. These implementation partners provide the leadership, community connection, and cross‐sector representation necessary to address health disparities. OMH provides guidance and technical assistance for the activities of the implementation partners to maximize their effectiveness and ensure alignment with the goals outlined in the Department’s National Stakeholder Strategy for Achieving Health Equity. FY 2017 Key Accomplishments OMH promotes integrated approaches, evidence‐based programs, and best practices to reduce health disparities. FY 2017 accomplishments support the Secretarial strategic goals as well as illustrate OMH’s commitment to enhancing and assessing the impact of all policies and programs on racial and ethnic health disparities.
Strategic Goal 1: Strengthen Health Care Key accomplishments in FY 2017 include:
OMH’s Center for Linguistic and Cultural Competency in Health Care (CLCCHC) supported: o Continued monitoring and promotion of the e‐learning programs on the Think Cultural
Health website (disaster preparedness and crisis response personnel, nurses, oral health professionals, physicians, and other providers and allied health professionals). Approximately 73,000 new participants registered and participants were awarded approximately 362,000 continuing education credits and participation statements towards their continuing education licensure requirements.
o Continued development of a new e‐learning program for behavioral health professionals, including holding focus groups, convening an advisory committee, drafting curriculum content, and creating a test website.
OMH furthered the adoption, implementation, and evaluation of the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (National CLAS Standards) Key accomplishments include: o Established six evaluation and data projects to assess awareness, adoption, and
implementation of the National CLAS Standards among diverse stakeholders, which includes the development of a toolkit to assist physicians to integrate and utilize the National CLAS Standards in private practice.
o Enhanced and implemented training activities for the U.S. Public Health Service

Page 93
Commissioned Corps personnel on culturally and linguistically appropriate services, using the National CLAS Standards.
o Continued discussions with three additional national organizations to form partnerships for promoting and adopting the National CLAS Standards.
Strategic Goal 2: Advance Scientific Knowledge and Innovation Key accomplishments in FY 2017 include:
Continued partnership between OMH and the National Center for Health Statistics (NCHS) for a Native Hawaiian and Pacific Islander (NHPI) National Health Interview Survey (NHIS) project to address the persistent lack of data for this hard to reach population. Data from this project were released to the public in March 2017.
NPA recognized as a model to achieve health equity, by the Robert Wood Johnson Foundation report – What is Health Equity? And What Difference Does a Definition Make? The report references the Federal Interagency Health Equity Team (FIHET) Data Compendium and the NPA as a resource for practitioners and decision‐makers looking for tools to help them design, implement, and evaluate initiatives to achieve health equity. (May 2017).
In conjunction with representatives from HHS operating divisions and staff divisions, including the Indian Health Service, provided coordination and support for the HHS American Indian and Alaska Native (AI/AN) Health Research Advisory Council (HRAC), which include: o Developed an Annual Health Research Report that includes summaries of various HHS
research projects focusing on AI/ANs, used as a resource to share research findings, topics, and available federal programs with tribes;
o HRAC held a session at NIHB’s Tribal Public Health Summit in Anchorage, Alaska, to discuss the Navajo Nation BRFSS survey conducted by the Navajo TEC, provide an overview of the HRAC mission and vision, and call attention to the nomination process for open HRAC positions;
o Developed strategic priority areas for FY 2018, including: Development of an HHS‐wide umbrella policy for conducting AI/AN research; Recommendation that HHS agencies include AI/AN culture‐specific modes of
intervention and indigenous practices in funding proposal requests; Encourage a stronger focus on social determinants of health among tribal and
HHS policymakers and health practitioners and a strong focus on social determinants of health research;
Advance specific initiatives in Indian Country that are designed to build local capacity to use research data to inform public health practice;
Creation of a web‐based, searchable AI/AN health research and reference collection with links to university and government libraries that encourages voluntary submissions of scholarly articles and projects;
Creation of an AI/AN‐specific Institutional Review Board (IRB) point of contact list published in the Federal Register annually;
Develop a tribal best practices and evidence base; and Focus on behavioral health.
o Participated in the Alaska Native Tribal Health Consortium, describing innovation to addressing rising incidence of Hepatitis C and HIV in rural Alaska.
o Developed a logic model to establish specific short‐, medium‐, and long‐term goals to enhance research and scientific knowledge in AI/AN communities.

Page 94
o Identified areas for research opportunities and concerns, including strategies to address them, during the quarterly meetings.
Strategic Goal 3: Advance the Health, Safety, and Well‐Being of the American People Key accomplishments in FY 2017 include:
Developed the Empowered Communities for a Healthier Nation Initiative, designed to reduce significant health disparities impacting racial and ethnic minorities and/or disadvantaged populations through implementing evidence‐based strategies with the greatest potential for impact. The program is intended to serve residents in communities disproportionately impacted by the opioid epidemic; childhood/adolescent obesity; and serious mental illness.
Developed and presented Zika education and awareness information to the public in both English and Spanish, including:
OMH web pages on Zika that are linked to all federal and state resources on Zika, which received over 10,000 hits; and
A Zika community event in Puerto Rico in which public health leaders and community based organizations shared best practices for public awareness, prevention and treatment.
Implemented various technical assistance and capacity building activities directed at community‐based organizations, health departments and institutions of higher education through OMH’s Resource Center (OMH is statutorily mandated to support a national minority health resource center).
Developed and implemented social marketing campaigns aimed at increasing awareness of hepatitis and HIV in communities of color. Twelve nonprofits covering the five racial and ethnic groups developed culturally tailored programming to increase awareness, and testing, of HIV and hepatitis, reaching an audience of more than 35.7 million people through 667 public service announcements; testing more than 12,000 individuals for HIV; and testing more than 10,000 individuals for hepatitis C.
Developed and implemented Spanish language curriculum for community health workers, to enhance awareness and educate communities about overall health issues.
Trained nonprofit health professionals in the Pacific Island territories to aid in the reduction of both infectious and non‐communicable diseases. In FY 2017, a health information campaign on HIV/AIDS awareness reached more than 98,000 individuals, through 62 community events and 15 public service announcements. Through this campaign, more than 650 individuals were tested for HIV.
Developed public health awareness campaigns to inform the public about health disparities and efforts to address them, through social media and online communication channels, reaching an estimated audience of more than 182 million individuals.
The National Partnership for Action to End Health Disparities (NPA):
The Federal Interagency Health Equity Team (FIHET), comprised of 12 different federal agencies plus 18 HHS StaffDivs and OpDivs: o Published a Compendium of Publicly Available Datasets and Other Data‐Related Resources,
a free resource of publicly available data relevant to research and programs aiming to reduce health disparities. It compiles descriptions of and links to 132 public datasets and resources that include information about health conditions and other factors that impact the health of minority populations.
o Conducted a series of webinars as part of its “Equity in All Policies” series, featuring innovative state and local programs nationwide that participants can adapt for their own

Page 95
states and communities. Participants included practitioners at all levels of government, as well as non‐profit, academia and community‐ and faith‐based organizations.
The Regional Health Equity Councils (RHEC): o Expanded RHEC activities and products. For example, RHEC II developed a report
highlighting the need to expand the collection and reporting of USVI health data. RHEC III administered the second phase of its CLAS/Cultural Competency Survey. RHEC IV partnered with various stakeholders and the NPA cross‐RHEC Oral Health workgroup on an Oral Health Needs Index Project. RHEC V led the cross‐RHEC Community Health Worker Coalition.
o Developed formal partnerships with external organizations to expand the RHECs’ reach. For example, RHEC VII has partnered with the HRSA Region VII Midwestern Public Health Training Center. This partnership will focus on workforce training, public health, rural health and chronic disease management, particularly in the area of diabetes. Also, a new partnership with the National Rural Health Association (NRHA) is addressing the needs of minority communities in rural areas, with a special focus on tribal communities. The NRHA will now integrate health equity and eliminating health disparities as an organizational priority.
o Developed regional blueprints for action and health equity report cards that highlight key health disparities issues affecting populations across several regions.
The Youth Health Equity Model of Practice (YHEMOP) program: o Established a 2017 summer cohort of 31 Health Equity Fellows with approximately 800
student applications received. The FY 2018 cohort will include approximately 25 Health Equity Fellows. Fellows are matched to health equity projects in organizations nationwide including federal agencies, state and county health departments, Regional Health Equity Councils, professional associations, FQHCs, and academic institutions. Fellows participate in a number of activities (e.g. webinars with Federal leaders, development of tailored Health Equity Impact Statements), and each present their work to OMH at the conclusion of the placement period.
Strategic Goal 4: Ensure Efficiency, Transparency, Accountability, and Effectiveness of HHS Programs OMH supports this goal by maintaining and strengthening OMH’s internal performance improvement and management system and evaluating implementation of the HHS Disparities Action Plan and the National CLAS Standards. Key accomplishments in FY 2017 include:
OMH’s Performance Improvement and Management System (PIMS) provides support to OMH and OMH grantees through the Evaluation Technical Assistance Center (ETAC) and the Performance Data System (PDS). The ETAC provides tailored evaluation support for OMH grantees. The PDS tracks OMH grantees on a common set of program performance measures.
OMH’s leadership of implementation of the HHS Disparities Action Plan included: o Evaluated health disparity impact statements for policies and programs. o Evaluated and assessed the development of a multifaceted health disparities data
collection strategy across HHS, as outlined in the HHS Disparities Action Plan. o Initial development of a framework for the long‐term evaluation of National CLAS
Standards. OMH completed an evaluation project in 2017 to systematically describe and examine the awareness, knowledge, adoption, and implementation of the National CLAS Standards.
OMH’s coordination of the NPA included: o Developed the fourth comprehensive NPA evaluation report and is using the information to
identify accomplishments and make adjustments in NPA implementation to maximize

Page 96
impact.
Funding History
Fiscal Year Amount FY 2014 $56,516,000 FY 2015 $56,670,000 FY 2016 $56,670,000 FY 2017 $56,541,000 FY 2018 Annualized CR $56,285,000
Budget Request The FY 2019 President’s Budget request for OMH of $53,956,000 is $2,320,000 below the FY 2018 Annualized CR level of $56,285,000. The FY 2019 request enables OMH to continue to provide leadership in coordinating policies, programs, and resources to support implementation and monitoring of both the HHS Disparities Action Plan and the NPA. OMH will continue coordination of HHS health disparity programs and activities; assessing policy and programmatic activities for health disparity implications; building awareness of issues impacting the health of racial and ethnic minorities; developing guidance and policy documents; collaborating and partnering with agencies within HHS, across the federal government, and with other public and private entities; funding demonstration programs; and supporting projects of national significance. At the reduced funding level, OMH will restructure or discontinue contracts, in order to fund the highest priorities and most effective approaches. Additionally, OMH will continue to serve in a critical leadership role within HHS in outreach and education of racial and ethnic minorities on access to quality health care through its many national, regional, state and territorial, tribal, and community‐based partnerships and networks across the nation. The Budget does not include funding for new grants in the Office of Minority Health. In FY 2019, OMH will continue to support program activities through leadership of workgroups and committees, grants, contracts, and strategic use of interagency agreements to achieve coordination of federal efforts related to health disparities such as:
American Indian/Alaska Native Health Equity Initiative (AI/AN HQI) will support projects that enhance the capacity to assess and implement culturally and linguistically appropriate intervention models addressing complex trauma, including behavioral health needs (e.g., mental health issues and substance use disorders) of AI/AN populations. In FY 2018, Tribes, Tribal Organizations, and Alaska Native‐Serving Organizations will form collaborative partnerships and alliances to improve access to quality health and human services and reach 500 youth, families, and community members. OMH supports four tribes and tribal organizations with awards that average $325,000 each annually for a total of $1,310,000 per year, for a five‐year period of performance that began FY 2017. Grants funded are expected to improve select AI/AN Health Equity Core Outcomes, such as improved resiliency among youth served.
Communities Addressing Childhood Trauma (ACT) is a multidisciplinary initiative to address unhealthy behaviors in minority and/or disadvantaged minority youth, ages 5 to 15 years at the start of the five‐year program, and provide them with opportunities to learn coping skills and gain experiences that contribute to more positive lifestyles and enhance their capacity to make healthier

Page 97
life choices. ACT grantees serve high‐risk minority and disadvantaged youth or adolescents and their families living in communities with significant rates of violence, homicides, suicides, substance use and misuse, depressive episodes, and incarceration/legal detention. FY 2017 ACT grantees reached approximately 17,000 youth, adolescents or families from minority and disadvantaged populations through community‐based, community‐focused intervention programs. Grants funded are expected to improve select ACT Core Outcomes, such as improved resiliency, consumption of healthy foods, and physical activity. OMH awarded ACT grants that average $300,000 each annually to seven community‐based agencies, for a total of $2.1 million annually for a five‐year period of performance.
Re‐Entry Community Linkages (RE‐LINK) program aims to improve coordination and linkages among criminal justice, public health, social service and private entities, to ensure health care access of the reentry population; reduce health disparities experienced by the reentry and justice‐involved population; increased access to needed public health, behavioral health, health care, coverage and/or social services; and reduced recidivism. In FY 2017, RELINK provided services to nearly 3,000 individuals to improve select Re‐Link Core Outcomes, such as health insurance coverage, identified unmet health needs, having regular source of care, enrollment in school or job training, living in stable housing, stable employment, and rate of re‐arrests. OMH supports eight grantee organizations with an average grant of $310,000 each, for a total of $2.5 million annually, for a five‐year project period, beginning FY 2016.
National Lupus Outreach and Clinical Trial Education Program (Lupus Program) seeks to reduce lupus related health disparities among racial and ethnic minority populations disproportionately affected by this disease by (1) implementing a national health education program on lupus (Priority A); and (2) developing, piloting and assessing clinical trial education interventions for health care providers and paraprofessionals focusing on improving recruitment and retention rates in clinical trials for minority populations affected by lupus (Priority B). In FY 2017, OMH awarded three Priority A grants that average $315,000 annually and two Priority B grants at $525,000 each annually, for a total of $2 million for a one‐year project period. The Lupus Program grantees reached approximately 3,800 persons affected by lupus and health care providers/paraprofessionals that serve racial and ethnic minorities living with lupus. Grants funded are expected to improve select Lupus Program Core Outcomes, such as (1) knowledge and skill in the diagnosis and treatment of lupus and knowledge and expertise in the signs and symptoms of lupus, treatment adherence, and screening among primary care providers (PCPs); (2) awareness of lupus symptoms and warning signs in minority populations; (3) dissemination of culturally and linguistically appropriate information to lupus patients and families; (4) implementation of the lupus outreach and health education program using rigorous tests to show improvements in project outcomes. The Lupus Program grants will also identify and test education program models that result in improvements in PCPs’ and other health care providers’ and paraprofessionals’ knowledge, attitudes, and intentions in (1) how to provide culturally and linguistically appropriate health care, and (2) educate, recruit, and, where appropriate, refer minority populations into clinical trials in a culturally and linguistically appropriate manner. OMH anticipates a similar one‐year program to reduce lupus‐related health disparities in FY 2018.
The State Partnership Initiative (SPI) to Improve Health supports State‐level partnerships to improve health outcomes in one to three leading health indicator topics in selected geographical hotspots throughout the state or territory. Leading health indicators being addressed by the states include childhood obesity. The state agencies such as departments of health and state offices of minority health will produce: (1) health disparities report cards, (2) implementation plans, (3) updated health disparities reports each year of the program showing progress, and (4) published results/articles that provide state‐level reports of improved health outcomes. The SPI directly

Page 98
impacted approximately 30,800 individuals in FY 2017, and supported 21 states and tribes with awards that average $200,000 each annually, for a total of $4.2 million annually, for a five‐year project period beginning FY 2015. Grants funded under the SPI address a broad range of health promotion activities and outcomes tailored to the leading health indicators selected by each grantee, such as smoking cessation, obesity prevention, management of chronic health conditions, reduced infant mortality, and increased breast feeding.
The National Workforce Diversity Pipeline (NWDP) Program supports projects that develop innovative strategies to identify promising students in their first year of high school and provide them with a foundation through their first year of college to pursue a successful career in a health profession. It is anticipated the NWDP will expand the diversity of health professional pipelines. In FY 2017, this program impacted approximately 14,525 minority and/or disadvantaged youth. NWDP awards average $425,000 each annually, for a total of $6.4 million each year, for a five‐year project period beginning FY 2015. Grants funded under the NWPD are expected to increase awareness and pursuit of careers in health care including behavioral health, and to increase the availability of science, technology, engineering and mathematics (STEM) education programs.
The Minority Youth Violence Prevention II program supports innovative approaches to significantly reduce the prevalence and impact of youth violence among racial and ethnic minority and/or disadvantaged at‐risk youth. MYVP II funds project interventions tailored to at‐risk racial and ethnic minority and/or disadvantaged youth (ages 12‐18 years at the start of the project), and requires a coordinated, multi‐discipline approach, including a public health agency, a local school and/or school district, a law enforcement agency, and an institution of higher education. These approaches are designed to address: public health, education, and public safety concerns; disparities in access to public health services; social determinants of health; and risk and protective factors; and will serve the project participants and comparison group members over a four year grant period. OMH awarded 10 grants to academic institutions, community‐based organizations, and a state health department that average $410,000 each annually, for a total of $4.1 million annually, for a four‐year project period beginning FY2017. MYVP II is expected to serve 1,200 youth and their families in year two. Projects funded are expected to improve select MYVP II Core Outcomes, such as: (1) increasing cultural competency and skills among those working with or serving at‐risk youth; (2) improving academic outcomes among MYVP II participants; (3) reducing law enforcement/justice encounters such as arrests and court referrals; (4) reducing crimes perpetrated by and against minority and/or disadvantaged youth; (5) reducing homicide and non‐fatal shooting incidents; (6) reducing stress and improvement in behavioral health; and (7) strengthening family engagement to create a positive and healthier home/community environment.
The Partnerships to Achieve Health Equity (Partnership) program is designed to demonstrate that multi‐partner collaborations that address social determinants of health and have a nationwide or regional reach, focus or impact can efficiently and effectively do one of the following: (1) improve access to, and utilization of, care by racial and ethnic minority and/or disadvantaged populations: (2) increase the diversity of the health workforce through programs at the high school or undergraduate level that focus on racial and ethnic health disparities and health equity and which include mentoring as a core component; or (3) increase data availability and utilization of data that increases the knowledge base regarding health disparities and facilitates the development, implementation and assessment of health equity activities. The Partnership program supports six organizations with awards that average $390,000 each annually, for a total of $2.3 million annually for a five‐year project period, beginning FY 2017. The Partnership program is expected to reach approximately 1,200 minorities and minority serving professionals in 2018. Projects funded are expected to improve select Partnership Core Outcomes, based on the project focus, such as (1) improvements in health measures (e.g., BMI, glucose, blood pressure, substance misuse, etc.); (2)

Page 99
increase in proportion of youth completing advanced placement science and math courses; and (3) increase in submission of manuscripts to peer review journals.
The Empowered Communities for a Healthier Nation Initiative (ECI) will support minority and/or disadvantaged communities disproportionately impacted by the opioid epidemic, childhood/adolescent obesity, or serious mental illness. ECI seeks to prevent opioid abuse, increase access to opioid treatment and recovery services, and reduce the health consequences of opioid abuse; reduce obesity prevalence and disparities in weight status among children and adolescents; and reduce the impact of serious mental illness and improve screening for serious mental illness at the primary care level. OMH will award up to 16 cooperative agreements that average $350,000 each annually for $5 million total, for each one‐year period of performance, for a project period of three years beginning in FY 2017. The ECI is expected to impact approximately 2,000 individuals in year one and 3,000 individuals in year two. Projects funded are expected to improve select ECI Core Outcomes, such as: (1) an increased number of persons receiving opioid overdose education and naloxone administration training designed to reduce opioid misuse and overdoses and reverse opioid overdoses; number of primary care providers trained in screening and diagnosis of opioid misuse and use disorder; number of primary care providers trained in motivational interviewing techniques to engage people in treatment, including medication‐assisted treatment, and number of community‐based pharmacies or other community‐based organizations with standing orders to dispense naloxone that are expected to result in a significant increase in the proportion of persons screened for opioid misuse and use disorder; significant increase in the proportion of persons with opioid use disorder entering evidence‐based treatment; identify and implement the most effective strategies to reach, engage, and retain people who inject drugs in substance abuse treatment, including medication‐assisted treatment for opioid use disorder, and identify innovative strategies to provide comprehensive services to people who inject drugs, including overdose reversal strategies; (2) an increased number of families with children ages 2‐19 years enrolled in obesity prevention programs that are expected to result in significant increases in consumption of fruits and vegetables, significant decrease in consumption of simple carbohydrates, and significant decrease in BMI among obese and overweight children ages 2‐19 years; (3) increased number of primary care providers trained to screen and diagnosis serious mental illness and/or trained in use of evidence‐based protocols for the proactive management of diagnosed mental disorders and increased number of persons diagnosed with serious mental illness participating in self‐management programs in communities with HPSA scores of 16 and higher which is expected to result in significant increase in the number of persons screened for serious mental illness and higher and significant reduction of symptoms among persons diagnosed with SMI in communities with HPSA scores of 16 and higher.
The Office of Minority Health Resource Center (OMHRC) will realign program priorities to address key issues of opioid abuse, mental health, and childhood obesity in communities of color. The resource center will host webinars and virtual workshops for a variety of external stakeholders including community based organizations (CBOs) on diseases and other issues that align with the strategic priorities of HHS; provide capacity building to institutions of higher education including minority serving institutions and CBOs; create campaigns to support initiatives and programs that promote health equity and the National Partnership for Action to End Health Disparities (NPA); increase the outreach of the Preconception Peer Health Educators (PPE) infant mortality prevention campaign; provide website development and support for OMH initiatives; support the development of content and manage OMH social media portals; increase digital access to the Knowledge Center library catalog; distribute electronic information and limited print publications; expand awareness of OMHRC programs and services by managing conference exhibits and other outreach activities; and support other OMH and HHS initiatives.

Page 100
The implementation of the National Partnership for Action to End Health Disparities (NPA) includes three contracts:
o Core Implementation of the NPA includes monitoring and updating the implementation strategy for the NPA; supporting and sustaining implementation at the state, territorial, regional, national, and federal levels; coordinating and streamlining the implementation‐related activities of OMH; documenting and sharing implementation successes, challenges, and lessons learned.
o Logistical support is provided throughout the year in the form of telephone and webinar conference coordination to increase efficiency as well as logistical technical support for the Federal Interagency Health Equity Team (FIHET).
o Core Evaluation includes evaluation planning, data collection, and reporting on the impact of the National Partnership for Action to End Health Disparities (NPA). Activities include collecting survey and qualitative data from NPA stakeholders to determine overall NPA functioning, accomplishments, and key challenges. Evaluation data assist OMH to track NPA progress, needed improvements, and best practices to inform strategies to increase impact.
The Center for Linguistic and Cultural Competency in Health Care (CLCCHC) has increased the support, promotion, and evaluation of its cultural and linguistic competency free e‐learning programs for physicians, nurses, disaster preparedness and crisis response personnel, oral health professionals, and allied health professionals with updates, additional on‐line resources, and expanded reach of each program. Health professionals may obtain continued education units for continued licensure through these programs, free of charge. CLCCHC has also continued supporting the development of new cultural and linguistic competency e‐learning programs and resources, including webinars, for other health professionals such as those in behavioral health professions. CLCCHC has continued developing partnerships with strategic organizations such as the U.S. Public Health Service. These types of activities serve to increase awareness of health disparities and the work of OMH. They also help ensure that health professionals are equipped to address issues of cultural competence and health disparities.
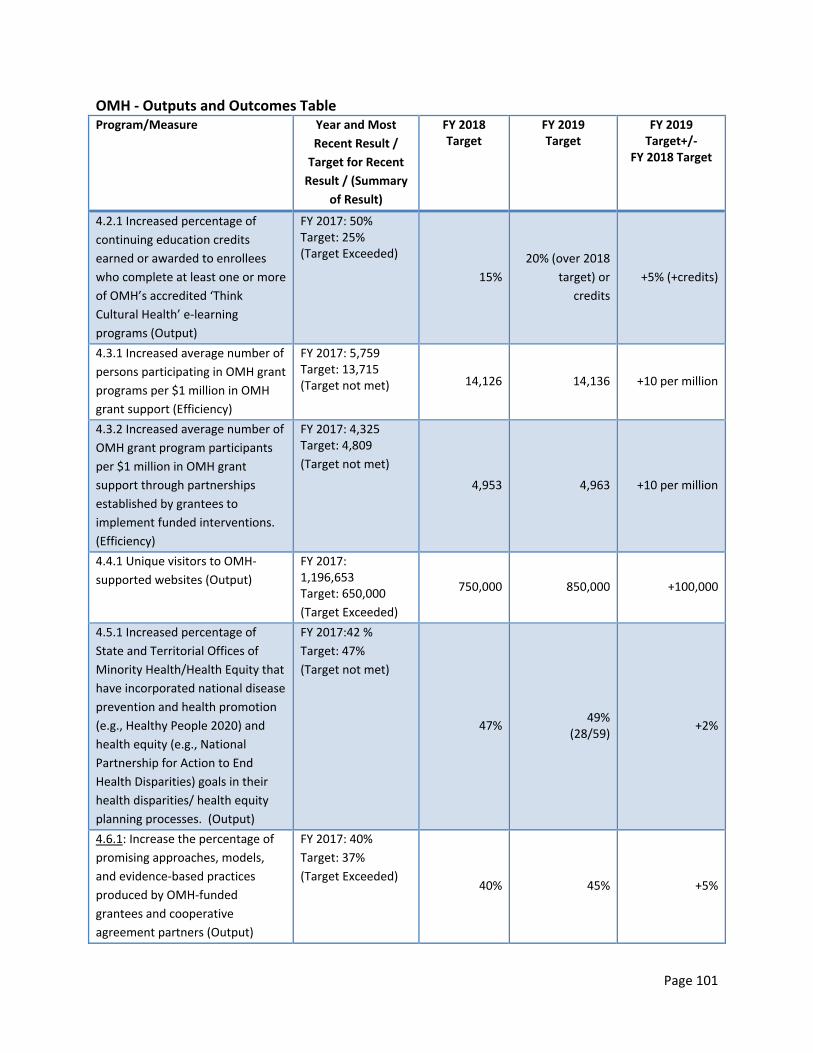
Page 101
OMH ‐ Outputs and Outcomes Table Program/Measure Year and Most
Recent Result /
Target for Recent
Result / (Summary
of Result)
FY 2018 Target
FY 2019 Target
FY 2019 Target+/‐
FY 2018 Target
4.2.1 Increased percentage of
continuing education credits
earned or awarded to enrollees
who complete at least one or more
of OMH’s accredited ‘Think
Cultural Health’ e‐learning
programs (Output)
FY 2017: 50% Target: 25% (Target Exceeded)
15%
20% (over 2018
target) or
credits
+5% (+credits)
4.3.1 Increased average number of
persons participating in OMH grant
programs per $1 million in OMH
grant support (Efficiency)
FY 2017: 5,759 Target: 13,715 (Target not met) 14,126 14,136 +10 per million
4.3.2 Increased average number of
OMH grant program participants
per $1 million in OMH grant
support through partnerships
established by grantees to
implement funded interventions.
(Efficiency)
FY 2017: 4,325 Target: 4,809
(Target not met)
4,953 4,963 +10 per million
4.4.1 Unique visitors to OMH‐
supported websites (Output)
FY 2017: 1,196,653 Target: 650,000
(Target Exceeded)
750,000 850,000 +100,000
4.5.1 Increased percentage of
State and Territorial Offices of
Minority Health/Health Equity that
have incorporated national disease
prevention and health promotion
(e.g., Healthy People 2020) and
health equity (e.g., National
Partnership for Action to End
Health Disparities) goals in their
health disparities/ health equity
planning processes. (Output)
FY 2017:42 %
Target: 47%
(Target not met)
47% 49%
(28/59) +2%
4.6.1: Increase the percentage of
promising approaches, models,
and evidence‐based practices
produced by OMH‐funded
grantees and cooperative
agreement partners (Output)
FY 2017: 40%
Target: 37%
(Target Exceeded) 40% 45% +5%

Page 102
Performance Analysis 4.2.1: Think Cultural Health (TCH) houses a suite of continuing education e‐learning programs dedicated to advancing health equity at every point of contact. The focus is on increasing provider awareness and, over time, changed beliefs and attitudes that will translate into better health care. With the addition of new e‐learning programs and resources for more health care and public health professionals and service providers, and sustained focus on the promotion and adoption of the National CLAS Standards, OMH expects to see a 30% increase in the number of continuing education (CE) credits earned or awarded to enrollees who complete at least one or more of OMH’s accredited Think Cultural Health e‐learning programs in their respective fields.
4.3.1 and 4.3.2: OMH provides grant funds to State Offices of Minority Health, community and faith‐based organizations, Tribes and tribal organizations, national organizations, and institutions of higher education. These grants play a critical role in supporting the HHS Disparities Action Plan and the Department’s priority goal to eliminate health disparities and achieve health equity. In FY 2019, OMH will continue a number of grant programs that address health disparities. OMH’s new and recent grant programs are designed to intensify and concentrate efforts in reducing health disparities, and, thus, OMH expects to see a 1% increase in the average number of people participating in OMH grant programs per $1 million.
4.4.1: OMH’s main website, www.minorityhealth.hhs.gov, is administered by the OMH Resource Center. The website includes access to the OMH Knowledge Center collection, which is a database comprised of 60,000 documents and more than 72% of the content is in digital format. The database contains minority health and health disparities data and literature, information on national and local minority health organizations, as well as resources for community‐ and faith‐based organizations and institutions of higher education (including minority‐serving institutions), and information about OMH.
The website supports community organizations and health disparities researchers in assembling accurate and comprehensive information and articles for use in program development and grant writing. The website serves as an information dissemination tool for the HHS Disparities Action Plan, the National Partnership for Action to End Disparities (NPA) (www.minorityhealth.hhs.gov/npa), and facilitates educational outreach to Black/African American, Hispanic/Latino, American Indian, Alaskan Native, Asian American, Native Hawaiian, and Pacific Islander communities. OMH expects to see at least 1,850,000 unique visitors to its main website in FY 2019. This increased number over its previously established target of 750,000 unique visitors reflects additional viewers brought in via OMH’s burgeoning social media accounts on Twitter, Facebook, YouTube and Instagram, and continual improvement of website content and features.
The NPA toolkit, which is housed on the revamped NPA website (https://minorityhealth.hhs.gov/npa/files/Plans/Toolkit/NPA_Toolkit.pdf) and is aimed at helping community organizations, has been viewed 1.7 million times since it was unveiled. OMHRC keeps NPA partners connected through its web page, electronic newsletter, blog, and related media.
Social Media has been a growing outlet for the dissemination of health information from OMH and its stakeholders. OMH has nearly 60,000 followers on its English Twitter handle with an extended outreach to more than 1+ million individuals and organizations. The OMH Facebook and Instagram pages, and Spanish Twitter handle are growing in followers.

Page 103
4.5.1: OMH builds strategic partnerships and provides leadership and coordination for State and Territorial Offices of Minority Health/Health Equity. OMH expects to see a 3.5% increase in the percentage of these entities that have incorporated national disease prevention and health promotion (e.g., Healthy People 2020) and health equity (e.g., National Partnership for Action to End Health Disparities) goals in their health disparities/health equity planning processes. 4.6.1: OMH is charged with advising the Secretary and the Department on the effectiveness of community‐based programs and policies impacting health disparities and to support research, demonstrations and evaluations to test new and innovative models. OMH funds demonstration grants to develop, test, and implement interventions to reduce health disparities. Results from these demonstration programs play a critical role in supporting the HHS Disparities Action Plan and the Department priority goal to eliminate health disparities and achieve health equity. Additionally, OMH is charged with ensuring on‐the‐ground implementation of initiatives and programs that provide access to quality health care and HHS Disparities Action Plan strategies. OMH expects to see a 1% increase in the percentage of promising approaches, models, and evidence‐based practices produced by OMH‐funded grantees and cooperative agreement partners per year. The expected performance of this measure is in line with the FY 2019 funding level.
Grants Grants (whole dollars)
FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
Number of Awards 101 101 101
Average Award $333,824 $341,748 $344,851
Range of Awards $175,000 ‐ $525,000 $175,000 ‐ $525,000 $175,000 ‐ $525,000
Program Data Chart Activity FY 2017
Final FY 2018
Annualized CR1 FY 2019
President’s Budget
Contracts
OMH Resource Center 4,610,000 4,610,000 3,800,000
Logistical Support Contract
2,030,000 2,030,000 1,800,000
National Partnership for Action to End Health Disparities
1,734,000 1,734,000 1,134,000
Center for Linguistic and Cultural Competency in Health Care
1,766,000 1,766,000 1,566,000
HHS Action Plan to Reduce Racial and Ethnic Health Disparities
600,000 600,000 600,000
Evaluation 900,000 900,000 900,000
Disparities Health Prevention
426,000 426,000 226,000
Secretary support Unaccompanied Children
129,000 0 0
Subtotal, Contracts 12,195,000 12,066,000 10,026,000
Grants/Cooperative Agreements

Page 104
State Partnership Programs
4,150,105 4,150,105 4,150,105
American Indian/Alaska Native Partnership
1,310,500 1,310,500 1,200,000
Specified Project – Lupus 2,000,000 2,000,000 2,000,000
Minority Youth Violence Prevention (MYVP)
0 0 0
Communities Addressing Childhood Trauma (ACT)2
2,082,400 2,792,269 2,792,269
Re‐entry Community Linkages (RE‐LINK)3
2,482,880 2,482,880 2,482,880
Multiple Chronic Condition Management (MCC)
0 0 0
HIV/AIDS Initiative for Minority Men (AIMM)
0 0 0
National Workforce Diversity Pipeline Program (NWDP)
6,360,745 6,360,745 6,360,745
Partnership to Achieve Health Equity
2,327,277 2,327,277 2,327,277
Minority Youth Violence Prevention II: Social Determinants of Health Collaborative Network
4,103,500 4,103,500 4,103,500
Empowered Communities for a Healthier Nation Initiative (ECI)4
5,000,000 5,000,000 5,000,000
Subtotal, Grants/Coop 29,817,407 30,527,276 30,416,776
Inter‐Agency Agreements (IAAs)
650,000 615,000 400,000
Operating Costs 13,878,593 13,076,724 13,113,224
Total 56,541,000 56,285,000 53,956,000
1 FY 2018 column displays comparable adjustments to reflect FY 2017 policy priority.
2 ACT FY2017 Notice of Awards (NOAs) noted the new funds ($2,082,400) and the carryover amounts (unobligated amount from FY2016 $709,870) to maintain the planned award amount 2017 and level funding FY2016 ($2,792,269). 3RELINK FY2017 NOAs listed the new funds ($2,482,879) and the carryover amounts (unobligated amount from FY2016 $279,262) to maintain the planned award amount 2017 and level funding FY2016 ($2,762,141). 4 ECI is a competitive cooperative agreement program initiated in FY 2017, which seeks to reduce the impact of and disparities in opioid abuse, childhood obesity, and serious mental illness, among racial and ethnic minority and/or other disadvantaged populations. The awards are planned for level funding in FY2018 and FY2019.

Page 105
OFFICE ON WOMEN’S HEALTH Budget Summary
(Dollars in Thousands)
Office on Women’s Health
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 32,067 31,922 28,454 ‐3,468
FTE 43 43 43 ‐
Authorizing Legislation:………….………………………………………………..........…..………….……Title II Section 229 of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………….Direct Federal, Competitive Grants, Contracts
Program Description and Accomplishments The Office on Women’s Health (OWH) was established in 1991 and statutorily authorized by the Patient Protection and Affordable Care Act (ACA) of 2010. The mission of OWH is to provide national leadership to improve the health of women and girls through policy, education, and innovative programs. OWH seeks to impact policy and produce educational and innovative programs that providers, communities, agencies, and other stakeholders across the country can replicate and expand. To achieve these goals, the office works with many partners, including federal agencies; nonprofit organizations; consumer groups; associations of health care professionals; tribal organizations; and state, county, and local governments.
Impact National Health Policy as it Relates to Women and Girls OWH coordinates women’s health policy, leads and administers committees, and participates in government‐wide policy efforts.
The HHS Coordinating Committee on Women’s Health, chaired by OWH, advises the Assistant Secretary for Health on current and planned activities across HHS that safeguard and improve the health of women and girls. Accomplishments in FY 2017 include:
o Collaborated on activities with agencies not traditionally focusing on women’s health, including HHS’s Office of the Assistant Secretary for Preparedness and Response, the Veterans Health Administration, and the Department of Transportation.
o Coordinated with the various partner agencies on educational presentations regarding the opioids crisis and its impact on women, childhood obesity, older women’s health care needs, suicide in women and girls, effects of childhood trauma, and addressing special health needs of American Indian and Alaska Native women through the Indian Health Service.
OWH co‐chairs the HHS Violence against Women (VAW) Steering Committee along with the Administration for Children and Families (ACF). The mission is to lead HHS in developing a blueprint for communities free from violence against women and girls, and to integrate the work of each HHS agency into its implementation. FY 2017 accomplishments include:
o Sponsored a joint federal panel presentation at the National Conference on Health and Domestic Violence where federal partners highlighted innovative approaches to education and partnership for health care providers and domestic violence and sexual assault victim advocacy organizations.
The Chronic Fatigue Syndrome Advisory Committee (CFSAC), which OWH manages, is composed of non‐federal researchers, clinicians, patient representatives, and federal ex‐officio representatives. This committee meets semi‐annually and makes recommendations to the Secretary on a broad range of topics including research, clinical care, and quality of life for

Page 106
patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Examples of 2017 activities include:
o Appointed new members from the Veterans Health Administration and patient/advocacy groups, as well as a new Chairperson.
o Received the first recommendations from the Pediatric Workgroup, which included participation from the Department of Education, an interagency partner.
OWH leads the Department in addressing the ongoing impact of the opioid epidemic on women’s health. Through this work, OWH has examined the prevention, treatment, and recovery issues for women who misuse, have use disorders, and/or overdose on opioids. Examples of accomplishments in FY 2017 include:
o Released the Final Report: Opioid Use, Misuse, and Overdose in Women, which provides a comprehensive overview of the impact of the epidemic on women’s health and will serve as a stepping‐off point for further activities on opioids and women.
o Funded 20 cooperative agreements via the Prevention of Opioid Misuse in Women: Office on Women’s Health Prevention Awards, which support primary and secondary prevention activities.
o Collaborated with CDC on the first Public Health Grand Rounds on Addressing the Unique Challenges of Opioid Use Disorder among Women.
OWH coordinates a federal working group with 11 other HHS offices and agencies to facilitate collaboration and information sharing around federal efforts addressing maternal mental health. Examples of accomplishments in FY 2017 include:
o Funded a public awareness campaign to educate women and their loved ones of the risks of postpartum depression.
Innovative and Model Programs on Women’s and Girls’ Health OWH supports activities and programs aimed at gathering evidence on effective strategies to help women and girls of all ages live healthier lives. OWH programs also focus on advancing the science on effective women's health interventions. For example, in FY 2017, OWH completed activities and the evaluation for the Intimate Partner Violence (IPV) Provider Network, which researches system changes for integrating intimate partner violence assessment and intervention into basic care, as well as evaluates collaboration models between healthcare providers and IPV programs. This initiative involves seven states: Arizona, California, Massachusetts, Minnesota, North Carolina, Texas, and West Virginia.
During FY 2017, grantees focused on finalizing efforts to reach recruitment goals; continued activities for the implementation phase of their intervention research; maintained partnerships with primary care clinics, health centers, hospital/university‐based clinics, domestic violence agencies, behavioral health specialists, and legal aid agencies interventions; and collected evaluation measures for their individual evaluation projects, as well as for OWH’s cross‐site evaluation project.
OWH is conducting a cross‐site evaluation to determine what system‐level factors support the integration of IPV service into clinical service, the barriers and facilitators to referring IPV victims to the appropriate referral services, and outcomes such as the patterns for the rate of screening, referrals, follow‐up, and services provided by the partner agencies.
In FY 2018, OWH will finish the final year of activities related to the Female Genital Cutting (FGC) Community‐Centered Health Care and Prevention Projects, community‐based efforts to address the health care needs of women and girls in the U.S. affected by, or at risk of undergoing, FGC.

Page 107
Activities in FY 2017 included work on developing or expanding existing culturally and linguistically sensitive health care services for women who have undergone FGC; building community dialogues, voices, and platforms for stressing the medical harms of the practice and the need for prevention; and developing community prevention toolkits designed for usability by other communities wanting to address FGC in the U.S.
In FY 2018, OWH will fund the final year of the College Sexual Assault Policy and Prevention Initiative, which supports grantee organizations in their work with colleges and universities to develop and implement sexual assault prevention programs and improve campus policies.
In FY 2017, efforts were focused on the establishment of Technical Advisory Groups and organizational partnerships that provided assistance to campus partners in establishing new prevention programs and reviewing their campus policies, as well as campus taskforces for prevention, leading to an increase in the number and reach of prevention programs that include a bystander intervention component.
Efforts were also made to encourage grantees to develop gender‐based prevention programming that focused on addressing the issue on sexual assault on campuses.
Additional activities included the establishment of campus Sexual Assault Response Teams, fielding campus climate surveys, and conducting reviews of campus sexual misconduct policies.
Education and Collaboration on Women’s and Girls’ Health OWH uses a mix of websites, webinars, written materials, Grand Round lectures, social media, partnership outreach, and interactive training modules to increase consumer and health professional knowledge of health issues, research, practices, programs, and policies that affect the health of women and girls. Examples include:
In FY 2017, OWH began developing trainings for health professionals to address the prevention and treatment of obesity in girls and young women. Based on needs assessments and identified gaps in training, OWH is developing educational materials that can be delivered via Web or in‐person. Focus areas for this topic may include a comparison of effectiveness of screening and brief counseling modalities or the use of decision aids that encourage provider‐patient engagement and behavior change. FY 2019 marks the final year for this project.
OWH administers the National Women’s Health Information Center, which utilizes websites, social media, print materials, and a telephone helpline to provide information to women across the nation. These resources allow women and girls to find scientifically accurate and reliable health information written at the 6th to 8th grade reading level in English and Spanish.
OWH continues its collaborative projects with the ACF Office on Trafficking in Persons. OWH provides funds to expand efforts to educate health care providers and social service workers about how to effectively identify and respond to victims of human trafficking, and to strengthen the health care and social service response. Additionally, OWH and ACF have partnered to evaluate the training project to educate health providers and social service workers.
In FY 2018, OWH funded the creation of a communication campaign to educate women and their loved ones of the risks of postpartum depression. The campaign will create PSAs, social media content, and written materials designed to destigmatize the disorder and promote treatment seeking in pregnant women and new mothers.
In FY 2017, OWH updated the Your Guide to Breastfeeding booklet. This high demand, easy‐to‐read publication features information and resources women need to promote breastfeeding through a child’s first birthday (as recommended by the American Academy of Pediatrics). The booklet was reprinted to be distributed by non‐profit women’s health partnership organizations,

Page 108
and is also available online. OWH extends the reach of the content of this publication by hosting educational webinars for consumers and health professionals.
In an effort to raise awareness of the significant health needs that women veterans face, and the federal resources that are available to help them, OWH partnered with the U.S. Department of Veterans Affairs (VA) to develop an educational webinar series. The first event of the series was a Facebook Live event held in FY 2017, which focused on mental health for women veterans. This event was viewed more than 1,200 times. Future topics include: suicide prevention, utilizing health benefits, and living with Post Traumatic Stress Disorder.
In response to a Senate report request, OWH launched a new campaign in FY 2017 to inform women about their options for breast reconstruction after a mastectomy. OWH partnered with the National Cancer Institute (NCI), Office of Minority Health (OMH), Centers for Medicaid & Medicare Services (CMS), CDC, and Health Resources and Services Administration (HRSA) to target breast cancer survivors and health care providers with messages about patient rights to receive breast reconstruction or prostheses after a medically necessary mastectomy. The campaign continues to create and disseminate consumer and health professional education activities to increase awareness of this health benefit.
Each year, OWH organizes the nationwide observance of National Women and Girls HIV/AIDS Awareness Day; this observance is designed to share information and empower women and girls to learn the importance of HIV and AIDS prevention, care, and treatment. Special efforts are made to reach African American and Latino women to raise awareness of their increased risk for HIV.
National Women’s Health Week is the second major observance that OWH leads. Held every May, this event encourages women to prioritize their health and take five simple steps improve their health at any age.
Funding History
Fiscal Year Amount
FY 2014 $33,958,000
FY 2015 $32,140,000
FY 2016 $32,140,000
FY 2017 $32,067,000
FY 2018 Annualized CR $31,922,000
Budget Request The FY 2019 President’s Budget request for OWH is $28,454,000, a decrease of $3,468,000 below the FY 2018 Annualized CR level of $31,922,000. OWH will reduce its Health Communications contract as part of this decrease. At the FY 2019 request level, OWH will continue to coordinate policies, programs, and information across HHS to support the implementation of the OWH Strategic Plan. The Budget does not include funding for new grants in the Office on Women’s Health.
In FY 2019, OWH’s projects will focus on one or more of OWH’s strategic areas, with a particular emphasis on preventing opioid misuse among women and girls, reducing childhood obesity, addressing

Page 109
mental health issues, reducing health disparities, promoting the health of women and girls across the lifespan, and supporting heath care services for women. Detailed OWH activities for FY 2019 include: Regional Women’s Health
OWH will support regional and national projects to promote women’s health through prevention initiatives and/or women’s health information dissemination.
Communications and Logistics
Health Communications: OWH’s health communications activities help the office achieve its mission of providing national leadership and coordination to improve the health of women and girls through policy, education, and model programs. OWH administers the National Women’s Health Information Center, which utilizes websites, social media, print materials, and a telephone helpline to provide information to women across the nation. These resources allow women and girls to find scientifically accurate and reliable health information written at the 6th to 8th grade reading level in English and Spanish.
Evaluation and Assessment OWH will routinely incorporate formal evaluation methods earlier in the program planning process.
OWH Program Evaluation: OWH will continue to support comprehensive evaluation and analysis of new and existing data to inform women’s health programs, policy, and outreach.
Health Information Gateway (formerly: Quick Health Data Online): In response to a Congressional mandate, OWH will continue to partner with the HHS Idea Lab to maintain its Health Information Gateway.
Trauma/Violence against Women
Addressing Violence against Women in High‐Risk Communities: OWH will fund awards for communities at most risk for perpetuating violence against women. The project will build upon the previously funded IPV Provider Network, which focused on integrating interpersonal violence assessment and intervention into basic care, as well as encouraging collaborations between healthcare providers, public health programs, and IPV programs. Using the knowledge gained from the Network, grantees will fill gaps in healthcare services for high‐risk women and bolster prevention efforts in communities where abusive practices persist at increased rates.
Data Policy Project on the Health of Incarcerated Women: In FY 2019, OWH will partner with the National Academies of Science, Engineering, and Medicine to develop recommendations that will improve the health care service delivery and response for women who are incarcerated and often experience violence. Funding will support research and development activities.
Women’s Health across the Lifespan
Federal Maternal Depression Workgroup: OWH coordinates a federal workgroup with other HHS offices and agencies to facilitate collaboration and information sharing around federal efforts addressing maternal mental health. Based on the information exchange and needs identified from this initiative, OWH plans to develop and support efforts to address maternal depression.
Paid Family Leave Policy Research: In FY 2019, OWH is funding year two of a three year research study in partnership with the Office of the Assistant Secretary for Planning and Evaluation to identify potential health outcomes associated with extending paid family leave.

Page 110
Education and Collaboration on Women’s and Girls’ Health
Postpartum Depression Destigmatization and Treatment Campaign: In FY 2019, OWH will continue to fund the creation of a communications campaign designed to educate women and their loved ones of the risks of postpartum depression. The campaign will create PSAs, social media content, and written materials designed to destigmatize the disorder and promote treatment seeking in pregnant women and new mothers.
Breastfeeding and Childhood Obesity: In FY 2019, OWH will continue its efforts around the evidence‐based association between breastfeeding and childhood obesity.
Health Disparities in Women
Health Disparities Initiative: OWH will continue to partner with agencies to increase the focus and/or collection of data on women’s health issues. Potential activities include the addition of specific women’s health questions to existing surveys and co‐funding grants/contracts.
Women and HIV/AIDS: In FY 2019, OWH will partner with the Office of HIV/AIDS and Infectious Disease Policy to further raise awareness and support action on emerging issues in HIV/AIDS and viral hepatitis issues affecting the health of women and girls. OWH will review and analyze research to ensure a gender focus, while leveraging the expertise of both offices.
Health Care Services for Women
Prevention of Opioid Misuse in Women: Office on Women’s Health Prevention Awards (OWHPA): In FY 2019, OWH will continue to support 20 cooperative agreements which fund primary or secondary prevention efforts to prevent the misuse of opioids by women across their lifespans. Selected regional, state, local, and community organizations will achieve this goal through: program development and implementation, health education targeting health professionals and/or women directly, or policy efforts. These grants are slated to be funded through FY 2019.
Model Programs for States to Address Serious Mental Illness in Women and Girls: OWH will award grants or cooperative agreements to fund model programs to address state‐level gaps that impact women’s mental health in selected states based on their serious mental illness prevalence, access to care ranking, or treatment spending level.
Health Professional Training to Reduce Childhood Obesity: OWH will continue to fund the creation of two new training modules on the obesity prevention and promotion of physical activity among girls.

Page 111
Office on Women’s Health ‐ Outputs and Outcomes Table
Program/Measure FY 2017 Results
Target (Summary of Result)
FY 2018 Target FY 2019 Target FY 2019 Target +/‐ FY 2018 Target
5.2.1 Number of users of OWH’s social media channels. (Output)
FY 2017: 8,500,000 Target: 1,500,000 (Target Exceeded)
1,500,000 1,750,000 +250,000
5.3.1 Number of users of OWH communication resources (Output)
FY 2017: 13,221,536 Target: 20,000,000 (Target Not Met)
20,000,000 21,500,000 +1,500,000
5.4.1 Number of girls ages 9‐17 and women
ages 18‐85+ that participate in OWH‐
funded programs (e.g., information sessions,
web sites, and outreach) per million dollars spent annually. (Efficiency)
FY 2017: 619,856 Target: 1,000,000 (Target Not Met)
1,000,000 1,500,000 +500,000
Performance Analysis OWH's outreach efforts will ensure the availability of a central source of reliable women's health information to the public. Data from national surveys indicate that women are more likely than men to search for health information online and that women are more likely to look for online health information on behalf of loved ones (Fox, 2013: http://www.pewinternet.org/2013/01/15/health‐online‐2013/). Metrics used to guide and support OWH’s outreach activities include data on the number of user sessions to the OWH websites, the number of users of OWH’s social media channels, call center and email subscriptions; and the number of women and girls served by OWH programs and initiatives. OWH's continued social media efforts will ensure that scientifically accurate women’s health information is available to the public in the most accessible and widely used formats (e.g., desktop, mobile, or tablet). Data from the Pew Research Center shows that 80% of women use social media in a typical day. As of FY 2017, more than 1.8 million users subscribed to OWH social media channels, and OWH is ranked as the #2 (@womenshealth) most popular Twitter channel at HHS and the @womenshealth OWH Twitter channel is in the Top Ten of all Federal Twitter channels for number of followers.
Grants Grants (whole dollars) FY 2017 Final FY 2018 Annualized CR FY 2019 President’s
Budget
Number of Awards 42 37 36
Average Award $234,785 $166,903 $152,777
Range of Awards $96,840 ‐ $1,028,115 $98,893 – $333,333 $98,893 – $250,000

Page 112
Program Data Chart Activity FY 2017 Final FY 2018 Annualized CR FY 2019 President’s Budget
Contracts
Program Evaluation 1,626,698 1,821,786 1,753,450
Health Communications 5,310,000 5,700,000 5,350,252
Women’s Health Across the Lifespan
731,018 1,500,000 1,000,000
Trauma/Violence Against Women
260,167 260,167 195,000
Health Disparities in Women
0 1,200,000 1,200,000
Health Care Services for Women
0 300,000 300,000
Education and Collaboration on Women’s and Girls’ Health
350,310 550,310 500,000
Subtotal, Contracts 8,278,193 11,332,263 10,298,702
Grants/Cooperative Agreements
Health Care Services for Women
1,993,893 1,993,893 3,500,000
Health Disparities in Women
2,019,704 2,019,704 0
Trauma/Violence Against Women
5,847,375 2,161,818 1,850,000
Education and Collaboration on Women’s and Girls’ Health
0 0 0
Subtotal, Grants/Cooperative Agreements 9,860,971 6,175,415
5,350,000
Inter‐Agency Agreements (IAAs)
3,669,7828 3,802,521 1,628,162
Operating Costs 10,258,054 10,611,801 11,177,136
Total 32,067,000 31,922,000 28,454,000

Page 113
OFFICE OF RESEARCH INTEGRITY Budget Summary
(Dollars in Thousands)
Office of Research Integrity FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 8,558 8,558 8,558 ‐
FTE 28 28 28 ‐
Authorizing Legislation..……………………….…………………………………………………………………….Section 493 of the PHS Act FY 2019 Authorization……………………………………………………………………………………………………………………..........Indefinite Allocation Method……………………………………………..………………………….……………………Direct federal, Contracts, Grants
Program Description and Accomplishments Since its inception in 1992, the mission of the Office of Research Integrity (ORI) has been to promote integrity in biomedical and behavioral research, reduce research misconduct, and maintain the public’s confidence in research supported by funds of the U.S. Public Health Service (PHS) agencies – supporting the Department’s goal to lead in science and innovation. ORI’s mission directly supports the Office of the Assistant Secretary for Health’s national leadership on the quality of public health systems. Recipients of PHS funds are required by federal regulation to foster an environment that promotes the responsible conduct of research, implement policies and procedures to respond to allegations of research misconduct, protect the health and safety of the public, and conserve public funds (42 C.F.R. Part 93). ORI functions through two divisions. The Division of Investigative Oversight (DIO) handles allegations of research misconduct and monitors institutional research misconduct processes. The Division of Education and Integrity (DEI) manages programs to ensure that PHS‐funded institutions have policies and procedures in place for handling allegations of research misconduct and provides educational resources to help institutions in promoting research integrity. ORI leads or collaborates in cross‐departmental training and oversight activities involving HHS’s Office for Human Research Protections (OHRP) and Office of Inspector General. ORI convenes periodic meetings with representatives from other departments and agencies responsible for handling allegations of research misconduct, including the National Science Foundation, Veterans Administration, Department of the Interior, Environmental Protection Agency, and Department of Defense and, within HHS, National Institutes of Health. As needed, ORI consults with individual departments and agencies when their funding may be involved in specific cases under review. ORI’s determinations usually take 1‐2 years, reflecting the deep analysis conducted on each case by ORI’s science investigators. Findings lead to HHS administrative actions that are publicly disclosed via the Federal Register, including mandated supervision over submission of research grants and papers, ban from serving on review panels, and debarment from federal funds (typically for 3 years, but spanning from 1 year to a lifetime). The purpose of these administrative actions is to stop the misuse of PHS funds, pursuant to the 2005 regulation. Nearly all ORI findings are adjudicated through a settlement process. If the respondent declines to enter into a settlement agreement, the case proceeds to the HHS Departmental Appeals Board where an Administrative Law Judge (ALJ) may hear the case. ORI currently
Page 114
has three significant cases before the DAB; one was heard in 2017, with determination anticipated in 2018. Scientists, graduate students, university administrators, and others regularly contact ORI with concerns about potential misconduct. In addition, ORI’s assurance process allows funded institutions to report allegations, inquiries, and investigations related to their funding. The accessions from the direct‐contact and assurance databases often do not align because of the timing and sources of the contacts with ORI. Nonetheless, over the past five years, ORI typically has handled 200‐450 accessions each year, opening 25‐40 cases per year, and closing 20‐45. Currently ORI has 131 active accessions and 36 active cases. ORI funds research grants on social and behavioral factors associated with research misconduct, and to develop tools to better detect research misconduct. ORI also funds grants to institutions to provide a forum for discussion and production of tangible outcomes related to at least one of several themes related to ORI’s mission: (1) training on responsible conduct of research; (2) fostering an environment that promotes research integrity; (3) prevention of research misconduct; (4) handling of research misconduct allegations; (5) whistleblowing; (6) international issues in research integrity; or (7) other topics clearly linked to research integrity and compliance with 42 C.F.R. Part 93. To date, ORI grants have yielded over 200 peer‐reviewed publications. ORI’s accomplishments in FY 2017 have furthered the goal of promoting research integrity as follows:
Responded to 220 allegations (accessions); 26 of these became formal ORI cases in 2017, though 24 of the 26 were from previous years.
Administratively closed 24 accessions, 14 of which were received in 2017.
Closed 23 cases, including 5 with findings of research misconduct.
Maintained the assurance database that tracks annual reports from the nearly 5,000 institutions worldwide that receive PHS funds for research, and ensured that they implement policies for handing allegations of research misconduct.
Managed 30 Freedom of Information Act (FOIA) requests.
Received over 100 website visits from each of more than 125 countries.
Produced web‐based materials to promote research integrity in basic and clinical research including a number of “infographics” that were viewed more than 50,000 times.
ORI hosted conferences and workshops on research integrity, including: a. Two Research Integrity Officer (RIO) Boot Camps for institutional officials (November
2016 and June 2017); b. Two Responsible Conduct of Research Instructor Workshops (April and September
2017); c. Sequestration of Evidence Workshop (August 2017), a pilot session for a topic critical to
quality institutional investigations; and d. Quest for Research Excellence Conference (August 2017).
ORI published semi‐annual newsletters and offered regular social media and blog postings throughout the year.
ORI disseminated two new grant Funding Opportunity Announcements seeking meritorious applications for conducting research on, and convening conferences related to, research integrity and completed OASH peer review process.

