Dengue Bulletin - World Health Organizationapps.searo.who.int/pds_docs/B0221.pdf · Dengue Bulletin...
211
D D e e n n g g u u e e B B u u l l l l e e t t i i n n Volume 27 December 2003 World Health Organization The South-East Asia and Western Pacific Region
Transcript of Dengue Bulletin - World Health Organizationapps.searo.who.int/pds_docs/B0221.pdf · Dengue Bulletin...

DDeenngguuee BBuulllleettiinn Volume 27 December 2003
World Health Organization
The South-East Asia and Western Pacific Region

ISBN 92 9022 256 5 © World Health Organization 2002
Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol 2 of the Universal Copyright Convention. For rights of reproduction or translation, in part or in toto, of publications issued by the WHO Regional Office for South-East Asia, application should be made to the Regional Office for South-East Asia, World Health House, Indraprastha Estate, New Delhi 110 002, India.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
The views expressed in this publication are those of the author and do not necessarily reflect the decisions or stated policy of the World Health Organization; however they focus on issues that have been recognized by the Organization and Member States as being of high priority.
Printed in India
Indexation: Dengue Bulletin is being indexed by BIOSIS and EMBASE, the EXCERPTA MEDICA database

From the Editor’s desk
engue fever (DF) and dengue haemorrhagic fever (DHF) continue to be a major health problem with ever-increasing incidence and severity of the disease is
promoted by the geographic spread of vectors as well as viruses. Some 2.5 billion people are globally at risk and as per estimates, nearly 50 million cases of DF with over 500,000 cases of DHF occur annually. Endemic countries usually face larger epidemics in 3-5 year cycles. However, urbanization stresses, i.e. rural to urban migration, scarcity of drinking water, developmental/industrial activities all put together have generated variable breeding potential of Aedes aegypti leading to build-up of local/focal endemic foci on a yearly basis in the metropolitan city of Delhi (India)
To reduce the disease burden and case fatality rates, endemic countries are striving hard to improve epidemiological and entomological surveillance through ‘DengueNet’ improving emergency preparedness to prevent and control epidemics, effective case management by developing sensitive diagnostics and other infrastructural improvements and finally by strengthening vector control activities in an integrated vector management (IVM) mode.
New initiatives during the year included generation of more field data for understanding the pathogenesis of DHF – i.e. immune enhancement or mutation, need for platelet transfusion in relation to degree of thrombocytopenia, methods of virus isolation and serotyping for resource constrained countries, improving entomological surveillance by ovitraps by adding bio-larvicide in hay infusion and an estimation of dengue among travellers in Europe through intensive networking.
Volume 27 of the Dengue Bulletin includes contributions from WPR (9), SEAR (8), EMR (2), AMRO/PAHO (4) and EURO (4).
We now invite contributions for Volume 28 (2004). The deadline for the receipt of contributions is 30 June 2004. Contributors are requested to follow the instructions carefully while preparing the manuscript. Contributions accompanied by computer diskettes using MS Word for Windows should be sent to the Editor, Dengue Bulletin, WHO/SEARO, Mahatma Gandhi Road, IP Estate, Ring Road, New Delhi-110 002, India, or by e-mail as a file attachment to the Editor at [email protected].
Readers desirous of obtaining copies of the Dengue Bulletin may contact the respective WHO Regional Offices in New Delhi or Manila or the WHO Country Representative in their country of residence.
Dr Chusak Prasittisuk Regional Adviser Malaria World Health Organization Regional Office for South-East Asia New Delhi, India
D

Dengue Bulletin – Vol 27, 2003 iii
Acknowledgements
Editor, Dengue Bulletin, WHO/SEARO, gratefully thanks the following for spending professional time and expertise to peer review manuscripts submitted for publication.
In-house Review Nand L. Kalra: Professional expert for scanning the manuscripts in respect of format check, contents, conclusions drawn, including condensation and omission of tabular and illustrative materials for clear, concise and focused presentation, bibliographic references and for overseeing the final stages involved in the printing of the Bulletin.
Peer Reviewers
1. Bridget Wills The University of Oxford Clinical Research Unit 190 Ben Ham Tu, Quan 5 Ho Chi Minh City, Viet Nam E-mail: [email protected]
2. Dana A. Focks Infectious Disease Analysis P.O. Box 12852 Gainesville, FL 32604, USA E-mail: [email protected]; [email protected]
3. Dinesh Srivastava Department of Medicine Dr Ram Manohar Lohia Hospital New Delhi – 110 001, India E-mail: [email protected]
4. Duane J. Gubler Division of Vector-Borne Infectious Diseases National Center for Infectious Diseases Centers for Disease Control and Prevention PO Box 2087 Fort Collins CO 80522, USA E-mail: [email protected]
5. Goro Kuno Division of Vector-Borne Infectious Diseases National Center for Infectious Diseases Centers for Disease Control and Prevention PO Box 2087 Fort Collins CO 80522, USA E-mail: [email protected]

iv Dengue Bulletin – Vol 27, 2003
6. Ichiro Kurane Division of Vector-Borne Viruses Department of Virology 1 National Institute of Infectious Diseases 1-23-1, Toyama, Shinjyuku-ku Tokyo 162-8640, Japan E-mail: [email protected]
7. Kevin Palmer Regional Office for the Western Pacific 12115 Manila, Philippines E-mail: [email protected]
8. Michael Nathan World Health Organization Headquarters 20 Avenue Appia 1211 Geneva 27, Switzerland E-mail: [email protected]
9. Natth Bhamarapravati Center for Vaccine Development Mahidol University at Salaya Nakhon Pathom, Thailand E-mail: [email protected]
10. Oon Chong Teik Tropical Medicine & Infectious Diseases Mt Elizabeth Hospital Singapore 228510 E-mail: [email protected]
11. Sushil Kumar Kabra Department of Paediatrics All India Institute of Medical Sciences Ansari Nagar New Delhi – 110 029, India Email: [email protected]
The quality and scientific stature of the Dengue Bulletin is largely due to conscientious efforts of the experts and also of the contributors for positive response to the comments and suggestions.

Dengue Bulletin – Vol 27, 2003 v
Contents
1. The Features of Imported Dengue Fever Cases Confirmed at National Institute of Infectious Diseases Japan, during 2001
Ken-Ichiro Yamada, Tomohiko Takasaki, Masaru Nawa, Reiko Nerome, Yohko T Arai, Kinjiro Morimoto and Ichiro Kurane
1
2. Towards Sustaining Behavioural Impact in Dengue Prevention and Control
E Renganathan, W Parks, L Lloyd, MB Nathan, E Hosein, A Odugleh, GG Clark, DJ Gubler, C Prasittisuk, K Palmer and J-L San Martin
6
3. Dengue in Jeddah, Saudi Arabia, 1994-2002 Mazen Fakeeh and Ali M Zaki
13
4. Dengue Haemorrhagic Fever in Taiwan Jien-Wei Liu, Boon-Siang Khor, Chen-Hsiang Lee, Ing-Kit Lee, Rong-Fu Chen and Kuender D Yang
19
5. Dengue in Brazil: Past, Present and Future Perspective Luiz Tadeu Moraes Figueiredo
25
6. Diagnosis of Imported Dengue Fever in the Czech Republic Pavel Chalupa, Marie Kolarova, Nada Sojkova and Jiri Januska
34
7. Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
M Sriprom, P Pongsumpun, S Yoksan, P Barbazan, J P Gonzalez and I M Tang
39
8. Virological and Serological Surveillance of Dengue Epidemics in 19 Provinces in Southern Viet Nam during 2001
Do Quang Ha, Vu Thi Que Huong, Huynh Thi Kim Loan, Vu Thien Thu Ngu, Hoang Thi Nhu Dao and Cao Minh Thang
46

vi Dengue Bulletin – Vol 27, 2003
9. Circulation of Dengue Viruses in North-Western Peru, 2000-2001
Ysabel Montoya, Susan Holechek, Omar Caceres, Ana Palacios, James Burans, Carolina Guevara, Fernando Quintana, Victor Herrera, Edwar Pozo, Elizabeth Anaya, Enrique Mamani, Victoria Gutierrez, Adriana Ladron de Guevara, Eduardo Fernandez, Percy Asmat, Victor Alva-Davalos, Carlos Hoguin, V Alberto Laguna, Ana M Morales, Percy Minaya and Tadeusz Kochel
52
10. Exploratory Temporal and Spatial Distribution Analysis of Dengue Notifications in Boa Vista, Roraima, Brazilian Amazon, 1999-2001
Maria Goreti Rosa-Freitas, Pantelis Tsouris, Alexander Sibajev, Ellem Tatiani de Souza Weimann, Alexandre Ubirajara Marques, Rodrigo Lopes Ferreira and José Francisco Luitgards-Moura
63
11. Isolation and Serotyping of Dengue Viruses by Mosquito Inoculation and Cell Culture Technique: An Experience in Bangladesh
Monira Pervin, Shahina Tabassum, Bijon Kumar Sil and Md Nazrul Islam
81
12. Epidemiology and Phylogenetic Relationships of Dengue Viruses Oswaldo Paulo Forattini
91
13. Development of IgM-capture Enzyme-Linked Immunosorbent Assay for Serodiagnosis of Dengue using Beta-propiolactone-inactivated Dengue Viral Antigens
Masaru Nawa, Tomohiko Takasaki, Ken-Ichiro Yamada, Ichiro Kurane and Toshitaka Akatsuka
95
14. Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
Hui-Yee Chee and Sazaly AbuBakar
100
15. Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
M Narayanan, M A Aravind, P Ambikapathy, R Prema and M P Jeyapaul
108
16. Dengue Fever: Its Laboratory Diagnosis, with Special Emphasis on IgM Detection
N Sathish, T S Vijayakumar, P Abraham and G Sridharan
116
17. Dengue – The Underestimated Risk in Travellers O Wichmann, N Mühlberger and T Jelinek
126

Dengue Bulletin – Vol 27, 2003 vii
18. Thrombocytopenia and Platelet Transfusions in Dengue Haemorrhagic Fever and Dengue Shock Syndrome
Alex Chairulfatah, Djatnika Setiabudi, Ridad Agoes and Robert Colebunders
138
19. Improvement of Case-Management - A Key Factor to Reduce Case-Fatality Rate of Dengue Haemorrhagic Fever in Southern Viet Nam
Nguyen Thanh Hung and Nguyen Trong Lan
144
20. Community Mobilization in Aedes aegypti Control Programme by Source Reduction in Peri-Urban District of Lautoka, Viti Levu, Fiji Islands
Arun K Raju
149
21. Field Evaluation of Ovitraps Consociated with Grass Infusion and Bacillus thuringiensis var. israelensis to determine Oviposition Rates of Aedes aegypti
S R A Santos, M A V Melo-Santos, L Regis and C M R Albuquerque
156
22. Impact of Intervention Measures on DF/DHF Cases and Aedes aegypti Indices in Delhi, India: An Update, 2001
Rakesh Katyal, Kaushal Kumar, Kuldip Singh Gill and R S Sharma
163
23. Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
Zeev Wiesman and Bishnu P Chapagain
168
24. The Impact of Health Education on Mother’s Knowledge, Attitude and Practice (KAP) of Dengue Haemorrhagic Fever
Tran Tan Tram, Nguyen Thi Ngoc Anh, Nguyen Thanh Hung, Nguyen Trong Lan, Le Thi Cam, Nguyen Phuoc Chuong, Le Tri, Lise Fonsmark, Anja Poulsen and Erik Deichmann Heegaard
174
25. Viral Vaccines for Dengue: The Present and the Future S Swaminathan and Navin Khanna
181
Short Notes
1. Dengue Haemorrhagic Fever - A threat to Global Health Somkiat Sopontammarak
192

viii Dengue Bulletin – Vol 27, 2003
2. Aedes albopictus (Skuse) Breeding in Plastic Cups around Tea-vendor Spots in Ernakulam City, Kerala State, India J Hiriyan, S C Tewari and B K Tyagi
195
3. Potential of Rubber Plantations as Breeding Source for Aedes albopictus in Kerala, India P K Sumodan
197
Book Review
1. Guidelines for the Evaluation of Dengue Vaccines in Populations Exposed to Natural Infection
199
Instructions for Contributors 201

Dengue Bulletin – Vol 27, 2003 1
The Features of Imported Dengue Fever Cases Confirmed at National Institute of Infectious Diseases
Japan, during 2001+π
by Ken-Ichiro Yamada*#, Tomohiko Takasaki*, Masaru Nawa**, Reiko Nerome*,
Yohko T Arai*, Kinjiro Morimoto* and Ichiro Kurane*
*Department of Virology 1, National Institute of Infectious Diseases, 1-23-1 Toyama, Shinjuku-ku, Tokyo 162-8640 Japan
**Department of Microbiology, Saitama Medical School, Japan
Abstract
The demographic features of the dengue cases confirmed during 2001 at the National Institute of Infectious Diseases, Japan, were determined. Thirty-five cases were confirmed to be of dengue fever, 18 cases were male and 17 female. The youngest case was 19 years old and the oldest was 64 years old. Thirty-four cases were determined to be of primary infection, and one was secondary. Most of the dengue patients developed illness after returning from countries in South-East and South Asia. In addition, two patients had visited Tahiti and one had visited Samoa before developing dengue fever. Dengue fever/dengue haemorrhagic fever is the infectious disease that should attract more attention in Japan.
Keywords: Dengue fever, imported cases, serodiagnosis, Japan.
#For correspondence: [email protected]
+Information generated on the circulation of dengue serotypes is equally important for ‘travellers contact’ countries. Introduction of new DEN serotype has been found to be a good predictive indicator for larger epidemics. During the present study, out of the 21 virus genome detections from countries of South-East and South Asia, 15 isolations belonged to DEN-1 and three each to DEN-2 and DEN-3. DEN-1 was the predominant virus circulating in the region during 2001. Besides, this information is important for DHF/DSS case management. In Thailand it has been established that the severity of DEN-1 and DEN-2 is associated with more plasma leakage, more shock and complication with fluid overload cases, whereas DEN-3 and DEN-4 severity is associated with hepatic dysfunction and encephalophathy. Advance stocking of DEN serotype-specific requirements in hospitals will result in better case management and help in lowering the case fatality rates. – Editor
πThis article was published in the last issue of Dengue Bulletin (Volume 26, December 2002, pp. 168-172). However, due to a mix-up during printing, the Abstract it carried actually belonged to another article. In order to give our readers the correct version, we are publishing this article once again. The error is very much regretted. - Editor

The Features of Imported Dengue Fever Cases Confirmed at NIID, Japan, during 2001
2 Dengue Bulletin – Vol 27, 2003
Introduction Dengue fever/dengue haemorrhagic fever is one of the infectious diseases that all physicians are required to report in Japan, according to the Japanese infectious disease control law. Dengue outbreaks occurred in Osaka, Kobe, Hiroshima and Nagasaki from 1942 to 1945(1). Dengue virus infection has not been epidemic in Japan since then, and there are no domestic dengue virus infections today. However, there have been dengue cases imported into Japan(2,3,4).
Laboratory diagnosis is essential for the confirmation of dengue virus infection. We have performed laboratory diagnosis of dengue virus infection upon request from hospitals and clinics. The features of imported dengue cases that were confirmed at the National Institute of Infectious Diseases from 1985 to 2000 have been previously reported(2,3,4,5).
Materials and methods Serum specimens were collected from dengue-suspected cases in clinics and hospitals, and sent to the Department of Virology 1, National Institute of Infectious Diseases, Tokyo, for laboratory diagnosis. In the present paper, we report the features of the dengue cases confirmed at our laboratory during 2001. Dengue virus infections were confirmed by IgM-capture enzyme-linked immunosorbent assay (ELISA), IgG-ELISA, rapid immuno-chromatographic test, haemmagglutination inhibition (HI) test, and reverse transcriptase-polymerase chain reaction (RT-PCR) as previously reported(3,4).
Commercial IgM-capture ELISA and IgG-ELISA (MRL, California, USA) and rapid immunochromatographic test (PanBio, East Brisbane, Australia) were purchased and used for serodiagnosis. RT-PCR was performed as previously reported(6,7). The primer sequences used to amplify each serotype of dengue viruses and target size were previously reported(6,7). HI test was done on microtiter plate, using 4 haemagglutinatin units of DEN-2 viral antigen as previously reported(2).
Results The summary of dengue cases confirmed at our laboratory during 2001 is given in the Table. Blood samples from 76 suspected cases were tested and 35 were confirmed to be of dengue. All the cases were of dengue fever, and there was no case of dengue haemorrhagic fever. Of the 35 confirmed dengue fever cases, 18 were male and 17 female. The youngest case was 19 years old and the oldest 64 years old.
Most of the Japanese dengue patients developed illness after they had visited countries in South-East and South Asia (Table), e.g. Indonesia (2), Thailand (8); Philippines (7); Cambodia (3), India (2), Tahiti (2), Viet Nam (1) and Samoa (1). There were nine patients who had visited more than one country. Thirty-four of the 35 cases were determined to be primary dengue virus infection based on antibody response. There was one patient (patient #27) who was determined to be of secondary dengue virus infection. This was the first secondary dengue case we experienced during the past five years.

The Features of Imported Dengue Fever Cases Confirmed at NIID, Japan, during 2001
Dengue Bulletin – Vol 27, 2003 3
Table. Demographic information of 35 dengue cases
No. Age, Sex Disease day Type (PCR) IgM-ELISA IgG-ELISA Countries of contact
1 33, F 9 − +(1.1) +(7.3) Indonesia 2
29, M
3 7 9
14
DEN-2 − − −
-(0.3) +(3.2) +(3.6) +(3.7)
−0.7) +(3.7) +(4.4) +(5.3)
Indonesia
3
30, M
6 17
DEN-3 nd
+(6.7) +(15.4)
−(0.6) +(3.8)
Thailand Malaysia
4
30, M
6 13
DEN-1 nd
−0.2) +(4.0)
−0.6) nd
India Thailand
5
25, F
8 10 13 17
DEN-3 nd nd nd
+(2.7) +(3.8) +(4.1) +(2.2)
+(5.9) +(7.9) +(9.1) +(9.5)
Cambodia
6
49, M
7 8
13
DEN-1 nd nd
+(1.5) +(2.3) +(5.2)
+(7.8) +(8.2) +(9.3)
Tahiti
7 56, M 18 − +(2.5) +(10.6) Viet Nam 8
53, F
9 10
− nd
+(4.4) +(3.8)
+(9.2) +(9.4)
Philippines
9
58, M
7 8
DEN-1 nd
+(1.7) +(2.8)
+(5.8) +(7.5)
Philippines
10 45, F 8 − +(11.3) +(2.4) Philippines
11
23, M
4 5 6
13
− − nd nd
−0.8) +(1.4) +(2.2) +(8.2)
+(4.6) +(6.7) +(8.6) +(9.3)
Thailand Cambodia
Laos
12
22, F
4 11
DEN-1 nd
−0.5) +(4.1)
−1.0) +(9.0)
Philippines
13
44, M
15 19
− nd
+(6.9) +(6.7)
+(8.1) +(7.9)
Thailand
14
35, F
8 19
DEN-1 nd
+(2.2) +(2.4)
+(6.8) +(3.0)
Singapore Malaysia Thailand Indonesia
15
42, M
2 8
14 27
DEN-1 nd nd nd
−(0.9) +(5.0) +(5.2) +(3.4)
−(0.7) +(3.4) +(1.6) +(1.7)
Samoa
16
43, M
5 12
DEN-1 nd
−(0.3) +(3.6)
+(2.2) +(3.0)
Thailand Cambodia
China

The Features of Imported Dengue Fever Cases Confirmed at NIID, Japan, during 2001
4 Dengue Bulletin – Vol 27, 2003
No. Age, Sex Disease day Type (PCR) IgM-ELISA IgG-ELISA Countries of contact
17
24, F
15 29
− nd
+(4.6) +(3.2)
+(1.5) +(1.5)
Thailand Cambodia
18
22, M
5 9
DEN-1 nd
-(0.2) +(2.5)
−(0.2) −(0.9)
Tahiti
19
26, M
6 13
DEN-2 nd
+(2.1) +(3.1)
+(1.1) +(1.8)
Thailand
20
51, M
4 9
DEN-2 nd
-(0.8) +(4.0)
−(0.1) −(0.3)
Philippines
21
32, F
8 16
− −
+(3.0) +(3.5)
+(1.3) +(1.6)
Cambodia
22
24, F
9 23
− nd
+(3.4) +(2.8)
+(1.7) +(1.7)
India
23
28, F
7 8
− nd
+(3.7) +(6.6)
nd −(0.4)
Thailand Cambodia
24
22, M
4 16
DEN-1 nd
−(0.7) +(7.6)
−(0.1) +(10.2)
India
25
26, F
8 23
DEN-1 nd
+(5.7) +(8.6)
−(0.4) +(6.5)
Thailand
26
28, F
7 16
DEN-1 nd
+(4.9) +(7.7)
−(1.0) +(1.8)
Thailand
27*
24, F
10 20
− nd
+(1.3) +(1.1)
+(2.0) +(2.0)
Philippines
28
19, M
6 16
− nd
+(4.1) +(6.5)
-(1.0) +(8.4)
Thailand
29
27, M
6 13
DEN-1 nd
−(0.8) +(5.6)
−(0.1) +(1.3)
Cambodia
30
21, F
5 6 8
DEN-3 nd nd
−(0.7) +(2.0) +(3.8)
−(0.4) −(0.9) +(1.2)
Philippines
31
25, M
2 7
DEN-1 nd
−(0.7) +(6.8)
−(0.2) −(0.1)
Thailand
32
27, F
4 7
DEN-1 nd
−(0.8) +(5.1)
−(0.2) +(1.1)
Thailand
33 28, F 9 − +(8.5) +(7.9) Thailand
34
25, F
7 29
DEN-1 nd
+(4.9) +(7.0)
+(1.3) +(7.0)
Thailand Laos
35
64, M
6 16
− nd
+(14.1) +(18.6)
+(6.9) +(8.7)
Myanmar Thailand
*: secondary infection −: not detected nd: not done Note: Numbers in parentheses are index values. The values greater than 1.0 were determined to be positive.

The Features of Imported Dengue Fever Cases Confirmed at NIID, Japan, during 2001
Dengue Bulletin – Vol 27, 2003 5
Discussion Dengue virus infection is a serious cause of morbidity and mortality in most countries in the tropical and subtropical areas of the world(8,9). Dengue is considered to be one of the most important infectious diseases in these regions. The cases that we confirmed to be of dengue at our laboratory accounted for only a part of the total imported cases in Japan. Nearly 5 million Japanese visit countries in the tropical and subtropical areas annually, and 2 million people visit Japan from these areas. Therefore, DF/DHF is one infectious disease that should attract more attention in Japan.
Acknowledgement We thank doctors of clinics and hospitals who provided serum samples for the laboratory diagnosis of dengue. This work was supported by grants from Research on Emerging and Re-emerging Infectious Diseases of the Ministry of Health and Welfare, Japan, and from Global Environment Research Coordination System, Ministry of the Environment, Japan, and by the Cooperative Research Grant 2001 (13-A-3) of the Institute of Tropical Medicine, Nagasaki University, Japan.
References1. Hotta S. Twenty years of laboratory experience
with dengue virus. In:Saunders M, Lennette EH eds. Medical and Applied Virology. St Louis, 1964: 228-256.
2. Yabe S, Nakayama M, Yamada K, Kitano T, Arai Y, Horimoto T, Masuda G, Mitou A and Tashiro M. Laboratory virological diagnosis of imported dengue cases. J Jap Assoc Infect Dis (In Japanese), 1996, 70: 1160-1169.
3. Yamada K, Takasaki T, Nawa M, Nakayama M, Arai Y, Yabe S, and Kurane I. The features of imported dengue fever cases from 1996 to 1999. Japanese Journal of Infectious Diseases, 1999, 52: 257-259.
4. Kurane I, Takasaki T, and Yamada K. Recent topics of flavivirus infections in Japan. Increase of imported dengue cases and isolation of tick-borne encephalitis virus. Emerging Infectious Diseases, 2000, 6: 569-571.
5. Yamada K, Takasaki T, Nawa M, Nakayama M, Arai YT, Morimoto K, Yabe S, and Kurane I. Demographic features of imported dengue fever cases serodiagnosed in Japan during 2000. Dengue Bulletin, 2000, 24: 42-45.
6. Yamada K, Takasaki T, Nawa M and Kurane I. Laboratory diagnosis of imported dengue cases. Jap J Trop Med Hyg, 1999, 27: 75-77.
7. Yamada K, Nawa M, Takasaki T, Yabe S and Kurane I. Laboratory diagnosis of dengue virus infections by reverse transcriptase polymerase chain reaction (RT-PCR) and IgM-capture enzyme-linked immunosorbent assay (ELISA). Jap J Infect Dis, 1999, 52:150-155.
8. Monath TP. Dengue: The risk to developed and developing countries. Proc Natl Acad Sci USA, 1994, 91: 2395-2400.
9. World Health Organization: Dengue haemorrhagic fever: diagnosis, treatmant and control. World Health Organization, Geneva, 1997: 12-23.

6 Dengue Bulletin – Vol 27, 2003
Towards Sustaining Behavioural Impact in Dengue Prevention and Control
by E Renganathan*, W Parks*, L Lloyd**, MB Nathan***, E Hosein*, A Odugleh*,
GG Clark+, DJ Gubler++, C Prasittisuk+++, K Palmer++++ and J-L San Martín+++++
*WHO Mediterranean Centre for Vulnerability Reduction, Tunis, Tunisia **Consultant, 3443 Whittier Street, San Diego, CA 92106, USA
***WHO, HQ, Geneva, Switzerland +Dengue Branch, Centers for Disease Control and Prevention, San Juan, Puerto Rico
++Division of Vector-Borne Infectious Diseases, Centers for Disease Control and Prevention, Fort Collins, USA +++WHO South-East Asia Regional Office, New Delhi, India
++++WHO Western Pacific Regional Office, Manila, Philippines +++++PAHO/WHO, Panama City, Panama
Abstract International recognition of the vital importance of social mobilization for prevention and control of dengue fever and dengue haemorrhagic fever has gathered pace in recent years. At the beginning of 2001, an international team of social scientists, communication specialists, and national programme managers were brought together to prepare a step-by-step guide on how to plan and manage sustainable interventions addressing behavioural issues associated with the prevention and control of DF/DHF (Planning Social Mobilization and Communication for Dengue Prevention and Control: A Step-by-Step Guide, Ed. Will Parks and Linda S Lloyd, WHO, 2004, in press, WHO/CDS/WMC/2004.2). In the first half of 2002, the draft guide was reviewed by a panel of international experts in the fields of dengue prevention and control, vector control, the diverse social sciences, and dengue programme management. Funds from the WHO Mediterranean Centre for Vulnerability Reduction and a Director’s Initiative Grant from the Special Programme for Research and Training in Tropical Diseases supported the writing and review process. The guide was revised, translated into Spanish, and pre-tested at two regional workshops, funded by the U.S. Centers for Disease Control and Prevention. The first workshop was held in the WHO Western Pacific Region (in partnership with the WHO South-East Asia Region) and the second was held in the Region of the Americas in partnership with the Pan American Health Organization and the Environmental Health Project of the United States Agency for International Development. The workshops, held in the first half of 2003, provided additional feedback and enabled final editorial changes to be made to the document.
This paper provides a brief overview of the guide’s purpose and content, and the progress made so far in responding to the international call for the preparation of a package of tools, approaches and guidelines that will assist national programmes in the design and implementation of appropriate behaviour change interventions.
Keywords: Social mobilization, behavioural impact, Aedes aegypti, dengue prevention and control.

Towards Sustaining Behavioural Impact in Dengue Prevention and Control
Dengue Bulletin – Vol 27, 2003 7
Introduction Dengue fever (DF) and its more severe form, dengue haemorrhagic fever (DHF), are causing ever-increasing levels of illness and death. An estimated 50 million dengue infections occur every year, including 500,000 cases of DHF that require hospitalization – equivalent to approximately one DHF case every minute. At least 21,000 deaths from DHF occur every year, mostly among children – equivalent to one young life lost to DHF every 25 minutes. Some 40% of the world’s population (2.5 billion people) now live in areas where transmission occurs. The disease is endemic in the Americas, the Eastern Mediterranean, South-East Asia, the Western Pacific, and in tropical areas of Africa. Recent research shows that the global burden of dengue could be in the same order of magnitude as many other infectious diseases such as malaria, tuberculosis, and sexually transmitted infections (excluding HIV/AIDS), the prevention and control of which receive far greater political and financial support than dengue(1,2).
To date, no specific medications are available for the treatment of dengue although early diagnosis and timely and appropriate clinical management of DHF can reduce case fatality rates. Vaccine candidates effective against all four virus serotypes are under development. However, their availability for public health use is at least several years away. Even then, it is likely that they will only complement rather than replace existing prevention and control measures. For the time being, the only methods for preventing and controlling DF/DHF are to control the mosquito
vector(s) and to reduce human–vector contact. A range of Aedes control methods now exist, many of which have been tried and proven for different situations (Box 1).
Box 1. Aedes Control Methods • Environmental sanitation measures to
reduce mosquito breeding sites, such as the physical management of water containers (e.g. mosquito-proof covers for water storage containers, polystyrene beads in water tanks), better designed and reliable water supplies, and recycling of solid waste such as discarded tyres, bottles, and cans.
• Biological methods (e.g. fish, copepods – small crustaceans that feed on mosquito larvae) to kill or reduce larval mosquito populations in water containers.
• Chemical methods against the mosquito’s aquatic stages for use in water containers (e.g. temephos sand granules).
• Chemical methods directed against adult mosquitoes, such as insecticide space sprays or residual applications.
• Personal protection through use of repellents, vaporizers, mosquito coils, and insecticide-treated screens, curtains, and bednets (for daytime use against Aedes).
Among those methods, there is often heavy reliance on space spraying of insecticide for adult mosquito control. This method must be repeated at frequent intervals, its cost is high, and its effectiveness is variable(3). The main vector, Aedes aegypti prefers to rest inside houses, typically in sheltered places such as dark corners and cupboards, where drifting insecticide spray droplets do not easily penetrate when the aerosol is applied outdoors, especially if householders do not comply with requests to open their doors and windows. Moreover,

Towards Sustaining Behavioural Impact in Dengue Prevention and Control
8 Dengue Bulletin – Vol 27, 2003
adult mosquito populations quickly rebound after spraying because larval habitats remain largely unaffected(4). Nevertheless, public trust in such measures is often high and complacency only increases the challenge of explaining the need for community involvement in the control of larval habitats(5).
The global strategy Until effective, safe, and affordable vaccines become available, the Global Strategy for the Prevention and Control of Dengue Fever and Dengue Haemorrhagic Fever, enunciated in 1995, recommends the application of integrated vector control measures, with community and intersectoral participation(6). In 2002, the necessary political will for the strategy’s implementation was formally reflected by the 55th World Health Assembly’s adoption of a Resolution on “Dengue fever and dengue haemorrhagic fever prevention and control” (Resolution WHA55.17)(7). The Strategy consists of five main elements (Box 2).
Most endemic Member Countries in WHO South-East Asia and Western Pacific Regions have prepared their action plans based on the Global (and Regional) Strategy and using the available infrastructure and resources. The Pan American Health Organization (PAHO) has drawn up guidelines for its Member countries, recommending that they introduce and promote more intersectoral actions in their prevention and control programmes(8,9). Many countries have embraced this approach and have incorporated it into their programmes.
Box 2. The Global Strategy for Prevention and Control of DF/DHF
• Selective, integrated mosquito control with community and intersectoral participation, in which control is directed towards geographical areas at highest risk of transmission, integrating all appropriate methods in the most cost-effective and economical manner;
• Active disease surveillance based on strong health information systems, involving clinical and laboratory-based dengue surveillance for early detection of epidemics and vector surveillance for monitoring and evaluation of control programmes;
• Emergency preparedness, necessitating development of emergency and contingency plans, including education of the medical community, hospitalization plans, case management, and emergency vector control;
• Capacity building and training, in surveillance, laboratory diagnosis, case management, and vector control at professional, supervisory, technical, and field levels; and
• Vector control research, including studies on vector biology and control, disease relationships, design and management of control programmes, including social and economic approaches, and cost–benefit analyses.
The need for behaviourally-focused social mobilization and communication To date, ministries of public health in the majority of dengue-endemic countries (and those countries prone to epidemics) have

Towards Sustaining Behavioural Impact in Dengue Prevention and Control
Dengue Bulletin – Vol 27, 2003 9
been unable to mount effective and sustainable behaviour change interventions with community involvement. Social mobilization and communication strategies for dengue prevention and control and the research results that form the basis for these strategies, have been largely the pursuit of individual social scientists, university departments and nongovernmental organizations (NGOs) implementing studies or field trials that are peripheral to national programme goals. Such strategies have tended to focus at the household and community levels, with less emphasis being given to broader social changes needed in such domains as urban planning, municipal services such as water supply and solid waste management, industry, and government institutions.
At an Informal Consultation held at WHO headquarters, Geneva, in 1999, dengue experts called for the preparation of a package of tools, approaches and guidelines that will assist national programmes in the design and implementation of appropriate behaviour change interventions(10). Early in 2001, an international team of social scientists, communication specialists, and national programme managers were brought together to prepare a step-by-step guide on how to plan and manage sustainable interventions addressing behavioural issues associated with the prevention and control of DF/DHF (Planning Social Mobilization and Communication for Dengue Prevention and Control: A Step-by-Step Guide, Ed. Will Parks and Linda S Lloyd, WHO, 2004, in press, WHO/CDS/WMC/2004.2).
In the first half of 2002, the draft guide was reviewed by an international panel of
experts in the fields of dengue prevention and control, vector control, the diverse social sciences, and dengue programme management. Funds from the WHO Mediterranean Centre for Vulnerability Reduction (WMC) and a Director’s Initiative Grant from the Special Programme for Research and Training in Tropical Diseases (TDR) supported the writing and review process. The guide was revised, translated into Spanish, and pre-tested at two regional workshops funded by the US Centers for Disease Control and Prevention (CDC). The first workshop was held in the WHO Western Pacific Region, in partnership with the WHO South-East Asia Region, and the second was held in the WHO Region of the Americas (in partnership with the Pan American Health Organization (PAHO) and the Environmental Health Project of the United States Agency for International Development (USAID). The workshops, held in the first semester of 2003, provided additional feedback and enabled final modifications to be made to the document.
Planning social mobilization and communication for behavioural impact: A step-by-step guide For the first time in relation to dengue, this guide offers a comprehensive and innovative managerial insight to planning social mobilization and communication for behavioural impact. The guide is intended for programme managers and individuals, NGOs, and other agencies with interests and/or expertise in integrating biological, chemical, environmental, and communication

Towards Sustaining Behavioural Impact in Dengue Prevention and Control
10 Dengue Bulletin – Vol 27, 2003
interventions to prevent and control DF/DHF. Some countries have produced or are currently producing national guidelines on community participation, behaviour change communication, and social mobilization for dengue prevention and control. It was felt that this WHO guide would contribute to the development and support of these local initiatives by demonstrating a breadth of international experiences.
A key aspect of the guide is its focus on measurable behavioural changes resulting from well-planned social mobilization and communication actions. The guide uses the “Communication for Behavioural Impact” (COMBI) model for planning, although examples of other effective planning models are described in Tool 4 of the guide’s “Toolbox.” The planning process is divided into a 15 step-by-step process (Box 3) illustrated with real-life examples taken from 12 detailed case studies of current dengue programmes from around the world(11).
The guide itself is divided into 16 sections. The first 15 sections explain specific tasks and issues associated with each COMBI Planning step. The authors offer suggestions, examples, and lessons learnt to help the reader successfully complete each step. Three essential managerial tasks will be accomplished if these 15 steps are successfully followed. First, clear behavioural objectives will be established. Second, the strategic roles of a variety of social mobilization and communication disciplines – for example, public relations, advocacy, administrative mobilization, community mobilization, advertising, interpersonal communication, and point-of-service promotion – in achieving and sustaining these objectives will be determined. And
third, these disciplines will be combined in a comprehensive plan that provides clarity, consistency, and maximum behavioural impact to social mobilization and communication efforts. Section 16 offers some final words of advice from several programme teams who have advanced the field of dengue prevention and control in recent years.
Box 3. Fifteen Steps of COMBI Planning
(1) Assembling a multidisciplinary planning team;
(2) Stating preliminary behavioural objectives;
(3) Planning and conduct formative research;
(4) Inviting feedback on formative research;
(5) Analysing, prioritizing, and finalizing behavioural objectives;
(6) Segmenting target groups;
(7) Developing the strategy;
(8) Pre-testing behaviours, messages, and materials;
(9) Establishing a monitoring system;
(10) Strengthening staff skills;
(11) Setting up a system to manage and share information;
(12) Structuring the programme;
(13) Writing a strategic implementation plan;
(14) Determining the budget, and
(15) Conducting a pilot test and revising the strategic implementation plan.
Five tools are also included in the guide: Tool 1 is a comprehensive annotated bibliography of journal and book references and useful web sites; Tool 2 describes key stages in the conduct of formative research

Towards Sustaining Behavioural Impact in Dengue Prevention and Control
Dengue Bulletin – Vol 27, 2003 11
on DF/DHF; Tool 3 is a “strengths and weaknesses” checklist for use during formative research on the status of dengue programmes; Tool 4 offers six different approaches to setting behavioural objectives; and Tool 5 provides 10 ideas for achieving the optimum budget for social mobilization and communication.
Dengue-COMBI in action An additional result of the regional workshops was the development of detailed social mobilization and communication plans (COMBI plans) by multidisciplinary teams from each country participating in the workshops. Teams included senior level ministry of health officials from the departments of epidemiology, vector control/national dengue control programme, health education/communications, and entomology. Included in the CDC workshop funding was a US$ 50,000 start-up grant for one of the four participant countries in the Americas (Costa Rica, Dominican Republic, Guatemala, and Nicaragua).
Countries were informed that a competitive process would be held, with the COMBI plans scored by a group of experts knowledgeable of the COMBI process. In addition to the COMBI plan, each Ministry of Health was required to submit a letter of support indicating that the ministry would support implementation of the project through in-kind expenses as described in the plan. Of the four Central American countries, two have received funding to date: Guatemala – recipient of the US$ 50,000 CDC start-up funds (funding is almost 100% of that requested, US$ 57,721) and Nicaragua – recipient of a grant from the
PAHO Country Office (funding is 100% of that requested, US$ 15,475). In the WHO Western Pacific and South-East Asia Regions (Cambodia, Indonesia, Lao People’s Democratic Republic and Thailand), funding was secured from USAID for the Laos dengue-COMBI plan.
The COMBI guide has received much interest and positive feedback from dengue experts, particularly from dengue programme staff participating in the workshops. As a result of this interest, PAHO has secured funds to conduct a second COMBI workshop for the remaining countries in Central America (Belize, El Salvador, Honduras and Panama), scheduled for the end of October 2003. The guide has also been used as part of the social science track of the Eighth International Dengue Prevention and Control course sponsored by PAHO and the Pedro Kourí Institute in Havana, Cuba, in August 2003. A dengue-COMBI training programme was recently conducted in Myanmar (supported by SEARO) and in September 2003 the Ministry of Health, Malaysia, sponsored another COMBI training programme that included national and provincial dengue programme staff. PAHO has adopted COMBI as the planning process for a new model of technical assistance for dengue (known as the Grupo Técnico, or GT-Dengue). Funds were recently received from the Canadian International Development Agency (CIDA) to pilot the Grupo Técnico concept. CDC has also provided additional funds for two further training workshops to be held in 2004 for 4 countries from the Andean region and 4 countries from the English-speaking Caribbean region, including support for one project in each region.

Towards Sustaining Behavioural Impact in Dengue Prevention and Control
12 Dengue Bulletin – Vol 27, 2003
Evaluations of the dengue-COMBI plans in Lao PDR, Nicaragua, Guatemala, and two plans developed at the 2004 workshops are expected to be conducted between 2004-2005. These evaluations will strengthen our collective insights into how to sustain behavioural impact and build programme capacity as well as strengthen ongoing
advocacy and fund-raising efforts in the prevention and control of DF/DHF. A special symposium on behavioural research and behaviour change interventions is to be included at the Second International Conference on DF/DHF in Havana, Cuba, 31 May to 3 June 2004. The guide will be officially launched at this symposium.
References
1. Meltzer MI, Rigau-Pérez JG, Clark GG, Reiter P and Gubler DJ. Using disability-adjusted life years to assess the economic impact of dengue in Puerto Rico: 1984–1994. American Journal of Tropical Medicine and Hygiene, 1998, 59: 265–271.
2. Gubler DJ and Meltzer M. Impact of dengue/dengue hemorrhagic fever on the developing world. Advances in Virus Research, 1999, 53: 35-70.
3. Gratz NG. Emergency control of Aedes aegypti as a disease vector in urban areas. Journal of the American Mosquito Control Association, 1991, 7: 353–365.
4. Reiter P. Status of current Aedes aegypti control methodologies. In: Halstead SB, Gomez-Dantes H, eds. Dengue: A worldwide problem, a common strategy. Proceedings of the International Conference on Dengue and Aedes aegypti community-based control. Mexico, Ministry of Health, 1992, 41–48.
5. Gubler DJ. Perspectives on the prevention and control of dengue haemorrhagic fever. Kaohsiung Journal of Medical Science, 1994, 10: 15–18.
6. World Health Organization. Report of the consultation on key issues in dengue vector control, toward the operationalization of a global strategy. Geneva, World Health Organization, 1996 (document CTD/FIL(DEN)/IC/96.1). For internet access, see: http://www.who.int/emc-documents/dengue/docs/whocdsdenic20001.pdf
7. For internet access, see: http://www.who.int/gb/ EB_WHA/PDF/WHA55/ea5519.pdf and http:// www.who.int/gb/EB_WHA/PDF/WHA55/ewha5517.pdf
8. Pan American Health Organization. Dengue and dengue haemorrhagic fever in the Americas: Guidelines for prevention and control. Washington, DC, Pan American Health Organization, 1994 (Scientific Publication No. 548).
9. Pan American Health Organization. A blueprint for action for the next generation: Dengue prevention and control. Washington, DC, Pan American Health Organization, 1999 (document OPS/HCP/HCT/139.99). For internet access see: http://www.paho.org/English/HCP/HCT/hct-136-99.pdf
10. World Health Organization. Strengthening implementation of the global strategy for dengue fever/dengue haemorrhagic fever prevention and control. Report of the Informal Consultation, 18–20 October 1999. Geneva, World Health Organization, 1999. For internet access, see: http://www.who.int/emc-documents/dengue/ whocdsdenic20001c.html
11. For information on COMBI, see: http://www.who.int/infectious-disease-report/2002/ behaviour.html and http://www.comminit.com/ pdf/Combi4-pager_Nov_14.pdf; and WHO [forthcoming]. Planning Communication-for-Behavioural-Impact (COMBI) Programmes for Health. Tunis, WHO Mediterranean Centre for Vulnerability Reduction.

Dengue Bulletin – Vol 27, 2003 13
Dengue in Jeddah, Saudi Arabia, 1994-2002
by
Mazen Fakeeh and Ali M Zaki
Virus Laboratory, Dr Solimon Fakeeh Hospital, Jeddah, Saudi Arabia
Abstract
Dengue virus (DEN-2) was first isolated from a fatal case of dengue haemorrhagic fever (DHF) in an adult in Jeddah, Saudi Arabia, in 1994. A surveillance system for dengue was established in 1994 and since then clinical, virological, serological and RT-PCR techniques were used to confirm dengue cases and, as a guide, to implement vector control measures in risk areas.
During February 1994-December 2002, a total of 1,020 suspected clinical cases were examined by laboratory methods. Dengue virus infection was confirmed in 319 (31.3%) cases, 209 by virus isolation and the rest by serological techniques. DEN-2, DEN-1 and DEN-3 were detected between 1994 and 2002 in that order of frequency. Using IgG immunofluorescent assay or haemagglutination–inhibition (HI) test, the prevalence of dengue reactive antibodies in the suspected group was confirmed in 515 (50.5%) of the 1,020 samples tested.
The application of reverse transcriptase-polymerase chain reaction (RT-PCR) on culture-positive blood samples gave a specificity and sensitivity of 100% and allowed rapid diagnosis within one day.
All cases that were diagnosed by laboratory methods as dengue had leucopenia, thrombocytopenia and elevated liver enzymes, ALT-AST. There were only two fatal cases; one of dengue haemorrhagic fever and another of dengue shock syndrome.
It can be said that: (i) three dengue serotypes (DEN 1, 2 and 3) were detected in Jeddah; (ii) nearly all cases were non-complicated, 99.4% of them were of dengue fever; (iii) prevalence of dengue antibodies was in 50.5% of all suspected cases; and (iv) RT-PCR is a rapid, sensitive and effective method for diagnosis.
Limited rains, active case-finding and effective anti-mosquito measures helped to bring the disease under control and were probably responsible for the very small numbers of new indigenous dengue cases after the 1994 outbreak.
Keywords: Dengue, dengue fever, Jeddah, Saudi Arabia.

Dengue in Jeddah, Saudi Arabia, 1994-2002
14 Dengue Bulletin – Vol 27, 2003
Introduction Dengue fever (DF), and its more severe form known as dengue haemorrhagic fever (DHF), is the most important arthropod-transmitted viral disease of humans in the world today with one third of the world's population at risk. Epidemics of a dengue-like disease appeared in the Arabian Peninsula in the late 18th century. The disease was described in Zanzibar, Dar es Salam, the East African coast, Arabia (Aden, Mecca, Madera), and Jeddah, in Saudi Arabia(1). In 1994, the dengue virus was isolated in Jeddah, Saudi Arabia, from a fatal case of DHF at the Dr Fakeeh Hospital(2). Active surveillance was established in 1994, based on clinical, followed by laboratory, methods to evaluate the prevalence and incidence of dengue, the serotypes detected, and the efficacy of the laboratory methods used for its diagnosis. This paper(2) reviews the surveillance data from 1994-1999; and this report extends these results to 2002 and adds data obtained by reverse transcriptase-polymerase chain reaction (RT-PCR).
Materials and methods
Case selection
All cases suspected of having dengue, with non-specific fever, with no localizing signs or symptoms, were examined clinically and blood samples collected when suspected cases were first seen.
Virus isolation
Blood samples were inoculated on C6/36 and after the seventh day, cells were examined for cytopathogenic effects (CPE) and also examined by indirect immuno-
flourescent assay (IFA) for detection of dengue antigen(3,4).
Serological methods
Haemagglutination-inhibition (HI) antibody method of Clarke and Casals(5) was modified for use in microtiter format. IgM capture ELISA was applied according to the method described by Kuno et al.(6). Antibodies of the IgG type were detected using IFA(7).
Nucleic acid
RT-PCR was done using commercial kits for the extraction of viral RNA, amplification of cDNA and detection of amplified products. Viral RNA was extracted from tissue culture supernatant or serum using Qiagen RNA kit (Qiagen Germany, catalogue number 29504). Primers and probes were as described by Lanciotti(8). RT-PCR was done using Qiagen one-step RT-PCR kit (Qiagen, Germany, catalogue number 210212) in 50 ul volumes.
Amplified products were detected, using DNA enzyme immunoassay (DEIA) (Dia Sorin Biomedica Saluggia, Italy) according to the manufacturer's instructions.
Results The number of clinically suspected cases was 1,020 (738 male and 282 female). Dengue virus infection was confirmed in 319 cases (31.3%). Virus isolation was obtained in 209 cases (65.5%) out of 319 cases and IgM capture ELISA detected 110 cases (34.5%). Three dengue serotypes, DEN-2, DEN-1 and DEN-3, were detected. Most of the cases (289, 90.6%) out of 319 were diagnosed in 1994 and the rest over the next eight years (Table 1).

Dengue in Jeddah, Saudi Arabia, 1994-2002
Dengue Bulletin – Vol 27, 2003 15
Table 1. Distribution of suspected and confirmed dengue cases, 1994–2002
Year Number of suspected
cases
Number of confirmed
cases 1994 673 289 1995 136 06 1996 57 02 1997 62 15 1998 31 00 1999 26 03 2000 17 00 2001 07 00 2002 11 04 Total 1020 319
The application of RT-PCR gave results comparable to virus isolation in all the samples that were tested. Typing of dengue isolates by RT-PCR, followed by hybridization using DEIA method gave the same results as culture followed by the use of type-specific monoclonal antibodies in an IFA (Table 2).
The prevalence of IgG antibodies by IFA assay showed 515 (50.5%) of the total tested cases (1,020) had IgG antibodies in the first sample submitted for laboratory diagnosis. IgM detected 110 cases, mostly by the end of the first week of infection.
Table 2. Results of RT-PCR followed by DEIA compared to gel electrophoresis after nested PCR and IFA following virus culture
Samples RT-PCR followed by DEIA
Nested PCR followed by gel electro-phoresis
Virus culture followed by IFA
detection
DEN-1 positive serum samples
28/28 28/28 28/28
DEN-2 positive serum samples
40/40 40/40 40/40
DEN-3 positive serum samples
12/12 12/12 12/12
Control negative serum samples
0/30 0/30 00/30
Dengue infected C6/36 cells
20/20 20/20 20/20
Dengue non-infected C6/36 cells
00/20 00/20 00/20
DEIA = DNA enzyme immunoassay, IFA = Indirect immunofluorescent assay

Dengue in Jeddah, Saudi Arabia, 1994-2002
16 Dengue Bulletin – Vol 27, 2003
Discussion and conclusions Dengue fever made its first appearance in Jeddah in 1994; by the end of the year, 289 cases had been diagnosed. Since that time, continuous surveillance showed that dengue was no longer endemic in Jeddah. Jeddah is a central area where a large number of pilgrims visiting Mecca transit every year for Haj (visiting Islamic holy places). The Haj provides a fertile opportunity for the introduction and exchange of infectious agents among pilgrims, including dengue viruses. Pilgrims come from many countries in South-East Asia, India, Indonesia, Malaysia, and Pakistan. Some of these persons may be in the incubation period of dengue infection and may actually be viremic during the time of Haj, infecting mosquitoes and subsequently infecting other pilgrims and residents. Also, pilgrims come from Africa, so in Jeddah and Mecca, there may be an exchange of dengue viruses among pilgrims. However, the little (less than 60 mm/year) rain and dry weather most of the year does not favour efficient spread of dengue. A case-control study indicated that water storage container facilities in or near construction sites were the focal points of dengue virus transmission in Jeddah as, in spite of the low rainfall, water storage containers served as the breeding sites for Aedes aegypti, the vector species(12).
It was during 1994 that two DEN-2 isolates were obtained and one of these was from a fatal haemorrhage case. Immediately after the isolation of DEN-2 virus surveillance was established by the Ministry of Health and information and guidelines were passed on to clinicians in the region. Clinically-suspected cases based on WHO criteria were sampled and blood was tested at the Dr Solimon Fakeeh Hospital by virus
isolation, IgM capture ELISA, and finally by an IFA (later RT-PCR was applied). Clinically, all cases were found to be of non-complicated dengue fever, except for two cases that were fatal. Despite the high prevalence of dengue antibody in the examined suspected cases, among the confirmed cases only these two showed DHF or DSS. Inoculation of acute phase sera on C6/36 cells detected 209 cases, mostly in the first days of the disease, a common finding elsewhere(4,9,13,14). Most of the confirmed cases were adults between 15-40 years of age and there were more male than female, a pattern consistent with the exposure at construction sites in Jeddah. The male/female ratio was similar to observations made in other dengue endemic areas in Brazil, Puerto Rico and, more recently, in the Philippines.
Three dengue serotypes were detected over the nine-year period from 1994 to 2002; DEN-2 (138 cases), DEN-1 (58 cases), and DEN-3 (13 cases). There were no DEN-4 isolates. The paucity of cases of DHF in the population in Jeddah could be attributed to factors such as viral, racial or nutritional.
Typing of the disease in this study was done using specific monoclonal antibodies(3,4). Most isolates were in 1994 (186) and the rest of the isolates were in the following eight years. IgM capture ELISA detected 110 cases that were culture negative, presumably because of the delay in collecting the blood samples. Samples were often taken by the end of the first week of the presentation of symptoms and signs. The IgM ELISA has a high sensitivity and specificity for dengue infection(9,10,11). Application of RT-PCR, followed by DNA enzyme immunoassay for the detection of amplified products, gave comparable results

Dengue in Jeddah, Saudi Arabia, 1994-2002
Dengue Bulletin – Vol 27, 2003 17
to virus isolation on tissue culture followed by typing with monoclonal antibodies. The main advantages of the RT-PCR method is its rapidity, done in one day, sensitivity and specificity of diagnosis(8).
The city of holy Mecca is 75 km from Jeddah. During Haj, large numbers of pilgrims come from disease-endemic areas all over the world, with the possibility of introduction of dengue viruses. Rapid and frequent travel between Jeddah and other endemic areas of the world favours the continued introduction of other strains and serotypes.
It is important to maintain dengue surveillance at high levels in order to detect early dengue activity and to take effective steps for the control of the vector.
Acknowledgements We thank Dr Robert E. Shope of the University of Texas Medical Branch at Galveston for his encouragement in this work and for reviewing the manuscript. We also thank Miss Amany Ibrahim Yousef for her technical assistance.
References
1. Gubler DJ. Dengue and dengue haemorrhagic fever: Its history and resurgence as a global health problem in DJ Gubler and G Kuno ed. Dengue and dengue haemorrhagic fever. CAB International, Willingford, Oxon, OX 10 8DE.UK, 1997: 1-22.
2. Fakeeh M and Zaki AM. Virologic and serologic surveillance for dengue fever in Jeddah, Saudi Arabia. The American Journal of Tropical Medicine and Hygiene, 2001, 65: 764-767.
3. Henchal EA, Mc Cown JM, Seguin MC, Gentry MK and Brandt WE: Rapid identification of dengue virus isolates by using monoclonal antibodies in an indirect immunofluorescent assay. American Journal of Tropical Medicine and Hygiene, 1983, 32: 164-169.
4. Gubler DJ, Kuno G, Sather GE, Velez M and Oliver A. Mosquito cell culture and specific monoclonal antibodies in surveillance for dengue viruses. American Journal of Tropical Medicine and Hygiene, 1984, 33: 158-165.
5. Clarke DH and Casals J. Techniques for hemagglutination and hemagglutination inhibition with arthropod-borne viruses. American Journal of Tropical Medicine and Hygiene, 1958, 7: 561-573.
6. Kuno G, Gomez I and Gubler DJ. An ELISA procedure for the diagnosis of dengue infection. Journal of Virological Methods, 1991, 33: 101-113.
7. Shope R and Sather G. Arboviruses. Lennette EH, Schmidt NJ eds Diagnostic procedures for viral, rickettsial, and chlamydial Infections. Fifth edition Washington DC: American Public Health Association, 1979: 767-814.
8. Lanciotti RS, Calisher CH, Gubler DJ and Vorndam AV. Rapid detection and typing of dengue viruses from clinical samples using reverse transcriptase-polymerase chain reaction. J Clin Microbiology, 1992, 30: 545-551.
9. Gubler DJ and Sather G. Laboratory diagnosis of dengue and dengue haemorrhagic fever. Proceedings of the international symposium on yellow fever and dengue. Rio de Janiero, Brazil May 15-19, 1988.
10. Innis BL, Nisalak A, Nimmannitya S, Kusalerdchariya S, Chongswadi V, Suntayakorn S, Puttisri P and Hoke CH. An enzyme linked immunosorbent assay to characterize dengue infections where dengue and Japanese encephalitis co-circulate. American Journal of Tropical Medicine and Hygiene, 1989, 40: 418-427.

Dengue in Jeddah, Saudi Arabia, 1994-2002
18 Dengue Bulletin – Vol 27, 2003
11. Cardosa MJ, Tio PH, Nimmannitya S, Nisalak A and Innis B. IgM capture ELISA for detection of IgM antibodies to dengue virus: Comparison of 2 formats using hemagglutinins and cell culture derived antigens. South-East Asian Journal of Tropical Medicine and Public Health, 1992, 23: 726-729.
12. Ghaznawi HI, Al-Khateeb TO, Akbar N, Afifi H and Nasser A. Surveillance for dengue fever in Jeddah. Eastern Mediterranean Health Journal, 1997, 3: 567-570.
13. Technical Advisory Group on dengue haemorrhagic fever/dengue shock syndrome. Dengue haemorrhagic fever diagnosis, treatment and control. Geneva, Switzerland: World Health Organization, 1986.
14. Chungue E, Burucoa C, Boutin JP, Philippon G, Laudon F, Plichart R, Barbazan P, Cardines R and Roux J. Dengue 1 epidemic in French Polynesia, 1988-1989: Surveillance and clinical, epidemiological, virological and serological findings in 1,752 documented clinical cases. Transactions of the Royal Society of Tropical Medicine and Hygiene, 1992, 86: 193-197.

Dengue Bulletin – Vol 27, 2003 19
Dengue Haemorrhagic Fever in Taiwan
by Jien-Wei Liu*, Boon-Siang Khor*, Chen-Hsiang Lee*, Ing-Kit Lee*,
Rong-Fu Chen** and Kuender D Yang**# *Division of Infectious Diseases, Department of Internal Medicine,
Chang Gung Memorial Hospital-Kaohsiung, Taiwan **Department of Pediatrics, Chang Gung Memorial Hospital-Kaohsiung, Taiwan
Abstract
A large outbreak of dengue fever occurred in Taiwan during 2001. There were more than 5,000 cases with dengue infections. Out of these, 120 patients were diagnosed as cases of dengue haemorrhagic fever (DHF) and admitted to the medical centre in Kaohsiung, Taiwan. This epidemic was caused by dengue virus DEN-2, following a previous large DEN-1 outbreak without the occurrence of DHF cases in the same areas, between 1987 and 1988. This observation provides an epidemiological evidence for the existence of the heterotypic secondary immune enhancement of DHF infections. In contrast to the predominance of paediatric patients with DHF in South-East Asia, all the patients with DHF in this series were adults, except for one patient who was 17 years old. The reason for the age difference in epidemics in different geographical locations is not clear. It might result from the differences in race and/or the virulence of the virus strains. It was also found that certain abnormal laboratory findings, including atypical lymphocytosis (56.3%), activated partial thromboplastin time prolongation (APTT) (97.5%), aspartate aminotransferase (94.9%), and alanine aminotransferase (80.7%), were significantly higher in patients with DHF than those with DF. The fact that patients with DHF had a significantly higher APTT but not prothrombin time (PT) suggests that vascular insults and not hepatic insufficiency contribute to patients with DHF. Further studies are needed to explore whether abnormal APTT can be a good predictor for early diagnosis of DHF.
Keywords: DF/DHF, DEN-2, activated partial thromboplastin time prolongation (APTT), Taiwan.
# For correspondence: [email protected]
Introduction
Dengue virus (DEN) is a mosquito-borne flavirirus and the most prevalent arbovirus in tropical and subtropical regions of the globe. This infectious disease is now widely
distributed in many countries in South-East and South Asia, Central and South Americas, and the Western Pacific(1). As for Taiwan, a number of dengue epidemics have occurred since the 1980s(2,3,4,5). Among the recent dengue epidemics on this island, one large

Dengue Haemorrhagic Fever in Taiwan
20 Dengue Bulletin – Vol 27, 2003
outbreak was recorded between 1987 and 1988 in southern Taiwan, which was caused by DEN-1(3), and a small number of clustered cases of dengue fever (DF) have been reported from this region ever since(6). A large dengue epidemic caused by DEN-2 emerged late in 2001 in the same regions where a dengue outbreak had occurred in 1987-1988, namely, the Kaohsiung city, Kaohsiung county and Pingtung county (Pingtung city has had the least number of cases) in southern Taiwan. There have been more than 5,000 cases of symptomatic dengue infections based on the passive surveillance in this epidemic, where there were many more cases of dengue haemorrhagic fever (DHF) than in the previous ones. To better understand the changing characteristics of dengue virus infections in Taiwan, we herein report the results of a hospital-based study on the patients with DHF admitted to Chang Gung Memorial Hospital-Kaohsiung (CGMH-KS), a 2,500-bed facility serving as a primary care and tertiary referral centre in southern Taiwan.
Materials and methods
Data collection of clinical manifestations
All the patients with suspected dengue fever who came to Chang Gung Memorial Hospital at Kaohsiung were localized in a certain area with appropriate vector control strategy in place. The staff of nosocomial infection control used a special chart for data collection, including demographic data, past
history and clinical manifestations. The patients with definite DF and DHF as described below were coded for analysis.
Diagnosis of DF and DHF
Patients with DF were confirmed by either positive reverse-transcriptase polymerase chain reaction (RT-PCR) detection of DEN-2 infections, positive enzyme-linked immunosorbent assay (ELISA) of specific dengue IgM in acute phase serum, or fourfold increase of dengue-specific haemagglutination inhibition titers in convalescent serum, as previously described(6,7). The quality assurance of the diagnostic tests was re-confirmed by the Center for Disease Control, Taiwan. The diagnosis of DHF was based on the criteria showing dengue fever complicated with reduced platelets (<100,000/mm3), petechial or haemorrhagic manifestations, and plasma leakage showing haemoconcentration =20%, pleural effusion, ascites or hypoalbuminemia(8).
Results A total of 450 patients with definite DF in this series were collected for analysis. One-hundred-and-twenty of the patients hospitalized fulfilled the criteria for DHF based on the WHO criteria(8), and were enrolled for analysis. As shown in Table 1, patients with DHF usually had fever and haemorrhagic manifestations. Only 5.8% patients developed shock although most patients had pleural effusion, ascites or hypoalbuminemia. The first three common

Dengue Haemorrhagic Fever in Taiwan
Dengue Bulletin – Vol 27, 2003 21
manifestations of bleeding were skin petechia (72.5%), gastrointestinal bleeding (29.4%) and gum bleeding (25.9%) (Table 2). To our surprise, epitaxis was not common in this study series. Based on these clinical presentations, it is not easy to differentiate between patients with DF and DHF, even between DF and other viral infections, particularly when other infectious aetiology concurrently prevails(9). As a result, we have further analysed laboratory data to investigate whether patients with DHF had unique parameters for early diagnosis.
Table 1. Clinical manifestations of 120 patients with DHF
Symptom and sign No. of patients
%
Fever 109 90.8
Bone pain 69 57.5
Abdominal pain 60 50.0
Headache 55 45.8
Cough 47 39.2
Skin rash 50 26.7
Arthralgia 23 19.2
Dizziness 13 10.8
Myalgia 14 11.7
Retro-orbital pain 13 10.8
Haemorrhage* 109 90.8
Shock 10 5.3
*Patients with DHF other than Grade I; see Table 2 for detailed haemorrhagic sites.
Note: An individual patient might have more than one symptom and/or sign.
Table 2. Haemorrhagic patterns of 109 patients with DHF other than Grade I
Haemorrhagic pattern
No. of patients %
Petechia 79 72.5
Gastrointestinal bleeding
32 29.4
Gum bleeding 28 25.9
Haemoptysis 11 10.1
Haematuria 11 10.1
Retinal haemorrhage 3 2.8
Subconjunctival haemorrhage
2 1.8
Vaginal bleeding 2 1.8
Epistaxis 2 1.8
Note: An individual patient might have more than one haemorrhagic pattern.
As shown in Table 3, of the 120 patients with DHF (11 Grade I, 102 Grade II, and 7 Grade III/IV), 62 were males and 58 females. The mean of their ages was 54.0 ± 13.6 years, and the median was 55 years, ranging from 17 to 88 years. The rates of laboratory abnormality of patients having DHF were compared with those of the patients having DF in our hospital, and are shown in Table 3. Chi-square of Fisher’s exact test was used for comparison, and a two-tailed P<0.05 was considered statistically significant. Of these 120 patients with DHF, leukopenia was found in 55.0%; leukocytosis in 4.2%; monocytosis in 27.7%; atypical lymphocytosis in 56.3%; activated partial thromboplastin time (APTT) prolongation (>20% than control) in 97.5%; elevated aspartate aminotransferase (AST) in

Dengue Haemorrhagic Fever in Taiwan
22 Dengue Bulletin – Vol 27, 2003
94.9%, and elevated alanine aminotransferase (ALT) in 80.7% of the patients. The rates of atypical lymphocytosis, APTT prolongation,
AST elevation and ALT elevation were significantly higher in patients with DHF than in those with DF (Table 3).
Table 3. Percentages of laboratory abnormality in DHF vs. DF
DHF DF
Variable No. of
patients/No. of patients with data available
%
No. of patients/No. of patients with data available
% P
Leukopenia (WBC< 4000/µL) 66/120 55.0 32/47 68.1 0.162
Leukocytosis (WBC >10000/µl) 5/120 4.2 3/47 6.4 0.689
Monocytosis (>12%) 31/112 27.7 13/43 30.2 0.843
Atypical lymphocytosis 63/112 56.3 13/43 30.2 0.004
APTT prolongation* 77/79 97.5 33/48 68.8 <0.001
PT prolongation† 2/66 2.0 1/47 2.1 0.626
AST elevation (> 40 IU/L) 94/99 94.9 19/33 57.6 <0.001
ALT elevation (> 40 IU/L) 71/88 80.7 17/33 48.6 0.002
*APTT prolongation was defined as >20% than control. †PT prolongation was defined as >3 sec than control; one patient had the underlying liver cirrhosis while another had acute hepatitis.
Discussion
Two major theories have been proposed to explain the pathogenesis of DHF, namely, the “antibody-dependent enhancement” (ADE) of infection theory(10) and the viral virulence theory(11,12). The ADE of infection theory is based on the epidemiological studies, mainly conducted in Thailand in 1960s-1970s, showing that DHF occurred predominantly in children having previous infection caused by DEN of different serotypes, especially in infants acquiring primary antibody from placenta transfer. According to this theory, the cross-reactive, non-neutralizing anti-bodies from a heterologous dengue virus
infection bind to the newly-infecting serotype and facilitate virus entry via Fc-receptor-bearing cells. This mechanism serves to increase the numbers of infected antigen-presenting cells during the second dengue episode, which can lead to the activation of pre-existing cross-reactive DEN-specific T-lymphocyte from the previous flavirirus infection. The self-amplifying cascade can, in turn, lead to the release of cytokines and chemical mediators that may cause plasma leakage accounting for the clinical manifestations of DHF. In contrast to predominant paediatric patients with DHF seen in South-East Asia, all the patients with DHF in this study, except one patient aged

Dengue Haemorrhagic Fever in Taiwan
Dengue Bulletin – Vol 27, 2003 23
17 years, were adults. Although we were uncertain if the patients in this series had a previous dengue virus infection, but in view of the presence of a dengue epidemic caused by DEN-1 in 1987-1988 in the same geographical locale, the possibility of experiencing a prior dengue episode by most of these patients was high. This observation supports the ADE of infection theory as pathogenesis of DHF. However, the age difference between patients with DHF from different geographical localities remains unclear. It might be due to differences in race and/or virulence of the virus strains.
The presence of monocytosis and atypical lymphocytosis indicating the aberrant immune activation in DHF was found in studies with a small number of specimens from patients with DHF(13,14,15). Our report disclosed the rates of this aberrant immune activation in a dengue epidemic caused by DEN-2. Likewise, this study unveiled the higher rates of APTT prolongation, as well as AST and ALT elevations in this dengue epidemic. Prolonged APTT as well as elevated AST and ALT were found in limited specimens from
patients with DHF(16,17). We are uncertain whether the higher rates of laboratory abnormalities in patients with DHF due to DEN-2 in Taiwan can be generalized to victims of DHF in epidemics caused by DEN of other serotypes or of other strains belonging to the same serotype, or in epidemics in other geographical locations where patients were genetically different. Further studies in other population groups are needed to elucidate this important information. A better understanding of these epidemiological implications will fortify the complementary role of the clinical-service-based laboratory data in making the diagnosis of DHF.
Acknowledgement
This study was in part supported by a grant (CMRP814) from Chang Gung Memorial Hospital at Kaohsiung. The authors would like to thank the staff of the Nosocomial Infection Control Section, Chang Gung Memorial Hospital at Kaohsiung, for their assistance in the collection of blood samples.
References 1. Gubler DJ. Dengue and dengue haemorrhagic
fever: Its history and resurgence as a global public health problem. In: Gubler DJ, Kuno G (ed.), Dengue and dengue haemorrhagic fever. CAB International, New York, NY, 1997, 1-22.
2. Wu YC. Epidemic dengue 2 in Liouchyou Hsiang, Pingtung County, in 1981. Chin J Microbiol Immunol, 1986, 19: 93-99.
3. Liu HW, Ho TL, Hwang CS and Liao YH. Clinical observations of virologically confirmed dengue fever in the 1987 outbreak in southern Taiwan. Kaohsuing J Med Sci, 1989, 5:42-49.
4. Wu YC. Epidemiology and control of Japanese encephalitis and dengue fever in Taiwan. Dengue Bulletin, 1996, 20: 51-54.
5. Harn MR, Chiang YL, Tian MJ, Chang YH and Ko YC. The 1991 dengue epidemic in Kaohsiung City. J Formos Med Assoc, 1993, 92 (suppl.): S39-43.
6. Shu PY, Chen LK, Chang SF, Yuen YY, Chow L, Chien LJ, Chin C, Yang HH, Lin TH and Huang JH. Potential application of nonstructural protein NS1 serotype-specific immunoglobulin G enzyme-linked immunosorbent assay in the seroepidemiological study of dengue virus infection: Correlation of results with those of the plaque reduction neutralization test. J Clin Microbiol, 2002, 40: 1840-1844.
Dengue Haemorrhagic Fever in Taiwan
24 Dengue Bulletin – Vol 27, 2003
7. Chen RF, Yeh WT, Yang MY and Yang KD. A model of the real-time correlation of viral titers with immune reactions in antibody-dependent enhancement of dengue-2 infections. FEMS Immunol Med Microbiol, 2001, 1278: 1-7.
8. Anonymous. Dengue haemorrhagic fever: Diagnosis, treatment and control. World Health Organization, Geneva, 1997.
9. Tofra AF, Defreitas RF, Smoak BL, Kanesa-thasan N, King AD, Burrous JM, McCarthy PO, Rossi C and Hoke CH Jr. Dengue fever in US military personnel in Haiti. JAMA, 1997, 277: 1546-1548.
10. Morens DM. Antibody-dependent enhancement of infection and the pathogenesis of viral disease. Clin Infect Dis, 1994, 19: 500-512.
11. Barnes WJS and Rosen L. Fatal hemorrhagic disease and shock associated with primary dengue infection on a Pacific island. Am J Trop Med Hyg, 1974, 23: 495-506.
12. Scott RM, Nimmannitya S, Bancroft WH and Mansuwan P. Shock syndrome in primary dengue infections. Am J Trop Med Hyg, 1976, 25: 866-874.
13. Liu CC, Huang KJ, Lin YS, Yeh TM, Liu HS and Lei HY. Transient CD4/CD8 ratio inversion and aberrant immune activation during dengue virus infection. J Med Virol, 2002, 68: 241-252.
14. Fadilah SA, Sahrir S, Raymond AA, Cheong SK, Aziz JA and Sivagengei K. Quantitation of T lymphocyte subsets helps to distinguish dengue haemorrhagic fever from classic dengue fever during the acute febrile stage. South-east Asian J Trop Med Publ Health, 1999, 30: 710-717.
15. Lei HY, Yeh TM, Liu HS, Lin YS, Liu SH and Liu CC. Immunopathogenesis of dengue virus infection. J Biomed Sci, 2001, 8: 377-388.
16. Huang YH, Liu CC, Wang ST, Lei HY, Liu HS, Lin YS, Wu HL and Yeh TM. Activation of coagulation and fibrinolysis during dengue virus infection. J Med Virol, 2001, 63: 247-251.
17. Kalayanarooj S, Vaughn DW, Nimmannitya S, Green S, Suntayakorn S, Kunentrasai N, Viramitrachai W, Ratanachueke S, Kiatpolpoj S, Innis BL, Rothman AL, Nisalak A and Ennis FA. Early clinical and laboratory indicators of acute dengue illness. J Infect Dis, 1997, 176: 313-321.

