

Deb Scroggins, M.S.R.S.(CV)(M)(CT) Diagnostic Imaging...
217
4/23/2012 Deb Scroggins, M.S.R.S.(CV)(M)(CT) Diagnostic Imaging Program – Education Coordinator University of Texas M.D. Anderson Cancer Center
Transcript of Deb Scroggins, M.S.R.S.(CV)(M)(CT) Diagnostic Imaging...

4/23/2012
Deb Scroggins, M.S.R.S.(CV)(M)(CT)
Diagnostic Imaging Program –
Education Coordinator
University of Texas M.D. Anderson
Cancer Center

TECHNOLOGIST CENSUS
CV 3,974
VI 1,736
CI 437
MAMMO 48,384
MRI 28,320
CT 48,352
QM 1,485
RAD 296,440
CERTS 468,043 March 2012

VI Exam 2011
2010 2011
Pass % 67.3% 63.7%
Mean score 77.5 76.6
First time 256
Repeat 109
TOTAL 365
Split exam offered for the first time in 2003.

CI Exam 2011
2010 2011
Pass % 73.1% 76.5
Mean score 78.6 78.9
Split Exam offered for first time in 2003

# of CI Examinees in 2011
First-Time 68
Repeat 13
Total 81

VI Exam Performance 2011
Content Categories – Mean Scaled Scores
Content Categories # Questions Score
Equipment/Instrumentation 23 7.7
Patient Care 37 8.0
Vascular-Interventional Procedures
Neurologic 15 7.3
Genitourinary 19 7.3
Gastrointestinal 26 7.5
Peripheral 28 7.7
Thoracic 12 7.6
Total 160 76.6
Pass Rate 63.7%

What about the Cardiovascular-
Interventional Technology Exam (CIT)?
The former CIT exam was available during 2005
only for candidates who did not pass a previous
first attempt and wanted to repeat the exam.
Those already certified in CIT may maintain
registration of that certificate even though the
exam is discontinued.

What do they call us??
R.T. (CV) CIT Exam
R.T. (CI) CI Exam
R.T. (VI) VI Exam
R.T. (CI)(VI) Pass both CI and VI Exams

WHY THE CHANGES IN 2003?
CIT EXAM became CI/ VI Exam in 2003
Split of the CIT Exam into two separate
exams

REASON FOR CHANGES
“New exams will focus on two major categories of
cardiovascular-interventional care.”
One focusing on cardiac care.
One incorporating all other vascular procedures.

4/23/2012
ARRT Exam Update!
“Reflecting the increasing specialization
of RT’s in interventional procedures,
ARRT’s current CIT Exam will soon be
following suit.”
“ It is a sign of the times”

Why did the ARRT discontinue the
CIT Exam?
1 in five vascular techs. are “generalists” performing all procedures to some extent.
1 in five spend virtually all of their time doing cardiac procedures.
Three-fifths of vascular techs. do essentially everything but cardiac.

What if I earned my CV in 2002?
Even after the CV exam is discontinued, ARRT
will continue to renew registration of CV
certificates. You may renew your CV credential
as long as you maintain eligibility.

CLINICAL EXPERIENCE
REQUIREMENTS
“All candidates for the certification in VI or CI
are required to perform certain clinical procedures
to establish eligibility for certification. This
document identifies the minimum core clinical
experience requirements for certification. The
ARRT encourages individuals to obtain education
and experience beyond these minimum
requirements”

Clinical Requirements for
the ARRT VI Registry

Clinical Requirements for the
ARRT VI Registry
The Clinical Experience Requirements for VI consist of 53 procedures in 6 different categories.
The 6 categories include:
A. Neurological
B. Thoracic
C. Genitourinary
D. Gastrointestinal
E. Peripheral
F. Miscellaneous

Clinical Requirements for the
ARRT VI Registry
Candidates must document the performance of complete, diagnostic quality procedures according to the following rules: 1. Choose a minimum of 10 of 53 procedures; more than 10 procedures may be
selected for completion.
2. Each selected procedure must be performed a minimum of 5 times (repetitions) in order for the candidate to receive credit for that procedure.
3. Each procedure may be counted a maximum of 20 times.
4. Each candidate must complete a total of 200 repetitions across all procedures selected for performance.

Clinical Requirements for the
ARRT VI Registry
Example 1
Candidate A: This person identified 10
different procedures from the list on the
following page and performed each of
those procedures 20 times (10 x 20 = 200)

Clinical Requirements for the
ARRT VI Registry
Example 2
Candidate B: This person identified 25
different procedures from the list on the
following page. This applicant performed
15 of those procedures 10 times (15 x 10
= 150), and the other 10 procedures 5
times (10 x 5 = 50)

Clinical Requirements for the
ARRT VI Registry
Example 3
Candidate C: This person identified 40
different procedures from the list on the
following page and performed each of
those procedures 5 times (40 x 5 = 200).

General Clinical Requirements for
the ARRT VI Registry
To qualify as a complete imaging procedure, the
candidate must demonstrate active participation in a
primary role with appropriate:
1. Preparation of supplies and maintenance of
equipment.
2. Evaluation of requisition and patient, patient
preparation, administration of medications as
required.
3. Follow-up patient care.
4. Image processing, including evaluation if images to
ensure they demonstrate correct anatomy,
radiographic techniques, and identification and
labeling.