Page 115
Funding History
Fiscal Year Amount
FY 2014 $8,558,000
FY 2015 $8,558,000
FY 2016 $8,558,000
FY 2017 $8,558,000
FY 2018 Annualized CR $8,558,000
Budget Request The FY 2019 President’s Budget request for ORI is $8,558,000, the same as the FY 2018 Annualized CR. The budget will support pay and non‐pay inflationary costs. At this level, ORI maintains staff needed to conduct investigative and educational activities. This includes managing contracts and grants that are needed to support the dissemination of educational information regarding research integrity, and training activities aimed at increasing awareness and technical skill in conducting research misconduct proceedings at PHS‐funded research institutions. ORI’s plans for the use of FY 2019 funds include: ORI will address DIO staff vacancies and enhance internal case handling processes. ORI staff spends significant time via email and telephone, providing technical assistance to RIOs who are responsible for investigating allegations at their respective institutions. ORI’s findings are dependent on quality investigations. ORI also participates in NIH regional conferences, and provides presentations for NIH grants management staff. ORI supports database and website development, including updating and enhancing the ORI website (https://ori.hhs.gov/) and developing a robust intranet portal and tracking system. Digital/web‐based communication is a critical tool for ORI to accomplish program goals and support program activities. The ORI website receives over 2,000,000 page views per year from users around the world, seeking information about ORI, misconduct cases, research education, and policies and procedures, including a secure Ask ORI mailbox to receive allegations of research misconduct. This mailbox is monitored daily, with ORI experts providing timely response. ORI uses a secure on‐line email program on a monthly basis to communicate with the biomedical research and research integrity communities. The ORI website requires intensive maintenance to ensure compliance with Federal Web Policies and HHS Web Communications and New Media Policies and Standards. Finally, the ORI Intranet Portal contains a Case Tracking System, used by the ORI investigative division to monitor and document the progress of research misconduct allegations and cases. ORI plans to conduct an expert assessment of its data needs and systems in 2018, ahead of awarding a new contract for this activity in FY 2019. ORI will support two Boot Camps designed to provide formalized training for RIOs and their legal counsel. ORI maintains a waiting list for RIOs and institutional counsel interested in this program, which helps institutions comply with 42 C.F.R. 93. When the process is mismanaged at the institutional level, whether domestically or abroad, ORI is unable to fulfil its regulatory mandate by making research misconduct findings against respondents. Attesting to the national importance of this training program, the Boot Camps have led to the creation of an independent professional association, the Association for Research Integrity Officers (ARIO), to provide a forum for RIOs across the country to convene. ORI experts provide lectures and technical consultation at the ARIO meetings.

Page 116
ORI will support two Workshops designed to provide formal training for Responsible Conduct of Research (RCR) instructors, in order to fulfill our regulatory requirement to promote research integrity at PHS‐funded institutions. To build upon momentum generated during previous meetings, and ensure compliance with 42 C.F.R. 93 on behalf of PHS‐funded institutions, ORI will host a bi‐annual global conference on research integrity in 2019. The conference will emphasize two themes: (1) Research Misconduct; and (2) Promoting Research Integrity. ORI anticipates at least 300 participants. ORI has reviewed hundreds of institutional research misconduct cases. Based on this experience and in‐depth conversations with RIOs, several topics arise as particular challenges to RIOs and institutions: correctly interviewing respondents, sequestering data, and understanding “intent” when assessing whether misconduct has occurred. ORI plans to offer a senior institutional leadership workshop or meeting in 2018, which may serve as a pilot for a 2019 offering. As a result of the sequestration workshop in 2017, that effort will be expanded in 2018 to a 3‐day interactive workshop for RIOs to demonstrate and role‐play appropriate handling of evidence. ORI expects to offer these or similar topics in two sessions in 2019. ORI plans to support twelve new grant awards for exploration of critical questions related to the promotion of research integrity and the proper stewardship of PHS research funds.
Grants Grants
(whole dollars) FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
Number of Continuations 2 3 ‐
Average Continuation Award
$262,500 $157,000
Range of Continuation Awards
$245,976 $261,762
Number of New Awards 9 8 12
Average New Award $109,722 $100,000 $100,000
Range of New Awards $49,393‐$135,763 $50,000‐$150,000 $50,000‐$150,000
Total Number of Awards 11 11 12

Page 117
EMBRYO ADOPTION AWARENESS CAMPAIGN Budget Summary
(Dollars in Thousands)
Embryo Adoption Awareness Campaign
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 998 993 1,000 +7
FTE ‐ ‐ ‐ ‐
Authorizing Legislation..………….………………………………………………..........…..…………….…………Section 1704 of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method……………………………………………………….………………………….Grants, Cooperative agreement, contracts
Program Description and Accomplishments The purpose of the embryo donation/adoption awareness campaign is to educate the American public about the existence of frozen embryos created through in‐vitro fertilization (IVF) that could be available for adoption by infertile individuals or couples. The program is also authorized to support medical or administrative services for people seeking to use embryo adoption as a method of family building. In the course of treatments for infertility, people usually produce more embryos than they can use. These supernumerary embryos are generally frozen while the couple who created them decides about their ultimate disposition. This freezing process is known as cryo‐preservation. The latest data suggest that there are more than 620,000 cryo‐preserved embryos in the United States. However, it is likely that the vast majority of these cryo‐preserved embryos are still being considered for use in the family‐building efforts of the couples who created them. Nevertheless, it is thought that 10% of those frozen embryos could potentially be made available for embryo donation/adoption (i.e., the transfer of the embryo to the uterus of a woman who intends to bear the child and to be that child's parent). The ultimate purpose of the program is to promote the use of embryo donation as a family‐building option.
In fiscal years 2002, and 2004 – 2017, funds were appropriated for an embryo adoption public awareness campaign. The purpose is to educate Americans about the existence of frozen embryos (resulting from in‐vitro fertilization), which may be available for donation/adoption for family building. In general, three to five grants have been awarded each year through a competitive process. The grants generally have a two year life‐span. In 2011, survey research conducted through an inter‐agency agreement with the National Center for Health Statistics (NCHS), suggested that nearly two‐thirds of women of child‐bearing age had heard of this method of family building. An interagency agreement with NCHS will support research starting in 2018 that investigates the public’s sources of information about frozen embryo adoption.
Funding History
Fiscal Year Amount
FY 2014 $1,000,000
FY 2015 $1,000,000
FY 2016 $1,000,000
FY 2017 $1,000,000
FY 2018 Annualized CR $993,000

Page 118
Budget Request The FY 2019 President’s Budget request for Embryo Adoption Awareness Campaign of $1,000,000 is $7,000 over the FY 2018 Annualized CR level of $993,000. The request will be used to pursue projects that increase public awareness about the availability of embryo donation/adoption, or which provide medical or administrative services that help couples to use embryo donation as a method of family building.
Grants (whole dollars)
FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Level
Number of Awards 3 2 3
Average Award $230,000 $269,000 $250,000
Range of Awards $150,000 ‐ $299,000 $239,000 ‐ $299,000 $150,000 ‐ $300,000

Page 119
SEXUAL RISK AVOIDANCE Budget Summary
(Dollars in Thousands)
Sexual Risk Avoidance
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +5% Initiative Level +/‐ FY 2018 President’s Budget
Budget Authority 14,966 14,898 ‐ ‐14,898
FTE ‐ ‐ ‐ ‐
Authorizing Legislation:……………………….……………………………..………………………………….………….…… P.L. 115‐31 FY 2017 Authorization.……….……………………………………………………………....................................................Annual Appropriation Allocation Method……………………………………………………………………………………………..………..………Direct Federal, Grants
Program Description and Accomplishments The Sexual Risk Avoidance program consists of competitive, discretionary grants to provide sexual risk avoidance education for adolescents. Grantees use an evidence‐based approach and/or effective strategies through medically accurate information referenced in peer‐reviewed publications to educate youth on how to avoid risks that could lead to non‐marital sexual activity. Projects are implemented using a Positive Youth Development (PYD) framework as part of risk avoidance strategies, to help participants build healthy life skills, build on or enhance individual protective factors that reduce risks, and empower youth to make healthy decisions. In FY 2016, 21 Sexual Risk Avoidance Education (SRAE) grantees were awarded $8.9 million. SRAE grantees are projected to serve over 16,000 youth in FY 2017.
Funding History
Fiscal Year Amount
FY 2014 $5,000,000
FY 2015 $5,000,000
FY 2016 $10,000,000
FY 2017 $15,000,000
FY 2018 Annualized CR $14,898,000
Budget Request The FY 2019 President’s Budget does not request funds for this program.
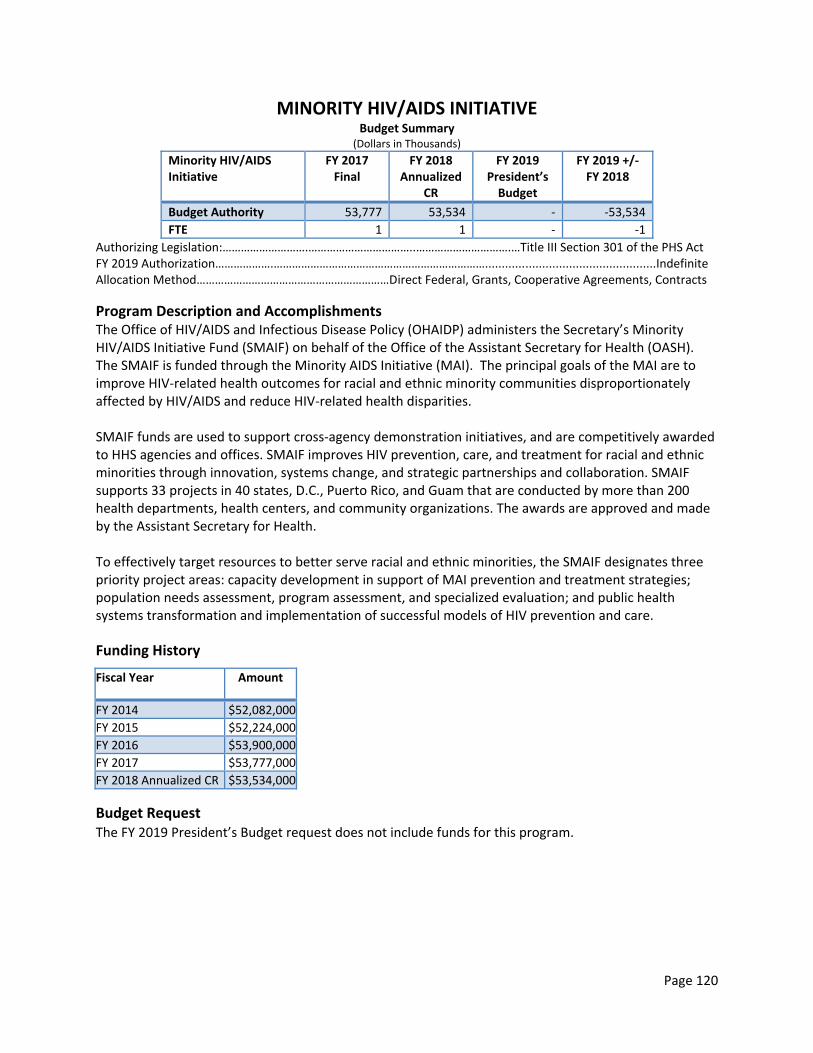
Page 120
MINORITY HIV/AIDS INITIATIVE Budget Summary
(Dollars in Thousands)
Minority HIV/AIDS Initiative
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 53,777 53,534 ‐ ‐53,534
FTE 1 1 ‐ ‐1
Authorizing Legislation:……………………….……………………………..………………………….…Title III Section 301 of the PHS Act FY 2019 Authorization……………….……………………………………………………………...................................................Indefinite Allocation Method………………………………………………………Direct Federal, Grants, Cooperative Agreements, Contracts
Program Description and Accomplishments The Office of HIV/AIDS and Infectious Disease Policy (OHAIDP) administers the Secretary’s Minority HIV/AIDS Initiative Fund (SMAIF) on behalf of the Office of the Assistant Secretary for Health (OASH). The SMAIF is funded through the Minority AIDS Initiative (MAI). The principal goals of the MAI are to improve HIV‐related health outcomes for racial and ethnic minority communities disproportionately affected by HIV/AIDS and reduce HIV‐related health disparities. SMAIF funds are used to support cross‐agency demonstration initiatives, and are competitively awarded to HHS agencies and offices. SMAIF improves HIV prevention, care, and treatment for racial and ethnic minorities through innovation, systems change, and strategic partnerships and collaboration. SMAIF supports 33 projects in 40 states, D.C., Puerto Rico, and Guam that are conducted by more than 200 health departments, health centers, and community organizations. The awards are approved and made by the Assistant Secretary for Health. To effectively target resources to better serve racial and ethnic minorities, the SMAIF designates three priority project areas: capacity development in support of MAI prevention and treatment strategies; population needs assessment, program assessment, and specialized evaluation; and public health systems transformation and implementation of successful models of HIV prevention and care.
Funding History
Fiscal Year Amount
FY 2014 $52,082,000
FY 2015 $52,224,000
FY 2016 $53,900,000
FY 2017 $53,777,000
FY 2018 Annualized CR $53,534,000
Budget Request The FY 2019 President’s Budget request does not include funds for this program.

Page 121
RENT, OPERATION, MAINTENANCE AND RELATED SERVICES Budget Summary (Dollars in Thousands)
Rent, Operation, and Maintenance and Related Services
FY 2017 Operating
Level
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ 2018
Budget Authority 15,866 15,980 16,089 +109
FTE ‐ ‐ ‐ ‐
Authorizing Legislation:………….………………………………………………..........…..………….………………………Title III of the PHS Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….……………………..………..Direct Federal
Program Description and Accomplishments The Rent/Operation and Maintenance (O&M) and Related Services account funds headquarters facilities occupied by the OS STAFFDIVS funded by the GDM account. Descriptions of each area follow:
Rental payments (Rent) to the General Services Administration (GSA) include funds to cover the rental costs of office space, non‐office space, and parking facilities in GSA‐controlled buildings.
O&M includes funds to cover the operation, maintenance, and repair of buildings for which GSA has delegated management authority to HHS; this includes the HHS headquarters, the Hubert H. Humphrey Building (HHH).
Related Services include funds to cover non‐Rent activities in GSA‐controlled buildings (e.g., space management, events management, guard services, other security, and building repairs and renovations).
Funding History
Fiscal Year Amount
FY 2014 $16,429,000
FY 2015 $15,798,000
FY 2016 $16,089,000
FY 2017 $15,866,000
FY 2018 Annualized CR $15,980,000
Budget Request The FY 2019 President’s Budget request for Rent, Operations Maintenance and Related Services of $16,089,000 is $109,000 above the FY 2018 Annualized CR level of $15,980,000. The increase will partially support pay and non‐pay inflationary increases.

Page 122
SHARED OPERATING EXPENSES Budget Summary
(Dollars in Thousands)
Shared Operating Expenses FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Request
FY 2019 +/‐ FY 2018
Budget Authority 11,544 11,466 12,562 +1,096
FTE ‐ ‐ ‐ ‐
Common Expenses/ Service and Supply Fund (SSF) Payment Common Expenses include funds to cover administrative items and activities which cut across and impact all STAFFDIVs under the GDM appropriation. The major costs in this area include:
Worker's Compensation
Federal Employment Information and Services
Records storage at the National Archives and Records Administration
Radio Spectrum Management Services
Federal Executive Board in Region VI
Telecommunications (e.g., FTS and commercial telephone expenses)
CFO and A‐123 audits
Federal Laboratory Consortium
Postage and Printing
Unemployment Compensation Payments to the SSF are included in the overall Common Expenses category, but are broken out separately here for display purposes. These payments cover the usage of goods and services provided through the SSF:
Personnel and Payroll Services
Finance and Accounting activities
Electronic communication services (e.g., voice‐mail and data networking)
Unified Financial Management System (UFMS) Operations and Maintenance FY 2018 HHS Enterprise Information Technology and Government‐Wide E‐Gov Initiatives The Budget includes $178,415 to support government‐wide E‐Government initiatives.

Page 123
* Specific levels presented here are subject to change, as redistributions to meet changes in resource demands are assessed.
Government‐wide e‐Gov initiatives provide benefits, such as standardized and interoperable HR solutions, coordinated health IT activities among federal agencies providing health and healthcare services to citizens; financial management processes; and performance management. They also improve sharing across the federal government of common budget formulation and execution practices and processes resulting in improved practices within HHS.
Funding History
Fiscal Year Amount
FY 2014 $13,982,000
FY 2015 $13,369,000
FY 2016 $11,924,000
FY 2017 $11,544,000
FY 2018 Annualized CR $11,466,000
Budget Request The FY 2019 President’s Budget request for Shared Operating Expenses of $12,562,000 is $1,096,000 above the FY 2018 Annualized CR. The FY 2019 request of $12,562,000 includes an inflation factor for overhead costs and additional Service and Supply Fund charges and other shared expenses.
FY 2018 E‐Gov Initiatives and Line of Business* Original Amount
Revised Amount
Budget Formulation and Execution Line of Business $2,400 $2,400
Disaster Assistance Improvement Plan $1,418 $1,418
E‐Rulemaking (moved from FFS) $21,815 $21,815
Federal Architecture $50,654 $50,654
Financial Management Line of Business $5,031 $5,031
Geospatial Line of Business $1,091 $1,091
Benefits.gov $9,506 $9,506
Human Resources Management Line of Business $2,988 $2,988
Integrated Acquisition Environment $81,771 $81,771
Performance Management $1,741 $1,741
FY 2018 E‐GOV Initiatives Total $178,415 $178,415

Page 124
PHS EVALUATION SET‐ASIDE Budget Summary
(Dollars in Thousands)
PHS Evaluation Set‐Aside FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
ASPE 41,243 40,963 43,243 +2,280
Health Care Evaluation 12,005 11,920 5,422 ‐6,498
ASFR 495 495 495 ‐
OASH 4,285 4,256 4,285 +29
Teen Pregnancy Prevention Initiative 6,800 6,754 ‐ ‐6,754
Total 64,828 64,388 53,445 ‐10,943
FTE 141 129 129 ‐
ASSISTANT SECRETARY FOR PLANNING AND EVALUATION (ASPE)
Budget Summary (Dollars in Thousands)
Assistant Secretary for Planning and Evaluation
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
PHS Evaluation 41,243 40,963 43,243 +2,280
FTE 141 124 124 ‐
Authorizing Legislation:…………………………………………………………………….43 U.S.C. 241 Public Health Service Act FY 2018 Authorization……………….……………………………………………….....................…..……………….…………..Indefinite Allocation Method……………………………………………….Direct Federal/Intramural, Contracts; Competitive Grants, Cooperative Agreement; Other (Salaries and Expenses, etc.)
Program Description and Accomplishments The Office of the Assistant Secretary for Planning and Evaluation (ASPE) is the principal advisor to the Secretary of HHS on policy development, and is responsible for major activities in policy coordination, legislative development, strategic planning, policy research, evaluation, and economic analysis. ASPE consists of a diverse group of professionals, including economists, statisticians, epidemiologists, lawyers, sociologists, scientists, psychologists and physicians who conduct quick turnaround and longer term policy research and analysis to support leadership decision‐making. ASPE also leads special initiatives on behalf of the Secretary, convenes work groups across the Department, conducts Congressionally mandated studies and evaluations, staffs certain Congressionally mandated federal advisory committees, and leads the Department’s legislative development process. In recent years, ASPE led the development and coordinated the implementation of a Department‐wide initiative to address the opioid epidemic, and currently serves as the HHS lead to coordinate the implementation of the National Action Plan to Combating Antibiotic‐Resistant Bacteria – an Administration‐wide initiative. ASPE also has a central role in behavioral health and works with Substance Abuse and Mental Health Services Administration (SAMHSA), National Institute of Mental Health, and other stakeholders to address serious mental illness. ASPE also leads significant mental health initiatives required by Congress in the 21st Century Cures Act. During a public health emergency or infectious disease outbreak, ASPE participates in efforts led by the Assistant Secretary for

Page 125
Preparedness and Response (ASPR), to ensure that HHS and Administration policies are implemented efficiently and effectively. ASPE works closely with the Administration for Children and Families to identify and test strategies that advance the health, safety, and well‐being of Americans, and is coordinating HHS welfare reform efforts to promote employment, personal responsibility, and economic independence. ASPE research on access to prescription drugs and spending across HHS programs, and international comparisons with other developed countries, is supporting efforts to develop policy options to encourage access, affordability, and innovation. ASPE research has played a central role in HHS efforts to assure that all Americans have access to quality, affordable health care and insurance coverage that works for them and meets their needs. ASPE analyses of regulatory burden have played a central role in the Department’s efforts to reduce burden, put patients first, and increase state flexibility in health insurance markets.
ASPE also maintains a diverse portfolio of intramural and extramural research and evaluation to inform policy formulation and decision‐making regarding the full portfolio of HHS programs. In addition, ASPE maintains a number of simulation models, databases, actuarial support, and other resources to support timely policy analysis and development. In developing research priorities, ASPE consults widely within the Department and the Administration so that it focuses on work that is central to Department priorities. Emphasis is placed on identifying areas for which ASPE work will add value to existing agency efforts and/or fill gaps, and where ASPE’s contributions will be meaningful. Agencies often request that ASPE undertake specific projects to support HHS priorities. Examples include numerous CMS requests on topics such as Medicare post‐acute bundled payments, insurance market simulation models, evaluation of new interventions (like assisted outpatient treatment) to serve people with serious mental illness, and conducting demonstrations to test new models of serving older individuals in home and community‐based settings. ASPE works across the Department, with the Office of Management and Budget, agencies throughout the federal government, and other stakeholders to develop analytic capacity to evaluate federal investments and support evidence‐informed policies. ASPE’s work in these areas is enhanced by participation at all levels in interagency collaborations, and ASPE convenes many operating and staff divisions which provide input on HHS priorities. ASPE also coordinates the development of the quadrennial HHS Strategic Plan. A strategic plan is one of three main elements required by the Government Performance and Results Act (GPRA) of 1993 (P.L. 103‐62) and the GPRA Modernization Act of 2010 (P.L. 111‐352). An agency’s strategic plan defines its mission, goals, and the means by which it will measure its progress in addressing specific national problems over a four‐year period. The following outlines ASPE’s programs and goals in FY 2019. Advance Scientific Knowledge and Innovation In FY 2019, ASPE will continue to use the Strategic Planning System to track progress on the Department’s implementation of the 21st Century Cures Act, as well as other Secretarial priorities. In addition to coordinating and engaging with HHS operating and staff divisions to implement the Act, ASPE will continue to respond to requests from Congress, and develop an overall strategy to evaluate HHS programs that serve people with serious mental illness and other behavioral health needs. Other priority projects under this goal include research and analysis to support regulatory risk assessment and management; the translation of biomedical research into every day health and health care practice; the development and adoption of innovation in health care; and food, drug, and medical

Page 126
product safety and availability. ASPE will build on an existing collaboration with the Food and Drug Administration (FDA), which is characterizing the activities and costs associated with validating new biomarkers for use in drug development. Information gleaned from this project may be useful to inform efforts to encourage biomarker validation, with the goal of facilitating the speed and efficiency of drug development so new therapies reach patients sooner. ASPE is also partnering with FDA on research to assess the costs of clinical trials, with a goal to identify policy interventions to improve the efficiency of the clinical trial process and encourage innovation. ASPE coordinates an HHS‐wide initiative to build data capacity for patient‐centered research. ASPE convenes agency leaders, researchers, data experts, and research networks to collect, link, and analyze real world data for research on a wide spectrum of issues. FY 2019 projects will address Secretarial priorities and may include the opioid epidemic, childhood obesity, serious mental illness, and emergency preparedness.
Coordination of efforts to build data capacity across HHS strengthens its research, analyses, and public reporting programs, while simultaneously reducing unnecessary duplication, inefficiencies, and reporting burdens on patients or health care providers. ASPE leads an HHS‐wide Analytics Team to provide recommendations for strengthening regulatory analysis, and provides technical assistance on regulatory impact analysis development to HHS agencies and offices. ASPE works in close partnership with HHS operating divisions on regulatory priorities and regulatory reform, and with the White House, the Office of Management and Budget, and the Federal Trade Commission to continue efforts to introduce more experimental evidence into decision making in the design of regulations. For example, ASPE has developed guidelines for HHS on analyzing the impact of regulations to improve the transparency and quality of regulatory decision making, and is leveraging the Analytics Team to provide thought leadership on regulatory costs and benefits under the rubric of Regulatory Reform, as newly required by Executive Orders 13771 and 13777. Finally, ASPE convenes and works collaboratively with other HHS operating and staff divisions, and statistical centers, such as Office of National Coordinator for Health Information Technology (ONC), Food and Drug Administration (FDA), Centers for Medicare & Medicaid Services (CMS) and Centers for Disease Control’s (CDC) National Center for Health Statistics (NCHS) to advance the goal of an electronic, nationwide interoperable healthcare system. This includes crafting health IT policies that support the development and use of standardized data to improve patient safety. Two examples of this type of work are ASPE’s contributions to development of FDA’s unique device identifier for tracking medical devices, and the evaluation and development of comparability ratios when converting to new standard data classifications (ICD9‐ICD10) in NCHS national surveys for tracking population health. Advance the Health, Safety and Well‐being of the American People ASPE’s priorities are to provide actionable research to advance the health, safety, and well‐being of Americans through self‐sufficiency and work that supports personal responsibility, independence, economic mobility, and – most importantly – family stability. Support for parents to work and care for their children is reflected in ASPE’s efforts to support workforce development, to examine the barriers in the welfare system to find and keep unsubsidized employment, and improve access to child care. In addition, ASPE evaluates methods to improve access to healthcare, promote the healthy development of children, and increase opportunities for learning and school success. When more help is needed with families at risk, ASPE provides for the study of strategies to improve the safety and well‐being of children involved in the child welfare system, refugee and homeless families, families affected by

Page 127
incarceration, and child support enforcement. ASPE is a leading support for the on‐going research and study of poverty and youth programs. ASPE conducts research on improving access to health care, including researching any economic burdens of the Affordable Care Act, and researching alternatives that will increase choice and competition, as required by Executive Orders 13765 and 13813. ASPE also is examining residential care alternatives for the aged, caregiver support, evidence‐based clinical and community‐based preventive services, mental health and substance use disorder programs, and disparities in health. During public health emergencies and infectious disease outbreaks, ASPE will provide technical and analytic support for policy decision‐making to support ASPR and the Secretary on behalf of individuals, families, and communities. ASPE assembles evidence that is critical to the design of departmental programs, and makes policy and program decisions based on the best available evidence, using data and analysis about the behavior of program participants, what interventions work, for whom, and under what circumstances. In the absence of direct evidence, ASPE uses the evidence‐informed methods (such as well calibrated simulation models) to expand approaches that work and fine‐tune programs and interventions that may have mixed results. Staff work to anticipate potential outcomes of policy actions, what programs and interventions work, improve upon what does not, and understand what actions to take when programs do not demonstrate improvement. In this context, analyses involve a range of information sources including survey data and analyses, program evaluation, analytical models and methods, as well as performance data and scientific evidence generated at multiple levels of study. ASPE’s goal is to work with HHS operating and staff divisions to create a culture of learning to ensure evidence‐based decision‐making is the norm throughout HHS. ASPE also will conduct research and evaluation for important initiatives, such as reducing childhood obesity, increasing economic independence, behavioral health (including early psychosis intervention), and addressing the opioid epidemic. ASPE intends to establish a coordinating function for the Department’s initiative on childhood obesity similar to that which had been established for the opioid epidemic. ASPE coordinates behavioral health parity implementation across HHS and other federal agencies working on parity, notably the Departments of Labor and Treasury. A number of ASPE‐identified action steps were included in the 21st Century Cures legislation, including that the Secretary of HHS host a public meeting on behavioral health parity. ASPE hosted this tri‐Department listening session last summer and will complete an Action Plan this coming year based on the listening session. ASPE leads the Administration’s efforts to combat Alzheimer’s disease and related dementias, including operating the National Advisory Council on Alzheimer’s Research, Care, and Services, which involves all HHS leaders engaged in dementia‐related work, as well as 12 national experts from the private sector. The group produces and updates an annual National Alzheimer’s Plan. At the end of last year, ASPE coordinated Departmental stakeholders, the Advisory Council, outside experts and contractors to convene a national summit on dementia care research on the NIH campus. In the coming year, ASPE will pursue follow up activities from the summit. ASPE also chairs the Interagency Working Group on Youth Programs, established by Executive Order 13459. The Working Group coordinates the activities of 20 federal agencies and offices in order to

Page 128
improve youth outcomes, promote positive youth development and successful transition to adulthood, disseminate evidence‐based practices, and strengthen youth engagement and youth/adult partnerships. Many of these goals are accomplished through the website www.youth.gov, a one‐stop shop for federal information and resources about youth. ASPE participates in interagency workgroups to support the alignment and public reporting of quality measures across HHS programs. One workgroup focuses on public reporting across HHS agencies. A second workgroup focuses on quality measure endorsement and input on the National Quality Strategy. ASPE has partnered with SAMHSA, CMS, and NIMH over the past few years to develop additional quality measures for behavioral health care. The measures address important issues regarding follow‐up after inpatient and emergency room treatment, screening and care for co‐morbid conditions, screening for risk of suicide or other violent behavior, and fidelity to evidence‐based treatments. ASPE has worked together to develop and promote these measures for use in various programs throughout the Department including the meaningful use measures used by the ONC and the reporting requirements used by CMS for the inpatient psychiatric facility prospective payment system in Medicare. In addition, ASPE has worked together to sponsor a study by the Institute of Medicine on developing quality standards for psychosocial interventions. Ensure Efficiency, Transparency, Accountability, and Effectiveness of HHS Programs Specific projects in FY 2019 under this goal include developing metrics for performance measurement, understanding needs of individuals with disabilities, research addressing the new Medicare quality payment program for physicians, and evaluating the impact of social risk factors in Medicare’s quality and resource use measures in value based purchasing programs. ASPE will coordinate HHS data collection and analysis activities; ensure effective long‐range planning for surveys and other investments in major data collection; and will proactively identify opportunities for transparency, data sharing, and dissemination through electronic posting of datasets on healthdata.gov and other means. ASPE maintains several databases, which allow for short‐term monitoring and evaluation of existing and newly‐implemented policies. It also extensively uses unique data sets, acquired from private vendors, to better monitor, evaluate, and track trends in important areas such as prescription drug policies; and employer sponsored health insurance. Additionally, ASPE maintains a small team focused on improving evaluation and the use of evidence across the Department through collaboration, coordination, and consultation with staff and leadership in operating and staff divisions. ASPE provides a number of data products and services that advance these goals in multiple programs. ASPE will continue to lead efforts to leverage HHS administrative data for research, policy, statistical, program and performance management and evidence building purposes. For example, ASPE is conducting a review to identify and document the major privacy issues or other limitations in accessing, using, and sharing administrative data for other purposes. Identification of limitations is a first step in the ability to reform policies, guidance, and procedures for linking administrative data for use in research, evaluation, or program improvement; disseminating results; and making available data sets for public use. This work will support the development of guidance to navigate potential limitations and increase access to administrative data. ASPE also supports the Department in its goals to enhance internal and external information sharing in accordance with privacy and civil liberties policies. ASPE reviews and advises on privacy policy involving

Page 129
the protection of individually identifiable information. Our goals are to ensure fairness and confidentiality while ensuring data is available for research, administration, and policy decision making.
Funding History
Fiscal Year Amount
FY 2014 $53,993,000
FY 2015 $53,743,000
FY 2016 $53,743,000
FY 2017 $41,243,000
FY 2018 Annualized CR $40,963,000
Budget Request The FY 2019 President’s Budget for ASPE of $43,243,000 is $2,280,000 above the FY 2018 Annualized CR. The increase will support the economic analysis and reports on drug pricing, including international drug prices. ASPE anticipates continuing its role in coordinating departmental implementation of the 21st Century Cures Act, given the cross‐cutting nature of the law’s provisions. ASPE plays an important role in providing coordination and department involvement in critical policy decisions related to authorities and mandates affecting HHS agencies with a focus on expediting the discovery, development and delivery of new therapies, making significant reforms to the mental health system, and increasing health care choice, access and quality. ASPE will continue support for a cooperative agreement to address public policy challenges with negative consequences for children, families, and communities. ASPE awards $1,600,000 per year to an academically based poverty research center to provide timely access to high‐quality, reliable research on the causes and consequences of poverty as well as policies and programs to remediate and alleviate poverty and its effects. This cooperative agreement, awarded to one university, harnesses the expertise of over 200 poverty scholars across the U.S. through creation and leadership of poverty research collaborative with other universities. The poverty center program conducts a broad range of research to describe and analyze national, regional, and state environments (e.g., economics, demographics) and policies affecting the poor, particularly families with children who are poor or at risk of being poor. For example, recent work identifies the social determinants of childhood obesity and interventions to reduce it. The Center also focuses on expanding ASPE’s understanding of the causes, consequences, and effects of poverty in local geographic areas, especially in states or regions with high concentrations of poverty such as rural areas, and on improving its understanding of how labor markets as well as family structure and function affect the health and well‐being of children, adults, families, and communities. It also develops and mentors social science researchers whose work focuses on these issues. The Center also hosts regular Learning Exchanges in which HHS leadership discusses implications of the latest policy research with leading research experts.

Page 130
Grants Grants
(whole dollars)
FY 2017 Final FY 2018 Annualized CR FY 2019 President’s
Budget
Number of Awards 1 1 1
Average Award $1,600,000 $1,600,000 $1,600,000
Range of Awards $1,600,000 $1,600,000 $1,600,000

Page 131
PHS EVALUATION HEALTH CARE EVALUATION
Budget Summary (Dollars in Thousands)
Health Care Evaluation FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 12,005 11,923 5,422 ‐6,501
FTE 5 5 5 ‐
Authorizing Legislation: …………….……………………..…………………………………………………………..…....Section 241 PHS Act FY 2019 Authorization…………………………………………….……………………………………………………………………..……….Indefinite Allocation Method………………………………………….………………………………………………………………Direct federal, Contracts
Program Description and Accomplishments The Immediate Office of the Secretary provides leadership, direction, policy, and management guidance to HHS and establishes Department priorities for evaluation of Public Health Service programs. These priorities include evaluating health care program effectiveness across HHS to improve the quality of public health and human service programs. This funding allows the Secretary the necessary flexibility to identify, refine, and implement programmatic and organization goals in response to evolving needs. Findings from the studies supported with these funds serve HHS and the Administration decision makers, as well as state and local government, private sector public health research, education, and practice communities by providing valuable information on the factors contributing to the determinations of how well programs are working. A key priority of the Secretary is to evaluate the effectiveness of HHS investments in data collection and management. Diverse sets of data assets include administrative, research, and public health data, all of which have the potential for tremendous value for program design to HHS and external organizations. These funds would support program review by the Office of the Chief Technology Officer to evaluate the effectiveness of HHS efforts to ensure uniform collection, storage and optimized use of HHS data assets. This effort enables HHS to make the best use of its wealth of data to identify, evaluate, and improve program performance, to prioritize investments, and to improve how HHS measures associated impact. Strengthen Health Care Priority projects for health care evaluation include providing analysis and developing data to measure, monitor, and evaluate the Department’s efforts to stabilize the individual and small group health insurance markets, respect and promote the patient‐doctor relationship, empower patients and promote consumer choice, enhance affordability, return regulatory authority to the states, and reduce unwarranted regulatory and economic burden. The Secretary is also encouraging state innovation to develop patient‐centered reforms to health care delivery, improving health care and nursing home quality, developing innovative payment and delivery systems, analyzing the performance of safety net and workforce distribution programs, identifying the best ways to serve individuals who are dually eligible for Medicare and Medicaid, modernizing Medicare and Medicaid, and improving care delivery in the Indian Health Service.

Page 132
The Secretary will identify key strategies to promote high‐value, consumer‐driven, effective care that lowers total health care cost growth. Priority projects will produce and/or streamline the measures, data, tools, and evidence that health care providers, insurers, purchasers, consumers, and policymakers need to improve the value and affordability of health care and to reduce disparities in costs and quality between population groups and regions. These projects include research required under the IMPACT ACT to determine the relationship between social risk (socioeconomic) factors and quality measures used in Medicare’s value based purchasing programs; research to support the implementation of new physician payment approaches under The Medicare Access and CHIP Reauthorization Act of 2015; and research to support development of post‐acute care payment models required by the IMPACT ACT.
Funding History
Fiscal Year Amount
FY 2014 $0
FY 2015 $0
FY 2016 $0
FY 2017 $12,005,000
FY 2018 Annualized CR $11,923,000
Budget Request The FY 2019 Presidents Budget request for Health Care Evaluation is $5,422,000, a decrease of ‐$6,501,000 below the FY 2018 Annualized CR level of $11,923,000. In FY 2019, the Secretary will proactively respond to the needs of the HHS, as it improves programs and services of the U.S. Public Health Service by evaluating the implementation and effectiveness of these programs, to ensure the return on the investment of program funding through meaningfully leveraging data to enable new insights for targeted interventions and programmatic improvement. The CTO will establish an enterprise level model to operationalize data for Departmental agencies and external stakeholders. Services will include the creation of a data supply chain built on a hybrid data platform – to move, manage, and utilize the ever growing types and amounts of HHS data. CTO will also consolidate and integrate cross‐HHS analytic, visualization, and reporting tools for efficiency, cost control and faster insights, facilitate user training and provide technical assistance on data access and use, enable on‐demand access to data for HHS programs and the private sector, and establish mechanisms that simplify access to databases and data analytics capabilities. The CTO will provide HHS‐wide governance to drive a coherent strategy to consolidate data, reduce duplication, and link data assets, to strengthen program evaluation and performance. Use cases such as the Opioid Epidemic will be leveraged to develop best practices and applications for current needs. In coordination with other HHS offices, the CTO will also establish agency‐wide data standards for interoperability, continuous cataloging, and standardized data use agreements.

Page 133
PHS EVALUATION ASSISTANT SECRETARY FOR FINANCIAL RESOURCES
Budget Summary (Dollars in Thousands)
PHS Evaluation – Assistant Secretary for Financial Resources
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 495 495 495 ‐
FTE ‐ ‐ ‐ ‐
Authorizing Legislation: …………….……………………..…………………………………..........…..…………….......Section 241 PHS Act FY 2018 Authorization……………………………………………………….……………………………………………………………………...Indefinte Allocation Method………………………………………….……………………………..………………………………..Direct federal, Contracts
Program Description and Accomplishments Office of Budget (OB) – OB manages the performance budget and prepares the Secretary to present the budget to the Office of Management and Budget (OMB), the public, the media, and Congressional committees. OB manages the implementation of the Government Performance and Results Modernization Act (GPRAMA) and all phases of HHS performance budget improvement activities.
Funding History
Fiscal Year Amount
FY 2014 $0
FY 2015 $0
FY 2016 $0
FY 2017 $495,000
FY 2018 Annualized CR $495,000
Budget Request The FY 2019 President’s Budget request of $495,000 is the same as the FY 2018 Annualized CR of $495,000. The FY 2019 request will be used to fund program evaluation activities within the ASFR Office of Budget. The Office of Budget manages the implementation of the Government Performance and Results Modernization Act (GPRMA) and all phases of HHS performance budget improvement activities. These funds will cover staff costs focused on program evaluation activities in the preparation of performance reports for OMB, the Congress, and the public. Funds will also go towards the continued development and operation of the electronic Program Performance Tracking System.

Page 134
PHS EVALUATION OFFICE OF THE ASSISTANT SECRETARY FOR HEALTH
Budget Summary (Dollars in Thousands)
PHS Evaluation – Office of the Assistant Secretary for Health
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 4,285 4,256 4,285 +29
FTE ‐ ‐ ‐ ‐
Authorizing Legislation: …………….……………………..…………………………………..........…..…………….......Section 241 PHS Act FY 2019 Authorization……………………………………………………….……………………………………………………………………...Indefinte Allocation Method………………………………………….……………………………..………………………………..Direct federal, Contracts
Program Description and Accomplishments The Office of Assistant Secretary for Health (OASH) performs an essential role in the Public Health Evaluation Set‐Aside program at HHS. Within OASH, the Immediate Office of the Assistant Secretary for Health (ASH) coordinates the Evaluation Set‐Aside program for the ASH. Each fiscal year, OASH program offices submit proposals in an effort to improve and evaluate programs and services of the U.S. Public Health Service, and identify ways to improve their effectiveness. Studies supported by these Set‐Aside funds serve decision makers in federal, state, and local government, and the private sector of the public health research, education, and practice communities by providing valuable information about how well programs and services are working. Projects that were approved for FY 2017 evaluation funds are listed below:
Evaluation of "Pathways to Safer Opioid Use,” an interactive training tool that promotes the safe and effective use of opioids ‐ Demonstrate the effectiveness of the multi‐modal, team based approach to promoting the appropriate, safe and effective use of opioids to manage chronic pain; assess the impact of the training tool on prescribing behaviors and patient engagement; and identify opportunities to improve the training tool.
Healthy People 2020: Monitoring and Assessing Progress in Achieving National Objectives – Assess progress in achieving the Healthy People 2020 (HP2020) targets. Identify population health disparities and gaps in data collection. Identify and communicate evidence‐based practices and programs that support achievement of the HP2020 objectives and address health disparities and social determinants of health.
Developing Healthy People 2030 – continue to initiate the Healthy People 2030 development process by evaluating past iterations of the national objectives and current public health priorities. Establish, convene, and manage the Secretary’s Advisory Committee on National Health Objectives for 2030, charged with advising the Secretary on the context and scope of Healthy People 2030. Garner public input on scope of the next decade’s objectives.
Evaluation of the National Viral Hepatitis Action Plan ‐ Monitor and evaluate the implementation activities by federal partners and others, as described in the Action Plan, and the intersections with the health care delivery system and the opioid abuse epidemic.
Physical Activity Guidelines for Americans 2018 (Phase 2) – Evaluate and coordinate development of Phase 2 of the Physical Activity Guidelines, a multi‐year project spanning FYs 2015 to 2019. Assess past research and establish future evaluative criteria.
U.S. Blood Inventory Network Analysis (BINA) Evaluation ‐ Collect real‐time inventory levels of U.S. blood products throughout the distribution cycle, and collect and analyze day‐to‐day pricing

Page 135
of blood products. Results will inform policy related to the industry‐wide financial crisis occurring in the U.S. blood community.
Organizational Modifications Associated with Improved Care and Health Outcomes for Minority Men with HIV/AIDS ‐ Assess the impact of the HIV/AIDS Initiative for Minority Men (AIMM) on care and health outcomes for minority men and identify modifications in organizational characteristics, practices, and service delivery protocols associated with improved health care delivery and health outcomes.
Evaluation of myhealthfinder ‐ Assess the impact of a personalized preventive service recommendation program (myhealthfinder) for rural primary care patients on the recommended preventive services, and measure performance improvements in preventive services in participating rural practices.
Healthy Aging Summit: State of the Science ‐ Convene national (and, potentially, international experts) to evaluate the current science related to healthy aging that will contribute to the understanding of established evidence‐based strategies to support healthy aging. Evaluation will also identify strategies that require additional research to evaluate their effectiveness and inform future federal activities to integrate resources to advance healthy aging.
Funding History
Fiscal Year Amount
FY 2014 $4,664,000
FY 2015 $4,285,000
FY 2016 $4,285,000
FY 2017 $4,285,000
FY 2018 Annualized CR $4,256,000
Budget Request The FY 2019 President’s Budget request for Office of the Assistant Secretary – PHS Evaluation Set‐Aside is $4,285,000, an increase of $29,000 over the FY 2018 Annualized CR level of $4,256,000. The increase will enable OASH to invest in additional program evaluations. In FY 2019, OASH program offices will submit proposals to improve and evaluate public health programs and identify ways to improve their effectiveness. The evaluation projects will continue to serve decision makers in federal, state, and local government, as well as support OASH priorities and the HHS Strategic Plan.

Page 136
PHS EVALUATION TEEN PREGNANCY PREVENTION
Budget Summary (Dollars in Thousands)
PHS Evaluation ‐ Teen Pregnancy Prevention
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 6,800 6,754 ‐ ‐6,754
FTE ‐ ‐ ‐ ‐
Authorizing Legislation: …………….……………..………………………………………….........................Section 241 of the PHS Act FY 2019 Authorization……………….………………..…………………………..........…..…………...………………………...………..Indefinte Method…………………………………………………………………………………….……….…………………..Direct Federal; Contracts; Grants
Program Description and Accomplishments The Office of Adolescent Health (OAH) supports several evaluation activities to build the evidence base to prevent teenage pregnancy and to support expectant and parenting youth and their families. OAH supports projects that make a significant contribution to these fields including Federal program evaluations, economic evaluations, the provision of rigorous training and technical assistance to evaluation grantees. Additionally, OAH funds research grants and collects and analyzes performance measures.
Funding History
Fiscal Year Amount
FY 2014 $8,455,000
FY 2015 $6,800,000
FY 2016 $6,800,000
FY 2017 $6,800,000
FY 2018 Annualized CR $6,754,000
Budget Request The FY 2019 request does not include funds for the Teen Pregnancy Prevention program. As a result, evaluation funds are not requested.

Page 137
PREGNANCY ASSISTANCE FUND Budget Summary (Dollars in Thousands)
Pregnancy Assistance Fund
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐ FY 2018
Budget Authority 23,275 23,350 25,000 +1,650
FTE 2 2 2 ‐
Authorizing Legislation: …………….………….…………………...Patient Protection and Affordable Care Act, Section 10214 FY 2019 Authorization…..................................................................................................................................FY 2019 Allocation Method…………………….……………………………………………………Direct Federal; Competitive Contracts; Grants
Program Description and Accomplishments The Office of Adolescent Health (OAH) is responsible for administering the Pregnancy Assistance Fund (PAF), a competitive grant program for States and Indian Tribes to develop and implement projects to assist expectant and parenting teens, women, fathers and their families. PAF is authorized by Sections 10211‐10214 of the Affordable Care Act (Public Law 111‐148). The Act appropriates $25,000,000 for each of fiscal years 2010 through 2019 and authorizes the Secretary of the Department of Health and Human Services (HHS), in collaboration and coordination with the Secretary of Education (as appropriate), to establish and administer the PAF program. PAF aims to strengthen access to, and completion of, education (secondary and postsecondary); improve child and maternal health outcomes; increase parenting skills for mothers, fathers, and families; strengthen co‐parenting relationships and marriage where appropriate; increase positive paternal involvement; improve services for pregnant women who are victims of domestic violence, sexual violence or assault, and stalking; and raise awareness of available resources. OAH manages a performance measurement system for all PAF grantees. The most recent data available, collected from August 2016 through July 2017, show that PAF grantees served almost 15,000 participants during the year and partnered with over 1,300 organizations. Of the participants served by PAF grantees, 55% were expectant or parenting mothers, 9% were expecting or parenting fathers, and 36% were children. The majority of participants were 15‐19 years of age – 38% were 17 years or under, 24% were 18‐19 years, 19% were 20‐24 years, and 19% were 25 or older. Overall, 47% of the participants were Hispanic. Almost half (48%) of the participants were white; 32% were Black or African American, 10% were American Indian and Alaska Native, 3% were Asian, and 6% were more than one race. The services most commonly provided were education services, parenting skills, case management, and concrete supports such as food, housing, and clothing. In FY 2017, OAH continued three grants first awarded in FY 2015 for an additional one year project period. Also, in FY 2017, OAH competitively awarded 16 new grants for a one‐year project period. In FY 2018, OAH will award a new cohort of competitive grants to States and Tribes for a two‐year project period. These new grants are expected to begin in summer 2018. FY 2019 funds will support the second and final year of these new FY 2018 grants. The additional $1.650 million in FY 2019 dollars will be used to fund 2‐3 new grantees.

Page 138
Funding History
Fiscal Year Amount
FY 2014 $23,200,000
FY 2015 $23,175,000
FY 2016 $23,300,000
FY 2017 $23,275,000
FY 2018 Annualized CR $23,350,000
Budget Request The FY 2019 President’s Budget request for PAF of $25,000,000 is $1,650,000 over the FY 2018 Annualized CR level of $23,275,000. FY 2019 funds will be used to support the second and final year of a new cohort of competitive grants to States and Tribes that will be awarded in summer 2018 for a two‐year project period. The additional $1,725,000 represents amounts to be sequestered in FY 2019. The FY 2019 level will continue to support project management, training, and technical assistance for the PAF grantees. The FY 2019 budget request also supports a portion of the OAH Strategic Communications contract to maintain the general OAH portions, as well as the PAF portion of the OAH website.

Page 139
Department of Health and Human Services Office of the Assistant Secretary for Health
FY 2019 Discretionary State Grants Pregnancy Assistance Fund (PAF)
State/Territory FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Level
FY 2019 President’s Level
+/‐ FY 2018 Annualized CR
California Department of Public Health
$1,360,939.61 - - -
Children’s Trust Fund of South Carolina
$1,360,939.61 - - -
Executive Office of the State of New Jersey
$1,360,939.61 - - -
Health Research, Inc. (New York) $1,304,608.61 - - - Iowa Department of Public Health
$1,350,591.96 - - -
Kansas Department of Health and Environment
$1,153,249.11 - - -
Massachusetts Department of Public Health
$1,360,939.61 - - -
Michigan Department of Health and Human Services
$1,360,939.61 - - -
Minnesota Department of Health $1,360,938.69 - - - Mississippi State Department of Health
$636,825.79 - - -
Missouri Department of Elementary and Secondary Education
$637,888.00
- - -
New Hampshire Department of Education
$381,731.00 - - -
Oklahoma State Health Department
$1,360,938.69 - - -
Oregon Department of Human Services
$1,360,938.69 - - -
Pennsylvania Department of Health
$811,152.42 - - -
Riverside‐San Bernardino County Indian Health
$709,547.77 - - -
Virginia State Board of Health $1,360,398.59 - - - Washington State Department of Health
$1,360,938.69 - - -
Wisconsin Department of Public Instruction
$1,360,938.69 - - -
New Grant Awards – TBD $23,350,000 $25,000,000 ‐
Subtotal States/Tribes $21,955,384.75 $23,350,000 $25,000,000 ‐
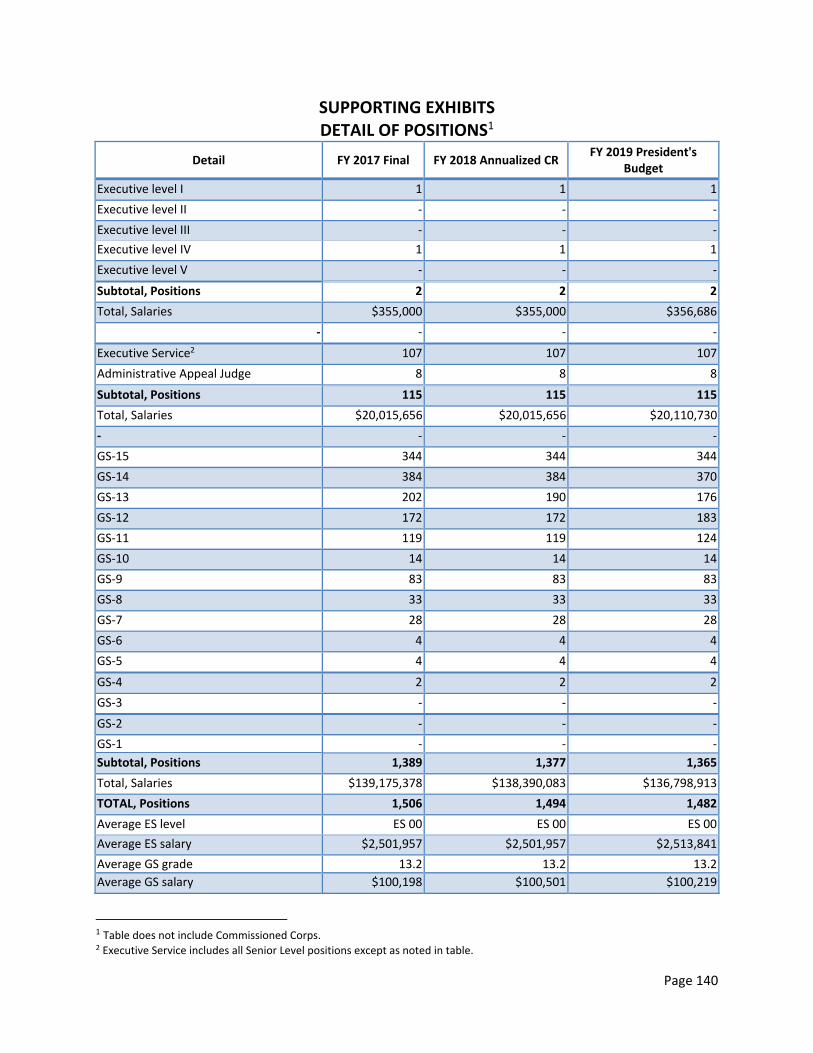
Page 140
SUPPORTING EXHIBITS DETAIL OF POSITIONS1
Detail FY 2017 Final FY 2018 Annualized CR FY 2019 President's
Budget
Executive level I 1 1 1 Executive level II ‐ ‐ ‐
Executive level III ‐ ‐ ‐
Executive level IV 1 1 1
Executive level V ‐ ‐ ‐
Subtotal, Positions 2 2 2
Total, Salaries $355,000 $355,000 $356,686
‐ ‐ ‐ ‐
Executive Service2 107 107 107 Administrative Appeal Judge 8 8 8
Subtotal, Positions 115 115 115
Total, Salaries $20,015,656 $20,015,656 $20,110,730
‐ ‐ ‐ ‐
GS‐15 344 344 344
GS‐14 384 384 370
GS‐13 202 190 176
GS‐12 172 172 183
GS‐11 119 119 124
GS‐10 14 14 14
GS‐9 83 83 83
GS‐8 33 33 33
GS‐7 28 28 28
GS‐6 4 4 4
GS‐5 4 4 4
GS‐4 2 2 2
GS‐3 ‐ ‐ ‐
GS‐2 ‐ ‐ ‐
GS‐1 ‐ ‐ ‐
Subtotal, Positions 1,389 1,377 1,365
Total, Salaries $139,175,378 $138,390,083 $136,798,913
TOTAL, Positions 1,506 1,494 1,482
Average ES level ES 00 ES 00 ES 00
Average ES salary $2,501,957 $2,501,957 $2,513,841 Average GS grade 13.2 13.2 13.2
Average GS salary $100,198 $100,501 $100,219
1 Table does not include Commissioned Corps. 2 Executive Service includes all Senior Level positions except as noted in table.
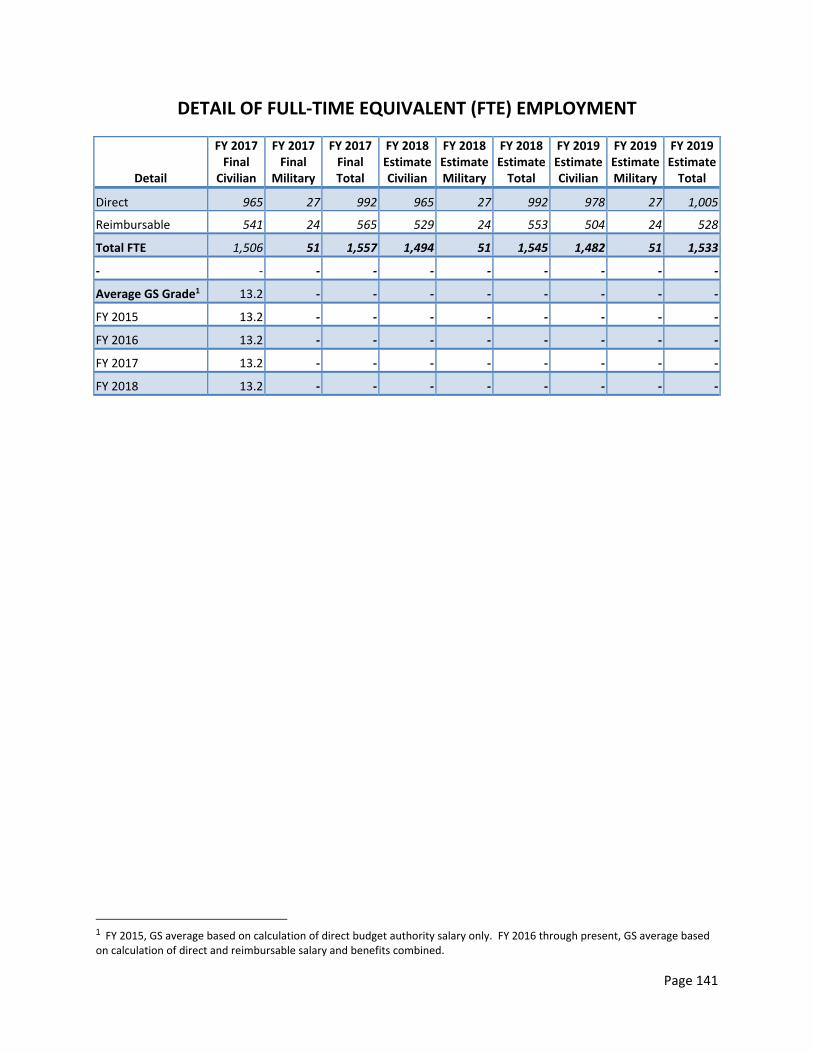
Page 141
DETAIL OF FULL‐TIME EQUIVALENT (FTE) EMPLOYMENT
Detail
FY 2017 Final
Civilian
FY 2017 Final
Military
FY 2017 Final Total
FY 2018 Estimate Civilian
FY 2018 Estimate Military
FY 2018 Estimate Total
FY 2019 Estimate Civilian
FY 2019 Estimate Military
FY 2019 Estimate Total
Direct 965 27 992 965 27 992 978 27 1,005 Reimbursable 541 24 565 529 24 553 504 24 528
Total FTE 1,506 51 1,557 1,494 51 1,545 1,482 51 1,533
‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
Average GS Grade1 13.2 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
FY 2015 13.2 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
FY 2016 13.2 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
FY 2017 13.2 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
FY 2018 13.2 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
1 FY 2015, GS average based on calculation of direct budget authority salary only. FY 2016 through present, GS average based on calculation of direct and reimbursable salary and benefits combined.