Dengue Bulletin – Vol 27, 2003 25
Dengue in Brazil: Past, Present and Future Perspective
by
Luiz Tadeu Moraes Figueiredo#
Vírus Research Unit of the School of Medicine of Ribeirão Preto, University of São Paulo, Av. Bandeirantes, 3900, 14049-900 Ribeirão Preto, SP, Brazil
Abstract
Brazil is the largest country in South America, with 165 million inhabitants largely exposed to dengue outbreaks in the last 16 years. Aedes aegypti was reintroduced in Brazil approximately 25 years ago. Following that, DEN-1, DEN-2 and DEN-3 outbreaks occurred in 1986, 1991 and 2001, respectively. These outbreaks started in Rio de Janeiro and spread to all regions of Brazil. With the continuous circulation of multi-serotypes, more than 2 million cases of dengue have been reported in Brazil in the last 16 years and more than 3,000 of these were cases of DHF/DSS. Vector control activities have not been able to control dengue transmission in the country. Thus, DHF has become a major public health problem in Brazil.
Keywords: Dengue outbreaks, DHF/DSS, major public health problem, Brazil.
#For correspondence: [email protected]
Introduction Brazil is the largest country in South America, with an area of 8,512,000 km2, mostly tropical, extensively covered by rain forests such as the Amazon, as well as by forests in the eastern and south-eastern coastal areas. The climate in most of the country is tropical with a large diversity of flora and fauna, suitable enough for the dissemination of zoonosis caused by arthropod-borne viruses. Brazil has a population of 165 million, most of them living in urban areas of large cities in the south-east and north-east regions. These
areas are infested by the mosquito Aedes aegypti and dengue has become an endemic disease in these urban centres.
Brazilian flaviviruses Presently, 11 flaviviruses are known to exist in Brazil: Bussuquara (BUS), Cacipacoré (CPC), dengue serotypes (DEN-1, DEN-2, DEN-3 and DEN-4), Iguape (IGU), Ilhéus (ILH), Rocio (ROC), Saint Louis encephalitis (SLE), and yellow fever (YF), including the wild virus and the 17DD vaccine strain(1). All flaviviruses are 60nm spherical enveloped

Dengue in Brazil: Past, Present and Future Perspective
26 Dengue Bulletin – Vol 27, 2003
viruses, with surface glycoprotein projections, possessing a single stranded RNA (+) genome, with approximately 11,000 nucleotides. The Flavivirus RNA contains a single open reading frame that encodes 10 proteins, as follows: 5'-C-preM-E-NS1-ns2a-ns2b-NS3-ns4a-ns4b-NS5-3'(2). A phylogenetic study based on 124 nucleotides of NS5 gene and 145 nucleotides of the 3’non-coding region showed that most of the Brazilian flaviviruses are included into two clades, one containing the dengue viruses and another including the Asiatic Japanese encephalitis virus and the related ILH, ROC, SLE and CPC. YF and IGU are still ungrouped and BUS was not included in this study(3).
Most of the Brazilian flaviviruses are maintained in nature as sylvatic zoonosis that only occasionally can attack man and domestic animals that come in contact with ecosystems where such viruses circulate(1). Dengue viruses constitute exceptions to this scenario, causing large urban epidemics(4). Likewise, there is a permanent risk of yellow fever re-urbanization into these cities, caused by the constant arrival of viremic patients from sylvatic areas(5).
History of dengue in Brazil Reports on dengue outbreaks in Brazil started in the 19th century. Mariano, in 1917(6), mentioned that an epidemic occurred in Rio de Janeiro in 1846. The disease was named polka because of the twitches that are characteristic of that dance, caused by myalgia and arthralgia in sick people. It is possible that dengue epidemics occurred in Rio de Janeiro more than once during the 19th
Century(7). Dengue outbreaks probably also occurred in the north-east and south regions of Brazil during the 19th century. Reis, in 1896(8), described the clinical picture of dengue cases that occurred during an outbreak in Curitiba, in south Brazil. Furthermore, in 1917, Mariano(6) reported an outbreak of dengue fever in the state of Rio Grande do Sul. Also, in 1923, Pedro(9) made an accurate description of the clinical manifestations of dengue fever on the basis of cases studied during the epidemic of 1922/1923, in Rio de Janeiro city.
In July 1981, following the spread of the dengue epidemics in Central America and the Caribbean, an outbreak occurred in Boa Vista, state of Roraima, Amazon region. It is presumed that 11,000 people were infected by DEN-1 or DEN-4; these two viruses were isolated from patients and from Aedes aegypti. The clinical presentation of the disease was a benign, non-specific viral fever and cases were reported until August 1982(10). The location where this outbreak occurred is shown in Figure 1.
During the last 16 years, Brazil suffered many dengue epidemics. The virus and the vector spread throughout the country and dengue outbreaks occurred in all regions including the most populated areas of Brazil. The first outbreak in the south-east of Brazil started in a town near Rio de Janeiro in March of 1986. Later, the virus spread into the metropolitan area of Rio de Janeiro. It was the beginning of a large epidemic caused by DEN-1(11). Approximately 95,000 cases of dengue were reported until 1987, and an estimated 3 million people became infected by dengue virus during this outbreak(12).

Dengue in Brazil: Past, Present and Future Perspective
Dengue Bulletin – Vol 27, 2003 27
Dengue in BrazilDengue types 1 and 4 - 1981Dengue type 1 – 1986Dengue type 2 – 1990Dengue type 3 - 2001
Rio deJaneiro
Boa Vista
North
Midwest
South
Southeast
Northeast
Dengue in BrazilDengue types 1 and 4 - 1981Dengue type 1 – 1986Dengue type 2 – 1990Dengue type 3 - 2001
Rio deJaneiro
Dengue in BrazilDengue types 1 and 4 - 1981Dengue type 1 – 1986Dengue type 2 – 1990Dengue type 3 - 2001
Rio deJaneiro
Boa Vista
North
Midwest
South
Southeast
Northeast
Dengue in Brazil DEN-1, DEN-4: 1981 DEN-1: 1986 DEN-2: 1990 DEN-3: 2001
The majority of the patients presented with either a benign undifferentiated febrile illness or the classic dengue fever, including severe headache, retro-bulbar pain, body aches, malaise, skin rash and pruritus. Haemorrhagic phenomena (epistaxis, intestinal bleeding) were rare(13). The epidemic spread toward the north-east of Brazil, with outbreaks in the states of Alagoas, in June 1986, and Ceará, in September 1986(14). Approximately 50,000
cases of dengue were reported in Ceará between 1986 and 1993(15). In the mid-west region of Brazil, DEN-1 caused an outbreak in 1987. From 1990 to 2002, DEN-1 outbreaks were reported in practically all regions of the country(14).
In April 1990, a new dengue epidemic started in the Rio de Janeiro metropolitan area. DEN-2 was then isolated for the first
Figure 1. Map of Brazil showing regions, sights where dengue outbreaks started and dengue viruses spreading

Dengue in Brazil: Past, Present and Future Perspective
28 Dengue Bulletin – Vol 27, 2003
time in Brazil (16). DHF/DSS represented 2% of the 17,000 total reported cases, with an uncertain number of fatalities(17). DHF/DSS cases were probably related to sequential infections. DEN-1 and DEN-2 have been circulating simultaneously in Rio de Janeiro in the last 12 years, and DEN-2 reached and caused outbreaks also in the northern region(18,19). DEN-2 spread and caused outbreaks in the Amazon region(20). This virus was introduced in north-east Brazil in 1994 and in the state of Ceará 27,000 cases were reported in three months. The occurrence of 26 DHF/DSS cases was confirmed and 14 patients died. DEN-1 was also isolated during the same outbreak(15). DEN-2 outbreaks have been reported in practically all regions of Brazil, in many cases associated to DEN-1, and at least one case of simultaneous infection by DEN-1 and DEN-2 has been described(14,21).
DEN-3 virus was isolated in Brazil for the first time in 1999, from a patient returning from Nicaragua (personal communication from Rocco IM, Adolfo Lutz Institute, 1999). This suggested that DEN-3 which circulated in Central America and in northern South America, could reach Brazil soon. In fact, in January 2001, the first reported Brazilian DEN-3 outbreak started in Rio de Janeiro(22). A massive outbreak has been in progress in Rio de Janeiro in 2002, with rapid spread to the north, north-east and south-east of Brazil(14). At the time of writing this paper in April 2002, hundreds of dengue cases are being reported daily in Brazil.
The spread of DEN-1, DEN-2 and DEN-3 in Brazil is shown in Figure 1.
4630
9
8840
7
1570
5367
3932
2
1043
38
1658
5658
4
1373
08
1837
41
2492
39
5283
62
2099
79
1147
94 4134
90
9689
0
7388
1
10
100
1000
10000
100000
1000000
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
*
Year
No
. of
rep
ort
ed c
ases
Source: Data from the Ministry of Health, Brazil * Denotes reported cases and deaths of dengue in January and February 2002
Figure 2. Number of reported cases of dengue in Brazil, 1986 to 2002

Dengue in Brazil: Past, Present and Future Perspective
Dengue Bulletin – Vol 27, 2003 29
In short, a total of 2,420,105 cases of dengue were reported in Brazil in the last 16 years(14). Figure 2 shows the annual number of reported cases and these numbers clearly indicate the seriousness of the problem in Brazil.
DHF/DSS in Brazil In spite of the fact that the majority of dengue cases in Brazil have been benign, 795 cases of DHF/DSS were reported until 1998, with a fatality rate of 5% (unpublished, Brasil - Ministério da Saúde, Situação do dengue no Brasil desde 1982, 1999). DHF/DSS cases were mostly associated with secondary infections that occurred during successive outbreaks caused by more than one virus type, and especially during DEN-2 epidemics after previous DEN-1 outbreaks. However, DHF/DSS cases associated with primary infections have also been reported(23). DHF/DSS cases occurred in the populated regions of the northeast and
south-east. Most of the DHF/DSS fatal cases occurred in adults and had started with classic dengue symptoms. After 2 or 3 days of the onset of the disease, they presented haemorrhagic disorders such as petechiae, gastrointestinal bleeding, low platelet count (less than 100,000 platelets/mm3), and a 45% or higher haematocrit level, suggesting that they had a capillary leak syndrome(17,19). It was also observed that patients who did not receive immediate treatment died.
A total of 3,288 DHF/DSS cases were reported in Brazil until February 2002, showing that this number has increased four times in the last three years, as shown in Figure 3. The fatality rate of Brazilian DHF/DSS cases is 4.3%. In January/February 2002, the DEN-3 outbreak in Rio de Janeiro claimed 854 cases of DHF/DSS, with 29 deaths, and, probably, many of them were not associated with secondary infection (personal communication from Schatzmayr H, 2002)(14).
274
188
0 0
24
112
69
35
93
72
888
679 85
4
8
0 0 0
11
2
1
5
13
5
45
29 29
1
10
100
1000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002*
Year
No
. of
rep
ort
ed c
ases
/dea
ths
No. of reported cases No. of deaths
Source: Data from the Ministry of Health, Brazil * Denotes reported cases and deaths of dengue in January and February 2002
Figure 3. Number of reported cases of DHF/DSS in Brazil, 1990 to 2002

Dengue in Brazil: Past, Present and Future Perspective
30 Dengue Bulletin – Vol 27, 2003
In order to detect DHF/DSS early and to start disease management as soon as possible, the Brazilian Ministry of Public Health recommends that suspected dengue cases should undergo careful medical observation during the first 48 to 72 hours of the onset. Dengue patients and/or their families should be warned about the appearing of symptoms and signs of DHF/DSS(24). In some medical centres the routine evaluation of dengue patients includes tourniquet test and haematocrit level determination.
During dengue outbreaks in Brazil at least eight fatal cases presented with an unusual and severe involvement of the central nervous system(25,26). In addition, one case of severe bilateral retinal occlusive vasculopathy was reported(27). A prospective study of 10 children whose mothers had dengue during pregnancy did not confirm congenital disease(28).
Genotypes of Brazilian dengue viruses The origins of Brazilian dengue viruses were determined in phylogenetic studies based on the entire E gene or the E/NS1 junction nucleotide sequences. DEN-1 strains isolated between 1986 and 2000 from different regions of Brazil were shown to belong to the same genotype II, the Caribbean one (personal communication from Pires Neto RJ and Fonseca BAL, 2002)(29). Likewise, DEN-2 isolates from different Brazilian regions showed to belong to the genotype III, the Puerto Rican topotype (personal communication from Pires Neto RJ and Fonseca BAL, 2002)(30,31). Probably, there was no introduction of new genotypes of DEN-1
in Brazil since 1986 and of DEN-2 since 1990. DEN-3 viruses, recently isolated in Brazil, were shown to belong to genotype III, Sri Lanka (personal communication from Miagostovitch M, 2001). All these viruses were probably introduced in Brazil from the Caribbean, Central America or northern South America, where they caused previous outbreaks.
Aedes aegypti and Aedes albopictus
Aedes aegypti, an anthrophagic mosquito, is the major vector of dengue as well as of yellow fever virus. It is possible that Aedes aegypti was introduced from Africa into Brazil in the 16th century with the slave trade. It probably happened many years before the arrival of dengue virus in the American continent(32).
The Brazilian Aedes aegypti eradication campaign was started by Oswaldo Cruz in 1904 to fight yellow fever. After 1920, with the technical assistance and financial support of the Rockefeller Foundation, the campaign was successful in eradicating the mosquito from Brazil, as confirmed in 1955(32). That campaign was probably the reason for the absence of dengue outbreaks in Brazil between 1923 and 1981. The reappearance of Aedes aegypti in Brazil after its eradication could be related to the beginning of dengue outbreaks. Firstly, Aedes aegypti infested the north of Brazil, reaching the state of Pará in the seventies, and in the following years expanding into the north-east(33). Between 1978 and 1984, almost all states in the north-east, south-east and mid-west of Brazil were infested by Aedes aegypti(34).

Dengue in Brazil: Past, Present and Future Perspective
Dengue Bulletin – Vol 27, 2003 31
Aedes albopictus, a mosquito from South-East Asia, and a known dengue vector, was introduced in the American continent after 1980. In 1986, it was observed in three different locations in Brazil. However, dengue transmission by Aedes albopictus has been reported only once during a Brazilian outbreak(35).
In 1998, all Brazilian states were infested by Aedes aegypti and dengue transmission was occurring in 22 of the 26 states(36).
The most important tool for dengue prevention so far is vector control. Since the beginning of dengue outbreaks, the Brazilian Ministry of Public Health, helped by state and county health agencies, monitored mosquito infestation levels and community clean-up programmes as well as mosquito control with insecticides were carried out(34). Innovative vector control programmes have been carried out in Brazil such as vertically structured programmes emphasizing destruction and/or treatment of larval habitats; education of schoolchildren resulting in the removal of large amounts of trash in community clean-up campaigns; cholinesterase level measurements in order to evaluate undesirable effects of the use of organophosphorate insecticides, and biological control of Aedes aegypti using copepods(4).
Evidence that vector control interrupts dengue transmission during dengue outbreaks was shown by the results of a dengue serological survey carried out in Ribeirão Preto city, Brazil, one year after the first DEN-1 outbreak that had led to an intensive Aedes aegypti control campaign
with destruction and/or treatment of larval habitats and removal of large amounts of trash in community clean-ups. It was estimated that 23,000 people had dengue infection during the outbreak and that most of the infected people lived in the district of Ipiranga in the north of Ribeirão Preto City(37). It is highly probable that the Aedes aegypti control campaigns limited the outbreak to that part of the city.
An Aedes aegypti eradication programme was submitted to the Brazilian community in 1996 in order to eliminate dengue transmission, to prevent the occurrence of DF/DHF/DSS, and to prevent vector spread to non-infected areas; and to prevent re-urbanization of yellow fever(38). However, this expensive and ambitious programme was not implemented.
Presently, the programme for the control of dengue in Brazil aims at lowering the Aedes aegypti infestation to under 5% of the houses. However, there has been a deficient infrastructure required to fight Aedes aegypti. After DEN-3 isolation in Rio de Janeiro in January 2001, a large outbreak was expected but the federal and state public health authorities were not able to put in place an effective vector control strategy, resulting in a serious DEN-3 outbreak in Rio de Janeiro in 2002.
Conclusion
The successive dengue epidemics in Brazil, caused by DEN-1, DEN-2 and DEN-3, led to the occurrence of DHF/DSS. The continuous circulation of three dengue types, with millions of reported dengue fever cases and

Dengue in Brazil: Past, Present and Future Perspective
32 Dengue Bulletin – Vol 27, 2003
with DHF/DSS, is becoming an endemic disease that is posing a serious public health threat. This situation is similar to what is found in South-East Asia(39). This scenario is worrisome because Brazil faces a severe
hospital management crisis and the system cannot support a sudden demand for the care of thousands of DHF/DSS cases requiring hospitalization.
References
1. Figueiredo LTM. The Brazilian Flaviviruses. Microbes and Infection, 2000, 2: 1643-1649.
2. Chambers TJ, Hahn CS, Galler R and Rice CM. Flavivirus genome organization, expression, and replication, Annual Review of Microbiology, 1990, 44: 649-688.
3. Batista WC, Kashima S, Marques AC and Figueiredo LTM. Phylogenetic analysis of Brazilian Flavivirus using nucleotide sequences of parts of NS5 gene and 3’ non-coding regions. Virus Research, 2001, 75:35-42.
4. Figueiredo LTM. Dengue in Brazil: history, epidemiology and research. Virus Reviews & Research, 1996, 1:9-16.
5. Vasconcelos PFC, Rosa APAT, Pinheiro FP, Rodrigues SG, Rosa EST, Cruz ACR and Rosa JFST. Aedes aegypti, dengue and re-urbanization of yellow fever in Brazil and other south American countries - Past and present situation and future perspectives. Dengue Bulletin, 1999, 23: 55-66.
6. Mariano F. A dengue. Considerações a respeito de sua incursão no Rio Grande do Sul, em 1916. Archivos Brasileiros de Medicina, 1916, 272-277.
7. Rego JP. Esboço histórico das epidemias que tem grassado na Cidade do Rio de Janeiro. 1872, Rio de Janeiro.
8. Reis TJ. A febre dengue in Curityba. Gazeta Médica da Bahia, 1896-97, 163-266.
9. Pedro A. O dengue em Nictheroy. Brazil Médico, 1923, 37: 173-177.
10. Osanai CH, Travassos da Rosa APA and Tang AT. Surto de dengue em Boa Vista, Roraima: Nota Prévia. Revista do Instituto de Medicina Tropical, São Paulo, 1986, 23: 53-54.
11. Schatzmayr HG, Nogueira RMR and Travassos da Rosa AP. An outbreak of Dengue virus at Rio de Janeiro. Memórias do Instituto Oswaldo Cruz, Rio de Janeiro, 1986, 81: 245-246.
12. Figueiredo LTM, Cavalcante SMB and Simões MC. Dengue serologic survey of school children in Rio de Janeiro, Brazil, 1986 and 1987. Bulletin of Pan American Health Organization, 1990, 24: 217-225.
13. Marzochi KBF, Carneiro MB and Schatzmayr HG. A Dengue no Rio de Janeiro: modêlo clínico- laboratorial. Revista da Sociedade Brasileira de Medicina Tropical, 1987, 20: 29-35.
14. FUNASA. Casos de dengue no Brasil.Brasília: Ministério da Saúde, 2002.
15. Vasconcelos PFC, Menezes DB, Melo LP, Pessoa ETFP, Rodrigues SG, Travassos da Rosa ES, Timbó MJ, Coelho ICB, Montenegro F, Travassos da Rosa JFS, Andrade FMO and Travassos da Rosa APA. A large epidemic of dengue fever with dengue hemorrhagic cases in Ceará State, Brazil. Revista do Instituto de Medicina Tropical, São Paulo, 1995, 37: 253-255.
16. Nogueira RMR, Miagostovich MP and Lampe E. Isolation of dengue type 2 in Rio de Janeiro. Memórias do Instituto Oswaldo Cruz, Rio de Janeiro, 1990, 85: 253.
17. Cunha RV and Netto GF. Aspectos clínico-epidemiológicos do Dengue Hemorrágico no Município do Rio de Janeiro. Revista da Sociedade Brasileira de Medicina Tropical, 1991, 24(Supl.2): 123-128.
18. Nogueira RMR, Zagne SMO and Martins ISM. Dengue haemorrhagic fever/dengue shock syndrome (DHF/DSS) caused by serotype 2 in Brazil. Memórias do Instituto Oswaldo Cruz, Rio de Janeiro, 1991, 86: 269-274.
Dengue in Brazil: Past, Present and Future Perspective
Dengue Bulletin – Vol 27, 2003 33
19. Zagne SMO, Alves VGF, Nogueira RMR, Miagostovich MP, Lampe E and Tavares W. Dengue haemorrhagic fever in the State of Rio de Janeiro, Brazil: a study of 56 confirmed cases. Transactions of the Royal Society of Tropical Medicine and Hygiene, 1994, 88: 677-679.
20. Vasconcelos PFC, Travassos da Rosa ES, Travassos da Rosa JFS, Freiras RB, Rodrigues SG and Travassos da Rosa APA. Epidemia de febre clássica de dengue causada pelo sorotipo 2 em Araguaina, Tocantins, Brasil. Revista do Instituto de Medicina Tropical, São Paulo, 1993, 35:141-148.
21. Rocco IM, Barbosa ML and Kanomata EHN. Simultaneous infection with dengue 1 and 2 in a Brazilian patient. Revista do Instituto de Medicina Tropical, São Paulo, 1998, 40: 151-154.
22. Nogueira RMR, Miagostovich MP, Filippis AMB, Pereira MAS and Schatzmayr HG. Dengue virus type 3 in Rio de Janeiro, Brazil. Memórias do Instituto Oswaldo Cruz, Rio de Janeiro, 2001, 96: 925-926.
23. Nogueira RMR, Miagostovich MP, Cunha RV, Zagne SM, Gomes FP, Nicol AF, Coelho JC and Schatzmayr HG. Fatal primary dengue infections in Brazil. Transactions Royal Society of Tropical Medicine Hygiene, 1999, 93: 418.
24. FUNASA. Manual de Dengue. Vigilância epidemiológica e atenção ao doente. Brasília: Ministério da Saúde, 1996.
25. Chimelli L, Hahn MD and Barretto Netto M. Dengue: Neuropathological findings in 5 fatal cases from Brazil. Clinical Neuropathology, 1990, 9: 157-162.
26. Vasconcelos PFC, Travassos da Rosa APA, Coelho ICB, Menezes DB, Travassos da Rosa E, Rodrigues SG and Travassos da Rosa JFS. Involvement of the central nervous system in dengue fever: three serologically confirmed cases from Fortaleza, Ceará, Brazil. Revista do Instituto de Medicina Tropical, Sâo Paulo, 1998, 40: 35-39.
27. Siqueira RC, Vitral NP and Oréfice F. Vasculopatia oclusiva retiniana associada ao dengue. Revista Brasileira de Oftalmologia, 1999, 58: 247-251.
28. Figueiredo LTM, Carlucci RH and Duarte G. Estudo prospectivo com crianças cujas mães tiveram dengue na gravidez. Revista do Instituto de Medicina Tropical, São Paulo, 1994, 36: 417-421.
29. Rico-Hesse R. Molecular evolution and distribution of dengue virus type 1 and 2 in nature, Virology, 1990, 174: 479-493.
30. Deubel V, Nogueira RMR and Drouet MT. Direct sequencing of genomic cDNA fragments amplified by the polymerase chain reaction for molecular epidemiology of dengue 2 viruses. Archives of Virology, 1993, 129: 197-210.
31. Miagostovich MP, Nogueira RMR, Schatzmayr HE and Lanciotti RS. Molecular Epidemiology of Den-2 Virus in Brazil. Memórias do Instituto Oswaldo Cruz, Rio de Janeiro, 1998, 93: 625-630.
32. Franco O. Historia da Febre Amarela no Brasil, Ministério da Saúde, Rio de Janeiro, 1976.
33. Marques AC. Sobre a viabilidade atual da erradicação do Aedes aegypti no controle da febre amarela no Brasil. Revista Brasileira de Malariologia e Doenças Tropicais, 1985, 37: 37-46.
34. Ministry of Health of São Paulo State, Brazil (SUCEN). Manual de atividades para controle dos vetores de dengue e febre amarela, 1993.
35. Serufo JC, Oca HM, Tavares VA, Souza AM, Rosa RV, Jamal MC, Lemos JR, Oliveira MA, Nogueira RMR.and Schatzmayr HG. Isolation of dengue virus type 1 from larvae of Aedes albopictus in Campos Altos City, State of Minas Gerais, Brazil, Memórias do Instituto Oswaldo Cruz, Rio de Janeiro, 1993, 88: 503-504.
36. FUNASA. Dengue. Instruções para pessoal de combate ao vetor. Manual de normas técnicas. Brasília: Ministério da Saúde, 2001.
37. Figueiredo LTM, Owa MA, Carlucci RH, Mello NV, Dal Fabbro AL, Capuano DM and Santili MB. Dengue Serologic Survey in Ribeirão Preto, SP, Brazil. Bulletin of the Pan American Health Organization, 1995, 29: 59-69.
38. Augusto LGS, Torres JPM, Costa AM, Pontes M and Novaes TCP. Programa de erradicação do Aedes aegypti: Inócuo e perigoso (e ainda perdulário). Cadernos de Saúde Pública, Rio de Janeiro, 1998, 14: 876-877.
39. Gubler DJ. Epidemic dengue and dengue hemorrhagic fever: A global public health problem in the 21st Century. In: Scheld WM, Armstrong D, Hughes JM (Eds.), Emerging Infections I, ASM Press, Washington DC, 1998: 1-14.

34 Dengue Bulletin –Vol 27, 2003
Diagnosis of Imported Dengue Fever in the Czech Republic
by Pavel Chalupa*#, Marie Kolarova**, Nada Sojkova*** and Jiri Januska‡
*Department of Infectious Diseases, Bohunice Teaching Hospital, Faculty of Medicine, Masaryk University in Brno, Jihlavská 20, 625 00 Brno, Czech Republic
**Division of Infectious Diseases, Epidemiology Department of Preventive Medicine, Masaryk University in Brno, Joštova 10, 662 44 Brno, Czech Republic
***Department of Virology, University Hospital Na Bulovce, Budínova 2, 180 81 Praha 8, Czech Republic
‡National Reference Laboratory for Arboviruses, Partyzánské nám 7, 702 00 Ostrava, Czech Republic
Abstract
Two institutions in the Czech Republic possess the facilities for the diagnosis of dengue fever (DF): the National Reference Laboratory for Arboviruses, Ostrava, and the Department of Virology, Teaching Hospital Na Bulovce, Prague. During 1997-2002, 417 patients were examined for suspected DF. Serological evidence, i.e. the presence of anti-dengue IgM and IgG antibodies, was based on ELISA using PANBIO kits. Epidemiological data on DF have been collected by the National Reference Center for Epidemiological Data Analysis in Prague since 1997. Up till now, 15 DF cases (diagnostic code A90) and one case of dengue haemorrhagic fever (DHF, diagnostic code A91) have been registered. The latter was a 45-year-old woman who experienced the acute phase of the disease with haemorrhagic signs without shock manifestation in a hospital in Bangkok and, after returning home, was admitted to the Department of Virology in Prague where the DHF diagnosis was confirmed serologically. Since 1999, the Czech Republic is part of the TropNetEurop, a European DF surveillance network.
Keywords: DF, DHF, anti-dengue IgM, anti-dengue IgG, surveillance, TropNetEurop, Czech Republic.
# For correspondence: [email protected]
Introduction A few years ago, dengue fever (DF) was still considered an exotic disease in the Czech Republic, known only from literature and beyond the concern of general medicine in
the country. It is certain that DF has been present here for some time but, not being recognized as such, it has passed under the diagnosis such as “a fever following return from a tropical country”, etc. It was only in the late 1990s that the disease received

Dengue in Brazil: Past, Present and Future Perspective
Dengue Bulletin – Vol 27, 2003 35
more attention and since then it has been found that, in the Czech Republic as in countries in Western Europe(1), DF ranks second only to viral hepatitis among the most frequently imported transmissible viral diseases(2). The objective of this study was to present the history of DF, including that of dengue haemorrhagic fever (DHF), in the Czech Republic with regard to its diagnosis and reporting.
Materials and methods
During 1997-2002, a total of 417 patients presenting clinical signs and symptoms of DF were examined in the Czech Republic. Anti-dengue antibodies were assessed by ELISA, using PANBIO kits (Brisbane, Australia). The specific IgM and IgG antibodies against DF were detected with the use of the Dengue IgM Capture ELISA Test and Dengue Indirect IgG ELISA Test, respectively. When the absorbance values were higher than the cut-off +10%, the sample was considered to be positive, which was in agreement with a relative value of 200 or higher. Since 2002, the results of the quantitative antibody examination have also been expressed in EU (ELISA UNITS) on the following scale: <9 EU, negative result; 9 to 11 EU, marginal result (trace amounts); >11 EU, positive result.
Results
The first DF case with serological evidence of DF was reported in the Czech Republic in 1991. The infection came from Taiwan, was caused by DEN-2 and was diagnosed at the
Department of Infectious Diseases, Prague, and confirmed by a serological examination at the State Institute of Health in Prague(2).
The next case of DF disease was diagnosed in 1996 (data from the Institute of Health Information and Statistics, Prague), but no detailed information on the case was made available.
In 1997, the National Reference Laboratory for Arboviruses, Ostrava, introduced procedures for DF diagnosis. The results of serological examinations done during 1997-2002 are given in Table 1. Out of the 89 patients examined, IgM anti-dengue antibodies were found in 16 patients and IgG anti-dengue antibodies in 22 patients.
The Department of Virology at the Teaching Hospital Na Bulovce, Prague, started routine diagnostic tests for DF in 1998. During 1998-2002, 328 patients were examined and serological evidence of acute DF (A90) was found in 15 patients. One case was diagnosed as “post-acute DHF” (A91). She was a 45-year-old woman who was admitted to the Department of Infectious Diseases, Prague. She had returned from Bangkok where she had been hospitalized for haemorrhagic fever, but free from shock manifestations, for three weeks (4-24 May 2002). In the Czech Republic, her diagnosis was confirmed at the Department of Virology at the Teaching Hospital Na Bulovce, Prague. The results of the serological examinations of anti-dengue antibodies carried out at this Department from 1998 to 2002 are presented in Table 2.

Diagnosis of Imported Dengue Fever in the Czech Republic
36 Dengue Bulletin – Vol 27, 2003
Table 1. Serological examination of DF cases in the National Reference Laboratory for Arboviruses, Ostrava¶
Antibody class detected by ELISA
Year of examination
Number of serum
samples
Number of positive
sera
Number of patients
examined
Number of positive patients
IgG IgM 1997
5 5
5 5
2 2
2 2
IgG IgM 1998
14 14
3 5
8 8
3 3
IgG IgM 1999
15 15
2 2
15 15
2 2
IgG IgM 2000
11 11
0 0
11 11
0 0
IgG IgM 2001
29 29
6 6
25 25
5 4
IgG IgM 2002
39 39
17 6
28 28
10 5
IgG IgM 1997-2002
113 113
33 24
89 89
22 16
¶ Higher number of positive sera than positive patients was due to withdrawal of more than one sera from some patients.
Table 2. Serological examination of DF cases in the Department of Virology, Teaching Hospital Na Bulovce, Prague¶
Antibody class detected by ELISA
Year of examination
Number of serum
samples
Number of positive
sera
Number of patients
examined
Number of positive patients
IgG IgM 1998
33 33
14 6
29 29
14 6
IgG IgM 1999
65 65
7 6
56 56
7 4
IgG IgM 2000
90 90
0 1
90 90
0 0
IgG IgM 2001
76 76
2 6
69 69
1 2
IgG IgM 2002
92 92
14 6
84 84
14 4
IgG IgM 1998-2002
356 356
37 25
328 328
36 16
¶ Higher number of positive sera than positive patients was due to withdrawal of more than one sera from some patients.

Diagnosis of Imported Dengue Fever in the Czech Republic
Dengue Bulletin – Vol 27, 2003 37
Table 3. Data on patients with DF infection reported to National Reference Center for
Epidemiological Data Analysis, Prague
Year Patient (sex)
Age (years)
Import from
Patient character-
istic 1998 M 46 Thailand Czech
tourist 1998 F 24 Thailand Czech
tourist 1998 M 24 Thailand Czech
tourist 1999 M 28 Malaysia Czech
tourist 1999 F 23 Indonesia Czech
tourist 2000 M 24 Indonesia Czech
tourist 2001 M 45 Thailand Czech
tourist 2001 M 32 Cameroon Czech
working abroad
2001 F 28 Indonesia Czech tourist
2001 F 27 India Czech tourist
2002 F 45 Thailand Czech tourist*
2002 F 26 Thailand Czech tourist
2002 M 37 Nepal Czech tourist
2002 M 48 Nepal Czech tourist
2002 M 53 Thailand Czech tourist
2002 M 28 Indonesia Czech tourist
* Patient with a post-acute form of DHF.
The cases of dengue fever (diagnostic code A90) diagnosed in the Czech Republic between 1998 and 2002 and reported to the National Reference Center for Epidemiological Data Analysis, Prague, are presented in Table 3. During this period, only one case of DHF (A91) was diagnosed. Because the patient had experienced the
acute stage of the disease with haemorrhagic signs in a hospital abroad, the diagnosis in the Czech Republic was confirmed only serologically and therefore this case was regarded as a “post-acute DHF”.
Discussion The two institutions which specialize in serological diagnostic procedures for DF in the Czech Republic are: the National Reference Laboratory for Arboviruses, Ostrava and the Department of Virology, Teaching Hospital Na Bulovce, Prague. The former has been providing diagnostic services since 1997 and the latter has introduced the laboratory diagnostic methods for DF since May 1998 in response to increasing demands from physicians who were seeing more patients presenting signs reminiscent of DF after their return from subtropical or tropical regions.
The system of reporting DF incidence in the Czech Republic has since improved.
The first and only DF case (diagnosed as A90) was recorded at the Institute of Health Information and Statistics, Prague, in 1996. The National Reference Center for Epidemiological Data Analysis established a comprehensive information system in 1997 and has provided detailed epidemiological information on DF cases that have occurred in the republic since then.
Ever since the detection of dengue fever in 1998 among returning travellers in the Czech Republic(2), the country has been included in the DF surveillance system of Europe since 1999. The lack of surveillance data for cases of infectious diseases imported into Europe prompted the establishment of the European Network on Imported Infectious Disease Surveillance (TropNetEurop) in

Diagnosis of Imported Dengue Fever in the Czech Republic
38 Dengue Bulletin – Vol 27, 2003
February 1999. This is an electronic network connecting hospitals and clinics that diagnose and provide treatment for imported infectious diseases. Although the organization of this network does not guarantee that the data collected will be representative of the entire continent of Europe, major referral centres are included, i.e. 37 hospitals in 14 European countries (including the Czech Republic). From the very beginning, DF has been one of the major target issues of this network. The results from the first year of sentinel surveillance of imported DF in Europe, and the DF patients in the Czech Republic, have also been included in this report.
The clinical signs in our patients have included a combination of fever, headache, fatigue and musculo skeletal symptoms such as arthralgia or myalgia, similar to most of the DF cases imported in Europe(3). Laboratory tests have shown leukopenia with relative lymphocytosis, thrombocytopenia and elevated transaminase levels (AST was usually higher than ALT). In all patients, treatment was symptomatic and none of them developed signs of DHF. All our patients were Czech citizens; foreign subjects or immigrants examined were free from the disease. All but one patient, who was on business in Cameroon, were tourists. The majority of DF cases were imported from south-east and south Asia and only one case was from Africa.
The standard method for serological diagnosis of DF was ELISA performed with PANBIO (Brisbane, Australia) kits. Screening with “Dengue Rapid Quick” tests based on immunochromatography was also attempted, but the results were not satisfactory, particularly where IgM antibody detection was concerned. From the results of the serological examination, it can be concluded that the presence of serum IgM antibodies is detected at about one week after the onset of the disease, while the first IgG antibodies appear at 10 to 14 days.
In view of the fact that up till now neither DF nor DHF has presented a serious health problem for the Czech health care system, the diagnostic methods so far used have not included serotyping.
Conclusions In the future, it can be expected that, with increasing tourism, more citizens will return home infected with DF or perhaps even with DHF. This will probably require the introduction of serotyping methods in diagnostic procedures as well as the inclusion of examination for DF in any subject presenting with a febrile condition after return from areas in which dengue fever is endemic.
References 1. Dobler G. Viren als unliebsame Reisemitbringsel.
Therapiewoche, 1996, 46: 1238-1239.
2. Chalupa P, Kubek J and Hejlova A. Dengue fever in the Czech Republic. Bratislava Medical Journal, 2001, 102(7): 322-325.
3. Jelinek T, Mühlberger N, Harms G, Corachán M, Grobusch MP, Knobloch J, Bronner U, Laferl H, Kapaun A, Bisoffi Z, Clerinx J, Puente S, Fry G,
Schulze M, Hellgren U, Gjørup I, Chalupa P, Hatz C, Matteelli A, Schmid M, Nielsen LN, Cunha S da, Atouguia J, Myrvang B and Fleischer Kl. Epidemiology and clinical features of imported dengue fever in Europe: Sentinel surveillance data from TropNetEurope. Clin Inf Dis, 2002, 35(9): 1047-1052.

Dengue Bulletin – Vol 27, 2003 39
Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
by
M Sriprom*, P Pongsumpun*, S Yoksan**, P Barbazan***, J P Gonzalez** and I M Tang+#
*Department of Mathematics, Faculty of Science, Mahidol University, Bangkok 10400, Thailand **Department of Physics, Faculty of Science, Mahidol University, Bangkok 10400, Thailand
***Center for Vaccine Development, Institute of Science and Technology for Research and Development, Mahidol University, Nakhon Pathom 73170, Thailand
+Research Center of Emerging Viral Diseases IRD, Institute of Science and Technology for Research and Development, Mahidol University, Nakhon Pathom 73170, Thailand
Abstract
The pathogenesis of dengue haemorrhagic fever (DHF) is looked for in the serological records of DHF patients (mainly children between the ages of one month and 16 years) at Siriraj Hospital in Thailand over a six-year period beginning 1998 (covering two three-year cycles). Based on the primary and secondary infections by both the haemagglutination-inhibition assay (HI) test and the IgM capture enzyme-linked immunosorbent assay (ELISA) test, it was found that in 1998, 14 of the cases for which paired sera specimens were tested using both HI and ELISA (or 9.6% of 146 cases) had resulted from primary infections. In 1999, 2000, 2001, 2002 and the first half of 2003, three out of 57 cases (5.3%); six out of 48 cases (12.5%); 85 out of 293 cases (29%); 23 out of 90 cases (25.6%) and 16 out of 56 cases (28.6%), respectively, resulted from primary infections. The percentages of primary infections during the last three years are well above 14.0% reported for cases occurring in Bangkok between 1988 and 2003.
Keywords: Dengue haemorrhagic fever, serological tests, primary-secondary infection.
# For correspondence: [email protected]
Introduction
Dengue fever (DF) is a rather benign febrile disease, afflicting mainly older children and adults(1) and often remaining unapparent in young children(2). The sudden onset of fever and a variety of non-specific signs and
symptoms characterize DF. The high fever lasts for two or three days, followed by additional symptoms. Its clinical presentations are similar to those of several other diseases, meaning thereby that many of the reported cases of DF could be due to other febrile illnesses and also that many

Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
40 Dengue Bulletin – Vol 27, 2003
dengue infections are not recognized. During the 1977 epidemic in Santiago de Cuba(3), only 3,012 out of 9,747 people who developed febrile illnesses and whose sera were tested, turned out to be infected with dengue fever. DF is caused by the dengue virus which belongs to the genus, Flavivirus, in the Flaviviridae family. There are four serotypes of this virus known as DEN-1, DEN-2, DEN-3 and DEN-4. Infection by any of the four serotypes causes similar clinical presentations, and confers permanent immunity to that particular serotype, but only a temporary one to the others.
The dengue virus is transmitted by the Aedes mosquitoes, i.e. Aedes aegypti and Aedes albopictus, in countries of South-East Asia. Introduction of the dengue virus by just one individual into a susceptible population residing in a locality where the above mosquitoes are prevalent can quickly lead to an epidemic. In many tropical countries, DF has now emerged as a major public health problem(4).
The pathogenesis of dengue haemorrhagic fever (DHF) is still a matter of controversy. According to one school of thought(5), pre-existing heterologous dengue antibodies recognize the infecting virus and form an antigen-antibody complex, which then binds the virus to the cell membrane of some leukocyctes. Since the antibodies are only heterologous, the virus is not neutralized and is free to replicate once inside the cell. It is then thought that these cells secrete vasoactive mediators in response to dengue infection. These mediators cause an increased vascular permeability, which leads to hypovolemia and shock. Since the antibodies have to be
pre-existing, this hypothesis terms it as the secondary infection or immune enhancement.
A cautionary note should be added here. It appears that the occurrence of DHF after a second infection depends on the strain of the serotype. During the 1996-1997 dengue epidemic in Belem Para, Brazil, none of the 24 patients who had been previously infected by the DEN-1 virus developed DHF after they had been re-infected by the DEN-2 virus(6). Watts et al(7) observed the same pattern during the 1995 epidemic in Iquitos, Peru. No cases of DHF/DSS were reported even though it was expected that between 887 to 10,247 cases would have occurred. The DEN-2 isolates were found to be of the American genotype (strain). Kochel et al(8), attributed the non-occurrence of DHF/DSS to the presence of common envelope epitopes in both the American strain of the DEN-2 virus and the DEN-1 virus and the absence of these epitopes in the Asian strain of the DEN-2 virus. The common epitopes could have been acquired through the recombination between the American DEN-2 and the DEN-1 virus co-circulating in the Americas or through genetic drift (mutation).
The other school of thought(5) maintains that the mutation of the viruses could have produced viruses with greater virulence and therefore greater epidemic potential. DHF would then be due to the appearance of these mutant strains among the circulating virus. This second hypothesis does not pre-suppose the presence of pre-existing antibodies and so the DHF/DSS infection would be the result of a primary infection. In an attempt to contribute to this debate, we

Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
Dengue Bulletin – Vol 27, 2003 41
reviewed the serological status of children suffering from DHF who were admitted to the Paediatrics ward of Siriraj Hospital (a tertiary-care medical centre with a 300-bed facility in Bangkok, Thailand) between 1998 and mid-2003. A similar review of children admitted to the Department of Paediatrics, Chulalongkorn Hospital, Bangkok, between 1985 and 1995 was made recently(9).
Materials and methods
Criteria for primary and secondary infections
The World Health Organization (WHO)(4) has established a set of criteria to determine whether a case of dengue fever is due to primary or a secondary infection. The determination is based on the results of either HI tests or ELISA tests or both, done on a paired set of sera taken at least seven days apart, one in the acute phase and the other in the convalescence phase. The criteria for primary infection are that, for a paired set of sera specimens there should be a fourfold increase in the IgM antibody response and HI titers of any of the DEN serotypes and the IgM/IgG ratio should be ≥1.8 and/or the HI titers in the convalescence phase should be <1,280. The criteria for determining secondary infection are that the IgM/IgG ratio should be <1.8 and/or the HI titers in the convalescence phase should be ≥2,560.
Patients
Admission to the ward was based on the clinical presentation of DHF as per the case
definition of WHO(4). Serological tests, i.e. haemagglutination inhibition (HI) assay(10) and IgM/IgG enzyme-linked immunosorbent assay (ELISA)(11), were used to determine whether the patients had dengue virus infection. Attempts were made to isolate the virus on Toxorhynchites mosquito to identify the serotype of the virus responsible for the illness.
Results The results of the laboratory survey are given in the Table. Of the 1,183 patients admitted, the serological tests established that 1,082 of them were confirmed as of DHF. A total of 214 patients were determined to be due to primary infections, 291 due to secondary infection and 577 remained undetermined. One hundred and one patients turned out not to be sick with DHF. The virus responsible for the infection was isolated in 373 cases. The predominant virus was DEN-1 (162), followed by DEN-2 (121), DEN-3 (70) and DEN-4 (17). Multiple viruses were found in three patients (not included in the table). On the basis of the serological tests and using the WHO criteria for primary and secondary infections, our study found that in 1998, 14 of the cases for which paired sera specimens were tested by both tests (or 9.6% of 146 cases) had resulted from primary infection. In 1999, 2000, 2001, 2002 and the first half of 2003, three out of 57 cases (5.3%), six out of 48 cases (12.5%), 85 out of 293 cases (29%), 23 out of 90 cases (25.6%) and 16 out of 56 cases (28.6%), respectively, had resulted from primary infection.

Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
42 Dengue Bulletin – Vol 27, 2003
Table. Summary of the serological records of DHF patients admitted to Siriraj Hospital, 1998-2003
Number of cases where virus were isolated Year
Number of patients admitted
Number sick with DHF
DEN-1 DEN-2 DEN-3 DEN-4 Total
1998 318 281 51 28 41 1 121
1999 137 112 9 13 3 4 29
2000 84 71 13 13 5 0 31
2001 334 334 49 36 17 8 110
2002 186 186 23 22 4 1 50
2003* 121 121 17 9 0 3 29
*From January – June 2003
Regarding the results of virus isolation, of the 121 cases where virus was isolated in 1998, 40.0% were of DEN-1, 24.2% were of DEN-2, 34.2% were of DEN-3 and 1.7% were of DEN-4. In 1999, the respective percentages were 31.0, 44.8, 10.3 and 13.8. In 2000, the percentages changed to 42, 42, 16.1 and 0, respectively. In 2001, they were 44.5, 32.7, 15.5 and 14.1. In 2002, they were 46.0, 44.0, 8.0 and 2.0 respectively. For the first half of 2003, the percentages were 58.6, 31.0, 0 and 10.3 respectively. Comparing the percentages year by year, we can quantify the relative amount of the virus in circulation during that year. The relative abundance of DEN-1 virus appears to be increasing year after year, while that of DEN-3 appears to be decreasing. Overall, DEN-2 appeared to be the second-most abundant serotype in circulation throughout the study period.
The age distribution of the patients suffering from DHF is given in the Figure.
This looks similar to the one of the DHF/DSS patients admitted to Yangon Children’s Hospital, Myanmar, between 1995 and 1996, but is different from that of the children admitted to the Children’s Hospital in Bangkok between 1995 and 1998(12). The age distribution pattern for the latter hospital shows a bimodal distribution, with the second maximum in infants below the age of one year. Halstead et al(12) proposed that this group should be the one to study for understanding primary infections. They found that infants with DHF/DSS constituted 4.9% of the patients in their study group. Only eight infants were recorded in our study group. A similarly small number of infants was seen in the study group of Pancharoen et al(9). Also shown in the Figure is the age distribution of the DHF cases resulting from primary infection. In all the three studies, DHF infections in infants were primary infections.

Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
Dengue Bulletin – Vol 27, 2003 43
Figure. Age distribution of primary infection and total DHF patients (1998-2003) The numbers listed are for the patients whose ages are
known and include those whose diagnoses are based on either single sera test or clinical presentations
8 13
42
134
166
187
138
39
10 86 5
16
33
42
32
14
8
2 2
0
20
40
60
80
100
120
140
160
180
200
<1 1-2 3-4 5-6 7-8 9-10 11-12 13-14 15-16 >16
Age (years)
Tota
l no.
of D
HF
patie
nts
Total DHF Primary infection
Discussion The period covered in the present study spans two complete three-year cycles in the month of incidence of DHF in Bangkok, Thailand, between January 1998 and June 2003. Hays et al(13) carried out a spectral density analysis of the data and found an annual variation and a super-annual variation (of three years). The 1998 epidemic was one of the peak years in the annual occurrence of DHF in Thailand. Based on this, Hays predicted during a dengue fever conference held in December
2000 in Chiang Mai that 2001 would be a peak year for DHF. This was borne out by the increase observed in the incidence of DHF in Bangkok in that year. Many of us also made similar predictions(14). As observed in this study, the incidence of DHF peaked in 1998 and then decreased in 1999 and again went down in 2000. It rose sharply in 2001 (a peak year in the three-year cycle) and then dropped in 2002. The decrease appeared to be continuing in 2003. Based on the previous trends, it is expected that there will be a rise in the incidence of DHF in 2004.

Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
44 Dengue Bulletin – Vol 27, 2003
In the present study, dengue virus was isolated only in 34.5% of the 1,082 DHF patients confirmed by serological examinations. This is far below the percentage isolated by Vaughn et al(15), who were able to isolate the virus in 98% of their patients. Their study was done in 1994. The difference in the percentages is due to the fact that Vaughn et al carried out their isolation within three days of the beginning of the high fever. Using similar criteria for differentiating between primary and secondary infections as the cause of the DHF illness, Vaughn et al established that only 8% of the acute dengue illnesses were due to primary infections (92% were due to secondary infections).
The relative abundance of the four serotypes observed by Vaughn et al, in 1994 was DEN-1 (20.3%), DEN-2 (28.8%), DEN-3 (16.9%) and DEN-4 (33.9%). Combining these numbers with the relative abundance observed in our study and in 1960(16), we observed that there was permanent
circulation of the four serotypes in Thailand. This is likely to be the cause of the short intervals between the high epidemic peaks, compared to what is observed, for example, in Polynesia where mono-serotype epidemics occur at an interval of at least six-to-seven years(17). Looking at the relative abundance of all the four serotypes on a year-to-year basis, we found that the relative abundance of DEN-4 was fluctuating the most, followed by DEN-3. No significant differences (p<0.05) were observed between confirmed primary and secondary infections for any serotype during any year.
The percentages of primary infections during the last three years are well above 14.0 reported for cases occurring in Bangkok between 1988 and 1995(9). This raises the question: Does the fact that the percentages of DHF/DSS arising from primary infections have almost doubled during the last three years signify that the dengue viruses have become more virulent or are there other factors at play?
References
1. Gubler DJ. Dengue and dengue haemorrhagic fever. Clin Microbiol Rev, 1998, 11(3): 480-496.
2. Burke DS, Nisalak A, Johnson DE and Scott RM. A prospective study of dengue infections in Thailand. Am J Trop Med Hyg, 1988, 38(1): 172-180.
3. Guzman MG, Kouri G, Valdes L, Bravo J, Alvarez M, Vazques S, Delgado I and Halstead SB. Epidemiologic studies on dengue in Santigo de Cuba, 1997. Am J Epidemiol, 2000, 152(9): 793-799.
4. World Health Organization, Dengue haemorrhagic fever: Diagnosis, treatment, prevention and control (2nd ed). WHO (Geneva), 1997.
5. Halstead SB. The pathogenesis of dengue. Molecular-epidemiology in infectious disease. Am J Epidemiol, 1981, 114: 632-648.
6. Travassos da Rosa APA, Vasconcelos PFC, Travassos da Rosa ES, Rodrigues SG, Mondet B, Cruz ACR, Sousa MR and Travassos da Rosa JFS. Dengue epidemic in Belem Para, Brazil, 1996-97. Emerg Inf Dis, 2000, 6(3): 298-301.
7. Watts DM, Porter KR, Putvatana P, Vasquez B, Calampa C, Hayes CG and Halstead SB. Failure of secondary infection with American genotype dengue 2 to cause dengue haemorrhagic fever. The Lancet, 1999, 354: 1431-1434.

Dengue Haemorrhagic Fever in Thailand, 1998-2003: Primary or Secondary Infection
Dengue Bulletin – Vol 27, 2003 45
8. Kochel TJ, Watts DM, Halstead SB, Hayes CG, Espinoza A, Felices V, Caceda R, Bautista CT, Montoya Y, Douglas S, Russell KL. Effect of dengue-1 antibodies on American dengue-2 viral infection and dengue haemorrhagic fever. The Lancet, 2002, 360: 310-312.
9. Pancharoen C, Mekmullica J and Thisyakorn U. Primary dengue infection: What are the clinical distinctions from secondary infections? Southeast Asian J Trop Med Public Health, 2001, 32(3): 476-480.
10. Clarke CW and Casals J. Techniques of hemagglutination and hemagglutination inhibition with arthropod viruses. Am J Trop Med Hyg, 1958, 7: 561-573.
11. Innis BL, Nisalak A, Nimmanitya S, Kusalerdchariys S, Chongswarsdi V, Suntayakorn S, Puttisri P. Hoke CH. An enzyme-linked immunosobent assay to characterize dengue infections where dengue and Japanese encephalitis co-circulate. Am J Trop Med Hyg, 1989, 40: 418-427.
12. Halstead SB, Lan NT, Myint TT, Shwe TN, Nisalak A, Kalyanarooj S, Nimmannitya S, Soegijanto, Vaughn DW and Endy TP. Dengue hemorrhagic fever in infants: Research opportunities ignored. Emerg Inf Dis, 2002, 8(12): 1474-1479.
13. Hay SI, Myers MF, Burke DS, Vaughn DW, Endy T, Ananda N, Shanks GD, Snow RW, and Rogers DJ. Etiology of interepidemic periods of mosquito-borne diseases. PNAS, 2000, 97(16): 9335-9339.
14. Barbazan P, Yoksan S and Gonzalez JP. Dengue hemorrhagic fever epidemiology in Thailand: Description and forecast of epidemics. Microbes and Infections, 2002, 4(7): 699-705.
15. Vaughn DW, Green S, Kalayanarooj S, Innis BL, Nimmannitya S, Suntayakorn S, Rothman AL, Ennis FA and Nisalak A. Dengue in the early febrile phase: Viremia and antibody responses. J Infect Dis, 1997, 176: 322-330.
16. Hammon VM and Sather GE. Virological findings in the 1960 hemorrhagic fever epidemic (dengue) in Thailand. Am J Trop Med Hyg, 1964, 13: 629-641.
17. Deparis X, Chungue E, Pauck S, Roche C, Murgue B and Gleize. Surveillance epidemiologique de la dengue: Methode et interet lors de l’epidmic de dengue 2 en Polnesie francaise en 1996. Trop Med and Intl Health, 1998, 3: 566-570.

46 Dengue Bulletin – Vol 27, 2003
Virological and Serological Surveillance of Dengue Epidemics in 19 Provinces in Southern Viet Nam
during 2001 by
Do Quang Ha#, Vu Thi Que Huong, Huynh Thi Kim Loan, Vu Thien Thu Ngu, Hoang Thi Nhu Dao and Cao Minh Thang
Laboratory of Arboviruses, Pasteur Institute, 167 Pasteur Street, District 3, Ho Chi Minh City, Viet Nam
Abstract
In 2001, 18 provincial centres for preventive medicine sent samples taken from DHF patients to the Arbovirus Laboratory at the Pasteur Institute, Ho Chi Minh City. The provinces with the highest rates of virus isolation were Tien Giang and Kien Giang. Dengue viruses were mostly isolated from patients diagnosed with viral syndrome and DHF grades I-II. Dengue-2 virus caused many cases of severe disease (grade III-IV), as compared with other serotypes. A total of 4,046 patient sera were tested by Mac-ELISA; the average positive rate was 56.13%. In areas with positive Mac-ELISA results, however, no control measures had yet been implemented to limit the increasing number of DHF outbreaks in the area.
Keywords: Dengue virus, serological surveillance, Mac-ELISA, Viet Nam.
# For correspondence: [email protected]
Introduction During 2001, 28,584 DHF patients from 19 provinces were reported to the Pasteur Institute, Ho Chi Minh City, Viet Nam, an increase of 52.53% in the number of cases as compared with 2000. Seventy-one patients died in 2001, an increase of 44.89% in the case fatality rate as compared with 2000. Tien Giang and Dong Thap were the two provinces with the highest morbidity rate per 100,000 population in the region and these rates were higher than the average morbidity rate for the five-year period 1996-2000. Virological and serological surveillance were a part of the National Programme for DHF Control; these surveillance activities were
carried out from the beginning of the year. The present paper includes data collected during 2001.
Results of virological surveillance and conclusions Virus isolation
During 2001, 18 out of 19 provincial centres for preventive medicine in southern Viet Nam sent blood samples from DHF patients to the Arbovirus Laboratory at Pasteur Institute, Ho Chi Minh City, for virus isolation(1). Eighty-three virus strains were isolated with an average positivity rate of 9.29% (Table 1).

Virological and Serological Surveillance in Viet Nam
Dengue Bulletin – Vol 27, 2003 47
Table 1. Results of virus isolation from18 provinces by month in southern Viet Nam during 2001
Provinces Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
An Giang – 3D2/11* 1D4/21 0/18 1D2/27 1D2/15 1D2/6 0/12 0/4 – – – 6D2,1D4/114 Bac Lieu – – – – – – – – – – – – 0/0 Ben Tre 0/9 0/12 0/13 0/15 2D4/15 1D2,
2D4/14 0/12 0/3 0/6 – 0/3 – 1D2,
4D4/102 Binh Duong
– – – – – – – – 0/3 1D2/1 – – 1D2/4
Binh Phuoc
– – – – – – – 0/5 – – – – 0/5
Ba Ria-Vung Tau
– 0/1 0/1 1D2/28 1D2/13 1D1, 1D2,
1D4/22
2D2, 1D3/14
3D2/29 1D2/7 – – – 1D1, 9D2, 1D3,
1D4/115 Can Tho – 0/1 – – 0/2 1D4/20 1D4/45 – – – – – 2D4/68 Ca Mau – – – – – 0/6 – 0/2 0/4 – – – 0/12 Dong Nai 0/1 – 0/1 – – 0/1 0/6 1D2/17 0/3 2D2/18 0/5 0/1 3D2/53 Dong Thap – 0/1 0/1 – 0/11 2D2/22 1D2,
2D3, 2D4/12
1D2/3 0/3 1D2/3 – – 5D2, 2D3, 2D4/56
Kien Giang 1D4/3 0/1 1D4/2 – – 3D3, 3D4/38
1D2, 3D3,
1D4/13
– – – 1D3/4 – 1D2, 7D3, 6D4/61
Lam Dong – – 0/7 0/2 – – – – 0/4 – – – 0/13 Long An – – – – 1D4/8 0/10 0/11 0/3 0/3 1D1,
1D2, 1D4/31
1D4/6 – 1D1, 1D2, 3D4/72
Soc Trang – – – – – 0/6 0/4 0/13 0/1 – 0/1 – 0/25 Tay Ninh 1D4/3 1D4/1 0/1 0/1 0/2 0/7 – 0/4 0/4 0/3 0/2 – 2D4/28 Tien Giang – – 6D4/14 4D4/11 0/4 1D4/11 1D2,
2D4/14 2D4/9 0/7 0/1 – 1D4/2 1D2,
16D4/73 HCM City – – – – 1D2/6 0/10 1D4/4 0/1 1D2/10 0/2 0/12 0/2 2D2, 1D4/47 Tra Vinh – – – – – 0/5 0/1 – – – – – 0/6 Vinh Long 0/1 – 0/1 – 0/1 0/1 0/5 0/4 2D2/7 0/7 1D2/7 0/5 3D2/39 Total 2D4 3D2,
1D4 8D4 1D2,
4D4 3D2, 3D4
1D1, 5D2, 3D3, 8D4
6D2, 6D3, 7D4
5D2, 2D4
4D2 1D1, 5D2, 1D4
1D2, 1D3, 1D4
1D4 2D1, 33D2, 10D3, 38D4
No. (+)/ total samples
2/17 4/28 8/62 5/75 6/89 17/188 19/147 7/105 4/66 7/66 3/40 1/10 83/893
*Number of isolates/Number of blood samples − denotes data not available, D1: DEN-1, D2: DEN-2, D3: DEN-3; D4: DEN-4 During 2001, 1 DEN-2 and 1 DEN-4 were also isolated in Buon Ma Thuot Province (2+/29). Six DEN-2 and 3 DEN-3 were also isolated in Binh Thuan province (9+/65) Note: All the four dengue serotypes co-circulated in southern Viet Nam, with the predominant serotypes being DEN-2 and DEN-4

Virological and Serological Surveillance in Viet Nam
48 Dengue Bulletin – Vol 27, 2003
Positivity rate of virus isolation by provinces
• Provinces with the highest positive rate included Tien Giang (23.29%) and Kien Giang (22.95%).
• In two other provinces, Ba Ria-Vung Tau and Dong Thap, the positivity rate ranged from 10-16%.
• In all the remaining provinces, the positivity rate was <7%.
Circulation of dengue serotypes in 2000 and 2001
Provinces showing DEN virus circulation during 2000 and 2001 are included in Table 2.
Table 2. Provinces showing DEN virus circulation during 2000 and 2001
DEN-1 DEN-2 DEN-3 DEN-4
2000 2001 2000 2001 2000 2001 2000 2001
Tay Ninh BR-VTau
Long An
B Duong
HCM City
Ben Tre
Vinh Long
An Giang
Kien Giang
BR-VTau
Binh Duong
Dong Nai
HCM City
Long An
Tien Giang
Ben Tre
Dong Thap
Vinh Long
An Giang
Kien Giang
HCM City
Long An
Ben Tre
Can Tho
Soc Trang
An Giang
BR-VTau
Dong Thap
Kien Giang
Long An
Ben Tre
Vinh Long
Kien Giang
An Giang
Dong Thap
BR-VTau
Tay Ninh
HCM City
Long An
Tien Giang
Ben Tre
Dong Thap
Can Tho
An Giang
Kien Giang
From Table 2, it is apparent that DEN-1
and DEN-3 retreated while DEN-2 and DEN-4 continued to be active in the country. DEN-4, which appeared during 1997 in one province, expanded its activities to 2, 3, 6 and 10 provinces during 1998, 1999, 2000 and 2001 respectively. Between 1997 and 2001, DEN-4 was circulating in 13 provinces.
Month-to-month variations of dengue serotypes in southern Viet Nam in 2001
Monthly variations in the circulating DEN viruses in south Viet Nam during 2001 are depicted in the Figure.