Verification Identification Page
Verifier’s Initials (handwritten)
Verifying technologist ARRT ID# and
credentials
Printed name
Mailing address (address that ARRT has on file)
City / State / Zip
Verifier’s initials (handwritten)

SUPPORTING CATEGORY FOR CI/VI
EXAMS
Cardiac-Interventional Technology
Radiography
Vascular-Interventional Technology
Radiography

APPLICATION FEES
Application Fee $200
Apply for re-examination $175

APPLICATION PROCESSING
Candidates may have only one application active at any time.
Allow up to four weeks from the date application is received for processing.
ARRT will send you an Candidate Status Report (CSR) when you application has been processed.

CANDIDATE STATUS REPORT
ARRT will mail an Candidate Status Report to
you after your application is processed and
eligibility determined.
Report contains: 1. Candidate identification information
2. Six-digit ARRT ID number
3. Examination window dates

EXAMINATION WINDOW
Exam windows begin on the Wednesday after the
application is processed and extend for 90
calendar days.
Persons who take an examination for ARRT CE
credit need to make sure the exam date occurs
within their assigned CE education biennium!

EXPIRED EXAM WINDOW
After exam window expires, the Candidate Status
Report is no longer valid, and a re-examination
application and fee are required.

CHANGING THE EXAM WINDOW
You may request a new window.
Written request must be made by mail or fax.
Candidates who have an existing appointment must cancel it before requesting a window change, scheduling a new exam date or changing the test center location.
ARRT must receive the written request for a new window on or before the last day of the current exam window.

CHANGING THE EXAM WINDOW
For Late requests (received after the last day of the
current window) or more than three window changes,
the candidate must submit a re-application form and
fee.

TEST CENTERS
ARRT Exams are administered by Pearson VUE Test Centers.
Geographic list of test centers appears in the handbook. Also at: www.pearsonvue.com/arrt
As soon as you receive your CSR, you may schedule your testing appointment.

ADMISSION TO TEST CENTER
You must show two forms of ID, both of which
show your pre-printed name and signature. One
must be a current official government-issued
photo ID. Primary ID:
Government-issued driver’s license
State ID card
Passport

ADMISSION TO TEST CENTER
You must show two forms of ID, both of which show your pre-printed name and signature.
Secondary ID:
Government-issued ID (Social Security Care)
Employee ID or work badge
School ID
Credit Card
Any form of ID on the primary list
ADMISSION TO TEST CENTER
Upon checking in, you will need to provide:
Digital signature
Palms scanned (beginning January 1, 2011, will
have their for identification purposes using palm
vein technology, rather than being fingerprinted).

TIMING OF THE TEST
EXAM TESTING TIME TOTAL TIME
CI 3.0 HOURS 3.5 HOURS
VI 3.25 HOURS 3.75 HOURS
Total column adds 30 min. to allow 20 min. for tutorial and 10 min. for the survey at the end of exam.

PILOT QUESTIONS ON TEST
Pilot questions are unscored questions imbedded in the test.
These questions are not identified as pilot questions and they appear just like any other question on the test.
Up to 25 questions may be unscored pilot questions. Your answers to these questions will not affect test scores.

Equip. & Instrumentation
Patient Care
Cardiac-Interventional Procedures
Diagnostic Cardiac Studies 32
Percutaneous Coronary
Intervention 20
Therapy 4
Hemodynamics and
Calculations 20
Conduction System Studies 4
30
35
80
TOTAL 145
Number of Questions
Content Specifications for CI Exam
Content Category

Equip. & Instrumentation
Patient Care
Vascular-Interventional
Procedures
Neurologic 16
Abdominal 25
GU, GI, non-vascular 15
Peripheral 20
Thoracic 12
Dialysis Management 11
Venous Access 9
24
28
100
TOTAL 160
Number of Questions
July 2012 - Content Specs. for VI
Exam Content Category

Equip. & Instrumentation
Patient Care
Vascular-Interventional
Procedures
Neurologic 15
Genitourinary 19
GI 26
Peripheral 28
Thoracic 12
23
37
100
TOTAL 160
Number of Questions
Content Specifications for VI Exam
Content Category

AMERICAN REGISTRY OF
RADIOLOGIC TECHNOLOGISTS
ARRT
1255 NORTHLAND DRIVE
ST. PAUL, MINNESOTA 55120-1155
TELEPHONE: (651)687-0048
www.arrt.org

What could they ask?
Use the Content Specifications as your guide.
This is the outline for the exam!

What should you study?
ARRT Examination in Cardiovascular
Interventional Technology: New Rudman’s
Questions and Answers on the CIT 2004
www.amzn.com/0837358175
Vascular & Interventional Radiography: A
Comprehensive Text & Examination Review
Book 2008
www.amzn.com/1438221835

How should you study?
1. A quiet place away from distractions such as
music and talking helps with concentration.
2. Group study sessions are valuable but should
be limited to 3-4 persons and should not be the
only study method.

How should you study?
3. Concentrate on a single topic area at one time
(such as procedures-patient care or
instrumentation).
4. Areas of difficulty should be noted for further
study by reading a different textbook, consulting
with an instructor, manager, physician or
attending a review session.

Patient Care Review

Patient Care Consent – The patient is required to provide
informed consent before the start of any invasive
procedure.
“Informed” includes discussing the risks, benefits, and
alternatives in language the patient can fully comprehend.

Patient Care
Implied Consent – occurs when a patient is in need
of immediate medical services but is unconscious or
is physically unable to consent to treatment. In this
case, services are rendered with the assumption that
the patient would consent if able.
A parent or legal guardian must sign the informed
consent form for a minor.