Page 142
FTEs Funded by the Affordable Care Act (Dollars in Thousands)
Program Section FY
2010 FY
2011 FY
2012 FY
2013 FY
2014 FY
2015 FY
2016 FY
2017 FY
2018 FY
2019
Pregnancy Assistance Fund Discretionary P.L. (111‐148)
Section 10214
25,000 25,000 25,000 22,825 23,200 23,275 23,300 23,275 23,350 25,000
Full Time Equivalents
‐ 2 2 2 2 2 2 2 2 2 2

Page 143
STATEMENT OF PERSONNEL RESOURCES Total Full‐Time Equivalents
Detail FY 2017 Target
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President's Budget
Direct Ceiling FTE 1,036 992 992 1,005
Reimbursable Ceiling FTE 565 565 553 528
Total Ceiling FTE 1,601 1,557 1,545 1,533
Total Civilian FTE 1,550 1,506 1,494 1,482
Total CC FTE 51 51 51 51

Page 144
RENT AND COMMON EXPENSES (Dollars in Thousands)
Details FY 2017 Final FY 2017
Annualized CR
FY 2018 President's Budget
FY 2019 +/‐
FY 2018
Rent ‐ ‐ ‐ ‐ GDM1 8,703 8,792 8,792 ‐ OGA 505 505 505 ‐
OGC 2,100 2,100 2,100 ‐
OASH 4,416 4,434 4,226 ‐208
Subtotal 15,724 15,831 15,623 ‐208
Operations and Maintenance ‐ ‐ ‐ ‐ GDM2 3,681 3,777 3,793 +16 ASA 268 271 271 ‐ ASFR 299 299 299 ‐
DAB 41 41 63 +22
OGA 218 177 218 +41
OGC 1,412 1,412 1,412 ‐ OASH 1,728 1,732 1,725 ‐7
Subtotal 7,647 7,709 7,781 +72
Service and Supply Fund ‐ ‐ ‐ ‐ GDM Shared Services 7,210 7,161 7,210 +49 GDM3 3,482 3,411 3,504 +93
ASA 2,120 2,226 2,337 +111
ASFR 5,436 5,708 5,993 +285 DAB 1,113 1,168 1,227 +58 OGA 965 1,014 1,064 +51 OGC 6,972 7,321 7,687 +366
OASH 7,527 7,903 8,299 +395
Subtotal 27,615 28,751 30,111 +1,360
1 GDM Rent covers expenses for STAFFDIVs except as noted in the tables. 2 GDM Rent covers expenses for STAFFDIVs except as noted in the tables. 3 GDM Rent covers expenses for STAFFDIVs except as noted in the tables.

Page 145
PHYSICIANS’ COMPARABILITY ALLOWANCE (PCA)
Office of the Assistant Secretary for Planning and Evaluation
Physician Categories FY 2017
Final
FY 2018 Annualized CR
FY 2019 President’s Budget
1) Number of Physicians Receiving PCAs 1 1 1
2) Number of Physicians with One‐Year PCA Agreements 0 0 0
3) Number of Physicians with Multi‐Year PCA Agreements 1 1 1
4) Average Annual PCA Physician Pay (without PCA payment) 160,300 160,300 160,300
5) Average Annual PCA Payment 30,000 30,000 30,000
6) Number of Physicians’ Receiving PCA’s by Category (non‐add) Category I Clinical Position 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category II Research Position 1 1 1
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category III Occupational Health 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category IV‐A Disability Evaluation 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category IV‐B Health and Medical Admin. 0 0 0 The Office of the Assistant Secretary for Planning and Evaluation (ASPE) offers physicians filling the Category II Research positions the maximum of $30,000 per employee. This physician provides expert medical advice and analysis on ASPE topics relating to medical care, informatics, and the management of chronic conditions and access of HHS data. The qualifications of this medical expert provide an exceptional level of skill, expertise and experience necessary to support the ASPE office’s initiatives. ASPE has traditionally had difficulty in recruitment of research and informatics physicians. The last recruitment in ASPE resulted in only three candidates; most were not a good fit. ASPE has had to pursue other avenues for physicians such as short term Intergovernmental Personnel Act (IPA) employees through universities which often result in higher costs. Recruiting physicians at the GS salary schedule would prove to be challenging without the ability to offer the PCA incentive, which assists in obtaining the qualifications and expertise useful to ASPE’s efforts.

Page 146
PHYSICIANS’ COMPARABILITY ALLOWANCE (PCA) ‐ OASH
Office of the Assistant Secretary for Health
Physician Categories FY 2017
Final
FY 2018 Annualized CR
FY 2019 President’s Budget
1) Number of Physicians Receiving PCAs 9 15 15
2) Number of Physicians with One‐Year PCA Agreements 1 2 2
3) Number of Physicians with Multi‐Year PCA Agreements 8 13 13
4) Average Annual PCA Physician Pay (without PCA payment) 160,300 163,185 166,122
5) Average Annual PCA Payment 24,022 24,014 24,014
6) Number of Physicians’ Receiving PCA’s by Category (non‐add) Category I Clinical Position 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category II Research Position 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category III Occupational Health 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category IV‐A Disability Evaluation 0 0 0
Number of Physicians’ Receiving PCA’s by Category (non‐add) Category IV‐B Health and Medical Admin. 9 15 15
There is a shortage of qualified licensed medical doctors federal government‐wide. OASH leads initiatives that require the qualifications and experience of licensed physicians (i.e., Zika, immunization, disease prevention, as well as a host of presidential and secretarial federal advisory committees to focus on health disparities, opioid addiction, chronic fatigue, etc.). The use of PCA and direct hire granted by OPM affords OASH the ability to compete with the private sector to attract and retain licensed medical doctors. OASH typically loses 2 plus highly qualified physicians per year due to competing offers from the private sector. Most positions go unencumbered for a period of not less than 6 months. OASH averages about 2 accessions (medical officers) per year. OASH consistently monitors staffing levels to include planned and unplanned vacancies. Succession planning is based on current and projected needs which align with the priorities of the Secretary and Department.

Page 147
Grants.Gov The following is presented pursuant to Sections 737(b) and (d) of the Consolidated Appropriations Act of 2008 (P.L. 110‐161). The Assistant Secretary for Financial Resources (ASFR) manages the Grants.gov program on behalf of the 26 federal grant‐making agencies. Grants.gov is the Federal government’s hub for grant applications and information on over 1,000 grant programs and approximately $120 billion awarded by the agencies and other organizations. The program enables federal agencies to publish grant funding opportunities and application packages online, while allowing the grant community of over one million organizations (state, local, and tribal governments, education and research organizations, non‐profit organizations, public housing agencies, and individuals) to search for opportunities, and download, complete, and electronically submit applications. Through the use of Grants.gov, the agencies are able to provide the public with increased access to government grant programs, and are able to reduce operating costs associated with online posting and application of grants. Additionally, agencies are able to improve their operational effectiveness through the use of Grants.gov, by increasing data accuracy and reducing processing cycle times. The initiative provides benefits to the following agencies:
Department of Agriculture
Department of Commerce
Department of Defense
Department of Education
Department of Energy
Department of Health and Human Services
Department of Homeland Security
Department of Housing and Urban Development
Department of the Interior
Department of Justice
Department of Labor
Department of State
U.S. Agency for International Development
Department of Transportation
Department of the Treasury
Department of Veterans Affairs
Environmental Protection Agency
National Aeronautical and Space Administration
National Archives and Records Administration
National Science Foundation Small Business Administration
Social Security Administration
Corporation for National Community Service
Institute of Museum and Library Services
National Endowment for the Arts

Page 148
National Endowment for the Humanities From its inception in 2003, Grants.gov has transformed the federal grants environment by streamlining and standardizing public‐facing grant processes, thus facilitating an easier application submission process for our applicants. The Grants.gov Program Management Office (PMO) works with agencies on system adoption, utilization, and customer satisfaction. RISK MANAGEMENT OVERVIEW: Risks are categorized and prioritized to facilitate and focus risk management activities. Risk categories are aligned with OMB risk management guidance, ensuring comprehensive consideration of possible risks and simplifying program reporting. Risk prioritization is based on the probability of occurrence and potential impact, and focuses project resources where they are most needed. All risks are tracked in the Grants.gov Risk Management Database, from identification through resolution. This online database is accessible to all Grants.gov team members and is updated regularly, in keeping with a continuous risk management process. Although physically separate, the Risk Management Database is considered an integral part of the Grants.gov Risk Management Plan. Risks are categorized to facilitate analysis and reporting. The Grants.gov risk categories are aligned with Office of Management and Budget (OMB) guidance on risk assessment and mitigation. The risk category describes potentially affected areas of the program, and helps put individual risks into context when assessing their severity. The categories are also used to drive risk identification: the lack of identified risks in a given category may indicate overlooked risks. The following risks have been identified to OMB: Risk 1: The global financial crisis of 2008 has dramatically reduced federal revenues and increased the federal deficit. Widespread calls to reduce federal spending could result in decreased funding for Grants.gov. The Grants.gov PMO operations, funded entirely by agency contributions, include: salaries and expenses for full‐time staff, and support contracts for system integration, hardware platforms, upgrades, software licenses, Independent Verification and Validation, outreach and liaison, contact center, performance metrics monitoring, and office support. If the PMO does not receive sufficient funding, or if the agency contributions are not provided in a timely manner, the PMO would have to limit or stop providing the services it offers to its stakeholders. Risk mitigation response: Grants.gov risk mitigation is a multifaceted approach that includes internal actions as well as external entities. Internally, the PMO times the majority of its contract actions toward the third and fourth quarters of the fiscal year, to accommodate the speed of incoming contributions. Additionally, if sufficient funding is not available, the PMO can reduce the scope of its contracts, reprioritize contract awards, and/or postpone awarding of contracts. All contract actions and award decisions are made in the context of ensuring full, reliable functionality of the Grants.gov system. The PMO closely monitors contract expenditures, and PMO activities such as training and travel expenditures, to ensure the available budget will cover the actual expense. By the end of the first quarter, the PMO develops and sends documentation to each funding agency to initiate funding transfers and then reports (monthly) the status of agency contributions to the Financial Assistance Committee for E‐Government (FACE), and OMB. Risk 2: A fundamental concept of electronic commerce is the standardization of a common set of terms to be used by trading partners during business communications. Grants.gov requires common data

Page 149
processes in order to function. The inability to define common data and processes could impede program goals. Risk mitigation response: The Grants.gov system was developed in accordance with the electronic standards for core grants data, Transaction Set 194, which were developed by the Inter‐Agency Electronic Grants Committee (IAEGC). The Grants.gov PMO worked with the PL 106‐107 workgroup and IAEGC to build consensus, and continues to work to minimize the required changes to agency and applicant processes. Agencies are being encouraged to simplify their forms and, if possible, develop a common set of forms and data definitions. To meet that goal, Grants.gov is consolidating already existing forms and working with Agencies for adoption to avoid duplicate forms used across the agencies. Grants.gov is also working to ensure compliance with DATA Act and Uniform Guidance requirements as they are finalized. FUNDING: The total development cost of the Grants.gov initiative by fiscal year ‐‐ including costs to date, estimated costs to complete development to full operational capability, and estimated annual operations and maintenance costs ‐‐ are included in the table below. Also included are the sources and distribution of funding by agency, showing contributions to date and estimated future contributions through FY 2019.

Page 150
GRANTS.GOV FY 2017 to FY 2019 Agency Contributions
Agency Total Total Total
FY 2017 FY 2018 FY 2019
CNCS 32,271 38,725 31,320
DHS 213,357 165,519 202,102
DOC 283,833 307,784 342,232
DOD 704,902 736,560 755,095
DOE 446,964 354,285 410,979
DOI 1,750,200 1,848,290 1,933,644
DOL 191,911 151,052 152,190
DOS 377,976 452,184 451,018
DOT 226,825 187,918 216,587
ED 427,881 391,690 321,448
EPA 217,262 307,283 275,652
HHS 6,073,905 6,193,979 6,315,818
HUD 172,882 119,797 201,977
IMLS 81,723 94,664 96,506
NARA 37,443 37,005 38,792
NASA 107,516 146,187 103,383
NEA 232,436 278,923 324,578
NEH 216,601 259,921 256,841
NSF 263,279 263,798 233,849
SBA 66,497 61,413 63,924
SSA 25,000 30,000 25,895
USAID 230,637 192,847 139,162
USDA 516,493 493,961 473,087
USDOJ 440,794 467,787 458,850
USDOT 76,462 83,806 91,396
VA 82,518 99,022 118,826
Grand Total 13,497,568 13,764,400 14,035,151

Page 151
Centrally Managed Projects The GDM Staff Divisions are responsible for administering certain centrally managed projects on behalf of all Operating Divisions in the Department. Authority for carrying out these efforts is authorized by either specific statute or general transfer authority (such as the Economy Act, 31 USC 1535). The costs for centrally managed projects are allocated among the Operating Divisions in proportion to the estimated benefit to be derived.
Project Description FY 2018 Funding
The Digital Accountability and Transparency Act
The funds will focus on developing a strategy and laying the groundwork to begin incorporating agreed upon standards into the Department of Health and Human Services’ policies, processes and systems to ensure full compliance with the Digital Accountability and Transparency Act.
$1,950,000
Department‐wide CFO Audit of Financial Statements
These funds cover the costs of auditing the HHS financial statements annually (as required by the CFO Act of 1990), and stand‐alone audit of CMS, producing Department‐wide financial statements, and coordinating the HHS audit process, including costs for FISMA.
$15,711,756
Bilateral and Multilateral International Health Activities
These funds support activities by the Office of Global Affairs in leading the U.S. government’s participation in policy debates at multi‐lateral organizations on health, science, and social welfare policies and advancing HHS’s global strategies and partnerships, and working with USG agencies in the coordination of global health policy and setting priorities for international engagements.
$6,603,001
Regional Health Administrators The RHAs provide senior‐level leadership in health, bringing together the Department’s investments in public health and prevention by providing a health infrastructure across the ten HHS regions. Particularly in the areas of prevention, preparedness, coordination and collaboration, the RHAs represent the Secretary, Assistant Secretary for Health, and Surgeon General in the Regions, and are key players in managing ongoing public health challenges.
$2,772,090
National Science Advisory Board for Bio‐Security (NSABB)
Funds will be used by the NSABB for providing guidance on ways to enhance the culture of responsibility among researchers, developing strategies for enhancing interdisciplinary bio‐security, recommending outreach strategies, engaging journal editors on policies for review, continuing international engagement, and develop Federal policy for oversight of life sciences research at the local level based on recommendations of the NSABBS.
$2,672,000
Tick‐Borne Disease Working Group
The Tick‐Borne Disease Working Group requires Department‐wide responsibility across Agencies with an interest in relevant aspects of Tick‐Borne Diseases. The Office of the Assistant Secretary for Health (OASH) shall establish, convene, coordinate, and support the Tick‐Borne Federal Advisory Committee for ongoing tick‐borne
$600,000

Page 152
research, programs, and policies, including those related to causes, prevention, treatment, surveillance, diagnosis, diagnostics, duration of illness, and intervention of individuals with tick‐borne diseases. The Working Group is an established requirement of the 21st Century Cures Act.
Secretary’s Advisory Committee on Blood Safety and Availability
The Committee advises the Secretary on a broad range of public health, ethical and legal issues related to blood transfusion and transplantation safety. Such issues require coordination across many of the Operating Divisions. Funds support Committee meetings, workshops, staff, and subject matter experts.
$1,500,000
President’s Commission for the Study of Bioethical Issues
The Commission, created by Executive Order 13521 on November 24, 2009, replaced the President’s Council on Bioethics. Its purpose is to advise the President on bioethical issues that may emerge as a consequence of advances in biomedicine and related areas of science and technology. Funding for the Council comes entirely from HHS.
$3,000,000
Pain Management Interagency Task Force
The Comprehensive Addiction and Recovery Act, P.L. 114‐198, charges the HHS, in cooperation with VA, DOD, and the DEA, to coordinate and lead the establishment of a Pain Management Best Practices Interagency Task Force. The Task Force shall review gaps in or inconsistencies between best practices for pain management (including chronic and acute pain); and propose updates, as necessary.
850,000
NIH Negotiation of Indirect Cost Rates
At the request of Operating Divisions, NIH has expanded its capacity to negotiate indirect cost rates with commercial (for‐profit) organizations that receive HHS contract and/or grant awards, to ensure that such indirect costs are reasonable, allowable, and allocable.
$1,203,000
Intradepartmental Council on Native American Affairs
These funds will be used for continued support of HHS‐wide tribal consultation; support new initiatives such as tribal emergency preparedness, suicide prevention and the HHS American and Alaska Native Health Research Advisory Council, and to continue to serve as the HHS focal point for Native American Health and Human Services.
$383,183
Chronic Fatigue Syndrome Advisory Committee (CFSAC)
CFSAC provides expertise in biomedical research in the area of CFS, health care delivery services, insurers and voluntary organizations concerned with the problems of individuals with CFS. They meet on research, patient care, education, and quality of life for persons with CFS.
$100,000
HHS Biosafety and Biosecurity Coordinating Council
The work of the Council will support HHS efforts to confront threats posed by the accidental or deliberate release of high‐consequence biological agents or toxins, and aligns with the principles articulated in the National Health Security Strategy; the National Strategy for Countering Biological Threats, and Executive Order 13546 (Optimizing the Security of Select Agents and Toxins).
$317,476

Page 153
President’s Advisory Council on Combating Antibiotic‐Resistant Bacteria
Executive Order 13676 directs the Secretary of Health and Human Services to establish the Advisory Council in consultation with the Secretaries of Defense and Agriculture. The Council also provides advice on programs and policies to preserve the effectiveness of antibiotics, to strengthen surveillance of antibiotic‐resistant bacterial infections, and the dissemination of up‐to‐date information on the appropriate and proper use of antibiotics to the general public and human and animal healthcare providers.
$1,125,000

Page 154
SIGNIFICANT ITEMS IN HOUSE, AND SENATE APPROPRIATIONS COMMITTEES
REPORTS
House Report 115-244
Breastfeeding The Committee recognizes the importance of breast milk in improving health outcomes for babies and mothers and requests HHS to report to the Committee on the impact of recommended breastfeeding rates on health outcomes and healthcare costs. The report should examine the impact of clinically recommended breastfeeding rates on associated Medicaid expenditures, urgent care costs, and direct and indirect medical costs, including workplace productivity and employee retention. The Committee also directs the Secretary to ensure that pregnant women have access to guidance on nutritional advice based on the latest scientific research on the health and cost benefits of human milk. Action taken or to be taken The Department of Health and Human Services (HHS) continues to support efforts to promote access to nutritional guidance on the benefits of breastfeeding on health outcomes. The HHS Office on Women’s Health (OWH) recently worked with Department agencies, including the Centers for Disease Control and Prevention (CDC) and the Agency for Healthcare Research and Quality (AHRQ) to conduct a systematic review and report on breastfeeding outcomes for mothers. They examine the most recent literature on the topic, with a specific focus on maternal outcomes related to breastfeeding, and programs and policies in highly and very highly developed countries designed to improve the rate and duration of breastfeeding. The premise of this research review and report is to build on current research and study which indicates that breastfeeding improves health outcomes for mothers and babies. The review and report focused on programs and strategies which documented best practices in breastfeeding and encourage women to start and continue breastfeeding their babies. The draft report, Breastfeeding Programs and Policies, Breastfeeding Uptake, and Maternal Health Outcomes in Developed Countries, published by AHRQ describes the findings from this systematic review. The report was posted online for public comment ending in January 2018. AHRQ will review the comments received. OWH anticipates that the review will be finalized, and the report will be published late Spring 2018.
The Department also continues to promote Supporting Nursing Moms at Work: Employer Solutions, an initiative designed to provide information, education, and resources to employers, to help them provide time and space solutions and support for lactating mothers upon their return to the workplace. Managed by OWH, this comprehensive online solutions-based project includes a compendium of successful model programs that demonstrate how employers in various industry groups utilize innovative and creative methods and strategies to overcome barriers and provide breastfeeding support particularly for workers in non-traditional, non-office worksite settings. Examples of these non-traditional worksite settings include manufacturing, retail, restaurants, and agriculture.

Page 155
Finally, OWH maintains a national breastfeeding helpline call center. The Call Center refers and provides information and resources to individuals in need of health-related advice, as well as providers, practitioners, and organizational representatives looking to obtain information. The Call Center currently receives approximately 5,000 calls per year referring callers with targeted information and resources on breastfeeding and a range of other women’s health issues.
Senate Report 115-150
Combating Antibiotic Resistant Bacteria (CARB) The Committee supports the CARB initiative that strengthens efforts to prevent, detect, and control illness and deaths related to infections caused by antibiotic resistant bacteria. The Committee directs the Department to continue to work with DOD, USDA, VA, and FDA to broaden and expand efforts to track and store both antibiotic resistant bacteria genes and the mobile genetic elements from antibiotic resistant bacteria along with metadata. The Committee also recognizes the importance of basic and applied research toward the development of new vaccines as a way to prevent future antibiotic resistance through infection prevention and control. The Committee encourages the Secretary to prioritize this research as part of its strategy to combat antibiotic resistance. The Committee also urges the Secretary to consider the use of existing vaccines in antibiotic stewardship efforts to help mitigate new resistance development. The Department shall include in the fiscal year 2019 Congressional Justification a detailed update on the progress being made to implement the CARB national strategy. Action taken or to be taken Antibiotic resistance poses a significant threat to our Nation’s public health. Many advances in medical treatment—like our ability to effectively treat patients with sepsis, cancer, organ transplants, burns, or trauma— and our ability to treat patients exposed to CBRN agents depend on the use of antibiotics to fight infections. To coordinate and enhance the public health response to the AR threat, the U.S. Government developed the National Action Plan for Combating Antibiotic-Resistant Bacteria (CARB). The CARB Task Force is co-chaired by HHS, the U.S. Department of Agriculture, and the U.S. Department of Defense. In the past two years, the U.S. made significant progress toward improving antibiotic use in human health, preventing the spread of resistant infections, and slowing the emergence of resistant bacteria through improving antibiotic stewardship, surveillance, and research. The National Action Plan on Combating Antibiotic-Resistant Bacteria (CARB) provides a five-year roadmap to guide the nation in reducing the prevalence of antibiotic-resistant bacteria by:
Slowing the emergence of resistant bacteria and preventing the spread of resistant infections.
Strengthening national surveillance efforts to combat resistance. Advancing development and use of rapid and innovative diagnostic tests for
identification of resistant bacteria. Accelerating research and development for new antibiotics, other therapeutics, and
preventive strategies, including vaccines.

Page 156
Improving international collaboration and capacities for antibiotic-resistance prevention, surveillance, control and antibiotic research and development.
The federal government has been working diligently to implement the Plan since its release in 2015. As part of U.S. Antibiotic Awareness Week, November 13-19, 2017, HHS, on behalf of the Interagency CARB Task Force, has released a Progress Report to detail the significant progress made during the first two years of implementation of the National Action Plan. Highlights of the Progress Report include:
The percentage of U.S. hospitals reporting antibiotic stewardship programs using CDC’s Core Elements for Stewardship rose to 64 percent in 2016, up from 46 percent in 2015. The goal is to reach 100 percent by 2020.
Methicillin-resistant Staphylococcus aureus (MRSA) in acute care hospitals declined by 13 percent between 2011 and 2014, and by a further 5 percent by 2016. C. difficile infections declined in acute care hospitals by 8 percent between 2011 and 2014, and by a further 7 percent by 2016.
CDC established the Antibiotic Resistance Laboratory Network, enhancing lab capacity to better detect, respond to, and contain, resistance and resistant infections. CDC has invested in labs in all 50 states, five large cities and Puerto Rico to detect and respond to CRE, “the nightmare bacteria.” CDC has also established seven regional labs to detect and support response to resistant organisms recovered from human samples.
Since the National Action Plan was released in March 2015, NIH has provided support to investigators through multiple funding opportunities and access to a wide array of preclinical resources designed to facilitate new drug development. These efforts are greatly expanding the pipeline of new drug candidates, at various stages of development, to treat antibiotic-resistant infections. In particular, the NIH-supported Antibacterial Resistance Leadership Group is pioneering an innovative clinical research agenda on antibacterial resistance.
As of April 2017, USDA’s Animal and Plant Health Inspection Service for the first time has begun conducting antibiotic use monitoring, resistance surveillance, and antimicrobial use surveys of beef feedlots and swine farms. These data are critical to understanding the relationships between antibiotic use and resistance in animals and humans.
In the past two years, FDA approved, cleared or granted marketing authorization for marketing several new diagnostic devices that may significantly enhance detection or prevention of antibiotic resistance.
Last year, NIH and the Biomedical Advanced Research and Development Authority (BARDA), in the Office of the Assistant Secretary for Preparedness and Response (ASPR), launched the Antimicrobial Resistance Diagnostic Challenge, which seeks tests that identify antibiotic-resistant bacteria or that distinguish between viral and bacterial infections to reduce unnecessary use of antibiotics.
The Multidrug-Resistant Organism Repository and Surveillance Network at the Walter Reed Army Institute of Research offers an almost unprecedented 48-hour turn-around time to all DOD hospitals for next generation sequencing to support outbreak investigations and has similar services available to non-DOD institutions.
In July of 2016, ASPR/BARDA launched CARB-X, a five-year, $450 million public-private partnership between BARDA, NIH, and the Wellcome Trust aimed at bolstering

Page 157
innovation in antibacterial product development. As of November 2017, CARB-X had granted awards to 23 biotech companies and research teams for drug discovery and development projects to tackle antibiotic resistance.
Diabetes The Committee urges the Secretary to convene a commission comprised of healthcare providers, patient advocates and Federal agencies that operate programs that impact the care of people with pre-diabetes and diabetes. The goal of such a commission would be to make recommendations about developing improved clinical resources and tools, innovative care models, quality measures and registries, diabetes screening programs and other prevention activities. Action taken or to be taken The Department of Health and Human Services (HHS) takes seriously the care of clinical resources and care available to individuals impacted by pre-diabetes and diabetes. The HHS Office of the Assistant Secretary of Health will establish a commission to make recommendations to the Secretary about developing improved clinical resources and tools, innovative care models, quality measures and registries, diabetes screening programs and other prevention activities. The Department anticipates convening the first meeting of the new commission in summer or fall of 2018. The Office of Disease Prevention and Health Promotion (ODPHP) is the lead organization overseeing this effort. Within ODPHP, the Division of Healthcare Quality promotes prevention of hypoglycemia due to diabetes agents through its collaboration with other HHS agencies on surveillance, research, and incentives and oversight of Adverse Drug Events. It oversees national measures and targets for hypoglycemia prevention in both inpatient and outpatient settings providing diabetes care. Making Eye Health a Population Health Imperative: Vision for Tomorrow The Committee commends the National Academies of Sciences, Engineering, and Medicine for the September 2016 release of its report "Making Eye Health a Population Health Imperative: Vision for Tomorrow" which includes recommendations regarding continued leadership by HHS to reduce the burden of vision impairment. The Committee requests an update from the Secretary regarding HHS' progress in implementing these recommendations in the fiscal year 2019 Congressional Justification. Action taken or to be taken At the 2017 annual meeting of the Association for Research in Vision and Ophthalmology, the largest and most respected eye and vision research organization in the world, the National Eye Institute (NEI) sponsored a broad public special interest group discussion on the National Academies of Sciences, Engineering, and Medicine (NASEM) report, at which panelists addressed the context of the report and its implications, as well as potential collaborations. An HHS working group, led by NEI and the Centers for Disease Control and Prevention (CDC), meets regularly to discuss and prioritize potential initiatives based on their potential public health impact and on available resources.

Page 158
The report recommends a coordinated public awareness campaign to promote eye and vision health across the lifespan. This aligns with the NEI-run National Eye Health Education Program (NEHEP).1 NEHEP oversees public and professional education programs and public awareness campaigns designed to (1) reach populations at higher risk for eye disease and vision loss, (2) to reduce health disparities, and (3) to promote the use of vision rehabilitation services. The NEHEP Partnership is made up of 65 national organizations, including CDC and other HHS agencies, non-profit organizations, professional societies, and health providers. Consistent with the NASEM recommendation, NEI aims to encourage consumers to engage in preventative behaviors and to recognize vision as a health priority. NEI will conduct research to inform the development of messaging, products, tools, and dissemination strategies to help broaden awareness of eye health. The messages and other resources developed in this effort will be shared with government agencies, vision research funders and advocacy groups. NIH is committed to improving public health by translating vision-saving research into improved health outcomes for patients. In recent years, NIH research has made significant strides in early detection and treatment of many chronic eye diseases, such as glaucoma, diabetic retinopathy, and macular degeneration. In January 2018, NEI initiated a planning process to engage the vision community in developing a new research agenda, including in the areas of population health and vision health disparities research. Working groups of the National Advisory Eye Council will meet to identify research needs, gaps and opportunities. Furthermore, NEI is initiating a collaboration with the Department of Defense Vision Research Program to fund a project that meets the vision needs of special populations such as military personnel and veterans. HIV Community-Based Testing Programs The Committee recognizes that several community-based programs have encouraged individuals at risk for HIV/AIDS to utilize FDA-approved homebased HIV testing technology to monitor their HIV status. The Committee continues to urge the OMH to consider a pilot or demonstration program within existing resources to gauge the effectiveness of this approach. Action taken or to be taken The Department takes seriously the need for individuals to know their HIV status. The Office of Minority Health (OMH) within the Office of the Assistant Secretary for Health, will work to collaborate across the Department to review the feasibility for a pilot or demonstration program within existing resources to gauge the effectiveness of the FDA-approved home-based HIV testing technology to monitor the HIV status of individuals at risk for HIV/AIDS. OMH will continue to support and promote HHS efforts to increase the number of individuals who know their HIV status, particularly in racial and ethnic minority communities. 1 https://nei.nih.gov/nehep

Page 159
HIV/AIDS and Hepatitis C The Committee continues to be concerned about the HIV/AIDS epidemic in the African American community, and is aware of the concurrent high rates of co-infection with Hepatitis C as outlined by the HHS 2015 Forum on Hepatitis C in African American Communities. The Committee encourages OMH to work aggressively to address opportunities to reduce the burden of HIV/AIDS and Hepatitis C by exploring partnerships for screening and implementing community engagement programs. Action taken or to be taken The Office of Minority Health (OMH) co-sponsored a study by the National Academies of Sciences, Engineering, and Medicine (second phase released March 2017) on eliminating viral hepatitis in the United States. The report, Eliminating the Public Health Problem of Hepatitis B and C in the United States, provides a U.S. strategy for eliminating hepatitis B and hepatitis C virus infection and the disease and mortality caused by these agents as public health threats by 2030. OMH partners with HHS’s Office of HIV/AIDS and Infectious Disease Policy (OHAIDP), CDC, and others, to implement the National HIV/AIDS Strategy and the National Viral Hepatitis Action Plan, which include African-Americans as one of the priority populations and goals for increasing awareness, screening, vaccination, and reducing the number of deaths for the African-American population. These plans improve our nation’s responses to HIV and viral hepatitis by setting goals and priorities with measureable targets and objectives that serve to focus our response on the outcomes. They promote the use of the most efficient and effective methods for preventing, detecting, and treating these infections. They also support the coordination and collaboration between agencies to promote consistent messaging and policies from HHS agencies that promote joint programs to better serve patients and people at risk. The indicator data used to monitor progress on the National HIV/AIDS Strategy show that progress is being made, but gains made in prior years on indicators used to monitor Viral Hepatitis Action Plan are being eased. The annual targets have been met on more than half of the HIV-related outcomes, but we are losing ground in the battle against viral hepatitis in the United States because of the opioid crisis. According to a recent CDC report, across the nation, researchers found substantial, simultaneous increases in acute hepatitis C (133 percent) and admissions for opioid injection (93 percent) from 2004 to 2014. These increases were seen at not only the national level, but also when data were analyzed by state, by age, and by race and ethnicity. Rates of opioid injection—especially injection of prescription opioid pain relievers, as well as heroin—and acute hepatitis C virus infections increased most dramatically from 2004 to 2014 among younger Americans (ages 18-39). The Office of Minority Health Resource Center (OMHRC) co-sponsored the 4th US Conference on African Immigrant and Refugee Health – Rethinking Integration, Challenges, and Empowerment, held in New York, NY in September 2016. This Conference included workshops on HIV/AIDS and Hepatitis C in African-American communities.

Page 160
OMHRC provided twelve subcontracts to organizations to raise awareness and reduce HIV and hepatitis co-infection rates in minority and hard-to-reach communities. Of these subcontracting agencies, three were focused on African American populations. Support for this project was provided by the HHS Office of HIV/ AIDS and Infectious Disease Policy (OHAIDP) and the Secretary’s Minority AIDS Initiative Fund. Each agency created and implemented hepatitis/HIV social marketing campaigns and testing across minority populations through coordination of activities, information and referrals. Through this initiative targeting African American communities, 5,115 individuals were tested for HIV with 6 positive results; and 7,348 individuals were tested for hepatitis with 161 positive results. In fiscal year (FY) 2017, OMH issued a competitive funding opportunity announcement for the Empowered Communities for a Healthier Nation Initiative (ECI). The ECI seeks to reduce significant health disparities impacting racial and ethnic minorities and/or disadvantaged populations through implementing evidence-based strategies with the greatest potential for impact. The program is intended to serve residents in communities disproportionately impacted by the opioid epidemic; childhood/adolescent obesity; and serious mental illness. A total of 15 awards were made, of which six projects focused on addressing the opioid epidemic and included screening/testing for viral hepatitis and HIV. OMH expects to support the ECI projects for a three-year project period ending in FY 2020. Through various health observances, such as Hepatitis Awareness Month in May, National HIV Testing Day in June, and World AIDS Day in December, and others throughout the year, OMH helps promote awareness of HIV/AIDS and Hepatitis, and screening and implementing community engagement programs through social media, Twitter chats, speeches and presentations, and other outreach activities. OMH will continue to explore partnerships to promote HIV/AIDS and Hepatitis C screening and the implementation of community engagement programs. Prenatal Opioid Use Disorders and Neonatal Abstinence Syndrome The Committee is aware that the Protecting Our Infants Act of 2015 requires the Secretary to conduct a review of the Department's planning and coordination activities related to prenatal opioid use disorders and neonatal abstinence syndrome, as well as address gaps in research and treatment. The act also requires the Secretary to develop recommendations for preventing and treating prenatal opioid use disorders and neonatal abstinence syndrome. The Committee requests an update on these activities in the fiscal year 2019 Congressional Justification. Action taken or to be taken HHS divisions are addressing the opioid crisis, including Neonatal Abstinence Syndrome (NAS), on several fronts. The following are some examples. Grantees in HRSA programs such as the Maternal, Infant and Early Childhood Home Visiting (MIECHV) and Healthy Start programs use evidence-based approaches to screen, intervene, and
Page 161
refer perinatal women and parents of young children to treatment and recovery support services. Front-line staff also provide health education and guidance for parents of young children, including caring for babies born with neonatal abstinence syndrome. For instance, the MIECHV Program supports voluntary, evidence-based home visiting services for at-risk pregnant women and parents with young children up to kindergarten entry. Similarly, the Healthy Start program supports organizations across the country to help reduce racial and ethnic disparities in maternal and infant health status in high-risk communities. Healthy Start supports women before, during, and after pregnancy through the baby’s second birthday, by providing care coordination and linkage to comprehensive health and social services, health education, strengthening family resilience, and engaging community partners to enhance systems of care. In addition, States and territories use Title V Maternal and Child Health (MCH) Services Block Grant Program’s formula grant funds received from HRSA to support a range of activities to improve care and outcomes for mothers, children, and families, which may include addressing NAS. A federal-state partnership, the State MCH Block Grant program gives states control and flexibility in meeting the unique health needs of their children and families, while HRSA assures accountability and impact through performance measurement and technical assistance. In the State MCH Block Grant FY 2018 Applications and FY 2016 Annual Reports, 21 of 59 states/jurisdictions reported activities to address NAS; and five states established an NAS-related State Performance Measure including measures to assess the rates of NAS diagnosis and early intervention for NAS-affected infants. As one of the State MCH Block Grant program’s National Outcome Measures, and in response to legislation, HRSA annually compiles and makes available to states, national and state-level data on the proportion of infants born with NAS. Finally, HRSA funds the national Alliance for Innovation in Maternal Health, or AIM, which consists of a variety of maternal safety bundles with the goal to reduce maternal mortality in the United States. Specifically the AIM National Collaborative on Maternal Opioid Use Disorder is one maternal safety bundle developed in CY 2017 for hospitals to help obstetricians and others appropriately manage care for women with opioid dependence. In FY 2018, the AIM National Collaborative on Maternal Opioid Use Disorder has engaged 14 states to implement the bundle and raise awareness about the need for treatment and services for women. Public Access The Committee commends HHS Operating Divisions that have issued plans in response to the directive issued by the White House Office of Science and Technology Policy to support increased public access to the results of research funded by the Federal Government. The Committee encourages the Department to continue its efforts towards full implementation of the directive, and requests that an update on progress made be included in its fiscal year 2019 Congressional Justification.

Page 162
Action taken or to be taken NIH Implementation Efforts towards Increasing Access to Scientific Publications and Digital Scientific Data The National Institutes of Health (NIH) has a long history and continued commitment to ensure that, to the fullest extent possible, the results of federally funded scientific research are made available to and are useful for the general public, industry, and the scientific community.1 In coordination with the United States Department of Health and Human Services (HHS),2 NIH responded to the White House directive by developing the National Institutes of Health Plan for Increasing Access to Scientific Publications and Digital Scientific Data from NIH Funded Scientific Research3 (“NIH Plan”), released in February 2015. The NIH Plan describes objectives for scientific publications and digital scientific data. An update on progress toward these objectives is provided below. Scientific Publications As described in the NIH Plan, NIH fully meets the memorandum’s objectives for increasing access to NIH-funded scientific publications. The NIH Public Access Policy4 was originally issued in 2005 to encourage NIH-funded investigators to post their final manuscripts to the NIH National Library of Medicine’s (NLM) PubMed Central (PMC), a publicly accessible, stable, permanent, and searchable electronic archive, to be made publicly available no later than 12 months after the official date of publication. The NIH Public Access Policy became mandatory in 2008, and permanent through the Omnibus Appropriations Act, 2009, Public Law 111-8. Under the policy, NIH funding is estimated to have helped generate approximately 980,000 peer-reviewed papers published from 2008 to May 2017. NIH has collected 865,000 of them in PMC, representing a compliance rate of 88 percent.5 To further support the Office of Science and Technology Policy (OSTP) directive, NIH has made its collection of authored manuscripts6 available to the public in a form that facilitates text-mining. The collection includes all manuscripts that have arisen from full or partial NIH funding, have a publication date of July 2008 or later, and are publicly available. PMC is a public-private partnership between NIH and publishers. As such, publishers also provide full text articles that are not funded by NIH. There are more than 4.6 million papers made publicly accessible in PMC. On a typical weekday, more than 1.75 million unique users retrieve more than 3.5 million articles from this archive. PMC serves as the repository for papers
1 https://grants.nih.gov/policy/sharing.htm 2 (http://www.hhs.gov/open/public-access-guiding-principles/index.html) 3 https://grants.nih.gov/grants/NIH-Public-Access-Plan.pdf 4 http://publicaccess.nih.gov/index.htm 5 Because of implementation timing and lags in submission, NIH calculates compliance from July 2008 to 6 months prior to the reporting month. Some of these papers may be embargoed. The paper-funding estimates may come from an acknowledgement statement in the article or from a separate association made by an author, e.g., during the process of submitting the manuscript to the NIH Manuscript Submission (NIHMS) system, or through the My Bibliography feature (http://www.ncbi.nlm.nih.gov/sites/books/NBK53595/) of the My NCBI service. These inclusion criteria are not perfect, and NIH may miss papers that are NIH supported and fall under the NIH Public Access Policy (e.g., papers posted to PMC without being associated with an institution’s award). It also may include papers that do not fall under the Policy, such as papers that are directly supported by NIH but are not peer-reviewed. 6 https://www.ncbi.nlm.nih.gov/pmc/about/authorms/

Page 163
collected under the NIH Public Access Policy and 10 other federal agency policies. Over the last 12 months, PMC added more than 110,000 federally-supported papers to PMC, including more than 4,000 papers supported by agencies other than NIH. Digital Scientific Data Effective data sharing relies upon appropriate identification, adoption, and crediting of good data management and sharing practices, thus, NIH is adopting principles to make data “FAIR” (Findable, Accessible, Interoperable, and Reusable).1 In order to implement the NIH Plan and move forward with ongoing commitments to the data sharing enterprise, NIH has been considering priorities for data management and sharing (e.g., which data types have the greatest value for sharing, the costs and value of sharing different data types, including the long-term resource implications), and how to expand upon its 2003 Data Sharing Policy. On November 14, 2016, NIH released a Request for Information (RFI) (NOT-OD-17-015)2 on Data Management, Sharing, and Citation. RFI feedback3 is being used to inform NIH activities and development of a future NIH policy for the management and sharing of digital scientific data generated from all NIH-supported research (intramural, grants, and contracts), which is intended to replace the 2003 NIH Data Sharing Policy. Additionally, in October 2017, in partnership with the National Science Foundation, NIH held a focused Science of Science Innovation Policy4 (SciSIP) workshop to discuss mechanisms for assessing the value of sharing biomedical data. Discussions from this workshop will inform research initiatives and priorities regarding data management and sharing. Furthermore, to support the long-term preservation of data and sustainability of repositories holding such data, NIH released the related “Request for Information (RFI): Metrics to Assess Value of Biomedical Digital Repositories”.5 (Key policy provisions for data management and sharing are currently being drafted based upon the feedback obtained from the RFIs, the workshop, and other NIH and interagency discussions. Some of these policy provisions include the scope and applicability, as well as the requirement for a Data Management and Sharing Plan (DMSP) (consistent with the requirements of the White House OSTP Memorandum on Increasing Access to the Results of Federally Funded Scientific Research)6 and the requirement for data sharing (under the authorities granted to NIH under the 21st Century Cures Act). NIH continues to actively participate in Federal efforts to support open science, specifically by co-chairing the Interagency Working Group on Open Science (IWGOS), as part of the Committee on Science of the White House National Science and Technology Council. The aim of the IWGOS is to build upon and extend the progress that federal agencies have made to date in implementing the 2013 OSTP directive. The IWGOS will publish a report that will articulate objectives and recommendations on Federal open science that can further enhance access to results of federally funded scientific research.
1 http://www.nature.com/articles/sdata201618 2 https://grants.nih.gov/grants/guide/notice-files/NOT-OD-17-015.html 3 https://osp.od.nih.gov/wp-content/uploads/Public_Comments_Data_Managment_Sharing_Citation.pdf 4 https://www.nsf.gov/funding/pgm_summ.jsp?pims_id=501084 5 https://grants.nih.gov/grants/guide/notice-files/NOT-OD-16-133.html 6 https://obamawhitehouse.archives.gov/sites/default/files/microsites/ostp/ostp_public_access_memo_2013.pdf

Page 164
NIH is continuing to increase public access to data and information from NIH-funded and supported research through policies, programs, and initiatives. Some of those can be seen on NLM’s Trans-NIH Biomedical Informatics Coordinating Committee (BMIC) website.1 Surgeon General Report on Poverty The Committee notes that too many children still live in poverty, compromising their ability to be healthy, succeed in school and raise healthy families themselves. A report by the Surgeon General on improving the health of children could increase awareness and generate additional effort on ameliorating this public health problem. Action taken or to be taken The Department of Health and Human Services (HHS) appreciates the Committee’s interest in the improving the health of Americans of all ages. As the Nation’s Doctor, the Surgeon General of the Public Health Service Commissioned Corps is focused on improving the country’s health. The Surgeon General communicates the best available scientific information to the public to reach individuals where they live, work, and play and by issuing scientific documents - Surgeon General’s Reports and Calls to Action – on critical public health issues. Topics for Surgeon General’s Reports are based on the highest priority public health needs of the Nation and they foster the Department’s abilities to ensure improved health outcomes related to the specific issue. The Surgeon General’s Report on health and the economy, will provide the evidence-base for the impact of the relationship between health and the prosperity of individuals of all life stages and the communities in which they live. The Surgeon General’s priority for better health through better partnerships seeks to engage government and non-government partners in addressing major public health challenges. For example, the opioid epidemic has created a crisis within the child welfare system. Through this priority partnership initiative, the Surgeon General seeks to increase awareness and generate additional public and private efforts to address the public health problems related to opioid misuse. This is an opportunity to bring together partners from a multitude of sectors to include the criminal justice system, education, employers, military, VA, and national security. Health Disparities The Committee believes that a comprehensive coordinated focus by OMH, HRSA and NIMHD will increase the probability of reducing health disparities. This coordinated focus should examine the factors that lead to health disparities, including but not limited to age, nutrition, medical conditions, and availability of medical support and an appropriate healthcare workforce in both underserved urban and rural settings. HHS is encouraged to partner with community-based organizations that are currently providing medical and nutritional support.
1 https://www.nlm.nih.gov/NIHbmic/nih_data_sharing_repositories.html

Page 165
Action taken or to be taken The Department of Health and Human Services (HHS) continues support for efforts to reduce health disparities. The Office of Minority Health’s (OMH) National Workforce Diversity Pipeline (NWDP) Program supports projects that develop innovative strategies to support development of an appropriate healthcare workforce in underserved settings. NWDP projects identify promising students in their first year of high school and provide them with a foundation to pursue successful careers in the health professions. The program seeks to address health disparities among racial and ethnic minorities by supporting networks of institutions focused on and with demonstrated commitment and capacity to establish pipeline programs to increase minority and disadvantaged students’ awareness and pursuit of careers in health care including behavioral health, and to increase the availability of science, technology, engineering and mathematics (STEM) education programs. NWDP projects began in FY 2015 and will end July 31, 2020. OMH will continue to coordinate efforts related to health disparities across the Department to examine the factors that lead to health disparities, including but not limited to age, nutrition, medical conditions, and the availability of medical support and an appropriate healthcare workforce in both underserved urban and rural settings. OMH will look to leverage this Department-wide coordination with community-based partners that also work to reduce health disparities. Rural Health The Committee encourages the Secretary to ensure that rural concerns and challenges are adequately represented in the Department's policies, programs, and activities, including policies related to the opioid epidemic. The Committee requests that the Secretary include a status of these activities in the fiscal year 2019 Congressional Justification. Action taken or to be taken The Department’s programs and resources play a key role in addressing rural concerns and challenges, including the fight against the opioid epidemic. The Department continues to target funding for critical rural health activities such as Rural Health Outreach Grants, Clean Water for Health program, and Telehealth. These investments continue to maintain access to quality health care services in rural areas across the United States. The Department has also implemented a five-point strategy to address America’s opioid crisis. The FY 2019 President’s Budget continues to invest in activities to fight opioid abuse and includes $10 billion in new resources to combat the opioid epidemic and address mental health. Public Health in Indian Country The Committee supports the Secretary's current initiatives to address public health crises such as viral hepatitis, HIV/AIDS and opioids that disproportionally impact Indian County. The Committee requests that HHS provide an update on these efforts in the fiscal year 2019 Congressional Justification.
Page 166
Action taken or to be taken Opioids Ending the public health crisis that opioid addiction represents and reducing the devastating impact it is having on our families and communities is a shared Administration priority and a top Departmental priority. The FY 2019 President’s Budget includes an additional $10 billion in new resources across HHS to combat the opioid epidemic and serious mental illness. This investment supports the Secretary’s five part strategy to:
Improve access to prevention, treatment, and recovery services, including the full range of medication-assisted treatments;
Improve the availability of overdose-reversing drugs; Strengthen our understanding of the crisis through better public health data and
reporting; Provide support for cutting edge research on pain and addiction; and Improve pain management practices.
The Budget includes an initial allocation of $150 million for IHS for additional opioid prevention, treatment and recovery support as part of the FY 2019 President’s Budget request of $10 billion in new resources to combat the opioid epidemic and address mental illness. HIV/AIDS The FY 2019 HHS Budget supports research, treatment and prevention of HIV/AIDS. The majority of HIV/AIDS spending is for care through Medicaid and Medicare, and other proposed resources. The Budget is aligned with the goals of the National HIV/AIDS Strategy to reduce new HIV infections, increase access to care and improve health outcomes for people living with HIV, reduce HIV-related health disparities, and achieve a more coordinated national response to the HIV epidemic. Additionally, the Budget is aligned with the goals of the HIV Care Continuum Initiative to accelerate efforts to better address drop-offs along the continuum, and increase the proportion of individuals in each stage along the continuum. Hepatitis The FY 2019 HHS Budget includes $34 million for CDC’s viral hepatitis activities. CDC is uniquely positioned to invest in, and partner with, state and local health departments, universities, medical centers, community-based organizations, and others to defend and protect the United States against viral hepatitis disease threats through four main activities, including:
Decrease mortality through diagnosing and treating people who are living with viral hepatitis.
o An early diagnosis, coupled with care and treatment of those infected, greatly reduces the risk of liver disease and mortality caused by viral hepatitis.
Reduce the Number of New Infections Associated with Injection Drug Use and Other Modes of Transmission.
o In at least six states in 2015, increases in Hepatitis B virus transmission joined the increases in Hepatitis C virus transmission. In response to the urgent need to curb the epidemic of Hepatitis B and Hepatitis C virus infections, CDC’s work in states with a substantial burden of viral hepatitis promotes improving viral hepatitis

Page 167
surveillance, investigating transmission networks, and providing training to support state and local health department staff.
Prevent Perinatal (Mother-to-Child) Transmission of Hepatitis B Virus and Hepatitis C Virus.
o CDC continues to support activities focused on the national goal of eliminating mother-to-child transmission of Hepatitis B virus. The cornerstones of preventing perinatal Hepatitis B virus transmission are testing all pregnant women for Hepatitis B virus infection, giving a birth dose of Hepatitis B virus vaccine to all infants within 24 hours of birth, and other interventions to newborns of infected mothers. CDC is developing recommendations for hepatitis B vaccination, testing, and treatment that protects the health of the mother and eliminates the risk of Hepatitis B virus for her newborn.
o Hepatitis C infections are increasing among pregnant women and their newborns, which is an emerging consequence of the increases in substance use among young adults. To improve detection, testing, and linkage to care, CDC will develop recommendations on appropriate curative Hepatitis C virus treatments for women of childbearing age, pregnant women, and children affected with Hepatitis C virus at birth.
Support State, Local, and Tribal Hepatitis B and Hepatitis C Elimination Programs. o CDC is a major partner in the national effort to eliminate the public health threat
of viral hepatitis and will continue to take action to prevent incidence, morbidity, and mortality associated with viral hepatitis. For example, building on the successes and progress of projects in the Cherokee Nation and other settings, CDC will continue to assist state/local and tribal development of HCV and HBV prevention programs that have goals and plans for eliminating HBV and HCV. The objectives of the programs are to identify best practices that can assist other state and local jurisdictions with developing similar programs that will save lives and save money. CDC is also investing in expanded surveillance that will support elimination projects -- enabling jurisdictions to better track trends and identify and respond to outbreaks swiftly -- and evaluating high impact strategies to prevent new HCV infections in high-risk populations.

Opioids Epidemic and Serious Mental Illness and Serious Emotional Disturbance Initiative

Page 1
All Purpose Table (Dollars in Thousands)
Opioids and Serious Mental Illness Initiative
FY 2017Final
FY 2018Annualized
CR
FY 2019 President’s Budget
Authority1
FY 2019 +/‐FY 2018
Discretionary Budget Authority ‐ ‐ 10,000,000 +10,000,000
Substance Abuse and Mental Health Services Administration (non add)
‐ ‐ 1,240,000 +1,240,000
Centers for Disease Control and Prevention (non add)
‐ ‐ 175,000 +175,000
Health Resources and Services Administration (non add)
‐ ‐ 550,000 +550,000
National Institutes of Health (non add) ‐ ‐ 750,000 +750,000
Food and Drug Administration (non add) ‐ ‐ 10,000 +10,000
Indian Health Service (non add) 150,000 +150,000
HHS‐Wide (non add) 125,000 +125,000
Additional resources (non add) 7,000,000 +7,000,0001. Represents initial allocation
Authorizing Legislation………….…Public Health Service Act; Food, Drug, and Cosmetic Act; Appropriations Language FY 2019 Authorization……………….………………………………………………..........…..………….………………………….….……......……TBD Allocation Method…………………………………………………………….……………………………….……………………… Transfer Authority
Appropriations Language For necessary expenses of the Department of Health and Human Services for activities relating to or in support of reducing opioid misuse and abuse and addressing mental health needs, including activities authorized by the PHS Act, $10,000,000,000, to remain available until expended: Provided, That such funds shall be in addition to any other funds available for the purposes provided herein: Provided further, That funds may be used for necessary expenses of grants, contracts, and other agreements for the following purposes: for research on reducing opioid misuse or abuse or on mental health; for surveillance of, prevention of, treatment of, and recovery from opioid misuse and abuse or mental health issues; for purchasing medical supplies and medication for such misuse or abuse; and for any purpose that the Secretary determines to be in furtherance of the objectives of this appropriation: Provided further, That funds may be used for the purposes of providing primary health services to assign National Health Service Corps ("NHSC") members to expand the delivery of substance use disorder treatment services, notwithstanding the assignment priorities and limitations in or under sections 333(a)(1)(D), 333(b), or 333A(a)(1)(B)(ii) of the PHS Act, and to make NHSC Loan Repayment Program awards under section 338B of such Act: Provided further, That funds appropriated under this heading may be transferred to other appropriation accounts of the Department of Health and Human Services, as determined by the Secretary to be appropriate, for the purposes provided herein: Provided further, That upon a determination by the Secretary that funds transferred pursuant to the previous proviso are not necessary for the purpose provided, such amounts may be transferred back to the account.

Page 2
Narrative by Activity
Program Description and Accomplishments
The FY 2019 Budget proposes a $10 billion historic investment to combat the opioid epidemic and address serious mental illness and serious emotional disturbance. Funding this proposal in the Office of the Secretary will further facilitate department‐wide collaboration on this important initiative. Coordination by the Office of the Secretary will also better enable the Department to address the opioids epidemic and focus on the unique needs of rural and underserved populations through evidence‐based approaches. These funds will expand efforts to prevent opioid abuse and help Americans seeking treatment to access overdose‐reversal drugs, treatment, and recovery support services. It will build on the Department’s five point strategy, which involves:
Improving access to prevention, treatment, and recovery services, including the full range of medication‐assisted therapies;
Targeting availability and distribution of overdose‐reversing drugs;
Strengthening our understanding of the epidemic through better public health data and reporting;
Supporting cutting‐edge research on pain and addiction; and
Advancing better practices for pain management. The Budget proposes an initial allocation for $3 billion of this funding across HHS. This initial allocation provides $1.24 billion in SAMHSA, including $1 billion to continue and expand State Targeted Response to the Opioid Crisis Grants, as well as new funding for reducing injection drug use, improving access to overdose reversal drugs for first responders, drug courts, and services for pregnant and post‐partum women. In NIH, the initial allocation provides $750 million to enhance existing research efforts to accelerate the development of safe, non‐addictive, and effective strategies to prevent and treat pain, opioid misuse, and overdose and to help optimize their implementation. In HRSA, the initial allocation provides $550 million for assistance to address substance abuse, with a focus on opioid abuse and the overdose crisis in high‐risk communities. This funding includes $400 million for health centers to address behavioral health or substance abuse issues, with a focus on opioid addiction, to meet the needs of the communities they serve. Further, the initial allocation provides $175 million in CDC to expand support to States through the Prescription Drug Overdose Prevention program and to expand state surveillance capacity. The initial allocation includes $150 million in IHS for grants to expand opioid abuse prevention, treatment, and recovery support in Indian Country, and $10 million in FDA to complement ongoing activities to support health professionals in more optimally delivering medication‐assisted treatments and to accelerate the development of generic versions of opioid drug products with abuse deterrent formulas.

Page 3
Finally, the initial allocation provides $125 million in the Office of the Secretary to support HHS‐wide activities to launch a nation‐wide digital and mass media campaign to raise awareness about opioids and reduce drug demand and to support a robust evaluation to strengthen the evidence of the impact of medication‐assisted treatment on reducing overdose deaths. The remaining $7 billion will be available for transfer across the Department to support additional work to address the opioid crisis and serious mental illness and serious emotional disturbance, including establishing a new grant program for clinics that provide services to individuals suffering from mental illness and meet Certified Community Behavioral Health Clinics standards.
Funding History
Fiscal Year Amount
FY 2014 $0
FY 2015 $0
FY 2016 $0
FY 2017 $0
FY 2018 Annualized CR $0
FY 2019 Budget Request
The FY 2019 President’s Budget request for the initiative to combat the opioids crisis and address serious mental illness Initiative is $10,000,000,000; an increase of $10,000,000,000 over the FY 2018 Annualized CR level. This request will support efforts to prevent opioid abuse, and help those that abuse opioids get access to overdose‐reversal drugs, treatment, and recovery support services. These funds would also address serious mental illness and serious emotional disturbance.

