
Deferential diagnosis of mesothelial proliferations and neoplasms
32
Deferential Diagnosis of mesothelial proliferations and neoplasms Dr. Svetoslav Bardarov
-
Upload
svetoslav-bardarov -
Category
Healthcare
-
view
648 -
download
0
Transcript of Deferential diagnosis of mesothelial proliferations and neoplasms

Deferential Diagnosis of mesothelial proliferations and
neoplasmsDr. Svetoslav Bardarov

Mesothelium
• Lines the pleural,peritoneal and pericardial cavities
• Composed of monolayer of epithelial-like cells on a thin basal membrane and subserosal connective tissue and blood vessels

Mesothelium- Function
• Thought to provide protective and suportive functions as well as prevent fricton
• It is now recognised to be a dynamic cellular membrane with broad functions:– Fluid transport– Immune and phagocytic functions– Production of extracellular matrix

Mesothelium – Embriology
• Bichart in 1827 observed that the internal organs are lined by a layer of flat cells
• Minot in 1890 proposed the term “mesothelium” after studing its development showed that its is epithelial lining from mesodermal origin.
• Now it is recognised that the intraembrionic mesoderm diferentiates in paraxial, intermediate and lateral mesoderm.
• Between 5-7 weeks the coelom subdivides into future pericardial, peritoneal and pleural cavities.
• Mesothelial cells are primitive mesodermal origin, but share charecteristics of both epithelial and mesechimal cells. ( Whitaker D, Shilkin KB (1992) The pathology of the mesothelium : p25-68)

Mesothelium – Morphology
• Morphology is similar between mamalian species
• The form a monolayer of flat squamoid appearing cells on thin basal membrane
• The average size is about 25µm
• Characteristic surface microvilli
• Well develped tight juctions, gap juctions and desmosomes.



Reactive Mesothelial Hyperplasia
• Trauma ( surgery )
• Infections ( peritonitis, pleuritis, peircarditis)
• Infarctions ( mesentheric thrombosis)
• Collagen vascular diseases
• Carcinomas
• Other



Reactive Mesothelial Hyperplasia

Nuclear Morphometry
• Compare the nuclear diameters of a benign resting mesothelial cell vs reactive vs mesothelioma
• The measurement is done using the commercially available software Adobe Photoshop CS3 Extended edition
• Lymphocytes are used as an internal reference for every case with the asuption that the lymphocyte size is fixed at 7µm

Nuclear MorphometryResting Reactive Malignant
Total Cells 50 (3 cases) 50( 5 cases) 50 (2 cases)
Nuclear diameter 5.8 + 0.7 (7.4) 12.6+ 2.2 31.5 + 7.3
Nucleoli 0 1-3 (cherry red) Variable (irregular)
Nuclear membrane irregularities
present present present
N:C ratio preserved preserved preserved
Bi-nucleation Occasional 2-3/ 10 hpf
Occasional 2-3 / 10 hpf
Often every field
Architecture Mostly single occasional groups
Flat sheets 2D to 3D groups with ~15-20 cells,
Single and 3D groups + many reactive in background
Variability of nuclear size
None ( 2 times lymphocyte)
Present from resting to enlraged 3 times the size of lymphocyte
Marked with size from resting to more than 3 times the size of lymphocyte