Patient Care Vital sign assessment is the measurement of basic
body functions to monitor critical information
regarding the patient’s physical condition.
Temperature
Heart rate
Blood pressure
Respirations

Vital Signs - Temperature
Body temperature is the physiologic balance between heat
produced in the body tissues and heat lost to the
environment. Body temperature is controlled by the
hypothalamus. Changes in body temp are regulated by:
Environment, time of day, age, weight, physical exercise,
digestion of food, disease, infectious injury

Vital Signs - Temperature Oral Body Temp’s:
Normal temps for an adult are:
37˚ C or 98.6˚F, ±0.5/1˚ is considered normal
Normal temps for children 3m to 3yrs:
37.2˚ C or 99˚ F to 37.7˚ C or 98.6˚ F
Normal temps for children 5yrs to 13yrs:
36.7˚ C or 97.8˚ F to 37˚ C or 98.6˚ F

Vital Signs - Temperature
Pyrexia is the term used when a patient’s body temp is above normal limits.
Hypothermia is a condition where a person’s body temp is below normal limits.

Vital Signs - Temperature
The four areas to measure body temp are:
Oral
Tympanic
Rectal
Axillary
Temperature-sensitive patches are also available that can be placed on the abdomen or forehead.

Pulse (Heart Rate)

Vital Signs - Pulse
As the heart beats, blood is pumped in a pulsating
fashion into the arteries.
The average pulse rate in an adult is b/w 60 and 90
b/min in resting stage.
The average pulse rate for an infant is 120 b/min.
The average pulse rate for a child from 4-10yrs of
age is b/w 90 t0 100 b/min.

Vital Signs - Pulse
Tachycardia is the term used to describe rapid heart
rate (over 100b/min).
Bradycardia- describes slow heart rate (below 60
b/min)
Usually, the pulse rate is rapid if the blood pressure is
low and slower if the blood pressure is high.

Vital Signs - Pulse
The pulse can be detected most easily in the following areas of the body.
Apical pulse- over the apex of the heart with a stethoscope
Radial pulse- over the radial artery on the wrist at the base of the thumb.
Carotid pulse- over carotid artery at the front of the neck.
Femoral pulse- over femoral artery in the groin.

Vital Signs - Pulse
Continued:
Popliteal pulse- at posterior surface of the knee.
Temporal pulse- over the temporal area in front of the ear.
Dorsalis pedis pulse- at the top of the foot in line with the groove between the first and second toe.
Posterior tibial pulse- on inner side of the ankles.
Brachial pulse- in the groove of the biceps and triceps groove above the elbow at anticubital fossa.

Vital Signs – Pulse
A pulse oximeter is an electronic device used to
measure pulse and respiratory status. The pulse
oximeter measures blood oxygen levels , which
are normally between 95% and 100%.

Pulse Oximetry
A photodetector attached to the sensor is able to
distinguish between oxygenated and
deoxygenated hemoglobin of the blood pulsing
through the tissue at the location of the sensor.
Values of less than 85% indicate the tissues are
not receiving adequate oxygen.

Vital Signs - Blood Pressure
The instrument used to measure BP is a
sphygmomanometer.
Blood
Pressure

Blood Pressure
Blood pressure is the amount of blood flow
ejected from the left ventricle of the heart during
systole (contraction) and the amount of resistance
the blood meets due to systemic vascular
resistance.

Vital Signs - Blood Pressure
Systolic- the highest point reached during
contraction of the left ventricle as it pumps blood
into the aorta.
Normal systolic pressure in adults range from 110 to 120
mm Hg.
Systole refers to contraction of the heart muscle
120/80

Vital Signs - Blood Pressure
Diastolic- the lowest point to which the pressure
drops during relaxation of the ventricles.
normal diastolic pressure in adults ranges from 60 to 80
mm Hg.
Diastole refers to relaxation of heart muscle

Vital Signs - Blood Pressure
Hypotensive
A patient is hypotensive
if the systolic blood
pressure is less than
90mm Hg.
Hypertensive
A patient is considered to be
hypertensive if the systolic
blood pressure is greater than
140mm Hg and the diastolic
pressure is consistently
greater than 90mm Hg.

Vital Signs – Blood Pressure
The cardiac cycle refers to the series of blood
flow related events that occur from the beginning
of one heartbeat to that of the next.
It is the frequency of the cardiac cycle that
determines the patient’s heart rate.

Electrocardiogram

Electrocardiograpm
(ECG or EKG)
A graphic representation of the electrical activity of the heart.
Evaluation of the heart rhythm and cycle.
Cardiac cycle can be divided into three distinct stages:

Diagram of ECG Waveform

Stage #1: Atrial depolarization
Contraction of the left and right atria.
Corresponds to the onset of the P wave of the waveform

Stage #2: Ventricular Contraction
Contraction of the left and right ventricles.
Beginning of the QRS complex

Stage #3: Complete cardiac diastole
-Period of relaxation after heart contraction.
-Consists of ventricular diastole and atrial diastole.
-Corresponds to the T- wave

Diastolic Phase
Cardiac CT images are typically reconstructed
from data acquired during the diastolic phase
(resting).
Patients with slower heart rates exhibit longer
diastolic phases, which yield higher-quality
cardiac CT exams.
Beta blockers may be used to reduce heart rate.
65 bpm is the preferred rate for optimal imaging
of the heart.

Vital Signs - Respiration
The average rate of respiration for an adult is 12-20
breaths/min.
The average rate of respiration for an child is 20-30
breaths/min.

Vital Signs - Respiration
Respirations of fewer than 10 breaths/min may
result in cyanosis, apprehension, and a change in
level of consciousness.
When a patient is having difficulty breathing they
are having an episode of “dyspnea”.