Office of Medicare Hearings and Appeals


3
Table of Contents
Organizational Chart ................................................................................................................................. 4
Organization Chart: Text Version .............................................................................................................. 5
Introduction and Mission .......................................................................................................................... 6
Overview of Budget Request .................................................................................................................... 7
Overview of Performance ......................................................................................................................... 7
All Purpose Table .................................................................................................................................... 10
Appropriations Language ........................................................................................................................ 10
Amounts Available for Obligation ........................................................................................................... 10
Summary of Changes .............................................................................................................................. 11
Budget Authority by Activity ‐ Direct ...................................................................................................... 12
Authorizing Legislation ............................................................................................................................ 12
Appropriation History Table ................................................................................................................... 13
Narrative by Activity ............................................................................................................................... 14
Program Description and Accomplishments........................................................................................... 14
Funding History ....................................................................................................................................... 16
FY 2019 Budget Request ......................................................................................................................... 16
Outputs and Outcomes Table ................................................................................................................. 19
Budget Authority by Object Class ........................................................................................................... 20
Salaries and Expenses ............................................................................................................................. 21
Detail of Full Time Equivalents ................................................................................................................ 22
Detail of Positions ................................................................................................................................... 23

4
Organizational Chart
Office of Medicare Hearings and Appeals
CHIEF ADMINISTRATIVE LAW JUDGE Nancy Griswold
Office of Program Integrity
DIRECTOR Karen Ames
Cleveland Field Office
ASSOCIATE
CHIEF ADMINISTRATIVE
LAW JUDGE Christian Knapp
HEARING OFFICE
DIRECTOR Steven Yelenic
IrvineField Office
ASSOCIATE
CHIEF ADMINISTRATIVE
LAW JUDGE Stuart Wein
HEARING OFFICE
DIRECTOR Andreas Frank
Miami Field Office
ASSOCIATE
CHIEF ADMINISTRATIVE
LAW JUDGE Vivian Rodriguez
HEARING OFFICE
DIRECTOR Elizabeth Nodal
Arlington Field Office
ASSOCIATE
CHIEF ADMINISTRATIVE
LAW JUDGE William Farley
HEARING OFFICE DIRECTOR
Carlton Drew
DEPUTY CHIEF ADMINISTRATIVE LAW JUDGE Brian Haring
Office of Management
DIRECTOR Eileen McDaniel
Kansas CityField Office
ASSOCIATE
CHIEF ADMINISTRATIVE
LAW JUDGE David Krane
HEARING OFFICE DIRECTOR Cindy Cento
Seattle Field Office
ASSOCIATE
CHIEF ADMINISTRATIVE
LAW JUDGE Lewis Booker
HEARING OFFICE
DIRECTOR Susan Brown

5
Organization Chart: Text Version Office of Medicare Hearings and Appeals
• Chief Administrative Law Judge, Nancy Griswold • Deputy Chief Administrative Law Judge, Brian Haring The following offices report directly to the Chief Administrative Law Judge: • Director, Office of Management
o Eileen McDaniel
• Director, Office of Program Integrity o Karen Ames
• Arlington Field Office
o Associate Chief Administrative Law Judge, William Farley o Hearing Office Director, Carlton Drew
• Cleveland Field Office o Associate Chief Administrative Law Judge, Christian Knapp o Hearing Office Director, Steven Yelenic
• Irvine Field Office o Associate Chief Administrative Law Judge, Stuart Wein o Hearing Office Director, Andreas Frank
• Kansas City Field Office o Associate Chief Administrative Law Judge, David Krane o Hearing Office Director, Cindy Cento
Miami Field Office o Associate Chief Administrative Law Judge, Vivian Rodriguez
o Hearing Office Director, Elizabeth Nodal
• Seattle Field Office
o Associate Chief Administrative Law Judge, Lewis Booker
o Hearing Office Director, Susan Brown

6
Introduction and Mission
The Office of Medicare Hearings and Appeals (OMHA), an agency of the U.S. Department of Health and Human Services (HHS), administers the third level of appeals nationwide for the Medicare program. OMHA ensures that Medicare beneficiaries, providers and suppliers have access to an independent forum and opportunity for a hearing conducted pursuant to the Administrative Procedure Act on disputed Medicare claims. By providing a timely and impartial review of Medicare appeals, OMHA encourages providers and suppliers to continue to provide services and supplies to Medicare beneficiaries. Such access to timely adjudication of disputes is essential to the integrity of the Medicare system. On behalf of the Secretary of HHS, the Administrative Law Judges (ALJs) within OMHA conduct impartial hearings and issue decisions on claim determination appeals involving Medicare Parts A, B, C, D, as well as Medicare entitlement and eligibility appeals.
Mission
OMHA is a responsible forum for fair, credible and timely decision‐making through an accomplished, innovative and resilient workforce. Each employee makes a difference by contributing to shaping American health care.
Vision
World class adjudication for the public good.
Statutory Decisional Timeframe
The Medicare, Medicaid, and SCHIP Benefits Improvement and Protection Act of 2000 (BIPA) envisions that OMHA will issue decisions on appeals of Part A and Part B Qualified Independent Contractor (QIC) reconsiderations within 90 days after a request for hearing is filed.

7
Overview of Budget Request The FY 2019 President’s Budget request for the Office of Medicare Hearings and Appeals (OMHA) is $251,060,000; an increase of $144,408,000 over the FY 2018 Annualized CR level of $106,652,000. This request includes $112,381,000 in discretionary budget authority, $125,000,000 in proposed mandatory funding, $10,000,000 in proposed access to Recovery Audit Contractor (RAC) collections, $3,679,000 in proposed user fee collections, and a suite of legislative proposals to address the backlog of Medicare appeals and to improve the Medicare appeals process. This request will allow OMHA to implement HHS and OMHA strategic initiatives to reduce the backlog, and improve the Medicare appeals process by more than doubling adjudicatory capacity while sustaining baseline operational inflationary increases. With the full enactment of the FY 2019 request, OMHA will be able to increase the agency’s overall adjudication capacity to a level that matches projected incoming receipts for the first time in eight years. This request would enable OMHA to implement its Adjudication Expansion Initiative, which will increase capacity from 92 ALJ teams to up to 198 ALJ teams nationwide, including establishing up to five new field offices and 775 new positions. The full impact of the 106 additional ALJ teams proposed in FY 2019 will be realized in out years after new adjudicators gain six to twelve months of experience and will increase ALJ adjudication capacity by more than 100,000 additional appeals annually. In addition, OMHA will be in the position to implement and sustain the Medicare Magistrate program to resolve appeals below the Federal District Court amount in controversy threshold ($1,600 in calendar year 2018 and updated annually) at a cost 43% lower than the cost of an ALJ team. OMHA projects staffing 100 Magistrates which would increase adjudication capacity by another 75,000 appeals, once the program is fully implemented and Magistrates gain necessary experience.
Overview of Performance OMHA remains committed to continuous improvement in the Medicare appeals process by implementing initiatives to enhance the quality and timeliness of its services within its legislative authorities and funding levels. Through increased process efficiency and targeted addition of support staff, OMHA has streamlined its business processes and has implemented a number of new initiatives to the maximum extent possible without sacrificing program integrity. Adjudication teams have more than doubled their productivity since 2009, with productivity hovering around the maximum sustainable level of approximately 1,000 appeals per ALJ team annually. In addition, creative solutions implemented as part of the Department’s administrative initiatives, combined with ALJ team productivity, have reduced the agency’s pending workload by over one third, from a high of approximately 900,000 pending appeals at the beginning of FY 2016 to its present level of approximately 530,000., Most of the Department’s higher impact initiatives represent one time reductions (such as settlements), and are neither repeatable nor sustainable and therefore OMHA cannot make lasting progress toward resolving the backlog of pending appeals until its adjudication capacity is in line with projected receipt levels. As OMHA’s workloads have grown dramatically, and it has become impossible for the agency to achieve its goals. As is noted above, appeals grew by 1,222 percent between FY 2010 and FY 2014. While appeals in FY 2017 were lower than FY 2014, as a result of departmental initiatives and the contracting pause in the RAC program, they were still 155 percent higher than the FY 2010 level. Although the backlog has gone down due to the impact of large initiatives which cannot be repeated, OMHA still has 6 years of work on its hand for its current ALJs, and additional cases are being added to the backlog each year that receipts exceed funded capacity. Between FY 2010 and FY 2017, OMHA's appeals receipt total

8
measured over 1.6 million appeals. Four primary drivers of the increase in volume include increases in the number of beneficiaries; updates and changes to Medicare and Medicaid coverage and payment rules; growth in appeals from Medicaid State Agencies with respect to dual eligible beneficiaries; and national implementation of the Medicare Fee‐for‐Service RAC Program. At present, projected annual receipts outpace OMHA’s sustainable adjudication capacity and initiatives. The dramatic increase in appeals has had a predictably detrimental impact on the agency’s performance and resulted in a backlog of approximately 530,000 pending appeals at Level 3 as OMHA entered FY 2018. Although departmental initiatives, including the Centers for Medicare & Medicaid Services (CMS) Part A Hospital Appeals Settlement Process and OMHA’s Settlement Conference Facilitation (SCF) with State Medicaid agencies, have improved OMHA’s pending appeals backlog in the short term (from a high of approximately 900,000 appeals at the beginning of FY 2016), the largest initiatives have resulted in one‐time reductions of OMHA’s pending workload which were possible due to economies of scale. These dramatic reductions are not repeatable. First, settlement of appeals without a review of the merits of those appeals undermines the government’s responsibility to protect the Medicare Trust Fund. Moreover, a large percentage of the appeals pending at OMHA were filed by appellants that are currently the subject of program integrity investigations and therefore not eligible for settlements. Second, the settlement of large numbers of appeals without consideration of the merits of the claim encourages the filing of meritless appeals and could increase the number of appeals filed at OMHA. Finally, even if these arguments are overcome, the settlement of large numbers of appeals without taking contemporaneous steps to fund adjudication capacity at OMHA to handle incoming receipts achieves only temporary relief. OMHA will continue to function with a large disparity between adjudication capacity and receipt levels. As long as receipts outpace maximum adjudication capacity, the backlog will re‐emerge. At OMHA’s FY 2018 Annualized CR funding level, OMHA is able to sustain 88,000 dispositions (accounting for historical ALJ attrition and the time required to hire and train new ALJs), which is significantly less than projected incoming receipts in FY 2018. OMHA has sought to increase its adjudication capacity through regulatory change, but its ability to do so is limited. On March 20, 2017, OMHA gained regulatory authority for an Attorney Adjudicator program allowing senior attorneys (attorney‐adjudicators) to decide cases which do not require a hearing, issue remands, dismiss a request for hearing when the appellant withdraws and dismiss a request for review for any reason. This program frees ALJs to devote more time to hearings, which is something that only an ALJ is allowed to conduct. However, the impact of the attorney adjudicator process is largely limited by appellants’ willingness to waive the right to an oral hearing. Because the Social Security Act provides appellants a right to a hearing before an ALJ, OMHA’s other administrative initiatives aimed at increasing productivity—such as settlement conference facilitations, and statistical sampling—are similarly at the discretion of appellants. As long as cases are being added to the backlog of pending appeals, the average processing time will continue to grow. Indeed, with the exception of beneficiary appeals which are prioritized, OMHA has not been able to issue decisions within the statutorily required 90 days for BIPA appeals since 2010. The average processing time on closed workload in FY 2016 was 877 days and has risen to 1,217 days in FY 2018 (data as of November, 2017). The average age of pending appeals at OMHA has also risen at an alarming rate and measures 1,157 days (data as of November, 2017), far above the 90‐day adjudication time frame envisioned by BIPA, indicating that processing times will continue to increase until the backlog of pending appeals has been resolved.

9
Although adjudication delays at OMHA have impacted almost all categories of appellants, OMHA is able to continue its support of the HHS priority to Reform and Strengthen the Nation’s Health Care System through the prioritization of appeals filed by beneficiaries. The average wait time to disposition for prioritized beneficiary appeals has decreased from 244 days for appeals filed in FY 2013, to 66 days for appeals filed in FY 2017 (data as of September 30, 2017). This processing time supports the conclusion that, when properly resourced, OMHA is able to resolve most pending appeals within the anticipated statutory timeframe. OMHA also continues its support of the HHS priority to Promote Effective and Efficient Management and Stewardship, in part through ongoing evaluation of its customer service through an independent assessment that captures the scope of the Level 3 appeals experience by randomly surveying selected appellants and appellant representatives. Measure 1.5 aims to ensure appellants and related parties are satisfied with their Medicare appeals experience regardless of the outcome of their appeal. The measure is evaluated on a scale of 1 to 5, 1 representing the lowest score (very dissatisfied) and 5 representing the highest score (very satisfied). In FY 2017, OMHA achieved a 3.9 level of overall appellant satisfaction nationwide, exceeding the FY 2017 target of 3.4. Despite the overall satisfaction level, the delays in adjudication have had a predictably detrimental impact on satisfaction scores as the non‐beneficiary appellants’ frustration with the amount of time it takes for cases to be assigned to an adjudicator continues to rise. Here, the non‐beneficiary appellants rated this part of the process only a 2.25 out of a possible 5, bringing down OMHA’s satisfaction scores in other areas. Moreover, the overall level of appellant satisfaction still falls short of the 4.3 recorded in FY 2010, prior to increases in processing times resulting from the backlog of pending appeals. In addition, OMHA organizes the Medicare Appellant Forum and open door calls, events designed to inform and educate the appellant community on the status of the OMHA program and challenges related to the appeals backlog, and available options for appellants. OMHA’s Appellant Forums and open door calls have included speakers from all levels of the appeals process and departmental leaders. A primary goal of these events is to be as transparent as possible concerning the challenges faced by the appeals system and to keep appellants informed about current initiatives, pending pilots, demonstration projects, and evolving plans designed to address the workload at all levels of appeal. OMHA conducted four Medicare Appellant Forums (February 2014, October 2014, June 2015, and February 2016), and in FY 2017 began conducting open door calls to provide targeted and specific topical information to the appellant community on new initiatives and the status of pending appeals.
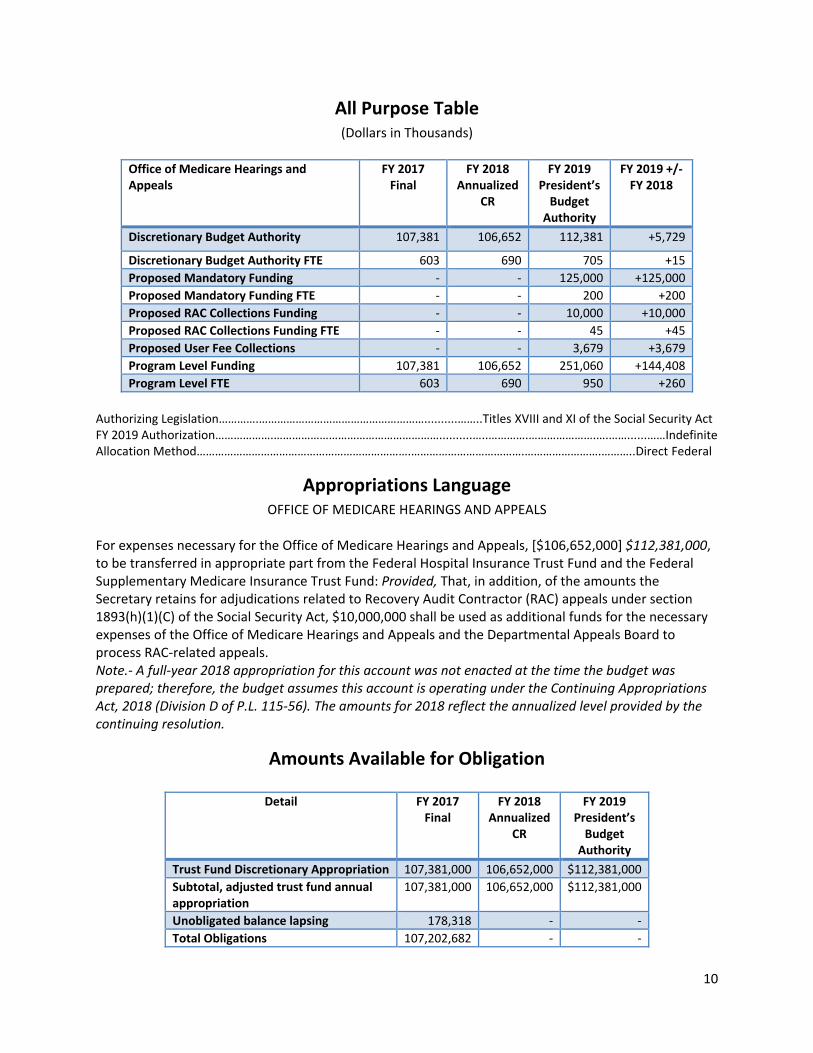
10
All Purpose Table (Dollars in Thousands)
Office of Medicare Hearings and Appeals
FY 2017Final
FY 2018Annualized
CR
FY 2019 President’s Budget
Authority
FY 2019 +/‐FY 2018
Discretionary Budget Authority 107,381 106,652 112,381 +5,729
Discretionary Budget Authority FTE 603 690 705 +15
Proposed Mandatory Funding ‐ ‐ 125,000 +125,000
Proposed Mandatory Funding FTE ‐ ‐ 200 +200
Proposed RAC Collections Funding ‐ ‐ 10,000 +10,000
Proposed RAC Collections Funding FTE ‐ ‐ 45 +45
Proposed User Fee Collections ‐ ‐ 3,679 +3,679
Program Level Funding 107,381 106,652 251,060 +144,408
Program Level FTE 603 690 950 +260
Authorizing Legislation………….………………………………………………..........……..Titles XVIII and XI of the Social Security Act FY 2019 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………….…………………….………..Direct Federal
Appropriations Language OFFICE OF MEDICARE HEARINGS AND APPEALS
For expenses necessary for the Office of Medicare Hearings and Appeals, [$106,652,000] $112,381,000, to be transferred in appropriate part from the Federal Hospital Insurance Trust Fund and the Federal Supplementary Medicare Insurance Trust Fund: Provided, That, in addition, of the amounts the Secretary retains for adjudications related to Recovery Audit Contractor (RAC) appeals under section 1893(h)(1)(C) of the Social Security Act, $10,000,000 shall be used as additional funds for the necessary expenses of the Office of Medicare Hearings and Appeals and the Departmental Appeals Board to process RAC‐related appeals. Note.‐ A full‐year 2018 appropriation for this account was not enacted at the time the budget was prepared; therefore, the budget assumes this account is operating under the Continuing Appropriations Act, 2018 (Division D of P.L. 115‐56). The amounts for 2018 reflect the annualized level provided by the continuing resolution.
Amounts Available for Obligation
Detail FY 2017Final
FY 2018Annualized
CR
FY 2019 President’s Budget
Authority
Trust Fund Discretionary Appropriation 107,381,000 106,652,000 $112,381,000
Subtotal, adjusted trust fund annual appropriation
107,381,000
106,652,000 $112,381,000
Unobligated balance lapsing 178,318 ‐ ‐
Total Obligations 107,202,682 ‐ ‐

11
Summary of Changes
*Full impact of FY 2019 hires realized in subsequent fiscal years.
Budget Year and Type of Authority Dollars FTE
FY 2018 Annualized CR 106,652 690
FY 2019 President’s Budget Authority 251,060 950
Net Change +144,408 +260*
Increases FY 2019 FTE
FY 2019 President’s Budget
Authority
FY 2019 +/‐
FY 2018 FTE
FY 2019+/‐
FY 2018 BA
Full‐time permanent 950 94,765 260 +34,223
Other personnel compensation ‐ 701 ‐ +174
Civilian personnel benefits ‐ 31,272 ‐ +11,174
Travel and transportation of persons ‐ 460 ‐ +260
Transportation of things ‐ 905 ‐ +639
Rental Payments to GSA ‐ 10,969 ‐ +3,590
Communications, utilities, and misc. charges ‐ 11,957 ‐ +8,265
Printing and reproduction ‐ 251 ‐ +67
Other services from non‐Federal sources ‐ 30,850 ‐ +30,085
Others goods and services from Federal sources ‐ 21,008 ‐ +10,917
Operation and maintenance of facilities ‐ 38,535 ‐ +37,681
Operation and maintenance of equipment ‐ 1,047 ‐ +93
Supplies and materials ‐ 2,910 ‐ +2,425
Equipment ‐ 5,430 ‐ +4,815
Total Increases 950 251,060 +260 +144,408
Total Changes FY 2019 FTE
FY 2019 President’s Budget
Authority
FY 2019 +/‐
FY 2018 FTE
FY 2019+/‐
FY 2018 BA
Total Increases 950 251,060 +260 +144,408
Total Decreases ‐ ‐ ‐ ‐
Total Net Change 950 251,060 +260 +144,408

12
Budget Authority by Activity ‐ Direct (Dollars in Thousands)
Authorizing Legislation (Dollars in Thousands)
OMHA
FY 2018 CRAmount
Authorized
FY 2018 Annualized CR
FY 2019 Amount
Authorized
FY 2019President’s Budget
Authority
Office of Medicare Hearings and Appeals, Social Security Act, Titles XVIII and XI
Indefinite 106,652
Indefinite $112,381
Total Appropriation ‐ 106,652 ‐ $112,381
Activity FY 2017 Final
FY 2018 Annualized
CR
FY 2019President’s Budget
Authority
Discretionary Budget Authority 107,381 106,652 112,381
Discretionary Budget Authority, FTE 603 690 705

13
Appropriation History Table
Details Budget Estimates to Congress
House Allowance
Senate Allowance
Appropriations
2009 ‐ ‐ ‐ ‐Trust Fund Appropriation 65,344,000 ‐ 63,864,000 64,604,000Subtotal 65,344,000 ‐ 63,864,000 64,604,000
2010 ‐ ‐ ‐ ‐Trust Fund Appropriation 71,147,000 71,147,000 71,147,000 71,147,000Subtotal 71,147,000 71,147,000 71,147,000 71,147,000
2011 ‐ ‐ ‐ ‐Trust Fund Appropriation 77,798,000 ‐ 77,798,000 71,147,000Rescissions (P.L. 112‐10) ‐ ‐ ‐ (142,000)Subtotal 77,798,000 ‐ 77,798,000 71,005,000
2012 ‐ ‐ ‐ ‐Trust Fund Appropriation 81,019,000 71,147,000 71,147,000 72,147,000Rescissions (P.L. 112‐74) ‐ ‐ ‐ (136,000)Subtotal 81,019,000 71,147,000 71,147,000 72,011,000
2013 ‐ ‐ ‐ ‐Trust Fund Appropriation 84,234,000 79,908,000 72,010,642Rescissions (P.L. 113‐6) ‐ ‐ ‐ (144,021)Sequestration (P.L. 112‐25) ‐ ‐ ‐ (3,622,567)Transfers ‐ ‐ ‐ 1,200,000
Subtotal 84,234,000 ‐ 79,908,000 69,444,0542014 ‐ ‐ ‐ ‐
Trust Fund Appropriation 82,381,000 ‐ 82,381,000 82,381,000 Subtotal 82,381,000 ‐ 82,381,000 82,381,0002015 ‐ ‐ ‐ ‐
Trust Fund Appropriation 100,000,000 ‐ ‐ 87,381,000 Subtotal 100,000,000 ‐ ‐ 87,381,0002016 ‐ ‐ ‐ ‐
Trust Fund Appropriation 140,000,000 ‐ ‐ 107,381,000Subtotal 140,000,000 ‐ ‐ 107,381,000
2017 ‐ ‐ ‐ ‐Trust Fund Appropriation 120,000,000 107,381,000 112,381,000 107,381,000
Subtotal 120,000,000 107,381,000 112,381,000 107,381,0002018 117,177,000 112,381,000 ‐ ‐ Subtotal 117,177,000 112,381,000 ‐ ‐2019 112,381,000 Subtotal 112,381,000

14
Narrative by Activity
Program Description and Accomplishments
OMHA opened its doors in July 2005 pursuant to the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) which sought to respond to the delays in processing of Medicare appeals that existed at the Social Security Administration (SSA) by establishing an Administrative Law Judge (ALJ) hearing forum dedicated solely to the adjudication of Medicare benefit appeals. According to the Government Accountability Office (GAO), SSA ALJs took on average 368 days to resolve appeals in 2003. While SSA had no statutory timeframe for case adjudication, the Medicare, Medicaid, and SCHIP Benefits Improvement and Protection Act of 2000 (BIPA) envisioned that most Medicare appeals would be decided by OMHA within 90 days of filing. Furthermore, the MMA provided for the addition of ALJs and staff as needed to insure for the “timely action on appeals before administrative law judges,” (MMA § 931(c), 117 Stat. 2398–99). However, since FY 2010, funding has not been appropriated at a level which would allow OMHA to handle the volume of appeals being received and a backlog of appeals awaiting disposition has developed. OMHA serves a broad sector of the public, including Medicare service providers and suppliers and Medicare beneficiaries who are often elderly and/or disabled. Ensuring that providers and suppliers have a forum for independent and timely resolution of their disputes over Medicare payments also contributes to the security of the Medicare system by encouraging the provider and supplier community to continue to provide services and supplies to Medicare beneficiaries. OMHA administers its program in six field offices, including Miami, Florida; Cleveland, Ohio; Irvine, California; Arlington, Virginia; Kansas City, Missouri; and Seattle, Washington. At the time of OMHA’s establishment, it was envisioned that OMHA would receive a traditional workload of Medicare Part A and Part B fee‐for‐service benefit claim appeals, and Part C Medicare Advantage program organization determination appeals. However, OMHA has seen an increased caseload due to the expansion of its original jurisdiction to include areas not originally envisioned to be within its authority. In 2007, OMHA was also given additional responsibility for conducting hearings and issuing decisions in Medicare Part B Income‐Related Monthly Adjustment Amount (IRMAA) appeals. OMHA also began receiving new cases as a result of the CMS Recovery Audit Contractor (RAC) program, which was piloted in six states beginning in 2007. This program included RAC reviews of Medicare Part A and Part B claims on a post‐payment basis, and reviews for Medicare Secondary Payer recoupments. In January 2010, the RAC program became permanent and was expanded to all 50 States. As a result of this expansion, OMHA received nearly 433,000 RAC appeals between FY 2013 and FY 2014, 50 percent of the total agency appeal receipts without receiving additional resources to handle this new workload. The number of RAC appeals declined from FY 2015 to FY 2017 due to the pause in the program while contracts were being re‐competed. Although the RAC expansion legislation provided funding for the administrative costs of the program at CMS, OMHA is functionally and fiscally independent of CMS, and OMHA’s administrative costs were not included in the legislation. Not only has the expansion of appeals from the RAC workload exacerbated OMHA’s workload challenges, but OMHA’s non‐RAC (traditional) workload also increased significantly. Between FY 2013 and FY 2014 OMHA also received 380,000 non‐RAC appeals as CMS contractors (for example, Medicare

15
Administrative Contractors and Zone Program Integrity Contractors) increased pre‐ and post‐payment reviews. Recognizing the importance of timely resolution of Medicare disputes, OMHA has taken a number of steps to maximize the productivity of its ALJ teams and improving the quality and timeliness of its services. These include:
The development of OMHA’s Electronic Case Adjudication Processing Environment (ECAPE) – March 2017 successful testing and roll out to the agency’s Central Operations Intake and Case Assignment Division
A revision to governing regulations (became effective on March 20, 2017) which expanded OMHA’s ability to process Level 3 appeals by authorizing attorney adjudicators to decide appeals that can be resolved without a hearing before an ALJ, adopted a number of processing efficiencies at OMHA, and resolved many areas of confusion among stakeholders
Prioritization of beneficiary appeals to optimize timely adjudication of beneficiary appeals
A re‐engineered field office staffing structure, allocating more of its funding to direct case‐support functions (a step which has allowed OMHA to increase ALJ support to include two legal assistants and two attorneys per ALJ)
An OMHA Case Policy Manual (OCPM) initiative to develop OMHA‐wide common business practices for the adjudicative process
A National Substantive Legal Training Program for new ALJs and attorneys and yearly judicial education to increase consistency in decision‐making and address program integrity issues
Strategic case assignments to assign appellants with a large number of filings to a single ALJ (these “big box” assignments are then rotated among ALJs in accordance with the Administrative Procedure Act), facilitating potential consolidated proceedings and more efficient adjudication
A Statistical Sampling Pilot to resolve large groups of appeals
Settlement Conference Facilitation as a less costly alternative to ALJ hearings
A Senior Attorney screening program to assist with identification and resolution of appeals which can be resolved without a hearing
Utilization of the Office of Personal Management’s Senior ALJ program, which allows for the reemployment of retired ALJs on a temporary and part‐time basis

16
Funding History
Fiscal Year Amount
FY 2014 $82,381,000
FY 2015 $87,381,000
FY 2016 $107,381,000
FY 2017 $107,381,000
FY 2018 Annualized CR $106,652,000
FY 2019 Budget Request
The FY 2019 President’s Budget request for the Office of Medicare Hearings and Appeals (OMHA) is $251,060,000; an increase of $144,408,000 over the FY 2018 Annualized CR level of $106,652,000. This request includes $112,381,000 in discretionary budget authority, $125,000,000 in proposed mandatory funding, $10,000,000 in proposed access to RAC collections, $3,679,000 in proposed user fee collections, and a suite of legislative proposals to address the backlog of Medicare appeals and improve the Medicare appeals process. This request will allow OMHA to implement HHS and OMHA strategic initiatives to reduce the backlog and improve the Medicare appeals process by more than doubling adjudicatory capacity, improving processing time, reducing overall cost of adjudication per claim, and eliminating the gap between yearly appeals receipts and adjudication capacity. Between FY 2010 and FY 2017, OMHA's appeals receipt total measured over 1.6 million appeals. OMHA experienced its most significant challenges during FY 2013 and FY 2014. OMHA’s appeal receipts grew by 228 percent in FY 2013 (from 117,000 appeals in FY 2012, to 384,000 appeals in FY 2013) while funding levels decreased by 4 percent from the prior year. In FY 2014, OMHA received a record 474,000 new appeals and struggled with fairly stagnant funding levels during the year. During each subsequent year, receipts have dropped slightly due to initiatives implemented at CMS in order to curb appeal levels at OMHA, but have continued to vastly outpace OMHA’s adjudication capacity. Thus, OMHA has been unable to recover from the backlogs developed in FY 2013 and FY 2014, or to keep up with incoming receipt levels. Despite the decline in FY 2015 to FY 2017 receipt levels, partly due to the temporary pause in the RAC program, OMHA still has nearly six years of backlogged work for its staff of 92 ALJ teams. Adjudication Expansion Initiative (AEI)
Despite agency‐wide initiatives to streamline business processes, workload demands upon OMHA’s ALJs have exceeded their sustainable capacity for case adjudication. This initiative will allow OMHA to increase its staffing levels above its planned FY 2018 Annualized CR level by up to 775 new positions. These positions will be brought on incrementally during FY 2019 equating to 190 FTE in FY 2019. The full impact of the additional positions will be realized in subsequent fiscal years. These additional resources will support up to five new field offices, the full expansion of the Seattle and Arlington field offices, and the augmentation of Headquarters operations necessary to support the expanded administrative, training, oversight and quality assurance requirements associated with the expansion. The additional resources include up to 106 new ALJ teams nationwide above the agency’s current 92 teams. Once these new teams have been trained and have become fully productive, their collective adjudication will increase OMHA’s output by 106,000 additional dispositions per year (a 125% increase in adjudicatory capacity). This strategy will enable OMHA to expedite backlog reduction efforts and improve

17
adjudication timeframes, while increasing staff towards a level that can address projected future receipts. The full impact of these additional ALJ teams will be realized in FY 2020 when the teams reach their full annual adjudication capacity.
OMHA will also invest in the hiring of 15 FTE to support its Attorney Adjudicator program. OMHA now has regulatory authority to allow attorney‐adjudicators to decide appeals that can be resolved without a hearing before an ALJ. Although the appellant must waive its right to an oral hearing to use this process, OMHA is optimistic that appellant interest in the program will allow for 5,000 dispositions in FY 2018. In addition, these new senior attorneys will support other administrative initiatives such as Settlement Conference Facilitation (SCF). OMHA has been encouraged by the results of SCF, which to date has resolved over 70,000 appeals or the equivalent of one year of work for 70 ALJ teams. While administrative efforts such as SCF are beneficial, they are insufficient to fully reduce the pending workload or manage new incoming receipts. The U. S. Government Accountability Office (GAO) has concurred that, despite these HHS actions, “the Medicare appeals backlog continues to grow at a rate that outpaces the adjudication process and will likely persist.” A summary of all GAO findings and recommendations, and a copy of the report are available through the GAO website at http://www.gao.gov/products/GAO‐16‐366. Medicare Magistrate Program
A portion of claims and coverage determinations appealed to OMHA involve an amount in controversy (AIC), or amount in dispute, that is far below the cost to adjudicate the claim. Therefore, OMHA has sought authority through a legislative proposal in the FY 2019 Budget for a Medicare Magistrate program in which senior attorneys would serve as independent adjudicators with binding decisional authority in cases with an AIC below the Federal District Court judicial review threshold.
Magistrates would adjudicate these lower value appeals based on a review of the record (in place of a hearing), resulting in a significant reduction in the overall time and cost of adjudications, and bringing the cost for adjudication of these appeals more in line with the amount at issue. This initiative is an ideal model to maximize the use of the agency’s most costly resource (ALJs) to conduct hearings and create a record on appeals in cases in which the amount in controversy is sufficient to allow an appeal to Federal court.
The FY 2019 request will allow OMHA to staff 100 magistrates and the required support positions. These new positions will be brought on incrementally during FY 2019 and equate to 55 FTE. The full impact of the additional positions will be realized in subsequent fiscal years. OMHA estimates these additional resources would further increase adjudication capacity by an estimated 75,000 appeals annually at a savings of 43% compared to an ALJ team.
Proposed Law – Improving the Medicare Appeals Process
The Budget also includes the following legislative proposals to improve the Medicare appeals process:
Provide Additional Resources for Medicare Appeals: This proposal would provide the Office of Medicare Hearings and Appeals (OMHA) and the Departmental Appeals Board (DAB) mandatory funding to address the backlog of pending appeals. The Secretary is authorized to transfer funding across levels 3 and 4 of the appeals system. Remand Appeals to the Redetermination Level with the Introduction of New Evidence: This proposal would remand an appeal to the first level of appeal when new documentary evidence is submitted into

18
the administrative record at the second level of appeal or above. Exceptions may be made if evidence was provided to the lower level adjudicator but erroneously omitted from the record, or an adjudicator denies an appeal on a new and different basis than earlier determinations. This proposal incentivizes appellants to include all evidence early in the appeals process and ensures the same record is reviewed and considered at subsequent levels of appeal.
Increase Minimum Amount in Controversy for ALJ Adjudication of Claims to Equal Amount Required for Judicial Review: This proposal increases the minimum amount in controversy required for adjudication by an ALJ to the Federal District Court amount in controversy requirement ($1,600 in calendar year 2018 and updated annually). This would allow the amount at issue to better align with the amount spent to adjudicate the claim. Appeals not reaching the minimum amount in controversy would be adjudicated by a Medicare magistrate.
Establish Magistrate Adjudication for Claims with Amount in Controversy Below New ALJ Amount in Controversy Threshold: As described above, this proposal allows OMHA to use Medicare magistrates for appealed claims below the Federal District Court amount in controversy threshold ($1,600 in calendar year 2018 and updated annually), reserving ALJs to conduct hearings and create the record on appeal in cases which have a higher amount in controversy and can reach Federal court.
Expedite Procedures for Claims with No Material Fact in Dispute: This proposal allows OMHA to issue decisions without holding a hearing if there is no material fact in dispute. These cases would include appeals, for example, in which Medicare does not cover the cost of a particular drug or the ALJ cannot find in favor of an appellant due to binding limits on authority.
Change the Medicare Appeal Council’s Standard of Review: Change the Medicare Appeals Council’s (Council) standard of review under Section 1869(d)(2)(B) of the Social Security Act from de novo to an appellate‐level standard of review. Under the proposed standard of review, the Council would be able to grant a request for review of a decision by an ALJ or other adjudicator of Medicare claims if: (1) there is an abuse of discretion; (2) there is an error of law material to the outcome of the case; (3) the findings of fact are not supported by substantial evidence; or (4) there is a need to clarify an important question of law, policy, or fact. The proposal would also clarify that the Council may deny a request for review.
Limit Appeals When No Documentation is Submitted: Limit the right to appeal a redetermination of a claim denied because no documentation was submitted to support the items or services billed, unless the appeal was filed by a beneficiary who is financially responsible for the items or services. If the necessary documentation is not submitted to the Qualified Independent Contractor (QIC) at Level 2, the request for reconsideration would be dismissed.
Require a Good‐Faith Attestation on all Appeals: Require all appellants to include in their appeal an attestation that they are submitting the appeal under a good‐faith belief that they are entitled to Medicare reimbursement. This proposal would also provide the Secretary the authority to sanction or impose civil monetary penalties on appellants who are found to be submitting appeals not in good‐faith. Appellants would be provided a right to challenge a sanction through an administrative review or judicial review. The Secretary would be provided the authority to establish criteria for determining when an appellant is not filing in good faith and associated remedies through regulation.
Establish a Post‐Adjudication User fee for Unfavorable Appellants at the 3rd and 4th Levels of Appeal: This proposal would establish a post‐adjudication user fee for Medicare Parts A and B claim appeals filed by a provider or supplier, or a State Medicaid Agency (SMA), with respect to appeals that are unfavorable to the appellant (that is, the outcome did not change from the prior level of appeal), and for appeals that

19
are dismissed. The user fee could be waived by the Secretary if the appealed claim were resolved through settlement or alternate dispute resolution.
The purpose of post‐adjudication user fee is to improve the responsiveness of the appeals process by reinvesting funds (e.g., hiring more staff to increase the number of appeals completed and decrease the length of time for review), to partially offset the government’s costs of processing appeals, and to encourage appellants to more carefully assess the merits of their appeals. Summary The FY 2019 President’s Budget is a critical step to enable OMHA to make significant strides in reducing the backlog and eliminating the gap between projected incoming receipts and resources. It is clear that OMHA will not be able to resolve the backlog until its adjudication capacity exceeds its projected receipt levels. With the proposed investment in additional adjudicatory resources, OMHA will be able to manage its projected incoming receipts for the first time in eight years, halt the growth in the backlog of appeals, begin to adjudicate the backlog of pending appeals, and ultimately return to the 90‐day processing times envisioned by statue.
Outputs and Outcomes Table Program/Measure Year and Most
Recent Result / Target for Recent Result / (Summary
of Result)
FY 2018 Target
FY 2019Target
FY 2019 Target +/‐FY 2018 Target
Reduce the percentage of decisions reversed or remanded on appeals to the Medicare Appeals Council
FY 2017: 0.6% Target: 1.0% (Target Exceeded)
1.0% 1.0% Maintain
Retain average results from appellants reporting good customer service on a scale of 1‐5 at the Medicare Appeals level
FY 2017: 3.9% Target: 3.4% (Target Exceeded)
3.4 3.4 Maintain

20
Budget Authority by Object Class (Dollars in Thousands)
Object Class Code
Description FY 2017 Final
FY 2018 Annualized CR
FY 2019 President’s Budget
11.1 Full‐time permanent 54,655 60,542 94,765
11.5 Other personnel compensation 453 526 701
Subtotal Personnel Compensation 55,108 61,068 95,466
12.1 Civilian personnel benefits 18,269 20,099 31,272
Total Pay Costs 73,377 81,167 126,738
21.0 Travel and transportation of persons 201 200 460
22.0 Transportation of things 266 266 905
23.1 Rental payments to GSA 8,374 7,379 10,969
23.3 Communications, utilities, and misc. charges 3,947 3,693 11,957
24.0 Printing and reproduction 177 184 251
25.2 Other services from non‐Federal sources 8,604 765 30,850
25.3 Other goods and services from Federal sources 9,211 10,090 21,008
25.4 Operation and maintenance of facilities 853 853 38,535
25.7 Operation and maintenance of equipment 954 954 1,047
26.0 Supplies and materials 421 485 2,910
31.0 Equipment 818 616 5,430
Total Non‐Pay Costs 33,826 25,485 124,332
Total Budget Authority by Object Class 107,203 106,652 251,060
Average Cost per FTE 122 118 133
FTE 603 690 950
AverageSalary 91 88 100

21
Salaries and Expenses (Dollars in Thousands)
Object Class Code
Description FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
11.1 Full‐time permanent 54,655 60,542 94,765
11.5 Other personnel compensation 453 526 701
Subtotal Personnel Compensation 55,108 61,068 95,466
12.1 Civilian personnel benefits 18,269 20,099 31,272
Total Pay Costs 73,377 81,167 126,738
21.0 Travel and transportation of persons 201 200 460
22.0 Transportation of things 266 266 905
23.3 Communications, utilities, and misc. charges 3,947 3,693 11,957
24.0 Printing and reproduction 177 184 251
25.2 Other services from non‐Federal sources 8,604 765 30,850
25.3 Other goods and services from Federal sources 9,211 10,090 21,008
25.4 Operation and maintenance of facilities 853 853 38,535
25.7 Operation and maintenance of equipment 954 954 1,047
Subtotal Other Contractual Services 24,213 17,005 105,013
26.0 Supplies and materials 421 485 2,910
Subtotal Non‐Pay Costs 24,634 17,490 107,923
Total Salary and Expenses 98,011 98,567 234,661
23.1 Rental payments to GSA 8,374 7,379 10,969
Total Salaries, Expenses, and Rent 106,385 106,036 245,630
Total Direct FTE 603 690 950

22
Detail of Full Time Equivalents
Detail
FY 2017 Final
Civilian
FY 2017 Final
Military
FY 2017 Final Total
FY 2018 Estimate Civilian
FY 2018 Estimate Military
FY 2018 Estimate Total
FY 2019 Estimate Civilian
FY 2019 Estimate Military
FY 2019 Estimate Total
Direct 603 ‐ 603 690 ‐ 690 950 ‐ 950
Reimbursable ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
Total FTE 603 ‐ 603 690 ‐ 690 950 ‐ 950
Fiscal Year Average GS
FY 2015 11/5
FY 2016 11/5
FY 2017 11/3
FY 2018 11/2
FY 2019 11/2

23
Detail of Positions
Detail
FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
ALJ I 1 1 1
ALJ II 7 7 12
ALJ III 86 86 187
Subtotal 94 94 200
Total – ALJ Salaries 14,789,567 15,570,630 33,129,000
ES 3 3 4
Total ‐ ES Salaries 509,122 519,482 669,482
GS‐15 15 15 33
GS‐14 34 36 152
GS‐13 52 57 111
GS‐12 168 176 202
GS‐11 70 76 76
GS‐10 ‐ ‐ ‐
GS‐9 24 30 339
GS‐8 114 130 196
GS‐7 37 43 49
GS‐6 22 29 280
GS‐5 15 20 51
GS‐4 7 7 17
GS‐3 ‐ ‐ ‐
GS‐2 ‐ ‐ ‐
GS‐1 ‐ ‐ ‐
Subtotal 558 619 1,506
Total ‐ GS Salary
39,809,271 43,831,888 60,966,518
Total Positions 655 716 1,710
Total FTE 603 690 950
Average ALJ Salary
157,336 163,064 165,645
Average ES salary 169,707 173,161 167,371
Average GS grade 11/3 11/2 11/2
Average GS Salary 66,019 63,524 64,175

Office for Civil Rights

DEPARTMENT of HEALTH
and HUMAN SERVICES
Fiscal Year 2019
Office for Civil Rights
Justification of Estimates for Appropriations Committees

/'uvrca.,."'
( 4- DEPARTMENT OF HEALTH & HUMAN SERVICES
",�
OFFICE OF THE SECRETARY
I am pleased to present the Office for Civil Rights (OCR) Fiscal Year 2019 Congressional Justification. This
budget supports the President's and Secretary's priority initiatives and reflects the goals and objectives
of the Department.
This budget submission supports the Administration's initiative to reduce federal spending and increase
government efficiencies, while still fulfilling OCR's vital mission. To this end, OCR will continue to seek
creative cost savings and productivity increases. In an environment of fiscal restraint, OCR will
supplement its enforcement of the Health Insurance Portability and Accountability Act (HIPAA) with
monetary settlements collected via OCR's HIPAA enforcement activities. In this way, OCR will continue
its robust enforcement mission to ensure that the public is protected to the fullest extent of the law.
OCR has implemented an important new initiative in support of the Administration's priority to
"vigorously enforce Federal law's robust protections for religious freedom," as announced in Executive
Order 13798, "Promoting Free Speech and Religious Liberty." In FY 2018, OCR created a Conscience and
Religious Freedom Division as a new component of its Headquarters' operations, dedicated exclusively
to enforcing laws that protect conscience and religious exercise, and that prohibit coercion and religious
discrimination in health care and human services. This new Division is reflected in OCR's FY 2019 budget
request.
This is an exciting time for OCR. With the establishment of the new Conscience and Religious Freedom
Division and many new efficiencies and innovations occurring throughout the other OCR Divisions, OCR
is poised to tinue to provide the American People with exemplary service and support in all aspects
of its op ti
R er Severino
Director, Office for Civil Rights
Page?

Office for Civil Rights
Page 3
Table of Contents
Section I: Introductory Items Organization Chart ........................................................................................................................................ 4 Section II: Executive Summary Introduction and Mission .............................................................................................................................. 6 Overview of the Budget Request .................................................................................................................. 7 Overview of Performance ............................................................................................................................. 8 All‐Purpose Table ........................................................................................................................................ 11 Section III: Office for Civil Rights Budget Exhibits
Appropriations Language ..................................................................................................................... 12 Amounts Available for Obligation ........................................................................................................ 13 Summary of Changes ............................................................................................................................ 14 Budget Authority by Activity ................................................................................................................ 15 Authorizing Legislation ......................................................................................................................... 16 Appropriations History ......................................................................................................................... 17
Activity Narratives Summary of the Request ...................................................................................................................... 19 Civil Rights Division ............................................................................................................................... 20 Health Information Privacy Division ..................................................................................................... 24 Conscience and Religious Freedom Division ....................................................................................... 28 Operations and Resources Division ...................................................................................................... 30
Section IV – Supplementary Tables Budget Authority by Object Class ............................................................................................................... 35 Salaries and Expenses ................................................................................................................................. 36 Detail of Full‐Time Equivalent Employment (FTE) ...................................................................................... 37 Detail of Positions ....................................................................................................................................... 38 Section V – Significant Items OCR Response to Appropriations Committee Report ................................................................................ 39

Office for Civil Rights
Page 4
Section I: Introductory Items
Organization Chart (January 2018)
Director
Roger Severino
Principal Deputy Chief of Staff
Robinsue Frohboese March Bell
Deputy Director, Civil Rights Division
Deputy Director, Health Information Privacy Division
Deputy Director, Conscience and
Religious Freedom Division
Deputy Director, Operations and
Resources Division
Vacant Timothy Noonan * Vacant Steve Novy
New England Region
Susan Rhodes
Eastern and Caribbean Region
Linda Colon
Mid‐Atlantic Region
Barbara Holland
Southeast Region
Timothy Noonan
Midwest Region
Steven Mitchell *
Southwest Region
Marisa Smith
Rocky Mountain Region
Andrea Oliver
Pacific Region
* = Acting Michael Leoz

Office for Civil Rights
Page 5
Organizational Chart: Text Version
Office for Civil Rights
Director Roger Severino
Principal Deputy Robinsue Frohboese
Chief of Staff March Bell The following offices report directly to the Director: 1 Deputy Director, Civil Rights Division 1.2 Vacant 2 Deputy Director, Health Information Privacy Division 2.2 Timothy Noonan (Acting) 3 Deputy Director, Conscience and Religious Freedom Division 3.2 Vacant 4 Deputy Director, Operations and Resources Division 4.2 Steve Novy
The following regional managers report to the Deputy Director, Enforcement and Regional Operations:
Susan Rhodes, New England Region
Linda Colon, Eastern & Caribbean Region
Barbara Holland, Mid‐Atlantic Region
Timothy Noonan, Southeast Region
Steven Mitchell (Acting), Midwest Region
Marisa Smith, Southwest Region
Andrea Oliver, Rocky Mountain Region
Michael Leoz, Pacific Region
Office for Civil Rights
Page 6
Section II: Executive Summary
Introduction and Mission The Office for Civil Rights (OCR), a staff division in the Office of the Secretary of the U.S. Department of Health and Human Services (HHS), ensures that individuals receiving services from HHS‐conducted or HHS‐funded programs are not subject to unlawful discrimination, individuals and entities can exercise their conscience and religious freedom rights, and people can trust the privacy, security, and availability of their health information. By rooting out discrimination and removing unlawful barriers to HHS‐conducted or HHS‐funded services, OCR carries out the HHS mission of improving the health and well‐being of all Americans and providing essential human services. By ensuring individuals and institutions can exercise their conscience rights, OCR furthers justice and tolerance in a pluralistic society. By promoting the right to access health information and protecting the privacy and security of this information, OCR helps empower people’s health care decision‐making and helps ensure the integrity of the health care system, both of which promote better health outcomes for the nation. Mission As the enforcement agency for HHS's civil rights, conscience and religious freedom, and health privacy rights law, OCR investigates complaints, enforces rights, and promulgates regulations, develops policy and provides technical assistance and public education to ensure understanding of and compliance with non‐discrimination and health information privacy laws. OCR accomplishes this by:
Ensuring that recipients of HHS federal financial assistance comply with federal civil rights laws that prohibit discrimination on the basis of race, color, national origin, disability, age, sex, and religion.
Ensuring that Federal agencies, state and local governments, health care providers, health plans, and others comply with federal laws guaranteeing the exercise of religious beliefs and moral convictions in HHS conducted or funded programs.
Ensuring the practices of health care providers, health plans, healthcare clearinghouses, and their business associates adhere to federal privacy, security, and breach notification regulations under the Health Insurance Portability and Accountability Act (HIPAA), as amended, through the investigation of complaints, self‐reports of breaches, compliance reviews, and audits.
Vision OCR enforces the laws prohibiting discrimination, including discrimination against those who exercise conscience and religious freedom rights, and protecting the rights of individuals to access their health information and the privacy and security of this information. Through these mechanisms, OCR helps to ensure equal access to health and human services, advances the health and well‐being of all Americans, protect individuals’ private health information, and provides the tools for provider awareness and full consumer engagement in decisions related to their health care.

Office for Civil Rights
Page 7
Overview of Budget Request OCR’s FY 2019 President’s Budget request of $30,904,000 discretionary budget authority represents a $7,631,000 decrease from the FY 2018 Annualized Continuing Resolution (CR) level of $38,535,000. In FY 2019 OCR will utilize $13,477,000 in monetary settlement funds; a Total Program Level of $44,381,000. The request supports OCR’s role in defending the public’s right to nondiscriminatory access to HHS funded health and human services, conscience and religious freedom, and access to, and the privacy and security of, individually identifiable health information. Program increases: Conscience and Religious Freedom (+$1.546 million): The increase allows for the expansion of this new division to perform policy, enforcement, and outreach activities. Funding consists of pay (+5 FTEs), attorney support services, and non‐pay costs to support Division operations. This important change to OCR’s organizational structure focuses on key policy, enforcement, and outreach activities. Program decreases: Health Information Privacy Division (‐$1.283 million Total Program Level): The HIP Division decrease of $1,283,000 reflects the reduction of funding from appropriations for pay, non‐pay, and contract costs to support HIPAA matters. As allowed by law, OCR will utilize monetary settlement funding collected from HIPAA enforcement activities to offset the decrease in appropriated funding. Operations and Resource Division (‐$4.632 million Total Program Level): ORD enforces OCR legal authorities, conducts investigations of all HIPAA complaints and high impact cases via its eight regions located nationwide. The ORD decrease of $4,632,000 reflects reductions in regional contract staff who work on HIPAA matters, contractual services related to legal services, information technology (IT) support, and service and supply fund costs. As allowed by law, OCR will utilize monetary settlement funding collected from HIPAA enforcement activities to offset the decrease in appropriated funding. Civil Rights (‐$0.312 million): This decrease reflects the transfer of attorney services and other support costs to the newly established Conscience and Religious Freedom Division, as it assumes these functions from the Civil Rights Division.

Office for Civil Rights
Page 8
Overview of Performance OCR’s overarching goals encompass multiple supporting objectives.
OCR Goal OCR Supporting Objectives
1. Raise awareness, increase understanding, and ensure compliance with all federal laws requiring non‐discriminatory access to HHS funded programs and protect the privacy and security of personal health information
A. Increase access to and receipt of non‐discriminatory quality health and human services while protecting the integrity of HHS federal financial assistance
B. Protect the privacy and security of personally identifiable health information for healthcare consumers (HIPAA rule activities and enforcement)
C. Provide information, public education activities, and training to representatives of health and human service providers, other interest groups, and consumers (Civil rights and health information privacy mission activities)
D. Increase the number of covered entities that take corrective action, including making substantive policy changes or developing new policies as a result of review and/or intervention
2. Enhance operational efficiency
A. Maximize efficiency of operations by streamlining processes and the optimal allocation of resources
B. Improve financial management and the integration of budget and performance data (Increase resource management process oversight, strengthen internal controls, maintain viable performance objectives)
C. Advance human capital management (Provide training, develop and mentor subordinates, promote effectiveness)

Office for Civil Rights
Page 9
The following Outputs and Outcomes Table presents the current OCR performance measures and results
along with the proposed FY 2019 targets:
Program/Measure Year and Most Recent Result /Target for Recent Result /
(Summary of Result)
FY 2018 Target
FY 2019 Target
FY 2019 Target+/‐
FY 2018 Target
#1 The number of covered entities taking corrective actions as a result of OCR intervention per year (Outcome)
FY 2017: 1523Target: 3,000 (Target Not Met)
1,000 1,000 Maintain
#2 The number of covered entities making substantive policy changes as a result of OCR intervention/year (Outcome)
FY 2017: 322 Target: 750 (Target Not Met)
250 250 Maintain
#3 Percent of closure for civil rights cases/ cases received each year (Outcome)
FY 2017: 81%Target: 90% (Target Not Met)
90% 90% Maintain
#4 Percent of closure for health information privacy cases/cases received each year (Outcome)
FY 2017: 98%Target: 80% (Target Exceeded)
90% 90% Maintain
#5 Percent of civil rights complaints requiring formal investigation resolved within 365 days (Output)
FY 2017: 71%Target: 41% (Target Exceeded)
41% 50% +9%
#6 Percentage of civil rights complaints not requiring formal investigation resolved within 180 days (Output)
FY 2017: 94% Target: 95% (Target Not Met)
95% 95% Maintain
#7 Percentage of health information privacy complaints requiring formal investigation resolved within 365 days (Output)
FY 2017: 74% Target: 68% (Target Exceeded)
68% 70% +2%
#8 Percentage of health information privacy complaints not requiring formal investigation resolved within 180 days (Output)
FY 2017: 97% Target: 95% (Target Exceeded)
95% 95% Maintain
In FY 2017, OCR exceeded its target for resolving its most complex health information privacy (HIP) cases (#7, Target: 68%, FY 2017 Actual: 74%) and its most complex civil rights enforcement work (#5, Target 41%, FY 2017 Actual: 71%) requiring formal investigation within 365 days. The timely completion of OCR’s most complex cases through formal investigation represents one of the most meaningful measures of the continued improvements being made by OCR towards fulfilling its core mission. As a law enforcement agency, OCR speaks to the regulated community, advocacy groups and individuals about compliance with the laws that OCR enforces, and OCR’s legal priorities through its completed investigations and letters of findings. OCR exceeded its productivity and closure targets for health information privacy cases by closing a high percentage of cases (#4, Target: 80%, FY 2017 Actual: 98%). This continues to be a high growth area for OCR, as the receipt of health information privacy cases increased 18% from FY 2016. OCR missed its target for civil rights cases (#3, Target: 90%, FY 2017 Actual: 81%). OCR experienced a 48% increase in civil rights cases from FY 2016. Additionally, on December 31, 2016, the Northern District Court of Texas issued an order in Franciscan Alliance, Inc. et al v. Burwell, enjoining HHS from enforcing, on a

Office for Civil Rights
Page 10
nationwide basis, the provisions of the regulation implementing Section 1557 of the Affordable Care Act that prohibit discrimination based on gender identity or termination of pregnancy. As a result of this injunction, OCR implemented a process in collaboration with the Office of General Counsel to review all complaints alleging sex discrimination to determine whether there was any potential for violating the injunction. This extra measure was necessary to ensure that the Department did not violate the injunction, but a consequence of this protective measure was the reduction of civil rights cases being processed and closed due to the extra time needed for OGC’s careful review of the cases. OCR anticipates that when the litigation is concluded, OCR will return to meeting or exceeding the target for civil rights. OCR did not meet its target for the performance objective for investigated complaints resulting in corrective action (#1, Target: 3,000 cases closed with corrective action, FY 2017 Actual: 1,523), and the number of covered entities making substantive policy changes (#2, Target: 750 cases closed with corrective action, FY 2017 Actual: 322). In response to yearly increases in complaints receipts, in FY 2016, OCR eliminated the review of Medicare Applications. OCR anticipated that there would be a reduction in the number of corrective actions and substantive changes in policy when this was eliminated and accordingly set the FY 2018 targets for 1,000 and 250 respectively. The elimination of the Medicare Applications has reduced OCR’s output of corrective actions, but it has allowed OCR to focus its resources on complex investigations, which yield greater impact on the regulated industry and the people affected by discrimination or the violation of health information privacy. OCR also continues to effectuate corrective action in other ways. A large number of complaints are resolved by OCR through the provision of technical assistance to the named entity without a formal investigation. These cases involve simple issues that, if substantiated, could easily be addressed by the entity with voluntary corrective action. The use of technical assistance to resolve these types of complaints is an efficient way for OCR to use its resources by notifying its regulated community about potential compliance deficiencies and requesting the entity to take any necessary voluntary corrective action. With regard to the management of administrative closures and the provision of technical assistance to cases that will not lead to a formal investigation, OCR has achieved significant and sustained success in two of its primary measures on timeliness (#6, Target: 95%, FY 2017 Actual: 94% and #8, Target: 95%, FY 2017 Actual: 97%). OCR increased the targets to 95% for the administrative closures for civil rights and HIP complaints from the previous targets of 80% and 75% respectively. These new targets present a significant challenge to OCR as OCR experienced a 23% increase in complaint receipts from FY 2016. However, continued innovations within the Centralized Case Management Operation section, where all new cases are triaged, has enabled OCR to sustain greater successes in case processing then realized in previous fiscal years, thus allowing the regional offices, which are the investigative units within OCR to apply their resources to investigations, technical assistance and outreach. Moving forward, OCR believes that these challenging targets will be met.