Virological and Serological Surveillance in Viet Nam
Dengue Bulletin – Vol 27, 2003 49
Age and sex distribution of virologically-confirmed cases
The distribution of the virologically-confirmed cases by age and sex during 2001 is given in Table 3.
Table 3. Age and sex distribution of virologically confirmed cases
Age-group Male Female No. (+%)
4 years ≤ 3 3 6 (7.23)
5 – 9 8 11 19 (22.89)
10 – 14 22 19 41 (49.40)
15 – 19 4 4 8 (9.64)
≥20 4* 2 6 (7.23)
Not reported 2 1 3 (3.61)
Total (%+) 43 (51.81%)
40 (48.19%)
83 (100)
*1 patient aged 74 years old
As previously reported in other publications(3,4,5), dengue viruses were most often discovered in children aged 5-14 years (72.28%) and there was no difference between males and females (χ2 = 0.22; p = 0.64).
Dengue serotypes isolated from DHF severity grades
The dengue serotypes isolated by the DHF severity grades are given in Table 4.
Table 4. Virus serotypes isolated from patients with different grades of severity
Severity grade DEN-1 DEN-2 DEN-3 DEN-4 Total
(%+) Viral Infection
1 11 6 25 43 (51.81)
DHF grade I - II
1 9 3 11 24 (28.92)
DHF grade III - IV
13 1 2 16 (19.28)
Total 2 33 10 38 83
Note: Dengue viruses were mostly recovered from mild patients diagnosed with viral infection or DHF grade I-II (80.72%). DEN-2 virus has caused more severe cases as compared with other serotypes.
Results of serological surveillance using Mac-Elisa tests
The results of serological surveillance using Mac-Elisa test by month and provinces for the year 2001 are included in Table 5.
Figure. Variations in prevalence of dengue serotypes by month during 2001
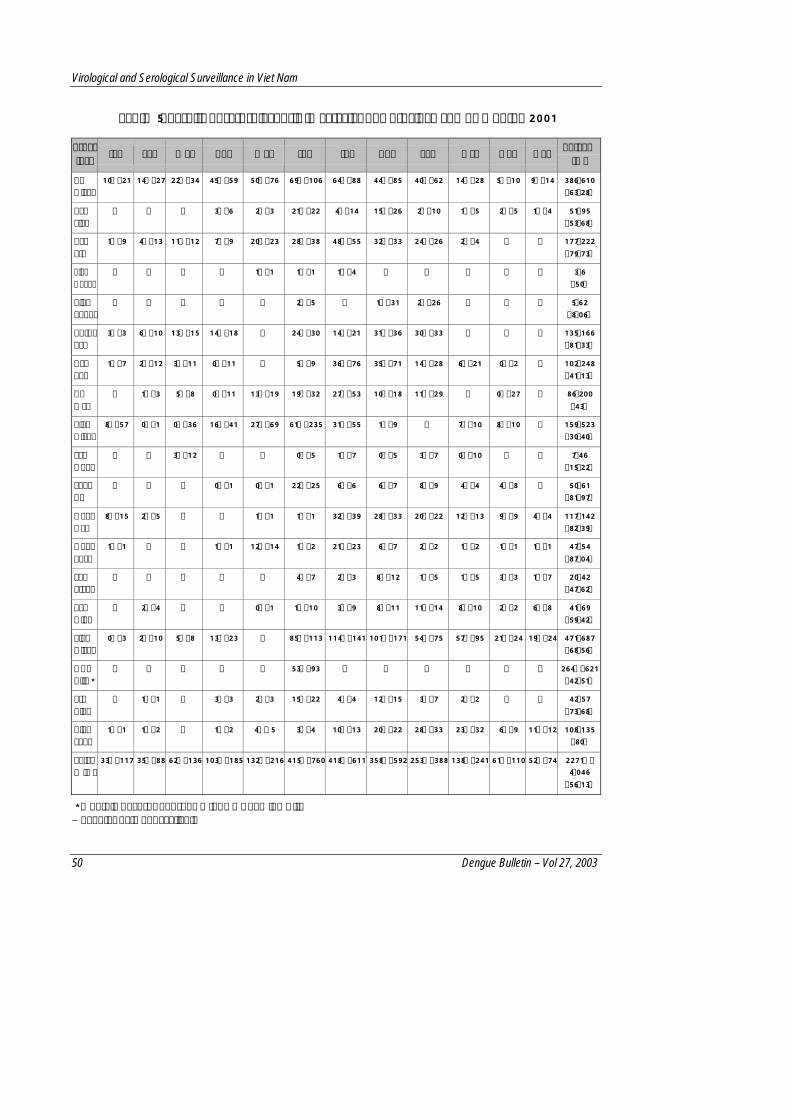
Virological and Serological Surveillance in Viet Nam
50 Dengue Bulletin – Vol 27, 2003
Table 5. Results of sero-diagnosis (Mac-ELISA) by province and by month, 2001
Prov–ince
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total % (+)
An Giang
10+/21 14+/27 22+/34 45+/59 50+/76 69+/106 64+/88 44+/85 40+/62 14+/28 5+/10 9+/14 386/610 (63.28)
Bac Lieu
– – – 3+/6 2+/3 21+/22 4+/14 15+/26 2+/10 1+/5 2+/5 1+/4 51/95 (53.68)
Ben Tre
1+/9 4+/13 11+/12 7+/9 20+/23 28+/38 48+/55 32+/33 24+/26 2+/4 – – 177/222 (79.73)
Binh Duong
– – – – 1+/1 1+/1 1+/4 – – – – – 3/6 (50)
Binh Phuoc
– – – – – 2+/5 – 1+/31 2+/26 – – – 5/62 (8.06)
BR-V. Tau
3+/3 6+/10 13+/15 14+/18 – 24+/30 14+/21 31+/36 30+/33 – – – 135/166 (81.33)
Can Tho
1+/7 2+/12 3+/11 0+/11 – 5+/9 36+/76 35+/71 14+/28 6+/21 0+/2 – 102/248 (41.13)
Ca Mau
– 1+/3 5+/8 0+/11 13+/19 19+/32 27+/53 10+/18 11+/29 – 0+/27 – 86/200 (43)
Kien Giang
8+/57 0+/1 0+/36 16+/41 27+/69 61+/235 31+/55 1+/9 – 7+/10 8+/10 – 159/523 (30.40)
Lam Dong
– – 3+/12 – – 0+/5 1+/7 0+/5 3+/7 0+/10 – – 7/46 (15.22)
Long An
– – – 0+/1 0+/1 22+/25 6+/6 6+/7 8+/9 4+/4 4+/8 – 50/61 (81.97)
Dong Nai
8+/15 2+/5 – – 1+/1 1+/1 32+/39 28+/33 20+/22 12+/13 9+/9 4+/4 117/142 (82.39)
Dong Thap
1+/1 – – 1+/1 12+/14 1+/2 21+/23 6+/7 2+/2 1+/2 1+/1 1+/1 47/54 (87.04)
Soc Trang
– – – – – 4+/7 2+/3 8+/12 1+/5 1+/5 3+/3 1+/7 20/42 (47.62)
Tay Ninh
– 2+/4 – – 0+/1 1+/10 3+/9 8+/11 11+/14 8+/10 2+/2 6+/8 41/69 (59.42)
Tien Giang
0+/3 2+/10 5+/8 13+/23 – 85+/113 114+/141 101+/171 54+/75 57+/95 21+/24 19+/24 471/687 (68.56)
HCM City*
– – – – – 53+/93 – – – – – – 264+/621 (42.51)
Tra Vinh
– 1+/1 – 3+/3 2+/3 15+/22 4+/4 12+/15 3+/7 2+/2 – – 42/57 (73.68)
Vinh Long
1+/1 1+/2 – 1+/2 4+/ 5 3+/4 10+/13 20+/22 28+/33 23+/32 6+/9 11+/12 108/135 (80)
Total % (+)
33+/117 35+/88 62+/136 103+/185 132+/216 415+/760 418+/611 358+/592 253+/388 138+/241 61+/110 52+/74 2271+/ 4.046 (56.13)
* Monthly Records not shown for Ho Chi Minh City − denotes data not available
Virological and Serological Surveillance in Viet Nam
Dengue Bulletin – Vol 27, 2003 51
An analysis of the data indicated that 4,046 sera samples received from 19 provinces were tested with an average positivity rate of 56.13%. The number of sera collected by province was as follows:
• 500 sera: HCM City, Tien Giang, An Giang, Kien Giang.
• ≥ 200 sera: Ben Tre, Can Tho, Ca Mau.
• From 100-199 sera: Ba Ria-Vung Tau, Dong Nai, Vinh Long.
• < 100 sera: 9 remaining provinces.
The Mac-ELISA positivity rates by province were as follows:
• >75%: 6 provinces: Ba Ria-Vung Tau, Dong Nai, Long An, Ben Tre, Dong Thap and Vinh Long.
• ≥50%: 6 provinces: Tay Ninh, Binh Duong, Tien Giang, Tra Vinh, Bac Lieu and An Giang.
• <50%: 7 provinces: Lam Dong, Binh Phuoc, Ho Chi Minh City, Can Tho, Soc Trang, Ca Mau and Kien Giang.
DHF patients were detected in the first quarter of the year in which the large DHF outbreak had not yet occurred.
Acknowledgements
We thank Dr D J Gubler, Director of the Centres for Disease Control (CDC), Colorado, USA, for supplying many biological products necessary for carrying out this study.
References 1. Gubler DJ. Application of serotype-specific
monoclonal antibodies for identification of dengue viruses. In: Yunker CE (Ed) Arbovirus in arthropod cells in vitro. CRC Press, Boca Raton, Florida. 1986, 2: 3-14.
2. Kuno G, Gomez I and Gubler DJ. Detecting artificial anti-dengue IgM immune complexes using an enzyme-linked immunosorbent assay. Am J Trop Med Hyg, 1987, 36: 153-159.
3. Do Quang Ha, Vu thi Que Huong, Huynh thi Kim Loan, Dinh Quoc Thong and Vincent Deubel. Dengue haemorrhagic fever in the south of Viet Nam during 1975-1992 and its control strategy. Jap Trop Med, 1994, 36(4): 187-201.
4. Do Quang Ha, Vu Thi Que Huong, Huynh Thi Kim Loan and Pham Kim Sac. Situation of dengue haemorrhagic fever in south Viet Nam, 1991-1994. Dengue Bulletin. 1996, 20: 55-61.
5. Vu Thi Que Huong, Cao Minh Thang, Huynh Thi Kim Loan, Do Quang Ha. Virological and serological surveillance of dengue haemorrhagic fever in southern Viet Nam, 2000. J. Hyg. Prev. Med. 2001, VII, 21: 5-9 (in Viet Namese).
6. Do Quang Ha and Truong Uyen Ninh. Virological surveillance of dengue haemorrhagic fever in Viet Nam, 1987-1999. Dengue Bulletin. 2000, 24: 18-23.

52 Dengue Bulletin – Vol 27, 2003
Circulation of Dengue Viruses in North-Western Peru, 2000-2001€
by Ysabel Montoya*, Susan Holechek*, Omar Caceres*, Ana Palacios**,
James Burans***, Carolina Guevara***, Fernando Quintana**, Victor Herrera�, Edwar Pozoψ, Elizabeth Anaya*, Enrique Mamani*, Victoria Gutierrez*, Adriana Ladron de Guevara��, Eduardo Fernandez���, Percy Asmat���,
Victor Alva-Davalos¶, Carlos Hoguin¶, V Alberto Laguna**, Ana M Morales**, Percy Minaya** and Tadeusz Kochel***#
*National Institute of Health, Peru **General Office of Epidemiology, Peru
***U.S. Naval Medical Research Center Detachment, Lima, Peru �Ministry of Health Regional Reference Laboratory, Tumbes, Peru
��Ministry of Health Regional Reference Laboratory, Lambayeque, Peru ���Ministry of Health Regional Reference Laboratory, La Libertad, Peru
¶Ministry of Health Regional Reference Laboratory, Piura, Peru ψMinistry of Health CICE-Luciano Castillo Colonna Sub-Region, Querecotillo, Peru
Abstract Prior to 2000, only DEN-1 and the American genotype DEN-2 viruses were isolated in Peru. During the dengue outbreak from May 2000 to May 2001 in the North-west departments of Peru, clinical data and blood samples were obtained from 1,652 patients who presented clinical manifestations comparable with those of dengue. Virus genome isolations were made from 278 (16.8%) of the samples. Serotype-specific monoclonal antibodies and polymerase chain reaction (PCR) were used to type isolations. The genotype of the majority of the DEN-2 isolations was determined by the restriction fragment length polymorphism (RFLP) analysis. Members of each serotype and two genotypes of DEN-2 virus were isolated: DEN-1 (n=93); Asian genotype DEN-2 (n=104); American genotype DEN-2 (n=1); DEN-2 genotype not determined (n=53); DEN-3 (n=25); and DEN-4 (n=2). Representatives of each serotype, and genotype for DEN-2, were confirmed by partial sequence analysis. Dengue antibodies as determined by Plaque Reduction Neutralization Test (PNT) were present in the acute serum from the single DHF Grade-II patient, in 19 of 31 (61%) acute sera from patients with DHF Grade-I and in 3 of 45 (7%) acute sera of DF patients, suggesting an association between pre-existing dengue antibody and disease severity.
Keywords: Dengue viruses, dengue transmission, dengue outbreak, Peru.
€ This research was supported by the US Naval Medical Research and Development Command NMMC, Bethesda, MD, Work Unit No 62787A8701447. The opinions and assertions contained herein are the private ones of the authors and are not to be construed as official or reflecting the views of the Navy Department of the Navy Service at large. # For correspondence: Naval Medical Research Center, Silver Spring, Maryland 20910-7500, USA; E-mail: [email protected]

Dengue Viruses of Peru, 2000-2001
Dengue Bulletin – Vol 27, 2003 53
Introduction Dengue viruses are single-stranded, positive-sense RNA viruses that belong to the genus Flavivirus, family Flaviviridae and they are transmitted primarily by the Aedes aegypti mosquito(1). There are four serotypes of dengue viruses (DEN 1-4), each of which can cause disease(2). Over the past 40 years, the number of DF cases has increased at least twentyfold and the number of DHF cases has similarly increased over the same time-period(3).
With the re-establishment of the Aedes aegypti vector in central and south America, the region observed an increased dengue virus activity and all four serotypes of dengue viruses are now widely distributed(4,5).
Epidemics of DF fever caused by DEN-2 and DEN-3 were reported from the Caribbean and northern South America in the 1960s and 1970s, respectively, and with the introduction of DEN-1 into the region in 1977, widespread epidemics of DF occurred in many different countries throughout Latin America(4,5,6). Although multiple serotypes of dengue virus were circulating in the Americas during the 1970s, no outbreak of DHF occurred until 1981 when the Asian genotype DEN-2 virus was introduced into Cuba(5,6). Since then, this virus and DHF have spread across the Americas.
Epidemiological studies have shown that the severity of the disease can be dependent on the infecting virus and on the individual’s previous history of infection by dengue viruses(7). Evidence of both mechanisms of dengue pathogenesis can be seen in the Americas. A primary dengue infection will usually be either sub-clinical or cause DF and the individual will develop
immunity to the infecting serotype of virus. Heterotypic immunity is short-lived and sequential heterotypic infections are hypothesized to lead to an increased disease severity by an antibody-dependent enhancement mechanism (ADE)(8,9). Increased disease severity has been associated with all combinations of sequential infections, but a greater percentage of the cases with the sequential infection combination of DEN-1, followed by DEN-2, have led to increased disease severity(10,11). In Peru, DEN-1 and the American genotype, DEN-2 virus, have been circulating since the 1990s without DHF(12,13). The lack of DHF may be attributed to a heterologous neutralization phenomenon. Sera from DEN-1-immune individuals cross-neutralize American, but not Asian, genotype DEN-2 virus in vitro(14). This heterologous neutralization is unidirectional (DEN-1 to American genotype DEN-2 only), and it was expected that when the other serotypes (and genotypes for DEN-2) of dengue virus were introduced into Peru, no heterologous protection (other than against the American genotype DEN-2 virus) would be available to individuals and DHF would be observed. By 2000, all four serotypes of dengue virus, with the Asian genotype representing most isolates of DEN-2, were present in countries of the region, including Peru(15).
From May 2000 to May 2001, 28,815 cases of DF and 251 cases of DHF were reported by the Peruvian Ministry of Health in the Northwest Departments of Peru(16,17). Blood samples were collected from 1,652 clinically-presenting dengue patients for the purpose of identifying the etiological agent(s) of the outbreak and to further our understanding of the pathogenesis of dengue viruses.

Dengue Viruses of Peru, 2000-2001
54 Dengue Bulletin – Vol 27, 2003
Materials and methods
Sample collection
During the outbreak, the regional clinics and hospitals in north-western Peru collected blood samples from patients with symptoms consistent with dengue disease (n=1,652), either dengue fever or a grade of dengue haemorrhagic fever as defined by the World Health Organization(18). Sera were prepared and stored at –700C until they were delivered on dry ice to laboratories in Lima, Peru, for virus isolation and antibody testing. Clinical and demographic data were collected from all sample-donating patients.
Virus isolation and identification
Sera were tested for virus in C6/36 cells propagated in T-25 cm2 flasks and viral isolates were identified by indirect fluorescent antibody testing using anti-dengue polyclonal and dengue serotype 1-4-specific monoclonal antibodies(19,20). The serotypes of virus isolates were confirmed by serotype-specific PCR(21). The genotypes of the DEN-2 virus isolates were determined by Restriction fragment length polymorphism (RFLP) analysis(22). The capsid, premembrane and envelope genes of representative DEN-1, DEN-3, DEN-4 and DEN-2 American and Asian genotype virus isolates were sequenced using the following protocol. PCR amplified envelope fragments were purified and ligated into the pGem-T vector (Promega). Recombinant plasmids were transformed in E. coli strain DH5α and purified by alkaline lysis. The nucleotide sequences of inserts were determined by primer extension dideoxy chain termination
method using AutoCycle Sequencing Kits and Taq Polymerase (Amersham Pharmacia Biotech) and an ALF Express Automatic DNA Sequencer.
Serology
Plaque Reduction Neutralization Test (PRNT)
A modified PRNT protocol of Morens et al was followed(23). Test sera were diluted twofold in media (E-MEM + Pen./Strep.) from 1:5 to 1:5,120. 200 ul media containing 40 to 80 PFU of assay virus was mixed with 200 ul diluted test serum and then incubated at 40C for 15 hours. In triplicate, 100 ul virus-serum mixture was added to 0.5 ml media containing 1.5 X 105 BHK21 cells and then added to a well of a 24-well tissue culture plate and incubated at 370C with 5% CO2 for three hours. The cells were then overlaid with 0.5 ml of overlay media (0.6% carboxymethyl cellulose, MEM w/o Phenol Red, 10% FBS, 0.075% NaHCO3 and Pen./Strep.) and incubated at 370C with 5% CO2 for five days. The media was then removed, the cells were rinsed with H2O and stained with 0.5 ml/well stain solution (0.1% (w/v) Naphthol Blue Black, 1.36% (w/v) Sodium Acetate, and 6% (v/v) Glacial Acetic Acid) for 30 min. The stain was removed and the plaques were counted. The results were expressed as the serum dilution, determined by probit analysis that reduced the number of plaques by 50% compared to that of normal human serum at the same dilution. A PRNT50 titer <1:20 was considered negative; a PRNT50 titer >1:20 was considered positive.

Dengue Viruses of Peru, 2000-2001
Dengue Bulletin – Vol 27, 2003 55
PRNT and RFLP viruses
DEN-1 virus 16007, DEN-3 virus 16562 and Asian genotype DEN-2 virus 16681 were isolated in Thailand in 1964 from DHF cases(2). DEN–4 virus 1036 was obtained from ATCC. The American genotype DEN-2 virus IQT 2913 was isolated in Iquitos, Peru, in 1996, by the Naval Medical Research Center Detachment, Lima, Peru.
IgM ELISA
Dengue IgM antibody capture ELISA were performed following the protocol of Wu, et al(24), with the substitution of DEN-1 virus suckling mouse brain preparation for cell culture supernatants DEN-1 virus preparation as antigen(24). Acute specimens with optical density readings two standard deviations higher in dengue antigen wells than negative antigen wells were positive. For paired sera, the criterion for seroconversion was a fourfold increase in antibody titer in the convalescent specimen as compared to that of the acute specimen.
Results Sera samples were collected from 1,652 patients presenting symptoms consistent with dengue. 171 of the patients also provided convalescent sera samples. Based on signs and symptoms the specimens were divided into three categories, those that were from DF (1,481), from DHF Grade-I (170) and from DHF Grade-II (1) patients. The most frequently observed symptoms were fever, chills, eye pain and body pain (Table 1). Anti-dengue IgM antibodies were present in 18.7% of the acute sera and 52.1% of the paired sera exhibited dengue IgM seroconversion. Dengue viruses were isolated from 278 (16.8%) of the total sera samples.
Table 1. Clinical symptoms and presentation
Symptoms %
Fever 100 Headache 98 Chills 82 Eye pain 82 Myalgia 81 Joint pain 45 Nausea, vomiting 47 Sore throat 40 Cough 36 Nasal congestion 28 Rash 28 Diarrhea 22 Malaise 14 Muscle pain 14 Bloody nose 6 Bloody gums 4 Jaundice 3 Bloody feces 3 Lack of appetite 3 Bone pain 4 Bloody vomit 2 Vaginal hemorrhage 2 Bloody urine 1 Abdominal pain 2 Photophobia 0.6 Itching 0.5 Enlarged lymph nodes 0.3 Cold skin 0.3 Pale 0.1 Unconsciousness 0.07 Rapid pulse 0.07 Presentation Number %
DF 1,481 89.7 DHF Grade-I 170 10.3 DHF Grade-II 1 0.06

Dengue Viruses of Peru, 2000-2001
56 Dengue Bulletin – Vol 27, 2003
Serotype isolation vis-à-vis disease manifestation included DEN-1 (93: DF - 89, DHF Gr.I - 4), DEN-2 (158: DF – 150, DHF Gr.I – 8), DEN-3 (25: DF – 23, DHF Gr.I – 2), DEN-4 (2: DF). No isolation was made for the lone DHF Gr.II case. The geographical distribution of the dengue isolates in north-western Peru, by serotype, for the year 2000-2001 is shown in Figure 1. DEN-1 virus was first isolated in La Libertad Department (May 2000) and subsequently in Piura (June 2000),
Lambayeque (February 2001) and Tumbes (April 2001). DEN-2 was first isolated in Tumbes (June 2000), followed by Piura (June 2000) and then La Libertad (February 2001) and Lambayeque (March 2001). DEN-3 was first isolated in Piura (August 2000), followed by Tumbes (September 2000) and the most southern affected department, Ancash (March 2001). DEN-4 was isolated in the department of Tumbes (June 2000) and subsequently detected by PCR in Piura (January 2001).
BOLIVIA
TUMBESDEN-1, DEN-2,DEN-3, DEN-4
ECUADOR
COLOMBIA
BRAZIL
CHILE
PACIFIC OCEAN
PIURADEN-1, DEN-2DEN-3, DEN-4
LA LIBERTADDEN-1, DEN-2
Lima, Capital of Peru
LAMBAYEQUEDEN-1, DEN-2
ANCASHDEN-3/
DEN-1*
DEN-2*
* DEN-1, DEN-2 (American genotype) in circulation in Peru since 1990
Figure 1. Dengue in north-west Peru, May 2000-May 2001

Dengue Viruses of Peru, 2000-2001
Dengue Bulletin – Vol 27, 2003 57
Since American and Asian genotypes of DEN-2 virus have been in circulation in the southern hemisphere, RFLP analysis was performed on the majority of the DEN-2 isolates to determine their genotype. Representative restriction digests of Asian and an American genotype DEN-2 virus isolates are shown in Figure 2. The DEN-2 isolates of lanes 5-7 yield restriction patterns
identical to the marker Asian genotype virus, lane 3. The DEN-2 isolate of lane 8 has an identical restriction pattern to the American genotype marker virus of lane 4. Greater than 99% (104/105) of the samples tested were of the Asian genotype. Only one isolate, from Piura, was of the American genotype.
Figure 2. RFLP Analysis of DEN-2 Isolates‡
1600 bp --
2400 bp --
100 bp --
200 bp --
400 bp --
800 bp --
1 2 3 4 5 6 7 8
1600 bp --
2400 bp --
100 bp --
200 bp --
400 bp --
800 bp --
1 2 3 4 5 6 7 8
[Lane 1: DNA molecular weight ladder, marker sizes are listed in the photo margin; lane 2: no template RT/PCR control reaction; lane 3: 295216 Asian DEN-2 marker virus; lane 4: IQT2124 American genotype DEN-2 marker
virus; lane 5-8: OBT 396, OBT 1242, OBT 1243 and OBS 9638 viruses, respectively.]
‡ RT/PCR products of DEN-2 virus isolates were digested with Alu I, electrophoresed through a 2.0% agarose gel, stained with ethidium bromide and photographed.
To further identify the viruses of the outbreak, portions of the capsid, premembrane and envelope genes of representative isolates of each serotype, and genotype for DEN-2, were sequenced. The
sequence of the DEN-1 isolates was ninety-eight per cent identical to DEN-1 viruses that were isolated in Peru in 1997. Similarly, the sequence of the American genotype DEN-2 isolates was 98% identical to an American

Dengue Viruses of Peru, 2000-2001
58 Dengue Bulletin – Vol 27, 2003
genotype isolate from Iquitos, Peru, during 1996. The Asian DEN-2 isolates were 98% identical to the Asian DEN-2 isolates of Maracay, Venezuela, in 1998. The DEN-3 isolates were 98% identical to the DEN-3
isolates of Guatemala (1998) and DEN-4 isolates were 98% identical to the DEN-4 isolates of the Dominican Republic (1981) (Table 2).
Table 2. Identity of representative dengue virus isolates
Serotype Gene Accession
number and strain
Place and year of
isolation
Accession number and
strain
Country and year
Identity (%)
DEN-1 E AF378171 Peru 9808-00
Piura, 2000 AF378172 Peru 5189-97
Peru 1997
98.03
DEN-2 Asian Genotype
E AY079424 Sullana 6663-01
Piura, 2001 AF163096 PTCOL 96
L10041 Clone 2A
AY044442 Mara 3
Colombia 1996
Brazil 1990
Venezuela 1990
98.529
98.162
97.61
DEN-2 American Genotype
E AF378163 Peru 9638-00
Piura, 2000 AF100465 Ven 2 AF264054 PR 152 AF100468 IQT 2913
Venezuela 1987 Puerto Rico 1969 Peru 1996
98.32
98.13
98.13
DEN-3 C/PrM AY079175 Peru 6682-01
Piura, 2001 AB038475 Guate 98-2
Guatemala 1998
98
DEN-4 C/PrM AY079176 Peru 6682-01
Piura, 2001 AF326573 Dominica 81
Domincan Republic 1981
98
Since DEN-1 and the American
genotype DEN-2 viruses have been in circulation in Peru during the last decade, it was expected that some persons infected with dengue viruses during this outbreak were experiencing secondary infections. In order to determine if pre-existing dengue antibodies influenced the disease presentation, the acute sera dengue antibody status of individuals with DF (n=45) and the more severe illnesses of DHF Grade-I (n=31) or DHF Grade-II
(n=1) were determined by PRNT. Primary dengue infections were identified by the absence of any dengue virus neutralizing antibody in the acute sera, while acute sera from secondarily infected individuals contained dengue neutralizing antibody against at least one serotype dengue virus. The acute sera that were selected for this analysis were dengue IgM antibody negative and were possible sera from which dengue virus had been isolated. Dengue viruses were

Dengue Viruses of Peru, 2000-2001
Dengue Bulletin – Vol 27, 2003 59
isolated from all 45 sera of DF-presenting patients, while dengue viruses were isolated from the sera of only four of the 31 patients that had DHF Grade-I, and no virus was isolated from the lone DHF Grade-II specimen that was available for analysis. By
PRNT, 7% (3 of 45) of the DF cases showed evidence of secondary heterologous serotype infections, while 61% (19 of 31) of the DHF Grade-I cases showed evidence of secondary heterologous serotype infections as did the DHF Grade-II case (Table 3).
Table 3. Dengue serostatus vs. disease severity
Disease 1o infection number Isolated virus 2o infection
number Pre-existing
antibody Isolated
virus
DF 42 DEN-1 (n=6) DEN-2 (n=31) DEN-3 (n=5)
3 DEN-1 (n=3) DEN-2 (n=2) DEN-3 (n=1)
DHF Grade I
12 DEN-2 (n=1) DEN-3 (n=1)
19 DEN-1 (n=5) DEN-2 (n=14)
0 DEN-1 (n=1) DEN-3 (n=1)
DHF Grade II
0 0 1 DEN-2 (n=1) 0
Discussion Here we report the isolation and characterization of DEN-1, DEN-2 (Asian genotype), DEN-2 (American genotype), DEN-3 and DEN-4 viruses as the etiological agents of the May 2000–May 2001 dengue outbreak in north-western Peru. Along with the introduction of the DEN-2 Asian genotype, DEN-3 and DEN-4, Peru has seen her first DHF Grade-II cases.
The viruses that were isolated during this outbreak were not new to South America. DEN-1 and the American genotype DEN-2 viruses have been in circulation in Peru prior to this outbreak and the Asian genotype DEN-2, DEN-3 and DEN-4 viruses are genetically identical to those that were isolated in Ecuador during a dengue outbreak six months prior to the Peruvian
outbreak(25). We speculate that the ease of trans-border travel between Ecuador and Peru facilitated the transmission of these dengue viruses into north-west Peru. The geographical distribution of virus isolates demonstrated the co-circulation of multiple serotypes, and genotypes of DEN-2, of dengue virus during this outbreak. The greatest number of virus isolations was made in Piura where DEN-1, DEN-2 (American and Asian genotypes), DEN-3 and DEN-4 viruses were isolated. Piura was also the department with the greatest number of severe cases. DEN-4 was the least isolated virus of this outbreak with only two isolations in the Tumbes department and one identification by PCR in the Piura department. DEN-4 was not isolated from the southern departments, but we cannot rule out its presence there, since acute sera from only a fraction of the clinically-

Dengue Viruses of Peru, 2000-2001
60 Dengue Bulletin – Vol 27, 2003
presenting patients were available for virus testing. The same possibility exists for the other departments where a serotype of dengue was not isolated. It must be noted that DEN-1 cases were being seen in the most southern city of Casma in the southern department of Ancash during the preparation of this manuscript.
Since we have isolated the American DEN-2 virus from this outbreak and from the outbreak in Ecuador the year before, it raises other possibilities to the hypothesis that the Asian DEN-2 virus has displaced the American DEN-2 virus in South America(7). Possibly, the American DEN-2 virus is less virulent, so infected people do not seek medical attention, and hence it is isolated less often. Support for this hypothesis comes from this report where 73% (14/19) secondary infected individuals with DHF Grade-I and the lone DHF Grade-II individual had DEN-2 antibodies in their acute sera. These antibodies were presumably from American genotype DEN-2 infections, since the Asian genotype DEN-2 virus had not been previously isolated in Peru. To avoid misinterpreting PRNT results for the determination of pre-existing dengue antibody, only IgM negative specimens were considered for this portion of the study.
Explanations of the pathogenesis of dengue have focused on two non-exclusive hypotheses, viral determinants and ADE(26,27,28). Evidences for both the theories exist in the Americas. The American genotype DEN-2 virus is relatively avirulent, while the Asian genotype DEN-2 virus is associated with severe disease(7,13). DEN-1 antibody positive individuals secondarily infected with the American genotype DEN-2 virus did not develop DHF Grade-II in Iquitos, Peru, while in other dengue
outbreaks in Central and South America, DEN-1 antibody-positive individuals secondarily infected with the Asian genotype of DEN-2 did(4,29,30). Here we report that the DHF Grade-II case and 61% of the DHF Grade-I cases were the products of secondary infections, while only 7% of DF patients had pre-existing dengue antibodies. This finding is supportive of the hypothesis that secondary heterologous infections result in a higher frequency of severe dengue disease as compared to primary dengue infections, but it must be noted that we are reporting on patients with DHF Grade-I and only one DHF Grade-II case. However, the trend of disease severity with pre-existing antibodies is evident. Few isolations were made from specimens from DHF Grade-I patients (4/31) and no virus was isolated from the DHF Grade-II patient’s sera. Possibly those samples were collected in the post-viremic stages of the illness or the virus isolation process was complicated by pre-existing antibody. Unfortunately, for the majority of the DHF Grade-I specimens and that of the DHF Grade-II patient, only clinical presentations were available for assignment of dengue disease.
Future studies are aimed at furthering our understanding of the transmission and pathogenesis of dengue viruses in South America.
Acknowledgements We thank Zonia Rios, Vidal Felices and Angelica Espinoza for technical assistance with virus isolation, PCR and RFLP, and PRNT assays, respectively. We also thank Juan Perez for data management assistance and Curtis Hayes and Douglas Watts for a critical review of this manuscript.

Dengue Viruses of Peru, 2000-2001
Dengue Bulletin – Vol 27, 2003 61
References1. Chambers TJ, Hahn CS, Galler R and Rice CM.
Flavivirus genome organization, expression and replication. A. Rev. Microbiol, 1990, 44: 649-688.
2. Leitmeyer KC, Vaughn DW, Watts DM, Salas R, Villalobos I de, Chacon Ramos C and Rico-Hesse R. Dengue virus structural differences that correlate with pathogenesis. J Virol, 1999, 73(6): 4738-4747.
3. World Health Organization, Removing obstacles to health. World Health Organization, 1999.
4. Pinheiro FP and Corber SJ. Global situation of dengue and dengue haemorrhagic fever and its emergence in the Americas. World Health Stat Q, 1997, 50(3-4): 161-169.
5. Gubler DJ. The global pandemic of dengue/dengue haemorrhagic fever: Current status and prospects for the future. Ann Acad Med Singapore, 1998, 27(2): 227-234.
6. Isturiz RE, Gubler DJ and Brea del Castillo J. Dengue and dengue haemorrhagic fever in Latin America and the Caribbean. Infect Dis Clin North Am, 2000, 14(1): 121-140, ix.
7. Rico-Hesse R, Harrison L M, Salas RA, Tovar D, Nisalak A, Ramos C, Boshell J, de Mesa MT, Nogueira RM and da Rosa AT. Origins of dengue type 2 viruses associated with increased pathogenicity in the Americas. Virology, 1997, 230(2): 244-251.
8. Halstead SB and Simasthien P. Observations related to the pathogenesis of dengue haemorrhagic fever II. Antigenic and biological properties of dengue viruses and their association with disease response in the host. Yale J Biol Med, 1970, 42: 276-292.
9. Kliks SC, Nisalak A, Brandt WE, Wahl L and Burke DS. Antibody-dependent enhancement of dengue virus growth in human monocytes as a risk factor for dengue haemorrhagic fever. Am J Trop Med Hyg, 1989, 40(4): 444-451.
10. Sangkawibha N, Rojanasuphot S, Ahandrik S, Viriyapongse S, Jatanasen S, Salitul V, Phanthumachinda B and Halstead SB. Risk factors in dengue shock syndrome: A prospective epidemiologic study in Rayong, Thailand. The 1980 outbreak. Am J Epidemiol, 1984, 120(5): 653-669.
11. Guzman MG, Kouri G, Bravo J, Soler M and Martinez E. Sequential infection as risk factor for dengue haemorrhagic fever/dengue shock syndrome (DHF/DSS) during the 1981 dengue haemorrhagic Cuban epidemic. Mem Inst Oswaldo Cruz, 1991, 86(3): 367.
12. Phillips I, Need J, Escamilla J, Colan E, Sanchez S, Rodriguez M, Vasquez L, Seminario J, Betz T and da Rosa AT. First documented outbreak of dengue in the Peruvian Amazon region. Bull Pan Am Health Organ, 1992, 26(3): 201-207.
13. Watts DM, Porter KR, Putvatana P, Vasquez B, Calampa C, Hayes CG, Halstead SB. Failure of secondary infection with American genotype dengue 2 to cause dengue haemorrhagic fever. Lancet, 1999, 354(9188): 1431-1434.
14. Kochel TJ, Watts DM, Halstead SB, Hayes CG, Espinosa A, Felices V, Caceda R, Buatista CT, Montoya Y, Douglas S and Russell KL. Effect of dengue-1 antibodies on American dengue-2 viral infection and dengue haemorrhagic fever. Lancet, 2002, 360(27 Jul): 310-312.
15. PAHO, Dengue in the Americas 2000 and Dengue in the Americas 2001, in Pan American Health Organization Travel Medicine Programme. 2002.
16. PAHO, Dengue Cases 2000.
17. PAHO, Dengue Cases 2001.
18. World Health Organization, Technical guidelines for diagnosis, treatment and control of dengue haemorrhagic fever. 2nd ed, WHO, 1997, Geneva.
19. Tesh RB. A method for the isolation and identification of dengue viruses, using mosquito cell cultures. Am J Trop Med Hyg, 1979, 28(6): 1053-1059.
20. Igarashi A. Isolation of a Singh's Aedes albopictus cell clone sensitive to dengue and chikunggunya viruses. J Gen Virol, 1978, 40: 531-544.
21. Lanciotti RS, Calisher CH, Gubler DJ, Chang G and Vordam V. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J Clin Microbiol, 1992, 30(3): 545-551.

Dengue Viruses of Peru, 2000-2001
62 Dengue Bulletin – Vol 27, 2003
22. Vorndam V, Kuno G and Rosado N. A PCR-restriction enzyme technique for determining dengue virus subgroups within serotypes. J Virol Meth, 1994, 48(2-3): 237-244.
23. Morens DM, Halstead SB, Repik PM, Putvatana R and Raybourne N. Simplified plaque reduction neutralization assay for dengue viruses by semimicro methods in BHK-21 cells: comparison of the BHK suspension test with standard plaque reduction neutralization. J Clin Microbiol, 1985, 22(2): 250-254.
24. Wu SJ, Hanson B, Paxton H, Nisalak A, Vaughn DW, Rossi C, Henchal EA, Porter KR, Watts DM and Hayes CG. Evaluation of a dipstick enzyme-linked immunosorbent assay for detection of antibodies to dengue virus. Clin Diag Lab Immunol, 1997, 4(4): 452-457.
25. Kochel TJ. Unpublished Result. 2001.
26. Halstead SB. Pathogenesis of dengue: Challenges to molecular biology. Science, 1988, 239(4839): 476-481.
27. Rosen L. "The emperor's new clothes" revisited, or reflections on the pathogenesis of dengue haemorrhagic fever. J Trop Med Hyg, 1977, 26: 337-343.
28. Gubler DJ and Kuno G. Dengue and dengue haemorrhagic fever. 1997: CAB International.
29. Guzman MG, Kouri G, Valdes L, Bravo J, Vazquez S and Halstead SB. Enhanced severity of secondary dengue-2 infections: Death rates in 1981 and 1997 Cuban outbreaks. Rev Panam Salud Publica, 2002, 4(Apr 11): 223-227.
30. Guzman MG, Alvarez M, Rodriguez R, Rosario D, Vazquez S, Valdes L, Cabrera MV and Kouri G. Fatal dengue haemorrhagic fever in Cuba, 1997. Int J Infect Dis, 1999, 3(3): 130-135.

Dengue Bulletin – Vol 27, 2003 63
Exploratory Temporal and Spatial Distribution Analysis of Dengue Notifications in Boa Vista, Roraima,
Brazilian Amazon, 1999-2001†
by
Maria Goreti Rosa-Freitas*, Pantelis Tsouris**#, Alexander Sibajev***, Ellem Tatiani de Souza Weimann**, Alexandre Ubirajara Marques**,
Rodrigo Lopes Ferreira** and José Francisco Luitgards-Moura***
*Laboratório de Transmissores de Hematozoários, Departamento de Entomologia, Instituto Oswaldo Cruz, Av. Brasil 4365, Manguinhos, 21045-900 Rio de Janeiro, RJ, Brasil
**Núcleo Avançado de Vetores – Convênio FIOCRUZ-UFRR BR 174 S/N - Boa Vista, RR, Brasil ***Centro de Ciências Biológicas e da Saúde, UFRR, BR 174 S/N - Boa Vista, RR, Brasil
Abstract
In Brazil, as in the rest of the world, dengue has become the most important arthropod-borne viral disease of public health significance. Roraima state presented the highest dengue incidence coefficient in Brazil in the last few years (224.9 and 164.2 per 10,000 inhabitants in 2000 and 2001, respectively). The capital, Boa Vista, reports the highest number of dengue cases in Roraima. This study examined the temporal and spatial distribution of dengue in Boa Vista during the years 1999-2001, based on daily notifications as recorded by local health authorities. Temporally, dengue notifications were analysed by weekly and monthly averages and age distribution and correlated to meteorological variables. Spatially, dengue coefficients, premises infestation indices, population density and income levels were allocated in a geographical information system using, Boa Vista 49 neighbourhoods as units. Dengue outbreaks displayed distinct year-to-year distribution patterns that were neither periodical nor significantly correlated to any meteorological variable. There were no preferences for age and sex. The derived maps showed that premises infestation indices, population density, income and dengue incidence were concentrated along a central horizontal east-west axis. Major risk areas of transmission during the three consecutive years were the central neighbourhoods. These neighbourhoods are of the highest income population in the city.
Keywords: Dengue, spatial information, Roraima, Brazil.
#For correspondence: [email protected] † This work was supported by the Brazilian Council for Science and Development-CNPq (521176/98-0), the Oswaldo Cruz Institute-FIOCRUZ and the Roraima Federal University-UFRR

Dengue in Boa Vista, Roraima, 1999-2001
64 Dengue Bulletin – Vol 27, 2003
Introduction The state of Roraima is located in the Amazon region at the border of Guyana and Venezuela. An outbreak with 12,000 dengue cases (incidence rate of 1,160/10,000 inhabitants) was registered in 1981-1982 in Boa Vista, Roraima(1,2). It was during this outbreak that dengue was diagnosed in Brazil by laboratory tests and isolated from human hosts and mosquito vectors for the first time (3). Currently, dengue is reported in all the 27 states in Brazil; 87% of these are situated in the south-eastern and north-eastern regions(4). Even though these regions report the largest number of cases, the importance of Roraima is due to the fact that this state alone presented the country’s highest coefficients of dengue incidence, i.e. 224.9 and 164.2 (per 10,000 inhabitants) for the years 2000 and 2001, respectively(4). Dengue is also assumed to display a seasonal variation in Brazil, with the majority of the cases occurring in the rainy season (February to May). However, in Boa Vista, it may peak either in the rainy (April-November) or dry (December-March) seasons. This reflects the fact that hosts, parasites, vectors and environmental factors are all dynamic factors that vary temporally and spatially in an epidemiological system(5,6,7).
Temporal changes in the environment are driven mostly by meteorological variables that determine the relationship between hosts, parasites and vectors(8). Variables linked to the human population such as density and socioeconomic status have also been considered important(9,10). Analyses and projection of geographical data allow spatial visualization in relation to physical maps and facilitate comparisons of longitudinal investigations(11).
This study examines the temporal and spatial dengue notification data in Boa Vista, Roraima, for the years 1999-2001, taking into account some meteorological, entomological and demographic factors.
Materials and methods Place of study
Roraima has an area of 225,116 km2 and a population of 321,397(12). The rural population density is 1.4/km2, while the population density of its capital, Boa Vista, is 26/km2 (38% of the state population)(12,13,14). Approximately 85% of the Roraima state is under forest, with the remaining 15% covered by savanna(15). The capital, Boa Vista (02049’11”N, 60040’24”W), with an area of 122,000 km2, is located by the Branco river (Figure 1). Savanna is the predominant ecological environment in Boa Vista. The climate is tropical humid with an average temperature of 27.80C (10-year average)(16) and an average rainfall of 429 mm (4-year average)(16) with low annual variation. The climate presents two distinct seasons, a rainy season between April and November, with high rainfall indices during the months of June and July, and a dry season from December to March(17). The city has 49 neighbourhoods (bairros) (Law 483 of 9 December 1999). Formerly, these neighbourhoods were 19 in number. The Census 2000 data, available at the IBGE Internet site(12) contains old neighbourhoods. This re-division makes the comparison between the old and new data difficult, since some new neighbourhoods encompassed the areas of old ones. Many streams (igarapés) and rivers cross the city. Most urban lakes were drained and land filled to avoid becoming mosquito breeding sites.

Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 65
The main river is the Branco, which crosses the city in the north-westerly direction. Approximately 90% of the homes have sanitary installations (even though most of them are not linked to the sewage system),
are linked to the city water system and have routine trash collection(12). There are four general hospitals and 13 health units. Around 69% of the population is literate. The average annual income is US$ 714(12).
Branco River
BOA VISTA
BRAZIL
Amazon
VENEZUELA
GUYANA
Boa Vista
RORAIMA
Figure 1. Brazil, Roraima and Boa Vista neighbourhoods

Dengue in Boa Vista, Roraima, 1999-2001
66 Dengue Bulletin – Vol 27, 2003
Dengue notifications
Compulsory notification for dengue was started in 1996 in Boa Vista. The dengue data from 1982 to 1998 were not comprehensive and were therefore excluded from this study. From 1999 onwards dengue notifications were registered daily by both the municipal and state health secretariats (Secretaria do Estado de Saúde de Roraima-SESAU and Secretaria Municipal de Saúde-SEMSA). Our data refers to people reporting dengue-related symptoms such as high fever, headache, myalgia, arthralgia and dizziness. Dengue notifications were analysed daily, and weekly and monthly averages were calculated from these daily values. Epidemiological weeks were used for averaging (epidemiological weeks were counted from Sunday to Saturday). Age and sex of individuals reporting dengue were also analysed to establish their distribution throughout the period and in relation to the normal population curve. From the daily notification reports, the following data were used: date, epidemiological week of report, age and neighbourhood of residence. Age was analysed in ranges to facilitate a comparison with the age census data that uses this format.
Entomological data
Premises infestation indices for Aedes aegypti were collected by FUNASA-RR. Indices were partial, available for the year 2001 and for a certain number of neighbourhoods only. Aedes albopictus was not found in Boa Vista (FUNASA-RR, unpublished data).
Meteorological data
Meteorological data registered daily for the period 1999-2001, rainfall(mm), humidity(%), temperature(°C), wind direction(°), wind velocity (knot) and atmospheric pressure (hpa) were provided by the Boa Vista Air Force Base (June 1999 data was based on monthly averages) (Serviço Regional de Proteção ao Vôo de Manaus, Relatório Climatológico Diário, unpublished data).
Census data
The demographic data used in the analyses, based on the census performed on 31 July/1 August 2000(12) were age, sex, population and income. The population density and income were analysed according to neighbourhoods(14).
Spatial analyses
Dengue coefficients, premises infestation indices, meteorological values and census data were integrated in the Geographical Information System Arc View 3.2-based software using Boa Vista map layers (Multispectral). Spatial analyses units were the 49 neighbourhoods of the capital, Boa Vista. The dengue incidence per neighbourhood (per 10,000 inhabitants) was plotted using the dot tool (1 notification = 1 dot, spread by chance in the polygon area). The premises infestation indices and average income per neighbourhood were plotted using the gradient tool.

Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 67
Results
Temporal analyses
Daily analysis of dengue notifications is liable to error due to the unequal distribution of dengue notifications. Notifications on weekends and holidays were minimal (Figure 2). For that reason, dengue notifications were analysed by weekly averages. Dengue outbreaks displayed distinct year-to-year distribution patterns (Figure 3) that were neither periodical nor significantly correlated to any meteorological variable (Figures 4 and 5) (Table 1). During the period of this study, the average wind velocity was 3.5 m/s. Correlation between dengue and population density and income varied from -0.01 to 0.44 (Table 2). The premises infestation indices and dengue showed a negative correlation of -0.10 for the year 2001 (Table 1). The correlation between dengue notification incidences and meteorological variables ranged from -0.27 to 0.31 (Table 1). In addition, the dengue incidence data showed no significant correlation when compared to
meteorological values shifted four days backwards (time of report delay corresponding to the average intrinsic incubation period) (data not shown).
Table 1. Correlation between premises infestation, population density, income and
meteorological variables and dengue incidence for the period 1999-2001 in Boa
Vista, Roraima, Brazil
Dengue incidence
1999 2000 2001
Premises infestation - - -0.10
Population density -0.01 0.28 0.14
Income 0.40 0.44 0.40
Rainfall 0.12 0.03 -0.18
Humidity 0.18 0.04 -0.27
Temperature -0.23 -0.18 0.05
Wind direction -0.07 0.06 -0.16
Wind velocity -0.08 0.10 0.31
Atmospheric pressure 0.06 0.14 -0.08
- indicates data not available.
123
2,560
1,571
1,8241,7191,796
216
0
500
1,000
1,500
2,000
2,500
3,000
Saturday Sunday Monday Tuesday Wednesday Thursday Friday
Weekday
No.
of n
otifi
catio
ns
Figure 2. Dengue notifications by weekday distribution for the period 1999-2001 in Boa Vista, Roraima, Brazil
Variable

Dengue in Boa Vista, Roraima, 1999-2001
68 Dengue Bulletin – Vol 27, 2003
010,00020,00030,00040,00050,00060,00070,00080,00090,000
100,000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Month
Den
gue
Braz
il
1999 2000 2001
0100200300400500600700800900
1,000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Month
Den
gue
Rora
ima
1999 2000 2001
¶ Data from CENEPI-FUNASA 2001
Figure 3. Monthly averages of total dengue notifications in the 27 Brazilian states and in the Roraima state during 1999-2001¶
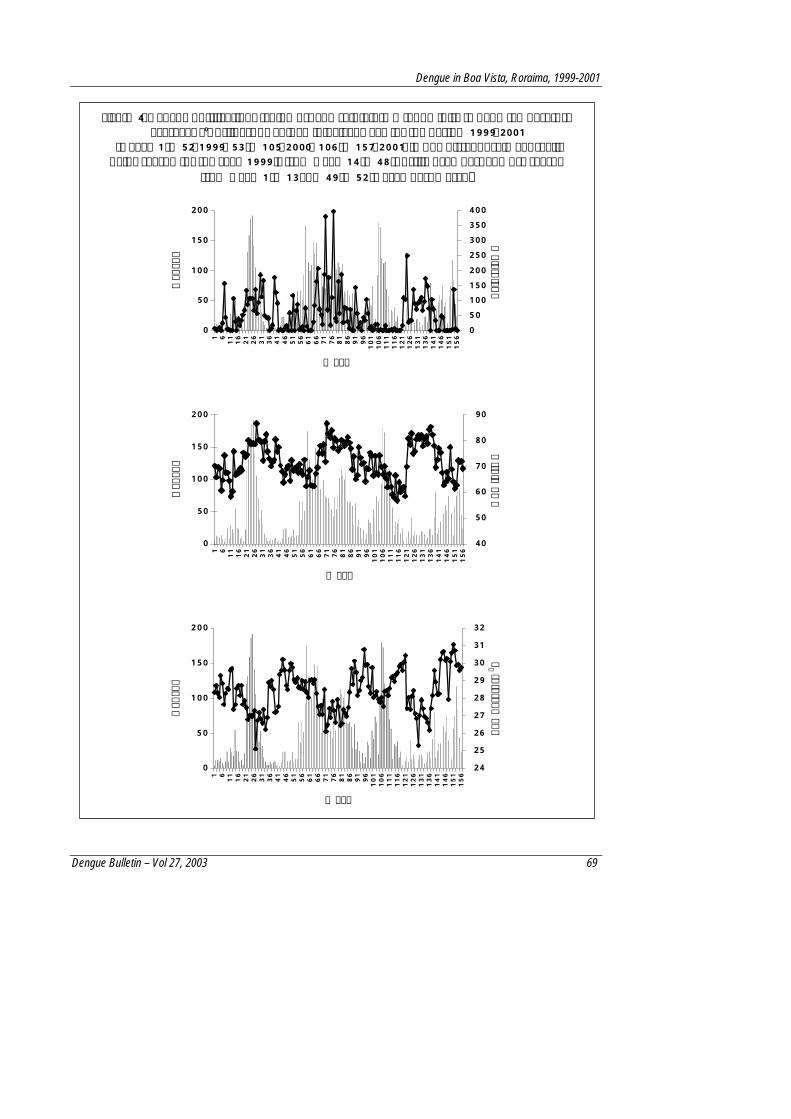
Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 69
0
50
100
150
2001 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
106
111
116
121
126
131
136
141
146
151
156
Week
Den
gue
050100150200250300350400
Rain
fall
mm
0
50
100
150
200
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
106
111
116
121
126
131
136
141
146
151
156
Week
Den
gue
40
50
60
70
80
90
Hum
idity
%
0
50
100
150
200
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
106
111
116
121
126
131
136
141
146
151
156
Week
Den
gue
24
25
26
27
28
29
30
31
32
Tem
pera
ture
o C
Figure 4. Dengue notifications (columns) and rainfall (mm), humidity (%) and temperature averages (0C) (lines) by epidemiological week for the period 1999-2001
(weeks 1 to 52-1999, 53 to 105-2000, 106 to 157-2001) in Boa Vista, Roraima, Brazil. Rainy season for the year 1999 is from week 14 to 48 (April-November) and dry season
from week 1 to 13 and 49 to 52 (December- March)

Dengue in Boa Vista, Roraima, 1999-2001
70 Dengue Bulletin – Vol 27, 2003
Figure 5. Dengue notifications (columns) and wind direction (°), wind velocity (knot) and atmospheric pressure (hpa) (lines) by epidemiological week for the period 1999-2001 (weeks 1 to 52-1999, 53 to 105-2000, 106 to 157-2001) in Boa Vista, Roraima, Brazil. Rainy season for the year 1999 is from week 14 to 48 (April -
November) and dry season from week 1 to 13 and 49 to 52 (December – March)
0
50
100
150
200
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
106
111
116
121
126
131
136
141
146
151
156
Week
Den
gue
0
50
100
150
200
250
Win
d D
irec
tion
º
0
50
100
150
200
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
106
111
116
121
126
131
136
141
146
151
156
Week
Den
gue
0
2
4
6
8
10
12
Win
d Ve
loci
ty k
not
0
50
100
150
200
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101
106
111
116
121
126
131
136
141
146
151
156
Week
Den
gue
996
998
1,000
1,002
1,004
1,006
1,008
1,010
Atm
osph
eric
Pre
ssur
e hp
a

Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 71
The population density showed an average positive correlation of 0.14 (Table 2). The average income per neighbourhood showed an average positive correlation of 0.41, indicating that neighbourhoods with higher incomes had a fairly accompanying increase in the number of dengue notifications. Dengue affected all ages
(Figure 6). The correlation values between age and dengue ranged from 0.93 (census and dengue in 1999) to 0.99 (census and dengue in 2000). Both sexes equally notified dengue. The ratios between males and females notifying dengue were 0.94 in 1999, 0.81 in 2000 and 1.09 in 2001 while in the population this ratio was exactly 1(12).
Table 2. Zones, neighbourhoods (bairros), population, average family income in US$, absolute number and incidence (per 10,000 inhabitants) of dengue notifications for the period
1999-2001 in Boa Vista, Roraima, Brazil
Dengue notifications Incidence
Zone Neighbourhood Population Density Income US$
1999 2000 2001 1999 2000 2001
Central Centro 6,057 22.1 799 168 264 126 277.37 435.86 208.02
Trinta e Um de Março 1,711 36.4 656 41 108 33 239.63 631.21 192.87
Aeroporto 2,741 2.6 412 1 3 12 0.00 10.94 43.78
Aparecida 5,165 33.4 726 41 165 94 79.38 319.46 181.99
Estados 4,560 52.2 585 36 246 91 78.95 539.47 199.56
Paraviana 3,104 7 898 10 74 30 32.22 238.40 96.65
São Francisco 4,024 23.6 989 29 206 114 72.07 511.93 283.30
North
Subtotal 21,305 25.9 711 158 802 374 74.16 376.44 175.55
Treze de Setembro 4,755 21.2 400 19 71 133 39.96 149.32 279.71
Calungá 2,070 24.3 483 6 33 42 28.99 159.42 202.90
Distrito Industrial Gov. Aquilino M. Duarte
177 0.2 204 1 0 1 56.50 0.00 56.50
Marechal Rondon 41 0.1 na 0 1 0 0.00 243.90 0.00
São Vicente 5,990 26.3 559 46 200 200 76.79 333.89 333.89
South
Subtotal 13,033 14.4 411.5 72 305 376 55.24 234.02 288.50
Caçari 2,913 3.6 1653 14 80 25 48.06 274.63 85.82
Canarinho 656 5.6 1401 2 13 8 30.49 198.17 121.95
São Pedro 1,072 18.4 977 73 15 28 680.97 139.93 261.19
East
Subtotal 4,641 9.2 1343.7 89 108 60 191.77 232.71 131.44
Alvorada 5,423 23.9 220 4 0 15 7.38 0.00 27.66
Asa Branca 10,017 53.3 335 21 315 215 20.96 314.47 214.64
Bela Vista 2,650 20.6 204 0 3 3 0.00 11.32 11.32
West
Buritis 8,693 46.8 382 42 226 308 48.31 259.98 354.31

Dengue in Boa Vista, Roraima, 1999-2001
72 Dengue Bulletin – Vol 27, 2003
Dengue notifications Incidence
Zone Neighbourhood Population Density Income US$
1999 2000 2001 1999 2000 2001
Caimbé 6,593 50 429 13 148 136 19.72 224.48 206.28
Cambará 4,110 43 485 15 30 36 36.50 72.99 87.59
Caranã 8,706 32.6 283 8 100 82 9.19 114.86 94.19
Cauamé 4,805 23.6 323 5 34 49 10.41 70.76 101.98
Centenário 3,677 14.5 310 5 22 8 13.60 59.83 21.76
Cidade Satélite 0 0 0 1 21 1 - - -
Cinturão Verde 1,683 9.3 310 3 15 28 17.83 89.13 166.37
Dr Silvio Botelho 7,011 51.9 245 0 1 10 0.00 1.43 14.26
Dr Silvio Leite 6,448 38.4 245 0 4 1 0.00 6.20 1.55
Equatorial 3,454 16.4 220 7 47 66 20.27 136.07 191.08
Jardim Caranã 2,235 30.7 283 0 0 5 0.00 0.00 22.37
Jardim Floresta 2,802 15.4 502 8 83 49 28.55 296.22 174.48
Jardim Primavera 3,306 41.6 265 5 37 41 15.12 111.92 124.02
Jardim Tropical 38 0.2 264 0 0 0 0.00 0.00 0.00
Hélio Campos 7,292 10.2 264 0 0 4 0.00 0.00 5.46
Jóquei Clube 4,493 18.4 310 6 117 28 13.35 260.41 62.32
Liberdade 6,275 56 405 19 261 143 30.28 415.94 227.89
Mecejana 6,108 21.5 742 20 172 89 32.74 281.60 145.71
Nova Canaã 3,770 82.1 245 5 20 25 13.26 53.05 66.31
Nova Cidade 1,545 5.9 204 0 4 10 0.00 25.89 64.72
Operário 1,020 2.4 198 0 1 1 0.00 9.80 9.80
Pintolândia 6,214 42 245 31 138 121 49.89 222.08 194.72
Piscicultura 911 25.3 265 5 51 7 54.88 559.82 76.84
Pricumã 6,797 34.9 708 14 192 160 20.60 282.48 235.40
Profa Araceli Souto Maior 777 1.7 198 2 11 0 25.74 141.57 0.00
Raiar do Sol 2,755 14.5 198 6 14 17 21.78 50.82 61.71
Santa Luzia 4,482 49.5 220 0 0 33 0.00 0.00 73.63
Santa Tereza 10,087 84.9 265 14 170 121 13.88 168.53 119.96
Tancredo Neves 6,735 47.6 265 12 217 101 17.82 322.20 149.96
União 1,150 10 283 0 0 10 0.00 0.00 86.96
Subtotal 152,062 30 303.5 271 2454 1923 17.821 161.341 126.431
Total Boa Vista 197,098 26 7141 758 40312 29623 33.201 172.241 125.251
Demographic data from the Roraima Section of the Geography and Statistics Brazilian Institute - IBGE-Roraima. The current 49 neighbourhoods division was carried out in December 1999 (Law 483 09/12/1999). Data for the new neighbourhoods is available only at IBGE-RR; Dengue data from SESAU; na = non available; 1mean, 2plus 98 and 3 plus 103 non-classified notifications.

Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 73
0
100
200
300
400
500
600
700
0 5 10 15 20 25 30Age
No.
of i
ndiv
idua
ls
1999 2000 2001 Census 2000
Spatial analyses
The dengue incidence, premises infestation index, population density and average income data plotted in maps indicated spatial variability at the neighbourhood level (Figures 7 and 8). The derived maps show that major risk areas of transmission were located in a central east-west horizontal axis 10.5 km from the Centro Cívico Square (02049’13.0”N, 60040’18.09”W). The dengue incidence coefficients showed that the three most affected neighbourhoods were: São Pedro, Centro, 31 de Março in 1999; 31 de Março, Piscicultura, Bairro dos Estados in 2000, and Buritis, São Vicente, São Francisco in 2001 (Figure 7) (Table 2). The premises infestation indices for Aedes
aegypti in 2001 showed that Santa Luzia, Paraviana and Buritis displayed the highest indices (Figure 8A) (Table 3). Neighbourhoods located in the central axis displayed premises infestation indices up to 13.73 (Figure 8A). Nonetheless, only 27 neighbourhoods were studied impairing further conclusions. The human population showed a concentration around the central axis (Figure 8B). The central and north-eastern areas of Boa Vista consisted of neighbourhoods with higher average family incomes (Figure 8C). The population density and average income are derived from the 2000 Census. The gradient map with dengue incidence for 2001 was plotted for comparison (Figure 8D).
Figure 6. Comparison of age distribution between individuals reporting dengue and population for the period 1999-2001 in Boa Vista, Roraima, Brazil

Dengue in Boa Vista, Roraima, 1999-2001
74 Dengue Bulletin – Vol 27, 2003
1999
2000
2001
Figure 7. Dengue notification coefficients per neighbourhood in Boa Vista, Roraima, for the period 1999-2001

Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 75
(A) (B)
(C) (D)
Figure 8. (A) Aedes aegypti premises infestation indices; (B) Population density; (C) Average family income (in US$) and (D) Dengue incidence per neighbourhood
for the year 2001 in Boa Vista, Roraima, Brazil

Dengue in Boa Vista, Roraima, 1999-2001
76 Dengue Bulletin – Vol 27, 2003
Table 3. Premises infestation indices for Aedes aegypti for 27 Boa Vista neighbourhoods, Roraima, Brazil, 2001
Neighbourhood House Index Breteau Index No. of premises
% of non-surveyed premises
Santa Luzia 13.73 13.73 102 3.8 Paraviana 2.44 2.44 164 24.1 Buritis 1.77 2.17 14,380 25.7 Tancredo Neves 1.72 1.84 5,586 22.5 Pricumã 1.41 1.78 16,965 31.2 Jardim Floresta 1.29 1.68 6,836 25.4 São Francisco 1.17 1.44 5,891 30 Dr Silvio Botelho 1.12 1.12 450 23.2 Caimbé 0.94 1.1 14,141 25.3 Caçari 0.91 1.36 4,418 32 Liberdade 0.88 1.03 12,378 26 Nova Canaã 0.88 0.88 1,138 28.3 Dr Silvio Leite 0.66 0.66 3,651 25.6 Santa Tereza 0.65 0.69 6,950 25.8 Caranã 0.61 0.67 4,937 26.3 Estados 0.59 0.72 6,270 27.5 Trinta e Um de Março 0.54 0.54 2,218 33.3 Cambará 0.53 0.55 6,398 29.7 Asa Branca 0.53 0.62 5,450 22.36 Canarinho 0.47 0.47 215 22.1 Centro 0.42 1.13 3,783 30 São Vicente 0.21 0.21 3,858 24.3 Jardim Primavera 0.1 0.1 2,882 25.3 Mecejana 0.08 0.08 1,292 20.6 Helio Campos 0.05 0.05 3,902 24.9 Alvorada 0.01 0.01 329 28.3 Treze de Setembro 0.01 0.01 0 29.9 Boa Vista 0.94 1.13 136,730 26.9
Data from FUNASA Dengue and Yellow Fever Antivectorial Service Information System-2001.
Types of breeding sites included: tyres, plant vases, discarded containers (construction material, car parts, glass or plastic bottles, aluminum cans), storage water containers (barrel, well, cistern, water tank), natural containers and swimming pools.
Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 77
Discussion Dengue is assumed to occur seasonally in Brazil, the majority of the cases occurring in the rainy period (February to May). Nonetheless, in Boa Vista, dengue cases may peak in either the rainy (April to November) or dry (December to March) seasons. This fact indicates that wide-ranging data analysis may not reflect local-level events. An understanding of the disease transmission at the local level can play a key role in the application of effective control measures.
Boa Vista has a strategic geopolitical position in Brazil. Neighboured by dengue endemic countries such as Venezuela and Guyana and a few hours’ travel from the Caribbean countries, it remains an inflowing spot for the disease and its vectors. The city of Boa Vista offers an above-average quality of life for an Amazonian city, with good infrastructural services and average income. Boa Vista also has good basic water and sanitary installations that are available in almost all houses in all neighbourhoods. Even so, endemic diseases such as dengue, malaria and Chagas’ disease present major public health problems for the urban population(18,19). The census data showed that most houses (95.8% of 196,687 premises) were linked to the city water system. Even though this data per se may not indicate that water supplies were indeed permanently available(9), the lack of large water storage receptacles inside and outside houses was indicative of the fact that water was fairly accessible (FUNASA unpublished data). Nonetheless, even though 96.5% of the houses have sanitary installations, the city sewage system is accessible to only 15.1%. Septic tanks are the most common method used here to treat sewage(13).
Our study used notifications of individuals presenting dengue-like symptoms reported daily to health authorities in Boa Vista. The preliminary serological survey pointed to the fact that only approximately 50% of the local notifications were actually confirmed by laboratory ELISA tests (LACEN, unpublished data). The unequal number of notifications on weekdays with rare reports occurring during weekends and holidays revealed the underestimated nature of data collected by spontaneous individual reports. Underestimation of cases is a common occurrence in reports that rely on passive registries(20,21,22). In a survey carried out among schoolchildren in the Rio de Janeiro metropolitan area, it was estimated that around one million dengue infections had occurred during the 1986-87 epidemics, while only tens of thousands were notified(20). Nonetheless, dengue infection coefficients seemed to vary in the same direction and proportion to the number of notifications as verified by a post-epidemic sero-epidemiological survey conducted in São Paulo, Brazil(21).
Previous data in the literature show dengue to display seasonal distribution following variation in meteorological factors(23,24,25). Dengue outbreaks in Boa Vista however, displayed distinct year-to-year distribution patterns, making prediction for intervention a complex task. Correlations between dengue notifications and meteorological variables were not significant. In an attempt to verify whether dengue notifications were correlated to meteorological values on the possible day of infection, meteorological values were shifted four days backwards in order to include the intrinsic incubation period(26) as the time of report delay. Again, there was no significant correlation. The absence of a correlation

Dengue in Boa Vista, Roraima, 1999-2001
78 Dengue Bulletin – Vol 27, 2003
between dengue incidence and rainfall indices and temperature was also observed in Puerto Rico(25). Although the temperature lagged three months behind the monthly dengue incidence (to include the extrinsic incubation period considered by the authors) tested significant, it was seen as a non-absolute determinant(25). These findings reaffirm the difficulty in making a seasonal dengue incidence prediction.
The weak correlation of dengue to meteorological variables could be explained by Aedes aegypti being a domesticated vector. Aedes aegypti, with its synanthropic habits, can find shelter with low fluctuations of temperature and humidity as well as abundant breeding and haematophagic sources in human dwellings(23,27). In Boa Vista, dengue affected all ages and both sexes following proportionally the age distribution among the population.
Dengue spatial analysis by neigh-bourhood levels, helped in a more detailed understanding of the epidemiological urban scenario. These smaller units better represent environmentally unified units, sharing a common landscape and socioeconomic characteristics(28). Even though statistical analysis showed a weak correlation between the parameters studied, one could observe the existence of spatial relationships (Figure 8). The concomitance of premises infestation and densely populated areas would account for such a distribution of dengue cases at that given moment. Big traffic arteries permit easy access to those areas. Demographic factors such as population density and income are related to the availability of blood sources and breeding sites. Premises infestation indices varied significantly from neighbourhood to neighbourhood. Approximately two-thirds of all premises and 55% of all neighbourhoods
were surveyed. While Santa Luzia displayed House and Breteau indices of 13.7, some neighbourhoods were free of infestation (Table 3). Premises infestation indices <1 and Breteau indices <5 are regarded as indicative of low transmission in a given area(29). Values, nonetheless, should be considered as an instantaneous finding that can rapidly modify due to the spreading of the vector(30,31) and the effectiveness of control campaigns. The lack of correlation between premises infestation indices and dengue cases showed that the risk factor will be linked to the nearby environment rather than to the house itself and will thus deserve better investigation. In Manaus, Pará state, large outdoor water containers were responsible for the maintenance of the Aedes aegypti density(32).
In Boa Vista, high-income neigh-bourhoods displayed a higher number of dengue cases. An average positive correlation of 0.41 indicates that neigh-bourhoods with higher incomes had a fairly high number of dengue notifications. A high number of dengue cases in individuals with high income was also observed in Fortaleza, Ceará state(22). Usually, populations with lower socio-economic conditions are found to be more affected(20,24,26,33,34). This is commonly due to the lack of basic services in lower socioeconomic communities where storage of water in non-covered receptacles and the disposing of utensils in the nearby peri-domestic environment are a frequent observation(9). Habits linked to rich populations, such as ways of construction of buildings, use of disposable containers(22), swimming pools(35), growing of ornamental plants(22,35), frequent travel to neighbouring endemic countries, and even a false sense of security(36) may interfere with the disease distribution. Recent results in Colima, Mexico, have indicated that educational campaigns

Dengue in Boa Vista, Roraima, 1999-2001
Dengue Bulletin – Vol 27, 2003 79
reduced the Aedes aegypti breeding sites more effectively than the use of chemical spraying(36).
Conclusion Small-scale temporal and spatial analyses should be integrated in local control programmes of vector-transmitted diseases. These analyses help to initiate early interventions, plan for the prevention of disease outbreaks and their spread, and assess the success of strategies(5,29).
Acknowledgements Grateful thanks are offered to Dra Ducinea Barros, Fundação Nacional de Saúde-FUNASA, Laboratório Central-LACEN, Instituto Brasileiro de Geografia e Estatística – IBGE-Roraima, Secretaria do Estado de Saúde de Roraima-SESAU, Secretaria Municipal de Saúde-SEMSA, and Prefeitura de Boa Vista.
References 1. Travassos da Rosa APA, Rocha JM, Silva OV and
Lins ZC. Surto de dengue em Boa Vista, Território de Roraima, Brasil. Bol Epidemiológico MS, 1982, 14(9): 93-100.
2. Osanai CH, Travassos da Rosa APA, Tang AT, Amaral RS, Passos AC and Tauil PL. Surto de dengue em Boa Vista, Roraima. Rev Inst Med Trop São Paulo, 1983, 25(1): 53-54.
3. Vasconcelos PFC, Travassos-da-Rosa APA, Pinheiro FP, Rodrigues SG, Rosa EST, Cruz ACR and Travassos-da-Rosa JFS. Aedes aegypti, dengue and re-urbanization of yellow fever in Brazil and other South American countries - Past and present situation and future perspectives. Dengue Bulletin, 1999, 23: 1-6.
4. Fundação Nacional de Saúde-FUNASA 2000 (http://www.funasa.gov.br).
5. Molyneux DH. Vector-borne infections in the tropics and health policy issues in the twenty-first century. Trans R Soc Trop Med Hyg, 2001, 95(3): 233-238.
6. Bergquist NR. Vector-borne parasitic diseases: New trends in data collection and risk assessment. Acta Trop, 2001, 79(1): 13-20.
7. Rushton G, Elmes G and McMaster R. Considerations for improving geographic information system research in public health. URISA J, 2000, 12(2): 31-49.
8. De La Rocque S, Michel JF and Cuisance D. Different potentials of a geographic information system for studies in epidemiology: Example of animal trypanosomiasis in the Sudan region [Article in French]. Med Trop, 2001, 61(4-5): 365-371.
9. Costa AIP and Natal D. Distribuição espacial da dengue e determinantes socioeconômicos em localidade urbana no Sudeste do Brasil. Rev Saúde Pub, 1998, 32: 232-236.
10. Hossain IM, Wagatsuna Y, Chowdhury MA, Ahmed TU, Uddin MA, Sohel SMN and Kittayapong P. Analysis of some socio-demographic factors related to DF/DHF outbreak in Dhaka city. Dengue Bulletin, 2000, 24: 34-41.
11. Indaratna K, Hutubessy R, Chupraphawan S, Sukapurana C, Tao J, Chunsutthiwat S, Thimasarn K and Crissman L. Application of geographical information systems to co-analysis of disease and economic resources: Dengue and malaria in Thailand. Southeast Asian J Trop Med Public Health, 1998, 29(4): 669-84.
12. Instituto Brasileiro de Geografia e Estatística-IBGE, 1996 (http://www.ibge.gov.br).
13. Prefeitura Municipal de Boa Vista Roraima PMBV/RR, Secretaria Municipal de Obras e Urbanismo–SEMOU, Coordenação do Projeto a Cidadania com Endereço Certo – CPCCEC.
14. Instituto Brasileiro de Geografia e Estatística-IBGE, Unidade de Roraima.