Oxygen Delivery
Must be prescribed by a
physician!

Oxygen Delivery
Nasal cannula- disposable plastic device with two hollow
prongs. 1-4 LPM for adults, 1/4-1/2 LPM for children.
Face mask- for short periods of time, no less than 5 LPM.
Tent- used when a need for humidity and higher
concentration is needed.

Patient Care Common lab values for IV contrast:
Blood Urea Nitrogen (BUN)- Used to indicate renal function.
Increase is associated with kidney disease, can be associated with dehydration.
By itself, BUN is not a sufficient indicator of renal insufficiency.
Normal Range is 7-25 (10-22) mg/dl

Patient Care Common lab values for IV contrast:
Creatinine- a measure of the kidney function. High
value indicates renal impairment.
Decreased values are result of pregnancy, minimal
muscle mass, and small stature.
Normal values: 0.6-1.5 mg/dl

Patient Care Common lab values for IV contrast:
Glomerular filtration rate (GFR)
This is a more accurate measure of renal function.
GFR is an approximation of creatinine clearance or the
rate by which creatinine is filtered from the blood
stream.
Patient Care Common lab values for IV contrast:
Glomerular filtration rate (GFR)
GFR – calculated using the patient’s measured serum
creatinine level and takes into account the patient’s:
Age
Sex
Race

Patient Care Common lab values for IV contrast:
Glomerular filtration rate (GFR)
Normal range of GFR is:
70 + 14 mL/min/m for men
60 + 10 mL/min/m for women

Prothrombin Time (PT)
Measures activity of coagulation in plasma.
Protein produced by the liver
Range is 12-15 seconds
PT is measured in the lab after the addition of a protein
called tissue factor to a patient’s blood sample.

Partial Thromboplastin Time (PTT)
This is an additional lab value used to detect abnormalities
in blood clotting.
Time required for clot formation in normal plasma
Normal Range is 25-35 seconds

Platelet Count
This is an additional lab value used to assess the patient’s
clotting ability.
Normal Range is 140,000 to 440,000 per mm of blood

D-dimer
D-dimer testing is utilized for the diagnosis of deep vein thrombosis
(DVT) and pulmonary embolism.
The presence of elevated amounts of D-dimer in the bloodstream may
indicate recently degraded blood clots.
If the D-dimer value is elevated, additional testing such as CT
angiography of the pulmonary arteries may be indicated.


Pharmacology
Anticoagulants: a drug used to help reduce
clotting to reduce the incidence of heart
attack/stroke.
Coumadin (warfarin-generic name)
Should be withheld for several days before invasive
exam.
Commonly used anticoagulant therapy to prevent the
formation of clots in veins and arteries and may
reduce the incidence of heart attack and stroke.

Pharmacology
Anticoagulants: a drug used to help reduce
clotting.
Heparin – should be stopped 2-6 hr. before a
procedure and 1-6 hr. after a study
Acetylsalicylic acid (ASA)(Aspirin)

Pharmacology
Metformin (Glucophage-brand name)
Used to treat type-2 diabetes.
Usually patients are instructed not to take a
metformin product for up to 2-days before and 2-days
following a contrast-enhanced exam.
(small risk of renal impairment from the contrast and reduced renal function can
cause a harmful retention of metformin in the body)

Contrast Agents
Positive contrast agents – radiopaque contrast
media (RCM)
RCM use iodine or barium
The degree of radiopacity of an iodinated or barium
contrast agent is directly proportional to the agent’s
concentration of iodine or barium.

Contrast Agents
There are two types of IV positive contrast agents
available: Ionic and Nonionic.
IV contrast agents are used to highlight any type of
tumor, infection, or abnormality in the body.
Remember contrast causes the area to have a higher
absorption of x-rays (hyperdensity).

Contrast Agents
Negative contrast agents – Air, gases and water
may be used as negative contrast agents:
Water – GI tract
Effervescent granules – Stomach/proximal small
bowel
Air – Enema in large bowel
CO-2 - Colonography

Contrast Media
Ionic Contrast media are salts consisting of sodium and/or meglumine. Each molecule consists of 3-iodine atoms. When injected into the bloodstream, each molecule dissociates into two charged particles (ions)
Cation- positive portion, provides stability, and is radiolucent.
Anion- negative portion, provides stability, and is radiopaque.

Contrast Media
Ionic
Brand Name
Conray
Hypaque
Ionic
Chemical Name
Iothalamate meglumine
Diatrizoate sodium

Patient Care – Contrast Media
Nonionic are non-salt
chemical compounds that
also contain 3 atoms of
iodine per molecule.
They do not dissociate
in solution
Nonionic
Less disruptive to the bbb (fewer reactions)
Hypo-osmolarity
Low-osmolar contrast media (LOCM)

Contrast Media
Continued:
Non-ionic low-osmolar- do not separate into an anion
and cation in the body.
Does not mean that there is no iodine in it.

Contrast Media
Non-ionic
Brand Name
Omnipaque
Isovue
Optiray
Non-ionic
Chemical Name
Iohexol
Iopamidol
Ioversol

Contrast Media
Non-ionic
Mg/ml
Omnipaque 300
Omnipaque 350
Optiray 240
Optiray 320
Non-ionic
Iodine Content
30%
35%
24%
32%

Iso-osmolar Contrast media (IOCM)
3rd type
Have the same osmolality as blood and therefore
may offer improved patient comfort and reduced
potential for side effects.
Visipaque (Iodixanol) is an example of a non-
ionic iso-osmolar contrast agent.