Office for Civil Rights
Page 11
All Purpose Table (Dollars in Thousands)
Activity FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 President’s Budget +/‐
FY 2018 Annualized
CR
Civil Rights Division 4,525 4,565 4,253 ‐312
Health Information Privacy Division
Budget Authority 4,156 4,802 1,519 ‐3,283
Civil Monetary Settlement Funds 1,745 2,245 4,245 +2,000
Total 5,901 7,047 5,764 ‐1,283
Conscience and Religious Freedom Division ‐ 602 2,148 +1,546
Operations and Resources Division
Budget Authority 30,027 28,566 22,984 ‐5,582
Civil Monetary Settlement Funds 6,382 8,282 9,232 +950
Total 36,409 36,848 32,216 ‐4,632
Discretionary Budget Authority 38,708 38,535 30,904 ‐7,631
Total Program Level 46,835 49,062 44,381 ‐4,681
FTE 150 153 148 ‐5

Office for Civil Rights
Page 12
Section III: Office for Civil Rights
Appropriations Language
For expenses necessary for the Office for Civil Rights, [$38,798,000] $30,904,000.

Office for Civil Rights
Page 13
Amounts Available for Obligation (Dollars in Thousands)
Detail FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
Appropriation 38,798 38,798 30,904
Across‐the‐board reductions ‐ ‐263 ‐
Subtotal, Adjusted Appropriation 38,798 38,535 30,904
Transfer of Funds to ACF ‐90 ‐ ‐
Subtotal, Adjusted General Fund Discretionary App 38,708 38,535 30,904
Total, Discretionary Appropriation 38,708 38,535 30,904

Office for Civil Rights
Page 14
Summary of Changes (Dollars in Thousands)
Budget Year and Type of Authority Dollars FTE
FY 2018 Annualized CR 38,535 153
FY 2019 President’s Budget 30,904 148
Net Change ‐7,631 ‐5
Program Increases
FY 2018Annualized
CR FTE
FY 2018Annualized
CR BA
FY 2019President’s Budget FTE
FY 2019 President’s Budget BA
FY 2019+/‐
FY2018 FTE
FY 2019+/‐
FY2018 BA
Comm, utilities, and misc. charges ‐ 249 ‐ 258 ‐ +9
Oth svcs from non‐fed sources ‐ 504 ‐ 510 ‐ +6
Opns and maint of facilities ‐ 433 ‐ 438 ‐ +5
Other personnel compensation ‐ 307 ‐ 311 ‐ +4
Opns and maint of equipment ‐ 377 ‐ 381 ‐ +4
Military personnel ‐ 94 ‐ 96 ‐ +2
Printing and reproduction ‐ 68 ‐ 70 ‐ +2
Military benefits ‐ 36 ‐ 37 ‐ +1
Transportation of things ‐ 2 ‐ 3 ‐ +1
Other than full‐time permanent ‐ 793 ‐ 793 ‐ ‐
Benefits for former personnel ‐ 20 ‐ 20 ‐ ‐
Equipment ‐ 30 ‐ 30 ‐ ‐
Total Increases ‐ 2,913 ‐ 2,947 ‐ +34
Program Decreases
FY 2018Annualized
CR FTE
FY 2018Annualized
CR BA
FY 2019President’s Budget FTE
FY 2019 President’s Budget BA
FY 2019+/‐
FY2018 FTE
FY 2019+/‐
FY2018 BA
Oth G&S from fed sources ‐ 9,883 ‐ 3,230 ‐ ‐6,653
Full‐time permanent 153 16,136 148 15,558 ‐5 ‐578
Rental payments to GSA ‐ 3,342 ‐ 3,108 ‐ ‐234
Civilian personnel benefits ‐ 5,771 ‐ 5,586 ‐ ‐185
Travel and transportation of persons ‐ 363 ‐ 349 ‐ ‐14
Supplies and materials ‐ 127 ‐ 126 ‐ ‐1
Total Decreases ‐ 35,622 ‐ 27,957 ‐ ‐7,665
Program Decreases
FY 2018Annualized
CR FTE
FY 2018Annualized
CR BA
FY 2019President’s Budget FTE
FY 2019 President’s Budget BA
FY 2019+/‐
FY2018 FTE
FY 2019+/‐
FY2018 BA
Total Increases ‐ 2,913 ‐ 2,947 ‐ +34
Total Decreases ‐ 35,622 ‐ 27,957 ‐ ‐7,665
Total Net Change 153 38,535 148 30,904 ‐5 ‐7,631

Office for Civil Rights
Page 15
Budget Authority by Activity (Dollars in Thousands)
Activity FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’sBudget
Civil Rights Division 4,525 4,565 4,253
Health Information Privacy Division 4,156 4,802 1,519
Conscience and Religious Freedom Division ‐ 602 2,148
Operations and Resources Division 30,027 28,566 22,984
Total, Budget Authority 38,708 38,535 30,904
FTE 150 153 148
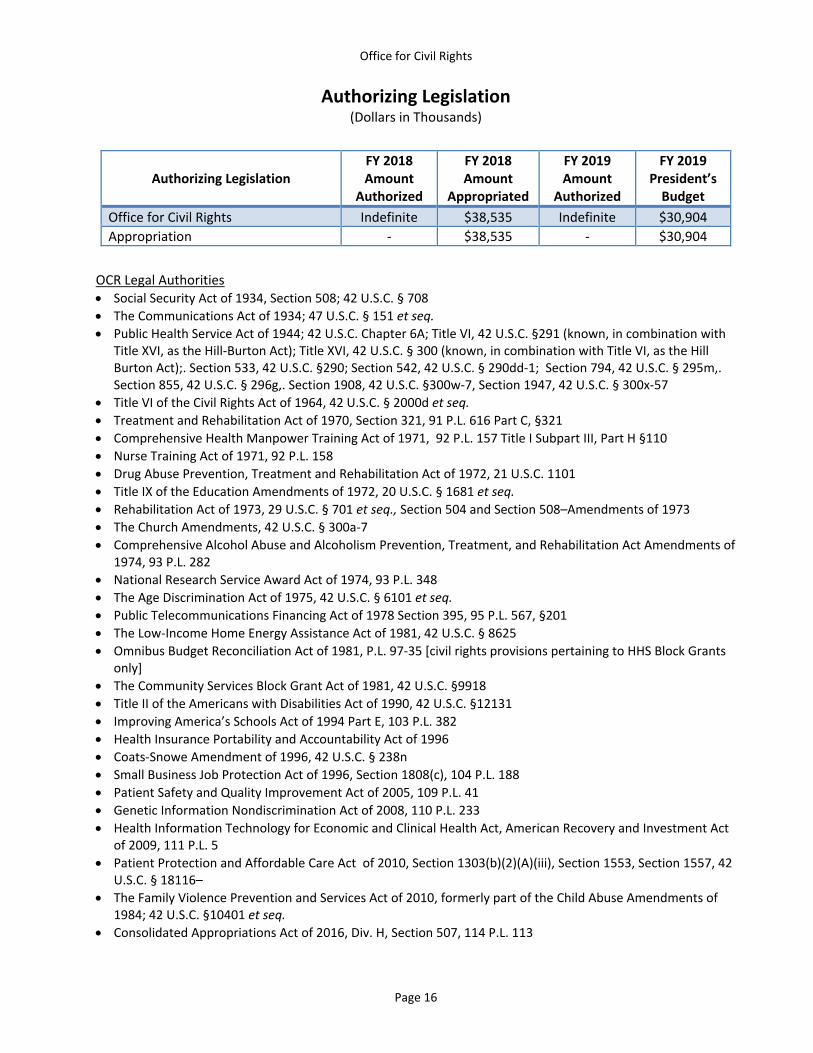
Office for Civil Rights
Page 16
Authorizing Legislation (Dollars in Thousands)
Authorizing Legislation FY 2018 Amount
Authorized
FY 2018 Amount
Appropriated
FY 2019 Amount
Authorized
FY 2019 President’s Budget
Office for Civil Rights Indefinite $38,535 Indefinite $30,904
Appropriation ‐ $38,535 ‐ $30,904
OCR Legal Authorities Social Security Act of 1934, Section 508; 42 U.S.C. § 708
The Communications Act of 1934; 47 U.S.C. § 151 et seq.
Public Health Service Act of 1944; 42 U.S.C. Chapter 6A; Title VI, 42 U.S.C. §291 (known, in combination with Title XVI, as the Hill‐Burton Act); Title XVI, 42 U.S.C. § 300 (known, in combination with Title VI, as the Hill Burton Act);. Section 533, 42 U.S.C. §290; Section 542, 42 U.S.C. § 290dd‐1; Section 794, 42 U.S.C. § 295m,. Section 855, 42 U.S.C. § 296g,. Section 1908, 42 U.S.C. §300w‐7, Section 1947, 42 U.S.C. § 300x‐57
Title VI of the Civil Rights Act of 1964, 42 U.S.C. § 2000d et seq.
Treatment and Rehabilitation Act of 1970, Section 321, 91 P.L. 616 Part C, §321
Comprehensive Health Manpower Training Act of 1971, 92 P.L. 157 Title I Subpart III, Part H §110
Nurse Training Act of 1971, 92 P.L. 158
Drug Abuse Prevention, Treatment and Rehabilitation Act of 1972, 21 U.S.C. 1101
Title IX of the Education Amendments of 1972, 20 U.S.C. § 1681 et seq.
Rehabilitation Act of 1973, 29 U.S.C. § 701 et seq., Section 504 and Section 508–Amendments of 1973
The Church Amendments, 42 U.S.C. § 300a‐7
Comprehensive Alcohol Abuse and Alcoholism Prevention, Treatment, and Rehabilitation Act Amendments of 1974, 93 P.L. 282
National Research Service Award Act of 1974, 93 P.L. 348
The Age Discrimination Act of 1975, 42 U.S.C. § 6101 et seq.
Public Telecommunications Financing Act of 1978 Section 395, 95 P.L. 567, §201
The Low‐Income Home Energy Assistance Act of 1981, 42 U.S.C. § 8625
Omnibus Budget Reconciliation Act of 1981, P.L. 97‐35 [civil rights provisions pertaining to HHS Block Grants only]
The Community Services Block Grant Act of 1981, 42 U.S.C. §9918
Title II of the Americans with Disabilities Act of 1990, 42 U.S.C. §12131
Improving America’s Schools Act of 1994 Part E, 103 P.L. 382
Health Insurance Portability and Accountability Act of 1996
Coats‐Snowe Amendment of 1996, 42 U.S.C. § 238n
Small Business Job Protection Act of 1996, Section 1808(c), 104 P.L. 188
Patient Safety and Quality Improvement Act of 2005, 109 P.L. 41
Genetic Information Nondiscrimination Act of 2008, 110 P.L. 233
Health Information Technology for Economic and Clinical Health Act, American Recovery and Investment Act of 2009, 111 P.L. 5
Patient Protection and Affordable Care Act of 2010, Section 1303(b)(2)(A)(iii), Section 1553, Section 1557, 42 U.S.C. § 18116–
The Family Violence Prevention and Services Act of 2010, formerly part of the Child Abuse Amendments of 1984; 42 U.S.C. §10401 et seq.
Consolidated Appropriations Act of 2016, Div. H, Section 507, 114 P.L. 113

Office for Civil Rights
Page 17
Appropriations History
Details Budget
Estimate to Congress
House Allowance
Senate Allowance
Appropriation
2010
Appropriation
Base 37,785,000 37,785,000 37,785,000 37,785,000
Rescission (PL 110‐161) ‐ ‐ ‐ (6,000)
Subtotal 37,785,000 37,785,000 37,785,000 37,779,000
Trust Funds
Base 3,314,000 3,314,000 3,314,000 3,314,000
Subtotal 3,314,000 3,314,000 3,314,000 3,314,000
2011
Appropriation
Base 44,382,000 44,382,000 44,382,000 37,785,000
Rescission (PL 111‐117) ‐ ‐ ‐ (76,000)
Subtotal 44,382,000 44,382,000 44,382,00 37,709,000
Trust Funds
Base 3,314,000 3,314,000 3,314,000 3,314,000
Rescission (PL 112‐10) ‐ ‐ ‐ (7,000)
Subtotal 3,314,000 3,314,000 3,314,000 3,307,000
2012
Appropriation
Base 44,382,000 41,016,000 41,016,000 41,016,000
Rescission (PL 112‐74) ‐ ‐ ‐ (78,000)
Subtotal 44,382,000 41,016,000 41,016,000 40,938,000
2013
Appropriation
Base 38,966,000 ‐ 38,966,000 40,938,000
Sequestration ‐ ‐ ‐ (2,059,000)
Rescission (PL 113‐6) ‐ ‐ ‐ (82,000)
Transfers (PL 112‐74) ‐ ‐ ‐ (182,000)
Subtotal 38,966,000 ‐ 38,966,000 38,615,000
2014
Appropriation
Base 42,205,000 ‐ 42,205,000 38,798,000
Subtotal 42,205,000 ‐ 42,205,000 38,798,000
2015
Appropriation
Base 41,205,000 ‐ 38,798,000 38,798,000
Subtotal 41,205,000 ‐ 38,798,000 38,798,000

Office for Civil Rights
Page 18
Appropriations History (Continued)
Details Budget
Estimate to Congress
House Allowance
Senate Allowance
Appropriation
2016
Appropriation
Base 42,705,000 ‐ 38,798,000 38,798,000
Subtotal 42,705,000 ‐ 38,798,000 38,798,000
2017
Appropriation
Base 42,705,000 38,798,000 38,798,000 38,798,000
Transfers ‐ ‐ ‐ (90,000)
Subtotal 42,705,000 38,798,000 38,798,000 38,708,000
2018
Appropriation
Base 32,530,000 38,798,000 ‐ ‐
Subtotal 32,530,000 38,798,000 ‐ ‐
2019
Appropriation
Base 30,904,000 ‐ ‐ ‐
Subtotal 30,904,000 ‐ ‐ ‐

Office for Civil Rights
Page 19
Summary of the Request (Dollars in thousands)
Division FY 2018
Annualized CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
Civil Rights Division 4,565 4,253 ‐312
Health Information Privacy Division
Total Program Level Including Civil Monetary Settlement Funds
7,047 5,764 ‐1,283
Conscience and Religious Freedom Division 602 2,148 +1,546
Operations and Resources Division
Total Program Level Including Civil Monetary Settlement Funds
36,848 32,216 ‐4,632
The U.S. Department of Health and Human Services (HHS) Office for Civil Rights (OCR) is the primary defender of the public’s right to privacy and security of protected health information and non‐discriminatory access to Federally funded health and human services. Through prevention and elimination of unlawful discrimination on the basis of race, color, national origin, disability, age, sex, and religion, and through protection of conscience and of the privacy and security of individually identifiable health information, OCR helps HHS carry out its overall mission of improving the health and well‐being of all people affected by the Department’s many programs.
OCR transitioned to a new organizational structure published in the Federal Register on December 28, 2016. Programs and Policy was eliminated as a consolidated entity to remove an unnecessary layer of senior management to allow the existing two Divisions to report to the Director of OCR. Additionally, a new Division was created that consolidated both the prior Enforcement and Regional Operations and Planning and Business Administration Management entities. This new Operations and Resources Division, or ORD, encompasses all operations conducted in OCR’s eight regional offices as well as the resource service functions designed to support the organization as a whole.
During FY 2018, OCR added a Conscience and Religious Freedom Division. This Division complements OCR’s other two existing programmatic Divisions – the Civil Rights Division and the Health Information Privacy Division – to ensure that OCR focuses equal and appropriate attention on this important priority of conscience and religious liberty, without diminishing OCR’s efforts to further its important mission areas of overall civil rights issues and the privacy and security of protected health information. Together, these three Divisions ensure that OCR and the Department at large are contributing to the Department’s overall mission and the Administration’s priorities in each of these areas. OCR’s budget request consists of four narratives, one for each of its Divisions.
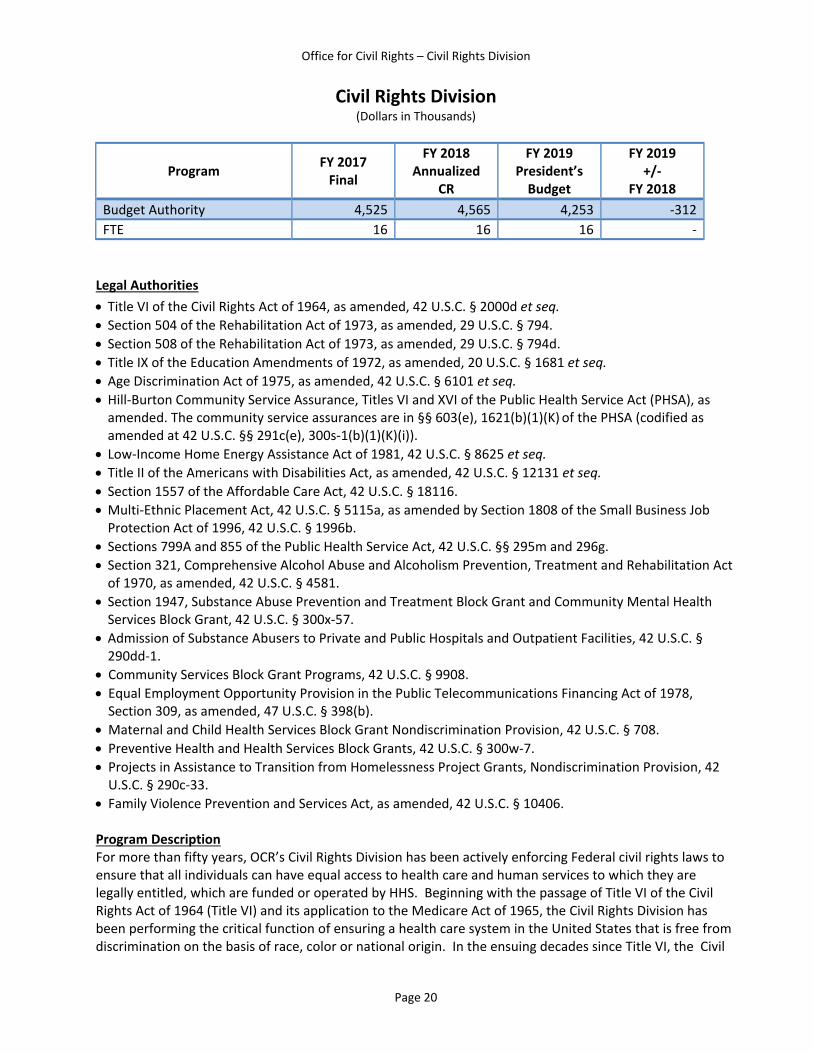
Office for Civil Rights – Civil Rights Division
Page 20
Civil Rights Division (Dollars in Thousands)
Program FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
Budget Authority 4,525 4,565 4,253 ‐312
FTE 16 16 16 ‐
Legal Authorities
Title VI of the Civil Rights Act of 1964, as amended, 42 U.S.C. § 2000d et seq.
Section 504 of the Rehabilitation Act of 1973, as amended, 29 U.S.C. § 794.
Section 508 of the Rehabilitation Act of 1973, as amended, 29 U.S.C. § 794d.
Title IX of the Education Amendments of 1972, as amended, 20 U.S.C. § 1681 et seq.
Age Discrimination Act of 1975, as amended, 42 U.S.C. § 6101 et seq.
Hill‐Burton Community Service Assurance, Titles VI and XVI of the Public Health Service Act (PHSA), as amended. The community service assurances are in §§ 603(e), 1621(b)(1)(K) of the PHSA (codified as amended at 42 U.S.C. §§ 291c(e), 300s‐1(b)(1)(K)(i)).
Low‐Income Home Energy Assistance Act of 1981, 42 U.S.C. § 8625 et seq.
Title II of the Americans with Disabilities Act, as amended, 42 U.S.C. § 12131 et seq.
Section 1557 of the Affordable Care Act, 42 U.S.C. § 18116. Multi‐Ethnic Placement Act, 42 U.S.C. § 5115a, as amended by Section 1808 of the Small Business Job Protection Act of 1996, 42 U.S.C. § 1996b.
Sections 799A and 855 of the Public Health Service Act, 42 U.S.C. §§ 295m and 296g.
Section 321, Comprehensive Alcohol Abuse and Alcoholism Prevention, Treatment and Rehabilitation Act of 1970, as amended, 42 U.S.C. § 4581.
Section 1947, Substance Abuse Prevention and Treatment Block Grant and Community Mental Health Services Block Grant, 42 U.S.C. § 300x‐57.
Admission of Substance Abusers to Private and Public Hospitals and Outpatient Facilities, 42 U.S.C. § 290dd‐1.
Community Services Block Grant Programs, 42 U.S.C. § 9908.
Equal Employment Opportunity Provision in the Public Telecommunications Financing Act of 1978, Section 309, as amended, 47 U.S.C. § 398(b).
Maternal and Child Health Services Block Grant Nondiscrimination Provision, 42 U.S.C. § 708.
Preventive Health and Health Services Block Grants, 42 U.S.C. § 300w‐7. Projects in Assistance to Transition from Homelessness Project Grants, Nondiscrimination Provision, 42 U.S.C. § 290c‐33.
Family Violence Prevention and Services Act, as amended, 42 U.S.C. § 10406. Program Description For more than fifty years, OCR’s Civil Rights Division has been actively enforcing Federal civil rights laws to ensure that all individuals can have equal access to health care and human services to which they are legally entitled, which are funded or operated by HHS. Beginning with the passage of Title VI of the Civil Rights Act of 1964 (Title VI) and its application to the Medicare Act of 1965, the Civil Rights Division has been performing the critical function of ensuring a health care system in the United States that is free from discrimination on the basis of race, color or national origin. In the ensuing decades since Title VI, the Civil

Office for Civil Rights – Civil Rights Division
Page 21
Rights Division has taken on responsibility for an increasing number of civil rights protections by enforcing non‐discrimination laws based on protected categories, including: disability (Section 504 of the Rehabilitation Act of 1973 (Section 504) and Title II of the Americans with Disabilities Act of 1990 (ADA)); age (the Age Discrimination Act of 1975); and race, color, national origin, disability, age, and sex in certain educational and health programs and activities (Title IX of the Education Amendments of 1972 and Section 1557 of the Affordable Care Act). The Civil Rights Division improves compliance with our Nation’s civil rights laws through: (1) regulations and sub‐regulatory guidance and other technical assistance material to assist covered
entities with civil rights compliance and inform stakeholders of their civil rights; (2) national outreach initiatives for covered entities and stakeholders to address civil rights compliance
concerns in health and human services; (3) leadership in the Department in civil rights matters on Departmental priorities and coordination with
other Federal agencies to ensure the HHS civil rights perspective is considered; (4) guidance to and partnership with OCR’s regional offices to ensure consistency in civil rights
enforcement efforts; and (5) reform of regulations and sub‐regulatory guidance issued by OCR and by other HHS components for
which the civil rights benefits are outweighed by the burden imposed. Particular areas of recent and ongoing emphasis include: Protecting the Rights of Children, Parents and Prospective Parents in the Child Welfare System As part of its enforcement, policy, and outreach work, the Civil Rights Division has entered into a partnership with the Department of Justice (DOJ) and the HHS Administration on Children and Families (ACF) to safeguard the civil rights of parents, prospective parents and children in the child welfare system. To formalize this Child Welfare Initiative, OCR entered into a Memorandum of Understanding with DOJ in January 2017. As the Federal government lead in this area, the Civil Rights Division coordinates Federal agency compliance, policy, and outreach efforts. As part of this cross‐agency collaboration, OCR, DOJ and ACF have conducted joint investigations and compliance reviews. In addition, OCR, DOJ, and ACF have conducted joint outreach at several conferences, including the National Council of Juvenile and Family Court Annual Training Conference (July 2017), American Bar Association Conference on Children and the Law and Parents Attorney Conference (April 2017) and American Association of Health and Human Services Attorneys National Training Conference (November 2016). Ensuring Language Access Services in Healthcare and Human Service Settings With external entities and other HHS agencies, the Civil Rights Division works to ensure that health care and human service providers receiving Federal funds take reasonable steps to ensure meaningful access by limited English proficient (LEP) individuals to programs or services. For example, since 2012, the OCR Director has chaired the HHS Language Access Steering Committee, which oversees and coordinates ongoing Departmental efforts to improve access for LEP individuals to programs conducted by HHS. In 2016, the Steering Committee successfully launched training on the HHS Language Access Plan for HHS employees through the HHS Learning Portal.

Office for Civil Rights – Civil Rights Division
Page 22
Promoting Effective Communication in Hospitals and Healthcare Settings Effective communication is critical in health care settings where miscommunication may lead to misdiagnosis and improper or delayed medical treatment. As part of its enforcement program, OCR works to ensure that hospitals and other health care organizations provide effective communications to patients who are deaf or hard of hearing, as well as their family members and friends. The Civil Rights Division provides national leadership to ensure consistency in enforcement and outreach efforts both in headquarters and the regions. Providing Civil Rights Training to Aspiring Doctors and Dentists To maximize civil rights compliance, OCR recognizes the importance of leveraging relationships with health care providers, associations, colleges and universities, industry stakeholders and state and local agencies. In 2016 and continuing into 2017, the Civil Rights Division reinvigorated a long standing relationship with the Association of American Medical Colleges (AAMC), whose members comprise all 147 accredited U.S. medical schools and nearly 400 major teaching hospitals and health systems. In a partnership with AAMC’s program for aspiring dental and medical school students, OCR’s headquarters and regional staff taught a civil rights compliance curriculum to several thousand students to help them understand how the equal treatment of patients, including LEP patients, is required by law and necessary to ensure safe and effective health care. OCR and AAMC presented the civil rights compliance curriculum at Columbia University, Howard University, Louisiana State University, Rutgers University, Western University, University of Alabama, University of California Los Angeles, University of Florida, University of Iowa, University of Louisville, University of Nebraska, University of Texas and University of Washington. Protecting Civil Rights during National Emergencies and Natural Disasters The Civil Rights Division serves as the OCR representative on various workgroups within HHS and external Federal agencies on planning for national emergencies and natural disasters to develop guidance and toolkits to ensure the inclusion of persons with disabilities and LEP individuals in these efforts. Accomplishments In the wake of the unprecedented 2017 hurricane season, the Civil Rights Division issued guidance to assist first‐responders in identifying practices and resources to provide equal access to emergency services for persons with disabilities and LEP individuals. These practices included: employing interpreters to assist LEP individuals and persons who have disabilities during response and recovery activities; making emergency messaging available in languages prevalent in the area and in multiple formats, such as audio, large print, captioning and accessible websites; and considering the needs of individuals with mobility impairments or durable medical equipment in providing transportation for evacuation. The Civil Rights Division continued to provide applicable guidance throughout the response phases of the multiple hurricanes during the Fall of 2017, including serving on a special disabilities task force convened by the Assistant Secretary for Preparedness and Response. In 2016 and 2017, the Civil Rights Division partnered with the Operations and Resources Division to re‐launch an Early Case Resolution (ECR) pilot to more efficiently achieve corrective action complaint closures early in the complaint process to ensure speedy and effective impact. The Civil Rights Division worked with OCR’s regions and successfully implemented the ECR pilot in all OCR regions. This enforcement tool has resulted in time and cost efficiencies across the regional offices and positive relationships between complainants and providers. Many providers have been quick to take corrective action and address

Office for Civil Rights – Civil Rights Division
Page 23
complainants’ concerns. In addition, ECR has proven to be a critical component in OCR’s efforts to address the significant increase in civil rights complaints that occurred in 2016 and 2017. In December 2016, OCR issued new guidance to assist providers of health care and health coverage to ensure that services that they offer through technology are accessible to all individuals, including individuals with disabilities. The use of electronic and information technology in the health care sector continues to grow exponentially as more providers integrate computerized systems to streamline operations and communicate with consumers. OCR’s guidance provides clarity on the application of Federal civil rights laws to electronic health record systems, websites and the more than 10,000 check‐in and diagnostic kiosks now in use by providers of health care and health coverage. In October 2016, OCR, DOJ and ACF issued a joint technical assistance letter to child welfare agencies and state court systems on preventing and addressing discrimination on the basis of race, color or national origin against children, parents or prospective parents. Previously, in August 2015, the three agencies issued a similar technical assistance document on preventing and addressing disability discrimination. In August 2016, HHS, DOJ and the Departments of Housing and Urban Development (HUD), Homeland Security and Transportation issued joint guidance to ensure that recipients of Federal financial assistance do not discriminate against individuals and communities on the basis of race, color or national origin, when providing emergency preparedness, response and recovery services. The joint guidance recommended, among other things, that recipients share information about housing, health services or other emergency‐related services to diverse racial, ethnic and LEP populations; engage with, and seek input from, diverse populations during planning; and widely disseminate evacuation and disaster preparedness plans, including translated documents for LEP populations. Similarly, in August 2016, HHS issued a joint letter with DOJ and HUD to remind recipients of Federal financial assistance that immigration status is not a bar to receiving services necessary to protect life or safety. Funding History
Fiscal Year Amount
FY 2014 $3,842,000
FY 2015 $3,950,000
FY 2016 $3,652,000
FY 2017 $4,525,000
FY 2018 Annualized CR $4,565,000
Budget Request The FY 2019 President’s Budget request for the Civil Rights Division of $4,253,000 is $312,000 below the FY 2018 Annualized CR level of $4,565,000. The decrease reflects the reduction of pay and non‐pay costs and transfer of attorney services to support the newly established division as it takes over responsibility for conscience and religious freedom enforcement.

Office for Civil Rights – Health Information Privacy Division
Page 24
Health Information Privacy (HIP) Division (Dollars in Thousands)
Program FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
Discretionary Budget Authority 4,156 4,802 1,519 ‐3,283
Civil Monetary Settlement Funds 1,745 2,245 4,245 +2,000
HIP Program Level 5,901 7,047 5,764 ‐1,283
FTE 15 18 8 ‐10*1
Legal Authorities
Administrative Simplification Provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA), section 264, Public Law 104‐191, 42 U.S.C. §1320d‐2 (note).
Social Security Act, section 1173(d), as added by HIPAA §262(a), 42 U.S.C. §1320d‐2(d). Confidentiality provisions of the Patient Safety and Quality Improvement Act of 2005 (PSQIA), Public Law 109‐41, 42 U.S.C. §299b‐21 – 299b‐26.
Title I of the Genetic Information Nondiscrimination Act of 2008 (GINA), Public Law 110‐233, section 105, 42 U.S.C. §1320d‐9.
Health Information Technology for Economic and Clinical Health Act (HITECH), American Recovery and Investment Act of 2009, 111 P.L. 5, sections 13400‐ 13423, 42 USC §§17921‐17953.
21st Century Cures Act of 2016, Public Law 114‐225, Section 4006(b).
Program Description The collection and sharing of health information is critical to improving the quality and safety of health care and advancing medical discoveries that can improve the health and wellbeing of individuals and populations. However, in the face of increasing cybersecurity threats targeting the health care sector and public concerns about the privacy and security of health data, active stewardship and enforcement of privacy and security regulations are critical to building and maintaining public trust in robust uses of health information. HIP works to ensure the protection of identifiable health information from unauthorized disclosure, the security of electronic identifiable health information, and to enforce the right of individual patients to access their health information pursuant to the following key legal authorities: the Health Insurance Portability and Accountability Act (HIPAA) of 1996; the Genetic Information Nondiscrimination Act of 2008 (GINA); the Patient Safety and Quality Improvement Act (PSQIA) of 2005, Section 1301; Subtitle D, of the HITECH Act (American Recovery and Reinvestment Act) of 2009; and Section 4006(b) of the 21st Century Cures Act. Through its innovative efforts to promote and enforce HIPAA privacy and security protections, HIP plays a leading role in supporting both public and private sector efforts to improve health care quality and reduce costs, including advancing interoperability of digital health information; empowering individuals to make health care decisions; building public trust in health data sharing pursuant to the newest statute in this area, the 21st Century Cures Act; helping to build the privacy and security framework for public and private sector research initiatives that yield medical discoveries; supporting public health surveillance and emergency preparedness and response activities; improving the ability of entities subject to HIPAA to prevent and effectively respond to
1 OCR will offset the FTE reduction with the use of HIPAA settlement funds as allowed by law.

Office for Civil Rights – Health Information Privacy Division
Page 25
cybersecurity threats; and improving the safety of health care by helping to facilitate confidential analysis of medical errors and other patient safety events. HIP improves compliance with the HIPAA privacy, security and breach notification regulations through: (1) robust policy guidance on a variety of topics and outreach to the public and industry
stakeholders, in order to enhance compliance by actively addressing common questions about the HIPAA regulations, including how the rules apply to novel circumstances and new technologies;
(2) periodic audits, as required by law, to proactively identify and address vulnerabilities before they result in breaches, unauthorized disclosures, or other HIPAA violations;
(3) Departmental leadership on cross‐cutting issues involving HIPAA privacy and security; (4) partnering with OCR’s regional offices to exercise OCR’s enforcement and civil monetary
penalty authority to both hold entities financially accountable for systemic compliance failures and to obtain corrective action; and
(5) reform of regulatory provisions for which the benefit to privacy and security is outweighed by the burden imposed.
Policy The HIPAA Privacy and Security Rules were initially written and implemented more than a decade ago, and much has changed in health care, including how health information is accessed, used, and disclosed. Recognizing that well‐intended regulations can lose their efficacy with the passage of time and that regulatory complexity can contribute to noncompliance, OCR is undertaking review of its HIPAA regulations and significant sub‐regulatory guidance to identify and modify, or eliminate, regulatory provisions and interpretations that are no longer effective or increase complexity for the regulated community without a corresponding benefit to privacy or security protections, or to individual empowerment. At the same time, OCR is actively working to implement provisions of HITECH and the 21st Century Cures Acts that mandate new regulations or the issuance of further guidance. OCR will seek input from the public as it undertakes this review, both informally as well as through applicable Administrative Procedure Act notice and comment processes. Audit Program As part of its enforcement portfolio, OCR examines the HIPAA compliance of randomly selected entities through OCR’s audit program, to help promote compliance with the HIPAA regulations. HIP’s audit program, required under the HITECH Act, leverages a proactive and systemic look at industry compliance successes and struggles. Following on the comprehensive evaluation conducted in the first pilot phase of OCR’s audit program, Phase 2 (conducted in 2016 and 2017) focused on desk audits of over 200 covered entities and business associates who submitted documentation of their efforts to comply with selected provisions of the HIPAA regulations. In 2018 and beyond, OCR will use its audit authority to conduct more regular, annual desk and onsite audits of entities covered by HIPAA. Although only a portion of covered entities and business associates are audited in a given year, the prospect of being subject to an audit helps foster a culture of compliance as entities self‐evaluate their compliance activities in anticipation of a potential audit. Audits and other enforcement tools help raise the bar for privacy and security protections for health information – but OCR’s audits and its enforcement authority can only extend so far. To more quickly achieve greater industry‐wide compliance, particularly among smaller health care providers and particularly with respect to improving cybersecurity, OCR is exploring how to leverage the work of private sector entities with experience in helping industry stakeholders achieve compliance with

Office for Civil Rights – Health Information Privacy Division
Page 26
the HIPAA regulations and recognized cybersecurity frameworks. OCR is also working with the HHS Office of the National Coordinator for Health IT (ONC) to help providers better evaluate the security functionalities of their certified electronic health record technology and encourage those providers to more consistently deploy those functionalities, which helps bolster their compliance with the HIPAA Security Rule. Accomplishments In December 2017, OCR launched an array of new tools and initiatives in response to the opioid crisis, while implementing the 21st Century Cures Act (Public Law 114‐255). These tools and initiatives fulfill requirements of the 21st Century Cures Act to ensure that the healthcare sector, researchers, patients, and their families understand how the Health Insurance Portability and Accountability Act (HIPAA) protects privacy and helps improve health and healthcare nationwide. Highlights of these actions include new HIPAA webpages focused on information related to mental and behavioral health; new HIPAA guidance on sharing information related to mental health and substance use disorder treatment with a patient's family, friends and others involved in the patient's care or payment for that care; new collaboration with partner agencies within HHS to identify and develop model programs and materials for training healthcare providers, patients, and their families regarding permitted uses and disclosures of the protected health information of patients seeking or undergoing mental health or substance use disorder treatment, and to develop a plan to share the programs and materials with professionals and consumers; updated guidance on HIPAA and research, as called for in the Cures Act; and launch of a working group to study and report on the uses and disclosures under HIPAA of protected health information for research purposes. The working group will include representatives from relevant federal agencies as well as researchers, patients, healthcare providers, and experts in healthcare privacy, security, and technology. The working group will release a report addressing whether uses and disclosures of PHI for research purposes should be modified to facilitate research while protecting individuals’ privacy rights. In October 2017, OCR released new guidance regarding when and how healthcare providers can share a patient’s health information with his or her family members, friends, and legal personal representatives when that patient may be in crisis and incapacitated, such as during an opioid overdose. Current HIPAA regulations allow healthcare providers to share information with a patient’s loved ones in certain emergency or dangerous situations. This includes informing persons in a position to prevent or lessen a serious and imminent threat to a patient’s health or safety. Misunderstandings about HIPAA can create obstacles to family support that is crucial to the proper care and treatment of people experiencing a crisis situation, such as an opioid overdose. It is critical for healthcare providers to understand when and how they can share information with patients’ family members and friends without violating the HIPAA Privacy Rule. By end of 2017, OCR will have audited 166 covered entities and 41 business associates pursuant to phase 2 of the HITECH audit program. The phase 2 audits focused on the HIPAA Security Rule risk analysis and risk management provisions, the HIPAA Breach Notification Rule requirements to notify individuals and HHS of breaches of health information, and the HIPAA Privacy Rule requirements to provide individuals with a Notice of Privacy Practices and to provide individuals with access to their health information. Individual reports were sent to each audited entity; OCR also will issue an overarching report to the public, identifying best practices as well as patterns of noncompliance that should be the focus of more targeted guidance and outreach (anticipated end of 2017/beginning 2018).

Office for Civil Rights – Health Information Privacy Division
Page 27
On July 25, 2017, OCR launched a revised web tool that puts important information about breaches of health information into the hands of individuals, empowering them to better identify recent breaches and to learn how they are investigated and resolved. The revised HIPAA Breach Reporting Tool provides transparency to the public and organizations covered by HIPAA, and helps highlight the importance of safeguards to protect the privacy and security of sensitive health care information. It features improved navigation, highlights the most recent breaches, and helps educate industry and the public on the types of breaches that are occurring and how breaches are commonly resolved. Since 2009, OCR has maintained the HIPAA Breach Reporting Tool (HBRT) consistent with its HITECH obligations. The HIPAA Privacy Rule requires covered entities, such as health care providers and health plans, to provide individuals with access to, and copies of, their health information, including the ability to download that information into mobile health care tools or “apps,” or to send their health information to a researcher or other entity. OCR has issued extensive guidance on this right, and has conducted extensive outreach to the public and regulated community, to help improve understanding of these provisions. In July 2017, OCR released a 30‐minute Medscape module that provides clear information on the HIPAA right of individual access; health care professionals viewing the module receive continuing medical or health professional education credit. In summer 2017, HHS also issued a poster and brochure, following on its successful “Information is Powerful Medicine” campaign launched in 2013, to help individuals better understand their HIPAA rights. These tools add to the wealth of material available from OCR on the HIPAA right of access, including consumer‐friendly videos in English and Spanish, developed on conjunction with ONC.
OCR has released a number of resources intended to help the health care industry effectively respond to cybersecurity threats. In 2017, OCR issued a checklist (and corresponding infographic) that clearly and concisely set forth the steps for a HIPAA covered entity or its business associate to take in response to a cyber‐related security incident. Since February 2016, HIP also has released monthly newsletters on timely cybersecurity topics. All of OCR’s resources on cybersecurity can be found on a dedicated page of its website. Funding History
Fiscal Year Amount
FY 2014 $3,841,000
FY 2015 $3,949,000
FY 2016 $3,651,000
FY 2017 $4,156,000
FY 2018 Annualized CR $4,802,000
Budget Request The FY 2019 President’s Budget requests $1,519,000 discretionary budget authority for the Health Information Privacy Division, $3,283,000 below the FY 2018 Annualized CR level of $4,802,000. In FY 2019 OCR will utilize $4,245,000 of monetary settlement funding collected from HIPAA enforcement activities to offset a portion of the decrease in appropriated funding; a program level of $5,764,000. The decrease reflects the reduction of pay, non‐pay, and contractual services costs.

Office for Civil Rights – Conscience and Religious Freedom Division
Page 28
Conscience and Religious Freedom Division (Dollars in Thousands)
Program FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
Budget Authority ‐ 602 2,148 +1,546
FTE ‐ 1 6 +5
Legal Authorities
Federal Conscience Rights Statutes, which include o Church Amendments, 42 U.S.C. § 300a‐7. o Coats‐Snowe Amendment, 42 U.S.C. §238n. o Weldon Amendment to the Annual Labor HHS Appropriations Act, e.g., Consolidated
Appropriations Act, 2017, Public Law 115‐31, Division H, §507(d).
Section 1553 of the Affordable Care Act, 42 U.S.C. § 18113. Equal Employment Opportunity Provision in the Public Telecommunications Financing Act of 1978, Section 309, as amended, 47 U.S.C. § 398(b).
Maternal and Child Health Services Block Grant Nondiscrimination Provision, 42 U.S.C. § 708.
Preventive Health and Health Services Block Grants, 42 U.S.C. § 300w‐7. Projects in Assistance to Transition from Homelessness Project Grants, Nondiscrimination Provision, 42 U.S.C. §290c‐33.
Family Violence Prevention and Services Act, as amended, 42 U.S.C. §10406.
Religious Freedom Restoration Act, 42 U.S.C. § 2000bb et seq. Program Description Protecting conscience and religious freedom and preventing coercion are foundational American values. In FY 2017 and continuing into FY 2018, OCR took active steps to support the Administration’s priority to “vigorously enforce Federal law’s robust protections for religious freedom,” as President Trump announced on May 4, 2017, in his Presidential Executive Order, Promoting Free Speech and Religious Liberty. To this end, OCR hired contractors in order to place a renewed emphasis on conscience and religious freedom and, in FY 2018, OCR created a component in its Headquarters’ operations, the Conscience and Religious Freedom Division, to ensure protection of conscience and religious freedom rights of individuals and entities in health care and human services. The new Division is actively engaged in outreach, enforcement, and policy making and has prepared and is taking comment on a proposed regulation entitled “Protecting Statutory Conscience Rights in Health Care.” In FY 2019 OCR looks forward to advancing and potentially finalizing this critical regulation. Through the Conscience and Religious Freedom Division, OCR provides a centralized point within HHS to coordinate, oversee, and ensure adequate compliance with Federal laws protecting conscience and religious liberty. OCR’s outreach mission compliments the separate work of the Center for Faith Based and Neighborhood Partnerships, through technical assistance, policy guidance, regulatory reform, and training both within HHS as well as with grantees, service providers, and the public on these important requirements of Federal law.
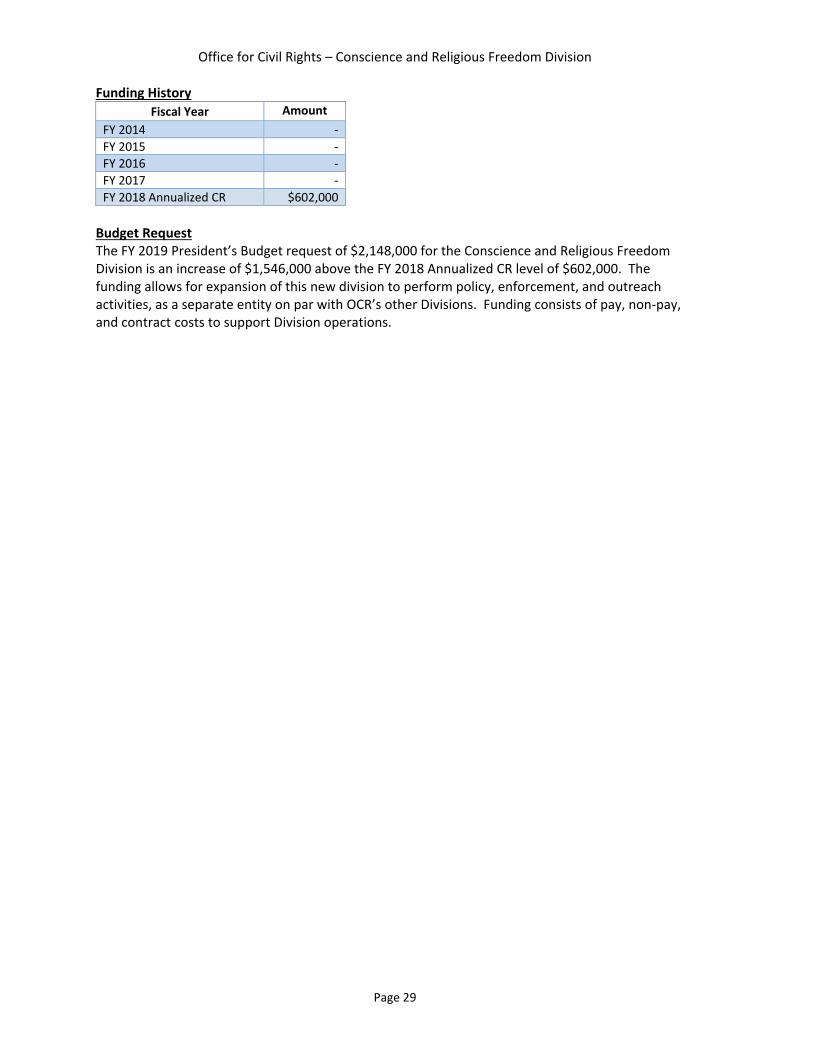
Office for Civil Rights – Conscience and Religious Freedom Division
Page 29
Funding History
Fiscal Year Amount
FY 2014 ‐
FY 2015 ‐
FY 2016 ‐
FY 2017 ‐
FY 2018 Annualized CR $602,000
Budget Request The FY 2019 President’s Budget request of $2,148,000 for the Conscience and Religious Freedom Division is an increase of $1,546,000 above the FY 2018 Annualized CR level of $602,000. The funding allows for expansion of this new division to perform policy, enforcement, and outreach activities, as a separate entity on par with OCR’s other Divisions. Funding consists of pay, non‐pay, and contract costs to support Division operations.

Office for Civil Rights
Page 30
Operations and Resources Division (Dollars in Thousands)
Program FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
FY 2019 +/‐
FY 2018
Discretionary Budget Authority 30,027 28,566 22,984 ‐5,582
Civil Monetary Settlement Funds 6,382 8,282 9,232 +950
ORD Program Level 36,409 36,848 32,216 ‐4,632
FTE 119 118 118 ‐
Legal Authorities
The Operations and Resources Division (ORD) acts as the enforcement arm for OCR. In that capacity, ORD enforces all legal authorities listed under the other OCR Divisions. Please refer to Civil Rights legal authorities on page 20, Health Information Privacy legal authorities on page 24, and Conscience and Religious Freedom legal authorities on page 28. Program Description ORD consists of the eight regional offices,2 the Centralized Case Management Operations (CCMO), and headquarters support personnel. The regions and CCMO are primarily responsible for enforcement of OCR’s legal authorities and meet their responsibility through the receipt, investigation, and enforcement of complaints as well as breach reports, compliance reviews, technical assistance, and local outreach activities. Operations: The Enforcement Lifecycle of Complaints and Compliance Reviews Complaint Processing The enforcement lifecycle begins with the Centralized Case Management Operations (CCMO), which receives complaints alleging the violation of one or more of OCR’s legal authorities by a covered entity. Members of the public can file complaints through OCR’s online complaint portal, mail, fax, or email. Complaints are assessed to determine which can be closed without formal investigation (e.g., as non‐jurisdictional, or with the provision of minor technical assistance), and which complaints should be transferred to an OCR regional office for further deliberation and possible investigation. As a result of recent efficiencies and innovations, the CCMO now makes decisions on administrative closures, technical assistance closures, and regional referrals within 15 days of receipt. Significant process redesign and automation improvements have enabled OCR to increase efficiency despite receipt of double the amount of complaints (24,523 in FY 2016 as compared to 12,705 in FY 2012) since OCR’s online complaint portal went live in FY 2012. Investigation Complaint investigations, breach report investigations, and compliance reviews are conducted by OCR regional offices. Each regional office utilizes highly skilled investigators responsible for examining allegations of discrimination or health information privacy/security violations, and determining covered entity or business associate compliance with its legal responsibilities. Through
2 The regional offices include New England Region (Boston), Eastern and Caribbean Region (New York), Mid‐Atlantic Region (Philadelphia), Southeast Region (Atlanta), Midwest Region (Chicago and Kansas City), Southwest Region (Dallas), Rocky Mountain Region (Denver), and Pacific Region (San Francisco, Seattle, and Los Angeles).

Office for Civil Rights
Page 31
the understanding and application of OCR’s legal authorities and jurisdiction, the staff conducts comprehensive fact‐finding investigations to determine levels of compliance across all regulations for each covered entity involved in a case. Investigations can result in a finding of no violation, the provision of technical assistance to address specific problem areas, or, where there are indications of systemic noncompliance, more formal enforcement action, including the negotiation of formal settlement agreements. Enforcement When OCR determines there has been a violation of one or more of its legal authorities, OCR takes enforcement action. In these instances, the regional office works closely with OCR Headquarters and the Office of the General Counsel to review the facts of the investigation and produce a letter of findings. When OCR sends the letter of finding to an entity, OCR may offer to provide technical assistance to promote voluntary compliance, or engage in a settlement negotiation with a corrective action plan, and, on occasion, payment of amounts to resolve the investigation. In instances where entities are uncooperative, OCR can, depending on the statute at issue, seek rescission of HHS funding to the entity, pursue civil money penalties, or refer the case to the Department of Justice for litigation. In addition to complaints submitted by the public, OCR is authorized to open compliance reviews of specific entities when it has reason to believe that an entity may have violated one of the laws that OCR enforces. OCR learns of such potential violations from a variety of sources, including media reports and situations in which significant numbers of individual complaints have been filed against an entity. Also, as required by HIPAA, OCR initiates an investigation in all cases where an entity has reported a health information privacy breach affecting 500 or more individuals. These compliance reviews and breach report investigations can enable OCR to evaluate compliance issues even before violations result and focus on systemic reform. The investigation and enforcement process for compliance reviews and breach report investigations, along with their outcome, follow the same processes noted above for complaint resolution. Technical Assistance In addition to OCR’s work to ensure compliance through enforcement, OCR promotes voluntary compliance through technical assistance and outreach. OCR delivers impact through strong technical assistance to covered entities. This collaboration across OCR teams ensures that covered entities can receive the information, guidance, and support required to achieve voluntary compliance with their legal responsibilities under civil rights, religious liberty, and privacy/security laws. Outreach Another major component of OCR’s compliance portfolio includes outreach. A robust outreach program informs individuals, consumer groups, advocacy groups, and other stakeholders of civil rights, religious liberty, and health information privacy laws, and obtains input about challenges and potential violations on which OCR should focus. Outreach also serves to educate covered entities about their responsibilities under civil rights, religious liberty, and health information privacy laws, and provide guidance on means to ensure compliance. This is accomplished through participating in conferences and briefings as well as smaller meetings and listening sessions; hosting workshops, webinars, and trainings; disseminating materials in a variety of forums; training law and medical students and other stakeholders; and convening and participating in various working groups. OCR’s regional staffs also participate in inter‐agency and intra‐agency activities, and work collaboratively with federal partners. OCR’s nationwide outreach efforts serve to educate, and provide guidance to,

Office for Civil Rights
Page 32
federal agencies, covered entities, consumers, and other stakeholders. These efforts allow OCR to build relationships, create opportunities for dialogue, provide opportunities for input on OCR’s work, and ensure that OCR is able to anticipate future challenges. Resources and Services Support ORD’s resources staff supports all OCR operations by assisting all three Divisions, including the regional offices, by providing budget, information technology, human resources, acquisition, security, property management, travel, ethics, Freedom of Information Act (FOIA), continuity of operations (COOP), and other related administrative support. The Budget Team, Human Resources Team, Information Technology Team, and the Executive Secretariat provide critical support to all programmatic staff to allow them to focus their attention on mission requirements. Accomplishments In December 2017, OCR reached a settlement agreement with 21 Century Oncology, Inc. (21CO), for multiple potential HIP violations. 21CO reported to OCR that the protected health information for 2,213,597 individuals was illegally obtained by an unauthorized third party through 21CO’s network database. OCR’s subsequent investigation revealed that 21CO failed to conduct an accurate and thorough assessment of the potential risks and vulnerabilities to the confidentiality, integrity, and availability of the electronic protected health information; failed to implement security measures sufficient to reduce risks and vulnerabilities to a reasonable and appropriate level; failed to implement procedures to regularly review records of information system activity, such as audit logs, access reports, and security incident tracking reports; and disclosed protected health information to third party vendors without a written business associate agreement. On May 25, 2017, 21CO filed for Chapter 11 bankruptcy protection in the United States Bankruptcy Court for the Southern District of New York. OCR’s settlement with 21CO for $2.3 million was approved by the Bankruptcy Court, and 21CO agreed to a corrective action plan to address the identified potential violations. In November 2017, OCR and DOJ entered into a voluntary resolution agreement requiring the University of Vermont Medical Center (UVMMC) to take remedial actions, including providing notice of the availability of auxiliary aids and services, implementing grievance procedures and feedback protocols, providing training to UVMMC personnel, updating policies and procedures through continuous improvement, and agreeing to pay the complainants $20,500 in compensatory relief. In 2016, OCR initiated a compliance review stemming from two complaints alleging violations of Title III of the Americans with Disabilities Act (ADA) and its implementing regulation. The complainants alleged UVMMC discriminated against them by failing to provide appropriate auxiliary aids and services necessary for effective communication during medical treatment. Both complainants are deaf and use American Sign Language as their primary means of communication. UVMMC is a recipient of HHS federal financial assistance and required to provide appropriate auxiliary aids and services to persons with impaired sensory, manual, or speaking skills, so that individuals have an equal opportunity to benefit from the services received. In March 2017, OCR resolved a complaint against Advanced Dermatology and Cosmetic Surgery (ADCS), the largest dermatology practice in the United States with over 180 locations nationwide. The complaint was initiated by an individual, who alleged her daughter and husband, LEP individuals whose primary language is Spanish, were turned away by ADCS and told that they could only return when they brought their own interpreter. Due to the technical assistance that OCR provided, ADCS took a number of steps to ensure its compliance, including creating and posting a new non‐

Office for Civil Rights
Page 33
discrimination policy, contracting with an interpreter service, and implementing a new grievance procedure for individuals who believe they have been victims of discrimination. In February 2017, OCR announced a settlement agreement with Memorial Healthcare Systems (MHS) for multiple potential HIP violations. MHS reported to OCR that the protected health information of 115,143 individuals had been impermissibly accessed by its employees and impermissibly disclosed to affiliated physician office staff. Although MHS had workforce access policies and procedures in place, MHS failed to implement procedures with respect to reviewing, modifying and/or terminating users’ right of access, as required by the HIPAA Rules. Further, MHS failed to regularly review records of information system activity on applications that maintain electronic protected health information by workforce users and users at affiliated physician practices, despite having identified this risk on several risk analyses conducted by MHS from 2007 to 2012. MHS agreed to a settlement monetary payment of $5.5 million, OCR’s second highest HIPAA settlement, and a corrective action plan to address the identified potential violations.
In February 2017, OCR announced its second HIPAA civil monetary penalty. The penalty was imposed against Children’s Medical Center of Dallas (Children’s) based on its impermissible disclosure of unsecured electronic protected health information (ePHI) and non‐compliance over many years with multiple standards of the HIPAA Security Rule. Specifically, Children’s failed to implement risk management plans, contrary to prior external recommendations to do so, and failed to deploy encryption or an equivalent alternative measure on all of its laptops, work stations, mobile devices and removable storage media until April 9, 2013. Despite Children's knowledge about the risk of maintaining unencrypted ePHI on its devices as far back as 2007, Children's issued unencrypted BlackBerry devices to nurses and allowed its workforce members to continue using unencrypted laptops and other mobile devices until 2013. After unsuccessful settlement discussions, OCR issued a Notice of Proposed Determination in accordance with 45 CFR 160.420. OCR subsequently issued a Notice of Final Determination, and Children's paid the full civil money penalty of $3.2 million. In January 2017, OCR announced a voluntary resolution agreement with the University of Connecticut Health Center (UConn Health) to ensure effective communication with individuals that are deaf or hard of hearing. The Agreement resolved a complaint filed on behalf of an individual who is deaf, alleging that UConn Health failed to provide timely auxiliary aids and services to effectively communicate with the patient during a visit to the John Dempsey Hospital’s Emergency Department. According to the complaint, despite requesting services upon arrival, the complainant was not provided an interpreter or video remote interpreting services; and replied on a companion to interpret during the hospital visit. As a result of OCR’s investigation, UConn Health agreed to take multiple actions to ensure the availability of auxiliary aids and services.
OCR resolved two major child welfare matters in late 2016. In October 2016, OCR resolved a complaint against the Nebraska Department of Health and Human Services (NDHHS), which provides child protection services to over 465,000 children living in Nebraska. After completing an investigation, OCR found that NDHHS had failed to develop policies and procedures to provide speech‐language pathology services or otherwise ensure effective communication with children who have communication disorders. To resolve the complaint, NDHHS agreed to implement statewide, and across all NDHHS divisions: (1) a nondiscrimination policy, program accessibility policy, and grievance procedure; (2) an auxiliary aids and services policy; and (3) a training program, including mandatory in‐person or online modules.