Dengue in Boa Vista, Roraima, 1999-2001
80 Dengue Bulletin – Vol 27, 2003
15. Silva ELS. Inventário preliminar das espécies arbóreas das florestas dos arredores de Boa Vista (Roraima), uma abordagem fitossociológica. Tese de Mestrado. INPA-Fundação Universidade do Amazonas. Manaus, 1993.
16. National Aeronautics and Space Administration NASA, 2001 (http://eosweb.larc.nasa.gov/sse).
17. Schmidt JCJ. O clima da Amazônia. Rev Bras Geog, 1942, 4: 465-500.
18. Silva-Vasconcelos AS, Kato MYN, Mourao EN, Souza RTL, Lacerda RNL, Sibajev A, Tsouris PA, Povoa MM, Momen H and Rosa-Freitas MG. Biting indices, host-seeking activity and natural infection of anopheline species in Boa Vista, Roraima, Brazil from 1996 to 1998. Memórias do Instituto Oswaldo Cruz, 2002, 97(2), 151-161.
19. Luitgards-Moura JF, Rosa-Freitas MG and Costa J. Epidemiological aspects of the Chagas disease in agricultural settlements areas in Roraima, Brazil. In Portuguese. [Aspectos epidemiológicos da doença de Chagas em áreas de colonização agrícola no estado de Roraima, Brasil]. Oswaldo Cruz Institute, Curso de Biologia Parasitária do Instituto Oswaldo Cruz, 2001: 82.
20. Figueiredo LT, Cavalcante SM and Simoes MC. Dengue serologic survey of schoolchildren in Rio de Janeiro, Brazil, in 1986 and 1987. Bull Pan Am Health Org, 1990, 24(2): 217-225.
21. Lima VLC, Figueiredo LTM, Correa HR, Leite OF, Rangel O, Vido AA, Oliveira SS, Owa MA and Carlucci RH. Dengue fever: A post-epidemic sero-epidemiological survey in an urban setting at a northwestern county of Sao Paulo State. In Portuguese. Rev Saude Pub, 1999, 33(6): 566-574.
22. Vasconcelos PFC, Lima JWO, Travassos-da-Rosa APA, Timbó MJ, Travassos-da-Rosa ES, Lima HR, Rodrigues SG and Travassos-da-Rosa JFS. Dengue pandemic in Northeastern Brazil: Random epidemiological serum survey. In Portuguese. Rev Saude Pub, 1998, 32(5): 447-454.
23. Souza-Santos R. Factors associated to the occurrence of immature forms of Aedes aegypti in the Ilha do Governador, Rio de Janeiro, Brazil. In Portuguese. Rev Soc Bras Med Trop, 1999, 32(4): 373-382.
24. Rebelo JMM, Costa JML, Silva FS, Pereira YNO and Silva JM. Distribution of Aedes aegypti and dengue in the state of Maranhao. In Portuguese. Cad Saude Pub, 1999, 15(3): 477-486.
25. Keating J. An investigation into the cyclical incidence of dengue fever. Soc Sci Med, 2001, 53(12): 1587-1597.
26. Gubler DJ. Dengue and dengue hemorrhagic fever. Clin Microb Rev, 1998, 11(3): 480-496.
27. Kuno G. Review of the factors modulating dengue transmission. Epidem Reviews, 1995, 17: 321-335.
28. Almeida Filho N and Rouquayrol MZ. Fundamentos Metodológicos da Epidemiologia In: Epidemiologia e Saúde. Rouquayrol MZ Ed. Rio de Janeiro-MEDSI, 1994, 4: 157-183.
29. Tauil PL. Critical aspects of dengue control in Brazil. In Portuguese. Cad Saude Pub, 2002, 18(3): 867-871.
30. Morrison AC, Getis A, Santiago M, Rigau-Perez JG and Reiter P. Exploratory space-time analysis of reported dengue cases during an outbreak in Florida, Puerto Rico, 1991-1992. Am J Trop Med Hyg, 1998, 58(3): 287-298.
31. Scott TW, Chow E, Strickman D, Kittayapong P, Wirtz RA and Edman JD. Detection of multiple blood feeding Aedes aegypti during a single gonotrophic cycle using a histologic technique. J Med Entomol, 1993, 30: 94-99.
32. Pinheiro VCS and Tadei WP. Frequency, diversity and productivity study on the Aedes aegypti most preferred containers in the city of Manaus, Amazonas, Brazil. Rev Inst Med Trop Sao Paulo, 2002, 44(5): 245-250.
33. Schatzmayr HG. Dengue situation in Brazil by year 2000. Mem Inst Oswaldo Cruz, 2000, 95(suppl.1): 179-181.
34. Teixeira MG, Costa MCN, Barreto ML and Barreto FR. Epidemiologia do dengue em Salvador, Bahia 1995-1999. Rev Soc Bras Med Trop, 2001, 34(3): 269-274.
35. Passos ADC, Rodrigues EMS and Dal-Fabbro AL. Dengue control in Ribeirão Preto, São Paulo. Cad Saúde Púb, 1998, 14 (suppl.2): 123-128.
36. Espinoza-Gomez F, Hernandez-Suarez CM and Coll-Cardenas R. Educational campaign versus malathion spraying for the control of Aedes aegypti in Colima, Mexico. Epidemiol Community Health, 2002, 56(2): 148-152.

Dengue Bulletin – Vol 27, 2003 81
Isolation and Serotyping of Dengue Viruses by Mosquito Inoculation and Cell Culture Technique:
An Experience in Bangladesh by
Monira Pervin*#, Shahina Tabassum**, Bijon Kumar Sil*** and Md Nazrul Islam**
*Department Of Virology, Dhaka Medical College, Dhaka, Bangladesh **Department of Virology, Bangabandhu Sheikh Mujib Medical University, Shahbag, Dhaka, Bangladesh
***Bangladesh Livestock Research Institute, Savar, Dhaka, Bangladesh
Abstract
Dengue virus isolation and serotyping was carried out in 105 clinically-suspected cases of dengue fever by the mosquito inoculation and cell culture techniques to find a suitable virus isolation technique for a resource-constrained country like Bangladesh and to identify the serotypes responsible for the dengue outbreak in 2000. Virus was identified by direct fluorescent antibody technique (DFAT) using FITC-conjugated anti-flavivirus antibody and serotyping was done by indirect fluorescent antibody technique (IFAT) using serotype-specific monoclonal anti-dengue antibody. Of the 105 cases, 97 (92.4%) were found sero-positive for anti-dengue IgM by ELISA and considered as having dengue infection. Dengue virus was isolated from 44 (45.4%) of the 97 anti-dengue IgM positive cases by Aedes aegypti mosquito inoculation and from 24 (24.7%) cases by C6/36 cell culture. The dengue virus isolation rate was significantly higher (p<0.01) by the mosquito inoculation than the cell culture inoculation technique. The isolation rate was also higher in patients who presented on the first day of the fever than in those who presented later. Dengue virus was isolated from patients who had a significantly higher mean body temperature (p<0.01) and the mean anti-dengue IgG level was significantly lower in those from whom virus was isolated (p<0.01). The serotyping revealed isolation of DEN-3 from 31 (70.5%) cases, which was the predominant serotype, followed by the isolation of DEN-1 from 6 (13.6%), DEN-4 from 4 (9.09%) and DEN-2 from 3 (6.8%) cases out of the total 44 positive cases. This indicates the hyperendemicity of dengue in Dhaka with epidemic potential, which needs careful monitoring by laboratory-based surveillance in order to predict the nature of future outbreaks. This is the first report of dengue virus isolation by mosquito inoculation and C6/36 cell culture in Bangladesh. It was revealed from the study that, for routine surveillance of dengue infection, isolation of virus by mosquito inoculation is a more sensitive, economical, easy and sustainable method. However serotyping by IFAT is more convenient in cell culture.
Keywords: Dengue, dengue haemorrhagic fever, virus isolation, cell culture, fluorescent antibody technique, serotyping, serotypes, Dhaka, Bangladesh.
# For correspondence: [email protected]

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
82 Dengue Bulletin – Vol 27, 2003
Introduction Dengue is an acute arboviral human disease caused by four serotypes of dengue viruses, which are closely related but antigenically distinct(1). Though classical dengue is a self-limiting febrile illness, its life-threatening severe forms, dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS) can be fatal unless the associated plasma leakage is treated early. The untreated case-fatality rate may be as high as 40%(2,3). Currently, it is an emerging/re-emerging disease throughout the tropical and subtropical areas and nearly half of the world’s population is at risk(4,5,6). The first reported outbreak of dengue in Bangladesh was the “Dacca fever” recorded in 1964(7,8). After that, the magnitude of infection was generally unknown until the outbreak of dengue in 1999(9). Recently, large outbreaks of DF/DHF have been recorded in Bangladesh(10). During the outbreak in 2000, 5,551 cases and 93 deaths and in 2001, 2,430 cases and 44 deaths were officially recorded(10) and reported(11). These cases were diagnosed clinically, except for a few which were diagnosed serologically. The mosquito inoculation technique(12) and cell culture in C6/36 cell line(13) are widely practised for the isolation of dengue viruses and hence were chosen in the present study as the tool for virus isolation. Serotyping was also carried out to explore the serotypes responsible for the outbreak to compare the different aspects of the methods, including sensitivity and suitability to set up and sustain, in a resource-constraint situation in Bangladesh.
Materials and methods The study was carried out among 105 clinically-suspected cases of dengue fever during an outbreak which started in June 2000. The patients were selected from the outpatient and inpatient departments of Paediatrics and Medicine and also from patients seeking diagnostic facility in the department of Virology, Bangabandhu Sheikh Mujib Medical University (BSMMU) during June-December 2000. Inclusion criteria were: patients having fever presented within five days from the onset; body temperature above 100°F at the time of sample collection; fulfilling the WHO case definition of DF and DHF(6); and agreeable to donate two blood samples during the early and convalescence stages, irrespective of age and sex. Exclusion criteria were: febrile cases of more than five days with definite source of infection (e.g. respiratory tract infection, urinary tract infection, meningitis); chronic illnesses like tuberculosis, bronchial asthma, congenital heart diseases, renal failure; and history of bleeding tendency since birth. With all aseptic precautions, 5 ml of venous blood was collected from patients during their first attendance and transferred to a sterile vacutainer. After the separation of serum, it was transferred to labelled cryovials and preserved at –70°C fridges immediately till inoculated into mosquitoes and C6/36 cells for the isolation of viruses and detection of antibody. A second sample of 5 ml venous blood was collected during convalescence 10-14 days after the collection of the first sample and used for the detection of antibody level by ELISA. Blood samples were collected from healthy individuals used for negative control.

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
Dengue Bulletin – Vol 27, 2003 83
Detection of dengue antibody by ELISA A commercially produced indirect ELISA (Pathozyme Dengue, Omega Diagnostics Limited, Scotland, UK) was used for the detection of anti-dengue IgM and IgG levels from both acute and convalescent sera. The test was performed according to the instruction of the manufacturer and an antibody index (AI) was calculated for both IgM and IgG comparing optical density (OD) of sample and average OD of low positive controls. AI>1 was considered as positive.
Isolation of dengue viruses by mosquito inoculation technique
Mosquito inoculation technique in Aedes aegypti mosquitoes(12) in the department of Virology, BSMMU, was used for virus isolation. One to five days old adult female mosquitoes were collected from fresh laboratory-reared mosquito colony in a cotton-stopper test tube and were immobilized by placing the tube in an ice-filled beaker for 15 minutes. Each mosquito was inoculated intra-thoracically with 0.17 µl of diluted patient’s serum (1:5 dilution with PBS diluents prepared with PBS PH- 7.4 with 0.5% gelatin and 5% foetal calf serum). For each patient, 50 mosquitoes were inoculated. After inoculation, mosquitoes were transferred into a labelled plastic drinking glass covered with a piece of mosquito net and incubated at 30 ± 2°C with 75-85% humidity for 14 days and fed with 10% sugar solution. Keeping the plastic glass for 10 minutes in deep freezer killed the survivors. The heads of the freshly killed mosquitoes were dissected along with salivary gland and head squashes were
prepared in pre-marked circles on glass slides with the help of 1% silicon-coated cover slip. After air-drying, the mosquito tissue was fixed with chilled acetone at –20°C for 15 minutes and stored at –70°C until the identification of virus isolates and their serotyping.
Cell culture
Cell culture was done in C6/36 cell line(13) with slight modification in the Virology Laboratory, Bangladesh Livestock Research Institute, Savar, Dhaka. Aedes albopictus cells (C6/36) adapted to grow at 33°C were used for virus isolation. Cells were maintained on Eagles Minimum Essential Media (MEM) in Earle’s balanced salt solution supplemented with 5% foetal calf serum (FCS), 2% L glutamine, 1% sodium bicarbonate, 2% penicillin, streptomycin, amphotericin B and 1% non-essential amino acid. Twenty-five sq cm screw-capped flat-bottomed flask was seeded with 3 ml of cells at a concentration of 4×105/ml. Fifty µl of patients serum was inoculated into each flask containing confluent mono layer of cells and 200 µl of PBS (PH-7.4) was added. The inoculated flask was incubated at 33°C for 45 minutes with frequent agitation. Five ml of maintenance media (growth media except with 1% FCS and 2% sodium bicarbonate) was added and incubation at 33°C maintained for seven days. Regular observation was kept under inverted microscope to detect visible cytopathic effect (CPE). During the incubation period the PH
of the medium was maintained at approximately 7 for maximum recovery of virus. At the end of each passage, irrespective of the presence of CPE, slides were prepared from inoculated cells for the

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
84 Dengue Bulletin – Vol 27, 2003
identification of viral antigen by DFAT. Cell suspension was spotted on pre-marked circles of glass slides, air-dried and fixed with acetone at –20°C. After air-drying the fixed slides were preserved at –70°C until the identification of isolated viruses and their serotyping.
Identification and serotyping of dengue viruses
The presence of viral antigen of the isolated viruses on glass slides was detected by DFAT using FITC-conjugated anti-flavivirus antibody(14). Serotyping of the isolated viruses was carried out by IFAT on both mosquito head squashes and spotted slides of cell culture materials using serotype-specific anti-dengue monoclonal antibody and FITC-conjugated goat anti-mouse IgG(15,18).
Statistical analysis
The numerical data obtained from the study were analysed and the significance of difference was estimated by using statistical methods. Data were expressed in frequency, percentage, mean and standard deviation as applicable. Comparison between groups was done by student’s ‘t’ test and ‘Chi square’ test as applicable. All data were analysed by using the computer-based SPSS programme. P value less than 0.05 were considered as significant.
Results Out of the 105 clinically-suspected DF patients, 97 were found positive for dengue IgM antibody by ELISA either in the first sample or in convalescent sera and were
considered as recent dengue infections, while eight cases were found negative for antibody. By virus isolation, these were diagnosed as non-dengue febrile illnesses and, therefore not considered for further analysis. In the study, the involvement of all age groups, with adult predominance, was reflected. The mean age of the study patients was 29.2 ± 12.9 years and no significant sex difference was found. Out of the 97 dengue patients, dengue virus was isolated from 44 (45.4%) cases by the mosquito inoculation technique and from 24 (24.7%) cases by cell culture (Table 1). The rate of dengue virus isolation was significantly higher by mosquito inoculation than by cell culture inoculation technique (p<0.01). Dengue virus isolation by mosquito inoculation was positive in 44 cases and negative in 61 cases, whereas among the 44 positive cases by mosquito inoculation, virus was isolated only in 24 (54.5%) cases by cell culture and 20 (45.5%) cases did not yield any virus. All the mosquito negative cases were also negative by cell culture.
Table 1. Isolation rate of dengue viruses by mosquito inoculation and cell culture (n=97)
Method of virus
isolation
Number of cases
from which
dengue virus was isolated
Isolation rate
*p value
Mosquito inoculation
44 45.4
Cell culture 24 24.7
0.0001
*p value reached from ‘chi square’ analysis

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
Dengue Bulletin – Vol 27, 2003 85
The serotyping revealed that all four dengue serotypes were isolated from the patients, DEN-3 being the predominant (70.5%) serotype during the study period (Figure 1). The rate of isolation of dengue viruses was higher in the serum collected on the first day of fever in both the isolation systems. Virus was isolated from 7 (77.7%) cases by the mosquito inoculation technique and from 4 (44.4%) cases by cell culture, out of the 9 patients whose serum were collected on the first day of fever. The rate of isolation decreased from the second day onwards up to the fifth day by both the techniques. Thus, on the fifth day, of the 26 sera, virus was isolated only from 5 (19.2%) cases by mosquito inoculation and from 2 (7.7%) cases by cell culture (Table 2).
Figure 1. Serotypes of isolated dengue viruses (n=44) from clinically-suspected
cases of dengue fever
4 (9.09%)
31 (70.5%)
3 (6.8%)
6 (13.6%)
0 10 20 30 40
DEN-1
DEN-2
DEN-3
DEN-4
Sero
type
Frequency
Table 2. Dengue virus isolation rates among dengue cases by mosquito inoculation and
cell culture by day of fever
Day of fever at
which the virus was isolated
Number of cases (n=97)
Positive by mosquito
inoculation
Positive by cell culture
1st day 9 7 (77.7) 4 (44.4)
2nd day 12 6 (50.0) 3 (25.0)
3rd day 27 14 (51.8) 9 (33.3)
4th day 23 12 (52.1) 6 (26.1)
5th day 26 5 (19.2) 2 (7.7)
Figures in parenthesis indicate rate of virus isolation.
In the present study, it was found (Table 3) that the mean temperature (101.97±1.2°F and 102.0±1.4°F) among the patients from whom virus was isolated was significantly higher than that (101.11±1.4°F and 101.32±1.4°F) of those from whom virus could not be isolated by both the isolation systems (p=0.001 in mosquito inoculation and p=0.041 in cell culture).
Although the mean level of the IgM antibody index was lower in patients where virus was isolated than that of the patients from whom virus was not isolated (Table 4), the difference was not statistically significant (p>0. 05), whereas virus isolation in the presence of IgG antibody was lower and the mean AI of IgG was also lower (‘(1.14±1.1 vs 2.35±1.5) in mosquito inoculation and (0.68±0.7 vs 2.17±1.5) in cell culture) in the sera from which virus was isolated than those from whom virus was not isolated by both the isolation techniques was statistically significant (p<0.01).
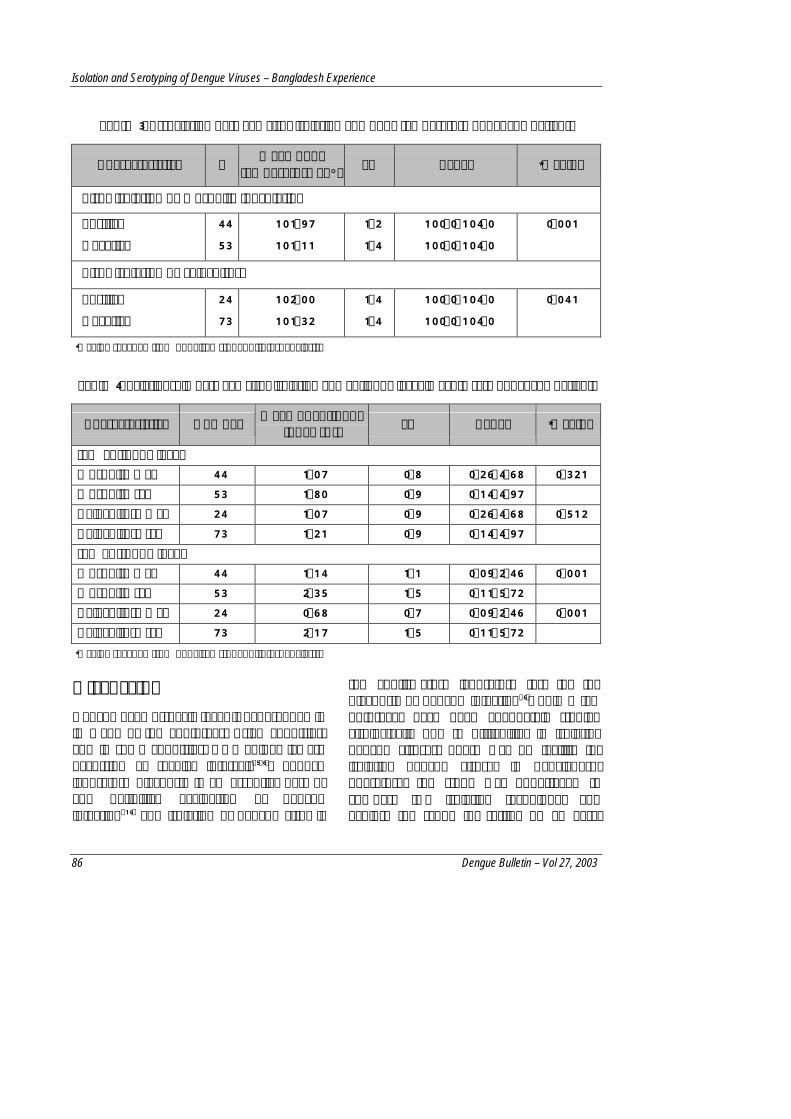
Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
86 Dengue Bulletin – Vol 27, 2003
Table 3. Association between virus isolation and body temperature of dengue patients
Characteristics n Mean body
temperature at °F SD Range *p value
Virus isolation by mosquito inoculation
Positive
Negative
44
53
101.97
101.11
1.2
1.4
100.0-104.0
100.0-104.0
0.001
Virus isolation by cell culture
Positive
Negative
24
73
102.00
101.32
1.4
1.4
100.0-104.0
100.0-104.0
0.041
*p value reached from unpaired student ‘t’ test analysis.
Table 4. Relationship between virus isolation and antibody level in acute sera of dengue patients
Characteristics Number Mean of antibody index (AI) SD Range *p value
IgM antibody level Mosquito +ve 44 1.07 0.8 0.26-4.68 0.321 Mosquito -ve 53 1.80 0.9 0.14-4.97 Cell culture +ve 24 1.07 0.9 0.26-4.68 0.512 Cell culture -ve 73 1.21 0.9 0.14-4.97 IgG antibody level Mosquito +ve 44 1.14 1.1 0.09-2.46 0.001 Mosquito -ve 53 2.35 1.5 0.11-5.72 Cell culture +ve 24 0.68 0.7 0.09-2.46 0.001 Cell culture -ve 73 2.17 1.5 0.11-5.72
*p value reached from unpaired student ‘t’ test analysis.
Discussion Dengue haemorrhagic fever is hyperendemic in many of the South-East Asian countries, and in some countries, DHF epidemics are occurring at regular intervals(5,6). Though laboratory diagnosis is an essential part of any definitive evaluation of dengue infection(16) and isolation of dengue virus is
the confirmatory laboratory test for the diagnosis of dengue infection(6), only a few outbreaks have been adequately studied virologically due to difficulties in isolating dengue viruses. There was no facility for isolating dengue viruses in Bangladesh. Therefore, the study was undertaken to compare two isolation techniques and explore the scope for setting up an easy,

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
Dengue Bulletin – Vol 27, 2003 87
economical, sensitive and specific laboratory method for the isolation and serotyping of dengue viruses suitable for Bangladesh. With a view to achieving these objectives, we used the widely-practised mosquito inoculation and C6/36 cell line culture techniques for the isolation of dengue viruses. We used DFAT for detecting dengue virus in mosquito and C6/36 cells and carried out serotyping of the isolates by IFAT to identify the serotypes responsible for the dengue outbreak of 2000.
The superiority of the mosquito inoculation technique over cell culture for the isolation of dengue virus is well-known(12,17,18,19) and this has also been reflected in the present study. Dengue virus was isolated from 45.4% of the patients by the mosquito inoculation technique whereas in cell culture, the isolation rate was only 24.7%. Similar findings have been reported from other studies(17,18,19,20). The mosquito inoculation technique consistently yielded a higher isolation rate than the cell culture technique from samples collected in the first to the fifth day of fever (Table 2). It was previously reported that the pre-inoculation of human sera in mosquitoes facilitated the isolation and identification of virus in cell culture by enhancing the infective virus titer(21). We also had similar findings. An important finding of the present study with regard to the isolation of virus by mosquito inoculation was that three samples collected during the third and fourth day of fever failed to be isolated by cell culture. However, after DFAT, positivity in these serum-inoculated mosquito head squash, the infected mosquito abdomens passed into cell culture resulted in visible CPE within 72 hours and in positive isolation. This finding indicates higher sensitivity of mosquito inoculation.
The low isolation rate in cell culture during the present study was perhaps due to less sensitivity and the toxic effect of serum on the cells. During the present study C6/36 cells frequently showed toxicity of serum even when it was diluted 1:5. The toxicity was found both in negative control serum and test specimens. Frequent susceptibility of C6/36 cells to serum toxicity was also reported from other studies(22,23). In a few instances, although there was no visible CPE in the cells during the first inoculation, following the identification of dengue virus antigen in the cells by DFAT, the second passage yielded CPE. A similar absence of visible CPE was also noticed in another study where lower dilution of serum was negative for CPE production(13). There have been varied reports on the efficiency of dengue virus isolation by cell culture. Thus, Singh and Paul (1969) reported frequent CPE produced both in C6/36 and Vero cells(21) whereas Gubler et al (1984) reported that some viruses grow slowly in C6/36 cells(18).
In the present study, it was evident that all four serotypes of dengue viruses were circulating in Dhaka city in 2000, with a predominance of DEN-3. A recent serological study by haemagglutination inhibition test conducted in Chittagong Medical College, situated in the south-eastern part of the country demonstrated that except for DEN-1, the other three serotypes were present in Chittagong(24). The presence of DEN-3 in Dhaka city was also documented during the first reported outbreak of dengue in Bangladesh in 1964, confirmed by virus isolation and serology(7,8). A serological survey was carried out among schoolchildren of Dhaka city in 1982-1983 where among 2,465 samples, 278 (11%) were serologically positive against DEN-1(25).

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
88 Dengue Bulletin – Vol 27, 2003
The presence of DEN-1 was also reported in Dhaka during another study in 1980(26). During the outbreak in 2000, DEN-3, DEN-2 and DEN-4 were detected from the serum of clinically-suspected dengue patients of Dhaka city by the polymerase chain reaction (PCR) analysis(27). Lack of detection of DEN-1 in this study was perhaps due to fewer number (45) of study subjects.
During the present study, the specific perinuclear fluorescence in the infected neurocytes of mosquito head squash and C6/36 cells were easily identified by DFAT. Similar findings about DFAT were reported in another study(14). Although background fluorescence created difficulty in IFAT of head squash of mosquito, there was no background fluorescence while carrying out IFAT in C6/36 cells for serotyping. Similar findings were reported from other studies(13,22).
In the present study, the virus isolation rate was 45.4% by mosquito inoculation. The isolation rate of dengue viruses by mosquito inoculation method varied widely in different studies carried out elsewhere in the world. It was 32% in Central Java, Indonesia(28), during an epidemic of DEN-3 in 1978, while in Jakarta, it was 34% in 1975-1978(17). A similar rate (33.3%) was reported in Pacific Island, Kingdom of Tonga, in 1974 during an epidemic of DEN-2(29). A lower rate (20%) and a higher rate (98%) were also reported in other studies(30,31). The high rate of virus isolation in the latter study was claimed to be due to the collection of sera at a very early febrile period. The rate of dengue virus isolation employing C6/36 cell culture was 24.7% in the present study. Report on the efficiency of isolation by mosquito inoculation and C6/63 cell culture is not available. However, a lower rate of
dengue virus isolation in C6/36 cell culture has been reported in some studies. An isolation rate of 16.7% was found in Rio de Janeiro, Brazil(32), in 1990-91 and 19.2% was reported from Puerto Rico in 1981(18). Singh and Paul (1969) had reported a very high isolation rate (88%) in C6/36 cell culture in India(21).
The dengue virus isolation rates are influenced by some factors which include the duration of viremia, the number of days after the onset of fever, body temperature and antibody level(33). It was found during the present study that the virus isolation rate was higher during the early days after the onset of fever (Table 2). It was also found (Table 3) that the mean temperature (101.97±1.2°F) among the 44 patients from whom virus was isolated was significantly higher than that (101.11±1.4°F) of those from whom virus could not be isolated (p<0.01). A similar finding was also reported from Cambodia(30) where the mean temperature at which the virus was isolated from patients’ sera was 100°F in comparison with 99°F of the patients from whom virus was not isolated (p < 0.01). Vaughn et al (2000) also reported a similar correlation between higher body temperature and viremia(19). It was also found in the present study that dengue virus isolation was affected by the presence of antibody. Virus was isolated in patients with a lower level of IgM and IgG antibody in the acute stage of the disease (Table 4). Thus, in conclusion, it can be suggested that for the routine surveillance of dengue infection, the isolation of virus by mosquito inoculation is a sensitive, economical and easy method, as, in our experience, maintenance of mosquito colony is easier and less expensive than maintenance of cell culture. However, serotyping by IFAT is more convenient in cell culture.

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
Dengue Bulletin – Vol 27, 2003 89
Acknowledgements
We express our sincere thanks to Dr Vorndam Vance, CDC Dengue Lab, San Juan, Puerto Rico, USA, and Dr Ichiro Kurane, Arbovirus Research Laboratory, NIID, Japan, for their support in providing C6/36 cell line and anti-dengue monoclonal antibodies. We are also grateful to the
patients who participated in the study. We would like to thank Mr Tauhid Uddin Ahmed, Ex PSO, IEDCR, Bangladesh, and Noor-e-Jannat for providing the mosquito colony and rearing techniques. We also express our gratitude to ICDDRB and the Department of Medicine, BSMMU, Bangladesh, for their support in the study.
References 1. Henchal EA and Putnak JR. The dengue viruses.
Clinical Microbiology Review, 1990, 3: 376-396.
2. Yamarat C. Thailand haemorrhagic fevers of 1958. Journal of Microbiological Society Thailand, 1959, 3: 18-28.
3. Srivastava VK, Suri S, Bhasin A, Srivastava L and Bharadwaj M. An epidemic of dengue haemorrhagic fever and dengue shock syndrome in Delhi: A clinical study. Annals of Tropical Pediatrics, 1990, 10: 329-334.
4. Halstead SB. The XXth century dengue pandemic: Need for surveillance and research. World Health Statistics Quarterly, 1992, 45: 292-298.
5. Chusak P, Andjaparidze AG and Kumar V. Current status of dengue/dengue haemorrhagic fever in WHO South-East Asia Region. Dengue Bulletin, 1998, 22: 1-11.
6. World Health Organization. Comprehensive guidelines for prevention and control of dengue and dengue haemorrhagic fever. WHO Regional Publication SEARO, No. 29, New Delhi, 1999.
7. Russel PK, Busescher EL, McCown JM and Ordonez J. Recovery of dengue viruses from patients during epidemics in Puerto Rico and East Pakistan. The American Journal of Tropical Medicine and Hygiene, 1966, 15: 573-579.
8. Aziz MA, Gorham JR and Gregg MB. Dacca fever - An outbreak of dengue. Pakistan Journal of Medical Research, 1967, 6: 83-92.
9. Alam MN. Dengue and dengue haemorrhagic fever in Bangladesh. The Orion, 2000, 6: 7.
10. Directorate-General of Health Services, Bangladesh. Dengue Register, Disease Control Directorate, Dhaka, 2000.
11. Yunus EB, Bangali AM, Mahmood MAH, Rahman MM, Chowdhury AR and Talukder RK. Dengue outbreak 2000 in Bangladesh: From speculation to reality and exercise. Dengue Bulletin, 2001, 25: 15-20.
12. Rosen L and Gubler DJ. The use of mosquitoes to detect and propagate dengue viruses. The American Journal of Tropical Medicine and Hygiene, 1974, 23: 1153-1160.
13. Tesh RB. A method for the isolation and identification of dengue viruses, using mosquito cell cultures. The American Journal of Tropical Medicine and Hygiene, 1979, 28(6): 1053-1059.
14. Kuberski TT and Rosen L. A simple method for the detection of dengue antigen in mosquitoes by immunofluorescence. The American Journal of Tropical Medicine and Hygiene, 1977, 26: 533-537.
15. Henchal EA, McCown JM, Seguin MC, Gentry MK and Brandt WE. Rapid identification of dengue virus isolates by using monoclonal antibodies in an indirect immunofluorescence assay. The American Journal of Tropical Medicine and Hygiene, 1983, 32(1): 164-169.
16. Dietz VJ, Gubler DJ, Rigau-Perez JG, Pinheiro P, Schatzmayr HG, Bailey R and Gunn RA. Epidemic dengue 1 in Brazil, 1986. Evaluation of a clinically based dengue surveillance system. The American Journal of Epidemiology, 1990, 131(4): 693-701.

Isolation and Serotyping of Dengue Viruses – Bangladesh Experience
90 Dengue Bulletin – Vol 27, 2003
17. Suharyono W, Gubler DJ, Lubis I, Tan R, Abidin M, Sie A and Sulianti SJ. Dengue virus isolation in Indonesia, 1975-1978. Asian Journal of Infectious Diseases, 1979, 3: 27-32.
18. Gubler DJ, Kuno G, Sather GE, Velez M and Oliver A. Mosquito cell culture and specific monoclonal antibodies in surveillance for dengue viruses. The American Journal of Tropical Medicine and Hygiene, 1984, 33(1): 158-165.
19. Vaughn DW, Green S, Kalayanarooj S, Innis BL, Nimannitya S, Suntayakorn S, Endy TP, Raengsakulrach B, Rothman AL, Ennis FA and Nisalak A. Dengue viremia titer, antibody response patterns and virus serotype correlated with disease severity. Journal of Infectious Diseases, 2000, 181: 2- 9.
20. Kalayanarooj S, Vaughn DW, Nimmannitya S, Green S, Suntayakorn S, Kunentrasai N, Viramitrachai W, Ratanachu-eke S, Kiatpolpoj S, Innis BL, Rothman AL, Nisalak A and Ennis FA. Early Clinical and laboratory indicators of acute dengue illness. Journal of Infectious Diseases,1997, 176: 313-321.
21. Singh KRP and Paul SD. Isolation of dengue viruses in Aedes albopictus cell cultures. Bulletin of the World Health Organization, 1969, 40: 982-983.
22. Kuno G, Gubler DJ, Velez M and Oliver A. Comparative sensitivity of three-mosquito cell lines for isolation of dengue viruses. Bulletin of the World Health Organization, 1985, 63(2): 279-286.
23. Kuno G. Dengue virus replication in a polyploid mosquito cell culture growth in serum-free medium. Journal of Clinical Microbiology, 1982, 16(5): 851-855.
24. Yunus EB, Banu D, Chowdhury MJH, Talukder KR and Bangali AM. Report on sero-epidemiological study of dengue and dengue haemorrhagic fever, ICOVD Project, Directorate-General of Health Services, 1998.
25. Khan M and Ahmed T. Dengue status in Bangladesh. Dengue Newsletter. WHO/SEARO, 1986, 12: 11.
26. Gaidamorich SY, Siddiqi SM, Haq F, Klisenko GA, Melnicova EE and Obukhova VR. Serological evidence of dengue fever in the Bangladesh Republic. Acta Virology, 1980, 24: 153.
27. Aziz MM, Hasan KN, Hasnat MA, Siddiqui MA, Salimullah M, Chowdhury AK, Ahmed M, Alam MN and Hassan MS. Predominance of the DEN-3 genotype during the recent dengue outbreak in Bangladesh. Southeast Asian Journal of Tropical Medicine and Public Health, 2002, 33(1): 42-48.
28. Gubler DJ, Suharyono S, Lubis I, Eram S and Gunarso S. Epidemic dengue 3 in Cental Java associated with low viremia in man. The American Journal of Tropical Medicine and Hygiene, 1981, 30(5): 1094-1099.
29. Gubler DJ, Reed D, Rosen L and Hitchcock JC. Epidemiological, clinical and virologic observations on dengue in the Kingdom of Tonga. The American Journal of Tropical Medicine and Hygiene, 1978, 27(3): 581-589.
30. Rathavuth H, Vaughn DW, Minn K, Nimmannitya S, Nisalak A, Raengsakulrach B, Rorabaugh ML, Yuvathak and Sophal O. Haemorrhagic fever in Cambodia caused by dengue viruses: Evidence for transmission of all 4 serotypes. Southeast Asian Journal of Tropical Medicine and Public Health, 1997, 28(1): 120-125.
31. Vaughn DW, Green S, Kalayanarooj S, Innis LB, Nimmannitya S, Suntayakorn S, Rothman AL, Ennis FA and Nisalak A. Dengue in early febrile phage: Viremia and antibody responses. The Journal of Infectious Diseases, 1997, 176: 322-330.
32. Nogueira RMR, Miagostovich PM, Lampe E, Souza RW, Zagne SMO and Schatzmaryr GH. Dengue epidemic in the state Rio de Janeiro, Brazil, 1990-91: Co-circulation of dengue 1 and 2 serotypes. Epidemiology and Infection, 1993, III: 163-170.
33. Gubler DJ, Suharyono RT, Abidin M and Sie A. Viremia in-patients with naturally acquired dengue infection. Bulletin of the World Health Organization, 1981, 59(4): 623-630.

Dengue Bulletin – Vol 27, 2003 91
Epidemiology and Phylogenetic Relationships of Dengue Viruses
by Oswaldo Paulo Forattini#
Department of Epidemiology, Núcleo de Pesquisa Taxonômica e Sistemática em Entomologia Médica (NUPTEM – Division for Taxonomic and Systematic Research in Medical Entomology),
School of Public Health, São Paulo University, Av. Dr. Arnaldo, 715 São Paulo, SP 01246-904 Brazil
Abstract
The mosquito-borne flaviviruses revealed two distinct epidemiological groups. The neurotropic viruses correlated with the Culex vectors, and the viruses associated with haemorrhagic diseases correlated with the Aedes vectors. About the last ones, it is hypothesized that the dengue viruses have evolved from sylvatic strains that are transmitted among non-human primates in West Africa and Malaysia by several Aedes mosquitoes.
Keywords: Neurotropic viruses, Culex vectors, haemorrhagic diseases, Aedes vectors, sylvatic strains.
# For correspondence: [email protected]
Introduction The Flavivirus genus of the Flaviviridae family consists of many viruses associated with emerging and re-emerging human infectious diseases including dengue and dengue haemorrhagic fever. The knowledge of virus evolution is important to understand the origin of these diseases.
Among that genus are the dengue RNA viruses, which contain four important human pathogens. There are antigenically distinct serotypes named DEN-1 to DEN-4. Although it is difficult to accurately estimate, at least 100 million cases of dengue occur each year, more than 500,000 of them as haemorrhagic fever (DHF) and shock syndrome (DSS), even of uncertain etiology(1). The increasing incidence of the disease in Latin America
coincides with the re-invasion by Aedes aegypti as an urban mosquito vector in the region.
Overview Flaviviruses comprise mosquito-borne, tick-borne and unknown vector viruses. There are several dozens of them known to be antigenically related and of widespread geographical distribution(2). They are RNA viruses and their genome has nearly 11.0 kb.
The virions contain three structural proteins: the capsid (C), the membrane (M) and the envelope (E). The infected cell has to contain seven non-structural proteins (NS) known by the abbreviations NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5(3).

Epidemiology and Phylogenetic Relationships of Dengue Viruses
92 Dengue Bulletin – Vol 27, 2003
Flavivirus evolution, epi-demiology and dispersal are believed to have been determined by a combination of several factors, which reflect the arthropod vector’s life cycle, vertebrate hosts and the impact of human commercial activities. For instance, the growth of dengue haemorrhagic fever was brought about because of increasing human and mosquito populations in urban areas. The envelope gene (E) sequence was used in the analysis of the phylogenetic tree structure, revealing a continuous and asymmetric branching in tick-borne flaviviruses contrasting with a relatively recent explosive radiation of mosquito-borne viruses(4).
Phylogenetic analysis As already mentioned, the genus comprises many viruses that are important human pathogens and cause diseases such as dengue
(DEN), Japanese encephalitis (JE), St. Louis encephalitis (SLE), and yellow fever (YF). Recently, there were reported outbreaks of West Nile (WN) meningitis in northeastern United States(5).
The NS5 gene phylogeny defined three major groups of the genus, divided as mosquito-borne, tick-borne and unknown vector viruses(6,7). Analyses also showed that three bat-associated viruses (Entebbe, Sokoluk, and Yokose) can be grouped as mosquito-borne viruses establishing a lineage along with yellow fever and Sepik viruses. When epidemiological characteristics of mosquito-borne viruses are mapped into phylogenetic trees, there is a correlation between the main vector genera and the main vertebrate hosts, those primarily isolated from Aedes and the ones isolated from Culex. Both are called here “clades” (Figure 1)(2).
Even though the genus was found to be
monophyletic, the two groups of Aedes can be considered as paraphyletics, including the yellow fever and dengue viruses. The latter were kept in sylvatic primate cycles, while birds were not strongly associated in the clade. Contrastingly none of the Culex viruses are kept in primate cycles. Aedes clades of mosquito-borne flaviviruses are normally associated with haemorrhagic
diseases, while Culex clades are commonly associated with encephalitic diseases. There are rare cases of dengue encephalitis(8,9).
Geographical distribution Flaviviruses now recognized as a diverse group could have emerged and spread in the last 10,000 years since the most recent ice
Clades
Culex
Aedes
Aedes
General clinical patterns
Encephalitic disease
Haemorrhagic disease
Haemorrhagic disease
Viruses
DEN (1 to 10)
Vertebrate hosts
Bird, Rodent (?)
Human, Primate
Human, Primate, Bats
Figure 1. Phylogeny of the Culex and Aedes clades based on NS5 gene sequence and E gene amino acid sequence (Gaunt et al. 2001)(2)

Epidemiology and Phylogenetic Relationships of Dengue Viruses
Dengue Bulletin – Vol 27, 2003 93
age(4). All viruses in the Aedes clades are found only in the Old World, except for the yellow fever virus and dengue serotypes that are also found in the New World. In contrast, viruses of the Culex clades can be seen worldwide.
Evolution Each of the four dengue serotypes shows substantial genetic variation and distinct genotypes. There are two genotypes for DEN-1 and DEN-4, four for DEN-2 and DEN-3. Most probably there are more genetic variations that could be promoting epidemics when new strains reach populations without an adequate level of immunity. For example, one of the four DEN-2 genotypes was found as having only a sylvatic cycle in West Africa. If so, this is suggestive of a minor role in dengue epidemics.
It is reasonable to hypothesize that dengue viruses may have evolved from sylvatic strains that are transmitted among
non-human primates. This transmission may be due to the activity of other Aedes species. That hypothesis was tested in phylogenetic studies using the enveloped protein gene sequences (E) of both endemic/epidemic and sylvatic virus strains(10).
Thus, it is possible to accept the occurrence of two DEN transmission cycles. One is the endemic/epidemic cycle, involving human hosts and vectors such as Aedes aegypti, Aedes albopictus and other Aedes mosquitoes. The other is an essentially zoonotic or sylvatic cycle, involving non-human primate hosts and several Aedes mosquitoes, which occurs mainly in sylvatic habitats of Africa and Malaysia. There are a series of mosquito species where African DEN-2 has been isolated. In Malaysia, all four DEN serotypes are kept in Aedes niveus and non-human primates. Hence, it may be inferred that the lack of human population concentrations prior to a few thousand years ago is suggestive of the sylvatic cycle’s ancestry. The endemic/epidemic form probably evolved after the advent of urban population (Figure 2).
Sylvatic cycle
Endemic/Epidemic
Sylvatic cycle
Endemic/Epidemic
Endemic/Epidemic
Endemic/Epidemic
Sylvatic cycle
DEN 4
DEN 1
DEN 3
DEN 2
Figure 2. Phylogenetic tree derived from E protein gene nucleotide of sylvatic and endemic/epidemic DEN (Wang et al. 2000)(10)

Epidemiology and Phylogenetic Relationships of Dengue Viruses
94 Dengue Bulletin – Vol 27, 2003
The different DEN serotypes probably diverged in a remote past. Emergence of human infections is a relatively recent event in the history of DEN and most likely occurred when sylvatic viruses infected non-human primates. The DEN ancestry probably arose in the Asian-Oceanic region and diverged into the four recognized serotypes.
Because Aedes. aegypti is scarce in that region, Aedes albopictus and other Aedes mosquitoes were probably the primitive human vectors. The introduction of Aedes aegypti as a vector from its African origin may have occurred a few centuries ago with the expansion of trading.
References
1. Holmes EC. Molecular epidemiology and evolution of emerging infectious diseases. British Medical Bulletin, 1998; 54: 533-543.
2. Gaunt MW, Sall AA, Lamballerie X de, Falconar AKI, Dzhivanian TI and Gould EA. Phylogenetic relationships of flaviviruses correlate with their epidemiology, disease association and biogeography. Journal of General Virology, 2001, 82: 1867-1876.
3. Rice CM. Flaviviridae: The viruses and their replication. In: Fields Virology, 3rd ed, Edited by Fields BN, Knipe DM, Howley PM. Philadelphia: lippincott-Raven: 931-959.
4. Zanotto PM de A, Gould EA, Gao GF, Harvey PH and Holmes EC. Populations dynamics of flaviviruses revealed by molecular phylogenies. Proc Natl Acad Sci, 1996, 93: 548-553.
5. Lanciotti RS, Roehrig JT, Deubel V, Smith J, Parker M, Steele K, Crise B, Volpe KE, Crabtree MB, Scherret JH, Hall RA, MacKenzie JS, Cropp CB, Panigrahy B, Ostlund E, Schmitt B, Malkinson M, Banet C, Weissman J, Komar N, Savage HM, Stone W, McNamara T and Gubler DJ. Origin of the West Nile virus responsible for an outbreak of encephalitis in the northeastern United States. Science, 1999, 286: 2333-2337.
6. Kuno G, Chang G-JJ, Tsuchiya R, Karabatsos N and Cropp CB. Phylogeny of the genus Flavivirus. Journal of Virology, 1998, 72: 73-83.
7. Billoir F, Chesse R de, Tolou H, Micco P de, Gould EA and Lamballerie X de. Phylogeny of the genus Flavivirus using complete coding sequences of arthropod-borne viruses and viruses with no know vector. Journal of General Virology, 2000, 81: 781-790.
8. Lum LCS, Lam SK, Choy YS, George R and Harun F. Dengue encephalitis: A true entity? Am J Trop Med Hyg, 1996, 54: 256-259.
9. Solomon T, Dung NM, Vaughn DW, Kneen R, Thao LT, Raengsakulrach B, Loan HT, Day NP, Farrar J, Myint KS, Warrell MJ, James WS, Nisalak A and White NJ. Neurological manifestations of dengue infection. Lancet, 2000, 355: 1053-1059.
10. Wang E, Ni H, Xu R, Barrett ADT, Watowich SJ, Gubler DJ and Weaver SC. Evolutionary relationships of endemic/epidemic and sylvatic dengue viruses. Journal of Virology, 2000, 74: 3227-3234.

Dengue Bulletin – Vol 27, 2003 95
Development of IgM-capture Enzyme-Linked Immunosorbent Assay for Serodiagnosis of Dengue
using Beta-propiolactone-inactivated Dengue Viral Antigens
by Masaru Nawa*#, Tomohiko Takasaki**, Ken-Ichiro Yamada**, Ichiro Kurane**
and Toshitaka Akatsuka*
*Department of Microbiology, Saitama Medical School, 38, Moroyama, Saitama 350-0495, Japan **Division of Vector-Borne Viruses, Department of Virology 1, National Institute of Infectious Diseases,
1-23-1, Toyama, Shinjyuku-ku, Tokyo 162-8640, Japan
Abstract
Dengue viral antigen was treated with beta-propiolactone (BPL) and used in immunoglobulin M (IgM)-capture enzyme-linked immunosorbent assay (IgM-capture ELISA) for the serodiagnosis of dengue. Dengue viruses lost infectivity after treatment with 0.2% BPL at 37oC for 10 minutes and longer. Forty-eight human serum samples, including both positives and negatives, were tested by IgM-capture ELISAs with untreated and BPL-treated dengue antigens. The results obtained by IgM-capture ELISA with BPL-treated dengue antigens were consistent with those obtained by ELISA with untreated dengue antigens. This IgM-capture ELISA system with BPL-inactivated dengue antigens is safe and more suitable for use in diagnostic laboratories.
Keywords: Dengue, IgM-capture ELISA, Beta-propiolactone.
# For correspondence: [email protected]
Introduction Dengue fever (DF)/dengue haemorrhagic fever (DHF) is a serious public health problem in many tropical and subtropical areas of the world(1). In recent years, epidemics of DF/DHF have dramatically increased in the Western Pacific, South-East Asia and South America because of rapid
population growth, uncontrolled urbanization and increased frequency of air travel(2). DF/DHF will continue to be a major public health problem in the world unless effective control measures are taken. Dengue surveillance is essential to monitor epidemics, both at national and international levels. Laboratory diagnosis is necessary to confirm dengue virus infections. We have

Development of IgM-capture ELISA for Serodiagnosis of Dengue using BPL
96 Dengue Bulletin – Vol 27, 2003
previously reported about dengue IgM-capture ELISA with a high sensitivity(3).
Four types of dengue viruses were combined and used as a tetravalent dengue antigen in the IgM-capture ELISA. Dengue viruses are a human pathogen, and the use of infectious viruses as antigens can be a potential problem in the assay. In the present study, we used beta-propiolactone (BPL)-inactivated dengue viruses as antigens in IgM-capture ELISA to access its specificity and sensitivity vis-à-vis infectious viruses as antigens.
Materials and methods
IgM-capture ELISA was performed as previously reported(3,4). Forty-eight serum specimens from 33 Japanese dengue-confirmed cases were used in the study. The sera were obtained in clinics and hospitals in Japan from 1998 to 2000 and sent to the Department of Virology 1, National Institute of Infectious Diseases, Tokyo, Japan. The sera were stored at –80oC before use. The serum samples (0.1 ml) diluted at 1:101 were subjected to ELISA. The result was obtained with a positive to negative (P/N) ratio: P/N ratio = A492, reading with the
viral antigen/A492, reading with uninfected
control antigen.
IgG purified from pooled dengue patients sera (H-IgG) and the flavivirus-specific monoclonal antibody, D1-4G2-4-15 (4G2)(5), were used as the detection antibodies. IgG was purified by protein G affinity column chromatography (Immuno-
Pure IgG Purification kit®, Perbio Science,
Erembodegen-Aalst, Bergium), and then conjugated with horseradish peroxidase (EZ-
Link Plus Activated Peroxidase kit®, Perbio Science).
Prototype dengue viruses were inactivated by incubation with BPL at a final concentration of 0.2% (v/v) for 30 min at 37oC. The infectivity of the virus was titrated by the focus-forming method in Vero cells(6).
Results and discussion
Prototype dengue virus strains: type 1, Hawaii; type 2, New Guinea C; type 3, H87 and type 4, H241, were propagated in mosquito cell clone, C6/36, and then inactivated by BPL. The infectivity of the viruses obtained before and after BPL treatment is presented in the Table. Dengue viruses lost infectivity after treatment with BPL for 10, 30 and 60 minutes (Table).
In order to prepare the assay antigen, BPL-treated antigen titration was carried out by an antibody sandwich ELISA according to the previously described method(3). (data not shown). The tetravalent antigen was prepared by mixing equal volumes of each monovalent antigen according to the method described previously(3,4).
The reactivity to H-IgG and 4G2 IgG was compared between the untreated and BPL-treated dengue antigens (Figure 1). The reactivity of the BPL-treated virus to H-IgG was low, while that to 4G2 IgG was high enough to be used as antigen in IgM-capture ELISA.

Development of IgM-capture ELISA for Serodiagnosis of Dengue using BPL
Dengue Bulletin – Vol 27, 2003 97
Table. Effect of BPL on infectivity of dengue viruses
Dengue virus serotypes
Original virus titres
FFU/0.025 ml
Incubation time (min)
No BPL treatment
FFU/0.025 ml
0.2 % BPL FFU/0.025 ml
DEN-1 6.9 x 105 10 30 60
6.9 x 105
6.2 x 105
5.9 x 105
< 1.0 x 102
< 1.0 x 102
< 1.0 x 102
DEN-2 1.2 x 105 10 30 60
1.2 x 105
1.1 x 105
1.0 x 105
< 1.0 x 102
< 1.0 x 102
< 1.0 x 102
DEN-3 1.3 x 104 10 30 60
1.3 x 104
1.3 x 104
1.3 x 104
< 1.0 x 102
< 1.0 x 102
< 1.0 x 102
DEN-4 4.8 x 104 10 30 60
4.6 x 104
4.6 x 104
4.6 x 104
< 1.0 x 102
< 1.0 x 102
< 1.0 x 102
FFU: focus formin unit
[Dengue antigen captured on the solid phase was detected by horseradish peroxidase-conjugated H-IgG (2.5 µg/ml, square) and 4G2 IgG (2.5 µg/ml, circle). Solid lines indicate mock-treated antigen, and broken
lines indicate BPL-treated antigen.]
Antigen dilution
0.0
0.5
1.0
1.5
2.0
2.5
3.0
1 x 2 x 4 x 8 x 16 x 32 x 64 x
ELIS
A O
.D.
Figure 1. Reactivity of the tetravalent BPL-treated dengue viral antigen
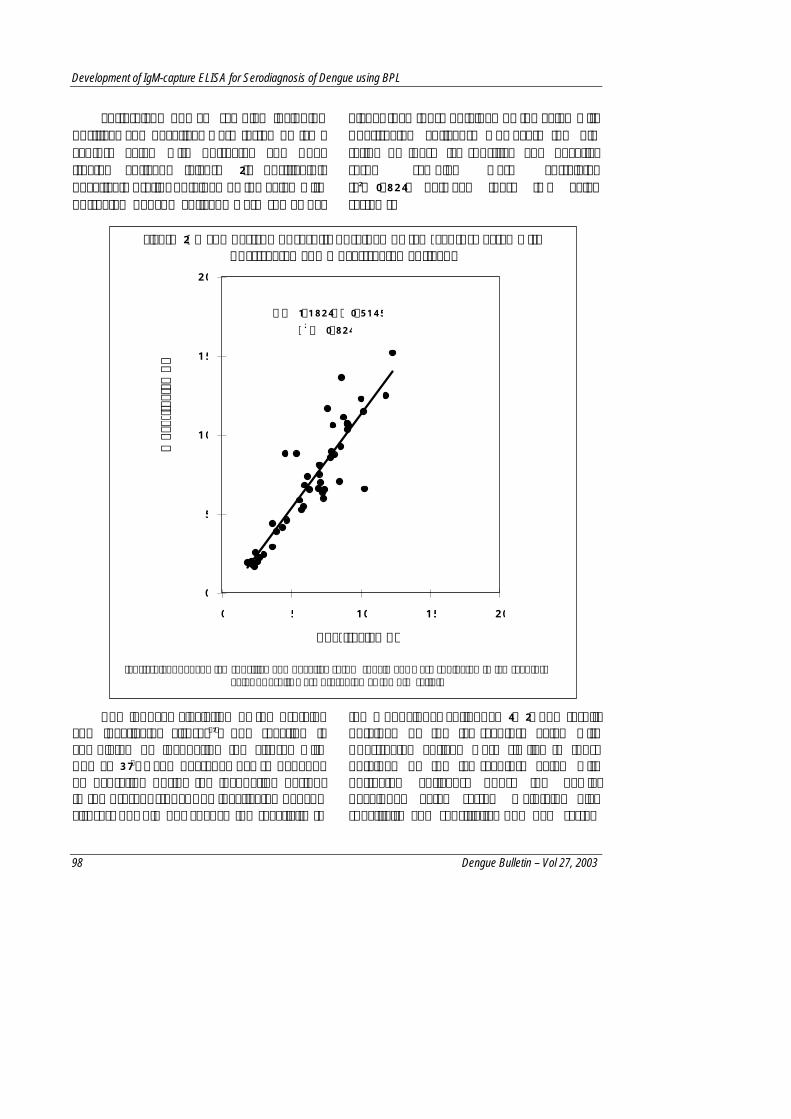
Development of IgM-capture ELISA for Serodiagnosis of Dengue using BPL
98 Dengue Bulletin – Vol 27, 2003
Forty-eight human samples including positives and negatives were tested by IgM-capture ELISA with untreated and BPL-treated antigens (Figure 2). Positive(P)/ negative(N) ratios obtained by the ELISA with untreated dengue antigens were somewhat
higher than those obtained by the ELISA with BPL-treated antigens. However, the P/N ratios of these IgM-positive and negative serum samples were correlated (r2=0.824) between these two ELISA systems.
[Forty-eight dengue IgM-positive and negative serum specimens were subjected to IgM-capture
ELISA. Results were presented as the P/N ratio.]
BPL induces alkylation of the proteins and inactivates viruses(7). The reaction is completed by incubating the viruses with BPL at 37oC, and degrades per se depends on hydration during the incubation period. In the present study, BPL inactivated dengue viruses, but did not change the reactivity to
the monoclonal antibody, 4G2. The results obtained by the IgM-capture ELISA with BPL-treated antigen were similar to those obtained by the IgM-capture ELISA with untreated antigens. Thus, the newly-developed ELISA system maintains high specificity and sensitivity. The new system
y = 1.1824x - 0.5145 r 2 = 0.824
0
5
10
15
20
0 5 10 15 20
BPL-treated Ag
Moc
k-tre
ated
Ag
Figure 2. A comparison of results obtained by IgM-capture ELISA with BPL-treated and mock-treated antigens

Development of IgM-capture ELISA for Serodiagnosis of Dengue using BPL
Dengue Bulletin – Vol 27, 2003 99
also has the advantage in the prevention of possible laboratory infections. The IgM-capture ELISA with BPL-inactivated dengue antigen is, therefore, suitable for use in diagnostic laboratories in developing countries.
Acknowledgement This work was supported by grants from the Research on Emerging and Re-emerging Infectious Diseases, Ministry of Health, Labour and Welfare, Japan.
References 1. McBride WJ and Bielefeldt-Ohmann H. Dengue
viral infections: Pathogenesis and epidemiology. Microbes Infect, 2000, 2: 1041–1050.
2. Gubler DJ and Melzer M. Impact of dengue/dengue haemorrhagic fever on the developing world. Adv Virus Res, 1999, 53: 35–70.
3. Nawa M, Takasaki T, Yamada K, Akatsuka T and Kurane I. Development of dengue IgM-capture enzyme-linked immunosorbent assay with higher sensitivity using monoclonal detection antibody. J Virol Methods, 2001, 92: 65–70.
4. Nawa M, Yamada K, Takasaki T, Akatsuka T and Kurane I. Serotype-cross-reactive immunoglobulin M responses in dengue virus infections determined by enzyme-linked immunosorbent assay. Clin Diagn Lab Immunol, 2000, 7: 774–777.
5. Gentry MK, Henchal EA, McCown JM, Brandt WE and Dalrymple JM. Identification of distinct antigenic determinants on dengue-2 virus using monoclonal antibodies. Am J Trop Med Hyg, 1982, 31: 548–555.
6. Despres P, Frenkiel MP and Deubel V. Differences between cell membrane fusion activities of two dengue type-1 isolates reflect modifications of viral structure. Virology, 1993, 196: 209–219.
7. Microbiology, 4th ed., pp 146–147. Edited by Prescott LM, Harley JP and Klein DA. (1999), WCB McGraw-Hill, London.