Properties of Contrast Agents
Osmolality- number of particles per kilogram of
solution.
Most important factor in determining discomfort and
vasodilation.
Osmolarity- number of particles per liter of solution.
Ionics are about 6-8 times as osmolar than blood plasma.
Nonionics are about 2-3 times as osmolar than blood plasma

Properties of Contrast Media
Continued:
Viscosity- the degree of stickiness or thickness of the
solution.
Strength- relates to iodine concentration; provides
opacity. Iodine is considered slightly more radiopaque
than lead.
Toxicity- the degree that the contrast agent is toxic or
noxious.
Miscibility- contrast must be solvent with blood to
thwart embolization.

Special Considerations
For patients who are given an iodinated contrast
agent attention should be paid to the 4-H’s:
History
Hydration
Have equipment and expertise ready.
Heads up!

Special Considerations
Possible contraindications to IV iodinated
contrast agents include:
Allergy to iodine
Prior severe allergic reaction to an iodinated contrast
agent
Renal insufficiency/failure

Reaction List
Mild Reactions
Nausea/vomiting
Mild urticaria
Sensation of feeling warm
Altered tase
Sweats/chills
Nasal stuffiness/sneezing
anxiety
Moderate Reactions
Mild bronchospasm
Moderate to severe
urticaria
Vasovagal response
Tachycardia from
hypotension

Reaction List Severe Reactions
Profound hypotension
Laryngeal edema
Severe bronchospasm
Pulmonary edema
Cardiac arrhythmia
Seizure
Cardiopulmonary arrest
Death

Management of acute reactions to
contrast media
Urticaria
Facial or Laryngeal Edema
Bronchospasm
Hypotension with Tachycardia
Hypotension with Bradycardia (Vagal Reaction)
Hypertension
Seizures or Convulsions
Pulmonary Edema

Venipuncture
Parenteral administration – injection directly into
the
bloodstream

Common sites used for IV injection
-Antecubital space
-Radial aspect of wrist
-Posterior portion of hand
-Anterior surface of forearm

Venipuncture Aseptic technique – To reduce infection
Thorough hand washing
between patients
- Wear disposable gloves
- Clean site of puncture in
circular motion
- Gentle pressure with
alcohol swab upon
removal

Patient Care Shock is the interruption of blood flow to vital
organs or a lack of the ability of tissues to use
oxygen and nutrients needed.
It affects all ages.
Caused by injury, disease or emotional trauma.

Patient Care Symptoms include:
Decreased blood pressure
Weak pulse
Increased heart rate
Shallow respiration
Cyanosis
Skin pallor
Restlessness
Confusion
Anxiety

Patient Care
Types of shock:
Hypovolemic- loss of blood.
Septic- microorganisms in the blood.
Anaphylactic –allergic reaction
Cardiogenic – failure of the heart to pump an
adequate amount of blood to the vital organs

Patient Care
Two major complications that can occur during a VI
procedure:
Anaphylactic shock- allergic reaction
Vasovagal reaction-stimulation of the vagus nerve (10th).

Patient Care
Anaphylactic Shock
Most common in VI as a reaction to contrast
Causes a release of histamines and causes contraction of smooth muscles specifically in the respiratory tract causing respiratory failure or even death.
Symptoms include tightness in the chest, itching, urticaria, choking, wheezing, increased heart rate.
Drug of choice: epinephrine (bronchodialator).

Patient Care Vasovagal reaction
Results from the stimulation of the vagus nerve (10th
cranial nerve) causing severe slowing of the heart, which
usually causes a sudden loss of consciousness from a
decreased cardiac output.
Can be triggered by pain, fright, trauma
Drug of choice is atropine, it increases the heart rate.
DIFFERENTIAL SYMPTOM IS HEART RATE!!!!!

Patient Care Other situations:
Diabetes- disorder of carb’s, fat, and protein metabolism, which affects the structure and function of blood vessels. It causes the pancreas to produce less insulin than necessary or the amount produced does not have the desired effect.
Hypoglycemia- insulin reaction; excess amount of insulin in the bloodstream or inadequate food intake to use the insulin.

4/23/2012
CIRCULATORY
SYSTEM REVIEW

BLOOD FLOW
THROUGH HEART:
Pulmonary Circulation
Systemic Circulation

SVC/IVC
Right Atrium
Right Ventricle
Pulmonary Artery
Pulmonary Vein
Left Atrium
Left Ventricle
Aorta
Arteries
Veins

4/23/2012
CEREBRAL VESSELS

Arch and the 3 main
branches:
Brachiocephalic
Left Common
Carotid
Left Subclavian

ARCH AND THE 3 MAIN
BRANCHES
1. Brachiocephalic Artery
2. Left Common Carotid
3. Left Subclavian



CIRCLE OF WILLIS
Anterior cerebral
Anterior communicating
Middle cerebral
Posterior cerebral
Internal carotid
Posterior communicating

CIRCLE OF WILLIS

Common Carotid
Injection
Internal carotid
Supplies the anterior
brain, orbital and
nasal regions and
face