Office for Civil Rights
Page 34
In December 2016, OCR also resolved two compliance reviews that examined allegations of discrimination in the foster care and adoption policies and practices of the Department of Human Services in Jefferson County, Colorado, which has a population of over 535,000; and the Department of Human Services in Arapahoe County, Colorado, which has a population of over 631,000. The compliance reviews were initiated to determine whether there were delays or denials of child placements on the basis of the race, color or national origin of the prospective parent or the child involved; and whether the policies and practices denied any individual the opportunity to be a foster or adoptive parent on the basis of the race, color or national origin of the individual, or of the child involved. To resolve the compliance reviews, OCR provided Jefferson County and Arapahoe County with substantial technical assistance, and each County agreed to implement an appropriate language assistance services program to ensure meaningful access to prospective foster and adoptive parents with LEP.
In October 2016, OCR provided technical assistance to over 100 health care providers and community representatives funded by the HHS Health Resources and Services Administration (HRSA) at the Primary Care Association Annual Conference in San Juan, Puerto Rico. OCR discussed the recent technical assistance letter developed by OCR and HRSA pertaining to effective communication to the deaf and hard of hearing in Puerto Rico, which was released in August 2016. Funding History
Fiscal Year Amount
FY 2014 $31,115,000
FY 2015 $30,899,000
FY 2016 $31,495,000
FY 2017 $30,027,000
FY 2018 Annualized CR $28,566,000
Budget Request The FY 2019 President’s Budget requests $22,984,000 discretionary budget authority for the Operations and Resources Division, $5,582,000 below the FY 2018 Annualized CR level of $28,566,000. In FY 2019 OCR will utilize $9,232,000 in monetary settlement funding collected from HIPAA enforcement activities to offset a portion of the decrease in appropriated funding; a program level of $32,216,000. The decrease reflects reductions in regional contract staff investigators, and other governmental and non‐governmental contractual services related to IT support, attorney services, and other shared services costs.
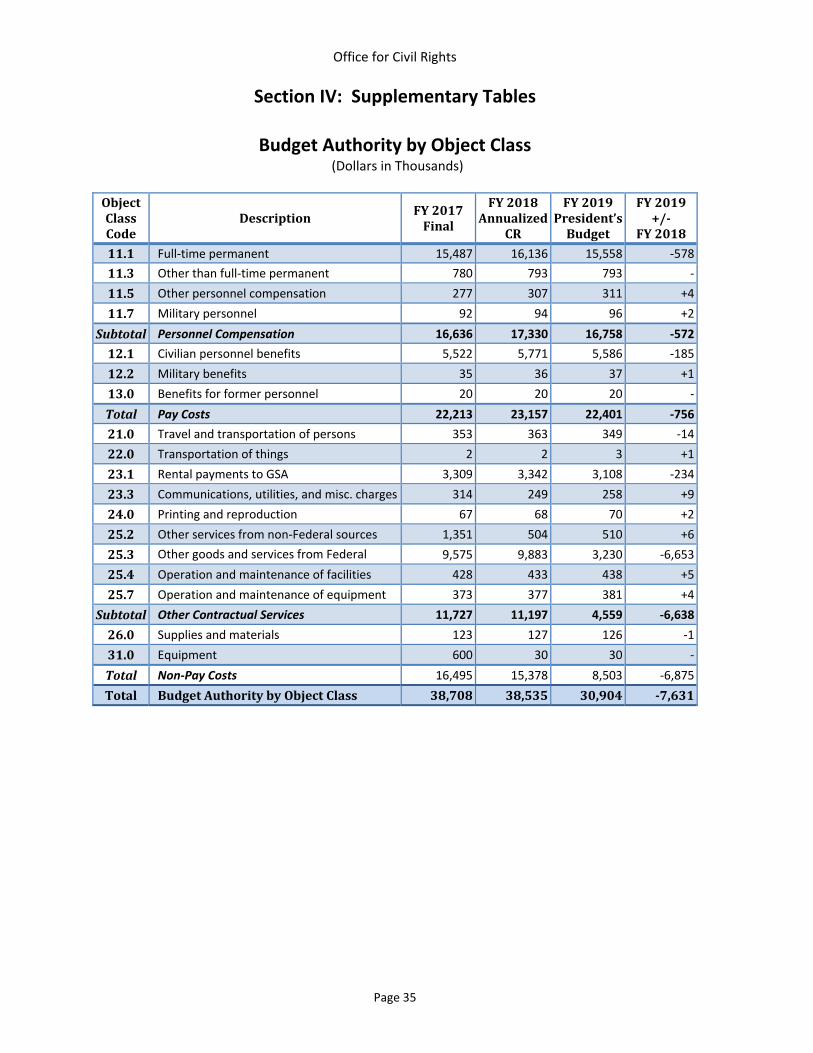
Office for Civil Rights
Page 35
Section IV: Supplementary Tables
Budget Authority by Object Class (Dollars in Thousands)
ObjectClassCode
DescriptionFY2017Final
FY2018Annualized
CR
FY2019President’sBudget
FY2019+/‐
FY2018
11.1 Full‐time permanent 15,487 16,136 15,558 ‐578
11.3 Other than full‐time permanent 780 793 793 ‐
11.5 Other personnel compensation 277 307 311 +4
11.7 Military personnel 92 94 96 +2
Subtotal Personnel Compensation 16,636 17,330 16,758 ‐572
12.1 Civilian personnel benefits 5,522 5,771 5,586 ‐185
12.2 Military benefits 35 36 37 +1
13.0 Benefits for former personnel 20 20 20 ‐
Total Pay Costs 22,213 23,157 22,401 ‐756
21.0 Travel and transportation of persons 353 363 349 ‐14
22.0 Transportation of things 2 2 3 +1
23.1 Rental payments to GSA 3,309 3,342 3,108 ‐234
23.3 Communications, utilities, and misc. charges 314 249 258 +9
24.0 Printing and reproduction 67 68 70 +2
25.2 Other services from non‐Federal sources 1,351 504 510 +6
25.3 Other goods and services from Federal 9,575 9,883 3,230 ‐6,653
25.4 Operation and maintenance of facilities 428 433 438 +5
25.7 Operation and maintenance of equipment 373 377 381 +4
Subtotal Other Contractual Services 11,727 11,197 4,559 ‐6,638
26.0 Supplies and materials 123 127 126 ‐1
31.0 Equipment 600 30 30 ‐
Total Non‐Pay Costs 16,495 15,378 8,503 ‐6,875
Total BudgetAuthoritybyObjectClass 38,708 38,535 30,904 ‐7,631

Office for Civil Rights
Page 36
Salaries and Expenses Table (Dollars in Thousands)
ObjectClassCode
Description FY2017Final
FY2018Annualized
CR
FY2019President’sBudget
FY2019+/‐
FY2018
11.1 Full‐time permanent 15,487 16,136 15,558 ‐578
11.3 Other than full‐time permanent 780 793 793 ‐
11.5 Other personnel compensation 277 307 311 +4
11.7 Military personnel 92 94 96 +2
Subtotal Personnel Compensation 16,636 17,330 16,758 ‐572
12.1 Civilian personnel benefits 5,522 5,771 5,586 ‐185
12.2 Military benefits 35 36 37 +1
13.0 Benefits for former personnel 20 20 20 ‐
Total Pay Costs 22,213 23,157 22,401 ‐756
21.0 Travel and transportation of persons 353 363 349 ‐14
22.0 Transportation of things 2 2 3 +1
23.3 Communications, utilities, and misc. charges 314 249 258 +9
24.0 Printing and reproduction 67 68 70 +2
25.2 Other services from non‐Federal sources 1,351 504 510 +2
25.3 Other goods and services from Federal 9,575 9,883 3,230 ‐6,649
25.4 Operation and maintenance of facilities 428 433 438 +5
25.7 Operation and maintenance of equipment 373 377 381 +4
Subtotal Other Contractual Services 11,727 11,197 4,559 ‐6,638
26.0 Supplies and materials 123 127 126 ‐1
Total Non‐Pay Costs 12,586 12,006 5,365 ‐6,641
Total Salary and Expenses 34,799 35,163 27,766 ‐7,397
23.1 Rental payments to GSA 3,309 3,342 3,108 ‐234
Total Salaries, Expenses, and Rent 38,108 38,505 30,874 ‐7,631
Total DirectFTE 150 153 148 ‐5

Office for Civil Rights
Page 37
Detail of Full‐Time Equivalents (FTE)
Detail FY 2017 Actual Civilian
FY 2017 Actual Military
FY 2017Actual Total
FY 2018EstimateCivilian
FY 2018EstimateMilitary
FY 2018EstimateTotal
FY 2019 Estimate Civilian
FY 2019EstimateMilitary
FY 2019EstimateTotal
Direct 149 1 150 152 1 153 147 1 148
Reimbursable 1 0 1 1 0 1 1 0 1
Total FTE 150 1 151 153 1 154 148 1 149
Average GS Grade FY 2015: GS 12 FY 2016: GS 12 FY 2017: GS 13 FY 2018: GS 13 FY 2019: GS 13
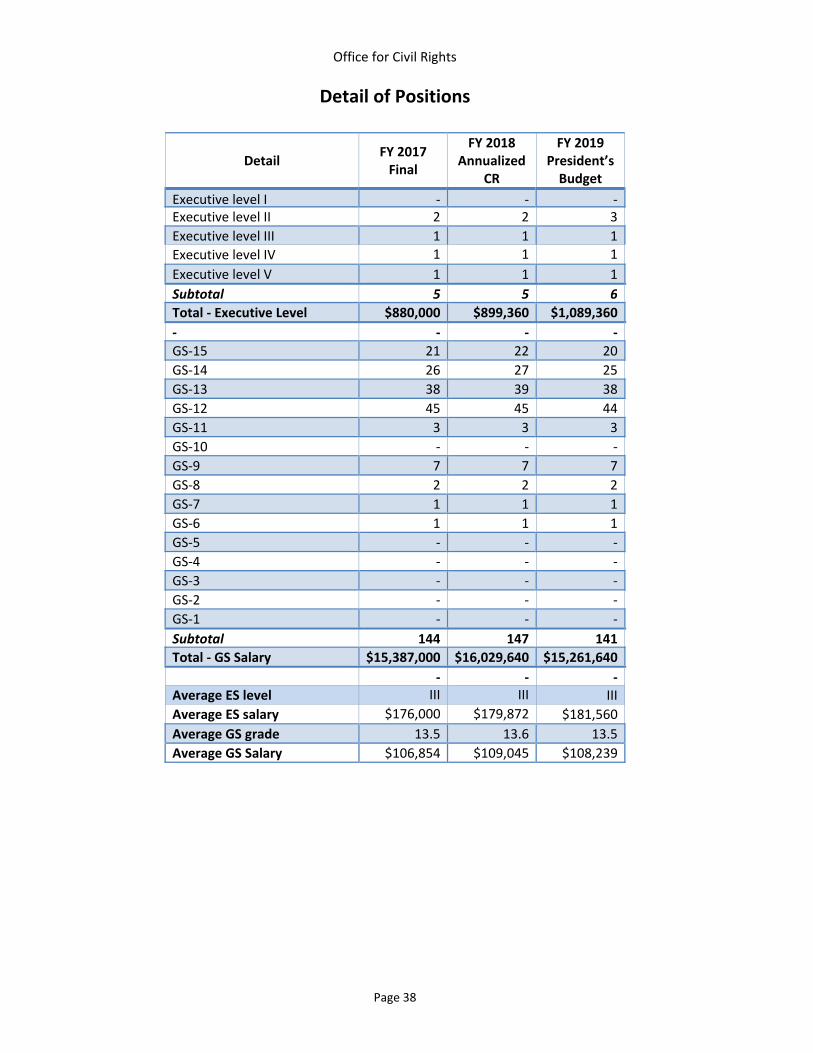
Office for Civil Rights
Page 38
Detail of Positions
Detail FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President’s Budget
Executive level I ‐ ‐ ‐ Executive level II 2 2 3
Executive level III 1 1 1
Executive level IV 1 1 1
Executive level V 1 1 1
Subtotal 5 5 6
Total ‐ Executive Level $880,000 $899,360 $1,089,360
‐ ‐ ‐ ‐
GS‐15 21 22 20
GS‐14 26 27 25
GS‐13 38 39 38
GS‐12 45 45 44
GS‐11 3 3 3
GS‐10 ‐ ‐ ‐
GS‐9 7 7 7
GS‐8 2 2 2
GS‐7 1 1 1
GS‐6 1 1 1
GS‐5 ‐ ‐ ‐
GS‐4 ‐ ‐ ‐
GS‐3 ‐ ‐ ‐
GS‐2 ‐ ‐ ‐
GS‐1 ‐ ‐ ‐
Subtotal 144 147 141
Total ‐ GS Salary $15,387,000 $16,029,640 $15,261,640
‐ ‐ ‐ Average ES level III III III
Average ES salary $176,000 $179,872 $181,560
Average GS grade 13.5 13.6 13.5
Average GS Salary $106,854 $109,045 $108,239

Office for Civil Rights
Page 39
Section V: Significant Items
“The Committee is concerned about reports of continued discrimination against persons with disabilities in organ transplant programs. Despite the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act prohibiting discrimination on the basis of disability in organ transplantation, a number of States have found it necessary to enact laws to address continued barriers to receiving this lifesaving care. These barriers are reported to include medical professionals and transplant centers refusing to approve organ transplants for people with disabilities who may need help in order to follow complicated post‐transplant treatment plans, or deciding that people with disabilities should be given a lower priority on waiting lists to receive an organ transplant. In coordination with HRSA, the Committee urges the Office for Civil Rights (OCR) to develop and issue guidance that clarifies the obligations of ADA‐ and Section 504‐covered entities participating in the transplant process to provide equal access to their programs to individuals with disabilities. In developing such guidance, the Committee encourages OCR to consider prohibiting such covered entities from, among other things, denying medical services related to organ transplantation, refusing to refer an individual to a transplant center or other related specialist for the purpose of evaluation or receipt of an organ transplant, and refusing to place an individual on an organ transplant waiting list, or placement of the individual at a lower‐priority position on the list than the position at which he or she would have been placed if not for his or her disability.” Action Taken or To Be Taken OCR is committed to ensuring non‐discrimination in organ transplant decision‐making and is continuing to coordinate with HRSA and CMS as specific issues arise. As part of this coordination, OCR is working with HHS components on the best ways to provide additional global guidance and technical assistance, which could include, for example, training on civil rights issues, notice of nondiscrimination, and outreach to HHS grantees and patients and their families about the application of disability non‐discrimination laws, including Section 504 of the Rehabilitation Act, the Americans with Disabilities Act, and Section 1557 of the Affordable Care Act, in the context of organ transplants. In addition, OCR incorporates issues about organ transplant decision‐making in its outreach activities to appropriate audiences. For example, OCR has developed a civil rights training curriculum for medical schools that includes a hypothetical involving civil rights issues in transplant decision‐making to raise awareness of these issues among pre‐med and medical school students through a partnership with the Association of American Medical Colleges. The curriculum is both on the MedEd portal for medical students to access and receive credit for completing and is also part of a summer training program sponsored by the AAMC in which OCR has used this transplantation hypothetical to teach thousands of pre‐med and pre‐dental students.

National Coordinator for Health Information Technology

DEPARTMENT of HEALTH
and HUMAN SERVICES
Fiscal Year
2019
Office of the National Coordinator for Health
Information Technology
Justification of Estimates for Appropriations Committee
OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
TABLE OF CONTENTS
TABLE OF CONTENTS ................................................................................................................... 1 LETTER FROM THE NATIONAL COORDINATOR ............................................................................ 1 ORGANIZATIONAL CHART ........................................................................................................... 2 ORGANIZATIONAL CHART: TEXT VERSION .................................................................................. 3 EXECUTIVE SUMMARY ................................................................................................................. 4
Introduction and Mission ...................................................................................................................... 4 Overview of Budget Request ................................................................................................................ 7 Overview of Performance ..................................................................................................................... 9 All Purpose Table ............................................................................................................................... 16
BUDGET EXHIBITS ...................................................................................................................... 17 Appropriations Language.................................................................................................................... 17 Language Analysis .............................................................................................................................. 17 Amounts Available for Obligation...................................................................................................... 18 Summary of Changes .......................................................................................................................... 19 Budget Authority by Activity ............................................................................................................. 20 Authorizing Legislation ...................................................................................................................... 21 Appropriations History ....................................................................................................................... 22
NARRATIVE BY ACTIVITY ............................................................................................................ 23 Health IT ............................................................................................................................................. 23
SUPPORTING EXHIBITS .............................................................................................................. 35 Budget Authority By Object Class - Program Level .......................................................................... 35 Salary & Expenses .............................................................................................................................. 36 Detail Of Full-Time Equivalent (FTE) Employment .......................................................................... 37 Detail Of Positions .............................................................................................................................. 38 Physicians’ Comparability Allowance ................................................................................................ 39

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 1
LETTER FROM THE NATIONAL COORDINATOR
I am pleased to present the fiscal year (FY) 2019 Congressional Justification for the Office of the National Coordinator for Health Information Technology (ONC). This budget focuses on two key priorities: (1) the interoperability of health information, and (2) provider burden reduction through increased usability of health information technology (health IT). The secure transmission of health information is central to the U.S. Department of Health and Human Services’s (HHS) core mission to enhance and protect the health and well-being of all Americans. Within the embedded landscape of large health care delivery networks as well as hundreds of thousands of small providers, ensuring the flow of information requires a technical, policy, and stakeholder engagement driven approach. In order to achieve this goal, achieve ONC’s key priorities, and facilitate a competitive IT enabled marketplace, this budget prioritizes work in the areas of policy coordination and interoperability. In addition, we will engage our stakeholder community and develop policies that improve the usability of health IT. These priorities will allow ONC to support efficient clinical care and advance the health of the country. To date, ONC’s policies have materially increased the use of health IT. Moreover, payment incentives authorized by Congress for electronic health record (EHR) adoption and use have resulted in 58 percent of office-based physicians (from 17 percent in 2008) and 84 percent of non-federal acute care hospitals (from 9 percent in 2008) using electronic health record technology as of 2015. Now that the healthcare system has a digital footprint, ONC’s FY 2019 Budget Request targets increasing interoperability and addressing the provider burden while improving the usability of health IT. ONC’s focus in FY 2019 on the interoperability of health information and burden reduction are priorities in ONC’s Budget Request and also in the legislatively mandated priorities in the 21st Century Cures Act (Cures Act). The Cures Act directs ONC to implement activities that advance interoperability through continued work to address information blocking and to advance health information exchange. A collective national goal of a more efficient healthcare system with manageable costs cannot be met without significant improvements in clinical data liquidity and administrative provider burden reduction. To facilitate this IT enabled market competition, ONC has built a two-part framework, consisting of (1) standards and (2) policies. The administrative infrastructure needed to deliver the complex messages surrounding these policies and standards is also critical. In FY 2019, ONC will coordinate federal efforts to ensure the reduction of regulatory and administrative burden related to the use of health IT, continue to improve the ONC Health IT Certification Program’s efficiency and effectiveness, and advance ONC’s work coordinating Health IT activities across the Federal Government. In FY 2019, ONC will continue to efficiently lead the U.S. Government’s efforts to ensure that electronic health information is available and can be securely and safely shared to improve the health and care of the American public. Thus, ONC’s FY 2019 Budget Request ensures ONC promotes public and private sector efforts to foster a cultural change with the flow of health information, including addressing information blocking and promoting common standards, as well as reducing the burdens associated with health IT use. Taken together, this work is crucial to achieving the promise and power of health IT that serves the needs of the American people and the mission of HHS. /Donald W. Rucker/ Donald W. Rucker, M.D. National Coordinator for Health IT

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
2
ORGANIZATIONAL CHART1
1 ONC is undergoing a reorganization which is planned to be completed in April 2018. The reorganization will gain organizational efficiencies by reducing the number of subordinate offices from ten to three and reallocating staff from across ONC to the Office of Policy and Office of Technology. The Office of the Chief Operating Officer continues to provide agency-wide services and support. This shift in FTE resources will allow ONC to more acutely focus on implementing the key provisions of the 21st Century Cures Act.
National Coordinator for Health Information Technology Donald Rucker
Principal Deputy National Coordinator
Genevieve Morris
Deputy National Coordinator Jon White
Deputy Assistant Secretary for Health Technology Reform
John Fleming
Deputy National Coordinator for Operations Lisa Lewis
(Chief Operating Officer)
Chief Medical Officer Thomas Mason
Office of Clinical Quality
and Safety
Andrew Gettinger
Office of Planning,
Evaluation, and Analysis
Seth Pazinski
Office of Standards
and Technology
Steve
Posnack
Office of the Chief
Operating Officer
Lisa Lewis
Office of Programs
and Engagement
Sherilyn
Pruitt
Office of Policy
Elise
Sweeney Anthony
Office of Public
Affairs and Communica-
tions
Zhan Caplan (Acting)
Office of Care
Transfo—rmation
Kelly
Cronin
Office of the Chief Scientist
Teresa Zayas Cabán
Office of the Chief Privacy Officer
Kathryn
Marchesini

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 3
ORGANIZATIONAL CHART: TEXT VERSION2
National Coordinator for Health Information Technology o Donald Rucker, M.D. Principal Deputy National Coordinator o Genevieve Morris
Deputy Assistant Secretary for Health Technology Reform o John Fleming, M.D. Deputy National Coordinator o Jon White, M.D. Deputy National Coordinator for Operations o Lisa Lewis Chief Medical Officer o Thomas Mason, M.D.
The following offices report directly to the Immediate Office of the National Coordinator: • Office of the Chief Privacy Officer
o Kathryn Marchesini • Office of Policy
o Elise Sweeney Anthony, J.D. • Office of Clinical Quality and Safety
o Andrew Gettinger, M.D. • Office of Care Transformation
o Kelly Cronin • Office of Standards and Technology
o Steven Posnack, M.S., M.H.S. • Office of the Chief Scientist
o Teresa Zayas Cabán, Ph.D. • Office of Programs and Engagement
o Sherilyn Pruitt • Office of Planning, Evaluation and Analysis
o Seth Pazinski • Office of Public Affairs and Communications
o Zhan Caplan (Acting) • Office of The Chief Operating Officer
o Lisa Lewis
2 ONC is undergoing a reorganization which is planned to be completed in April 2018. The reorganization will gain organizational efficiencies by reducing the number of subordinate offices from ten to three and reallocating staff from across ONC to the Office of Policy and Office of Technology. The Office of the Chief Operating Officer continues to provide agency-wide services and support. This shift in FTE resources will allow ONC to more acutely focus on implementing the key provisions of the 21st Century Cures Act.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 4
EXECUTIVE SUMMARY
Introduction and Mission Agency Overview The Office of the National Coordinator for Health Information Technology (ONC), a staff division of the U.S. Department of Health and Human Services (HHS), is the lead agency charged with formulating the Federal Government’s health information technology strategy and coordinating federal health IT policies, standards, and investments.
The 2016 enactment of the 21st Century Cures Act (the Cures Act) represented a pivotal point in ONC’s history. Under the Cures Act, ONC is charged with improving the flow and exchange of electronic health information, advancing interoperability, prohibiting information blocking, and supporting patient access to their personal health information. Since ONC’s inception through executive order in 2004 and codification in 2009 through the Health Information Technology for Economic and Clinical Health (HITECH) Act, ONC’s mission has always been to improve the quality, safety, and efficiency of healthcare through interoperable health systems. The Cures Act strengthened this mission through its provisions that address the current state of health IT in the nation’s healthcare system.
Prior to the Cures Act, ONC helped drive the rapid adoption of health IT and the digitization of the healthcare system. ONC was instrumental in leading the adoption by 2015 of at least basic electronic health record (EHR) technology by 58 percent of office-based physicians, an increase from 17 percent in 2008, and 84 percent of non-federal acute care hospitals, an increase from 9 percent in 2008. Building upon that success and expertise, the Cures Act directed the HHS Secretary to adopt standards and policies that increase health IT interoperability, privacy, and security; to enable and stimulate the trusted exchange of electronic health information when and where it is needed; and to encourage the development of more user-friendly technologies and solutions that support a broader range of healthcare delivery needs. As ONC continues to fully implement the Cures Act, there is a significant need of resources in order to execute specific requirements and policies regarding information blocking and nationwide measurement of EHR interoperability and usability.
Vision Improve the health and well-being of individuals and communities through the use of technology and health information that is accessible when and where it matters most. Mission To help lower healthcare costs, empower consumer choice, and improve provider satisfaction, ONC will work to make health information more accessible, decrease the documentation burden, and support EHR usability. Introduction Achieving nationwide interoperability is a foundational pillar at ONC, and a major provision in the Cures Act. Interoperable health IT supports a healthcare system that promotes high-quality care and increases access by reducing costs, encouraging free market innovation, and stimulating consumer choice. A major key to interoperability is the ability for data to move freely. Data liquidity can lead to new and not yet anticipated market efficiencies and heightened competition in multiple inpatient and outpatient markets.
Rapid EHR adoption has stimulated demand for interoperability and the need for a growing range of health IT products and services. ONC is working towards meeting this demand by coordinating between the government and the private sector, advancing federally recognized standards, enhancing the certification program, and delivering key policy directives. ONC’s work in standards and policies
OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 5
provides extraordinary value to the country by providing entry points for market forces which can lower the cost of care and put patients back in control. ONC’s multi-pronged approach is addressing the technical, policy, and stakeholder requirements necessary to achieving interoperability.
In addition to achieving greater interoperability, ONC is also committed to advancing the usability and development of health IT, while reducing provider burden. These burdens are felt by providers who are responsible for adhering to complex documentation and reporting requirements. ONC’s clinical perspective provides a unique insight into addressing numerous policies impacting providers, and how those policies can reduce EHR-related burdens. Rulemaking that minimizes unintended consequences and unnecessary regulatory burden is time and labor intensive, as is the implementation of the rules. ONC will continue to work with stakeholders to identify where the burdens exist and support efforts across the federal government to consider how health IT can best be used to support the needs of health professionals and their patients for patient-centered and provider-focused care. ONC’s unique technical and policy expertise, leveraging of existing authorities, and strong relationships with the private sector make ONC pivotal and fundamental to achieving interoperability and enhancing the level of patient-centered and provider-focused health IT systems to ultimately provide the healthcare all Americans deserve.
Policy Development and Coordination ONC develops and coordinates federal policies that are outlined in legislation such as the Cures Act, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), and the HITECH Act. The aforementioned legislation increased ONC’s ability to foster innovative solutions that reduce provider burden and coordinate policies to encourage an interoperable learning health system. Specific activities include: • Health IT Policy: As a part of implementing the Cures Act, ONC stood up a single Health IT
Advisory Committee, which has aided in ONC’s policy development, in early 2018. ONC also engages stakeholders through other methods, such as meetings and listening sessions, to continue to forge consensus-based solutions. As public and private value-based programs advance, providers and communities can benefit from health IT that supports interoperability and promotes patient access to their health information.
• Health IT Usability and Burden Reduction: ONC works to identify new tools and activities that will advance the usability and timeliness of health IT, clinical decision support (CDS), and quality measurement. ONC’s unique expertise allows for new innovations to be fostered that reduces providers’ data-related burdens, improve the care they provide, and ensure accurate performance measurement.
• Privacy of Health IT and Patient Access to Health Information: ONC, working closely with HHS’s Office for Civil Rights (OCR), ensures that privacy and security standards are addressed in a consistent manner that reinforces the protection of private health information. A core element of an interoperable health system is patients’ trust in the privacy and security of their health data.
• Strategic Planning: Under the HITECH Act, ONC is required to prepare the Federal Health IT Strategic Plan. As a reflection of collective efforts of federal entities, this plan advances person-centered care, fosters research, encourages innovation, and enhances the nation’s health IT infrastructure.
Standards, Interoperability, and Certification ONC leads a variety of efforts designed to accelerate nationwide progress towards an interoperable health IT infrastructure. By providing standards coordination and development, participating and encouraging pilot activities, and supporting industry-wide health IT testing, ONC helps to create innovative and interoperable health IT solutions. Specific activities include:

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 6
• Standards and Technology Coordination: In order to enable secure and interoperable health IT systems, ONC collaborates with industry to identify best practices and common approaches to implementing security technologies and techniques. ONC focuses on ways to accelerate consensus and, where necessary, convenes broad communities together for the purposes of identifying and developing additional standards guidance. ONC supports health IT development, implementation, and post-deployment use through investing in testing tools and resources that tackle specific interoperability challenges. ONC provides health IT developers with clear criteria for developing their products by issuing certification criteria for the ONC Health IT Certification Program. ONC administers the ONC Health IT Certification Program, which includes oversight of ONC-Authorized Certification Bodies (ONC-ACBs) and ONC-Authorized Testing Labs (ONC-ATLs) which, together, test and certify health IT products.
• Scientific Innovation: ONC develops and establishes scientific policy related to health IT. This fosters healthcare advancement by anticipating, identifying, and tracking innovation of health IT.
Agency Wide Support ONC’s agency-wide support team provides dynamic and flexible support to ONC’s offices and programs through centralized services with responsibility for overall agency efficiency and effectiveness. Activities include: acquisitions and grants; budget formulation and performance management, execution and financial management; travel and conference management; human capital; program integrity; facilities management; monitoring and analysis of ONC’s financial, human capital, and operational internal controls and data; ethics and freedom of information act; executive secretariat; and ONC’s internal information technology deployment, systems planning and management; and maintaining ONC’s statutorily required website, HealthIT.gov. Agency-wide support also provides resources for the shared services that are required by HHS for ONC to operate.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 7
Overview of Budget Request The FY 2019 Budget Request for ONC is $38.4 million in Budget Authority. The FY 2019 Budget Request focuses on the interoperability of health information and provider burden reduction through increased usability of EHRs. The Budget prioritizes ONC’s work supporting policy, rulemaking, standards implementation, and certification efforts to fulfill ONC’s commitment to efficiently create a nationwide interoperable health system. With a landscape of large health care delivery networks and hundreds of thousands of small providers, achieving interoperability among various health IT systems requires ONC to focus on technical, policy, and stakeholder engagement. ONC’s FY 2019 Budget emphasizes ONC’s continued policy development and coordination work, while using ONC’s Health IT Advisory Committee to inform ONC’s policy and program development. ONC will also focus on preventing and reducing information blocking, and other policy and rulemaking activities required under the Cures Act, MACRA, and the HITECH Act. In FY 2019, ONC will accelerate industry progress towards the interoperability of health information through its work on standards coordination, implementation, and testing. ONC will also continue to focus on the liquidity of health information. Improved data liquidity will improve patients’ ability to be an active member of their care team and their ability to competitively shop for healthcare services. Data liquidity is not only key to enabling a truly competitive healthcare market, but it also supports HHS’s goal of delivering person-centered care that marries human services and healthcare. ONC will help coordinate federal efforts to ensure the improvement of health IT usability. Efforts funded by ONC’s FY 2019 Budget also include continued updates to HealthIT.gov and performance planning, evaluation, and monitoring activities required under the Cures Act, MACRA, and the HITECH Act. The following activities demonstrate how ONC is working to create a safe, secure, and interoperable health IT infrastructure, in order to improve health and healthcare for all Americans: Policy Development and Coordination The FY 2019 Budget supports the development and coordination of federal policies that aim to combat information blocking and increase market competition to support an interoperable health system, and addresses burdens felt by providers. In FY 2019, ONC will move FY 2018 close-out costs for adoption and meaningful use programs to Standards, Interoperability, and Certification. This request supports ONC’s continued work implementing the Cures Act. This includes funding to support the Health IT Advisory Committee, which informs ONC’s policies and programs. In FY 2019, ONC will combat information blocking and advance other rulemaking activities as required under the Cures Act, MACRA, and the HITECH Act. This request also includes ongoing policy work to ensure consumers and healthcare providers are engaged and participated in the policy development and coordination process. As required by the HITECH Act, ONC will continue to formulate the Federal Health IT Strategic Plan, which reflects the collective efforts of multiple federal entities to appropriately send, receive, find, integrate, and use interoperable health information to improve healthcare, individual, community and public health, and advance research, all in collaboration with private industry. Standards, Interoperability, and Certification The FY 2019 Budget supports programs and efforts that underpin nationwide progress towards an interoperable and modern health IT infrastructure. In FY 2019, ONC will focus on supporting interoperability among health IT systems by establishing consensus with stakeholders around standards development activities and policies related to the Cures Act, MACRA, and the HITECH Act. To ensure proper implementation of the Cures Act, ONC will continue to administer and provide oversight to the ONC Health IT Certification Program; support modifications to the Certified Health IT Product List (CHPL); support testing tools to ensure products conform to the technical standards adopted for use as

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 8
part of the ONC Health IT Certification Program, FHIR standards, and other potential standards referenced in the Interoperability Standards Advisory; use the Health IT Advisory Committee to identify priority use cases for health IT; and further improve the implementation and ongoing evolution of application programming interfaces (APIs). In addition to the aforementioned provisions, ONC will conduct targeted research and analysis to assess interoperability progress throughout the health IT community. Agency-Wide Support ONC’s agency-wide support team provides dynamic and flexible support to ONC’s offices and programs through centralized services with responsibility for overall agency efficiency and effectiveness. In FY 2019, the Performance Management, and Engagement and Outreach activities will be moved to Agency-Wide Support. These funds continue to support the shared services required by HHS for ONC to operate, including financial and grants management systems, as well as contract management fees and costs related to ONC’s space in HHS’s Southwest Complex. ONC’s Agency-Wide Support team provides expertise in the areas of acquisitions and grants; budget formulation and performance management, execution and financial management; travel and conference management; human capital; program integrity; facilities management; monitoring and analysis of ONC’s financial, human capital, and operational internal controls and data; ethics and freedom of information act; executive secretariat; and ONC’s internal information technology deployment, systems planning and management. Another key function of the Agency-Wide Support team is maintaining and updating HealthIT.gov with content related to ongoing FACA, interoperability, and rulemaking activities, including activities relate d to ONC’s implementation of the Cures Act.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 9
Overview of Performance ONC’s authorizing legislation and overarching mission are set forth in the HITECH Act, and its current priorities are defined in relation to MACRA and the Cures Act. • Pub. L. No: 111-5 Title VIII, Health Information Technology for Economic and Clinical Health
(HITECH) Act https://www.congress.gov/111/plaws/publ5/PLAW-111publ5.pdf • Pub. L. No: 114-10, Medicare Access and CHIP Reauthorization Act (MACRA):
https://www.healthit.gov/sites/default/files/fulfilling_section_106b1c_of_the_medicare_access_and_chip_reauthorization_act_of_2015_06.30.16.pdf
• Pub L. No: 114-255, 21st Century Cures Act, https://www.congress.gov/bill/114th-congress/house-bill/34
During FYs 2016 and 2017, ONC’s efforts were built upon numerous, successful federal and private partnerships that made progress to the ONC mission outlined in the Federal Health IT Strategic Plan. These efforts also galvanized ONC towards achieving the national goal of widespread interoperable health information exchange by FY 2019. ONC’s efforts specifically targeted making electronic health information more accessible, decreasing EHR related documentation burdens, and supporting EHR usability under the Cures Act and MACRA. Below are examples of deliverables produced through ONC’s efforts implemented in FY 2017. These accomplishments demonstrate the type of work undertaken by ONC with funding provided during the FYs 2016 and 2017 timeframe.
Deliverables and Accomplishments from FY 2017 Health IT Certification Program
• Enhanced Oversight and Accountability Final Rule was published • Certified Health IT Product List (CHPL) was updated with corrective action plans for
developers Federal Rulemaking and Guidance
• Leading and supporting health IT components of HHS rulemaking efforts, including: o CMS rulemaking, including Long-Term Care Facility CoP Final Rule, 2017 Physician
Fee Schedule Final Rule, Quality Payment Program, Outpatient Perspective Payment Systems Rule, Episode Payment Model Rule
o Substance Abuse and Mental Health Services Administration (SAMHSA) rulemaking, including SAMHSA Part 2 rule
• Guidance on policies related to health IT interoperability and usability o 2017 Interoperability Standards Advisory published
Health IT Demonstrations • Health IT Playbook was updated with sections related to EHR safety and patient portals • Security Risk Assessment Tool was updated to reflect 2017 policies • EHR Contract Guide with model contract terms was published • Roadmap on state privacy policy was published in collaboration with National Governors
Association • Numerous pilots and challenge grants to spur private sector innovations were launched
Federal Coordination • Interoperability standards measurement framework proposal was published with a comment
period • Policy framework for patient generated health data was published

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 10
In keeping with ONC’s focus on achieving widespread interoperable exchange of health information, and in continuation of the strategy set in FY 2016 for meeting MACRA §106(b) requirements, the performance measures reported in this document focus on providers’ capabilities for interoperable health information exchange, including sending, receiving, finding, and using a common clinical dataset. ONC also continues to monitor the consumer perspective with a measure following consumer access to any information from their EHR. Measure: Provider capability in key domains of interoperable health information exchange (2015)3
Provider group Office- based
physicians Non-federal acute care hospitals
(2015) (2016) • are electronically sending or receiving patient information
with any providers outside their organization 48% 89%
• can electronically find patient health information from sources outside their health system
34% 55%
• can easily integrate (e.g. without manual entry) health information received electronically into their EHR
31% 41%
• had necessary patient information electronically available from providers or sources outside their systems at the point of care
36% 48%
Measure Group: Citizen’s perspective on consumer access and attitudes4 • In 2016, 52 percent of Americans have been given electronic access to any part of their healthcare
record by their healthcare provider or insurer.
3 2016 estimates will not be computable for physicians due to delays in the survey fielding process that occurred during 2016. At the President’s Budget request level, funding for the two annual surveys used to create these measures may not be available. 4 2016 estimates will be computed during fall 2017.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 11
Description of ONC’s Performance Management Process The performance management process at ONC crosscuts policy, standards, and agency-wide efforts. The process gives ONC and its stakeholders a framework to understand agency goals, monitor and discuss progress towards goal attainment, and make revisions to established plans when necessary. ONC’s process includes specific efforts related to: (1) priority setting, (2) measurement and analysis, (3) regular performance reviews, and (4) priority, strategic, and/or operational updates based on findings from performance reviews.
(1) Priority Setting Priority setting in ONC is driven by a set of complementary processes related to (1.1) complying with specific legislative authorities and dated requirements; (1.2) conducting federal strategic planning; (1.3) establishing tactical and action plans; and (1.4) performance management and reporting. Alongside this process, ONC regularly receives and integrates requests from Congress, the Government Accountability Office (GAO), and the Office of the Inspector (OIG) into its priorities and plans for updates on ONC activities, or new or reformed efforts focused on emerging topics.
1.1 Complying with Specific Legislation Authorities, Requirements, and Requests ONC’s authorizing legislation, the HITECH Act, outlines a number of responsibilities and authorities that ONC prioritizes significantly. The HITECH authorities and requirements establish the need for a portfolio of regulatory, convening, program management and coordination, and planning/research projects. Additionally, other legislation, such as annual appropriations, and more recently MACRA and the 21st Century Cures Act, regularly establish new requirements.
1.2 Conducting Federal Strategic Planning Pursuant to HITECH Section 3001(c) (3) (A), ONC coordinates the development of a federal health IT strategic plan. The current plan covering 2015 – 2020 contains the following goals and can be accessed online at http://healthit.gov/strategic-plan/.
Goal 1: Advance Person-Centered and Self-Managed Health Goal 2: Transform Health Care Delivery and Community Health Goal 3: Foster Research, Scientific Knowledge, and Innovation Goal 4: Enhance Nation's Health IT Infrastructure
ONC will be coordinating federal partners to update the strategic plan during the FY 2018 – 2019 timeframe. Additionally, pursuant to the 21st Century Cures Act Section 4001(a), during FYs 2017 and 2018, ONC is leading an HHS-wide effort to establish a goal, strategy, and recommendations for reducing regulatory and administrative burden relating to the use of EHRs.
1.3 Tactical and Action Planning To implement multi-year strategic plans, ONC routinely translates vision, goal, and strategy documents into implementable tactical action plans that can be managed and monitored regularly. The following action plans have helped form the basis for ONC’s current tactical orientation: • Nationwide Interoperability Roadmap: http://www.healthit.gov/policy-researchers-
implementers/interoperability; and, • Roadmap for Patient Safety and Health IT: http://www.healthit.gov/buzz-blog/health-it-
safety/roadmap-improving-health-safety/.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 12
1.4 Performance Management and Reporting ONC’s multi-year strategic and action plans inform the development of performance plans that align organizational components, senior executives, initiative leads, and staff to shared priorities. ONC’s annual organizational and National Coordinator’s performance plans are formulated according to the Department’s Senior Executive Service (SES) performance planning schedule, which is aligned to the fiscal year calendar. In practice, the method for establishing these plans involves a disciplined and detail-oriented series of conversations where the National Coordinator, ONC’s executives, and subject matter experts define and align milestones that must occur in the upcoming fiscal year. Typically, the plan is organized according to ONC’s roles in federal coordination, rulemaking, certification program management, and health IT demonstrations. An annual milestone plan and priority monitoring list is then established alongside development of the following fiscal year’s operating budget. Once the organizational and National Coordinator’s performance plans are finalized, key information is cascaded into the performance plans of senior executives. Each ONC senior executive has a performance plan listing milestones they are responsible to oversee. SES plans also include critical elements related to on-going exhibition of core management and leadership competencies. After the National Coordinator and SES performance plans are in place, typically by December, the process to cascade align employee performance plans with expected milestones begins. (2) Measurement and Analysis Research, data analysis, and evaluation projects are routine throughout ONC, enabling its leaders to make informed decisions. The research, data analysis, and evaluation activities directly support the agency’s needs to have the best administrative, program and external data available when and where they need it most. Because of the relevance of ONC analyses to the federal policy and program administration decision-making processes, the agency makes many of its findings public. The findings are found throughout the federal advisory committee website https://www.healthit.gov/hitac/ and throughout the agency’s websites at http://healthit.gov/dashboard and http://dashboard.healthit.gov/. (3) Regular Performance Reviews The regular review of performance information is commonplace at all levels of ONC using a number of management meetings, documents, and coordination mechanisms, including the following: • Weekly Senior Leadership Management and Policy Meetings; • Monthly Performance Planning and Risk Reviews; • Quarterly Dashboards (reports) of Progress to Critical Milestones; • Quarterly Office Reconciliation Meetings; • Quarterly Leadership Risk Reviews; • Semi-Annual Progress Reviews (e.g., portfolio analyses, mid-year SES and PMAP assessments); • Annual Assessments of Progress to Goal (e.g., Organizational Assessment, end-of-year SES and
PMAP assessments, Annual Performance Report); and, • Multi-year, summative reviews (Congressional Health IT Adoption & Use Report, Health IT
Strategic Plan Progress Reports).

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 13
(4) Priority, Strategic and/or Operational Updates Based on Findings from the Review The processes for planning, reviewing progress, and re-establishing priorities is robust and continuous in an organization where change is expected. Through a culture of continuous quality improvement, a predictable set of senior leadership team meetings, crosscutting priority group meetings, and planning exercises, each ONC staff person has an important contribution to ensuring the most effective and efficient methods are used to achieve agency goals. Outputs and Outcomes Tables ONC’s FY 2018 and 2019 budget performance measures follow nationwide trends in interoperable health information exchange capability and consumer access to the electronic health information maintained by their providers. The measures are based on nationally representative surveys and lag performance of the nation by six months to one year. As such, these measures are best understood as contextual indicators depicting the extent of progress towards nationwide health IT goals. The measures are not meant for depicting the marginal benefit/short-term return on investment for ONC activities. To an extent that the measures can be viewed as outcome measures reflecting on specific ONC activity, it is reasonable to believe that agency efforts undertaken during the 2014-15 timeframe bore impacts on the changes to national measures reported for 2016-17 timeframe. For more information on the relationship of recent advancements in health IT adoption to HHS and ONC policy efforts, see “HITECH Act Drove Large Gains In Hospital Electronic Health Record Adoption” in the peer reviewed journal Health Affairs.5 Taken together, the measures shown in ONC’s budget demonstrate the need for continued efforts and progress in order to achieve nationwide interoperability goals. Performance Measures
Measure to Report against MACRA Section 106(b)(1)
Program/Measure
Most Recent Result / Target /
Summary FY 2018 Target
FY 2019 Target
FY 2019 Target +/- FY 2018 Target
Office-Based Professionals^ 1.E.11 Percent of office-based physicians who can easily integrate (e.g. without manual entry) health information received electronically into their EHR
FY 2015: 31%
(Baseline)
Not Set Not Set --
1.E.14 Percent of office-based physicians who can electronically find (query) patient health information from sources outside their health system
FY 2015: 34%
(Baseline)
Not Set Not Set --
1.E.16 Percent of office-based physicians who had necessary patient information electronically available from providers or sources outside their systems at the point of care
FY 2015: 36%
(Baseline)
Not Set Not Set --
5 HITECH Act Drove Large Gains In Hospital Electronic Health Record Adoption in Health Affairs: http://content.healthaffairs.org/content/36/8/1416.abstract

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 14
Program/Measure
Most Recent Result / Target /
Summary FY 2018 Target
FY 2019 Target
FY 2019 Target +/- FY 2018 Target
1.E.17 Percent of office-based physicians who are electronically sending or receiving patient information with any providers outside their organization
FY 2015: 48%
(Baseline)
Not Set Not Set --
Non-Federal Acute Care Hospitals^^ 1.E.12 Percent of non-federal acute care hospitals that can easily integrate (e.g. without manual entry) health information received electronically into their EHR
FY 2016: 41%
Target: 45% (Target not
met but improved)
Not Set Not Set --
1.E.13 Percent of non-federal acute care hospitals that can electronically find (query) patient health information from sources outside their health system
FY 2016: 55%
Target: Not
Set
Not Set Not Set --
1.E.15 Percent of non-federal acute care hospitals that had necessary patient information electronically available from providers or sources outside their systems at the point of care
FY 2016: 48%
Target: Not
Set
Not Set Not Set --
1.E.18 Percent of non-federal acute care hospitals that are electronically sending or receiving patient information with any providers outside their organization
FY 2016: 89%
Target: Not
Set
Not Set Not Set --
Measures to Understand Consumer Access
Program/Measure
Most Recent Result / Target /
Summary FY 2018 Target
FY 2019 Target^^^^
FY 2019 Target +/- FY 2018 Target
1.F.1 Percent of Americans who have been given electronic access to any part of their health care record by their health care provider or insurer
FY 2016: 52%
Target: 50%
Not Set Not Set --
Data Sources & Notes:
• Physician measures: National Electronic Health Records Survey (NEHRS), which is a supplemental mail survey to the National Ambulatory Medical Care Survey (NAMCS). The NERHS was formerly called the NAMCS EMR Supplement. ONC partially funds the supplement through interagency agreements with the CDC National Center for Health Statistics, which fields

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 15
the broader survey. Due to funding delays and constraints during FY 2016, 2016 estimates will not be available. FY 2017 estimates will be reported during the fall of 2018.
• Hospital measures: American Hospital Association (AHA) Information Technology (IT) Supplement to the AHA Annual Survey, which ONC partially funds through cooperative agreement.
• The Office of the National Coordinator for Health Information Technology's (ONC) Consumer Survey of Attitudes toward the Privacy and Security Aspects of Electronic Health Records and Health Information Exchange. The survey was conducted by NORC at the University of Chicago with MITRE in FY 2013 and 2014, however due to funding constraints, ONC did not field the survey in FY 2014, and so for FY 2015 no estimates will be available. In FY 2015, the survey questions were merged into the NIH-sponsored Health Information National Trends (HINTS) Survey. The next survey estimates will be available for FY 2016, which will be report during calendar year 2017.
• Targets are not set for the performance measures currently in ONC’s Budget Request due to the effects of resource constraints on the underlying surveys and ONC’s research team, which has shifted to support other aspects of the agency’s agenda. Efforts are currently underway within ONC to revise the President’s Budget measures away from the current survey-based measures to measures that better reflect the product and near term benefits of investments in ONC.
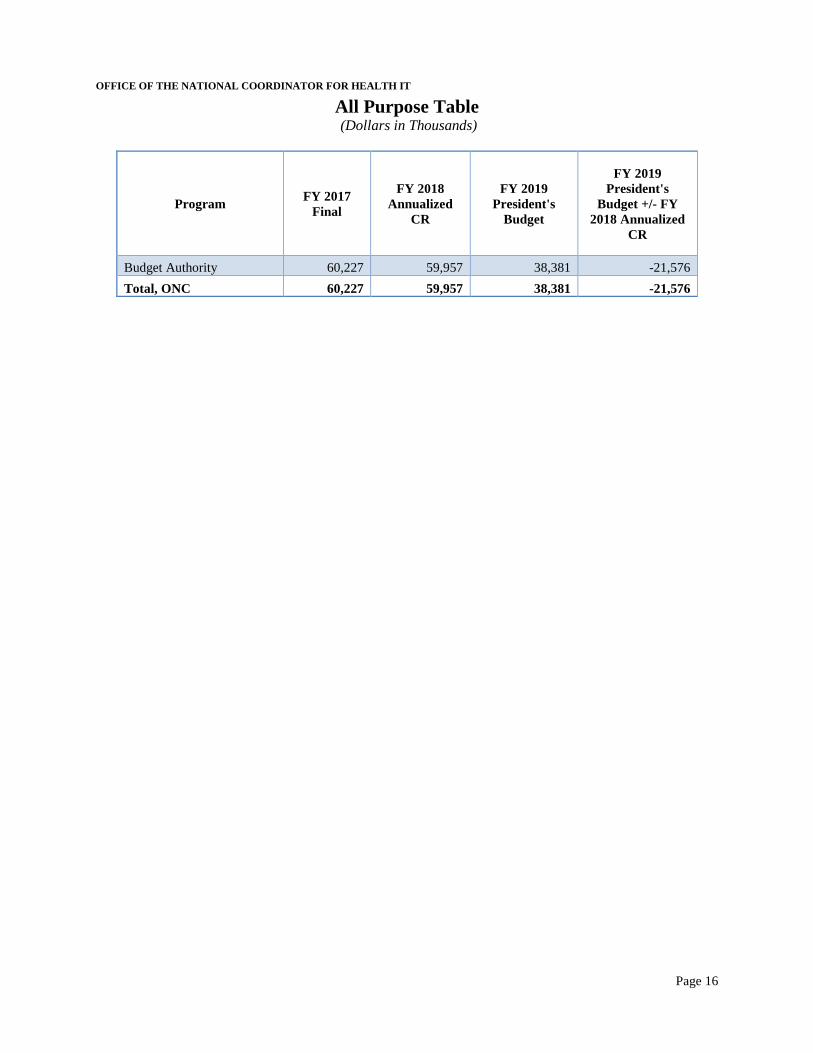
OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 16
All Purpose Table (Dollars in Thousands)
Program FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President's
Budget
FY 2019 President's
Budget +/- FY 2018 Annualized
CR
Budget Authority 60,227 59,957 38,381 -21,576
Total, ONC 60,227 59,957 38,381 -21,576
OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 17
BUDGET EXHIBITS Appropriations Language
For expenses necessary for the Office of the National Coordinator for Health Information Technology, including grants, contracts, and cooperative agreements for the development and advancement of interoperable health information technology, $38,381,000.
Language Analysis
Language Provision Explanation
$38,381,000 Provides ONC’s budget from Budget Authority

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 18
Amounts Available for Obligation
Detail FY 2017 FY 2018 FY 2019
Final Annualized CR President's Budget
General Fund Discretionary Appropriation:
Annual, B.A 60,367,000
60,367,000 38,381,000
Subtotal, Appropriation 60,367,000
60,367,000 38,381,000
Transfer of Funds to: “ACF” 140,000
Across-the-board Reductions (L/HHS) 409,952 38,381,000
Subtotal, Adjusted Budget Authority 60,227,000 59,957,048 38,381,000
Total, Discretionary Appropriation 60,367,000 59,957,048 38,381,000
Total Obligations 60,227,000 59,957,048 38,381,000

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 19
Summary of Changes (Dollars in Thousands)
2018 Annualized CR
Total estimated program level.................................................................................................................................... 59,957
2019 President's Budget Total estimated program level.................................................................................................................................... 38,381
Net Change program level.......................................................................................................................................... -21,576
FY 2018 Annualized
CR FY 2019 PB
FY 2019 +/-
FY 2018
FTE Program Level FTE Program
Level FTE Program Level
Decreases: A. Program:
1. Health IT.................................................................. 164 59,957 164 38,381 0 -21,576
Subtotal, Program Decreases........................................... 164 59,957 164 38,381 0 -21,576 Net Change......................................................................... 164 59,957 164 38,381 0 -21,576

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 20
Budget Authority by Activity
(Dollars in Thousands)
Activity
FY 2017 FY 2017 FY 2018 FY 2018 FY 2019 FY 2019
Final FTE Final Annualized
CR FTE Annualized
CR
President's Budget
FTE
President's Budget
Health IT Annual Budget Authority 187 60,227 164 59,957 164 38,381 Total, Annual Budget Authority 187 60,227 164 59,957 164 38,381
Total, Program Level 187 60,227 164 59,957 164 38,381

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 21
Authorizing Legislation (Dollars in Thousands)
2018 2018 2019 2019
Health Information Technology Activity: Authorized Amount
Appropriated Authorized President’s
Budget
Title XXX of PHS Act as added by the HITECH Act (PL 111-5) and the Cures Act (PL 114-255) Indefinite
- Indefinite
-
Budget Authority Indefinite
59,957 Indefinite
38,381
Total Request Level
59,957
38,381

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 22
Appropriations History (Dollars in Thousands)
Details Budget
Estimates to Congress
House Senate Appropriations Allowance Allowance
2010 Annual B.A. $42,331 $0 $42,331 $42,331 PHS Evaluation Funds $19,011 $61,342 $19,011 $19,011 Subtotal $61,342 $61,342 $61,342 $61,342
2011 Annual B.A. $78,334 $69,842 $59,323 $42,331 PHS Evaluation Funds $0 $0 $19,011 $19,011 Rescissions (Secretary’s) ($85) Subtotal $78,334 $69,842 $78,334 $61,257
2012 Annual B.A. $57,013 $0 $42,246 $16,446 PHS Evaluation Funds $21,400 $28,051 $19,011 $44,811 Rescissions (P.L. 112-74) ($31) Subtotal $78,413 $28,051 $61,257 $61,226
2013 Annual B.A. $26,246 $16,415 $16,415 $16,415 PHS Evaluation Funds $40,011 $44,811 $49,842 $44,811 Rescissions ( P.L. 113-6) ($33) Sequestration ($826) Subtotal $66,257 $61,226 $66,257 $60,367
2014 Annual B.A. $20,576 $20,290 $15,556 PHS Evaluation Funds $56,307 $51,307 $44,811 User Fee $1,000 $1,000 $0 Subtotal $77,883 $0 $72,597 $60,367
2015 Annual B.A. $0 $61,474 $61,474 $60,367 PHS Evaluation Funds $74,688 $0 Subtotal $74,688 $61,474 $61,474 $60,367
2016 Annual B.A. $0 $60,367 $60,367 $60,367 PHS Evaluation Funds $91,800 $0 $0 $0 Subtotal $91,800 $60,367 $60,367 $60,367
2017 Annual B.A. $0 $65,367 $60,367 $60,227 PHS Evaluation Funds $82,000 $0 $0 $0 Subtotal $82,000 $65,367 $60,367 $60,227
2018 Annual B.A. $38,381 $38,381 $60,367 $59,957 PHS Evaluation Funds $0 $0 $0 $0 Subtotal $38,381 $38,381 $60,367 $59,957
2019 Annual B.A. $38,381 PHS Evaluation Funds $0 Subtotal $38,381

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 23
NARRATIVE BY ACTIVITY
Health IT
Budget Summary (Dollars in Thousands)
Health IT FY 2017 Final
FY 2018 Annualized
CR
FY 2019 President's
Budget
FY 2019 +/- FY 2018
Budget Authority 60,227 59,957 38,381 -21,576
Total, Program Level 60,227 59,957 38,381 -21,576
FTE 187 164 164 - Authorizing Legislation: Enabling Legislation Citation…..…..Title XXX of PHS Act as added by the HITECH Act (PL 111-5) and
amended by the Cures Act (PL 114-255) Enabling Legislation Status……….…………………………...................................…................Permanent Authorization of Appropriations Citation……….………...…No Separate Authorization of Appropriations Allocation Method………………...…......…....…Direct Federal, Contract, Cooperative Agreement, Grant Program Description and Accomplishments A health IT system that allows clinical data to move freely and reduces provider burden is key to achieving a more efficient healthcare system with reduced costs. The nearly unanimously enacted Cures Act provided ONC with powerful tools to encourage market competition and personal electronic ownership of data, and to combat information blocking. In order to achieve an efficient healthcare system with manageable costs, significant improvements in clinical data liquidity and administrative provider burden reduction must be made. To facilitate this IT enabled market competition, ONC has built a two-part framework, consisting of: (1) Policy and (2) Standards. An administrative infrastructure is also crucial to ensuring the complex messages surrounding these policies and standards are delivered adequately. ONC continues to support the development and coordination of federal policies and rulemaking activities, which promote interoperability and reduce provider burden. ONC also supports interoperability among health IT infrastructures, by working to develop consensus around standards development activities and policies. ONC uses its statutorily required website, HealthIT.gov, as a key method of engaging stakeholders, educating and disseminating nationwide best practices and solutions to common challenges that providers and consumers face related to adoption and use of health IT. ONC’s unique technical and policy expertise and strong relationships with the private sector make ONC pivotal to achieving interoperability and enhancing the level of patient-centered and provider-focused health IT systems, ultimately providing the healthcare all Americans deserve.
Policy Development and Coordination ONC coordinates federal policies and strategies to build the necessary data and technology foundation for an interoperable learning health system that can support a wide variety of national priorities and assure that data can be securely captured, and shared with, and used by, the right people at the right time. This will advance a patient-centered health care system which focuses on promoting quality care, while