100 Dengue Bulletin – Vol 27, 2003
Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
by Hui-Yee Chee and Sazaly AbuBakar#
Department of Medical Microbiology, Faculty of Medicine, University of Malaya, Lembah Pantai, 50604 Kuala Lumpur, Malaysia
Abstract
Dengue virus type-2 (DEN-2) has been isolated in Malaysia for more than three decades. The virus caused two major outbreaks in the early 1990s and late 1990s. Phylogenetic analyses performed using available E/NS1 junction sequences identified two DEN-2 genotypes: DEN-2 Asian 1 and DEN-2 Cosmopolitan. DEN-2 Cosmopolitan/Malaysia is the predominant genotype comprising more than 80% of the total isolates. Two different clades of DEN-2 Cosmopolitan/Malaysia genotype were identified. Clade I consisted of mainly the older isolates, whereas Clade II consisted of the more recent isolates, including that responsible for both the major DEN-2 outbreaks. Two different strains of DEN-2 Cosmopolitan/Malaysia genotype were involved in the outbreaks, yet both strains appeared to share a common ancestral lineage with isolates from the early 1970s. Isolates from the late 1990s showed higher sequence similarities to the late-1960s isolates than the early-1990s isolates. These findings raised the possibility that the different DEN-2 strains noted over the last three decades in Malaysia might have evolved from a pre existing DEN-2 gene pool.
Keywords: Dengue, genotypes, outbreak, phylogenetic, Malaysia.
# For correspondence: [email protected]
Introduction The existence of dengue fever (DF) in Malaysia was first described following an outbreak in Penang, a northern state in the Malaysian peninsula, in 1902(1). In 1954, the first-ever isolate of dengue virus, a DEN-1 was obtained during an outbreak in Kuala Lumpur(2). Eighteen years later (1962), the first case of dengue haemorrhagic fever (DHF) was reported(3). Dengue has since become endemic in Malaysia, with an average incidence of about 400 to 7,000
cases of DF/DHF annually. All four serotypes are found co-circulating in the country with DEN-2 and DEN-3 being the most commonly isolated serotypes. A recent analysis of the trend and pattern of dengue in Malaysia over the last few decades showed that major DF/DHF outbreaks occurred in a cyclical pattern of approximately eight years and it involved mainly DEN-1, DEN-2 and DEN-3(4). The cycle is thought to be associated with the switching of the predominant dengue virus serotypes in the population. For example, it

Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
Dengue Bulletin – Vol 27, 2003 101
was reported that a major outbreak of DF/DHF involving predominantly DEN-1 that occurred in Malaysia between 1997 and 1998 was preceded by high levels of DEN-3 in the population. Similarly, the outbreak in 1990-1991 involving mainly DEN-2 was preceded by a high occurrence of DEN-1(4). The outbreaks involving DEN-4, however, occurred only in the 1960s and it has not been reported ever since. The disappearance of outbreaks involving DEN-4 coincided with its replacement by other dengue virus serotypes, especially DEN-2 as the dominant serotype, in Malaysia. Though DEN-2 emerged as a major serotype in the late 1960s until the early 1970s, it has since persisted in the country and has been responsible for the major outbreaks that occurred in late 1980s to early 1990s and the subsequent outbreak in late 1990s to early 2000s. It is not presently known, however, if a similar DEN-2 strain was responsible for these outbreaks and whether that the strain has also persisted in the population over the last three decades. In an effort to address these issues, we sequenced the E/NS1 gene junction of twelve DEN-2 isolates from the two outbreaks and examined the phylogenetic relationships of these isolates against those of the earlier isolates.
Materials and methods Three sets of DEN-2 isolates obtained from DF/DHF patients treated at the University of Malaya Medical Center (UMMC) during 1989-1991, 1995-1996 and 1998-2000 were used in the present study. The five isolates each from 1989-1991 (early 1990s) and 1998-2000 (late 1990s) were from the two outbreaks involving DEN-2, whereas the 1995-1996 isolates represented the in-between outbreak strains. The isolates were
initially serotyped using specific monoclonal antibody and subsequently confirmed using multiplex RT-PCR(5) and DNA sequencing. The E/NS1 sequences were amplified using two pairs of oligonucleotide primers that amplify DEN-2 sequence from nucleotide positions 1777-2512 and 2422-3477. The amplification conditions, parameters and DNA sequencing were performed as previously described(6). Contigs and consensus sequences were assembled using Sequencher version 4.0.5 (Gene Codes Corporation, USA) and the nucleotide sequences generated after removing the extra nucleotides were used. Phylogenetic analyses were performed as previously described(6) with additional analysis using the maximum likelihood method as implemented in PHYLIP 3.6(7). The E/NS1 junction sequence was used in the present study as unlike other genes, this gene region is not under the immune selection pressure; hence, is most suitable as a marker for long-term evolutionary study(8). Furthermore, several studies, apart from our own (data not shown), have shown that phylogenetic trees constructed using this genome region are robust and correspond well with trees constructed using other genes such as E(9), NS1(10) and the full-length genome(11).
Results A total of 63 DEN-2 E/NS1 sequences were used in the present study. These included 27 sequences obtained from the GenBank which included a sylvatic DEN-2 isolate (PM33974), a representative DEN-2 American genotype (Genotype I; Ven2), a representative DEN-2 Asian 1 genotype (K0010), a representative DEN-2 Asian 2 genotype (Genotype II; NGC) and a representative DEN-2 Cosmopolitan genotype (Genotype IV; 975). The remaining

Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
102 Dengue Bulletin – Vol 27, 2003
sequences were from the Malaysian isolates, which included 24 sequences obtained from Fong et al,(12) one sequence from the GenBank (LF5-99) and 12 sequences obtained from the present study (Table). A neighbour-joining (NJ) tree depicting the phylogenetic relationships of the isolates was obtained using DEN-2 sylvatic isolate (PM33974) as the outward group (Figure 1). The NJ-generated trees were very similar to that generated with the maximum-likelihood (ML) method, with minor branch swapping at the terminal nodes (data not shown). From the phylogenetic tree, it was noted that the Malaysian DEN-2 isolates were grouped into two different genotypes, Asian 1 and Cosmopolitan, with approximately 83.3% (30/36) of the isolates grouped into the Cosmopolitan genotype(13). The Cosmopolitan genotype included isolates from as early as 1968 to as recently as 2000. The Cosmopolitan genotype, DEN-2, also included two isolates from Sarawak (East Malaysia), KS30 and LF5-99 and three isolates from outside the Klang Valley.
Isolates belonging to the Asian 1 genotype included those obtained in 1982, 1987, 1988, 1991 and 1995. The average percentage of nucleotide divergence between the two DEN-2 genotypes, Asian 1 and Cosmopolitan, was 7.1% (range 4% to 11%) with the average percentage of nucleotide divergence within the Cosmopolitan and Asian 1 genotypes at 3.5% (range 0% to 7%) and 2.8% (range 0% to 7%), respectively. Incidentally, the DEN-2 Asian 1 genotype consisted mainly of isolates from Thailand and Myanmar, whereas the Cosmopolitan genotype included isolates from other parts of the world. Among the 12 isolates sequenced in the present study, 11 were of Cosmopolitan genotype, of which nine were from DHF patients and two were from DF patients (isolates MY91-99133 and MY00-21986). The relationships between genotypes and clinical manifestations, however, could not be ascertained as no additional information on the disease severity was available for most of the isolates.
Table. DEN-2 isolates used in the study
*Isolate Year of isolation
Location of isolation Diagnosis GenBank accession no.
MY89-83995 1989 Klang Valley DHF AJ556803 MY89-88549 1989 Klang Valley DHF AJ556804 MY91-94129 1991 Klang Valley DHF AJ556805 MY91-95062 1991 Klang Valley DHF AJ556806 MY91-99133 1991 Klang Valley DF AJ556807 MY95-2303 1995 Klang Valley DF AJ556808 MY96-5176 1996 Klang Valley DHF AJ556809 MY98-15996 1998 Klang Valley DHF AJ556810 MY98-17933 1998 Klang Valley DHF AJ556811 MY99-19575 1999 Klang Valley DHF AJ556812 MY99-19586 1999 Klang Valley DHF AJ556813 MY00-21986 2000 Klang Valley DF AJ556814
* Other DEN-2 E/NS1 sequences used in the present study are available from GenBank and Fong et al, 1998(12).
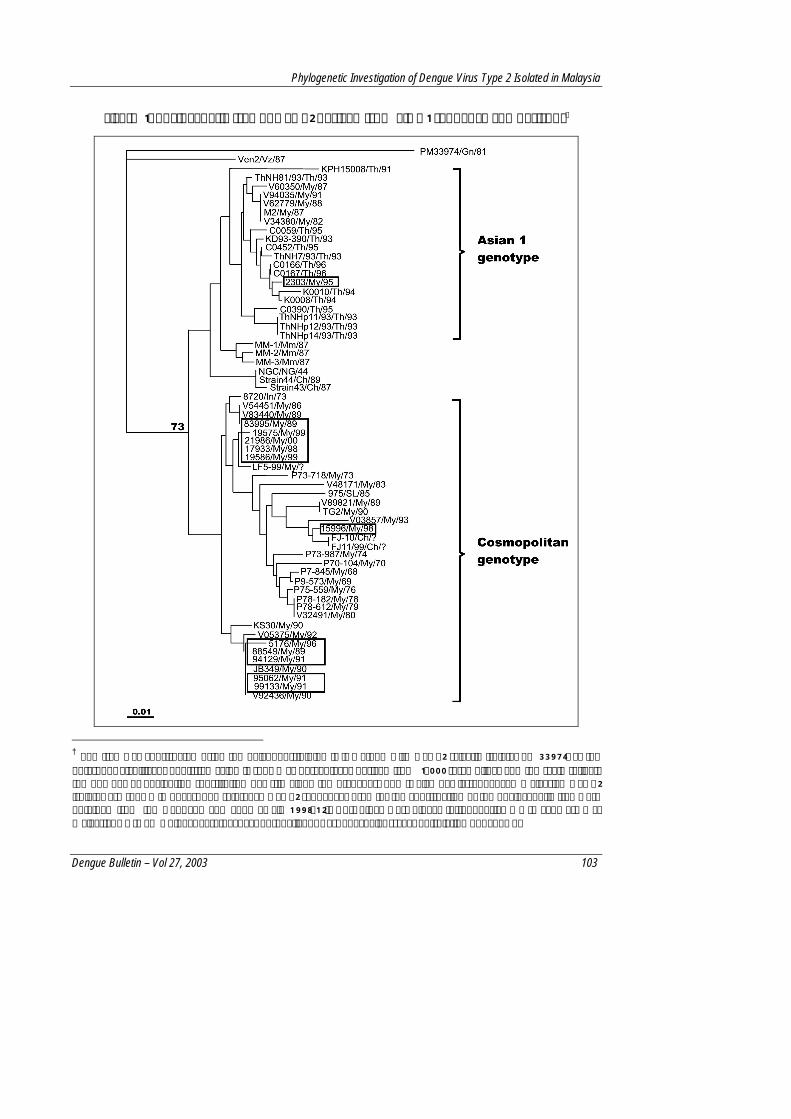
Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
Dengue Bulletin – Vol 27, 2003 103
Figure 1. Phylogenetic tree of DEN-2 derived from E/NS1 sequence comparisons†
† The tree was constructed using the neighbour-joining (NJ) method with DEN-2 sylvatic isolate, PM33974, as the outgroup. Significant bootstrap value is shown as percentages derived from 1,000 resamplings and the scale reflects the number of nucleotide substitution per site along the branches. The twelve newly-sequenced Malaysian DEN-2 isolates are shown in boxes. The reference DEN-2 sequences used for the construction of the phylogenetic tree were obtained from the GenBank and Fong et al, 1998(12). Ch-China; Gn-Guinea; In-Indonesia; Mm-Myanmar; My-Malaysia; NG-New Guinea; SL-Sri Lanka; Th-Thailand; Vz-Venezuela; ?-year of isolation not known.

Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
104 Dengue Bulletin – Vol 27, 2003
Figure 2. Phylogenetic relationships amongst DEN-2 Cosmopolitan genotype isolated in Malaysia‡
‡ The phylogenetic tree was derived from E/NS1 sequence comparisons and constructed using the neighbour-joining (NJ) method. The tree is shown with DEN-2 sylvatic isolate, PM33974 as the outgroup. Significant bootstrap value is shown as percentages derived from 1,000 re samplings and the scale reflects the number of nucleotide substitution per site along the branches.
Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
Dengue Bulletin – Vol 27, 2003 105
A phylogenetic tree drawn using only the Malaysian Cosmopolitan genotype isolates (Figure 2) showed that the isolates were grouped into at least two clades (Clade I and Clade II), with an average percentage of nucleotide divergence of 2.2% (range 1% to 3%). Clade I showed two clusterings (Ia & Ib) of the isolates with isolates from the late 1960s (P7-845 and P9-573) and 1970s (P70-104, P73-987, P75-559, P78-182, P78-612 and V32491) grouped into cluster Ib. Within this cluster all the isolates from late 1970s (1976–1980) were grouped together away from the 1968-1969 isolates. The early-1970s isolates (1970-1974) formed the outer group. The bootstrap values supporting these groupings, however, were low. The other cluster (Ia) within Clade I comprised isolates from 1980s (V48171 and V89821) and also 1990s (TG2, V03857 and MY98-15996). Similar to Clade I, two main clusterings of isolates were also noted in Clade II (IIa & IIb) with the main cluster (IIb) comprising isolates from 1986–1996 (early 1990s) and the other cluster consisted of isolates mainly from 1999 to 2000 (late 1990s). The separation of these two later clusters received a strong bootstrap support (>75%), suggesting that the two isolates were different. Hence, this supports the involvement of two different strains of DEN-2 Cosmopolitan genotype in the two major DEN-2 outbreaks in Malaysia. Comparisons of the representative consensus sequences of each cluster showed only four nucleotide differences at nucleotide positions 75, 85, 99 and 234 that differentiated the early- and late-1990s DEN-2 isolates. These substitutions, however, did not result in any amino acid changes. On the other hand, comparisons made between the representative consensus
sequences of isolates from 1968-1969 with those of the early- and late-1990s isolates revealed nine and five nucleotide differences, respectively. The nine nucleotides substitution noted in the sequence of the early-1990s isolates occurred at positions 9, 15, 75, 85, 99, 183, 186, 228 and 234 whereas the five nucleotides substitution for the late-1990s isolates occurred at positions 9, 15, 183, 186 and 228. It was apparent from these results that isolates from the late 1990s shared higher-sequence similarities to the much older DEN-2 isolates than that of the early-1990s isolates.
Discussion The findings from the present study revealed the presence of at least two main DEN-2 genotypes in Malaysia. The Cosmopolitan genotype(13), also known as genotype IV(8), is the dominant genotype comprising more than 80% of all DEN-2 isolates of Malaysia. This genotype includes two of the oldest DEN-2 isolates, P7-845 and P9-573, which were isolated in 1968 and 1969, respectively. The other minor genotype present in Malaysia belongs to the Asian 1 genotype, also known as genotype II. This later genotype comprised mainly of isolates from Thailand and Myanmar; hence, raised the possibility that the Malaysian Asian 1 isolates may not be native to Malaysia, but perhaps were associated with the Malaysia-Thailand cross-border economic activities, as Malaysia shares it northern land border with southern Thailand. It is interesting to note that despite the long borders and vigorous cross-border economic activities and travels, the DEN-2 genotypes dominant in the two

Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
106 Dengue Bulletin – Vol 27, 2003
countries are different. While the Asian 1 genotype appeared localized mainly in Thailand, the Cosmopolitan isolates dominant in Malaysia have been isolated in as far as Burkina Faso in West Africa. The Cosmopolitan genotype has also been isolated in Singapore, India, Sri Lanka, Seychelles, Somalia, Uganda and Australia(13), all of which once used to be part of the British colonial empire. Whether the spread or the lack of it between the two genotypes was related to historical reasons involving movement of people between different countries and regions, Malaysia, unlike Thailand which has never been under the British rule, was a British colony until 1957 or involved different mosquito vectors remains to be investigated.
The phylogenetic analyses of the dominant Cosmopolitan/Malaysian genotype DEN-2 isolated in Malaysia over the last three decades did not suggest a clear evolution of the DEN-2 virus from a single common ancestral lineage. Instead, two clades with two sub-clusters each were noted with the 1968-1969 isolates belonging to Clade I, which, incidentally, has an isolate from 1983 as the apparent ancestor, and Clade II which appeared to have arisen from a 1973 isolate. While the bootstrap support for the tree branches was weak, there was a clear trend suggesting a clustering of the isolates by the year of isolation; with the bulk of the isolates from 1970s found in Clade I and the isolates mainly from the early 1990s and late 1990s well segregated in Clade II. Using the calculated estimate of the rate of nucleotide substitution for DEN-2 (7.19 X 10-4 subs/site/year)(14), and with the assumption that the late-1960s isolates consensus sequence as the most recent
common ancestor, it was noted that the isolates from the early 1990s had approximately three times more nucleotide substitutions (9 nucleotides) within this short sequence over 20 years when compared to the expected values of 3.4 nucleotides. This is in contrast to the isolates from the late 1990s, which had only five nucleotide substitutions over 30 years, which is within the predicted substitution rate of 5.1 nucleotides. From this simple estimate, it appeared that the sequence of isolates from the early 1990s underwent a much faster rate of nucleotide changes than expected. As the lineage of these isolates did not prevail a decade later, one wonders if this high rate of nucleotide changes within the E/NS1 junction is mirrored also in other genes and hence affected the ability of the virus to replicate efficiently. Furthermore, the appearance in the late-1990s outbreak of isolates with higher sequence similarity to the late-1960s isolates also raised the possibility that the different DEN-2 strains noted over the last three decades in Malaysia may have evolved from the pre-existing DEN-2 gene pool. As intra- and inter-typic recombination amongst dengue viruses are more common than once thought(6,15), it will be interesting to monitor whether DEN-2 genotype Asian 1 sequence will eventually end up in the Malaysian DEN-2 gene pool.
Acknowledgement This study received financial support from the Ministry of Science, Technology, and the Environment, Malaysia, IRPA Grants #06-02-03-0303/0304, and the University of Malaya Research Grants.

Phylogenetic Investigation of Dengue Virus Type 2 Isolated in Malaysia
Dengue Bulletin – Vol 27, 2003 107
References 1. Skae FMT. Dengue fever in Penang. British
Medical Journal, 1902, 2: 1581-1582.
2. Smith CEG. Isolation of three strains of type 1 dengue virus from a local outbreak of the disease in Malaysia. Journal of Hygiene, 1956, 54: 569-580.
3. Rudnick A, Tan EE, Lucas JK and Omar M. Mosquito-borne haemorrhagic fever in Malaya. British Medical Journal, 1965, 1: 1269-1272.
4. AbuBakar S and Shafee N. Outlook of dengue in Malaysia: A century later. Malaysian Journal of Pathology, 2002, 24: 23-27.
5. Seah CL, Chow VT, Tan HC and Chan YC. Rapid, single-step RT-PCR typing of dengue viruses using five NS3 gene primers. Journal of Virological Methods, 1995, 51: 193-200.
6. AbuBakar S, Wong P-F and Chan Y-F. Emergence of dengue virus type 4 genotype IIA in Malaysia. Journal of General Virology, 2002, 83: 2437-2442.
7. Felsenstein J. PHYLIP-Phylogeny Inference Package (Version 3.2). Cladistics, 1989, 5: 164-166.
8. Rico-Hesse R. Molecular evolution and distribution of dengue viruses type 1 and 2 in nature. Virology, 1990, 174: 479-493.
9. Lewis JA, Chang GJ, Lanciotti RS, Kinney RM, Mayer LW and Trent DW. Phylogenetic relationships of dengue-2 viruses. Virology, 1993, 197: 216-224.
10. Blok J, Gibbs AJ, McWilliam SM and Vitarana UT. NS 1 gene sequences from eight dengue-2 viruses and their evolutionary relationships with other dengue-2 viruses. Archives of Virology, 1991, 118: 209-223.
11. Leitmeyer KC, Vaughn DW, Watts DM, Salas R, de Chacon VI, Ramos C and Rico-Hesse R. Dengue virus structural differences that correlate with pathogenesis. Journal of Virology, 1999, 73: 4738-4747.
12. Fong MY, Koh C-L and Lam S-K. Molecular epidemiology of Malaysian DEN-2 viruses isolated over twenty-five years (1968-1993). Research in Virology, 1998, 149: 457-464.
13. Twiddy SS, Farrar JJ, Chau NV, Wills B, Gould EA, Gritsun T, Lloyd G and Holmes EC. Phylogenetic relationships and differential selection pressures among genotypes of dengue-2 virus. Virology, 2002, 298: 63-72.
14. Twiddy SS, Holmes EC and Rambaut A. Inferring the rate and time-scale of dengue virus evolution. Molecular Biology and Evolution, 2003, 20: 122-129.
15. Worobey M, Rambaut A and Holmes EC. Widespread intra-serotype recombination in natural populations of dengue virus. Proceedings of the National Academic of Sciences USA, 1999, 96: 7352-7357.

108 Dengue Bulletin – Vol 27, 2003
Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
by M Narayanan#, M A Aravind, P Ambikapathy, R Prema and M P Jeyapaul
Institute of Social Paediatrics, Government Stanley Medical College and Hospital, Washermanpet, Chennai – 600 001, Tamil Nadu, India
Abstract
This study was conducted on seropositive cases of dengue less than 12 years of age admitted in a tertiary-level referral centre during the outbreak of dengue in Chennai, India, between October and December 2001.
Fifty-nine cases were admitted during the study period and detailed clinical history, physical examination and laboratory values were recorded on presentation. The cases were followed-up daily for the clinical and laboratory parameters. These children were stratified based on the presence or absence of complications like shock and haemorrhage. The frequency of various signs and symptoms and the values of laboratory tests were compared between the children with and without complications. The proportions were statistically analysed and the odds ratio for the development of complications based on the presence of each parameter was computed.
Sixteen clinical features and eight laboratory investigations were analysed in these patients. The factors related to shock were drowsiness (p=0.0002), positive tourniquet test (p=0.0004), low platelet count (p=0.005) and raised renal parameters (p=0.002). Parameters associated with bleeding manifestations were retro-orbital pain (p=0.006), more hepatomegaly (p=0.002) and low platelet count (p=0.045). Fall of haematocrit by more than 20% on fluid therapy was slightly more in the bleeding group (p=0.07).
There was no correlation between tourniquet test positivity and other bleeding manifestations. Bleeding was related to very low platelet counts (<50,000). However, moderately low platelet counts (50,000-100,000/cu.mm) were not associated with increase in the frequency of bleeding manifestations. Patients who did not develop shock were more likely to complain of body pain (p=0.07).
These results showed that children with dengue who present with drowsiness, retro-orbital pain, positive tourniquet test, platelet counts below 50,000/cu.mm and a fall of haematocrit on therapy by more than 20% and those who do not have body pain should be monitored very carefully, as they are more prone to develop complications.
Keywords: Dengue, complications, associations, Chennai.
#For correspondence: 4, Rohini Street, Rajaji Nagar, Villivakkam, Chennai-600049, Tamil Nadu, India. E-mail: [email protected]
Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
Dengue Bulletin – Vol 27, 2003 109
Introduction Dengue fever (DF) is the commonest of the arboviral infections in humans(1). The global incidence of DF dengue haemorrhagic fever (DHF) has increased dramatically in recent decades(1,2). In India, epidemics are becoming more frequent(1,2) and are straining the limited resources of the public health system. Many DF cases are self-limiting but its complications like haemorrhage and shock can be life-threatening. If untreated, mortality from the complications of DF is as high as 20%, whereas if recognized early and managed properly, mortality is less than 1%(2). Hence, it will be useful if certain symptoms, signs and laboratory parameters associated with the development of complications are identified so that such cases would receive more attention.
Many studies that focus on the difference between the frequency of clinical findings in DHF and dengue shock syndrome (DSS) with respect to classical DF have been published(3,4). The present study analyses the differences in the clinical findings between patients who develop complications (without strictly following the WHO case definitions(1)) and those who do not so that the parameters that are associated with, and hence may anticipate future complications, can be identified. These patients can then be admitted and treated with extra care so that mortality can be reduced.
Objectives The main objective of this study was to identify symptoms, signs and laboratory values in dengue fever associated with complications like shock and haemorrhage,
so that such patients could be admitted and monitored carefully.
Subjects and methods This study was conducted on seropositive cases of dengue less than 12 years of age admitted in the Paediatrics Department of the Government Stanley Medical College and Hospital, Chennai, during an outbreak of dengue in the city between October-December 2001.
Eighty-nine children identified as probable cases by clinical suspicion (any acute febrile illness with one of the following symptoms: myalgia, headache, retro-orbital pain, bleeding, altered sensorium, shock or low platelet count) were registered in the study, informed consent was obtained and a detailed clinical history, physical examination and baseline investigations were undertaken. For all cases, the rapid IgM-IgG capture ELISA test, which has become the gold standard for the serological diagnosis of dengue fever(1,5), was done at the King’s Institute of Preventive Medicine, Guindy, Chennai. Children positive for IgM alone or both IgM and IgG were followed-up for clinical profiling. Patients with an identified bacterial focus or any other identified specific infection were excluded. The number of cases included in the study, based on the above criteria, was 59, which included two children who satisfied the WHO criteria(1) for the diagnosis of DHF but died before serodiagnosis.
Children who were dengue seropositive were stratified into those with or without complications. Of the 59 children included in the study, 13 had shock and 39 had bleeding manifestations. Symptoms and signs

Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
110 Dengue Bulletin – Vol 27, 2003
like presence of fever, vomiting, headache, retro-orbital pain, body pain, abdominal pain, bleeding tendency, drowsiness, rash, bradycardia, lymphadenopathy, conjunctival suffusion, hepatomegaly, presence of fluid in third space and tourniquet test positivity were compared between the children with these complications and those without them. Laboratory investigations which were carried out in these patients included routine haematology – haemoglobin, total and differential leukocyte count, haematocrit, platelet count, routine biochemical investigation including liver function tests and urine examination. Complete blood counts including haematocrit was repeated daily during the acute phase of the illness. Chest X-ray was taken to demonstrate pleural effusion in all cases. CSF analysis was done in patients with convulsions or meningeal signs. The results of laboratory investigations were also compared between the two groups.
Statistical analysis
The relationship between the frequencies of the clinical parameter (risk factor) and complication (disease) was analysed after constructing a 2x2 table and applying the statistical test of significance (chi-squared test or Fisher’s exact test). Continuous data was analysed using student’s t-test. By univariate analysis, odds ratio (OR) along with the 95% confidence interval (CI) was determined. Multivariate analysis was done to remove the confounding effect of patients who had both shock and haemorrhagic manifestations. The statistical analysis was conducted by the package PEPI version 4.0 for Windows® (Abramson JH and Gahlinger PM (2001), Sagebrush Press, Salt Lake City).
Results Fifty-nine children between seven months and 12 years of age, with seropositive dengue, were included in the study; of these 13 developed shock and 39 had bleeding manifestations. Four children were in impending shock or manifest shock at the time of admission and 10 had bleeding manifestations on presentation at the hospital. On classifying the cases strictly according to the WHO criteria(1), five had DSS, 11 had DHF, 23 had dengue fever syndrome with unusual haemorrhage (DFB), and 20 had classical dengue fever (DF). Five patients with shock were in the DSS group, three in DFB and five in the DF group.
A comparison of the demographic characters showed that shock was more frequent in younger patients but the difference was not significant (p=0.36) (Table 1). Bleeding manifestations were equally common in all age groups. There was no predilection for any gender among the patients who developed complications.
On an analysis of the symptoms (Table 1), it was seen that children with dengue fever who did not have shock were eight times more likely to report body pain (p=0.004) (OR=0.12, 95% CI=0.02-0.67). Drowsiness was found to be significantly more frequent in patients who developed shock (p=0.008) (OR=6.5, 95% CI=1.65-32). Vomiting was also more common in those with shock, but the difference was not significant (p=0.29). Children who had complained of retro-orbital pain had a significantly higher frequency of bleeding (p=0.045).

Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
Dengue Bulletin – Vol 27, 2003 111
Table 1. Comparison of symptoms between children who developed complications and those who did not
S. No Characteristic N With Shock
Without Shock P Value* With
Bleed Without
Bleed P Value*
1 Total no. 59 13 46 - 39 20 -
2 Age (mean s.d.) - 6.07 (2.9) 6.96 (3.3) 0.36 (t) 6.92 (3.4) 7.1 (3) 0.55 (t)
3 Male sex (%) 31 7 (53.8) 24 (52.1) 0.92 (x) 21 (53.8) 10 (50) 0.78 (x)
4 Fever (%) 58 13 (100) 45 (97.8) 0.8 (f) 38 (97.4) 20 (100) 0.67 (f)
5 Vomiting (%) 49 12 (92.3) 37 (80.4) 0.29 (f) 33 (84.6) 16 (80) 0.45 (f)
6 Body pain (%) 32 2 (15.3)** 28 (60.8) 0.004 (x)N 20 (51.3) 12 (60) 0.52 (x)
7 Headache (%) 17 3 (23.1) 14 (30.4) 0.44 (f) 11 (28.2) 6 (30) 0.89 (x)
8 Retro-orbital pain (%) 7 1 (7.7) 6 (13.0) 0.51 (f) 7 (17.9) 0 (0) 0.045 (f)N
9 Drowsiness (%) 14 7 (53.8) 7 (15.2) 0.008 (f)N 9 (23.1) 5 (25) 0.56 (f)
10 Abdominal pain (%) 14 1 (7.7) 13 (28.3) 0.12 (f) 10 (25.6) 4 (20) 0.44 (f)
11 Bleeding (%) 39 8 (61.5) 31 (67.4) 0.46 (f) - - -
* The letter in parenthesis gives the statistical test employed in each case (t-student’s t-test; x-chi-squared test; f-Fisher’s exact test) ** Two patients had body pain only after recovery from shock N - The odds ratio and 95% confidence intervals were calculated for these-given in text
An analysis of the clinical signs (Table 2) showed that positive tourniquet test (TT) was more frequent in children who developed shock (p=0.004) (OR=6.5, 95% CI=1.4 to 31.9). However, it was not associated with bleeding from other sites in our patients [39 children had bleeding, of which five had TT positivity as the sole bleeding manifestation. So, among the 34 with frank bleeding, nine had positive TT (26.5%) and among the other 25 patients, five had positive TT (20%) (p value for no difference between these proportions = 0.56)].
Among the laboratory indices (Table 3), it was seen that patients who had platelet counts less than 50,000/cu.mm developed shock more frequently (p=0.01) (OR=6.5, 95% CI=1.4 to 31.9) and those with counts above 100,000/cu.mm developed shock less
frequently (p=0.01) (odds ratio could not be estimated). Raised values of blood urea and serum creatinine were found more frequently in those who developed shock (p=0.03) (OR=6.3, 95% CI=1 to 45). Patients who developed shock had a tendency to have higher haematocrit when compared to the other group but the difference was not statistically significant.
Bleeding was significantly related to severe thrombocytopenia (platelet counts below 50,000/cu.mm) (p=0.01) (OR=9.1, 95% CI=1.11 to 211). However, bleeding was not related to moderate thrombo-cytopenia (platelet counts between 50,000 and 100,000/cu.mm). Most of the patients who had bleeding had a decrease of haematocrit by >20% after treatment (p=0.01) (OR=9.1, 95% CI=1.11 to 211).

Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
112 Dengue Bulletin – Vol 27, 2003
Table 2. Comparison of clinical signs between children who developed complications and those who did not
S. No. Characteristic N With
shock§ Without shock§ P value* With bleed§ Without
bleed§ P value*
1 Total no. 59 13 46 - 39 20 - 2 Hepatomegaly 32 9 (69.2) 23 (50) 0.22 (x) 19 (48.7) 12 (60) 0.41 (x) 3 3rd space fluid 6 1 (7.7) 5 (10.9) 0.6 (f) 5 (12.8) 1 (5) 0.33 (f) 4 Lymph nodes 6 1 (7.7) 5 (10.9) 0.6 (f) 5 (12.8) 1 (5) 0.33 (f) 5 Conjunctival
suffusion 9 0 (0) 9 (19.6) 0.09 (f) 6 (15.4) 3 (15) 0.64 (f)
6 Bradycardia 6 2 (15.4) 4 (8.7) 0.39 (f) 4 (10.3) 2 (10) 0.67 (f) 7 Non bleeding rash 5 2 (15.4) 3 (6.5) 0.3 (f) 4 (10.3) 1 (5) 0.44 (f) 8 Positive
tourniquet test 14 7 (53.8) 7 (15.2) 0.004 (f)N 9/34 (26.5) 5/25 (20) 0.56 (x)
9 Shock 13 - - - 8 (20.5) 5 (25) 0.47 (f)
* The letter in parenthesis gives the statistical test employed in each case (t-student’s t-test; x-chi-squared test; f-Fisher’s exact test) N - Odds ratio with 95% confidence interval was calculated in these cases – see text § Figures in parenthesis represents percentage of cases
Table 3. Comparison of laboratory values between dengue cases with complications and those without
S. No. Characteristic N With
shock§ Without shock§ P-value* With
bleed§ Without bleed§ P-value*
1 Total no. 59 13 46 - 39 20 - 2 Hb% mean (s.d) - 11.1 (0.9) 10.7 (1.2) 0.28 (t) 10.8 (0.9) 10.8 (0.6) 1 (t) 3 Haematocrit mean (sd) - 34.4 (3.2) 32.9 (3.4) 0.15 (t) 32.3 (2.8) 32.2 (2.0) 0.83 (t) 4 Haematocrit fall >20%
on Rx - 4 (30.7) 10 (21.7) 0.38 (f) 13 (33.3) 1 (5) 0.01 (f)
5 PLCN <50,000 14 7 (53.8) 7 (15.2) 0.01 (f) 13 (33.3) 1 (5) 0.01 (f) 6 PLCN 50,000-100,000 29 6 (46.1) 23 (50) 0.83 (x) 16 (46.2) 13 (65) 0.08 (x) 7 PLCN >100,000 16 0 (0) 16 (34.8) 0.01 (f) 10 (28.2) 6 (25) 0.72 (x) 8 Raised ASTN 42 7/11 (63.7) 35 (76.1) 0.31 (f) 25/37 (67) 16 (80) 0.32 (x) 9 Raised ALTN 34 7/11 (63.7) 27 (58.7) 0.52 (f) 21/37 (57) 13 (65) 0.54 (x) 10 Raised SAPN 24 5/11 (45.5) 19 (41.3) 0.53 (f) 12/37 (32) 11 (55) 0.09 (x) 11 Albuminuria 20 6 (46.2) 14 (30.4) 0.23 (f) 12 (30.7) 8 (40) 0.47 (x) 12 Raised renal
parameters 7 4 (30.7) 3 (6.5) 0.03 (f) 4 (10.2) 3 (15) 0.44 (f)
* The letter inside parenthesis gives the statistical test employed in each case t-student’s t-test; x-chi-squared test; f-Fisher’s exact test § Figures in parenthesis represents percentage of cases PLC-platelet count per cu.mm. AST-Aspartate aminotransferase ALT-Alanine aminotransferase SAP-Serum alkaline phosphatase (in IU/L)

Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
Dengue Bulletin – Vol 27, 2003 113
The parameters found to be significantly different between the groups by univariate analysis were then subjected to multivariate analysis to exclude the effect of the other complication as eight patients were found to share both complications. The factors found related to shock were drowsiness (p=0.0002), positive tourniquet test (p=0.0004), low platelet count (p=0.005) and raised renal parameters (p=0.002). Less body pain was also associated with shock. However, the difference was not significant (p=0.07). Parameters related to bleeding manifest-ations were retro-orbital pain (p=0.006), more hepatomegaly (p=0.002) and low platelet count (p=0.045). Fall of haematocrit by more than 20% on fluid therapy was slightly more in the bleeding group (p=0.07).
Discussion There are many studies comparing the clinical features in DHF and DSS with classical DF. However there are few studies like the one done among Vietnamese children(6) comparing the clinical findings in children who develop complications like shock and haemorrhage without respect to strict WHO classification. This is important because there are many dengue cases who developed shock and haemorrhage without meeting all the WHO criteria for DHF/DSS(8), and these children are at equal risk of death as those who meet all the WHO criteria.
It is seen that children developing shock are in the younger age group but the difference is not statistically significant. Patients who developed shock had a significantly higher incidence of drowsiness. This has been noted before by Bethell et al(6).
This may be because of cerebral hypoperfusion. In our patients, we found body pain to be significantly less in the presence of shock. The low incidence of body pain in DHF as compared to DF is a very common finding included in the WHO manual(1), and it could be because these children were too drowsy to report any pain. However, Bethell et al(6) did not find any difference in the frequency of this symptom between children with or without shock. Moreover, on applying the multivariate analysis, the difference was not found to be significant at 5% level. Abdominal pain was not more common in our patients who developed shock, unlike the findings to the contrary in other studies(1,6).
On comparing the symptomatology of children with or without bleeding, retro-orbital pain being associated with bleeding is a new finding and has not been reported before. Bleeding in the loose connective tissue of the retro-orbital region leading to an increased intra-orbital pressure could be an initial, unnoticed bleeding manifestation in these patients and could contribute to the increased incidence of retro-orbital pain in the bleeders. No other symptom was found to be significantly different between those with bleeding manifestations and those without them.
Among the clinical signs, we noticed a higher proportion of tourniquet test positivity among children with shock. Association of shock with the presence of positive tourniquet test has been observed before(7). This also corroborates the finding by Bethell et al.(6) of the increased proportion of skin bleeding in patients with shock. No other signs analysed in our patients were found to be significantly associated with shock. The incidence of fluid leakage into the third

Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
114 Dengue Bulletin – Vol 27, 2003
space was also found to be equal between the two subgroups unlike the study done in Delhi(8), which had found this finding to be exclusive to those who had developed shock.
Children who had frank bleeding manifestations did not have a higher proportion of tourniquet test positivity unlike the findings by Wali et al.(9). Studies comparing DHF with classical DF report either a higher incidence of tourniquet test positivity in DHF as in Delhi(7) or Manila(10) or no difference between the two groups as in Thailand(4). These variable findings could be because the pathogenesis of tourniquet positivity and other bleeding manifestations in dengue cases are different and the defect which leads to increased capillary fragility could also predispose to the development of shock, which leads to a better correlation of the test to shock rather than to haemorrhage. Haemorrhagic manifestations were also associated with hepatomegaly.
Platelet counts were significantly lesser in patients who developed shock as noted by other authors(6). Bleeding has a correlation to
platelet count only when it is less than 50,000/cu.mm. The lack of correlation between moderately low platelet counts and bleeding manifestations has been noted in previous studies on dengue patients(11). Raised renal parameters also are associated with shock as in many other studies(8). However, there was no statistically significant difference in liver enzyme levels between patients with or without complications, which is contrary to previous studies(3,8,12).
Conclusion Thus, patients with dengue who are drowsy and have positive tourniquet test should be carefully watched for the development of shock and those who have retro-orbital pain should be monitored for development of bleeding manifestations. All suspected dengue cases with platelet count less than 50,000/cu.mm. should be hospitalized and observed as they have a high tendency to develop complications. However, more such studies are required with more patients so that these findings could be confirmed.
References 1. World Health Organization. Dengue haemorrhagic
fever: Diagnosis, treatment, prevention and control. 2nd edition. Geneva, 1997.
2. World Health Organization. WHO report on global surveillance of epidemic-prone infectious diseases. http://www.who.int/emc-documents/ surveillance/docs/whocdscsrisr2001.htm.
3. Wahid SF, Sanusi S, Zawawi MM and Ali R. A comparison of the pattern of liver involvement in dengue hemorrhagic fever with classic dengue fever. Southeast Asian J Trop Med Public Health, 2000, 31: 259-263.
4. Kalayanarooj S, Vaughn DW, Nimmannitya S, Green S, Suntayakorn S, Kunentrasai N, Viramitrachai W, Ratanachu-eke S, Kiatpolpoj S,
Innis BL, Rothman AL, Nisalak A and Ennis FA. Early clinical and laboratory indicators of acute dengue illness. J Infect Dis, 1997, 176: 313-321.
5. Vaughn DW, Nisalak A, Solomon T, Kalayanarooj S, Nguyen MD, Kneen R, Cuzzubbo A and Devine PL. Rapid serologic diagnosis of dengue virus infection using a commercial capture ELISA that distinguishes primary and secondary infections. Am J Trop Med Hyg, 1999, 60: 693-698.
6. Bethell DB, Gamble J, Loc PP, Dung NM, Chau TTH, Loan HT, Thuy TTN, Tam DTH, Gartside IB, White NJ and Day NPJ. Non-invasive measurement of microvascular leakage in patients with dengue hemorrhagic fever. Clin Infect Dis, 2001, 32: 243-253.

Dengue Fever – Clinical and Laboratory Parameters Associated with Complications
Dengue Bulletin – Vol 27, 2003 115
7. Kabra SK, Jain Y, Pandey RM, Madhulika, Singhal T, Tripathi P, Broor S, Seth P and Seth V. Dengue haemorrhagic fever in children in the 1996 Delhi epidemic. Trans R Soc Trop Med Hyg, 1996, 93: 294-298.
8. Srivastava VK, Suri S, Bhasin A, Srivastava L and Bharadwaj M. An epidemic of dengue haemorrhagic fever and dengue shock syndrome in Delhi: A clinical study. Ann Trop Paediatr, 1990, 10: 329-334.
9. Wali JP, Biswas A, Aggarwal P, Wig N and Handa R. Validity of tourniquet test in dengue haemorrhagic fever. J Assoc Physicians India, 1999, 47: 203-204.
10. Hayes CG, Manaloto CR, Gonzales A and Ranoa CP. Dengue infections in the Philippines: Clinical and virological findings in 517 hospitalized patients. Am J Trop Med Hyg, 1988, 39: 110-116.
11. Gomber S, Ramachandran VG, Kumar S, Agarwal KN, Gupta P, Gupta P and Dewan DK Hematological observations as diagnostic markers in dengue hemorrhagic fever – A reappraisal. Indian Pediatr, 2001, 38: 477-481.
12. Kuo CH, Tai DI, Chang-Chien CS, Lan CK, Chiou SS and Liaw YF. Liver biochemical tests and dengue fever. Am J Trop Med Hyg, 1992, 47: 265-270.

116 Dengue Bulletin – Vol 27, 2003
Dengue Fever: Its Laboratory Diagnosis, with Special Emphasis on IgM Detection
by N Sathish, T S Vijayakumar, P Abraham and G Sridharan#
Department of Clinical Virology, Christian Medical College, Vellore-632 004, India
Abstract
Rapid diagnosis of dengue is crucial for proper patient care. As IgM antibody appears early during the disease course, its detection is a valuable tool for rapid diagnosis.
We evaluated and compared two commercial tests, the PanBio Rapid Immunochromatographic Card Test (Brisbane, Australia) and the PanBio Microwell IgM ELISA with an IgM Capture ELISA (National Institute of Virology, Pune, India). A total of 154 samples from individuals with febrile illness having dengue fever (DF)-like symptoms were tested.
The NIV IgM Capture ELISA (MAC-ELISA) showed a high positivity rate (38.9%) as compared to the PanBio Rapid (22.7%) and the PanBio IgM ELISA (20.7%). The NIV MAC-ELISA showed a high sensitivity (96%) as compared to PanBio Rapid (73%) and PanBio IgM ELISA (72%). But the specificity was low (81%) when compared to PanBio Rapid (95%) and PanBio IgM ELISA (97%) using the latent class analysis model.
The MAC-ELISA, though a three-day procedure, should be a valuable screening test because of its high sensitivity rates. But rapidity gets compromised, as batch testing is required along with technical difficulty in performance. The “Rapid” test is an easier option in small peripheral laboratories in India because of its obvious advantages.
Keywords: Dengue, IgM detection, NIV IgM capture ELISA, PanBio Rapid Immunochromatographic Card Test, PanBio Microwell IgM ELISA.
# For correspondence: [email protected]
Introduction Early symptoms of dengue fever (DF) mimic other diseases often prevalent in areas where it is endemic, such as malaria and leptospirosis(1). Thus, a rapid differential diagnosis is crucial for proper patient care.
The most straightforward diagnosis of a recent infection is achieved by the detection of the virus in the patient’s blood, either by virus isolation in susceptible cell cultures(2) or by identifying the viral RNA with PCR techniques(3,4). But these methods are laborious and also require specialized
Serological Diagnosis of Dengue Fever with IgM Detection
Dengue Bulletin – Vol 27, 2003 117
laboratory facilities. In addition, it has been shown that the level of the circulating virus wanes as the antibodies become detectable and so these procedures are successful only when done within a few days of the onset of illness(5).
General methodological issues The isolation of dengue viruses is usually carried out by inoculation into either 1-3-day-old mice, mammalian cell cultures, mosquito cell cultures or by intrathoracic inoculation of adult mosquitoes(6). Inoculation into suckling mice, previously carried out in our laboratory, was seen to require numerous passages to adapt the viruses to replicate in mice. Mammalian cell cultures have many of the demerits associated with suckling mice and are also not recommended(6).
Mosquito inoculation, though the most sensitive method for dengue virus isolation, has its associated demerits that include labour-intensiveness and requirement of an insectary to produce large numbers of mosquitoes for inoculation(6).
For the serological diagnosis of dengue, traditionally in the past, the HI assay has been the most widely used method(2). However, the variable potency of haemagglutinins made in different laboratories(5), the extensive cross-reaction encountered and the non-availability of results within a short period of time due to the requirement of both acute and convalescent sera collected at least seven days apart, have compromised the general applicability of this assay in the diagnosis of dengue fever. Extensive cross-reactivity among the viruses posing a problem in HI
was encountered in our laboratory also(7). The Compliment Fixation Test (CFT), another serological method of diagnosis, is not widely used currently for routine diagnostic testing. The major demerits of this test include difficulty in the performance of the test and the requirement of highly trained personnel(6). As for HI, cross-reactivity among the viruses was a problem encountered in our laboratory(8). It was observed that CFT titers to other arboviruses was equal to and sometimes even higher than the agent involved and more often these heterologous titers were noted with Japanese encephalitis (JE) and (West Nile) WN antigens.
The neutralization test, though the most specific and sensitive serological test for dengue infections, also has major demerits. The turnaround time of the test, coupled with technical difficulty, have led to this test being less routinely employed(6).
The most challenging problem associated with patient management in dengue infection is rapid diagnosis. Due to the aforesaid disadvantages of the various tests, they cannot be made use of for a rapid diagnosis of dengue fever. In this respect, commercially available ELISAs offer improvements over the HI assay for the serological diagnosis of dengue infections. Unlike HI assays, pre-treatment of sera is not required, and a diagnosis can be made from a single sample. Differentiation between primary and secondary infections may also be made with a single dilution of serum rather than with a series of dilutions.
As IgM antibody appears early during the disease course, and as a diagnosis can be made from a single serum sample, detection of IgM antibody seems to be a valuable tool

Serological Diagnosis of Dengue Fever with IgM Detection
118 Dengue Bulletin – Vol 27, 2003
for the rapid diagnosis of acute viral infection.
Previously in our laboratory, from the middle of 1996 to the end of 1999, the dengue IgM blot (Genelabs Diagnostics), a qualitative enzyme immunoblot assay, was used for the detection of dengue IgM antibodies. This test was not very rapid and involved a series of incubation steps with addition of various reagents after the incubation steps. Even the shortened version of the original protocol (a two-day procedure, with overnight incubation in between) was a day-long procedure. As it was a long procedure, only batch testing of samples could be performed. All these samples were later confirmed by the NIV MAC-ELISA. For detection of dengue IgG antibodies, a separate dengue IgG blot was available. Since 1999, the blot assays were replaced by the PanBio Rapid Immunochromatographic Card test which was quick to perform and both dengue IgM and IgG responses could be detected using a single card.
Specific methodology In a more recent study carried out in our department of Clinical Virlology, three tests employed for the detection of dengue IgM antibody from serum samples, the PanBio Rapid Immunochromatographic Card Test (Brisbane, Australia), the PanBio INDXRIVDTM Microwell ELISA for IgM only (Baltimore, USA), and the IgM antibody Capture ELISA (MAC-ELISA) (National Institute of Virology, Pune, India) were compared.
Serum samples were received at our department from 154 patients with DF-like febrile illnesses attending the Paediatric and
Medicine clinics of the Christian Medical College, Vellore, India, during June 2000-September 2000. The clinical basis for diagnosing the patients as having dengue fever was based on standard criteria like presentation of febrile illness of 2-7 days’ duration, with features like headache, myalgia, arthralgia, rash, haemorrhagic manifestation and leucopenia. Clinical information about the stage of the disease at which sampling was done was unavailable for most samples, and hence not taken into account.
PanBio Rapid Immuno-chromatographic Card Test
This is a rapid (<10 minutes) immuno-chromatographic test for the detection of both dengue specific IgM and IgG in a test-card format. Anti-dengue virus IgM and IgG antibodies in the test sample (30µl of undiluted serum per test) were detected simultaneously on the same card by using an antibody capture format with a cocktail of all the four dengue virus serotypes. The test is considered positive for primary dengue virus infection if two purple/pink lines (IgM and Control) are seen in the viewing window after five minutes(9). This test format has been earlier described by others(9). In this study, we were primarily interested in the IgM antibody results for comparison with the other two tests.
PanBio INDXRIVDTM Microwell ELISA (IgM only)
In the PanBio Microwell ELISA kit, wells were coated with purified dengue virus type 2 antigen cultured in Vero cells. The test was performed according to the manufacturer’s instructions.

Serological Diagnosis of Dengue Fever with IgM Detection
Dengue Bulletin – Vol 27, 2003 119
Samples were considered negative if the optical density (OD) values were in the range 0.0-0.3 OD units, weak positive if in the range 0.5-1.0 OD, and positive if >1.0 OD. Samples were interpreted as indeterminate if the OD values were in the range 0.3-0.5 units.
IgM Antibody Capture ELISA (MAC-ELISA) (NIV, Pune, India)
The test is designed to detect IgM antibodies to any one or three of the flaviviruses prevalent in India (DEN-2, JE and West Nile). The procedure starting with the coating of anti-IgM was performed according to the protocol provided. For each test sample the number of antibody units was calculated based on the formula:
OD (Test) – OD (NC)* OD (Weak PC)** – OD (NC)
X 100
*NC: Negative Control **Weak PC: Weak Positive Control
The test sample was considered positive for IgM antibody against that particular antigen if the antibody units were =50; if <50 the sample was considered negative.
Statistical analysis
As there was no gold standard among the three tests done, the accuracy of the tests was assessed through “Latent Class Models”(10,11,12). The true prevalence, sensitivity and specificity of the three tests were estimated using 2LC latent class model using expectation-maximization algorithm. The analysis was done using Latent software version 3.0 (Courtesy Dr SD Walter, McMaster University, Canada). As the conservative, asymptotic Gausian confidence
interval has the overshooting aberration when the parameter estimates are at or near the maximum and minimum values (1 or 0), the Wilson ‘score’ method(13) with continuity correction was employed to obtain the 95% confidence intervals.
Results Of the 154 serum samples tested, 60(38.9%) were positive by the MAC-ELISA (NIV, Pune, India) while 35(22.7%) were positive by the PanBio Rapid Immunochromatographic card test, and 32 (20.7%, excluding 15 indeterminate results) were found positive by the PanBio Microwell IgM ELISA. The number of samples positive in a single or in a combination of tests is shown in Table 1.
Table 1. Reactivity patterns of 154 samples in the three dengue IgM assays
Positive status category
No. of samples positive
Percentage positivity
NIV IgM Capture only 23 14.9
PanBio rapid only 5 3.2
PanBio ELISA only 3 1.9
Three methods (NIV, PanBio Rapid & ELISA)
20 12.9
NIV IgM Capture & PanBio Rapid 9 5.8
NIV IgM Capture & PanBio ELISA 8 5.2
PanBio Rapid & PanBio ELISA 1 0.6

Serological Diagnosis of Dengue Fever with IgM Detection
120 Dengue Bulletin – Vol 27, 2003
The estimated prevalence of dengue in the study population was 25%. The sensitivity and specificity of the three tests computed using 2LC Latent class model are presented in Table 2. The estimated sensitivity was 96% in the NIV MAC-ELISA, while it was 73% and 72% in PanBio Rapid and PanBio ELISA respectively. However, the PanBio Rapid and the PanBio ELISA tests had a high specificity as compared to the NIV MAC-ELISA. The difference in sensitivity and specificity amongst the three tests was found to be significant.
Table 2. Prevalence, sensitivity, specificity and their 95% confidence intervals (CI) of three tests using 2LC Latent Class model
Tests Prevalence (95%CI)*
Sensitivity (95%CI)*
Specificity (95%CI)*
NIV MAC-ELISA
0.96 (0.91, 0.98)
0.81 (0.74, 0.87)
PanBio Rapid
0.25 (0.19, 0.33)
0.73 (0.65, 0.80)
0.95 (0.90, 0.98)
PanBio ELISA
0.72 (0.64, 0.78)
0.97 (0.92, 0.99)
*95% CI Wilson ‘score’ method with continuity correction was used.
Difference in sensitivity of NIV MAC-ELISA in comparison to PanBio Rapid and PanBio ELISA was statistically significant (p<0.001).
Difference in specificity of NIV MAC-ELISA in comparison to PanBio Rapid and PanBio ELISA was statistically significant (p<0.001).
A total of 68 samples (of the original 154) were analysed by the NIV MAC-ELISA format for IgM antibodies additionally to two other flaviviruses (JE and WN). The total number of samples which were positive for IgM antibodies to one, two or all three flaviviruses is shown in Table 3 along with the findings in the PanBio Rapid and PanBio
ELISA on those samples. (The first 68 samples were chosen based on the NIV MAC-ELISA kit availability). This was based on the known cross-reactivity among the flaviviruses, expecting 30-70% of the sera to show heterologous cross-reactivity. Investigation of this phenomenon needs a sample size of 30 positives (confidence level 99.9%). In the 68 samples tested for the three agents, there were 31 positive samples, thus this panel was found to be sufficient to examine for heterologous reactivity.
Table 3. Positivity in the PanBio Rapid and PanBio ELISA tests on serum samples
categorized on the basis of flavivirus reactivity in the IgM Capture ELISA (NIV MAC-ELISA)
Positive category by NIV IgM MAC-
ELISA (n)
No. positive by PanBio
Rapid Dengue IgM n (%)*
No. positive by PanBio
Dengue IgM ELISA n (%)*
Dengue only (8) 2 (25.0) 2 (25.0)
Dengue and JE IgM (10)
1 (10.0) Nil
Dengue and WN IgM (4)
2 (50.0) 2 (50.0)
Dengue, JE and WN IgM (7)
5 (71.4) 5 (71.4)
JE and WN IgM (2) 1 (50.0) Nil
* row percentages JE: Japanese B encephalitis, WN: West Nile
Discussion A rapid and accurate method for the diagnosis of dengue fever is important for proper patient management, keeping in view the complications and fatality rate associated with it. Several studies have compared and

Serological Diagnosis of Dengue Fever with IgM Detection
Dengue Bulletin – Vol 27, 2003 121
evaluated the different serological tests available for the diagnosis of dengue viral infection.
The PanBio Rapid Immuno-chromatographic card test, following its introduction, has been evaluated in two separate studies(9,14). In the first study(9), it was seen that the test demonstrated 100% sensitivity in the diagnosis of dengue viral infection and was able to distinguish between primary and secondary dengue virus infections through separate determinations of IgM and IgG. It was seen that cross-reactivity with JE was only a concern for a small proportion of the patients with secondary dengue infections. In the other study(14), it was seen that, of the total number of patients with primary infection, 88% were IgM positive and IgG negative while, of the total number with secondary infection, 97% were IgG positive with or without IgM. Both the studies, alluded to the finding that the rapid test could be a useful aid in rapid diagnosis of dengue viral infection.
This rapid test seemed to have definitive advantages over the previously available Blot tests in the market, in that no pre-treatment of sera to remove competing IgG or rheumatoid factor was required. Preparation and dilution of reagents along with multiple incubation steps as in Blots could be avoided.
PanBio has also marketed the PanBio Dengue Duo ELISA, which is a capture ELISA format for the detection of IgM and IgG in two separate assays. A study which evaluated this assay(15) revealed that the ELISA was able to diagnose significantly more cases of dengue than the HI assay (55% versus 14%)
through the use of the first serum sample alone. The results of the IgG Capture ELISA gave a significant correlation with those of the HI assay and it could be used to distinguish primary from secondary dengue infection. One demerit of the PanBio Dengue Duo ELISA was the need to run two separate assays (for IgM and IgG), thereby preventing laboratories from using this due to financial constraints.
To overcome this disadvantage, screening ELISAs were introduced by PanBio, wherein both anti-human IgG and anti-human IgM were applied as a coating to the same assay wells. The level of the anti-human IgG applied as a coating to the well was set to detect high levels of IgG characteristic of secondary dengue infections alone. A study(16), which evaluated this kit, found a sensitivity of 95% and a specificity of 94% in primary and secondary dengue.
In a study(17), comparing two commercially available IgM capture ELISAs (MRL Den Fever Virus IgM Capture ELISA and PanBio Duo ELISA), it was seen that both these performed well, taking into consideration both sensitivity and specificity.
In another study(18), comparing six immunoassays for the detection of dengue IgM and IgG antibodies, the authors arrived at the conclusion that the PanBio Rapid Immunochromatographic test (RIT) was the simplest and the fastest assay to perform. It was seen that the best complete dengue IgM and IgG detection system was the PanBio ELISA. If separate assays were to be performed, a combination of PanBio RIT for IgM detection and PanBio IgG ELISA was found to be the most sensitive and specific combination.

Serological Diagnosis of Dengue Fever with IgM Detection
122 Dengue Bulletin – Vol 27, 2003
In the light of all these studies, we chose to compare three tests useful in the diagnosis of dengue viral infection. In our study, the PanBio Rapid Immuno-chromatographic Card test did not show a good correlation with the NIV IgM Capture ELISA format. Though the sensitivity of this test was found to be low in comparison to the NIV IgM Capture ELISA, it had other advantages. It is a simple and a rapid test that can be performed in five minutes, does not require highly trained personnel or sophisticated equipment such as in field situations thus, enabling its performance even in areas lacking extensive laboratory facilities. Due to the use of standardized reagents for the test, inter-laboratory variation stands reduced. The “Rapid” test is also capable of detecting antibodies to all the four dengue virus types, as the antigen employed for the test is a cocktail of all the four serotypes, enabling its use in any geographical location. The test gives information about both the dengue IgM and IgG responses.
The IgG response detected with this test is set to detect high levels of IgG (HI Titer-1:2560), thus indicative of a secondary infection and just not residual antibodies from a previous infection. Thus, the IgG response detectable by this assay may be helpful for clinicians in diagnosing a susceptibility to DHF, and hence can be used as an initial screening test. This kit also has an extended shelf-life of approximately a year when stored at 40C.
In comparison to IgM-detecting ELISAs, which require testing of samples in batch formats, the “Rapid” test can be performed as and when samples are received in the
laboratory. This might specially prove useful in epidemic situations and in post-monsoon months where many samples are expected to be received in the laboratory, thereby ensuring rapidity in giving the results.
The PanBio Rapid Immuno-chromatographic Card test has now been replaced by a Rapid Immuno-chromatographic Strip test, which is essentially based on the same principle as above, except that the card is replaced by a strip. This is presently being used in our laboratory.
The PanBio Microwell IgM ELISA can be modified according to the manufacturer’s instructions for the detection of total Ig (IgM and IgG, by avoiding treatment with anti-human IgG) against dengue, but this might not provide useful information, as it merely gives an indication about the antibody response with no differentiation. As the current study focused only on IgM detection, the samples were treated with anti-human IgG supplied with the kit, and carried through the assay. The test, being an ELISA, requires batch testing; thereby rapidity stands compromised. As the microtiter wells are coated with DEN-2 antigen, it cannot be guaranteed that the serotypes of dengue virus other than DEN-2 will be detected with equal efficiency, though cross-reaction exists among the four dengue serotypes. Also, for some samples, the kit gives indeterminate results from which a definitive diagnosis cannot be reached. The protocol requires an ELISA reader for the measurement of OD values, thereby compromising the utility of this test in remote peripheral laboratories in developing countries.

Serological Diagnosis of Dengue Fever with IgM Detection
Dengue Bulletin – Vol 27, 2003 123
The PanBio Duo ELISA, which has not been evaluated in this study, is an IgM Capture ELISA. This overcomes most of the demerits of the former. Also as in the Rapid test, a cocktail of all the four dengue virus serotypes is used as the antigen. This test seems to account for rapidity as it is a two-hour ELISA and at the same time is a much superior version to the former. Unlike the Rapid strip test which is a qualitative test, this assay gives the result as IgM antibody units. The PanBio IgG ELISA, which can be concomitantly performed along with the Dengue IgM Capture ELISA, gives the IgG response as IgG PanBio units obtained could be used to distinguish between primary and secondary dengue.
In case of the NIV MAC-ELISA, the superiority of this test over the other two tests is clearly brought out by its very high sensitivity (96%). The specificity is also relatively high. The capture format of the MAC-ELISA, coupled with the use of dengue virus-specific antigen, eliminates potential background caused by extraneous antibody, resulting in less frequent non-specific reactions and also removing false positive reactions caused by the rheumatoid factor. Also, the use of biotinylated antiviral antibody and avidin HRP conjugate seems to increase the sensitivity of this test which might have contributed to the high positivity seen in the study. Additionally, by this test, IgM antibody against all the three commonly encountered flaviviruses (dengue, JE, West Nile viruses) can be detected using the specific viral antigens in a single run, and it also has the advantage in that, depending on the strength of the antibody units obtained to a particular flaviviral antigen, presumptive diagnosis of a particular arboviral infection
can be made in conjunction with clinical presentation.
An additional advantage of the NIV-MAC ELISA test is that it allows testing of CSF samples in contrast to the PanBio tests.
In spite of its high sensitivity, the MAC-ELISA requires batch testing of samples and is a three-day procedure, thereby compromising on rapidity in giving the results. Such an assay requires trained personnel to carry out the test, and cannot be easily carried out in small laboratories, as a certain amount of infrastructure is needed. As only dengue virus DEN-2-specific antigen is employed, as in the former test, there exists a possibility where infection with other serotypes might not be efficiently picked up. This might account for some samples being positive by the “Rapid” test but negative by the MAC-ELISA.
Taking into account the aforesaid advantages of the NIV IgM Capture ELISA, coupled with its very high sensitivity, this assay should be a valuable screening test for the diagnosis of DF in routine diagnostic laboratories despite being a three-day procedure. Hence, even if samples can be tested by “Rapid” tests due to their rapidity in giving results, they are to be confirmed by the IgM Capture ELISA, as it gives information on the IgM antibody status not only to dengue virus, but also to JE and WN, using the specific viral antigens in separate assays. This might prove to be very useful in geographical locations where all the three flaviviruses are prevalent, facilitating generation of useful epidemiological data.
Thus, while the “Rapid” test can be more feasible in small peripheral laboratories

Serological Diagnosis of Dengue Fever with IgM Detection
124 Dengue Bulletin – Vol 27, 2003
and in field situations, in well-established laboratories in India, the concomitant performance of the “Rapid” test, with confirmation by the MAC-ELISA on those samples, ensures both rapidity as well as quality of reported results.
As dengue IgM antibody appears quite early in the course of illness, and its detection requires only a single, properly-timed blood sample with the testing procedure being relatively easy, compared to other classical methods of diagnosing dengue infections, detection of dengue IgM antibody seems to be a better option. Of more importance is the fact that IgM responses are usually less virus cross-reactive. Depending upon the status and facilities available in a laboratory, dengue IgM detection by any of
the tests mentioned above can turn out to be an easier and more reliable option for diagnosing dengue viral infections that can ultimately result in appropriate patient management and effective control measures, thereby preventing outbreaks and reducing the associated case fatality.
Whichever the test, the complexity of flavivirus diagnosis cannot be disregarded, showing thereby that a single assay alone cannot be totally relied upon. Thus, a diagnosis of a particular flavivirus should always be made taking into account the clinical presentation of the patient, the performance characteristics of the serological test employed and the knowledge of the flaviviruses circulating in that particular geographical region.
References
1. Monath TP and Tsai TF. Flaviviruses In: Richman DD, Whitley RJ, Hayden FG (Eds.). Clinical Virology, New York Churchill Livingstone Inc, 1997: 1133-1186.
2. Henchal EA and Putnak JR. The dengue viruses. Clinical Microbiology Reviews, 1990, 3: 376-396.
3. Lanciotti RS, Calisher CH, Gubler DJ, Chang GJ and Vorndam AV. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. Journal of Clinical Microbiology, 1992, 30: 545-551.
4. Henchal EA, Polo SL, Vorndnam V, Yaemsiri C, Innis BL and Hoke CH. Sensitivity and specificity of a universal primer set for the rapid diagnosis of dengue virus infections by polymerase chain reaction and nucleic acid hybridization. American Journal of Tropical Medicine and Hygiene, 1991, 45: 418-428.
5. Innis BL, Nisilak A, Nimmannitya S, Kusalerdchariya S, Chongswadi V, Suntayakorn S,
Puttisri P and Hoke CH. An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese encephalitis co-circulate. American Journal of Tropical Medicine and Hygiene, 1989, 40: 418-427.
6. Gubler DJ. Dengue and dengue haemorrhagic fever. Clinical Microbioogy Reviews, 1998, 11: 480-496.
7. Myers RM, Carey DE, Rodrigues FM and Klontz CE. The isolation of dengue type 4 virus from human sera in south India. Indian Journal of Medical Research, 1964, 52: 559-565.
8. Carey DE, Myers RM, Reben R and Rodrigues FM. Studies on dengue in Vellore, south India. American Journal of Tropical Medicine and Hygiene, 1966, 15: 580-587.
9. Vaughn DW, Nisilak A, Kalayanarooj S, Solomon T, Dung NM, Cuzzubbo A and Devine PL. Evaluation of a rapid immunochromatographic test for diagnosis of dengue virus infection. Journal of Clinical Microbiology, 1998, 36: 234-238.

Serological Diagnosis of Dengue Fever with IgM Detection
Dengue Bulletin – Vol 27, 2003 125
10. Walter SD and Irwig LM. Estimation of test error rates, disease prevalence and relative risk from misclassified data: A review. Journal of Clinical Epidemiology, 1988, 41: 923-937.
11. Qu Y, Tan M and Kutner MH. Random effect models in latent class analysis for evaluating accuracy of diagnostic tests. Biometrics, 1996, 52: 797-810.
12. Rindskopf D and Rindskopf W. The value of latent class analysis in medical diagnosis. Statistics in Medicine, 1986, 5: 21-27.
13. Newcombe RG. Two-sided confidence intervals for the single proportion: Comparison of seven methods. Statistics in Medicine, 1998, 17: 857-872.
14. Sang CT, Hoon LS, Cuzzubbo A and Devine P. Clinical evaluation of a rapid immunochromatographic test for the diagnosis of dengue virus infection. Clin Diagn Lab Immunol, 1998, 5: 407-409.
15. Sang CT, Cuzzubbo AJ and Devine PL. Evaluation of a commercial enzyme-linked immunosorbent assay for detection of immunoglobulin M and G antibodies produced during dengue infection. Clin Diagn Lab Immunol, 1998, 5: 7-10.
16. Lam SK, Ew CL, Mitchell JL, Cuzzubbo AJ and Devine PL. Evaluation of a capture screening enzyme-linked immunosorbent assay for combined determination of immunoglobulin M and G antibodies produced during dengue infection. Clin Diagn Lab Immunol, 2000, 7: 850-852.
17. Cuzzubbo AJ, Vaughn DW, Nisalak A, Solomon T, Kalyanarooj S, Aaskov J, Dung NM and Devine PL. Comparison of PanBio Dengue Duo enzyme-linked immunosorbent assay (ELISA) and MRL Dengue Fever virus immunoglobulin M capture ELISA for diagnosis of dengue virus infections in Southeast Asia. Clin Diagn Lab Immunol, 1999, 6: 705-712.
18. Groen J, Koraka P, Velzing J, Copra C and Osterhaus AD. Evaluation of six immunoassays for detection of dengue virus-specific immunoglobulin M and G antibodies. Clin Diagn Lab Immunol, 2000, 7: 867-871.