Common Carotid
Injection
External carotids
Supply the exterior
head, face, meninges,
and neck
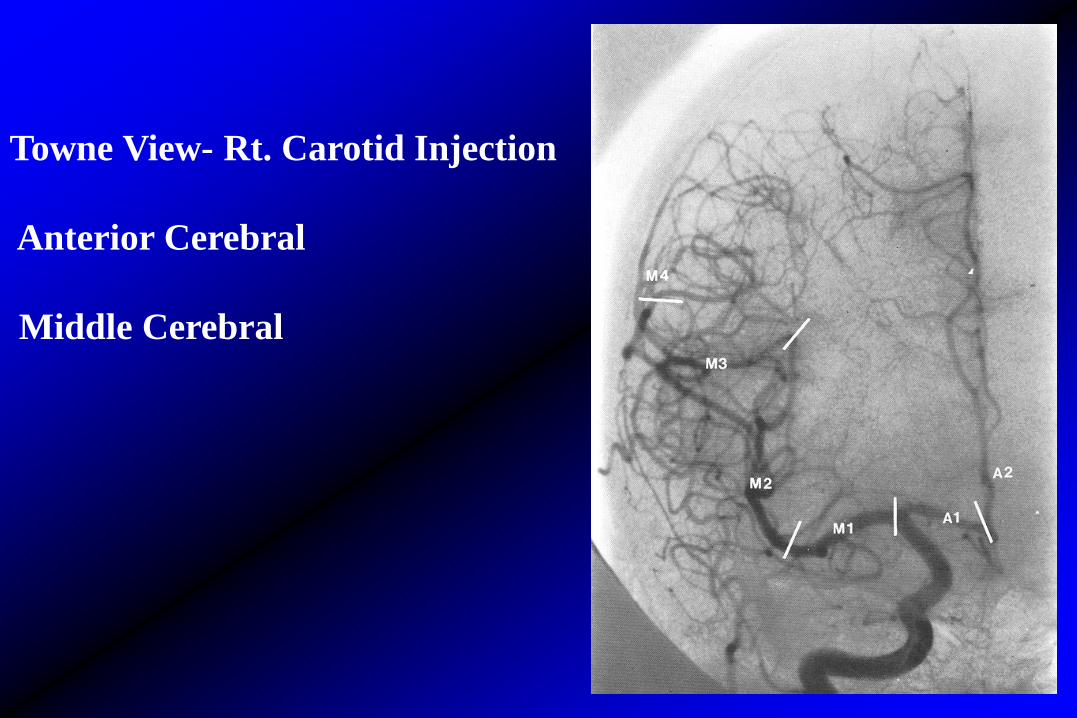
Towne View- Rt. Carotid Injection
Anterior Cerebral
Middle Cerebral

Lateral Rt.
Carotid
Injection

SYLVIAN TRIANGLE
Loops of branches
of Middle Cerebral
Artery

Towne View - Rt. Vertebral Artery Injection

Lateral Vertebral Artery Injection

4/23/2012
ABDOMEN VESSELS

Celiac Artery
Common Hepatic Artery
Left Gastric Artery
Splenic Artery
Superior Mesenteric Artery
Renals
Inferior Mesenteric Artery

CT Angiogram of Abdominal Aorta

Other
Abdominal
Arteries

Selective Celiac Arteriogram

Selective SMA Arteriogram
J- Jejunal
I – Ileal
IC - Ileocolic
RC – Right colic
MC – Middle colic

Flush Aortagram for Renals

Selective IMA Arteriogram
LC – Left colic
S – Sigmoid
SH – Superior rectal

IVC
The major vein in the
abdomen that is
responsible for
bringing the blood
back to the heart.

4/23/2012
PELVIS VESSELS

Arteries of the Pelvis
Aorta bifurcates – L4
Rt & Lt common iliac

Common Femoral Artery
Superficial femoral artery
Profunda femoral (Deep
femoral artery)

4/23/2012
EXTREMITY VESSELS

Superficial Femoral and
Popliteal Arteries
LFC - Lat. Fem. Circumflex
PF - Profunda Femoris
Mbr - Muscular branch of SF

Normal AP distal lower extremity arteriogram
ar - Arcuate
AT - Anterior Tibial
P - Popliteal
Pe – Peroneal- branch of PT
PT - Posterior Tibial
s - Sural

Lateral distal leg arteriogram
AT - Anterior Tibial
DP - Dorsalis Pedis
Pe- Peroneal
PT - Posterior Tibial

4/23/2012
QUESTIONS AND
COMMENTS

SAMPLE TEST QUESTIONS
The resolution of a computerized or digital image can be improved by increasing which of the following?
1. Pixel size
2. Matrix size
3. Area of the x-ray beam
A. 1 only
B. 2 only
C. 3 only
D. 1 and 3

SAMPLE TEST QUESTIONS
The resolution of a computerized or digital image can be improved by increasing which of the following?
1. Pixel size
2. Matrix size
3. Area of the x-ray beam
A. 1 only
*B. 2 only
C. 3 only
D. 1 and 3

A
B
C
D
E F
G

What structure is “B” pointing to on
the image below?
A SVC
B IVC
C Thoracic aorta
D Abdominal aorta B
A
C

What structure is “B” pointing to on
the image below?
A SVC
*B IVC
C Thoracic aorta
D Abdominal aorta B
C
A

The special anastomosis of the cerebral vessels that
permit collateral circulation of a vessel blockage is
which of the following?
A. Carotid sinus
B. Carotid siphon
C. Genu
D. Circle of Willis

The special anastomosis of the cerebral vessels that
permit collateral circulation of a vessel blockage is
which of the following?
A. Carotid sinus
B. Carotid siphon
C. Genu
D. *Circle of Willis

Swelling at or above the puncture site during or
after the injection is an indication of which of the
following?
A. Urticaria
B. Dyspnea
C. Extravasation
D. Thrombus formation

Swelling at or above the puncture site during or
after the injection is an indication of which of the
following?
A. Urticaria
B. Dyspnea
C. *Extravasation
D. Thrombus formation

As the iodine concentration ________ the viscosity
of the substance will _________.
A. Increases, decrease
B. Increases, increase
C. Decreases, increase
D. Decreases, remain unchanged