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 24
increasing accessibility and affordability, augmenting innovation, and empowering patients. Achieving interoperability will lead to informed consumers who have a choice in their healthcare. Within the embedded landscape of large insular health care delivery networks, and a vast number of smaller providers, achieving interoperability requires a technical, policy, and stakeholder engagement driven approach. In collaboration with federal partners and by engaging with a broad range of health IT stakeholders, ONC sets the direction of federal health IT policy, seeking to achieve interoperability and providing a policy framework to address emerging health IT issues regarding the use and exchange of electronic health information. This policy framework inspires trust and confidence in health IT by integrating privacy, security, and clinical best practices into every phase of health IT policy development and implementation. ONC’s health IT policies enable care transformation through improved care coordination, increased patient engagement, and enhanced population health management. ONC identifies emerging issues, and gaps in existing policies; formulates solutions; and provides guidance to federal agencies and stakeholders so that individuals, care providers, and public health workers can get the health information they need in an electronic format when and how they need it. By integrating a clinical perspective into its policy development and coordination activities, ONC helps foster innovative solutions to reduce health IT-related burdens on providers. These federal health IT policies support interoperability, health IT usability, and support tools like quality measures that help providers manage the vast array of information needed to deliver the safest and best care possible. ONC develops and coordinates federal health IT policy to achieve national priorities set forth by the Administration and the HHS Secretary in accordance with statutory requirements under the Cures Act, MACRA, and the HITECH Act, among other laws. MACRA, and specifically the Quality Payment Program, provides new tools and resources to support providers as they transition to value-based reimbursement and methods of delivering care. As public and private value-based programs advance, providers and communities can benefit from health IT that supports interoperability, and promotes patient access to their health information. Stakeholder Coordination and Support ONC guides the achievement of goals and objectives outlined in the Federal Health IT Strategic Plan 2015-2020 through ongoing collaboration with federal partners, states, and engagement of stakeholders. ONC monitors the progress of and aligns federal activities with national priorities, goals, and objectives. Accomplishments include: • As required by the Cures Act, ONC is transitioning its current Health IT Policy and Health IT
Standards Federal Advisory Committees—established by the HITECH Act—to a single Health IT Advisory Committee. The stakeholder input received from these two sunsetted committees played a critical role in ONC’s policy development. The committees also helped ONC better understand the needs of patients and providers, develop pilots, studies, and other programs, and advance standards, implementation specifications, and certification criteria that support interoperability. ONC expects the new committee, whose inaugural meeting occurred in January 2018, will play a similar role in advising ONC’s work.
• ONC finalized implementation of the “ONC Health IT Certification: Enhanced Oversight and Accountability” final rule which further enhances the safety, reliability, transparency, and accountability of certified health IT for users. This rule furthers ONC’s ability to address and correct non-conformities found in certified health IT products that cause or contribute to serious risks to public health or safety. Additionally, the rule empowers health IT consumers to make more informed choices by making more information available about how an individual certified health IT product performs in the field.
• ONC implemented the 2015 Edition Certification Rule which builds on past certification rules and is designed to support innovation and the establishment of a nationwide interoperable health

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 25
information infrastructure. To support stakeholder implementation of the final rule, ONC issued certification, surveillance, and transparency guidance and education materials, including the creation of a website that compiles certified health IT product information to provide more transparency to users regarding what a product does or does not do.
Interoperability of Health Information Exchange ONC is working with stakeholders, health information organizations, service providers, and other entities to ensure trust among participants, as well as interoperability across networks, so that health information can follow a patient regardless of where and when they access care. For example, ONC enabled a web-based public comment mechanism for stakeholders to inform ONC’s work on critical elements of health information exchange that could advance patient care and will inform ONC’s work to implement provisions in Section 4003 of the Cures Act related to the establishment of a national trusted exchange framework and the development or support of a common agreement. Health IT Usability and Burden Reduction ONC provides leadership and coordinates activities with key stakeholders to advance the availability, usability, and timeliness of health information, clinical decision support (CDS), and quality measurement. In accordance with Section 4001 of the Cures Act, ONC will continue to identify usability challenges that impede providers from efficiently providing care. Ensuring providers have adequate resources and improving the usability of health information technology will help improve direct care to patients and reduce provider burden. Automated measurement tools, such as electronically specified clinical quality measures (eCQMs) and clinical data registries that automate data abstraction from EHRs, allow for timely performance feedback and patient outcomes monitoring, while reducing providers’ data-related burdens. CDS brings clinical best practices to the point of care, converting data to knowledge in user-friendly, actionable electronic forms. CDS helps clinicians better manage the vast array of information needed to deliver the safest and best care possible, especially to those with multiple, chronic or rare conditions. CDS helps providers by ensuring they have the most up-to-date and clinically relevant information to identify the best course(s) of treatment, and promoting discussion of those options with the patient. There is significant potential for this support to improve our state of preparedness for response to emergent public health threats, such as infectious-disease outbreaks or environmental emergencies. Accomplishments include: • Developed an electronically specified measure of patient safety, which addresses meaningful issues to
patients and providers, without adding to their data burden by ensuring that the measure relies on data already generated during care. This measure, and the results of its feasibility testing for use within patient settings, will be available in the first half of 2018.
• Developed and tested a usability-improvement toolkit for hospital and provider practice IT and performance improvement teams. The toolkit is designed to help small, rural, and other hospitals and practices without access to specialized usability expert resources. The toolkit will help provider IT and performance improvement teams determine how to make their systems work better and pose fewer usability challenges for their providers, patients, and other care team members. The toolkit will be available in the first half of 2018.
Privacy of Health IT and Patient Access to Health Information Patient trust in the privacy and security of health data is a core requirement of an interoperable health system. ONC ensures this requirement is met by advising on health information privacy, security, and data stewardship policies. Key components of the work involve working with the HHS Office for Civil Rights (OCR), in order to demonstrate how the Health Insurance Portability and Accountability Act (HIPAA) and other privacy laws and regulations support, rather than impede, information flow in an electronic environment. ONC also develops and supports approaches that ensure information is shared electronically and is kept secure. Accomplishments include:

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 26
• In accordance with the access provisions of Section 4006 of the Cures Act, worked with OCR to develop education materials and guidance for providers and policymakers on how HIPAA enables data sharing.
• Updated the Model Privacy Notice (MPN) and launched the Privacy Policy Snapshot Challenge. The MPN is a voluntary, openly available resource designed to help developers clearly convey information about their privacy and security policies to their users. The Privacy Policy Snapshot Challenge leveraged updated MPN content, with feedback from OCR, the Federal Trade Commission, and other private and public stakeholders that identify certain areas that should be highlighted for the consumer.
Strategic Planning ONC develops the Federal Health IT Strategic Plan. This Plan reflects the collective efforts of federal entities to advance person-centered health and self-management; transform health care delivery and community health; foster research, scientific knowledge, and innovation; and enhance the nation’s health IT infrastructure. Accomplishments include: • Published The Federal Health IT Strategic Plan 2015 – 2020, representing the collaborative efforts
across the Federal Government, with more than 35 federal entities contributing to its development. In 2017, ONC convened the Federal Health IT Coordinating Council, an internal federal body with the mission of coordinating federal health IT policy decisions and creating a forum to discuss program alignments for existing and emerging health and health IT matters. The 2017 task of this body was to coordinate and prioritize implementation accountabilities to advance interoperability and the health IT provisions in the Cures Act.
• In 2016, in accordance with MACRA, established metrics to determine if, and the extent to which, Congress’s national objective to achieve widespread exchange of health information through interoperable certified EHR technology nationwide by December 31, 2018, is accomplished.
Standards, Interoperability, and Certification ONC makes strategic investments in standards coordination, implementation, testing, and pilots, to accelerate industry progress in specific areas that require interoperability. This work focuses on interoperability improvements related to care coordination, medication management, patient engagement, clinical research, privacy and security, and population health. Through the ONC Health IT Certification Program, ONC outlines processes for health IT developers to demonstrate how their health IT conforms to specific certification criteria and standards. ONC supports the creation and publication of “certification companion guides” and test procedures under the Certification Program. In collaboration with the National Institute of Standards and Technology (NIST) and health IT stakeholders, ONC leads the development of the electronic testing tools and test procedures that are used to test health IT products to specific certification criteria. ONC strives to maintain an innovative health IT environment by continuing to support entrepreneurs and health technology developers as they seek to improve the accessibility and usability of health information. These initiatives work together to advance the national health IT infrastructure and improve the health and well-being of the nation. Standards and Technology Coordination ONC will continue to play a key role as a leader and convener of the health IT community through structured coordination and collaboration. In order to continue to improve interoperability, it is necessary for the health IT ecosystem to reduce variability and consistently implement common standards that enable specific functionalities that are relevant to the end user. Moreover, ONC collaborates with industry to identify best practices and common approaches to implementing security technologies and techniques in order to enable secure, interoperable health IT systems. ONC focuses on ways to accelerate consensus

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 27
and, where necessary, convenes broad communities together for the purposes of identifying and developing additional standards guidance. Accomplishments include: • Published the Interoperability Standards Advisory via an online platform that provides a detailed list
of the standards and implementation specifications that can be used to address various interoperability needs.
• Awarded a cooperative agreement in collaboration with a standards development organization to support the acceleration and development of new technology specifications for application programming interfaces (APIs).
• Supported and participated in public-private partnerships that advance technology interests consistent with the Cures Act.
• Collaborated with OCR and health IT stakeholders to identify and provide technical security information and guidance associated with implementing APIs and other health IT capabilities.
• Supported the Interoperability Proving Ground (IPG), which is an open community platform where users can share, learn, and be inspired by interoperability projects occurring in the United States (and around the world). The IPG currently has over 200 entries of on-the-ground efforts that advance the interoperable exchange of health information. Entries have been submitted by stakeholders across the health IT industry such as developers, health information exchanges (HIEs), standards developing organizations (SDOs), and health insurers.
Certification The ONC Health IT Certification Program provides comprehensive and independent mechanisms for health IT to be evaluated for conformance to standards and functional requirements adopted in regulation. ONC also maintains the Certified Health IT Product List (CHPL), a publicly available list on ONC’s website of all health IT products certified through the ONC Health IT Certification Program. The CHPL generates a CMS EHR ID number that is representative of the Certified Electronic Health Record Technology (CEHRT) used to participate in several CMS payment programs. Accomplishments include: • ONC, in collaboration with NIST, completed development of, and deployed, the 2015 Edition Test
Method for the adopted 2015 Edition certification criteria, which includes test procedures, test data, and test tools for use by Accredited Testing Labs (ATLs). The 2015 Edition adheres to more rigorous conformance criteria than were used for prior editions and includes more electronic and automated testing tools.
• Supported the ongoing maintenance of Certification Companion Guides (CCG) to help health IT developers quickly understand and interpret ONC’s regulatory requirements so they may focus on product development. A CCG has been developed for each certification criterion and will serve as the single, consolidated information source for any clarifications related to a certification criterion.
• Revised the CHPL website to align with the 2015 Edition final rule’s additional data needs and offered new ways to view product details in order to support greater transparency and open data accessibility. The new CHPL website includes additional functionality, such as advance search, product compare, and API methods to enable stakeholders the ability to openly access and combine CHPL data with their datasets.
• Approved private sector developed testing methods for use as alternatives to the government-developed test methods in the ONC Health IT Certification Program.
Public-Private Testing To reach nationwide interoperability, ONC continues to invest in priority testing tools and resources that support health IT development, implementation, post-implementation, and use. ONC provides an open testing environment that allows health IT developers and the provider community to verify that their systems have implemented interoperability standards in a consistent manner. Each ONC-led activity tackles a critical interoperability challenge through processes that recognize and consider the clinical uses

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 28
in scope, identification, and harmonization of existing technical specifications, implementation guidance, pilot projects, and mechanisms for feedback to evaluate effectiveness. Accomplishments include: • Standards Implementation and Testing Environment (SITE) provides conformance testing and
validation tools for certain health IT functionality, in support of the ONC Health IT Certification Program. SITE facilitates resolution of standards implementation issues by working closely with the standards community and IT developers. SITE also provides an established venue to disseminate identified solutions to a broad community of health IT developers and users.
• Created a Consolidated Clinical Document Architecture (C-CDA) scorecard (“C-CDA Scorecard”) to give both health IT developers and providers the ability to benchmark system performance.
• Created the “One Click Scorecard” which enables health care providers to test the performance of their health IT (relative to direct transactions and the C-CDA) as it’s deployed in real world settings.
Health IT Infrastructure and Innovation ONC leads efforts designed to encourage a vibrant health IT marketplace, where systems are interoperable and stakeholders have the ability to obtain “best-of-breed” solutions from among a number of choices. ONC works to encourage the development of innovative solutions to health IT challenges, and also to find ways to better support the innovation community. ONC encourages innovation in health IT by coordinating vendors, startups, the venture capital community, incubators, providers, and researchers that are at the leading edge of health IT. Accomplishments include: • Supported a market transparency project that helped health care stakeholders more easily identify the
costs associated with health IT interoperability services. • Hosted publicly available webinars on various health IT topics to showcase interoperability in action
and inform a broader stakeholder base about interoperability and innovation activities. Scientific Innovation ONC makes critical advancements in interoperability in the service of biomedical and health services research. ONC continues to foster healthcare advancement by anticipating, identifying, and fostering innovation of health IT. In particular, ONC plays a vital role in the Precision Medicine Initiative (PMI) and is spearheading relevant patient-centered outcomes research (PCOR) projects. Accomplishments include: • Completed the technical development for the Sync for Science (S4S) project, conducted with the
National Institutes of Health (NIH). Following S4S integration with NIH’s All of Us Research Program (AoURP) application programing interface (API), participants at pilot sites will be able to utilize the API to share their electronic health data with the AoURP. Pilot testing is planned to begin early 2018.
• Concluded the S4S Privacy and Security project (S4SPS), in which several S4S EHR developers and health care provider organizations agreed to participate. Independent testing and assessment results were shared with participants to address any potential privacy and security issues uncovered during testing. Aggregate testing results and key findings were shared with NIH and OCR.
• The first phase of the Sync for Genes project, established to facilitate clinical genomics at the point of care, and in research studies such as the NIH AoURP, concluded in June 2017. In Phase 1, five pilots focused on testing the HL®FHIR® Clinical Genomics standard utilizing use cases that were identified as priority focus areas to support the AoURP. The pilot participants provided feedback which was relayed back to the HL7 Clinical Genomics Work Group. The pilot process, feedback, lessons learned, and recommendations for next steps, are available in the final report, which was released in the Fall of 2017.
• ONC’s ongoing PCOR projects continued to address interoperability challenges. In 2017, ONC executed prize challenges focusing on patient matching, health data provenance, and Block chain, and funded the development of implementation guides to expand the ability of users to create value out of their data. Additionally, ONC partnered with stakeholders on pilot tests and demonstrations to field

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 29
test resources developed across the PCOR projects, focusing on topics such as patient-generated health data and structured data capture.
• Completed a patient matching algorithm challenge and launched security challenges, including a data provenance challenge and secure API server challenge.
Agency-Wide Support ONC launched a number of crosscutting efforts to ensure ONC’s management is enhanced, customer service is improved, programs are efficiently supported, grantee and contractor performance is optimized, a world-class workforce continues to be developed, and budget processes and operational services are enhanced. Development is collaborative in nature, and ONC continues to increase efficiency in its program support partnership activities. These cost effective efforts ensure that ONC is exemplifying care of public resources, in order to advance a health care system centered on the patient, and focusing on promoting quality care, increasing accessibility, bolstering innovation, and empowering patients. Procurement and Grants Management ONC enhanced its grants management and procurement efforts, implementing best practices to optimize grantee and contractor performance. Using a risk-based financial monitoring framework for grants and contracts, ONC fosters program success and financial accountability. ONC has built a strong monitoring, analysis, and data management capability, and manages nimble procurement and grants training programs to ensure proper stewardship of federal funds. Enterprise Risk Management ONC carries out financial and programmatic oversight responsibilities, employing a robust internal review methodology to achieve high-impact results and fostering data-driven and risk-based decision making. ONC enhanced its operational reporting and data management capabilities, and established an Enterprise Risk Management framework within ONC. In addition, ONC improved its ethics, audit liaison, and executive secretariat processes. Human Capital ONC’s human capital experts provide leadership, oversight, and guidance to ONC in hiring and maintaining a talented workforce. ONC optimizes its strong and high-performing organization through strategic workforce planning and innovative recruitment and retention strategies, including those for students and Veterans and through enhanced professional development opportunities. Budget, Performance Management and Operational Services ONC’s Budget, Performance Management, and Operational Services functions include budget formulation and execution and space and facilities management, along with the crosscutting policy, technical, and program management efforts which provide different levels of ONC staff with clear and common agency-wide goals. ONC initiated improvements in its annual budget processes and budget/performance integration. In addition, ONC continues to strengthen management controls over its financial processes. ONC’s telecommunications and technical infrastructure initiatives have yielded cost savings and improved value. These initiatives include ONC’s space consolidation efforts within the HHS Southwest Complex, and improvements in ONC’s internal information technology deployment strategies. Stakeholder Engagement ONC’s statutorily required website, HealthIT.gov, is a key method of educating and disseminating, nationwide, best practices and solutions to common challenges that providers and consumers face with respect to the adoption and use of health IT. ONC’s website is updated with ongoing federal advisory committee, interoperability, and rulemaking activities.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 30
Funding History Health IT
Fiscal Year Amount
FY 2015 60,367,000
FY 2016 60,367,000
FY 2017 60,367,000
FY 2018 Annualized CR 59,957,048
FY 2019 President's Budget 38,381,000 Budget Request Health IT ONC requests $38.4 million in FY 2019 to support activities related to policy development and coordination, standards and technology, and scientific innovation, a decrease of $21.6 million below the FY 2018 Annualized CR. This request includes funding for 164 FTEs. These funds will continue to support ONC’s mission of achieving a health IT system that allows clinical data to move freely and reduces provider burden in order to achieve a more efficient healthcare system with reduced costs. ONC continues to support the development and coordination of federal policies, rulemaking and activities, and interoperability among health IT infrastructures which promote interoperability and reduce provider burden. Policy Development and Coordination The FY 2019 Budget reflects a continued commitment to improving care for the nation by enabling a secure, interoperable health system that reduces burden and improves patient access. ONC will continue to combat information blocking by prioritizing the policy and rulemaking activities that are included in the Cures Act, MACRA, and the HITECH Act. ONC will continue to use the Health IT Advisory Committee to inform ONC’s policies and programs. ONC will continue to support privacy and patient safety by developing rules and policies that enhance the safety, reliability, transparency, and accountability of certified health IT. In FY 2019, ONC will also revise the Federal Health IT Strategic Plan. These specific policy priorities will allow ONC to be a more lean and effective organization, while still striving to achieve widespread interoperability and usability of health IT. ONC’s budget request supports continued health IT efforts required under the HITECH Act, MACRA, and the Cures Act to meet the needs of providers, patients, and researchers who rely on health IT, as well as work with stakeholders and policymakers at the federal, state, and provider level to propel the safe and secure movement of health information in order to ensure that care teams have the right information when and where it is needed.
Stakeholder Coordination and Support Funding will support ONC’s continuous operation of the Health IT Advisory Committee, which is required in the Cures Act. This committee will play a critical role in ONC’s policy development and the advancement of standards, implementation specifications, and certification criteria to support interoperability across the care continuum. Through these efforts, ONC is able to work directly with relevant stakeholder groups to more quickly understand where improvements to interoperability could be made and determine where more focused industry coordination is necessary.
In FY 2019, ONC will work to support implementation of the recommendations included in the planned report to Congress, as required by Section 4001 of the Cures Act (to be released in 2019), addressing strategies and recommendations with respect to the reduction of regulatory or administrative burdens relating to the use of electronic health records. ONC will continue its engagement with Congress, federal

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 31
partners, and other stakeholders to implement the strategies and recommendations outlined in legislatively required reporting.
Interoperability of Health Information Section 4003 of the Cures Act directs ONC to develop or support a trusted exchange framework, including a common agreement among health information networks nationally. In FYs 2017 and 2018, ONC engaged, and continues to engage, with stakeholders to receive comment and feedback on a trusted exchange framework and common agreement related to health information exchange. The framework and common agreement will help (1) advance health information exchange, (2) advance the interoperable flow of health information across disparate networks, and (3) create supportive principles related to enabling trusted exchange nationally. In FY 2019, ONC will focus on the implementation of the framework and common agreement completed in FY 2018, including working with the private sector and identifying technical needs to support interoperable exchange across disparate networks.
In accordance with Section 4004 of the Cures Act, ONC will continue to address and discourage information blocking by finalizing and aggressively implementing ONC Certification Program rules, creating and promoting clear channels for reporting information blocking, and providing technical assistance to the HHS Office of Inspector General (OIG) and OCR on mechanisms for enforcing information blocking provisions, as directed by the Cures Act.
Health IT Usability and Burden Reduction ONC will further its goal of enhancing the usability of health IT to decrease documentation burden, and support new business models and software applications that promote intuitive and functional health IT tools for patients and clinicians. In accordance with Section 4001 of the Cures Act, ONC is required to engage with stakeholders including other federal partners to develop a goal, strategy, and recommendations to leverage health IT to reduce provider, administrative, and regulatory burden. In FY 2019, ONC will implement strategies and recommendations related to burden reduction, as presented to Congress pursuant to Section 4001 of the Cures Act. As described in the Cures Act, these will include activities related to health information technology certification; standards; patient access; simplifying quality measurement; and aligning data requirements across federal programs and other payers. Consistent with Section 4001 of the Cures Act, ONC anticipates recommendations will address actions that help clinicians improve patient care quality and safety, such as by ensuring that complete and accurate information on each person’s current medications, medical conditions, and any allergies, is available whenever and wherever that person needs care. ONC will continue to work with CMS on the implementation of MACRA provisions associated with the Quality Payment Program. Specifically, ONC will work with CMS to engage with stakeholders, and to develop and implement policies supporting provider participation in the CMS Quality Payment Program and alternate payment models established under MACRA. This will ensure health IT serves as a tool to reduce physician administrative reporting burden and administrative burden associated with chart abstraction, while trimming the waste of misaligned reporting requirements across programs and incentivizing program participation that provides actionable feedback based on a health care organization’s specialty and patient population. Privacy of Health IT and Patient Access to and Control over Health Information ONC will continue to work with OCR to address privacy and security concerns that may serve as a barrier to interoperability. ONC will address information blocking and enhance usability by continuing to clarify how HIPAA supports the exchange of electronic health information and consumer access to their health information. ONC will continue to assure that policies that address the protection of private and secure health information are in place. ONC will also work with OCR on efforts to clarify patients’ rights to access and share health information. In accordance with Section 4006 of the Cures Act, ONC will provide

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 32
subject matter expertise on how HIPAA and health IT innovation support patient access rights, and work to resolve issues such as identity management that might impede health information exchange. Strategic Planning In FY 2019, ONC will update the Federal Health IT Strategic Plan: 2020-2024. The plan will provide a federal blueprint to further the goals of interoperability and reduction of provider burden across the federal landscape.
Standards, Interoperability, and Certification The FY 2019 budget will support advancing nationwide interoperability and coordinating the technical activities needed to advance the standards and health IT certification requirements envisioned by the Cures Act. ONC will engage the public and private sectors to identify and fill gaps in the current health IT infrastructure. ONC will also coordinate standards development and enhancement, and ensure that the governance of our nation’s health data supports equity, scalability, integrity and sustainability of information sharing for everyone in the United States. Achieving interoperability will lead to shoppers who have an informed choice in their healthcare. Standards Coordination and Collaboration In FY 2019, ONC’s efforts will build upon recent accomplishments to make continued progress toward modernizing the nation’s health IT infrastructure, in order to support transformative, interoperable learning health care. Further, ONC will continue to support collaborative initiatives to accomplish accelerated and coordinated standards work. Achieving interoperability requires a technical, policy, and stakeholder engagement driven approach. This funding and work is important for ONC, and for the many other HHS agencies that ONC has collaborated with in the past, including CMS, the Assistant Secretary for Planning and Evaluation (ASPE), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Agency for Healthcare Research and Quality (AHRQ),6 the Centers for Disease Control and Prevention (CDC), the Department of Defense (DoD), the Department of Veterans Affairs (VA), and other federal agencies. ONC will focus on coordinating the interoperability, standards, and certification requirements outlined in the Cures Act, and will continue to play a key role as a leader and convener of the health IT community. Additionally, ONC will focus on ways to accelerate consensus and, where necessary, convene broad communities together for the purposes of identifying and developing additional standards and implementation guidance. ONC will support advances in interoperability throughout the entire health IT community by conducting research and analysis, as well as maintaining the Interoperability Standards Advisory. Further, ONC will support Cures Act requirements in Section 4003 that require the Health IT Advisory Committee to identify priority use cases for health IT and the standards and implementation specifications available to support such use cases. Through this work, ONC seeks to ensure that technical developments are aligned with, and connected to, the business and regulatory drivers of health care and vice versa. In FY 2019, ONC’s standards coordination will include a focus on application programming interface (API) standards in order to improve the specificity, implementation, and use of APIs. This will include working with industry on clinical data standardization, as well as on the security standards necessary to enable patient- and provider-facing applications and services to innovate in a competitive marketplace. Similarly, staff will provide coordination and technical expertise within HHS associated with the development and implementation of policies focused on Section 4001 of Cures Act and provider burden reduction.
6 The FY 2018 Budget consolidates AHRQ's activities within the National Institutes of Health (NIH).

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 33
Certification Funding will support the ongoing maintenance of standards conformance test tools, ONC Health IT Certification Program administration and oversight, and the ongoing support of the Certified Health IT Product List (CHPL), which provides detailed information on each certified product and open data access on each product. Resources will also be allocated to support new testing, certification, and surveillance requirements, and to the CHPL modifications that are necessary to implement the Cures Act. In coordination with NIST, ONC will maintain the testing tools necessary for certification and work with the industry to coordinate the development of test methods to ensure products conform to the technical standards. The program will continue its oversight responsibilities, and look to improve its overall surveillance of certified products for ongoing adherence to technical, security, and regulatory requirements for interoperability, as well as any potential for information blocking. As part of Section 4002 of the Cures Act, the Secretary must establish and administer new “conditions of certification” requirements for health IT developers, in order to address a broad range of topics, including deterring unreasonable business practices that interfere with the exchange of health information or prevent providers from reporting or discussing issues with their technology; requiring real-world testing of certified technologies; and requiring the publication of APIs to promote interoperability of existing technologies and enable new and innovative solutions. In FY 2019, ONC will support a limited implementation of this provision through staff activities focused on: • Developing and publishing regulatory, guidance, and educational materials; and • Incorporating public input in the ongoing development of maintenance of certification health IT
policies, through request(s) for public comment, convening federal advisory committee workgroup(s), and facilitating intra- and inter-agency meetings to develop policy priorities, options, and decisions (consistent with applicable law).
Public-Private Testing ONC will continue to engage with industry through public-private partnerships to enhance existing interoperability testing tools and encourage greater industry-driven testing to advance nationwide interoperability. ONC will continue to support, through the Standards Implementation and Testing Environment (SITE), an open testing environment that allows health IT developers and the provider community to verify that their systems have implemented interoperability standards in a consistent manner. Federal Health Architecture The Federal Health Architecture (FHA) will sunset by the end of FY 2019. ONC will continue to serve as the program manager for FHA on behalf of HHS by continuing to provide staff support for the management and oversight of FHA while the projects close out. A select number of projects will continue to be transitioned throughout FY 2019 to be run by federal agencies such as the Department of Defense, or through public-private partnerships. ONC will continue coordinating with other federal agencies and Departments such as the Department of Veterans Affairs and the Department of Defense, through the Federal Health IT Coordinating Council. Scientific Innovation ONC is identified by the Cures Act as a leading agency for advancing interoperability to reduce barriers to scientific innovation. ONC’s Chief Scientist partners with the NIH, FDA and others to implement scientific initiatives of national importance. In FY 2019, ONC will continue to coordinate with the public and private sectors to develop health IT policy and standards that advance interoperability in the service of biomedical and health services research.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 34
Agency-Wide Support In FY 2019, ONC will continue the cost reductions included in the FY 2018 President’s Budget related to information technology, staff training, and agency travel. ONC will continue to seek further reductions in these costs through negotiations with ONC’s HHS partners and service providers. The FY 2019 Budget also moves Performance Management, and Engagement and Outreach activities to Agency Wide Support. ONC’s FY 2019 request continues to fund the shared services required by HHS for ONC to operate, including financial and grants management systems, as well as contract management fees and costs related to ONC’s space in HHS’s Southwest Complex.

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 35
SUPPORTING EXHIBITS Budget Authority By Object Class - Program Level
(Dollars in Thousands)
Object Class Code Description FY 2017
Final
FY 2018 Annualized
CR
FY 2019 President's
Budget
FY 2019
+/- FY 2018
11.1 Full-time permanent 18,532 17,899 17,984 -85
11.3 Other than full-time permanent 2,255 1,519 1,526 -7
11.5 Other personnel compensation 573 554 557 -3
11.7 Military personnel 318 322 329 -7
Subtotal Personnel Compensation 21,678 20,294 20,396 -102 12.1 Civilian personnel benefits 6,600 5,161 5,186 -25
12.2 Military benefits 126 126 129 -3
13 Benefits for former personnel 0 0 0 0
Total Pay Costs 28,404 25,581 25,710 -129 21 Travel and transportation of persons 382 191 191 0
22 Transportation of things 2 2 2 0
23.1 Rental payments to GSA 3,784 2,268 2,160 -108
23.3 Communications, utilities, and misc. charges 588 411 411 0
24 Printing and reproduction 131 125 125 0
25.1 Advisory and assistance services 585 100 100 0
25.2 Other services from non-Federal sources 12,152 14,635 4,100 -10,535
25.3 Other goods and services from Federal sources 11,697 15,873 4,811 -11,062
25.4 Operation and maintenance of facilities 254 191 191 0
25.5 Research and development contracts 0 0 0 0
25.6 Medical care 45 0 0 0
25.7 Operation and maintenance of equipment 15 8 8 0
25.8 Subsistence and support of persons 536 268 268 0
Subtotal Other Contractual Services 30,171 34,072 12,367 -21,705 26 Supplies and materials 275 192 192 0
31 Equipment 177 112 112 0
32 Land and Structures 0 0 0 0
41 Grants, subsidies, and contributions 1,200 0 0 0
42 Insurance claims and indemnities 0 0 0 0
44 Refunds 0 0 0 0
Total Non-Pay Costs 1,652 304 304 0
Total Total Budget Authority by Object Class 60,227 59,957 38,381 -21,576

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 36
Salary & Expenses (Dollars in Thousands)
Object Class Code FY 2017
Final
FY 2018 Annualized
CR
FY 2019 President's
Budget
FY 2019 +/- FY 2018
11.1 Full-time permanent 18,532 17,899 17,984 -85
11.3 Other than full-time permanent 2,255 1,519 1,526 -7
11.5 Other personnel compensation 573 554 557 -3
11.7 Military personnel 318 322 329 -7
Subtotal Personnel Compensation 21,678 20,294 20,396 -102 12.1 Civilian personnel benefits 6,600 5,161 5,263 -102
12.2 Military benefits 126 126 129 -2
13 Benefits for former personnel 0 0 0 0
Total Pay Costs 28,404 25,581 25,787 -206 21 Travel and transportation of persons 382 191 191 0
22 Transportation of things 2 2 2 0
23.3 Communications, utilities, and misc. charges
588 411 411 0
24 Printing and reproduction 131 125 125 0
25.1 Advisory and assistance services 585 100 100 0
25.2 Other services from non-Federal sources
12,152 14,635 4,100 -10,535
25.3 Other goods and services from Federal sources
11,697 15,873 4,811 -11,062
25.4 Operation and maintenance of facilities
254 191 191 0
25.5 Research and development contracts 0 0 0 0
25.6 Medical care 45 0 0 0
25.7 Operation and maintenance of equipment
15 8 8 0
25.8 Subsistence and support of persons 536 268 268 0
Subtotal Other Contractual Services 26,387 31,804 10,207 -21,597 26 Supplies and materials 275 192 192 0
Subtotal Non-Pay Costs 275 192 192 0 Total Salary and Expenses 55,066 57,577 36,186 -21,391 23.1 Rental payments to GSA 3,784 2,268 2,160 -108
Total Salaries, Expenses, and Rent 58,850 59,845 38,346 -21,499
Total Direct FTE 187 164 164 0

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 37
Detail Of Full-Time Equivalent (FTE) Employment
Average GS Grade
Grade: Step: FY 2015................................ 13 8 FY 2016................................ 13 8 FY 2017................................ 13 9 FY 2018................................ 13 9 FY 2019................................ 13 9
Detail FY 2017 Civilian
FY 2017 Military
FY 2017 Total
FY 2018 Civilian
FY 2018 Military
FY 2018 Total
FY 2019 Civilian
FY 2019 Military
FY 2019 Total
Direct 185 2 187 162 2 164 162 2 164
Reimbursable
Total FTE 185 2 187 162 2 164 162 2 164

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 38
Detail Of Positions
Detail FY 2017 FY 2018 FY 2019
Final Annualized CR President’s Budget
Executive level 0 0 0
Total - Exec. Level Salaries 0 0 0
SES 8 8 8
Total - SES Salaries 1,253,958 1,783,179 1,790,312
Total - ES Salary 1,253,958 1,783,179 1,790,312
GS-15 57 45 45
GS-14 58 51 51
GS-13 45 38 38
GS-12 18 12 12
GS-11 12 8 8
GS-10
GS-9 9 2 2
GS-8 1 1
GS-7 1
GS-6
GS-5
GS-4 1 1 1
GS-3
GS-2
GS-1
Subtotal 209 166 166
Total, GS Salary 20,624,483 18,188,507 18,195,782
Commissioned Corps 2 2 2
Total, Commissioned Corps Salary
318,302 322,314 329,083
Total Positions 211 168 168
Total FTE 187 164 164

OFFICE OF THE NATIONAL COORDINATOR FOR HEALTH IT
Page 39
Physicians’ Comparability Allowance
In 2017, ONC needed physicians with prominent medical backgrounds to engage with a wide variety of clinical stakeholders and to provide a clinically based perspective on ONC policies and activities. This includes clinical issues around EHR safety, usability, clinical decision support, and quality measures. Without PCA, it is unlikely that ONC could have recruited its current physicians, nor is it likely that ONC will be able to recruit without PCAs in future years. PCAs were awarded at the maximum amount allowed in all of these cases.
FY 2017 (Actual)
FY 2018 FY 2019 (Estimates) (Estimates)
1) Number of Physicians Receiving PCAs 4 3 3
2) Number of Physicians with One-Year PCA Agreements 0 0 0
3) Number of Physicians with Multi-Year PCA Agreements 4 3 3
4) Average Annual PCA Physician Pay (without PCA payment) $134,226 $136,273 $136,273
5) Average Annual PCA Payment $23,444 $19,000 $19,000
6) Number of Physicians Receiving PCAs by Category
(non-add)
Category I Clinical Position 0 0 0
Category II Research Position 0 0 0
Category III Occupational Health 0 0 0
Category IV-A Disability Evaluation 0 0 0
Category IV-B Health and Medical Admin. 4 3 3

Health Insurance and Implementation Fund

Page 1
HEALTH INSURANCE REFORM IMPLEMENTATION FUND Budget Summary (Dollars in Thousands)
FY2017 FY2018 FY2019
Obligations* ‐$591 $5,669 0
* $1,000,000,000 was appropriated in the Health Care and Education Reconciliation Act of 2010
Authorizing Legislation.………….……………………….Health Care and Education Reconciliation Act, Section 1005, FY 2010 FY 2018 Authorization……………….………………………………………………..........…..………….………………….….……......……Indefinite Allocation Method…………………………………………………………….……………………………..Direct Federal, Competitive Contract
Program Description and Accomplishments
Section 1005 of the Health Care and Education Reconciliation Act of 2010 (P.L. 111‐152) appropriated
$1,000,000,000 to the Health Insurance Implementation Fund within the Department of Health and
Human Services (HHS). The Fund was used for Federal administrative expenses necessary to carry out
the mandates of the Patient Protection and Affordable Care Act of 2010 (P.L. 111‐148) and the Health
Care and Education Reconciliation Act of 2010.
HHS used implementation funds to primarily support salaries, benefits, contracts, and infrastructure for
various provisions, including rate review and medical loss ratio. A portion of these funds also supported
the establishment of the Exchanges, including the building of IT systems.
The Department of Treasury required funding to implement multiple tax changes, including the Small
Business Tax Credit, expanded adoption credit, W‐2 changes for loan forgiveness, charitable hospital
requirements, and planning for Exchanges. The Department of Labor required funds to conduct
compliance assistance; modify or develop IT systems that support data collection, reporting, policy and
research; and develop infrastructure for the newly required Multiple Entity Welfare Arrangements
reporting and registration within Obamacare.
The Office of Personnel Management (OPM) required funding to plan for implementing and overseeing
Multi‐State Plan Options for the Exchanges and allowing Tribes and Tribal organization to purchase
Federal health and life insurance for their employees. OPM also assisted HHS by implementing an
interim Federal external appeals process prior to the establishment of a permanent Federal appeals
process.
Budget Request
In FY 2017, a net $591,510 of this funding was deobligated by agencies within HHS and external federal
partners. In FY 2018, HHS estimates that the small amount of remaining funds will be obligated. It is the
Department’s current projection that no remaining funds from this account will be available for
obligation in FY 2019.

Nonrecurring Expenses Fund

Nonrecurring Expenses Fund
Page 1
Nonrecurring Expenses Fund Budget Summary (Dollars in Thousands)
FY 20172 FY 20183 FY 2019
Notification1 $430,000 TBD TBD
Authorizing Legislation:
Authorization……………….…………….Section 223 of Division G of the Consolidated Appropriations Act, 2008 Allocation Method…………………………………………………………….……………..Direct Federal, Competitive Contract
Program Description and Accomplishments The Nonrecurring Expenses Fund (NEF) permits HHS to transfer unobligated balances of expired discretionary funds from FY 2008 and subsequent years into the NEF account. Congress authorized use of the funds for capital acquisitions necessary for the operation of the Department, specifically information technology (IT) and facilities infrastructure acquisitions.
In FY 2017, HHS allocated funds to support the decommissioning and new construction of the NIH E‐Wing in Rockville, Maryland. The E‐Wing project will provide new research laboratory space, replace existing laboratories in adjoining wings, and replace a vital clinical program now functioning in a deficient space. HHS also allocated NEF funds to invest in facilities and equipment for the Indian Health Service (IHS). IHS used these funds to enhance their capacity to provide effective and seamless health care by starting construction at two health centers and continuing construction at numerous other medical facilities.
Additionally in FY 2017, HHS invested in Department‐wide IT systems updates related to cybersecurity enhancements, Digital Accountability and Transparency Act compliance, and financial system upgrades. HHS also allocated funds to the Centers for Medicare & Medicaid Services to develop systems needed to effectively implement several provisions in the Medicare Access and CHIP Reauthorization Act, including system changes needed to remove Social Security numbers from Medicare cards.
Budget Allocation
In FY 2018, HHS will continue to use the Fund to obligate funds for previously notified information technology and facility infrastructure projects across the Department over time, as expired funds become available to the Fund. Specifically, HHS will use available funds to support a CDC facility consolidation project for National Institute for Occupational Saferty and Health (NIOSH), IHS facilities, and to continue IT and Cybersecurity investments across the Department. In FY 2019, the amount allocated will depend on total resources available and the infrastructure needs of HHS. HHS will notify Congress before obligating funds towards projects, consistent with prior year notifications. 1 Pursuant to Section 223 of Division G of the Consolidated Appropriation Act, 2008, notification is required of planned use.
2 Notification submitted to the Committees on Appropriations in the House of Representatives and the Senate on January 4, 2017.
3 HHS has not yet notified for FY 2018.

Service and Supply Fund

1
Service and Supply Fund Table of Contents SERVICE AND SUPPLY FUND ......................................................................................................................... 3
Statement of the Budget .............................................................................................................................. 3
Service and Supply Fund Overview and Activity Narratives ......................................................................... 3
Program Support Center ............................................................................................................................... 4
PSC Financial Management Portfolio (FMP): ............................................................................................ 4
PSC Occupational Health Portfolio (FOH): ................................................................................................ 4
PSC Real Estate, Logistics and Operations Portfolio (RLO): ...................................................................... 5
Non‐PSC Activities ......................................................................................................................................... 8
Office of the Assistant Secretary for Administration (ASA) .......................................................................... 9
Office of Business Management and Transformation (OBMT) ................................................................. 9
High Performing Organizations, Commercial Services Management Reporting (HPO&CSM): ............ 9
Office of the Chief Information Officer (OCIO) ......................................................................................... 9
Office of Enterprise Application and Development (OEAD): ................................................................ 9
Office of Information Security (OIS): ................................................................................................... 10
Office of Information Technology Infrastructure Operations (ITIO): .................................................. 10
Office of Information Technology Strategy, Policy and Governance (OSPG) (includes Departmental
IT Management and E‐Gov Initiatives): .............................................................................................. 10
EEO Compliance and Operations Division (EEOCO): ............................................................................... 11
Office of the Assistant Secretary for Human Resources (OHR) .............................................................. 11
Office of Human Resources (OHR): ..................................................................................................... 11
Office of the Assistant Secretary for Financial Resources (ASFR) ............................................................... 11
Office of the Deputy Assistant Secretary of Finance .............................................................................. 11
Office of Program Audit Coordination (OPAC) (formerly Audit Resolution): ..................................... 12
Unified Financial Management Systems (UFMS): ............................................................................... 12
Office of the Deputy Assistant Secretary of Grants and Acquisition Policy and Accountability ............. 12
Acquisition Integration and Modernization (AIM): ............................................................................. 12
Category Management (CM): ............................................................................................................. 12
Departmental Contracts Information System (DCIS): ......................................................................... 13
2
Grants.gov: .......................................................................................................................................... 13
HHS Consolidated Acquisition Solution (HCAS): ................................................................................. 13
Office of Small and Disadvantaged Business Utilization (OSDBU): ..................................................... 13
Tracking Accountability in Government Grants System (TAGGS): ...................................................... 14
Office of the Assistant Secretary for Public Affairs (ASPA) ......................................................................... 14
Digital Communications Division (DCD): ................................................................................................. 14
Freedom of Information Act (FOIA): ....................................................................................................... 14
HHS Broadcast Studio: ............................................................................................................................ 15
Media Monitoring and Analysis: ............................................................................................................. 15
Office of the Assistant Secretary for Planning and Evaluation (ASPE) ........................................................ 15
Strategic Planning System (SPS): ............................................................................................................. 15
Office of the General Council (OGC) ........................................................................................................... 15
Departmental Ethics Program: ................................................................................................................ 15
Office of the General Council (OGC) Claims: ........................................................................................... 16
Agency for Children and Families (ACF) ...................................................................................................... 16
GrantSolution Center of Excellence: ....................................................................................................... 16
All Purpose Table (APT) ............................................................................................................................... 17
Object Classification Table – Reimbursable Obligations ............................................................................. 18
Service and Supply Fund Organizational Chart ........................................................................................... 19

3
SERVICE AND SUPPLY FUND (Dollars in Thousands)
SSF
FY17 Actuals
FY 2018
FY 2019
FY 2019 +/‐
FY 2018
BA $1,616,960 $1,849,094 $1,802,734 ‐$46,360
FTE 1,001 1,001 1,001 0
Authorizing Legislation…………………………………………………………………………………………………………..42 USC §231 2019 Authorization…………………………………………………………………………………………………………..…..……Indefinite Allocation Method ……………………………………………………………………………………………………………Contract, Other
Statement of the Budget
The overall FY 2019 estimate for the Service and Supply Fund (SSF) is $1,802,734, which reflects a decrease of $46,360 below FY 2018. The Program Support Center’s (PSC) FY 2019 estimate of $1,353,438 represents a decrease of $41,844 below the FY 2018 level of $1,395,282. The total FY 2019 request for the non‐PSC SSF Activities is $449,438 which is a decrease of $4,374 below the FY 2018 level of $453,812. Service and Supply Fund Overview and Activity Narratives This section describes the activities funded through the HHS’ Service and Supply Fund (SSF), which is a revolving fund authorized under 42 USC §231. The SSF provides consolidated financing and accounting for business‐type operations which involve the provision of common services to customers. The SSF is governed by a Board of Directors, consisting of representatives from each of the Department’s ten Operating Divisions (OPDIV), the PSC and the Office of the Secretary. A representative from the Office of Inspector General (OIG) serves as a non‐voting member of the SSF Board. The SSF does not have its own annual appropriation but is funded entirely through charges to its customers for their usage of goods and services. The SSF is comprised of two categories of activities: the Program Support Center and those activities which are performed by other components (Non‐PSC). Each activity financed through the SSF is billed to the Fund’s customers by either fee‐for‐service billing, which is based upon actual service usage, by an allocated methodology, or by agreement with the customer. Details of the FY 2019 SSF activities are described in the remainder of the narrative.

4
Program Support Center
The Program Support Center (PSC) organizationally resides under the Assistant Secretary for Administration, Office of the Secretary and operates under authorizing legislation 42 USC §231 as amended. The PSC is committed to providing the best value in terms of cost and service quality to its customers. In a proactive effort to contain costs, the PSC again deployed its SMART (Save, Manage and Assess our Resources Together) Program for the FY 2018/2019 budget formulation process. This comprehensive, “bottom‐up, zero‐based budget” review of PSC’s operations continues to identify areas for additional cost reductions, efficiencies, and cost avoidance. PSC tracks performance in terms of its strategic goals. These goals focus primarily on delivering products and services that are recognized both as high quality, and as providing value. The organization strives to achieve three primary outcomes: higher service quality, lower operating costs and reduced rates for customers. By working to reach these outcomes, PSC supports the Department’s efforts for responsible stewardship and effective management. Details are outlined in the performance review section.
PSC Financial Management Portfolio (FMP):
The PSC Financial Management and Procurement Portfolio (FMP) serves as a major foundation of the Department’s finance, accounting, and procurement operations through: the administration of grant payment management services; accounting and fiscal services; debt management services; rate review/negotiation/approval services; and fully integrated acquisition and strategic support services. FMP provides these services on behalf of the Department and other Federal agencies. Fiscal and technical guidance is offered to assist in implementing new initiatives across HHS and other agencies and to ensure compliance with regulatory requirements. FMP also provides guidance and oversight for HHS Financial Policy, and ensures compliance where appropriate. FMP continues to be a leader in supporting the Department’s clean audit opinions from independent audit firms. FMP services are organized into three Service Areas:
Accounting Services – covers a range of financial support services associated with Unified Financial Management System (UFMS) and includes accounting, debt collection and financial reporting.
Acquisitions Management Services (AMS) – offers a range of acquisition support services including simplified and negotiated contracts.
Grants Finance and Administration Services – provides federal grant funding support, negotiating indirect costs for grant providers and issuing grant payments to grantees.
PSC Occupational Health Portfolio (FOH): The Federal Occupational Health (FOH) provides comprehensive, high‐quality, customer‐focused occupational health services in strategic partnership with Federal agencies nation‐wide to improve the health, safety, and productivity of the Federal workforce. Approximately 93% of FOH’s services are provided to Federal agencies outside of HHS. FOH is organized in four Service Areas:

5
Clinical Health Services (CHS) consists of seven cost centers: Exams and Clinical Outreach, FedStrive Advantage, Onsite Occupational Health Centers, Medical Surveillance/Clearance Reviews, Medical Employability and Workers Compensation Management and Psychological Testing which has been moved from Behavioral Health to better align with the Medical Review oversight required. CHS provides services which includes exams and related procedures, health screenings to prevent illness, immunizations for illness prevention and work related activities, reasonable accommodation request, workers compensation management reviews, medical surveillance and clearance required based upon an employee’s job duties and other medical services.
Wellness and Health Promotion Services (WHP) is a single cost center which provides fitness center oversight and health promotion activities, such as health coaching, health education, and promotion of programs to support healthy behaviors which contributes to increased employee productivity through better health behaviors.
Behavioral Health Services (BHS) consists of two cost centers: Employee Assistance Program/Work Life Services and Organizational Development and Leadership. Psychological Testing was part of this service area in FY17 and has been moved to Clinical Health Services for FY18. BHS provides professional services for: assessment, short‐term counseling, referral, and critical incident response. This improves the well‐being of federal employees, and helps employees better manage their personal and professional responsibilities which in turn helps improve productivity.
Environmental Health and Safety Services (EHS) consists of two cost centers Environmental Health and Safety (EHS) and the Automated External Defibrillator (AED) program. EHS offers a wide variety of services including environmental and occupational safety compliance, industrial hygiene assessments, laboratory analysis of environmental samples, urgent response management, and other environmental consulting services. In addition, EHS provides the mandatory policy services to HHS. The AED program helps agencies set up a program within their facility aiding them in the procurement of devices, certification training, and ensuring the appropriate medical oversight is provided.
PSC Real Estate, Logistics and Operations Portfolio (RLO): Real Estate, Logistics and Operations Portfolio (RLO) provides real estate, logistics and a wide range of administrative, technical and security support services to customers within HHS and other federal agencies; RLO also provides policy guidance to HHS entities. In order to gain efficiencies and improvements in organizational performance, ASA/PSC merged two of PSC’s operating portfolios, Administrative Operations Portfolio (AOP), and Real Estate and Logistics Portfolio (REL), into a single Real Estate and Logistics Portfolio (RLO) portfolio. Additionally, all but a small component of the SSF functions of the Office of Security and Strategic Intelligence (OSSI) were transferred to RLO to better align with related services such as Building Operations. The only function not included in this transfer was a small component associated with Personnel Security functions concerning National Security Adjudications which was transferred to the Immediate Office of the Secretary, and will continue to be billed through the SSF. Once this integration is complete, it may allow for a reduction in overhead and administrative support costs, resulting in lower rates to our customers.

6
The services associated with each of the merged portfolios will remain intact as proposed in the FY 2018 Budget Request, and will be executed accordingly. Cost Centers and budgets will remain intact, apart from a minor change in Personnel Security as explained above. The resulting cost structure will be budget‐neutral compared with the originally submitted request for FY 2018. The new RLO Portfolio includes:
Badging Operations – Provision of HSPD‐12 Badges associated with the issuance of a new or
replacement Personal Identity Verification (PIV) and related smartcards. This service also
provides Non‐HSPD‐12 Badges that does not contain an electronic chip.
Building Operations Services – facilities operations, maintenance, shredding, parking service,
regional support services and conference room services
FedResponse Services – Customer Contact Center, and the HHS Toll Free Hotline;
HSPD‐12 – HSPD‐12 / Identity, Credential, and Access Management (ICAM) Program is the
Departmental program focused on meeting Federal requirements to enable the right individual
to access the right resource at the right time for the right reason
Mail and Publishing Services – digital conversion services, printing procurement, Departmental
Forms Management, HHS Printing Policy, mail screening, mail operations, and HHS Mail Policy
ORR / DCS (Unaccompanied Children) – Provides security support to the ACF Division of
Children’s Services (DCS) program that provides a safe and appropriate environment for
unaccompanied children, from the time they are placed into Office of Refugee Resettlement
custody until they are reunified with family members or sponsors in the U.S., or returned to
their country of origin by Department of Homeland Security immigration officials
Board for Corrections – manages and conducts the appeals process for U.S. Public Health
Service Commissioned Corps Officers who believe there is an error or injustice in their personnel
records
Personnel Security – Responsible for developing and implementing policies and procedures to
ensure effective, efficient, and timely completion of adjudications for suitability security and
HSPD‐12 eligibility
Physical Security – 560, HHH, Outbuildings and Switzer – Provides services for the tenants of
these buildings. Services include: physical security programmatic support, Facility Security
Planning, Assessments, operations, guard force management, and emergency management
Real Property Management Services – Space design planning, utilization and compliance,
management for transfer of surplus real property to non‐profit entities (McKinney‐Vento
Homeless Assistance Act), and real property oversight/policy development
Supply Chain Management Services – personal property management, warehousing,
distribution, medical supply fulfillment, publication fulfillment, personal property disposal and
labor services
Transportation Services – Transit subsidy program management, executive drivers, travel policy,
travel program management, travel charge card management, purchase card management,
fleet card management, fleet policy, vehicle leasing services.

7
PSC/RLO now provides HHS components with a wide range of critical security services that are funded
under the SSF.
Badging Operations
The PSC/RLO Badging Operations business line includes two Card Provisioning services:
Card Provisioning ‐ PIV is a one‐time cost associated with the issuance of a new or replacement
PIV and related smartcards Alternate Logon Tokens (ALT) issued to staff with two network
accounts or those requiring elevated network privileges, which contain an electronic chip. Cards
are issued to new staff (federal staff, contractors, and affiliates) for a period up to six years
unless replaced sooner, due to a change in organization, name, change lost card, or other
significant demographic.
Card Provisioning ‐ Non‐PIV is a one‐time cost associated with the issuance of a new or
replacement identity card. This card does not contain an electronic chip and does not allow for
logical and physical binding of other government issued HSPD‐12 PIV cards to the Health and
Human Services (HHS)/Office of the Secretary (OS) system. These cards are issued to individuals
who are most often visitors that are not HHS staff that only require physical access to HHS
facilities.
HSPD‐12 System
The HSPD‐12 PMO leads the Department's implementation of strong authentication, including the
required use of the Personal Identity Verification (PIV) card and other solutions to access HHS networks
and systems. The continued implementation of Homeland Security Presidential Directive (HSPD)‐12 /
Identity, Credential, and Access Management (ICAM) Program is the security discipline that allows HHS
to enable the right individual to access the right resource at the right time for the right reason. ICAM
encompasses the tools, policies, and systems to manage, monitor, and secure access to protect
resources. These resources may include: electronic files, computer systems, or physical resources such
as server rooms and buildings.
Personnel Security
PSC/RLO is responsible for ensuring that HHS meets timeliness goals for the initiation and adjudication
phases of the personnel security clearance process as prescribed in the Intelligence Reform and
Terrorism Prevention Act of 2004 (IRTPA).
The Background Investigations Cost Center provides customer agencies with support in processing
suitability investigations for federal employees, Commissioned Corps officers and contractors.
Support for Administration for Children and Families, Office of Refugee Resettlement, Division of
Children’s Services
The PSC/RLO Division of Children’s Services (DCS) program recognizes the importance of providing a safe
and appropriate environment for unaccompanied children, from the time they are placed into Office of
Refugee Resettlement (ORR) custody until they are reunified with family members or sponsors in the
U.S., or returned to their country of origin by D DHS immigration officials. PSC/RLO is responsible for
facilitating background investigations which include Special Agency Checks (SACs)/FBI National Criminal

8
History Check, Child Abuse and Neglect Checks, and Central Indexing System/D DHS Immigration Status
Checks on potential sponsors seeking custody of the unaccompanied child. PSC/RLO also provides other
support for ACF/ORR as part of its reunification program to unite unaccompanied children with families
and sponsors.
Physical Security: 5600, HHH, Switzer and Other
Physical Security and Emergency Management at 5600 Fishers Lane provides physical security services
for the tenants that include: physical security programmatic support, facility security planning,
assessments, operations, guard force management, and emergency management. PSC/RLO manages
the contract for contractor security guard personnel to control access for employees, visitors, deliveries
and contractors performing construction at 5600 Fishers Lane. Funds also provide for operations and
maintenance to the physical access control system (PACS) at 5600 Fishers Lane, and for security
equipment (i.e., video cameras, alarms, security command center displays, etc.) that are installed.
The primary mission of the Office of Security and Strategic Information (PSC/RLO) Physical Security and
Emergency Management Hubert H. Humphrey (HHH) building is to provide physical security services for
the OS and those OpDivs that reside within the facility. These services include, but are not limited to,
physical security program management, facility security planning, assessments, operations, guard force
management, and emergency management. Funds also provide for operations and maintenance to the
PACS infrastructure within the South West (SW) Complex, and for security equipment (i.e., video
cameras, alarms, security command center displays, etc.) that are installed.
Physical Security and Emergency Management, Switzer provides physical security programmatic support
including: facility security planning, assessments, operations, emergency management and deployment
of the PACS security services for the tenants of the Mary E. Switzer building. PSC/RLO provides for
operations and maintenance of the PACS, and for security equipment (i.e., video cameras, alarms,
security command center displays, etc.) that are installed at the Mary E. Switzer building.
Physical Security (Other) provides guard services to the Federal Drug Administration (FDA) via a pass
through arrangement. Additional security services include the provision of Physical Access Control
Systems (PACS) and associated services to facilities that will be charged on the basis of Rentable Square
Footage (RSF). Design services and physical security guidance is provided throughout these security
installation.
Non‐PSC Activities The non‐PSC activities support all components of HHS, providing support in areas such as acquisitions management, audit resolution, responding to and processing Federal tort claims, collecting and managing grants data to ensure HHS’ ability to respond to regulatory requirements, providing human resources and equal employment opportunity services, and providing IT support and devices.