126 Dengue Bulletin – Vol 27, 2003
Dengue – The Underestimated Risk in Travellers
by O Wichmann#, N Mühlberger and T Jelinek
Institute of Tropical Medicine, Humboldt University Berlin, Spandauer Damm 130, 14050 Berlin, Germany
Abstract
In recent decades, the incidence, distribution and clinical severity of dengue have increased dramatically in most tropical and subtropical areas worldwide. As a consequence, and due to the expanding international tourism, health care providers in European travel clinics are more and more confronted with dengue, reflecting its global impact.
Based on data of the European Network on Imported Infectious Disease Surveillance (TropNetEurop) and the German Surveillance Network on Imported Infectious Diseases (SIMPID), a total of 483 confirmed and probable cases of dengue fever, including 13 cases of dengue haemorrhagic fever were reported to the networks’ coordination centre between January 1999 and December 2002. There was a wide range of epidemiological and clinical features. Non-European travellers (immigrants or foreign visitors) were at 4.3-times higher risk of developing dengue haemorrhagic fever compared to European travellers. Infections were acquired in all endemic regions of the world, with highest frequencies in South-East Asian countries.
Persons travelling to areas where dengue is endemic should avoid exposure to mosquitoes, and health care providers should consider dengue as a differential diagnosis in febrile travellers returning from the tropics after discounting malaria. Surveillance of imported dengue is crucial to monitor the risk of infection for travellers and to strengthen clinical awareness of the disease.
Keywords: Dengue fever, dengue haemorrhagic fever, traveller, Europe.
# For correspondence: [email protected]
Introduction Dengue viruses are members of the Flaviviridae and are usually transmitted by the bites of an infected mosquito vector. Four groups of serologically distinct dengue viruses are currently recognized (DEN-1 to 4). Generally, man is the primary vertebrate
host and Aedes mosquito is the primary vector of infection(1,2).
Dengue occurs principally in the tropical areas of Asia, Oceania, Africa and the Americas. In the past 30 years, there has been a dramatic emergence of epidemic dengue activity in the tropics worldwide(3,4).

Dengue – The Underestimated Risk in Travellers
Dengue Bulletin – Vol 27, 2003 127
An estimated 2.5 billion people are living at risk of dengue infection, resulting annually in an estimated 50 to 100 million cases of dengue fever (DF) and 250,000 to 500,000 cases of its more severe manifestation, dengue haemorrhagic fever (DHF)(5,6). In South-East Asia, the mean number of annual cases of dengue haemorrhagic fever has increased from below 10,000 in the 1950s and 1960s to over 200,000 in the 1990s. The same pattern is now unfolding in the Americas(3,6). At the root of the emergence of dengue are changes in human demography and behaviour, leading to unchecked populations of and increased exposure to the principal domestic mosquito vector(7).
Another factor, which has had a great impact on the emergence of DF/DHF, is the increased air-travel of humans who are incubating the viruses and thus providing ideal mechanisms for transporting pathogens between population centres of the tropics(3). Therefore, travellers not only have the potential to acquire a dengue infection, but also to spread new and potentially more virulent strains to different parts of the world. One major factor for the increased air-travel is expanding international tourism: in 2002, the number of international tourists, for the first time in history, exceeded the 700 million mark. The preliminary statistics of the World Tourism Organization showed that in that year, more than 130 million international tourist arrivals were registered in Asia and the Pacific, which many regard as the destination of the future, and 120 million in the Americas(8). Therefore, not surprisingly, supported by higher awareness of physicians in travel clinics and better surveillance systems, reports on dengue infections in travellers became more
frequent(9). Several studies revealed dengue as the second most common tropical disease after malaria causing fever in returned travellers(10,11,12).
This article reviews the current situation – epidemiology, risk and clinical manifestations – of dengue in European travellers in the setting of the global emergence of the disease based on data provided by the European Network on Imported Infectious Disease Surveillance (TropNetEurop) and the German Surveillance Network (SIMPID).
Surveillance of dengue in Europe Dengue fever is currently not reported in most European public health systems. Our knowledge about the incidence and risk of dengue in travellers is based on a small number of systematic studies.
The European Network on Imported Infectious Disease Surveillance (TropNetEurop) was founded in 1999 in order to detect emerging infections of potential regional, national or global impact at their point of entry into the European population. From the very beginning, dengue has been a disease of concern to the network. This has recently resulted in a publication elsewhere(13). Briefly, TropNetEurop is the largest network for the surveillance of travel-acquired diseases worldwide and currently consists of 47 clinical member-sites in most West and Central European countries(14). Although the organization does not guarantee that collected data will be representative for Europe, most major referral centres of the
Dengue – The Underestimated Risk in Travellers
128 Dengue Bulletin – Vol 27, 2003
continent are represented and cover approximately 63,000 patients post-travel and 220,000 pre-travel advices annually. The data on which this article is based were collected by single member sites and submitted by standardized questionnaires to the TropNetEurop coordination centre. The present analysis includes cases of dengue infections reported from January 1999 through December 2002.
For a broader overview, we also included data of SIMPID, a similarly designed national surveillance network in Germany for imported infectious diseases. The network is linked to TropNetEurop and currently consists of 51 participating member sites. Data have been collected within this network since May 2001.
Case reports from both networks name the most accurate diagnostic procedure applied to derive the diagnosis, which was used to distinguish “suspected”, “probable” and “confirmed” dengue infections according to the WHO classifications(15). For a diagnosis of “confirmed” dengue, the virus was detected by viral isolation, PCR, or a fourfold or greater change in reciprocal IgM or IgG antibody titres in paired serum samples. The “probable” diagnosis of dengue was supported by a single positive IgM antibody test on a late acute or convalescent-phase serum specimen only. A variety of test kits were used by the reporting centres, all of which are established and widely used assays. “Suspected” cases lacked supportive serology, and diagnosis was based entirely on clinical features and travel history. In the following analysis, only cases of confirmed or probable dengue infection were included.
Epidemiology of dengue in travellers
Between January 1999 and December 2002, an overall 562 cases with a diagnosis of dengue or dengue haemorrhagic fever were reported to the TropNetEurop and SIMPID coordination centre, of which 483 (86%) were assigned either as laboratory-confirmed (n=411) or as probable (n=72). The total number of the annually reported dengue cases in these two networks increased from 39 cases in 1999 to 208 cases in 2002. However, the increase has to be attributed primarily to the increased number of reporting sites of the networks rather than to an increased incidence of dengue infections in travellers.
Figure 1 shows the frequencies of dengue cases reported per month between January 1999 and December 2002. Besides the increase of total numbers of dengue cases, we noted a peak of 38 cases in April 2002. During this month, 70% of all cases were imported from Thailand.
Travel history within two weeks before illness was available in most of the patients. Figure 2 and Table 1 demonstrate frequencies and percentages of imported dengue cases per country or region where the infection had been acquired. A high percentage of dengue cases (45%) was acquired by patients who travelled to countries in South-East Asia, 91 cases (19%) were imported from the South and Central America, 77 cases (16%) from the Indian subcontinent, 56 cases (12%) from the Caribbean and 38 cases (8%) from Africa.

Dengue – The Underestimated Risk in Travellers
Dengue Bulletin – Vol 27, 2003 129
Figure 1. Dengue-infections reported within the networks of TropNetEurop and SIMPID between January 1999 and December 2002 (n = 483)
0
5
10
15
20
25
30
35
40
Jan
99Fe
b 99
Mar
99
Apr 9
9M
ay99
Jun
99Ju
l 99
Aug
99Se
p 99
Oct
99
Nov
99D
ec 9
9Ja
n 00
Feb
00M
ar 0
0Ap
r 00
May
00Ju
n 00
Jul 0
0Au
g 00
Sep
00O
ct 0
0N
ov00
Dec
00
Jan
01Fe
b 01
Mar
01
Apr 0
1M
ay01
Jun
01Ju
l 01
Aug
01Se
p 01
Oct
01
Nov
01D
ec 0
1Ja
n 02
Feb
02M
ar 0
2Ap
r 02
May
02Ju
n 02
Jul 0
2Au
g 02
Sep
02O
ct 0
2N
ov02
Dec
02
Month of presentation
N
< 2% 2-4% 4-6% 6-8% 8-10% > 10% Countries by % of total
Dengue 1999/2002 (N=465)
Figure 2. Countries in which travellers acquired dengue infection by percentage of total (n = 465) reported cases

Dengue – The Underestimated Risk in Travellers
130 Dengue Bulletin – Vol 27, 2003
Table 1. Frequencies of travel-acquired dengue infections by region of travelling
(n = 481)
Region of infection No. of
patients (%)
Africa 38 (8)
South/Central America 91 (19)
The Caribbean 56 (12)
Indian subcontinent 77 (16)
South-East Asia and Oceania
219 (45)
This distribution mainly reflects the global dengue activity which is known to be the highest in South-East Asia, followed by the Americas and the Caribbean islands. The surveillance for dengue in Africa is poor. Therefore, the fact that 8% of all dengue infections are reported in travellers returning from Africa underlines the need that dengue should also be included as a differential diagnosis for fever in travellers returning from this continent.
Furthermore, this distribution also reflects the popularity of the countries as a tourist destination. Thailand, Viet Nam and Indonesia are not only high-endemic areas of dengue viruses, but also the countries with an expanding tourism sector. Thailand alone was responsible for 134 cases (28%) of all travel-acquired dengue infections over the past four years in our networks. In contrast, the surprising decrease of reported dengue infections in travellers returning from India (from 18% in 2001 to 4% in 2002) might reflect, in addition to other factors (such as low epidemicity), its decreased popularity as a tourist destination, as there was a 6.6% decrease in international tourist arrivals reported by the World Tourism Organization for India in 2002(8).
Overall, many confounding factors will have an influence on the epidemiology of travel-acquired dengue: activity and possibly variations in the virulence of dengue viruses, vector activity, both related and seasonally distributed with an irregular occurrence of outbreaks on one side and the activity of travelling on the other.
Only few data are available in literature about the risk in travellers to acquire dengue infection. Several research groups have studied the rates of dengue infections in travellers, but most of them focused on febrile patients presenting with symptoms at a clinical site. A retrospective study performed among a small cohort of Swiss travellers with fever showed a surprisingly high prevalence (8%) of antibodies to dengue virus(16). A prospective study performed in 130 returned febrile German travellers revealed rising dengue antibodies in 6.9% (17). Among the 335 febrile travellers presenting at a different German travel clinic, 13 (3.9%) cases of DF were laboratory-confirmed(12).
Incidence rates might change in cases of outbreaks: An extensively high attack rate of 69% during a dengue virus outbreak among a group of young short-term community aid workers was reported in a Caribbean island with no documented asymptomatic infection(18).
Of great interest were two prospective studies performed in travellers by collecting serum samples before and after travel. One study was performed in 104 long-term travellers from Israel to various dengue endemic countries which revealed a dengue seroconversion in 6.7% of all travellers with a median of 5.3 months stay abroad, and three out of seven infections were asymptomatic(19). The other study was

Dengue – The Underestimated Risk in Travellers
Dengue Bulletin – Vol 27, 2003 131
performed in Dutch short-term travellers with destinations to endemic areas in Asia and demonstrated an incidence rate of 30/1,000 person-month. The clinical-to-subclinical infection ratio was 1:3.3(20).
All results showed that dengue infection is a realistic threat not limited only to long-term travellers to South-East Asia. In outbreaks, high attack rates might occur, with variable clinical to subclinical ratios, possibly reflecting the role of different virulent virus strains, the importance of initial viral load, or host factors (e.g. susceptibility of different ethnic groups) in the disease severity. Two prospective studies on dengue seroconversion in travellers showed that a high percentage of infections might occur asymptomatically, a phenomenon that has been described in immune and non-immune populations − both adults and children − in Thailand and during outbreaks in Cuba(21,22). Furthermore, in a certain percentage of travellers, the course of the disease will occur entirely during the stay in the endemic country, since the incubation period for dengue infection is relatively short (typically 5 to 7 days) and the disease is self-limiting (typically after 4 to 6 days), and will therefore not be reported to health authorities at home(23,24). Thus, only the tip of the iceberg is reported, making dengue infection one of the most under-reported tropical diseases in travellers.
Patients’ characteristics
The vast majority of the 483 laboratory-confirmed or probable dengue cases reported to TropNetEurop and SIMPID were Europeans living in Europe (87%). Only 31 infections (6.4%) were reported in immigrants, and 14 cases (2.9%) in foreign visitors. The major purpose of travel for
Europeans was tourism (82%), followed by business (5%) and missionary work (4%). Immigrants were mostly infected during visits to their former home country (74%).
The median age in our population was 32 years (range 1–69 years). Males were slightly more frequently affected with a male to female ratio of 1.2:1.
The median duration of travel, during which subjects acquired the dengue infection, decreased from 38 days (range 10–880 days) in 1999 to 23 days (range 3–1,825 days) in 2002.
Since our data were passively collected in symptomatic patients who presented at one of the networks’ clinical member sites, we are not able to extrapolate any particular risk factors to acquire dengue infection during travel, but travel destination as well as duration of travel tend to be associated with risk.
One of the two above-mentioned prospective studies on seroconversion was not able to show any association of developing dengue-like illness with age, sex, travel destination and season, but subjects were only included when travelling to Asia(20). The other study performed among long-term Israeli travellers revealed a trend of higher risk when travelling to South-East Asia, and during the summer season(19).
Clinical manifestations
Dengue virus infection may be asymptomatic as described above or may lead to undifferentiated febrile illness (viral syndrome), dengue fever (DF), or dengue haemorrhagic fever (DHF) with or without shock, depending largely on age and immunological conditions(25,26).

Dengue – The Underestimated Risk in Travellers
132 Dengue Bulletin – Vol 27, 2003
Generally, dengue haemorrhagic fever occurs rarely in travellers, but several cases have been reported(27,28,29,30). In our population, 470 cases were reported as classical dengue fever and 13 as dengue haemorrhagic fever (incidence rate of DHF-cases/100 dengue infections: 2.7). Out of 465 travellers with dengue infection, 421 (91%) were reported to have fever, 63% suffered from headache, 52% from muscle or joint pain, 42% from fatigue, 23% complained of diarrhoea, and 34% developed a macular or a maculopapular rash (Table 2). The presented clinical manifestations refer mainly to Caucasian adults with DF and therefore differ in several aspects from that in children in endemic countries with DF or DHF(5).
Table 2. Signs and symptoms of travel-acquired dengue infections in 465 Europeans
and immigrants (multiple entries possible)
Symptom No. of patients
(%)
Fever 421 (91)
Headache 295 (63)
Myalgia or arthralgia 241 (52)
Fatigue 197 (42)
Rash 158 (34)
Diarrhoea 106 (23)
Vomiting 55 (12)
Lymphadenopathy 31 (7)
Respiratory symptoms 29 (6)
ENT symptoms 28 (6)
Neurological symptoms 12 (3)
Psychological symptoms 7 (2)
Other symptoms 70 (15)
In our network, it is optional to report clinical details of complications associated with the notified disease. Therefore, only limited data on this issue were available. Interestingly, there were two reports on dengue infection associated with ocular involvement, one resulting in prolonged visual impairment(31).
In eight cases, the subjects were reported to have dengue infection with hepatic involvement (reported as hepatitis or highly elevated liver enzymes). Most certainly, this manifestation is by far underreported, since liver function abnormalities seem to be quite common in dengue with aspartate aminotranferase (AST) higher than alanine aminotransferase (ALT). In a study of 275 patients with classical dengue fever in Taiwan, it was found that liver enzymes were increased in 93% of the cases, in 11% the elevation was tenfold or higher(32). Other studies reported that the severity of liver involvement seems to be associated with disease severity(33,34). In a series of 18 Israeli travellers with dengue, all had liver-function abnormalities(35).
In our population, the disease severity in most cases was mild to moderate. The majority of patients were treated as outpatients (n=355, 74%), while 125 (26%) were hospitalized due to an aggravation of clinical symptoms.
Dengue haemorrhagic fever and fatality in travellers
The pathogenesis of DHF is poorly understood, and several hypotheses have emerged to explain why DHF occurs in some individuals who are infected with dengue virus. The observations that classical dengue fever without complications occurs

Dengue – The Underestimated Risk in Travellers
Dengue Bulletin – Vol 27, 2003 133
in non-indigenous foreigners while DHF occurs in indigenous children, and that most aspects of the disease become prominent only after several days of illness when fever and viremia remit, support an immunological explanation for these phenomena: the so-called antibody-dependent enhancement theory(36,37,38,39,40,41).
Interestingly, from a traveller’s point of view, cross-reactive heterotypic immunity has been reported to last between two and 12 months(42). In infants, the dual role of maternal dengue antibodies has been demonstrated in vivo and in vitro: in the first six months, they protect infants from dengue infection, but at 7-8 months they cause a period of greatest risk to acquire DHF/DSS because of enhancing antibodies. Beyond this critical two-month period, further IgG degradation results in a decrease of infection-enhancing antibodies(39). This observation would explain why DHF is rare in travellers.
However, a few cases of DHF have also been described in patients with primary dengue infection(27,30,43,44), as well as the absence of DHF despite hyperendemic dengue virus transmission(45,46). Therefore, other hypotheses suggest that DHF/DSS results from infection by a more virulent serotype or strains within serotypes of the virus(41,47,48). A third theory proposes cross-reactive T cells to cause tissue damage and cytokine secretion(49).
Over a period of four years, 13 cases of DHF have been reported to our networks (2.7% of all dengue infections). Interestingly, the history of travel revealed that the infection was acquired in all endemic regions: seven in South-East Asia, two in Central America, two in South America, one on the Indian subcontinent, and one in Central Africa.
While nine cases of DHF were found in a total of 437 travellers of European origin (2%), four cases of DHF occurred in a total of 45 foreign visitors or immigrants (9%). Therefore, in our population, immigrants or foreign visitors were 4.3 times at higher risk to present with manifestations of dengue haemorrhagic fever when compared with European travellers (95% CI: 1.4–13.5, p-value 0.025). The median travel duration in patients with DHF was 29 days and was not significantly longer compared with patients who developed DF (26 days, p-value 0.38).
No deaths occurred among the 483 reported patients. Since TropNetEurop is also used as a platform for information exchange and discussions by the e-mail system, three fatal cases of dengue in Europe have been reported to the network from sources outside its immediate membership. The first one occurred in 1997 in the United Kingdom and was not published. The other two patients died of DHF in 2002: a Bangladeshi immigrant living in the United Kingdom who returned after visiting his homeland(30), and a young Finnish journalist travelling in South-East Asia (publication in progress).
Conclusion Even though there is considerable lack of data regarding the actual frequency of dengue infection in international travellers, increasing reports of travel-acquired dengue and first fatal cases indicate that dengue infection is a real threat also to travellers(50). The dramatic increase in the number of international travellers to tropical countries and the increased incidence of dengue fever and dengue haemorrhagic fever as well as epidemics of both are two major factors responsible for the increased risk to travellers. The shift in age distribution

Dengue – The Underestimated Risk in Travellers
134 Dengue Bulletin – Vol 27, 2003
towards elderly patients in DHF populations of South-East Asia(51,52) and increasing reports on unusual clinical manifestations(53,54,55,56,57) may reflect variations in the virulence of dengue viruses and will, therefore, also have an impact on the course of travel-acquired dengue.
The development of a live attenuated tetravalent dengue vaccine is currently the best strategy to obtain a vaccine against dengue viruses(58,59,60). Vaccine trials with several candidates are under way, but the necessity of a durable protective immunity to all four serotypes is posing a difficult challenge to researchers.
As long as a vaccine is commercially not available, the single most effective measure of dengue prevention for travellers is to avoid mosquito bites by using insect repellents and protective clothes. Aedes mosquitoes are most active in early mornings and late afternoons.
Health care providers should consider dengue in the differential diagnosis for patients recently returned from endemic areas. Serological techniques provide the tools for screening and confirming the diagnosis, but seroconversion occurs most often after the cessation of clinical symptoms; thus, negative IgM results during the first week of the illness period are
inconclusive. Pre-vaccinations in travellers against Japanese encephalitis and yellow fever might decrease the specificity of the IgG assays(12,41,61,62).
Acknowledgements We wish to thank all TropNetEurop and SIMPID sites staff, who provided invaluable help in collecting data locally: G Burchard, M Corachán, J Clerinx, N Suttorp, H Laferl, J Knobloch, A Björkmann, A Kapaun, I. Gjørup, U Hellgren, A Benito, Z Bisoffi, J Richter, J Beran, K Fleischer, BW Zieger, MH Schulze, P Hartmann, H Siikamaki, S Schubert, B Myrvang, C Hatz, G Carosi, G Fätkenheuer, M Schmid, S da Cunha, G Fry, N Frühwein, B Kreft, T Weinke, L Prüfer-Krämer, T Glück, P Kern, LN Nielsen, L Zöller, G Boecken, J Atouguia, J Cuadros, J Delmont, F Vogel, P Schomerus, B Rieke and PC Döller.
We also thank Associate Professor Pornthep Chantavanich and Assistant Professor Chukiat Sirivichayakul (both of the Faculty of Tropical Medicine, Mahidol University, Bangkok) for reviewing the manuscript.
Financial support for the network SIMPID from the Robert Koch Institute, Berlin, Germany, is gratefully acknowledged.
References 1. Rigau-Pérez JG, Clark GG, Gubler DJ, Reiter P,
Sanders EJ and Vorndam AV. Dengue and dengue haemorrhagic fever. Lancet, 1998, 352: 971-977.
2. Rico-Hesse R. Molecular evolution and distribution of dengue viruses type 1 and 2 in nature. Virology, 1990, 174: 479-493.
3. Gubler DJ. Epidemic dengue/dengue haemorrhagic fever: A global public health problem in the 21st century. In: World Health
Organization, the South-East Asia and Western Pacific Region. Dengue Bulletin, 1997, 21: 1-13.
4. Pinheiro F and Nelson M. Re-emergence of dengue and emergence of dengue haemorrhagic fever in the Americas. In: World Health Organization, the South-East Asia and Western Pacific Regions. Dengue Bulletin, 1997, 21: 16-23.
5. World Health Organization. Dengue haemorrhagic fever. Diagnosis, treatment, prevention and control, 2nd ed. Geneva: WHO, 1997: 12-23.
Dengue – The Underestimated Risk in Travellers
Dengue Bulletin – Vol 27, 2003 135
6. Gibbons RV and Vaughn DW. Dengue: An escalating problem. British Medical Journal, 2002, 324: 1563-6.
7. Monath TP. Dengue: The risk to developed and developing countries. Proceedings of the National Academy of Science USA, 1994, 91: 2395-2400.
8. World Tourism Organization. Preliminary tourism statistics for 2002. Madrid: 2003. http://www.world-tourism.org (accessed 2nd Feb 2003).
9. Centre of Disease Control, CDC. Imported dengue – United States, 1997 and 1998. Morbidity and Mortality Weekly Report, 2000, 49: 248-253.
10. Suh KN, Kozarsky PE and Keystone JS. Evaluation of fever in the returned traveller. Medical Clinics of North America, 1999, 83: 997-1017.
11. O’Brien D, Tobin S, Brown GV and Torres J. Fever in returned travellers: Review of hospital admissions for a 3-year period. Clinical Infectious Diseases, 2001, 33: 603-609.
12. Stephan C, Allwinn R, Brodt HR, Knupp B, Preiser W and Just-Nübling G. Travel-acquired dengue infection: Clinical spectrum and diagnostic aspects. Infection, 2002, 30: 225-228.
13. Jelinek T, Mühlberger N, Harms G, Corachán MP, Knobloch J, Bronner U, Laferl H, Kapaun A, Bisoffi Z, Clerinx J, Puente S, Fry G, Schulze M, Hellgren U, Grørup I, Chalupa P, Hatz C, Matteelli A, Schmid M, Nielsen LN, da Cunha S, Atouguia J, Myrvang B and Fleischer K for the European Network on Surveillance of Imported Infectious Diseases. Epidemiology and clinical features of imported dengue fever in Europe: Sentinel surveillance data from TropNetEurop. Clinical Infectious Diseases, 2002, 35: 1047-1052.
14. The European Network on Imported Infectious Disease Surveillance (TropNetEurop). http://www.tropnet.net (accessed 15th Feb 2003).
15. World Health Organization. Dengue haemorrhagic fever. Diagnosis, treatment, prevention and control, 2nd ed. Geneva: WHO, 1997: 12-23.
16. Settah SG, Vernazza PL, Morant R and Schultze D. Imported dengue fever in Switzerland – Serological evidence for a hitherto unexpectedly high prevalence. Schweizer Medizinische Wochenschrift, 1995, 125: 1673-1678.
17. Jelinek T, Dobler G, Hölscher M, Löscher T and Nothdurft HD. Prevalence of infection with dengue virus among international travelers. Archives of Internal Medicine, 1997, 157: 2367-2370.
18. Lyerla R, Rigau-Perez JG, Vorndam AV, Reiter P, George AM, Potter IM and Gubler DJ. A dengue outbreak among camp participants in a Caribbean island, 1995. Journal of Travel Medicine, 2000, 7: 59-63.
19. Potasman I, Srugo I and Schwartz E. Dengue seroconversion among Israeli travellers to tropical countries. Emerging Infectious Diseases, 1999, 5: 824-827.
20. Cobelens FGJ, Groen J, Osterhaus ADME, Leentvaar-Kuipers A, Wertheim-van Dillen PME and Kager PA. Incidence and risk factors of probable dengue virus infection among Dutch travellers to Asia. Tropical Medicine and International Health, 2002, 7: 331-338.
21. Burke DS, Nisalak A, Johnson DE and Scott RM. A prospective study of dengue infection in Bangkok. American Journal of Tropical Medicine and Hygiene, 1988, 38: 172-180.
22. Guzman MG, Kouri GP, Bravo J, Soler M, Vazquez S and Morier L. Dengue haemorrhagic fever in Cuba, 1981: A retrospective seroepidemiologic study. American Journal of Tropical Medicine and Hygiene, 1990, 42: 179-184.
23. Schwartz E, Moskovitz A, Potasman I, Peri G, Grossman Z and Alkan ML. Changing epidemiology of dengue fever in travellers to Thailand. European Journal of Clinical Microbiology and Infectious Diseases, 2000, 19: 784-786.
24. Thavara U, Tawatsin A, Phan-Urai P, Ngamsuk W, Chansang C, Mingtuan L and Zhijun L. Dengue vector mosquitoes at a tourist attraction, Ko Samui, in 1995. South-East Asian Journal of Tropical Medicine and Hygiene, 1996, 27: 160-163.
25. Nimmannitya S. Clinical manifestations of dengue/dengue haemorrhagic fever. In: World Health Organization, Regional Office for South-East Asia. Monograph on dengue/dengue haemorrhagic fever. Regional Publication No. 22. New Delhi: WHO, 1993: 48-54.
26. Kalayanarooj S, Vaughn DW, Nimmannitya S, Green S, Suntayakorn S, Kunentrasai N, Viramitrachai W, Ratanachu-eke S, Kiatpolpoj S, Innis BL, Rothman AL, Nisalak A and Ennis FA. Early clinical and laboratory indicators of acute dengue illness. Journal of Infectious Diseases, 1997, 176: 313-321.
27. Morens DM, Sather GE, Gubler DJ, Rammohan M and Woodall JP. Dengue shock syndrome in an American traveller with primary dengue 3 infection. American Journal of Tropical Medicine and Hygiene, 1987, 36: 424-426.

Dengue – The Underestimated Risk in Travellers
136 Dengue Bulletin – Vol 27, 2003
28. Lopez-Velez R, Perez-Casas C, Vorndam AV and Rigau J. Dengue in Spanish travelers returning from the tropics. European Journal of Clinical Microbiology and Infectious Diseases, 1996, 15: 823-836.
29. Wittesjo B, Eitrem R and Niklasson B. Dengue fever among Swedish tourists. Scandinavian Journal of Infectious Diseases, 1993, 25: 699-704.
30. Lawn SD, Tilley R, Lloyd G, Finlayson C, Tolley H, Newman P, Rice P and Harrison TS. Dengue haemorrhagic fever with fulminant hepatic failure in an immigrant returning to Bangladesh. Clinical Infectious Diseases, 2003, 37: e1-4.
31. Haritoglou C, Dotse SD, Rudolph G, Stephan CM, Thurau SR and Klauß V. A tourist with dengue fever and visual loss. Lancet, 2002, 360: 1070.
32. Kuo CH, Tai DI, Chang-Chien CS, Lan CK, Chiou SS and Liaw YF. Liver biochemical tests and dengue fever. American Journal of Tropical Medicine and Hygiene, 1992, 47: 265-270.
33. Wahid SF, Sanusi S, Zawawi MM and Ali RA. A Comparison of the pattern of liver involvement in dengue haemorrhagic fever with classic dengue fever. South-East Asian Journal of Tropical Medicine and Public Health, 2000, 31: 259-263.
34. Murgue B, Deparis X, Chungue E, Cassar O and Roche C. Dengue: An evaluation of dengue severity in French Polynesia based on an analysis of 403 laboratory-confirmed cases. Tropical Medicine and International Health, 1999, 4: 765-773.
35. Schwartz E, Mendelson E and Sidi Y. Dengue fever among travelers. American Journal of Medicine, 1996, 101: 516-520.
36. Kliks SC, Nisalak A, Brandt WE, Wahl L and Burke DS. Antibody-dependent enhancement of dengue virus growth in human monocytes as a risk factor for dengue haemorrhagic fever. American Journal of Tropical Medicine and Hygiene, 1989, 40: 444-451.
37. Sangkawibha N, Rojanasuphot S, Ahandrik S, Viriyapongse S, Jatanasen S, Salitul V, Phanthumachinda B and Halstead SB. Risk factors in dengue shock syndrome: A prospective epidemiologic study in Rayong, Thailand. American Journal of Epidemiololy, 1984, 120: 653-669.
38. Thein S, Aung MM, Shwe TN, Aye M, Zaw A, Aye K, Aye KM and Aaskov J. Risk factors in dengue shock syndrome. American Journal of Tropical Medicine and Hygiene, 1997, 56: 566-572.
39. Kliks SC, Nimmanitya S, Nisalak A and Burke DS. Evidence that maternal dengue antibodies are important in the development of dengue haemorrhagic fever in infants. American Journal of Tropical Medicine and Hygiene, 1988, 38: 411-419.
40. Halstead SB. Pathogenesis of dengue: Challenges to molecular biology. Science, 1988, 239: 476-481.
41. Vaughn DW, Green S, Kalajanarooj S, Innis BL, Nimmannitya S, Suntayakorn S, Rothman AL, Ennis FA and Nisalak A. Dengue in the early febrile phase: Viremia and antibody responses. Journal of Infectious Diseases, 1997, 176: 322-330.
42. Nimmannitya S. Dengue fever and dengue haemorrhagic fever. In: Manson´s Tropical Diseases. 20th ed. London, 1996: 721-729.
43. Gubler DJ, Reed D, Rosen L and Hitchcock JC. Epidemiological, clinical, and virologic observations on dengue in the Kingdom of Tonga. American Journal of Tropical Medicine and Hygiene, 1978, 27: 581-589.
44. Barnes WJS and Rosen L. Fatal haemorrhagic disease and shock associated with primary dengue infection on a Pacific island. American Journal of Tropical Medicine and Hygiene, 1974, 23: 495-506.
45. Halstead SB, Streit TG, Lafontant JG, Putvatana R, Russell K, Sun W, Kanesa-Thasan N, Hayes CG and Watts DM. Haiti: Absence of dengue haemorrhagic fever despite hyperendemic dengue virus transmission. American Journal of Tropical Medicine and Hygiene, 2001, 65: 180-183.
46. Watts DM, Porter KR, Putvatana P, Vasquez B, Calampa C, Hayes CG and Halstead SB. Failure of secondary infection with American genotype dengue 2 to cause dengue haemorrhagic fever. Lancet, 1999, 354: 1431-1434.
47. Leitmeter KC, Vaughn DW, Watts DM, Salas R, de Chacon IV, Ramos C and Rico-Hesse R. Dengue virus structural differences that correlate with pathogenesis. Journal of Virology, 1999, 73: 4738-4747.
48. White NJ. Variation in virulence of dengue virus. Lancet, 1999, 23: 1401-1402.
49. Loke H, Bethell DB, Phuong CXT, Dung M, Schneider J, White NJ, Day NP, Farrar J and Hill AVS. Strong HLA Class I-Restricted T cell responses in dengue haemorrhagic fever: A double-edged sword? Journal of Infectious Diseases, 2001, 184: 1369-1373.
Dengue – The Underestimated Risk in Travellers
Dengue Bulletin – Vol 27, 2003 137
50. Jelinek T. Dengue fever in international travelers. Clinical Infectious Diseases, 2000, 31: 144-147.
51. Nimmannitya S. Dengue haemorrhagic fever in Thailand. South-East Asian Journal of Tropical Medicine and Public Health, 1987, 18: 292-294.
52. Hadinegoro SR and Nathin MA. The changing patterns of clinical manifestations in dengue haemorrhagic fever: Ten years observations. South-East Asian Journal of Tropical Medicine and Public Health, 1990, 21: 694.
53. Nimmannitya S, Thisyakorn U and Hemsrichart V. Dengue haemorrhagic fever with unusual manifestations. South-East Asian Journal of Tropical Medicine and Public Health, 1987, 18: 398-406.
54. Sirivichayakul C, Sabcharoen A, Chanthavanich P, Pengsaa K, Chokejindachai W and Prarinyanupharb V. Dengue infection with unusual manifestation: A case report. Journal of the Medical Association of Thailand, 2000, 83: 325-329.
55. Pancharoen C, Kulwichit W, Tantawichien T, Thisyakorn U and Thisyakorn C. Dengue infection: A global concern. Journal of the Medical Association of Thailand, 2002, 85 (Suppl 1): S25-S33.
56. Solomon T, Dung NM, Vaughn DW, Kneen R, Thao LTT, Raengsakulrach B, Loan HT, Day NPJ, Farrar J, Myint KSA, Warrell MJ, James WS, Nisalak A and White NJ. Neurological manifestations of dengue infection. Lancet, 2000, 355: 1053-1059.
57. Cam BV, Fonsmark L, Hue NB, Phuong NT, Poulsen A and Heegaard ED. Prospective case-control study of encephalopathy in children with dengue haemorrhagic fever. American Journal of Tropical Medicine and Hygiene, 2001, 65: 848-851.
58. Bhamarapravati N and Sutee Y. Live attenuated tetravalent dengue vaccine. Vaccine, 2000, 18: 44-47.
59. Kanesa-thasan N, Sun W, Kim-Ahn G, Van Albert S, Putnak JR, King A, Raengsakulsrach B, Christ-Schmidt H, Gilson K, Zahradnik JM, Vaughn DW, Innis BL, Saluzzo JF and Hoke Jr CH. Safety and immunogenicity of attenuated dengue virus vaccines (Aventis Pasteur) in human volunteers. Vaccine, 2001, 19: 3179-3188.
60. Sabchareon A, Lang J, Chanthavanich P, Yoksan S, Forrat R, Attanath P, Sirivichayakul C, Pengsaa K, Pojjaroen-Anant C, Chokejindachai W, Jagsudee A, Saluzzo SF and Bhamarapravati N. Safety and immunogenicity of tetravalent live-attenuated dengue vaccines in Thai adult volunteers: Role of serotype concentration, ratio and multiple doses. American Journal of Tropical Medicine and Hygiene, 2002, 66: 264-272.
61. Schwartz E, Mileguir F, Grossmann Z and Mendelson E. Evaluation of ELISA-based sero-diagnosis of dengue fever in travelers. Journal of Clinical Virology, 2000, 19: 169-173.
62. Innis BL, Nisalak A, Nimmannitya S, Kusalerdchariya S, Chongswasdi V, Suntayakorn S, Puttisri P and Hoke CH. An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese encephalitis co-circulate. American Journal of Tropical Medicine and Hygiene, 1989, 40: 418-427.

138 Dengue Bulletin – Vol 27, 2003
Thrombocytopenia and Platelet Transfusions in Dengue Haemorrhagic Fever and Dengue Shock Syndrome
by Alex Chairulfatah*#, Djatnika Setiabudi*, Ridad Agoes** and
Robert Colebunders***
*The Department of Child Health, Padjadjaran University Medical School, Dr Hasan Sadikin General Hospital, Jl. Pasteur 38 Bandung, Indonesia
**The Department of Parasitology, Padjadjaran University Medical School, Dr Hasan Sadikin General Hospital, Jl. Pasteur 38 Bandung, Indonesia
***Institute of Tropical Medicine, Antwerp, Belgium
Abstract
The presence of thrombocytopenia was determined in 1,300 patients with dengue haemorrhagic fever (DHF) (1,198; 92%) and dengue shock syndrome (DSS) (102; 8%) admitted to four major hospitals in Bandung, Indonesia. A dengue serological test was performed on 1,100 (85%) of the patients with a positive result in 763 (69%), HI test on 243 patients (22%), IgG dengue blot on 489 patients (44%) and IgM dengue blot on 25 patients (2.3%). Since an accurate diagnosis was found only in a small proportion of the cases (positive HI test), all the clinically-diagnosed DHF/DSS cases were analysed. Thrombocyte count of less than 100,000/µl was present in 445 (34%) cases on admission and in 637 (49%) cases during hospitalization. In the serologically-confirmed cases, the prevalence of thrombocytopenia (count less than 100,000/µl) was 58% on admission and 83% during hospitalization. Severe bleeding was recorded in 76 (6%) of all DHF/DSS cases and occurred more often in patients with severe thrombocytopenia. One hundred and fifty-six (12%) DHF/DSS cases received a platelet transfusion; among them only 30 (19%) had a platelet count below 25,000/µl. No difference in the frequency of bleeding was observed comparing patients who received or those who did not receive a platelet transfusion (even in those with a platelet count < 25,000/µl).
In conclusion, a large number of patients with DHF/DSS in Bandung hospitals receive platelet transfusions, even if thrombocyte counts are above 25,000/µl. This study suggests that in most DHF/DSS cases, platelet transfusions do not influence the incidence of severe bleeding. Treatment costs for DHF/DSS cases could be reduced if these unnecessary platelet transfusions are avoided. Further studies undertaken only in accurately confirmed cases are needed to clarify this finding.
Keywords: Dengue haemorrhagic fever, dengue shock syndrome, thrombocytopenia, platelet transfusions.
# For correspondence: [email protected]

Thrombocytopenia and Platelet Transfusions in DHF and DSS
Dengue Bulletin – Vol 27, 2003 139
Introduction The clinical diagnosis of dengue haemorrhagic fever (DHF), especially in the early phase of illness, is not easy. Laboratory findings such as thrombocytopenia and a rising haematocrit in DHF cases are usually observed by day 3 or 4 of the illness(1). Several studies have revealed a variable prevalence of thrombocytopenia. Sumarmo(2) found a prevalence of thrombocytopenia in 81% of the cases in the Department of Child Health, Cipto Mangunkusumo National Hospital, Jakarta, Indonesia. Ten years later, a prevalence of 59% was observed in the same department(3). In the confirmed DHF cases, Samsi et al.(4), in Jakarta, observed thrombocytopenia in 9% of the cases on admission and in 38% during hospitalization.
The use of platelet transfusions in DHF/DSS patients, therefore, remains controversial.
One of the aims of this study was to evaluate the effect of platelet transfusions to prevent bleeding in DHF/DSS patients.
Materials and methods This study was part of a DHF/DSS hospital-based surveillance study which was carried out in Bandung, Indonesia, between August 1995 and March 1996. The study included all patients with a DHF/DSS diagnosis on admission and discharge, according to the opinion of the attending physician.
The medical records of DHF/DSS patients, hospitalized from April 1994 until June 1995 in four major hospitals in Bandung (Dr Hasan Sadikin General Hospital, St. Borromeus Hospital, Immanuel Hospital and St. Yusuf Hospital, were reviewed.
Laboratory tests to confirm dengue infection included the haemaglutination inhibition (HI) test, using the Cassal and Clark microtechnic modification, the IgG dengue blot (GeneLab, Kalbe) and the IgM dengue blot test (GeneLab, Kalbe). The HI test was performed on paired sera, while the IgG and IgM dengue blot tests were performed on acute sera only.
The age of the patient, duration of fever before admission, result of the dengue serological test, platelet count on admission and during hospitalization, presence of severe bleeding manifestations and date of onset of bleeding, administration of platelet transfusions and dates of transfusions were recorded. Severe bleeding manifestations included haematemesis, melena, haematemesis-melena and disseminated intravascular coagulation (DIC). Since epistaxis is commonly observed during febrile illness, epistaxis was not used as a criterion of severe bleeding except if it was massive.
Statistical analysis
χ2 analysis was used to detect trends. Proportions were compared using the Pearson χ2-test; the calculated p-values were Yates-corrected. For all analysis a p-value lower than 0.05 was considered significant. Statistics were performed using EPI-INFO 6.
Results Of the 1,300 clinical DF/DSS cases, 1,198 (92%) were considered to have DHF and 102 (8%) DSS; 673 (52%) were male and 627 (48%) female; most patients were between 6-10 years of age (mean 13 years old) (Table 1).

Thrombocytopenia and Platelet Transfusions in DHF and DSS
140 Dengue Bulletin – Vol 27, 2003
Table 1. Prevalence of DHF and DSS cases by age and sex
Age (years) Male Female Total
< 2 8 - 8
2-5 78 79 157
6-10 161 166 327
11-14 111 98 209
15-20 105 84 189
21-30 115 126 241
31-40 55 46 101
41-50 26 19 45
> 50 14 9 23
Total 673 627 1,300
For 168 cases (13%), there was no information about the duration of the fever in the medical records. Where the information was available, 673 (66%) had 3-5 days of fever prior to admission (Table 2). Seventy-one DSS patients (70%) developed shock after 3 to 5 days of fever, most of them were admitted in shock, and only two patients (2%) developed shock during hospitalization.
A dengue serological test was performed on the sera of 1,100 patients (85%) which gave a positive result in 763 patients (69%), including a positive HI test in 243 patients (22%), a positive IgG dengue blot test in 489 patients (44%) and a positive IgM dengue blot test in 25 patients (2.3%) (Table 3). A negative IgG dengue blot result was observed in 45 of 72 children (62%) under six years of age (Table 3). Since the number of patients with accurate diagnosis (positive HI test) who received platelet transfusions and its outcome were too small
for statistical analysis, the analysis was performed in all clinically diagnosed DHF/DSS patients.
Table 2. Duration of fever prior to admission of DHF/DSS cases
DHF DSS
n % n %
1 25 2 3 3 2 161 16 10 10 3 246 24 22 22
4 222 22 23 23 5 205 20 26 26 6 71 7 14 14 7 90 9 4 4
8 8 1 - - 9 2 0.2 - - 1,030 100 102 102
Table 3. DHF and DSS cases with a positive serological test
Positive
DHF DSS Total Name of the
serological test
No. tested
(n) n % n % n %
HI 498 219 44 24 5 243 49
IgG D blot 561 454 81 35 6 489 87
IgM D blot 30 25 83 - - 25 83
HI + IgG D blot
3 3 100 - - 3 100
IgG + IgM D blot
5 2 40 1 20 3 60
Not performed
203 - - - - - -
1,300 703 54 60 4 763 59
HI = Haemaglutination inhibition test IgG D blot = IgG dengue blot test IgM D blot = IgM dengue blot test
Duration of fever at home
(days)

Thrombocytopenia and Platelet Transfusions in DHF and DSS
Dengue Bulletin – Vol 27, 2003 141
Of all the clinically diagnosed DHF/DSS patients, a thrombocytopenia less than 100,000/µl was present in 445 cases (34%) on admission and in 637 cases (49%) during hospitalization. In the serologically confirmed cases, the prevalence of thrombocytopenia less than 100,000/µl was 58% on admission and 83% during hospitalization. Thrombocytopenia was present in 561 (47%) of the DHF cases and in 76 (74%) of the DSS cases. The majority of cases developed thrombocytopenia between the third and seventh day of illness, with no difference between DHF and DSS cases (Table 4).
Severe bleeding was recorded in 76 of the dengue cases (6%) and included haematemesis in 44 of them (58%), melena in 16 (21%), haematemesis-melena in 12 (16%) and DIC in 4 of the cases (5%). Severe
bleeding occurred more often in patients with severe thrombocytopenia (χ2 trend = 51,406, p<0.001) (Table 5).
Table 4. Day of onset of thrombocytopenia <100,000/µl in DHF and DSS cases
DHF DSS Total
n % n % n %
1 6 1 - - 6 1
2 31 5 3 4 34 6
3 92 16 11 14 103 16
4 116 22 12 16 128 20
5 154 27 20 26 174 27
6 68 12 18 24 86 13
7 60 11 9 12 69 11
8 14 2 1 1 15 2
> 8 20 4 2 3 22 4
561 100 76 100 637 100
Table 5. Degree of thrombocytopenia and the presence of severe bleeding
Severe bleeding Platelet count (000) Total n
DIC H M H-M n Total % OR*
< 25 59 - 5 4 2 11 19 1
25-49 164 2 6 6 2 16 10 0.55
50-74 205 1 14 3 5 23 11 0.45
75-100 209 1 11 3 2 17 8 0.39
> 100 663 - 8 - 1 9 1 0.06
1,300 4 44 16 12 76 6
DIC: Disseminated intravascular coagulation H: Haematemesis M: Melena H-M: Haematemesis–Melena OR: Odds ratio * χ2 for trend
Day

Thrombocytopenia and Platelet Transfusions in DHF and DSS
142 Dengue Bulletin – Vol 27, 2003
Such bleeding was particularly frequent in patients with a thrombocyte count <15,000/µl [occurred in 5 (36%) of the 14 patients].
One hundred and fifty-six (12%) of all DHF/DSS cases — 152 with a thrombocyte count of less than 100,000/µl and 4 with a thrombocyte count of more than 100,000/µl — received a platelet
transfusion. No difference in the frequency of bleeding was observed comparing the patients who received a platelet transfusion or the ones who did not receive (even in those with a platelet count <25,000/µl) (Table 6). In 25 cases a platelet transfusion was given after the onset of the bleeding. Only 30 (19%) of those who received a platelet transfusion had a thrombocyte count below 25,000/µl.
Table 6. Bleeding in patients with or without a platelet transfusion
Without platelet transfusion (000)
With platelet transfusion
Bleeding Bleeding
Platelet count (000)
Total n n %
Total n n %
OR CI P**
<25 23 3 13 36 8 22 0.52 (0.10-2.60) 0.502
25-49 62 2 3 102 14 14 0.21 (0.03-1.02) 0.054
50-74 31 1 3 174 22 13 0.23 (0.01-1.71) 0.213
75-100 13 1 8 196 16 8 0.94 - 1.000
> 100 2 - - 661 9 1 0 - 1.000
131 7 5 1169 69* 6 0.90 * 25 of these patients also received a platelet transfusion, but after the onset of bleeding ** comparison χ2 test (Yates corrected) OR: Odds ratio CI: Confidence interval
Seventeen of all cases died (1%), 8 (47%) within 24 hours and 9 (53%) more than 24 hours after admission. The fatality rate of 48 cases, discharged against medical advice, and 4 cases, transferred to other hospitals, could not be traced.
Discussion DHF is a major public health problem in Indonesia. Bandung is one of the big cities in Indonesia where DHF is endemic. This study showed that the majority of DHF cases were
children, with the largest proportion in the age group of 6-10 years (Table 1). This is in accordance with other studies in Indonesia. As per other workers, in the serologically and virologically confirmed cases, most patients were in the 5-9-year age group(3,4).
Early in the infection, it may be difficult to differentiate DHF from other febrile illnesses. Later, usually after three or four days, when thrombocytopenia and haemoconcentration are present, DHF is easier to diagnose. In this study, 432 dengue cases (42%) were admitted before day 4 of their illness.

Thrombocytopenia and Platelet Transfusions in DHF and DSS
Dengue Bulletin – Vol 27, 2003 143
Thrombocytopenia was found in 58% of the confirmed cases on admission and in 83% during hospitalization. This prevalence is in accordance with the findings of Sumarmo(2), but differs from those of other investigators(3,4,5). However, in these studies, different definitions of DHF have been used(6). Similar to other studies, thrombocytopenia was found in the majority of cases between day 3 and day 7 after the onset of fever(1,6,7) (most often day 5). Severe bleeding occurred significantly more often in patients with more severe thrombocytopenia. Bleeding during DHF may result from a combination of factors such as thrombocytopenia, coagulation defects and vasculopathy(8). In this study, a similar percentage of patients developed severe bleeding, whether or not they received a platelet transfusion.
In conclusion, a large number of patients with DHF/DSS in Bandung hospitals receive platelet transfusions, even if thrombocyte counts are above 25,000/µl. This study suggests that these platelet transfusions do not influence the incidence of severe bleeding in most DHF/DSS cases. Treatment costs for DHF/DSS cases could be reduced if these unnecessary platelet transfusions were not given. A further study performed only in accurate confirmed cases is needed to clarify the findings of this study.
Acknowledgements We thank Professor A Meheus and the Department of Epidemiology, Antwerp University, for their assistance, and the Belgium Ministry of Development Cooperation, for their financial support.
References 1. World Health Organization. Dengue haemorrhagic
fever: Diagnosis, treatment and control. 2nd ed., 1997, WHO, Geneva.
2. Sumarmo Poorwosudarmo. Dengue haemorrhagic fever (thesis). University of Indonesia Press, 1983.
3. Harun SR. Clinical aspects of dengue haemorrhagic fever in children: In proceedings of the seminar and workshop on dengue haemorrhagic fever and its control. Jakarta, 27-28 November 1990: 63-68.
4. Samsi TK and Sugianto D. Evaluation on concentrated platelet transfusion in severe dengue haemorrhagic fever: In proceedings of the national conference of Indonesian Paediatrics Association, Ujung Pandang, 1990: 138-139.
5. Chairulfatah A, Djatnika S, Agoes R and Colebunders R. Clinical manifestations of dengue haemorrhagic fever in children in Bandung, Indonesia. Annales de la Societe Belge de Medecine Tropicale, 1996, 75: 291-295.
6. Natth B. Foreword on international symposium on dengue and dengue haemorrhagic fever in children and adult. South-East Journal of Tropical Medicine and Public Health, 1990, 41: 634-635.
7. Sugianto D, Samsi TK, Wulur H, Dirgagunsa SA and Jenning GB. The changes of platelet count in dengue haemorrhagic fever. Cermin Dunia Kedokteran, 1994, 92: 14-17.
8. Natth B. Pathology of dengue haemorrhagic fever: In monograph on dengue and dengue haemorrhagic fever. SEARO Regional Publication No. 22, New Delhi, 1993, 22: 72-79.

144 Dengue Bulletin – Vol 27, 2003
Improvement of Case-Management - A Key Factor to Reduce Case-Fatality Rate of Dengue Haemorrhagic
Fever in Southern Viet Nam
by
Nguyen Thanh Hung# and Nguyen Trong Lan
Department of Dengue Haemorrhagic Fever, Children’s Hospital N.1, 341 Su Van Hanh St., Dist 10, Ho Chi Minh City, Viet Nam
Abstract
Dengue haemorrhagic fever (DHF) is a leading cause of hospitalization and death in children in Viet Nam since 1960. This paper emphasizes on the measures taken to improve case management of DHF/dengue shock syndrome (DSS) patients in the country - to reduce the case-fatality rate (CFR) of the disease. These included early diagnosis, correct treatment, and careful monitoring of DHF/DSS patients, as well as counseling mothers/caretakers on measures to take care of DHF patients at home in order to detect warning signs of shock and early admission. These measures had a dramatic effect on reducing the mortality among DHF patients from 8.26% during the period from 1964 to 1974 to 0.26% during the period from 1996 to 2000. CFR of DSS also reduced to between 1.44 and 2% during 1999-2001.
Keywords: DHF/DSS, case-fatality rate, case management, Viet Nam.
# For correspondence: [email protected]
Introduction Dengue haemorrhagic fever (DHF) has emerged as a major public health problem in Viet Nam since 1960. It is a leading cause of hospitalization and death in children(1). In 1998, a widespread DHF epidemic affected 51 out of 67 provinces of the country with 234,866 cases and 383 deaths. Reducing the mortality being the primary objective of the DHF Control Programme(2), a number of
measures were taken to improve case management of DHF/dengue shock syndrome (DSS) patients by the medical staff at all levels of the health care system. These included early diagnosis, correct treatment and careful monitoring of DHF/DSS patients, as well as counselling mothers/caretakers on how to take care of DHF patients at home in order to detect the warning signs of shock for early admission(3).

Improvement of Case-Management as a Key Factor to Reduce CFR of DHF in Southern Viet Nam
Dengue Bulletin – Vol 27, 2003 145
This paper outlines the impact the above-mentioned measures have made on reducing the case-mortality rate of the disease over the last 20 years in Southern Viet Nam.
Elements of improved case management of DHF/DSS patients
Early diagnosis
Two main pathophysiological changes occur in DHF: (i) increased vascular permeability resulting in plasma leakage, haemo-concentration, hypovolemia and shock; and (ii) abnormal haemostasis due to vasculopathy, thrombocytopenia and disseminated intravascular coagulopathy (DIC), leading to various haemorrhagic manifestations(4). These are the scientific bases for WHO’s clinical diagnostic criteria(4). To strictly follow WHO’s criteria, early diagnosis of DHF can be made before most patients reach the critical stage of shock. Early clinical diagnosis of DHF is confirmed by serological tests and/or virus isolation or RT-PCR. This approach met a success rate of 90.6% and 96.2% of the total DHF and DSS cases, respectively, at the Children’s Hospital N.1, Ho Chi Minh City(5,6). A child having fever for two or more days should alert a clinician to make an early diagnosis of DHF, and this practice proves to be a good management tool before the patient goes into shock.
Management of DHF/DSS patients
Replacement of plasma loss received the highest priority in the management of DHF/DSS (Figure 1). It should be borne in
mind that not all DHF patients need intravenous (IV) fluid replacement. Patients with non-shock DHF can be managed as outpatients and followed closely everyday from day 3 onwards of their illness, until they are afebrile for more than 48 hours without the use of antipyretics. In these patients, oral rehydration can be achieved by encouraging the child to drink fluids such as oral rehydration solution (ORS), fruit juice and plain water as much as possible. The mothers/caretakers should be advised on how to care for the child at home, and how to recognize the warning signs of shock in order to bring the child back to the nearest hospital in case of emergency. IV fluid therapy in the hospital is necessary in about one-third of the non-shock DHF patients. When these patients have one or more of the following signs/symptoms, IV fluid therapy with the isotonic crystalloid fluids (physiological saline, Ringer’s lactate) should be indicated:
• Repeated vomiting
• Acute, severe abdominal pain; rapid liver enlargement
• Haematemesis, melaena, frank gingival bleeding, severe epistaxis
• Lethargy
• Cold extremities and rapid pulse
• High degree of haemo-concentration, rapidly rising haematocrit.
Early volume replacement of lost plasma by IV fluid therapy in these patients can modify the severity of the disease(5).

Improvement of Case-Management as a Key Factor to Reduce CFR of DHF in Southern Viet Nam
146 Dengue Bulletin – Vol 27, 2003
For patients with DSS, early detection of shock, proper treatment and careful monitoring are of vital importance. DSS patients should be admitted immediately to an emergency/intensive care ward. Prompt and adequate fluid resuscitation is the basic treatment for DSS. The recommended regimen for the treatment of DSS patients is as follows:
• Immediate and rapid replacement of the plasma loss with crystalloid or, in the case of profound shock, colloid solutions.
• Continued replacement of further plasma losses to maintain effective circulation for 24-48 hours.
• Correction of metabolic and electrolyte disturbances.
• Blood transfusion – only to cases with severe bleeding.
Careful monitoring of DHF/DSS patients, a mandatory requirement
DHF/DSS patients should be kept under constant and careful observation round the clock by medical staff (both doctors and nurses) in order to detect early and treat correctly the patients with impending shock as well as severe complications such as recurrent shock, massive bleeding, fluid overload, fulminant hepatitis and dengue encephalopathy.
Measures taken to improve DHF/DSS case management in Southern Viet Nam The key measures taken to improve DHF/DSS case management in Southern Viet Nam during the past 20 years are:
Figure 1. Replacement of plasma loss as the principle of management of DHF/DSS
Plasma leakage
Haemorrhage IV fluid replacement
Blood transfusion
EC
EC
EC: Endothelial cells
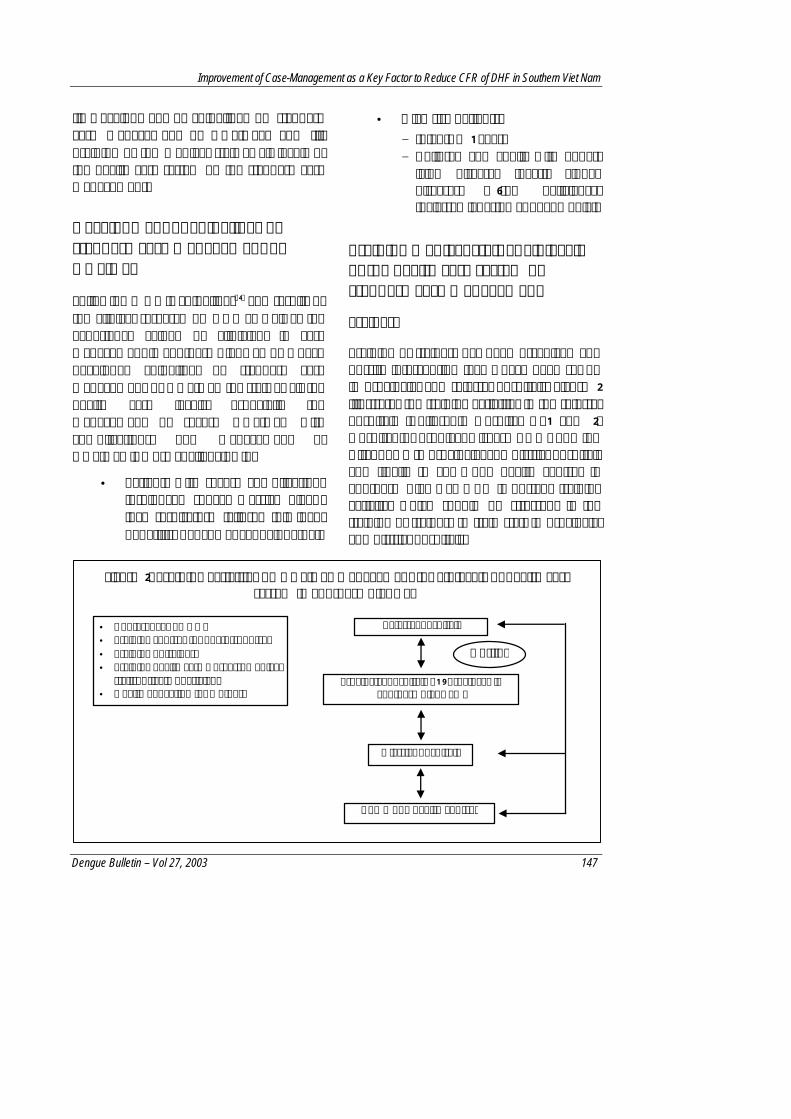
Improvement of Case-Management as a Key Factor to Reduce CFR of DHF in Southern Viet Nam
Dengue Bulletin – Vol 27, 2003 147
(i) Development of guidelines on standard case management of DHF/DSS; and (ii) Training of the medical staff at all levels of the health care system on the standard case management.
Development of guidelines on standard case management of DHF/DSS
Following WHO’s guidelines(4) and results of the clinical research on DHF as well as the experience gained by clinicians in case management in Southern Viet Nam, we have developed guidelines on standard case management of DHF/DSS for staff at all the health care levels, especially the management of severe DHF/DSS with complications. The management of DHF/DSS is more challenging in:
• Patients with severe complications (prolonged shock; massive bleed-ing; respiratory failure; fulminant hepatitis; dengue encephalopathy).
• High risk patients: − Infants <1 year. − Children and adults with under-
lying diseases (heart, kidney diseases; G6-PD deficiency; thalassemia; asthma; pneumonia).
Training medical staff at all levels of the health care system on standard case management
Trainers
Training of trainers has been organized and on-site intervention teams have been set up in provincial and referral hospitals. Figure 2 illustrates the training activities in the referral hospitals (Children’s Hospital N.1 and 2; Hospital for Tropical Disease - Ho Chi Minh City) down to provincial and district hospitals and finally to commune health centres in Southern Viet Nam. An important training activity, which should be stressed, is the training of trainers to train staff in provincial and district hospitals.
• Conferences on DHF • Training courses for doctors, nurses • Training of trainers • Training health care workers, medical
staffs, private physicians • Health education for mothers
Referral hospitals
District hospitals
Commune health centres
Hotline
Provincial hospitals (19 provinces in Southern Viet Nam)
Figure 2. Training activities on DHF/DSS management for all levels of health care system in Southern Viet Nam

Improvement of Case-Management as a Key Factor to Reduce CFR of DHF in Southern Viet Nam
148 Dengue Bulletin – Vol 27, 2003
Trainees Training on DHF/DSS case management has been organized for medical staff (physicians, nurses, medical students, health workers) at all levels of the health care system. Health education on DHF for mothers/caretakers is also focused.
Frequency of training courses Training activities have been organized continuously every year before, during and after the outbreak of DHF. A hotline has been set up to connect all the health care facilities by telephone, fax and e-mail in order to exchange information and experience on DHF/DSS case management.
Impact of improved DHF/DSS case management Improvement in the case management of DHF/DSS patients has had a dramatic effect on the case-fatality rate (CFR) in Southern Viet Nam over the last 20 years.
At the Children’s Hospital N.1, Ho Chi Minh City, from 1975 to1981, there were
1,143 deaths among a total of 29,397 DHF/DSS cases recording a CFR of 3.88%(7). After the implementation of the improved case management system at the Department of Dengue Haemorrhagic Fever, 29,416 DHF/DSS patients have been treated [among them there were 8,103 (27.5%) patients with DSS], of whom 73 cases died, thus reducing the CFR to as low as 0.24% during the period from 1991 to 2002. Meanwhile, the CFR of DSS patients was brought down significantly from 12.5% in 1975 to 5.4% in 1986, and to 0.5-1.4% during the period 1991 to 2002.
In Southern Viet Nam, 25,289 DHF/DSS patients with 2,090 deaths were reported from 1964 to 1974, recording a high CFR of 8.26%(1). Since 1976 up to now, outbreaks of DHF have occurred with thousands of cases reported each year. In the peak outbreak of DHF in 1998, there were 119,429 cases of DHF with 342 deaths reported in 19 provinces of Southern Viet Nam. With the improvement of case management of DHF/DSS patients at all levels of the health care system, the CFR of DHF has been reduced significantly to 0.26% during 1996-2001; and that of DSS to 1.44- 2% during 1999-2001(2).
References 1. Bui Dai. Dengue haemorrhagic fever. 2nd edition,
Publishing House of Medicine, Hanoi, 1999 (in Viet Namese).
2. Pasteur Institute, Ho Chi Minh City. Report and Plan of National Target DHF Control Programme in Southern Viet Nam in 2002, Ho Chi Minh City, January, 2002 (in Viet Namese).
3. Nguyen Trong Lan, Nguyen Thanh Hung, Do Quang Ha, Bui Thi Mai Phuong, Le Bich Lien, Luong Anh Tuan, Vu Thi Que Huong, Lu Thi Minh Hieu, Tieu Ngoc Tran, Le Thi Cam and Nguyen Anh Tuan. Treatment of dengue haemorrhagic fever at Children's Hospital N.1, Ho Chi Minh City, 1991-1996. Dengue Bulletin, 1997, 22: 150-161.
4. World Health Organization. Dengue haemorrhagic fever: Diagnosis, treatment, prevention and control. 2nd edition. Geneva: WHO, 1997.
5. Nimmannitya S. Dengue haemorrhagic fever: Diagnosis and management. In: Gubler DJ, Kuno G, editors. Dengue and dengue haemorrhagic fever. Wallingford, UK: CAB International, 1997: 133-146.
6. Nguyen Thanh Hung and Nguyen Trong Lan. Treatment of dengue haemorrhagic fever at Children's Hospital N.1, Ho Chi Minh City, 1991-2000. Medical Journal HCM City, 2001, 3: 149-152 (in Viet Namese).
7. Nguyen Thi Ngoc Anh. Dengue haemorrhagic fever: Early diagnosis and correct treatment. Reports on DHF in Children’s Hospital N.1, Ho Chi Minh City, September, 1982 (in Viet Namese).
Dengue Bulletin – Vol 27, 2003 149
Community Mobilization in Aedes aegypti Control Programme by Source Reduction in
Peri-Urban District of Lautoka, Viti Levu, Fiji Islands by
Arun K Raju#
National Vector Control Unit, National Centre for Scientific Services on Virology & Vector Borne Diseases, Ministry of Health, Private Mail Bag, Tamavua, Suva, Fiji Islands
Abstract
A larval source reduction campaign in Fiji was evaluated using the vector surveillance programme of the Ministry of Health. Due to inadequate solid waste disposal, used tyres, trash and drums used for storage of water provide numerous breeding sites for dengue vectors because of intermittent water supply. With modest support from the Environmental Health Unit of the Ministry of Health, Fijian communities significantly reduced Aedes aegypti breeding sites. Prior to the intervention, 51% of tyres and 21% of drums contained Aedes aegypti. With active community participation, the number of container habitats for Aedes aegypti was significantly reduced during the nine months. As a result, Breteau indices dropped from 29 in January to below five in nine months after the start of the programme. Dengue and vector control programmes must convince people to remove breeding habitats or, alternatively, to prevent Aedes aegypti from having access to water containers and other household items that are its potential breeding sites.
Keywords: Aedes aegypti, used tyres, drums, community participation, Fiji Islands.
# For correspondence: [email protected]
Introduction Dengue haemorrhagic fever (DHF) first appeared in Fiji in 1975, with subsequent outbreaks occurring every 10 years (e.g. 1979-80, 1989-90 and 1997-98). The 1997-98 outbreak of dengue fever (DF) resulted in more than 24,000 reported cases and 13 deaths, when the disease also spread to rural areas(1). Fiji is unique because it is the only country in the world where four-to-six species of mosquitoes may transmit the
dengue viruses. The primary vector is Aedes aegypti, but secondary vectors include Aedes albopictus, Aedes polynesiensis, Aedes pseudoscutellaris, Aedes horrescens and Aedes rotumae (in Rotuma only)(1).
Aedes aegypti is recognized as the most efficient vector globally due to its close association with humans and its highly domestic breeding habitats in artificial containers in and around houses, thereby putting human populations at risk of disease transmission.