As the iodine concentration ________ the viscosity
of the substance will _________.
A. Increases, decrease
B. *Increases, increase
C. Decreases, increase
D. Decreases, remain unchanged

Conscious sedation is achieved by administrating a
combination of which of the following medications?
A. Versed and midazolam
B. Versed and Sublimaze
C. Fentanyl and lidocaine
D. Lidocaine and Versed

Conscious sedation is achieved by administrating a
combination of which of the following medications?
A. Versed and midazolam
B. *Versed and Sublimaze
C. Fentanyl and lidocaine
D. Lidocaine and Versed

All of the following are catheter types used for
pulmonary angiography except?
A. Berman balloon flotation
B. Swan-Ganz
C. Grollmen
D. Miller-Levine

All of the following are catheter types used for
pulmonary angiography except?
A. Berman balloon flotation
B. Swan-Ganz
C. Grollmen
D. *Miller-Levine

Which of the following organs is not supplied by
the celiac trunk?
A. esophagus
B. liver
C. kidney
D. pancreas

Which of the following organs is not supplied by
the celiac trunk?
A. esophagus
B. liver
C. *kidney
D. pancreas

The renal arteries normally branch off from the
aorta at the level of which of the following?
A. T11-T12
B. L1-L2
C. L2-L3
D. L4-L5

The renal arteries normally branch off from the
aorta at the level of which of the following?
A. T11-T12
B. *L1-L2
C. L2-L3
D. L4-L5
If the proximal portion of the subclavian artery is
stenosed, the subclavian artery may “steal” blood
from which artery?
A. Vertebral
B. Carotid
C. Braciocephalic
D. Axillary

If the proximal portion of the subclavian artery is
stenosed, the subclavian artery may “steal” blood
from which artery?
A. *Vertebral
B. Carotid
C. Braciocephalic
D. Axillary

Which of the following contrast media volumes
would be appropriate for a selective cerebral
angiogram?
A. 4 – 6 mL/sec for 8 to 10 mL total volume
B. 10 – 20 mL/sec for 20 to 40 mL total volume
C. 15 – 30 mL/sec for 30 to 60 mL total volume
D. 30 – 40 mL/sec for 60 to 80 mL total volume

Which of the following contrast media volumes
would be appropriate for a selective cerebral
angiogram?
A. *4 – 6 mL/sec for 8 to 10 mL total volume
B. 10 – 20 mL/sec for 20 to 40 mL total volume
C. 15 – 30 mL/sec for 30 to 60 mL total volume
D. 30 – 40 mL/sec for 60 to 80 mL total volume

Cysts visualize during what phase of a renal
angiogram?
A. Arterial
B. Nephrogram
C. Venous
D. None of the above

Cysts visualize during what phase of a renal
angiogram?
A. Arterial
B. *Nephrogram
C. Venous
D. None of the above
The nephrogram phase best demonstrates the outline
of the kidney as well as the renal hilum.

What artery supplies blood to the rectosigmoid
area?
A. SMA
B. IMA
C. Left gastric
D. Spenic

What artery supplies blood to the rectosigmoid
area?
A. SMA
B. *IMA
C. Left gastric
D. Spenic

At what level of the aorta does the celiac axis arise?
A. T11
B. T12
C. L1
D. L2

At what level of the aorta does the celiac axis arise?
A. T11
B. *T12
C. L1
D. L2

In order to demonstrate anterior and middle cerebral
circulation, what exam is performed?
A. Carotid arteriogram
B. Vertebral arteriogram
C. Aortic arch arteriogram
D. None of the above

In order to demonstrate anterior and middle cerebral
circulation, what exam is performed?
A. *Carotid arteriogram
B. Vertebral arteriogram
C. Aortic arch arteriogram
D. None of the above

At what level of the spine does the common carotid artery
bifurcate into internal and external carotid arteries?
A. C2
B. C4
C. C6
D. T1

At what level of the spine does the common carotid artery
bifurcate into internal and external carotid arteries?
A. C2
B. *C4
C. C6
D. T1

Which of the following defines a potentially life-
threatening condition in which disruption of the intima
permits blood to enter the wall of the aorta and separate its
layers?
A. Saccular aneurysm
B. Fusiform aneurysm
C. Congenital coarctation
D. Dissection of the aorta

Which of the following defines a potentially life-
threatening condition in which disruption of the intima
permits blood to enter the wall of the aorta and separate its
layers?
A. Saccular aneurysm
B. Fusiform aneurysm
C. Congenital coarctation
D. *Dissection of the aorta
The principle advantage of using a
heparin coated guidewire is which of
following?
A. Improved flexibility
B. Reduced internal friction
C. Reduced thrombogenicity
D. Improved torqability

The principle advantage of using a
heparin coated guidewire is which of
following?
A. Improved flexibility
B. Reduced internal friction
C. *Reduced thrombogenicity
D. Improved torqability

The effective half-life of heparin is about
A. 30 minutes
B. 90 minutes
C. 2 days
D. 5 days

The effective half-life of heparin is about
A. 30 minutes
B. *90 minutes
C. 2 days
D. 5 days
Heparin 90 minutes PTT
Coumadin (warfarin sodium) days PT

Which of the following neurologic pathologies
would necessitate a longer imaging time?
A. AVM and increased intracranial pressure
B. AVM and arterial spasm
C. Increased intracranial pressure and
arterial spasm
D. AVM, increased intracranial pressure and
arterial spasm