60 years old female with ascitesCurrant medical history:60 years old female present to the Cancer Center clinic with abdominalDistension, bloating and “not feeling right”. The has some mild back pain as well.The patient undergoes CT scan which shows multiple loculated areas in the Abdominal cavity as well as ascites.
Past medical history:Total abdominal histerectomy and bilateral salpingo-oopohorectomy for a ovarian serous cystadenoma in 1997.Cholecistectomy 1986.
Family history: UnremarkableSocial history: quit cigarettes 12 years ago.Comprehensive exam and labs: unremarkable
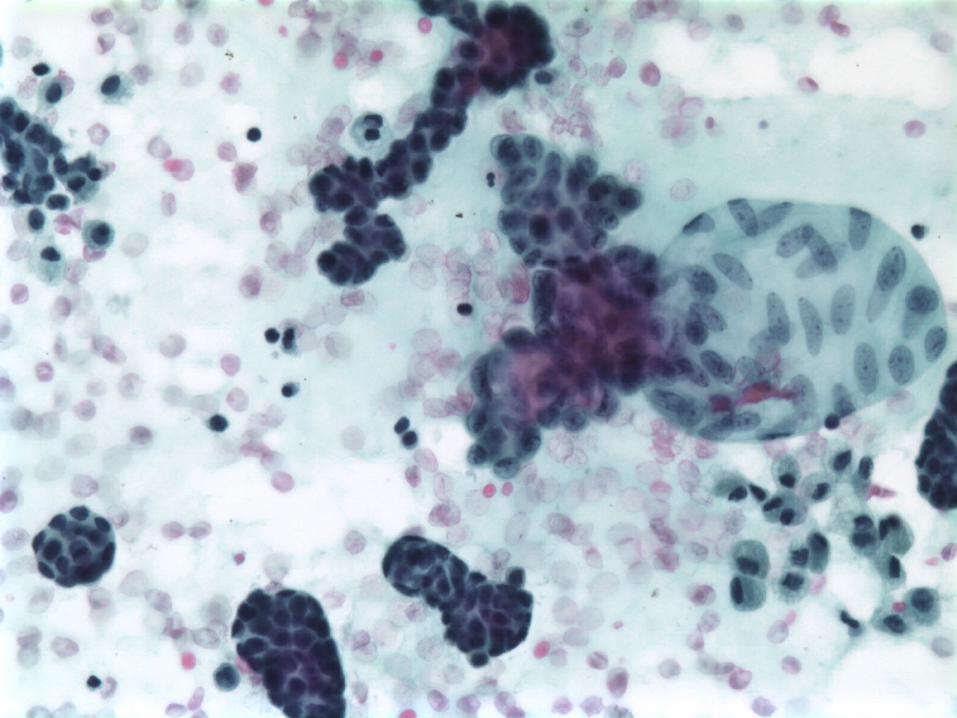
The patient undergoes CT-scan guided drainage of the ascites. The cytopathologyShows reactive mesothelial hyperplasia. Microbiology was also negative.






Differential Diagnosis
• Papillary mesothelial hyperplasia
• Well differentiated papillary mesothelioma of the peritoneal cavity
• Tubulo-papillary Mesothelioma
• Low-grade adenocarcinoma of the peritoneal cavity
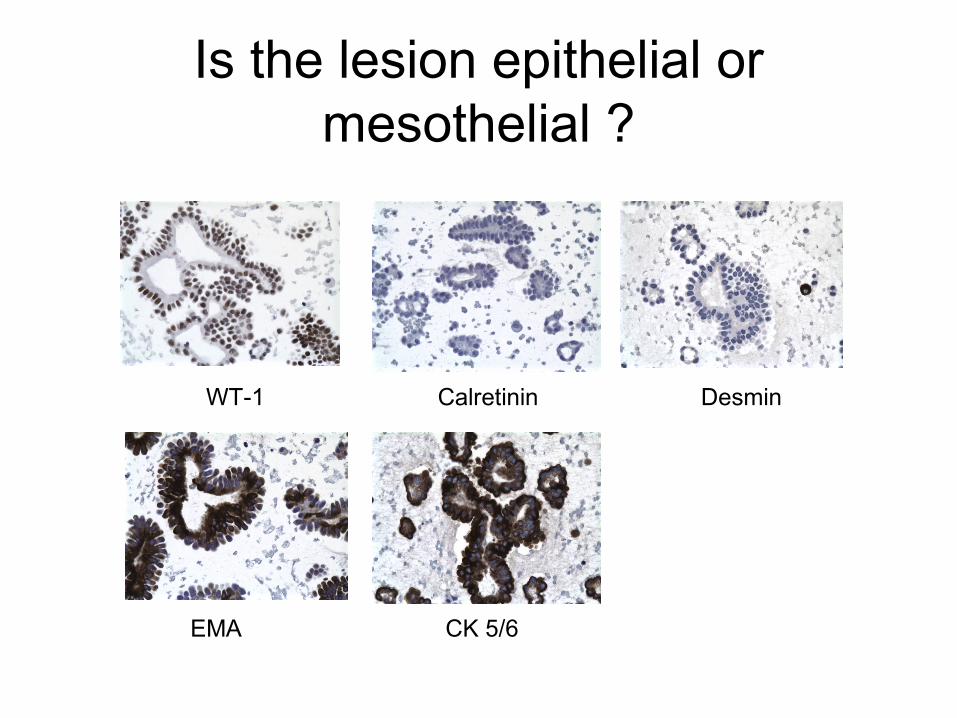
Is the lesion epithelial or mesothelial ?
WT-1 Calretinin Desmin
EMA CK 5/6