9
Office of the Assistant Secretary for Administration (ASA) ASA provides leadership for HHS Departmental administration, including human resource policy, information technology, and departmental operations. Office of Business Management and Transformation (OBMT) OBMT supports the HHS mission by identifying, developing, implementing, and evaluating efficient and effective business practices throughout the Department. OBMT acts as an internal consulting group to other parts of HHS, maximizing return on taxpayer dollars by undertaking initiatives to improve services, reduce costs, and streamline bureaucracy. Its projects are often team‐based and cross‐functional in ways that include staff from supported organizations. High Performing Organizations, Commercial Services Management Reporting (HPO&CSM): OBMT High Performing Organizations, Commercial Services Management Reporting & Insourcing supports HHS‐wide Commercial Services Management reporting (CSM), the inventory and reporting of the Federal Activities Inventory Reform (FAIR) Act inventory, the active sponsorship of High Performing Organizations (HPO), and insourcing through central service activities. Additionally, this program offers organizational redesign services to the Department to promote mission effectiveness, cost‐savings and increase efficiencies. Office of the Chief Information Officer (OCIO) OCIO supports the HHS mission by leading the development and implementation of an enterprise information technology (IT) infrastructure across HHS. The OCIO is responsible for providing a reliable, cost effective, scalable, and flexible enterprise computing platform that supports and enhances customer IT needs and capabilities from requirements gathering through design, development, testing, and implementation. The OCIO is also responsible for the development and implementation of a cybersecurity program which includes the security technologies that provide an enterprise‐wide capability to monitor HHS’ computers and networks for security incidents and attacks through HHS’ secure Internet gateways, intrusion detection systems, network security forensics and analysis, and other enterprise security technologies throughout HHS. In response to the National Security Presidential Directive (NSPD) 54 / Homeland Security Presidential Directive (HSPD) 23, OCIO partners with OPDIVs at HHS to provide the Trusted Internet Connection (TIC) for all of HHS. The OCIO provides information technology services for the development, configuration, and integration of multiple systems for HHS and the Office of the Secretary. In addition, OCIO supports the following activities for HHS: Enterprise Strategy & Governance, Vendor Management, Investment Portfolio Management and Control, and Enterprise Architecture. Office of Enterprise Application and Development (OEAD): OEAD provides information technology services for the design and development, configuration and integration, and application support services for multiple departmental systems for HHS and the Office of the Secretary. In addition, OEAD provides production reporting and business intelligence

10
query/dashboard capabilities for its many customers. The development capabilities provided by OEAD include collaboration and workflow automation technologies that promote the deployment of repeatable business processes in order to achieve customer efficiencies and effectiveness. OEAD’s Integration Services collects and renders data for systems and end‐user consumption and reporting that help to improve decision making across the Department. The support functions provide OEAD customers with cost effective operations and maintenance, systems administration, and database support services that ensure applications and platform availability for secure and continuous business operations. Office of Information Security (OIS): The HHS Office of Information Security (OIS) assures that all automated information systems throughout HHS are designed, operated, and maintained with the appropriate information technology security and privacy data protections. OIS is tasked with implementing a comprehensive, enterprise‐wide cybersecurity program to protect the critical information with which the Department is entrusted. To accomplish this, OIS provides and engages in:
Implementing specific cybersecurity capabilities
Cultivating cybersecurity partnerships in the public and private sectors
Engaging in HHS‐wide security collaboration activities
Providing security services and solutions to the enterprise
Enhancing HHS’ security capabilities through current and future programs and projects
Directly providing cybersecurity and privacy support for the Office of the Secretary (OS) OIS is also tasked with executing the HHS Trusted Internet Connection (TIC.) This program aims to improve the Federal Government’s security posture through the consolidation of external telecommunication connections and establishing a set of baseline security capabilities through enhanced monitoring and situational awareness of all external network connections. Office of Information Technology Infrastructure Operations (ITIO): ITIO is responsible for providing a reliable, cost effective, scalable and flexible enterprise computing platform that supports and enhances customer IT needs and capabilities from requirements gathering through design, development, testing, and implementation. ITIO supports over 22 customer organizations comprised of over 11,000 users, including all HHS Staff Divisions (StaffDivs) and participating Operating Divisions (OpDivs). Office of Information Technology Strategy, Policy and Governance (OSPG) (includes Departmental IT Management and E‐Gov Initiatives): The Office of Strategy, Policy and Governance (OSPG) provides support to the enterprise for: Enterprise Strategy & Governance, Vendor Management, Investment Portfolio Management and Control, and Enterprise Architecture. OSPG is comprised of two services:
The Program and Project Management (P&PM), formerly known as the Departmental IT Management (DITM), includes the following activities: Enterprise Strategy & Governance, Vendor Management, Investment Portfolio Management and Control (which incorporates business integration/center of excellence activities), and Enterprise Architecture. FY 2018

11
allocation methodology is based on Operating (OpDiv) and Staff (StaffDiv) Divisions’ percentage of Total IT amount (excluding grants) from the OMB reported IT Dashboard as of conclusion of the prior [completed] fiscal year.
The E‐Government (E‐Gov) team within OSPG provides a central funding point for OMB‐mandated contributions to Government‐wide E‐Gov initiatives.
EEO Compliance and Operations Division (EEOCO): EEOCO works to promote a discrimination–free work environment focused on serving DHHS by preventing, resolving, and processing EEO discrimination complaints in a timely and high‐quality manner. In compliance with the Civil Rights Act of 1964 as amended, and other federal laws, regulations, directives, and policies prohibiting discrimination and harassment of protected individuals, EEOCO processes EEO complaints for DHHS employees, applicants for employment, and former employees. Complaint processing services include counseling, Alternative Dispute Resolution (ADR), procedural determinations, and investigations. EEOCO also administers the ADR program to manage conflict and prevent and resolve disputes through mediation, conflict coaching, group facilitation, and assessments. Additionally, EEOCO manages the Reasonable Accommodation program for DHHS which is funded through Inter‐Agency Agreements Office of the Assistant Secretary for Human Resources (OHR) The Office of Human Resources (OHR) provides leadership for the development, execution, and management of the human resources program to ensure the Department builds and retains a highly skilled and diverse workforce. In coordination with the Operating Divisions (OPDIVs) OHR provides human resource programs and policies developed to support and enhance the HHS mission. Office of Human Resources (OHR): OHR provides leadership in creating and sustaining a diverse workforce and an environment free of discrimination. OHR works proactively to enhance the employment of women, minorities, veterans, and people with disabilities through efforts that include policy development, program oversight, complaint resolution, diversity outreach, commemorative events, and standardized education and training programs. OHR also provides technical assistance to the HHS OPDIVs to effectively and efficiently accomplish the OPDIV’s mission through improved planning and recruitment of human resources and serves as the Departmental liaison to central management agencies on related matters. In addition, OHR works in collaboration with the various HHS Equal Employment Opportunity offices on conducting Department‐wide program reviews to determine barriers to diversity and inclusion.
Office of the Assistant Secretary for Financial Resources (ASFR)
The Office of the Assistant Secretary for Financial Resources (ASFR) provides advice and guidance to the Secretary on all aspects of budget, financial management, grants and acquisition management, and provides for the direction and implementation of these activities across the Department. Office of the Deputy Assistant Secretary of Finance
The mission of the Office of Finance is to provide financial accountability and enhance program integrity through leadership, oversight, collaboration, and innovation.

12
Office of Program Audit Coordination (OPAC) (formerly Audit Resolution): OPAC includes the Division of Audit Resolution (ARD), the Division of Payment Integrity Improvement (DPII), and the Division of Audit Tracking and Analysis (DATA), under the Office of the Secretary, Assistant Secretary for Financial Resources, Office of Finance. ARD, along with resolution officials in HHS, is required to issue a management decision on single audit findings within a six‐month time frame in accordance with the Office of Management and Budget’s (OMB) Uniform Guidance (2 CFR Part 200). The Single Audit Act, as amended, has been incorporated in the Uniform Guidance. On behalf of the OPDIVs, ARD resolves cross‐cutting single audit findings that affect the awards of multiple OPDIVs. The audit resolution function includes: (1) reviewing findings and the related corrective action plans; (2) issuing management decisions to grantees in reference to audit findings; (3) monitoring grantees’ corrective actions to ensure that these actions are appropriate and timely; (4) providing Departmental leadership and policies; (5) identifying grantees for follow‐up by OPDIVs who have failed to submit their required annual single audit report; and (6) implementing the Department’s Shared Single Audit Resolution Vision to comply with the Uniform Guidance. Unified Financial Management Systems (UFMS): The UFMS environment including the Unified Financial Management Systems, the Consolidated Financial Reporting System (CFRS), the Financial Business Intelligence System (FBIS), and the governance function are under the purview of the DAS OF within the Office of the Assistant Secretary for Financial Resources. The UFMS environment provides the Department a secure, stable platform for effectively processing and tracking its financial and accounting transactions. UFMS is the core accounting system for 10 Operating Divisions and 18 Staff Divisions. UFMS integrates with over 50 program, business, and administrative systems (i.e., mixed systems) to create a secure, reliable, and highly available financial management environment. Office of the Deputy Assistant Secretary of Grants and Acquisition Policy and Accountability
The Office of Grants and Acquisition Policy and Accountability (OGAPA) provides Department‐wide leadership and management in the areas of grants and acquisition management. Acquisition Integration and Modernization (AIM): The AIM Program was created to capture knowledge, create standardization and provide one source for the HHS Acquisition Workforce (HHSAW) to access policies, guidance, and other acquisition tools. The program support the acquisition related mission needs of the Department, providing tools to insure that the acquisition lifecycle processes are efficiently executed and complies with statutory requirements. The AIM program is managed by the Office of Acquisition Policy within the Division of Acquisition. Category Management (CM): CM is a purchasing approach in which spending is organized into common categories and managed strategically. Fortune 500 companies and several governments have adopted category management in the last 20‐30 years because it’s a commercial best practice for buying and selling. In accordance with the Federal Acquisition Regulation (FAR) and further reinforced via the OMB Memorandums 17‐22 and M‐17‐26, to the maximum extent practicable, [HHS] shall use existing contract solutions such as: a) Federal Supply Schedules; b) Government‐wide acquisition contracts; c) multi‐agency contracts; d) and any other procurement instruments intended for use by multiple agencies (e.g. Best‐In‐Class) for common supplies and services. Leveraging these sources: (a) decreases administrative costs; (b)

13
prevents repetitive/ unnecessary contract actions; (c) permits acquisition staff to focus on high‐priority and agency unique procurements/ requirements; and (d) enables agencies to better manage spending through such actions as standardization, participating in volume buying events, and applying best practices. Departmental Contracts Information System (DCIS): The DCIS program supports the acquisition related mission needs of the Department and ultimately assures compliance with various open government and transparency initiatives. The DCIS program is managed by the Office of Acquisition Business Systems within the Division of Acquisition. DCIS provides procurement data collection and reporting capabilities to enable the OPDIVs to comply with requirements under Public Law 93‐400 and FAR Subpart 4.6 regarding the reporting of contract actions to the Federal Procurement Data System (FPDS) and DATA Act. DCIS provides a single system capability within HHS that collects, edits, and stores information on the individual procurement and contracting actions executed by OPDIVs and other offices of HHS totaling more than $24 billion and consisting of more than 88,000 individual actions. In addition, the DCIS program oversees the HHS FedDataCheck program. The FedDataCheck service is offered to all OPDIV/STAFFDIV HCAs to monitor and improve FPDS data. Since implementing FedDataCheck, there has been a 10% improvement in HHS FPDS and USAspending data quality. Grants.gov: The Grants.gov system (www.grants.gov) is the federal government's single site for the public to find and apply for federal discretionary grants. The Grants.gov program manages the Grants.gov system including associated operations, maintenance, enhancement, user support, and stakeholder communications. Grants.gov provides all potential applicant organizations a single website where they can find and apply for over $120 billion worth of grants distributed annually. On the grantor side, Grants.gov empowers smaller agencies with limited resources to improve the reach of their grant programs, and provides larger agencies with the benefit of process standardization, cost savings, and increased visibility. Grants.gov supports 26 federal grant‐making agencies. HHS Consolidated Acquisition Solution (HCAS): HCAS was launched in 2009 and provides consolidated acquisition functionality, capabilities and critical to the contract execution operations for seven of the Department’s ten Contracting Activities. This is a commercial‐off‐the‐shelf software application called “PRISM” which allows end‐users to formulate, administer and distribute contractual documents that comply with the Federal Acquisition Regulation. In addition, HCAS supports OGAPA’s efforts to standardize acquisition end‐to‐end business processes through the launch of Health and Human Services Acquisition Lifecycle Framework (HALF) and the HHS Acquisition Lifecycle – Consolidated Acquisition Management System (HALF‐CAMS) Office of Small and Disadvantaged Business Utilization (OSDBU): OSDBU is the focal point for the Department's policy formulation, implementation, coordination, and management of small business programs. Organizationally, OSDBU is administratively supported by the OGAPA Immediate Office, but reports directly to the Deputy Secretary of HHS. The office ensures that small businesses are given a fair and transparent opportunity to compete for contracts that provide goods and services to HHS; establishes, manages and tracks small business goal achievements; provides technical assistance and small business program training to OPDIV contracting and program officials; and conducts outreach and provides marketing and technical guidance to small businesses on contracting opportunities with HHS.

14
Tracking Accountability in Government Grants System (TAGGS): TAGGS provides a central repository for all HHS financial assistance information and continues to add needed data sets for additional business needs. TAGGS is overseen by the Office of Grants Systems Management within the Division of Grants. The TAGGS system is maintained in a manner that supports: the Open Government Initiative, adherence to federal reporting requirements, and ensures the availability of HHS data for internal and external stakeholders use. TAGGS also adheres to all system requirements set forth by the HHS Office of the Chief Information Officer (OCIO). TAGGS continues to serve as a central data repository for grants business information and reporting of grant award data generated by HHS’s Staff Divisions and Operating Divisions. TAGGS grants data is made available to the public on the TAGGS Website (http://taggs.hhs.gov) and includes the DATA Act requirements. HHS’s grant awards data is submitted to USASpending.gov twice a month. Office of the Assistant Secretary for Public Affairs (ASPA) ASPA serves as the Secretary's principal counsel on public affairs. ASPA conducts national public affairs programs, provides centralized leadership and guidance for public affairs activities within HHS' OPDIVs and regional offices, manages the Department’s digital communications, and administers the Freedom of Information and Privacy Acts (FOIA). The Division leads the planning, development, and implementation of emergency incident communications strategies and activities for the Department. The ASPA reports directly to the HHS Secretary. Digital Communications Division (DCD): DCD leads ASPA’s Digital work. ASPA Digital’s approach is to deliver “instant gratification,” by connecting customers to Agency content quickly and fully, and to demonstrate impact, while also building in the ability to adapt and improve every day. ASPA Digital currently manages HHS.gov, the HHS Intranet, and numerous OS Office websites, as well as multiple topic‐oriented websites that promote Agency and cross‐federal agency work. To reach the public with Agency content DCD uses multiple social media channels and will be working through FY18 to implement two‐way engagement with Department stakeholders. Overall, ASPA Digital manages the tools, content and infrastructure that in 2016 supported 957,866 Twitter followers, 420,705 Facebook followers, 18,845,561 YouTube views, 1,311,393 email subscribers, 30,909,885 unique website visitors, and 69,526,798 website page views.
Freedom of Information Act (FOIA):
The Freedom of Information Act (FOIA) is a federal statute that allows individuals to request access to federal agency records, except to the extent records are claimed as exempt from disclosure under one or more of the nine exemptions of the FOIA. FOIA performs initial requests including identification of responsive records, release and denial determinations for the Program Support Center (PSC), Agency for Healthcare Research and Quality (AHRQ), and all components of the Office of the Assistant Secretary for Health (ASH). FOIA also performs administrative appeals of initial FOIA determinations, reviewing the OPDIV’s denial action to determine consistency with the FOIA, HHS FOIA regulations, and case law, for the eight (8) Public Health Service (PHS) OPDIVs: AHRQ, Centers for Disease Control (CDC)/Agency for Toxic Substances and Disease Registry (ATSDR), Food and Drug Administration (FDA), Health Resources and Services Administration (HRSA), Indian Health Service (IHS), National Institutes of Health (NIH), ASH, and Substance Abuse and Mental Health Services Administration (SAMHSA).

15
HHS Broadcast Studio:
The HHS Broadcast Studio supports the entire Department with video production and AV Services. The services provided to the Department range from multi‐camera studio productions; audio‐visual support in the Humphrey Auditorium, Great Hall and Room 800; video streaming via HHS.gov/live and Facebook Live; satellite media tours; motion graphics and video editing, and delivery to multiple social media platforms and channels. In FY2016 we performed 2,338 unique services for our customers; that is a 73% increase over FY2015 (1,351). Media Monitoring and Analysis:
Media Monitoring and Analysis provides the Secretary, Department, agency leadership and staff with the latest analysis of what the media is reporting about Department‐wide and Agency‐specific priorities, initiatives and programs. This Department‐wide tool has been effective since 2009. The OPDIV‐specific requirements and additional levels of effort are provided through a contract vehicle with Bulletin Intelligence. Office of the Assistant Secretary for Planning and Evaluation (ASPE) The Assistant Secretary for Planning and Evaluation (ASPE) is the principal advisor to the Secretary of the U.S. Department of Health and Human Services on policy development, and is responsible for major activities in policy coordination, legislation development, strategic planning, policy research, evaluation, and economic analysis. Strategic Planning System (SPS):
SPS is a web‐based, password‐protected application that centralizes information about strategic plans that agencies within HHS are implementing. The SPS was built in response to a request from the Deputy Secretary and is supported by a contract managed by ASPE. More than 150 strategic plans are currently included in the SPS. ACF, ACL, AHRQ, ASA, ASFR, ASPR, CDC, CMS, FDA, HRSA, IHS, NIH, OASH, OGA, OGC, OIG, OMHA, ONC, PSC, and SAMHSA currently use the SPS to track implementation of strategic plans to which they contribute. Office of the General Council (OGC) The OGC is the legal team for the Department, providing quality representation and legal advice on a wide range of highly visible national issues. OGC supports the development and implementation of the Department's programs by providing the highest quality legal services to the Secretary of HHS and the organization's various agencies and divisions. Departmental Ethics Program: The Departmental Ethics Program was established in 2004, pursuant to 5 C.F.R. § 2638.202(a) and Executive Order 12731, § 301(e), to ensure that operating and staff divisions’ decision‐making is untainted by improper bias or the influence of special interests. The Ethics Division provides ethics advice, it administers the financial disclosure program, and it ensures lobbying activities comply with the applicable rules. Its goals include strengthening grant and procurement integrity; ensuring human subject protections; enhancing public confidence in health science research and drug approval and monitoring; and inviting acceptance of healthcare reform because policy determinations–ranging from coverage and financing decisions to health information technology improvements–are made by

16
administrators and regulators free of financial and personal conflicts and affiliations that would otherwise lead reasonable persons to question their impartiality. Office of the General Council (OGC) Claims: OGC Claims receives all tort claims filed against the Department. These torts can range from “slips” and “falls” in Departmental facilities, to motor vehicle accidents involving Departmental vehicles, or medical malpractice in health clinics. OGC reviews and processes all of these claims. Two clients typically account for approximately ninety‐six percent of the Claims Activity workload: the Health Resources and Services Administration (83%) and the Indian Health Service (13%). There are approximately 1,200 communities served under the health center program, increasing the number of patients served from 10.3 million in 2001 to more than 24 million in 2015. Currently, 13,209 free clinic health professionals and staff are covered under Federal Tort Claims Act (FTCA), and employed in 221 free clinics. The first FTCA claim under this program was received in FY 2008 and more will follow reflecting significant increases in both free clinic and health center program claims. The most recent data is that approximately 190,000 health community center employees (officers, contractors, and other staff) are covered by the FTCA. Agency for Children and Families (ACF) ACF promotes the economic and social well‐being of children, families, individuals and communities with leadership and resources for compassionate, effective delivery of human services. GrantSolution Center of Excellence: GrantSolutions (GS), a Center of Excellence, is a partnership between the HHS and a number of cabinet level and independent agencies. The President’s budget for FY 2007 codified GrantSolutions as one of three shared service providers for the grants management line of business e‐gov initiative. GS is responsible for awarding, monitoring, and financially reporting on grants to states, tribes, territories, and other non‐profit organizations. In FY 2016, GS supported 32,432 grants, processed 75,829 award actions (a 10.7% increase over FY 2015), and net obligated a total of $78.41 billion across more than 1500 programs.

17
Service and Supply Fund All Purpose Table (APT)
(Dollars in Thousands)
Service and Supply Fund Activities FY 2017 Actuals
FY 2018
FY 2019
PSC
Financial Management/Procurement Portfolio 758,380 840,282 856,132
Occupational Health Portfolio 157,655 189,432 192,917
Real Estate, Logistics and Operations Portfolio 250,218 303,817 304,388
Unfilled Customer Orders 48,092 54,820
PSC Annual Leave Liability 3,554 5,160
PSC Reserves 3,032 1,770 ‐
PSC Subtotal 1,220,931 1,395,282 1,353,438
Non‐PSC
AIM 862 992 992
Category Management 617 959 959
CCFM 24,152 27,801 27,601
DCIS 1,832 1,767 1,767
Departmental Ethics Program 3,438 4,312 4,380
DITM (Includes E‐Gov Initiatives) 17,031 17,571 17,571
Digital Communications 18,413 28,933 28,933
EEO Services 3,203 5,130 4,883
Freedom of Information Act 794 1,193 1,193
Grants.gov 5,595 6,194 6,316
Grants Solutions Center of Excellence 50,463 54,990 55,562
HCAS 7,258 7,671 7,671
HHS Broadcast Studio 2 1,920 2,131 2,131
HPO & Commercial Services Mgmt 181 262 262
ITIO 99,006 93,358 93,358
Media Monitoring and Analysis 821 1,017 1,017
OEAD 27,535 30,127 30,127
OGC Claims 1,393 1,565 1,590
OHR 42,569 54,365 54,365
OIS 23,482 29,713 29,713
OPAC 2,186 3,234 3,247
OSSI 1,100 1,364 1,364
Small Business Consolidation 2,670 3,359 3,438
Strategic Planning System 338 525 525
TAGGS 3,423 3,760 4,110
UFMS 45,362 46,534 66,221
Non‐PSC Annual Leave Liability 5,318 5,655
Non‐PSC Reserves 5,067 19,332 ‐
Non‐PSC Subtotal 396,029 453,812 449,296
Total SSF Revenue 1,616,960 1,849,094 1,802,734

18
Service and Supply
Object Classification Table – Reimbursable Obligations (Dollars in Thousands)
Object Class FY 2017 Actuals
FY 2018
FY 2019
Reimbursable Obligations Personnel Compensation: Full – Time Permanent (11.1) 93,434 104,324 105,206 Other Than Full – Time Permanent (11.3) 3,713 5,335 3,573 Other Personnel Compensation (11.5) 2,856 2,603 2,632 Military Personnel (11.7) 6,444 6,913 6,997 Special Personnel Services Payments (11.8) 8,758 8,597 9,856 Subtotal, Personnel Compensation 115,206 127,772 128,264 Civilian Personnel Benefits (12.1) 30,651 33,338 34,465 Military Personnel Benefits (12.2) 3,194 2,496 2,526 Benefits to Former Personnel (13.0) 135 509 517 Subtotal, Pay Costs 149,185 164,116 165,771 Travel (21.0) 1,565 2,049 2,074 Transportation of Things (22.0) 2,043 4,592 4,662 Rental Payments to GSA (23.1) 19,440 20,445 20,651 Rental Payments to Others (23.2) ‐ ‐ ‐ Communications, Utilities and Miscellaneous Charge (23.3) 8,003 12,345 12,477
Printing and Reproduction (24.0) 5,348 6,433 6,531
Other Contractual Services: Advisory and Assistance Services (25.1) 121,906 170,319 172,447 Other Services (25.2) 1,101,907 1,156,098 1,133,072
Purchases from Govt. Accounts (25.3) 86,829 99,447 99,800
Operation & Maintenance of Facilities (25.4) 9,995 14,354 14,392 Research & Development Contracts (25.5) ‐ Medical Services (25.6) 22,956 54,818 35,357 Operation & Maintenance of Equipment (25.7) 44,584 75,631 66,058 Subsistence& Support of Persons (25.8) Subtotal, Other Contractual Services 1,388,176 1,570,667 1,521,125 Supplies and Materials (26.0) 39,535 62,475 63,430 Equipment (31.0) 3,458 4,914 4,941 Grants (41.0) Other (32), (42), (61) 207 1,059 1,072 Subtotal, Non – Pay Costs 1,467,774 1,684,978 1,636,962
Total, Reimbursable Obligations 1,616,960 1,849,094 1,802,734

19
Service and Supply Fund Organizational Chart
Program Support Center
Program Support Center
Financial Management
Portfolio
Occupational Health Portfolio
Real Estate Logistics
Operations Portfolio

20
Assistant Secretary for Administration
Acronym Key: EEOCO – Equal Employment Opportunity Compliance and Operations HPO & CMS – High Performing Organizations and Commercial Services Management ITIO – Information Technology Infrastructure and Operations OEAD – Office of Enterprise Application Development OIS – Office of Information Security OISPG – Office of IT Strategy, Policy and Governance SSF Activities are italicized
DHHS Secretary
Assistant Secretary for
Administration
EEOCOOffice of Business
Management Transformation
HPO & CSM
Office of the Chief Information
Officer
ITIO OEAD OIS OISPG
Office of Human Resources*

21
Non‐PSC Activities (1 of 2)
Acronym Key: AIM – Acquisition Integration and Modernization DCIS – Departmental Contracts Information System HCAS – HHS Consolidated Acquisition Solution TAGGS – Tracking Accountability in Government Grants System UFMS – Unified Financial Management System SSF Activities are italicized
DHHS Secretary
Agency for Children and
Families
Grants Solution Center of
Excellence
Assistant Secretary of
Financial Resources
Office of the Budget
Fund Manager
Office of Finance
Audit Coordination UFMS
Office of Grants and Acquisitions
AIM Category Management DCIS Grants.gov HCAS Small Business TAGGS

22
Non-PSC Activities (2 of 2)
Acronym Key: FOIA – Freedom of Information Act UFMS – Unified Financial Management System AIM – Acquisition Integration and Modernization DCIS – Departmental Contracts Information System HCAS – HHS Consolidated Acquisition System TAGGS – Tracking Accountability in Government Grants System SSF Activities are italicized
DHHS Secretary
Agency for Children and
Families
Grants Solution Center of
Excellence
Assistant Secretary of
Financial Resources
Office of Finance
Audit Coordination UFMS
Office of Grants and
Acquisitions
AIM Category Management DCIS Grants.gov HCAS Small Business TAGGS
Assistant Secretary for Public Affairs
FOIAHHS
Broadcast Studio
Media Monitoring WEB
Assistant Secretary for Planning and Evaluation
Strategic Planning Systems
Office of the General Counsel
Claims Ethics
Office of the Assistant
Secretary for Health
Commissioned Corps Force Management

Retirement Pay & Medical Benefits for Commissioned Officers

RETIREMENT PAY AND MEDICAL BENEFITS FOR COMMISSIONED OFFICERS
Authorizing Legislation 42 U.S.C., Chapter 6A; 10 U.S.C., Chapter 73; 10 U.S.C., Chapters 55; and Section 229(b) of the Social Security Act.
FY 2019 Authorization…………………………………………………………………Indefinite. Rationale for Budget This appropriation provides for retirement payments to Public Health Service (PHS) Commissioned Corps officers who are retired for age, disability, or a specific length of service as well as payments to survivors of deceased retired officers who had elected to receive reduced retirement payments. This appropriation also funds the provision of medical care to active duty and retired members of the Corps under the age of 65, dependents of active duty and retired members, and dependents of deceased members. This account includes payments to the Department of Defense (DoD) Medicare-Eligible Retiree Healthcare Fund for the accrued costs of health care for beneficiaries over the age of 65. The Accrual Health Care Benefits amount is an estimate of $4,471 per officer, provided by the DoD Office of the Actuary, multiplied by the estimated total number of active duty positions (6,719 in FY 2019), for a baseline contribution of $30,040,649. The FY 2019 estimate is a net decrease of $1,925,281 over the FY 2018 level. The overall request reflects increased costs in medical benefits, an average increase of 3% over the past five years in Retired Pay, and a net increase in the number of retirees and survivors during FY 2019.
FY 2020 FY 2021 FY 2022 FY 2023 FY 2024 Retirement Payments $483,482,784 $498,151,319 $513,264,888 $528,836,992 $544,881,543
Survivor’s Benefits 32,793,333 33,864,122 34,969,875 36,111,734 37,290,878
Medical Care Benefits 135,794,468 143,830,878 152,342,889 161,358,647 170,907,963
Sub Total $652,070,585 $675,846,320 $700,577,653 $726,307,373 $753,080,384
Accrued Health Benefits $32,000,000 $34,000,000 $36,000,000 $37,000,000 $37,000,000
Total $684,070,585 $709,846,320 $736,577,653 $763,307,373 $790,080,384
FY 2017 FY 2018 FY 2019 FY 2019
+/-FY 2018
Retirement Payments $441,126,028 $455,428,781 $469,246,177 $13,817,396 Survivor's
Benefits 29,844,587 30,752,261 31,756,403 1,004,143
Medical Care Benefits 122,449,383 121,043,638 128,207,084 7,163,446
Sub Total $593,419,998 $607,224,679 $629,209,664 $21,984,985
Accrued Health Care Benefits $27,873,208 $31,965,930 $30,040,649 ($1,925,281)
Total $621,293,206 $639,190,609 $ 659,250,313 $20,059,704

HHS General Provisions

Page 1
TITLE II—GENERAL PROVISIONS SEC. 201. Funds appropriated in this title shall be available for not to exceed $50,000 for official reception and representation expenses when specifically approved by the Secretary. SEC. 202. None of the funds appropriated in this title shall be used to pay the salary of an individual, through a discretionary grant or other extramural mechanism, at a rate in excess of Executive Level V, except that this section shall not apply to the Head Start program. SEC. 203. Notwithstanding section 241(a) of the PHS Act, such portion as the Secretary shall determine, but not more than 2.9 percent, of any amounts appropriated for programs authorized under such Act shall be made available for the evaluation (directly, or by grants or contracts) and the implementation and effectiveness of programs funded in this title. (TRANSFER OF FUNDS) SEC. 204. Not to exceed 1 percent of any discretionary funds (pursuant to the Balanced Budget and Emergency Deficit Control Act of 1985) which are appropriated for the current fiscal year for HHS in this Act may be transferred between appropriations, but no such appropriation shall be increased by more than 3 percent by any such transfer: Provided, That the transfer authority granted by this section shall not be used to create any new program or to fund any project or activity for which no funds are provided in this Act: Provided further, That the Committees on Appropriations of the House of Representatives and the Senate are notified at least 15 days in advance of any transfer. SEC. 205. In lieu of the timeframe specified in section 338E(c)(2) of the PHS Act, terminations described in such section may occur up to 60 days after the execution of a contract awarded in fiscal year 2019 under section 338B of such Act. SEC. 206. None of the funds appropriated in this Act may be made available to any entity under title X of the PHS Act unless the applicant for the award certifies to the Secretary that it encourages family participation in the decision of minors to seek family planning services and that it provides counseling to minors on how to resist attempts to coerce minors into engaging in sexual activities. SEC. 207. Notwithstanding any other provision of law, no provider of services under title X of the PHS Act shall be exempt from any State law requiring notification or the reporting of child abuse, child molestation, sexual abuse, rape, or incest. SEC. 208. None of the funds appropriated by this Act (including funds appropriated to any trust fund) may be used to carry out the Medicare Advantage program if the Secretary denies participation in such program to an otherwise eligible entity (including a Provider Sponsored Organization) because the entity informs the Secretary that it will not provide, pay for, provide coverage of, or provide referrals for abortions: Provided, That the Secretary shall make appropriate prospective adjustments to the capitation payment to such an entity (based on an actuarially sound estimate of the expected costs of providing the service to such entity's enrollees): Provided further, That nothing in this section shall be construed to change the Medicare program's coverage for such services and a Medicare Advantage organization described in this section shall be responsible for informing enrollees where to obtain information about all Medicare covered services.

Page 2
SEC. 209. None of the funds made available in this title may be used, in whole or in part, to advocate or promote gun control. SEC. 210. In order for HHS to carry out international health activities, including HIV/AIDS and other infectious disease, chronic and environmental disease, and other health activities abroad during fiscal year 2019:
(1) The Secretary may exercise authority equivalent to that available to the Secretary of State in section 2(c) of the State Department Basic Authorities Act of 1956. The Secretary shall consult with the Secretary of State and relevant Chief of Mission to ensure that the authority provided in this section is exercised in a manner consistent with section 207 of the Foreign Service Act of 1980 and other applicable statutes administered by the Department of State.
(2) The Secretary is authorized to provide such funds by advance or reimbursement to the Secretary of State as may be necessary to pay the costs of acquisition, lease, alteration, renovation, and management of facilities outside of the United States for the use of HHS. The Department of State shall cooperate fully with the Secretary to ensure that HHS has secure, safe, functional facilities that comply with applicable regulation governing location, setback, and other facilities requirements and serve the purposes established by this Act. The Secretary is authorized, in consultation with the Secretary of State, through grant or cooperative agreement, to make available to public or nonprofit private institutions or agencies in participating foreign countries, funds to acquire, lease, alter, or renovate facilities in those countries as necessary to conduct programs of assistance for international health activities, including activities relating to HIV/AIDS and other infectious diseases, chronic and environmental diseases, and other health activities abroad.
(3) The Secretary is authorized to provide to personnel appointed or assigned by the Secretary to serve abroad, allowances and benefits similar to those provided under chapter 9 of title I of the Foreign Service Act of 1980, and 22 U.S.C. 4081 through 4086 and subject to such regulations prescribed by the Secretary. The Secretary is further authorized to provide locality‐based comparability payments (stated as a percentage) up to the amount of the locality‐based comparability payment (stated as a percentage) that would be payable to such personnel under section 5304 of title 5, United States Code if such personnel's official duty station were in the District of Columbia. Leaves of absence for personnel under this subsection shall be on the same basis as that provided under subchapter I of chapter 63 of title 5, United States Code, or section 903 of the Foreign Service Act of 1980, to individuals serving in the Foreign Service.
(TRANSFER OF FUNDS) SEC. 211. The Director of the NIH, jointly with the Director of the Office of AIDS Research, may transfer up to 3 percent among institutes and centers from the total amounts identified by these two Directors as funding for research pertaining to the human immunodeficiency virus: Provided, That the Committees on Appropriations of the House of Representatives and the Senate are notified at least 15 days in advance of any transfer. (TRANSFER OF FUNDS) SEC. 212. Of the amounts made available in this Act for NIH, the amount for research related to the human immunodeficiency virus, as jointly determined by the Director of NIH and the Director of the Office of AIDS Research, shall be made available to the "Office of AIDS Research" account. The Director of the Office of AIDS Research shall transfer from such account amounts necessary to carry out section 2353(d)(3) of the PHS Act.

Page 3
SEC. 213. (a) AUTHORITY.—Notwithstanding any other provision of law, the Director of NIH ("Director") may use funds available under section 402(b)(7) or 402(b)(12) of the PHS Act to enter into transactions (other than contracts, cooperative agreements, or grants) to carry out research identified pursuant to such section 402(b)(7) (pertaining to the Common Fund) or research and activities described in such section 402(b)(12). (b) PEER REVIEW.—In entering into transactions under subsection (a), the Director may utilize such peer review procedures (including consultation with appropriate scientific experts) as the Director determines to be appropriate to obtain assessments of scientific and technical merit. Such procedures shall apply to such transactions in lieu of the peer review and advisory council review procedures that would otherwise be required under sections 301(a)(3), 405(b)(1)(B), 405(b)(2), 406(a)(3)(A), 492, and 494 of the PHS Act. SEC. 214. Not to exceed $45,000,000 of funds appropriated by this Act to the institutes and centers of the National Institutes of Health may be used for alteration, repair, or improvement of facilities, as necessary for the proper and efficient conduct of the activities authorized herein, at not to exceed $3,500,000 per project. (TRANSFER OF FUNDS) SEC. 215. (a) The Biomedical Advanced Research and Development Authority ("BARDA") may enter into a contract, for more than one but no more than 10 program years, for purchase of research services or of security countermeasures, as that term is defined in section 319F‐2(c)(1)(B) of the PHS Act (42 U.S.C.247d–6b(c)(1)(B)), if—
(1) funds are available and obligated— (A) for the full period of the contract or for the first fiscal year in which the contract is in
effect; and (B) for the estimated costs associated with a necessary termination of the contract; and
(2) the Secretary determines that a multi‐year contract will serve the best interests of the Federal Government by encouraging full and open competition or promoting economy in administration, performance, and operation of BARDA's programs. (b) A contract entered into under this section—
(1) shall include a termination clause as described by subsection (c) of section 3903 of title 41, United States Code; and
(2) shall be subject to the congressional notice requirement stated in subsection (d) of such section.
SEC. 217. Section 229 of division H of Public Law 114–113 shall continue in effect through January 1, 2020. SEC. 218. (a) IN GENERAL.—Under the conditions listed in subsection (b), the Secretary or the head of a major organizational unit within the Department may in this fiscal year enter into a reimbursable agreement with the head of another major organizational unit within the Department or of another agency under which—
(1) the head of the ordering agency or unit delegates to the head of the servicing agency or unit the authority to issue a grant or cooperative agreement on behalf of the ordering agency or unit;
(2) the servicing agency or unit will execute or manage a grant or cooperative agreement on behalf of the ordering agency or unit; and

Page 4
(3) the ordering agency or unit will reimburse the servicing unit or agency for the amount of the grant or cooperative agreement and for the service of executing or managing the grant or cooperative agreement. (b) CONDITIONS.—The conditions for making an agreement described in subsection (a) are that —
(1) amounts are available; (2) the head of the ordering agency or unit decides the agreement is in the best interest of the
United States Government; and (3) the agency or unit to execute or manage the grant or cooperative agreement is able to
provide that service. (c) PAYMENT.—Payment shall be made promptly through the Intra‐governmental Payment and Collection system at the request of the agency or unit providing the service. Payment may be in advance or on providing all or part of the service, and shall be for any part of the estimated or actual cost as determined by the agency or unit providing the service. A bill submitted or a request for payment is not subject to audit or certification in advance of payment. Proper adjustment of amounts paid in advance shall be made as agreed to by the heads of the agencies or units on the basis of the amount of the grant or cooperative agreement and the actual cost of the service provided. (d) LIMITATIONS ON FUNDS.—A condition or limitation applicable to amounts for grant or cooperative agreements of the ordering agency or unit applies to an agreement made under this section and to a grant or cooperative agreement made under such agreement. (e) OBLIGATION OF APPROPRIATIONS.—An agreement made under this section obligates an appropriation of the ordering agency or unit. The amount obligated is deobligated to the extent that the agency or unit providing the service has not incurred obligations, before the end of the period of availability of the appropriation, in —
(1) awarding the grant or cooperative agreement; or (2) providing the agreed‐on services.
(f) NO EFFECT ON OTHER LAWS.—This section does not affect other laws about reimbursable agreements. SEC. 219. There is hereby established in the Treasury of the United States a fund to be known as the "Federal Emergency Response Fund" (the Fund). Amounts in the Fund shall be available, in addition to any other amount appropriated for such purposes, to carry out titles II, III, and XVII of the PHS Act with respect to domestic preparedness and global health; to prevent, prepare for, or respond to a chemical, biological, radiological, or nuclear threat.; to prevent, prepare for, or respond to an emerging infectious disease; and to purchase or lease, and provide for the insurance of, passenger motor vehicles for official use in foreign countries. Amounts in the Fund may only be used for a public health threat or emergency that the Secretary determines has significant potential to occur and potential, on occurrence, to affect national security or the health and security of United States citizens, domestically or internationally. The Secretary may transfer to the Fund in this fiscal year and hereafter such amounts as are necessary from any discretionary amounts (pursuant to the Balanced Budget and Emergency Deficit Control Act of 1985) appropriated in this and subsequent Acts, provided that no such appropriation is reduced by more than 1 percent. Such transferred amounts shall remain available until expended. When implementing response activities, amounts in the Fund may be transferred to other accounts of the Department of Health and Human Services for the purposes provided in this section. The Committees on Appropriations of the House of Representatives and the Senate shall be notified promptly of the initiation of response activities under this authority and of any transfer made under the authority provided in this section. The Committees on Appropriations of the House of Representatives and the Senate shall receive a report not later than 45 days after the end of each quarter in a fiscal year on the unobligated balances in the Response Fund and all actual obligations incurred for that fiscal year,

Page 5
including obligations by program, project, or activity. The transfer authorities in this section are in addition to any other transfer authority otherwise available to the Department of Health and Human Services. Products purchased using amounts in the Fund may, at the discretion of the Secretary of Health and Human Services, be deposited in the Strategic National Stockpile under section 319F‐2 of the PHS Act. SEC. 220. Funds appropriated in this Act to accounts that received appropriations in the Department of Health and Human Services Appropriations Act, 2017, for the administrative expenses of programs or activities that do not receive appropriations from this Act shall be available for necessary expenses to carry out closure of such programs or activities. SEC. 221. Notwithstanding section 1864(e) of the Social Security Act (42 U.S.C. 1395aa(e)), the Secretary shall charge health care facilities or entities fees in cases where such facilities or entities have been cited for deficiencies during initial certification, recertification, or substantiated complaint surveys to cover all or a portion of the costs incurred for conducting substantiated complaint surveys and revisit surveys on such health care facilities and entities. Such fees shall be in addition to any other funds available for conducting such surveys and shall be credited to the "Department of Health and Human Services—Centers for Medicare and Medicaid Services—Program Management" account, to remain available until expended for such purpose. No such fees shall be charged to an Indian Health Program (as that term is defined in section 4 of the Indian Health Care Improvement Act). SEC. 222. Section 340B of the Public Health Service Act (42 U.S.C. 256b) is amended— (a) in subsection (a)(5)(C)—
(1) by striking "A covered entity shall permit" and inserting "(i) DUPLICATE DISCOUNTS AND DRUG RESALE.—A covered entity shall permit"
(2) by inserting at the end the following: "(ii) USE OF SAVINGS.—A covered entity shall permit the Secretary to audit at the
Secretary's expense the records of the entity to determine how net income from purchases under this section are used by the covered entity.
"(iii) RECORDS RETENTION.— Covered entities shall retain such records and provide such records and reports as deemed necessary by the Secretary for carrying out this subparagraph.".
(b) by adding at the end the following new subsection: "(f) REGULATIONS.—The Secretary may promulgate such regulations as the Secretary determines necessary or appropriate to carry out the provisions of this section.". SEC. 223. (a) IN GENERAL.—A State or tribal organization which receives grant funds attributable to appropriations under the heading "Department of Health and Human Services—Administration for Community Living—Aging and Disability Services Programs" to carry out programs under parts B, C, D, or E of title III (with respect to States) or under title VI (with respect to tribal organizations) of the Older Americans Act of 1965 (OAA) may elect to transfer up to 100 percent of such received funds among such title III or title VI programs (respectively), subject to OAA sections 306(a)(9) and 307(a)(9) but notwithstanding any otherwise‐applicable limitations on such transfers under the OAA or such heading. (b) NOTIFICATION OF PROPOSED TRANSFER; SECRETARIAL APPROVAL.—A State or tribal organization which elects to make a transfer under subsection (a) shall notify the Secretary of Health and Human Services of such proposed transfer, including a description of the amount to be transferred, the purposes of the transfer, the need for the transfer, and the impact of the transfer on the provision of

Page 6
services from which the funding would be transferred. The Secretary shall approve any such transfer unless the Secretary determines that such transfer is not consistent with the objectives of the OAA. (c) RULES OF CONSTRUCTION.—No transfer of grant funds by a State or tribal organization under this section shall be construed—
(1) as inconsistent with the authorized use of such funds under the OAA, including for purposes of OAA administration and oversight by the Secretary; or
(2) to relieve the State or tribal organization from applicable reporting requirements under the OAA regarding the use of such funds.
SEC. 224. Funds available to the Secretary under this or any prior Act that are available for acquisition of real property or for construction or improvement of facilities shall also be available to make transportation and infrastructure related improvements on property located directly adjacent to property owned by the Federal Government, provided that the primary benefit of such improvements accrues to HHS or the component thereof funding the improvements. SEC. 225. With respect to an individual who is serving as principal investigator on one or more grants or cooperative agreements funded by the National Institutes of Health (NIH) under this title, none of the funds made available to NIH by this title shall be used, together with any funds from the analogous title in any previous appropriations act, to pay the salary of such individual at a rate exceeding 90 percent of such salary. SEC. 226. Funds appropriated in this or any prior Act or the Patient Protection and Affordable Care Act that are available for salaries and expenses of employees of the Department of Health and Human Services shall also be available for the primary and secondary schooling of eligible dependents of HHS personnel stationed in the Commonwealth of Puerto Rico, the Commonwealth of the Northern Mariana Islands, and the possessions of the United States at costs not in excess of those paid for or reimbursed by the Department of Defense. SEC. 228. Funds appropriated in this or any prior Act or the Patient Protection and Affordable Care Act that are available for salaries and expenses of employees of the Department of Health and Human Services shall also be available to pay travel and related expenses of such an employee or of a member of his or her family, when such employee is assigned to duty, in the United States or in a U.S. territory, during a period and in a location that are the subject of a determination of a public health emergency under section 319 of the Public Health Service Act and such travel is necessary to obtain medical care for an illness, injury, or medical condition that cannot be adequately addressed in that location at that time. For purposes of this section, the term "U.S. territory" means Guam, the Commonwealth of Puerto Rico, the Northern Mariana Islands, the Virgin Islands, American Samoa, or the Trust Territory of the Pacific Islands. SEC. 229. Notwithstanding section 12(b) of the Federal Advisory Committee Act, funds made available by this Act for the "National Institutes of Health—Office of the Director" account shall also be available to establish and operate the Research Policy Board authorized by section 2034(f) of Public Law 114–255. TITLE V—GENERAL PROVISIONS (TRANSFER OF FUNDS) SEC. 501. The Secretaries of Labor, Health and Human Services, and Education are authorized to transfer unexpended balances of prior appropriations to accounts corresponding to current appropriations

Page 7
provided in this Act. Such transferred balances shall be used for the same purpose, and for the same periods of time, for which they were originally appropriated. SEC. 502. No part of any appropriation contained in this Act shall remain available for obligation beyond the current fiscal year unless expressly so provided herein. SEC. 503. (a) No part of any appropriation contained in this Act or transferred pursuant to section 4002 of Public Law 111–148 shall be used, other than for normal and recognized executive‐legislative relationships, for publicity or propaganda purposes, for the preparation, distribution, or use of any kit, pamphlet, booklet, publication, electronic communication, radio, television, or video presentation designed to support or defeat the enactment of legislation before the Congress or any State or local legislature or legislative body, except in presentation to the Congress or any State or local legislature itself, or designed to support or defeat any proposed or pending regulation, administrative action, or order issued by the executive branch of any State or local government, except in presentation to the executive branch of any State or local government itself. (b) No part of any appropriation contained in this Act or transferred pursuant to section 4002 of Public Law 111–148 shall be used to pay the salary or expenses of any grant or contract recipient, or agent acting for such recipient, related to any activity designed to influence the enactment of legislation, or appropriations, regulation, administrative action, or Executive order proposed or pending before the Congress or any State government, State legislature or local legislature or legislative body, other than for normal and recognized executive‐legislative and State‐local relationships, for presentation to any State or local legislature or legislative body itself, or for participation by an agency or officer of a State, local or tribal government in policymaking and administrative processes within the executive branch of that government. (c) The prohibitions in subsections (a) and (b) shall include any activity to advocate or promote any proposed, pending or future Federal, State or local tax increase, or any proposed, pending, or future requirement or restriction on any legal consumer product, including its sale or marketing, including but not limited to the advocacy or promotion of gun control. SEC. 504. The Secretaries of Labor and Education are authorized to make available not to exceed $28,000 and $20,000, respectively, from funds available for salaries and expenses under titles I and III, respectively, for official reception and representation expenses; the Director of the Federal Mediation and Conciliation Service is authorized to make available for official reception and representation expenses not to exceed $5,000 from the funds available for "Federal Mediation and Conciliation Service, Salaries and Expenses"; and the Chairman of the National Mediation Board is authorized to make available for official reception and representation expenses not to exceed $5,000 from funds available for "National Mediation Board, Salaries and Expenses". SEC. 505. When issuing statements, press releases, requests for proposals, bid solicitations and other documents describing projects or programs funded in whole or in part with Federal money, all grantees receiving Federal funds included in this Act, including but not limited to State and local governments and recipients of Federal research grants, shall clearly state— (1) the percentage of the total costs of the program or project which will be financed with Federal money; (2) the dollar amount of Federal funds for the project or program; and (3) percentage and dollar amount of the total costs of the project or program that will be financed by non‐governmental sources.

Page 8
SEC. 506. (a) None of the funds appropriated in this Act, and none of the funds in any trust fund to which funds are appropriated in this Act, shall be expended for any abortion. (b) None of the funds appropriated in this Act, and none of the funds in any trust fund to which funds are appropriated in this Act, shall be expended for health benefits coverage that includes coverage of abortion. (c) The term "health benefits coverage" means the package of services covered by a managed care provider or organization pursuant to a contract or other arrangement. SEC. 507. (a) The limitations established in the preceding section shall not apply to an abortion—
(1) if the pregnancy is the result of an act of rape or incest; or (2) in the case where a woman suffers from a physical disorder, physical injury, or physical
illness, including a life‐endangering physical condition caused by or arising from the pregnancy itself, that would, as certified by a physician, place the woman in danger of death unless an abortion is performed. (b) Nothing in the preceding section shall be construed as prohibiting the expenditure by a State, locality, entity, or private person of State, local, or private funds (other than a State's or locality's contribution of Medicaid matching funds). (c) Nothing in the preceding section shall be construed as restricting the ability of any managed care provider from offering abortion coverage or the ability of a State or locality to contract separately with such a provider for such coverage with State funds (other than a State's or locality's contribution of Medicaid matching funds). (d) (1) None of the funds made available in this Act may be made available to a Federal agency or program, or to a State or local government, if such agency, program, or government subjects any institutional or individual health care entity to discrimination on the basis that the health care entity does not provide, pay for, provide coverage of, or refer for abortions.
(2) In this subsection, the term "health care entity" includes an individual physician or other health care professional, a hospital, a provider‐sponsored organization, a health maintenance organization, a health insurance plan, or any other kind of health care facility, organization, or plan. SEC. 508. (a) None of the funds made available in this Act may be used for—
(1) the creation of a human embryo or embryos for research purposes; or (2) research in which a human embryo or embryos are destroyed, discarded, or knowingly
subjected to risk of injury or death greater than that allowed for research on fetuses in utero under 45 CFR 46.204(b) and section 498(b) of the Public Health Service Act (42 U.S.C. 289g(b)). (b) For purposes of this section, the term "human embryo or embryos" includes any organism, not protected as a human subject under 45 CFR 46 as of the date of the enactment of this Act, that is derived by fertilization, parthenogenesis, cloning, or any other means from one or more human gametes or human diploid cells. SEC. 509. (a) None of the funds made available in this Act may be used for any activity that promotes the legalization of any drug or other substance included in schedule I of the schedules of controlled substances established under section 202 of the Controlled Substances Act except for normal and recognized executive‐congressional communications. (b) The limitation in subsection (a) shall not apply when there is significant medical evidence of a therapeutic advantage to the use of such drug or other substance or that federally sponsored clinical trials are being conducted to determine therapeutic advantage.

Page 9
SEC. 510. None of the funds made available in this Act may be used to promulgate or adopt any final standard under section 1173(b) of the Social Security Act providing for, or providing for the assignment of, a unique health identifier for an individual (except in an individual's capacity as an employer or a health care provider), until legislation is enacted specifically approving the standard. SEC. 511. None of the funds made available in this Act may be obligated or expended to enter into or renew a contract with an entity if— (1) such entity is otherwise a contractor with the United States and is subject to the requirement in 38 U.S.C. 4212(d) regarding submission of an annual report to the Secretary of Labor concerning employment of certain veterans; and (2) such entity has not submitted a report as required by that section for the most recent year for which such requirement was applicable to such entity. SEC. 512. (a) None of the funds made available in this Act may be used to request that a candidate for appointment to a Federal scientific advisory committee disclose the political affiliation or voting history of the candidate or the position that the candidate holds with respect to political issues not directly related to and necessary for the work of the committee involved. (b) None of the funds made available in this Act may be used to disseminate information that is deliberately false or misleading. SEC. 513. None of the funds appropriated in this Act shall be expended or obligated by the Commissioner of Social Security, for purposes of administering Social Security benefit payments under title II of the Social Security Act, to process any claim for credit for a quarter of coverage based on work performed under a social security account number that is not the claimant's number and the performance of such work under such number has formed the basis for a conviction of the claimant of a violation of section 208(a)(6) or (7) of the Social Security Act. SEC. 514. None of the funds appropriated by this Act may be used by the Commissioner of Social Security or the Social Security Administration to pay the compensation of employees of the Social Security Administration to administer Social Security benefit payments, under any agreement between the United States and Mexico establishing totalization arrangements between the social security system established by title II of the Social Security Act and the social security system of Mexico, which would not otherwise be payable but for such agreement. SEC. 515. Notwithstanding any other provision of this Act, no funds appropriated in this Act shall be used to purchase sterile needles or syringes for the hypodermic injection of any illegal drug: Provided, That such limitation does not apply to the use of funds for elements of a program other than making such purchases if the relevant State or local health department, in consultation with the Centers for Disease Control and Prevention, determines that the State or local jurisdiction, as applicable, is experiencing, or is at risk for, a significant increase in hepatitis infections or an HIV outbreak due to injection drug use, and such program is operating in accordance with State and local law. SEC. 516. (a) None of the funds made available in this Act may be used to maintain or establish a computer network unless such network blocks the viewing, downloading, and exchanging of pornography. (b) Nothing in subsection (a) shall limit the use of funds necessary for any Federal, State, tribal, or local law enforcement agency or any other entity carrying out criminal investigations, prosecution, or adjudication activities.

Page 10
SEC. 517. (a) Federal agencies may use Federal discretionary funds that are made available in this Act to carry out up to 10 Performance Partnership Pilots. Such Pilots shall be governed by the provisions of section 526 of division H of Public Law 113–76, except that in carrying out such Pilots section 526 shall be applied by substituting "Fiscal Year 2019" for "Fiscal Year 2014" in the title of subsection (b) and by substituting "September 30, 2023" for "September 30, 2018" each place it appears. (b) In addition, Federal agencies may use Federal discretionary funds that are made available in this Act to participate in Performance Partnership Pilots that are being carried out pursuant to the authority provided by section 526 of division H of Public Law 113–76, section 524 of division G of Public Law 113–235, and section 525 of division H of Public Law 114–113. SEC. 518. EVALUATION FUNDING FLEXIBILITY. (a) This section applies to:
(1) the Office of the Assistant Secretary for Planning and Evaluation within the Office of the Secretary and the Administration for Children and Families in the Department of Health and Human Services; and
(2) the Chief Evaluation Office and the statistical‐related cooperative and interagency agreements and contracting activities of the Bureau of Labor Statistics in the Department of Labor. (b) Amounts made available under this Act which are either appropriated, allocated, advanced on a reimbursable basis, or transferred to the functions and organizations identified in subsection (a) for research, evaluation, or statistical purposes shall be available for obligation through September 30, 2023. When an office referenced in subsection (a) receives research and evaluation funding from multiple appropriations, such offices may use a single Treasury account for such activities, with funding advanced on a reimbursable basis. (c) Amounts referenced in subsection (b) that are unexpended at the time of completion of a contract, grant, or cooperative agreement may be deobligated and shall immediately become available and may be reobligated in that fiscal year or the subsequent fiscal year for the research, evaluation, or statistical purposes for which the amounts are made available to that account. SEC. 519. (a) Notwithstanding any other provision of law, none of the discretionary appropriations, as such term is defined by section 250(c)(7) of the Balanced Balanced Budget and Emergency Deficit Control Act of 1985 (2 U.S.C. 900(c)(7)), made available by this Act may be made available either directly, through a State (including through managed care contracts with a State), or through any other means, to a prohibited entity. (b) PROHIBITED ENTITY.—The term "prohibited entity" means an entity, including its affiliates, subsidiaries, successors, and clinics—
(1) that, as of the date of enactment of this Act— (A) is an organization described in section 501(c)(3) of the Internal Revenue Code of
1986 and exempt from tax under section 501(a) of such Code; (B) is an essential community provider described in section 156.235 of title 45, Code of
Federal Regulations (as in effect on the date of enactment of this Act), that is primarily engaged in family planning services, reproductive health, and related medical care; and
(C) performs, or provides any funds to any other entity that performs, abortions, other than an abortion—
(i) if the pregnancy is the result of an act of rape or incest; or (ii) in the case where a woman suffers from a physical disorder, physical injury,
or physical illness that would, as certified by a physician, place the woman in danger of

Page 11
death unless an abortion is performed, including a lifeendangering physical condition caused by or arising from the pregnancy itself; and
(2) for which the total amount of Federal grants to such entity, including grants to any affiliates, subsidiaries, or clinics, under title X of the Public Health Service Act in fiscal year 2017 exceeded $23,000,000. (c) (1) END OF PROHIBITION. —The definition in subsection (b) shall cease to apply to an entity if such entity certifies that it, including its affiliates, subsidiaries, successors, and clinics, will not perform, and will not provide any funds to any other entity that performs, an abortion as defined in subsection (b)(1)(C).
(2) REPAYMENT. —The Secretary of Health and Human Services shall seek repayment of any Federal assistance received by any entity that had made a certification described in paragraph (1) and subsequently violated the terms of such certification.
(CANCELLATION) SEC. 520. Of any available amounts appropriated under section 108 of Public Law 111–3, as amended, $53,544 are hereby permanently cancelled. TITLE V—GENERAL PROVISIONS—LEGISLATIVE PROPOSAL SEC. 500. Contingent upon the enactment of authorizing legislation, of the amounts deposited in the Child Enrollment Contingency Fund from appropriations to the Fund under section 2104(n)(2)(A) of the Social Security Act, including for both semi‐annual allotment periods for fiscal year 2019 under section 2104(n)(2)(A)(ii) of that Act, and the income derived from investment of those funds pursuant to section 2104(n)(2)(C) of that Act, $667,000,000 shall not be available for obligation in this fiscal year. SEC. 501. Contingent upon the enactment of authorizing legislation, of the funds made available for purposes of carrying out section 2105(a)(3) of the Social Security Act, $3,118,000,000 are hereby permanently cancelled. HHS is not seeking a general provision that has been enacted in previous years that specifically related to the Risk Corridors program, as the Risk Corridors program period has concluded. In addition, the CMS Program Management lump‐sum appropriation is for program management expenses, and not for the program payments themselves.