Delivery at Scale 3millionlives Stephen Johnson Deputy Director Head of Long Term Conditions...
20
Delivery at Scale 3millionlives Stephen Johnson Deputy Director Head of Long Term Conditions [email protected]
-
Upload
logan-matthew-ross -
Category
Documents
-
view
212 -
download
0
Transcript of Delivery at Scale 3millionlives Stephen Johnson Deputy Director Head of Long Term Conditions...
Delivery at Scale
3millionlives
Stephen JohnsonDeputy Director
Head of Long Term Conditions

2
WHY ?
3
A few facts ……………
• NHS - over 1 million patient contacts every 36 hours
• In England over 15 m people have a long term condition with numbers set to increase in the next 5 to 10 years, especially co-morbidity
• People with long term conditions use 72% of inpatient beds, 68% of out-patient appointments and 55% of GP appointments
• Treatment and care of those with LTCs account for 70% of the total health and social care spend in England, or almost £7 in every £10 spent
4
Health care professionals may only interact with people with achronic disease for a few hours a year…
the rest of the time patients care for themselves…
5
5
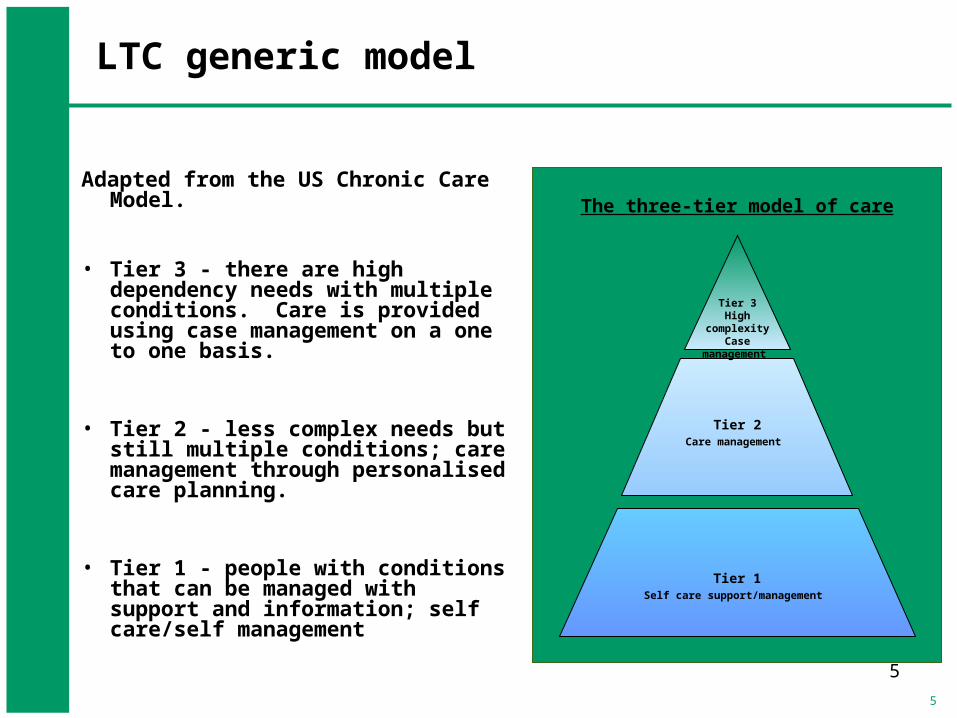
LTC generic model
Adapted from the US Chronic Care Model.
• Tier 3 - there are high dependency needs with multiple conditions. Care is provided using case management on a one to one basis.
• Tier 2 - less complex needs but still multiple conditions; care management through personalised care planning.
• Tier 1 - people with conditions that can be managed with support and information; self care/self management
Tier 1Self care support/management
Tier 2Care management
Tier 3High complexity
Case management
The three-tier model of care

6
This is about improving people’s lives, making a difference, giving people control, confidence and empowerment
Supporting people to live life with a long term condition rather than having their condition dominate their life
Using all the tools available including telehealth and telecare

7
EVIDENCE ?

8
The Whole System Demonstrator programme
• A DH funded RCT focused on gathering evaluated evidence of telehealth and telecare
• Announced in 2006, designed in 2007, launched in 2008 as a two year study
• Across 3 sites (Newham, Kent & Cornwall), 238 GP practices and over 6,197 people – diabetes, COPD and CHD
• Five themes– Theme 1 - impact on service use– Theme 2 - participant reported outcomes and clinical effectivness– Theme 3 - cost and cost effectiveness– Theme 4 – participant, carer and profesisonal experience– Theme 5 – organisational challenges to adoption
• Evaluation co-ordinated by 6 leading academic institutions
• Different suppliers at each site
• Sites were rural, urban and mixed – so results will translate