Community Mobilization in Aedes aegypti Control Programme in Fiji Islands
150 Dengue Bulletin – Vol 27, 2003
In Fiji, for vector control, the primary emphasis is on “source reduction” through basic environmental sanitation, health promotion and community participation, backed by law enforcement. Chemical control is not used for routine dengue prevention in Fiji, but is reserved for the control of epidemics.
Aedes aegypti breeds in tyres, drums, plant containers and flower vases, miscellaneous containers such as tin cans, plastic food containers and, to a lesser degree, in coconut shells and old motor parts and, least of all, in ground pools(2).
However, studies in Fiji have shown that tyres and drums comprise 10-20% of the total containers found positive for Aedes larvae and are responsible for 83-99% of the adult Aedes mosquito production(3). The present study includes the results of community-based “source reduction” campaign to suppress Aedes aegypti population.
Study area
The dengue risk transmission or target areas included the Saweni, Lawaki, Viriba, and Tomuka squatter and Velovelo settlements with a population of approximately 17,000 in the peri-urban district of Lautoka, Viti Levu, Fiji Islands.
Methodology
Entomological surveillance
Health inspectors in all urban and rural areas carried out monthly Aedes larval surveys.
During each survey, at least 100 premises were inspected, which included residential, commercial and industrial zones in dengue transmission risk areas (target areas). Searches were conducted both indoors and outdoors within a 15-metre perimeter of house fences.
Nine monthly larval surveys were carried out from January to September 2002. Different types of wet containers, tyres, drums, tins, plant containers, etc., were inspected for Aedes breeding using the 10 immatures per container method.
Immatures were collected from water-filled containers at each house and put into a labelled vial with (Macgregor’s) preserving solution and brought to the laboratory. The larvae collected from these sources were mounted on slides for species identification using the keys of Belkin(4).
Survey results were expressed as the following indices:
• Premises Index (PI): The percent-age of houses positive for larvae;
• Container Index (CI): The percent-age of water-filled containers positive for larvae;
• Breteau Index (BI): The number of mosquito positive containers per 100 houses.
Source reduction campaign
The elimination of mosquito breeding sources constitutes the main environmental mosquito control measures used in Fiji. Health inspectors are authorized to enter and inspect premises for mosquito breeding

Community Mobilization in Aedes aegypti Control Programme in Fiji Islands
Dengue Bulletin – Vol 27, 2003 151
and harbourage and to advise on the elimination and destruction of breeding sites.
Health inspectors are responsible for conducting community awareness and participate in source reduction activities. This led to the following initiative in the Lautoka peri-urban district.
Dengue and its vector control messages were delivered to the communities through radio broadcasts and during personal visits to homes, with major emphasis on the creation of awareness in the communities about the serious threat of DF/DHF to children and families. Communities were trained for a planned intervention for the elimination of breeding foci.
Community awareness was conducted from February till mid-March. During this period, communities protected the potential breeding waters from ovipositing females and arranged for the elimination of mosquito breeding habitats. The communities also collected solid waste and trash in and around their houses and placed these along the roadside for collection and disposal from 18 to 21 March 2002. Loading machines and trucks were used to cart the solid waste to the dump site under the supervision of health inspectors.
Results A summary of the number of Aedes aegypti breeding sites by types of containers as detected in the peri-urban district of Lautoka, Viti Levu, Fiji Islands, from January
to September 2002 are given in Table 1. The most abundant breeding sites were tyres and drums. Tins, flower vases, plant containers, shells and others (discarded household equipment, motor parts, etc.) were of secondary importance.
The number of primary positive containers for Aedes aegypti was the highest from January to March which being the wet months during the study period (refer to climatological information in Figure 1). In January, tyres represented 51%, drums 21%, tins and others were 10% and 18%, respectively, of the total breeding sites positive for Aedes aegypti. There was a considerable reduction in the number of positive containers, especially tyres and drums, from March after the clean-up operation, but some of these containers (tyres and drums) remained positive till August.
The percentage of primary positive containers for Aedes albopictus also reduced significantly from 33% to 5% for tyres and from 42% to 8% for drums (Table 2).
The Breteau index (Figure 2) dropped from 29 in January to nil in September when Aedes aegypti breeding was almost eliminated. A similar observation was made for Aedes albopictus, when the Breteau index dropped significantly from 44 in January to 4 in September. All three mosquito indices (PI, CI and BI) were considerably lower after the clean-up operation in March and remained below 5 thereafter. In September, Aedes aegypti was not found in the larval survey.

Community Mobilization in Aedes aegypti Control Programme in Fiji Islands
152 Dengue Bulletin – Vol 27, 2003
Table 1. Containers commonly found positive for Aedes aegypti larvae in peri-urban district of Lautoka, Viti Levu, Fiji Islands, for January – September 2002
Primary breeding containers
Secondary breeding containers
Tyres Drums Tins Flower vase
Plant containers Shells Others Month
S P S P S P S P S P S P S P Jan 58 31 36 13 12 6 16 - 31 4 8 4 21 11 Feb 30 16 10 3 22 10 - - 24 9 3 - 20 3 Mar 36 11 22 4 47 9 5 1 13 2 9 - 23 4 Apr 22 8 25 6 6 1 29 - 6 3 4 - 8 6 May 16 8 7 - 13 5 - - 6 - - - 20 2 Jun 18 6 6 3 15 3 - - 2 1 - - 15 - Jul 16 5 20 4 10 - 4 - 22 1 5 - 14 1 Aug 16 5 23 2 1 1 3 - 5 - 1 - 6 2 Sep 22 - 24 - 4 - 4 - 7 - - - 6 - Tot 234 90 173 35 130 35 61 1 116 20 30 4 133 29 S = Wet containers searched. P = Containers found positive for Aedes aegypti larvae
Table 2. Containers commonly found positive for Aedes albopictus larvae in peri-urban district of Lautoka, Viti Levu, Fiji Islands, 2002
Primary breeding containers
Secondary breeding containers
Tyres Drums Tins Flower vase Plant containers Shells Others
Month
S P S P S P S P S P S P S P Jan 58 19 36 15 12 7 16 0 31 2 8 3 21 7 Feb 30 3 10 2 22 5 - 0 24 8 3 0 20 2 Mar 36 8 22 3 47 6 5 0 13 1 9 0 23 3 Apr 22 0 25 5 6 0 29 0 6 1 4 0 8 0 May 16 3 7 0 13 0 - 0 6 0 - 0 20 2 Jun 18 3 6 0 15 0 - 0 2 1 - 0 15 0 Jul 16 4 20 4 10 0 4 0 22 1 5 0 14 0 Aug 16 2 23 2 1 0 3 0 5 0 1 0 6 0 Sep 22 1 24 2 4 0 4 0 7 1 - 0 6 0 Total 234 43 173 33 130 18 61 0 116 15 30 3 133 14
S = Wet containers searched P = Containers found positive for Aedes albopictus larvae
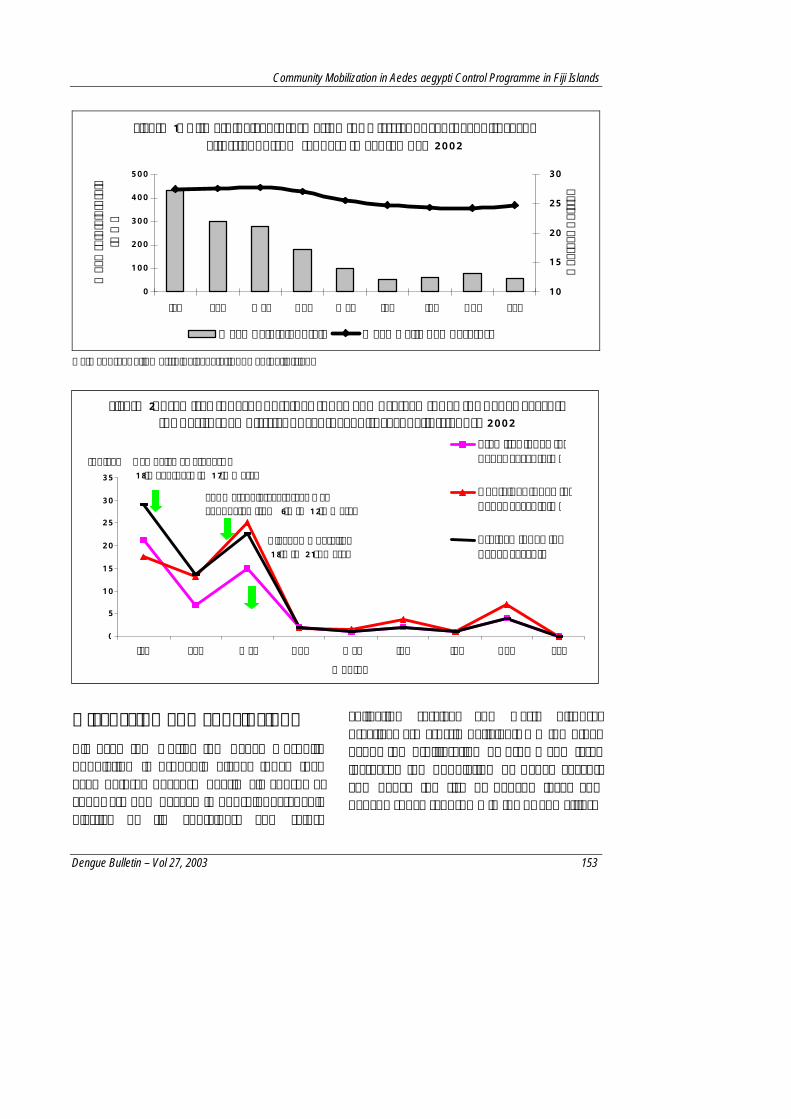
Community Mobilization in Aedes aegypti Control Programme in Fiji Islands
Dengue Bulletin – Vol 27, 2003 153
Figure 1. Climatological Information for District of Lautoka, Viti Levu, Fiji Island, from January to September 2002
0
100
200
300
400
500
Jan Feb Mar Apr May Jun Jul Aug Sep
Mea
n ra
infa
ll to
tals
(m
m)
10
15
20
25
30
Deg
rees
Cel
sius
Mean Rainfall Totals Mean Daily Temperature
Data Source: Fiji Metriological Station, Nadi, Fiji Island
0
5 10
15
20
25 30
35
Jan Feb Mar Apr May Jun Jul Aug Sep Months
Indices Premises Index for Aedes aegypti (%)
Container Index for Aedes aegypti (%)
Breteau Index for Aedes aegypti
Campaign awareness - 18th February to 17th March
Cleanup Operation 18th to 21st March
For March, larval survey was conducted from 6th to 12th March
Discussion and conclusions All over the world, the Aedes mosquito population is probably higher today than ever before, because nearly all consumer goods are now packed in non-biodegradable plastics or tin containers and refuse
collection services and waste disposal practices are grossly deficient. On the other hand, the proliferation of drums and tyres increases the population of Aedes aegypti and hence the risk of dengue fever and dengue shock syndrome in towns and cities.
Figure 2. Premises Index, Container Index and Breteau Index for Aedes aegypti for peri-urban district of Lautoka, Viti Levu, Fiji Islands, 2002

Community Mobilization in Aedes aegypti Control Programme in Fiji Islands
154 Dengue Bulletin – Vol 27, 2003
In Fiji, squatter settlements are growing in peri-urban areas and housing problems are becoming acute(5). Higher urban population densities, urban water storage practices and poor or non-existent mechanisms for waste water and solid waste disposal create numerous breeding sites for vectors. In the study community water storage drums remains a significant factor for oviposition, as there are no specific or regulated methods employed to cover them. The population normally covers drums with plastic or nylon sheeting to prevent oviposition. Other crude covers include corrugated iron sheets or wooden boards, which contributed to lower indices observed between April and August despite less rainfall at the conclusion of the programme. Regular visits of health inspectors and health awareness had created considerable awareness among populations to be more cautious about avoiding oviposition by mosquitoes. The intervention by the health officials in association with community participation had reduced the observed wet and dry containers, but was unable to clearly associate the change with the weather pattern. The community awareness programme in January 2002 was started to reduce the number of breeding containers. The Aedes aegypti control programme in Fiji aims to make people aware of the threat that dengue haemorrhagic fever poses to their health, and to educate them on how they can reduce this threat by either eliminating the domestic containers which harbour the mosquito larvae or by preventing mosquitoes from having access to water-holding containers for egg-laying that are used in or around houses.
In Fiji, automobile tyres discarded, stored or used around people’s homes provide perfect larval habitats for the dengue mosquito. It should be noted that water storage often occurs in the presence of piped water systems because of intermittent water supply and collected rainwater. House-owners are legally required to prevent mosquito breeding in Fiji. The numbers of drums breeding Aedes aegypti were reduced after community consultation and intervention messages. Recent KAP studies on dengue fever and dengue mosquitoes in Fiji suggested that to mobilize communities, campaigns must address community concerns. In addition, health inspectors must demonstrate the need to cover drums to prevent mosquito breeding, and they must also help communities to manage and destroy containers(6). Targeted source reduction is one way of selectively attacking the most important types of containers(7).
Dengue control programmes must include surveillance of mosquito populations to assess the effectiveness of source reduction campaigns, and targeted mosquito control measures. The success of any prevention programme depends on either convincing individuals to change their behaviour or changing the environment to remove factors that place individuals at risk of disease.
For dengue control activities, community education programmes may not be sufficient to generate sustainable behavioural change, unless other factors are taken into consideration as part of the overall strategy. In this peri-urban district, refuse collection was a key requirement for the control of larval production sites. Because of water shortage problems, there is a need to

Community Mobilization in Aedes aegypti Control Programme in Fiji Islands
Dengue Bulletin – Vol 27, 2003 155
design appropriate covers or biological control methods for water storage containers as an important component of a sustainable control programme. If community participation is viewed as a means to shift responsibility and costs from the government to residents without the provision of adequate services to support residents in their ability to carry out the recommended control measures, the prospects for sustainability may not be realistic.
Acknowledgements I am grateful to Ms Rupa Gordon, Vector Control Officer of the Department of Health, Lautoka, and her staff for consistency in mosquito surveillance and control measures that generated this data.
I would like to thank Dr Thomas R Burkot of CDC, Colorado, USA, for reviewing this manuscript.
References 1. Prakash G, Raju AK and Koroivueta. DF/DHF
Control in Fiji. Dengue Bulletin, 2001: 21-27.
2. Goettel MS, Toohey MK and Pillai JS. The urban mosquitoes of Suva, Fiji: Seasonal incidence and evaluation of environmental sanitation and ULV spraying for their control. Journal Trop Med Hyg, 1980, 83: 165-171.
3. Kay BH, Prakash G and Andre RG. Aedes albopictus and other Aedes (Stegomyia) species in Fiji. Journal of Am Mosq Control Assoc, 1995,11: 230-234.
4. Belkin JN. The Mosquitoes of the South Pacific. California: University of California Press. Volume 2, 1962: 1-5.
5. Government of Fiji (GOF)/United Nations Children’s Fund (UNICEF). A situation analysis of children and women in Fiji. Suva, Fiji: UNICEF, 1996, 41-42.
6. Secretariat of the Pacific Community. Rising to the challenge! A report of the first community-based study of knowledge, attitudes and practices regarding dengue fever and dengue mosquitoes in Fiji. Noumea: Secretariat of the Pacific Community, Pacific Regional Vector Borne Diseases Project, 1999.
7. Focks DA, Brenner RJ, Hayes J and Daniels E. Transmission thresholds for dengue in terms of Aedes aegypti pupae per person with discussion of their utility in source reduction efforts. Am J Trop Med Hyg, 2000, 62(1): 11-18.

156 Dengue Bulletin – Vol 27, 2003
Field Evaluation of Ovitraps Consociated with Grass Infusion and Bacillus thuringiensis var. israelensis to
determine Oviposition Rates of Aedes aegypti
by SRA Santos*, MAV Melo-Santos**, L Regis** and CMR Albuquerque*#
*Departamento de Zoologia Universidade Federal de Pernambuco, Mestrado em Biologia Animal – Av. Prof. Moraes Rego S/N, CEP 50.670-420, Recife, PE, Brazil
** Departamento de Entomologia, Centro de Pesquisas Aggeu Magalhães/FIOCRUZ, Recife, PE, Brazil
Abstract
The aim of this study was to evaluate the oviposition response of Aedes aegypti to ovitraps loaded with grass infusions and a larvicide based on Bacillus thuringiensis israelensis (Bti). The ovitraps consisted of a container of either tap water, 10% grass infusion or 30% grass infusion and Bti larvicide (0.18 mg/ml). Traps were placed in the field and paired with Bti-free controls. The oviposition response by Aedes aegypti mosquitoes was quantified using the Ovitrap Positivity Index (OPI) and the per cent proportion of eggs laid in each trap. The persistence of the Bti larvicide under these conditions was analysed over 15 days. The OPI response of paired Bti and control ovitraps was similar, irrespective of the treatment. Traps containing only tap water or 10% grass infusion were found to have a significantly higher number of eggs than those treated with Bti. The reverse was true for traps containing the 30% grass infusion and Bti, where the percentage of eggs laid was higher than in the control. A higher proportion of eggs were laid in traps containing 30% grass infusion and Bti than those with 10%+Bti. At the test dose of 0.18 mg/ml, over a period of 15 days, 100% of larvae were killed in all of the traps. The results demonstrate that the presence of Bti does not alter the choice of oviposition site; however, Bti may influence the quantity of eggs that are laid in proportion to infusion concentration. Since the larvicide remains effective for 15 days, ovitraps may be safely used in the field over an extended period.
Keywords: Ovitraps, grass infusion, Bacillus thuringiensis israelensis, Aedes aegypti, Brazil.
# For correspondence: [email protected]
Introduction The dengue endemicity in Brazil has led many workers to conduct studies on different aspects of the ecology of the vector
species Aedes aegypti. In the absence of any effective vaccine, interruption of viral transmission through vector control is the only option. To achieve this objective, information on vector prevalence is being

Oviposition Rates of Aedes aegypti in Bti –treated Ovitraps
Dengue Bulletin – Vol 27, 2003 157
collected and the types of breeding containers utilized by the species are being monitored through larval surveys which entail active search for breeding sites and laboratory identification of immature larval stages. This method is labour-intensive and is a poor indicator of measuring the vector population density.
In recent years, ovitrap surveys for monitoring the Aedes aegypti population have found greater acceptability, as these have been found to be sensitive even at times when vector densities are at low levels(1,2,3,4). These traps enable workers to establish the Ovitrap Positive Index (OPI) and the Egg Density Index (EDI) to indicate, respectively, the extent and intensity of the vector prevalence. This technique has been further improved by adding 'hay infusion' in different strengths to enhance its attractiveness to egg-laying females(2,5). This method not only yielded higher number of eggs, but its attractiveness remained unchanged despite seasonal variations(5).
The use of an insecticide-treated oviposition strip incorporated in an ovitrap was suggested by Zeichner and Perich(6), in order to make the trap lethal to both larvae and adult Aedes aegypti. However, this combination has limitations in areas where insecticide resistance is known. Since the existing populations of Aedes aegypti in Brazil are already resistant to chemical insecticides used for their control, this excludes the use of insecticide-treated ovitraps(7). On the other hand however, the use of the biological larvicide Bacillus thuringiensis var. israelensis (Bti), which is highly effective against Aedes aegypti larvae, would reduce the possibility of resistance
because of its highly specific mode of action(8). Besides, Bti is eco-friendly and safe to handle. In this study, the effect of Bti as a biological larvicide in ovitraps serving as oviposition sites for Aedes aegypti mosquitoes was analysed under field conditions. Although the ovitrap is a method that is operationally viable, if it remains in the field for more than the maximum of seven days, it becomes a potential breeding site by itself. Therefore, the persistence of Bti was also assessed over 15 days, with the objective of enabling the ovitrap to be used safely for a more prolonged period.
Materials and methods Study area
The study was carried out in the neighbourhood of Sucupira, in the city of Jaboatão dos Guararapes, Pernambuco, Brazil, from September to November 2001. The area consisted of 492 blocks and a total of 9,911 residences. The Aedes aegypti house index as determined during November 2001 for the specified area was 0.45%, as per data from the Public Health Department.
Ovitraps
Traps were adapted from the model described by Fay and Perry(9) (1965) and consisted of 500 ml black plastic pots, 15 cm tall by 12 cm wide. The oviposition substrate was a 12 x 2 cm strip of a wooden Eucatex pallet attached to the inside of the jar with a paperclip. A grass infusion of Eleusine indica (Poaceae) in concentrations of 10% and 30% was used to attract female mosquitoes (220
Oviposition Rates of Aedes aegypti in Bti –treated Ovitraps
158 Dengue Bulletin – Vol 27, 2003
ml/trap). The grass stock infusion was prepared by adding 30 g of grass to two litres of tap water and stagnated for seven days. A granular formulation of BtiΦ was used as the larvicide @ 40 mg per trap, thus giving a test dose of 0.18 mg/ml. Bti is a commercial preparation containing 0.2% of the active ingredient.
Effect of Bti on the choice of ovitrap as an oviposition site
To evaluate the effect of Bti on the Aedes aegypti oviposition response, pairs of ovitraps were placed in shaded areas of living quarters, under four different experimental conditions:
(1) Ovitrap containing tap water and Bti, and ovitrap containing tap water without Bti.
(2) Ovitrap containing 10% grass infusion with Bti and without Bti.
(3) Ovitrap containing 30% grass infusion with Bti and without Bti.
(4) Ovitrap containing 10% grass infusion and 30% grass infusion with Bti.
For the first three experimental groups, the ovitraps were placed adjacent to each other and remained in position for four days. In the fourth group, the ovitraps were placed two metres apart and remained there for 15 days. At the end of this period in the field, the ovitraps were transferred to the laboratory. Pallets were dried at room temperature (28±2°C; 70-90% RH) and the number of eggs counted.
Φ VectoBacG
Evaluation of the Bti-based larvicide used in the ovitraps
The efficacy and persistence of Bti larvicide used in the ovitraps was estimated from the number of hatched eggs per pallet compared to the presence of live fourth instar larvae, pupae and pupal exuvia observed in the ovitrap.
Statistical analysis
The effect of Bti on the choice of trap for oviposition was evaluated based on the OPI, expressed as the percentage of ovitraps positive for eggs from the total of number of traps examined (Number of ovitrap X 100 / Total ovitraps). The efficiency of ovitraps in egg-collection (EDI) was evaluated according to the average number of eggs laid per positive ovitrap for each treatment (Total number of eggs / Total positive ovitraps). The percentages were compared with the respective controls using the χ2 test for proportions.
Results Table 1 indicates the number of ovitraps used, their positivity and the total number of eggs of Aedes aegypti harvested under different experimental groups in the field. The following inferences have been drawn from these results:
(1) Effect of Bti on choice of ovitrap as oviposition site: There was no significant difference in OPIs between paired ovitraps with ordinary tap water (χ2 = 0.10; p= 0.751), 10% grass infusion (χ2= 0.04; p = 0.97) or 30% grass infusion (χ2= 0.0; p = 1.0) (Figure 1).

Oviposition Rates of Aedes aegypti in Bti –treated Ovitraps
Dengue Bulletin – Vol 27, 2003 159
0
10
20
30
40
50
60
70
1 2 3 4Treatment
OPI
Control group Test group
1 – Drinking water and drinking water+Bti 2 – 10% infusion and 10% infusion+Bti 3 – 30% infusion and 30% infusion+Bti 4 – 10% infusion+Bti and 30% infusion+Bti
With regard to the number of eggs deposited, accentuated differences were noted between the ovitraps of the same experimental group (Table 1).
Compared to ovitraps that contained Bti, there was an increase in the percentage of eggs collected in paired ovitraps
containing only tap water (χ2 = 99.56; p = 0.001) or 10% grass infusion (χ2 = 471; p > 0.001 (Figure 2)). In the ovitraps containing 30% grass infusion, however, the percentage of eggs (EDI) was significantly larger in the traps containing Bti (χ2 = 824.84; p> 0.001) (Figure 2) compared to the control.
0
10
20
30
40
50
60
70
1 2 3 4Treatment
EDI
Control group Test group
1 – Drinking water and drinking water+Bti 2 – 10% infusion and 10% infusion+Bti 3 – 30% infusion and 30% infusion+Bti 4 – 10% infusion+Bti and 30% infusion+Bti
Table 1. Number of ovitraps placed, positivity and total number of eggs of Aedes aegypti harvested under different experimental groups
No. of ovitraps Eggs/Ovitrap Experimental
group Treatment Total
Positive/ percent
Total no. of eggs Mean ± SD (variation)
1 Tap water Tap water+Bti
20 20
11 (55.0) 10 (50.0)
449 261
40,8 ± 8,4 (07 – 106) 26,1 ± 6,0 (03 – 69)
2 Infusion 10% Infusion 10%+Bti
12 12
9 (75.0) 8 (66.6)
1,764 962
196,0 ± 78,3 (15 – 732) 120,0 ± 53,0 (05 – 394)
3 Infusion 30% Infusion 30%+Bti
12 12
11 (91.6) 11 (91.6)
1,362 2,648
123,8 ± 22,6 (30 – 272) 240,7 ± 53,7 (22 – 630)
4 Infusion 10%+Bti Infusion 30%+Bti
40 40
37 (92.5) 33 (82.5)
3,456 5,263
93,4 ± 54,9 (01 – 315) 159,5 ± 52,7 (01 – 724)
Figure 1. Ovitrap Positivity Index (OPI) for Aedes aegypti under different
experimental groups
Figure 2. Egg Density Index (EDI) in Aedes aegypti ovitraps under different
experimental groups

Oviposition Rates of Aedes aegypti in Bti –treated Ovitraps
160 Dengue Bulletin – Vol 27, 2003
(2) Persistence of larvicide activity in the ovitraps: Of the total number of eggs collected (8,719) in the 80 ovitraps that remained in the field for 15 days, 57.1% had already hatched when examined in the laboratory. Neither live larvae, pupae, nor pupal exuvia were found, proving that the product continued to eliminate 100% of the larvae during the period of evaluation.
(3) Effect of infusion concentration on oviposition in ovitraps associated with Bti: A total of 5,263 eggs were harvested from the 40 ovitraps containing 30% grass infusion during the 15-day evaluation period, compared with 3,456 eggs harvested from the same number of ovitraps containing only 10% grass infusion (Table 1), when placed two metres apart from one another. These results are statistically significant (χ2 = 749.0; p < 0.001) and demonstrate that 1.5 times as many eggs were harvested from traps containing 30% grass infusion compared with traps containing 10% grass infusion.
Discussion The small difference in OPIs between traps with and without Bti suggests that the larvicide does not interfere in the choice of trap for oviposition by gravid Aedes aegypti females. Although the presence of Bti appears not to influence the choice of ovitrap as an oviposition site, the test results suggest that the larvicide does influence the number of eggs laid and that this effect may depend on the infusion concentration. It is possible that female mosquitoes are not able to detect the larvicide or a component of the test product when used with high infusion concentrations.
No previous studies have been performed combining Bti with grass infusions. Studies using dry grass infusions (hay infusion) alone as a mosquito attractant are extremely controversial. Reiter et al(5) (1991) noted significantly more Aedes aegypti eggs in traps containing 10% hay infusion compared with 100%. These authors suggest that whereas more concentrated infusions may attract females from further afield, less concentrated infusions are preferred as oviposition sites. Under similar experimental conditions but using a different species of grass, Chadee et al(1) noted quite different results. They found a similar number of eggs in all ovitraps tested, regardless of the concentration used (10%, 20%, 60% or 80%).
The fact that at the test dose of 0.18 mg/ml of Bti, it eliminated 100% of larvae for 15 days in traps containing infusions of 10% or 30%, demonstrates that the presence of rotting organic material in the suspension does not reduce its efficacy over this period. This permits it to be used in the field for longer than seven days, the average post-embryonic development time for Aedes aegypti mosquitoes, removing the real risk of transforming an ovitrap into a breeding site. The increased time for which an ovitrap can remain in the field could greatly reduce the operational cost of control programmes. The number of eggs collected may also increase. It is known, for example, that female Aedes aegypti mosquitoes prefer to lay their eggs in sites already containing eggs or larvae(10). The resultant metabolites from the bacterial growth within the ovitrap may also be a contributing factor for increased oviposition and ovitrap attractiveness(11).

Oviposition Rates of Aedes aegypti in Bti –treated Ovitraps
Dengue Bulletin – Vol 27, 2003 161
We believe that the intensive use of Bti ovitraps throughout the infested areas for a maximum of 15 days may be a useful tool in control programmes. If the traps serve as a permanent oviposition site, female mosquitoes will tend not to disperse in search of other breeding grounds. According to Reiter et al(12) (1995), control methods that reduce accessibility to breeding grounds result in increased dispersion of female mosquitoes and, consequently, to dissemination of any arbovirus they transmit. Another advantage of large-scale ovitrap use is that eggs are removed en masse. In the absence of traps, these eggs would be deposited in otherwise unmonitored breeding sites in the vicinity. The use of these traps may be particularly effective in the dry season in order to collect eggs. If these eggs are deposited in other sites, they could enter a period of dormancy of up to a year(13). As such, the systematic elimination of eggs associated with continued larval control programmes could result in a significant reduction in the Aedes aegypti population in the long run.
The results of this study demonstrate that the presence of Bti does not compromise the ovitrap performance in terms of its attractiveness for the female gravid mosquitoes, and that the traps can safely remain in the field for up to 15 days when used with Bti. The technical information generated from this study has since been passed to the Municipal Department of Health, Recife. Ovitraps with Bti are currently in use (2002) at strategic locations within the municipality, particularly in the cemeteries.
Acknowledgements Thanks are due to Dr Rod Chalk for his critical reading of the manuscript and helpful comments, and to Ulisses Montarroyos for statistical support. We thank the community of Sucupira for allowing house inspections during the experiments, and the inspection team for operational help.
References 1. Chadee DD, Lakhan A, Ramdath WR and Persad
RC. Oviposition response of Aedes aegypti to different concentrations of hay infusion in Trinidad, West Indies. Journal of the American Mosquito Control Association, 1993, 9(3): 346-348.
2. Rawlins SC, Martinez R, Wiltshire and Legall G. A comparison of surveillance systems for the dengue vector Aedes aegypti in Port of Spain, Trinidad. Journal of the American Mosquito Control Association, 1998, 14(2): 131-136.
3. Braga IA, Gomes AC, Nelson M, Mello RCG, Bergamaschi DP and Souza JMP. Comparação entre pesquisa larvária e armadilha de oviposição para detecção de Aedes aegypti. Revista Brasileira de Medicina Tropical, 2000, 33(4): 347-353.
4. Marques CCA, Marques GRAM, Brito M, Santos-Neto U, Ishibashi VC and Gomes FA. Estudo comparativo de eficácia de larvitrampas e ovitrampas para vigilância de vetores de dengue e febre amarela. Revista de Saúde Pública, 1993, 27(4):237-241.
5. Reiter P, Amador MA and Colon N. Enhancement of the CDC ovitrap with hay infusions for daily monitoring of Aedes aegypti populations. Journal of the American Mosquito Control Association, 1991, 7(1): 52-55.
6. Zeichner BC and Perich MJ. Laboratory testing of a lethal ovitrap for Aedes aegypti. Medical and Veterinary Entomology, 1991, 13: 234-238.

Oviposition Rates of Aedes aegypti in Bti –treated Ovitraps
162 Dengue Bulletin – Vol 27, 2003
7. Macoris MLG, Andrighetti MTM, Takaku L, Glasser CM, Garbeloto VC and Cirino VCB. Alteração de resposta de susceptibilidade de Aedes aegypti a inseticidas organofosforados em municípios do Estado de São Paulo, Brasil. Revista de Saúde Pública, 1999, 33(5): 521-522.
8. Gill SS, Cowles EA and Pietrantonio PV. The mode of action of Bacillus thuringiensis endotoxins. Annual Review of Entomology, 1992, 37: 615-636.
9. Fay RW and Perry AS. Laboratory studies of ovipositional preferences of Aedes aegypti. Mosquito News, 1965, 25: 276-281.
10. Allan SA and Kline DL. Larval rearing water and preexisting eggs influence oviposition by Aedes aegypti and Aedes albopictus (Diptera: Culicidae). Journal of Medical Entomology, 1998, 35(6): 943-947.
11. Benzon GL and Apperson CS. Reexamination of chemically mediated oviposition behavior in Aedes aegypti (L.) (Diptera: Culicidae). Journal of Medical Entomology, 1988, 25 (3): 158-164.
12. Reiter P, Amador MA, Anderson RA and Clark GG. Short report: Dispersal of Aedes aegypti in an urban area after blood feeding as demonstrated by rubidium-marked eggs. American Journal of Tropical Medicine and Hygiene, 1995, 52: 177-179.
13. Silva HHG and Silva IG. Influência do período de quiescência sobre o ciclo de vida de Aedes aegypti (Linnaeus, 1762) (Diptera: Culicidae) em condições de laboratório. Revista da Sociedade Brasileira de Medicina Tropical, 1999, 32 (4): 349-355.

Dengue Bulletin – Vol 27, 2003 163
Impact of Intervention Measures on DF/DHF Cases and Aedes aegypti Indices in Delhi, India: An Update, 2001
by Rakesh Katyal*, Kaushal Kumar*, Kuldip Singh Gill* and RS Sharma**
*National Institute of Communicable Diseases, 22 Shamnath Marg, Delhi – 110054, India **National Anti-Malaria Programme, 22 Shamnath Marg, Delhi – 110054, India
Abstract
Health education of communities on source reduction of Aedes aegypti in houses and offices, both in the government and private sectors, supplemented by legislative actions by municipal health authorities resulted in a remarkable decline in the incidence of DF/DHF in Delhi from 10,252 dengue cases and 423 deaths in 1996 to 180 cases and two deaths in 2000. Similarly, the annual House Index showed a decline from 16.1% in 1996 to 5.3% in 2000. However, the increasing trend of cases in 2001 (322) and deaths (3), inspite of declining house index in 2001 (4.2%) indicated that in Delhi, DF/DHF is a local/focal phenomenon and falling house index at macro level has no predictive value. Prevention requires local actions for control of DF/DHF in identified disease foci.
Keywords: DF/DHF, Aedes aegypti, health education, legislative measures, Delhi.
Introduction In India, DF/DHF outbreaks have been reported in various parts of the country during the last four decades(1). Delhi has been endemic for DF/DHF for quite some time now and still maintains high vulnerability due the high influx of international tourist traffic into the metropolis and the extensive breeding potential of Aedes aegypti(2). Delhi recorded epidemics of dengue fever during the years 1967, 1970, 1982, 1988, 1991, 1992 and 1996(1,3). During the 1988 outbreak of DF/DHF, about 33% mortality was reported among children admitted in a hospital(4),
while during 1996,
10,252 cases were hospitalized and 423 deaths recorded(3). This epidemic peaked in September when an Aedes aegypti larval House Index of 43.70% was recorded. Since then, regular
monitoring of larval density of Aedes aegypti and dengue cases is in place to study the trends and to prevent any recurrence of an outbreak. The findings of the study period 1996-2001 are presented in this paper.
Methodology Larval searches for Aedes aegypti were made by an entomological survey team from the National Institute of Communicable Diseases, Delhi, in some sentinel localities of Delhi as per the standard techniques(5). House Index (HI), Container Index (CI) and Breteau Index (BI) were calculated for each month. Data on DF/DHF cases admitted to various hospitals in the city that have been diagnosed as per the WHO guidelines and deaths attributed to DF/DHF are being monitored

Impact of Intervention Measures on DF/DHF in Delhi
164 Dengue Bulletin – Vol 27, 2003
by the National Anti-Malaria Programme as the nodal agency. The Municipal Corporation of Delhi (MCD) and the New Delhi Municipal Council (NDMC) are the implementing agencies for dengue control activities in their respective areas. Data on the implementation of legislative measures by way of notices issued and cases penalized by law for each year were also collected from two civic agencies.
Results and discussions Data on HI, CI and BI calculated for each year is presented in Table 1. HI data indicates that there
are two peaks of Aedes aegypti in Delhi. A smaller peak occurs in March/April and a larger peak in September/October. The smaller peak pertains to the dry season and is supported by domestic storage of water, while the larger peak builds up during monsoons (July-October) when domestic breeding extends to rainwater-filled containers in peri- and extra-domestic habitats. Transmission seems to be negligible during the dry season, but builds up during the monsoon/post-monsoon season because of very favourable climatic conditions.
Table 1. Month-wise House Index, Container Index and Breteau Index in Delhi, 1996-2001
House Index (%) Container Index (%) Breteau Index Month
1996 1997 1998 1999 2000 2001 1996 1997 1998 1999 2000 2001 1996 1997 1998 1999 2000 2001
Jan 1.08 0.96 1.17 0.0 0.0 0.0 1.06 0.6 1.09 0.0 0.0 0.0 1.08 0.96 1.17 0 0 0
Feb 3.2 4.5 3.5 0.0 0.0 3.5 2.4 4.0 3.6 0.0 0.0 2.9 3.2 5.3 3.5 0 0 3.5
Mar 11.4 1.4 3.3 8.4 0.8 0.0 10.0 2.4 4.1 5.3 0.5 0.0 11.4 2.5 3.3 8.4 0.8 0
Apr 14.5 15.3 5.8 6.8 1.8 16.2 12.3 8.2 3.5 4.9 1.1 11.9 14.5 15.7 5.8 6.8 1.8 16.2
May 11.4 16.4 8.4 1.7 5.2 1.5 7.5 14.0 6.0 0.8 3.4 0.8 11.4 27.4 9.4 1.7 5.2 1.7
June 18.7 9.0 12.0 5.4 3.2 9.3 8.6 5.0 9.3 3.3 1.8 4.5 18.7 10.0 12 5.4 3.2 11.7
July 36.6 28.9 13.8 12.2 5.0 5.5 33.3 14.5 12.0 8.1 2.8 3.8 40.6 37.5 15.2 12.2 5.9 6.5
Aug 39.3 32.4 14.4 10.5 13.0 11.0 38.4 33.8 11.6 6.3 9.3 7.3 45.4 40.2 14.4 10.5 14.7 15.0
Sept 43.7 17.6 8.4 14.7 8.0 6.0 39.1 17.9 4.8 13.6 6.3 3.6 56.2 26.6 8.4 25.0 9.3 7.0
Oct 21.7 18.8 18.9 3.5 8.6 1.4 19.0 12.8 16.4 1.4 6.8 1.0 23.9 18.8 25.3 3.5 8.9 1.4
Nov 18.1 8.0 5.0 1.7 3.8 0.1 18.5 5.7 5.3 1.9 3.9 0.08 19.6 8.8 5 1.7 3.8 0.1
Dec 0.0 0.0 1.0 0.0 3.4 0.0 0 0.0 0.7 0.0 2.6 1.0 0 0 1 0 3.4 0
Annual 16.1 14.6 8.6 5.3 5.3 4.2 15.1 11.2 7.5 3.7 4.0 2.8 18.3 18.4 10.3 6.3 5.7 0
Figures in bold indicate maximum House Index in the year.Dengue cases and deaths along with Aedes
aegypti HI are presented in Figure 1. It is apparent that DF/DHF cases and deaths have substantially declined from 10,252 cases and 423 deaths in 1996 to 180 cases and two deaths in 2000.
Similarly, the annual HI declined from 16.1% in 1996 to 5.3% in 2000. BI and CI also showed a similar decline. However, during 2001, an increasing trend of cases was observed (322 cases and three deaths) inspite of a further declining

Impact of Intervention Measures on DF/DHF in Delhi
Dengue Bulletin – Vol 27, 2003 165
trend of HI (4.2%). This means that transmission of DF/DHF is a local/focal phenomenon and falling HI at macro level has no predictive value. Preventive actions at local level are essential for control of DF/DHF in identified disease foci. The month-wise incidence of cases and deaths during 2001 is given in Table 2. It is apparent that cases start building up during the post-monsoon months, i.e.
September-November, with maximum cases recorded during the month of October 2001. The age- and sex-wise distribution of cases during 2001 is shown in Table 3. The most affected group was of males above 14 years of age. Male predominance may indicate more transmission at work sites.
Figure 1. Dengue/DHF cases and deaths with Aedes aegypti index in Delhi from 1996 to 2001
273 333
168 180
322423
1
5
2 23
16.10%
14.60%
8.60%
5.30%
4.20%
5.30%
1
10
100
1,000
10,000
No.
of c
ases
and
dea
ths
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Years
Ann
ual h
ouse
inde
x
Cases Deaths Annual House Index
1996 1997 1998 1999 2000 2001
Table 2. Month-wise DF/DHF cases and deaths recorded in Delhi hospitals during 2001
Cases Month
Dengue DHF Total Deaths
January 0 0 0 0
February 0 0 0 0
March 0 0 0 0
April 1 0 1 0
May 0 0 0 0

Impact of Intervention Measures on DF/DHF in Delhi
166 Dengue Bulletin – Vol 27, 2003
June 0 0 0 0
July 2 0 2 0
August 2 1 3 1
September 26 0 26 0
October 154 1 155 1
November 111 1 112 1
December 23 0 23 0
Total 319 3 322 3
Table 3. Age- and sex-wise DF/DHF cases recorded in Delhi during 2001
Male Female Age*
DF DHF DF DHF Total
0–11 months 1 0 2 0 3
11–23 months 0 0 2 0 2
2–4 years 10 0 5 0 15
5–9 years 31 1 13 0 45
10–14 years 29 1 18 0 48
>14 years 155 1 50 0 206
Total 226 3 90 0 319
* Age of 3 cases not known
The decline in the density of the vector mosquito and fever cases is due to widespread health education imparted to communities through
wall slogans, posters, television and radio. Health staff undertaking larval surveys also interacted with communities and stressed on the need to empty containers holding water, particularly water evaporation coolers, on a weekly basis. The impact of health education was further supplemented by the implementation of legislative measures by municipal health authorities. This was evident from the increasing number of legal notices issued to owners of premises where the breeding of Aedes aegypti was detected and the number of prosecutions made. Legal notices served and prosecutions made during 1999, 2000 and 2001 were 1,579, 14,130 and 22,947 and 4,884, 3,762 and 8,689 respectively. Office premises in both the government and private sectors were also penalized for breeding Aedes aegypti. Regular monitoring of the situation made officers and staff working in government and private offices more vigilant in keeping their premises free of Aedes breeding.
Thus, it can be concluded that DF/DHF in Delhi is a local/focal phenomenon which emphasizes the need for identification of such potential disease foci. Prevention and control by health education and supported by strict legislative measures at local level can help in lowering the risk of DF/DHF. For detection of Aedes aegypti foci, new surveillance tools at micro level are required to be of any predictive value.
References
1. Yadava RL and Narsimham MVVL. Dengue/dengue haemorrhagic fever and its control in India. Dengue Newsletter, 1992, 17: 3-8.
2. Kalra NL, Kaul SM and Rastogi RM. Prevalence of Aedes aegypti and Aedes albopictus - Vectors of dengue and dengue haemorrhagic fever in north, north–east and central India. Dengue Bulletin, 1997, 21: 84-92.
3. Kaul SM, Sharma RS, Sharma SN, Panigrahi N, Phukan PK and Shiv Lal. Preventing dengue and DHF: The role of entomological surveillance. J Comm Dis, 1998, 30: 187-192.

Impact of Intervention Measures on DF/DHF in Delhi
Dengue Bulletin – Vol 27, 2003 167
4. Kabra SK, Verma IC, Arora NL, Jain V and Kalra V. Dengue haemorrhagic fever in children in Delhi. Bull WHO, 1992, 45: 105-108.
5. Katyal R, Gill KS, and Kumar K. Seasonal variations in Aedes aegypti population in Delhi, India. Dengue Bulletin, 1996, 20: 78-81.

168 Dengue Bulletin – Vol 27, 2003
Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
by Zeev Wiesman# and Bishnu P Chapagain
The Institutes for Applied Research, Ben Gurion University of the Negev, P.O. Box 653, Beer-Sheva 84105, Israel
Abstract
Quillaja saponaria is a South American saponin-producing plant and the Balanites aegyptiaca is an African - Asian saponin-producing plant. The efficacy of these two plant sources of natural saponins for the control of Aedes aegypti and Culex pipiens was studied in laboratory.
The data showed that extracts of these two natural saponin plant sources can be used for an efficient bioactive preparation in Aedes aegypti and Culex pipiens mosquito control.
Due to the fact that saponins are efficient in mosquito control, safe to mammals and available in high concentrations in many plant species all over the world, the cost of intensive use of saponin plant extract preparations should be relatively low and affordable to poor communities in the world.
Keywords: Aedes aegypti, Culex pipiens, dengue fever, West Nile virus, Balanites aegyptiaca, Quillaja saponaria, Saponin.
# For correspondence: [email protected]
Introduction
Aedes aegypti is the principal vector of dengue fever and dengue haemorrhagic fever. It infects more than 100 million people every year in more than 110 countries in the tropics(1). The regions of the Americas, Africa and South-East Asia are the most affected areas. Children are the most vulnerable to dengue infection and 95% of all dengue cases are those under 15 years of age.
Culex pipiens (northern house mosquito) is the vector of the West Nile virus (WNV) that causes encephalitis or meningitis. Generally, people over the age of
50 years are at greater risk to serious illness when infected with WNV. The disease affects the brain tissue and the most serious of the cases can result in permanent neurological damage and even be fatal(2). WNV is distributed throughout Africa, the Middle East, and the southern temperate and tropical Eurasia. It was recently introduced into North America as well(3).
Since there are no vaccines for these two arbovirus diseases, vector control is the only option available for reducing the morbidity. The most widely-used vector intervention methods are insecticide-based. Insecticides are generally chemical agents,

Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
Dengue Bulletin – Vol 27, 2003 169
which are expensive and harmful to the environment as well as to humans. This study reflects a broad international interest in finding eco-friendly natural systems for vector control. Our research focuses on insect control using saponins.
Saponins are high molecular weight glycosylated plant secondary metabolites, consisting of a sugar moiety linked to a triterpene or steroid aglycone(4). Detergent properties are the typical characteristics of saponins. They produce stable foam when dissolved in water, which is why some saponin-containing plants have been used as soaps for hundreds of years. Saponin-containing plants are used as folk medicines, especially in Asia, and are intensively used in food, veterinary and medical industries(5). The pesticidal activity of saponins has long been reported(6). Saponin-glycosides are very toxic to cold-blooded organisms, but apparently not to mammals(5,7). Plant extracts containing a high percentage of saponins are commonly used in Africa to treat water supplies and wells contaminated with disease vectors; after treatment, the water is safe for human drinking(7). The following saponin-containing plants have been exploited for the industrial production of saponins: horse chestnuts (Aesculus), climbing ivy (Hedera), peas (Pisum), cowslip (Primula), soapbark (Quillaja), soapwort (Saponaria), sugar beet (Beta) and balanites (Balanites aegyptiaca)(5,7).
In this study, we demonstrate the efficacy of two plant sources (Quillaja saponaria and Balanites aegyptiaca) of natural saponins for the control of Aedes aegypti and Culex pipiens. Quillaja saponaria is a large evergreen tree with shiny, leathery leaves and a thick bark which is native to Peru and the arid region of Chile(8) while
Balanites aegyptiaca is a spiny evergreen tree about 6-10 metres in height which is found in the drier regions of Africa, the Arabian peninsula, India and Myanmar(7). Our aim is to find an efficient, safe and low-cost mosquito control system that might be suitable for a wide range of communities most affected by these disease vectors.
Materials and methods
Saponin sources
We tested a commercial saponin mixture extracted from quillaja bark (S7900, Sigma, USA) containing quillaic acid, a triterpene, as its main sapogenin. We also used a methanol extract of balanites fruit mesocarp, which contains steroid saponins. Both extracts were tested against larvae of Aedes aegypti and Culex pipiens. The sapogenin content was not less than 10% as quoted by the suppliers for quillaja and about 4% for balanites extract(9).
Larvicidal bioassay
Eggs of laboratory-grown Aedes aegypti and Culex pipiens were hatched in tap water in a growth chamber with a 16-hour photoperiod, at a temperature of 25 ± 3°C. Twenty to twenty-five larvae at late third or early fourth instars were placed into 150-ml disposable plastic cups containing 100 ml of tap water together with a water-soluble saponin solution (1,000, 500, and 0 mg/L extract in the quillaja saponin experiment and 1000 and 0 mg/L extract for the balanites saponin experiment) in three replicates. During the experiments, treated and control (0 mg/L extract) cups were examined every 2, 3, 6, 7, 11 and 14 days and the number of live larvae or adults counted. The data are presented in both
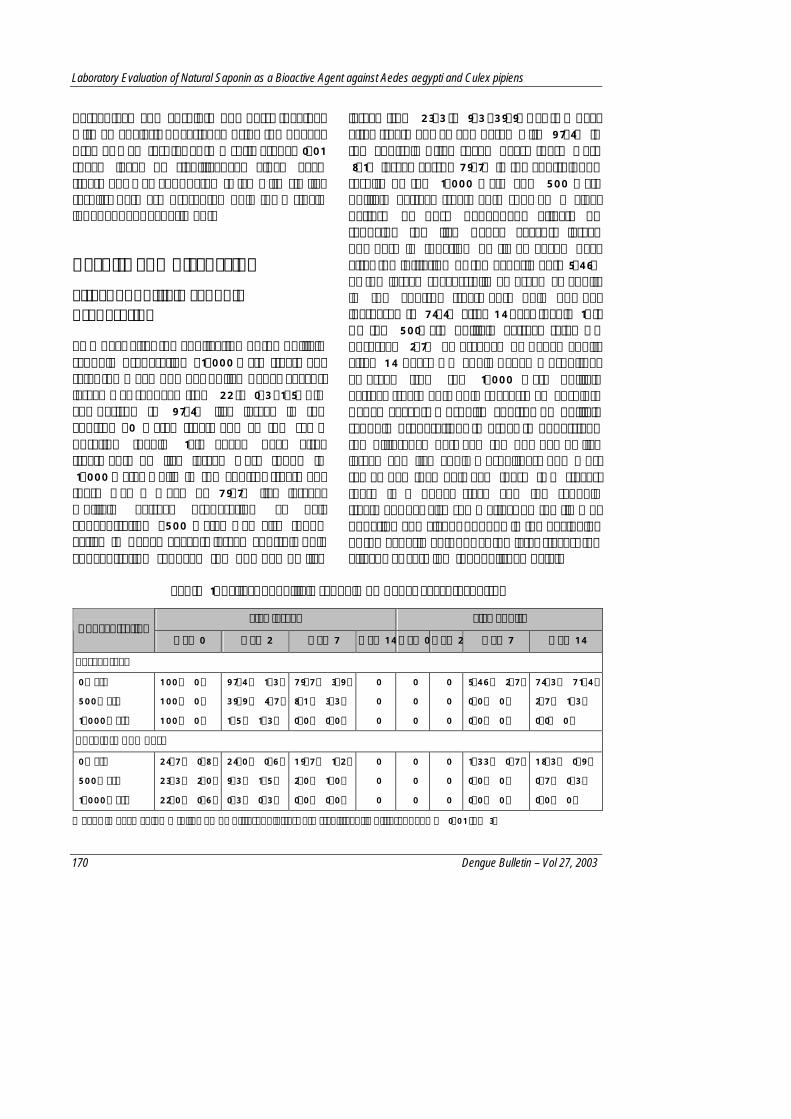
Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
170 Dengue Bulletin – Vol 27, 2003
percentage and absolute numbers, together with an analysis of variance using the Tukey-Kramer HSD test (SAS, JMP software) at 0.01 space level of significance. Since each treatment was conducted twice with similar results, data are presented only for a single independent experiment.
Results and discussion
Effect of quillaja saponin preparation
Two days after the application of the quillaja saponin preparation (1,000 mg/L treatment rate) the mean number of live Aedes aegypti larvae was reduced from 22 to 0.3 (1.5%) in comparison to 97.4% live larvae in the control (0 mg/L) treatment at the same duration (Table 1a). Seven days after treatment, no live larvae were found in 1,000 mg/L, while in the control treatment there was a mean of 79.7% live larvae. Quillaja extract preparation at half concentration (500 mg/L) was also found active in Aedes aegypti larvae control. This concentration reduced the number of live
larvae from 23.3 to 9.3 (39.9%) at two days after treatment as compared with 97.4% in the control. After seven days, there were 8.1% larvae versus 79.7% in the control. The results of the 1,000 mg/L and 500 mg/L quillaja extract treatments showed a clear pattern of dose dependent effects on reducing the live Aedes aegypti larvae numbers in function of time. Seven days after the initiation of the experiment, 5.46% of the larvae successfully emerged as adults in the control treatment. This number increased to 74.4% after 14 days (Table 1A). At the 500mg/L quillaja extract rate, we observed 2.7% emergence of Aedes adults after 14 days. No adult Aedes mosquitoes emerged from the 1,000 mg/L quillaja extract treatment. This suggests an absolute Aedes aegypti mosquito control by quillaja saponin preparation. In order to understand the difference between the number of live larvae and live adult mosquitoes, one must remember that between these two stages, there is a pupal stage and the saponin treatment has also some effect on the time of pupation and vigour of pupa in the beginning of the experiment, but at the later stages, the effect was very low (unpublished data).
Table 1A. Effect of quillaja saponin on Aedes aegypti control
Live larvae Live adults Concentration
Day 0 Day 2 Day 7 Day 14 Day 0 Day 2 Day 7 Day 14
Percentage
0 mg/L
500 mg/L
1,000 mg/L
100 ± 0 a
100 ± 0 a
100 ± 0 a
97.4 ± 1.3 a
39.9 ± 4.7 b
1.5 ± 1.3 c
79.7 ± 3.9 a
8.1 ± 3.3 b
0.0 ± 0.0 c
0
0
0
0
0
0
0
0
0
5.46 ± 2.7 a
0.0 ± 0 a
0.0 ± 0 a
74.3 ± 71.4 a
2.7 ± 1.3 b
0.0± 0 b
Absolute numbers
0 mg/L
500 mg/L
1,000 mg/L
24.7 ± 0.8 a
23.3 ± 2.0 a
22.0 ± 0.6 a
24.0 ± 0.6 a
9.3 ± 1.5 b
0.3 ± 0.3 c
19.7 ± 1.2 a
2.0 ± 1.0 b
0.0 ± 0.0 c
0
0
0
0
0
0
0
0
0
1.33 ± 0.7 a
0.0 ± 0 a
0.0 ± 0 a
18.3 ± 0.9 a
0.7 ± 0.3 b
0.0 ± 0 b
Means in each column followed by different letters are significantly different at P = 0.01 (n=3)

Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
Dengue Bulletin – Vol 27, 2003 171
A similar effect of quillaja saponin preparation on Culex pipiens mosquito control was also obtained (Table 1B). The higher concentration (1,000 mg/L) of quillaja saponin extract provided an absolute control of adult Culex pipiens emergence during the 14 days of the experiment. The lower concentration (500 mg/L) reduced the mean number of live
larvae from 20 to 15 at two days. After seven days, the mean number of live larvae dropped to 6.3. In this treatment, the number of emerged adults averaged to one out of 20 (5%) after 14 days. In the control treatment at seven days, 50% live larvae were recorded and after 14 days, the emerged adults reached 13.3 (66.5%) out of 20.
Table 1B. Effect of quillaja saponin on Culex pipiens control
Live larvae Live adults Concentration
Day 0 Day 2 Day 7 Day 14 Day 0 Day 2 Day 7 Day 14
Percentage
0 mg/L 100 ± 0 a 100 ± 1.3 a 50.0 ± 7.5 a 0 0 0 6.6 ± 3.5 a 66.5 ± 5.2 a
500 mg/L 100 ± 0 a 75 ± 4.7 b 31.7 ± 1.7 a 0 0 0 1.5 ± 1.5 a 5.0 ± 0.4 b
1,000 mg/L 100 ± 0 a 1.7 ± 1.7 c 0.0 ± 0.0 b 0 0 0 0.0 ± 0 a 0.0 ± 0 b
Absolute numbers
0 mg/L 20 ± 0 a 20.0 ± 0 a 10 ± 1.5 a 0 0 0 1.33 ± 0.9 a 13.3 ± 1.3 a
500 mg/L 20 ± 0 a 15 ± 0 b 6.3 ± 0.3 a 0 0 0 0.3 ± 0.3 a 1.0 ± 0.0 b
1,000 mg/L 20 ± 0 a 0.3 ± 0.3 c 0.0 ± 0.0 b 0 0 0 0.0 ± 0 a 0.0 ± 0 b
Means in each column followed by different letters are significantly different at P = 0.01 (n=3).
Effect of balanites saponin preparation
The second source of saponin we tested, a methanol extract of Balanites aegyptiaca fruit mesocarp, also showed an effective biocontrol of both Aedes aegypti and Culex pipiens mosquitoes (Table 2A and 2B). Three days after treatment, the number of live Aedes larvae was reduced in the balanites saponin preparation (1,000 mg/L) from 21 larvae to 2.3 (11%) in comparison to 96.7% live larvae in the control treatment (Table 2A). The percentage of adult mosquitoes
emerging after six and 11 days was 0% and 5%, respectively. In the control treatment, 85% of the larvae emerged as adult Aedes mosquitoes after 11 days.
The effect of balanites saponin extract on Culex pipiens was more moderate than on Aedes aegypti (Table 2b). A mean of 23.3% of the larvae were alive after both three and six days in comparison to 90% and 43.3% in the control, respectively. At the end of the study, a mean of 20% of the initially treated Culex larvae had reached the adult stages as compared with 83.3% in the control.

Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
172 Dengue Bulletin – Vol 27, 2003
Table 2A. Effect of blanites saponin on Aedes aegypti control
Live larvae Live adults Concentration
Day 0 Day 3 Day 6 Day 11 Day 0 Day 3 Day 6 Day 11
Percentage
0 mg/L 100 ± 0 a 96.7 ± 1.7 a 36.7 ± 4.4 a 0 0 0 21.6 ± 6.0 a 85 ± 2.9 a
1,000 mg/L 100 ± 0 a 2.9 ± 1.6 b 0.0 ± 0.0 b 0 0 0 0.0 ± 0 a 5.0 ± 2.8 b
Absolute numbers
0 mg/L 20 ± 0.8 a 19.3 ± 0.3 a 6.77 ± 0.8 a 0 0 0 4.3 ± 1.2 a 17.0 ± 0.6 a
1,000 mg/L 21 ± 0.6 a 2.3 ± 0.3 b 0.0 ± 0.0 b 0 0 0 0.0 ± 0 a 1.0 ± 0.6 b
Means in each column followed by different letters are significantly different at P = 0.01 (n=3).
Table 2B. Effect of balanites saponin on Culex pipiens control
Live larvae Live adults Concentration
Day 0 Day 3 Day 6 Day 11 Day 0 Day 3 Day 6 Day 11
Percentage
0 mg/L 100 ± 0 a 90 ± 5.8 a 43.3 ± 0.3 a 0 0 0 23.3 ± 3.3 a 83.3 ± 3.3 a
1,000 mg/L 100 ± 0 a 23.3 ± 3.3 b 23.3 ± 2.3 b 0 0 0 16.7 ± 6.6 a 20.0 ± 5.7 b
Absolute numbers
0 mg/L 10 ± 0 a 9.0 ± 0.6 a 4.3 ± 0.3 a 0 0 0 2.33 ±0.3 a 8.3 ± 0.3 a
1,000 mg/L 10 ± 0 a 2.3 ± 0.3 c 2.3 ± 0.3 b 0 0 0 1.7 ± 0.7 a 2.0 ± 0.6 b
Means in each column followed by different letters are significantly different at P = 0.01.
A moderate effect of mosquito control from balanites saponin preparation should be expected due to its lower content of saponin in comparison to the quillaja saponin preparation (as stated in Materials and methods). The result of 20% of the initial larvae emergence to the adult stage at the end of the experiment in Culex pipiens indicates that a higher concentration of balanites extract would be needed to make the control of Culex mosquitoes effective.
In a previous study, we demonstrated the effect of the quillaja saponin extract on larvae mortality(10). In this study, we focused on the effect on the survival of larvae and
adult mosquitoes of two sources of saponin: Quillaja saponaria representing South American saponin-producing plants and Balanites aegyptiaca, representing African and Asian saponin-producing plants. In both the South American and Afro-Asian sources, the plant material used for the preparation of the saponin is low cost and affordable for many communities. The data previously reported about the safe use of saponin plant extracts for mammals(5), together with their larvicidal effects(10,11) and common ethno-medicinal uses in many areas of the world, make saponin plant preparations very good candidates for practical use in the control of dengue and WNV vectors.

Laboratory Evaluation of Natural Saponin as a Bioactive Agent against Aedes aegypti and Culex pipiens
Dengue Bulletin – Vol 27, 2003 173
Conclusions The following conclusions can be drawn based on the experimental results demonstrated in the present study:
(1) Various saponin sources can be used for efficient bioactive preparation in Aedes aegypti and Culex pipiens mosquito control.
(2) Due to the fact that saponins are effective in mosquito control, safe to mammals and available in high concentrations in many plant species all over the world, the cost
of intensive use of saponin plant extract preparations should be relatively low and affordable to poor communities in many parts of the world.
Acknowledgments The authors thank Dr Dan Pelach, Dr Zana Abramovich, Mr Steven Maranz and Dr Arie Markus for their valuable suggestions and technical help. Thanks are also due to the Dibner Foundation (Wilton, Connecticut) for supporting this study.
References1. Halstead SB. Global Perspective on Dengue
Research. Dengue Bulletin, 2000, 24: 77-82.
2. Hubalek Z and Halouzka J. West Nile Fever- A reemerging mosquito-borne viral disease in Europe. Emerging Infectious Diseases, 1999, 5: 650-653.
3. Campbell GL, Martin AA, Lanciotti RS and Gubler D. West Nile Virus. The Lancet Infectious Diseases, 2002, 2: 519-529.
4. Price KR, Johnson IT and Fenwick GR. The chemistry and biological significance of saponins in foods and feeding stuffs. C R Food Sci Nutr, 1987, 26: 127-135.
5. Hostettmann K and Marston A. Saponins (Chemistry and pharmacology of natural products). 1995, University Press, Cambridge.
6. Irvine FR. Woody plants of Ghana with special reference to their uses. 1961, Oxford University Press, London, UK.
7. Hall JB and Walker DH. Balanites aegyptiaca Del.- A Monograph. 1991, School of Agricultural and Forest Science, University of Wales, Banger, UK.
8. Leung AY. Encyclopedia of Common Natural Ingredients Used in Foods, Drugs, and Cosmetics, 1980. Weily, NY.
9. Neuwinger HD. Poisons and Drugs - African Ethnobotany, 1996. Chapman & Hall Publishers.
10. Pelah D, Abramovich Z, Markus A and Wiesman Z. The use of commercial saponin from Quillaja saponaria bark as a natural larvicidal agent against Aedes aegypti and Culex pipiens. J Ethnopharmacol, 2000, 81: 407-409.
11. Zarroug IMA, Nugud AD, Bashir AK and Mageed AA. Balanites aegyptiaca as a mosquito larvicide. International Journal Crude Drug Research, 1990, 28: 267-271.

174 Dengue Bulletin – Vol 27, 2003
The Impact of Health Education on Mother’s Knowledge, Attitude and Practice (KAP) of
Dengue Haemorrhagic FeverΨ
by
Tran Tan Tram*, Nguyen Thi Ngoc Anh*, Nguyen Thanh Hung*#, Nguyen Trong Lan*, Le Thi Cam*, Nguyen Phuoc Chuong*, Le Tri*, Lise Fonsmark**, Anja Poulsen** and Erik Deichmann Heegaard**
* Directorate, Department of Dengue Haemorrhagic Fever and the Project Office, Children’s Hospital N.1, 341 Su Van Hanh St., Dist 10, Ho Chi Minh City, Viet Nam
**Departments of Intensive Care, Paediatrics, and Clinical Microbiology, University State Hospital, Rigshospitalet, Copenhagen, Denmark
Abstract
A mother’s knowledge, attitude and practice (KAP) study before and after health education of dengue haemorrhagic fever (DHF) was carried out in four communes in Southern Viet Nam. The study showed that health education had made a strong impact on the mothers’ KAP of DHF. The KAP of mothers (how to recognize the child with DHF, how to take care of the child at home, and how to prevent the disease) were improved significantly after health education. This effective programme of health education on DHF can be implemented in other communities as part of the national programme for dengue control.
Keywords: Knowledge, attitude, and practice (KAP), mother, dengue haemorrhagic fever, dengue control, Viet Nam.
Ψ This work was financially supported by the Danish-Viet Namese Cooperative Project on Dengue Haemorrhagic Fever. # For correspondence: [email protected]
Introduction
Dengue haemorrhagic fever (DHF) is one of the leading causes of hospitalization and death in children in Southern Viet Nam. In 1998, a widespread DHF epidemic affected 51 out of 67 provinces of the country. Most cases were in 19 provinces of Southern Viet
Nam (119,429 cases of DHF and 342 deaths)(1). As there is no effective vaccine at present to prevent the disease or a drug to cure DHF, the only measure available to control it is to prevent its transmission by the vector, Aedes aegypti mosquito(2,3). Health education increases people’s knowledge about the disease and motivates them to

Impact of Health Education on Mother’s KAP on DHF
Dengue Bulletin – Vol 27, 2003 175
participate actively in control measures. It is one of the objectives of our dengue project which collaborated with the Danish-Viet Namese Association in order to reduce the morbidity and mortality caused by DHF in Southern Viet Nam. Recognizing DHF patients early, treating them correctly and taking proper care of them play an important role in reducing the mortality. Health education to improve the knowledge of mothers in order to change their attitudes and practices is essential to bring down the morbidity and mortality of DHF in the community. We conducted the study to investigate the impact of health education on the knowledge, attitude, practice (KAP) of DHF of mothers having children aged less than 15 years in four communes in the dengue project area.
Materials and methods¶
This was a descriptive, cross-sectional study. Mothers of children under 15 years of age and living in the four communes where dengue is endemic, namely, Hung Long (Binh Chanh district, Ho Chi Minh City), Binh Chau (Xuyen Moc district, Ba Ria-Vung Tau province), Hoi An (Cho Moi district, An Giang province) and Gia Thuan (Go Cong Dong district, Tien Giang province), were enrolled in the study. The sample size of each commune was based on the calculator programme of the Epi-Info version 6.0, CDC, USA.
¶The study was approved by the Scientific and Ethical Committee of Children’s Hospital N.1, HCM City, Viet Nam.
The first survey on mothers’ KAP (Pre-KAP) was carried out for 115, 117, 126 and 104 mothers having children aged under 15 years at Hung Long, Binh Chau, Hoi An, Gia Thuan communes respectively. Each mother of these communes was educated once by the medical staff of the commune clinics (who had been trained earlier on how to educate mothers on DHF) from June to October in 1997 and in 1998. At the end of the programme, we conducted the second survey in August 1999 (Post-KAP).
Every mother was interviewed by the commune staff based on a prepared questionnaire. Doctors from district hospitals and the Children’s Hospital N.1 supervised this interview. All the health staff and the doctors had been trained on how to conduct the survey.
The data collected were analysed by software SPSS version 6.0.
Results
The number of the mothers interviewed in the Pre-KAP and Post-KAP was 463 and 456 respectively. Table 1 presents the distribution by age of the mothers. Most mothers were 40 years of age or younger. 5.2-6.1% of the mothers were illiterate, about half of them had education levels of primary school Grade 5 or less, and remainder had received secondary schooling (Table 2). There were no significant changes in the age distribution and education levels of the mothers before and after the intervention (Tables 1 and 2).