Which of the following neurologic pathologies
would necessitate a longer imaging time?
A. AVM and increased intracranial pressure
B. AVM and arterial spasm
C. *Increased intracranial pressure and
arterial spasm
D. AVM, increased intracranial pressure and
arterial spasm

A serious cardiac arrhythmia that is
characterized by a rapid, ineffective
contraction is termed?
A. Hypertrophy
B. Hypotrophy
C. Fibrillation
D. Premature atrial contraction

A serious cardiac arrhythmia that is
characterized by a rapid, ineffective
contraction is termed?
A. Hypertrophy
B. Hypotrophy
C. *Fibrillation
D. Premature atrial contraction

When a patient presents with labored or
difficulty breathing which term would
best describe the condition?
A. Epistaxis
B. Diaphoresis
C. Eclampsia
D. Dyspnea

When a patient presents with labored or
difficulty breathing which term would
best describe the condition?
A. Epistaxis
B. Diaphoresis
C. Eclampsia
D. *Dyspnea

When the clinical diagnosis is amaurosis
fugax, injection would occur in which
vessel?
A. Splenic artery
B. Carotid artery
C. Pudendal artery
D. Vertebral artery

When the clinical diagnosis is amaurosis
fugax, injection would occur in which
vessel?
A. Splenic artery
B. *Carotid artery
C. Pudendal artery
D. Vertebral artery

The procedure indicated for the control of
gastrointestional hemorrhage, hormonally
active tumors, trauma, and AVM would
be which of the following?
A. Vascular stenting
B. Balloon angioplasty
C. Embolization
D. Thrombolysis
E. Two of the above are correct.

The procedure indicated for the control of
gastrointestional hemorrhage, hormonally
active tumors, trauma, and AVM would
be which of the following?
A. Vascular stenting
B. Balloon angioplasty
C. *Embolization
D. Thrombolysis
E. Two of the above are correct.
Which of the following describes the
pulmonary circulation?
A. Right ventricle to lungs to left atrium.
B. Right ventricle to lungs to right atrium.
C. Right ventricle to lungs to left ventricle.
D. Left ventricle to lungs to right atrium.

Which of the following describes the
pulmonary circulation?
A. *Right ventricle to lungs to left atrium.
B. Right ventricle to lungs to right atrium.
C. Right ventricle to lungs to left ventricle.
D. Left ventricle to lungs to right atrium.

Fibromuscular dysplasia is primarily a
disease found in which of the following
groups of people?
A. Young African-American females
B. Young Caucasian females
C. Young African-American males
D. Young Caucasian males

Fibromuscular dysplasia is primarily a
disease found in which of the following
groups of people?
A. Young African-American females
B. *Young Caucasian females
C. Young African-American males
D. Young Caucasian males
Accounts for 20-50% of renal hypertension in young caucasian females

What vein is formed by the junction of the common
illiacs?
A. Superior vena cava
B. Inferior vena cava
C. Inferior mesenteric vein
D. Superior mesenteric vein

What vein is formed by the junction of the common
illiacs?
A. Superior vena cava
B. *Inferior vena cava
C. Inferior mesenteric vein
D. Superior mesenteric vein

Which of the following calculates left ventricular stroke
volume?
A. End systolic volume minus end diastolic
volume x heart rate
B. End diastolic volume minus end systolic
volume x heart rate
C. End systolic volume divided by end diastolic
volume x heart rate
D. End diastolic volume divided by end systolic volume +
heart rate

Which of the following calculates left ventricular stroke
volume?
A. End systolic volume minus end diastolic
volume x heart rate
B. *End diastolic volume minus end systolic
volume x heart rate
C. End systolic volume divided by end diastolic
volume x heart rate
D. End diastolic volume divided by end systolic volume +
heart rate

Which laboratory study has a normal value of
0.6 - 1.5 mg/dl?
A. Hematocrit
B. Creatinine
C. Blood urea nitrogen
D. Bilirubin

Which laboratory study has a normal value of
0.6 - 1.5 mg/dl?
A. Hematocrit
B. *Creatinine
C. Blood urea nitrogen
D. Bilirubin
BUN – 7 – 22 mg/dL (blood chemistry)
Hematocrit – 37 – 49% (coagulation profile)

In most patients the celiac artery presents as a
trifurcation of which of the following arteries?
A. Right gastric, left gastric, hepatic
B. Left gastric, hepatic, right colic
C. Left gastric, hepatic, splenic
D. Right gastric, pancreatoduodenal, splenic

In most patients the celiac artery presents as a
trifurcation of which of the following arteries?
A. Right gastric, left gastric, hepatic
B. Left gastric, hepatic, right colic
C. *Left gastric, hepatic, splenic
D. Right gastric, pancreatoduodenal, splenic

Which valve is situated between the left atrium
and the left ventricle?
A. Pulmonic valve
B. Aortic valve
C. Mitral valve
D. Tricuspid valve

Which valve is situated between the left atrium
and the left ventricle?
A. Pulmonic valve
B. Aortic valve
C. *Mitral valve (bicuspid)
D. Tricuspid valve

Which of the following indicates normal right
ventricular pressure?
A. 25 mm Hg to 30 mm Hg systolic
B. 30 mm Hg to 60 mm Hg systolic
C. 90 mm Hg to 150 mm Hg systolic
D. None of the above are correct ranges.

Which of the following indicates normal right
ventricular pressure?
A. * 25 mm Hg to 30 mm Hg systolic
B. 30 mm Hg to 60 mm Hg systolic
C. 90 mm Hg to 150 mm Hg systolic
D. None of the above are correct ranges.
Left ventricle pressure 120 – 130 systolic


