Papillary Mesothelial Hyperplasia
In favor of Papillary Mesothelial Hyperplasia
• Groups of cells aranged in groups• Nuclear size similar to that of a lymph• Hypercellular specimen• No-binucleation• No variability in nuclear size
Against Papillary Mesothelial Hyperplasia
• Recurrent ascites• No cause found ( infection etc.)• No single cells in the background
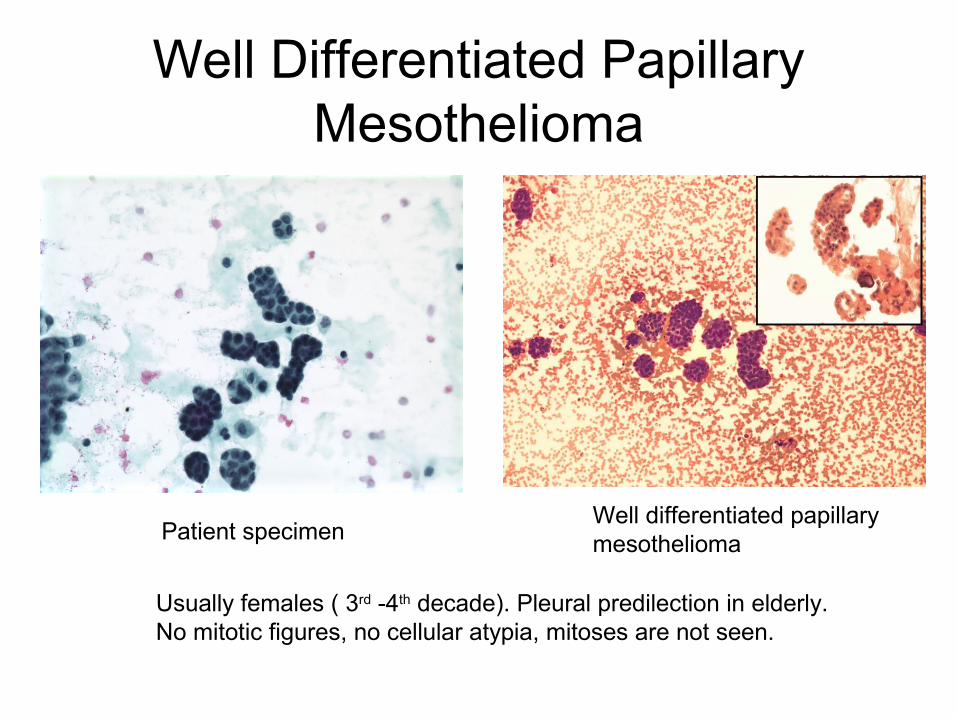
Well Differentiated Papillary Mesothelioma
Patient specimenWell differentiated papillary mesothelioma
Usually females ( 3rd -4th decade). Pleural predilection in elderly. No mitotic figures, no cellular atypia, mitoses are not seen.

Tubulo-papillary Mesothelioma
Patient specimen Tubulo-papillary mesothelioma
Tubulo-papillary mesothelioma is malignant. The patient is still alive > 1 yearafter the onset of the ascites. The patient was not treated but was followed up closely.

Low-grade Serous Papillary Adenocarcinoma of the peritoneum
Patient specimen Low-grade Serous Papillary Adenocarcinoma
Value of estrogen and progesterone receptor immunostaining in distinguishing between peritoneal mesotheliomas
and serous carcinomas.
Ordonez NG.
Reactivity for ER was obtained in:
• 88% of the metastatic serous carcinomas of the ovary • 86% of the primary peritoneal serous carcinomas• 0% epithelioid mesotheliomas • 0% Well-differentiated papillary mesotheliomas• 0% Adenomatoid tumors
It is concluded that, because of its high sensitivity for serous carcinomas, ER immunostaining could be very useful in distinguishing between serous carcinomas and peritoneal mesotheliomas. Immunostaining for PR, however, has little practical utility.
Hum Pathol. 2005 Nov;36(11):1163-7. Epub 2005 Sep 22


Final Diagnosis: Low-grade papillary serous
adenocarcinoma of the peritoneum


