9
Hospital use and mortality during trial
Control group (n=1584)
Intervention group (n=1570)
Absolute difference (95% CI)
Percentage difference (95% CI)
Admission proportion (%)
48.2 (n=763) 42.9 (n=674) -5.2 (-8.7 to -1.8) -10.8% (-18.1% to -3.7%)
Mortality (%) 8.3 (n=131) 4.6 (n=72) -3.7 (-5.4 to -2.0) -44.5% (-65.3% to -23.8%)
Emergency admissions per head
0.68 (1.41) 0.54 (1.16) -0.14 (-0.23 to -0.05) -20.6% (-33.8% to -7.4%)
Elective admissions per head
0.49 (1.31) 0.42 (0.99) -0.07 (-0.15 to 0.01) -14.3% (-30.6% to 2.0%)
Outpatient attendances per head
4.68 (6.81) 4.76 (6.74) 0.08 (-0.39 to 0.55) 1.7% (-8.3% to 11.8%)
Emergency department visits per head
0.75 (1.58) 0.64 (1.26) -0.11 (-0.21 to -0.01) -14.7% (28.0% to -1.3%)
Bed days per head 5.68 (15.10) 4.87 (14.35) -0.81 (-1.84 to 0.22) -14.3% (-32.4% to 3.9%)
Tariff cost per head (£)
2448 (4099) 2260 (4117) 188 (-474 to 98.8) -7.7% (-19.4% to 4.0%)
Source: Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial (Steventon A and others) BMJ 2012;344:e3874 doi: 10.1136/bmj.e3874
First paper published 22 June 2012
10
Understanding what WSD tells us
• A better quality of care, lower mortality rates and reduced unplanned hospital admissions are within reach
– mortality by 45%– emergency admissions by 20%– A&E visits by 15%– bed days by 14%– elective admissions by 14%
• Busts the myth of lower quality of life as a result of isolation
• Cost benefits are achievable – we need to get the price point right
• Technology alone does not bring the change – you need service transformation
• Patients on the whole like this type of intervention and age is no barrier
The key is service transformation with technologyNot buying the kit

11
OPPORTUNITY
12
Looking ahead to the future• People will live longer, with more LTCs especially multiple co-morbidities
• More freedom and choice will be the norm
• Today’s teens/twenty-somethings will be tomorrow’s decision makers and healthcare users – they are growing up with technology
• People will want to live their lives as they want, with fewer hospital visits, not tied to clinics of bricks and mortar and will see technology as common place
• Telehealth will play a major role in that future - the question is not ‘if’ it will happen but ‘when’
• In 30 years time we will look back in disbelief at how we use hospital beds

13
Barriers to telehealth
MarketBuilding
QualityStandards
OrganisationalReadiness
Awareness
Levers &IncentivesEvidence
&Business
Case

14
Three Million Lives
• Not a traditional campaign – we are not setting national targets
• Will need a new offer from industry (low capital cost, revenue based with risk share)
• Will mean NHS/social care responding to that offer by building different service models
• Government will need to create the right environment for success
• Will mean growing awareness and support amongst patients & workforce
• This is about transformational change
• One of six high impact innovation changes in Innovation Health & Wealth
Improve 3 million lives within 5 years
www.3millionlives.co.uk

15
Industry Leadership Group
• TSA• ABHI• Intellect• Medilink UK• BT Health• Tunstall• Technology Strategy
Board• Air Products• Harmoni
• Philips• Telehealth Solutions• Bosch• Peaks and Plains Housing
Trust• S3 Group• Cisco• O2 Health• Pfizer• Care Innovations• Circle - Invicta Telecare

16
Roles and Responsibilities
• Government – Create the right environment for delivery – New tariff for assistive technology– Make it a priority in NHS Operating Framework– Delivery linked to CQUIN (IH&W)– “How to Guides” and implementation support (framework contracts, benchmarking for costs) for the
NHS and social care
• Industry– Capital investment & technology roll-out– Partnership development & support– Interoperability solutions & industry code of practice– Patient and Professional awareness & marketing (e.g. media campaign)
• NHS– Scope opportunities for use of assistive technology– Build clinical and operational advocacy– Engage with industry & key local stakeholder groups (including Local Authorities)– Trajectories for roll-out in business planning (2012/13)
Supported by an overarching communications programme

17
Willing to challenge beliefs, values, norms, rules.
Able to develop and share a vision.
Ability to make decisions quickly.
Good project management skills.
Team worker.
Determined & resilient.
Pragmatic.
Empathetic.
We need leaders to make a change

18
LEGACY
19
• People in control of their lives
• More freedom and choice
• People will live their lives as they want, with fewer hospital visits, not tied to clinics of bricks and mortar and technology is common place
• More flexibility for carers
• Better decision making
No doubt in my mind TH/TC will transform healthcareWe can lead or we can follow