Impact of Health Education on Mother’s KAP on DHF
176 Dengue Bulletin – Vol 27, 2003
Table 1. Age distribution of mothers enrolled in the study
Age (years) Pre-KAP No. (%)
Post-KAP No. (%) P-value†
<20 1 (0.2) 13 (2.8) 0.1
20-30 158 (34.1) 182 (39.9) 0.4
31-40 200 (43.1) 177 (38.8) 0.5
>40 104 (22.4) 84 (18.4) 0.5
Total 463 (100) 456 (100) † P-value of comparison between the first and the second survey (Pre-KAP and Post-KAP).
Table 2. Distribution of education levels of mothers enrolled in the study
Education level
Pre-KAP No. (%)
Post-KAP No. (%) P-value†
Illiterate 24 (5.2) 28 (6.1) 0.7
Primary school
255 (55.1) 231 (50.7) 0.5
Secondary school
184 (39.7) 197 (43.2) 0.6
Total 463 (100) 456 (100)
† P-value of comparison between the first and the second survey (Pre-KAP and Post-KAP).
Table 3 shows the proportion of the mothers who had knowledge about DHF and its transmission. In Pre-KAP we found that high fever, which is the main symptom of DHF, was known only by 55.3% of the mothers; bleeding manifestations such as epistaxis, gum bleeding, haematemesis and melena which are important signs and symptoms in the diagnosis, were mentioned by only 15.3% of the mothers. Only a small proportion of the mothers (12.5-25.2%) knew about the dangerous signs such as
severe vomiting, abdominal pain, haematemesis and melena. The proportion of the mothers who knew about the symptoms/signs and dangerous signs of DHF increased significantly after they had been educated about the disease. More particularly, the proportion of mothers who did not know anything about the symptoms/signs and dangerous signs of DHF was brought down significantly from 16.8% to 0.9% and from 17% to 1.3%, respectively (P<0.00007, and P<0.0001, respectively).
The proportion of the mothers who knew that mosquitoes transmitted DHF from person to person and that mosquitoes attacked children during daytime increased significantly from 83.4% to 97.6%, and from 25.2% to 68%, respectively, after health education (P<0.0006, and P<0.00001). Only 0.7% of the mothers did not know about the transmission of DHF after health education in comparison with 15.8% before health education (Table 3).
Table 4 shows the way mothers took care of their children with fever at home. In Pre-KAP we noted that not all mothers knew how to correctly take care of a child with DHF at home: 52.8% of the mothers brought the child to a doctor; 66.9% of them sponged the child with high fever; only 34.2% and 6.1% of them encouraged the child to drink as much fluid as possible and eat normal food. In Post-KAP we found that the proportion of mothers who gave proper care to their children (giving antipyretic drugs; sponging; encouraging children to drink and eat; seeking doctors) had significantly improved. Seeking a doctor when their children had high fever was mentioned by 83.6% of the mothers. However, there were still 13.5% of them who bought drugs from a pharmacy.

Impact of Health Education on Mother’s KAP on DHF
Dengue Bulletin – Vol 27, 2003 177
Table 3. Proportion of mothers responding to selected DHF knowledge
DHF knowledge Pre-KAP No. (%)
Post-KAP No. (%) P-value†
Symptoms/signs • Fever >2 days • Petechia • Bleeding (epistaxis, melena,
haematemesis) • Cold extremities • Adominal pain • Others • Don’t know
256 (55.3) 234 (50.5) 71 (15.3)
92 (19.9) 46 (9.9)
70 (15.1) 78 (16.8)
430 (94.3) 392 (86.0) 337 (73.8)
175 (38.4) 227 (49.6)
3 (0.7) 4 (0.9)
< 0.0001 < 0.0001 < 0.0001
0.0039
< 0.0001 < 0.0001 0.00007
Dangerous signs • Lethargy, cold extremities • Severe vomiting • Abdominal pain • Bleeding • Others • Don’t know
212 (45.7) 12 (25.3) 58 (12.5) 76 (16.4) 84 (18.1) 79 (17.0)
346 (75.9) 289 (63.3)
228 (50) 405 (88.9)
6 (1.3) 6 (1.3)
0.00001
<0.00001 <0.00001 <0.00001
0.00006 0.0001
Transmission • Mosquito bites • Direct contact • Others • Don’t know
386 (83.4)
8 (1.7) 9 (1.9)
73 (15.8)
445 (97.6)
5 (1.1) 7 (1.5) 3 (0.7)
0.0006
0.7 0.8
0.0001 Biting time of the mosquito
• Daytime • Night • Both daytime and night • Don’t know
118 (25.2) 171 (36.9) 125 (26.9) 51 (11.1)
310 (68.0)
26 (5.7) 114 (25.0)
6 (1.3)
<0.00001 <0.00001
0.7 0.0036
Breeding places of the mosquito • Water storage containers
− With covers − Without covers − Both of them
• Don’t know
177 (38.3) 266 (57.4)
4 (0.9) 16 (3.5)
56 (12.2) 393 (86.2)
5 (1.1) 2 (0.4)
0.00002 <0.00001
0.8 0.1
† P-value of comparison between the first and the second survey (Pre-KAP and Post-KAP).

Impact of Health Education on Mother’s KAP on DHF
178 Dengue Bulletin – Vol 27, 2003
Table 4. Measures mothers took to care for their children with fever at home
Measure Pre-KAP No. (%)
Post-KAP No. (%) P-value†
Giving antipyretic drugs
190 (41.1) 352 (77.3) <0.00001
Sponging 310 (66.9) 388 (85.2) 0.0024
Encouraging to drink much water
159 (34.2) 344 (75.5) <0.00001
Encouraging to eat normal food
28 (6.1) 217 (47.6) <0.00001
Buying drugs from pharmacy
130 (28.1) 62 (13.5) 0.0109
Skin cut, chiropractic with medicated oil
39 (8.4) 8 (1.7) 0.03
Seeking doctor 245 (52.8) 381 (83.6) <0.00001
Others 44 (9.5) 0
† P-value of comparison between the first and the second survey (Pre-KAP and Post-KAP).
The proportion of mothers and the measures they took to prevent the disease in the Pre-KAP and Post-KAP periods is presented in Table 5. The proportion of mothers who did not know about DHF transmission and the measures needed to prevent it were brought down to 1.5% and 0.7%, respectively. We found that the proportion of mothers who said that larvicides were the best control measure to prevent DHF was significantly increased (P<0.0001).
The dominant sources from which the mothers received health information on DHF in the Pre-KAP period were health personnel (44.9%), other people (41.7%), and television (29.2%). In the Post-KAP period, the proportion of the mothers receiving information on DHF from health personnel was significantly increased to 86.4% (Table 6).
Table 5. Control measures mentioned by mothers to prevent DHF
Measure‡ Pre-KAP No. (%)
Post-KAP No. (%) P-value†
Cleansing trees around houses, draining water
95 (20.5) 35 (7.6) 0.008
Discarding disused water storage containers
296 (63.9) 236 (51.7) 0.08
Both of them 65 (14) 182 (40.0) 0.00003
Don’t know 7 (1.5) 4 (0.7) 0.5
Larvicides 111 (24.0) 395 (86.7) <0.0001
Using insecticides
280 (60.5) 56 (12.2) <0.0001
Others 107 (23.1) 5 (1.1) <0.00001
‡ Some mothers reported more than one measure. † P-value of comparison between the first and the second survey (Pre-KAP and Post-KAP).
Table 6. Sources of information on DHF which mothers received
Source of information
Pre-KAP No. (%)
Post-KAP No. (%) P-value†
Health personnel
208 (44.9) 394 (86.4) <0.00001
Other people
213 (46.0) 130 (28.4) 0.01
Television 135 (29.2) 295 (64.8) <0.00001
Radio 111 (24.0) 137 (30.0) 0.3
Newspaper 24 (5.2) 58 (12.8) 0.06
Others 15 (3.2) 1 (0.2) 0.1
Don’t know 20 (4.3) 1 (0.2) 0.05 † P-value of comparison between the first and the second survey (Pre-KAP and Post-KAP).

Impact of Health Education on Mother’s KAP on DHF
Dengue Bulletin – Vol 27, 2003 179
Discussion The aim of health education on DHF was to inform people of available scientific knowledge of the disease, so that they could use this knowledge to bring about change of attitudes and practices for better health. DHF education increased their understanding of the problem and encouraged their participation in prevention and control measures against the disease(4).
In the Pre-KAP period, we found that about half of the mothers knew that fever and petechia were the symptoms/signs of DHF, while only a small proportion of mothers (12.5-25.2%) knew about the dangerous signs such as severe vomiting, abdominal pain, haematemesis and melena. This explains why mothers sometimes brought their children with profound shock to the hospital very late. Therefore, in DHF education, we advised mothers on how to recognize DHF and to bring their children to the hospital immediately(5).
In the Pre-KAP period we knew that only a small proportion of the mothers gave proper care to their children with fever. So, in DHF education, the mothers were advised how to take care of the child with DHF at home. The fact that the proportion of mothers who gave proper care to their children (giving antipyretic drugs; sponging; encouraging the child to drink, to eat; seeking doctors) in the Post-KAP period was significantly improved showed the impact of health education on KAP of the mothers. However, still 13.5% of them bought drugs from a pharmacy. It raised the need to educate private pharmacies in any future programme on DHF education.
Up to 83.5% of the mothers said that mosquito transmitted the disease, but only 25.2% of them knew in the Pre-KAP period that mosquito bit children during the daytime. Concerning prevention of DHF, only 24% of the mothers noted that the use of larvicides was the best control measure. It told us to advise the mothers on how to prevent the disease effectively, and motivate them to participate in its control. The fact that the proportion of mothers who did not know about DHF transmission and measures to prevent the disease from occurring was brought down to 0.7%, and those who understood that the use of larvicides was the best control measure to prevent DHF was significantly increased, was encouraging.
The main sources from which the mothers received information about DHF were health personnel and other people. So, transmission of information on DHF directly from person to person was very effective. We concentrated on training health staff and improved advising the mothers on DHF. We also kept in mind that the education levels of most mothers were low, so while advising the mothers, health workers had to use simple words which were easy to understand. Health workers spoke slowly and sometimes repeated what they said in order to help the mothers remember. Leaflets and posters that were developed for DHF education had more pictures and less text. In the Post-KAP period, the proportion of mothers who received information on DHF from health personnel increased from 44.9% to 86.4%. This showed that our programme of health education had made a strong impact on the mothers’ KAP of DHF.

Impact of Health Education on Mother’s KAP on DHF
180 Dengue Bulletin – Vol 27, 2003
Besides health education for mothers, we included in the project other activities such as motivating the commune people’s committee, the youth and women’s unions to participate actively in the programme of dengue control in their communities. These activities also contributed to the improvement of the mothers' KAP of DHF.
Conclusion The purpose of health education on DHF for mothers was to raise their level of knowledge about the disease: how to recognize the child with DHF; how to take care of the child at home; how to recognize the dangerous signs in order to bring the child to hospital in time; and how to prevent the disease. They were also advised to change their attitudes and practices in order to
control the disease in their communities. At the end of the project, we witnessed encouraging results. Health education had made a strong impact on the mothers' KAP of DHF. The need now would be to sustain this programme and implement it in other communities as part of the national programme for dengue control.
Acknowlegements We thank the doctors and other health staff of the provincial and district hospitals and the commune clinics who were involved in the dengue project, for providing health education on dengue haemorrhagic fever to mothers.
References 1. Do Quang Ha, Nguyen Thi Kim Tien, Vu Thi Que
Huong, Huynh Thi Kim Loan and Cao Minh Thang. Dengue epidemic in southern Viet Nam in 1998. Emerging Infectious Disease, 2000, 6: 522-525.
2. WHO. Dengue haemorrhagic fever: Diagnosis, treatment, prevention and control. 2nd edition. Geneva: WHO, 1997.
3. Gubler DJ. Dengue and dengue haemorrhagic fever. Clin Microbiol Rev 1998; 11:480-496.
4. Rigau-Perez JG, Clark GG, Gubler DJ, Reiter P, Sanders EJ and Vorndam AV. Dengue and dengue haemorrhagic fever. Lancet, 1998, 352: 971-977.
5. Nguyen Thanh Hung and Nguyen Trong Lan. Treatment of dengue haemorrhagic fever at Children's Hospital N.1, Ho Chi Minh City, 1991-2000. Medical Journal HCM City, 2001, 3: 149-152.

Dengue Bulletin – Vol 27, 2003 181
Viral Vaccines for Dengue: The Present and the Future
by
S Swaminathan# and Navin Khanna
RGP Laboratory, International Centre for Genetic Engineering and Biotechnology, PO Box 10504, Aruna Asaf Ali Marg, New Delhi-110067, India
Abstract
Infection with dengue viruses, of which there are four antigenically distinct serotypes, has re-emerged as a significant global public health threat. Sequential infection in areas of hyperendemicity, where multiple serotypes co-circulate, has the potential to trigger life-threatening disease. Therefore, a safe and effective dengue vaccine must be ‘tetravalent’ capable of providing solid and long-lasting immunity to all four serotypes. The development of a vaccine against dengue has been a high priority of the World Health Organization (WHO) for decades. Currently, six different virus-based vaccines are in various stages of development. Two of these are traditional tissue culture-based live attenuated vaccines whereas the remaining four are chimeric recombinant vaccine viruses developed using infectious clone technology. In all these instances, the vaccine viruses are monovalent in that each one is specific to one dengue serotype. A tetravalent dengue vaccine is based on producing vaccine formulations by mixing all four monovalent vaccine viruses. Recent studies in both monkeys and man have shown that such tetravalent formulations can elicit unbalanced immune responses due to the phenomenon of viral interference. While efforts are under way to optimize the tetravalent formulations, the inherent risk of viral interference associated with the current strategy of producing tetravalent dengue vaccine warrants investigation of other recombinant viral systems that eliminate this risk, especially the replication-defective adenovirus-based vector system that may permit the creation of a single vaccine vector capable of conferring tetravalent protection.
Keywords: Dengue virus, dengue vaccine, adenovirus.
# For correspondence: [email protected]
Introduction
Dengue viruses are mosquito-borne, positive-stranded RNA viruses of the genus Flavivirus. These are human pathogens with a worldwide prevalence. About 2.5 billion people in more than a hundred countries are
estimated to be at risk of dengue virus infection, with millions of cases occurring every year around the world(1). There are four antigenically distinct serotypes of dengue viruses (DEN-1, 2, 3 and 4), which can cause a broad spectrum of illness ranging from mild febrile sickness to severe
Viral Vaccines for Dengue: The Present and the Future
182 Dengue Bulletin – Vol 27, 2003
haemorrhagic, sometimes fatal, disease. To date, there is no licensed vaccine to prevent dengue infection.
Developing a vaccine for dengue is a very challenging task because of two important reasons. First, dengue infections can be more severe in individuals who have dengue antibodies acquired either passively through maternal transmission or actively from a prior episode of dengue infection with a heterologous serotype(2). Thus, protection against only one or two dengue viruses could actually increase the risk of potentially fatal dengue haemorrhagic fever and dengue shock syndrome through antibody dependent enhancement (ADE) of infection. Thus, a successful vaccine must be ‘tetravalent’, capable of simultaneously inducing a high level of long-lasting immunity to all four serotypes. Secondly, a suitable animal model to evaluate candidate dengue vaccines is not available. These setbacks notwithstanding, many laboratories worldwide are exploring multiple approaches towards developing dengue vaccines. A major part of current research efforts on dengue vaccine development focuses on the use of live-attenuated and infectious clone-derived vaccines(3,4). Various laboratories are engaged in exploring other alternative strategies, including DNA vaccines(5), protein vaccines and immunogens vectored by various recombinant systems(6).
The provision of an effective means to stimulate both the humoural and cellular arms of the immune response is crucial to vaccine development. Protein-based vaccines elicit potent antibody responses
(humoural response) while failing to elicit an effective cellular response. In contrast, DNA- and virus-based vaccines can elicit both humoural and cellular immune responses. However, DNA-based vaccines tend to induce relatively low antibody titres, presumably due to the poor efficiency of target cell transduction and concomitant low-level antigen expression(7). Induction of low titres of antibodies is potentially risky in the context of ADE. Virus-based vaccines are decidedly more effective in this regard as they can mediate efficient antigen gene transfer and high-level production of authentic protein antigens directly within the cells of the immunized host in the natural context of an ongoing infection and thus provide for a balanced stimulation of both arms of the immune system and resultant long-lasting immunity(8). Recent investigations using virus-based recombinant and non-recombinant dengue vaccine candidates in monkeys(9,10) and man(11,12), respectively, have shown that the current strategy of creating tetravalent dengue vaccine formulations can lead to an unbalanced immune response, specific to only one particular serotype. This has been attributed to ‘viral interference’ that apparently comes into play when four monovalent vaccine viruses are mixed to create a tetravalent formulation. This article reviews the current status of these vaccine candidates and examines the potential of alternate viral vector systems that might eliminate the phenomenon of viral interference and pave the way towards achieving a balanced immune response against all four dengue virus serotypes.
Viral Vaccines for Dengue: The Present and the Future
Dengue Bulletin – Vol 27, 2003 183
Conventional vaccines Empirically attenuated strains of all four dengue serotypes have been created by repeated serial passage in non-permissive cell lines independently by Mahidol University in Thailand and the Walter Reed Army Institute for Research (WRAIR) in USA (3,4). In both cases physical mixtures of the four different attenuated strains are prepared to produce tetravalent formulations. The Mahidol vaccine has been licensed to Aventis Pasteur (AvP) in France for large-scale production under Good Manufacturing Practice (GMP) conditions. The first clinical trial carried out using the Mahidol/AvP tetravalent vaccine in US volunteers revealed that antibody responses were predominantly directed against DEN-3 with low or undetectable titres against the remaining three serotypes(11). This outcome has been attributed to preferential replication of DEN-3 in the tetravalent vaccines. The mechanism of such viral interference is not known. But, it has been suggested that the ratio of the four attenuated viruses in the tetravalent formulation may be an important factor. A subsequent clinical study in Thailand(12) showed that varying and reducing the concentrations of the serotype 3 strain resulted in improved clinical safety profile of the tetravalent vaccine. About 71% seroconversion (against all four serotypes) was observed after a two-dose vaccination schedule in this study. Several different reformulations of the tetravalent vaccine are being evaluated in order to get a more balanced immune response to each serotype. The WRAIR vaccine, licensed to GlaxoSmithKline in Belgium, has recently been quoted to have been tested in a phase
I study of 50 adult volunteers. It has been further quoted that this study, which evaluated 16 different formulations of the tetravalent vaccine, reported an 80-90% seroconversion against all four serotypes after two immunizations(3,4).
Flavivirus-based recombinant dengue vaccines A different approach for creating viral vaccines against dengue has taken advantage of the infectious clone technology. This technology permits the recovery of infectious dengue virus from cells transfected in vitro with RNA transcripts derived from a full-length cDNA clone of the dengue virus genome. Using this strategy, infectious recombinant viruses can be created from cDNA clones engineered to carry defined attenuating mutations. It is also possible to produce monovalent chimeric viruses by replacing the structural genes of the full-length cDNA clone with those of different DEN virus serotypes. Infectious clone technology-based approaches (as well as other recombinant virus vectored vaccines, see below) have focused on the dengue virus envelope (E) protein (the major structural protein), for a variety of reasons(13,14,15,16,17,18) summarized in Table 1, the most important ones being that it mediates virus entry by interacting with host cell surface receptors(13) and is the primary target of the neutralizing antibody response(14,15). Most vaccine designs also include another structural protein, the premembrane (prM) protein, implicated in the maintenance of the structural/antigenic integrity of the E protein(19).

Viral Vaccines for Dengue: The Present and the Future
184 Dengue Bulletin – Vol 27, 2003
Table 1. Most recombinant dengue vaccine efforts focus on the E protein
Properties/functions of the E protein
References¶
• Binds host cell surface receptor
Chen et al, 1996(13)
• Target of neutralizing antibodies
Mégret et al, 1992(14)
• Elicits the first antibody response with the longest-lasting activity
Churdboonchart et al, 1991(15)
• Several monoclonal antibodies specific to receptor binding domain of E protein block virus adsorption and infectivity
Crill and Roehrig, 2001(16)
• Anti-E monoclonal antibodies can confer passive protection
Kaufman et al, 1987(17)
• Purified E protein can induce neutralizing antibodies and protective immunity
Feighny et al, 1992(18)
¶ Reference numbers are shown in parentheses
Intertypic chimeric vaccines
In this approach, pioneered by Lai’s group at the National Institutes of Health, Bethesda, USA, the structural genes from the cDNA copy of an attenuated strain of dengue virus
of a given serotype is replaced by the corresponding genes of a different dengue virus serotype. The resultant intertypic chimeras are monovalent in that they elicit antibody responses specific to the serotype from which their structural genes are derived(20). Current initiatives that seek to develop intertypic vaccine viruses are focusing on the use of attenuated (either by conventional methods or by site-directed mutagenesis) strains of DEN-1(21,22), DEN-2(23,24) and DEN-4(25) as vectors to carry heterotypic structural genes (see Table 2).
For example, the structural genes from a cDNA copy of the Mahidol vaccine candidate DEN-2 PDK-53 (attenuated by repeated serial passaging in primary dog kidney cells and tested in US and Thai volunteers) have been replaced with the corresponding genes of DEN-1 using infectious clone technology(23). A DEN-4 mutant bearing a 30-nucleotide (nt) deletion in its 3’ untranslated region (UTR) has been tested in 20 human volunteers who exhibited only minor symptoms with 100% neutralising antibody seroconversion(25). The high degree of immunogenicity and very mild reactogenicity of this mutant virus have prompted efforts to use it as a vector for the construction of chimeric viruses encoding the structural proteins of DEN-1, DEN-2 and DEN-3. More recently, this 30-nt deletion has also been introduced into the 3’ UTR of wild-type DEN-1 virus with resultant attenuation(22). This finding opens up the possibility that a tetravalent vaccine could be generated by the introduction of this 30-nt deletion into wild-type dengue viruses of all four serotypes.

Viral Vaccines for Dengue: The Present and the Future
Dengue Bulletin – Vol 27, 2003 185
Table 2. Attenuated dengue virus strains for development of intertypic chimeric vaccines
Vaccine strain (parent virus)
Location of attenuating mutations
Attenuation strategy References¶
rDen1mutF (DEN-1)
3’ SLψ site-directed mutagenesis
Markoff et al, 2002(21)
rDen1? 30 (DEN-1)
3’ UTR site-directed mutagenesis
Whitehead et al, 2003(22)
PDK-53 (DEN-2)
5’UTR NS1, NS3
serial passage in PDK cells
Huang et al, 2000(23) Butrapet et al, 2000(24)
2A? 30 (DEN-4)
3’UTR site-directed mutagenesis
Durbin et al, 2001(25)
¶ Reference numbers are shown in parentheses ψ Abbreviations: SL, stem-loop; UTR untranslated region; NS1 and NS3, non-structural proteins 1 and 3; PDK, primary dog kidney cells
ChimeriVax vaccines
The most successful flavivirus vaccine is the empirically attenuated 17D strain of yellow fever (YF) virus(26). A single immunization with the YF17D vaccine strain can confer immunity against yellow fever in nearly 100% of vaccinated individuals. Using the YF17D vector, Acambis, USA, has developed a promising platform, known as ChimeriVax technology, for the development of dengue vaccines. In this strategy, the structural genes (prM and E) of YF17D in a full-length cDNA clone are replaced with the corresponding genes from dengue viruses. The only difference with respect to the intertypic strategy is that the ChimeriVax approach is based on the use of the attenuated YF17D vector rather than attenuated dengue virus vectors. Acambis has created four monovalent chimeric vaccine viruses using this technology (YF/DEN-1 to DEN-4), each encoding the structural genes of one of the four dengue serotypes(9) and licensed these to Aventis Pasteur, France. Immunization of
monkeys with a tetravalent formulation (physical mixture of equal concentrations of each monovalent YF/DEN chimeric virus) of the YF/DEN chimeric vaccine resulted in the highest immune response being directed against the YF/DEN-2 virus, a situation reminiscent of that noted earlier for the live attenuated Mahidol/AvP vaccine(11). A dose adjustment for the YF/DEN-2 chimera resulted in a more balanced response against DEN-1, DEN-2 and DEN-3 viruses, but a somewhat higher response against the chimeric DEN-4 virus(10). Additional formulations will have to be evaluated in monkeys before undertaking Phase I human trials.
Recombinant dengue vaccines based on non-flavivirus vectors Apart from the use of attenuated flaviviruses derived from different serotypes of dengue

Viral Vaccines for Dengue: The Present and the Future
186 Dengue Bulletin – Vol 27, 2003
viruses and YF virus, efforts are on to use several well-characterized heterologous viral vector systems for the expression of dengue structural antigens. Prominent among these are vectors derived from baculovirus(27) and vaccinia virus(28). Recent work suggests that baculoviruses can transduce a variety of mammalian cells; however, their use as live viral vaccine vectors does not appear to be currently feasible due to their inactivation mediated by complement(29). This section will review work that pertains to the use of vaccinia virus vectors which have been tested as potential candidate dengue vaccines in animal models and adenovirus vectors, which have not been evaluated for the expression of dengue antigens so far, despite their tremendous potential to serve as safe and efficacious viral vaccine vectors(30).
Vaccinia virus vectors
Recombinant vaccinia vectors harbouring different flavivirus genes have been constructed and tested as vaccines in animal models during the late eighties and early nineties(31,32,33,34). Mice immunized with a recombinant vaccinia vector encoding DEN-4 structural proteins prM and E, and the non-structural protein NS1 (either singly or in combination) were protected against lethal dengue encephalitis(31). Despite the observed protection, only low levels of E-specific neutralizing antibodies were detected. The vaccinia expressed DEN-4 E was found to be poorly immunogenic in monkeys as well(32). In a subsequent report, it was shown that a vaccinia recombinant, which expressed a carboxy-terminally truncated version of DEN-4 E, was more immunogenic than
recombinants expressing full-length DEN-4 E(33). Co-expression of prM and E using vaccinia vectors can lead to the secretion of extracellular sub-viral particles capable of eliciting high levels of neutralizing antibodies(34). However, safety concerns exist with the use of vaccinia virus-vectored vaccines because of the undesirable side-effects demonstrated during the WHO-directed smallpox eradication programme. As most of the recombinant vaccinia vectors designed to express dengue antigens have been based on the virulent WR strain, these are unacceptable for human use(35). These concerns have led, in the last few years, to the use of a highly-attenuated vaccinia virus vector called modified vaccinia virus Ankara (MVA) as a potential dengue vaccine vector. A recent study(28) which investigated the use of MVA to express the carboxy-terminally truncated versions of the E proteins of DEN-2 and DEN-4 showed that mice immunized with MVA-DEN-2E, but not MVA-DEN-4E, induced a neutralizing antibody response. Furthermore, it was shown that MVA-vectored DEN-2E could protect monkeys against the DEN-2 virus challenge(28). Though the safety of the MVA virus in humans has been well-documented, it appears to be associated with inconsistent antigen-specific immune responses(36).
Adenovirus vectors
The feasibility of using adenovirus (Ad)-based vaccine vectors for expressing dengue antigens has not been explored so far, despite its many advantages(8,30,37,38,39,40,41,42,43,44,45). The salient features of Ad vectors are summarized in Table 3.

Viral Vaccines for Dengue: The Present and the Future
Dengue Bulletin – Vol 27, 2003 187
Table 3. Adenovirus has several features suitable for its development as a tetravalent
dengue vaccine vector
Features of Ad vectors References¶
Well-documented human safety
Gaydos & Gaydos, 1999(37)
No significant pathology
Horwitz, 2001(38)
Large insert capacity (7.5-35Kb)
Wang & Huang, 2000(39)
Oral immunization Top et al, 1971(40, 41)
Can elicit humoural, cell-mediated and mucosal immunity
Imler, 1995(42) Rolph and Ramshaw, 1997(8)
Replication-defective Ad is superior to poxvirus vectors
Gonin et al, 1996(43) Xiang et al, 1996(44) Shiver et al, 2002(45)
¶ Reference numbers are shown in parentheses
A major factor in favour of exploring Ad-vectored dengue vaccine candidates is Ad’s safety record. Live Ad vaccines have been successfully and safely administered orally to millions of US military recruits(37). Ad is not associated with any significant pathology in humans(38). It can be propagated to very high titres of about 1011-12 plaque forming units (pfu)/ml(42,46), (unlike flaviviruses which yield titres of only around 106-7 pfu/ml), in permissive cell lines and can be purified relatively easily using column chromatographic methods(47). A number of viral antigens derived from several different viruses have been expressed using Ad-based vectors. These recombinant Ad vectors have been tested in several animal models and have been shown to elicit humoural, cell-mediated and mucosal immunity.
Furthermore, protection against virus challenge has been demonstrated in a number of experimental models(8,42,43,45,48). Two of the most promising recent reports pertaining to non-human primate models of the Ebola virus(48) and the human immunodeficiency virus(45) emphasize the potential of Ad-based vaccine strategy. Comparison with attenuated poxvirus vectors such as New York vaccinia (NYVAC)(43) and MVA(45) have shown Ad to be safer and more efficacious. Our preliminary work has demonstrated that a recombinant Ad expressing the DEN-2E protein is capable of eliciting antigen-specific neutralizing antibodies(49). The most widely used Ad vectors are all replication-defective. This will ensure that Ad will not disseminate in the vaccinee, thus minimizing the risk of adverse side-effects(30). As Ad is a ubiquitous virus, a potential disadvantage with the use of Ad-based vaccines is the issue of prior Ad immunity. However, this may no longer be a serious concern. Co-injection of gel foam (a collagen-based matrix) with the antigen-encoding Ad vaccine virus has been demonstrated to abrogate the inhibitory effects of Ad immunity(50). A more recent report has shown that potential interference by pre-existing immunity to the viral vaccine can be effectively overcome by DNA priming before vector boosting(51).
Conclusions Dengue infection has emerged as a leading public health concern in over a hundred tropical and sub-tropical countries in south-east Asia, the Caribbean and Central and South Americas. A vaccine is urgently needed to lessen the global dengue disease

Viral Vaccines for Dengue: The Present and the Future
188 Dengue Bulletin – Vol 27, 2003
burden. No vaccine is currently licensed for human use. Developing a dengue vaccine has been an elusive goal because of the need to confer solid and long-lasting tetravalent protection and the lack of a good animal model in which to evaluate the experimental vaccines. Dengue vaccine research focuses on several strategies. The major focus is on the use of live-attenuated and infectious clone-derived vaccines. Currently, six different virus-based vaccines are in advanced stages of development. Two of these are traditional tissue culture-based live attenuated vaccines, whereas the remaining four are chimeric recombinant vaccine viruses developed using infectious clone technology. In all these instances, the vaccine viruses are monovalent in that each one is specific to one dengue serotype. A tetravalent dengue vaccine is based on producing vaccine formulations by mixing all four monovalent vaccine viruses. Recent studies have shown that both the live attenuated(11) and the ChimeriVax(10) tetravalent dengue vaccine formulations elicit unbalanced immune response due to viral interference. The occurrence of this phenomenon, which tends to skew the immune response predominantly towards one serotype (especially in the case of the ChimeriVax dengue vaccine in which all the four monovalent vaccine viruses have
identical backbones), emphasizes the limitations and, more importantly, the risks associated with mixing four monovalent vaccine viruses to create a tetravalent vaccine.
While efforts are under way to optimize the tetravalent formulations, the risk of viral interference inherent in the current strategy of producing tetravalent dengue vaccine warrants investigation of other recombinant viral vector systems that may permit the creation of a single vaccine vector capable of conferring tetravalent protection. Promising progress in the development of alternative vaccine strategies, particularly those using live viral vectors, have the potential to be developed into single component vaccines incorporating all the key antigens from all four DEN serotypes. Viral vectors derived from vaccinia virus and adenovirus have fairly large insert capacities and are potential candidates for exploring the possibility of developing such a single tetravalent vaccine vector. While the use of poxvirus vectors is associated with safety concerns(35), replication-defective adenoviruses are not associated with any significant human pathology(38). The large insert capacity, ranging from 7.5-35 kb(39), its ability to grow to very high titres (1011-12 pfu/ml) and the ease of scale-up and purification(46), confer on Ad the potential to be developed into a cost-effective tetravalent dengue vaccine.
References 1. Gubler DJ. Epidemic dengue/dengue
haemorrhagic fever: A global public health problem in the 21st century. Dengue Bulletin, 1997, 21: 1-15.
2. Morens DM. Antibody-dependent enhancement of infection and the pathogenesis of viral disease. Clin Infect Dis, 1994, 19: 500-512.
3. Halstead SB and Deen J. The future of dengue vaccines. Lancet, 2002, 360: 1243-1245.
4. Almond J, Clemens J, Engers H, Halstead S, Khiem HB, Pablos-Mendez A, Pervikov Y and Tram TT. Meeting report: Accelerating the development and introduction of a dengue vaccine for poor children, 5-8 December 2001, Ho Chi Minh City, Vietnam. Vaccine, 2002, 20: 3043-3046.

Viral Vaccines for Dengue: The Present and the Future
Dengue Bulletin – Vol 27, 2003 189
5. Raviprakash K, Kochel TJ, Ewing D, Simmons M, Phillips I, Hayes CG and Porter KR. Immunogenicity of dengue virus type 1 DNA vaccines expressing truncated and full-length envelope protein. Vaccine, 2000, 18: 2426-2434.
6. Trent DW, Kinney RM and Huang CY-H. Recombinant dengue vaccines in “Dengue and dengue haemorrhagic fever” (Gubler DJ and Kuno G, Eds.). 1997, 379-403, CAB Inernational, Wallingford.
7. Thalhamer J, Leitner W, Hammerl P and Brtko J. Designing immune responses with genetic immunization and immunostimulatory DNA sequences. Endocrine regulations, 2001, 35: 143-166.
8. Rolph MS and Ramshaw IA. Recombinant viruses as vaccines and immunological tools. Current Opin Immunol, 1997, 9: 517-524.
9. Guirakhoo F, Arroyo J, Pugachev KV, Miller C, Zhang Z-X, Weltzin R, Georgakopoulos K, Catalan J, Ocran S, Soike K, Ratterree M and Monath TP. Construction, safety, and immunogenicity in nonhuman primates of a chimeric yellow fever-dengue virus tetravalent vaccine. J Virol, 2001, 75: 7290-7304.
10. Guirakhoo F, Pugachev K, Arroyo J, Miller C, Zhang Z-X, Weltzin R, Georgakopoulos K, Catalan J, Ocran S, Draper K and Monath TP. Viraemia and immunogenicity in nonhuman primates of a tetravalent yellow fever-dengue chimeric vaccine: Genetic reconstructions, dose adjustment and antibody responses against wild-type dengue virus isolates. Virology, 2002, 298: 146-159.
11. Kanesa-thasan N, Sun W, Kim-Ahn G, Van Albert S, Putnak JR, King A, Raengsakulsrach B, Christ-Schmidt H, Gilson K, Zahradnik JM, Vaughn DW, Innis BL, SaluzzoJ-F and Hoke Jr CH. Safety and immunogenicity of attenuated dengue virus vaccines (Aventis Pasteur) in human volunteers, Vaccine, 2001, 19: 3179-3188.
12. Sabchareon A, Lang J, Chanthavanich P, Yoksan S, Forrat R, Attanath P, Sirivichayakul C, Pengsaa K, Pojjaroen-Anant C, Chokejindachai W, Jagsudee A, Saluzzo J-F and Bhamarapravati N. Safety and immunogenicity of tetravalent live-attenuated dengue vaccines in Thai adult volunteers: Role of serotype concentration, ratio, and multiple doses. Am J Trop Med Hyg, 2002, 66: 264-272.
13. Chen Y, Maguire T and Marks RM. Demonstration of binding of dengue virus envelope protein to target cells. J Virol, 1996, 70: 8765-8772.
14. Mégret F, Hugnot JP, Falconar A, Gentry MK, Morens DM, Murray JM, Schlesinger JJ, Wright PJ, Young P, van Regenmortel MHV and Deubel V. Use of recombinant fusion proteins and monoclonal antibodies to define linear and discontinuous antigenic sites on the dengue envelope glycoprotein. Virology, 1992, 187: 480-491.
15. Churdboonchart V, Bhamarapravati N, Peampramprecha S and Srinavin S. Antibodies against dengue viral proteins in primary and secondary dengue hemorrhagic fever. Am J Trop Med Hyg, 1991, 44: 481-493.
16. Crill WD and Roehrig RT. Monoclonal antibodies that bind to domain III of dengue virus E glycoprotein are the most efficient blockers of virus adsorption to Vero cells. J Virol, 2001, 75: 7769-7773.
17. Kaufman BM, Summers PL, Dubois DR and Eckels KH. Monoclonal antibodies against dengue 2 virus E-glycoprotein protect mice against lethal dengue infection. Am J Trop Med Hyg, 1987, 36: 427-434.
18. Feighny R, Burrous J, McCown J, Hoke C and Putnak R. Purification of native dengue-2 viral proteins and the ability of purified proteins to protect mice. Am J Trop Med Hyg, 1992, 47: 405-412.
19. Guirakhoo F, Bolin RA and Roehrig JT. The Murray valley encephalitis virus prM protein confers acid resistance to virus particles and alters the expression of epitopes within the R2 domain of the E glycoprotein. Virology, 1992, 191: 921-931.
20. Lai CJ, Bray M, Men R, Cahour A, Chen W, Kawano H, Tadano M, Hiramatsu K, Tokimatsu I, Pletnev A, Arakai S, Shameem G and Rinaudo M. Evaluation of molecular strategies to develop a live dengue vaccine. Clin Diagn Virol, 1998, 10: 173-179.
21. Markoff L, Pang X, Houng H-S, Falgout B, Olsen R, Jones E and Polo S. Derivation and characterization of a dengue type 1 host range-restricted mutant virus that is attenuated and highly immunogenic in monkeys. J Virol, 2002, 76: 3318-3328.

Viral Vaccines for Dengue: The Present and the Future
190 Dengue Bulletin – Vol 27, 2003
22. Whitehead SS, Falgout B, Hanley KA, Blaney Jr JE, Markoff L and Murphy BR. A live, attenuated dengue virus type 1 vaccine candidate with a 30-nucleotide deletion in the 3’ untranslated region is highly attenuated and immunogenic in monkeys. J Virol, 2003, 77: 1653-1657.
23. Huang CY-H, Butrapet S, Pierro DJ, Chang G-JJ, Hunt AR, Bhamarapravati N, Gubler DJ and Kinney RM. Chimeric dengue type 2 (vaccine strain PDK-53)/dengue type 1 virus as a potential candidate dengue type 1 virus vaccine. J Virol, 2000, 74: 3020-3028.
24. Butrapet S, Huang CY-H, Pierro DJ, Bhamarapravati N, Gubler DJ and Kinney RM. Attenuation markers of a candidate dengue type 2 vaccine virus, strain 16681 (PDK-53), are defined by mutations in the 5’ noncoding region and non-structural proteins 1 and 3. J Virol, 2000, 74: 3011-3019.
25. Durbin AP, Karron RA, Sun W, Vaughn DW, Reynolds MJ, Perreault JR, Thumar B, Men R, Lai C-J, Elkins WR, Chanock RM, Murphy BR and Whitehead SS. Attenuation and immunogenicity in humans of a live dengue virus type-4 vaccine candidate with a 30-nucleotide deletion in its 3’-untranslated region. Am J Trop Med Hyg, 2001, 65: 405-413.
26. Monath TP. Yellow fever in “Vaccines” 3rd edition (Plotkin SA and Orenstein WA, Eds.). WB Saunders Co, Philadelphia, 1997: 815-880.
27. Kelly EP, Greene JJ, King AD and Innis BL. Purified dengue 2 virus envelope glycoprotein aggregates produced by baculovirus are immunogenic in mice. Vaccine, 2000, 18: 2549-2559.
28. Men R, Wyatt L, Tokimatsu I, Arakaki S, Shameem G, Elkins R, Chanock R, Moss B, and Lai C-J. Immunization of rhesus monkeys with a recombinant of modified vaccinia virus Ankara expressing a truncated envelope glycoprotein of dengue type 2 virus induced resistance to dengue type 2 virus challenge. Vaccine, 2000, 18: 3113-3122.
29. Kost TA and Condreay JP. Recombinant baculoviruses as mammalian cell gene-delivery vectors. Trends Biotechnol, 2002, 20: 173-180.
30. Stephenson J. Defective adenoviruses as novel vaccines for the Flaviviridae. Clin Diagn Virol, 1998, 10: 187-194.
31. Bray M, Zhao BT, Markoff L, Eckels KH, Chanock RM and Lai C-J. Mice immunized with recombinant vaccinia virus expressing dengue 4 virus structural proteins with or without nonstructural protein NS1 are protected against fatal dengue virus encephalitis. J Virol, 1989, 63: 2853-2856.
32. Lai C-J, Zhang YM, Men R, Bray M, Chanock RM, Dubois DR and Eckels KH. Immunization of monkeys with baculovirus recombinant-expressed dengue envelope and NS1 glycoproteins induces partial resistance to challenge with homotypic dengue virus in “Modern approaches to new vaccines, including prevention of AIDS” (Chanock RM, Ginsberg HS, Brown F and Lerner RA, Eds.), CSHL Press, Cold Spring Harbor, NY, 1991, 251-257.
33. Men RH, Bray M and Lai C-J. Carboxy-terminally truncated dengue virus envelope glycoproteins expressed on the cell surface and secreted extracellularly exhibit-increased immunogenicity in mice. J Virol, 1991, 65: 1400-1407.
34. Bray M and Lai C-J. Dengue virus premembrane and membrane proteins elicit a protective immune response. Virology, 1991, 185: 505-508.
35. Ertl HCJ and Xiang Z. Novel vaccine approaches. J Immunol, 1996, 156:3579-3582.
36. Polo JM and Dubensky Jr TW. Virus-based vectors for human vaccine applications. Drug Discovery Today, 2002, 7: 719-727.
37. Gaydos CA and Gaydos JC. Adenovirus vaccines in “Vaccines” 3rd edition (Plotkin SA and Orenstein WA, Eds), WB Saunders Co, Philadelphia, 1999: 609-628.
38. Horwitz MS. Adenoviruses in “Fields Virology” 4rd edition (Knipe DM. and Howley PM, Eds-in-Chief), Lippincot Williams and Wilkins, Philadelphia, 2001: 2301-2326.
39. Wang Y and Huang S. Adenovirus technology for gene manipulation and functional studies. Drug Discovery Today, 2000, 5: 10-16.
40. Top FH, Grossman RA, Bartelloni PJ, Segal HE, Dudding BA, Russell PK and Buescherr EL. Immunization with live type 7 and 4 vaccines. I. Safety, infectivity, antigenicity and potency of adenovirus type 7 vaccine in humans. J Infect Dis, 1971a, 124: 148-154.

Viral Vaccines for Dengue: The Present and the Future
Dengue Bulletin – Vol 27, 2003 191
41. Top FH, Buescher EL, Bancroft WH and Russell PK. Immunization with live type 7 and 4 vaccines. II. Antibody response and protective effect against acute respiratory disease due to adenovirus type 7. J Infect Dis, 1971b, 124: 155-160.
42. Imler J-L. Adenovirus vectors as recombinant viral vaccines. Vaccine, 1995, 13: 1143-1151.
43. Gonin P, Oualikene W, Fournier A and Eloit M. Comparison of the efficacy of replication-defective adenovirus and NYVAC poxvirus as vaccine vectors in mice. Vaccine, 1996, 14: 1083-1087.
44. Xiang ZQ, Yang YP, Wilson JM and Ertl H. A replication-defective human adenovirus recombinant serves as a highly efficacious vaccine carrier. Virology, 1996, 219: 220-227.
45. Shiver JW, Fu T-M, Chen L, Casimiro DR, Davies M-E, Evans RK, Zhang Z-Q, Simon AJ, Trigona WL, Dubey SA, Huang L, Harris VA, Long RS, Liang X, Handt L, Schleif WA, Zhu L, Freed DC, Persaud NV, Guan L, Punt KS, Tang A, Chen M, Wilson KA, Collins KB, Heidecker GJ, Fernandez VR, Perry HC, Joyce JG, Grimm KM, Cook JC, Keller PM, Kresock DS, Mach H, Troutman RD, Isopi LA, Williams DM, Xu Z, Bohannon KE, Volkin DB, Montefiori DC, Miura A, Krivulka GR, Lifton MA, Kuroda MJ, Schmitz JE, Letvin NL, Caulfield MJ, Bett AJ, Youil R, Kaslow DC and Emini E A. Replication-incompetent adenoviral vaccine vector elicits effective anti-immunodeficiency-virus immunity. Nature, 2002, 415, 331-335.
46. Hitt MM, Addison CL and Graham FL. Human adenovirus vectors for gene transfer into mammalian cells in “Advances in Pharmacology, Vol. 40” (August JT, Ed), Academic Press, California, 1997: 137-206.
47. Huyghe BG, Liu X, Sutjipto S, Sugarman BJ, Horn MT, Shepard HM, Scandella CJ and Shabram P. Purification of a type 5 recombinant adenovirus encoding human p53 by column chromatography. Hum Gene Ther, 1995, 6: 1403-1416.
48. Sullivan NJ, Sanchez A, Rollin PE, Yang Z-Y and Nabel GJ. Development of a preventive vaccine for Ebola virus infection in primates. Nature, 2000, 408: 605-609.
49. Jaiswal S, Khanna N and Swaminathan S. A replication-defective adenoviral vaccine vector for the induction of immune responses to dengue virus type 2. J Virol, 2003, In press.
50. Siemens RD, Elzey BD, Lubaroff DM, Bohlken C, Jensen RJ, Swanson AK and Ratliff TL. Restoration of the ability to generate CTL in mice immune to adenovirus by delivery of virus in a collagen-based matrix. J Immunol, 2001, 166: 731-735.
51. Yang Z-Y, Wyatt LS, Kong W-P, Moodie Z, Moss B and Nabel GJ. Overcoming immunity to a viral vaccine by DNA priming before vector boosting. J Virol, 2003, 77: 799-803.

192 Dengue Bulletin – Vol 27, 2003
Short Note 1
Dengue Haemorrhagic Fever - A threat to Global Health by
Somkiat Sopontammarak#
Department of Paediatrics, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
# For correspondence: [email protected]; [email protected]
Introduction Over the past few years, the mortality rate and the number of dengue haemorrhagic fever/dengue shock syndrome (DHF/DSS) cases have remained high throughout the Kingdom of Thailand. In spite of vector control measures taken to reduce transmission of the virus, the results are poorer than expected. Elsewhere, DHF/DSS is a growing global health problem since dengue infection now occurs in over 100 countries and territories. Currently, 100 million cases of dengue fever and more than 100,000 cases of DHF occur each year(1). Only Africa and the Middle East have thus far been spared large DHF outbreaks(1,2).
Dengue is endemic in the South-East Asia, Western Pacific and American regions of WHO, with a potential of importation of dengue infection for transmission in areas and countries where Aedes aegypti and/or Aedes albopictus are present, including the United States and Japan(3).
The most important vectors transmitting dengue viruses are Aedes aegypti and Aedes albopictus(4,5). In addition, Aedes polynesiensis and other members of the subgenus Stegomyia transmit dengue in restricted geographical areas(2). The presence of Aedes albopictus, which adapts well to cold climate and survives round the year, is endemic in the US and Japan, whereas Aedes aegypti and Aedes albopictus are present in South-East Asia, including Taiwan. There remains a possibility of importing Aedes aegypti infected with dengue viruses by air or ship into Japan during summer, with the risk of involvement of Aedes albopictus in any subsequent transmission. Aedes aegypti mosquitoes normally feed on a single vertebrate host, but a small percentage of each of the two species feed on more than one host during one gonotrophic cycle(6). Their multiple-feeding behaviour is of epidemiological significance. Despite the fact that the vectors have the ability to travel up to 2.5 km daily in an open environment, in one study, only 0.7% of Aedes aegypti
Dengue Haemorrhagic Fever – A Threat to Global Health
Dengue Bulletin – Vol 27, 2003 193
visited more than four houses(7). A study from India(8) showed that most Aedes aegypti were from indoor habitats, indicating the endophilic nature of the species. On the contrary, Aedes albopictus is exophilic (outdoor habitat) in nature.
The possibility of these vectors transmitting viruses and infectious agents other than dengue viruses exists, as in a case report of concomitant DHF and Kawasaki disease (KD) or Kawasaki syndrome (KS) by Sopontammarak(9). This raises several possibilities, including the concept that dengue virus may be one of the potential aetiological causes of KD, and Aedes mosquitoes may transmit the causative agent of KS along with dengue virus. Dengue viruses induce cell proliferation and morphological changes of endothelial cells from human umbilical cord vein(10) and potentially cause arteritis, including coronary arteritis, which is the hallmark of KS. A preliminary study at Songklanagarind Hospital at Prince of Songkla University revealed that three out of 12 patients with clinical and echocardiographically proved KS (25%) had dengue IgM titer ≥40 U.
At present, the causative agent of KD remains elusive(4). A matched case-control study in Colorado(11) indicated that a humidifier in a child’s room before onset of KS was significantly associated with KS.
Future research questions should include the following:
(1) Could dengue viruses be one of the causative agents of KS?
(2) What is the distribution of dengue vectors in Japan, the US and cold climate countries at present?
Conclusion DHF/DSS is a growing global health problem. Measures for the prevention and control of dengue have not been effective. Also, a dengue vaccine has not been developed in a timely fashion compared to other infectious diseases. Dengue vectors may potentially cause epidemics of DHF/DSS in Japan and the US and possibly carry the causative agent of KS.
References
1. Gubler DJ. In: Gubler DJ, Kuno G (eds.). Dengue and dengue haemorrhagic fever. Cambridge: University Press, 1997: 1-22.
2. Gregson A and Edelman R. Dengue virus infection. Pediatric Infect Dis J, 2003, 22: 179-181.
3. Yamada KI, Takasaki T, Nawa M, Nakayama M, Arai YT, Yabe S and Kurane I. The features of imported dengue fever cases from 1996 to 1999. Jap J Infect Dis, 1999, 52: 257-259.
4. Monath TP. Dengue: The risk to developed and developing countries. Proc Natl Acad Sci U S A, 1994, 91: 2395-2400.
5. Henchal EA and Putnak R. The dengue viruses. Clin Microbiol Rev, 1990, 3: 376-396.
6. Scott TW, Clark GG, Lorenz LH, Amerasinghe PH, Reiter P and Edman JD. Detection of multiple blood feeding in Aedes aegypti (Diptera: Culicidae) during a single gonotrophic cycle using a histological technique. J Med Entomol, 1993, 30: 94-97.

Dengue Haemorrhagic Fever – A Threat to Global Health
194 Dengue Bulletin – Vol 27, 2003
7. Trpis M and Haussermann W. Dispersal and other population parameters of Aedes aegypti in an African village and their possible significance in epidemiology of vector-borne diseases. Am J Trop Med Hyg, 1986, 35: 1263-1279.
8. Tandon N and Ray S. Host feeding pattern of Aedes aegypti and Aedes albopictus in Kolkata, India. Dengue Bulletin, 2000, 24: 117-120.
9. Sopontammarak S and Preukprasert P. Concomitant dengue haemorrhagic fever with Kawasaki disease: South-East Asian J Trop Med Public Health, 2000, 31: 190-191.
10. Rowley AH and Shulman ST. Kawasaki syndrome. Clin Microbiol Rev, 1998, 11: 405-414.
11. Treadwell TA, Maddox RA, Holman RC, Belay ED, Shahriari A, Anderson MS, Burns J, Glode MP, Hoffman RE and Schonberger LB. Investigation of Kawasaki syndrome risk factors in Colorado. Pediatr Infect Dis J, 2002, 21: 976-978.
Dengue Bulletin – Vol 27, 2003 195
Short Note 2
Aedes albopictus (Skuse) Breeding in Plastic Cups around Tea-vendor Spots in Ernakulam City,
Kerala State, India by
J Hiriyan, S C Tewari and B K Tyagi# Centre for Research in Medical Entomology, 4, Sarojini Street, Chinna Chokkikulam,
Madurai - 625 002, India
# For correspondence: [email protected]; [email protected]
Introduction Both Aedes aegypti (Linnaeus) and Aedes albopictus (Skuse) are known vectors of dengue fever in the South-East Asian Region(1). While Aedes aegypti is considered to be the principal vector of dengue virus, Aedes albopictus is suspected of playing a secondary role in the disease transmission. While Aedes aegypti is widely adapted to varied urban/semi-urban situations, Aedes albopictus is generally known to inhabit sylvan and forest-fringe areas.
Since the initial finding of Aedes albopictus breeding in latex collecting cups of rubber trees became established(2), it has spread rapidly to newer suburban and urban areas too.
In this brief note an observation is brought on record to highlight the possibility
of the propagation of Aedes albopictus in a coastal district, Ernakulam, in Kerala State, through a stupendous littering of discardable plastic tea cups (DPTC) at the sites of fast food stalls/jaunts and ice-cream parlours, etc., as a relatively new mode of vector dissemination engineered by man.
Observation and discussion During the course of an entomological investigation about the emergence of dengue fever in Ernakulam district in June 2002, it was observed that a large number of DPTCs were littered in the public garden along the seashore. The DPTCs that were mostly placed facing upwards in the furrows of the iron fence around the garden had often collected some rain water which is a common happening along the shore line. Interestingly,

Aedes albopictus (Skuse) Breeding in Plastic Cups around Tea-vendor Spots in Ernakulam City
196 Dengue Bulletin – Vol 27, 2003
such DPTCs were found to breed immatures of Aedes albopictus, the identification of which was confirmed by rearing the immatures in the laboratory to the adult stage by following the keys of Y M Huang(3).
A total of 175 DPTCs were examined within a 50-metre length of the garden fence. Water collection was found in 25 DPTCs, of which nine (36%) were found to be breeding only Aedes albopictus. It was noted that most of the DPTCs which were positive for Aedes albopictus breeding contained rich organic matter due to the decay of foliage from the overhanging trees. While on one hand the copious presence of the fourth instar larvae and a few pupae confirmed prolonged water–holding in the DPTCs, the presence of the first instar larvae, on the other hand, indicated a continuous breeding process. Also that Aedes albopictus had seemingly adapted commensurably to the DPTC, a new man-made breeding site for this vector species.
The available information indicates that Aedes albopictus competes for the same
peri-domestic breeding habitats as Aedes aegypti(4), which is highly prevalent in coastal areas like Thiruvananthapuram. Being a strong parasympetric species with regard to another important vector of dengue, Aedes aegypti, Aedes albopictus is known to displace the domains of Aedes aegypti in spreading its distribution(5). It will be advisable, meanwhile, that a proper manner of disposing of the DPTCs, a rather simple and minor-looking unhygienic habit which might fulminate into a major breeding mode of Aedes albopictus in future, may be ensured through public awareness and health laws.
Acknowledgements The authors are grateful to the Officer on Special Duty, Centre for Research in Medical Entomology, Madurai, for encouragement and permission. They are also thankful to Mr G Baskaran and Mr V Murugesan for providing technical assistance.
References 1. Gubler DJ and Kuno G. Dengue and dengue
haemorrhagic fever. CAB Publs, New York, 1997: 496.
2. Sumodan PK. Potential of rubber plantations as breeding source for Aedes albopictus in Kerala, India, Dengue Bulletin, 2003, 27: In press.
3. Huang YM. Contri Am Entomol Inst (Ann Arbor), 1972, 9: 109.
4. Bruce Knudsen A. The significance of the introduction of Aedes albopictus into the southeastern United States with implications for the Caribbean and prospectives of the Pan American Health Organization. J Am Mosq Cont Assoc, 1986, 2 (4): 420-423.
5. Spielman A and M D’Antonio. Mosquito-story of man’s deadliest foe. Faber and Faber Ltd, London: 247.

Dengue Bulletin – Vol 27, 2003 197
Short Note 3
Potential of Rubber Plantations as Breeding Source for Aedes albopictus in Kerala, India
by
P K Sumodan# Post Graduate Department of Zoology, Government College, Madappally, Vadakara-2, Kerala, India
# For correspondence: [email protected]
Introduction Ever since the major outbreak of DF/DHF during 1996 in Delhi(1), dengue fever has been receiving manifold attention from health authorities and researchers all over India. For the first time, one imported dengue case was reported in Wayanad district of Kerala and a death due to suspected dengue haemorrhagic fever in the neighbouring Kannur district in June 2002. Vector surveys in localities associated with these cases indicated that the dominant breeding site for Aedes albopictus, the second most important dengue vector(2), was artificial containers used for collecting rubber sap. During the south-western monsoon (June-September) season, it is a practice to suspend tapping temporarily in some plantations leading to accumulation of rainwater in these containers, thus providing ideal breeding sites for mosquitoes. Against this backdrop a systematic study to substantiate the potential of rubber plantations as sources for the proliferation of
Aedes albopictus was conducted in three villages each in Kannur and Wayanad districts from July to September 2002.
Kannur and Wayanad are two neighbouring districts in north Kerala. Kannur district has 57,823 rubber plantations of different sizes occupying a total area of 33,944 hectares, while Wayanad has 10,244 rubber plantations occupying 6,450 hectares. The two districts receive on an average 300 mm of annual rainfall.
Two categories of rubber plantations were selected for the study. They were (i) with active tapping using rain guards; and (ii) where tapping was suspended with sap-collecting containers intact but without rain guards. Ten plantations each were selected under each category from both districts. In each plantation, 100 trees were surveyed at random for mosquito breeding. Immature stages of mosquitoes were collected in plastic containers and transported to the laboratory for emergence and identification.

Potential of Rubber Plantations as Breeding Source for Aedes albopictus in Kerala, India
198 Dengue Bulletin – Vol 27, 2003
Results and discussions In both districts the plantations with active rubber tapping, no sap-collecting containers were found to be having rainwater. However, in the plantations where tapping had been suspended, sap-collecting containers had rainwater collection and also mosquito breeding (Table). In Kannur district, of the 1,000 trees surveyed, 802 (80.2%) had sap-collecting containers with rainwater. A total of 788 (98.3%) of these containers were positive for Aedes albopictus breeding in association with other Aedine sp.
This species constituted 23.2% of the adult mosquitoes that emerged in the laboratory. In Wayanad district, 917 out of 1,000 trees surveyed had sap-collecting containers with water. However, only 807 (88.0%) supported mosquito breeding. Breeding of Aedes albopictus was found only in 534 (58.2%) containers. The percentage of Aedes albopictus adults that emerged in the laboratory was 12.8%. On an average, each hectare of rubber plantations had 330 trees. The capacity of a sap-collecting container was 500 ml.
Table. Aedes albopictus breeding in rubber plantations where tapping was suspended
District No. of trees
surveyed
No. of trees with
containers having water
(%)
No. of containers with
mosquito breeding (%)
No. of containers with
Aedes albopictus
breeding (%)
Percentage of Aedes
albopictus to total
emergence
Kannur 1,000 802 (80.2) 788 (98.3) 788 (98.3) 23.2
Wayanad 1,000 917 (91.7) 807 (88.0) 534 (58.2) 12.8
This study emphatically indicates the potential of rubber plantations as important sources for the proliferation of Aedes albopictus. In view of the fact that rubber plantations play a significant role in the economy of the region, increased contact of the human population with Aedes albopictus acquires greater epidemiological importance. The study also revealed that those plantations where tapping was not abandoned during the rainy season did not have any potential for mosquito breeding. This is a positive aspect of the entire issue, as encouraging rubber tapping during the rainy season using rain guards could be one of the most plausible solutions for the problem.
Acknowledgements The author is thankful to the Director of Health Services, Kerala, for providing the necessary facilities and to Mr CM Vinod, District Malaria Officer, Kannur, for his assistance in carrying out the study. He is also grateful to the Rubber Board authorities at Kottayam for providing facilities for the conduct of the study.
References 1. Anuradha S, Singh NP, Rizvi SN, Agarwal SK, Gur R
and Mathur MD. The 1996 outbreak of dengue haemorrhagic fever in Delhi, India. South-East Asian J Trop Med Public Health, 1998, 29(3): 503-506.
2. Shroyer DA. Aedes albopictus and arboviruses: A concise review of the literature. J Am Mosq Control Assoc, 1987, 2: 424-428.

Dengue Bulletin – Vol 27, 2003 199
Book Review
Guidelines for the Evaluation of Dengue Vaccines in Populations Exposed to Natural Infection#
(TDR/IVR/DEN/02.1)
# (http://www.who.int/tdr/diseases/dengue/pubs.htm)
This document is addressed to national health authorities, in particular to those of dengue endemic countries interested in the potential use of dengue vaccines for the control of dengue, and to research scientists interested in the development and field evaluation of such vaccines. The guidelines may help public health officials, with the assistance of their technical advisers, to make decisions about dengue vaccine trials to be conducted in their countries, including not only field trials, but also the earlier clinical trials required before proceeding to field trials. The guidelines may help research scientists to clarify the technical decisions required before designing an actual field trial protocol.
Dengue is an acute febrile disease caused by any one of four related viruses. Classic dengue is characterized by fever of 3-5 days’ duration, headache, muscle and joint pain, and a rash. The classic form is self-limited and usually results in complete recovery. Dengue haemorrhagic fever (DHF) is the severe form of dengue. DHF is
characterized by the signs and symptoms of classic dengue followed by increased vascular permeability and haemorrhage which may lead to vascular collapse (dengue shock syndrome [DSS]) and death.
Basic research towards the develop-ment of dengue vaccines continues. Candidate vaccines are reviewed elsewhere (Natth, 1997; WHO, 2000) and include those attenuated by passage in dog kidney cells, chimeric flaviviruses, and others. In this document, the terms “immune” and “immunity” indicate resistance to infection, or to some of its clinical consequences, or resistance to becoming infective, all these kinds of resistance resulting from previous infection or vaccination. “Immune responses” is used to describe the host’s humoural or cellular immune responses which follow exposure to antigens, through infection or vaccination, but which do not necessarily reflect or correlate with a state of protection against infection or its adverse effects. A vaccine’s immunogenicity is its capacity to generate immune responses.

Guidelines for the Evaluation of Dengue Vaccines in Populations Exposed to Natural Infection
200 Dengue Bulletin – Vol 27, 2003
Vaccine potency is a measure of functional activity, which again may or may not correlate with efficacy (clinical protection) in the target group. A clear rationale for the testing of candidate antigens in humans is required. “Disease” will refer to uncomplicated dengue disease, “severe disease” to severe and complicated dengue including DHF and DSS. The trials considered here are concerned with efficacy against natural challenge, as well as with safety and immunogenicity.
In spite of the knowledge accumulated recently, some issues remain undecided, indeed controversial. These guidelines will reflect some of these uncertainties, rather than try to settle them. The circulation of the guidelines may contribute to the settlement of some of the pending questions.
This document was developed using contributions and comments from many
persons. The background and model for these guidelines comes from a 1997 UNDP/World Bank/WHO/TDR document “Guidelines for the Evaluation of Plasmodium falciparum vaccines in populations exposed to natural infection.” The reader is referred to the European Agency for the Evaluation of Medicinal Products document “Note for Guidance on Clinical Evaluation of New Vaccines” (1999) for a detailed discussion of clinical trial design and methods. WHO is developing Guidelines on preclinical evaluation of vaccines and also on Regulatory Expectations for Clinical Evaluation of Vaccines (WHO, 2001a). The principles and specifications given in these complementary WHO documents provide additional guidance and should also be consulted. Information on the status of these guidelines may be obtained from the Coordinator, Quality Assurance and Safety of Biologicals, WHO, Geneva.
References
1. Natth B and Yoksan S. Live attenuated tetravalent dengue vaccine. In: Gubler, D.J. Dengue and Dengue Hemorrhagic Fever, CAB International, Wallingford, UK, 1997.
2. WHO (1997) (UNDP/World Bank/WHO/TDR/ MAL/VAC/97).
3. WHO (1999) (TDR/TDP/SOP/99.1).
4. WHO (2001a) (BS/01/1940).

Dengue Bulletin – Vol 27, 2003 201
Instructions for contributors
The Dengue Bulletin welcomes all original research papers, short notes, review articles, letters to the Editor and book reviews which have a direct or indirect bearing on dengue fever/dengue haemorrhagic fever prevention and control, including case management. Papers should not contain any political statement or reference.
Manuscripts should be typewritten in English in double space on one side of white A4 size paper, with a margin of at least one inch on either side of the text and should not exceed 15 pages. The title should be as short as possible. The name of the author(s) should appear after the title, followed by the name of institution and complete address. E-mail address of the corresponding author should also be included.
References to published works should be listed on a separate page at the end of the paper. References to periodicals should include the following elements: name and initials of author(s); title of paper or book in its original language; complete name of the journal, publishing house, or institution concerned; volume and issue number, relevant pages and date of publication, and place of publication (city and country). References should appear in the text in the same numerical order (Arabic numbers in parenthesis) as at the end of the article. For example:
(1) Nimmannitaya S. Clinical spectrum and management of dengue haemorrhagic fever. The Proceedings of the International Conference on Dengue Haemorrhagic Fever, Kuala Lumpur, September 1-3, 1983:16-26.
(2) Gubler DJ. Dengue and dengue haemorrhagic fever: Its history and resurgence as a global public health problem. In: Gubler DJ, Kuno G (ed.), Dengue and dengue haemorrhagic fever. CAB International, New York, NY, 1997, 1-22.
(3) Nguyen Trong Lan, Nguyen Thanh Hung, Do Quang Ha, Bui Thi Mai Phuong, Le Bich Lien, Luong Anh Tuan, Vu Thi Que Huong, Lu Thi Minh Hieu, Tieu Ngoc Tran, Le Thi Cam and Nguyen Anh Tuan. Treatment of dengue haemorrhagic fever at Children's Hospital N.1, Ho Chi Minh City, 1991-1996. Dengue Bulletin, 1997, 22: 150-161.
Figures and tables (Arabic numerals), with appropriate captions and titles, should be
included on separate pages, numbered consecutively, and included at the end of the text with instructions as to where they belong. Abbreviations should be avoided or explained. Graphs or figures should be clearly drawn and properly labeled, preferably using MS Excel, and all data clearly identified.

Instructions for Contributors
202 Dengue Bulletin – Vol 27, 2003
Articles should include a self-explanatory abstract at the beginning of the paper of not more than 300 words explaining the need/gap in knowledge and stating very briefly the area and period of study. The outcome of the research should be complete, concise and focused conveying the conclusions in totality. Appropriate keywords and a running title should also be provided.
Articles submitted for publication should be accompanied by a statement that they
have not already been published, and, if accepted for publication in the Bulletin, will not be submitted for publication elsewhere without the agreement of' WHO, and that the right of republication in any form is reserved by the WHO Regional Offices for South-East Asia (SEARO) and the Western Pacific (WPRO).
One hard copy, original and clear figures/tables and a computer diskette indicating the name of the software, of the manuscript should be submitted to:
The Editor Dengue Bulletin WHO Regional Office for South-East Asia Mahatma Gandhi Road New Delhi 110002 India Telephone: 91-11-23370804 Fax: 91-11-23379507, 23370972 E-mail: [email protected]
Manuscripts received for publication are subjected to in-house review by a
professional expert and are peer-reviewed by experts in the respective disciplines. Papers are accepted on the understanding that they are subject to editorial revision, including, where necessary, condensation of the text and omission of tabular and illustrative material.
Original copies of articles will not be returned. The principal author will receive 10 reprints of his article published in the Bulletin. A PDF file can be supplied on request.